Embed Size (px)
Citation preview

126
A geing and the M usculoskeletal S ystem Christopher McCarthy • Aubrey Monie • Kevin Singer
C H A P T E R 1 2
This chapter is divided into two sections. Section one describes some of the physiological mechanisms of ageing, to introduce the reader to the changes we face when dealing with the ageing musculoskeletal system. The second section details the more specifi c changes ageing brings to the axial spine.
AGEING OF THE MUSCULOSKELETAL SYSTEM
Ageing is the declining ability to respond to stress and by virtue of the increasing homoeostatic imbalance and incidence of pathology, death remains the ultimate con-sequence of ageing. 1 There are a number of theories regarding ageing, with a quick reference list displayed in Table 12-1 . For a more detailed overview of this area please consider the excellent review by Weinert and Timiras published in 2003. 2
Numerous hypotheses regarding the diminishing function of cells with time exist. Mechanisms that have been proposed to be life- and/or function-limiting for cells include cumulative oxidative damage to proteins, accumulation of mutations and genomic instability, gly-cation of proteins and telomere (the protective region of the chromosome) dysfunction. 1 Ageing of tissues is accompanied by increases in genome rearrangements and mutations, which may cause cell senescence and/or apop-tosis (programmed cell death). Cell senescence refers to the temporal decrements in the ability of cells to repli-cate, repair and maintain tissue, and is induced by both cell-intrinsic and cell-extrinsic mechanisms. 1
The cellular senescence theory of ageing (1965) describes a process where there is a limit to the number of cell divisions normal human cells can undergo in culture. This ‘limit in replicative capacity’ occurs after a characteristic number of cell divisions and results in ter-minally arrested cells with altered physiology. 2 Classical descriptions of cell senescence most often refer to the loss of the ability of mitotic cells to further divide in culture after a period of 30–40 population doublings. However, cell senescence appears to be much more complex than simple cell-cycle arrest occurring after a fi nite number of cell divisions. More recently, attention has been drawn to other forms of cell senescence sometimes referred to as ‘extrinsic’ or ‘stress-induced’ senescence as opposed to the intrinsic senescence resulting from replication. 3,4 Stress-induced senescence can occur from diverse stimuli including oxidative damage, activated oncogenes and chronic infl ammation. 4 Stress-induced senescence due to
oxidative stress fi ts well with one of the long-standing theories of ageing that suggests that free radicals could be mediators of ageing. 5
Ageing Joints Oxidative damage from the chronic production of endog-enous reactive oxygen species and free radicals has been associated with ageing in various human tissues and has long been thought to play a central role in the ageing process. 5 Increased production of reactive oxygen species leads to oxidative stress, a condition within cells where the amount of reactive oxygen species exceeds the anti-oxidant capacity of the cell. Human articular chondro-cytes can actively produce reactive oxygen species and have been found to increase directly with age. 5,6
Some of the changes observed in ageing joints and their contribution to the development of osteoarthritis are detailed in Table 12-2 .
Ageing Muscles In both young and aged skeletal muscle, it has been shown that oxidative stress increases in response to unloading (lack of activity/immobilization) and may have an important role in mediating muscle atrophy. 8 Decline of muscle mass is primarily due to type II fi bre atrophy and loss of muscle fi bre numbers. Increased variability in fi bre size, accumulation of scattered and angulated fi bres and expansion of extracellular matrix are characteristic to muscle atrophy. 8,9 The rate of muscle loss has been esti-mated to range from 1–2% per year past the age of 50, 25% in persons under the age of 70 and 40% of those older than 80 years are sarcopenic. 10 Signifi cant loss of myofi brils results in an increased negative nitrogen balance which exacerbates reductions in strength and endurance. 11
With advancing age, muscles display ‘hybrid’ muscle fi bre characteristics. Ageing muscle demonstrates selec-tive loss of fast motoneurons, leading to ‘orphan’ fast twitch muscle fi bres that are adopted by the relatively more abundant slow motor units. These fi bres partially convert to slow twitch fi bres, ending with a hybrid phe-notype showing the characteristics of both fast and slow fi bres. 11 When, fast type II muscle fi bres are incorporated into slow motor units (and eventually turned into a hybrid fi bre), there are irregularities in the size distribution of motor units. This, in turn, affects motor accuracy, espe-cially with low force movements, as the recruitment order does not adjust well to the previously small motor

12 Ageing and the Musculoskeletal System 127
proprioceptive) fi bres in peripheral nerves. 11 In addition to reductions in the number of fast myelinated fi bres, within the nerve the speed of signal conduction within the axon also reduces with age. 13 Neuromuscular junc-tions have been shown to demonstrate age-related reduc-tions in size and speed of conduction, thereby reducing the effi ciency of efferent transmission to the muscles. 10 These widespread physiological changes have been shown to result in poorer performance on cognitive and motor tests. 14,15
From the review by Weinert and Timiras 2003. 2
Biological Level/Theory Description
Evolutionary Mutation accumulation Mutations that affect health at older ages are not selected againstDisposable soma Somatic cells are maintained only to ensure continued reproductive success; after
reproduction, soma becomes disposableAntagonistic pleiotropy Genes benefi cial at younger age become deleterious at older ages
Molecular Gene regulation Ageing is caused by changes in the expression of genes regulating both development and
ageingCodon restriction Fidelity/accuracy of mRNA translation is impaired due to inability to decode codons in mRNAError catastrophe Decline in fi delity of gene expression with ageing results in increased fraction of abnormal
proteinsSomatic mutation Molecular damage accumulates, primarily to DNA/genetic materialDysdifferentiation Gradual accumulation of random molecular damage impairs regulation of gene expression
Cellular Cellular senescence-
Telomere theoryPhenotypes of ageing are caused by an increase in frequency of senescent cells. Senescence
may result from telomere loss (replicative senescence) or cell stress (cellular senescence)Free radical Oxidative metabolism produces highly reactive free radicals that subsequently damage lipids,
protein and DNAWear-and-tear Accumulation of normal injuryApoptosis Programmed cell death from genetic events or genome crisis
System Neuroendocrine Alterations in neuroendocrine control of homoeostasis results in ageing-related physiological
changesImmunologic Decline of immune function with ageing results in decreased incidence of infectious diseases
but increased incidence of autoimmunityRate-of-living Assumes a fi xed amount of metabolic potential for every living organism (live fast, die young)
TABLE 12-1 Theories of Ageing
units having grown bigger and stronger, and is one of the main reasons that motor and locomotor skills deteriorate with age. 12
Ageing Nervous System In the central nervous system there are age-related reduc-tions in the total number of brain cells and fi bres and the organization of fi bres within the brain ’ s white matter in addition to the reduction to the large diameter (A-beta
Ageing Change Contribution to Osteoarthritis
Accumulation of cells exhibiting the senescent secretory phenotype
Increased cytokine and MMP production stimulates matrix degradation
Oxidative stress/damage Increased susceptibility to cell death and reduced matrix synthesis
Decreased levels of growth factors and decreased growth factor responsiveness
Reduced matrix synthesis and repair
Increased AGE formation Brittle tissue with increased fatigue failureReduced aggrecan size and cartilage hydration and
increased collagen cleavageReduced resiliency and tensile strength
Increased matrix calcifi cation Altered mechanical properties and potential activation of infl ammatory signalling
TABLE 12-2 Ageing and Its Contribution to Osteoarthritis
MMP, Matrix metalloproteinases; AGE, Advanced glycation end-products. From Shane and Loeser (2010). 7

128 PART II Advances in Theory and Practice
absence of large-scale, long time-lapse epidemiological surveys to discern patterns and to test predictions. Post-mortem surveys and large radiological population-based studies 21,22,23 agree that spinal degenerative and age changes have an extremely high prevalence in adult populations. Of late, subtle differences in disc degen-eration patterns are being realized as genomic sequenc-ing emerges as an investigatory tool. 24 In the current era of Western society, osteoporosis is acutely studied given the cost and morbidity associated with the de-clining bone mineral health of the axial skeleton and its attendant fracture risk. This trend is not surprising, as over the last 100 years developed societies have evolved from physically demanding occupations to be-coming increasingly urbanized and inactive. The call to add physical activity to counter the epidemic of poor lifestyle choices (i.e. inactivity, smoking, poor nutrition) has become urgent given the projected cost and negative health outcomes for society. 25
Our biology uses both ageing and degeneration strate-gies to constrain the musculoskeletal system against further injury or damage. In the case of the spine, which serves the principal objectives of mobility, stability and protection of neural elements, overload or dynamic loading strains can induce a spectrum of either local or regional trauma and degenerative changes. Consequently, this chapter draws upon literature that represents both age-related and degeneration models, and their outcomes for the axial skeleton.
Normal physiological strains are well accommodated by each functional mobile segment, which comprises an intervertebral disc (IVD) with an anulus fi brosus and nucleus pulposus, and the vertebral end-plates (VEP). Paired synovial zygapophysial joints link both vertebrae posteriorly and articulate closely to regulate both load and movement of the segment. Applied moments from muscle actions and axial compressive loads may be coupled with shear, bending (rotations) and torsion about the long axis of the spine, which are in turn moderated by the unique geometry of the segment ’ s zygapophysial and ligamentous anatomy ( Fig. 12-1 ). Inertial strains from dynamic loading, even several times body weight, may also be tolerated by the spine given its unique capac-ity to attenuate energy. 26 The regional response to loading is refl ected in different patterns of injury or degeneration.
Vertebral bone adapts to loading by the cyclic remod-elling which is optimal by the third decade of life and declines variously thereafter. 27 Loss of trabecular con-nectivity, endocortical bone trabeculation and intra-cortical porosity are the late stages of remodelling. VEP collapse occurs due to trabecular bone fragility, with ver-tebral body fracture the clinical end-point in some cases. IVD degeneration is considered a normal process of ageing, but may be precipitated by multiple factors including genetic, anatomical, mechanical (occupational, overload, torsion, vibration), cell-mediated molecular cascades, trauma, infection and toxins as major infl uences to disc health 28–30 ( Fig. 12-2 ).
Osteoarthritis of the spine develops as a consequence of the natural ageing process coupled with attrition, and is associated with a degenerative cascade that may involve
Ageing, Falling and Pain Rates of falls among community-living, generally healthy elderly people (age ≥ 65) are of the order of (0.3–1.6 per person annually), with about 5% of these resulting in a fracture or hospitalization. Fall rates rise steadily with age and are about doubled for persons aged > 75 years. Persons living in long-term care institutions have much higher fall rates (0.6–3.6 annually). Falls among those in institutions also tend to result in more serious complications; with 10–25% of such falls resulting in fracture or laceration. It is often reported that older adults experience greater prevalence of pain, greater pain intensity and pain at more sites than younger adults. 15,16
It has long been thought that the increase in the preva-lence of pain among older adults is partly due to the progressive musculoskeletal degeneration that accompa-nies ageing. Another explanation for increased pain in older populations has been that ageing is associated with greater sensitivity to painful stimuli that results from changes in the structure and function of the nociceptive system. 17
Ageing and the Benefi cial Effects of Movement It is thought that mechanical forces are important regula-tors of several biological functions, with mechanical signals having been shown to mediate the development of a variety of tissues (e.g. skeletal muscle, bone, carti-lage). 18,19 Mechanical signals can affect diverse cellular processes including cell growth, differentiation, cellular migration, gene expression, protein synthesis and apop-tosis. 18,19 Given the potential importance that mechanical signalling functions have in maintaining cellular homoeo-stasis, it is likely that changes in mechanotransduction may also play a role in the pathophysiology of disease. 19 Recent data strongly support this, as it is recognized that many aspects of sarcopenia may be related to alteration in cellular mechanotransduction. 19 The ability of cells involved in the musculoskeletal system to sense, process and respond to mechanical stimuli deteriorates with age and that these changes may be involved in the aetiology of ageing-associated disease. 20 Encouragingly, movement quantity, quality, locality and intensity are relatively mod-ifi able infl uences and are certainly infl uences within the scope of the manual therapists. The infl uence of mecha-notransduction on tissue health and the symptoms of ageing are exciting areas for future research, particularly for those of us involved in the provision and prescription of therapeutic movement.
THE AGEING SPINE
Most individuals achieve old age with some evidence of degenerative or pathological changes in spinal joints, which refl ect the interactions between: genetics, oc-cupation, lifestyle, nutrition, trauma and destiny. Most published reviews on the health of the spine are seen through the prism of clinical perspectives, with an

12 Ageing and the Musculoskeletal System 129
VEPs 34 or through vessels that communicate directly with the outer annular layers. Consequently, disruption to either system occurring through normal ageing, surgi-cal intervention, spinal deformity or trauma can disrupt and lengthen the pathways of nutritional support to the disc and is presumed to contribute to subsequent disc degeneration. The consequence of either ageing or injury to the functional mobile segment may be degeneration of its elements with initial progressive increase in strain tolerance beyond the normal, which may progress to increased segmental mobility. One mechanical response to such changes, particularly affecting the stability and function of the IVD, is spondylosis, initiated through osteogenic stimulation in the junctional region between the VEP periphery and the annulus, resulting in the early formation of osteophytes. 35 Experimentally induced osteoarthrosis of the paired zygapophysial joints has been associated with anular rim lesions of the IVD. 36 The posterior paired costotransverse and costovertebral zyg-apophysial joints are true synovial joints invested with hyaline articular cartilage, a capsule and synovium. These joints contribute stability of the respective segment(s) and facilitate respiratory excursions of the thorax and regional mobility within the vertebral column, respec-tively. Each may respond to overload with degenerative patterns of synovial joints characterized by mechanical changes of the articular cartilage. Subchondral bone scle-rosis, fi ssuring and detachment of the cartilage, and mar-ginal joint osteophytosis may follow changes in the IVD, particularly a loss of vertical height which in turn alters the mechanical alignment of the respective superior and inferior articular processes of the posterior joints. Bumper fi brocartilage formations at the joint margin are associ-ated with evidence of articular cartilage degeneration and fi ssuring, ossifi cation of the ligamentum fl avum, and reactive hyperplasia at the posterior joint margins. A further consequence of degenerative changes leading to altered morphology of the IVD and vertebral bodies is the response by the spinal ligaments. With progressive deformation of the segment, ligaments may demonstrate buckling and, in response to exaggerated segmental motion strains, subsequent hypertrophic changes may contribute to stenotic change within the vertebral and intervertebral canals. 37 Ossifi cation within the ligamen-tum fl avum may occur as a consequence of degeneration of the articular triad, although this tends to predominate in the region of the lower thoracic and upper lumbar segments. 38
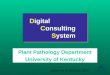
Patterns of spinal degeneration and age changes become evident when merged onto a common model of the axial skeleton; the mobile cervical and lumbar seg-ments, and their respective stiffer transitional junctions display different trends. The general pattern is for spinal motion to decline in all directions with age, and this feature is illustrated with the combined movement exam-ination assessment for the lumbar spine ( Fig. 12-3 ). Where segmental mobility is greatest degeneration of the disc and facet joints dominate. In the case of the bony thorax, focal changes are seen at the respective costo-vertebral joint articulations of the fi rst and last ribs, a consequence of transferring large torques from the mus-culature of the neck and trunk, respectively. When one
the discrete elements or an entire functional mobile segment, individually or regionally. 31,32
The IVD is essentially aneural apart from the periph-eral superfi cial outer third, although with injury to the disc, vascular ingrowth associated with repair may con-tribute vasomotor nerves. 33 The disc is also avascular, apart from the peripheral annulus, with a reliance upon nutritional substances transported via diffusion across the
FIGURE 12-2 ! The infl uences on the intervertebral disc associ-ated with ageing.
DISCdisease
Biochemical Nutrition I mm
une Neurogenic Infec
tive
To
xins Biochemistry
Gen
es •
Mechanical • Structural • Age
FIGURE 12-1 ! The regional patterns of injury and degeneration in the spine. AOJ , Atlanto-occipital joint; CTJ , Cervicothoracic joint; DD , Disc degeneration/Disc disease?; L , Lumbar; LSJ , Lumbosacral joint; OA , Osteoarthritis; T , Thoracic; TLJ , Thoraco-lumbar joint;. # , these sites along the column are disposed to trauma and fracture.
TAOJ
#, OA
#, OA
#, OA
#, OA
DD
DD
DD
CTJ
#
TLJ
LSJ
L
Torsion
Shear
Rotation

130 PART II Advances in Theory and Practice
highest prevalence of disc degeneration is in the mid-cervical, mid-thoracic and mid-lumbar discs as these regions show a marked degree of reactive changes of the vertebral bodies with marginal osteophyte formation ( Fig. 12-4 ). Early post-mortem studies by von Lushka 45 demonstrated a large proportion of cervical discs with fi ssures and clefts. This was considered to be a normal characteristic of the region, with complete transverse clefts extending across and into the region of the unco-vertebral joints found in the middle of healthy cervical discs on coronal section. 46 From similar post-mortem reviews of the thoracic spine, the most severely affected discs are located predominantly within the middle seg-ments, peaking between T6–T7, with a greater incidence in males. 47 Given the tendency to axial plane segmental motion in the mid-thoracic spine, reported in the classic paper by Gregersen and Lucas, 48 such degenerative changes may relate to the large rotation strains imposed upon these segments. Investigations by Farfan et al. 49 into the effects of torsion on lumbar IVDs concluded that relatively small rotation strains > 2° per segment induced potential injury in the anulus fi brosus. The pattern of age-related decline in anterior disc height in men typifi es the disc ageing process associated with senile kyphosis whereby the cumulative effects of axial loading and tor-sional stresses result in degeneration of the anterior anulus and osteophytosis. 21 In females, however, loading through the anterior aspect of the kyphotic curve is more likely to produce progressive change of the vertebral bodies, causing the wedge deformity commonly associ-ated with spinal osteoporosis. 50 Mechanically, the middle vertebral segments are predisposed to greater axial com-pressive and bending moments, due to their position within the apex of the thoracic kyphosis. 51
Osteophytosis
Osteophyte formation and its associated IVD degenera-tion has been recognized as an attempt to distribute force more uniformly across the VEPs to achieve stress reduc-tion on the segment. 52 Where thoracolumbar disc degen-eration is present, marginal osteophyte formation of the
FIGURE 12-3 ! The decline in range of motion in all planes, observed when using the combined movement examination of the lumbar spine. F, fl exion; FwRSF, fl exion with right side fl exion; RSF, right side fl exion; EwRSF, extension with right side fl exion; E, extension; EwLSF, extension with left side fl exion; LSF, left side fl exion; FwLSF, fl exion with left side fl exion; For colour version see Plate 11.
Flexion
Extension
EwLSF EwRSF
FwLSF FwRSF
0
10
20
30
40
50
LSF RSF
20s30s40s50s60s
A
Flexion
Extension
EwLSF EwRSF
FwLSF FwRSF
0
10
20
30
40
50
LSF RSF
B
considers the complete vertebral column as a multiseg-mented curved rod, with physiological infl exions that cross the neutral axis line, the literature presents evidence of different responses to stress accumulations at points of both maximum and minimum change in curve. The seg-ments adjacent to the transitional junctions, having less relative motion, are designed more for stability and rep-resent locations where axial compressive load is greater, the change in spinal curvature is least and where arthrosis of these synovial joints is found. In contrast, where the curvature away from the neutral axis line is maximum, as in the middle region of the lordosis and kyphosis, respec-tively, and where bending, torsion and shear stresses are relatively higher, the trend is for greater disc degenera-tion (see Fig. 12-1 ).
The major degenerative conditions reviewed in this chapter include osteoporosis and anomalies of spinal cur-vature, and changes that arise secondary to trauma. Infl ammatory disease of the spine is excluded from this discussion; the interested reader is directed to the com-pilation by Klippel and Dieppe 39 for a comprehensive review. Degenerative conditions that principally have a spinal manifestation may involve all elements of the func-tional mobile segment, either singularly as in the case of early IVD degeneration, or across the joint complex, exemplifi ed by late zygapophysial joint arthrosis coinci-dent with IVD degeneration. 40,41
Disc Degeneration
Literature describing the incidence of disc degeneration throughout the vertebral column concentrates predomi-nantly on the lumbar and cervical regions of the spine. 42 From post-mortem studies, discs with altered vascularity during the second decade of life show precursor changes to early degeneration. 43 The pathway of age-related degeneration change has been described as compromised nutrition, loss of viable cells, cell senescence, post-translational modifi cation of matrix proteins, accumula-tion of degraded matrix molecules, a reduction in pH levels that may impede cell function and ultimately induce cell death, and fi nally fatigue failure of the matrix. 44 The

12 Ageing and the Musculoskeletal System 131
occurs with gait, acts as a ‘pump’ to assist diffusion of nutrients within the vascular vertebral body across the VEP and into/away from the disc. Abrupt or fatigue axial loading of the spine may cause localized failure of the VEP resulting in either a frank sharply demarcated ver-tebral intra-osseous prolapse, often termed a Schmorl ’ s node, or marked irregularity of the end-plate. The repair process for both lesions often results in bony sclerosis which can signifi cantly impair the normal nutrient exchange to the IVD by reducing the effectiveness of this diffusion pathway. Schmorl ’ s nodes have been reported to occur during the late teens, 55 with lesions as frequent in the young as in the older individual. 21 Cadaveric studies of lumbar spines have indicated that Schmorl ’ s nodes develop at an early age and can exhibit advanced degen-erative changes. 35 Schmorl ’ s nodes are found most com-monly in males and are considered to be related to a genetic disposition, strenuous occupations 21 or sports involving dynamic and violent axial loading as might occur with a heavy landing in fl exion. 55 Most authors agree that the inferior end-plate is more susceptible to infraction 53,56 which implies that the VEP fails under compression ( Fig. 12-5 ).
Zygapophysial and Costovertebral Joint Degeneration
There appear to be specifi c sites within the spine where preferential degeneration of the synovial joints occur. The upper and lower segments of the thoracic region show a tendency for zygapophysial and costovertebral joint degeneration. 57,58,59 Similar trends for osteophytic remodelling of the zygapophysial joints of the lumbo-sacral junction have been reported. 60,61 This may be due to the design of these elements that provide stability and protection in contrast to the adjacent mobile segments which show a correspondingly higher frequency of disc disease 62 (see Fig. 12-1 ). The development of osteophytes and eventual bony fusion of costovertebral and costo-transverse joints in aged vertebral columns was also noted by Schmorl and Junghans 21 in their extensive survey of spinal pathology. The cervicothoracic junction and tho-racolumbar junction represent transitional areas between mobile and relatively immobile regions of the spine. At the cervicothoracic junction, Boyle et al. 63,64 found evident IVD and VEP changes, along with osteophytic formation that were more pronounced in the mobile seg-ments immediately above the transition. The upper tho-racic region and thoracic cage acted to impede intersegmental motion and thus safeguard these levels from marked degeneration. 64 At the thoracolumbar junc-tion, Malmivaara et al. 53 demonstrated that particular pathologies tended to be concentrated at each segment. The T10–T11 segment was characterized by disc degen-eration, vertebral body osteophytosis and Schmorl ’ s nodes; the T11–T12 segment tended to show both ante-rior and posterior degeneration, involving zygapophysial and costovertebral joints, while the T12–L1 joint was characterized primarily by posterior joint degeneration. A comparison of zygapophysial joint orientation with degenerative fi ndings suggested that the posterior ele-ments play a signifi cant role in resisting torsional loads.
vertebral body is frequently seen. 22,35 This pattern of excess bone formation, commonly referred to as spondy-losis deformans, is seen in approximately 60% of women and 80% of men. 21 The degree of intervertebral space narrowing and subsequent tilting of the vertebral bodies, resulting from disc degeneration, often determines the extent and the type of marginal osteophytes. 53 In summary, the segments that appear susceptible to osteophytes are often the most mobile regions with the higher levels of disc degeneration, or where local stress may be accumulated.
Vertebral End-Plate Lesions and Schmorl ’ s Nodes
The vertebral end-plate is a membrane of tissue compris-ing hyaline cartilage and a 0.5-mm-thin trabecular layer at the discovertebral junction. 54 Its role is to mediate axial compressive load applied to the IVD and permit transfer of this energy within the subchondral and cancellous bone of the vertebral body. Physiological axial loading, as
FIGURE 12-4 ! Macroscopic view of the L2–L3 (top) and T10–T11 (bottom) discs sectioned in the horizontal plane of two elderly cases to highlight disc herniation and advanced degeneration. The T10–T11 section depicts a central disc prolapse deforming the anterior dural sac. At L2–L3, age-related changes are dem-onstrated in the form of the large right-sided anterolateral osteophyte and advanced disintegration of the nucleus. A central fi ssure is evident through the posterior anulus.

132 PART II Advances in Theory and Practice
it may be induced through disordered metabolism and is accelerated following menopause in women. 68 A gender difference in bone fragility emerges due to the dynamic change in relationship between the mechanics of load transfer and the margins of safety. Males accumulate more periosteal bone than females, with a corresponding increase in vertebral cross-sectional area which confers a relatively higher load-bearing capability such that reduc-tions in bone strength are less dramatic than seen in women. During ageing, this ratio is disturbed and frac-ture risk increases as the stress on bone begins to approxi-mate its strength. Twenty per cent of postmenopausal women have a stress-to-strength ratio imbalance, whereas only 2–3% of men are at risk of fracture due to the greater preservation of bone strength. 69 The epidemiol-ogy of osteoporosis is well known whereby the risk factors of age, gender and racial contributors to bone loss and corresponding fracture risk increase exponentially with age. For the thoracic spine, one in four women over the age of 60 years will show at least one vertebral body fracture on radiographic examination, while the inci-dence increases to 100% in women over 80 years of age; 70 for men, there is a decade offset before osteopenia and osteoporosis develops. 71 The mid-thoracic segments are the most vulnerable to osteoporotic collapse or progres-sive wedge deformity due to the mechanical disadvantage of these segments situated within the apex of the thoracic kyphosis. 47 The second peak for thoracic osteoporotic fracture is at the thoracolumbar junction where more rapid loading of the thoracic spine can induce a hinging of the stiffened thorax on the upper lumbar spine. These
Asymmetry in the zygapophysial joint orientation tended to result in degenerative changes occurring mostly on the sagittal facing facet, 53 an observation originally made by Farfan et al. 49 at the lumbosacral junction.
Degenerative Spinal Curvature Anomalies
Idiopathic scoliosis involves a lateral curvature of the spine that is introduced through a disturbance in the longitudinal growth of the spine. It may occur early in the growth of the child and particularly during the early adolescent years. 65 Four main curve patterns have been identifi ed: thoracic, lumbar, thoracolumbar and double major curves. Each of these curvature patterns has its own characteristics and predictable end-point. 65 It is well accepted that the severity of the scoliosis can continue to progress through the life span. 66,67 Disc degeneration is known to develop due to the often extreme compression and ipsilateral tension strains experienced within wedged scoliotic IVDs. A cascade of degenerative changes occur in advanced scoliosis due to the attempt to stabilize against the increasingly asymmetric mechanical loads induced by this deformity ( Fig. 12-6 ).
Osteoporosis and Osteoporotic Fracture
Osteoporosis is an endocrine disease characterized by decreased bone mass and micro-architectural deteriora-tion of bone, which may lead to bone fragility and sub-sequently to an increased rate of fracture. Although resorption of bone follows the normal process of ageing,
FIGURE 12-5 ! ( A ) Intravertebral protrusions, or Schmorl ’ s nodes, are depicted from several views to highlight their location and extent. They may project cranially and/or caudally through the vertebral end-plate (arrows). End-plate irregularities are typically in the lower thoracic spine, as represented by the inferior end-plate of T11 (arrow). ( B ) A depression on the superior end-plate of a 2-mm-thick bone section from T11 with slight sclerosing of the end-plate compared with the regular thin inferior end-plate. ( C ) A central Schmorl ’ s node at T12 in a 100-mm-thick horizontal histological section shows disc material surrounded by sclerotic bony margins. ( D ) Multiple Schmorl ’ s nodes are shown at the thoracolumbar junction, all approximately in the same location and affect-ing the inferior vertebral end-plate, a characteristic of Scheuermann ’ s disease. c, Spinal cord; d, Disc; ep, End-plate; pll, Posterior longitudinal ligament; sn, Schmorl ’ s nodes. (Adapted from Singer 2000. 47 )
A
B
C D

12 Ageing and the Musculoskeletal System 133
the human spine, including those degenerative processes that are secondary to metabolic disease, spinal deformity or trauma. Ageing of the spine is not merely a chrono-logical process, as remodelling and repair follow such insults as trauma, disease, deformity or surgery and refl ects a biological strategy to stabilize against further segment damage from imposed loads. 73 While ageing is an unavoidable certainty, skeletal loading remains a criti-cal requirement for optimal function. Loading the mus-culoskeletal system throughout its dynamic range, over the lifespan, is crucial for sustaining not just musculo-skeletal health but health in general.
REFERENCES 1. Carrington JL . Ageing bone and cartilage: cross-cutting issues .
Biochem Biophys Res Commun 2005 ; 328 ( 3 ): 700 – 8 . 2. Weinert BT , Timiras PS . Invited review: theories of ageing . J Appl
Physiol (1985) 2003 ; 95 ( 4 ): 1706 – 16 . 3. DelCarlo M , Loeser RF . Chondrocyte cell death mediated by reac-
tive oxygen species-dependent activation of PKC-betaI . Am J Physiol Cell Physiol 2006 ; 290 ( 3 ): C802 – 11 .
4. Loeser RF . Ageing and osteoarthritis: the role of chondrocyte senescence and ageing changes in the cartilage matrix . Osteoarthri-tis Cartilage 2009 ; 17 ( 8 ): 971 – 9 .
5. Loeser RF . The effects of ageing on the development of osteo-arthritis . HSS J 2012 ; 8 ( 1 ): 18 – 19 .
6. Loeser RF . Age-related changes in the musculoskeletal system and the development of osteoarthritis . Clin Geriatr Med 2010 ; 26 ( 3 ): 371 – 86 .
7. Shane AA , Loeser RF . Why is osteoarthritis an age-related disease? Best Pract Res Clin Rheumatol 2010 ; 24 ( 1 ): 15 – 26 .
8. Seene T , Kaasik P , Riso EM . Review on ageing, unloading and reloading: changes in skeletal muscle quantity and quality . Arch Gerontol Geriatr 2012 ; 54 ( 2 ): 374 – 80 .
9. Seene T , Kaasik P . Role of exercise therapy in prevention of decline in ageing muscle function: glucocorticoid myopathy and unloading . J Ageing Res 2012 ; 2012 : 172492 .
more dynamic loads may be suffi cient to cause marked wedge compression fractures. Degenerative change to the IVD is not common in osteoporosis, suggesting a sparing of the IVD despite the vertebral body deformation.
Intervertebral Disc Prolapse
Clinically, the regions susceptible to prolapse of the intervertebral disc and the resulting disc degeneration typically are those with higher levels of mobility within the mid to lower cervical region and lower lumbar seg-ments. 42 What is not often appreciated is the high fre-quency of macroscopic discal prolapse within the thoracic region 47 (see Fig. 12-4 ) with the T11–T12 level most commonly involved. This trend may be due to the rela-tively greater disc height and volume at this region, coupled with localization of torsional forces that can occur immediately above the level of thoracolumbar junction transition. Markolf 72 proposed that the eleventh and twelfth thoracic vertebrae represented a site of struc-tural weakness for stresses in the vertebral column, due to the reduced constraint of the ribcage and the change in zygapophysial joint morphology that facilitated rota-tion above the transitional levels and impeded it below. The implication of disc prolapse is mechanical decom-pression of the nucleus, fi ssuring of the annulus and the cascade of changes that follow this injury. 44
Summary The human spine contributes a large proportion of the musculoskeletal presentations seen in manual therapy practice. This chapter has reviewed the effect of age on
FIGURE 12-6 ! An elderly macerated spinal column depicting severe kyphoscoliosis and marked osteophytic fusion across several segments within the region of the thoracolumbar transition, depicted from the ( A ) posterior and ( B ) anterior aspect. Note the remark-able osseous degeneration and remodelling. ( C ) A surface contour image of a marked scoliosis in an elderly woman, showing the typical rib hump appearance and asymmetry of the thoracic cage.
A
B C
–200 –100 0 100 200

134 PART II Advances in Theory and Practice
37. Weinstein P , Ehni G , Wilson C . Clinical features of lumbar spon-dylosis and stenosis . In : Weinstein PREG , Wilson CB , editors . Lumbar Spondylosis, Diagnosis, Management and Surgical Treat-ment . Chicago : Year Book ; 1977 .
38. Maigne JY , Ayral X , Guerin-Surville H . Frequency and size of ossifi cations in the caudal attachments of the ligamentum fl avum of the thoracic spine. Role of rotatory strains in their development. An anatomic study of 121 spines . Surg Radiol Anat: SRA 1992 ; 14 ( 2 ): 119 – 24 . [ Epub 1992/01/01 ].
39. Klippel JH , Dieppe PA . Rheumatology . London : Mosby ; 2008 . 40. Oegema TR Jr , Bradford DS . The inter-relationship of facet joint
osteoarthritis and degenerative disc disease . Br J Rheumatol 1991 ; 30 ( Suppl. 1 ): 16 – 20 .
41. Fujiwara A , Lim TH , An HS , et al. The effect of disc degen-eration and facet joint osteoarthritis on the segmental fl exibility of the lumbar spine . Spine 2000 ; 25 ( 23 ): 3036 – 44 . [ Epub 2001/01/06 ].
42. Kramer J . Intervertebral disk diseases. Causes, Diagnosis, Treat-ment and Prophylaxis . Stuttgart : Georg Thieme Verlag ; 1990 .
43. Boos N , Weissbach S , Rohrbach H , et al. Classifi cation of age-related changes in lumbar intervertebral discs: 2002 Volvo Award in Basic Science . Spine 2002 ; 27 ( 23 ): 2631 – 44 . [ Epub 2002/12/04 ].
44. Buckwalter JA . Ageing and degeneration of the human interverte-bral disc . Spine 1995 ; 20 ( 11 ): 1307 – 14 . [ Epub 1995/06/01 ].
45. von Luschka H . Die Halbbgelenke des Menschlichen Körpers . Berlin : Druck und Verlag von Georg Reimer ; 1858 .
46. Tenhave H , Eulderink F . Degenerative changes in the cervical-spine and their relationship to its mobility . J Pathol 1980 ; 132 ( 2 ): 133 – 59 .
47. Singer KP . Pathology of the thoracic spine . In : Giles LGF , Singer KP , editors. Clinical Anatomy and Management of Thoracic Spine Pain . Oxford : Butterworth Heinemann ; 2000 . p. 63 – 82 .
48. Gregersen GG , Lucas DB . An in vivo study of the axial rotation of the human thoracolumbar spine . J Bone Joint Surg Am 1967 ; 49 ( 2 ): 247 – 62 . [ Epub 1967/03/01 ].
49. Farfan HF , Cossette JW , Robertson GH , et al. The effects of torsion on the lumbar intervertebral joints: the role of torsion in the production of disc degeneration . J Bone Joint Surg 1970 ; 52 ( 3 ): 468 – 97 . [ Epub 1970/04/01 ].
50. Goh S , Price RI , Leedman PJ , et al. The relative infl uence of ver-tebral body and intervertebral disc shape on thoracic kyphosis . Clin Biomech 1999 ; 14 ( 7 ): 439 – 48 . [ Epub 1999/10/16 ].
51. Singer K , Edmondston S , Day R , et al. Prediction of thoracic and lumbar vertebral body compressive strength – correlations with bone-mineral density and vertebral region . Bone 1995 ; 17 ( 2 ): 167 – 74 .
52. Nathan H . Osteophytes of the vertebral column – An anatomical study of their development according to age, race, and sex with considerations as to their etiology and signifi cance . J Bone Joint Surg 1962 ; 44 ( 2 ): 243 – 68 .
53. Malmivaara A , Videman T , Kuosma E , et al. Facet joint orientation, facet and costovertebral joint osteoarthrosis, disc degeneration, vertebral body osteophytosis, and Schmorl ’ s nodes in the thoraco-lumbar junctional region of cadaveric spines . Spine 1987 ; 12 ( 5 ): 458 – 63 . [ Epub 1987/06/01 ].
54. Grignon B , Grignon Y , Mainard D , et al. The structure of the cartilaginous end-plates in elder people . Surg Radiol Anat 2000 ; 22 ( 1 ): 13 – 19 . [ Epub 2000/06/23 ].
55. Fisk JW , Baigent ML , Hill PD . Scheuermann ’ s disease. Clinical and radiological survey of 17 and 18 year olds . Am J Phys Med 1984 ; 63 ( 1 ): 18 – 30 . [ Epub 1984/02/01 ].
56. Yasuma T , Saito S , Kihara K . Schmorls nodes – correlation of X-ray and histological-fi ndings in postmortem specimens . Acta Pathol Jpn 1988 ; 38 ( 6 ): 723 – 33 .
57. Shore LR . On osteo-arthritis in the dorsal intervertebral joints – A study in morbid anatomy . Br J Surg 1935 ; 22 ( 88 ): 833 – 49 .
58. Shore LR . Some examples of disease of the vertebral column found in skeletons of ancient Egypt – A contribution to palaeopathology . Br J Surg 1935 ; 24 ( 94 ): 256 – 62 .
59. Nathan H , Robin GC , Weinberg H , et al. Costovertebral joints anatomical-clinical observations in arthritis . Arthritis Rheum 1964 ; 7 ( 3 ): 228 – 40 .
60. Cihak R . Variations of lumbosacral joints and their morphogenesis . Acta Univ Carol [Med] (Praha) 1970 ; 16 ( 1 ): 145 – 65 .
61. Resnick D . Degenerative diseases of the vertebral column . Radiol-ogy 1985 ; 156 ( 1 ): 3 – 14 .
10. Kaya RD , Nakazawa M , Hoffman RL , et al. Interrelationship between muscle strength, motor units, and ageing . Exp Gerontol 2013 ; 48 ( 9 ): 920 – 5 .
11. Jokl P . The biology of ageing muscle: quantitative versus qualitative fi ndings of performance capacity and age . In : Nelson C , Dwyer AP , editors . The Ageing Musculoskeletal System . Toronto : The Col-lamore Press ; 1984 . p. 49 – 58 .
12. Hausdorff JM , Levy BR , Wei JY . The power of ageism on physical function of older persons: reversibility of age-related gait changes . J Am Geriatr Soc 1999 ; 47 ( 11 ): 1346 – 9 .
13. Mittal KR , Logmani FH . Age-related reduction in 8th cervical ventral nerve root myelinated fi ber diameters and numbers in man . J Gerontol 1987 ; 42 ( 1 ): 8 – 10 .
14. Hausdorff JM , Edelberg HK , Cudkowicz ME , et al. The relation-ship between gait changes and falls . J Am Geriatr Soc 1997 ; 45 ( 11 ): 1406 .
15. Rubenstein LZ . Falls in older people: epidemiology, risk factors and strategies for prevention . Age Ageing 2006 ; 35 ( Suppl. 2 ): ii37 – 41 .
16. Rubenstein LZ , Josephson KR . The epidemiology of falls and syncope . Clin Geriatr Med 2002 ; 18 ( 2 ): 141 – 58 .
17. Cruz-Almeida Y , Black ML , Christou EA , et al. Site-specifi c dif-ferences in the association between plantar tactile perception and mobility function in older adults . Front Ageing Neurosci 2014 ; 6 : 68 .
18. Duncan RL , Turner CH . Mechanotransduction and the functional response of bone to mechanical strain . Calcif Tissue Int 1995 ; 57 ( 5 ): 344 – 58 .
19. Shwartz Y , Blitz E , Zelzer E . One load to rule them all: mechanical control of the musculoskeletal system in development and ageing . Differentiation 2013 ; 86 ( 3 ): 104 – 11 .
20. Isermann P , Lammerding J . Nuclear mechanics and mechanotrans-duction in health and disease . Curr Biol 2013 ; 23 ( 24 ): R1113 – 21 .
21. Schmorl G , Junghanns H . The Human Spine in Health and Disease . New York Grune and Stratton ; 1971 .
22. Lawrence JS . Rheumatism in Populations . London : William Heinemann Medical Books ; 1977 .
23. Prescher A . Anatomy and pathology of the ageing spine . Eur J Radiol 1998 ; 27 ( 3 ): 181 – 95 .
24. Colombier P , Clouet J , Hamel O , et al. The lumbar intervertebral disc: from embryonic development to degeneration . Joint Bone Spine 2014 ; 81 ( 2 ): 125 – 9 . [ Epub 2013/08/13 ].
25. Trost SG , Blair SN , Khan KM . Physical inactivity remains the greatest public health problem of the 21st century: evidence, improved methods and solutions using the ‘7 investments that work’ as a framework . Br J Sports Med 2014 ; 48 ( 3 ): 169 – 70 .
26. Adams MA , Bogduk N , Burton K , et al. The Biomechanics of Back Pain . Edinburgh : Churchill Livingstone ; 2013 .
27. Tobias JH , Gould V , Brunton L , et al. Physical activity and bone: may the force be with you . Front Endocrinol 2014 ; 5 : 20 . [ Epub 2014/03/14 ].
28. Battie MC , Videman T , Kaprio J , et al. The twin spine study: contributions to a changing view of disc degeneration . Spine J 2009 ; 9 ( 1 ): 47 – 59 . [ Epub 2008/12/30 ].
29. Gopal D , Ho AL , Shah A , et al. Molecular basis of intervertebral disc degeneration . Adv Exp Med Biol 2012 ; 760 : 114 – 33 . [ Epub 2013/01/03 ].
30. Neidlinger-Wilke C , Galbusera F , Pratsinis H , et al. Mechanical loading of the intervertebral disc: from the macroscopic to the cel-lular level . Eur Spine J 2014 ; 23 ( Suppl. 3 ): S333 – 43 .
31. Laplante BL , DePalma MJ . Spine osteoarthritis . PM & R 2012 ; 4 ( Suppl. 5 ): S28 – 36 . [ Epub 2012/06/01 ].
32. Vo N , Niedernhofer LJ , Nasto LA , et al. An overview of underlying causes and animal models for the study of age-related degenerative disorders of the spine and synovial joints . J Orthop Res 2013 ; 31 ( 6 ): 831 – 7 .
33. Palmgren T , Gronblad M , Virri J , et al. An immunohistochemical study of nerve structures in the anulus fi brosus of human normal lumbar intervertebral discs . Spine 1999 ; 24 ( 20 ): 2075 – 9 .
34. Dolan P , Luo J , Pollintine P , et al. Intervertebral disc decompres-sion following endplate damage implications for disc degeneration depend on spinal level and age . Spine 2013 ; 38 ( 17 ): 1473 – 81 .
35. Vernon-Roberts B , Pirie CJ . Degenerative changes in interverte-bral disks of lumbar spine and their sequelae . Rheumatol Rehabil 1977 ; 16 ( 1 ): 13 – 21 .
36. Osti OL , Vernonroberts B , Moore R , et al. Annular tears and disk degeneration in the lumbar spine – a postmortem study of 135 disks . J Bone Joint Surg Br 1992 ; 74 ( 5 ): 678 – 82 .

12 Ageing and the Musculoskeletal System 135
68. Kanis JA . Textbook of Osteoporosis . Oxford : Blackwell Science ; 1996 .
69. Seeman E . During ageing, men lose less bone than women because they gain more periosteal bone, not because they resorb less end-osteal bone . Calcif Tissue Int 2001 ; 69 ( 4 ): 205 – 8 .
70. Melton JL . Epidemiology of fractures . In : Melton LRJ , editor. Osteoporosis: Etiology, Diagnosis, and Management . Philadelphia : Lippincott-Raven ; 1995 . p. 225 – 47 .
71. Seeman E . The dilemma of osteoporosis in men . Am J Med 1995 ; 98 : S76 – 88 .
72. Markolf KL . Deformation of the thoracolumbar intervertebral joints in response to external loads: a biomechanical study using autopsy material . J Bone Joint Surg Am 1972 ; 54 ( 3 ): 511 – 33 . [ Epub 1972/04/01 ].
73. Kirkaldy-Willis WH , Farfan HF . Instability of the lumbar spine . Clin Orthop Relat Res 1982 ; 165 : 110 – 23 . [ Epub 1982/05/01 ].
62. Resnick D , Niwayama G . Diffuse idiopathic skeletal hyperostosis (DISH): ankylosing hyperostosis of Forestier and Rotes-Querol . In : Resnick D , editor. Diagnosis of Bone and Joint Disorders . Phila-delphia : Saunders ; 1995 . p. 1463 – 508 .
63. Boyle JJW , Singer KP , Milne N . Pathoanatomy of the interverte-bral discs at the cervicothoracic junction . Man Ther 1998 ; 3 : 72 – 7 .
64. Boyle JWW , Milne N , Singer KP . Clinical anatomy of the cervico-thoracic junction . In : Singer LGK , editor. Clinical Anatomy and Management of Cervical Spine Pain . Oxford : Butterworth Heine-mann ; 1998 . p. 40 – 52 .
65. Weinstein SL . Adolescent idiopathic scoliosis: prevalence and natural history . In : Weinstein S , editor. The Pediatric Spine . New York : Raven ; 1994 . p. 463 – 78 .
66. Ascani E , Bartolozzi P , Logroscino CA , et al. Natural history of untreated idiopathic scoliosis after skeletal maturity . Spine 1986 ; 11 ( 8 ): 784 – 9 . [ Epub 1986/10/01 ].
67. Gillespy T 3rd , Gillespy T Jr , Revak CS . Progressive senile scolio-sis: seven cases of increasing spinal curves in elderly patients . Skel-etal Radiol 1985 ; 13 ( 4 ): 280 – 6 . [ Epub 1985/01/01 ].