Embed Size (px)
Citation preview

Emily Richards, CRNA
Carcinoid Tumors: Anesthetic Considerations
Objectives Describe the pathophysiology of carcinoid tumors and
carcinoid syndrome.
Describe signs and symptoms of carcinoid syndrome and carcinoid crisis.
Discuss current recommended anesthetic management of patients with carcinoid disease.
Describe how to prevent and treat a carcinoid crisis in the perioperative period.

Case Study 61 year old man with metastatic carcinoid disease admitted
to teaching hospital for lethargy, sweats, & malaise.
Extensive liver involvement
Received his usual monthly dose of lanreotide 120 mg sq on time on admission
For 2 days had over 20 abdominal exams by physician trainees.
2nd evening of hospital stay, patient developed STach, hypoxia, hypotension, hypoglycemia.
Morrisroe, et al., 2012

Case Study Patient was transferred to ICU where he continued to
deteriorate
Echo confirmed severe carcinoid heart disease
Carcinoid Crisis was suggested as diagnosis
Octreotide 100 mcg/hour IV and decadron started
Resulted in rapid improvement
Rapid response from octreotide treatment confirmed diagnosis of carcinoid crisis precipitated by repeated abdominal exams, despite receiving his lanreotide on time.
Morrisroe, et al., 2012

Case Study Excellent example of
potential mortality associated with unrecognized crisis
Crisis that occurred without surgical or procedural stimulation
Crisis may still occur despite current somatostatin-analog treatment
Carcinoid Tumor Incidence
Dierdorf, 2003;Quaedvlieg, 2001; Vaughn & Brunner, 1997; van der Leely & de Herder, 2005
Rare, but incidence of diagnosis is increasing
Current incidence is between 0.2-10 in 100,000 people
Autopsy incidental findings as high as 8%
75-80% of patients with carcinoid syndrome have small bowel tumors
5 year survival rate overall 80% Survival rate decreases to 18-19% with distant metastasis
25% of carcinoid tumors produce carcinoid syndrome and <10% of people with tumor develop syndrome

Carcinoid Pathophysiology
Melnyk, 1997; Modlin, et al., 2005
Neuroendocrine tumors that arise from GI tract or lungs other rare sites
Tumors synthesize, store, and release up to 40 bioactive mediators Amount and effect to a specific symptom is unclear.
Most prominent are serotonin, tachykinins, kallikrein, & prostaglandins
Liver usually inactivates mediators secreted into the portal circulation GI tumors usually only develop syndrome with distant
metastasis



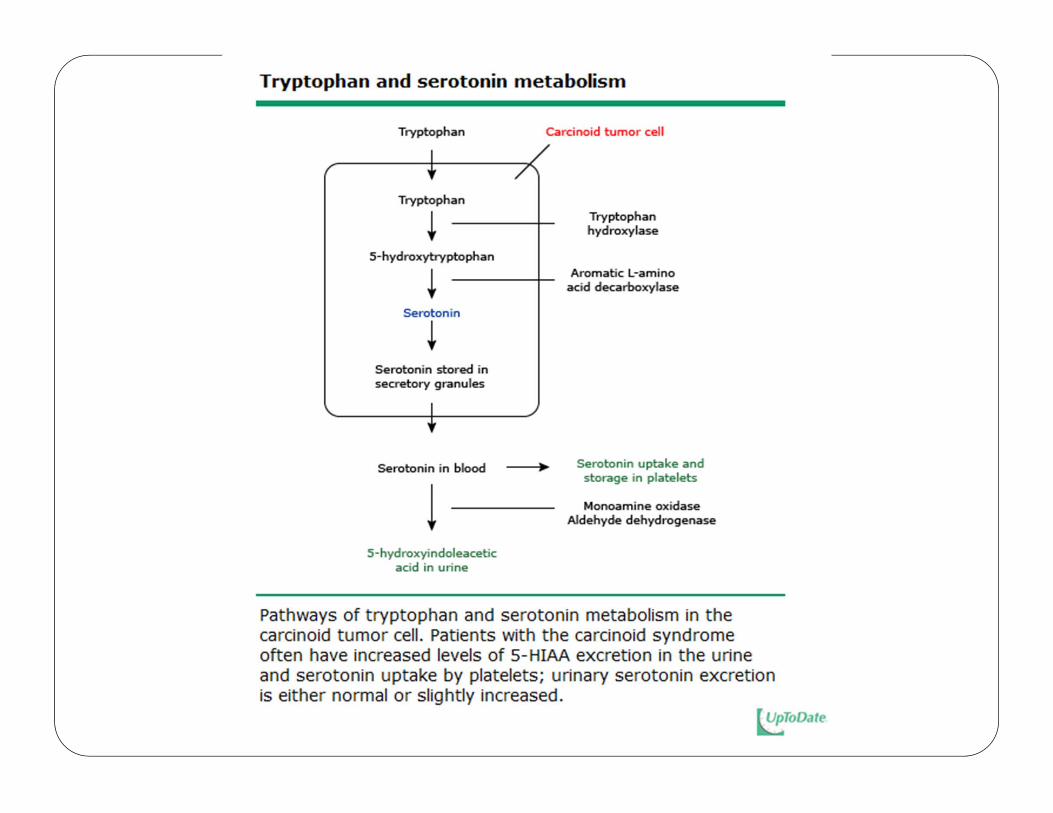
Tryptophan Metabolism
Feldman, 1987; Swain, Tavill, & Neale, 1976
1% of dietary tryptophan is converted into serotonin
In carcinoid syndrome, 70% of tryptophan is converted
Serotonin is metabolized into 5-hydroxyindoleascetic acid (5-HIAA)
Some foregut (gastric, bronchial) carcinoids lack aromatic amino acid decarboxylase Produce 5-hydroxytryptophan and histamine instead Hindgut (distal colon and rectum) rarely secrete serotonin or
any other hormones and are unassociated with hormonal syndromes even when metastatic
Tryptophan Deficiency
Swain, Tavill, & Neale, 1976
The 70 fold increase in serotonin synthesis may result in tryptophan deficiency Decreased protein synthesis Muscle wasting Hypoalbuminemia Nicotinic acid deficiency Pellagra

Pellagra
Swain, Tavill, & Neale, 1976
Rough scaly skin
Glossitis
Angular stomatitis
Mental confusion

Serotonin
Hendrix, et al., 1957; von der Ohe, et al., 1993; Lie, 1982
Most likely cause of diarrhea in carcinoid syndrome Stimulates intestinal secretion, motility, and inhibits absorption Stools up to 30/day, watery and non-bloody Occurs in 80% of carcinoid syndrome patients
Stimulates fibroblast growth and fibrogenesis Can lead to peritoneal and cardiac valvular fibrosis May be cause of severe abdominal cramping

Signs and Symptoms
Flushing
Grahame-Smith, 1987; Maton, 1988; Törnebrandt, et al., 1983; Marsh, et al., 1987; Claure, et al., 2000
Sporadic flushing is clinical hallmark of carcinoid syndrome
Occurs in 85% of patients with carcinoid syndrome
Begins suddenly, lasts 30 seconds to 30 minutes
Involves face, neck, and chest: red to purple color
Mild burning sensation
Potential mediators are bradykinins, prostaglandins, tachykinins, substance P &/or histamine

Flushing
Grahame-Smith, 1987; Maton, 1988; Törnebrandt, et al., 1983; Marsh, et al., 1987; Claure, et al., 2000
Maybe accompanied by severe hypotension and tachycardia
As disease progresses, flushing lasts longer, and may become more diffuse and cyanotic
May be triggered by: Certain foods & alcohol Defecation Emotional events Mechanical stimulation Anesthesia Episodes triggered by anesthesia may last hours and present with severe
hypotension

Wheezing
Warner, 1985
10-20% of patients with carcinoid syndrome have wheezing and dyspnea, often during flushing
Should not be mistaken for bronchial asthma
Treatment with beta agonists can trigger intense, prolonged vasodilation (controversial)
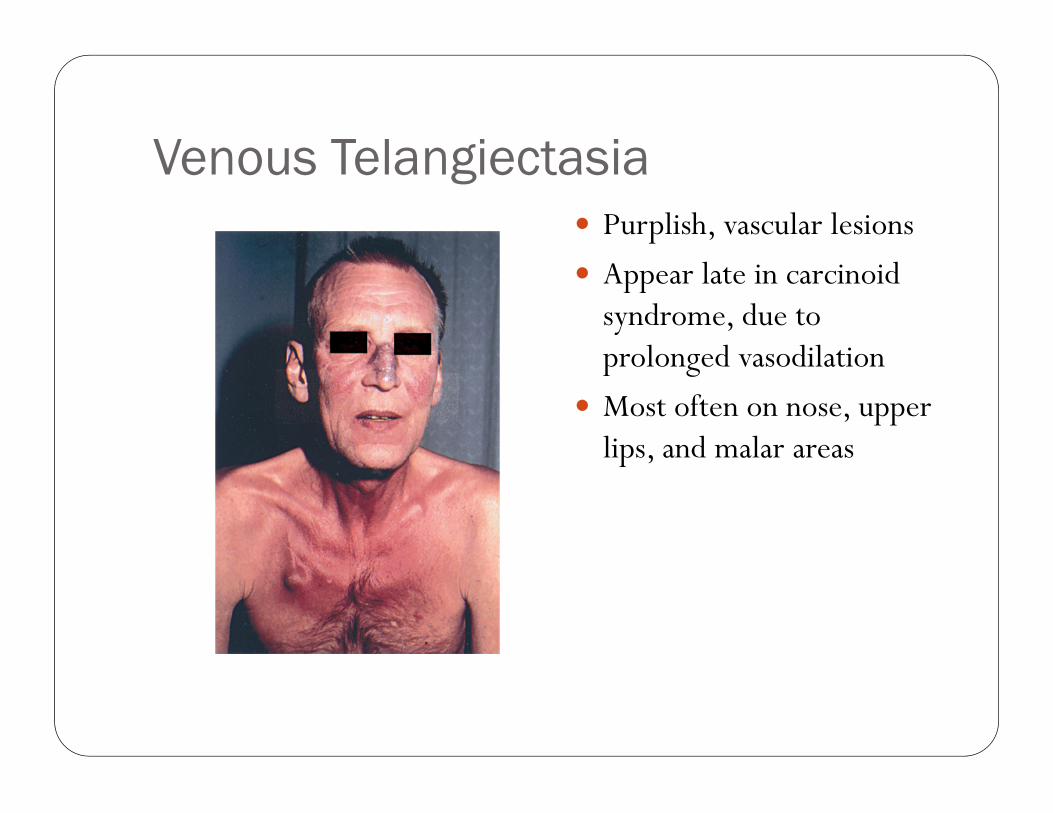
Venous Telangiectasia Purplish, vascular lesions
Appear late in carcinoid syndrome, due to prolonged vasodilation
Most often on nose, upper lips, and malar areas

Figure 1: A 72-year-old man with carcinoid syndrome, showing flushing, cyanosis and telangiectasia.
Rehman H u CMAJ 2009;180:1329-1329
©2009 by Canadian Medical Association
Atypical Carcinoid Syndrome
Melmon, Sjoerdsma, & Mason, 1965
Bronchial & carcinoids outside GI tract can release substances directly into systemic circulation & are not immediately cleared by the liver syndrome can be present without mets
Bronchial carcinoids exhibit atypical carcinoid syndrome flushing and diaphoresis
Other symptoms are tremor, periorbital edema, lacrimation, salivation, disorientation, hypotension, tachycardia, diarrhea, dyspnea, asthma, oliguria, and edema

Atypical Carcinoid Flush
Vaughn & Brunner, 1997;Roberts, Marney, & Oates, 1979
Patchy, sharply demarcated, serpiginous, and cherry red
Intense Pruritis
Severe and prolonged, lasting days
Also associated with primary gastric carcinoids that produce histamine
May be treated with H1 & H2 antagonism
Carcinoid Heart Disease
van der Lely & der Herder, 2005
Carcinoid syndrome can lead to carcinoid heart disease in up to 66% of patients
Plaque-like, fibrous endocardial thickening involving usually the right side of the heart Causes retraction and fixation of leaflets of the tricuspid and
pulmonary valves
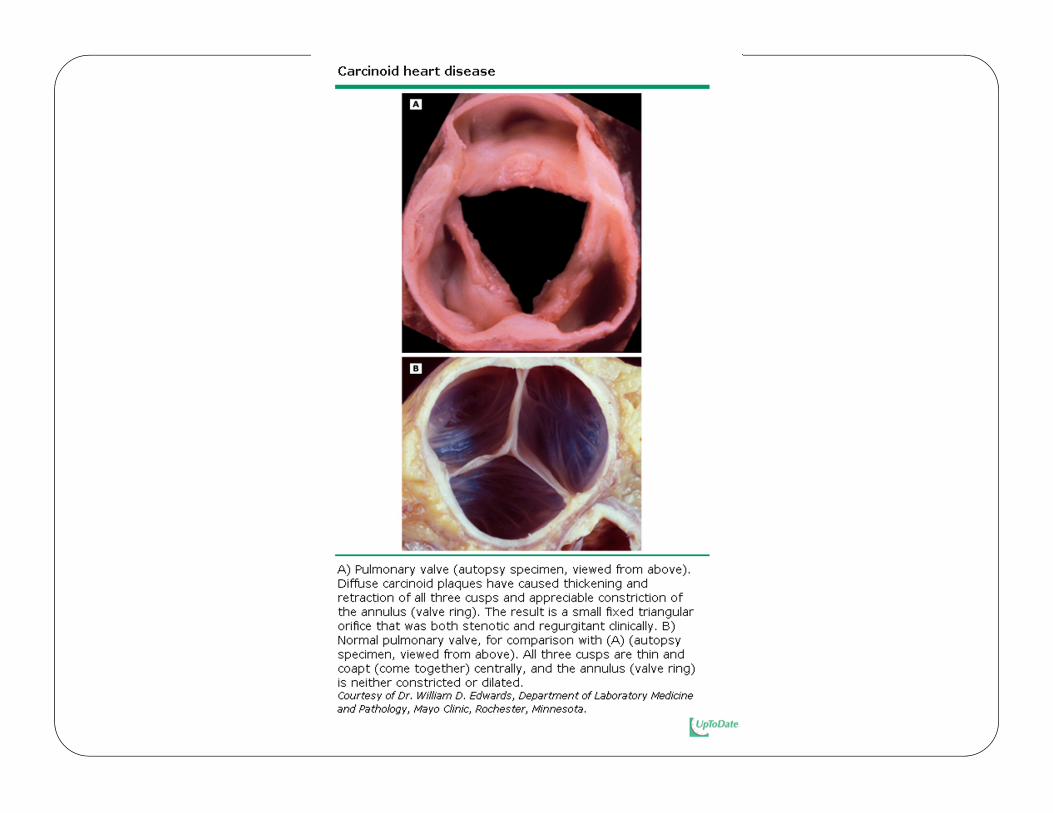

Carcinoid Heart Disease Tricuspid regurgitation is most common Tricuspid stenosis, pulmonary regurgitation & stenosis also
occur
Left-sided carcinoid heart disease occurs in less than 10% of patients and is usually associated with atrial right to left shunt (PFO) or primary bronchial carcinoid
Patients should have thorough assessment to look for signs of cardiac dysfunction
van der Lely & de Herder, 2005; NCCN, 2011
Signs of Carcinoid Heart Disease
Powell, Mukhtar, & Mills, 2011
Reduced exercise tolerance
Orthopnea
Paroxysmal dyspnea
Peripheral edema
Coronary artery spasm may occur with flushing episodes

Severe Carcinoid Heart Disease with Pulmonary Stenosis Creates high right-sided heart pressures
Tricuspid Regurgitation
Hepatomegaly
Pulsatile liver
Hepatic resection may be impossible without large blood loss due to high venous pressures and hepatic vein pressures Seriously consider pulmonary valve surgery before hepatic
resection in this patient population
Powell, Muhktar, & Mills, 2011
Carcinoid Crisis Results from overwhelming amount of bioactive mediators
from tumor
Predominant symptom is wide blood pressure fluctuations Usually hypotension Serotonin may cause vasoconstriction or vasodilation, therefore
hypotension or hypertension may be seen
Calcium and catecholamines may provoke release of mediators from tumor Typical anesthesia management of hypotension may escalate the
crisis
Vaughan & Brunner, 1997; Woodside, Townsend & Mark-Evers,2004; Déry,1971; Memom & Nelson, 1997
Carcinoid Crisis Case Report(Marsh, et. al., 1987) Pt had 5-HIAA confirmed carcinoid syndrome presenting for
resection of primary tumor in terminal ileum. No mention of pretreatment with steroids, H1 or H2
antagonists, or other 5-HT2 antagonist Induction of anesthesia uneventful 5 minutes after induction, the abdominal wall was exposed
and vigorously scrubbed with betadine. Flushing occurred and BP unattainable by manual BP cuff, no
peripheral pulses, HR 140. In 10 minutes, patient received 1000ml D5LR, 140 mcg
phenylephrine, 1 gram CaCl, 1 mg epinephrine
Marsh, et.al., 1987 continued VTach occurred after
epinephrine was given Resolved to sinus rhythm
after 50 mg lidocaine
Radial cut-down site bloodless
Patient was cyanotic
Only carotid pulses palpable

Marsh, et al. Conclusion Permission was obtained for use of experimental drug,
Sandoz 201-995
50 mcg IV was given twice
Within 40 seconds, peripheral flow resumed, cut down site bled, arterial puncture was accomplished
Systolic arterial pressure maintained throughout the remainder of lengthy surgery
Sandoz 201-995 is known today as octreotide
1987

Anesthetic Management of Carcinoid Tumors and Syndrome
Somatostatin-analogues Somatostatin is a 14-amino
acid peptide that inhibits the secretion of a broad range of hormones. Acts by binding to
somatostatin receptors , which are expressed in the majority of carcinoid tumors
Somatostatin analogs (octreotide and lanreotide) bind to somatostatin receptors on tumor cells Highly effective at inhibiting
the release of bioactive amines
Reubi, et al., 1990; Veal, et al., 1994; Bloom & Polak, 1987
Somatostatin-analogues Octreotide (also called sandostatin) is an octapeptide analog
of somatostatin Longer duration of action then endogenous somatostatin
Flushing and diarrhea are significantly improved in >80% of carcinoid syndrome patients
Increasing the dose of octreotide usually controls refractory symptoms
Other somatostatin-analogues Octreotide LAR (monthly injection) Lanreotide (monthly injection also available) Pasireotide (not yet available in US or other countries)
Veall, et al., 1994; Bloom & Polak, 1987; Kvols, et al., 1986; Rubin, et al., 1999; Schmid & Schoeffter, 2004
Preoperative Assessment Search for preoperative comorbidities: Obstruction Malnutrition Dehydration Anemia Electrolyte imbalance Diarrhea Flushing and other symptoms of carcinoid syndrome Cardiovascular history upmost importance due to higher risk of
right-sided & biventricular heart disease
Powell, Muhktar, & Mills, 2011

Communication Successful anesthetic management dependant on pre-op
optimization
Good communication between endocrinologist, anesthesia provider, and surgeon
Seek advice from centers with more expertise in managing carcinoid syndrome
Patients should be viewed as having multi-system disease
Require thorough pre-planning and post-op managements in ICU environment, by clinicians familiar with carcinoid management
Powell, Mukhtar, & Mills, 2011; Mancuso, et al., 2011
Perioperative Risk Kinney, et al. (2001) published a retrospective study of 119
carcinoid syndrome patients that underwent elective resection by same surgeon in same institution over 14 years
Perioperative deaths or complications occurred in 15 (12%) patients Flushing, sustained hypotension, bronchospasm, acidosis, VT Higher frequency of carcinoid heart disease than in those who
did not have complications (53% vs 15%, P = 0.002) Urinary 5-HIAA output was significantly higher in this group All 119 patients had elevated 5-HIAA
3 patients died >10 days post op d/t comorbidities or sepsis 2 had severe carcinoid heart disease
Kinney, et al., 2001

Preoperative Assessment Carcinoid Syndrome symptoms should be controlled with
necessary somatostatin analogs before treatment directed at tumor debulking in order to prevent crisis Recheck urinary 5-HIAA levels after control of symptoms
before proceeding to surgery
Multiple current articles advocate for pre-op echo in all patients with carcinoid syndrome for correct management of cardiac disease
Vaughan, Howard, & Brunner, 2000; Yates, 2010; Powell, Muhktar, & Mills,2011

Preoperative Assessment Kinney, et al. (2001) concluded that presence of carcinoid
heart disease and high pre-op urinary 5-HIAA were significant risk factors for perioperative complications, including death
Veall, et al. (1994) reviewed 22 records of patients with carcinoid syndrome undergoing laparotomy and found noassociation between high 5-HIAA levels and perioperative morbidity Poor predictor of cardiovascular stability. One patient had lower abnormal 5-HIAA level, but very severe
hypotension
Preoperative Assessment Mancuso, et al. (2011) provide a current article on anesthetic
considerations for carcinoid syndrome based on literature review and unpublished data from LSU
Concludes that the severity of carcinoid syndrome does not predict the severity of perioperative complications Urinary 5-HIAA provides an indicator of disease progression,
not risk of severity of intraoperative response to tumor manipulation
Chemistry, urinary 5-HIAA, CBC, glucose, EKG, low threshold for cardiology consult
Carcinoid Crisis Prophylaxis Even if carcinoid tumor patient lacks carcinoid syndrome,
prophylaxis with octreotide is essential because stimulus that may release vasoactive mediators is much greater than daily living stimuli
Tumor activity must be minimized at least the day before surgery with octreotide
Multiple articles recommend starting a continuous infusion at 50 mcg/hour at least 12 hours prior to surgery
Increase octreotide dose until symptoms of carcinoid syndrome are abated before proceeding with surgery
Powell, Mukhar, & Mills, 2011; Yates, 2010; Ramage, et al., 2005

Carcinoid Crisis Prophylaxis In their case study, Yazbek-Karam (2009) state pre-op SQ
doses of octreotide used did not prevent crisis during RFA, & recommend pre-op octreotide infusions of 100-300 mcg/hr before manipulation of liver mets
Yates (2010) recommends starting 12 hours before surgery and continuing for an minimum of 48 hours postoperatively especially important in patients with carcinoid heart disease that may not be
able to compensate for severe hemodynamic changes

Carcinoid Crisis Prophylaxis Veall, et al.(1994) found that after octreotide was given,
hypotension less severe and more responsive to additional boluses of octreotide
Vaughan, Howard, & Brunner (2000) recommend additional prophylaxis of chlorpheniramine & ranitidine for H1 & H2
antagonism to prevent any histamine effects from tumor manipulation
Avoiding Sympathomimetics Epinephrine and norepinephrine could be hazardous Norepinephrine shown to activate kallikrein in the tumor and lead to
synthesis and release of bradykinin paradoxically worsening vasodilation and hypotension However hypertensive responses have been seen
Powell, Muhktar, & Mills (2011) recommend cautious small doses of phenylephrine
Vaughan & Brunner (1997) feel phenylephrine or other adrenergic agonist are dangerous as they may trigger further peptide release In other case studies, phenylephrine had no effect on hypotension
In Zimmer, et al. (2003), most extreme hypotensive and tachycardicevent occurred after administration of atropine, phenylephrine & theoadrenaline-caffedrine
Powell, Muhkar, & Mills, 2011; Cortinez, 2000
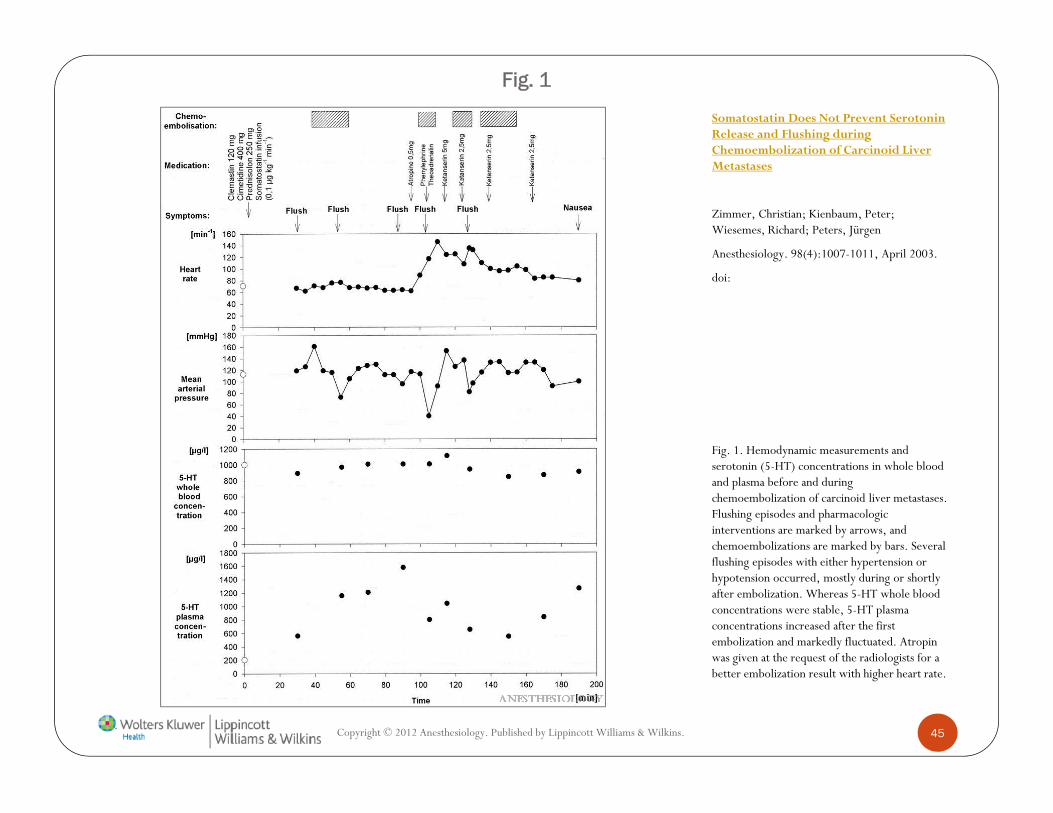
Fig. 1
Fig. 1. Hemodynamic measurements and serotonin (5-HT) concentrations in whole blood and plasma before and during chemoembolization of carcinoid liver metastases. Flushing episodes and pharmacologic interventions are marked by arrows, and chemoembolizations are marked by bars. Several flushing episodes with either hypertension or hypotension occurred, mostly during or shortly after embolization. Whereas 5-HT whole blood concentrations were stable, 5-HT plasma concentrations increased after the first embolization and markedly fluctuated. Atropin was given at the request of the radiologists for a better embolization result with higher heart rate.
Copyright © 2012 Anesthesiology. Published by Lippincott Williams & Wilkins. 45
Somatostatin Does Not Prevent Serotonin Release and Flushing during Chemoembolization of Carcinoid Liver Metastases
Zimmer, Christian; Kienbaum, Peter; Wiesemes, Richard; Peters, Jürgen
Anesthesiology. 98(4):1007-1011, April 2003.
doi:
Anesthesia Technique Anesthetic goal is to prevent mediator release that may be
caused from stress, induction of anesthesia, intubation, and tumor manipulation Stable, controlled conditions Avoid BP variation Stable induction Adequate depth of anesthesia prior to intubation Maintenance of anesthesia and analgesia Hypothermia may trigger release as well
Invasive monitoring should be used for quick detection of cardiac instability
Mancuso, et al., 2011; Powell, Muhktar, & Mills, 2011
Anesthesia Technique GA usually plan of choice to prevent sympathectomy that
accompanies neuroaxial anesthesia Epidural and subarachnoid blocks have been successful in
patients with carcinoid syndrome
SAB has been successful with preopeative fluids, octreotide, and low dose spinal anesthetic supplemented with low dose intrathecal opiods
Hypotension must be avoided to prevent release of tumor mediators and treatment with sympathomimetic agents that may further release tumor mediators
Orback-Zinger, Lombroso, & Eidelman, 2002;Vaughan & Brunner, 1997; Mancuso, et al., 2011

Anesthetic Technique Choice of technique should be made based on familiarity and
preference TIVA and inhalational techniques have both been successful Morphine and atracurium should be avoided due to histamine
release Abdominal defasciculations with succinlycholine may cause
release of peptides from tumors Remifentanil (0.05-0.2 mcg/kg/min) may be ideal for
optimized intubation, titratable analgesia, and intraoperative BP control Benefits must be balanced by risk of hypotension & bradycardia
Powell, Muhkar, & Mills, 2011
Epidural Anesthesia Thoracic epidural insertion before induction of GA
recommended for stable analgesia to reduce risk of carcinoid crisis triggered by pain or stress intra-op and post-op
Drug volumes and concentrations should to titrated cautiously to prevent hypotension the would need to be treated with sympathomimetics Hypotension and sympathomimetics both may lead to mediator
release
Powell, Muhkar, & Mills 2011
Hepatic Resection
Powell, Muhkar, & Mills, 2011
Carries the most significant risk for carcinoid patients
May be especially useful in hepatic resection to maintain low CVP during clamping of hepatic artery and portal vein to avoid backflow into liver and venous bleeding, which would further exacerbate hypotension

Anesthetic Equipment Large bore IV access
Fluid warmers
Rapid infusion system
Invasive monitoring depending on local resources & cardiac involvement A-line CVP TEE
Powell, Muhkar, & Mills, 2011; Vaughn, Howard, & Brunner, 2000

Intraoperative Octreotide Kinney, et al.’s study of 119 patients began in 1983. Octreotide
received FDA approval in 1988 and use began the same year.
0/45 patients receiving octreotide experienced significant intra-op complications compared with 8/73 pts who did NOT receive octreotide.
41 (38%) patients received intra-op octreotide Median dose 350 mcg Range30-4000 mcg
Analysis demonstrated that patients receiving octreotide intra-op experienced significantly fewer intra-op complications
Intraoperative Octreotide Drug of choice to treat hypotension in carcinoid crisis in
addition to fluid boluses Should be ordered, available, and administered in the OR prior
to induction
Treats hemodynamic instability in 15 seconds to 10 minutes
10 mcg SQ/IV until effect minimum published dose
500 mcg IV until effect in other publications
At LSU, drips up to 500 mcg/hour have been given in over 300 major resection cases without crisis or adverse effect Also up to1 mg IV boluses for crisis
Mancuso, et al., 2011; Koopmans, et al., 2005

Octreotide Adverse Effects Only serious side effect is
prolonged QT interval, therefore avoid other medications with same effect (e.g. ondansetron)
Treating Hypotension If Hypotension is refractory to high-dose octreotide and
fluids, decrease anesthetic depth, and have surgeon halt tumor stimulation (Mancuso, et al. 2011) Fluids if cardiac function is good
Vasopressin have been used with limited success.
Use Aprotinin (kallikrein inhibitor) as back up when octreotide fails to treat hypotension during tumor manipulation Also with limited success
Powell, Muhkar, & Mills, 2011; Vaughan & Brunner, 1997, Vaughan, Howard, & Brunner, 2000

Treating Hypertension Octreotide
Deepen anesthesia
Beta blockers
Ketanserin (serotonin receptor antagonist)
Labetalol infusions
Alpha blockade
Mancuso, et al., 2011; Powell, Muhkar, & Mills, 2011

Treating Bronchoconstriction
Mancuso, et al., 2011
If refractory to octreotide, antihistamines and nebulized iprotropiumshould be used instead of beta agonists to prevent mediator release.

Postoperative Management Should be monitored for mediator release due to delayed
recovery from anesthesia from high serotonin levels Undetected metastases may still secrete peptides Preoperative drug therapy with octreotide should be
continued and possibly reduced slowly over the first week post op
Fluids and electrolytes should be monitored closely due to large fluid shifts
Analgesia to prevent excess sympathetic activity and stress prevents post-op crisis
Fentanyl and epidural analgesia has been used with success
Mancuso, et al., 2011

Postoperative Management Powell, Muhktar, & Mills
(2011) also recommend ICU care with invasive monitoring
IV and then SQ octreotide for at least 48 hours to minimize post-op crisis
Further Study Needed Further study is needed to compare prophylaxis regimens.
Is SQ dosing every 8 hours as effective as continuous IV administration?
Is octreotide still the most effective compared to other newer somatostatin analogues?

Conclusions Anesthesia providers need to be aware of carcinoid syndrome
symptoms for patients presenting for resection of tumors with unknown pathology.
Providers need to know clinical picture of carcinoid crisis to appropriately manage it
Patients with carcinoid syndrome should have symptoms well controlled with somatostatin-analogue prior to surgery to prevent complications
Thorough preoperative assessment including cardiology consult when indicated is essential

Conclusions Octreotide infusion 50-500 mcg/hr infusion should be
initiated prior to any anesthetic in patients with known carcinoid tumors.
Continue octreotide for at least 48 hours postoperatively in ICU setting
Invasive Monitoring with minimum of A-line
Smooth induction and maintenance of anesthesia with steady BP control
Anxiolysis and analgesia are important to prevent crisis not only in OR, but post op as well

Conclusions Neuroaxial anesthesia may be used with octreotide and BP
control Epidural is preferred for post op analgesia and less
sympathectomy
Hemodynamic instability, flushing, and bronchospasm should be rapidly treated with IV octreotide and fluid boluses to effect Octreotide up to 1 mg IV bolus (each dose)

Conclusions If hypotension continues despite octreotide and fluid,
consider aprotinin, vasopressin, and small cautious doses of phenylephrine Sympathomimetics should be avoided
Hypertension refractory to octreotide should be treated with deepening anesthesia, beta blockers, labetolol, alpha antagonists, or 5-HT2 antagonist such as Ketanserin
ReferencesBorch, K., Ahrén, B., Ahlman, H., et al. (2005). Gastric carcinoids: biologic behavior and
prognosis after differentiated treatment in relation to type. Annals of Surgery, 242, 64.Bloom, S.R. & Polak, J.M. (1987). Somatostatin. British medical journal, 295, 288-290.Claure, R.E., Drover, D.D>, Haddow, G.R., Esquivel, C.O., Angst, M.S., (2000).
Orthotopic liver transplantation for carcinoid tumour metastatic to the liver: anesthetic management. Canadian journal of anaesthesia, 47, 334-337.
Cortinez, F. (2000). Refractory hypotension during carcinoid resection surgery. Anaesthesia, 55(5), 505-506. doi:10.1046/j.1365-2044.2000.01425-27.x
Cunningham, J.L., Janson, E.T., Agarwal, Sl, et al. (2008). Tachykinins in endocrine tumors and the carcinoid syndrome. European Journal of Endocrinology, 159, 275.
Davi, M.V., Bodei, L., Francia, G., et al. (2006). Carcinoid crisis induced by receptor radionuclide therapy with 90Y-DOTATOC in a case of liver metastases from bronchial neuroendocrine tumor (atypical carcinoid). Journal of Endocrinology Investigation, 29, 563.
Déry, R. (1971) Theorectical and clinical considerations in anaesthesia for secreting carcinoid tumors. Canadian Anaesthesia Society Journal, 18, 245.
Dierdorf, S. (2003). Carcinoid tumor and carcinoid syndrome. Current opinion in anaesthesiology, 16, 343-347.

ReferencesFeldman, J.M. Carcinoid tumors and syndrome. (1987). Seminars in Oncology, 14, 237.Fink, G., Krelbam, T., Yellin, A., et al. (2001). Pulmonary carcinoid: presentation,
diagnosis, and outcome in 142 cases in Israel and review of 640 cases from the literature. Chest, 119, 1647.
Gates, J., Hartnell, G.G., Stuart, K.E., Clouse, M.E. (1999). Chemoembolization of hepatic neoplasm: safety, complications, and when to worry. Radiographics, 19¸399.
Gillams, A., Cassoni, A., Conway, G., Lees, W. (2005). Radiofrequency ablation of neuroendocrine liver metastases: the Middlesex experience. Abdominal Imaging, 30, 435.
Gough, D.B., Thompson, G.B., Crotty, T.B., et al. (1994). Diverse clinical and pathologicafeatures of gastric carcinoid and the relevance of hypergastrinemia. World Journal of Surgery, 18, 473.
Grahame-Smith, D.G. (1987). What is the cause of the carcinoid flush? Gut, 28, 1413.Hendrix, T.R., Atkinson, M., Clifton, J.A., Ingelfinger, F.J. (1957). The effect of 5-
hydroxytryptamine on intestinal motor function in man. American Journal of Medicine, 23, 886.
Kharrat, H.A., Taubin, H. (2003) Carcinoid crisis induced by external manipulation of liver metastasis. Journal of Clinical Gastroenterology, 36, 87.

ReferencesKinney, M.A., Warner, M.E., Nagorney, D.M., Rubin, J., Schroeder, D.R., Maxson, P.M.,
and Warner, M.A. (2001). Perianaesthetic risks and outcomes of abdominal surgery for metastatic carcinoid tumours. British Journal of Anaesthesia, 87(3), 447.
Koopman, K.P., Brouwers, A.H., De Hooge, M.N., Van der Horst-SChrivers, A.N., Kema, I.P., Wolffenbuttel, B.H., De Vries, E.G., Jager, P.L. (2005). Carcinoid crisis after injection of 6-18F-fluorodihydroxyphenylalanine in a patient with metastatic carcinoid. Journal of nuclear medicine, 46, 1240-1243.
Kvols, L.K., Moertel, C.G., O’Connell, M.J., et al. (1986). Treatment of the malignant carcinoid syndrome. Evaluations of a long-acting somatostatin analogue. New England Journal of Medicine, 315, 663.
Lie, J.P. (1982). Carcinoid tumor, carcinoid syndrome, and carcinoid heart disease. Primary Cardiology, 8, 1963.
Majeed, F., Porter, T.R., Rarntolo, S., et al. (2007) Carcinoid crisis and reversible right ventricular dysfunction after embolization in untreated carcinoid syndrome. European Journal of Echocardiography, 8, 386.
Makridis, C., Theodorsson, E., Akerström, G., et al. (1999). Increased intestinal non-substance P tachykinin concentrations in malignant midgut carcinoid disease. Journal of Gastroenterology & Hepatology, 14, 500.
ReferencesMancuso, et al. (2011). Carcinoid syndrome and perioperative anesthetic considerations.
Journal of Clinical Anesthesia, 23. 329-341.Marsh, H.M., Martin, J.K, Kvols, L.K., et al. (1987) Carcinoid crisis during anesthesia:
successful treatment with a somatostatin analogue. Anesthesiology, 66, 89. Maton, P.N., (1988). The carcinoid syndrome. Journal of American Medical Association, 260,
1602.Melmon, K.L., Sjoerdsma, A., Mason, D.T. (1965). Distinctive clinical and therapeutic
aspects of the syndrome associated with bronchial carcinoid tumors. American Journal of Medicine, 39, 568.
Melnyk, D.L. (1997). Update on carcinoid syndrome. AANA, 65, 265-270.Memon, M.A., Nelson, H. (1997). Gastrointestinal carcinoid tumors: current management
strategies. Diseases of the colon and rectum, 40, 1101.Metz, S.A., McRae, J.R., Robertson, R.P. (1981). Prostaglandins as mediators of
paraneoplastic syndromes: review and update. Metabolism, 30, 299.Modlin, I.M., Kidd, M., Latich, I., et.al. (2005). Current status of gastrointestinal
carcinoids. Gastroenterology, 128, 1717.

ReferencesMorrisroe, K. K., Sim, I. W., McLachlan, K. K., & Inder, W. J. (2012). Carcinoid crisis
induced by repeated abdominal examination. Internal Medicine Journal, 42(3), 342-344. doi:10.1111/j.1445-5994.2012.02719.x
Nathanson, L., Sochet, A., Williams, M.E. (1989). Migratory thrombophlebitis during sandostatin (SMS 201-995, Sandoz) therapy for malignant carcinoid syndrome. Investigational new durgs, 7(2-3), 285-287.
National Comprehensive Cancer Network (NCCN) guidelines available online at www.nccn.org
Oates, J.A. (1986). The carcinoid syndrome. New England Journal of Medicine, 315, 702.Oates, J.A., Pettinger, W.A., Doctor, R.B. (1966). Evidence for the release of bradykinin in
carcinoid syndrome. Jounral of Clinical Investigation, 45, 1973.Oberg, K., Kvols, L., Caplin, M., et al. (2004). Consensus report on the use of
somatostatin analogs for the management of neuroendocrine tumors of the gastroenteropancreatic system. Annals of Oncology, 15, 966.
Ockert, D., White, R. (1988). Anesthetic management of patients with carcinoid heart disease undergoing cardiac surgery: two case reports and a review of previous experience. Journal of cardiothoracic anesthesia, 44, 143-148.

ReferencesOrbach-Zinger, S., Lombroso, R., Eidelman, L.A. (2002) Uneventful spinal anesthesia for a
patient with carcinoid syndrome managed with long-acting octreotide. Canadian journal of anaesthesia, 49, 678-681.
Powell, B., Mukhtar, A., & Mills, G. (2011). Carcinoid: the disease and its implications for anaesthesia. Continuing education in anesthesia, critical care & pain, 11(1). 9-13.
Quaedvlieg, P., Visser, O., Lamers, C., Janssen-Heijen, M., Taal, B. (2001). Epidemiology and survivial in patient with carcinoid disease in The Netherlands. An epidemiological study with 2,391 patients. Annal of Oncology, 12, 1295-1300.
Reubi, J.C., Kvols, L.K., Waser, B., Nagorney, D.M., Heitz, P.U., Charboneau, J.W., Reading, C.C., Moetrel, C. (1990.) Detection of somatostatin receptors in surgical and percutaneous needle biopsy samples of carcinoids and islet cell carcinomas. Cancer Research, 50(18), 5969-77.
Roberts,L.J., Marney, S.R., Oates, J.A. (1979). Blockade of the flush associated with metastatic gastric carcinoid by combined histamine H1 and H2 receptor antagonists. Evidence for an important role of H2 receptors in human vasculature. New England Journal of Medicine, 300, 236.
ReferencesRoy, R.C., Carter, R.F., Wright, P.D. (1987). Somatostatin, anaesthesia, and the carcinoid
syndrome. Peri-operative administration of a somatostatin analogue to suppress carcinoid tumour activity. Anaesthesia, 42, 627-632.
Rubin, J., Ajani, J., Schirmer, W., et al. (1999). Octreotide acetate long-acting formulation versus open-label subcutaneous octreotide acetate in malignant carcinoid syndrome. Journal of Clinical Oncology, 17, 600.
Ruszniewski, P., Ducreux, M., Chauvialle, J.A., et al. (1996). Treatment of the carcinoid syndrome with the long-acting somatostatin analogue lanreotide: a prospective study in 39 patients. Gut, 39, 279.
Sandler, M., Karim, S.M., Williams, E.D., (1968). Prostaglandins in amine-peptide-secreting tumours. Lancet, 2, 1053.
Schmid, H.A., & Schoeffter, P. (2004). Functional activity of the multiligand analog SOM230 at human recombinant somatostatin receptor subtypes supports its usefulness in neuroendocrine tumors. Neuruendocrinology, 80(1), 47.
Swain, C.P., Tavill, A.S., Neale, G. (1976). Studies of tryptophan and albumin metabolism in a patient with carcinoid syndrome, pellagra, and hypoproteinemia. Gastroenterology, 71, 484.
ReferencesTörnebrandt, K., Nobin, A., Ericsson, M., Thomson, D. (1983). Circulation, respiration
and serotonin levels in carcinoid patients during neurolept anaesthesia. Anaesthesia, 39, 957.
Van der Lely, A.J., & de Herder, W.W. (2005). Carcinoid syndrome: diagnosis and medical management. Arq bras endocrinol metabol, 49, 850-860.
Vaughan, D.J. & Brunner, M.D. (1997). Anesthestia for patients with carcinoid syndrome. Internationa Anesthesiology Clinics, 35, 129.
Vaughan, D. J., Howard, J. M. & Brunner, M. D. (2000), Refractory hypotension during carcinoid resection surgery. Anaesthesia, 55: 927.
Veall, G.R., Peacock, J.E., Bax, N.D., Reilly, C.S. (1994). Review of the anaestheticmanagement of 21 patients undergoing laparotomy for carcinoid syndrome. British Journal of Anaesthesia, 72, 335.
Vinik, A.I., McLeod, M.K., Fig, L.M., et al. (1989) Clinical features, diagnosis, and localization of carcinoid tumors and their management. Gastroenterology Clnics of North America, 19, 865.
von der Ohe, M.R., Camilleri, M., Kvols, L.K. Thomforde, G.M., (1993). Motor dysfunction of the small bowel and colon in patients with the carcinoid syndrome and diarrhea. New England Journal of Medicine, 329, 1073.
ReferencesWarner, R.R.P. (1985). Carcinoid tumors. Gastroenterology. Berk, J.E. (Ed). Philadelphia:
WB Saunders.
Warner, R.R., Mani, S., Progeta, J., Grunstein, E. (1994). Octreotide treatment of carcinoid hypertensive crisis. Mount Sinai Journal of Medicine, 61, 349.
Woodside, K.J., Townsend, C.M., Mark-Evers, B. (2004). Current management of gastrointestinal carcinoid tumors. Journal of Gastrointestinal Surgery,8, 742.
Yazbek-Karam, V., Haswani, R., Mousallem, N., Abou Jaoude, E., Nassar, N., Hirbli, K., & ... Aouad, M. (2009). Severe intra-operative carcinoid crisis in a patient having carcinoid heart disease. Acta Anaesthesiologica Scandinavica, 53(3), 414-415. doi:10.1111/j.1399-6576.2008.01870.x.
Zimmer, C., Kienbaum, P., Wiesemes, R., Peters, J. (2003). Somatostatin does not prevent serotonin release and flushing during chemoembolization of carcinoid liver metastases. Anesthesiology, 98(4), 1007-1011





























