Embed Size (px)
Citation preview

Archives of the Balkan Medical UnionCopyright © 2017 Balkan Medical Union
vol. 52, no. 2, pp. 221-224June 2017
INTRODUCTION
Described for the first time by John Kelso Ormond in 1948, idiopathic retroperitoneal fibrosis usually involves Gerota’s fascia and compresses the
ureters leading to the apparition of progressive lum-bar pain and urinary dysfunction inducing various degrees of renal failure1. In certain cases, other organ might be affected inducing a different clinical aspect, in the absence of urinary tract involvement signs.
RÉSUMÉ
Un cas rare de cholécystite aigue et d’obstruction des voies biliaires du à la maladie d’Ormond- rapport de cas et revue de la littérature
La fibrose rétropéritonéale idiopathique, également connue sous le nom de maladie d’Ormond, com-prime généralement les structures rétropéritonéales, en particulier les urètres. Dans de rares cas, d’autres structures telles que le système biliaire peuvent être impliquées. Nous rapportons le cas d’un patient de 49 ans diagnostiqué avec la maladie d’Ormond deux ans auparavant, qui a développé une jaunisse et une cholé-cystite aiguë en raison de la progression de la fibrose rétropéritonéale.
Mots-clés: fibrose rétropéritonéale idiopathique, l’obstruction des voies biliaires, la cholécystite aiguë
ABSTRACT
Idiopathic retroperitoneal fibrosis, also known under the name of Ormond’s disease usually compresses the retroperitoneal structures, especially the ureters. In rare cases other structures such as the biliary system can be involved. We report the case of a 49-year-old patient diagnosed with Ormond’s disease two years be-fore, who developed jaundice and acute cholecystitis due to the progression of the retroperitoneal fibrosis.
Keywords: idiopathic retroperitoneal fibrosis, com-mon bile duct obstruction, acute cholecystitis.
CASE REPORT AND MINIREVIEW
A RARE CASE OF ACUTE CHOLECYSTITIS AND COMMON BILE DUCT OBSTRUCTION DUE TO ORMOND’S DISEASE – A CASE REPORT AND LITERATURE MINI REVIEW
Nicolae Bacalbașa1, Irina Bălescu2, Iulian Brezean1
1 „Ion Cantacuzino“ Clinical Hospital, “Carol Davila“ University of Medicine and Pharmacy, Bucharest, Romania2 „Ponderas“ Academic Hospital, Bucharest, Romania
Corresponding author: Nicolae Bacalbașa
Dimitrie Racoviță Street, no. 2, Bucharest, Romania. Tel.: +40 723540426, e-mail:

A rare case of acute cholecystitis and common bile duct obstruction due to Ormond’s disease – BACALBAȘA et al
222 / vol. 52, no. 2
For example, retroperitoneal fibrosis might affect the common biliary duct, inducing the appearance of jaundice or unexplained elevated serum hepatic enzymes in association with significant biliary duct enlargement. In the meantime, the presence of jaun-dice and cholestasis in the absence of upper abdomi-nal pain is usually significantly suggestive for malig-nancy. Most often performing preoperative studies such as magnetic resonance imaging or endoscopic retrograde cholangiopancreatography usually pro-vides a good orientation of the diagnosis. However, in certain cases this fact is not possible, imposing the necessity of surgery2-4.
Extensive primary retroperitoneal fibrosis, also known as Ormond’s disease is most often character-ized by the involvement of perirenal tissues although mesenteric and biliary system involvement has been reported so far in extremely rare situations5,6.
Its pathogenesis is not fully understood, various hypothesis such as immunologic mechanisms being suspected so far5.
CASE REPORT
A 47-year-old patient with medical past history of diabetes presented for diffuse abdominal pain, weight loss and nausea and was diagnosed after performing a computed tomography with a large retroperitoneal tumor measuring 54x47x84 mm developed in the mesenteric root, rounding the abdominal aorta and inferior vena cava. The patient was submitted to sur-gery, at that moment a biopsy being performed. The histopathological studies revealed the presence of an idiopathic diffuse retroperitoneal fibrosis (Ormond’s disease) with fibro-inflammatory elements. The im-munohistochemical studies revealed the diffuse posi-tivity of actin, cluster designation (CD) 68, CD 34 (at the level of the blood vessels) and the negativity of ALK1, AE1-AE3 while Ki67 proved to be positive in up to 5% of the tumoral cells. Postoperatively the patient was submitted to adjuvant chemotherapy with six series of ifosfamide, dacarbazine and epirubicin. Two years later the patient presented for upper ab-dominal pain, jaundice and nausea. The computed tomography revealed the presence of a large retrop-eritoneal mass measuring 146/65/73 mm invading the abdominal aorta and compressing the common bile duct, inducing an intrahepatic biliary ducts dila-tation; in the meantime the gallbladder presented diffuse thickened walls with local signs of acute lithi-asic cholecystitis. The patient was referred to surgery; intraoperatively a typical aspect of acute lithiasic pyocholecystitis and common bile duct lithiasis was found so cholecystectomy and Kehr drainage were performed. The postoperative course was uneventful
the patient being discharged in the fifth postopera-tive day.
DISCUSSION
The definitive cause of Ormond’s disease is not well established so far, although autoimmune and immunological disorders have been incriminated. Most authors sustain the hypothesis of the presence of antibodies against ceroid, although other causes such as medication (hydralazine, bromocriptine, methysergide, beta-blockers), malignant processes (carcinoids, lymphomas, sarcomas, breast, colorectal or bladder carcinomas), radiation therapy, surgery for aortic aneurysms or infections (tuberculosis) have been cited so far6-8.
Most of the cases are diagnosed due to the pres-ence of direct and indirect signs of ureteral compres-sion, although other structures such as nerves, blood vessels or bile ducts might be affected. According to Ormond’s theory, the course of the disease includes the onset of the process followed by fibrosis of the retroperitoneal tissues and contracture of the fibrous mass inducing compression of the affected structures. More recent studies sustain the influence of immu-noglobulin G4 (IgG4) producing plasma cells which induce tumor swelling of certain viscera and different degrees of fibrosis9. As a consequence, the tumefac-tion of the involved organ might appear which leads to its destruction.
Biliary obstruction due to Ormond’s disease has been reported for the first time in 1964; from that moment, fourteen cases have been reported so far. Eleven cases were submitted to surgery while the other three cases have been managed conservatively. However, biopsy should be always performed in order to differentiate the benign subtype from the malig-nant one. Malignant proliferation has been reported in up to 8% of cases10.
The goals of therapeutic strategy in Ormond’s disease consist in relieving the obstruction, stop the progression of the disease and prevent the recurrence.
The main therapeutic options consist in stent placement or other surgical procedures in order to relieve the compressed structures followed by medical treatment based on corticosteroids and immunosup-pressive agents in order to prevent the evolution of the disease11. In cases presenting secondary retrop-eritoneal fibrosis, the treatment is addressed to the cause which has led to this pathology while in cases with idiopathic fibrosis prednisolone has been re-ported as the first intention therapy. In case of inad-equate response, azathioprine, methotrexate, rituxi-mab or mycophenolate mofetil may be added while other authors sustain the benefits of tamoxifen’s

Archives of the Balkan Medical Union
June 2017 / 223
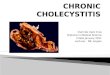
Figure 1. The aspect of retrograde dissection of the gallbladder
Figure 3. Releasing lithiasic material from the common bile duct
Figure 2. The aspect after cholecystectomy – retroperitoneal fibrosis and common bile duct dilatation
Figure 4. Placing a Kehr’s tube

A rare case of acute cholecystitis and common bile duct obstruction due to Ormond’s disease – BACALBAȘA et al
224 / vol. 52, no. 2
administration as first line therapy12. The effect of tamoxifen in Ormond’s disease is related to the in-hibition of fibroblast proliferation and angiogenesis; however, this action proved to be efficient especially in non-malignant conditions. In von Bommel’s study published in 2006 which included 19 cases with non-malignant Ormond’s disease administration of tamoxifen (20 mg twice daily) significantly improved the outcomes13.
CONCLUSION
Ormond’s disease is a very rare entity indu cing retroperitoneal fibrosis which usually affects the ureters. However, in certain cases other structures such as the common bile duct might be affected. In these cases severe modifications such as common bile duct stenosis, lithiasis and acute cholecystitis might be observed. In order to provide a good outcome of these cases, biliary duct decompression followed by systemic therapy should be taken into consideration.
Acknowledgement: This work was supported by a grant from the Romanian National Authority for Scientific Research and Innovation, CNCS – UEFISCDI, project number PN-II-RU-TE-2014-4-2533.
REFERENCES
1. William Haubrich. Ormond of Ormond’s Disease. Gastroenterology, 2007;132(3):838.
2. Cohen S, Bacon BR, Berlin JA et al. National Institutes of Health State-of-the-Science Conference Statement: ERCP for diagnosis and therapy. Gastrointest Endosc 2002; 56: 803-9.
3. Hunerbein M, Stroszczynski C, Ulmer C, Handke T, Felix R, Schlag PM. Prospective comparison of transcutaneous 3-dimensional US cholangiography, magnetic resonance cholangiography, and direct cholangiography in the evalu-ation of malignant biliary obstruction. Gastrointest Endosc 2003; 58: 853-8.
4. Holstege A, Zolinski P, Woidy L, Permanetter W. The pa-tient with unexplained elevated serum liver enzymes. Best Pract Res Clin Gastroenterol 2007; 21: 535-50.
5. Khalil F, Ouslim H, Mhanna T, Barki A. Extensive primary retroperitoneal fibrosis (Ormond’s disease) with common bile duct and ureteral obstruction: a rare case report. Int J Surg Case Rep 2015; 13: 5-7.
6. Vega J, Goecke H, Tapia H, Labarca E, Santamarina M, Martinez G. Treatment of idiopathic retroperitoneal fibrosis with colchicine and steroids: a case series. Am J Kidney Dis 2009; 53: 628-37.
7. Zhao MF, Tian Y, Guo KJ, Ma ZG, Liao HH. Common bile duct obstruction due to fibrous pseudotumor of pancreas associated with retroperitoneal fibrosis: a case report. World J Gastroenterol 2004; 10: 3078-9.
8. Fairweather J and Jawad ASM. Ormond disease: an old dis-ease with a new name. Grand Rounds Vol 14 pages L1–L3. Specialities: Landmark case report. 2014 e-MED Ltd.
9. Zen Y, Sawazaki A, Miyayama S, Notsumata K, Tanaka N, Nakanuma Y. A case of retroperitoneal and mediastinal fibrosis exhibiting elevated levels of IgG4 in the absence of sclerosing pancreatitis (autoimmune pancreatitis). Hum Pathol 2006; 37: 239-43.
10. Tamura S, Yokoyama Y, Nakajo K, Morita T, Wada K, Onishi S. A rare case of idiopathic retroperitoneal fibrosis involving obstruction of the mesenteric arteries, duodenum, common bile duct, and inferior vena cava. Intern Med 2003; 42: 812-7.
11. Matthew Smith B and Grove D. Obstructive jaundice sec-ondary to retroperitoneal fibrosis: long term nonsurgical management resulting in regression of obstruction. AJG 95 (9), 2000.
12. Stone JH, Zen Y, Deshpande V. IgG4-related disease. N Engl J Med 2012; 366: 539-51.
13. van Bommel EF, Hendriksz TR, Huiskes AW, Zeegers AG. Brief communication: tamoxifen therapy for nonmalignant retroperitoneal fibrosis. Ann Intern Med 2006; 144: 101-6.