Embed Size (px)
Citation preview

www.elsevier.com/locate/humpath
Human Pathology (2013) xx, xxx–xxx
Case study
A novel 5-way translocation t(9;11;13;19;22) in a case ofchronic-phase chronic myeloid leukemiaShantashri Vaidya MSc a, Dolly Joshi PhDa, Kanjaksha Ghosh MDa,Prantar Chakrabarti MDb, Babu Rao Vundinti PhDa,⁎
aNational Institute of Immunohaematology (ICMR), Mumbai, Maharashtra 400012, IndiabInstitute of Haematology and Transfusion Medicine, Kolkata, West Bengal 700073, India
Received 1 October 2012; revised 8 January 2013; accepted 6 February 2013
(B
0h
Keywords:BCR/ABL gene;Chronic myeloidleukemia;Chronic phase;5-Way translocation
Summary Chronic myeloid leukemia (CML) is a hematopoietic stem cell disorder that occurs becauseof t(9;22)(q34;q11) translocations. Complex translocations have been reported in CML. We report anovel 5-way translocation 46,XY,t(9;11;13;19;22)(9q34.12;11p11.12;13q21.31;19q13.12;22q11.21)using GTG banding, fluorescence in situ hybridization, and spectral karyotyping in a case ofchronic-phase CML. Molecular analysis revealed the presence of 2 types of transcripts (b3a2, b2a2).The patient was responding to the imatinib treatment. However, the patient needs to be carefullymonitored at various intervals.© 2013 Elsevier Inc. All rights reserved.
1. Introduction
Chromosomal translocations are common in cancer cells,and some translocations produce oncogenes that are respon-sible for malignant transformation. Complex chromosomaltranslocations are defined as structural chromosomal re-arrangements and exchanges of genetic material between 2or more chromosomes. Chronic myeloid leukemia (CML) isa hematopoietic stem cell disorder. It occurs because oftranslocations between chromosomes 9 and 22, designatedas t(9;22)(q34;q11), forming a malignant BCR/ABL fusiongene on a novel chromosome called Philadelphia chromo-some (Ph). The classical pattern of the Ph chromosomeoccurs in 95% of CML cases; the remaining cases showadditional chromosomes or complex translocations. Here,we report a novel case of CML in chronic phase with
⁎ Corresponding author. Parel, Mumbai, Maharashtra 400012, India.E-mail addresses: [email protected], [email protected]
. R. Vundinti).
046-8177/$ – see front matter © 2013 Elsevier Inc. All rights reserved.ttp://dx.doi.org/10.1016/j.humpath.2013.02.021
complex Ph translocation involving the 5 chromosomes 9,22, 19, 11, and 13.
2. Case history
A 29-year-old man with no significant medical history wasreferred for cytogenetic investigation because of leukocytosis.No significant unusual clinical or morphologic feature wasobserved in the patient. A complete hemogram showed ahemoglobin level of 7.4 g/dL with a mean corpuscular volumeof 88, platelet count of 659 erythrocyte sedimentation rate, andwhite blood cell count of 223 800/μL with a differential countof 35% polymorphs, 7% basophils, 6% blasts, 5% promye-locytes, 24% myelocytes, and 23% metamyelocytes. Bonemarrow trephine biopsy showed a hypercellular marrow withmyeloid hyperplasia with left-shifted maturation. Physicalexamination and computed tomography scan of the abdomenrevealed hepatosplenomegaly (liver 8 cm and spleen 10 cm

2 S. Vaidya et al.
below left costal margin). CML was confirmed with bonemarrow analysis, and the patient was immediately started onimatinib (400 mg/d) and achieved a complete hematologicresponse at the end of 1 month.
3. Materials and methods
3.1. Conventional cytogenetics
Conventional cytogenetic analysis was performed on thebone marrow sample of the patient according to the standardprocedure. The chromosomal preparations were subjected toGTG banding. Thirty well-spread and banded metaphaseswere analyzed and karyotyped according to the 2009 Inter-national System for Human Cytogenetic Nomenclature [1].
3.2. Molecular cytogenetics
Fluorescence in situ hybridization (FISH) was done using aBCR/ABL probe (Vysis, Abbott Molecular Inc., Des Plaines,IL), andwhole chromosome paint probes for chromosomes 11,13, and 19 were used to identify the translocations. In an effortto understand the 5-way complex translocation in a better way,spectral karyotyping (SKY) was performed.
SKY hybridization, detection, and image analysis wereperformed essentially as described previously [2], in a seriesof steps including slide treatment, denaturation/hybridiza-tion, detection and imaging, and spectral analysis.
3.3. Molecular analysis
RNAwas extracted using the Trizol procedure from a freshperipheral blood sample of the patient and converted tocomplementary DNA (RevertAid First Strand cDNA Synthe-sis Kit; Fermentas, Lithuania, EU.). The entireBCR/ABL gene,including the regulatory regions and kinase domain of the ABLgene, was amplified and sequenced in forward and reversedirection using big dye terminator chemistry and 3130xLGenetic Analyser (Applied Biosystems, Foster City, CA,USA) [3].
Quantification of the BCR/ABL transcript was done usingTaqMan chemistry (BCR-ABL Mbcr FusionQuant Kit forthe Real-Time Quantitative PCR Analysis of BCR-ABLMbcr p210 Transcripts; Ipsogen, France), according to themanufacturer's instructions.
4. Results
4.1. Conventional cytogenetics
Conventional cytogenetics on the bone marrow samplegave the impression of a complex Ph translocation involving
the 5 chromosomes 9, 22, 11, 19, and 13 (Fig. 1A and B).However, the translocation of the 3′ part of the BCR genewas untraceable. To get a clear picture of the translocations,molecular cytogenetic methods like FISH and SKYwere used.
4.2. Molecular cytogenetics
FISH using a dual-color, dual-fusion BCR/ABL proberevealed BCR/ABL single fusion in 95% of metaphase andinterphase cells. The signal pattern observed was 2 green(normal chr[22] and 3′ part of BCR gene), 2 red (normal chr[9] and 5′ part of ABL gene), and 1 yellow (BCR/ABL fusiongene; Fig. 1C).
SKY analysis could trace the 3′ part of the BCR gene,which was translocated on chr(13) (Fig. 2A and B). Thus thekaryotype of the 5-way translocation observed by GTGbanding, FISH, and SKY can be written as 46,XY,t(9;11;13;19;22)(9q34.12;11p11.12;13q21.31;19q13.12;22-q11.21) (Fig. 2C).
4.3. Molecular analysis
Direct sequencing revealed either no mutation in theBCR/ABL kinase domain or the regulatory SH3-SH2 domainof the BCR/ABL fusion gene. However, sequencing the SH3-SH2 region revealed the presence of both types of transcripts,b3a2 and b2a2 (Fig. 3). Real-time polymerase chain reactionquantification of the BCR/ABL mRNA revealed a transcriptratio of 89% for BCR/ABL to ABL.
5. Discussion
Additional chromosomal abnormalities are observed atdiagnosis in less than 10% of the cases of CML-chronicphase (CP). Occurrence of additional chromosomal abnor-malities in Ph-positive cells can be a primary event or asecondary event. The complex chromosomal abnormalitiesalso have been reported in CML cases. However, 5-waytranslocation is a rare occurrence. In our case, thechromosomes 9, 11, 13, 19, and 22 were involved incomplex translocation including the Ph chromosome. The 5-way translocation involving chromosomes 9, 11, 13, 19, and22 is a first case to the best of our knowledge. According tothe literature, only 9 cases with 5-way translocation inpatients with CML have been reported [4]. Most of the casesof 5-way translocations reported show good response toimatinib treatment. In our case, the patient was followed up,and the patient was found to be responding to the treatment.
The patients with complex translocations respond to thetreatment when the Ph chromosome is a primary event.Zaccaria et al [5] reported cytogenetic data of 36 patients, ofwhom 22 showed occurrence of the Ph chromosome as aprimary event. Complete clinical response was obtained in22 cases (17 with low-to-intermediate Sokal scores), whereas

Fig. 1 G-banded and FISH evaluations of complex translocation. A, G-banded metaphase showing der(9), der(11), der(13), der(19), andder(22) chromosomes. B, Karyotype showing Ph′ chromosome and der(9), der(11), der(13), and der(19). C, FISH showing BCR/ABL fusionon chromosome 22, BCR translocation on chr(13), and ABL insertion on chr(11). D, Whole chromosome painting (WCP) showing t(11;19),t(13;22), and t(9;13). E, WCP showing t(11;19) on der(11) and der(19).
3Chronic-phase chronic myeloid leukemia
no response was observed in 8 patients (5 with high Sokalscores). Thus, the authors hypothesize that Sokal score playsa role in obtaining a response in patients in whom the Phchromosome occurs as a primary event [5].
Marzocchi et al [6], in their study of 30 patients with varianttranslocations, reported that the clinical characteristics ofpatients with variant translocations and outcomes as a result ofimatinib as a frontline therapy are similar to those with theclassical Ph′ translocation. Therefore, their data suggest thatpatients with variant translocations do not constitute a“warning” category in the imatinib era [6]. In contrast, anotherstudy performed by Stagno and colleagues [7] reportedcontradictory data. The results of that study suggested thatthe variants might confer an unfavorable clinical outcomebecause only 2 patients achieved an optimal response totyrosine kinase inhibitor (imatinib or nilotinib) treatment, of the
10 patients with CML carrying variant translocations among153 newly diagnosed CP cases [7]. The investigators assumedthat the involvement of additional chromosomes in the BCR/ABL rearrangement could adversely affect outcome when aselective tyrosine kinase inhibitor such as imatinib was usedbecause these genetic changes might be markers of genomicinstability and can be considered as clonal evolution [8].
The exact mechanism of formation of complex trans-locations is not completely known. However, complex trans-locations are reported to be inherently linked to the spatialarrangement of the involved chromosomes because theyrequire the physical interaction of the translocation partners.Studies on spatial rearrangement of chromosomes in thenucleus have shown that the position of chromosomes in thenucleus depends on the stage of the cell cycle. In interphase,at the beginning of the G1 phase, gene-rich chromosomes
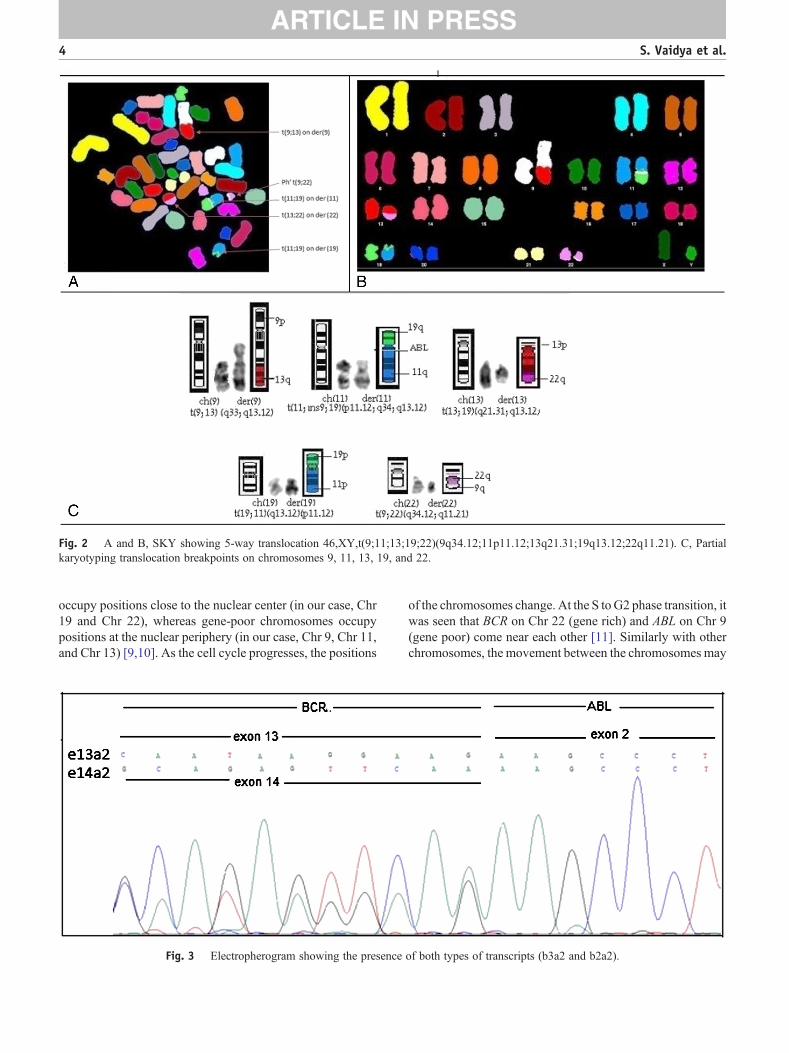
Fig. 2 A and B, SKY showing 5-way translocation 46,XY,t(9;11;13;19;22)(9q34.12;11p11.12;13q21.31;19q13.12;22q11.21). C, Partialkaryotyping translocation breakpoints on chromosomes 9, 11, 13, 19, and 22.
4 S. Vaidya et al.
occupy positions close to the nuclear center (in our case, Chr19 and Chr 22), whereas gene-poor chromosomes occupypositions at the nuclear periphery (in our case, Chr 9, Chr 11,and Chr 13) [9,10]. As the cell cycle progresses, the positions
Fig. 3 Electropherogram showing the presence
of the chromosomes change. At the S toG2 phase transition, itwas seen that BCR on Chr 22 (gene rich) and ABL on Chr 9(gene poor) come near each other [11]. Similarly with otherchromosomes, the movement between the chromosomes may
of both types of transcripts (b3a2 and b2a2).

5Chronic-phase chronic myeloid leukemia
facilitate the collision of individual genes and thus result ina complex translocation. Mechanisms such as illegitimateV(D)J or switch recombination, presence of repetitivesequences such as ALU sequences, and error-prone non-homologous end joining have been proposed to explain thetranslocation. There is a single Alu element in M-Bcr, andmore than 70% of breakpoints occur within a 3-kb regionencompassing that element. Alu sequences are also overrep-resented at sites of recombination in the ABL gene comparedwith their overall incidence throughout the genome.
Prognosis of patients having 5-way complex transloca-tions in response to drugs such as busulphan, carafate, andthyrolar in the pre–imatinib era was mixed [12–14]. In thepost–imatinib era, no significant difference was foundbetween patients with and patients without variant trans-locations [7,15,16].
In our case, good response to imatinib suggested that theoccurrence of the Ph′ chromosome was a primary event. Thecombination of GTG banding, FISH, and SKY revealed thepatient karyotype as 46,XY,t(9;11;13;19;22)(9q34.12;11p11.12;13q21.31;19q13.12;22q11.21). Two different trans-locations were observed on der(11), translocation of 19q andABL on 11q. To the best of our knowledge, such a translocationis not reported elsewhere. Sequencing analysis of the entirekinase domain, before the start of imatinib therapy, revealedthe presence of both types of transcripts, b3a2 and b2a2.
Coexpression of b2a2 and b3a2 is not a rare occurrence inCML and is supposed to be a result of alternative splicingmechanisms, a posttranscriptional modification. Studiesindicate no co-relation between the presence of varianttranscripts and clinical features and likelihood of treatmentresponse in CML [17]. However, such observations shouldbe monitored with caution because the types and levels oftranscripts change in the course of tyrosine kinase inhibitortreatment. Interestingly, 3 translocations on the der(11)chromosome were detected in our case. However, lack ofdata on the clinical outcome of the patients with 3 trans-locations on a single chromosome along with the presence ofboth types of transcripts, b3a2 and b2a2, leaves us cluelessabout the long-term response of the patient to imatinib.Moreover, our patient is reported to have a high Sokalscore, which might result in a poor outcome [8]. Thus,close long-term monitoring of such patients is advisable,not only for the reason that the therapy protocols can bemodified in CML but also for the in-depth understand-ing about the different markers that might lead to genomicinstability in other hematologic malignancies. This wouldmake it possible for us to draw parallel conclusions about thedifferent genetic aberrations and the response to the therapy.
References
[1] Shaffer LG, Slovak ML, Campbell LJ, editors. ISCN: An internationalsystem for human cytogenetic nomenclature. Basel, Switzerland: S.Karger; 2009.
[2] Heng HHQ, Liu G, Lu W, et al. Spectral karyotyping (SKY) of mousemeiotic chromosomes. Genome 2001;44:293-8.
[3] Azam M, Latek R, Daley G. Mechanisms of autoinhibition and STI-571/imatinib resistance revealed by mutagenesis of BCR-ABL. Cell2003;112:831-43.
[4] Yokota S, Nakamura Y, Bessho M. A novel five-way translocationt(7;11;9;22;9)(q22;q13;q11.2;q34) involving Ph chromosome in apatient of chronic myeloid leukemia: a case report. Mol Cytogenet2012;5:20.
[5] Zaccaria A, Testoni N, Valenti A, et al. Chromosome abnormalitiesadditional to the Philadelphia chromosome at the diagnosis of chronicmyelogenous leukemia: pathogenetic and prognostic implications.Cancer Genet Cytogenet 2010;199:76-80.
[6] Marzocchi G, Castagnetti F, Luatti S, et al. Variant Philadelphiatranslocations: molecular-cytogenetic characterization and prognosticinfluence on frontline imatinib therapy, a GIMEMAWorking Party onCML analysis. Blood 2011;117:6793-800.
[7] Stagno F, Vigneri P, Del Fabro V, et al. Influence of complex variantchromosomal translocations in chronic myeloid leukemia patientstreated with tyrosine kinase inhibitors. Acta Oncol 2010;49:506-8.
[8] Cortes JE, Talpaz M, Giles F, et al. Prognostic significance of cyto-genetic clonal evolution in patients with chronic myelogenous leuke-mia on imatinib mesylate therapy. Blood 2003;101:3794-800.
[9] Karen JM, Misteli T, Soutoglou E. Spatial genome organization in theformation of chromosomal translocations. Semin Cancer Biol 2007;17:80-90.
[10] Bridger JM, Boyle S, Kill IR, Bickmore WA. Re-modelling of nucleararchitecture in quiescent and senescent human fibroblasts. Curr Biol2000;10:149-52.
[11] Neves H, Ramos C, Gomes da Silva M, Parreira A, Parreira L. Thenuclear topography of ABL, BCR, PML, and RARA genes: evidencefor gene proximity in specific phases of the cell cycle and stages ofhematopoietic differentiation. Blood 1999;93:1197-207.
[12] Nakajima F, Takagi Tsuchiya K, et al. A five-way complex translocationin a patient with chronic myelocytic leukemia: t(4;18;13;9;22)(q12;q11.2;q14;q34;q11.2). Cancer Genet Cytogenet 1988;30:163-4.
[13] Potter AM, Watmore AE, Cooke P, Lilleyman JS, Sokol RJ.Significance of non-standard Philadelphia chromosome in chronicgranulocytic leukemia. Br J Cancer 1981;44:51.
[14] Young C, Di Benedetto J, Glasser Jr L, Mark HFL. A Philadelphiachromosome positive CML patient with a unique translocation studiedvia GTG-banding and fluorescence in situ hybridization. Cancer GenetCytogenet 1996;89:157-62.
[15] Achkar WA, Wafa A, Mkrtchyan H, Mooassass F, Liehr T. Novelcomplex translocation involving 5 different chromosomes in a chronicmyeloid leukemia with Philadelphia chromosome: a case report. MolCytogenet 2009;2:21.
[16] Lkuta K, Torimoto Y, Jimbo J, et al. A novel five-way chromosomaltranslocation observed in chronic myelogenous leukemia. CancerGenet Cytogenet 2008;183:69-71.
[17] Khorashad JS, Milojkovic D, Reid AG. Leukemia reflect alternativesplicing of ABL1 in normal variant isoforms of BCR-ABL1 in chronicmyelogenous. Mol Cancer Ther 2010;9:2152.





























