Upload
nyucd17
View
224
Download
0
Embed Size (px)
Citation preview
8/10/2019 51/52: Periodontist and Periodontium
1/32
Transcribed by Anam Khalid Monday, October 20th, 2014
1
What is a periodontist and what do they do? Diagnosis and Treatment of Oral
Disease by Dr. Peter M. Loomer
&
The Periodontium in Health by Dr. Julie Yip [Page 15]
[Slide #1] [The specialty of periodontics][Dr. Loomer]Good afternoon everybody. Thank you for coming today. Im Peter
Loomer. Im going to introduce the first lecture in the series of lectures on
periodontics. And what Im going to talk about is just an overview of what the
specialtys all aboutthe different things that the field of periodontics encompass.
And then youre going to have a series of lectures from faculty from our department
talking about the different procedures that youre going to be doing. And then it
continues with another course that Dr. Brawl will teach you next year looking at
more in-depth cases and all that. Okay.
[Slide #2] [Periodontics]
[Dr. Loomer]So periodontics is really these are the topics that well cover today but its a surgical specialty that deals with controlling inflammation and infection
and actually we do more than that. But thats sort of the basic behind it. Youre
treating the disease, periodontal disease, and different treatments available to
control that. But your basic goal is control of infection and inflammation.
[Slide #3] [Control of Infection & Inflammation]
[Dr. Loomer]And I have a bunch of slides to show you just on things that we do to
control that. So this is your classic patient whos neglected themselves, their oral
hygiene. You see a lot of inflammation, erythemaerythema meaning redness of the
gingiva. Gingiva when theres infection and inflammation will look swollen or
edematous. Youll get that erythema which is redness thats due to dilation of thecapillaries in the area so you get increased blood flow when theres more
inflammation. You may get pus coming out of the pockets or clear fluid thats called
exudate. And thats as the inflammation and infection causes more drainage of the
crevicular fluid so youll see that as well. Or if you probe the area you might get
some white pus which are basically dead tissue cells coming out of the area. Those
are some of the signs of inflammation. People can also feel sometimes their gingiva
is hot. Thats not very common but sometimes patients will complain about that. Or
even pain. Theyll have pain from the gingiva when its very swollen and maybe an
abscess has developed.
[Slide #4] [N/A][Dr. Loomer]So how do you treat that? Well, lets look at a case here. This is a case
we just described with the redness, inflammation. The first step to treating
periodontal disease is really oral hygiene instruction. You want to get the patient,
number one to understand that they have a disease. Its not just plaque but its part
of a disease, either gingivitis or periodontal disease. Now, the distinction is if theres
bone loss or attachment loss. So gingivitis means inflammation of the gingiva. If you
have no bone loss, no attachment loss, which were going to tell you about in a few
8/10/2019 51/52: Periodontist and Periodontium
2/32
Transcribed by Anam Khalid Monday, October 20th, 2014
2
lectures down the road. But if theres inflammation and theres been no loss of tissue
or bone around the teeth thats gingivitis. If you have inflammation but you also
have loss of bone or loss of gingiva, recession, around the teeth, that would be then
called periodontitis or periodontal disease. And theres various types of periodontal
disease which youll learn in subsequent lectures. But the first thing is you get the
patient to understand what kind of disease they have, what causes it, that its causedby bacteria and the bacteria elicit the host response, your own response to release
inflammatory cytokines to cause inflammation and its the inflammation that
destroys the teeth. And basically what the bodys trying to do is prevent the bacteria
from penetrating to attacking more vital organs like the heart for example. So its
trying to make the teeth fall out so that the bacteria have no place to live. Because
the bacteria like to live around the teeth, so keeping the bacteria at low levels by
good oral hygiene, good brushing, flossing, will make the risk for periodontal
disease minimal. So thats how you control periodontal disease. So, I find educating
your patient the most effective but you also need to clean up the plaque and the
calculus thats there and we do that with scaling and root planing.
[Slide #5] [N/A]
[Dr. Loomer]And I know youve started in the clinic working on each other to do
some cleaning and of course you learned last year also the different instruments
that you use to do it. And of course youre going to get more practice starting in
January and in your third and fourth years. And this is how it looks after the scaling
root planing has been done. The tissue doesnt look red anymore. Its nice and tight.
Its not edematous. It has all theseyou see all these dots here? Thats called
stippling. The gingiva looks stippled like an orange peel. Thats a sign that things are
nice and healthy. And if you would probe the area you wouldnt get any bleeding
when you probe. Bleeding when you probe means theres inflammation in the
pocket.
[Slide #6] [N/A]
[Dr. Loomer]Heres another case well look at. You can see also this patient has a
lot of erythema, a lot of redness which we didnt have the light there but I guess its
always on but inflammation around the gingival margin. You see the edema. You
can see some redness here. The patients been probed recently so theres still some
bleeding around the gingiva where theyve been probed. And scaling and root
planing was done. A good discussion on oral hygiene, how to keep that patient
how to keep the area clean was done
[Slide #7] [N/A][Dr. Loomer]And afterwards looks much better. And one of the things youll notice
if you look at the gingiva. It certainly looks nice and thin. Its not edematous or
swollen at the margin. You dont see any redness. But you can also see theres a little
bit of recession there. There was if we go back
[Slide #6] [N/A]
[Dr. Loomer]Its a little hard to see but there was some recession there before
8/10/2019 51/52: Periodontist and Periodontium
3/32
Transcribed by Anam Khalid Monday, October 20th, 2014
3
[Slide #7] [N/A]
[Dr. Loomer]But sometimes after you do the cleaning if its very swollen, when it
resolves youll get a little more recession. So thats not uncommon after scaling and
root planing. Everything is shrinking back to be tighter and now there may be a little
bit of recession there. But of course its a healthier situation now.
[Slide #8] [N/A]
[Dr. Loomer]This is another case. Very severe gingivitis. This patient had no
attachment loss, no periodontal disease, just a gingivitis case. You can see how
swollen it is. Its almost covering part of the enamel. Very very swollen
interproximally. This patient when they brush they basically, normally brush up to
there. They never floss and they missed removing the plaque along the gingival
margin at this area of the tooth. And once you do some oral hygiene, some nice
scaling and root planing
[Slide #9] [N/A][Dr. Loomer] cleaning of the teeth, you can see its all back to normal. So it looks
nice and healthy. So you can see a real dramatic improvement just by controlling the
plaque and getting that under control and removing any calculus, any plaque. And
patients really will see a difference before and after. So it makes a big difference.
[Slide #10] [N/A]
[Dr. Loomer]And this is just a picture of the patient further down the road, long-
term evaluation. And they were able to maintain it so whats important for your
patients to realize is youve treated it, youve got them back to health but it wont
stay that way unless theyre a partner and they keep their teeth clean and they come
in to see you for periodic cleanings. But youve controlled the disease. You haventcured the disease. There is no cure. But theres ways to prevent it from recurring by
good oral hygiene and regular dental care. And of course oral hygiene is the key
because you know, we have youve heard that expression, you should visit your
dentist every six months. Thats not based on any science. Thats based on
toothpaste ads. So back in I think it was the fiftys or the fortys, it was one of the
toothpaste companies that when they added fluoride to toothpaste, theyd say brush
your teeth twice a day and visit your dentist every six months. So it was really a part
of an advertising campaign for toothpaste. Sort of caught on and people do do that
just to make sure things are under control but if you have a good patient whos
really good at oral hygiene or you think about yourselfyoure flossing, youre
brushing really carefullyyou dont need to come every six months. You couldstretch it out longer. And of course people who are less compliant maybe you want
to see them every three months.
[Slide #11] [Guided Tissue Regeneration]
[Dr. Loomer]So lets talk about some of the surgical procedures that you can do in
periodontics because often, you know, you can treat a patient with scaling and root
planing but theyll still have defects around the teeth. Theyve had extensive bone
8/10/2019 51/52: Periodontist and Periodontium
4/32
Transcribed by Anam Khalid Monday, October 20th, 2014
4
loss and you need to treat it some way or the other to get them back to health. And
surgery is very often needed after the initial therapy to get patients under control
for their inflammation. And one of the procedures we use is called guided tissue
regeneration. And well go through a few surgical procedures. And this patient has
some bone loss. You can see around this tooth if you look at the line. The line is
drawing the most incisal extent of the bone. And you could see on this tooth usually the bone should be within 1 to 2 mm of the CEJ. So if your CEJ is here, a
normal bone level would be about there. And on this tooth, about there. So this
patient has quite a bit of bone loss. When youhave bone loss thats different on
adjacent teeth. You can see here the bone level is the same on the central incisor and
on the lateral incisor. So thats horizontal bone loss. Because the bone loss
originally the bone should be about there and its been lost up to there but in a
horizontal fashion. In this case, between these two teeth, youve got some vertical
bone loss because the bone loss is no longer flat across. Its got a vertical component
to it. And one way to treat vertical bone loss is through guided tissue regeneration.
And that refers to guiding the bone cells to populate this areathe bone cells and
the periodontal ligament cells and excluding the gum cells or the gingival cells fromgetting into that area. So youre guiding the kind of tissue that you want to
regenerate. We want to grow back the bone and of course the periodontal ligament
that attaches the bone to the tooth and hopefully even the cementum. So you want
to guide those kinds of cells, those kinds of tissues, to regenerate the area without
excluding the cells that we dont want to regenerate which are the gum or the
gingival cells. And youll learn more about that as well down the road.
[Slide #12] [N/A]
[Dr. Loomer]If you do a flap so you do an incision around the tooth. You push
back the gingiva. Clean out the area with your curet just like you did with the scaling
and root planing but you go into the pocket where the bony defect is. You can seehere that theres bone covering the tooth here but you can see theres a loss of bone
in between these teeth interproximally between these two teeth here the central
incisors.
[Slide #13] [N/A]
[Dr. Loomer]And whats done actually let me see here I think I skipped over
one
[Slide #12] [N/A]
[Dr. Loomer]So what you would do here is you would clean out the area, place a
bone graft in there. You can buy bone-grafting material in little packets. And bone-grafting material can be made out of various things. It can be just calcium phosphate
which is the main mineral in bone. It can be from cadavers. So there are bone banks
where they take bone from cadavers, chop it up into very tiny particles. Sometimes
50 microns up to maybe 200 microns usually. And you can buy it kind of looks like
salt but a little bit more granular. And you add some sterile water. You can pack it
into that defect. And sometimes you can buy bone graft, which is combined with
growth factors such as platelet derived growth factor or enamel proteins, which
8/10/2019 51/52: Periodontist and Periodontium
5/32
8/10/2019 51/52: Periodontist and Periodontium
6/32
Transcribed by Anam Khalid Monday, October 20th, 2014
6
like 1 to 2 mm below that. So youve lost a lot of bone. But you clean out that area
really well.
[Slide #16] [N/A]
[Dr. Loomer]And heres the bone graft placedin the area. And its freeze dried
demineralized bone which you buy in a bottle and you reconstitute it. You add somesterile saline to it to hydrate it. A little bit and make it a little more packable.
[Slide #17] [N/A]
[Dr. Loomer]And then this is how it looks on the radiograph. Again, you can sort of
see where it was. And itll take a long time. You know, six to twelve months, before it
completely is gone and new bone has formed.
[Slide #18] [N/A]
[Dr. Loomer]And this is how it looks at a follow-up. So tissue looks nice and
healthy. And in reality not every case works out so perfect. But it ideally, if you have
a successful procedure, when you probe the area its going to be minimal probing.Yes?
[Student]Is there a difference between cadaver bone versus just regular calcium
phosphate?
[Dr. Loomer]So, yes. The question is is there a difference between cadaver bone or
just using a calcium phosphate material. Cadaver bone and its available in
demineralized freeze-dried and freeze-dried non-demineralized and the studies
really are about equivalent, whether you use demineralized or not. It also has some
matrix proteins. So should have a certain amount of bone growth factors different
proteins that are available in the extracellular matrix. You know, bone is mostlycalcium phosphate and collagen type I. And then theres a small amount of the extra
of other types of proteins like osteopontin, osteocalcin other proteins that are
part of the other proteins that will induce or promote osteogenesis, bone
formation. So in a cadaver theres a small amount of that. The challenge is it varies.
Because it depends if its an old cadaver or if its a young cadaver. Young cadaver
will have more cadaver from a young person will have more of that protein so its
very variable. So what some manufacturers have tried to do is make calcium
phosphate but then add in a growth factor like platelet-derived growth factor so you
can be consistent on the amount of growth factor you have. So thats sort of the
newer way of looking at it. Of course you do have patients who dont want anything
from a cadaver. I mean, its been tested for everything but there against that forwhatever reason so you have that. You also have bovine bone grafts. So from cows
for example and theres also been porcine as well. So there are different animals that
have been used as well for harvesting bone grafts. And human bone grafts in many
countries are not allowed. So a lot of European countries, they dont its not an
option to even use it.
[Slide #19] [N/A]
8/10/2019 51/52: Periodontist and Periodontium
7/32
Transcribed by Anam Khalid Monday, October 20th, 2014
7
[Dr. Loomer]So lets look at another thing you might want to do with bone grafting.
This is an area where theres an edentulous area in the premolar-molar region. And
theres been a lot of bone loss there. Theyd like to place implants but there isnt
enough bone there because you also have the sinus above it.
[Slide #20] [N/A][Dr. Loomer]But you can do a bone graft in that area. We dont have the pictures of
it to show you just for expediency but basically the area can be grafted with bone as
well to increase the dimension there to allow for enough room for bone graft for
implant placement. Sometimes you just want to increase the bone so that when you
have a denture you have more of a ridge for the denture to hold onto for as well for
retention purposes.
[Slide #21] [N/A]
[Dr. Loomer]Ortho-perio. Sometimes youll have patients who have impacted teeth
such as cuspids. And you can expose them partially expose them. Do a little flap to
partially expose the tooth. Put a little bracket on with usually like a chain, like adaisy link. And to then orthodontically pull that tooth down into alignment. And
usually the orthodontist will work with the periodontist. Its also oral surgeons do
this as well to put that tooth into alignment as well.
[Slide #22] [N/A]
[Dr. Loomer]Heres another view of that area. Another thing that periodontist
interact with orthodontists is through the use of mini-implants for the use of
anchorage. So lets say you were
[Slide #20] [N/A]
[Dr. Loomer]Lets go back to this case for a second. Lets say you wanted to letssay this was a crowded area here between the premolars between sort of the
canine and the lateral and you wanted to create more space. You wanted to pull this
tooth back but you dont have any posterior teeth for anchorage. You can place a
little mini-implant in the posterior. Use that for anchorage to pull your teeth back.
So to create some space for the anteriors. And there are these very small implants.
Once you place them, once you use them, you pull the teeth back, they can be easily
removed. So theyre temporary anchorage for orthodontic purposes.
[Slide #21] [N/A]
[Dr. Loomer]And actually, some of those implants we did a study not long ago
using those mini-implants for over-dentures, you know when you have a completelyedentulous ridge and you want to have a couple of implants so that the denture is
retained really well. The mini-implants actually work very well and theyre easy to
place as well. Dont require a lot of bone.
[Slide #24] [N/A]
[Dr. Loomer]So implant therapy is probably very these days in periodontics
probably I dont know 60 to 70% of the practices these days are spent doing
8/10/2019 51/52: Periodontist and Periodontium
8/32
Transcribed by Anam Khalid Monday, October 20th, 2014
8
implants or getting the patient ready for implants. Because a lot of the bone grafts
that Ive shown you, you need to do in areas where youre going to place implants
because typically implants are a loss because well, for a variety of reasons but
the most common reason is due to periodontal disease. So youve got bone loss
around the area. Tooth is now hopeless. Youre unable to restore it through
conventional means. Tooth is removed and implant needs to be placed but becauseyouve lost all that bone, there isnt enough bone for an implant so often you have to
build back the area with bone for implant. So this is just showing you an anterior
tooth
[Slide #25] [N/A]
[Dr. Loomer] where the implant is placed.
[Slide #26] [N/A]
[Dr. Loomer]And actually anterior the front of the mouth is probably the most
challenging area for implants because youre not only managing the implant
placement but youre managing the aesthetics and whats really key of course is the
[Slide #27] [N/A]
[Dr. Loomer] the smile line because, you know, the patients going to bottom
line is theyre going to look at that implant once youve restored it how does it
look in terms of the aesthetics. So this is very key. You can see here I thinkthey
should have used slightly they didnt match the shade that correctly. It should be a
little bit more yellow there. But the form looks really nice. And whats really critical
here is they were able to maintain that interdental papilla. Thats probably the
biggest challenge in dentistry. When youre doing an implant, is to maintain that
interdental papilla. Because you can have a really nice fitting crown but if youregingiva recedes and you have a black triangle there its not going to be very
aesthetic. So how do you maintain that once the tooth is gone is very critical.
[Slide #28] [N/A]
[Dr. Loomer]Okay. And you can see in this area the tooth is missing but the
interdental papilla has been really well maintained. When you do surgery in that
area you want to make sure that youre able to maintain that. That you dont
traumatize the area and cause that gingiva to recede because its almost impossible
to regenerate it.
[Slide #29] [N/A][Dr. Loomer]This is just showing the other slide
[Slide #30] [N/A]
[Dr. Loomer]And this is with the crown as well. So they maintained
[Slide #31] [Site development]
8/10/2019 51/52: Periodontist and Periodontium
9/32
Transcribed by Anam Khalid Monday, October 20th, 2014
9
[Dr. Loomer]So lets look at a little bit about site development. Thats what we
were talking about earlier where you lost a tooth but you got to kind of develop the
site so that its now suitable for an implant.
[Slide #32] [N/A]
[Dr. Loomer]And this is the posterior maxillary posterior area. Often you have asinus in the area.
[Slide #33] [N/A]
[Dr. Loomer]Just above where youd like to place the implants. And in that case
you may not have enough bone there. If theres a sinus there. So what you want to
do is do some kind of grafting into the sinus where you create a window. You raise a
flap, you create a window through the sinus. Sinus is basically an air space. And you
can place bone graft into the sinus, cover it up again with a membrane. And that will
turn to regular calcified tissue into which you can place your implant. So whats kind
of interesting is that the sinus, you know, you can fill the sinus with bone and people
dont seem to have any problems. So its almost as if the sinus really doesnt have areal mandatory function anymore.
[Slide #34] [N/A]
[Dr. Loomer]And this is just showing that area as well.
[Slide #35] [N/A]
[Dr. Loomer]Another area where you may want to try to do something to make it
more aesthetic is when you have a bridge and often when you take out teeth, the
area will shrink both the soft tissue and the hard tissue. When theres no force
placed on an area it tends to want to shrink. Disuse atrophy. Its kind of like when
the astronauts go into space and theyre in a zero gravity area. Theres no force ontheir bones and so their bones start to lose calcium. Muscles will start to atrophy
and if theyre out for long enough when they come back to earth they have trouble
walking. And they have to be sort of rehabilitated to normal gravity. Well the same
thing kind of happens in the oral cavity when you lose the teeth for whatever
reason. Often the area will shrink back. So this area here you can see a gap between
these pontics and where the soft tissue is and that wasnt always like that. It was
closer when they first did the extraction but as everything healed and with many
years of lack of use, that shrinks back and now youve got a space there. And of
course patients dont like that because its an area where food can get trapped. If
youre going to keep it or if youre planning on redoing it and putting any implants
youre not going to have enough bone in that area. So you want to redevelop thatsite.
[Slide #36] [N/A]
[Dr. Loomer]So, what you would do. Of course, youd want to remove your bridge
and assess the area. Theres different ways that that can be managed. If youre just
looking at soft tissue, you just want to plump out the area so theres no space
between your bridge and the actual soft tissue ridge so that foods not getting stuck
8/10/2019 51/52: Periodontist and Periodontium
10/32
Transcribed by Anam Khalid Monday, October 20th, 2014
10
underneath the bridge. You can do whats called the soft tissue graft where you
would do an incision here. You take soft tissue from the palate, tuck it underneath
the tissue here and that would plump out the area. And thats connective tissue
graft.
[Slide #37] [N/A][Dr. Loomer]And this is just looking at that area radiographically. Now, in this case,
you may say well, I want to do that but I also need some bone there because I know
that one day Id like to do some implants in that area. And you can see here all the
bone loss in that area. So youd like to kind of graft that area, build it up because you
can graft beyond the socket sure, you can just graft in the socket but if you want to
really make it wider you can go beyond the socket. Put all your particulate bone
graft and then cover it with a membrane so as to retain it in the area.
[Slide #38] [N/A]
[Dr. Loomer]And thats what was done in this case. So they did a bone graft. You
can see here that its much thicker or more radiopaque so they built up that area
[Slide #39] [N/A]
[Dr. Loomer]And then clinically you can see its a better fit. So, not perfect but often
that kind of a procedure may require both a bone graft to build it up and a soft-
tissue graft to build it up a little bit further. And so it may require more than one
surgery to do that. But the result is an improvement for the patient.
[Slide #40] [Esthetics]
[Dr. Loomer]Periodontal plastic surgery, as its been called, or esthetic procedures
that are done to improve the patients smile.
[Slide #42] [N/A]
[Dr. Loomer]And different things can be done. This is kind of your ideal smile.
When you look at the teeth and you look at the patients. Youregoing to retract the
lips. Youre going to look at the gingiva. And what youre looking foryoure looking
for nice, obviously, color, contour of the gingiva. Look for symmetry. Doesnt have to
be perfect but you ideally you have nice symmetry between one side and the other.
You can see its pretty good. The lateral is a little bit longer on this side than on that
side so you dont have perfect symmetry. Midline is something people look at. Its
not exactly matching but its close. And you want, of course,your centrals to be
longer than your laterals. Your canines to be longer than your laterals. So youre
looking for a nice smile. And of course this patient has no recession so you dontshow any tooth root which may be a different color. But thats only one way you
want to look at.
[Slide #43] [N/A]
[Dr. Loomer]When you assess someones smile you want to assess it with their lips
relaxed. Either at relaxation and also when they smilea big smile. Because you
want to see how much gingiva is exposed. And sometimes the patients complaint
8/10/2019 51/52: Periodontist and Periodontium
11/32
Transcribed by Anam Khalid Monday, October 20th, 2014
11
would be, I have a gummy smile. So when they smile they show too much gingiva.
Usually its a discrepancy between the amount of the tooth exposed and the amount
of gingiva showing. So sometimes making the teeth longer by doing a surgical
procedure where you cut away some of the gingiva may help. Or sometimes it
requires a little bit further treatment where you may even remove a little bit of
tissue and bone to make a longer tooth. Sometimes its an orthodontic issue wherethe upper teeth have overgrown based on the bite. So it cant always be fixed using
periodontal techniques but you want to do what they call a smile analysis. Youll
sometimes see dentists advertising that. Because if you dont get the factors right as
to why the smile looks the way it is then its hard to treat it correctly. So, in this case,
you know, if you looked at this patients smile and if theyre happy with it then of
course thats whats most important, not what you want but what they want. But
they show a little bit of gingiva in the maxillary teeth but nothing in the lower.
[Slide #44] [N/A]
[Dr. Loomer]This patient in here has some localized recession so you could see the
gingiva looks pretty good here. Theres a little bit of recession there but this onepremolar has quite a significant amount of recession. You can see this is your CEJ.
This is the gingival margin. This tooth has the the cuspid has a little bit of
recession but their complaint here was the tooth is sensitive when they drink
something hot or cold. That was their chief complaint and theyre not happy with
the appearance as well. Although it is on the sidewhen they smile it shows. So
theres different ways to manage that. If you did a composite resin over that you can
see theres a little bit of tooth brush abrasion in that area. If you did a composite
resin over that to cover the exposed dentinal tubules, that might help with the
sensitivity. Fluoride varnish might help as well. But that wouldnt solve the aesthetic
concern for that area. So is there something we can do to grow back that gum tissue,
that gingiva in that area? That would solve both problems? And of course there is,its called a gingival graft and
[Slide #45] [N/A]
[Dr. Loomer] its where you takea piece of tissue from the palate and the area is
that tissue is grafted into this area, placed on to the area. And youre going to get a
lecture on grafting down the road. But basically you can transplant tissue from the
palate. It all grows back without any scar. Its all regenerated. And this tissue will
integrate into this area to cover this area. This was a month after surgery.
[Slide #46] [N/A]
[Dr. Loomer]And then this is further down the road. You could see its blended inquite nicely. And whats very critical here, of course, is figuring out why it occurred
so you dont want the patient to for that to reoccur. If it occurred due to
aggressive tooth brushing you want to make sure theyre brushing gently using a
soft toothbrush. If it occurred because of tooth position its usually a combination of
tooth position the tooth is a little more bucally placed towards the cheek and
therefore when they brush, they hit that one first. Sometimes that can be fixed
8/10/2019 51/52: Periodontist and Periodontium
12/32
Transcribed by Anam Khalid Monday, October 20th, 2014
12
orthodontically. But often, you want to just make sure the patients using a soft
toothbrush and theyre gently cleaning the area.
[Slide #47] [N/A]
[Dr. Loomer]Okay. And thats another area where you can see where the graft is
now now in this case whats interesting to note is theres some, you know, racialpigmentation in this patient. And when you take a graft piece of tissue from the
palate to another area, the genetic message is all in the connective tissue and itll
retain the color of the palate. So, if you take it if you have an area that has a
different pigmentation and you transplant tissue from another area, youre going to
see a bit of a difference. So, you can see it looks pinker because the palatal tissue
doesnt have as much pigmentation, as much melanin in it. So, some of things just to
be careful of or to warn the patient you may have that issue.
[Slide #48] [N/A]
[Dr. Loomer]So, thats sort of something thats kind of interesting in periodontics
because youre doing procedures but all the procedures have a lot of biology to it.Youve got to understand how the bone cells work, how the gingiva, the cytokines,
the immune system, microbiology, the bacteria so its a biologic science. You may
be doing procedures that have a certain technical demandknowing how to do
them. But you have to understand the biology and respect the biological principles
or your procedures are going to fail. If youre doing a surgery and you, you know,
make your incisions incorrectly your tissue may die because you didnt really abide
by the basic biological principles to keep the tissue viable. So, thats what I think also
makes it an interesting area and in your lectures youll always hear about the
biology.
[Slide #49] [N/A][Dr. Loomer]This is another case where a patient has a very excessive amount of
gingiva partly due to a deep class II overbite where the upper teeth have actually
sort of super-erupted not just in terms of teeth but also the whole maxilla. And
youve got excess gingival appearance.
[Slide #50] [N/A]
[Dr. Loomer]So one way to look at how much lets say you want to increase the
amount of gingiva you want to decrease the amount of gingiva by cutting some
gingiva away or doing what they call a crown lengthening which can involve cutting
away some of the gingiva but also removing some bone to physically make the tooth
longer. That will allow you to expose more tooth structure for more of a balancedappearance. But how much should you remove is very important to try to analyze
that and determine that before the surgery. So the dentist who would be working on
the case to restore the area, to put new crowns or to have a final product, can take
an impression of the area, pour up the model. On the model you can remove some
gingiva until you get a nice dimension and then you make a little stent, a clear stent,
an acrylic stent here where you model where exactly youd like it. So when the
surgeon goes to remove some of the gingiva or do what they call a crown
8/10/2019 51/52: Periodontist and Periodontium
13/32
Transcribed by Anam Khalid Monday, October 20th, 2014
13
lengthening where you make the crown longer at the expense of the root, of course,
they can put this little plastic stent which fits over the teeth. Its kind of a little
looks like Invisalign retainer if youve seen those. And it tells them exactly where
theyd like the new margin of the gum tissue of the gingiva to end. So this way you
have a more accurate idea because sometimes what one dentist may think is what
they want may not be exactly what the patient wants. So this way if you create this,patient can see exactly how long their teeth are going to be after the surgery ahead
of time. And you can adjust it in advance.
[Slide #51] [N/A]
[Dr. Loomer]And you may say, well it looks a bit long. And yes, I would agree, I
think its still a little bit long. Butthey have less gingiva so that was, you know, a
benefit for that patient. And sometimes that can be combined with doing veneers to
adjust the lower edge or to just adjust the tooth so you may have to do a
combination, restorative and periodontic procedure to get the desired final look that
you want. So these are fun cases because when youre dealing with aesthetics, you
know, getting it exactly right is a lot of artistry involved which is always fun.
[Slide #52] [Pre-Prosthetic Therapy]
[Dr. Loomer]Pre-prosthetic therapy is basically similar so these teeth are very
short because the patient has worn them down. So they dont like their look because
when they smile, they have very short teeth and that makes them look old, you
know somebody whos been wearing down their teeth. And that may not be the
case. It could be they just have ... theyve been grinding a lot and their teeth have
become very thin. Sometimes, excessive consumption of acid will cause erosion and
the teeth will then grind down more easily. So you would like to on these people as
well youd like to increase the crown length. Maybe you want to make new crowns
as well because youve got chips. But you dont want to make the new crowns untilyou increase the crown dimension.
[Slide #53] [N/A]
[Dr. Loomer]So, you can pour up the model. This is the teeth that we just showed
you. And then on the model, you pencil in where youd like the final look to be. And
then you can wax it up and make your acrylic stent. The, basically, like an Invisalign
tray to this wax-up. But you can use acrylic so it doesnt you know, the wax form is
you heat up the wax form to produce it so you want something thats not going
to melt. You wouldnt use wax. But some kind of acrylic. And that can then be
smoothed off and that can be used as your form for figuring out how much gingiva
and bone you need to remove.
[Slide #54] [N/A]
[Dr. Loomer]And thats showing what they did. This is before new crowns were
made.
[Slide #55] [N/A]
[Dr. Loomer]And then this is after. So got quite a nice result.
8/10/2019 51/52: Periodontist and Periodontium
14/32
Transcribed by Anam Khalid Monday, October 20th, 2014
14
[Slide #56] [Periodontal Medicine]
[Dr. Loomer]And the final thing Im just going to mention very briefly because
youre going to have lectures on this. But, theres a lot of research now looking at the
effect of periodontal disease or more specifically, inflammation on various states of
disease. and it can be a relationship to the bacteria so if certain bacteria hae beenimplicated in the pathogenesis of periodontal disease and some of these bacteria
have been found in other external sites such as the heart and the lungs. So it could
be an interaction of the bacteria thats caused periodontal disease are being seated
in distant sites and causing damage. Or it could be due to the increase in
inflammation in the periodotium. Increase in the amount of C-reactive protein for
example. And thats causing the damage to other organs in the body. So theres a lot
of research on that. Its not an easy thing to prove because a lot of diseases are very
slow to develop so to show that in an animal you might be able to do because an
animals life is short, typically. But in humans, thats very difficult to show a cause
and effect. You can show a relationship. You can show people who have heart
disease also have more periodontal disease but one doesnt necessarily cause theother. But its a good area to research and these are some of the things that have
been studied extensively in terms of periodontal disease. Diabetes, in particular
theres been some trials looking at diabetes and the effect of therapy on diabetes
kind of control diabetic outcome. Youll notice in your patients, once you start to see
them, people who have diabetes theres a higher risk of periodontal disease because
a lot of diabetics have poor healing. Theyre able to control infection less than
normal individuals. So theres more periodontal disease in diabetics. So is the
reverse true? If you can control periodontal disease, will that help you to control
diabetes and it really the verdictis not in. Some studies have shown yes. Some
studies have shown no. But it probably depends on not just on the periodontal
disease but other factors as well. And so it may be one of the factors and if youcontrol a lot of factors youll control the diabetes but maybe if you only control
periodontal disease, that may not be the only thing involved.
[Slide #57] [N/A]
[Dr. Loomer]Cardiovascular disease, its been shown that arthromas contain
bacteria from the oral cavity that are common found in the oral cavity in
particular, ones in periodontal disease. Now, when you have a lot of inflammation in
the pockets you have very open capillaries. When you brush your teeth you get a lot
of bacteria invading into the pocket and these can then travel from the bloodstream
to the heart and are those causing disease or are they already if the heart has
damaged and then you have periodontal bacteria floating by now they can attachto this damaged heart valve, for example. Or a wall the atrial wall and then cause
further damage. So thats some of the theory behind that.
[Slide #58] [N/A]
[Dr. Loomer]And this is just showing you from a surgery the infected patient
with periodontal disease.
8/10/2019 51/52: Periodontist and Periodontium
15/32
Transcribed by Anam Khalid Monday, October 20th, 2014
15
[Slide #59] [Respiratory Disease]
[Dr. Loomer]Respiratory disease. its sort of a newer area. And two ways
periodontal disease can affect the lungs through direct aspiration of bacteria where
a patient swallows a nidus of bacteria. But also through inflammation causing more
pulmonary disease. So these are just some of the things that have been researched.
[Slide #60] [Research]
[Dr. Loomer]And of course, theres a lot of research a lot of journals in
periodontology. Id say, of the areas in dentistry, really periodontics has the most
amount of research because its really dealing with a disease. so theres more things
that you can research. Its not a there are techniques that are described. Say, for
example, the International Journal of Periodontics and Restorative Dentistry. We
used to call that one the coloring book because it has a lot of nice colored pictures.
But its looking atmore surgical techniques to improve aesthetics or implants. Its
really a technique-driven journal. Journal of Periodontology. Journal of Periodontal
Research have a combination of clinical techniques new techniques to do things
but also research looking at cytokines, bacteria, inflammation, diseases, all sorts ofstuff. So, its a good area as well if youre interested in a career. Youre thinking
about a career, its an area where theres lots to research in. And thats it for today,
for my lecture. Are there any questions? Just an overview of the topic. Youre going
to get more detailed lectures from the faculty. I think you have another lecture after
this talking probably about examination Im not sure. And then next year, in the
advanced course The clinic on 5W you get to do in the clinic basic treatment of
periodontal disease and there is an honors course where you can learn to do
surgery. Theres even an implant honors course where you can learn to do surgery
for placement of implants. Its also run by the perio department. But you can also
anytime youre more than welcome to come to the clinic on 5W. Its the perio clinic.
And help out with the different surgeries. Its very interesting, the techniques thatyoull learn and its actually helps you as a general dentist as well because you can
see once you see how the bone and how the decay is affected and the tissue it
helps you in determining your crown design and whats going to work, etcetera. And
so if you have any time during the week, please feel free to come down any time. The
residents are always happy to see you there. Thank you again and I guess you have a
little bit of a break until your next lecture. Thats it. Okay.
The Periodontium in Health by Dr. Julie Yip
[Slide #1] [The Periodontium in Health]
[Dr. Yip]Hello! Okay. Sorry I have a black screen. Yeah. Afternoon. Im Dr. Yip. Ill be
giving you 4 lectures. The lectures are all on the internet at the moment and for thislecture, for the first time, because your exam is going to be very clinical so Ive
decided not to post the 40 page mucho mucho lecture for this lecture. Okay? So you
just have to go through the slides. So, I mean its on the you know, in your what do
you call that thing the I what is that thing called? Itunes, yeah. Its on your iTunes,
on your classes, you know? But the thing is that if you have this, its easier to read.
The PDF. Its clearer. So thats what you study from, okay? Pardon? Not that 40-page
thing. Okay? Because last year I was shocked that I mean I posted my questions
8/10/2019 51/52: Periodontist and Periodontium
16/32
Transcribed by Anam Khalid Monday, October 20th, 2014
16
usually we give 4 questions per lecture but they decided to do it case-based so being
case-based, I dont have control over what questions come out. So I dont feel that
its fair for you to read that 40-page thing. And I dont know whats coming up. You
understand what Im saying? Then I dont know what to emphasize, you know, and
its 40 pages. I said, oh, I feel so bad making the last class go through 40 pages. Okay?
So, this year, its just the outline is 83 slides. Its not too bad. Okay? So its the basicstuff about the periodontium. I mean, its like that was actually the textbook, the
40 pages. I didnt make it up. It was like the textbook. I actually bulleted for people.
So they found it very useful but anyway. But its like I guess I have to say that,
right? Because its otherwise oh, my gosh, I wasted all my time blah blah blah,
right? Yeah, thats not very if I can get this to work. Because my laptop somehow it
doesnt show this is not good. Where is my it doesnt look the same as it usually
does. So I dont know where things are there we go. Well, at least we can see that
there. Thats why I needed a clicker. But luckily they came so everything is working
out. Okay, so this lecture is giving you the basis of health. You all had lectures on the
histology, right? So this should be mucho easy. Had it on histology? But I heard in
histology, it's a bit fragmented. Is that true? But this is periodontium. Okay, so whatis the periodontium made up of? Does anyone know? Gums! Okay? So one is the
gingiva. Okay. What you dont see is called the periodontal apparatus. Apparatus.
And that is consisting of the supporting structure of the teeth which is the
cementum, the PDL, and the? Alveolar bone! Excellent! Okay? So that's what we're
going to be doing today. It's all about the periodontium. Okay? I guess I should go to
... I dont have a as you can see I am using the screen because my screen is black.
That is not good okay. Okay, so lets see whether this works so that I can walk
around.
[Slide #2] [The Periodontium]
[Dr. Yip]So there you go. Right? Thats what were just talking about. So
[Slide #3] [The Periodontium]
[Dr. Yip]And you dont have to write any notes unless its extra of this. So ... you all
know about this is I like this slide because it gives you both the cross-section of
the tooth, okay? And then it gives you the photo. So this is what you see everyday.
This is actually the gingiva. And this is the alveolar mucosa. Okay? And this portion
here, this is the interdental papilla, okay? And this is the marginal gingiva and below
the marginal gingiva and were going to go through the landmarks, okay? This is
very important because youre going to do this actually you did it clinically
already, except now this is the background. This is like upside down. Unfortunately,
that's NYU. Okay? Its like, you know, everything is... I said, oh yeah, I havent givenyou the lecture yet. So now were going to give you the lecture. So this is the
attached gingiva. So, what's different from the marginal and the attached? Its that
the marginalwhat have you been doing in the clinic? When your friend says, ouch,
ouch, ouch? Youve been probing. So that part where its you can probe, thats the
free gingiva. So the keratinized gingiva is made of two sectionsthe marginal and
attached. Attached is where its attached to mucous and were going to go through
that, okay? And this is what you dont see. Okay? The cementum, the PDL, and then
8/10/2019 51/52: Periodontist and Periodontium
17/32
Transcribed by Anam Khalid Monday, October 20th, 2014
17
the bone. And of course, just to give you a rough age, the bone is made up of three
components, okay? And that isthe socket, which is alveolar bone proper, okay, and
then you have the trabecular bone, and then you have the cortical plant on the facial
and the lingual cortical plate. Okay? So its basically the socket is cortical and then
sandwiched in between you have the trabecular bone and then again on the other
side you have the cortical plate of bone on the buccal and lingual. Okay? So lets havea look at the next one Oh, and one more thing I want to point out is that at the
base of your pocket when you are probing what is that structure? Before your friend
says ouch? Very good. Junctional epithelium. And one thing is that I want to point
out to youwhere is the junctional epithelium in health, okay? So, were going to do
that. Suspense, suspense. Okay?
[Slide #4] [The Oral Mucosa]
[Dr. Yip]So the oral mucosa, okay? There are three parts to it, okay? First you have
the gingiva and the palate, which is called the masticatory mucosa. Then you have
the tongue, the dorsum of the tongue which has got the specialized mucosa because
its got taste buds, right? And then you have the oral mucous membrane on the rest the alveolar mucosa, the buccal mucosa, all that. Okay? And then
[Slide #5] [The Gingiva]
[Dr. Yip]Of course, you have the mucogingival junction as usual. Okay? Thats the
mucogingival junction separating the gingiva from the alveolar mucosa.
[Slide #6] [The Gingiva]
[Dr. Yip]So, you know where the gingiva is, okay? It covers the alveolus as well as
around the necks of the teeth, right? And it is three parts, again. What are they
again? The marginal, the attached gingiva, and interdental gingiva. Okay?
[Slide #7] [The Gingiva]
[Dr. Yip]So, the same slide okay. So you know attached, okay. So the attached is
separated from the marginal, just to point out, okay by the marginal groove. Okay?
Its present in 50% of patients and basically and Im going to do this later so I
wont talk about it okay.
[Slide #8] [Marginal Gingiva]
[Dr. Yip]So, the marginal gingiva. So you have been probing is actually the sulcus
depth, right? For most of you have 1 millimeter or so, right? And where is the
gingival margin located normally? Is it at the CEJ? If it tells you that usually the
sulcus is 1 millimeter wide. And we know that junctional epithelium is at the CEJ. Sowhere is the marginal gingiva located?
[Student]At the CEJ?
[Dr. Yip]--Coronal? Very good. It's about a millimeter. Okay? Above. Because if this is
a millimeter, then of course it has to be a millimeter. Okay, in the interproximal area,
roughly, its like --what is present interproximally? That you have to take into
8/10/2019 51/52: Periodontist and Periodontium
18/32
Transcribed by Anam Khalid Monday, October 20th, 2014
18
consideration when you probe? How far do you think ... when you draw in, in your
chart, where do you think the gingival margin is interproximally? You know it goes
scallop? Right? So if its scalloped, its a big higher interproximally so its about 2
millimeters in health. Okay? So when you draw your periodontal charting, okay,
make sure that you dont draw it everything at the CEJ because thats a mistake most
students make and what happens if you draw the gingival margin at the CEJ?Everybody has periodontitis, right? Because youre actually saying that that is there
and then so you have a pocket depth of 2 millimeters, which means your junctional
epithelium is 2 millimeters below the CEJ, which means? Periodontitis! Okay? So
everybody, young people, everybody has periodontitis. Okay? So, very important
that you draw the gingival margin at the right position. Okay? In health usually, as I
said, its about a millimeter above in the buccal and in the lingual of the lower. And,
lets see, even on the upper, even on the palate, okay? So its about a millimeter
above in the buccal and palatal area and in the interproximal usually its about 2,
okay? Because or else, as I said, everybody will have periodontitis. Okay.
[Slide #9] [Gingival Sulcus][Dr. Yip]So the base of the pocket or the sulcus is the junctional epithelium. Why
do you think your friends have pain? Does the epithelium have nerves? Nerve
endings? No. Why do you think there's pain? They start saying your friend says--
ouch! You know then it starts bleeding. You say, ooh, it's bleeding.
[Student]Youre in connective tissue!
[Dr. Hip]--You're probably in connective tissue. Excellent. You're in connective
tissue. So that sometimes happens. And also the bleeding comes about because
theressometimes the subepithelium may be ulcerated. Okay? So we're going to go
through that. So remember that in the pocket, in the sulcus, one side is the sulcularepithelium, the junction is a base. Okay? The base is the what am I doing okay.
The base is junctional epithelium. This is sulcular epithelium. On the top margin is
the margin of the gingiva, the gingival margin. And of course, on this side is the
tooth. Okay? So you have this little area here where the bacteria hide, right? Thats
why when we brush the teeth, it has to be aimed at this area here, okay? Subgingival
if possible. So its v-shaped, as you can see. And allows your probe to go in, okay?
[Slide #10] [Depth of the Gingival Sulcus]
[Dr. Yip]So what's the difference between biologic probing depth and clinical
probing depth? So the differenceIll go into a little bit more detail next time. But
basically this one is when you do histological sections, you actually see where thejunctional epithelium is. In the probing depth, as I said, most of you or most of us,
because if theres a little bit of inflammation, we probe into the connective tissue. So
thats the difference. So sometimes after theres health has returned to the area, you
know, the inflammation has gone away, the collagen fibers would toughen up and
you actually probe in the junctional epithelium then. And so thats why the decrease
in pocket depth may be because of the decrease in inflammation and thats more
8/10/2019 51/52: Periodontist and Periodontium
19/32
Transcribed by Anam Khalid Monday, October 20th, 2014
19
resistance to your probe. Okay? And well talk about more about that next time.
Okay?
[Slide #11] [Depth of the Gingival Sulcus]
[Dr. Yip]But I just want you let you know there is a difference between the, you
know, what the biological depth and the histologic depth is and what we actuallyprobe. What we probe is usually more. Okay? Especially when theres inflammation.
Okay, so, lets see. So usually in most caseswhen we are in the clinic, a healthy
pocket depth is about 1 millimeter, 2 millimeters. Okay? By the time it reaches 4,
that's considered a bit deep and a bit diseased. Plaque can accumulate easily and
most patients cannot keep clean. Okay? So they actually, in histologic sections,
determine 1.8 so it varies between 0 and 6 mm and the reason for the variation is
because in some areas like the distal of the molars its very much deeper. Thats
what they say, okay, but I find that 6 is a bit unacceptable. There was one study that
show that range. So usually we say its about 1 to 2 mm. Thats about it. Okay.
[Slide #12] [Attached Gingiva][Dr. Yip]And then, as we know pocket depth is a very important diagnostic
criteria. Okay, so attached gingiva. Now, let's go to the gingiva. I dont want you to
get mixed up between attachment level and attached gingiva. So let's review this
again. What can you see in the mouth? That means what do you normally see when
you look in the mirror? It's the teeth and the gingiva. Right? You will see the gingiva.
You'll see the alveolar you will not see the attachment clinical attachment level
where the junctional epithelium is. Remember that because students always I ask
them whats the significance of the keratinized gingiva and they look at me like, oh,
is it the clinical attachment level? I said no, keratinized gingiva has nothing to do
with clinical attachment level. Because remember I told you the periodontium is
divided into the gingiva which is what were talking about and the periodontalsupporting apparatus which is the attachment levelwhich is the cementum, PDL,
and bone.
Okay? Dont get mixed up. That means the gingiva is what you see. Dont get
whenever I mention anything or gingiva you determine it from it's nothing to
do with your attachment. Okay? Just remember that. Okay? Your attachment is the
junctional epithelium and then all the fibers beneath that, okay? So let's have a look
at this. So we know that attached gingivaitsapical to the marginal gingiva, which
is the part that you probe. Okay? And it is firm and resilient and tightly bound onto
mucoperiosteum. So basically its this portion here. Its all bound down and it
doesnt move. The marginal gingiva, on the other hand, can be detached from thetooth surface with your probe. As well as sometimes you just blow air and the thing
is flopping around, okay? That happens sometimes and you say oh, my goshand
Im going to give you the reason why it flops around, okay? Were going to go
through the histology of that.
So, on the facial aspect you would see that it actually it is moveablethe alveolar
mucosa but the attached gingiva is not moveable. So that a way to distinguish it
8/10/2019 51/52: Periodontist and Periodontium
20/32
Transcribed by Anam Khalid Monday, October 20th, 2014
20
would be to move the lip and then youll find that the alveolar mucosa will move,
okay? And then the mucogingival junction, very importantseparates the gingiva
from the mucosa. Just like its name implies. Mucogingival junction. Its a junction
between mucosa and the gingiva. Okay?
[Slide #13] [Attached Gingiva][Dr. Yip]So the width of the attached gingiva is determined by taking the entire
keratinized gingiva, and minusing your pocket depth or your marginal gingiva.
Okay? So basically the attached gingiva is fromis a projection ofon the exterior
of the base of the pocket to the mucogingival junction. Okay so that part is attached.
Remember we talked about that in the previous slide. So it is this distance uh, lets
see. Its from the base of the pocket up to the mucogingival junction. So, to calculate
that you would take the entire keratinized gingiva minus the pocket depth. Okay? So
if they ask you what is the attached gingiva nothing to do with attachment level. It
is just indirectly, youre taking the pocket depth and minusing it out. Okay?
[Slide #14] [The Periodontium][Dr. Yip]So, its pocket depth its not you know that part is detached from the
tooth. Thats why you can probe. Okay, so the non-attached gingivawe used to
think that you need a certain amount. Now we know that people with a small
amount of attached gingiva can still have health as long as they keep it clean. But it's
usually greatest in the area of the incisors, you know, the central incisors. 3.5 to 4.5
millimeters in the upper maxillary incisors. And about 3.3 to 3.9 in the mandibular,
in the incisors. Okay? And the least is the first premolar area. Okay? In that area and
usually its only about 1.9 and 1.8. Okay? In the maxilla and mandible.
[Slide #15] [Interdental Gingiva]
[Dr. Yip]So the interdental gingiva now. Remember we did the marginal, we did theattached, and now the interdentalthird component of the gingiva. And that is
determined by the shape of the gingival embrasure. You know the embrasure is the
area under the contact area. And it's determined by the shape of the teeth, right?
The mesiodistal distance between them. And then also on the health, depends on the
contact point. The absence or presence of gingival recession. If theres gingival
recession like in this case, you see that? Its no longer fills the entire embrasure
space. And usually when theres recession, what does it mean? When does recession
occur in the interdental area? If you see this, what must have occurred? Excellent.
Bone loss. Very good. You guys are good, man. Okay? This one you can see mucho
inflammation. Mucho red. Mucho shiny. Okay? So all the symptoms of inflammation
are present. You see that? Okay?
[Slide #16] [Interdental Gingiva]
[Dr. Yip]So, this is a very important point, okay? The interdental papilla, usually it's
pyramidal in health. And also col shaped. Col shape is this valley-like depression
only in the molars usually. Teeth that have great buccolingual width, okay? Because,
when it's pyramidal like in the anteriors, there's only one papilla. So it's like a
pyramid. There's only one papilla, okay? Whereas, in the posterior teeth, because of
8/10/2019 51/52: Periodontist and Periodontium
21/32
8/10/2019 51/52: Periodontist and Periodontium
22/32
Transcribed by Anam Khalid Monday, October 20th, 2014
22
keratohyaline granules, okay? And then in the corneum they lose the nucleus
completely in orthokeratinized. In parakeratinization, its like they have big nuclei,
okay? So lets have a look at this.
[Slide #20] [Gingival Epithelium]
[Dr. Yip]So, the keratinocytes are joined by desmosomes, okay? So, usuallyanybody does music here? So, its made of two hemidesmosomes one
hemidesmosome, another hemidesmosome. One desmosome, okay? And its got this
dense plaque where all the tonofilaments get all the tonofibrils get attached to.
Thats basically the cytoskeleton of the keratin proteins. It gives the cells like, you
know, I guess its like a skeleton, okay? So, other epithelial cells have tight
junctions so remember all these junctions, they allows fluids to move, okay?
Between the cells. Ions and fluids but not it prevents like particulate matter from
going from one cell to the next.
[Slide #21] [Gingival Epithelium]
[Dr. Yip]So let's have a look at the melanocytes. Do you think that's normal? Havingmelanin? Absolutely. They say that actually everybody has melanin. It's a matter of
degree except the albinos. Okay? And what actually happens is that theyre dendritic
cells, okay? And theyre usually found in the basal and spinous layers and its
basically a hydroxylation process. Theres tyrosinase and then it kind of
hydroxylates the tyrosine to dopa and then from there it gets converted to melanin.
Okay? So usually it starts in the melanosomes.
[Slide #22] [Epithelium-Connective Tissue Junction]
[Dr. Yip]So, lets have a look at the basement membrane. This is a very this one
always comes up. You guys, when doing the part I boards next year, right?
[Slide #23] [Epithelium-Connective Tissue Junction]
[Dr. Yip]This is a very, very important structure. Because they always ask question
on this because its very confusing. The basal lamina is actually oh, my gosh. What
did I do? Ugh. Sorry. Pressed the stop button. I didnt know okay, so. Sorry.
[Slide #22] [Epithelium-Connective Tissue Junction]
[Dr. Yip]Im very newbie with this. Okay? But this is better than cellphone. Im a
retard. I call myself a cellphone retard. I dont know how to get rid of messages. Its
two messages. Im like how the hell do I get rid of these two messages. I still havent
figured that out yet. Okay. So, the basement membrane is below the basal layer of
epithelial cells.
[Slide #23] [Epithelium-Connective Tissue Junction]
[Dr. Yip]It's usually about 400 angstroms below that, okay? And its about three to
four hundred angstroms thick. Very, very important structure, because this is how
the epithelial cells connect with the connective tissue, and the other way. So, always
remember when you have this interface between the epithelial cells and connective
tissue you will have a basal lamina. And the basal lamina is basically made up of two
8/10/2019 51/52: Periodontist and Periodontium
23/32
Transcribed by Anam Khalid Monday, October 20th, 2014
23
parts. Lamina lucida and lamina densa. You all learned this, right? And very easy. I
never understood this until I had to prepare for this lecture. So, very easy to
remember it. Just rememberepithelial cells, lucida, very light. Okay? So, always
when its next to epithelial cells its always lucida. So the epithelial cell will have
lucida on this side, lucida on this side, okay? And then the connective tissue cells will
connect to the densa, which is actually type IV collagen. Whereas, the lucida islaminin. So laminin always epithelial cells. So just remember that. So epithelial cells
get lucida, lucida, okay? Because remember in the tooth, there are two basal laminas
for the junctional epithelium. The junctional epithelium cell will have lucida then
tooth, okay? And then you have lucida, densa, and then connective tissue. Okay? So,
when it connects to the connective tissue its always the anchoring fibrils. Okay?
Very important because they always ask you the order of the basal laminas in the
junctional epithelium. So its always connective tissue, lamina densa, lamina lucida,
junctional epithelium, lamina lucida, lamina densa, tooth.
[Slide #24] [Oral or Outer Epithelium]
[Dr. Yip]Very easy. I mean, just remember, lucida next to junctional epithelium.Lucida, lucida, and then you have the densa right to connective tissue. The densa
next to so you want dense. Dense is tooth. Okay? So just remember that. I mean, I
could never get it until I said ahhh! Finally! You know how it is aha moment?
Ah! Oh, I got it! So, just remember that. Lucida is epithelial cells. And always when
its connecting to the lucida, its always with the hemidesmosomes because thats
how you know epithelial cells join to something. Okay?
[Slide #25] [Oral or Outer Epithelium]
[Dr. Yip]So, just remember that the oral epithelium--the oral epithelium in the
cavity, in the oral cavity, is mostly parakeratnized, okay? It's a bit less keratinized
than the fully keratinized form, which is the orthokeratnied. That means it's got a lotof corneum, a lot of keratin. Okay. So, they found that the degree of keratinization
decreases with age as well with menopause, okay? And the keratinization of the oral
mucosa varies. Okay? So the palate is the most keratinized. Then you have the
gingiva. Then you have the ventrals of the tongue and then you have the cheek. The
cheek is the least keratinized. Thats why when patients bite the cheek, you know,
its very thin, okay? So the least keratinized. Not very protective.
[Slide #26] [Sulcular Epithelium]
[Dr. Yip]Sulcular epithelium. So it lines the gingival sulcus as we said. It is non-
keratinized. Okay, remember? Non-keratinized stratified squamous epithelium. Has
no rete pegs, okay? And it lacks--of course, because, whenever it is non-keratinizedgingiva, it will always I mean non-keratinized tissue epithelium, it will always lack
granulosum and corneum. So, spinosum and basale, okay?
[Slide #27] [Sulcular Epithelium]
[Dr. Yip]So they found that actually the sulcular epithelium has ability to keratinize
if you invert it and expose it to the oral cavity. Okay because of functional needs it
will keratinize. Then they found this is the bacterial actually keep it non-keratinized.
8/10/2019 51/52: Periodontist and Periodontium
24/32
Transcribed by Anam Khalid Monday, October 20th, 2014
24
A bit of irritation, you know? So, it keeps it non-keratinized. Somehow, I mean, I
thought that was a bit strange, but thatswhat they found, okay? And, the sulcular
epithelium is important, because, you know, it allows because its non-
keratinized, there is this free form. Remember I told you about the col area? Same
thing. So theres a free flow. Semipermeable and allows noxious things to go into the
gingiva which is why when the plaque is in the sulcus what happens? Inflammation,okay? So thats why very important to keep, you know, like patients homecare
should be very good. To keep the area clean, okay? And also allows gingival
crevicular fluid to actually come you know like the fluids come out and form
gingival crevicular fluid.
[Slide #28] [Junctional Epithelium]
[Dr. Yip]Okay, which is the fluid that's in the sulcus. Okay? And we're going to go
through that. Ah, this is the mucho important structure. Okay? Once again, it's non-
keratinized stratified squamous epithelium. The junctional epithelium, right? And
usually it ranges from 0.25 to 1.35 millimeters. This is very important because 0.25
is, of course, the short junctional epithelium, right? Very short. But it has somepropensity to multiply and actually form the long junctional epithelium. When do
you get long junctional epithelium? Uh, recession? What do you say? Excellent. After
scaling and root planing. Excellent. So thats what we aim for. Long junctional
epithelium. Yay! So we want that because after you clean it, its like Velcro. So it kind
of the junctional epithelium kind of like sticks to the tooth. Adheres to it. So its
like Velcro. If theres inflammation again it can un-Velcro itself, basically. So, there
are a lot of questions about whether or not it is as strong as if it had a true
attachment. But hey, Ill take anything that decreases a pocket depth, right? So its
like this is long junctional epithelium thats what we get. After any surgical
procedure, it's also long junctional epithelium. Okay? And you have this around an
implant. Okay? So the PMNs are routinely found at junctional epithelium whereas itis not so often found in the sulcular epithelium. So this is important. That means the
defenses are always there. Theres always some inflammation, okay? And you see, at
first, its 3 to 4 layers thick and then it just increases in life. But, of course, as I said,
after scaling, many more layers, okay? And it just sticks to the tooth.
[Slide #29] [Junctional Epithelium]
[Dr. Yip]So it is actually formed by the confluence of the reduced enamel
epithelium and oral epithelium as the tooth erupts. So these tooth structure join
up together and form the junctional epithelium. So then as the tooth erupts out of
the mucosa, you have the junctional epithelium at the CEJ. Okay? Actually it's a bit
above the CEJ. CEJ and up, you know, when it first erupts. Okay? And very importantis that the REE is not essential and that's why you get it reforming after scaling and
root planing. So thank goodness for that, okay?
[Slide #30] [Attachment of Junctional Epithelium]
[Dr. Yip]Okay, so this is, again, very important. So, remember, the internal basal
lamina is the one next to the tooth. And again, you have the tooth, then you have the
lamina densa. Then the lamina lucida. Then you have the junctional epithelium.
8/10/2019 51/52: Periodontist and Periodontium
25/32
Transcribed by Anam Khalid Monday, October 20th, 2014
25
Then next to thegoing out towards the connective tissuethen you have the
external basal lamina which is made of next to the epithelial tissue is again the
lamina lucida. And then the densa is next to connective tissue. Okay? So remember
that the internal basal lamina the question that might come up in the exam might
be something like whats the difference between internal basal lamina and any other
basal lamina? So it lacks type IV collagen in the lamina densa because its just youhave some organic strands coming out to the, you know, from the tooth to anchor it.
So it doesnt have type IV collagen. All the other lamina densas in other basal lamina
is usually type IV collagen because its next to connective tissue. But because in the
tooth its not next to any connective, its a tooth, right? So it doesnt have type IV
collagen, just laminin. And on the basal you see the side and on the other side its
just anchoring fibrils, the organic strands from enamel. Okay? So just remember
that. Okay.
[Slide #31] [Attachment of JE to Tooth]
[Dr. Yip]So thats just a picture. So its the this is of the internal basal lamina.
Tooth, lamina densa, lamina lucida, and the hemidesmosomes of the epithelial cells,okay?
[Slide #32] [Attachment of Junctional Epithelium]
[Dr. Yip]Okay, the important thing is the junctional epithelium remember I told
you that the marginal gingiva just flop? Like you blow air and its like ehhh, like
that. You know? Literally like ehhh. You know? Its like usually its very firm,
right? You know? In health? Like the gingiva is against the tooth surface. The other
one you blow it and it like just flaps open and you see all the calculus inside. And you
know why that happens? Because the gingival fibers actually surround the tooth.
Theyre these circular fibers and Im going to show you a picture of that. Andbecause theyre destroyed during inflammation theres no more hugging effect. So
the gingiva is kind of flappy. Very floppy. Okay? You just blow air and it flops down,
okay? So thats the reason why. So that unit which is actually junctional epithelium
and the gingival fibers together which form this tight, you know, like keeps the
gingiva to the tooth surface is called the dental gingival unit. So I can imagine that
could be another question that comes up in your board exams. You know what I
mean? Like what is it called? Its the dental gingival unit. Or what is the dental
gingival unit made up of? So its the junctional epithelium and the gingival fibers.
Okay?
[Slide #33] [Gingival Fluid][Dr. Yip]So the gingival fluid is, I told you, it seeps in, you know, and then it's inside
the sulcus. It cleanses material and plasma proteins help in adhesion, okay? And
then you have microbial properties and then you have antibody properties, okay?
[Slide #34] [Gingival Connective Tissue]
[Dr. Yip]And then connective tissue you have the papillary layer and the reticular
layer and the ground substance. This, you can read yourself. Okay?
8/10/2019 51/52: Periodontist and Periodontium
26/32
Transcribed by Anam Khalid Monday, October 20th, 2014
26
[Slide #35] [Gingival Connective Tissue]
[Dr. Yip]So the important part about the gingival connective tissue is what is inside
there. You have these fibers which are made of type I collagen, okay? Type IV is
usually the basement membrane.
[Slide #36] [Gingival Fibers]
[Dr. Yip]So these gingival fibersthere are three types. Gingivodental, circular and
transseptal so lets have a look at that.
[Slide #37] [Gingival Fibers]
[Dr. Yip]So you see they brace the marginal gingiva, like I told you, firmly against
the tooth. Very important. And so it doesnt get deflected away during mastication.
Very important. And it unites the marginal gingiva with the attached gingiva and
with the cementum.
[Slide #38] [Gingival Fiber Groups][Dr. Yip]So, these are the three groups. The gingivodental group. They are actually
like one, two and three. One goes up to the crest. Two goes out to the epithelium.
And three goes on to the periosteum. So thats actually the gingivodental group. So it
goes from the cementum, if you can imagine. Goes one, out the epithelium, and then
the periosteum. Okay? And interproximally it goes up to the crest of the interdental
papilla. Okay?
[Slide #39] [Gingival Fiber Groups]
[Dr. Yip]And the circular fibers are number 4. Okay? They go around the tooth.
Remember I told you? When they get broken down the tissue becomes very flaccid.
Okay? The marginal gingiva just flaps around, okay? And when you blow it, it willjust come apart. So it encircles the tooth in a ring-like manner.
[Slide #40] [Gingival Fiber Groups]
[Dr. Yip]And then you have the transseptal group. Very interesting group because
sometimes it considers as part of the periodontal fiber group. So this is a gingival
fiber group. Youllsee it being thrown it goes from one the cementum of one
tooth to the cementum of the adjacent tooth, okay? And its in between the
junctional epithelium and the crest of the alveolar bone. Okay?
[Slide #41] [Gingival Blood Supply]
[Dr. Yip]So lets have a look. Okay, these are the vessels. You have three. So theresintraseptal, supraperiosteal and then you have the PLD vessels supplying the
gingiva.
[Slide #42] [The Tooth Supporting Structures]
[Dr. Yip]So, the attachment apparatus. Lets switch gears. Now, this is what you
cannot see. Okay? This is part of that clinical attachment that supports the tooth
basically. So you have the cementum, PDL, and bone. Okay?
8/10/2019 51/52: Periodontist and Periodontium
27/32
Transcribed by Anam Khalid Monday, October 20th, 2014
27
[Slide #43] [The Periodontium]
[Dr. Yip]So, you already saw this.
[Slide #44] [Periodontal Ligament]
[Dr. Yip]So, lets go. What's the PDL? So the PDL is that part that connects thecementum to the bone. Right? And it's like a hammock. I would say it's like, you
know, like the two sides ... and what is ... What are the fibers that go into bone and
cementum called? Very good. Sharpey's fibers. So the two ends are calcified inside. It
goes boing-boing-boing! Whichever way, depending on which direction the fibers
go. Itslike when the tooth is depressed these are the fibers that are actually kind of
bounce around. Its like theyre actually wavy but they can be pulled taut when the
tooth is being depressed. Can you imagine that? Okay. So, it contours with the
connective tissue of the gingiva and it also communicates very important point.
Okay? It communicates with remember I told you at one end you have the bone?
So the bone is the alveolar you have the alveolar bone proper, right? Which is
what it is. What is the enemy for alveolar bone proper? Tooth socket? Right?Cribriform plate. Remember cribriform plate? Yeah? Thats what it is. Its all the
same thing. Cribriform plate. So there are all these holes there. Theres called
cribriform plate. So the PDL actually communicates with the marrow spaces and
actually thatswhat happens when you go boing-boing-boing! Its like there is this
fluid theory that the fluid from the fibers actually go into the marrow spaces. So that
means when you can have a rebound basically when fluid goes back in, okay? So it
has important implications when you take an impression actually.
[Slide #45] [Periodontal Ligament]
[Dr. Yip]But lets have a look at this first. So the PDL fibers, okay, are the most
important fibers in the connective tissue, okay? Thats the important component.Made up of type I collagen. Gives it good tensile strength, okay? And we talked about
Sharpeys fibers.
[Slide #46] [Periodontal Ligament]
[Dr. Yip]Okay, so in terms of as they fall. As the tooth erupts, first you have the
transseptal. Then you have the alveolar crest. Then horizontal. Oblique. Apical and
then interradicular, okay?
[Slide #47] [Principal Fibers of PDL]
[Dr. Yip]So, lets have a look at each. So transseptal we already said that. And
embedded in cementum.
[Slide #48] [Principal Fibers of PDL]
[Dr. Yip]Okay. Important thing is that when theres periodontal disease and these
fibers get destroyed, they get reformed again. Somehow its like they are always
there. So destroy, they reform again. So very important. Okay?
[Slide #49] [Principal Fibers of PDL]
8/10/2019 51/52: Periodontist and Periodontium
28/32
Transcribed by Anam Khalid Monday, October 20th, 2014
28
[Dr. Yip]Alveolar crest fibers. These are the fibers that you know when you have
orthodontic treatment and sometimes the tooth is rotated? They actually cut these
fibers because they actually resist lateral movement as well as they prevent
extrusion. So when a tooth is actually rotated they sometimes cut fibrotomy
they cut these fibers. But they found that cutting these fibers you know, its kind of
like they dont want the fibers to form back in this twisted location. So when the newfibers form after you like, you know, de-rotate the tooth. It wont go back to the
same location if you understand what Im saying. Yeah, so they actually cut these
fibers. Otherwise the fibers always keep on making the tooth go back into that old
position which is the rotated position.
[Slide #51] [Principal Fibers of PDL]
[Dr. Yip]But cutting the fibers doesnt increase mobility. Very important. Okay?
[Slide #51] [Principal Fibers of PDL]
[Dr. Yip]And then the horizontal fibers are at right angles to the long axis of the
tooth. It goes from cementum to bone.
[Slide #52] [Principal Fibers of PDL]
[Dr. Yip]Okay, and the largest group, of course, are the oblique fibers. Theyre the
ones I told you boing, boing, boing. So they kind of like go from the cementum and
coronally in a coronal direction they attach obliquely, in a coronal direction,
attach to the bone. So theyre like this. Okay? So when you depress a tooth, this thing
will pull taut. Okay? The fibers will, EH, like that, okay? So
[Slide #53] [Principal Fibers of PDL]
[Dr. Yip] and they bear the brunt of all those vertical masticatory forces. The
apical group fibers, very important to note, they do not form like incompletelyformed teeth roots. Okay? Very important. And its very irregular, in this area,
okay? And interradicular fibers, theyre in the furcation area.
[Slide #54] [Periodontal Ligament]
[Dr. Yip]Okay, so the functions of PDL are physical, formative, nutritional and
sensory.
[Slide #55] [Periodontal Ligament]
[Dr. Yip]Okay, so physicalmost important. It forms the casing. Its protective
function. Okay, now, of course, masticatory forces. We talked about that.
Transmission of the occlusal forces to the bone as well as shock absorption.Remember I told you about, you know, the fluid going out? So this is the favored
theory now, the viscoelastive system theory. But then they found that just the
tension of, you know, like just bearing the brunt like that is not enough to actually,
you know, for it to take all the forces. So they believe now there is this like shock
absorption kind of like ability. You know, the fluid going out to the marrow spaces
and then coming back later on when the forces are released, okay? So that actually is
very important. And then lets see the next one.
8/10/2019 51/52: Periodontist and Periodontium
29/32
Transcribed by Anam Khalid Monday, October 20th, 2014
29
[Slide #56] [Periodontal Ligament]
[Dr. Yip]Okay. So always remember that when you tip a tooth, it always rotates in
kind of like axis of rotation and its usually in the middle to apical third more
towards the apical. So remember that, okay? So whenever you tip a tooth, this part
here, theres compression on the cervical part as well as the apical part. When youtip a tooth this direction okay? So .. and then theres an area of tension at the other
side. So whenever that happens what happens? Whenever you move a tooth? When
you have tension its actually the other way. When you have compression then
theres resorption. So that youre trying to move a tooth, you know what I mean? But
orthodontics. So, when you have tension, thats where the deposition will occur
here. And then itll resorb here. Okay? So lets have a look so theres a bit of
deformation of the bone. First, it tries to take all the stress itself, the fibers. Then
gradually, as theres greater force, there will be some deformation of the bone in this
area and this area, okay? Usually no resorption unless youre using forces like
orthodontic forces, prolonged forces. Then you start getting resorption. Okay.
[Slide #57] [Periodontal Ligament]
[Dr. Yip]So, and then, we also know that PDL cells also participate in forming
cementoblasts and osteoblasts. Okay? And so it's very, very important because
actually all this turnover the PDL is a very important cell when it comes to that.
And in fact, the rate of turnover in the PDL is two times that of the gingiva and four
times that of skin. Can you imagine? Very mucho important. Okay? And the
interesting thing about the gingivaI dont know if I talked about the gingival
healing because its high turnover and then the way that its very quick in the
turnover. Theres very little scarring. When you cut the gingiva thats why
periodontal surgery you dont get much scarring at all. In fact, you get much more
in the mucosal area. So, I mean, thats really very good, okay? So remodeling okay. So, cementum.
[Slide #58] [Cementum]
[Dr. Yip]So cementumis an avascular mesenchymal tissue. You know that there
are two types, right? Acceullular and cellular. Okay? Acellular is the primary. It
actually occurs before the tooth reaches occlusal planeit starts forming. And then
usually its in the coronal 1/3 to of the tooth, okay?
[Slide #59] [Cementum]
[Dr. Yip]Whereas the cellular is formed later. Its cementocytes embedded in
lacunae. Okay? And the most important thing to remember iswhere does thesource of the fibers come from? For the acellular? This forms first. Okay? There are
no cells--so it comes from the PDL. They're the Sharpey's fibers. Thats where all the
collagen, the fibers actually come from that make up cementum in the coronal half.
And because its got no cells, what happens when you SRP? Any regeneration? You
scrape away mucho cementum. Thats why a patient can get sensitivity. Theres no
regeneration. Okay? Very important to remember that. So dont over-instrumentate
it. So thats a lesson. Theres no its acellular because thats the cervical third to



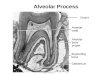


![PERIODONTIUM (10) [EDocFind.com]](https://img.dokumen.tips/doc/110x75/577d2ee51a28ab4e1eb0488d/periodontium-10-edocfindcom.jpg)






















