Embed Size (px)
Citation preview

Research study
Page 1 of 5
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
For citation purposes: Choudhury PR, Sarda P, Baruah P, Singh S. A magnetic resonance imaging study of congenital Chiari malformations. OA Case Reports 2013 Aug 08;2(8):73. Co
mpe
ting
inte
rest
s: n
one
decl
ared
. Con
flict
of i
nter
ests
: non
e de
clar
ed.
All a
utho
rs c
ontr
ibut
ed to
the
conc
eptio
n, d
esig
n, a
nd p
repa
ratio
n of
the
man
uscr
ipt,
as w
ell a
s rea
d an
d ap
prov
ed th
e fin
al m
anus
crip
t.Al
l aut
hors
abi
de b
y th
e As
soci
ation
for M
edic
al E
thic
s (AM
E) e
thic
al ru
les o
f disc
losu
re.
A magnetic resonance imaging study of congenital Chiari malformations
PR Choudhury1*, P Sarda2, P Baruah1, S Singh3
ConclusionThe magnetic resonance imaging technique gives better visualisation of Chiari malformations and thus this entity has rapidly evolved over the past decade.
Introduction A complex range of anomalies of the hindbrain formation appearing at various stages of growth and devel-opment of the central nervous sys-tem are included under the group called Chiari malformations. Chiari malformation is the most common anomaly of the craniovertebral junc-tion involving both the skeletal as well as the neural structures1.
Professor Chiari first described the abnormalities that we now refer to as Chiari malformations around 1890. His observations were all made on stillborn babies or newborns, and he classified the abnormalities by the severity of tonsillar and cerebellar descent as type 1 being the least and type 4 the most severe2.
The incidence of Chiari type 1 malformation by neuroimaging tech-niques range from 0.1 to 1%3 and it is least obvious clinically and may not be diagnosed until adult life. It con-sists of tonsillar herniation through the foramen magnum with or with-out varying degrees of elongation of the medulla oblongata and fourth ventricle. Chiari type 2 is virtually always with thoracolumbar mye-lomeningocele and associated with caudal herniation of medulla, vermis and the fourth ventricle4. Chiari types 3 and 4 have the major deformi-ties with cerebellar hypoplasia and downward displacement of the brain stem and a high cervical or occipital encephalocele4.
Today, we have a much clearer understanding of these conditions due to the advent of magnetic reso-nance imaging (MRI) scanning2. As a result, this entity has rapidly evolved over the past decade with newer visualisation techniques, thus pos-ing new challenges to diagnosis and management1. The aim of this work was to study an MRI study of congen-ital Chiari malformations.
Materials and methodsThe study is based on the cases referred to the Department of Radi-ology for MRI from Departments of Neurology and Paediatric surgery with common symptoms of headache, swallowing problems, dizziness, nys-tagmus, etc. Informed consent of the patients and their attendants were taken. The study was approved by the Institutional Ethics Committee of the Medical College and Hospital, where the study was carried out.
Altogether 45 cases were consid-ered for the study. The cases were classified into three groups as ‘A’, ‘B’ and ‘C’, according to Chiari type 1, 2 and 3, respectively (shown in Table 1).
The readings and evaluations were made by professors, demon-strators and postgraduate trainees
Abstract IntroductionChiari malformations are develop-mental anomalies with the hernia-tion of the brainstem medulla and the cerebellar tonsils and vermis through the foramen magnum. The patients manifest with headache, neck pain, progressive scoliosis and cerebellar dysfunction due to cervico-medullary compression. These malformations range from the simpler to the more complex varieties of presentation, signifying their stages of appearance during embryological differentia-tion and development. The aim was to study various types of Chiari mal-formations with the help of magnetic resonance imaging techniques. Materials and methodsIn this study, 45 cases of Chiari mal-formations were considered.ResultsAmong 45 cases, 37, 6 and 2 were type 1, 2 and 3 Chiari malformations, respectively. 53.33% cases were male and rest were female cases. The hydrocephalus and syringomyelia were present in 28.89% and 48.89% of cases, respectively. Length of her-niated cerebeller tonsil in 56.76% cases of type 1 Chiari malformations are in between 10 mm and less than 20 mm.
*Corresponding authorEmails: [email protected]; prabahita [email protected] Department of Anatomy, Fakhruddin Ali
Ahmed Medical College, Barpeta, Assam, India
2 Department of Radiology, Gauhati Medical College, Guwahati, Assam, India
3 Department of Radiology, B. Borooah Cancer Institute, Gopinath nagar, Guwahati, Assam, India
Radi
olog
y
Table 1 Different types of Chiari malformations with their number and percentage
GroupsNumber of cases
Percentage (out of 45)
Group A 37 82.22Group B 6 13.33Group C 2 4.45Total 45 100

Research study
Page 2 of 5
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
For citation purposes: Choudhury PR, Sarda P, Baruah P, Singh S. A magnetic resonance imaging study of congenital Chiari malformations. OA Case Reports 2013 Aug 08;2(8):73.
of Department of Radiology and Anatomy with 3–10 years of experi-ence. The study was conducted from January 2008 to December 2012.
The data obtained from the MRI studies of 45 cases were tabulated, compared and calculated. The rela-tive frequencies were calculated and p value was evaluated with the help of Student’s t-test probabilities.
ResultsThere were 24 males with a percent-age of 53.33 out of 45 total cases and the rest were female. Distributions of male and female in different groups A, B and C (Figure 1) with percent-ages, mean, standard deviations and standard error of mean are shown in Table 2.
It can be concluded from Table 3 and Figure 2 that the maximum num-ber of cases in groups A and B are in between the age groups of 15 years to less than 20 years and less than 5 years, respectively.
Relative frequency of Chiari mal-formations in between groups ‘A’, ‘B’ and ‘C’ can be studied from Table 4 and Figure 3.
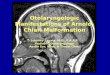
The hydrocephalus and syrin-gomyelia (syringomyelia shown in Figure 4) are present in 28.89% (13 out of 45 cases) and 48.89% (22 out of 45 cases) of cases, respectively, which can be con-cluded from Table 5. Lumbosacral meningomyelocele is found to be
Table 2 Number and percentage of male and female cases for groups ‘A’, ‘B’ and ‘C’
GroupsMale Female
Number of cases
Percentage(out of 24)
Number of cases
Percentage(out of 21)
Group A 20 83.33 17 80.95Group B 3 12.5 3 14.29Group C 1 4.17 1 4.76Sum 24 100 21 100Mean 8 33.33 7 33.33SD ±10.44 ±43.498 ±8.718 ±41.512SEM ±6.028 ±25.114 ±5.033 ±23.967SD, standard deviation; SEM, standard error of mean
Table 3 Number of cases in different ages for the groups A, B and C
Age groups (years)Groups
Group A Group B Group C
Less than 5 2 5 15 to <10 5 0 110 to <15 6 0 015 to <20 7 0 020 to <25 6 0 025 to <30 5 0 030 to <35 4 0 035 to <40 2 0 040 and above 0 1 0Sum 37 6 2Mean 4.11 0.667 0.222SD ±2.315 ±1.658 ±0.4410SEM ±0.7718 ±0.5528 ±0.1470SD, standard deviation; SEM, standard error of mean
Figure 1: Different types of Chiari malformations according to sex.
present in all the cases of type 2 Chiari malformations.
Length of herniated cerebel-ler tonsil (shown in Figure 4) in 56.76% (21 out of 37 cases) cases of type 1 Chiari malformations are in between 10 and less than 20 mm (Table 6). The smallest length of cerebeller tonsil in type I Chiari malformation is 5.2 mm and longest being 28 mm.
The level of significance of differences of Chiari malformations between

Research study
Page 3 of 5
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
For citation purposes: Choudhury PR, Sarda P, Baruah P, Singh S. A magnetic resonance imaging study of congenital Chiari malformations. OA Case Reports 2013 Aug 08;2(8):73.
Table 4 Distribution of frequency and relative frequency of Chiari malformations in groups ‘A’, ‘B’ and ‘C’
Class interval (years)
Group A Group B Group C
Simple frequency (f)
Relative frequency (fr)
Simple frequency (f)
Relative frequency (fr)
Simple frequency (f)
Relative frequency (fr)
Less than 5 2 0.054 5 0.833 1 0.55 to <10 5 0.136 0 0 1 0.510 to <15 6 0.162 0 0 0 015 to <20 7 0.189 0 0 0 020 to <25 6 0.162 0 0 0 025 to <30 5 0.135 0 0 0 030 to <35 4 0.108 0 0 0 035 to <40 2 0.054 0 0 0 040 and above 0 0 1 0.167 0 0Sum 37 1.00 6 1.00 2 1.00
Figure 2: Different types of Chiari malformations in different age groups.
Figure 3: Relative frequency of groups ‘A’, ‘B’ and ‘C’.
male and females is not significant (p = >0.05) whereas that of groups A and B, and groups A and C accord-ing to age groups is very significant (p = <0.01) and very highly significant (p = <0.001), respectively (Table 7).
Discussion Arnold–Chiari malformation is a com-plex syndrome in which the brain-stem medulla, and the cerebellar
Figure 4: Magnetic resonance imag-ing showing tonsiller herniation (indicated by red arrow) and syrin-gomyelia (indicated by white arrow).

Research study
Page 4 of 5
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
For citation purposes: Choudhury PR, Sarda P, Baruah P, Singh S. A magnetic resonance imaging study of congenital Chiari malformations. OA Case Reports 2013 Aug 08;2(8):73.
Table 7 The level of significance of differences of Chiari malformations in dif-ferent groups
Serial number
Comparisons of cases of Chiari malformations between
‘t’ p value
1 Male and Female 0.1273 >0.05
2 Group A and B according to age groups 3.628 <0.01
3 Group A and C according to age groups 4.950 <0.001
4 Group B and C according to age groups 0.7770 >0.05
5 Presence and absence of hydrocephalus 0.7027 >0.05
6 Presence and absence of syringomyelia 0.04203 >0.05
tonsils and vermis herniate through-out the foramen magnum5.
The Chiari malformation is classi-fied into four types. Type 1 is the most commonly seen clinical entity and characterised by tonsillar herniation greater than 5 mm below the formen magnum. Syringomyelia is common with type 1 Chiari malformations1. In this study, 82.22% cases fall into type 1 category which also contains the maximum number of syringomy-elia cases (Table 5).
Type 2 Chiari malformation is characterised by caudal descent of cerebellar vermis along with the brainstem and fourth ventricle. This type of Chiari malformation is associated with myelomenin-gocele. Presence of hydrocephalus is a common finding in this type1. In this study, 50% cases of type 2 is associated with hydrocephalus (Table 5). Type 3 is the rarest and most severe form, characterised by occipital or high cervical encepha-locele containing herniated cere-bellar or brainstem tissue. Marked
Table 6 Length of herniated cerebeller tonsils in type 1 Chiari malformations
Length of herniated cerebeller tonsil in mm
Type 1 Chiari malforma-
tions
5 to <10 1110 to <20 2120 to <30 530 and above 0Total 37
Table 5 Presence and absence of hydrocephalus and syringomyelia in groups ‘A’, ‘B’ and ‘C’
Type of Arnold–Chiari malformations
Presence of hydrocephalus
Presence of syringomyelia
Absence of hydrocephalus
Absence of syringomyelia
Group A 9 19 28 18Group B 3 1 3 5Group C 1 2 1 0Total 13 22 32 23
cerebeller hypoplasia or aplasia is the main feature of type 4 Chiari malformation1.
A discussion of the modern theo-ries describing the aetiology of the congenital Chiari malformations begins with Gardner’s work6. The ‘hydrodynamic theory’ relates the development of tonsillar herniation and other dysraphic states to disor-dered embryogenesis in and around the foetal hindbrain. The initial insult is the failure of pathways for cerebro-spinal fluid egress from the embryo-logical fourth ventricle to open normally at the foramina of Luschka and Magendie. This blockage at the normal exits of the fourth ventricle results in increased pressure. The cerebellar tonsils migrate caudally in response to this pressure gradi-ent, causing the hallmark finding of crowding of the foramen magnum. This elevated pressure can also be transmitted through the obex to the spinal cord and continued pressure allows for persistence or dilatation of the central canal of the spinal
cord, resulting in the formation of hvdromyelic cavity7.
According to Alden et al.8, the exact origin of Chiari type 1 malformation is unknown; however, it appears to be caused by a mismatch between the volume of the posterior fossa neural elements and the posterior fossa cra-nial content. Several theories have been proposed to describe the result-ant pathophysiology of this mismatch. It is clear, however, that abnormal cerebrospinal fluid flow and velocity play a role in the symptoms and signs associated with this disorder8.
The common symptoms related to Chiari malformation are head-ache, particularly precipitated by coughing, straining, sneezing, etc. (Valsalva maneuvers), dizziness, eye symptoms, most commonly nystag-mus, swallowing problems, and sleep disturbances2.
Type 1 Chiari malformations has been described in association with many different genetic disorders of established inheritance patterns, including Klippel–Feil syndrome,

Research study
Page 5 of 5
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
For citation purposes: Choudhury PR, Sarda P, Baruah P, Singh S. A magnetic resonance imaging study of congenital Chiari malformations. OA Case Reports 2013 Aug 08;2(8):73.
reformatted computed tomography can define accurately the surgical anatomy and aid in surgical planning.
References 1. Vannemreddy P, Nourbakhsh A, Willis B, Guthikonda B. Congenital Chiari malformations. J Neurol Soc India. 2010 Mar;58(1):6–14.2. Batzdorf U. Chiari I malformation with syringomyelia. Evaluation of surgical therapy by magnetic resonance imaging. J Neurosurg. 1988 May;68(5):726–30.3. Meadows J, Kraut M, Guarnieri M, Haroun RI, Carson BS. Asymptomatic Chiari type I malformations identified on magnetic resonance imaging. J Neuro-surg. 2000 Jun;92(6):920–6.4. Sutton D, Stevens J, Miszkiel K. Intrac-ranial lesions (1). In: Sutton D, editor. Text book of radiology and imaging 7th ed. Noida, U.P (India): Elsevier; 2009.p1728.
5. Zollty P, Sanders MH, Pollack IF. Chiari malformation and sleep-disorder breathing: a review of diagnostic man-agement issues. Sleep. 2000 Aug;23(5): 637–43.6. Gardner WJ. Hydrodynamic mecha-nism of syringomyelia: its relation-ship to myelocele. J Neurol Neurosurg Psychiatry. 1965 Jun;28(3):247–59.7. Jacob RP, Rhoton AL. The chiari I malformation. In: Anson JA, Benzel EC, Awad IA, editors. Syringomyelia and the chiari malformations. South Washington street, Park Ridge, IL: AANS Publication Committee; 1997.p58.8. Alden TD, Ojemann JG, Park TS. Surgical treatment of Chiari I malforma-tion: indications and approaches. J Neu-rosurg. 2001 Jul;11(1):1–5.9. Speer MC, George TM, Enterline DS, Franklin A, Wolpert CM, Milhorat TH. A genetic hypothesis for Chiari I malfor-mation with or without syringomyelia. Neurosurg Focus. 2000 Mar;8(3):E12.
Carpenter syndrome and Hadju–Cheney syndrome. But syndromic type 1 Chiari malformations accounts for less than 1% of prevalence of type Chiari malformations, with most occurring as isolated phenomena9.
ConclusionMRI has become the imaging tech-nique of choice to diagnose Chiari malformations. It is accurate, spe-cific and noninvasive. In the excep-tional case when MRI cannot be performed, computed tomogra-phy-myelography/cisternography with formatted reconstructions can provide sufficient diagnostic infor-mation. In a number of cases, MRI alone may not be sufficient to clearly define the anatomy at the skull base or bony abnormalities in the cervical spine. The combination of MRI and










![Rx161 Arnold-Chiari Malformationfinalcopy0048502.netsolhost.com/.../pdfs/RXforms/Arnold_Chiari_Malformation.pdfArnold-Chiari malformation [Chiari malformation (CM)] is a congenital](https://img.dokumen.tips/doc/110x75/5ab9a8f17f8b9ac60e8e5491/rx161-arnold-chiari-malforma-malformation-chiari-malformation-cm-is-a-congenital.jpg)