Embed Size (px)
Citation preview

Folia Psychiatrica et Neurologica Japonica, Vol. 19, No. 4, 1965
A NEW APPROACH TO THE TREATMENT OF GLOSSO- PHARYNGEAL NEURALGIA, USING THE GREAT
AURICULAR NERVE BLOCK
BY Hideo AOKI and Yuko TOKUNAOA
From the Second Surgical Division, Yamaguchi University Medical School
Facial neuralgia was divided into two groups by Frazier and Russelll). The first was typical neuralgia or trigeminal neuralgia. The second was the atypical group. In this classification glossopharyngeal neuralgia is included in the latter group. But it is a disease similar to trigeminal neuralgia except that the pain usually starts from the pharyngeal region and sometimes radiates to the ear. Glossopharyngeal neuralgia of the symptomatic type was first described by Weisenburg in 191039), and a paroxysmal or idiopathic type of pain localized in the tonsillar region was reported in 1920 by Sicard and R ~ b i n e a u ~ ~ ) and in 1921 by Harris5tZ5). Since these reports the designation “glossopharyngeal neuralgia” has been generally accepted, but some authors have described this disease in other terms: glossopharyngeal ti&), geniculate ganglion n e ~ r a l g i a ~ ~ o ~ ~ ) and tympanic plexus n e ~ r a l g i a ~ ~ ~ 0 ) .
In the treatment of this disease the section of the ninth cranial nerve, the inferior cervical sympathetic ganglion and the pharyngeal branches of the vagal nerve in the neck was reported by Sicard and R ~ b i n e a u ~ ~ ) . Extracranial section of the ninth nerve was performed by Adson (1924)l), but the recurrence of the pain was observed. Then he performed an intracranial section, which was carried out in 1925 but not reported by Love until 19445). Therefore, the first report of intracranial section of this nerve was described by Fay in 19261°) and Dandy in 19279). Thereafter, this procedure has been generally accepted as the preferred method of treating this disease. On the other hand, a great auricular neurotomy or anesthetic block of this nerve was performed by Mason”) as a treatment of tic douloureux in 1953. In our clinic this procedure has been carried out on various types of chronic headache, such as post-traumatic headache, atypical facial neuralgia etc. since 1955, and generally in about 80 per cent of cases relief of the pain has been observed2s3). Two cases of glossopharyngeal neuralgia (oropharyngeal type) were included in our series and in both cases we were successful in relieving pain by anesthetic block and section of the great auricular nerve respectively. No recurrence has been observed for 5 and 3 years since the treatment.
CASE REPORT
CASE 1: K. H., male, aged 57, had suffered from severe paroxysmal attacks The attack of lancinating pain in the right pharyngeal region, for about 6 months.
Received for publication Sept. 4, 1965

A New Approach to the Treatment of Glossopharyngeal Neuralgia 347
had been precipitated by the movements involved in talkins or swellowing. The duration of the pain was about 10 to 20 seconds, but in the intervals between the attacks he sometimes complained of dull pain or discomfort in the throat, and some- times was completely free of pain. In spite of every kind of treatment, excluding the glossopharyngeal neurotomy, this intractzble condition remained unrelieved and because of the pain he could not eat for the last 10 days prior t o the treatment.
On July 20, 1960, a block of the right great auricular nerve with 2 per cent xylocaine (Lidocaine hydrochloride) was performed in the superficial layer of t h e right side of the neck, according to Mason’s d e s c r i p t i ~ n ~ . ~ ? ~ ~ ) . A few minutes after the injection the patient’s expression became relaxed and he could talk and swallow at will without pain. Though a mild attack appeared a few hours after the block, he still could talk and eat. The second and third block of the same nerve were done in the same manner on the following two days. Thereafter, the neuralgia disappeared completely 2nd no recurrence of the pain has been observed in the 5 years following the block.
The anesthetic block of the great auricular nerve in the neck successfullv relieved the pain due to glossopharyngeal neuralgia. This excellent result was not expected previously. The anesthetic agent was injected into the layer between the platisma and sternocleidomastoid muscle, in which the great auricular nerve runs. However, since the ninth cranial nerve runs in the deep layer under the neck muscles, the effect of the anesthetic may not reach to this nerve. A section of the great auricular nerve was performed on the second case for the purpose of elimination of the ninth nerve from the effect of anesthetics and clarifying the role of the great auricular nerve in the treatment of glossopharyngeal neuralgia.
COMMENT.
CASE 2: Y. K., male, aged 63, complained of paroxysmal attacks of stabbing or burning pain in the right side of the pharynx about 3 years prior to admission on January 10, 1963. The condition usually worsened in the winter and was improved in the warmer season. Since last October, three months prior to admission, h e complained of attacks about 30 times a day and the degree advanced progressively. The pain lasted for about 30 seconds and was referred to the mental region. T h e attacks were induced by swallowing or talking. An anesthetic block of the great auricular nerve with 2 per cent xylocaine was carried out. Relief of the pain W ~ S
observed but there was a recurrence about 2 hours after the block. This result was the same as that experienced in case I .
The day after the operation, the pain which had been complained of preoperatively disappeared com- pletely. However, a mild aching pain of about 30 seconds duration several times a day, appeared in front of the ear, this pain had not been observed in the patient’s preoperative course. This pain was thought to be the so-called “otitic” type of glossopharyngeal neuralgia5). Therefore, the oropharyngeal type of this disease changed to the otitic type following the operation. An anesthetic block of the upper branch of the great auricular nerve was then carried out in the infra-auricular region. In this procedure the tip of the injected needle was inserted beneath the platisma. Pain no longer appeared after several instances of this blocking. H e was discharged in satisfactory condition on the 10th postoperative day and n o recurrence has been observd in the 3 years following the operation.
In this case a great auricular neurotomy was carried out.

348 H. Aoki and Y. Tokunaga
COMMENT. In the second case, the otitic type of pain was observed after the great auricular neurotomy, but not complained of preoperatively. The appearance of the otitic pain may be due to the integration of the upper branch of the great auricular nerve during the operation, because this condition was treated completely by the infiltration of anesthetics into the superficial layer of the infra-auricular region. Therefore, the great auricular nerve block should be applied in the otitic type of this disease. It was very interesting that glossopharyngeal neuralgia was treated successfully by the procedure above mentioned. The following experiment was carried out by one of us (Y. T.) in order to eluciate the mechanism of this treatment.
EXPERIMENTAL STUDY
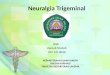
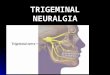
The cervical sensory nerves C11 and C1 11 were dissected and sectioned in the neck of a dog. The animal was sacrificed one week after the operation and degene- rated nerve fibers were sought histologically in the pharyngeal region. The nerve fibers were stained by Birshowsky’s method modified by Suzuki. The degenerative nerve fibers, almost unmyelinated, were found numerously in the posterior and lateral wall of the pharynx (Fig. 1, 2) . These fibers penetrated the lamina muscularis miiicosa and terminated in the epithelial layer of the pharyngeal mucous membrane as free endings. From this result it was demonstrated that the sensory nerve from the upper cervical segment was distributed in the pharyngeal wall. In other words, a part of the afferent impulse from the pharynx was carried to the cortex via the cervical sensory nerve. Therefore, the peripheral overlap over the ninth cranial nerve and the upper cervical nerves in the pharynx was proved by our experimental study.
h’Fig. 1. Degenerated nerve fiber was found in the lateral wall of the pharynx. x200.

A New Approach to the Treatment of Glossopharyngeal Neuralgia 349
Fig. 2. Degenerated nerve fiber was found in the submucous layer of posterior wall of the pharynx. x800.
DISCUSSION
Glossopharyngeal neuralgia is a rare disease. The incidence of this disease t o trigeminal neuralgia is reported approximately one to one h ~ n d r e d 5 . q ~ ~ ) or one to fofty2YJ1). In our country the report of this disease has been published only by Kitamura el and Kudo et aLZ5) reported 6 cases of this disease at the 3rd annual meeting of the Japan Neurological Society. Therefore, in general, this disease has not been widely described. It is though t o be the first step for the correct diagnosis that we must keep in mind about this disease.
Ordinarily this disease is characterized by paroxysmal attacks of severe pain, usually starting in the tonsillar region or at the base of the tongue and frequently radiating to the ear, and being precipitated by eating, talking, swallowing or by the movement of the pharynx and tongue. The character of the pain is most commonly described as "burning", "lancinating", and less frequently as "stabbing", or "cutting". From the point of view of pain onset the disease may, for the sake of convenience, be divided into two groups as it was by Bohm5). The criterion of the two groups is described as follows.
A. 0titic.-Pain in and around the ear. ( I) ( 2 ) ( 3 ) External auditory canal. (4 ) Mzstoid region. ( 5 ) Combination of I to 4.
( I ) Side or back of pharynx. ( 2 ) Tongue (posterior one-third).
Deep in the ear. In front of the ear.
B. Oropharyngeal.

350 H. Aoki and Y. Tokunaga
(3) Fauces. (4 ) Tonsil. ( 5 ) Soft palate. (6) Combination of 1 to 5 .
Some authors described the former as plexus tympanicus neuralgia or geniculate ganglion n e ~ r a l g i a ~ 4 * * ~ ~ .
Glossopharyngeal neuralgia associated with disturbances of the caridiac and cerebrovascular function is a rarer disorder2*.*9J1). In 1964 Kong et al.") collected 16 patients from the literature and in addition reported their own case. It is charac- terized by paroxysms of neuralgic pain in the throat and neck accompanied by brady- cardia or asystole. hypotension, syncompe, and sometimes seizure. But no case of this type has been reported in our country.
In the treatment of glossopharyngeal neuralgia, a tractotomy of the spinal trigeminal nuclei in the first cervical segment was reported by B ~ e s " ~ ) . This pro- cedure has not been generally accepted for fear of the possible occurrence of severe complications, though its logical ground is very interesting. lntracrdnial section of the ninth and a part of the tenth cranial nerve has been the most useful procedure, therefore the operation on the peripheral cervical sensory nerve has not been performed in this field. The anesthetic block and section of the great auricular nerve carried out by us is the first report of this method to the treatment of this disease. Anesthetic block of the right ninth cranial nerve in the area of the jugular foramen was attempted by Kong et aI.**). They observed the development of a transient right facial weakness, paralysis of the VII. X and XI1 cranial nerves as well. The attacks of pain were abolished completely for the period of an hour but when the effect of the anesthetics wore off, the pain recurred as previously observed. This observation closely resembled our experience. In our cases the psin disappeared following the anesthetic block of the great auricular nerve, and several hours later the pain attack recurred though its intensity was decreased and the pain free interval became longer than in the preoperative state. Moreover, complete release of the pain was observed in case 1 after three application of this nerve block. The most outstanding difference between Kong's observation and ours is that the object of the nerve block was the cranial nerve in the former, while it was the cervical nerve in the latter.
On the other hand, much of interest has been published about the functional correlation of the upper cervical roots with headache and facial pain4.1".'6.1s.20,21.26).
Patrickaa) in 1918, described head pain originating in the cervical roots and radiating toward the frontal areas of the head. In 1939, Cyriax showed that an injection of hypertonic saline into the suboccipital region produced pain in the forehead20'. This relationship between the fifth cranial nerve and the upper cervical nerves has been wcll known as the great occipital trigeminus syndrome (GOTS)34). A procaine injection in the cervical region for the treatment of headache was carried out by Jones and Brown'7). In our country, the post-traumatic GOTS type of headache was studied electromyographycally by Asano et aL4) and a hypertonic saline or procaine solution was injected into the upper cervical paravertebral tissue for the treatment of this condition16). Among the cervical nerves the great occipical nerv: is the most interesting one as mentioned above, but the great auricular nerve appears to receive scant attention until Mason's report24). He described that the posterior

A New Approach to the Treatment of Glossopharyngeal Neuralgia 351
branch of the great auricular nerve joins to the posterior auricular branch of the facial nerve and communicates with the auricular branch of the vagus. A commu- nication from the cervical plexus joins the hypoglossal nerve and with it passes into the tongue in which it communicates with the lingual nerve. In addition, the d-escending tract of the fifth nerve lies in the third or fourth segment of the cord18JflW. Hence, all pain impulses in the head and neck eventually pass into the upper four cervical segment.
In 1954 Campbell and Lloid8) reported as follows: “we tried the Mason’s operation in several cases of true trigeminal neuralgia but were not able to convince ourselves of any improvement.” They, however, found dramatic relief of pain in the case of atypical facial neuralgia by using the anesthetic block of this nerve. Penman and Walsh27) reported that great auricular neurotomy had no effect on tic douloureux and the same result was observed by us293). In our opinion this procedure may be applied to the patient complaining of pain in the temporal or periauricular area. In our clinic various types of chronic headache, atypical facial pain, migraine, headache due to hypertension, post-traumatic headache, tension headache etc. were treated by this procedure and in about 80 per cent of the cases pain was successfully relieved.
The mechanism of the effect of this procedure on glossopharyngeal neuralgia is not completely clear, but the site of the effect may be divided into two parts: peripheral and central.
1. Peripheral overlap of the pain sensation in the pharyngeal region. Pain in the pharyngeal region may be transmitted to the cortex mainly via the
ninth and tenth cranial nerves. Sensory changes in the pharyngeal region after the intracranial section of the ninth nerve were studied by Uihlein et al.3s). In sixty- one patients with glossopharyngeal neuralgia intracranial section- of the ninth nerve was carried out. No objective sensory loss in the posterior part of the pharynx was detected postoperatively in 35 cases. There was a definite sensory deficit in 20 cases. In one of our patients (the second case) , slight hypoesthesia was detected postoperatively in the pharynx while the first one was not examined. This variation of the postoperative sensory change in the pharyngeal wall may be due to the peripheral overlap between the ninth cranial nerve and the upper cervical nerves.
General visceral afferent fibers of the glossopharyngeal nerve conduct sensation from the pharynx and posterior third of the tongue to the nucleus solitarius12). According to our clinical and experimental results together with this description, one of the action points of the great auricular nerve block is thought to be in the peripheral block of a part of the sensory conduction from the pharyngeal wall. In this point we agree with Bohm’s opinion that the pain overflow into the ajacent trigeminal and cervical segment in glossopharyngeal neuralgia is almost certainly a peripheral effect and not central through the descending tract of the fifth nerve5). But in the otitic type of this disease it may be considered that not only Peripheral overlap but the central connection between the cranial and cervical nerves is involved in the mechanism.
2.
Six were not tested postoperatively.
Central correlation between the cranial and cervical nerves. The general sommatic afferent fibers of the glossopharyngeal nerve conduct

352 H. Aoki and Y. Tokunaga
pain from the external ear into the spinal nucleus of the trigeminal nerve12), extend- ing to the third segment in catsla) and spreading down to the fourth segment in dogs3'), man and monkeys3e). Moreover, Kerrm) concluded that observation of the spinal tract of the fifth nerve had its relation to the cervical dorsal roots of cervical nerves one to three in the cat showed clear-cut areas of anatomic overlap of these two afferent systems in the dorsal horn at the first and second cervical levels. Nearly the same observation was demonstrated by one of us3?). Fibers from the glosso- pharyngeal nerve to the spinal trigeminal nucleus as mentioned above were identified in the dorsal horn of the first and second cervical segmentl9). Therefore, an anatomical connection between the ninth cranial nerve and the cervical sensory nerves may exist in the upper cervical segment. The correlation of the cranial and cervical nerves in the central nervous system may be seen not only in the spinal cord but also in the supranuclear region. However, anatomical and physiological explora- tion has not yet fully developed, and many interesting problems remain unsolved.
SUMMARY
Two cases of glossopharyngeal neuralgia (oropharyngeal type) were treated suc- cessfully by means of either anesthetic block or section of the great auricular nerve respectively. Pain was relieved completely and no recurrence has been observed for the 5 and 3 years following the treatment.
The intracranial section of the ninth cranial nerve has been thought to be the preferred method of treating this disease. The great auricular nerve block was introduced by us in this field and two sites of the effect of this treatment were clarified by the clinical and experimental studies: ( 1 ) the peripheral sensory overlap over the upper cervical nerves and the ninth cranial nerve was demonstrated in the pharyngeal region, and (2) intraspinal connection of these nerves might exist in the upper cervical segment. Therefore, it was revealed that the nerves relating to the mechanism of the pain in this disease were not only the ninth cranial nerve but also the upper cervical nerves.
In our opinion all cases of glossopharyngeal neuralgia should be treated by this procedure at first, because of the following reasons: (1) simplicity of the method, (2) no side effect is observed and (3) the effect of this treatment can be estimated confidently to occur several minutes after the nerve block. Therefore, more com- plicated treatment should be applied to the case without any favorable effect follow- ing this procedure.
REFERENCES
1) Adson. A. W.: Surgical treatment of glossopharyngeal neuralgia. Arch. Neurol. & Psychiat. 12: 487, 1924.
2) Aoki, H.: Great auricular neurotomy for headache (in Japanese). Brain and Nerve. 12: 135, 1960.
3 ) Aoki, H. and Tokunaga, Y.: Great auricular nerve block in the headache (in Japa- nese). J. Therap. 44: 808, 1962
4) Asano, Y., Matsunaga, H. and Hirata, M.: A contribution to the differential diagnosis in the posttraumatic headache (in Japanese). Saishin Igaku. 14: 3473, 1959.
5) Bohm, H. and Strang, R. R.: Glossopharyngeal neuralgia. Brain, 85: 371, 1962.

A New Approach to the Treatment of Glossopharyngeal Neuralgia 353
6 ) Bues, E.: Tic douloureux des Nervus facialis, Studie zum Problem des Tic douloureux. Deutsche Ztschr. Nervenheil. 168: 142, 1962.
7) Bues, E. : Tractotomie bei Glossopharyngeus und Facialis-Neuralgie. Acta Neurochir. 3: 38, 1952.
8 ) Campbell, A. M. G. and Lloid, J. K.: Atypical facial pain. Lancet. 269: 1034, 1954. 9) Dandy, W. E.: Glossopharyngeal neuralgia (Tic douloureux) Its diagnosis and
treatment. Arch. Surg. 15: 198, 1927. 10) Fay, T. : Intracranial division of glossopharyngeal nerve combined with cervical
rhizotomy for pain in inoperable carcinoma of the throat. Ann. Surg. 84: 456, 1926. 11) Frazier, F. H. and Russel, E. LL.: Neuralgia of the face: Analysis of seven hundred
and fifty four cases with relation to pain and other sensory phenomena before and after operation. Arch. Neurol. & Psychiat. 11: 557, 1924.
12) Friedman, A. P. and Merritt, H. H.: Headache, Diagnosis and treatment. Davis Co, Philadelphia, 1'959, p. 327.
13) Glaser, M. A.: Atypical facial neuralgia. Arch. Int. Med. 65: 340, 1940. 145 Heidrich, R., Calus, R. U. u. Stojanow, W.: Zum Problem der Plexus Tympankus
Neuralgie. Dtsch. A. Nervenheil. 184: 419, 1961. 15) Hunter, L. R. and Meyfield, F. H.: Role of upper cervical roots in productitn of
pain in head. Am. J. Surg. 78: 743, 1949. 16) Ishii, S., Tani, E., Kondo, H. and Waga, S.: Clinics and therapy of cervical syndrome
(in Japanese). Surg. Therapy. 6: 393, 1962. 17) Jones, 0. W. Jr. and Brown, H. A.: Treatment of post-traumatic head pain. J. Neurol.
& Ment. Dis. 99: 668, 194.4. 18) Kerr, F. W. L.: Structural relation of the trigeminal spinal tract to upper cervical
roots and the solitary nucleus in the cat. Experimental Neurol. 4: 134, 1961. 19) Kerr. F. W. L.: Facial, vagal and glossopharyngeal nerves in the cat. Arch. Neurol.
6: 24, 1962. 20) Kerr, F. W. L.: Mechanism, diagnosis and management of some cranial and facial
pain syndrome. Surg. Clin. North Am. 43: 951, 1963. 21) Kitamura, K., Asakura, T., Maruoka, M. and Miyazato, Y.: A case report of glosso-
pharyngeal neuralgia, coexistent multiple diverticles of intestine and colon. (in Japa- nese). Rinsho Geka. 13: 1171, 1958.
22) Kong, Y., Heyman, A.. Entman, M. L. and McIntosch, H. D.: Glossopharyngeal neuralgia associated with bradycardia, syncope, and seizures. Circulation 30: 109, 1964.
23) Kudo, T., Masuda, K., Hirai, H. and Totani, S.: Glossopharyngeal neuralgia (in Japanese). Clinical Neurol. 2: 184, 1962.
24) Mason, R. W.: The nature of tic douloureux, Treatment by alcoholic block or section of the great auricular nerve. Brit. Med. J. No. 48128: 119, 1953.
25) Olivecrona, H. und Tonis, W.: Handbuch der Neurochirurugie. Bd. VI. s. 52. Springer Verlag, Berlin, 1957.
26) Patrick, H. T.: 27) _Penman, J. and Walsh, L. S.: Great auricular neurotomy for tic douloureux. A con-
28) The use of cervical plexus block in the diagnosis
29) Ray, B. S. and Stewart, H. J.: Glossopharyngeal neuralgia. A case report of cardiac
30) Reichert, F. L.: Tympanic plexus neuralgia. J.A.M.A. 100: 1744, 1933. 31) Glossopharyngeal neuralgia with syncompe and
32) Sakamoto, H. and Tanaka, K.: Headache (in Japanese). Igakushoin, Tokyo, 1933. 33) Sicard, J. A. et Robineau: Communications et presentation. I. Algie velopharyngke
Induration on or rheumatic headache. J.A.M.A. 71: 82, 1918.
trolled clinical trial. Brit. Med. J. 5009: 22, 1957. Pentecost, P. S. and Adriani, J.: and treatment of atypical cephalagia of cervical origin. Anesthesiol. 16: 726, 1955.
arrest. Am. Heart J. 35: 458, 1948.
Richburg, P. L. and Kerm, L. E.: convulsioas. J.A.M.A. 152: 703, 1955.

354 H. Aoki and Y. Tokunaga
essentielle. Traitment chirurugical. Revue neur. 34: 256, 1920. (sited by Olivecrona) . 34) Skillern, P. G.: Great occipital trigeminus syndrome as revealed by induction of
block. Arch. Neurol. & Psychiat. 72: 335, 1954. 35 ) Smith, G. W.: Diagnosis and treatment of facial pain. J.A.M.A. 166: 857, 1958. 36) Taren, J. A. and Kahm, E. A,: Anatomic pathways related to pain in face and neck.
J. Neurosurg. 19: 116, 1962. 37) Tokunaga, Y.: to be published. 38) Uihlein, A., Love, I. G. and Corbin, K. B.: Intracranial section of the glossopharyngeal
nerve. Arch. Surg. 74: 320, 1955. 39) Weisenburg, T. H.: Cerebello-pontine tumor diagnosed for six years as tic douloureux.
The symptoms of irritation of the ninth and tenth cranial nerves. J.A.M.A. 54: 1600, 1910.
40) Wolf€, H. G.: Headache and other bead pain. Oxford University Press, New York, 1950.