Embed Size (px)
Citation preview

Friday, March 31, 8:15 A;M.
A COMPARISON OF LOCAL ANESTHETIC DOSAGE REQUIREMENTS IN EPIDURAL
ANESTHESIA IN THE PREGNAXT AND POSTPARTUM PATIENT
It is a clinical impression that the pregnant patient at term requires less local anesthetic in the epidural space to achieve any equivalent block compared with the non-pregnant patient. Brommage (B.J.A.1962, Vo1.34, p 161) has shown that the dose requirement can be as much as one-third less in the pregnant group. On the other hand, Hehre (1966 Anesthesia and Analgesia, p 848) produced figures showing no significant difference between the two.
With patients undergoing bilateral tubal ligations in the recent postpartum period, epidural anesthesia is one of the anesthetics of choice. At H.U.P. it has been found that the dosage requirements to achieve satisfactory block levels in those done acutely at postpartum are comparable to the dosage that would be used in epidural anesthesia for Cesarean sections (i.e., pregnant patients).
We propose to assess the patient with regards to epidural anesthesia before and after she has delivered her child. We will therefore be able to use the same patient as her own control and examine the levels of block achieved following re- gular intermittent injections of local anesthetics in the epidural space over a period of 24 hours following delivery. A comparison will be made with the first (pregnant) epidural injection produced.
The technique will be standardized and follow a rigid ,protocol for aech "injection." Having obtained special informed consent from the patient, lumbar epidural anesthesia will be administeredwith the patient sitting. A Husted 18 gauge needle will be placed at L3-4/L4-5. A teflon catheter will be threaded in the usual manner and fixed in place to a depth of 1% to 2 cm. in the epidural space. A test dose will be injected - 2 ml. of 2% Nesacaine, followed one minute later by 12 ml. of 2% Nesacaine injected over a period of thirty seconds. The time will be taken from the end of the total injection. Once three minutes has elapsed from the end of the injection, the patient will be returned to a supine position with a wedge placed beneath the right hip in an attempt to avoid aorta- caval compression. The levels will be assessed bilaterally by cold and pinprick stimuli attwo minute intervals from the end of the injection for a period of fifteen minutes. The time of onset of subjective analgesia will be recorded. Perineal anesthesia will be assessed at fifteen minutes together with distal limb motor function. Serial assessments of height of block achieved with respect to the period after delivery can be made referring back to the control data from the initial epidural produced in the pregnant state.
Data: This study has just commenced and the results will be able to be presented in time for the S.O.A.P. meeting.
N.B. Special Informed Consent will be obtained from the patient.
David H.C. Milliner, M.D.* Barbara Turner Blake, M.D.* Brett B. Guts&e, M.D.**
*Fellow in Anesthesia **Associate Professor of Anesthesia Associate Professor of Obstetrics and Gynecology Department of Anesthesia Hospital of the University of Pennsylvania
8
-
-
-
-

Friday, March 31, 8:30 A.M.
EPIDURAL ANESTHESIA FOR CESAREAN SECTION: A COMPARISON OF ETIDOCAINE, BUPIVACAINE, AND CHLOROPROCAINE
S. Datta, W.U. Brown, Jr., B.C. Corke, G.W. Ostheimer, J.B. Weiss, M.H. Alper
Department of Anesthesia, Boston Hospital for Women, and Harvard Medical School
Epidural anesthesia is a popular method of pain relief for elective cesarean section. This study was undertaken to compare the use of etidocaine (l%), bupivacaine (0.75%) and chloroprocaine (3%) for this procedure.
Thirty healthy parturients at term were evaluated. The choice of local anesthetic drug was determined randomly.
Significant differences were found among the groups. These data are presented in the following table:
Etidocaine Bupivacaine Chloroprocaine p
Number of patients
10 10 10
Onset of anesthesia 15+1* 35*1 1521 <O.OOl§ (min)
Induction to de- livery interval (min)
37+2 53t3 39?2 <O.OO1°
Recovery room stay (min)
94?8 156+22 5622 <O.OOl§
Sensory anesthesia 2” 3 3 co. OOl@ score
*Mean+SE § ANOVA TMedian (scale: l=fair, 2=satisfactory, 3=excellent) QChi square
Onset of anesthesia was significantly slower and the re- covery room stay longer for the group who received bupivacaine. The average recovery room stay ,was less than an hour for those mothers given chloroprocaine. Sensory anesthesia was excellent for all mothers given bupivacaine, for 9 of the mothers who re- ceived chloroprocaine, but for only 2 of those given etidocaine. Muscle relaxation was excellent in every instance. All infants had Apgar scores of 7 or higher and normal acid-base states. Analysis of neurobehavioral tests of the newborns indicated no significant difference in performance among the three groups.
9
-
-
-
-
-
Friday, March 31, B:45 A.M.
BLOOD PRESSURE CHANGES DURING SPINAL ANALGESIA FOR VAGINAL DELIVERY: A COMPARISON BETWEEN NORMAL AND PREECLAMPTIC PARTURIENTS
E. Aboulelsh, M.D., F. Taylor, Ph.D. University of Pittsburgh School of Medicine
The study consists of two groups, each consisting of 100 patients who have subarachnoid block for vaginal delivery. Analgesia is produced by 5% lidocafne in 7.5% dextrose without epfnephrine. Group A is composed of 100 oarturfents who have had a normal course of pregnancy. Group B is eclampsfa.
1) Gestation age
2)
3)
comprised of 100 patients who have had a history of pre- The two groups are compared in regard to:
Original sysbolic and diastolic blood pressures
Incidence of hypotension which is arbitrarily considered as a 20% fall of the systolic and/or diastolic blood pressures
Duration of hypotension 4)
5)
5)
7)
B1
9)
10)
Fluid intake before and during splnal analgesia
Need for use of a vasopressor and the dose required
Analgesia level as determined by pinprick at 10 minutes following the induction of the block
Average neonatal weight
Administrationof magnesium sulphate
Neonatal condition as evidenced by the Apgar scores, need for resuscitation, and the time to sustained breathing
II) Any significant correlation among these parameters.
The data are being analyzed by computer, and the results of the study and their significance will be presented.
10
-
-~
-
-
.-

Friday, March 31, 9:00 A.M. _
PROPHYLACTIC EPHEDRINE PRECEDING EPIDURAL ANESTHESIA FOR CESAREAN SECTION
M. W. Moore, D.O., D. L. Shoults, M.D., .I. M. Mathers, M.D. --
Department of Anesthesiology Naval Regional Medical Center, San Diego, California
It has been well documented that hypotension in the parturient with a concommittant decrease in uterine artery blood flow is often accompanied by an undesirable fetal acidosis. Ephedrine has been iden- tified as the most desirable vasopressor for restoring the parturient to a normotensive state because, unlike other vasopressors, ephedrine appears to produce the least effect on uterine artery blood flow. stu- dies have been done which seem to indicate the desirability for the ad- ministration of ephedrine prior to spinal anesthesia in the parturient, to prevent hypotension.1 This study attempts to determine the efficacy of the administration of ephedrine prior to epidural anesthesia to pre- vent hypotension.
Patients included in this study were healthy women at 38 weeks or more gestation who were undergoing primary or repeat cesarean section. Cesarean sections complicated by fetal distress, hemorrhage, toxemia of pregnancy, or other maternal medical conditions were excluded from the study. All patients were ASA Class 1.
Through a large bore peripheral intravenous catheter, all patients were hydrated with 1000 cc of iv 5% Dextrose in Lactated Ringers solu- tion within 30 minutes prior to anesthesia. The infusion continued at a rate of 50-75 cc per hour. The patients were given 30 cc of antacid orally at least 30 minutes prior to anesthesia. They received no pre- medication. A standard roll was placed under the right hip to produce left uterine displacement while in the supine position. Maternal blood pressures were recorded prior to anesthesia and at 1 minute intervals after the injection of anesthetic into the epidural space. This monitor- ing continued for 15 minutes and at 5 minute intervals thereafter. Each patient received either 50 mg of ephedrine or an equal volume of saline, as a deep I.M. injection, from 5 to 15 minutes prior to the induction of anesthesia. A double blind technique was utilized. Anesthesia was accomplished with single dose epidural technique using 3/4X Marcaine in volumes necessary to achieve an upper sensory level to T4. If the sys- tolic blood pressure fell below 100 torr, the patient was vigorously treated with further displacement of the uterus and the rapid iv infus- ion of fluid. If this was unsuccessful in correcting the hypotension, 5 mg increments of ephedrine was administered intravenously as needed. From a double-clamped segment of umbilical cord obtained at birth before neonatal respirations were established, venous blood was sampled for Po2, Pco2, and pH determination.
Jl. Gutsche B: Prophylactic ephedrine preceding spinal analgesia for cesarean section. Anesthesiology 45~462-465, 1976.
-
-
~-
-
11
Friday, March 31, 9:15 A.M.
LUMBAR EPIDURAL ANALGESIA: A COMPARISON OF CONTINUOUS INFUSION AND INTERMITTENT INJECTION TECHNIQUE
BY
Antoun Koht. M.D,, Alex J. Bart, M.D., Mgner, M.D.,
Eveline A. Ricciarelli, * *, Richard Depp, M.D.
Departments of Anesthesia & Obstetrics and Gynecology Northwestern University Medical School
Lumbar epidural anal esia continues to enjoy popularity as a technique for pain re ief during labor and delivery. In f many cases intermittent injections of local anesthetic are given through an epidural catheter so that the duration of anal- gesia can be extended as it is needed. An effective alternate method, lumbar epidural analgesia by continuous infusion of local anesthetic, has been used for relief of labor pain by Zadar et al., and for post-operative pain relief by Green. However, a comparative study of the two techniques has to our knowledge not been done. We therefore have attempted to design a study to compare dose requirements, efficacy, patient accept- ance, and maternal and fetal well-being parameters for the two methods of anesthesia administration.
Healthy nulliparas for whom epidural analgesia was a like- ly choice for pain relief for labor were interviewed, and in- formed consent was obtained. A random number table was used to assign patients to either the continuous infusion group or the intermittent injection group.
Epidural catheter placement is accomplished by similar techniques for both groups. For the continuous infusion group, analgesia is provided with an initial bolus followed by a Holter- pump-driven infusion of 0.5% 2-chloroprocaine. The infusion rate may be adjusted as needed to maintain adequate analgesia. Blood pressure, level and intensity of analgesia and degree of motor blockade are assessed every five minutes for the,initial fifteen minutes and every fifteen minutes thereafter. Changes in fetal heart rate and in the frequency of uterine contractions are recorded by means of a fetal monitor.
For the intermittent injection group, analgesia is provided with intermittent doses of 2% 2-chloroprocaine. Moni- toring is essentially as described for the first group.
Neonatal well-bein is assessed b by umbilical cord (arterial) pH and PC&.
Apgar score and
The two groups will be can ared for total local anesthetic dose, quality and duration of pa n relief, and incidence of ! maternal, fetal and neonatal deleterious side effects. Our pre- liminary results will be presented.
,-
-
-.
12

-- Friday, March 31, 9:30 A.M.
DOUBLE BLIND STUDY OF BUPIVACAINE (MARCAINE (R)) AND TRmucAINR (PONTOCAINE(~)) FOR SPINAL ANESTHESIA IN THE OBSTETRIC PATIENT
Zeenee David-Mian. M.D., Brett B. Gutsche, M.D., Nancy Kenepp, M.D., A.Scott Wheeler, M.D. _ Department of Anesthesia, Hospital of the University of Pennsylvania, Philadelphia, Penna.
Data on bupivacaine (Marcaine (R)) f or spinal anesthesia in the obstetric patient was presented to the Society of Obstetric Anesthesia and Perinatology Meeting, April, 1975. From this preliminary study of 20 obstetric patients who received bupivacaine spinal anesthesia it was concluded that bupivacaine appeared to be a safe anesthetic for obstetric analgesia. Preliminary data obtained from an on-going double blind study of bupivacaine and tetracaine spinal analgesia in the obstetric patient is presented below. To date 46 patients have been studied. In the United States the use of bupivacaine in the subarachnoid space has not been approved except for investigational study. consent is obtained from the unpremeditated patient prior to its usa.
Informed _
After a skin preparation with iodine and alcohol, the subarachnold space is en- tered at L3-4 or L4-5 using a 625 guage spinal needle with the patient in the right lateral _ decubitus position. 0.75% bupivacaine or tetracaine with 8.25% dextzose is injected into the subarachnold space. The patient is then placed supine with a 10 tilt to the left. Hypotension is treated with acute hydration of approximately 1 liter of balanced salt solution intravenously,feft uterine displacement and ephedrine in 10 mg. I.V. doses as necessary.
Dose of Drug used:
Cesarean Section: 1.0 - 1.4 ml. or 7.5 to 10.5 mgms. Bilateral Tubal Ligation: 1.0 - 1.6 ml. or 7.5 to 12.0 mgms.
Bupivacaine
Characteristics Number of Mean of Analgesia Patients Minutes S.E.M.
Onset of Analgesia 9 0.83 0.08 Maximum Analgesia 9 13.44 2.10 Onset of Regression 9 86.56 9.05 Regain of Complete Sensation 9 216.33 17.55
Onset of Analgesia 9 2.22 0.55
Tetracaine Maximum Analgesia 9 11.22 1.55 Onset of Regression 9 84.89 13.50 Regain of Complete Sensation 9 259.11 23.22
The onset of analgesia appears to be faster with bupivacaine, though the duration of analgesia of bupivacaine and tetracaine is approximately equal when epinephrine is not - used. Addition of epinephrine to the anesthetic solution increased the duration of anal-, gesia with tetracaine but not with bupivacaine.
In bilateral tubal ligation patients who had the spinal analgesia one day post- partum, the mean drug dose was greater than in patients having Cesarean section; whereas the sensory level was higher in the C-section patients.
In the subarachnoid space, the onset of analgesia with bupivacaine is faster than - tetracaine. The duration of analgesia of bupivacaine appears to equal tetracaine without epinephrine and duration of block is not prolonged by the addition of epinephrine to bu- pivacaine. -,
Sensory analgesia and muscle relaxation from both drugs was adequate and similar. dissipation of the analgesia with bupicaine was subjectively comfortable for the patients. Patients receiving tetracaine complained of dysasthesla more frequently during regression .- of the analgesia.
*This st udy has been made possible by a generous grant from Winthrop Laboratories

Friday, March 31, 9:45 A.M.' 4
Earlyand Late Onset Convulsions Following Regional Anesthesia For Cesarean Section --~ -
Robert Hodgkinson Obstetrical Anesthesia Unit San Antonio, Texas
Four patients developed convulsions following regional block in the Course of 12,000 deliveries. Two followed pudendal block (1 aspirated, fortunately after receiving antacids) and 2 followed epidural anesthesia for C.S. using 0.75% bupivacaine.
In both of the case records that follow the patients were free of medical complications including hypertension and epilepsy and no permanent sequelas were observed in the mothers or babies as a result of their convulsions.
Case One: A 17 year old primigravida (ht 54", wt 115 lbs) received an epidural block at L 3/4 preparatory to Caesarian section. No blood or C.S.F. was obtained on gentle aspiration at any time during the procedure. A test dose of 2 ml (15 mg) of bupivacaine 0.75% given through the epidural needle produced no side effects. After five minutes a further 10 ml (75 mg) was given through an epidural (f/20) catheter. There was an immediate onset of severe convulsions. Following 100 mg of succinylcholine the patient was intubated and 100% oxygen administered. Ventricular tachycardia developed approximately 3 minutes after the onset of the convulsions. D.C. electro- shock was administered and normal sinus rhythm restored. General anesthesia was later administered. The baby's Apgar at birth was 3 at one minute and 8 at 5 minutes.
Case Two: A 27 year old primigravida (ht 62", wt 108 lbs) was given an epidural block at L 3/4 preparatory to Caesarian Section. The patient was apprehensive and hyperventilating. No blood or fluid was aspirated from the epidural needle and 20 ml of 0.75% bupivacaine were given slowly with a pause for questioning the patient and aspirating after 2, 5, 10, 15 and 20 ml had been given. An epidural catheter was inserted. Approximately 5 minutes later, the patient complained that she felt dizzy and sleepy. After 15 minutes slow generalized seizures affecting the whole body occurred atid lasted 3 to 4 minutes. These consisted of a tonic spasm affecting the whole body which lasted about 15 seconds. Following each of 3 such spasms she gave a few gasps of breath. The patient was not cyanosed and no treatment other than oxygen was given. The patient was later delivered by Caesarian section and general anesthesia. The baby's Apgar score was 9 at 1 minute and 10 at 5 minutes.
Our original technique for C.S. was to give a 1% ml test dose of 0.75% bupivacaine through the epidural needle followed by 18% ml through the catheter. Eighty-four patients were treated by this method. After treating the severe convulsions of case 1, reviewing the literature and realizing the difficulty of being certain the catheter changed our technique to injecting 20 ml needle at L 3/4 or 14 ml at L l/2. Case anesthetized by this method.
was not in an epidural vein we of 0.75% bupivacaine through the 2 occurred in the next 330 C.S.
14 -.

Friday, March 31, lo:30 A.M. .
BRAINSTEM EVOKED RESPONSE IN NEONATES
Sinai Hospital of Baltimore
Baltimore, Maryland
Phillip J. Goldstein, M.D., A. Krumholz, M.D., J. Felix, M.D. D. Shannon, Ph.D., R.F. Carr
Departments of Obstetrics, Pediatrics, Neurology, Rehabilitative Medicine
Infants ranging in gestational age from 26 to 40 weeks have been tested using brain stem evoked responses (BSER). The BSER measures conduction in the central nervous system, related in time to a peripheral sensory stimulus. The auditory BSER is of particular interest since each peak is anatomically linked. 4,000 to 10,000 auditory clicks, (E-12/set at 80 dB), were corn @tar averaged to obtain a response. Weekly evaluation of !O neonates less than 35 weeks gestational age was conducted and compared to 30 normal term neonates (Dubowitz). A defined pattern seemed to appear at 31 weeks gestational age with the more prominent waves being I, III & V. The latency of wave V decreased by 0.2 milisecond/week to full term. Waves I & III achieved a mature pattern earlier (34-37 weeks). The variability of wave V seems to preclude its use for gestational age definition. The rapid development of a mature pattern, however, suggests that this test might be useful in detecting early auditory deficits and for monitoring maturation of the CNS. Alterations in latency well beyond the mean were seen in neonates with either gross CNS lesions or accelerated pulmonary maturity.
15
Neonatal Intensive Emotional Care:
John W. Scanlon, M.D., Department of
Friday, March 31, lD:45 A.M. -.
Results of a Nationwide Survey
Pediatrics, Georgetown~ University
That parents of ill or dying newborns need intensive emotional support has become an axiom in modern perinatal care. Furthermore, professional NICU staff need their own emotional support and specific training in this area to take optimal care of critically ill newborns. Much data have been published about why such support should be provided. However, little information exists about how it is currently provided, who does this care, and how it is funded. Therefore, the 280 members of the AAP's Section on Perinatal Medicine were surveyed by questionnaire. 118 neonatal/perinatal specialists (42%) responded to this survey.
-
-
Eighty-three percent reported that, besides NICU nurses and physicians, social service workers provided such intensive emotional support in their unit. Twenty-four percent used psychiatrists, 17% utilized child development specialists, 14% used chaplains and 9% used psychologists. Many units obviously - had several different emotional support caretakers. There were many other different types of specialists giving this care.
The availability of social service personnel was divided between daytime alone and 24 hours on call. About 50% had such services available around the clock. On the other hand, psychologists, psychiatrists and family counselors were more often employed only on a consultative basis. Most chaplains were available all the time. Thus the continuous availability of social service personnel, with consultative backup support from more specifically trained psychologists and psychiatrists, is the national norm for intensive emotional support in the NICU.
-.
Training and counseling for the NICU professional staff was largely provided by social service personnel. However, over 41% of the respondants noted that psychologists and/or psychiatrists provided direct counseling for professional staff. Seventeen percent reported that these specialists were directly involved in staff training as well. A similar although lesser -
percentage of involvement for professional counseling and training was noted for the child development specialist and chaplain.
Twenty-one percent of the respondants indicated they had established specific programs for such care. Among this group, the most cormnon mechanisms were periodic rounds, in-service educational programs, parent support groups guided by professionals, and follow-up clinic consultation. There were several very innovative and comprehensive programs described in considerable detail.
Sixty percent of the emotional support was directly funded by the hospital. Sixteen percent was funded by research grants. Eleven percent of such service were funded by direct patient charges. The remaining services were supported by direct university programs, or volunteer staffing. For 3%, there was no direct funding.
-
The respondants were given an opportunity to make any comments they wished about this subject. A general concensus was that not enough support or interest has been shown for such programs to date and that much more is needed before optimal care is reached. Insufficient time to perform adequate parental and staff counseling was also widely noted. Finally, many respondants noted the insufficient availability of specific training for personnel working in this area.
16
*-
Friday, March 31, 11:OO A.M. _
-
THE EFFECT OF MATERNAL STRESS ON PLASMA CATECHOLAMINES AND UTERINE BLOOD FLOW IN THE PREGNANT EWE
Wright P.G, Shnider SM, Levinson G, P.oizen NF, Wallis L, Rolbin SH, Craft JB, Johnson JL and Jones MJ
Department of Anesthesia, University of California, San Francisco
Exogenous norepinephrine infusion1 or electrical stimulation of the major sympathetic branch of the hypogastric plexus2 significantly reduce uterine blood flow in the pregnant ewe. In pregnant Monkeys anesthetized with pentobarbitol, fetuses regularly develop hypoxia, acidosis and bradycardia as the monkeys are awakening3. These changes are reversed by reestablishing anesthesia. Studies from our laboratory indicate that maternal stress in pregnant ewes results in an elevation in maternal arterial pressure with an accompanying decrease in uterine blood flow. We postulated that the decrease in uterine blood flow is catecholamine mediated and determined the effects of noxious stimulation on both uterine blood flow and plasma norepinephrine levels in I awake pregnant ewes near term.
using our chronic maternal-fetal sheep preparation4 experiments were performed with the animal lying quietly on her side breathing oxygen. During a 30 rain- ute control period during which maternal and fetal cardiovascular and acid base variables were stable, blood was taken from the maternal artery at 15 and 30 minutes for plasma norepinephrine levels and values meaned. A noxious 33 volt electrical stimulus was then applied to the skin with the Winston Electronic Pain Producing Stimulator. Maternal arterial blood was sampled for norepinephrine just prior to the termination of stimulation which lasted 30 to 60 seconds and again 1, 3 and 10 minutes later. Both maternal and fetal blood pressure and pulse rate as well as uterine blood flow were continually monitored.
Results: During stimulation maternal blood pressure rose 46.9% while uterine blood flow fell 54.4%. Maternal blood pressure returned to control within 1 to 3 minutes of termination of stimulation while the return of uterine blood flow was more gradual occurring between 3 and 10 minutes. Maternal norepi- nephrine levels were 24.1% above control during stimulation, 20.9% above con- trol 1 minute later and 20.0% above control 3 minutes later. By 10 minutes norepinephrine levels had returned to control. Fetal cardiovascular status did not change throughout the experimental period.
Conclusion: Maternal stress producing an elevation in blood pressure is associated with a decrease in uterine blood flow and simultaneous elevation of maternal plasma norepinephrine levels.
-1 J *Barton MD et al: Proc Sot Exp Biol Med 145:996, 1974
Greiss Jr F et al: Am J Obstet Gynec, 1967 (21 \/3
4"
Myers RE: Am J Obstet Gynec 122:47, 1975
Ralston DH et al: Anesthesiology 40:354, 1974
-
17

Neonatal Intubation Friday, March 31, 11:15 A.M.
C.P. Gibbs, M.D., R.M. Nelson, M.D.
University of Florida College of Medicine
- The most important part of resuscitation of the newborn is ventilation. Although ventilation by mask is sometimes difficult and more than occasionally ineffective, endo- tracheal intubation is an effective and sure way to provide an adequate airway. How- ever, because it is often said and occasionally written that endotracheal intubation can - be traumatic to the newborn, the procedure is sometimes withheld too long. Since we believe that the risk of trauma has been overemphasized, and since there are no studies relating to the effects of short term intubation, we decided to study the incidence of - trauma caused by intubation attempts during resuscitatilon of the newborn at our hospital.
Methods: All infants requiring intubation at the time of delivery from October 12, 1977 to January 16, 1978 were evaluated. Trauma was assumed to have occurred if: 1) there was gross blood at the time of intuba~tion; 2) if hoarsness developed within 24 hours after intubation; 3) if there was any visible damage to pharynx or cords on extubation. The number of attempts per infant was tabulated as well as the level of expertise of the person or persons intubating.
_
Results: From October 12, 1977 to January 16, 1978 there were 806 infants born at the Shands Teaching Hospital. intubation.
Of these 806 infants, 72 or 9% were thought to require The indications for intubation were:l) meconium stained fluid (54%);
2) low Apgar score of 6 or less (25%); 3) both low Apgar score and meconium stained fluid (21%). One hundred thirty-seven attempts at intubation were made on the 72 infants. Twenty-eight received one attempt; 32 received 2 attempts; 7 received 3; one received 4; _ and 4 received 5 attempts. (Table 1) All but 6 tubes were removed within lo-15 minutes after insertion. The level of training of those persons performing the intubation and the mean number of intubations attempted per level is seen in Table 2. The level of training ranged from first year nurse anesthetist trainee to faculty. All had had at - least an introduction to the technique of intubation, but few had had extensive experience. There was no evidence of trauma in any of the 137 intubation attempts. In veiw of'the above we feel that endotracheal intubation of the neonate is a relatively benign proced- ure which should not be feared, but rather should be mastered and utilized by all con- cerned with the inediate care of newborn infants.
Table 1
1 Total
Table 2 Attempts and Level of Training
Post Graduate Yr.* No. % No./Child
: 75 11 [?I 1:;;
3 ;3 (faculty)
4; 13431 ;.;3
Total 137 *Includes obstetricians. oediatricians. anesthesiolooists and anesthetists
-
-
18
Friday, March 31, 11:30 A.M. -
Rase Excess in the Evaluation of Fetal Outcome
West Virginia University Medical Center
X.L. Kennedy, M.D.
Base excess, the numerical value indicating the metabolic component of acid-base evaluation, is frequently used to evaluate fetal outcome both in research and the clinical setting. In research, it is a valuable expression for comparison of intra- par-turn management regimens in that i.t provides an index of the degree that oxygen lack occurred during the regimen under consideration. It is, therefore, of the utmost importance to adhere to the strictest standards for consistancy and accuracy in the determination of this parameter.
There are three variations currently being used to calculate base excess (BE): (1) BE determined using the hemoglobin concen- tration of whole blood, (2) BEECF determined by using hemoglobin concentration of 5 gm, derived from the concept that hemoglobin buffers the total extracellular fluid (ECF) rather than whole blood alone and (3) BE using hemoglobin concentration for blood and corrected to full 02 saturation.
From an example of normal umbilical arterial (UA) blood gas values, pH 7.30, PC02 47, and PO2 15, the three BE values that may be reported are BE-4, BEECF-3, and BE-7.6 (corrected to full saturation).
Because non-volatile acids or bases do not cross the placenta, the BE in both umbilical arterial (UA) and venous (UV) blood should be equal except for the difference produced by oxygen saturation between the UA and UV. The equality should take place at the appropriate hemoglobin. Using the concept BEBCF the usual variations in total hemoglobin and the oxygen saturation correction will be less than lMEq/L. BEUV will be lower than UA because oxyhemoglobin is more acid.
Evidence and examples will be presented to confirm that : (1) BE should be reported for hemoglobin of 5 gm as BEECF and that this become a standard, (2) Presentation of data should specify methods of determination and (3) Correction to full saturation will provide erroneous interpretation.
-
-
19
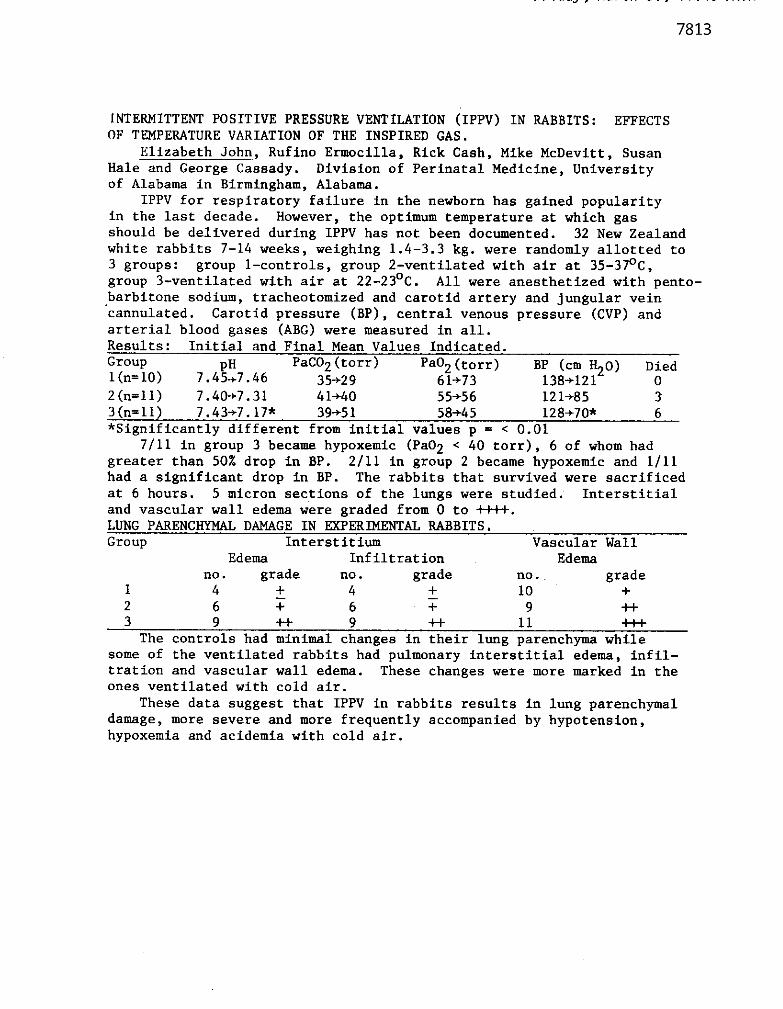
~INTERMITTENT POSITIVE PRESSURE VENTILATION (IPPV) IN RABBITS: EFFECTS OF TEMPERATURE VARIATION OF THE INSPIRED GAS.
Elizabeth John, Rufino Ermocilla, Rick Cash, Mike McDevitt, Susan Hale and George Cassady. Division of Perinatal Medicine, University of Alabama in Birmingham, Alabama.
IPPV for respiratory failure in the newborn has gained popularity in the last decade. However, the optimum temperature at which gas should be delivered during IPPV has not been documented. 32 New Zealand white rabbits 7-14 weeks, weighing 1.4-3.3 kg. were randomly allotted to 3 groups: group l-controls, group Z-ventilated with air at 35-37’C, group 3-ventilated with air at 22-23’C. All were anesthetized with pento- barbitone sodium, tracheotomized and carotid artery and jungular vein ‘cannulated. Carotid pressure (BP), central venous pressure (CVP) and arterial blood eases (ABG) were measured in all.
Friday, March 31, 11:45 A.M. -
-
Results: Initial a&Final Mean Values Indicated. Group 1 (n= 10) 7.4Ff7.46
PaC02 (torr) Pao2 (torr) Died 35+29 61+73
BP (cm H20) 138-+121 0
2(n=11) 7.40+7.31 4 l-t40 55+56 121+&35 3 3(n=ll) 7.43+7.17x 39+5 1 58445 128+70* 6 *Significantly different from initial values p = < 0.01
7/11 in group 3 became hypoxemic (Pa02 < 40 torr), 6 of whom had greater than 50% drop in BP. Z/11 in group 2 became hypoxemic and l/11 had a significant drop in BP. The rabbits that survived were sacrificed at 6 hours. 5 micron sections of the lungs were studied: Interstitial and vascular wall edema were nraded from 0 to ++I+. LUNG PARENCHYMAL DAMAGE IN &ERIMENTAI RABBITS. Group Interstitium Vascular Wall
Edema Infiltration Edema no. grade no. grade no. grade
1 4 + 4 + 10 + 2 6 T 6 T 9 -H 3 9 ++ 9 -I+ 11 +I+
The controls had minimal changes in their lung parenchyma while some of the ventilated rabbits had pulmonary interstitial edema, infil- tration and vascular wall edema. These changes were more marked in the Ones ventilated with cold air.
These data suggest that IPPV in rabbits results in lung parenchymal damage, more severe and mcxe frequently accompanied by hypotension, hypoxemia and acidemia with cold air.
-
20

Saturday, April 1, 8:00 A.M.
A RAPID PORTABLE ~IHOD FOR D~INI~JG P,O, ON MICR~~PMPES David Eric Lees, M.D. Georgetown University School of Medicine Michael H. Loughuane, M.S. (Bioengineer) Temple University School of Medicine
Paul Beckman, Consultant
A portable aud rapid means of perfOrming bedside Pa02 determinations of microsamples would be of great benefit in both the delivery room and in the transport of critically ill neonates. Such a system has been developed and a prototype model produced. The system uses a disposable "open" type oxygen electrode housed on a leadless capillary sensor with a luer fitting on one end. No wires, membranes or electrolytes are required for use. A sample of blood is simply aspirated or injected into the sensor and the
,
sensor is inserted into the analyzer. pO2 is read after a 25 second equilibration time and before the well known poisoning effect can occur at the cathode.
The analyzer 1s a battempowersd hand-held device with a self-contained heater which holds the specimen at 37' for the determination, as well timing and amplification circuitry. The system is calibrated before each determination by filling the sensor with O.lM KC1 tonometered to the p0 th s 2
of room air. A microtonometer has subsequently been developed for purpose.
A study undertaken to assess the accuracy and linearity of response of the system compared the results obtained with the microsampler against those from a conventional IL 213 blood gas analyzer on 130 samples of blood. Results obtained were subjected to linear regression analysis and plqted with respect to a line of agreement. A summary of the results is depicted in the graph.
While the accuracy of this system is not intended to surpass that of a conventional
gas analyzer, it may to be a useful and screening device where
there is not access blood gas laboratory
21
k,,
.-

Saturday, April 1, 8:15 A.M. -
MATERNAL AND FETAL EFFECTS OF ~-~~LLN~~PRocA~NE (NESACAIME)*
USED IN INTRAPARTUM PARACERVICAL BLOCK
Rodolfo Almonte. M.D., Robert R. Weiss, M.D. and Simon Halevy, M.D. From The Departments of Obstetrics 6 Gynecology and Anesthesiology Nassau County Medical Center, and the Health Sciences Center
SUNY at Stony Brook, New York 11790
-
The use of paracervfcal block (PCB) for pain relief in the first stage of labor is con- troversial due to reports of adverse effects of the local anesthetic on the fetus. In - the past, amide-type local anesthetics were almost exclusively used in PCB. The transfer of these drugs across the placenta and their toxic effect on the fetal myo- cardium has been demonstrated in a n&r of investigations.
2-Chloroprocaine (2CP) is a non-amide type local anesthetic. It has an ester bond in the molecule and, therefore, is rapidly hydrolyzed by plasma cholinesterase. This prospective study was designed to evaluate the effects of paracervfcal block with 2CP on the fetus and neonate. The study was conducted in two phases.
1. A prospective single drug study involving a study group of thirty term low risk gravfdas in labor. Upon entering the aotive phase of labor all patients received a paracervical block using 10 ml of of 2% 2CP at a controlled depth of 5mn. Good to excellent pain relief was accomplished in all but one case. The duration of action was short (man 38.9 mtn.) requiring repeat blocks in 6/30 cases. The fetal heart rate and uterine contractions were electronically monitored, and the fetal acid-base status was periodically checked by fetal scalp pti measurements. PCB related fetal brbdycardia was observed in 3/30 cases, but in only one case PCB was the only cause for the bradycardfa.
2. The second part of the study was designed as a double-blind drug evaluation where 2% 2CP was canpared to 1% lidocaina. To date thirty six cases were studied. Orug related bradycardia was observed in two of the controls (lidocaine) but none of the 2CP patients.
Preliminary Results
I. Fetal acidosis was not observed in any of our cases to date (this includes all five cases with fetal bradycardia).
2. No instances of neonatal depression or acidosis as expressed by the one and five-minute Apgar scores and cord blood acid-base evaluation were observed.
3. The mean duration of pain relief for all cases was 38.6 min.
4. It is suggested that PCB using ZCP is an effective though short acting method of pain relief in labor, and when properly monitored, is safe for both mother and fetus,
aPenwalt Corporation Pharmsceutical Ofvision, Rochester, New York
-
22

Saturday, April 1, 8:30 A.M. -
JET INJECTION OF LIDOCAINE FOR PARACERVICAL BLOCK. Ray McKenzie, M.D., Department of Anesthesiology, Magee-Wornens Hospital, University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania 15213.
The use of paracervical block for pain relief during the first stage of labor has been restricted by the high incidence of fetal bradycardia and occasionally fetal demise. Toxic levels of local anesthetic drug reaching the fetus have been held responsible. Since there are three mil I ion deliveries each year in the United States and skilled anesthesiologists capable of inducing epidural anesthesia are not available for all parturients, we investigated the performance of a modified jet injector compared with the standard technique using a syringe and needle. Twelve healthy patients undergoing dilatation, evacuation and curettage for therapeutic abortion were divided at random into two groups. The jet- injected group received a total dose of 40 mg. The syringe and needle group received a total dose of 200 mg of lidocaine. Samples of venous blood were taken before injection and at ten-minute intervals for one hour. Venous blood levels of lidocaine were estimated by liquid gas chromatography. Clinically equianalgesic blocks were achieved. Results showed that the venous blood levels of lidocaine in the jet-injected group were approximately one-third of these recorded in the syringe and needle group. Paracervical block by jet injection is a safer technique reducing the haxard of toxic levels of lidocaine.
23
-
-
-
Saturday, April 1, 8:45 A.M. -
-
FEMORAL AND BRACBIAL BLOOD PReSSURES DURING THE PRENATAL PERIOD
Farkhanda J. Husain. M.D., and Gertie F. Marx, M.D.
Department of Anesthesiology Albert Einstein College of Medicine
Bronx, New York
In 170 unselected pregnant women, femoral and brachial arterial pressures were taken in both supine and left lateral positions at prenatal visits during the second and third trimesters to ascertain:
a) the earliest recordable evidence of aortocaval compression, and b) the relationship, if any, between aortocaval compression and preeclampsia.
Blood pressures were measured twice with appropriately sized cuffs on the right leg and arm. Fifty teenage primigravidse of the group had "roll-over" tests performed in addition.
RESULTS.
(1) Reproducible decreases in femoral arterial pressure exceeding 10 torr in the supine position were observed in 57 women (34%). and in both femoral and brachial pressures in 65 women (38%). Decreases in femoral pressure exceeding 20 torr occurred in 53 of the above (31%). and in brachial pressure in 24 of the above (14%). Thirteen of the women with brachial pressure decreases (8%) developed clinical signs and symptoms of supine hypotensive syndrome. The earliest evidence of femoral pressure decline was noted at 19 weeks of gestation; thereafter, the incidence increased progressively. In contrast, declines in brachial pressure were detected only after the 28th week.
(2) Preeclampsia developed in 21 patients of the group (12%). The disease was diagnosed in three of the 57 women with femoral pressure decline (5X), in 10 of the 65 women with femoral and brachial pressure decreases (15X), and in eight of the 48 women with no fall in either pressure (17%).
(3) Roll-over tests were positive in 31 of the 50 teenagers (62X), and preeclamp- sia developed in 10 of these (32%). Roll-over tests were negative in 19 patients (38%). and preeclampsia developed in only one (5%).
CONCLUSIONS.
(1) Compression of the lower aorta by the uterus in the supine position is demonstrable earlier and with greater frequency than inferior vena cava compression.
(2) There appears to be no relationship between aortocaval compression and the development of preeclampsia.
(3) A negative roll-over test is prognostically more meaningful than a positive test.
-
-
-
24

Saturday, April 1, 9:00 A.M. -
'-PHYSIOLOGIC EFFECTS OF FOODSTUFF ASPIRATION. J.W. Wynne. D.J. Schwartz, C. Gibbs and C.I. Hood, University of Florida College of Medicine, Gainesville, FL.
It is generally held that the lung damage caused by aspiration of stomach contents results from the effect of acid at ph x2.5 or from obstruction of airways by large food particles. We have recently demonstrated that nonacid (ph >2.5) small particle ( <2tma) foodmatter can also cause aspiration pneumoni- tis. However, the physiologic significance of this lung damage is not known.
In order to evaluate the physiologic changes associated with aspiration of small particle foodmatter, 33 healthy mongrel dogs were divided into 4 groups. Two cc/kg of the following aspirates were administered with the do
9 s
Group I (n=13) saline, Group 2 lightly
anesthetized, breathing room air: n=8) HCL ph 1.8, Group 3 (n=6) foodstuff ph 5.9 obtained from the stomach of a normal dog 90 minutes after a meal of ground beef and vegetables, Group 4 (n=6) foodstuff adjusted to ph 1.8.
After administration of the aspirate the animals received no therapy other than I.V. fluids. Arterial blood gases, systemic and pulmonary arterial pressures, a-i DO , and shunt fraction (Qs/QT) were assessed prior to aspira- tion and at 10, 36, 60, 90, 120. 180, 240 minutes and 24 and 48 hrs after aspiration. Data were analyzed using Duncan's analysis of variance. Survi- ving animals were sacrificed at 48 hours. The lungs of all animals were prepared for histologic examination by inflation with fixative. There were no significant differences among groups in any variable prior to aspiration. After aspiration Pa0 was reduced, and Qs/QT increased in all animals (see table). These chang Z s were significantly worse (~~0.05) for Group 2 than for Group 1. There were no significant differences between Groups 3 and 4 but both groups were significantly worse (~~0.05) than Groups 1 or 2. There were bo deaths in Groups 1 or 2 but 33% of Group 3 and 100% of the animals in Group 4 died within 48 hrs.
POST ASPIRATION FINDINGS 1
GROUP N ASPIRATE pH Mean MaxAPa02 Mean MaxAQS/QT MORTALITY
1 13 Saline 5.9 -22 Torr +18% o/13
2 8 HCL 1.8 -43 Torr +52% O/8
3 6 Foodstuff 5.9 -53 Torr +65% 216
1 4 1 6 1 Foodstuff 1.8 1 -58 Torr +73% 616
Histologic examination of lungs from animals in Group 1 revealed normal lungs, the lungs of Group 2 animals were characterized by hemorrhagic pulmon- ary edema varying from small focal patches to extensive confluent areas. Necrosis of alveolar septae was occasionally seen. Group 2 animals manifested a distinct peribronchial inflaasaation composed of PMN's and macrophages associated in many instances with hemorrhagic edema. Group 4 animals had an amalgum of the changes seen in Groups 2 and 3.
We conclude that the aspiration of small particulate foodmatter can induce severe respiratory insufficiency even at a ph>2.5. The effects of foodstuff and acid may be additive.
-
-
-
-.
-
25

Saturday, April 1, 9:15 A.M. -
ANTACID PULMONARY ASPIRATION
Charles P. Gibbs, M.D., Dan J. Schwartz, M.D., James W. Wynne, M.D., C. Ian Hood, M.B. -
University of Florida College of Medicine, Gainesville, FL -
It has been suggested that oral administration of 15-30 cc antacid solution before general anesthesia might reduce the severity of damage due to acid aspiration. Although antacid administration does increase the pH of gastric contents in most instances, the results of antacid aspiration itself has not been studied thoroughly. - Kuchling, Joyce, and Cook studied several antacids in a small number of rabbits and found no changes in post-aspiration blood gases, but varying degrees of histological damage. Taylor and Pryse-Davies reviewed the lung damage done to - rats given antacid and found that several experienced pulmonary damage. No cardio- vascular or blood gas datawereobtained. We believed,therefore, that the question of lung damage due to antacid aspiration deserved a more thorough look.
- Four groups of dogs were studied and were grouped according to the type aspirate given via an endotracheal tube. Group I received 2cc/kgm of saline (pH 5.9); Group II received 2cc/kgm HCl (pH 1.8); Group III received 2cc/kgm of antacid mixture consisting of 0.5 cc antacid and 1.5 cc saline (pH 8.3); and Group IV received 2cc/kgm of saline with pH adjusted to pH 8.3. Systemic and pulmonary arterial pressures were monitored continuously. Arterial blood and central venous blood were sampled prior to aspiration and at 10, 30, 60, 90, 120, 180 and 240 - minutes after aspiration. Blood gas determination, a-vD02 and fractional shunt (Qs/Qt) data were obtained via these samples. Arterial samples were again taken at 24 and 48 hours and the dog sacrificed. The lungs were removed and prepared for histological examination.
RESULTS: Pa02 and Qs/Qt results are shown in Tables 1 and 2. The saline and alkaline saline group were affected only minimally. The acid and antacid groups were affected more severely and nearly to the same degree. -
Histological sections from Groups I and IV demonstrated either completely nOrMI lungs or small, widely scattered foci of inflanatory cells. Group II (acid) sections exhibited an alveolar exudate consisting of edema, fibrin, hemorrhage and polymorphonuclear leukocytes that varied from small patches to extensive confluent areas. Sections from Group III (antacid) were the most dramatic. All had extensive bronchopneumonia which consisted of an exudate composed of polys and macrophages in about equal proportions.
-
TABLES 1 and 2 -- Pa02 and Qs/Qt
TIk
ASPIRATE (pH) 0 10
Saline (5.9) :I HCl (1 8)
81.2 59.6
III Antacid (8.3) 77.1 34.1*t 83.5 45.8*
IV Saline (8.3) 82.8 57.8
:I Saline HCl (1.8) (5.9) 15.2 14.1 66.2*t 33.6
III Antacid (8.3) 13.1 47.4* IV Saline (8.3) 16.3 42.0*
* p < 0.05 vs Group I
t p < 0.05 Group II vs Group III
I -
90 I 120 1 180 1 240
70.8 46.6* 52.6* 68.5
72.8 50.0* 54.7* 69.7
74.8 53.9* 51.4* 69.9
22.6 46.0* 40.0* 22.8
19.2 19.2 44.4* 34.6* 38.4* 37.7* 20.0 22.0
-
-
-
26
Saturday, April 1, 9:30 A.M.
DOES MAGNESIUM SULFATE PREVENT SIJCCINYLCHOLINE-INDUCED FASCICULATIONS? -
UNIVERSITY OF CALIFORNIA, IRVINE
Jay S. DeVore, M.D. and Rajkumari Asrani, M.D.
Toxemia of pregnancy is still an extremely common disease and remains
one of the major causes of maternal mortality. Since many toxemic patients
require cesarean section for both fetal and maternal indications, it is important
for the anesthesiologist to understand the interaction between drugs used in
anesthesia and those used to treat toxemia.
Magnesium sulfate has been and remains the standard primary form of
therapy for toxemia. One of the effects of magnesium is to create a partial
neuromuscular blockade. This is evidenced by the fact that one of the complica-
tions of magnesium overdose is respiratory paralysis.
Since most cesarean sections on toxemic8 are emergencies involving a full
stomach, part of the induction technique for general anesthesia involves a
"defasciculating dose" of curare. On several occasions we have observed
profound effects on the patient from this minute dose. This led us to investigate
the question of whether or not magnesium sulfate-treated patients will fasciculate
at all given succinylcholine and what level of magnesium is necessary to prevent
succinylcholine-induced fasciculations.
Twenty patients having been treated with magensium sulfate for toxemia of
pregnancy and undergoing cesarean section will be observed. The total dose of
magnesium, duration of therapy, and time since last dose will be recorded. Degree
of fasciculations with succinylcholine, if any, will be noted, and blood will be
drawn for magnesium levels. Other variables will also be observed.
Preliminary data indicate that very low levels of magnesium are necessary
to prevent succinylcholine-induced fasciculations, and that the magnesium-treated
patient need not be given a defasciculating dose of curare.
-
-
-
-
-
-
-
-
-
-
-
-
-
27
Saturday April 1, 9:45 A.M.
-
Fetal Blood Concentrations of Etomidate Following Maternal Administration
West Virginia University Medical Center University of Iowa
R. Kennedy. M.D., M. VanHamme, Ph.D. M. Choneim, M.D.. J. Robillard, M.D.
Etomidate is an imidazole hypnotic currently under investi- gation for use as an intravenous anesthetic induction agent. Its reported advantages include minimal cardiovascular and respiratory changes with a rapidonset of action, a short duration and uneventful recovery. The drug disappears rapidly from the blood, however, tissue concentrations especially in the brain are higher than found in the blood. This drug is an ester and metabolic degradation occurs mainly by deesterification. The resulting metabolite appears in 30 minutes, is inactive and is excreted in the urine. Etomidate is a weak base with a pK of 4.24 so that almost 100% exists in the non-ionic form and, therefore, free for placental passage. Protein binding by plasma is 76.5% in humans. It is moderately lipophilic (log P-2.99 between octanol and water at pH 6.65).
We questioned whether its use as an anesthetic induction agent in obstetrics is appropriate. Using pregnant ewes with chronically implanted intravascular cannulas, we evaluated the fetal blood concentrations that developed following maternal administration.
Following etomidate injection intraveneously over 60 seconds, maternal and fetal arterial blood samples were drawn simultane- ously at 1, 5, 10. 15, 30, and 60 minutes. Each sample was analyzed for etomidate using gas liquid chromatography-mass spectrometry and single ion monitoring, a technique known as mass fragmentography. Additional sampling of maternal and fetal sheep blood were incubated with known concentrations of etomidate to evaluate the ability of the plasma to hydrolize this drug.
Etomidate appears rapidly in fetal arterial blood and at one minute almost equals the maternal concentration. The fetal/maternal ratio (F/M) rapidly rises to 3.0 at 15 minutes and declines to 1.6 at 60 minutes. The cholinesterase activity was found to be approximately 10% of that in human plasma. There was no hydrolysis in 60 minutes when etomidate was incubated with plasma in either maternal or fetal blood.
The rapid appearence in the fetal blood and the high F/M suggests caution for the use of this drug for obstetrical anesthesia. Since brain concentration has been reported to exceed the blood concentration, a disproportionate fetal pharma- cological effect might be anticipated following a maternal hypnotic dose. As previously reported in humans, metabolic degradation does not occur in the blood.
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
28
Saturday, April 1, 2:30 P.M. -
-
'DEPRS-TERMSMALLF0RGE5TATICN(SGA)INFANT: A'IXQYEAR~UP STUDY. B.R. Vohr, W. Oh, A.G. Fuxenfield, R.M. Cowett. Brawn University Program in Medicine, Wxnen and Infants Hospital, Department of Pediatrics, Providence, Rhcde Island.
Previous investigators have reported unfavorable neurological and developnantal outcme of SGA infants (birth weight (b.w.1 ~1500 grams) born at term or at ~30 wks of gestation. Since obstetrical considerations for the delivery of an SGA fetus often arise between 30-38 wks, the out- - of these survivors becanes a relevant issure. In 1975-76, 28 of 41 such infants survived and 21were followed sequentially during the first 2 yrs. Their b.w. was 1220 f 195 g @&SD) and the gestation 33.4?2 wks. Each SGA infant was paired with a b.w. - matched appropriate for gestation @GA) infant whose b.w. was 1195+190 g and gestation 29t2 wks. They have cmparable sex distributions, perinatal risk scores, maternal educa- tion, occupational status and caloric intake during the first 3 months. The weight, length, and head cinnnnference of the SGA infants attained the 1Othpercentile by 6-8 months andware similar to the AGAgroup. Quarterly neurological examinations showed similar findings during the first year in the 2 groups. At 2 yrs., 2 SGA (diplegia) and 1 AGA infant (hesniplegia) wereabnormal. The guarterly Sayley scores of the SGA infants ware lawer during the first year lxtat18-24nonths, the 2 groups had similar notor and cognitive developnental guotients. The data tiicate a favorable outcane in both AGA and SGA preterm infants weighing ~1500 gns; the favora- ble result in SGA infants may form an additional basis for the delivery of sucha fetus at30-38 wksifotherobstetricalfactors so indicated.
-
-,
-
44
-

Saturday, April 1, 2:45 P.M. -
THE INFLUENCE OF RUPTURED MEMBRANES ON SURVIVAL IN LOW BIRTHWEIGHT INFANTS - Richard P. Perkins, M.D., Associate Professor, Head, Division of Maternal- Fetal Medicine, Milton S. Hershey Medical Center, The Pennsylvania State University, Hershey, Pennsylvania
A retrospective study was made of 330 pregnancies resulting in low birth-" weight infants over a three year period at Colorado General Hospital. The in- fluence of ruptured membranes on admission was examined. Records on 356 infants were available for study. A policy of non-agresssive management of ruptured membranes was pursued. The first eighteen months was characterized by a general non-agressive approach to babies estimated at less than 800 grams. The second time period was characterized by faculty-level aggressive involvement with labors, deliveries, and early neonatal care in babies esti- mated at greater than 600 grams or 26 weeks gestational age. Febrile patients were administered antibiotics and delivered expeditiously. Betamethasone was not used. Breech presentation was managed by cesarean section when possible, particularly in the s&ond time period.
There were significantly fewer babies in the 500-900 gram group with rup- tured membranes than in other weight classes. The numbers in the remaining weight classes (901-1200, 1201-1500, 1501-2000) did not differ. Survival for the entire group with ruptured membranes was significantly better than the rest (123/137 versus 170/228, p = 0.0007). When compared by weight class, clearly enhances survival was seen in the 500-1200 gram group (p < 0.01).
-
-
-
-
Significant differences (p < 0.05) occurred only when both time periods were combined in the following groups: babies less than 30 weeks by dates and neonatal evaluation; with low forceps delivery; and with one-minute Apgar score 7 or greater. Significant differences were noted in each time period with absence of the following factors: meconium staining; cesarean section; cervical cerclage; oxytocin use; history of maternal urinary tract infection; fetal distress; fetal blood sampling indications. Significant detrimental influences were noted when the mother was febrile (901-1500 g.); and when she was referred from elsewhere (901-1200 g. only).
Significant differences were noted in the first time period and with both periods combined in the following areas: low indices of respiratory and general morbidity; normal labor tolerance; absence of DIC; one-minute Apgar score '7; and five-minute Apgar score <7. Significant differences were noted only in the second time period and with data combined intie following areas: intermediate morbidity index; and average fetal growth.
-
-
-
Following categories showed an advantage to the newborn regardless of their presence or absence: sex of the newborn (data combined); breech versus nonbreech presentation (data combined); and the absence of a history of maternal urinary tract infection. The following factors were found to have no apparent
-
demonstrable influence when associated with ruptured membranes: significant respiratory or general morbidity; absence of labor; spontaneous vaginal delivery; mid-forceps delivery; cesarean section; breech delivery; small for gestational -
age status; meconium staining; abnormal fetal blood or cord blood sampling; gestational age 30 weeks or greater; DIC; hyperbilirubinemia or its absence; fetal distress; cervical cerclage; oxytocin use; maternal history of urinary tract infection; and five-minute Apgar score 7 or greater.
CONCLUSIONS: Ruptured membranes appeared to exert a favorable influence on outcome in babies under 30 weeks gestation. This effect was noted only after 48 hours. Aggressive and experienced involvement in labor, delivery, and neonatal - care appears to be of additional benefit in certain cases. Perinatal compli- cations can nullify this advantage. These generalizations do not apply after 29 weeks gestation.
45

ANTEPARTUM FETAL HEART RATE TESTING: THE
EFFECT OF PHENOBARBITAL ON THE NON STRESS TEST
Kirk A. Keegan, M.D.
Richard H. Paul, M.D.
Harci A. Smith, R.N.
Dorothy McCart, R.N., B.S.
Paula Broussard, R.N.
Saturday, April 1, 3:00 P.M. -
-
During the period of May 1975 to April, 1577, 1,163 patients had antepartum non-stress testing performed at Los Angeles County-Univer- sity of Southern California Women’s Hospital, Los Angeles, California. A total of 2,422 tests were performed on these 1,163 patients. A test was considered reactive if the fetus demonstrated five accelerations of greater than 15 BPM associated with fetal movement in one of two 20 minute periods. A test was considered non-reactive if less than 5 accelerations with fetal movement were noted. 1,547 tests (64%) were reactive, 829 tests (34%) were non-reactive. Included in the 1,163 patients tested were 111 patients being treated with phenobarbital for pre-eclampsia (93%), chronic hypertension, and seizure disorder. 176 tests were performed in this group. 81 (46%) were reactive. 95 tests (54%) were non-reactive. A significant difference (p < 0.0005) ex- isted between reactivity in the phenobarbital and non-phenobarbital group. Fetal movement was plotted per unit time of test and was noted to be less in the phenobarbital group as a whole. 36 patients had multiple tests. The first test served as a reliable predictor for successive tests, especially in the non-reactive group, suggest- ing that the fetus does not accommodate to the drug. No control group of pre-eclamptic patients not on phenobarbital were evaluated since most pre-eclamptic patients were hospitalized and treated with phenobarbital prior to testing. However, 18 tests were per- formed on non pre-eclamptic patients taking phenobarbital. 67% of the tests were non-reactive, implicating phenobarbital and not pre- eclampsia as the etiology of the non-reactive test.
-
-_
-
-
-
-
-
-
-
-
-
-
-
- 46

Saturday, April 1, 3:15 P.M.
Epidural Anesthesia: Causal or Casual Relationship to Mid-Forcep Rotation?
Authors: Robert N. Miller, M.D. & W.Ross Mayfield, M.D.
Institution: St. John’s Mercy Medical Center 621 South New Ballas Rd., Creve Coeur, MO. 63141
In March 1975, a change was initiated in the practice of Anesthesia for Obstetrics at St. John’s Mercy Medical Center. Patients who had been interviewed by one of the authors in the seventh month of gestation could receive segmental epidural anesthesia. This office appointment served to allow a better patient-physician relationship to exist between the anesthesiolo- gist and the parturient. as well as randomizing the patient popula- tion as to type of labor. The departure from the previous practice of an epidural for “the difficult patient in labor” or “the patient with difficult labor” was viewed with mixed emotion among the obstetricians.
Many publications in either textbooks or medical journals have indicated a marked increase in the percentage of transverse, or posterior arrest of the presenting vertex when epidural anesthesia was administered for analgesia during labor and delivery. The authors have made a strong case condemning epidural anesthesia as causal in the relationship to mid-forcep or Malmstrom rotation, rather than casual.
We examined our experience with 1,833 epidural anesthetics, 1,308 caudal anesthetics and 5,413 paracervical-pudenda1 anesthe- tics for vaginal delivery from March 1975 through August 1977. The data are presented in the three time references. March 1975 through March 1976 was a period when 60% of the patients were anesthetized “on request” by the obstetrician and 40% were random- ized having been seen prior to entering the hospital in active labor. April 1976 through August 1977 represents a period when all but four patients had been seen for epidural anesthesia prior to entering the hospital in active labor. The aggregate data are then presented.
Title: Incidence of Mid-Forceps or Malmstrom Assisted Deliveries.
Time period Epidural (Total) Caudal(Tota1) Para-Pud. (Total) March 1975- March 1976 11.1% ( 414) 8% (1308) 7.9% (2380) April 1976- August 1977 7.82% (1419) 3.43%( 496) 6.23% (3032) March 1975- August 1977 8.56% (1833) 6.26%(1308) 6.98%, (5412) Conclusion: These data indicate that there is a small increase
in the incidence of malpresentation requiring mid-forceps or Malmstrom rotation associated with continuous segmental epidural anesthesia. We believe that the small percentage increase may be due to the preponderance of epidural anesthesia given for primiparous patients. Our conclusion is that in our practice, the relationship of epidural anesthesia to mid-forcep or Malmstrom rotation is casual rather than causal.
47
-
-
-
-
-
-
-
-

Saturday, April 1, 3:30 P.M. -
PLASMANOPEPINEPHHINE AND UTE~NEBLOODFLOWCHANGES DWNG ENCQl'RAm
DlTUEIATION AND GENERAL ANEBTHZiIA IN THE PREGNANT EWE
Shnider SM, Wright HG, Levinson G, Boizen MF, P.olbin SH, Biehl DR, Johnson JL and Jones MJ
Department of AneSthSSid, UniVerSity Of California, San Francisco
Anesthetic agents modify sympathetic activity. Halothane reduces plasma norepinephrine in rats1 and nitrous oxide increases serum norepinepbxine in human voluuteersl. We postulated that nitrous oxide anesthesia may decrease uterine blood flow through elevation of endogenous norepinephrine and that this potentially deleterious effect eight be avoided by the addition of low concentrations of halothane or enflurane. Using our chronic maternal fetal sheep preparation3 we performed the following experiments in 12 pregnant sheep near term.
Following a 30 minute control period with the animal lying quietly on her side breathing 100% oxygen, anesthesia was induced with thiopental 4 rag/kg. Intuba- tion was facilitated with .25 mg/kg of succinylcholine. On separate days anesthesia was maintained by positive pressure ventilation with one of 3 anesthetic mixtures, N20 50% or N20 59% and halothane 0.5% or N20 508 and
enflurana 1.0%. Each study consisted of 2 sequential periods of 30 minutes each: a period of anesthesia with noxious stimulation superimposed,and a period of anesthesia without noxious stimulation. Selection of anesthesia and sequence of the 2 periods were randomly assigned.
Intravenous induction with direct laryngoscopy and endotracheal intubation resulted in an increase in plasma norepinepbrine of 89% from control. Blood pressure rose 65%, uterine blood flow fell 24% and uterine vascular resist- ance rose 42%. These acute cardiovascular changes quickly diminished with termination of airway manipulation. Noxious stimulation during N20:02 anesthesia was associated with an increase in maternal blood pressure of 15% (Fig. 11, a decrease in uterine blood flow of 16% (Fig. 2) and an increase in plasma norepinephrine of 71% (Fig. 3) from the awake control state. By contrast noxious stimulation during N20:02 anesthesia that was supplemented with either 0.5% halothane or 1% enflurane did not increase plasma catechol- amines. Blood pressure remained unchanged in both groups and uterine hlood flow increased 22% with halothane but did not change with enflurane. ._
I
-
-
-
. .
-
I
Fbizen MF et al: Anesthesiology 41:432, 1974. smith NT et al: Anesthesiology 32:410, 1970. 1d - Ralston DH et al: Anesthesiology 40:354, 1974.
48 i -

-
Sunday, April 2, 8:00 A.M.
-
ENFLURANE ANALGESIA FOR VAGINAL DELIVERY
Rolbin SH, Wright RG, Shnider SM, Craft JB, Henriksen E, Abboud T, Johnson JL, Jones MJ and Levinson G
Departments of Anesthesia, University of California, San Francisco and University of Southern California, Los Angeles
We investigated the use of enflurane in subanesthetic doses for analgesia during the second stage of normal vaginal deliveries and compared it to nitrous oxide.
Each patient gave informed consent for the administration of either nitrous oxide (55 patients) or enflurane (50 patients). Inhalation agents were administered in a randomized manner by an anesthesiologist with both the patient and obstetrician unaware of which drug was being used. Patient groups were comparable in age, parity, method of delivery, local anesthetic administration and duration of analgesia prepartum. The range of anesthetic concentrations administered with oxygen varied between .25 to 1.25% for enflurane and 30 to 60% for nitrous oxide. Delivered concentration was adjusted so that patients remained awake, conversant and cooperative. Analge- sia for the time of delivery was evaluated by the patient, obstetrician and anesthesiologist and ranked on a scale ranging from 0 or no relief to 4+ or excellent pain relief. Amnesia for delivery and patient willingness to receive the agent again were also determined. Apgar scores were assigned at one and five minutes of age.
Upon admission to the study, blood was drawn for hemoglobin, hematocrit, WBC, electrolytes, BUN, creatinine , uric acid, fluoride ion concentration and osmolality. A urine specimen was obtained for osmolality, sodium, potassium, protein, glucose and fluoride ion. Blood and urine laboratory investigations were repeated 12 to 24 hours after inhalation analgesia. A cord specimen was obtained for blood gas analysis and serum fluoride ion concentration. A newborn urine was analyzed for osmolality, fluoride ion, sodium, potassium, glucose and protein.
Enflurane:02 was rated satisfactory (3+ or 4+) by 89% of the mothers and 80% of the anesthesiologists, ratings not significantly different than with nitrous oxide. The obstetrician, however, rated the enflurane:02 mixture superior. The incidence of amnesia for delivery was low: approximately 10% for both agents. Almost all patients in both groups expressed a willingness to receive the agent again for subsequent deliveries. The newborns of mothers receiving both agents were vigorous and comparable when assessed by Apgar scores and cord blood gases. The estimate of blood loss (obstetrician's estimate, follow-up Hgb and Hct) was similar in both groups. Postanesthesia maternal serum inorganic fluoride concentrations were not significantly increased from preanesthetic with either agent. Mean umbilical cord serum inorganic fluoride ion concentration in the enflurane group was 2.4 + .2 u moles/L and in the nitrous oxide group 1.8 + .l u mole/L. These values are well below those associated with nephrotoxicity. There was no biochemical evidence of renal toxicity.
Conclusion: Enflurane:02 is an effective analgesic for delivery. In analge- sic concentrations for delivery it does not increase uterine bleeding, depress the neonate or significantly elevate the serum inorganic fluoride ion concentration.
-
-
._
-
-
-
-
-
53

Sunday, April 2, 8:15 A.M.
EFFECT OF DIFFERENT ROUTES OF ADMINISTRATION ON THE PLACENTAL TRANSFER OF MEPERIDINE.
H. Pedersen, M.D.; M. Finster, M.D.; H.O. Morishima, M.D., Ph.D.; J.M. Perel, Ph.D.; Departments of Anesthesiology and Psychiatry, College of Physicians and Surgeons, Columbia University, New York, N.Y.
The placental transfer and fetal uptake of meperidine, following its intra- venous or intramuscular administration to the mother, has never been measured directly. In the present study, pregnant guinea pigs at term receive an injection of 14 C meperidine, 0.5 mg/kg, by either the intra- venous or intramuscular route. At predetermined intervals, varying from 2 to 60 minutes, they are stunned and killed by immersion in liquid nitrogen. After rewarming, fetuses and placentae are removed in toto. Blood samples are obtained from mothers and fetuses by cardiac puncture. Plasma and fetal tissue homogenates are analyzed for meperidine using a
! liquid scintilla-
tion counter. This method measures mostly the parent c mpound, since the metabolic pathways involve cleavage of the labelled N-methyl group and sub- sequent removal as volatile products during analysis. Indeed, thin layer chromatography, performed on samples obtained from 2 experiments, has shown that at least 80% of the radioactivity emanated from unchanged meperidine. Preliminary results, obtained from 16 experiments, indicate that following I.V. injection, a consistently greater proportion of meperidine was trans- ferred to fetuses than after I.M. administration. In animals killed between 5 and 45 minutes after injection-time fetal tissues contained 4-5% of the dose per 100 g weight, after I.V., and only 2-3% per 100 g after I.M. in- jection. Substantial differences between the I.V. and the I.M. groups were noted in the placental uptake of the drug up to 15 minutes. During this period, the proportion of meperidine, in the I.V. group, declined from approximately 15.0 to 7.5% per 100 g of placental tissue. After I.M. injec- tion, the placental content of the drug rose from approximately 1.5 to 6.5% of the dose per 100 g.
In conclusion, intravenous administration of meperidine results in a sig- nificantly greater proportion of the drug being transferred into the fetus. Initially, placental uptake of the drug is also higher when meperidine is given by this route.
In order to determine distribution of meperidine in fetal vital organs, future experiments will include measurements of drug levels in myocardium and brain.
Supported in part by NIGMS Grant GM-09069-15
-
-
.-
-
-
;.

Sunday, April 2, 8:30 A.M. -
THE EFFECT OF APPROPRIATE ANALGESIA ON LACTATE LEVELS
Virginia K. Bond, M.D.
Department of Anesthesiology, Indiana University School of Medicine, Indianapolis, Indiana
This study was undertaken as an effort to document a measurable "cost" for lack of analgesia in labor. There has been considerable publicity con- cerning the negative effects of analgesia upon the fetus or the mother. The effects of anixiety, pain and tension are not easily quantified.
We have been measuring lactate levels at delivery in two groups of patients. Group A consists of those who are unable to cope with the labor and delivery experience. These patients demonstrate acute anxiety by cry- ing and failing to respond to coaching suggestions. Group B patients are provided analgesia which seems appropriate for the individual. Analgesic techniques include epidural, paracervical, prophylaxis plus any of the preceding.
spinal,gas analgesia or psycho-
Each patient was interviewed on admission, as is the routine for the service. Group A patients have either refused analgesia or were denied it by obstetrician preference.
Arterial samples are obtained at the time of delivery. Lactate is measured using the procedure set up by Sigma Company.
As is seen in Fig. 1 no correlation is seen between lactate and length of labor. There is an elevation inlactate level in the patients denied analgesia as compared with those provided appropriate analgesia.
-
-
-
Fig. 1. Delivery lactates show no correlation with time. Group A lactate levels are higher than Group B. Normal resting arterial lactate is u-10

Sunday, April 2, 8:45 P.M. -
DELIVERY ROOM RESUSCITATION OF THE NEONATE:
AN EXERCISE IN PERINATAL CARE
David H. Ralston, M.D.
Department of Anesthesiology University of Washington
Seattle, Washington
Competition for care of the depressed neonate is characteristic of many Level III hospitals, where numerous specialties interface in the Delivery Room.~ Obstetrics, Pediatrics, Anesthesiology, Nursing, and others, although all concerned about care of the newborn, often interact non-productively when confronted with a neonatal emergency. As a consequence, patient care suffers, teaching comes to a standstill, research is impossible, and bitter feuds often result, tending to perpetuate an unsatisfactory (and often dangerous) situation.
A genuine perinatal approach to Delivery Room resuscitation of the neonate will be presented. Implementation began gradually in July of 1977 and is still evolving. It includes attending physicians, housestaff from Obstetrics, Pediatrics and Anesthesiology, and Nurses involved in neonatal care.
The primary goal is to provide excellence in neonatal patient care. Other goals include:
1. Teaching of neonatal resuscitation 2. On-going evaluation, review and assessment of clinical performance 3. Research in neonatal resuscitation
A brief overview of past experiences, details of our approach to Delivery Room resuscitation of the neoiate and preliminary assessment of the program thus far will be presented.
-
-
-
56

Sunday, April 2, 9:OO A.M. -
THE UTERINE AND CARDIOVASCULAR EFFECTS OF AMINOPHYLLINE. Jeffrey Lipshitz, M.D., University of Tennessee Center for the Health Sciences, Department of Obstetrics & Gynecology, Division of Maternal- Fetal Medicine, Memphis, Tennessee.
-
-
Aminophylline, a methylxanthine derivative, blocks the action of
phosphodiesterase and thereby causes an accumulation of cyclic AMP. It
has been shown to reduce uterine motility in non-pregnant women and has
been used in the treatment of premature labor. It was studied in the
same model previously used by us to evaluate certain B-sympathomimetic
drugs. Ten patients, with intact membranes, had labor induced by an
oxytocin infusion. Intrauterine pressure was recorded via a trans-
abdominal intra-amniotic cannula and the area under the pressure curve
was used to calculate uterine activity. The maternal pulse rate was
recorded on the same cardiotocograph using EKG leads. Blood pressure
was recorded every 2 minutes by a Roche Arteriosonde. Aminophylline,
250 mg, was infused intravenously over a 5 minute period and the next
two 15 minute periods was compared to a similar pre-infusion area.
RESULTS: Uterine activity decreased to 87% (P < 0.01) during the
15 minutes after the infusion but was not significantly reduced during
the next 15 minutes. The intensity of the contractions decreased to 80%.
The frequency increased from a pre-infusion rate of 4.9 to 5.3 during the
second 15 minute period. A maternal tachycardia was produced (33 bts/min)
and the fetal heart increased in rate (5-30 bts/min) and beat-to-beat
variability. Blood pressure changes were not significant. By prolonging
the infusion time of Aminophylline to 10 minutes (double dose), an
unacceptably high maternal tachycardia was produced without added uterine
benefits.
CONCLUSION$_: The unfavorable cardiovascularltocolytic ratio produced
by Aminophylline precludes its use in obstetric practice.
57
-
-
-
-
-
-
-.
-
-

Sunday, April 2, 9:15 A.M.
MEPERIDINE AND NORMEPERIDINE LEVELS IN THE MOTHER, FETUS, AND NEONATE FOLLOWING MEPERIDINE ADMINISTRATION DURING LABOR.
B.R. Kuhnert, Ph.D.; P.M. Kuhnest, Ph.D.; M.G. Rosen, M.D. Perinatal Clinical Research Center, CWRU, Cleveland, Ohio.
Meperidine is a very widely used analgesic in obstetrics. However,
the pharmacokinetics of meperidine have not been well studied in obstetrical patients since the availability of new, sensitive analytical techniques.
Therefore, the purpose of this study was to use gas chromatographic and mass spectrometric techniques to study meperidine and its active metabolite, normeperidine in obstetrical patients during labor and in their infants following birth. The concentrations of these compounds were determined in the
maternal plasma during labor, (Figure I) in the umbilical cord venous and
arterial plasma at delivery, and in the urine of the neonate for three days
postpartum. The results indicate that when meperidine is used for maternal
medication during labor (50 mg. I.V.), measureable quantities of meperidine as well as normeperidine reach the fetus. Further, the data suggest that fetal exposure to meperidine is highest 2-3 hours after maternal medication
(Figure II) whereas fetal exposure to normeperidine is highest 4 hours or more after medication. The results of this study may partially explain the more frequent respiratory depression and poor psychophysiological test performance of neonates with long drug-delivery intervals.
Figure I Figure II
-
-

Sunday, April 2, 9:30 A.M. -
-
LIDOCAINE DISPOSITION KINETICS IN
THE PREGNANT AND NONPREGNANT EWE
Duane C. Bloedow, Ph.D., David H. Ralston, M.D. and John C. Hargrove, M.D.
Department of Anesthesiology University of Washington School of MedFcine
Seattle, Washington
Local anesthetic disposition kinetics during pregnant and nonpregnant states may be markedly different. These differences may relate to pregnancy-induced maternal changes, such as changes in blood and/or tissue binding of the drugs, changes in rate or distribution of blood flow, and changes in rate of drug metabolism. In addition, the fetal-placental unit with its capabilities to bind, distribute, and clear drugs will influence maternal disposition kinetics. In this report, the pharmacokinetics of lidocaine in the pregnant ewe are presented and compared to the pharmacokinetics of lidocaine in the nonpregnant ewe.
Intravenous bolus doses of lidocaine hydrochloride were administered at three dose levels (0.5, 1.0, or 2.0 mg/kg) to chronically-catheterized pregnant ewes and at one dose level (1.0 mg/kg) to chronically-catheterized nonpregnant ewes. Arterial blood was sampled at 1, 2, 5, 10, 15, 20, 30, 45, 60, 90, 120 and 150 minutes following injection for determination of lidocaine blood concentration by gas chromatography. The lidocaine blood concentration-time curves were computer-fitted to a two-compartment open model and selected pharmacokinetic parameters were calculated.
In the pregnant ewe, the total body clearance of lidocaine (42 ml/min/kg) was independent of dose over the dose range studied and was linearly correlated with cardiac output. The half-life of the distributive phase and the apparent volume of distribution of the central compartment increased with increasing dose. The half-life of the post-distributive phase and the volume of distribu- tion of the body increased as the dose was increased from 0.5 to 1.0 mglkg. These observations suggest dose-related disposition of lidocaine in the pregnant ewe.
The total body clearance of lidocaine in the pregnant ewe was not different from that in the nonpregnant ewe (39 ml/min/kg) following 1.0 mg/kg doses; however, the half-life of the post-distributive phase, the volume of distribu- tion of the central compartment, and the volume of distribution of the body were all greater in the pregnant ewe than in the nonpregnant ewe. BeCaUse total body clearance between the pregnant and nonpregnant animals remains relatively constant, the greater appa&t volumes of distribution indicate that differences in disposition kinetics may be due to changes in drug distribution. These changes in distribution may result from alterations due to pregnancy in lidocaine binding in maternal blood and/or peripheral tissues and the presence or the fetus with its capacity to distribute and bind the drug.
Supported by HIH Grants GM15991 and GM01160 and NICHD Grant 5POl-HD02274.
-.
59

Sunday, April 2, 9:45 A.M. -
THE EFFECT OF PREGNANCY, INDOMETHACIN AND ANGIOTENSIN II ON BLOOD PRESSURE, UTERINE BLOOD FLOW AND RENAL BLOOD FLOW.
Bruce R. Parks, Ben H. Douglas, and John E. Rawson. Deptartments of ---- Pediatrics and Anatomy, University of Mississippi Medical Center, Jackson, Mississippi.
Normotensive rats and rabbits and spontaneously hypertensive rats (SHR) were used in this study. Ten SHR with a blood pressure of approximately 175 mmHg were bred. Pregnancy produced a decrease in blood pressure. TWO days prior to delivery their blood pressure decreased by 16%. Ten additional - pregnant SHR which received 2 mg/kg/da indomethacin during the last 10 days of pregnancy exhibited a 9% decrease in blood pressure just prior to delivery indicating that prostaglandins may be responsible for some of the blood _. pressure changes observed during pregnancy. The administration of 5 rug/kg/da indomethacin to male SHR for a lo-day period did not alter their blood pressure. Uterine and renal artery flow and blood pressure were monitored acutely in pregnant rabbits (a) before angiotensin II (AII) infusion, (b) during the infusion of 15 ng/kg/min AI1 and (c) during the infusion of AI1 after blocking prostaglandin synthesis with indomethacin. Electromagnetic flow probes were used to measure flow and blood pressure was measured via a catheterized femoral artery. The AI1 infusion produced an increase in blood pressure and uterine artery flow. The AI1 infusion following indomethacin administration also produced an increase in arterial pressure but the changes in uterine artery flow were too variable to assess signifi- cance. Renal artery flow was well autoregulated during the study. These findings are consistent with the suggestion that prostaglandins may mediate changes in blood pressure and flow during pregnancy.
.-
60
-
Sunday, April 2, lo:30 A.M. -
IMPROVED PROGNOSIS OF INFANTS WITH HYALINE MEMBRANE DISEASE TREATED WITH MECHANICAL VENTILATION USING HIGH INVERSE INSPIRATORY/EXPIRATORY RATIO AND LOW PEEP. N.A. Memon, P.A. Branca, G.W. Atkinson, J.J. Kagen, R. Dave, A. Pizzica, R. Fuller. Jefferson Medical College, Philadelphia, PA.
Seven premature infants (group A) with a mean gestational age of 30 weeks, weighing between 1024 and 1645 grams (mean 1354 grams) born with hyaline membrane disease required mechanical ventilation because of hypoxemia (Pa02 29-60 mnHg, mean = 53 mmHg) on FIO2 airway pressure (ET-CPAP).
>0.90 and endotracheal continuous positive These infants were treated with high inverse
inspiratory-expiratory ratio (inverse I/E) and low positive-end-expiratory- pressure ventilation (low PEEP) of less than 5 cm. H20. The mortality and morbidity of group A infants was compared to a similarly affected group of seven infants (group B) with a mean gestational age of 31 weeks, weighing a mean of 1497 grams with a mean Pa02 of 46 nHg on an FIO2 >0.90 with ET-CPAP, who were treated with standard mechanical ventilation and PEEP in excess of 5 cm. H20.
High inverse I/E ratios of 2:l were achieved with either a Bournes BP200 or Servo-900B ventilator by reversing the inspiratory-expiratory time cycling of the ventilator and adding inspiratory pause time. peak airway pressures were limited to 30 cm.
In group A patients,
to 30 per minute while in group B patients, H 0 and respiratory frequency
ef ective ! ventilation often re- quired peak airway pressures as high as 60 cm. H20 with respiratory freauen- ties in excess of 50.
Without changing the FIO2, group A ventilated patients increased the mean Pa02 by 375% with an associated decrease in the mean A-a 02 gradient of 35% compared with group B patients in whom the mean Pa02 and A-a gradient changes were only 225% and 15% respectively. These changes in group A patients were unaccompanied by a drop in mean systemic blood pressure or increase in mean tracheal pressure, whereas, the opposite was true in group B patients. Six group A infants survived with only one instance of pneumothorax, one instance of mild bronchopulmonary dysplasia and no pulmonary hemorrhage. On the other hand, only three group B patients survived and all had had pneumothorax and pulmonary hemorrhage; one of the surviving infants has severe bronchopulmonary dysplasia while the other one has: bronchopulmonary dysplasia to a lesser degree.
Group A patients could be weaned from high FIO2 immediately with an average total time of mechanical ventilation of six days. The FIO2 concentration at 12 and 72 hours in these patients averaged 0.60 and 0.30 respectively. In group B patients the mean delay in weaning from high FIO2 was 7.4 hours and the av- erage total time of ventilation in the survivors was 6.8 days. This "control" group of patients had FIO2 concentrations at 12 and 72 hours of 0.85 and 0.62.
The data indicate that inverse I/E ratio ventilation combined with low PEEP is an effective method of oxygenation in infants with hyaline membrane disease without compromising pulmonary mechanics or hemodynamics. This mode of therapy has greatly reduced the morbidity associated with high PEEP, sub- stantially reduced incidence of bronchopulmonary dysplasia and increased the survival ratio significantly when compared with standard therapy. It should be regarded as the treatment of choice in infants with hyaline membrane dis- ease requiring mechanical ventilation.
-
-
61
Sunday, April 2, lo:45 A.M. -
ADVERSE UTERINE CONTRACTILITY FOLLOWING MEPHENTERMINE ADMINISTRATION EPIDURAL ANESTHESIA
Robert H. Hall, M.D. Department of Obstetrical Anesthesia Utah Valley Hospital Provo, Utah
-
-
-
-
Over a period of two months there was an alarming incidence of abnormal uterine activity observed in obstetric patients during labor and shortly after institution of continuous lumbar epidural anesthesia. Within minutes of the onset of anesthesia, as the patients were being observed with vital signs plus fetal monitoring, prolonged depression of fetal heart rate and vari- ability. The monitoring findings were accompanied by extremely rapid cervical dilatation and precipitate termination of labor. Such changes simulated those seen in premature separation of the placenta. Fortunately, all infants sur- vived delivery in satisfactory physical condition with relatively normal Apgar scores and neonatal responses. In no case was there clinical evidence of abruption of the placenta at the time of delivery. Eight cases were ob- served in approximately 320 patients receiving epidural anesthesia. All patients were given epidural anesthesia by the same anesthesiologist in one private hospital. In none of the cases was there evidence of increased uterine activity prior to the onset of the tetanic uterine contraction pattern.
Inasmuch as this repetitive display was new to the obstetrical unit of the hospital and not observed by anesthesiologists administering obstetrical anesthesia in other private hospitals nearby, a careful review of each case was made to identify one or more details at variance with the procedure followed in hospitals where this phenomenon had not been observed. The only item of management which differed was the administration of mephentermine instead of ephedrine sulfate for treatment of hypotension observed after the -
onset of epidural anesthesia. It is presumed that a marked rise in peripheral vascular resistance characteristic of mephentermine therapy which is not seen following ephedrine administration is responsible for a change in intra- uterine hemodynamics which incites the uterine myometrium to a state of extreme hypertonus.
Individual case presentations outlining time sequences of this abnormal uterine activity in connection with drug administration and technique will be presented.
62

.-
Sunday April 2, 11:OO A.M. -
EVALUATION OF SKIN TEMPERATURE CHANGES DURING EPIDURAL ANESTHESIA USING ADHESIVE TEMPERATURE STRIPS (TE~+A-STRIP) ---
- A. L. Herren, M.D., J. M. Mathers, M.D., S. M. Millbern, M.D.
Anesthesiology Department Naval Regional Medical Center, San Diego, California
Skin temperature changes have bean known to occur in the anesthe- tized area of the body following regional block anesthesia. It is customary to assume that a rise in skin temperature occurs because of the blockage of the autonomic nerves that regulate regional blood flow. Current clinical methods (i.e. pin prick, alcohol swab, etc.) to evaluate the extent of regional blockade are imprecise and rely on patient cooperation. The measurement of skin temperature changes does not require patient cooperation and may be easily quantitated. With the introduction of the self adhesive temperature strip (TEMP-A-STRIP), -
it is possible to easily and accurately monitor the skin temperature. We studied skin temperature changes following epidural block for the management of labor and delivery. SATS were placed at the level of the umbilicus and on the dorsal foot. Standard continuous lumbar epidural technique was employed. Before and after each injection, oral and cutaneous temperatures were recorded. Data presented will correlate skin temperature changes with (1) usage of epidural anes- thesia, (2) core temperature (P.O.), (3) dosages of local anesthesia, and (4) clinical signs such as shivering, nausea, hypotension, etc.
Supported in part by CIP #868-16-1121‘PS BM6S. -
-
-
63
ACID BASE PARAMETERS LATION WITH MATERNAL
IN THE AMNIOTIC FLUID OF NORMAL LATE PREGNANCY. cow- BLOOD. By Hossam E. Fadel, M.D., F.A.C.O.G.t, Gretajo
Northrop, M.D.. Ph.D., H. Robert Misenhimer. M.D., F.A.C.O.G.tt, and H.
Sunday April 2, 11:15 A.M.
Rollie j: Harp; M.S."; From the Departments of Obstetrics and Gynecology and Internal Medicine, Rush Presbyterian St. Luke's Medical Center, Chicago, Illinois 60612, and *Systems and Computer Services, Medical College of Georgia, Augusta, Georgia 30902.
Amniotic fluid (AF) and arterial (radial) blood were obtained almost simul- taneously from 59 healthy third trimester pregnant women. Oxygen and car- bon dioxide tensions (Pq, Pcoz), pH, standard bicarbonate (Bicarb), total carbon dioxide (TCOz), lactate (L), and pyruvate (P) concentrations were measured. AF-Bicarb, AF-TC02, AF-pH, and AF-P showed a statistically sig- nificant negative correlation with gestational age. There was no correla- tion between the other parameters and gestational age. AF-Po2 was low, AF-Pcoz was higher than maternal Pacoz. Both AF-Bicarb, and AF-TC02 were lower than in maternal blood. The AF-pH was 7.07 f 0.08 compared to a ma- ternal pH of 7.42 + 0.03. AF-L was about 6 times, and AF-P 2 times the ma- ternal blood levels. These high levels are believed to be of fetal origin and represent a greater dependence on anaerobic metabolism. The high AF-L contributes to the markedly decreased AF-Bicarb levels and to tie low AF-pH. However, the "acidosis" of AF is not purely metabolic. A respiratory com- ponent is evident (high AF-Pcoz). AF-pH was found to be affected not only by fetal, but also by maternal var- iables, notably maternal PH. On the other hand there was no correlation between AF-Po2, and Paoz, or between AF-Pcoz and Paco2. It may be that AF- Po2, AF-Pcoz, and possibly AF-L correlate better with the intrauterine fetal status than AF-pH. The normal values for the various parameters obtained in this study should be useful as a baseline to monitor changes in the intra- uterine environment in abnormal pregnancies.
I' Present Address: Department of Obstetrics and Gynecology, Medical College of Georgia, Augusta, Georgia 30902. tt Present Address: R.E. Thomason General Hospital, El Paso, Texas 79998
-
-
-
-
64

w% Sunday, April 2, 11:30 A.M.
HYPOTENSION DURING SPINAL ANESTHESIA FOR CESAREAN SECTION: ITS INFLUENCE ON INFANT OUTCOME
Barry C. Corke, M.B. Ch.B., F.F.A.R.C.S., Sanjay Datta, M.D. and Milton H. Alper, M.D.
Department of Anesthesia, Boston Hospital for Women + Harvard Medical School
Despite intensive efforts at its prevention, hypotension still occurs in a significant number of cases during the course of spinal anesthesia for cesarean section. This study was set up to determine whether this hypotension was likely to influence acid-base status of mother and baby and to alter the neurobehavioral responses in the baby.
Eighteen patients scheduled for elective cesarean section under spinal anesthesia, all at term following a normal pregnancy, were studied. All pa- tients were pre-loaded with 500-1000 ml 5% dextrose in lactated Ringer's prior to the administration of spinal anesthesia. Tetracaine, 7-9 mg, was used for the spinal block, the height of the block was T6 with a maximum spread to T2. A left lateral tilt was instituted insnediately following completion of the block.
Any patient having a fall in systolic blood pressure to below 90 torr was classified as having hypotension. Eight-one per cent of the patients studied had hypotension, all were of short duration, maximum 2 minutes, and responded to ephedrine, lo-25 mg. The average time from induction of the block to delivery of the infant was 15 minutes.
_
Umbilical artery and venous blood were drawn from a doubly clamped segment of cord, and maternal arterial blood was taken at the time of delivery for blood gas data.
The babies were subjected to a neurobehavioral test, as described by - Scanlon, between the second and fourth hour following delivery.
Maternal,arterial and umbilical arterial pH's in the hypotensive group were significantly more acidotic, but there was no significant difference found between the two groups with respect to umbilical artery and vein pO2 and pCO2. The neurobehavioral tests showed no significant differences between the two groups (Table 1).
-
Table 1
Non-Hypotensive (n=5~) '.
Hypotensive Significance (n=13)
Maternal Artery 7.46* 7.40 < 0.01
Umbilical Artery 7.33 7.22 < 0.025
*Mean
65
-,

EFFECT OF MATERIAL ANTIHYPERTENSIVE THERAPY ON OFFSPRING ORGAN DEVELOPMENT. Ben H. Douglas and Kenneth V. Smith, Department of Anatomy, Univ. Miss. Med. Ctr., Jackson, Ms. 39216.
Spontaneously hypertensive rats (SHR) were used to determine the effects of antihypertensive therapy on the development of offspring. Ten SHR received 32 mg chlorothiazide, 0.04 mg reserpine and 3 mg hydrala- zinc each day during pregnancy. Five SHR served as controls. This combination of drugs reduced the blood pressure from a control level of 172 + 4 mmHg to 110 + 5mmHg (p 0.01). The offsprings of the treated animals had a reduced growth rate which persisted to maturity. At 6 weeks the male offsprings of the untreated SHR were 46% larger than the offsprings of the treated SHR and the female offsprings of the untreated SHR were 49% larger than the offsprings of the treated SHR. Organ weight/ body ratios of the offsprings were determined. Although blood pressure of the offsprings were not different the heart weight/body weight ratio was larger (pLO.025) in the offsprings of the treated animals (5.7 X lob3 for the males, 5.6 X 10e3 for the females) than in the offsprings of the untreated animals (4.6 X 10-3 for the males and 4.9 X 10-3 for the females). There was a satistically significant difference between the weight of the pituitary glands of the males and females (of both groups) with the female pituitary glands being larger (0.005/ p LO.01. The pituitary weight/body weight ratio was smaller in the offsprings of the untreated animals. These data demonstrate that this type of antihyper- tensive therapy of pregnant SHR adversely affects the growth of the offsprings.
Sunday, April 2, 11:45,A.M. -
-
-
-
66

Sunday, April 2, 12:OO P.M. -
SUCKING IN TERM INFANTS FROM BIRTH TO FOUR HOURS POST BIRTH, AS MEASURED WITH AN ELECTRONIC SUCKOMETER. Gene C. Anderson-Shanklin, College of Nursing, Uni- versity of Florida; Melen McBride, School of Nursing, University of Michigan; & Dharmapuri Vidyasagar, Department of Pediatrics, University of Illinois at the Medical Center, Chicago.
The development of the sucking response was studied in full-term infants from I minute to 4 hours post birth. Thirty infants (9 male and 21 female; 15 Black, 9 Spanish surname, and 6 white) were studied at the University of Illi- nois Hospital in Chicago. Mean and standard error of the mean values were 39.8 (+ .2) weeks for gestational age, 8.30 (5 .14) for l-minute Apgar score,
3282.2 (+ 95.2) grams for birth weight, and 8.87-(+ .13) for 5-minute Apgar
score. The sucking response has a suction (negative pressure) and an expression
or biting down (positive pressure) component. Maximum intensity pressures of these components were measured at pre-specified times for eight consecutive 15- second intervals with a silastic nipple attached to a portable electric sucko- meter. The suckometer records a digitized output of pressure transducers on a printer which issues data on paper tape. The mean of the eight pressures has been calculated for each baby. The mean of these means for each component and each time of measurement is presented in Figure 1. Sucking pressures at 1 and and 5 minu,tes post birth were measured in the delivery room. The infant was then ad- mitted to the nursery and placed in a warm incubator for the remainder of the study. Varied positions were allowed. Following measurement at 4 hours post birth, the in- fant was fed and the feeding was evaluated with a feeding scale.
The suction pressures peaked at 103 torr at 90 minutes post birth (see Figure 1) and steadily decreased thereafter to 65 torr at 4 hours post birth. The expression scores correlated (r = .50; df = 316; p < .OOl). A better correlation is obviated be- .’ cause expression is present before suction : appears in some infants immediately following birth. Expression may be a more sensitive indicator of condition. Expression pres- sures are sometimes present in term newborns before any suction pressures appear, and ex- o pression pressures are the last to disap- I, Q pear if the sucking response weakens. Mean expression pressures correlated with feeding
fi*n I. Yom rtim ti W” upa -c -I In Y)tii*h~Y,h%U+*Ilar.rxntbnth
scores (r = .44; df = 24; p < .025), but ,_.swfi@ _.L*a,
suction pressures did not (r = .26; df = 24; ” p < .l).
Normative data were gathered on’lb additional term newborns in the alert inactive state on the first and second days post birth. These newborns had all received at least two formula feedings. The suction pressures were 95.8 and 103.3 torr, respectively. Expression pressures were 25.0 and 24.0 torr. These values are in approximately the same range as are those of the transitional new- born between 1 Andy 2 hours post birth. Perhaps these normative data, considered together with the transitional newborn data presented in Figure I, indicate the full-Lurm transitional newborn is able to feed at least as well between 1 and 2 hours post birth as at 4 hours post birth.
-
-
-
-
-
67

Sunday, April 2, 12:15 P.M. -
-
IMPACT OF MATERNAL DIABETES ON AMNIOTIC FLUID CHROMIUM (AFCr) Edward D. Conner and George Cassady. Division of Perinatal
Medicine, University of Alabama in Birmingham, Alabama. Fetal 'leaching' of maternal Cr has been suggested by scattered
observations of elevated Cr levels in the term and unusually low Cr levels in the pre-term infant as well as be diminishing maternal Cr levels with increasing gestation and parity. Available data suggest an inverse relation between Cr levels and glucose tolerance. This study represents an ongoing attempt to develop normative data on Cr in the perinatal period.
AFCr was measured in a graphite furnace (coeff of var. 11%: _ . recovery rate 95-105%) in 46 AF from 37 patients. GROUP n(WOMEN/AF) AGE PARITY L/S GESTATION AFCr (range)
Diabetics (DM) 20/22 24.8 0.9* 2.3 36.6" 2.2*(0.3-4.4) High-Risk (H-R) 7/10 28.0 1.8 1.7 34.6* 2.9(0.1-9.6) C/Section (C/S) IO/l4 22.4 3.0 2.0 38.6 3.4(0.7-7.4) (Mean values; *p < 0.05 by t test)
AFCr was < 3.0 PPB in 16/22 samples from DM but was > 3.0 PPB in 7/14 samples from women undergoing repeat C/S (x2 < 0.057. AFCr was found to increase directly with gestational age in all groups but this was significant only in the control group (r = 0.62).
The data support the concept that Cr increases during gestation in the fetal unit as reflected by the increasing AFCr levels. The data also suggest that AFCr (and fetal accretion of Cr) is reduced in pregnancies complicated by diabetes when they are compared to normal pregnancies.
-
-
-
-
-
-
-
68
-
-.
-
.-
-
In1977 we presented a series of patients undergoingCesareansection in whnlwe maswxd gastric pl in an effort to find a reliable metlrd of elevating thep~shve the critical aspirationlevelof 2.5.
(Xlrearlierstudiesin~lvedacantrolgKXlPWfiiChreceived.4~of atmpine, and ti dose levels of glycopyrrolate 2 nq snd -004 nq/kg. Briefly, reviewingthosefinlings,wefounlthatthosereceivingatropineandlawdose glympyrrolate - still at risk (40% and 55% respectively). Evenwiththe high &se of glyaqyrmlate mre than 30% had pH of 2.5 or less.
Therefore,wedecided to stuiy 2 nrxe series of patients. lb mewe administered an antacid alone as premdicationwithlO% being found at risk. Theothergmupisbeinggivensntacidtiglycopyrro late .004 q/kg. The resultsofthissMygroupwillbepresentedatthemeeting.
J. IQger Bulkml, M.D. Assistant Pmfessor Departnent of Anesthesiolcqy Cbstetrics andGynecology
William E. Marks, Jr., M.D. AssociateFmfessor Ikpartmnt of Anesthesiology
Msdical university of Sn~thC.zolina 171Ashhy Avenue c!harleston, south Carolina 29403
71
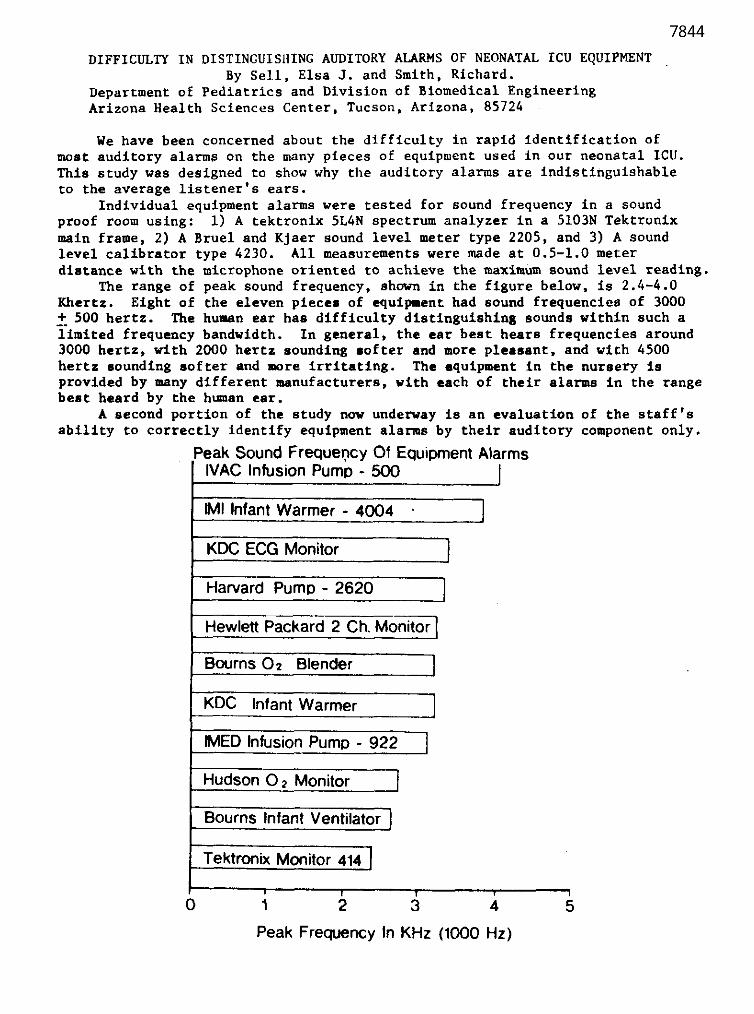
-
r.
DIFFICULTY IN DISTINGUISRING AUDITORY ALARMS OF NEONATAL ICU EQUIPMENT By Sell, Elsa J. and Smith, Richard.
Department of Pediatrics and Division of Biomedical Engineering Arizona Health Sciences Center, Tucson, Arizona, 85724
We have been concerned about the difficulty in rapid identification of most auditory alarms on the many pieces of equipment used in our neonatal ICU. This study was designed to show why the auditory alarms are indistinguishable to the average listener's ears.
Individual equipment alarms were tested for sound frequency in a sound proof room using: 1) A tektronix 5L4N spectrum analyzer in a 5103N Tektronix main frame, 2) A Bruel and Kjaer sound level meter type 2205, and 3) A sound level calibrator type 4230. All measurements were made at 0.5-1.0 meter distance with the microphone oriented to achieve the maximum sound level reading.
The range of peak sound frequency, shown in the figure below, is 2.4-4.0 Khartz. Eight of the eleven pieces of equipment had sound frequencies of 3000 _+. 500 hertz. The human ear has difficulty distinguishing sounds within such a limited frequency bandwidth. In general, the ear best hears frequencies around 3000 hertz, with 2000 hertz sounding softer and more pleasant, and with 4500 hertz sounding softer and more irritating. The equipment in the nursery is provided by many different manufacturers, vith each of their alarms in the range beat heard by the human ear.
A second portion of the study now underway is an evaluation of the staff's ability to correctly identify equipment alarms by their auditory component only.
Peak Sound Frequency Of Equipment Alarms IVAC Infusion Pump - 500
I
M Infant Warmer - 4004 1 J
KDC ECG Monitor 1
Harvard Pump - 2620
Hewlett Packard 2 Ch. Mom
Bourns 02 Blender I
Hudson 0 2 Monitor I
Bourns Infant Ventilator
Tektronix Monitor 414
, 1 1 0 1 2 3 4 5
Peak Frequency In KHz (1000 Hz)
72

Effect of Variations of pK and Protein Binding on the Transplacental Equilibrium of Local Anesthetics
West Virginia University Medical Center University of Iowa
R.L. Kennedy, M.D., M.K. Comstock, M.D.
Local anesthetfcs used 1n obstetrics produce fetal/maternal concentration ratios (F/M) within a range consistant for each drug. The ratios appear consistant from one study to another regardless of actual observed blood concentrations and the sampling time following administration. This suggests that a maternal-fetal equilibrium occurrs which is responsible in maintaining the F/M within a range characteristic for each drug. The pK and protein binding ability are physical properties that vary from one drug to another and are noted to be related to placental transfer.
In this study we have assumed that there is indeed an equilibrium established and have attempted to demonstrate how the pK and protein binding affects the equilibium.
Protein binding of a local anesthetic leaves a free fraction available for placental transfer. The free fraction will equilibrate across the placenta and, therefore, will be equal on both sides of the placenta. Protein binding also occurs in fetal plasma. Hence, the maternal free fraction (FWF) times the total maternal concentration (CM) will equal the fetal free fraction (FFF) times the fetal total concentration CC,).
CMXFMF = FFFxCF
Equation 1 CF = FMF
CM FFF
The relationship of the pK to the equilibrium may be examined by solving the Henderson-Hasselbalch equation for maternal and fetal blood and is expressed:
CF 10PK-PHF + 1 Equation 2
-z
cM lOPK-PHW + 1
Three drugs, bupivacaine, lidocaine, and mepivacaine were used as examples of commonly used local anesthetics with different pK's and protein binding abl.lities. Using a program- mable calculator, the F/M was calculated and plotted using maternal pH values of 7.4, 7.5, and 7.6 and fetal pE values from 6.9 to 7.4. The curves were replotted to demonstrate the additional effect of protein binding.
The results show that: (I) The F/M increases directly with the pK. At normal pH values, the pK effect is small, (2) Protein binding produces the greater effect. For a fetal concentration less than the maternal, the fetal binding rate must be less. Being highly bound in the maternal blood provides a small numer- ator and a large denominator is derived from a lower fetal binding ability (Equation 1).
73

ELECTROLYTE AND WATER BALANCE IN PREGNANT NGRMOTENSIVE AND HYPERTENSIVE ANIMALS. Ben H. Douglas, P. Lynn Brown, and Roger A. Norman. Depts. Anatomy and Physiology, Univ. Miss. Med. Ctr., Jackson, Ms. 39216.
A technique has recently been developed which allows for the determination of the steady-state relationship between mean arterial pressure (AP) and the output of sodium and water (Norman, R. A., s &., Am. J. Physiol., in press, 1978) in the experimental animal. The present study was designed to determine the steady-state relationship between AP and the output of sodium and water in pregnant spontaneously hypertensive rats (PSHR) and in pregnant normotensive control rats (PNQO. Five animals from each group were studied as follows: Sodium and water was infused at various rates over a period of several days. Control intake was set at 30 ml/day Ringer’s solution via intravenous infusion. The infusion was increased progressively to 60, 90, and 120 ml/day. The Ringer’s solution was infused for 24 hr at each rate. Intake and output Na and water were measured and the AP was monitored continuously. The increase in salt and water intake was accompanied by almost equal in- creases in salt and water output. The blood pressure of the PNCR either did not change or decreased a few m&g at the highest infueion rates but the blood pressure of the PSUR increased by 9% at the higher infusion rates. The arterial pressure-urinary output relationship in the PSRR was almost parallel to that in the PNCR but it was shifted to higher AP levels. Therefore, to excrete the same fluid load the PSHR required an increased AP and the parallel shift indicated reduced glomerular filtra- tion coefficient or renal vasoconstriction.
74

INTERPERSONAL SKILLS: IMPLICATIONS IN THE CARE OF THE OBSTETRIC PATIENT
W.U. Brown, Jr., M.D.
Department of Anesthesia, Boston Hospital for Women, and Harvard Medical School
Health care professionals need to have effective interpersonal skills in order to attend and respond to obstetric patients, their families and other professiona
Expertise in this area can be developed through brief intensive training programs. These skills can effect both emotional and physical functioning of patients. In obstetrics, situations involving maternal and neonatal complications, birth defects etc. can be managed in a constructive helpful manner.
Interpersonal description of the Case examples will
skills will be defined and a brief training methodology will be given. be discussed.
.S.
75
LIDOCAINE DISPOSITION KINETICS IN THE
PREGNANT AND NONPREGNANT GUINEA PIG
John C. Har rove, M.D., David H. Ralston, M.D., Duane C. Bloedow, Ph.D.
Department of Anesthesiology University of Washington School of Medicine
Seattle, Washington
Pharmacokinetic parameters are essential to understand drug disposition and physiologic effect. Pregnancy may modify the disposition kinetics and physiologic effects of local anesthetics. The present study was designed to compare lidocaine pharmacokinetics after bolos administration to the pregnant and nonpregnant guinea pig and to measure maternal and fetal lidocaine tissue concentrations after constant-rate infusions.
Both nonpregnant and r.ear-term pregnant guinea pigs were anesthetized with halothane and nitrous oxide for placement of central arterial and venous catheters. Following a two-hour recovery period, a 3 mg/kg bolus dose of lidocaine hydrochloride was administered over 10 seconds into the maternal venous catheter. Arterial blood was sampled at 1, 2, 5, 10, 15, 20, 30, 45, 60, 90, 120 and 150 minutes following injection, for determination of lidocaine concentration by gas chromatography. Lidocaine blood concentration data were analyzed using a two-compartment open model of drug disposition. In constant- rate infusion studies, lidocaine hydrochloride was infused intravenously for approximately three 6 half-lives. At the termination of the infusion, arterial blood was sampled, the animal was sacrificed and maternal and fetal tissue samples were obtained for determination of lidocaine concentration.
Comparisons of pharmacokinetic parameters following lidocaine bolus administra- tion to the pregnant and nonpregnant guinea pigs indicate significant differences in the 6 half-life, total body clearance, volume of distribution of the peripheral compartment, and the elimination rate constant. The volumes of distribution of the body and of the central compartment were unchanged by pregnancy. Preliminary results from the constant rate infusion studies show little differences between maternal and fetal tissue levels.
The longer 6 half-life in the pregnant guinea pig presumably results from the decreased total body clearance of lidocaine during pregnancy and not from a change in distribution since the volumes of distribution of the body and of the central compartment were unchanged with pregnancy. Although the volume of distribution of the peripheral compartment is greater during pregnancy, the kinetic parameters of the two compartment model suggest that the long B half- life is not a result of low clearance of lidocaine from the peripheral compart- ment. The decreased total body clearance of lidocaine during pregnancy in the guinea pig may reflect a decrease in hepatic blood flow or a decrease in hepatlc extraction or metabolism of lidocaine.
Future plans to define pharmacokinetic parameters include additional bolos studies in pregnant and nonpregnant guinea pigs and constant-rate infusion studies to determine maternal and fetal tissue levels of various local anesthetics under steady-state conditions.
Supported in part by NIH Grants GM15991 and GM01160 and NICHD Grant 5POl- HD02274.
76

LUMBAR STMPATBBTIC BLOCK WITH BDPIVACAINE: ANALGESIA FOR LABOR
Ramon V. Meguiar, LT. MC and A. Scott Wheeler, LCDR, MC N&al Regional Medical Center. Portsmouth, Virginia
Bilateral paravertebral lumbar sympathetic block for analgesia during la- bor has been reported to be easily administered, efficacious, and is associated with a low incidence of maternal complications. Although the block may accel- erate labor, it has been infrequently used, due to the brief duration of anal- gesia provided by procaine, xylocaine, and tetracaine. Our experience with bu- pivacaine sympathetic blocks corroborated those cited above, except that the duration of analgesia was acceptable with 0.5% bupivacaine.
This report describes the clinical parameters of this anesthetic in 40 primigravidas with an average age of 21.1 years and an average gestation of 40 weeks. Thirty three were in the active phase of labor having a mean (*SD) cervical dilation of 4.8+ 0.9 cm, Patients were included only if the fetal heart rate pattern was normal for a period exceeding thirty minutes before blockade. Frequency of contractions, FRR, maternal blood pressure and pulse, and skin temperature (foot) were measured before and every five minutes after blockade. Following an intravenous infusion of 500 ml of D5RL, sympathetic blocks' were administered bilaterally at L2 with 10 ml of 0.5% bupivacaine and 1:200~000 epinephrine being injected per side. Patients were returned to the lateral position. The times to peak analgesia and reappearance of abdominal and back pain were noted, as was the time from block to complete cervical di- lation. Pudendal, caudal, saddle block, or infiltration anesthesia were given for delivery. Apgar scores were assigned at 1 and 5 minutes.
Results: Good analgesia was obtained in 38 patients with maximal effect at 7.5 % 3 minutes (mean f SD). Twenty eight patients delivered prior to resolution of the block; in the remaining 12, the mean duration of analgesia was 283 f 103 minutes. Maternal blood pressure and pulse were similar to the pre-block values at all times after infusion. In the 33 patients in active labor, the mean time from sympathetic block to complete cervical dilatation was 158 f 92 minutes. Significant change in the frequency of contractions was not noted. Noticeable changes in fetal heart rate were not observed, and the mean Apgar scores were 7.9 * 1.3 and 9.0 l 0.8 at 1 and 5 minutes, respectively.
Sympathetic blockade with 0.5% bupivacaine provides reliable analgesia of a long duration and has a low incidence of undesirable side effects.
(1) Moore, DC: Paravertebral block of the second lumbar sympathetic ganglia, in Anesthetic Techniques for Obstetrical Anesthesia and Analgesia. Springfield, Charles C. Thomas, 1964, pp 125-128.
77

MATERNAL AND FETAL BLOOD LEVELS OF PANCURONIUM DURING CESAREAN SECTION
by
Ezzat Abouleish, M.D., L. Wingard, Ph.D., R. McKenzie, M.D. S. de la Vega, M.D., N. Uy. M.D.
University of Pittsburgh School of'Medicine
This in-progress study is designed to determine the maternal and fetal ratios of pancuronium (P) during elective cesarean section and the effect of the speed of injection on these levels.
The.procedure is explained to the patient and a consent form is obtained. None of the patients has had a systemic disease, antibiotic, or magnesium sulphate. The course of pregnancy has been normal to the full-term, and there has been no fetal distress or compromise. No premeditation is ordered with the preoperative visit. On arrival to the Delivery Room, an intravenous cannula is inserted and 5 ml of blood is collected and used as control for P estimation. The uterus is displaced to the left, 0.4 mg atropine is injected intravenously, ECG applied, 02 administered, blockade monitor attached, and the abdomen is cleansed. Thiamylal dose, 4 mg/kg is calculated; two thirds of the dose is injected intra- venously followed by 0.1 mg/kg P. According to the rate of P injection, the cases are randomly divided into two groups:
A P is rapidly administered in the form of a "bolus". B 1 ;,,~~~;;ed in 10 ml saline, is steadily injected in
Respiration is controlled using 02 until adequate muscle paralysis is obtained. The remaining portion of surital is then injected and intubation is performed. Anesthesia is maintained by 4:2 N20-02 mixture. At the delivery, maternal arterial (FlA), maternal venous (MV), umbilical venous (UV), and umbilical arterial (UA) blood samples are collected separately for P estimation using fluorimetry. Also, blood samples are collected for determing the acid-base states of the mother and fetus. Following delivery, the anesthesia is supplemented by intravenous injection of 0.2 mg/kg morphine and 0.1 mg/kg diazepam. At the end of surgery, the residual muscular paralysis is reversed by atropine and prostigmine injection.
The baby's condition is evaluated using Apgar scores, time to breathing, any need for resuscitation, and the acid-base state. The ratios of P levels, namely MA/WV, UV/UA, and MA/UV are calculated. The results of the study and their significance will be presented.

z-
-
>-
-
'1YrJCARDIAL INFARCTION DURING PREGNANCY: ANESTHETIC
MANAGEMENT OF A CASE FOR CESAREAN SECTION
Medical College of Georgia, Augusta, Georgia
Skina ii. Fadel, M.D.
MYocardial infarction associated with pregnancy and labor is rare and frequently fatal. A forty-year-old white female, thirty,-two weeks' gestation, was admitted on January 2, 1976, to the coronary care unit with a diagnosis of acute myocardial infarction. The patient has a history of chronic bronchial asthma; hypertension for five years and Type IV hyperlipedemia for One-Year. In May, 1975, a diagnosis of early pregnancy was made when the patient presented with chief complaint of nausea and vomiting. The patient did not seek prenatal care, and discontinued all her medications on her own because of persistent nausea and vomiting.
In the coronary care unit, the patient showed frequent PVCs and changes indicating acute subepicardial injury of the antero-lateral wall. The arrhy- thmia was controlled by intravenous lidocaine as well as propranolol 20 mg tablets orally every six hours. The patient also received aldomet and was heparinized. OnJanuary 20, 1976, the patient had precordial pain not relieved by two nitroglycerin tablets and EKG revealed inverted T-wave in V5-V6. Termin- ation of pregnancy by cesarean section was recommended.
Continuous lumbar epidural anesthesia was selected for the patient. The relation of myocardial oxygen demand to coronary perfusion is the most import- ant factor in patients with myocardial infarction. As a result of sympathetic blockade accompanying regional anesthesia, the venous return is decreased, the myocardial stretch (or tension) is reduced, and the cardiac output is diminished. However, the peripheral vaso-dilatation and consequent drop in total peripheral resistance results in reduction of the ventricular after laad. The end-result, therefore, appears to be that even though the coronary perfusion is reduced, it is well tolerated by the patient due to reduced myocardial work and oxygen demand. Heparin was discontinued twenty-four hours prior to surgery while methl dopa and propranolol were maintained until the night of surgery.
In the operating room, a radial artery catheterization and a Swan-Ganz cath- eter were performed. Arterial and venous pressures were continously displayed on a multichannel oscilloscope and recorder. 500 ml of 5% dextrose in LR were infused intravenously before injecting 25 ml of 0.5% bupivacaine in the epidural space. The operating table was tilted to the left, and left manual displacement of the uterus was maintained. Ten minutes later, the blood pressure dropped to 70/40 and the heart rate was 60/min and regular, the rate of fluid infusion was increased, ephedrine 10 mg intravenous was injected and repeated twice. This was followed by a rise in blood pressure to 190/100 and an increase in heart rate to lO/min. No arrhythmia or chest pain occurred. The blood pressure and pulse rate dropped slow- ly to 100/50 and 90/min over the following five minutes. The level of anesthesia was between T5-T4. A live, male infant with Apgar score of 9-10 was delivered. The patient did well post-operatively and was discharged on the 11th post-operative day on the following medication: digoxin, nitroglycerin, aldomet, Atromid-S, chlorthalidone (hygroton), and Quibron tablets.
On June 6, she was found to be in fair condition and was maintained on the same therapy.
79

,-
c-
-
NORMAL PREGNANCY: A MODEL OF SUSTAINED RESPIRATORY ALKALOSIS. By Hossam E. Fadel, M.D., F.A.C.0.G.t. Gretajo Northrop, M.D., Ph.D., H. Robert Misen- himer, M.D., F.A.C.O.Gltt, and H. Rollie .I. Harp, M.S.*. From the Depart- ments of Obstetrics and Gynecology and Internal Medicine, Rush Presbyterian St. Luke's Medical Center, Chicago, Illinois 60612, and *Systems and Com- puter Services, Medical College of Georgia, Augusta, Georgia 30902.
Blood gases and other acid base parameters were studied in arterial blood samples from normal third trimester pregriant women. Compared to the non- pregnant status, the oxygen tension (Paoz) and Oxygen saturation were slightly increased. Carbon dioxide tension (Pacoz), standard bicarbonate, carbon dioxide content, and base excess were all markedly decreased. The pH was slightly increased, but still in the normal range. Blood lactate was slightly increased, while blood pyruvate was normal or slightly in- creased. There is increased maternal oxygenation in pregnancy and no evi- dence of ventilation/perfusion defect nor significant shunting of blood in the lungs during pregnancy. Hyperventilation of pregnancy results in hy- pocapnia. This sustained hypocapnia would lead to respiratory alkalosis were it not for the compensatory buffer systems, including the renal re- sponse. In fact, the sustained respiratory alkalosis is maximally corn- pensated. There was no evidence of metabolic acidosis. The hyperlacta- temia of pregnancy is possibly secondar
HJ to stimulation of the glycoly-
tic pathway by the slightly decreased activity. Prkgnancy therefore is a unique natural model for this acid base status "maximally compensated respiratory alkalosis". Significance bands were cfnstructed to give the 95% confidence limits of anticipated response of H and Bicarb to chang- ing Pacoz.
t Present Address: Department of Obstetrics & Gynecology, Medical College of Georgia, Augusta, Georgia 30902 tf Present Address: R.E. Thomason General Hospital, El Paso, Texas 79998
80
.-
-
?-
.-
-
_-
PAPILLARY MUSCLE NECROSIS (M-N): A COMMON NEONATAL AUTOPSY FINDING Emmalee Setzer, Rufino Ermocilla, and George Cassady, Division Perinatal Medicine, University of Alabama, Birmingham, Alabama.
136 consecutive neonatal autopsies, during a 6 month period, were re-examined for evidences of myocardial ischemia. New sections were cut from both right and left ventricular apices and anterior papillary muscles of tricuspid and mitral valves. Autopsies of patients,with congenital heart disease (19), multiple congenital anomalies (3), or with cardiac tissue unavailable (30) were excluded. 22 of the remaining 84 (26%) had ischemic changes in papillary muscles. These included coagulation necrosis, contraction bands, and/or vacuolar degeneration. In 17 of 22 the lesions were more prominent or were found soley in the right ventricle: 10 were bilateral; 11 were in the right ventricle; and 1 was in the left ventricle.
Selection of the next-consecutive-neonatal autopsy after each case of MN yielded a control population of 22 cases. Race, sex, inborn/outborn ratio, and incidence of asphyxia as determined by fetal monitoring and/or Apgar score were similar in MN and control groups. Gestational age and birth weight more commonly exceeded 34 wk (13/22) and 3000 g (8/22) in the MN group than in the controls (6/22 and 2/22; pc.05). Meconium aspiration syndrome was also more common in MN (8/22) than in controls (2/22).
MN, especially involving the right ventricle, is a frequent neonatal autopsy finding. The lesion seems to be more common in dying neonates who are more mature, of greater birth weight and with meconium aspi- ration syndrome.
81
PHAIL'IACOKINETICS AND PHYSIOLOGIC RESPONSE TO LIDOCAINE IN NEONATAL LAMBS:
INFLUENCE OF POSTNATAL AGE
c
David H. Ralston, M.D. and Duane C. Bloedow, Ph.D.
Department of Anesthesiology University of Washington School of Medicine
Seattle, Washington
Drug dis~position kinetics in the neonate are poorly understood. Amide local anesthetics administered to the parturient during regional anesthesia are present in neonatal blood and may produce significant physiologic effects. Neonates, in fact, may be more sensitive than the adult to the toxic effects of local anesthetics. Impaired clearance of drug may account in part for the increased sensitivity of the neonate to certain amide local anesthetics.
-.
To define more precisely lidocaine disposition kinetics and physiologic effects in the neonate, we studied five neonatal lambs at weekly intervals from birth to four weeks of age. In addition, two of these animals were studied at six months of age.
We administered lidocaine hydrochloride (3.0 mg/kg) intravenously over ten seconds to five awake lambs. Arterial blood samples were drawn at 1, 2, 5, 10, 15, 20, 30, 45, 60, 90, 120 and 150 minutes following the injection. Lidocaine 'was measured with gas-liquid chromatography and blood concentration-time curves fitted by computer to a two-compartment open model of drug distribution. Blood pressure, heart rate and temperature were measured continuously while arterial blood gases and hematocrit were obtained during a thirty minute control period and at five and 150 minutes following the injection.
Arterial blood lidocaine concentrations at one minute increased with increasing postnatal age (from 2.75 "g/ml on days 0 to 3 to 9.33 pg/ml at week four postnatally). Total body clearance of lidocaine (53.2 ml/kg/min) and the half- life of the post-distributive phase (46.9 min) did not appear to change with age although considerable variability was present.
No significant changes in heart rate, mean arterial blood pressure, acid-base status, or oxygenation occurred in response to the 3.0 mg/kg lidocaine dose at any age period studied. No visible evidence of seizures or muscle twitching occurred.
Our findings indicate that the non-asphyxiated neonatal lamb at birth, and up to four weeks of age, tolerates a 3.0 mg/kg bolus injection of lidocaine without difficulty. Pharmacokinetic analysis shows significant differences in peak drug levels with increasing postnatal age. No significant differences in clearance or elimination rate of lidocaine were seen in the groups as a whole. However, three out of five lambs in the immediate postnatal age group (O-3 days) had clearances less than 30 ml/min/kg, indicating need for further pharmacokinetic studies during this critical postnatal period of adaptation.
Supported in part by NIH Grants GM15991 and GM01160 and NICHD Grant SPOl- HD02274.
82
,-
r-
.-,
r
r
P
,-
I
f-
e
PLACENTAL TRANSFER OF DIAZEPAM AND RO 21-3981, A NEW BENZODIAZEPINE DERIVATIVE.
UNIVERSITY OF CALIFORNIA, IRVINE and UNIVERSITY OF CALIFORNIA, LOS ANGELES
Charles W. Graham, M.D Ph D * Kenneth A. Conklin, M.D., _.---___-_-.-_--~:'--z_." Ph.D., Ronald L. Katz, M.D.;
and Charles R. Brinkman, III, M.D.
RO 21-3981 is a new, water soluble benzodiazepine derivative with sedative
properties similar or superior to diazepam. 1
Unlike diazepam, however, its
low lipid solubility suggests that little placental transfer and subsequent fetal
effects would occur. To assess this, the present study compared placental
transfer of RO 21-3981 and diazepam in pregnant ewes. Seven sheep with singleton
pregnancies of approximately 100 days gestation were instrumented with maternal
and fetal vascular c,atheters and a common iliac artery flow probe. Following
5 days convalescence, 0.2 mg/kg diazepam or RO 21-3981 was injected IV bolus, and
maternal and fetal arterial blood samples were obtained at 1, 5, 15, 30, 60, 120,
and 180 minutes for assay of diazepam and RO 21-3981 by gas chromatography.
Arterial blood gases were determined periodically, and fetal and maternal
hemodynamics were monitored throughout, as well as uteroplacental blood flow.
Rapid placental transfer of both diazepam and RO 21-3981 was apparent by
1 minute (40-115A/min). In marked contrast to diazepam, however, fetal
maternal ratios of RO 21-3981 were significantly lower (0.05 VS. 0.5). These
ratios did not change with time for either drug. Fetal as well as maternal
arterial blood gases remained unaltered, and hemodynamlcally the only observed
alteration occurred in fetal heart rate which increased 20-40% for diazepam and
lo-25% for RO 21-3981. This tachycardia persisted 30 minutes for diazepam and
60 minutes for RO 21-3981. The low fetal-maternal ratios and minimal hemodynamic
alterations associated with RO 21-3981 when compared to diazepam suggest that
RO 21-3981 may be well suited for use as a psychotropic adjunct in women undergoing
labor and delivery.
1 Conner JT, et al.: RO 21-3981 for intravenous surgical premeditation and
induction of anesthesia. Anesth Analg. IN PRESS. _--._ _-__,__
83

t-
?-
F
,-
,-
STUM OF ANESTHESIA FOR CESAREAN SECTION: -A Revi% of 376 Cases - ---
Barry L. Balonsky, M.D. Gertie F. Marx. M.D. Albert Einstein College of Medicine. Bronx. N.Y.
Because of the increased incidence in recent yesra in CesSrean Sections, we reviwed those performed in our institution during 1977 to determine which anesthetic technique produced the beat results from both maternal and fetal points of view.
.
Our techniques were ss follows: A. General Anesthesia: Patient induced with either Pentothsl 4 ma&; Ketsmine 1 mq/K~: or a combination of Ketsmine $ mc?;/Kg with Pentothsl 1 mziW. Succinylcholine wss then i?lven, patient intubsted and N20: 02 given in a 40:60% ratio, combined with Succinylcholine 0.1% solution I.V. until infant delivered. Anesthesia was then continued in a routine fashion.
B. Regional Anesthesia: (1) Extrsdursl: A Ep$dursl cstheter was inserted at L3-4; and 15-20 cc
of 3% 2-Chloro-procaine sdministered to achieve s T4 senssry level. After delivery of infant the epidursl wsa continued with either 2-Chloro-procaine 3% or 0.5% Bupivscsine. To avoid any significant hypotenstion the patient was well hydrated with 500-750 cc Ringers lactate in 5% Dextrose rater and Left Uterine Displacement wss used in sll cssss.
(2) spinsl: 7-10 Ian: Tetrscaine in s hyperbaric solution was given. The ssine precautions of hydration snd Left Uterine Diaplscement was followed.
The results obtsined sre summeriaed in the following table; (General Anesthesia is grouped tottether because the results were very similar irrespective of technique used).
1 Percentage of Infants with 1 Minute Apgsr Scores
[
Elective (121 Cases)
--__II
I Y of Cases ._ ..~.. __. .,... ,... --
Ernl?r~*nCy
I 1 :255 Cases)
i 1 i # Of Csses [
-
t
.,
i
i...
Apuar Score ~___.
8 - 10 ..~ .,,.~...,
5- 7
a4

,-
THE EFFECTS OF A B2-SYMPATHOMIMETIC DRUG ON MATERNAL GLUCOSE, INSULIN, GLUCAGON AND FREE FATTY ACID LEVELS. Jeffrey Lipshitz, M.D., University of Tennessee Center for the Health Sciences, Department of Obstetrics and Gynecology, Division of Maternal-Fetal Medicine, Memphis, Tennessee.
The introduction of Qsympathomimetic drugs, such as hexoprenaline, which have minimal maternal cardiovascular side-effects, has made it possible to extend the use of these drugs in obstetrics from premature labor to a wide variety of obstetric emergencies, including fetal distress in labor. However, the metabolic effects caused by these drugs may have important consequences to both the mother and the baby.
METHODS: After an overnight fast, 9 women in the 3rd trimester of pregnancy had 3 basal blood samples drawn at 15 minute intervals. A 4 ml bolus of normal saline was given and 3 further samples were taken at 45, 60 and 90 minutes, then 10 ug of hexoprenaline in 4 ml diluent was injected and further samples taken at 100, 110, 120, 135, and 150 minutes.
RESULTS: Before Peak After Time to Peak
Hexoprenaline Hexoprenaline Value (Minutes)
Glucose mg/lOO ml 53.2 60.9 30 Insulin uU/ml 13.3 30.0 Glucagon pg/ml 65.1 80.8 :: Free Fatty Acids p mol/L 519.3 913.3 30
COMMENTS: Figure)sts
The time taken for the metabolites to reach maximum values (see the following: The rise in glucose and FFA were not responsible
for changes in insulin and glucagon concentrations. The rise in insulin occurred before the rise in glucose and did not cause a fall in plasma glucose. It is concluded that B receptor stimulation has direct actions on insulin and glucagon release and on g ? ucose and free fatty acid metabolism.
These the use of patient in
changes in the maternal metabolic milieu will be discussed relative to hexoprenaline in the treatment of acute fetal distress and the diabetic labor.
GLUCOSE
00
ig
0 . .
INSULIN . :
i .
: GLUCAGON A : . *
.
10 j.lG HEXOPRENALINE TIME MINUTES
85

THE HEIGHT OF EPIDURAL SENSORY BLOCK OBTAINED FOLLOWING THE ROUTINE
USE OF 20 ml OF 0.75% OF BUPIVACAINE FOR CAESARIAN SECTION
R. Hodgkinson and Farkhanda Husain
Obstetrical Anesthesia Unit, University of Texas at San Antonio
Apart from safety the primary aim in producing epidural block for Caesarian Section must be to produce adequate analgesia. To produce adequate analgesia for Caesarian Section in the context of an obstetrical teaching program a T-4 level is needed for most patients.
Epidural block was induced for Caesarian Section in 150 patients using a standard dose of 20 ml of 0.75% bupivacaine given directly through the epidural needle in the lateral position. The injection of bupivacaine was given at a standard rate of 1 cc per second and the table was maintained in the horizontal position. In patients in whom an epidural was already in place for the control of labor pain the injection was made through the epidural catheter with the patient in the dorsal position or through an epidural needle.
The height of the block was measured at 5, 10, 15, 20 and 30 minutes after injection, at the time of removal of the epidural catheter when the vertebral spines were accessible for identifying the exact level of sensory block and in the recovery room.
The height of the block obtained will be analyzed with reference to the effect of
1. Obesity 2. Patient height 3. Previous administration of local anesthetic in those
patients who had received an epidural block for the alleviation of labor pain
4. The interspace entered
86

THE SAN ANTONIO BARS AS AN AID TO ESTABLISHING EPIDURAL BLOCK FOR CAESARIAN SECTION
Robert Hodgkinson, M.D.
Obstetrical Anesthesia Unit, University of Texas at San Antonio
The San Antonio Bars consists Of tW0 removable vertical bars clamped to the side of the O.R. table at the level of the patient shoulders and hips. They can be attached and detached in approximately the time needed to attach an arm board to the operating table.
They serve the following functions during epidural anesthesia:
1. to prevent the patient falling from the table and give her a sense of security. The San Antonio Bars are safer than relying on a nurse holding the patient. In practice her attention to the patient is frequently distracted by requests for tape etc. With the bars in place she can concentrate on improving patient position and giving other assistance.
2. as a teaching tool to show good position (i.e., that one shoulder is vertically above the other, one hip is vertically above the other and the spine is not twisted. By the patient pressing against the bars the amount of flexion can be increased.)
3. as an aide to the positioning of patients unable to communicate in English or experiencing difficulty in understanding how to position herself.
The San Antonio Bars have been used in several hundred eeidural blocks for Caesarian Sections during 1977.
Modification of the bars for use on a bed allows their use in epidural anesthesia for vaginal delivery.
87

USE'OF EIAZQXIDG 11: PREIWTDRE LABOR
William W. Bethea, M.D.* Pederico G. Mariona, M.D.
*Hutzel Hospital Wayne State University School of Qdicine
Detroit, Nichigan
Prematurity is observed in 10.5% of the obstetrical pntients seen In
the Out-Patient Clinic at'Hutze1 Hospital. The goal of this on-going study is
to reduce prematurity thro'ugh active management of patients presentin:: only
premature labor and no other pathology. The agent being used is diazoxide--a
benzothindiazine derivative--that relaxes smooth muscle and inhibits uterine
contractions.
Patients
tractions prior
obstetrical and
who were admitted with the complaint of rhythmic uterine con-
to term were selected at random. A complete menstrual,
medical history was obtained on each patient in addition to
review of the current antenatal care record. They were then placed under the
protocol forthreatened premature delivery if, as stated above, no concoxitanr
illness was suspected or present. The patient's weight was recorded and
gestational age established according to the date of the last ~~orm;.l menses
plus uterine growth and size which were dctermincd upon physical examination.
The pa,t:ie~lt was excludrti from tha study if the &eStdtiOZil a&z by air,e..r;o~rhe;
and uterine size by exalrdnation varied by more than four we&s.
Cervical effacement and dilation were detenr,il;cd a;ld chsrted upon pelvic
examination. Effacement of more than 50% and/or dil.ation greater than 2 CCL'S
were considered diagnostic. Indirect obstetrical monitorin:: was used to
SSCertairt the presence of utrrjnc contrnctions and--ff presznr--their frequz?cy
._ ,_ 2
F-
,-
.-
active trcatm~:nt and again upon ending the infusion of Diazoxide. Diazoxide--
an antihypcrtensive drug that is devoid of diuretic cffccts--was diluted in .
250 cc's of normal raline and intravenously given at a dosage of 5mz$kg
body weight and at a rate of .125 mg/kg/minute for a period of 35 to 40
minutes consistently. Maternal pulse and blood pressure were monitored at
S-minute intervals by conventional methods. The fetal heart rate and uterine
contractions were continuously controlled by use of a two-channel electronic
obstetrj.cal monitor (Hewlett-Packard, 803OA).
Upon recurrence of rhythmic contractj:ons, a second dose of Dinzor.i.dc
proportionate with the first was administered by the same route and time period.
The dose was never repeated unless a minimum of 6 hours had elapsed, and no
more than 4 doses were given within a 24 hour period. The number of infusions
given during the treatment period was one at minlnum and four maximum.
The treatment was considered successful if labor was inhibited for
seven days or more. Of the 18 patients treated in this manner, 2 developed
obvious clinicd signs of amnionitis with gross signs of chorioamnionitis
present at delivery. The management, results and delivery outcome of'these
2 patients plus the remaining 16 are presented.
89