Embed Size (px)
Citation preview
Ophthalmic Epidemiology, 2014; 21(5): 339–344! Informa Healthcare USA, Inc.
ISSN: 0928-6586 print / 1744-5086 online
DOI: 10.3109/09286586.2014.949782
ORIGINAL ARTICLE
A Population-based Study of Corneal Arcusand its Risk Factors in Iran
Hassan Hashemi1,2, Mehdi Khabazkhoob1, Mohammad Hassan Emamian3,Mohammad Shariati4, and Akbar Fotouhi5
1Noor Ophthalmology Research Center, Noor Eye Hospital, Tehran, Iran, 2Farabi Eye Hospital, TehranUniversity of Medical Sciences, Tehran, Iran, 3Shahroud University of Medical Sciences, Shahroud, Iran,
4Department of Community Medicine, School of Medicine, Tehran University of Medical Sciences, Tehran, Iran,and 5Department of Epidemiology and Biostatistics, School of Public Health, Tehran University of Medical
Sciences, Tehran, Iran
ABSTRACT
Purpose: To determine the prevalence of corneal arcus, its risk factors, and its relationship to ocular and visualindices.
Methods: In this cross-sectional study, 300 clusters were randomly selected from Shahroud in the north of Iran,using multistage sampling. A total of 20 people were invited to participate from each cluster. After enrollment,all optometric, biometric and ophthalmic exams were conducted on site.
Results: Of 6311 people invited, 5190 (82.2%) participated in the study. The prevalence of corneal arcus was23.3% (95% confidence interval, CI, 22.1–24.6), and 98.4% were bilateral cases. The prevalence of corneal arcuswas higher in men (odds ratio, OR, 2.02, 95% CI 1.8–2.3, p50.001) and increased with age (OR 1.1/year,p50.001). In a multivariable-adjusted regression model, age (OR 1.1/year, p = 0.006), male sex (OR 1.30,p = 0.001), diabetes (OR 0.7, p50.001), smoking (OR 1.5, p = 0.003), outdoor activity (OR 1.4, p = 0.006), systolicblood pressure (OR 1.01, p = 0.012), and diastolic blood pressure (OR 0.99, p = 0.016) were significantlycorrelated with corneal arcus. Including biometric components in another model, corneal thickness (OR 0.99,p50.001), anterior chamber depth (OR 0.68, p50.001) and corneal radius of curvature (OR 1.59, p50.001) weresignificantly correlated with corneal arcus.
Conclusion: This study adds valuable information to the epidemiology of corneal arcus in Iran and the MiddleEast. In people aged over 60 years, nearly 50% of the study population had corneal arcus. Older age, male sex,smoking, and systolic hypertension were risk factors for corneal arcus. Corneal arcus was also associated withthin and flat corneas and shallow anterior chamber depth.
Keywords: Corneal arcus, cross-sectional study, Iran, Middle East, prevalence, risk factors
INTRODUCTION
Corneal arcus is a common degeneration also knownas arcus senilis because of its high incidence amongthe elderly, and appears as a whitish ring in thestromal layer of the peripheral cornea. The conditionhas no particular ocular or visual side effects, none-theless, its histopathology is characterized by lipiddeposits, and studies have shown a relationship with
hypercholesterolemia and cardiovascular disease.1,2
The Framingham Heart Study demonstrated thatcorneal arcus can be a predictor of coronary arterydisease and cardiovascular disease.3 It has been usedas a marker in cardiovascular disease for over 2decades, and is suggested as a sign of hyperlipid-emia when detected before the age of 50 years.4–6
There is even evidence that the severity of cornealarcus is directly correlated with the severity of
Correspondence: Akbar Fotouhi, MD, PhD, Epidemiology and Biostatistics Department, School of Public Health, Tehran University of MedicalSciences, Tehran, Iran. Tel: +98 21 88987381-2. Fax: +98 21 88989664. E-mail: [email protected]
Received 3 November 2013; Revised 16 February 2014; Accepted 15 March 2014; Published online 13 August 2014
339
Oph
thal
mic
Epi
dem
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y G
azi U
niv.
on
11/0
4/14
For
pers
onal
use
onl
y.

atherosclerosis.7 In a study in Singapore, corneal arcuswas found to be related to systemic inflammatorymarkers and chronic kidney disease.2 Epidemiologicstudies describing the prevalence of corneal arcus arefew.8 Reported rates include 57.9% in the populationaged 40–80 years in Singapore and 65% in the over 49-year-old population-based Blue Mountains Eye Studyin Australia.1 Progressive cases of this ocular condi-tion can easily be detected by non-ophthalmologists,and in light of its association with important life-threatening diseases, detecting it in a patient shouldbe suggestive of risk for such diseases. Studying thismarker in middle-age and elderly populations candetermine the proportion of the population at risk ofdisease associated with corneal arcus. Since there arefew epidemiologic studies showing the prevalence ofcorneal arcus around the world, here we report theprevalence and risk factors of corneal arcus in a 40- to64-year-old Iranian population.
MATERIALS AND METHODS
The present report is part of the first phase of theShahroud Eye Cohort Study (ShECS). Details of themethodology and protocol of this cross-sectionalstudy have already been published,9 so are reviewedhere only briefly. The target population of ShECSconsisted of people aged 40–64 years living inShahroud, a city in the north of Iran. Overall, 300clusters were randomly chosen through stratifiedsampling. Each of the nine healthcare centers ofShahroud City was used as one stratum and thenumber of clusters was calculated based on thepopulation of each center so that the sample popula-tion was proportionate to the city population aged40–64 years.
A systematic random sampling procedure wasused to select index households for each clusterfrom the archives of households in the healthcarecenters. After identification of the index household ineach cluster, enumeration of the neighboring house-holds continued from the right side of that householdin the cluster until at least 20 eligible individuals werefound. As all 40–64-year-old members of each house-hold were entered in the study, depending on thenumber of eligible individuals in the last household,each cluster included at least 20 individuals.
All examinations were performed at one site. In thefirst stage, signed consent forms were obtained fromrespondents, and then their demographics and othergeneral information such as occupational status,socioeconomic status, history of smoking, and oph-thalmic and medical history were recorded.
Ocular biometry was performed for all participantsusing the Allegro Biograph (WaveLight AG, Erlangen,Germany). Recorded indices included axial length,
anterior chamber depth, lens thickness, and cornealradius of curvature.
Blood pressure was measured twice on the sameday, with an interval of 3 minutes. After two meas-urements, if there was a difference 410 mmHgbetween systolic readings and/or45 mmHg betweendiastolic readings, blood pressure was measured athird time and the two readings with the leastdifference were recorded. Average systolic and dia-stolic readings in these two measurements were usedfor systolic and diastolic blood pressure.
For each participant, a blood sample was collectedto determine blood glucose level. All participants whodeclared a history of diabetes, had a blood glucoselevel 4200 mg/dL, or were taking antidiabetic medi-cation were recorded as diabetic.
Visual acuity was tested for far and near vision,and refraction was determined using three differentretinoscopy, cycloplegic, and subjective techniques.Ophthalmic examinations were performed in twostages, before and after pupil dilation. Before dilation,slit lamp biomicroscopy and intraocular pressuremeasurement were performed, and retinal examswere done using direct and indirect ophthalmoscopy.
Diagnosis of corneal arcus was made by an oph-thalmologist during the slit-lamp exam.
In this study, corneal arcus was defined as theobservation of hazy white colored lipid in the cornealstroma, mostly in the superior or inferior pole,separated from the limbus by a transparent rim,sometimes forming a complete (360�) ring.10
Cataract was graded and classified using the LensOpacities Classification System III.11 Myopia andhyperopia were defined as spherical equivalent refrac-tion worse than �0.5 and 0.5 diopters, respectively.
Statistical Analysis
The prevalence of corneal arcus is reported aspercentages and 95% confidence intervals (CI). Weused unadjusted and multivariable adjusted logisticregression to examine the relation of corneal arcuswith other variables, and calculated odds ratios (ORs)and 95% CIs to demonstrate the strength of relation-ships. Also, in light of the cluster sampling method,adjustments were made when calculating standarderrors and CIs.
The ethics committee of Shahroud University ofMedical Sciences approved the study, which wasconducted in accordance with the tenets of theDeclaration of Helsinki.
RESULTS
Of the 6311 people selected for enrollment in thisstudy, 5190 people (82.2%) responded. The mean age
340 H. Hashemi et al.
Ophthalmic Epidemiology
Oph
thal
mic
Epi
dem
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y G
azi U
niv.
on
11/0
4/14
For
pers
onal
use
onl
y.

of respondents was 50.9 ± 6.3 years (40–60 years), and2977 (57.4%) were female.
The prevalence of corneal arcus was 23.3% (95% CI22.1–24.6%) and 98.4% of cases were bilateral. The ratewas significantly higher in men (OR 2.02, 95% CI 1.8–2.3, p50.001). Table 1 shows the prevalence of cornealarcus by age and sex. Rates significantly increasedfrom 10.1% in the 40–44-year age group to 44.1% inthe 60–64-year age group (p50.001). Logistic regres-sion showed that the prevalence of corneal arcusincreased significantly with age (OR 1.11/year, 95% CI1.09–1.12/year, p50.001).
Prevalence rates of corneal arcus were significantlyhigher in males in all age groups. Prevalence ofcorneal arcus by level of education is presented inTable 2; the rate was higher among illiterate peoplecompared to all other groups, except those withcollege education. As demonstrated in Table 2, the
prevalence of corneal arcus was 13% higher insmokers compared to non-smokers. Logistic regres-sion revealed that the odds of corneal arcus were 1.92times (95% CI 1.6–2.3) higher in smokers than non-smokers (p50.001). Rates did not differ significantlybetween diabetics and non-diabetics (p = 0.151).The prevalence of corneal arcus was 20% amongthose with indoor occupations, significantly lowerthan those whose jobs involved outdoor activities(p50.001). Mean systolic blood pressure in thosewith and without corneal arcus was 131.3 mmHg(95% CI 130.1–132.5 mmHg) and 128.4 mmHg(95% CI 127.70–129.05 mmHg), respectively (p50.001). Diastolic blood pressure did not differ signifi-cantly between people with and without cornealarcus (p = 0.480). Mean arterial pressure was alsosignificantly higher in people with corneal arcus(p50.001).
TABLE 2. Prevalence of corneal arcus by general and ocular variables and their associations by unadjustedlogistic regression, Shahroud, Iran.
Corneal arcus
Variable % (95% CI) OR (95% CI) p value
EducationIlliterate 31.0 (26.3–35.6) 1Primary school 21.5 (19.7–23.2) 0.61 (0.48–0.77) 50.001Guidance school 24.7 (21.3–28.2) 0.73 (0.55–0.98) 0.034High school 22.1 (19.7–24.5) 0.63 (0.49–0.81) 50.001College 27.6 (23.7–31.5) 0.85 (0.63–1.14) 0.278
SmokingNo 21.7 (20.4–23.0) 1Yes 34.7 (31.0–38.5) 1.92 (1.60–2.30) 50.001
DiabetesNo 23.6 (22.3–24.9) 1Yes 20.9 (17.6–24.3) 0.85 (0.68–1.06) 0.151
ActivityIndoor 20.0 (18.6–21.3) 1Outdoor 33.9 (30.6–37.1) 2.05 (1.75–2.41) 50.001
CataractNo 22.6 (21.4–23.9) 1Yes 30.0 (25.3–34.6) 1.46 (1.17–1.84) 50.001
Refractive errorEmmetropia 21.5 (19.7–23.3) 1Myopia 21.7 (19.4–24.0) 1.01 (0.85–1.20) 0.898Hyperopia 26.6 (24.3–29.0) 1.32 (1.14–1.54) 50.001
CI, confidence interval; OR, odds ratio
TABLE 1. Prevalence of corneal arcus by age and sex in the population aged 40–64 years in Shahroud, Iran.
Corneal arcus, % (95% CI)
Age, years n Males Females Total
40–44 960 17.5 (12.8–22.2) 6.3 (4.5–8.1) 10.1 (8.1–12.1)45–49 1390 22.1 (18.9–25.3) 11.3 (9.0–13.6) 15.7 (13.9–17.6)50–54 1285 30.6 (26.8–34.4) 19.0 (16.1–21.9) 24.1 (21.9–26.4)55–59 954 38.4 (33.9–42.9) 29.0 (24.8–33.2) 33.5 (30.3–36.7)60–64 601 49.7 (43.8–55.5) 39.0 (33.3–44.6) 44.1 (40.1–48.2)Total 5190 30.6 (28.6–32.6) 17.9 (16.4–19.4) 23.3 (22.1–24.6)
CI, confidence interval
Corneal Arcus and its Risk Factors 341
! 2014 Informa Healthcare USA, Inc.
Oph
thal
mic
Epi
dem
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y G
azi U
niv.
on
11/0
4/14
For
pers
onal
use
onl
y.
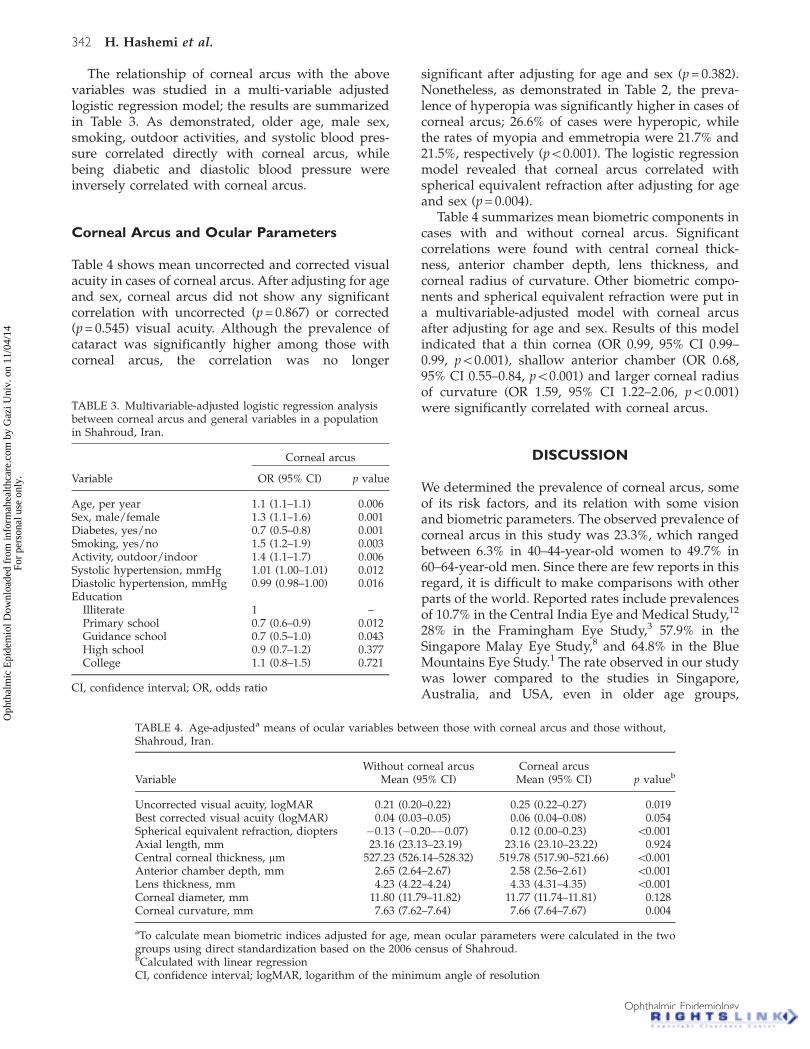
The relationship of corneal arcus with the abovevariables was studied in a multi-variable adjustedlogistic regression model; the results are summarizedin Table 3. As demonstrated, older age, male sex,smoking, outdoor activities, and systolic blood pres-sure correlated directly with corneal arcus, whilebeing diabetic and diastolic blood pressure wereinversely correlated with corneal arcus.
Corneal Arcus and Ocular Parameters
Table 4 shows mean uncorrected and corrected visualacuity in cases of corneal arcus. After adjusting for ageand sex, corneal arcus did not show any significantcorrelation with uncorrected (p = 0.867) or corrected(p = 0.545) visual acuity. Although the prevalence ofcataract was significantly higher among those withcorneal arcus, the correlation was no longer
significant after adjusting for age and sex (p = 0.382).Nonetheless, as demonstrated in Table 2, the preva-lence of hyperopia was significantly higher in cases ofcorneal arcus; 26.6% of cases were hyperopic, whilethe rates of myopia and emmetropia were 21.7% and21.5%, respectively (p50.001). The logistic regressionmodel revealed that corneal arcus correlated withspherical equivalent refraction after adjusting for ageand sex (p = 0.004).
Table 4 summarizes mean biometric components incases with and without corneal arcus. Significantcorrelations were found with central corneal thick-ness, anterior chamber depth, lens thickness, andcorneal radius of curvature. Other biometric compo-nents and spherical equivalent refraction were put ina multivariable-adjusted model with corneal arcusafter adjusting for age and sex. Results of this modelindicated that a thin cornea (OR 0.99, 95% CI 0.99–0.99, p50.001), shallow anterior chamber (OR 0.68,95% CI 0.55–0.84, p50.001) and larger corneal radiusof curvature (OR 1.59, 95% CI 1.22–2.06, p50.001)were significantly correlated with corneal arcus.
DISCUSSION
We determined the prevalence of corneal arcus, someof its risk factors, and its relation with some visionand biometric parameters. The observed prevalence ofcorneal arcus in this study was 23.3%, which rangedbetween 6.3% in 40–44-year-old women to 49.7% in60–64-year-old men. Since there are few reports in thisregard, it is difficult to make comparisons with otherparts of the world. Reported rates include prevalencesof 10.7% in the Central India Eye and Medical Study,12
28% in the Framingham Eye Study,3 57.9% in theSingapore Malay Eye Study,8 and 64.8% in the BlueMountains Eye Study.1 The rate observed in our studywas lower compared to the studies in Singapore,Australia, and USA, even in older age groups,
TABLE 4. Age-adjusteda means of ocular variables between those with corneal arcus and those without,Shahroud, Iran.
Without corneal arcus Corneal arcusVariable Mean (95% CI) Mean (95% CI) p valueb
Uncorrected visual acuity, logMAR 0.21 (0.20–0.22) 0.25 (0.22–0.27) 0.019Best corrected visual acuity (logMAR) 0.04 (0.03–0.05) 0.06 (0.04–0.08) 0.054Spherical equivalent refraction, diopters �0.13 (�0.20–�0.07) 0.12 (0.00–0.23) 50.001Axial length, mm 23.16 (23.13–23.19) 23.16 (23.10–23.22) 0.924Central corneal thickness, mm 527.23 (526.14–528.32) 519.78 (517.90–521.66) 50.001Anterior chamber depth, mm 2.65 (2.64–2.67) 2.58 (2.56–2.61) 50.001Lens thickness, mm 4.23 (4.22–4.24) 4.33 (4.31–4.35) 50.001Corneal diameter, mm 11.80 (11.79–11.82) 11.77 (11.74–11.81) 0.128Corneal curvature, mm 7.63 (7.62–7.64) 7.66 (7.64–7.67) 0.004
aTo calculate mean biometric indices adjusted for age, mean ocular parameters were calculated in the twogroups using direct standardization based on the 2006 census of Shahroud.bCalculated with linear regressionCI, confidence interval; logMAR, logarithm of the minimum angle of resolution
TABLE 3. Multivariable-adjusted logistic regression analysisbetween corneal arcus and general variables in a populationin Shahroud, Iran.
Corneal arcus
Variable OR (95% CI) p value
Age, per year 1.1 (1.1–1.1) 0.006Sex, male/female 1.3 (1.1–1.6) 0.001Diabetes, yes/no 0.7 (0.5–0.8) 0.001Smoking, yes/no 1.5 (1.2–1.9) 0.003Activity, outdoor/indoor 1.4 (1.1–1.7) 0.006Systolic hypertension, mmHg 1.01 (1.00–1.01) 0.012Diastolic hypertension, mmHg 0.99 (0.98–1.00) 0.016Education
Illiterate 1 –Primary school 0.7 (0.6–0.9) 0.012Guidance school 0.7 (0.5–1.0) 0.043High school 0.9 (0.7–1.2) 0.377College 1.1 (0.8–1.5) 0.721
CI, confidence interval; OR, odds ratio
342 H. Hashemi et al.
Ophthalmic Epidemiology
Oph
thal
mic
Epi
dem
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y G
azi U
niv.
on
11/0
4/14
For
pers
onal
use
onl
y.

although our participants showed a higher prevalencethan the Indian population. Racial differences in theincidence of this ocular degeneration have previ-ously been demonstrated; it appears to start at anearlier age and be more prevalent among blackscompared to whites.13,14 Since the correlation betweencorneal arcus and cardiac disease has already beenconfirmed, the observed rates indicate that a consid-erable percentage of the study participants in all agegroups might be at risk of cardiovascular disease andhyperlipidemia.
As demonstrated, prevalence was significantlycorrelated with age in men and women, and inagreement with our results, several studies haveshown lower prevalence rates in women.1,2,8,12,15–17
According to our findings, the prevalence of cor-neal arcus increased by 10% per 5 years of age.A correlation with age has been shown in manystudies1,2,12,16 and the correlation is so evident that thecondition is also known as arcus senilis and arcussenilis cornea, although it may rarely be seen in theyoung as well. Since the arcus is composed ofdeposited lipids such as cholesterol, phospholipids,and triglycerides,18 increased rates of corneal arcuscan be due to age-related impairment of lipidmetabolism.
We observed a significantly higher prevalence ofcorneal arcus among smokers. Other studies haveinconclusive results on this association. Ang andcolleagues,17 Wu and colleagues2 and Fernandezand colleagues15 have shown that corneal arcus andsmoking are related, while studies by Vurgese andco-workers,12 Chua and co-workers1 and Hughesand co-workers19 did not show such an association.
In our study, diabetes correlated inversely withcorneal arcus. Vurgese and co-authors12 found norelationship, but other studies mostly confirm thatsuch an association exists. For example, contrary toour observations, diabetes and corneal arcus corre-lated directly in the Blue Mountains Eye Study1 and inreports by Hickey and co-authors20 and Barchiesi andco-authors.21 In light of derangements of lipid metab-olism in the process of diabetes, the relation betweencorneal arcus and diabetes is expected. The inversecorrelation seen in our study could thus be due to aninaccurate definition of diabetes which was based onthe person’s history, blood glucose level, and use ofantidiabetic medications.
In this study, we observed that corneal arcussignificantly correlated with higher systolic bloodpressure and lower diastolic blood pressure. Chenand colleagues22 reported a similar relation, while agreater number of studies did not show any relationwith systolic blood pressure.2,12,17 Since the relationbetween corneal arcus and blood pressure remainedin the multivariable adjusted model after adjustingfor age and sex, the association is not due to age.According to Wu and co-authors2, corneal arcus is
related to chronic renal disease, which may partlyexplain the association with blood pressure.
As observed above, the prevalence of corneal arcuswas significantly higher in illiterate participants,followed by those with university education thanparticipants with primary and guidance school edu-cation. Few studies have reported the same finding. Ina study in India, Vurgese and co-workers12 reportedthat mean educational level was higher in individualswith corneal arcus. It is rather difficult to explainthis relationship biologically and it may merely be astatistical correlation; however, it may be possible thatthe low knowledge and information of the illiterateparticipants makes them more prone to hypercholes-terolemia and the development of corneal arcus.This hypothesis is supported by the finding that theprevalence of arcus is higher in individuals who haveoutdoor occupations, since most educated peoplehave desk jobs and low educated people are mostlyactive outdoors. However, further studies arerequired to confirm the relationship between educa-tion, type of occupation and corneal arcus.
In addition to risk factors, we examined howcorneal arcus might relate to vision and ocularparameters. There was no significant correlationbetween corneal arcus and vision after adjusting forage and sex. Few studies have performed workaround this relationship. Pe’er and co-workers23
found no significant difference in visual acuitybetween arcus and non-arcus groups. Studies exam-ining corneal arcus have mostly concentrated on itsimportance and role as a marker for cardiovasculardisease, and evidently, the degeneration does notimpact vision. Nonetheless, in agreement withVurgese and co-workers,12 we found the prevalenceof hyperopia was significantly higher in corneal arcuscases. As revealed in the final multivariable-adjustedmodel, corneal arcus and spherical equivalent refrac-tion did not correlate in the presence of corneal radiusof curvature, in other words, the association betweencorneal arcus and spherical equivalent refraction wasdue to radius of curvature. In our study, the radius ofcurvature was significantly higher in cases of cornealarcus compared to those without in unadjusted andmultivariable-adjusted models. We believe the accu-mulation of lipid droplets in the peripheral corneacauses the corneal radius of curvature to increase andthe cornea to flatten. Based on our findings, eyes withcorneal arcus also had thinner corneas. In this regard,Vurgese and colleagues12 and Wu and colleagues8
confirm our results.The present study has strengths and limitations.
The most important strength was studying cornealarcus in a large sample in the Middle East. Since thereis insufficient information about this ocular degener-ation in this region and around the globe, results ofthis study can be very valuable. Nonetheless, sincecorneal arcus was diagnosed by slit lamp examination
Corneal Arcus and its Risk Factors 343
! 2014 Informa Healthcare USA, Inc.
Oph
thal
mic
Epi
dem
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y G
azi U
niv.
on
11/0
4/14
For
pers
onal
use
onl
y.
rather than imaging, we could not determine itsdegree and severity. Another major limitation of thisstudy was that participants were not fasting and itwas impossible to evaluate their lipid profile. The lackof information about cardiovascular disease, andfailure to measure fasting blood sugar are limitationsof this study.
This study adds valuable information to ourknowledge of the epidemiology of corneal arcus inIran and the Middle East. This study showed that inpeople aged over 60 years, nearly 50% of the studypopulation had corneal arcus. Older age, male sex,smoking, and higher systolic blood pressure wereamong risk factors for corneal arcus. Also, cornealarcus was related to thickness and radius of thecornea and shallow anterior chamber depth.
DECLARATION OF INTEREST
The authors report no conflicts of interest. The authorsalone are responsible for the content and writing ofthe paper.
This project is funded in part by the NoorOphthalmology Research Center and ShahroudUniversity of Medical Sciences.
REFERENCES
1. Chua BE, Mitchell P, Wang JJ, Rochtchina E. Corneal arcusand hyperlipidemia: findings from an older population.Am J Ophthalmol 2004;137(2):363–365.
2. Wu R, Wang JJ, Tai ES, Wong TY. Cardiovascular riskfactors, inflammation, and corneal arcus: the SingaporeMalay Eye Study. Am J Ophthalmol 2010;150(4):581–587.
3. Fernandez AB, Keyes MJ, Pencina M, et al. Relation ofcorneal arcus to cardiovascular disease (from theFramingham Heart Study data set). Am J Cardiol 2009;103(1):64–66.
4. Nishimoto JH, Townsend JC, Selvin GJ, De Land PN.Corneal arcus as an indicator of hypercholesterolemia.J Am Optom Assoc 1990;61(1):44–49.
5. Rifkind BM. Corneal arcus and hyperlipoproteinaemia.Surv Ophthalmol 1972;16(5):295–304.
6. Winder AF, Jolleys JC, Day LB, Butowski PF. Corneal arcus,case finding and definition of individual clinical risk in
heterozygous familial hypercholesterolaemia. Clin Genet1998;54(6):497–502.
7. Zech Jr LA, Hoeg JM. Correlating corneal arcus withatherosclerosis in familial hypercholesterolemia. LipidsHealth Dis 2008;7:7.
8. Wu R, Wong TY, Saw SM, et al. Effect of corneal arcus oncentral corneal thickness, intraocular pressure, and pri-mary open-angle glaucoma: the Singapore Malay EyeStudy. Arch Ophthalmol 2010;128(11):1455–1461.
9. Fotouhi A, Hashemi H, Shariati M, et al. Cohort profile:Shahroud Eye Cohort Study. Int J Epidemiol 2013;42(5):1300–1308.
10. Kaufman HE, Barron BA, McDonald MB, Kaufman K.The cornea. Oxford: Butterworth-Heinemann Limited; 1998.pp. 486–487.
11. Chylack LT Jr, Wolfe JK, Singer DM, et al. The Lens OpacitiesClassification System III. The Longitudinal Study ofCataract Study Group. Arch Ophthalmol 1993;111:831–836.
12. Vurgese S, Panda-Jonas S, Saini N, et al. Corneal arcus andits associations with ocular and general parameters: theCentral India Eye and Medical Study. Invest Ophthalmol VisSci 2011;52(13):9636–9643.
13. Klein B, Klein R, Haseman J, et al. Corneal arcus andcardiovascular disease in Evans County, Georgia. ArchIntern Med 1975;135(4):509–511.
14. Macaraeg Jr PV, Lasagna L, Snyder B. Arcus not so senilis.Ann Intern Med 1968;68(2):345–354.
15. Fernandez A, Sorokin A, Thompson PD. Corneal arcus ascoronary artery disease risk factor. Atherosclerosis 2007;193(2):235–240.
16. Moss SE, Klein R, Klein BE. Arcus senilis and mortality in apopulation with diabetes. Am J Ophthalmol 2000;129(5):676–678.
17. Ang M, Wong W, Park J, et al. Corneal arcus is a signof cardiovascular disease, even in low-risk persons. Am JOphthalmol 2011;152(5):864–871.
18. Andrews JS. The lipids of arcus senilis. Arch Ophthalmol1962;68(2):264–266.
19. Hughes K, Lun KC, Sothy SP, et al. Corneal arcus andcardiovascular risk factors in Asians in Singapore. Int JEpidemiol 1992;21(3):473–477.
20. Hickey N, Maurer B, Mulcahy R. Arcus senilis: its relationto certain attributes and risk factors in patients withcoronary heart disease. Br Heart J 1970;32(4):449–452.
21. Barchiesi BJ, Eckel RH, Ellis PP. The cornea and disordersof lipid metabolism. Surv Ophthalmol 1991;36(1):1–22.
22. Chen HT, Chen HC, Hsiao CH, et al. Corneal arcus andcardiovascular risk factors in middle-aged subjects inTaiwan. Am J Med Sci 2009;338(4):268–272.
23. Pe’er J, Vidaurri J, Halfon ST, et al. Association betweencorneal arcus and some of the risk factors for coronaryartery disease. Br J Ophthalmol 1983;67(12):795–798.
344 H. Hashemi et al.
Ophthalmic Epidemiology
Oph
thal
mic
Epi
dem
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y G
azi U
niv.
on
11/0
4/14
For
pers
onal
use
onl
y.





























