Embed Size (px)
Citation preview
Genaitourin Med 1994;70:40-45
A prospective study of the psychological impacton patients with a first episode of genital herpes
Orla Carney, Emma Ross, Chris Bunker, George Ikkos, Adrian Mindel
The AcademicDepartment ofGenitourinaryMedicine, UniversityCollege and MiddlesexSchool ofMedicine,James Pringle House,The MiddlesexHospital, LondonW1N 8AA0 CarneyE RossA MindelDepartment ofPsychiatry, MiddlesexHospital, LondonG IkkosDepartment ofDermatology,Middlesex Hospital,LondonC BunkerAddress correspondence to:Professor A Mindel,Academic Unit of SexualHealth Medicine, SydneyHospital, GPO Box 1614,Sydney 2001, Australia.Accepted for publication13 October 1993
AbstractObjectives-To assess the psychologicalimpact of first episode of genital herpes,and to determine whether this changesover time.Setting and subjects-The Departmentsof Genitourinary Medicine (GUM), andDermatology, Middlesex HospitalLondon. The study group consisted ofpatients attending the department ofGUM with a clinically proven firstepisode of genital herpes. Two controlgroups were recruited; firstly patientswithout herpes attending the GUMDepartment and secondly patientsattending the Dermatology Departmentout patients with chronic dermatoses.Methods-Patients and controls com-pleted an 87 item, self-adinisteredpsychological questionnaire at 3 monthlyintervals for a year. The questionnaireconsisted of the General HealthQuestionnaire (GHQ); the HospitalAnxiety and Depression Questionnaire(HADQ); Illness Attitude Scales andIllness Concern. Patients were alsoasked questions about their sexualbehaviour.Results-Ninety one patients (68 women,23 men) with genital herpes, 61 GUMcontrols (42 women, 19 men) and 56dermatology controls (36 women, 20men) participated. There were no statis-tically significant demographic differ-ences between patients and controls. Atfirst visit the proportion of patients clas-sified as "cases" by the GHQ (GHQcases) were similar for primary herpespatients 62% (56191) and Dermatologycontrols 52% (29156) while a significantlysmaller proportion ofGUM controls 34%(21161) were classified as GHQ cases. Theprimary herpes group were significantlymore concerned about their illness thaneither the GUM controls or theDermatology controls (p < 0.002). Theproportion of primary herpes patientsclassified as "cases" by the GHQreduced significantly over the initialthree month period with 67% of patientsclassified as "cases" at their first visitbecoming "noncases" after three months(p < 0.0001). Also 50% of those classifiedas "cases" at first visit by the HADQbecame "noncases" after the initial threemonths (p = 0.007). The illness concernscores also decreased significantly fromvisit one to visit two (means 14.7 vs. 12.3;p < 00001).
Conclusion-The diagnosis of a firstepisode of genital herpes has a profoundemotional effect on patients. If they donot have recurrent episodes, their emo-tional state improves. For those who dohave recurrences, the level of anxiety andconcern remains as high as at the time oftheir first diagnosis. Clinicians must besensitive to the emotional impact such adiagnosis may bring.
(Genitourin Med 1994;70:40-45)
IntroductionGenital herpes is a common sexually trans-mitted infection. It is often recurrent andsometimes painful. Primary infections can beacute and debilitating, causing systemic ill-ness as well as severe genital disease.Recurrent infection varies in frequency andseverity, however, both primary and recurrentepisodes are self limiting and cause no physi-cal sequelae. There is, however, a wealth ofresearch to suggest that there is a psychologi-cal morbidity associated with genital her-pes.'-7 In 1981 Luby and Gillespiel describeda syndrome, akin to Kubler-Ross' stages ofbereavement that patients may experiencewhen they realise that they have genitalherpes: denial, belief that there is a cure,realisation that they have herpes, loneliness,anger towards sexual partners, fear of sexualdeprivation, and development of poor selfimage.
However, a mythology seems to haveevolved around affect and recurrences,namely that negative mood directly reacti-vates the virus. Consequently, most previouswork has concentrated on the cause andeffect of recurrent infection. In one study,participants were asked to keep prospectivediaries of stressful events, and to monitortheir recurrence rate. They were then askedafter the event what they felt had caused reac-tivation of the virus. "Retrospective reportsalmost unanimously identified stressful ante-cedents of herpes reactivation, yet concurrentassessment failed to confirm this".3 AsKemeney et al have said "the associationfound between depressive mood and herpesrecurrences may be attributable to the feelingof depression that results from having a highrate of recurrences".4 One may surmise that,because of the capricious nature of the infec-tion, such retrospective reasoning resultsfrom an attempt to have some control, albeittenuous, over the virus.
Little work has been done on what impact
40
on 28 July 2018 by guest. Protected by copyright.
http://sti.bmj.com
/G
enitourin Med: first published as 10.1136/sti.70.1.40 on 1 F
ebruary 1994. Dow
nloaded from
A prospective study of the psychological impact on patients with a first episode ofgenital herpes
the first episode of herpes has on the individ-ual. It is not therefore known whether there ispsychological morbidity associated with a firstepisode that is absent in the case of other sex-ually transmitted infections. If such a morbid-ity were found to exist it might alter overtime, or be dependent on whether the patienthas recurrences or not. Conversely, such amorbidity might be used as a predictor for thephysical pattern of the disease, if as is sug-gested by Goldmeier et al,7-9 the emotionalstate of the patient helps to trigger recur-rences.We therefore designed a study with the fol-
lowing aims: (1) To assess the psychologicalmorbidity of patients with a first episode ofgenital herpes infection, (2) To monitorwhether this changes over time, (3) To assesswhether subsequent episodes had any bearingon adjustiment to the illness.
MethodsBetween March 1988 and October 1990, allpatients who presented with a first episode ofgenital herpes to the department ofGenitourinary Medicine of the MiddlesexHospital, London, were invited to take part inthe study at their follow up visit, 7-10 daysafter initial presentation. This was to ensurethat the diagnosis had been confirmed andfully discussed with the patient according toclinic protocol.
There were two control groups: (1) Newpatients of the same sex presenting to theGUM department on the same day as theindex case, but who did not have herpes(GUM controls), (2) Patients with chronicdermatoses attending as out-patients atthe Middlesex Hospital (dermatology con-trols).The former group was included because
previous studies have suggested that there is ahigher psychiatric morbidity in patientsattending genitourinary clinics than in thegeneral population.1014 Because there is alsowork to suggest that there is a psychologicalmorbidity associated with both chronic ill-ness, and skin disorders,15-21 a second controlgroup was included, which was comprised ofpatients of roughly the same age as thoseattending the GUM clinic, who had achronic, recurrent, but not sexually transmit-ted, disorder. Informed consent was obtainedfrom all participants.
QuestionnaireParticipants were asked to complete an 80item, self administered questionnaire, dividedinto four sections, each consisting of a wellestablished psychological questionnaire: (1)General Health Questionnaire (GHQ) (30items), (2) Hospital Anxiety and Depression(HAD) (14 items), (3) Illness Attitude Scales(IAS) (27 items), (4) Illness concern (nineitems).The GHQ measures non psychotic psychi-
atric illness. In this, responses are onlycounted as being present if the patient con-siders that they represent a deviation from
their own norm. The 30 item inventory wasused, and "caseness" was defined as a scoreof five or more in keeping with previousstudies.2223 However, some of the responsesmay be influenced by concurrent physical ill-ness. To control for this we also used theHAD inventory.2425 This is said to be unbi-ased by coexisting physical illness, since itavoids questions which may have a somaticcause. Case definition is taken as a score ofeight or more on either of the anxiety ordepression subscales. For the purposes ofanalysis, GHQ and HAD scores were treatedas dichotomous variables (case or non case)using the cut-off points described above.The IAS measure fears, beliefs and atti-
tudes associated with hypochondriasis andabnormal illness behaviour. Characteristics ofother psychiatric syndromes are excluded.26There are nine scales, each consisting of threequestions. The IAS is scored from 0-12.
Conversely, illness concern assesses theactual and potential emotional impact causedby the specific problem which has broughtthem to the clinic, and scores range from2-27.
Seven questions were also asked, aboutsexual orientation, numbers of sexual part-ners, and frequency and enjoyment of sex.
In addition, those with herpes were askedquestions on their basic knowledge of thevirus. The rationale for this was to ascertainwhether misconceptions about genital herpeswould lead to increased anxiety, compared tothose who were more informed about thesubject. Patients and controls were asked torepeat the questionnaire at three monthlyintervals for a year.
AnalysisPoor follow-up rates meant that statisticalcomparisons were confined to the assess-ments of the three groups at their first visit(to establish whether primary HSV has a sub-stantial effect on patients) and to the first twoassessments (to establish whether there wereany changes in the outlook of these patientsbetween their initial visit and their first 3month follow-up attendance).
Within the primary HSV group, patientswho had recurrences at visit two were com-pared with those who did not have recur-rences to establish whether recurrences werean influential factor in determining thepatients psychological state.
Analysis of variance (ANOVA) was used totest for any difference in the age distributionsof the groups of patients, and the Chi squaretest was used to test for evidence of an associ-ation between the dichotomous variables("case"/"non-case") and patient group. Thedistributions of the data for the three groupswere compared using the Kruskal-WallisANOVA by ranks.27 Comparison of these dis-tributions in any two groups were made usingthe Mann--Whitney U statistic. To investigateany difference in patients attitudes from visitone to visit two McNemar's test for changesin proportion and Wilcoxon's test for com-paring scores were applied.27
41
on 28 July 2018 by guest. Protected by copyright.
http://sti.bmj.com
/G
enitourin Med: first published as 10.1136/sti.70.1.40 on 1 F
ebruary 1994. Dow
nloaded from
Carney, Ross, Bunker, Ikkos, Mindel
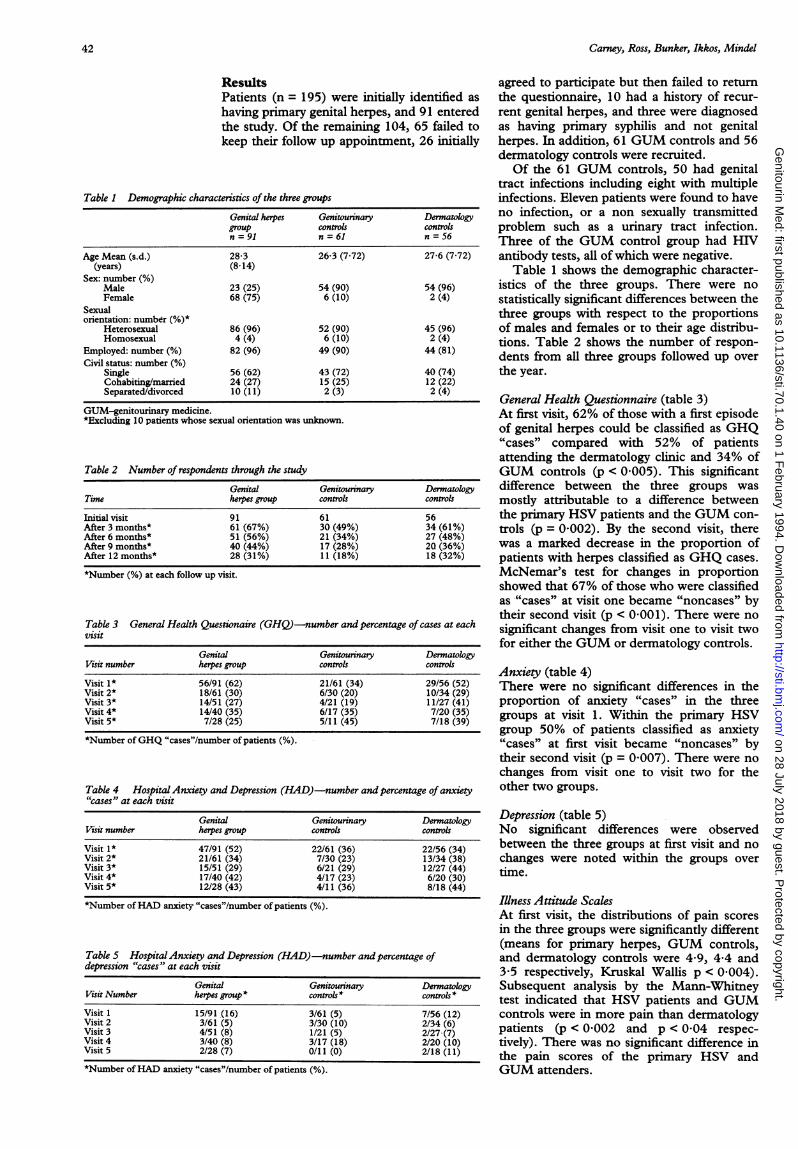
ResultsPatients (n = 195) were initially identified ashaving primary genital herpes, and 91 enteredthe study. Of the remaining 104, 65 failed tokeep their follow up appointment, 26 initially
Table 1 Demographic characteristics of the three groups
Genital hres Genitounnary Denmatologygroup controls controlsn = 91 n = 61 n = 56
Age Mean (s.d.) 28-3 26-3 (7.72) 27-6 (7.72)(years) (8.14)
Sex: number (%)Male 23 (25) 54 (90) 54 (96)Female 68 (75) 6 (10) 2 (4)
Sexualorientation: number (%)*
Heterosexual 86 (96) 52 (90) 45 (96)Homosexual 4 (4) 6 (10) 2 (4)
Employed: number (%) 82 (96) 49 (90) 44 (81)Civil status: number (%)
Single 56 (62) 43 (72) 40 (74)Cohabiting/married 24 (27) 15 (25) 12 (22)Separated/divorced 10 (11) 2 (3) 2 (4)
GUM-genitourinary medicine.*Excluding 10 patients whose sexual orientation was unknown.
Table 2 Number of respondents through the study
Genital Genitourinary DermatologyTime herpes group controls controls
Initial visit 91 61 56After 3 months* 61 (67%) 30 (49%) 34 (61%)After 6 months* 51 (56%) 21 (34%) 27 (48%)After 9 months* 40 (44%) 17 (28%) 20 (36%)After 12 months* 28 (31%) 11 (18%) 18 (32%)
*Number (%) at each follow up visit.
Table 3 General Health Quesiionaire (GHQ)--number and percentage of cases at eachvisit
Genital Genitourinary DermatologyVisit number herpes group controls controls
Visit 1* 56/91 (62) 21/61 (34) 29/56 (52)Visit 2* 18/61 (30) 6/30 (20) 10/34 (29)Visit 3* 14/51 (27) 4/21 (19) 11/27 (41)Visit 4* 14/40 (35) 6/17 (35) 7/20 (35)Visit 5* 7/28 (25) 5/11 (45) 7/18 (39)
*Number ofGHQ "cases"/number of patients (%).
Table 4 HospitalAnxiety and Depression (HAD)-number and percentage of anxiety"cases" at each visit
Genital Genitourinary DermatologyVisit number herpes group controls controls
Visit 1* 47/91 (52) 22/61 (36) 22/56 (34)Visit 2* 21/61 (34) 7/30 (23) 13/34 (38)Visit 3* 15/51 (29) 6/21 (29) 12/27 (44)Visit 4* 17/40 (42) 4/17 (23) 6/20 (30)Visit 5* 12/28 (43) 4/11 (36) 8/18 (44)
*Number ofHAD anxiety "cases"/number of patients (%).
Table 5 HospitalAnxiety and Depression (HAD)-number andpercentage ofdepression "cases" at each visit
Genital Genitourinary DermatologyVisit Number herpes group* controls * controls*
Visit 1 15/91 (16) 3/61 (5) 7/56 (12)Visit 2 3/61 (5) 3/30 (10) 2/34 (6)Visit 3 4/51 (8) 1/21 (5) 2/27 (7)Visit 4 3/40 (8) 3/17 (18) 2/20 (10)Visit 5 2/28 (7) 0/11 (0) 2/18 (11)
*Number ofHAD anxiety "cases"/number of patients (%).
agreed to participate but then failed to returnthe questionnaire, 10 had a history of recur-rent genital herpes, and three were diagnosedas having primary syphilis and not genitalherpes. In addition, 61 GUM controls and 56dermatology controls were recruited.Of the 61 GUM controls, 50 had genital
tract infections including eight with multipleinfections. Eleven patients were found to haveno infection, or a non sexually transmittedproblem such as a urinary tract infection.Three of the GUM control group had HIVantibody tests, all of which were negative.
Table 1 shows the demographic character-istics of the three groups. There were nostatistically significant differences between thethree groups with respect to the proportionsof males and females or to their age distribu-tions. Table 2 shows the number of respon-dents from all three groups followed up overthe year.
General Health Questionnaire (table 3)At first visit, 62% of those with a first episodeof genital herpes could be classified as GHQ"cases" compared with 52% of patientsattending the dermatology clinic and 34% ofGUM controls (p < 0.005). This significantdifference between the three groups wasmostly attributable to a difference betweenthe primary HSV patients and the GUM con-trols (p = 0.002). By the second visit, therewas a marked decrease in the proportion ofpatients with herpes classified as GHQ cases.McNemar's test for changes in proportionshowed that 67% of those who were classifiedas "cases"Y at visit one became "noncases" bytheir second visit (p < 0.001). There were nosignificant changes from visit one to visit twofor either the GUM or dermatology controls.
Anxiety (table 4)There were no significant differences in theproportion of anxiety "cases" in the threegroups at visit 1. Within the primary HSVgroup 50% of patients classified as anxiety"cases" at first visit became "noncases" bytheir second visit (p = 0 007). There were nochanges from visit one to visit two for theother two groups.
Depression (table 5)No significant differences were observedbetween the three groups at first visit and nochanges were noted within the groups overtime.
Illness Attitude ScalesAt first visit, the distributions of pain scoresin the three groups were significantly different(means for primary herpes, GUM controls,and dermatology controls were 4*9, 4-4 and3.5 respectively, Kruskal Wallis p < 0 004).Subsequent analysis by the Mann-Whitneytest indicated that HSV patients and GUM-controls were in more pain than dermatologypatients (p < 0.002 and p < 0.04 respec-tively). There was no significant difference inthe pain scores of the primary HSV andGUM attenders.
42
on 28 July 2018 by guest. Protected by copyright.
http://sti.bmj.com
/G
enitourin Med: first published as 10.1136/sti.70.1.40 on 1 F
ebruary 1994. Dow
nloaded from

43A prospective study of the psychological impact on patients with a first episode ofgenital herpes
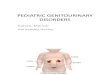
Figure 1 Mean illnessconcern at each visitcomparing patients withprimary genital herpes,genitourinary controls, andpatents with chronicdermatoses. All threegroups showed a decreasein Illness Concern, but thisdecrease was onlysignificantly different in theherpes group (p < 0-0001comparing visits 1 and 2).
0)0Coca)
cJ0C.00(D
on
a,
Mean Illness Concern Scores at Each Visit one (mean 12-3 vs 15.8, p = 0-0003).16 <McNemar's test showed a change in the pro-
E g---Primary HSV portion of GHQ cases with 73% who were14 --o-- GUM Controls initially classified as "cases" being classified
- DermatologY as "noncases" three months later (p <0.0001). The same pattern was observed
12_ | amongst anxiety "cases" with 55% of those
classified as "cases", at visit one becoming'"noncases" at visit two (p = 0-006). Those
8 - *. - - patients who did have recurrences remaineda as concerned at visit two as at visit one, and
61 , , there were no significant changes in the pro-12 3 4 5 portion defined as cases at either visit (13/26
Visit number (50%) at visit one vs 11/26 (31%) at visittwo). Taking all 60 primary herpes patientswho were followed up to visit two, 58%
With respect to their treatment experiencethe three g~ps were also different (meansfor primary HSV, GUM control', and derma-tology controls were 4-9, 5-8, and 6-4respectively Kruskal Wallis p = 0-0001).The Mann-Whitney test suggested thedermatology group scored significantly higherthan the primary HSV patients (p < 00001)and the GUM controls scoring higher thanthe patients with primary HSV (p = 0-013).The dermatology patients scored higher thanGUM patients (p = 0-033).From visit one to visit two there was no
statistically significant change in the scoreswithin each of the three groups.
Illness Concern (figure)At first visit there was a statistically ssignificantdifference between the scores of'the threegroups (means for primary HSV, GUMcontrols, dermatology controls' were 14-4,10-4, and 10-9 respectively Kruskal Wallisp < 0-0001). Subsequent Mann-Whitneytests indicated that the primary ,HSV groupwere more concerned about .t,heir illnessthan either GUM controls or dermatologypatients (p < 0-0001, p < 0-002, respec-tively). Primary HSV patients jbecame lessconcemed at visit two compared ,o visit one(mean 12-3 vs 14-7; p < 0-0001).
Sexual behaviourNo statistically significant diffexences werefound between the study group anid. the con-trols with respect to the quality ox frequencyof their sexual intercourse.
Herpes knowledgeNo association was found betwe,en herpesknowledge scores and scores in other. sectionsof the questionnaire. However, women didscore consistently higher than men.
Recurrences of herpesOf the 61 herpes patients who completed.' thesecond questionnaire 26 (six male, 20 female)had had at least one recurrence, whilst'34(nine male, 25 female) had none. Data were-missing on one female patient. ,Selectmingthose patients Wvho had no recurren:cewitiinthe first- three months, and comparing theirscores at visit one and visit two, the Wilcoxontest showed their Illness Concern scores to'be,significantly lower at visit two thaniat'tvisit'
(15/26) of those known to have had recur-rences were defined to be GHQ cases at visitone versus 76% (26/34) of those who did notexperience recurrences. The respective fig-ures for ANX cases were 50% (13/26) versus59% (20/34). At visit two, 38% (10/26) ofthose with recurrences were defined as GHQcases versus 24% (8/34) of those with norecurrences. The figures for ANX cases atvisit two were 42% (11/26) and 29% (10/34)respectively (p > 0-2 in each case).
DiscussionThe majority of previous studies on the psy-chological impact of genital herpes have con-centrated on the cause and effect of recurrentinfection. Little has been written on the psy-chological morbidity of those who presentwith a first episode of genital herpes, or onwhether this has any bearing on the subse-quent disease pattern, and vice versa.Previous studies have suggested that thosewith a high GHQ score at the time of theirfirst episode are likely to experience recur-rences sooner than those with low scores(7-9), the suggestion being that the patient'semotional state has a direct impact on reacti-vation of the virus. However, our study sug-gests that, whilst 62% of patients with genitalherpes could be classified as GHQ "cases" atthe time of the first episode only those withrecurrences tended to continue as "cases",whilst those who did not experience recur-rences were likely to become "noncases".This same pattern was seen amongst anxiety"cases", and in a decrease in their IllnessConcern scores from visit one to visit two.
However, our study does not allow directcomparison with the studies mentionedabove,7-9 because it was designed very differ-ently. Goldmeier et al in 19889 studied allgenital herpes patients presenting to an STDclinic. Fifty seven patients with first episodegenital herpes were compared with 50patients with frequently recurring herpes.GHQ scores were statistically higher in thosewho presented with recurrent genital herpes.Our study took only first episode -genital her-pes and assessed them as recurrent or nonrecurrent at their second visit (three monthsafter entry). It may be that patients withmany recurrences have more psychologicalm'orbidity than those presenting with the first
1
1
1
1
on 28 July 2018 by guest. Protected by copyright.
http://sti.bmj.com
/G
enitourin Med: first published as 10.1136/sti.70.1.40 on 1 F
ebruary 1994. Dow
nloaded from

Carney, Ross, Bunker, Ikkos, Mindel
episode. Goldmeier and Johnson7 analysedthe role of recurrences in primary HSVpatients by survival analysis, looking atwhether it was higher in patients with preex-isting psychiatric illness. They were able to dothis as they took the date of the primaryattack to the date a patient presented with arecurrent episode within 30 weeks of theirdate of entry. Patients who did not presentwere assumed to have had no recurrences.Our patients, however, were requested toreturn every 3 months and complete a ques-tionnaire, whether or not they had symptoms,and recurrences were therefore all noted atthe same time points. The conclusionreached by Goldmeier and Johnson was thatrecurrence rates in those with GHQ scores> 12 were higher than in those with scores< 11. Poor follow up in our study did notallow for a similar assessment.
It would seem from the results in the pre-sent study that a first episode of genital her-pes does place a severe emotional burden onpatients, but that this may lessen over time ifthey do not experience recurrences. However,with only 50% of patients initially diagnosedas primary genital herpes entering the study,patient self selection may have influenced theresults, and generalisations to the majority ofpatients with herpes should be made withcaution.At first visit we would have expected to
find more acute anxiety and depression, asdesignated by the HAD questionnaire.However, with the high scores at first visit forIllness Concern, it would seem that it is geni-tal herpes which is the focus of their emo-tional concerns. Given that Illness Concernalso measures potential worries regardingtheir illness, and for those who do not haveany recurrences within the first three monthstheir scores drop, we could extrapolate that itis the physical reality of the actual blisters andsores which causes emotional problems.
Basic knowledge about the virus did notseem to be associated with low scores on anysection of the questionnaire or identificationas a "case"5 on the GHQ or HAD question-naire, reiterating the adage that health educa-tion does not necessarily lead to behaviouralor attitudinal change.What is also interesting is that, as a group,
those with a first episode of genital herpeswould seem to have a higher incidence of psy-chiatric morbidity than other patients attend-ing a genitourinary clinic for the first time,and those with chronic dermatoses attendingas dermatology out-patients on a regularbasis. Previous studies have shown that30-40% of GUM attenders can be classifiedas GHQ "cases"." 12 This compares with 34%in our study population. Using the HADinventory, Barczak et a124 found the preva-lence of psychiatric disorder within the GUMclinic to be 31%, whereas we found it to beapproximately 36%, suggesting that this con-trol group was similar to those in previousstudies. It is rather those with a first episodeof herpes who seemed to have a higher psy-chiatric morbidity (62% classified as GHQ
cases and 52% as HAD anxiety cases) thanthe already high morbidity of those attendingGUM clinics.Much work on emotional problems relat-
ing to skin disorders has been anecdotal, sug-gesting that those who have dermatologicalproblems have high levels of anxiety, guiltand shame, and lack self confidence.'7Wessely and Lewis found that, using the 12item inventory, 42.7% of dermatologypatients could be classified as GHQ "cases". 7This compares with 52% (29/56) at first visit,which fell to 39% (7/18) at final visit, in thepresent study population. In 1983, Hughes eta120 found that using the 30 item GHQ inven-tory, 30% of dermatology out patients couldbe classified as GHQ "cases". In addition,those who had visible skin lesions, on handsor the face, were found to have higher scoresthan those with less visible conditions. Thislast-point is interesting, given the intimatenature of the majority of genital herpeslesions.We would suggest that we cannot deter-
mine who will have recurrences from theirpsychological profile at first visit. Recurrencesmay be independent of mood per se, but inthemselves can have a damaging effect on theindividual's well-being. The severity of prob-lem specific scores compared with those ofthe two control groups, and the lower scoresfor general states would seem to underlinethis and appropriate counselling shouldalways be considered.
Clinicians need to acknowledge that notonly may patients with a first episode of geni-tal herpes be experiencing an acute and debil-itating physical illness, but also that itsdiagnosis may precipitate further emotionalreactions.
1 Luby ED, Gillespie 0. Psychological responses to genitalherpes. Helper 1981;3:2-3.
2 Manne S, Sandler I. Coping and adjustment to genitalherpes. JBehav Med 1984;7:391-410.
3 Vanderplate C, Aral S. Psychosocial aspects of genitalherpes virus infection. Health Psychol 1987;6:57-72.
4 Kemeny M, Cohen F, Zegans L, Conant M.Psychological and immunological predictors of genitalherpes recurrence. Psychosom Med 1989;51:195-208.
5 Luby E, Klinge V. Genital herpes: a pervasive psycho-social disorder. Arch Dermatol 1985;121:494-7.
6 Rand K, Hoon EF, Massey JK, Johnson JH. Daily stressand recurrence of genital herpes simplex. Arch InternMed 1990;150:1889-93.
7 Goldmeier D, Johnson A. Does psychiatric illness affectthe recurrence rate of genital herpes? Br 7 Venereal Dis1982;58:40-3.
8 Goldmeier D, Johnson A, Jeffries D, Walker GD,Underhill G, Robinson G, Ribbans H. Psychologicalaspects of recurrences of genital herpes. Jf Psychosom Res1986;30:601-8.
9 Goldmeier D, Johnson A, Byrne M, Barton S.Psychosocial implications of recurrent genital herpessimplex virus infection. Genitourin Med 1988;64:327-30.
10 Wells BWP. Personality study of VD patients. Br JfVenereal Dis 1970;46:498-501.
11 Pedder JR, Goldberg DP. A survey by questionnaire ofpsychiatric disturbance in patients attending a venerealdisease clinic. BrJ Venereal Dis 1970;40:56-61.
12 Mayou R. Psychological morbidity in a clinic for sexuallytransmitted disease. BrJ Venereal Dis 1975;51:57-60.
13 Catalan J, Bradley M, Gallwey J, Hawton K. Sexual dys-function and psychiatric morbidity in patients attendinga clinic for sexually transmitted diseases. BrJ Psychiatry1981;138:292-6.
14 Fulford WM, Catterall RD, Hoinville E, Lim KS, WilsonD. Social and psychological factors in the distribution ofSTD in male clinic attenders. Br J Venereal Dis 1983;59:381-5.
44
on 28 July 2018 by guest. Protected by copyright.
http://sti.bmj.com
/G
enitourin Med: first published as 10.1136/sti.70.1.40 on 1 F
ebruary 1994. Dow
nloaded from

A prospective study of the psychological impact on patients with a first episode ofgenital herpes
15 Wessely SC, Lewis GH. The classification of psychiatricmorbidity in attenders at a dermatology clinic. Br JfPsychiary 1989;155:686-91.
16 Logan RA. Self help groups for patients with chronic skindiseases. BrJDernatol 1988;118:505-8.
17 Cotterill JA. Psychiatry and the skin. Br Jf Hosp Med1989;42:401-4.
18 Beaman K, Luzzatto P. Psychological approaches to thetreatment of skin dcleases. Nursing 1988;29:1061-3.
19 Hardy GE, CotterTl JA. A study of depression andobessionality in dysmorphophobic and psoriaticpatients. BrJ'Psychiatry 1982;140:19-22.
20 Hughes JE, Barraclough BM, Hamblin LG, White JE.Psychiatric symptoms in dermatology patients. BrPsychiatry 1983;143:51-4.
21 Bombardier CH, D'Amico C, Jordan JS. The relationshipof appraisal and coping to chronic illness adjustment.
Behav Res Ther 1990;28:297-304.22 Goldberg DP. The detection ofpsychiatrc illness by question-
naire. Maudsley Monographs (OUP) 1972; No. 21.23 Benjamin S, Decalmer P, Haran D. Community screening
for mental illness: a validity study of the general healthquestionnaire. BrJ' Psychiatry 1982;140:174-80.
24 Barczak P, Kane N, Andrews S, Congdon AM, Clay JC,
Betts T. Patterns of psychiatric morbidity in a genito-urinary clinic. BrJ Psychiatry 1988;152:698-700.
25 Lewis G, Wessely S. Comparison of the general healthquestionnaire and the hospital anxiety and depressionscale. BrJlPsychiatry 1990;157:860-4.
26 Kellner R. Abridged Manual of the IUlness Attitude Scale.Department of psychology school of medicine.University ofNew Mexico. 1986.
27 Siegel S. Non-parametric statistics for the behaviouralsciences. McGraw-Hill, New York. 1956.
45
on 28 July 2018 by guest. Protected by copyright.
http://sti.bmj.com
/G
enitourin Med: first published as 10.1136/sti.70.1.40 on 1 F
ebruary 1994. Dow
nloaded from