Embed Size (px)
Citation preview

9th Panhellenic Conferenceon Alzheimer's Disease &
1st Mediterranean onNeurodegenerative Diseases

Non-pharmacological strategies:Scientific evidence versus the real world
Luisa Bartorelli, geriatrician & gerontologistPresident, Alzheimer Uniti Association Italy

Alzheimer Planet
AnticholinesteraseMemantine
Anti-oxidentsAnti-inflammatoriesEstrogenAnti-amiloidogeni
Pharmacologicalstrategies


WHAT CAN WE REALISTICALLY ASK OF THECURRENT DRUG THERAPY?
No side effects Slowing the progress of the disease Better functional state Improvement in the quality of life
Delay in institutionalization Moderate cost

The world changes.
Expectations evolve.
Needs grow.
The treatments include:a human dimensiona social dimension.
There are more complexlegal obligations.There are ethical andphilosophical questions inthe oldest old.

Care Systems
Clinical and scientific advances.Economy.Innovative technology.Organizing assistance.Increase of awareness of rights and of duties.Reduction of tolerance levels.
It is important to become aware, avoid nostagia andbehaviour from the past.

NarrativeMedicine
Slow Medicine
A zone ofcomplexity
AcademicMedicine
ControlledOrder
The big question …..
Rational responses (EBM) orcontinuous adjustments to thevariability of the person and tocontinous changes of the realworld?

Lon S. Schneider Int. J. Geriatr. Psychiatry 2006
“How much is an ADAS-cog point worth in central London?”
The Recipients
frail peopleaffected by much lossbut often still able to function andrich in emotions

Beyond the drugs
THE PERSONTHE CAREGIVERTHE ENVIRONEMENTTECNOLOGY
Global reactivation
Cognitive deficits
Behavioural disturbances
Functional deficits

……..…. evidence shows that a largeproportion of these so-called “behaviorproblems” stem from a degree to whichtheir environment fulfills these needs.
ALZHEIMER DIS ASSOC DISORD – VOL 19, 1, JANUARY-MARCH 2005

REACTIVATION
To slow the course of the disease. To conserve the patient’s existing capacities. To preserve the quality of life for the patient and
the family.
GENERALOBJECTIVES

The complexity of the disease
Tailored medicine
The person, his characterhis own story, his identity……good days, bad days.
From the academic view to a therapeuticalliance.

18
THE REPORT QF UK ALZHEIMER SOCIETY : A GOOD LIFE OF DEMENTIA
1.How to better support people with dementia to maintain their senseof uniqueness and personal identity (Respecting identity: 'It's not onesize fits all')2.Achieving the right balance between memory-based activities andenjoying the here and now (Embracing now: 'It's a moment-living life')3.Ensuring people with dementia are able to experience meaningfulhuman connections (Sustaining relationships: 'You don't always needwords')4.Ensuring people with dementia are able to experience a full range ofemotions (Valuing contrast: 'Good days and bad days')5.Taking risks - what are we protecting people with dementia from?(Supporting agency: 'What's there to worry about?')6.Promoting good overall health for those who are living with dementiaincluding physical and emotional wellbeing (Maintaining health: 'Mypriority in life'). MARCH 19 2014
(UK Alzheimer’s Society, March 19, 2014)

Space for freedom

CDCD HOMECARE
THE PERSONH
DAY HOSPITAL
RESPITEBEDS
FAMILYGP
DAYCENTRE
NURSINGHOME

ENVIRONMENTAL DESIGN AND TECHNOLOGY
Impaired of memory
Impaired learningImpaired reasoningHigh level of stress
Human factors solutions
Using tech. for people with dementia


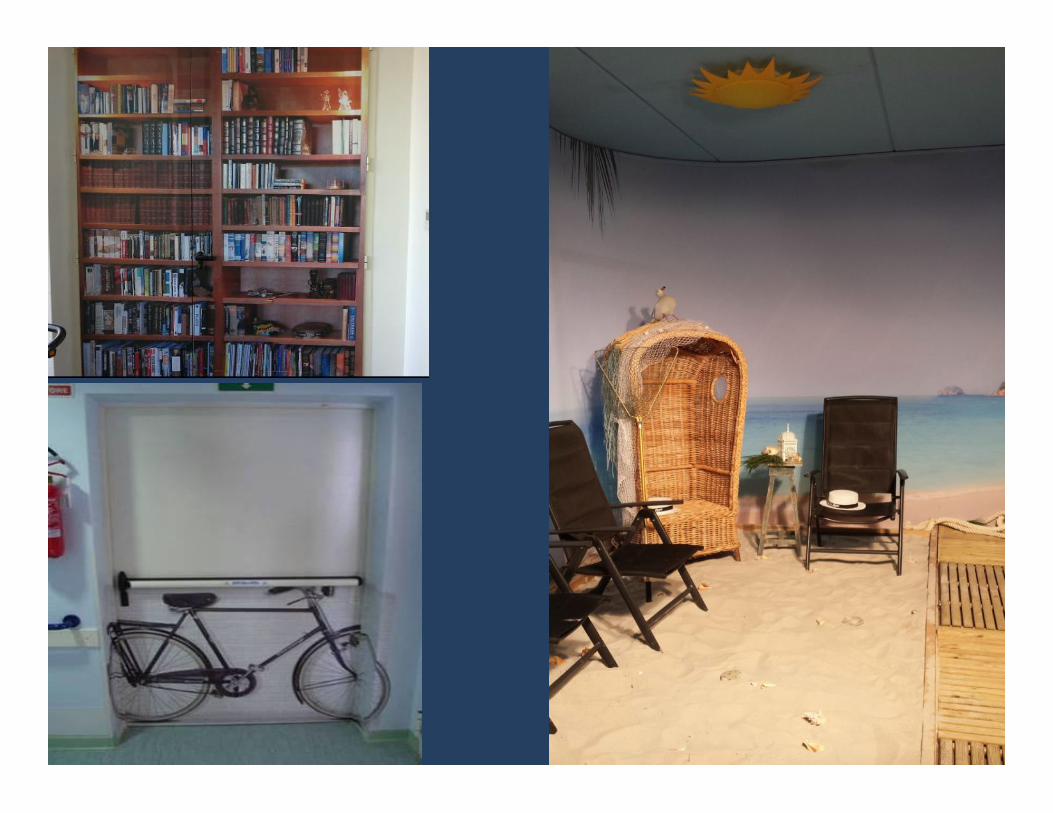
ENVIRONEMENTNOT A “SETTING” BUT A “LIVING SPACE”
Integrated system:
architectural aspects (organization of thephysical space)
components of the organization (activities)
social context (formal and informal caregivers)
FEATURESARCHITECTURALLY ADAPTED
Nursing Home
NURSING HOME
hortus conclusus an exclusio?

OBJECTIVE
Adapting environmental conditions to guaranteesecurity, stability and trust, taking intoconsideration the emerging symptoms andavoiding stressful stimulation. …well-being………..

ENVIRONMENT: INCREASING DIFFICULTIES
Spatial disorientation
Visual-spatial problems
Behavioural changes
Motorial uncertainty
Risks of falling

Osvaldo Sponzilli : Iniziazione alla Cromoterapia. Edizioni Mediterranee 2010
Some aspects of colour perception among patients with Alzheimer'sdisease. Wijk H, Sivik L, Scand J Caring Sci 1995.

Environmental Facilities
• Signs to explain• Special forniture (with rounded edges)• Utensils and objects in an appropriate form• Soft and colorful objects
(for their ease)• Clothing

SENSORIALAPPROACH
ALZHEIMER GARDEN (OR TERRACE)
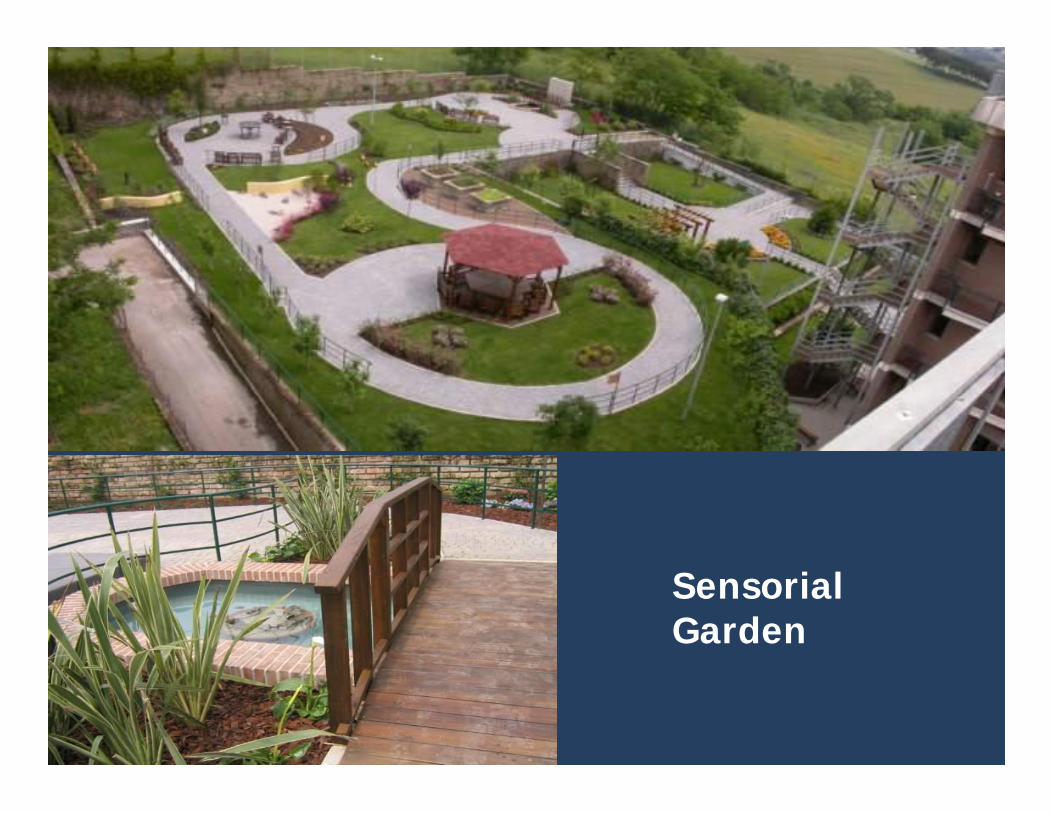
Il Giardino Sensoriale Alzheimer
SensorialGarden

Another space: Alzheimer café


Places for care
What about
museum?

Increase in self-esteem and reinforcement of identity
Cognitive and sensorial stimulation
Reactivation

Motivation, socialization and interest in the outside world
Caregiver satisfaction
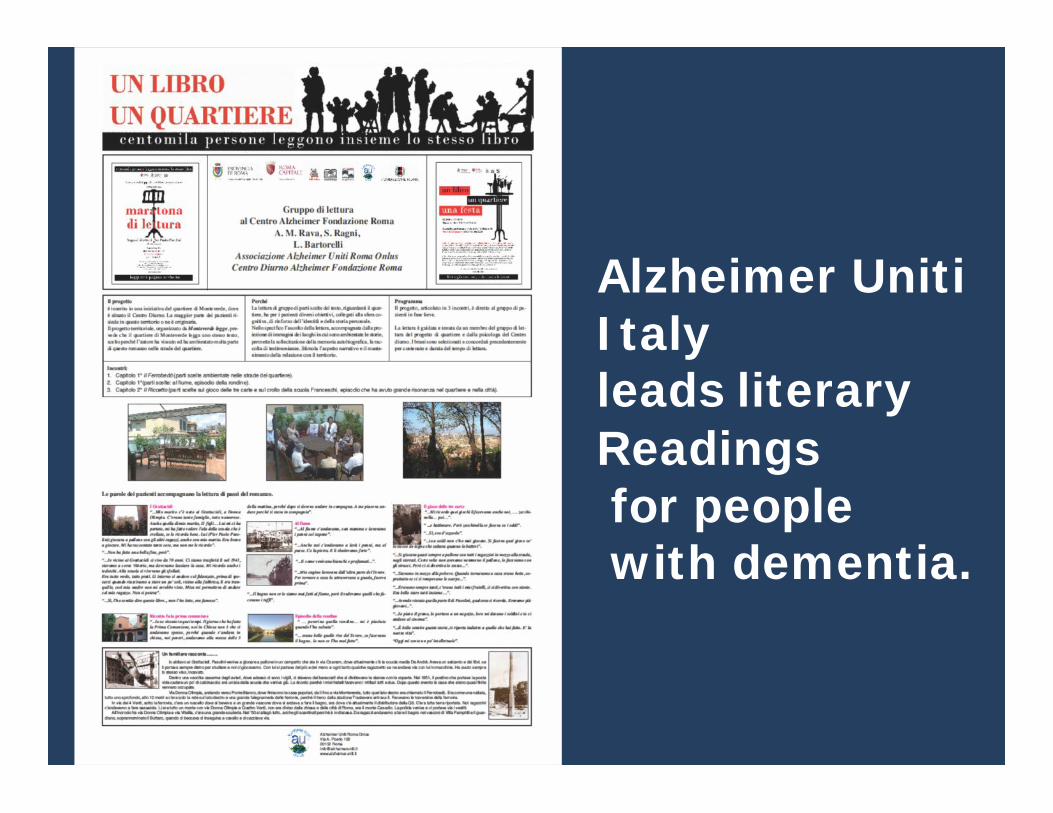
Alzheimer UnitiItalyleads literaryReadingsfor peoplewith dementia.

Rational basis of non pharmacology therapyfor AD
Adaptation of the environmentreduces the level of disability.
Mechanism of plasticity, organizationand functional adaptation of SNCallow partial rehabilitation.
Exercise is able to delay functional impairment.
”use for not lose”

Prevention of falls
Awareness ofoneself in aspaceEmotionalexperiences fromthe activity
Perception of one’sbody and burden
Equilibrium



DANCE-MOVEMENT THERAPY

Cognitive Therapy
ROT
Reality Orientation Therapy(formal and informal)Memory Training(Spaced-retrieval technique;compensation,categorization, facilitation)
ROT + Terapia farmacologica
“Efficacy of a home-based realityorientation theraphy programmecombined with cholinesteraseinhibitors for patient with Alzheimer’sdesease: a randomised controlledtrial.”
Onder G., Zanetti O., Giacobini E., Frisoni G.B.,Bartorelli L. et Al., BMJ 2006.


Psychosocial treatments of behavior symptoms indementia: a systematic review of reports meetingquality standards.O’Connor DW, Ames D, Gardner B, King M, Department of PsychologicalMedicine, Monash University, Melbourne, Australia, Int Psychogeriatr2009 Apr;21(2):225-40.
Cognitive intervention programs for individualswith mild cognitive impairment: systematic review, .School of Psychology, Laval University and Institut universitaire en santémentale de Québec, Quebec City, Canada. Jean L, Bergeron ME, ThiviergeS, Simard M. Am J Geriatr Psychiatry. 2010 Apr;18(4):281-96
terapy occupazionale 3.wmv
Should we use individual cognitive stimulationtherapy to improve cognitive function in people withdementia?rrell M, Woods B, Spector A. 2011UCL Mental Health Sciences Unit, University College London, London,UK.O

People with dementia musthave interventions that arecognitively stimulating,independent of the course oftheir pharmacologicaltreatment.
‘NICE-SCIE Guide in themanagement of dementia.”
Interventions on Cognition in Dementia
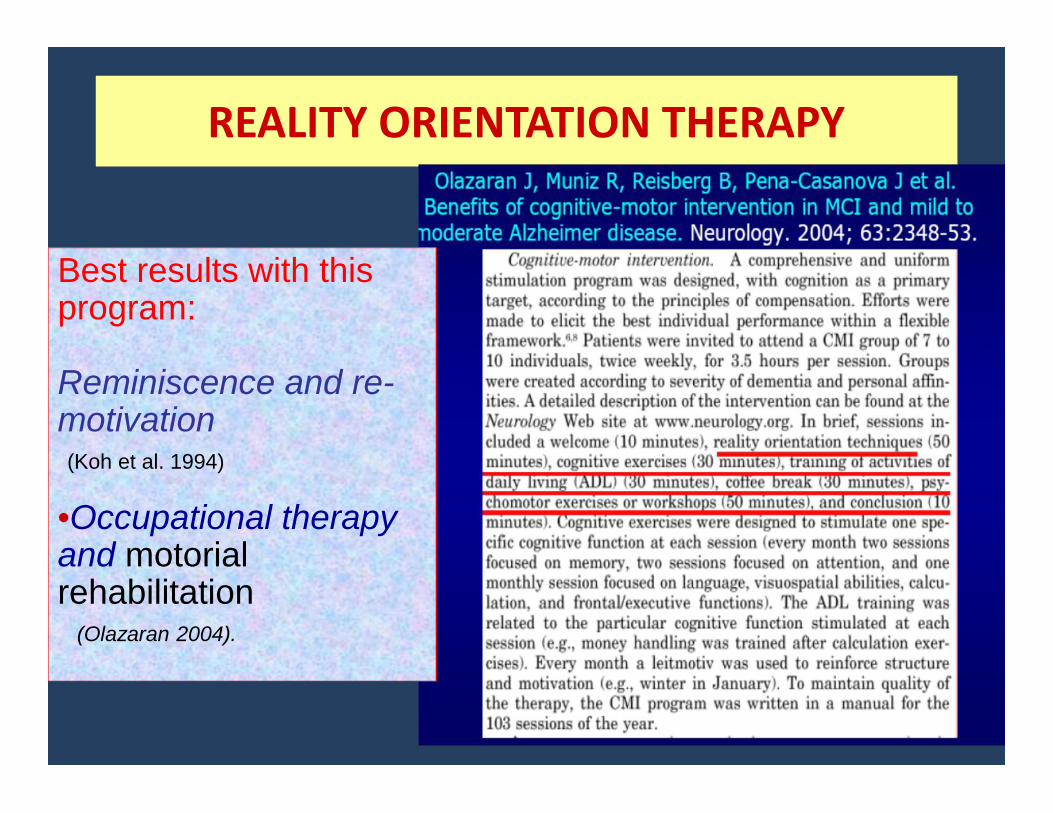
REALITY ORIENTATION THERAPY
Best results with thisprogram:
Reminiscence and re-motivation(Koh et al. 1994)
•Occupational therapyand motorialrehabilitation
(Olazaran 2004).

ValidationTherapy
“Validation theory and themyth of the therapeutic lie”Feil N., Altman R. Am. J. ofAlzheimer’s disease and otherdementias, 19(2): 2014

Occupational therapy and workshops expression•excercise for fine motor skills•maintenance of capabilitiescreativity•self-esteem•gratification

Community occupationaltherapy for older peoplewith dementia and their
caregiversThe COTiD-program (English)
orEDOMAH programma (Dutch)OrThe COTiD- It program (Italian)
Dr. Maud Graff (PhD, OT)Radboud University NijmegenMedical Center, TheNetherlands

"Un violino nelle mani del malato di Alzheimer:una sfida ed una possibilità" in Atti delSeminario" Il contributo delle Uvanell'assistenza dei pazienti con demenza",Istituto Superiore di Sanità, Roma 2010
The Effect of music therapy on reducingagitation in patients with Alzheimer desease.Zare et Al. Inter J Geriatric Psychiatric. ShirazUniversity Iran 2010
Application of music therapy on managingagitated behaviour in older people withdementia. Fung HC et Al Hu Li Za Zhi 2009 HongKong University
Effect of music therapy on anxietyand depression for people with Alzheimerdesease. Guetin S. et Al Geriatric and cognitivedisorders. 2009 Service de NeurologieMontpellier

Music Therapy
Listen to me!I am here.


Art therapy may be benefitial for reducing stress--relatedbehaviours in people with dementia--case report.Mimica N, Kalinic D, University Department, Vrapče PsychiatricHospital, Bolnička cesta 32, 10090 Zagreb, Croatia, Psychiatric Danub 2011Mar;23(1):125-8.

Drama Therapy
CreativitySpontaneous expressionConstruction of stories
Role identificationUse of space
AZIONE SCENICA E MEMORIA: DRAMATHERAPY E ROT IN CENTRO DIURNO ALZHEIMERRagni Silvia, Pariante Assunta, Attaianese Fulvia, Boccardo Mauro, Giubilei Annalisa, Bartorelli LuisaCentro Alzheimer Fondazione Roma - Atti del Convegno AIP 2013

Pet-Therapy
Animal-assisted therapy for dementia: a review of the literature.Filan SL, Llewellyn – Jones RH, Department of Psychological Medicine, University of Sydney, NSW, Australia,Int Psychogriatr. 2006 Dec;18(4):597-611

Caffè
Lavanda
Miele
Olfatto, memoria, emozione:un’occasione per la riattivazione.”
Bartorelli L. et Al. Giorn. Geront.Vol. 49, n° 7, 2001, 360.
Sense of smell, touch, memory andemotions:An opportunity for cognitive stimulationRagni S., Tancorre I., Attaianese F.,Boccardo M., Giubilei A., Levi S.,Bartorelli L.Atti Congresso Nazionale AIP 2014


Horticulturetherapy

Characteristics of visual target influence detection ofchange in naturalistic scenes in Alzheimer disease.Neargarder SA, Cronin-Golomb A,. Department of Psychology,Bridgewater State College, Bridgewater, Massachusetts 02325, USA,Cogn Behav Neurol. 2005 Sep;18(3):151-8.
Cartoons

SNOEZELEN ROOM Ball J, et al. Creating a multisensoryenvironment for dementia: the goals of a Snoezelen room.J.Geront.Nurs.2005


Environmental determinants of quality of lifein nursing home residents with severe dementia.Garre Olmo J Am Ger Soc 2012 Jul;60(7)


Non-drug interventions for Alzheimer’sdisease. Last Update July 2013Institute for Quality nd Efficiency in HealthCare (IQWiG) GermanyNon-drug interventions for Alzheimer’s disease include things like memorytraining, mental and social stimulation, and physical exercise programs. Some ofthese strategies could possibly improve mental abilities and increase people’sindependence.As Alzheimer’s disease progresses, it becomes more and more difficult for peopleto do everyday activities on their own. They become forgetful and increasinglyhave problems expressing themselves in words. Their orientation in space andtime gets worse and their personality changes. This makes good-quality care andsupport all the more important: people who have dementia need loving and stablerelationships and a tolerant environment.There is currently no cure for Alzheimer’s disease. As well as medications, thereare non-drug interventions that aim to delay the loss of mental abilities, to helppeople stay independent in everyday life for as long as possible, and to increasetheir wellbeing and quality of life. Non-drug strategies include things like memoryor orientation training. Other interventions include art therapy, aromatherapy,music therapy, animal-assisted therapy and caregiver education programs.

Overview of non-pharmacological intervention for dementia andprinciples of brain-activating rehabilitation.Yamaguchi H, Maki Y, Yamagami T , Gunma University School of Health Sciences, GeriatricsResearch Institute and Hospital, Maebashi, Japan, Psycogeriatrics 2010 Dec 10(4):206-13

Multi-professional team
Geriatrician
Nurse
Psychologist
Social worker
Physiotherapist
Occupational therapist
Health care worker.

TRAINING
AREAS: cognitive, emotional, psychological, socialActive involvement of the person,Positive environment.
NaturalReserve
Plasticity
Redundancy
……ensemble c’est possible
• Combattre lastigmatisation
• Mettre en réseau toutesles ressoursesdisponibles
• Chercher des solutionscréatives aux problèmes
• Partager, partager….!

Care always
Curare ancora !

R.Magritte Le mistère du quotidien
THANKYOU !

MERCI !
ALLIANCE ALZHEIMER MEDITERRANÉENNEDE LISBOA 2014 A THESSALONIQUE 2015





























