Embed Size (px)
Citation preview

A pilot quality-of-life instrument for acne rosacea
Kimberly Nicholson, MD,a Liana Abramova, MD,b Mary-Margaret Chren, MD,c
Jensen Yeung, MD,d Susan Y. Chon, MD,e and Suephy C. Chen, MD, MSa,f
Atlanta, Georgia; St Louis, Missouri; San Francisco, California;
Toronto, Ontario, Canada; and Houston, Texas
Background: No rosacea-specific quality-of-life (QOL) instrument exists.
Objective: We sought to develop a validated, reliable rosacea-specific instrument.
Methods: From 6 in-depth interviews, we composed 21 rosacea-specific items. These items and Skindex-29 were administered in a validation cohort (n = 59). Internal consistency reliability and reproducibilitywere measured with Cronbach’s coefficient a and intraclass correlation coefficient, respectively. Respon-siveness was assessed comparing baseline with 4- to 6-month responses. Construct validity was assessedwith principal axes factor analyses. Discriminant validity was examined with an additional 38 patientscomparing differences in responsiveness between the rosacea-specific QOL instrument and Skindex.
Results: Reliability was high (Cronbach’s a: 0.82-0.97, intraclass correlation coefficient: 0.70-0.95). Therosacea-specific QOL instrument showed preliminary responsiveness for patients with improved disease (P #
.05). Principal axes factor analyses correlated to hypothesized scales (r = 0.57-0.82). Discriminant validity wasillustrated with greater differences in responsiveness using the rosacea-specific QOL instrument (P = .008).
Limitations: Potential selection bias and lack of generalizability was a limitation.
Conclusions: The rosacea-specific QOL instrument, RosaQoL, appears to be a reliable and valid QOLinstrument and shows preliminary responsiveness for patients with improving rosacea. ( J Am AcadDermatol 2007;57:213-21.)
Rosacea is a chronic skin condition with manysymptoms that can be both frustrating andsocially stigmatizing to patients. Rosacea af-
fects up to 10% of the general population1 with apredilection for Caucasian persons of Celtic ancestry,although it can occur in darker-skinned individuals.It is more common in women than in men.1 There are4 subtypes of rosacea as defined by the NationalRosacea Society, each with its own constellation ofsigns and symptoms: erythematotelangiectatic,
From the Department of Dermatology, Emory University School of
Medicine, Atlantaa; Department of Dermatology, Washington
University School of Medicine, St Louisb; Departments of Der-
matology and Medicine, University of California at San Francisco
and the Dermatology Service, San Francisco Department of
Veterans Affairs Medical Centerc; Department of Dermatology,
University of Torontod; Department of Dermatology, University
of Texas MD Anderson Cancer Centere; and Department of
Health Services Research and Development, Division of Derma-
tology, Atlanta Department of Veterans Affairs Medical Center.f
Supported in part from an American Skin Association (ASA) Health
Services Research Grant, the ASA David Martin Carter Research
Scholar Award, and an Emory Skin Disease Research Center
Pilot and Feasibility grant (No. P30AR42687) from the National
Institute on Arthritis and Musculoskeletal and Skin Disease
(NIAMS), National Institutes of Health (NIH). Dr Chen is
papulopustularpersistent, phymatous, and ocular.2
The presentation of rosacea is highly variable evenwithin subtypes, and the symptoms and visual man-ifestations of the disease can significantly affect apatient’s quality of life (QOL).3
Current treatments for many of the symptoms ofrosacea, including flushing and phymatous changes,are insufficient.4 Pharmaceutical companies con-stantly develop new products to control the diseaseand could benefit from a reliable and validated
supported in part by a Mentored Patient Oriented Career
Development Award (No. K23AR02185-01A1) from NIAMS, NIH.
Disclosure: Dr Chen holds the copyright and would receive licensing
royalties from use of the RosaQoL. Drs Nicholson, Abramova,
Chren, Yeung, and Chon have no conflicts of interest to declare.
Data from this manuscript were presented as abstracts at the 2004
and 2005 American Academy of Dermatology Annual Meetings
(in Washington, DC and New Orleans, LA, respectively).
Accepted for publication January 29, 2007.
Reprint requests: Suephy C. Chen, MD, MS, Department of
Dermatology, Emory University, 101 Woodruff Circle, Atlanta,
GA 30322. E-mail: [email protected].
Published online April 20, 2007.
0190-9622/$32.00
ª 2007 by the American Academy of Dermatology, Inc.
doi:10.1016/j.jaad.2007.01.048
213

J AM ACAD DERMATOL
AUGUST 2007
214 Nicholson et al
instrument to measure patient-reported therapeuticimpact over time. A standard grading system formeasuring the severity of clinical symptoms hasrecently been established by the National RosaceaSociety.5 However, the authors noted that additionalfactors are important in determining severity accord-ing to the patient, including psychologic, social, oroccupational effects of rosacea. Moreover, studieshave demonstrated that objective clinical parametersof skin disease are often poorly correlated with QOLimpact and that most physicians underestimate theimpact of skin disease on a patient’s QOL.6 Thus, aninstrument that can measure and quantify rosacea-related QOL would be helpful for both physiciansand researchers. Although there are several genericcutaneous QOL instruments, a rosacea-specific sur-vey does not exist. Generic instruments are useful forcomparing QOL impact among different diseasesand populations but may not be sensitive to disease-specific issues. A rosacea-specific instrument wouldbe more sensitive to QOL issues and may also bemore sensitive to changes in the disease over time.7
We developed a rosacea-specific instrument, calledRosaQoL, and tested its psychometric properties.
METHODSAll patients were recruited from two university
dermatology clinics. All protocols were approvedand consents obtained in accordance with the insti-tutional review board at both institutions.
Item developmentUsing in-depth interviews, we asked patients with
rosacea open-ended questions to elicit any and allways that their skin condition affected their lives. Weinterviewed patients to a point of saturation whereno new information was elicited. Based on all patientmentions and their frequency, we composed rosa-cea-specific items. We conceptualized 3 major con-structs from these items that explain the way rosaceaaffects patients’ QOL: symptoms, functioning, andemotions. We administered the rosacea-specificitems in addition to the 29-item version of Skindex8
to comprehensively assess the constructs patientsfound relevant. For all items, we used the same formatas for Skindex-29 items, but changing the wording‘‘skin condition’’ to ‘‘rosacea.’’ All items inquired aboutthe last 4 weeks; response categories were ‘‘never,’’‘‘rarely,’’ ‘‘sometimes,’’ ‘‘often,’’ and ‘‘all the time.’’
Sample population, measures,and data collection
A list of patients from dermatology clinics wasobtained based on the International Classificationof Diseases, Ninth Revision code for rosacea. Patients
were randomly selected from the list. Patients werecontacted during a period of 4 years such that allseasons of the year were represented. By telephone,interviewers administered the 29-item version ofSkindex, the 21 rosacea-specific items, 5 globalquestions about their general health and rosacea,and 3 demographic questions to patients. The pa-tients answered all questions at baseline, at 72 hours(allowable range: 3-7 days), and at 4 to 6 months.Demographic questions were omitted in the lattertwo time points. Patients were asked to self-rate theirrosacea at the 4- to 6-month time point as ‘‘im-proved,’’ ‘‘worsened,’’ or ‘‘no change’’ based on thequestion, ‘‘How is your rosacea compared to the lasttime you filled out this survey?’’
AnalysesAll statistical analyses were performed with soft-
ware (SPSS, Version 10.0 and 13.0 for Windows, SPSSInc, Chicago, Ill).9 Nonparametric tests were per-formed given the nonnormal distribution of data.The specific tests are further delineated in psycho-metric evaluation.
Item reductionItems to which more than 60% of patients chose
‘‘never’’ as their response were eliminated to yieldthe final instrument.
ScoringA patient’s scale score was the average of his or
her responses to items in a given scale. For example,the scale score for emotion was the average of allresponses to the items in the emotion scale.
The responses to the items were: ‘‘never,’’‘‘rarely,’’ ‘‘sometimes,’’ ‘‘often,’’ and ‘‘all the time.’’The responses were recorded on a 1 (never)-to-5 (allthe time) scale. This scoring system was also used forSkindex-29, which purposefully differs from itsrecommended 0-to-100 scoring. This approach wastaken to compare scores from the rosacea-specificQOL instrument with Skindex-29. Patients’ totalscores were calculated as well. This included theaverage of all responses, with individual scale scoresweighted equally.
Psychometric evaluationWe tested the instrument for reliability, validity,
and responsiveness. We evaluated reliability withinternal consistency by Cronbach’s a coefficient andwith reproducibility (test-retest reliability) by intra-class correlation coefficient. We tested for respon-siveness by applying the Wilcoxon signed ranks testto the baseline and 4- to 6-month answers for 3groups: those who reported improvement, no

J AM ACAD DERMATOL
VOLUME 57, NUMBER 2
Nicholson et al 215
change, or worsening of their rosacea. Both the scalescores for each of the hypothesized constructs andthe total scores were evaluated for responsiveness.The total score included all hypothesized constructsweighted equally.
We confirmed validity by examining face, content,and construct validity. We ensured face and contentvalidity of the instrument by interviewing patientswith rosacea in the focus group interviews. We testedconstruct validity in two ways. We had hypothesizedthat the items would cluster into 3 factors that couldbe labeled as ‘‘symptom,’’ ‘‘functioning,’’ and ‘‘emo-tion.’’ We tested this hypothesis by using principalaxes factor analyses followed by an orthogonalrotation. We retained only those factors with eigen-values greater than 1 and by application of the screetest.10 We identified the factor onto which itemsloaded by selecting the largest coefficient of that itemamong all the retained factors. Each factor waslabeled by thepredominant trait of the heavily loadeditems. We compared the a priori hypothesized scaleassigned to each item with the factor onto which eachitem loaded. We also compared the regression factorscores with the unweighted hypothesized scalescores by Spearman correlation coefficients.
The second way we tested construct validity wasby comparing the symptom, emotion, and functionscale scores with the self-reported severity of rosaceausing a Jonckheere-Terpstra test for trend.11 Wehypothesized that the scale scores would correlatewith the severity of rosacea.
Discriminant validity is the extent to which oneinstrument measures a certain health characteristicbetter than another instrument. Because Skindex-29is a generic QOL instrument, we hypothesized that itwas not as sensitive as the rosacea-specific QOLinstrument in measuring QOL issues specific torosacea. We tested for discriminant validity by com-paring scores from the rosacea-specific QOL instru-ment with Skindex-29 in two ways. First, weexamined the relative degree of responsivenessover time by comparing the difference in respon-siveness for the rosacea-specific QOL instrumentversus Skindex-29 for patients whose rosacea hadimproved between baseline and 4 to 6 months usingthe Wilcoxon signed ranks test. Discriminant validitywas also tested by comparing the number of insen-sitive items in the rosacea-specific QOL instrumentversus Skindex-29 in a second cohort of patients.Initial item reduction for the rosacea-specific QOLinstrument included removing any item for whichgreater than 60% of participants chose ‘‘never’’ astheir answer. This would theoretically remove allitems that were insensitive to rosacea QOL. Afterexamination of the distribution of the answers to a
given item in the second cohort, we compared thenumber of insensitive items from the rosacea-specific QOL instrument with those from Skindex-29 using these same parameters.
RESULTSDemographics
We contacted and invited 6 patients to participatein face-to-face in-depth interviews. After designingthe initial instrument from these interviews, wecontacted a total of 274 patients by telephone forthe instrument validation. Approximately 100 pa-tients from the first dermatology clinic were con-tacted, and 36 agreed to participate. All patientscompleted the survey at the 72-hour time point, butnone were included in the 4- to 6-month time point.We had not designed the responsiveness componentof the study when these patients were enrolled. In all,174 patients from the second dermatology clinic werecontacted in the first sample of patients, of which 26agreed to participate. Of these, 3 patients dropped outat the 72-hour time point. Overall, a total of 59 patientsagreed to participate in the initial study (the validationgroup). The overall median age was 53 years (inter-quartile range 43-64). There were 43 women and 16men overall. In all, 64% were married or living with apartner at the time of the interview, and 100% ofpatients interviewed from the second dermatologyclinic were Caucasian. Race information was notcaptured for patients from the first dermatology clinic.
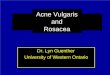
We tested responsiveness and discriminant valid-ity using both patients in the validation group fromthe second dermatology clinic and in a secondcohort of patients. This second cohort consisted of38 patients from the second dermatology clinic whowere contacted at a later date after designing theresponsiveness analysis. In all, 217 patients werecalled, of which 38 completed the instruments in full.The median age of participants was 63 years (inter-quartile range 52-73). There were 33 women and 5men overall. In all, 63% were married or living with apartner at the time of the interview. Of the 38 patientsinterviewed in this second cohort, 35 were Caucasian(92%). The other 3 patients were African American(1), Hispanic (1), and American Indian (1). At the endof the data collection, a total of 64 patients from thesecond dermatology clinic had completed the base-line surveys. Of these 64 patients, 40 completed therosacea-specific QOL instrument again at either 6months (the validation group, 13 patients) or at 4months (the second cohort, 27 patients) (Fig 1).
Disease characteristicsBased on patient self-rated severity during the
prior 4 weeks for the validation group, 24% of

J AM ACAD DERMATOL
AUGUST 2007
216 Nicholson et al
Fig 1. Patient flowchart.
patients had poor to fair rosacea and 76% of patientshad good to excellent rosacea. The majority ofpatients (61%) had experienced rosacea for 2 to 10years. In the discriminant validity group, 37% re-ported poor to fair rosacea and 63% reported goodto excellent rosacea. The majority of patients (74%)had experienced rosacea for 5 years or more.
Item developmentFrom the in-depth interviews, we developed 21
rosacea-specific items that were not included inSkindex-29. We administered these items in additionto the items from Skindex-29. The average durationto answer all 51 questions was 14.85 minutes (SD:6.12 minutes).
Item analysis and reductionOf the 51 items, the patients demonstrated that
their rosacea-related QOL was most affected byflushing with a median score of 4.0 (interquartilerange 3.0-4.0). QOL was least affected by interfer-ence with a patient’s sex life with a median score of
1.0 (1.0-1.0). Median scores for all items are listed inTable I.
Several items proved to be relatively insensitive;greater than 60% of the patients answered ‘‘never’’ tothese items. Note that Skindex-29 actually contains30 items, of which only 29 are scored. Item 18 inSkindex-29 is not included when calculating the finalscore. This item was found to be sensitive to rosacea-specific QOL based on our population. Thus, item 18from Skindex was not included when calculatingnontransformed Skindex-29 scores for this study, butwas included when calculating the rosacea-specificQOL instrument scores. Overall, the total number ofinsensitive items included 20 questions from Skindex-29 and 10 rosacea-specific items (Table I). Thus, thefinal rosacea-specific QOL instrument questionnaireconsisted of the 21 sensitive items (Table II).
ReliabilityItems in each of the 3 scales demonstrated internal
consistency reliability with Cronbach’s a coefficientranging from 0.86 to 0.97. Systematically deleting one

J AM ACAD DERMATOL
VOLUME 57, NUMBER 2
Nicholson et al 217
Table I. Rosacea-specific quality-of-life instrument retained and deleted items
Retained items Deleted (insensitive) items
Question Percentage Median Score Question Percentage Median Score
Appearance of my skin 16.4 3.0 Avoid public speaking 73.8 1.0Self-conscious 36.1 2.0 Questions 82 1.0Cover up rosacea 39.3 3.0 Self-confidence 62.3 1.0Bothered by persistence 34.4 3.0 Spend time 63.9 1.0Avoid food or drinks 52.5 1.0 First thing noticed 73.8 1.0Feels bumpy 37.7 3.0 Cost 65.6 1.0Flushes 6.6 4.0 Raw 68.9 1.0Skin is irritated easily 27.9 3.0 Disfigured 70.5 1.0Eyes bother me 52.5 1.0 Scratch 75.4 1.0Think about my rosacea 31.1 2.0 Picture taken 72.1 1.0Avoid certain environments 57.4 1.0 Hurts 77 1.0Serious 59 1.0 How well I sleep 90.2 1.0Burns or stings 54.1 1.0 Work or hobbies 78.7 1.0Worry about scars 59 1.0 Social life 68.9 1.0May get worse 29.5 3.0 Depressed 72.1 1.0Medication side effects 57.4 1.0 Stay at home 83.6 1.0Irritated 37.7 2.0 Itches 60.7 1.0Embarrassed 45.9 2.0 Close with those I love 83.6 1.0Frustrated 41 2.0 Ashamed 63.9 1.0Sensitive skin 21.3 3.0 Do things by myself 88.5 1.0Annoyed 34.4 3.0 Angry 72.1 1.0
Water bothers 70.5 1.0Showing affection 85.2 1.0Interactions 77 1.0Problem for those I love 90.2 1.0Desire to be with people 82 1.0Humiliated 78.7 1.0Bleeds 77 1.0Sex life 93.4 1.0Tired 93.4 1.0
All 51 items from the original rosacea-specific quality-of-life instrument are listed here. Columns on the left display items that were retained
after item reduction. Columns on the right display items that were discarded as insensitive. Percentages represent the percent of
participants who answered ‘‘never’’ to a specific question and relates to the sensitivity of the item.
item from the analysis did not significantly increasethe coefficients. Items in each of the 3 scales alsodemonstrated reproducibility with intraclass correla-tion coefficient ranging from 0.75 to 0.95 (Table III).
ResponsivenessPatients were divided into 3 categories (better,
worse, or no change) based on their self-ratedevaluations. Ten patients reported improvement, 5reported worsening, and 25 reported no changefrom baseline. Using the rosacea-specific scale scoresand the total score from all hypothesized constructsfrom baseline and 4- to 6-month interviews, wefound improvement in the QOL scores of thosepatients who reported improvement in their rosacea;the difference was statistically significant for allhypothesized constructs and for total impact, whichincluded all constructs weighted equally (P # .05,Wilcoxon signed ranks test). We found no significant
differences in the scores of those who reported eitherno change or worsening of their rosacea. Results forall categories are listed in Table IV.
Construct validityAfter factor analysis with orthogonal rotation, 3
factors were retained according to the criteria out-lined in the ‘‘Methods’’ section. From the items thatloaded most heavily on factor 1, we could see thatthe predominant trait was emotion. Factor 2 wasclearly symptom, and factor 3 was function. TheSpearman correlation coefficient comparing the re-gression factor scores and the unweighted hypoth-esized scale scores ranged from 0.57 to 0.82 (allP values\ .01). The correlation between the regres-sion factor scores and the other two scales (eg, factor1 with symptom or function) were lower, in the rangeof 0.40 to 0.48 (Table III).

J AM ACAD DERMATOL
AUGUST 2007
218 Nicholson et al
Table II. The final version of rosacea-specific quality-of-life instrument after removal of insensitive items
RosaQoL items Hypothesized construct
1. I worry that my rosacea may be serious Emotion2. My rosacea burns or stings Symptom3. I worry about getting scars from my rosacea Emotion4. I worry that my rosacea may get worse Emotion5. I worry about side effects from rosacea medications Emotion6. My rosacea is irritated Symptom7. I am embarrassed by my rosacea Emotion8. I am frustrated by my rosacea Emotion9. My rosacea makes my skin sensitive Symptom
10. I am annoyed by my rosacea Emotion11. I am bothered by the appearance of my skin (redness, blotchiness) Emotion12. My rosacea makes me feel self-conscious Emotion13. I try to cover up my rosacea (with makeup) Functioning14. I am bothered by persistence/reoccurrence of my rosacea Emotion15. I avoid certain foods or drinks because of my rosacea Functioning16. My skin feels bumpy (uneven, not smooth, irregular) Symptom17. My skin flushes Symptom18. My skin gets irritated easily (cosmetics, aftershaves, cleansers) Symptom19. My eyes bother me (feel dry or gritty) Symptom20. I think about my rosacea Emotion21. I avoid certain environments (heat, humidity, cold) because of my rosacea Functioning
The remaining sensitive items included 10 items from Skindex-29 and 11 rosacea-specific items that were gathered during focus sessions
with patients with rosacea. The appropriate hypothesized construct is listed to the right of each question.
RosaQoL, Rosacea-specific quality-of-life instrument.
Table III. Psychometric test results
Psychometric test Symptoms Functioning Emotion
Cronbach a coefficient 0.86-0.93 0.92-0.95 0.88-0.97Intraclass correlation coefficient 0.75-0.87 0.86-0.91 0.79-0.95Correlation between RF and
unweighted hypothesizedscale score*
RF1: 0.422 (0.183, 0.610) 0.552 (0.341, 0.706) 0.823 (0.715, 0.890)RF2: 0.809 (0.694, 0.881) 0.510 (0.288, 0.675) 0.547 (0.224, 0.636)RF3: 0.466 (0.234, 0.643) 0.527 (0.309, 0.688) 0.396 (0.153, 0.590)
RF, Regression factor.
*All results significant at the .01 level. Spearman correlation coefficients shown with 95% confidence intervals.
We compared the scale scores (symptoms, func-tioning, and emotion) from the final version of therosacea-specific QOL instrument with self-reportedseverity of rosacea. The severity levels were analyzedon a 5-point scale: poor, fair, good, very good, andexcellent. Statistical significance was noted for all 3scale scores (P \ .05 for all, Jonckheere-Terpstratest). Median scores within each hypothesized con-struct improved significantly as the self-reportedseverity of rosacea improved (P \ .05), as shown inTable V.
Discriminant validityWe demonstrated the discriminant validity of the
rosacea-specific QOL instrument as compared withSkindex-29 in patients who reported improving
rosacea during the responsiveness analysis. Therosacea-specific QOL instrument had a higher de-gree of responsiveness over 4 to 6 months thanSkindex-29 for the total score, including all hypoth-esized constructs (P = .008 by Wilcoxon signed rankstest). On further analysis, it was shown that thefunction construct was most responsible for thisdifference. A statistically significant difference inresponsiveness for the function construct existedbetween the rosacea-specific QOL instrument andSkindex-29 (P = .03) as compared with no statisticallysignificant difference between the symptom andemotion constructs.
We also ascertained that the rosacea-specific QOLinstrument was relatively more sensitive to rosaceaQOL issues than Skindex-29 with our item analysis

J AM ACAD DERMATOL
VOLUME 57, NUMBER 2
Nicholson et al 219
Table IV. Rosacea-specific quality-of-life instrument responsiveness data for patients who reportedimprovement, worsening, or no change in their rosacea
Baseline score
median and IQR
4- to 6-mo Score
median and IQR P value
Improved rosacea (n = 10) Symptom 2.21 (1.75-3.89) 1.93 (1.61-3.39) .006Emotion 2.36 (2.16-4.00) 2.14 (1.23-3.84) .051Functioning 2.83 (2.33-3.67) 2.17 (1.50-2.83) .020Total 2.43 (2.05-3.77) 2.17 (1.49-3.49) .012
No change (n = 25) Symptom 2.71 (2.29-3.21) 2.71 (2.00-3.14) .432Emotion 2.55 (1.68-3.45) 2.45 (1.77-3.18) .245Functioning 2.33 (1.33-2.83) 2.00 (1.17-3.00) .061Total 2.57 (2.14-3.14) 2.43 (2.12-3.05) .185
Worsening rosacea (n = 5) Symptom 3.43 (3.00-3.57) 3.29 (2.57-3.79) .581Emotion 3.00 (2.45-3.36) 2.36 (2.05-2.73) .063Functioning 2.33 (2.33-3.00) 2.33 (1.33-3.00) .194Total 2.90 (2.83-3.24) 2.57 (2.31-2.98) .066
The median scores for each hypothesized construct and for the average of all responses weighted equally (total) are shown along with the
interquartile ranges for each score.
IQR, Interquartile range.
Table V. Jonckheere-Terpstra test for trend comparing self-rated severity of rosacea with scale score for all3 hypothesized constructs (symptom, emotion, function)
Mean score Poor rosacea Fair rosacea Good rosacea Very good rosacea Excellent rosacea Significance
Symptom 3.29 3.00 (2.14-4.29) 2.93 (2.14-3.29) 2.43 (2.00-2.86) 1.14 (1.00-2.14) P \ .001Emotion 3.91 3.18 (2.00-4.45) 2.45 (1.19-2.73) 2.09 (1.55-2.45) 1.00 (1.00-1.09) P \ .001Functioning 3.67 2.67 (1.67-4.00) 3.00 (2.00-3.33) 2.33 (1.33-2.33) 1.00 (1.00-1.00) P \ .001
The self-rated severity levels were analyzed on a 5-point scale: poor, fair, good, very good, and excellent. Statistical significance was noted
for all 3 scales. Median scores and interquartile ranges within each hypothesized construct are shown for the different levels of severity. Note
that there was only one patient of 59 who rated his or her rosacea as poor; thus, there is no interquartile range for these values.
in the second cohort of 38 patients from the seconddermatology clinic (the discriminant validity group).In 2 of 21 rosacea-specific items (9.5%), at least 60%of the patients answered ‘‘never’’ as compared with19 of 30 (63.3%) Skindex-29 items. Note that 10 of theitems are used in both the rosacea-specific QOLinstrument and Skindex-29.
DISCUSSIONThis study represents a preliminary validated QOL
instrument created specifically for patients with ro-sacea. Through our work, we have demonstrated thereliability and validity of the pilot instrument. Wedemonstrated the reliability of the rosacea-specificQOL instrument by two methods: high internalconsistency as shown by considerable Cronbach a
coefficients for the 3 scales, and reproducibility asshown by high intraclass correlation coefficients.This ensures that the rosacea-specific QOL instru-ment will yield consistent results for a given patientunder similar conditions and is relatively free fromrandom error. We verified preliminary data forresponsiveness by demonstrating that individualconstruct and total scores improved in those patientswho reported improvement in their rosacea and that
the scores did not change in those patients whoreported no change. Data for the 5 patients whoreported worsening in their disease paradoxicallyshowed decreases or stabilization in scores despitereporting of worsening rosacea during the past 4weeks. However, analysis of these data must beconsidered with caution because of the small samplesize. Further work will be done to verify that patientscores increase with worsening rosacea in a largerpopulation.
This pilot instrument appears to demonstratereliability and validity. We ensured face and contentvalidity by developing the rosacea-specific itemsfrom in-depth interviews with patients with rosacea.We confirmed construct validity by finding thatsymptom, functioning, and emotion scale scorescorrelated with self-reported rosacea severity. Wealso demonstrated construct validity by confirmingthat our hypothesized 3 constructs (symptoms, emo-tions, and functioning) correlated with the factoranalysis of the data. Lastly, we demonstrated theincreased discriminant validity of the rosacea-spe-cific QOL instrument to QOL issues as compared withSkindex-29 by illustrating that the rosacea-specificQOL instrument detected responsiveness over time

J AM ACAD DERMATOL
AUGUST 2007
220 Nicholson et al
better than Skindex-29. We also qualitatively dem-onstrated that the rosacea-specific QOL instrumentwas more sensitive to QOL issues than Skindex.
The results of this study are limited by severalfactors. First, the responsiveness of the rosacea-specific QOL instrument has only been validated inpatients whose disease was either improved orunchanged from baseline. This may limit the use ofthe instrument in investigational studies until furtherdata are published regarding the instrument’s re-sponsiveness in patients with worsening disease.Second, there is potential for selection bias in ourvalidation population. Patients being seen at bothacademic institutions may have been referred fromanother site and, thus, might have rosacea that ismore refractory to treatment. In addition, the patientpopulation is more likely to be educated with higherincomes as compared with patients seen at a countyhospital or rural clinic. These factors should be takeninto consideration when using the rosacea-specificQOL instrument. In addition, we only administeredthis survey by telephone. Although we do notanticipate that face-to-face administration or self-administration would make a significant difference,the survey should be used cautiously in thesesettings. Lastly, we did not capture other baselinecharacteristics such as tendencies toward depressio-n/anxiety or attitudes toward cosmesis.
Despite these limitations, the current form of therosacea-specific QOL instrument represents a prom-ising patient-reported outcome measure of diseaseburden as a result of rosacea and might be practicalfor use in a clinical or research setting. In the clinicalarena, most evaluations of therapeutic interventionsare established with clinical parameters. However,QOL is another important outcome and can greatlyaffect both the patient-doctor relationship andpatient compliance with treatment. The rosacea-specific QOL instrument can be useful in determin-ing aspects of disease that are most important ordetrimental to an individual patient. For example,some patients may be most affected by symptoms,whereas others are bothered by the emotional con-sequences of rosacea. This can differ greatly be-tween individuals and, thus, the rosacea-specificQOL instrument can help to personalize the treat-ment and advice offered. In addition, the rosacea-specific QOL instrument can be used in a clinicalsetting to track a patient’s response to therapeuticsover time. Lastly, clinicians can use the impact onQOL data to petition managed care and insurancecompanies when coverage is denied for specifictherapies. This can be especially problematic in adisease such as rosacea, which may be cited as acosmetic issue.
In the research setting, the rosacea-specific QOLinstrument may be useful as a secondary or copri-mary end point in addition to an objective severityrating by clinicians for clinical trials testing newtherapies. The Food and Drug Administration hasrecently provided guidance regarding patient-reported outcomes, thus, emphasizing the impor-tance of well-developed QOL instruments. Thedevelopment strategy of the rosacea-specific QOLinstrument has complied with these guidelines andfits a gap in the research arena for a rosacea-specificQOL patient-reported outcome.12
Lastly, the rosacea-specific QOL instrument maybe useful as an end point for epidemiologic andburden of disease studies. At the time of the rosacea-specific QOL instrument’s initial development, astandard classification system for rosacea did notyet exist and is, thus, not addressed in our instru-ment. The National Rosacea Society has now estab-lished such a system that may be beneficial for use insurvey form. Simple questions to identify whichsubtype or subtypes affect a patient may be addedto the rosacea-specific QOL instrument to further aidin evaluation. Differences in QOL may exist betweenthe subtypes of rosacea and are currently beinginvestigated. Future studies may investigate the rea-sons for QOL changes in rosacea (eg, therapy vsseasonal effects).
Future studies need to take place for the rosacea-specific QOL instrument to be used with confidencein a general population. Validation needs to takeplace with less-educated patients, patients from anonacademic environment, patients with differingattitudes toward cosmesis, and patients with varyingpsychologic backgrounds. In addition, responsive-ness needs to be verified in patients with worseningdisease in a larger population of patients. Futurestudies may also explore other uses of the rosacea-specific QOL instrument. Face-to-face administrationor self-administration should also be verified to usethese venues for application of the rosacea-specificQOL instrument. Because the rosacea-specific QOLinstrument equally weights the responses from allthe questions, future work can explore the possibil-ity of patient-derived weights.
REFERENCES
1. Rebora A. The red face: rosacea. Clin Dermatol 1993;11:
225-34.
2. Wilkin J, Dahl M, Detmar M, Drake L, Feinstein A, Odom R,
Powell F. Standard classification of rosacea: report of the
National Rosacea Society expert committee on the classifica-
tion and staging of rosacea. J Am Acad Dermatol 2002;46:584-7.
3. Panconesi E. Psychosomatic dermatology. Clin Dermatol 1984;
2:94-179.
4. Powell FC. Rosacea. N Engl J Med 2005;352:793-803.

J AM ACAD DERMATOL
VOLUME 57, NUMBER 2
Nicholson et al 221
5. Wilkin J, Dahl M, Detmar M, Drake L, Liang MH, Odom R, et al.
Standard grading system for rosacea: report of the National
Rosacea Society expert committee on the classification and
staging of rosacea. J Am Acad Dermatol 2004;50:907-12.
6. Chren M, Lasek R, Quinn L, Mostow E, Zyzanski S. Skindex, a
quality-of-life measure for patients with skin disease: reliability,
validity, and responsiveness. J Invest Dermatol 1996;107:707-13.
7. Wright J, Young N. A comparison of different indices of
responsiveness. J Clin Epidemiol 1997;50:239-46.
8. Chren MM, Lasek R, Flocke S, Zyzanski S. Improved discrim-
inative and evaluative capability of a refined version of
Skindex, a quality-of-life instrument for patients with skin
diseases. Arch Dermatol 1997;133:1433-40.
9. SPSS. 10.0 and 13.0 eds. Chicago: SPSS Inc; 1999, 2004.
10. Dillon W, Goldstein M. Multivariate analysis: methods and
applications. New York: John Wiley and Sons; 1984.
11. Hollander M, Wolfe D. Nonparametric statistical methods. New
York: John Wiley and Sons; 1973.
12. Patient-reported outcome measures: use in medical product
development to support labeling claims. US Food and Drug
Administration. February 2006. Available from: http://www.fda.
gov/CDER/GUIDANCE/5460dft.pdf. Accessed November 1, 2006.