Embed Size (px)
Citation preview
8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 1/90
Retno Lestari

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 2/90
• Latin demens (without mind),
• Sindrom klinis o/k ggn organik
– karakteristik onset lambat
– Pe fs. kognitif
– Disfs. ADL
• 10% > 65th,• > 50 % > 85th

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 3/90

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 4/90
Non-Reversible Types of Dementia
Alzheimer’s disease
Vascular Dementia
Dementia with Lewy bodies
Fronto-Temporal Dementia
Others:
Parkinson’s Disease
Huntington’s Disease
Creutzfeldt JakobDisease
ProgressiveSupranuclear Palsy
Korsakoff’sSyndrome
Infection-RelatedDementia (HIV,
Syphilis)

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 5/90
Reversible Dementia
Malnutrisi
Dehidrasi
Disfungsi Metabolik
Defisiensi Vitamin B12
Depresi
Delirium

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 6/90
Perubahan Otak Saat lahir, otak > 100 trilliun sel syaraf/neurons
Dementia neurons pd bbrp bagian mati o/kpeny.ttt
Massa otak dpt ber< s.d 50%
Beberapa tipe: Alzheimer‟s (~55%),
vascular dementia (~20%), dementia with Lewybodies
(~15%), and frontotemporal dementia (~5%).
Parkinson‟s with dementia, Creutzfeldt-Jakob and
Huntington‟s disease.

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 7/90

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 8/90

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 9/90

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 10/90
Dementia- defined
Memory problems AND at least one
additional cognitive deficit:
– Aphasia
– Apraxia
– Agnosia
– Problems with “executive functioning”
8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 11/90
8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 12/90
Apraxia
“impaired ability to pantomime the use of
known objects or to execute known motor
acts”

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 13/90
Agnosia
Trouble recognizing or identifying things
despite intact sensations (ex. You can see
fine, but you can’t recognize a stop sign)
May include difficulty recognizing family
members or even themselves in the mirror

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 14/90
Disturbances in Executive
FunctioningAbstract thinking
Planning, initiating, sequencing, and
stopping behaviors
May manifest as trouble with novel tasks or
new situations

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 15/90
Masalah psikiatri
Agitation
Wandering
Insomnia
Catastrophic
reactions
Psychosis
Depression
Anxiety
Agnosia
Aphasia
Apraxia
Deficits in abstractthinking
8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 16/90
Psychometric tests „Mini-Mental State Examination‟ Sensitif thd kultur dan sosial
dpt berubah, harus dikaji lg
Brain-imaging Structural imaging (CT and MRI scans)
functional imaging (PET and SPET scans)
Cairan tubuh CSF

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 17/90
TREATMENT Agitasi
Perilaku
Lingk. Nyaman dan
aman
Stimulus fs. kognitif
Music
Terapi cahaya
Siang hari exercise,<i istirahat siang
Medications
Typical antipsychotics
(Haldol)
Atypical antipsychotics
(Risperdal)
Antidepressants -- watch
for agitated depression,
harus dikaji
benzodiazepines

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 18/90
Intervensi
DemensiaOrientasi
Tujuan membantu klien berfungsi di lingk
Tulis nama petugas pd kamar klien yg jelas,
besar dan terbaca Orientasikan barang pribadi, waktu, tempat,
orang
Penerangan di malam hari
Jam besar, kalender harian
Kontak personal dan fisik
Aktifitas kelompok
8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 19/90
Komunikasi
Komunikasi verbal: jelas, ringkas, tdk buru2
Topik percakapan dipilih klien Pertanyaan tertutup
Pelan dan diplomatis dlm menghadapi persepsi ygsalah
Empati, hangat, perhatianPenguatan koping
Kaji sumber kecemasan, koping masa lalu
Kurangi agitasi
Beri penjelasan, pilihan
Jadual harian
Penyaluran energi
Saat agitasi: senyum, sikap bersahabat

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 20/90
Keluarga dan Masyarakat
Siapkan kelg dan fasilitas di masy Perlu bantuan dlm merawat 24 jam di rumah
Home care

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 21/90
CHARACTERISTICS DEMENTIA DELIRIUM DEPRESSION

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 22/90
CHARACTERISTICS DEMENTIA DELIRIUM DEPRESSION
Onset Tdk terlihat, lambatdan tdk dikenali
Tiba2, mendadak Baru2 ini, b.d perub.hidup
Course over 24 hours Cukup stabil, berubah jika ada stres
Fluctuasi, gelisahmalam hari
Cukup stabil, mgknburuk saat pagi hari
Consciousness Sadar berkurang kesadaran sadar
Alertness Normal Meningkat, menurun,variasi
Normal
Psychomotor activity Normal, apraxia Meningkat, menurun,kombinasi
Variasi, agitasi/retardasi
Duration Berbulan2 s.dbertahun2
Ebrjam2 s.dberminggu2
Variasi (min 6 mgg),dpt berbulan2 s.dbertahun2
Attention umumnya normal Berubah, fluktuasi Sedikit ggn, mudahterdistraksi
Orientation Sering ggn (answermay be close to right)
Biasanya terganggu,variasi
biasanya normal, jawaban “saya tdktahu”
Speech Sulit mencari kata Sering incoherent,slow or rapid
Mungkin lambat
Affect Labile Variable Flat

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 23/90
Pseudo Dementia
( Depression )
Dementia
More acute onsetInsidious onset
Emphasizes failureDelights in accomplishments
UncommonSun downing Common
(increase confusion at night)
Often answer “Don‟t Know”Guess at answer ( confabulate )
Pt is aware of problemPt unaware of problem

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 24/90
Case 1
Ny. E, 80 th
keluhan: < tidur, nafsu makan <, BB turun
sedikit.
riwayat incontinence, cardiovascular disease,diabetes.
Bagaimanakah pendekatan intervensi yg
akan dilakukan o/ perawat?

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 25/90
Case 2
Tn. G, 74 th
Keluhan: otot nyeri, dizziness, constipation.
Uncooperative, marah >>.
Istri meninggal 2 th lalu; jatuh
8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 26/90

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 27/90
Kriteria Diagnostik DSM-IV
5 > gejala yg berlangsung >2 mgg, terjadi
perubahan:
Depressed mood dan atau kehilangan
perhatian/ketertarikan
<< tidur, << energi, tdk nafsu makan/BB <<,
rasa tidak berdaya/bersalah, perubahan
psikomotor, << konsentrasi dan fokus, pikiranbunuh diri

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 28/90
SIG E CAPS
Sleep
Interest
Guilt (“Are you a burden to others?”)
Energy
Concentration
Appetite
Psychomotor changes
Suicidality (“Do you wish you could die?”)
8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 29/90
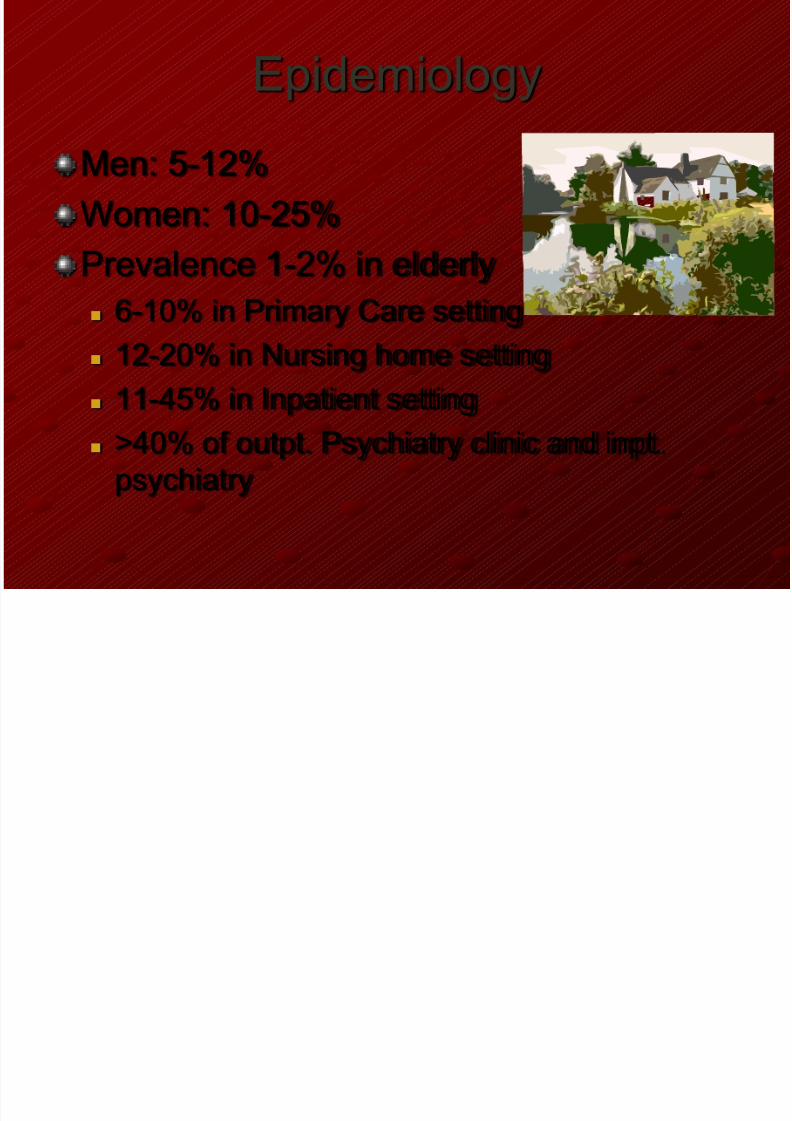
Epidemiology
Men: 5-12%
Women: 10-25%
Prevalence 1-2% in elderly 6-10% in Primary Care setting
12-20% in Nursing home setting
11-45% in Inpatient setting
>40% of outpt. Psychiatry clinic and inpt.
psychiatry

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 30/90
Diagnosis is Difficult
Coexistence of manyother problems
medical
physical social
economic
“normal” aging May “mask”
depression
8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 31/90
TRUE FALSE

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 32/90

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 33/90
Indirect Suicide
Starvation, refusingto eat
Refusing needed
medicationsMixing medications
Alcohol abuse
Loss of “will to live”

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 34/90
Poor Outcomes
Comorbid Conditions Anxiety
Medical problems
Cognitive impairmentConcurrent Problems & Issues
Psychotic depression
Impaired social supportStressful life events
Multiple previous episodes

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 35/90
Major Depression
Depressed mood most of the day,
everyday
ORLoss of interest or pleasure nearly every
day
and at least 4 additional symptoms . . .

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 36/90
Major Depression, cont.
Significant weight lossor gain
Insomnia orhypersomnia
Psychomotoragitation orretardation
Fatigue or loss ofenergy
Feelings ofworthlessness,inappropriate guilt
Loss of ability to think,concentrate, makedecisions
Recurrent thoughts ofdeath, suicidalideation
FOUR ADDITIONAL SYMPTOMS
8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 37/90
MINOR Depression
Also known as subsyndromal
depression
subclinical
depression mild depression
2 - 4 times more
common than major
depression
Associated with: subsequent major
depression
greater use of health
services reduced physical,
social functioning
loss of quality of life
Responds to sametreatments!

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 38/90
Common Causes of Depression
CHAIN OF EVENTS
Stress & loss
Biological depressionPhysical illness and
its treatment interact
with depression in older adults

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 39/90
Stress and Loss in Late Life
Decreased sensorycapacity
vision
hearing
Changes in socialstatus, responsibility
to others
Loss of family,friends
Relocation due tochanging abilities
Declining social
contacts due to
health limitations
Reduced functional
status
Dwindling financialresources

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 40/90
Stress and Loss in Late LifeLoss of meaningful
roles
productivity
purpose in living
Loss of self-esteem helplessness
powerlessness
Decreased coping
options
8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 41/90
Biological Depression
Genetic cause vs. “reaction” to stress
seems to come out of “nowhere”
family, personal history more common
increased risk of severity, reoccurrence
Effects of environment and physicalillness are still important to
address!!
8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 42/90
8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 43/90
Physical Illness & Depression
Physical illness can cause a reaction ofdepression by causing
chronic pain,
fear of pain
disability, loss of
function
loss of self esteem
increased dependence fear of death
2
8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 44/90
Physical Illness & Depression
Depressed elderly may present withsomatic (physical) complaints
aches, pains
appetite, weight fatigue, loss of energy
constipation
tachycardia insomnia
3

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 45/90

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 46/90

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 47/90
AssessmentDepression symptoms
Suicidal thoughts
Psychiatric history
personal
family
Physical health/illness
Medications
Recent loss/stressResources/abilities

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 48/90
Geriatric Depression Scale
Score “0” or “1”
Add up points (0-30)
Further assessment if
> 10Remember!
Screening tool;
assess symptoms
further!!

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 49/90
Suicide AssessmentAlways ASK!!!
“Have you thought that life isn’t worth living?”
If YES, then . . .
“Have you thought about harming yourself?
If YES, then . . .
“Do you have a plan?”
If YES, examine lethality. . .
Is the plan viable? Can they execute it?
Are means deadly, available?

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 50/90
Look
carefully!!
Psychiatric HistoryPrevious episodes of
depression Check chart/record
Undiagnosed
Bad nerves; nervous
breakdown; went to
bed sick
After childbirth, (post-
partum), children leave
(empty nest), death ofloved one, retirement
8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 51/90
Physical Health/Illness
Consider factors that increase isolation,loneliness, fear, orworthlessness!! Loss of mobility
Level of disability
Worry about decliningabilities
Pain resulting fromhealth conditions
Look for factors that directly increasedepression symptoms Medications
New?
Change in dose?
New onset of physicalillness
Influenza? Change in status of
chronic diseases

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 52/90
Recent Loss
___ recent relocation? ___ change in relationships?
___ change in health?
___ change in functional abilities? ___ change in sensory status?
___ change in financial status?
___ death of loved one? (even a pet)
___ loss of control over daily routines?
___ loss of significant role?

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 53/90
Resources & Abilities
___ family support? ___ community support?
___ social network?
___ physical abilities? ___ functional abilities?
___ cognitive abilities?
___ financial resources?
___ personality traits? personal history?
___ experiences, beliefs, convictions?

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 54/90
Person-Centered
Appreciate the older person‟sperspective and experience:
control, power loss
unwanted dependency
meaning of functional
losses, relationship
to activity, meaningand purpose in living
Facility,
Staff

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 55/90

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 56/90
Interventions
Every interaction has“Therapeutic Potential”
Social environment
or “milieu” is powerful Support, encouragement
Safety, security
Interaction, involvement
Validate worth by the way we treat them!

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 57/90
Interventions
First-Line Interventions
Communicate caring
Help see they are
unusually sad or blue
Provide accurate
information about depression
Create a healthy physical and socialenvironment.

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 58/90

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 59/90
Interventions
Help to realize they are
UNUSUALLY sad, blue
Suggest: more than "down in the dumps"
Help: identify the things that are troubling
Recall: past positive events things haven't
always been this bad
Note: Positive attributes, characteristics they do still have worth!!

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 60/90
Interventions
Provide informationabout DEPRESSION
An ILLNESS, like physical illness
Symptoms are part of depression Common in people of all ages
Has a treatment AND treatment worksMedications
Talking therapies
Increased involvement in activities

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 61/90
Promote Mental Health
Reduce “depressing effects” of the environment
Adjust factors in the social
environment Promote health & well-being
Alter approaches to care
Offer different activities/experiences
Promote positive health outcomes!!

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 62/90
Monitor Physical Health
Nutrition
Elimination
Sleep/rest patterns
Physical comfort
Pain management
relaxation methods
medication alternative therapies
8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 63/90
Encourage Physical ActivityExercise program
Referrals
physical therapy
occupational therapy
recreational therapyDevelop daily
activity schedule
Involve in
meaningful activity

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 64/90

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 65/90
Focus on PositiveCurrent abilities
knowledge, wisdom
experiences
attitudes, beliefs
attributes
Reminiscence
promotes self worth
strengthens tie to
identify, “former self” stimulates interests,
conversation

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 66/90
Employ Alternative Therapies
Pet therapy unconditional positive
regard
sensory stimulation
sense of responsibility,meaningful role
aroma therapy
maintain mobility

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 67/90
Encourage Group Activities
Psychosocial therapies
Reminiscence
Remotivation
Health, stress management
Sensory stimulation
Many benefits
Social interaction
Mastery experiences
Realization “I am not alone in this!

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 68/90
Promote Creativity
Lots of alternatives:
Singing, playing music
Story-telling
Drawing, painting
Poetry, writing
Making crafts, jewelry
Associated with positive health outcomes Decreased depression, loneliness
Increased health, morale, satisfaction, activity

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 69/90
Enhance Social Support
Identify a “point person” to
help identify, mobilize
resources
family member friend, neighbor
church members
clergy
volunteer visitor peer counselor
8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 70/90
Professional Interventions
Individual therapy
Group therapy
Medication therapy
Antidepressants
– most common
Others may be needed
for anxiety or psychotic symptoms
Depression

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 71/90
Depression
A
REASONFOR
HOPE

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 72/90
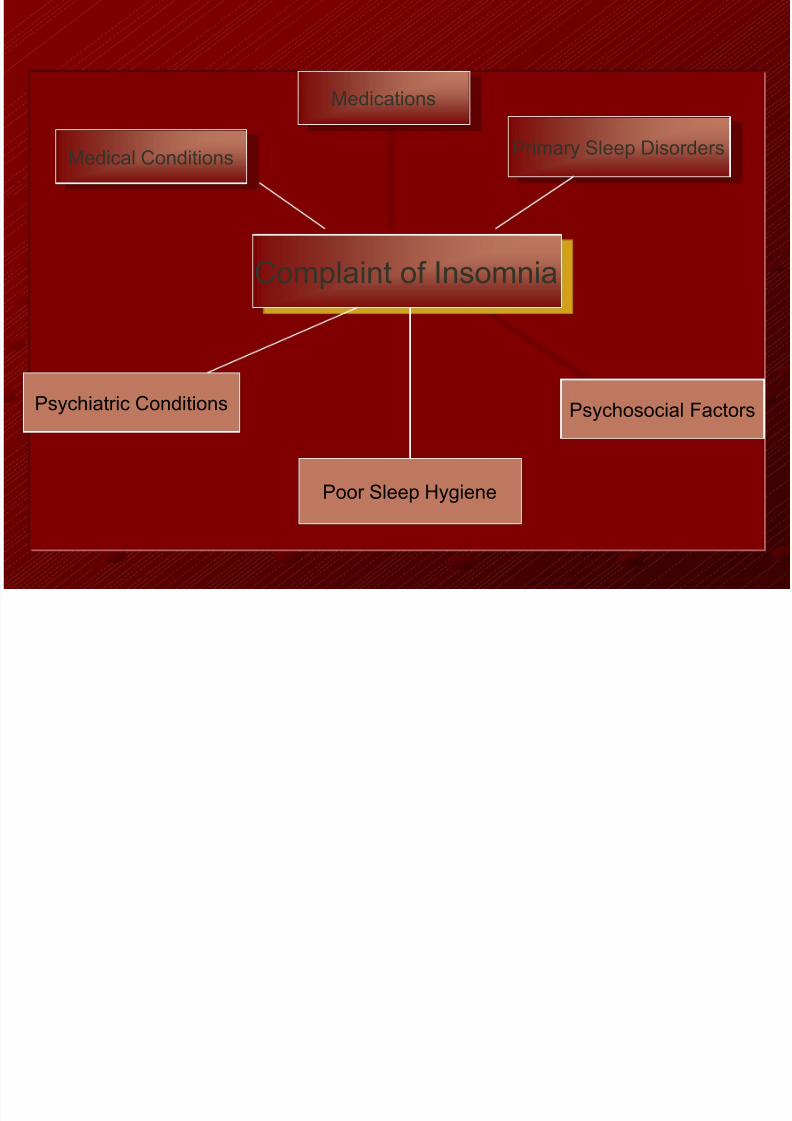
Sleep Disturbances-Incidence increase with aging
-Difficulty sleeping, Daytime drowsiness & Daytime napping
-Causes:
*medical conditions.
*Environment.*Medications.
*Normal changes associated with aging .
8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 73/90
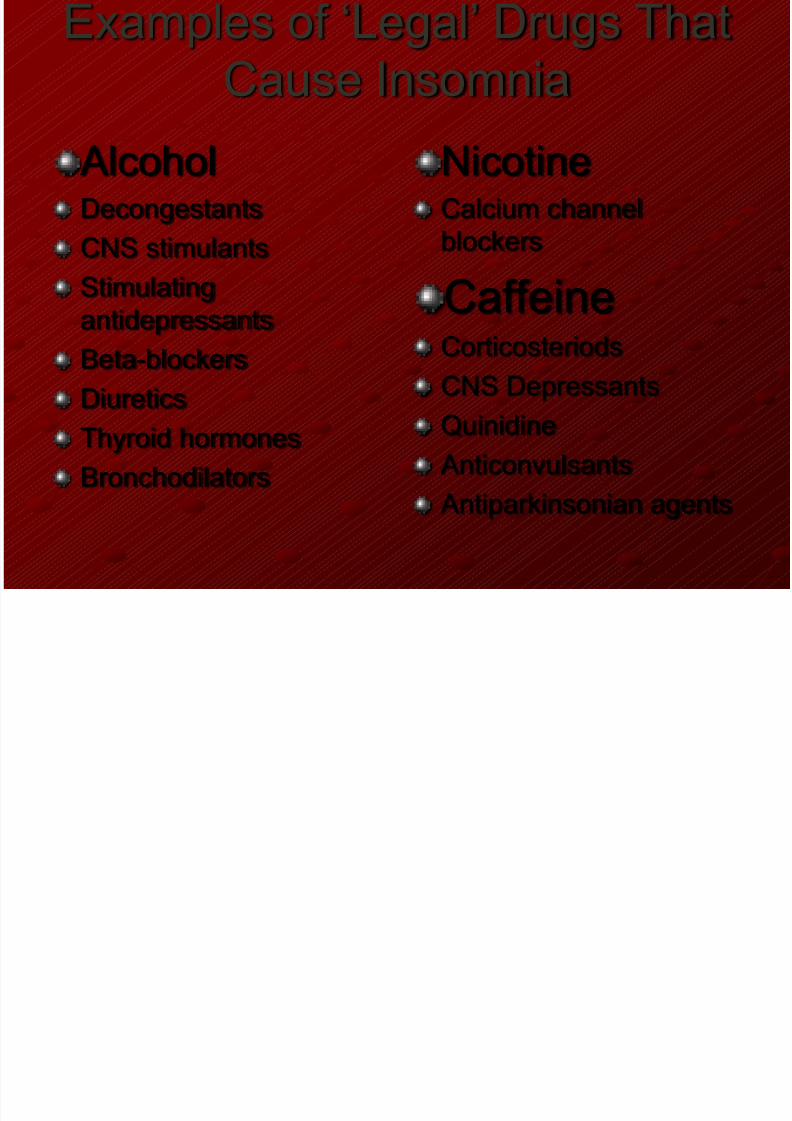
Examples of „Legal‟ Drugs That
8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 74/90
p g gCause Insomnia
AlcoholDecongestants
CNS stimulants
Stimulatingantidepressants
Beta-blockers
Diuretics
Thyroid hormones
Bronchodilators
NicotineCalcium channel
blockers
CaffeineCorticosteriods
CNS Depressants
Quinidine Anticonvulsants
Antiparkinsonian agents
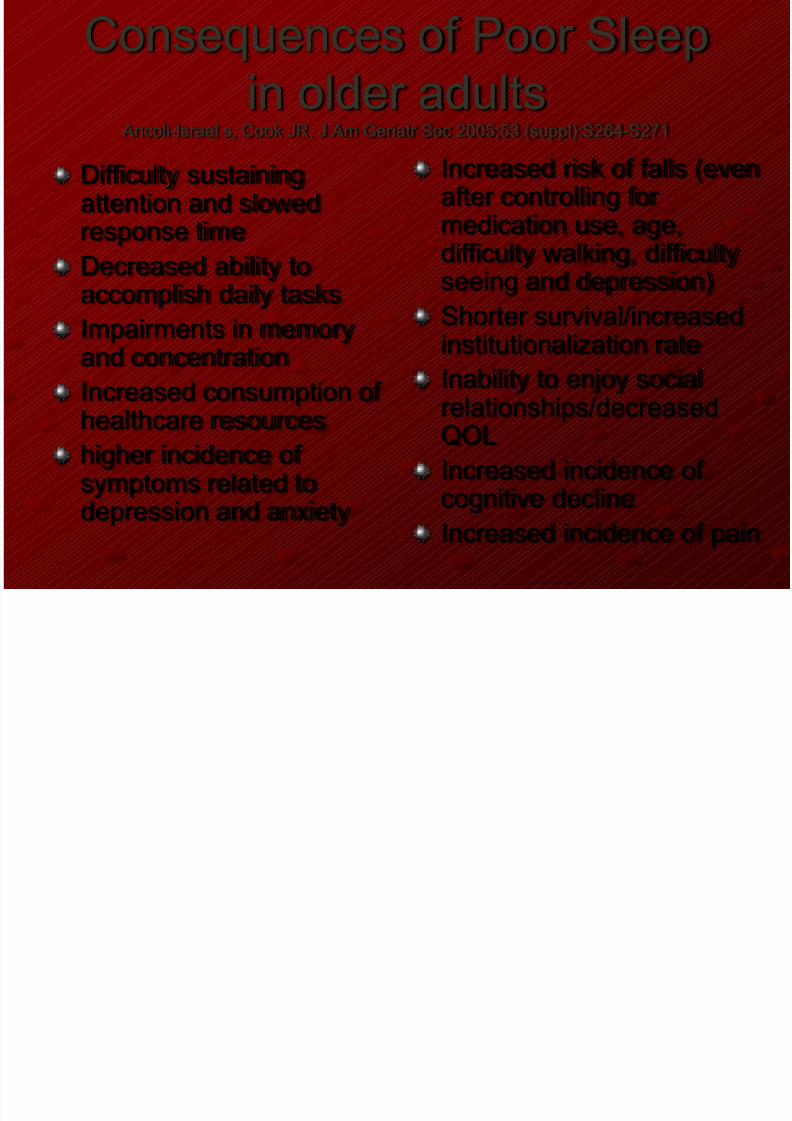
Consequences of Poor Sleep
8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 75/90
q p
in older adults Ancoli-Israel s, Cook JR. J Am Geriatr Soc 2005;53 (suppl):S264-S271
Difficulty sustainingattention and slowedresponse time
Decreased ability to
accomplish daily tasksImpairments in memoryand concentration
Increased consumption of
healthcare resourceshigher incidence ofsymptoms related todepression and anxiety
Increased risk of falls (evenafter controlling formedication use, age,difficulty walking, difficulty
seeing and depression)Shorter survival/increasedinstitutionalization rate
Inability to enjoy socialrelationships/decreasedQOL
Increased incidence ofcognitive decline
Increased incidence of pain

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 76/90
Tx of Sleep Disturbances-Approaches should be tried first: Alcohol cessation, Increased structure of daily routine, Elimination of
daytime naps & treatment of underlying medical conditions
-Sedative HypnoticsHydroxyzine (Vistaril) & Zolpidem (Ambien)
Important Note prefer not to be used due to their S/E in elderly likememory impairment, ataxia, paradoxical excitement & reboundinsomnia
8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 77/90
CaseNy. S, 69 th tinggal di rumah dg suaminya 72 th yg pensiun, dan2 anaknya laki2 yg telah menikah. Suaminya punya toko baju,dan skrg dijalani oleh anak2nya. Ny. S adalah IRT, lulusan S1.
Bbrp thn setelah anaknya menikah, mereka minta sharing dantokonya, dan skrg mereka hidup terpisah di rumah yg sama,tmasuk masak. Ny. S masak sndr u/ dia dan suaminya, dan punyapembantu u/ bersih2. Namun skrg, anak2nya suka teriak,marah2 dan mengancam akan mengeluarkan mereka dr rumah .Sementara istri mereka pura2 tdk tahu. Ny. S berpikir ini mgknhasutan dr istri2nya. Ny. S merasa tdk berdaya dan tdk punyakekuatan u/ melawan. Selama ini Ny.S hidup dgn uang pensiundan anak2nya tdk pernah memberikan uang.

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 78/90

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 79/90
Eld Ab

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 80/90
Elder Abuse
Elder abuse is physical or psychologicmistreatment, neglect, or financialexploitation of the elderly.
Common types of elder abuse include
physical abuse, psychologic abuse,neglect, and financial abuse. Eachtype may be intentional or unintentional.The perpetrators are usually a spouseor adult children but may be otherfamily members or paid or informalcaregivers. Abuse usually becomes
more frequent and severe over time.
8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 81/90
Physical abuse is use of force resulting in physical orpsychologic injury or discomfort. It includes striking, shoving,shaking, beating, restraining, and forceful or improper feeding.It may include sexual assault (any form of sexual intimacy
without consent or by force or threat of force).Psychologic abuse is use of words, acts, or other means tocause emotional stress or anguish. It includes issuing threats(eg, of institutionalization), insults, and harsh commands, as
well as remaining silent and ignoring the person. It alsoincludes infantilization (a patronizing form of ageism in whichthe perpetrator treats the elderly person as a child), whichencourages the elderly person to become dependent on theperpetrator.

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 82/90
Neglect is the failure to provide food, medicine,personal care, or other necessities. Neglect thatresults in physical or psychologic harm is consideredabuse.
Financial abuse is exploitation of or inattention to a
person's possessions or funds. It includes swindling,pressuring a person to distribute assets, andmanaging a person's money irresponsibly.
Risk Factors for Elder Abuse

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 83/90
Factor Comments
For the victim
Social isolation Abuse of isolated people is less likely to bedetected and stopped. Social isolation can
intensify stress.
A chronic disorder,
functional impairment,or both
The ability to escape, seek help, and
defend self is reduced.Such elderly people may require more
care, increasing stress for the caregiver.
Cognitive impairment Risk of financial abuse and neglect is
particularly high.
People with dementia may be difficult to
care for, frustrating caregivers, and may be
aggressive and disruptive, precipitating
abuse by overwhelmed caregivers.
For the perpetratorSubstance abuse Alcohol or drug abuse, intoxication, or substance withdrawal may
lead to abusive behavior Substance dependent caregivers may

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 84/90
lead to abusive behavior. Substance-dependent caregivers may
attempt to use or sell drugs prescribed to the elderly person,
depriving the person of treatment.
Psychiatric disorders Psychiatric disorders (eg, schizophrenia, other psychoses) may
lead to abusive behavior.Patients discharged from an inpatient psychiatric institution may
return to their elderly parents' home for care. These patients,
even if not violent in the institution, may become violent at home.
History of violence A history of violence in a relationship (particularly between
spouses) and outside the family may predict elder abuse. One
theory is that violence is a learned response to difficult life
experiences and a learned method of expressing anger and
frustration. Because reliable information about past family
violence is difficult to obtain, this theory is unsubstantiated.
Dependence of the
perpetrator on theelderly person
Dependence on the elderly person for financial support, housing,
emotional support, and other needs can cause resentment,contributing to abuse. If the elderly person refuses to provide
resources to a family member (especially an adult child), abuse is
more likely.
Stress Stressful life events (eg, chronic financial problems, death in the
family) and the responsibilities of caregiving increase the
likelihood of abuse.

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 85/90
For both victim and perpetrator
Shared livingarrangements Elderly people living alone aremuch less likely to be abused.
When living arrangements are
shared, opportunities for the
tension and conflict that usuallyprecede abuse are greater.
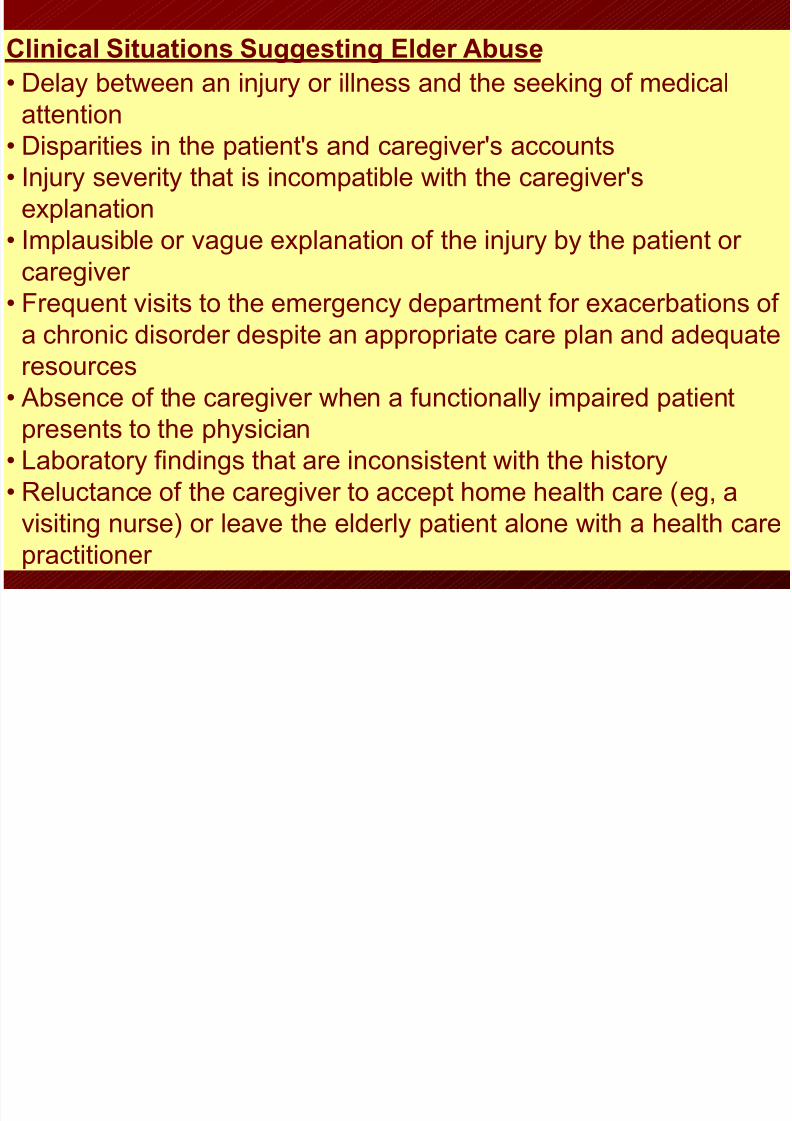
Clinical Situations Suggesting Elder Abuse
8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 86/90
gg g
• Delay between an injury or illness and the seeking of medical
attention
• Disparities in the patient's and caregiver's accounts• Injury severity that is incompatible with the caregiver's
explanation
• Implausible or vague explanation of the injury by the patient or
caregiver
• Frequent visits to the emergency department for exacerbations of
a chronic disorder despite an appropriate care plan and adequate
resources
• Absence of the caregiver when a functionally impaired patient
presents to the physician• Laboratory findings that are inconsistent with the history
• Reluctance of the caregiver to accept home health care (eg, a
visiting nurse) or leave the elderly patient alone with a health care
practitioner
8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 87/90

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 88/90
Preventing elder abuse and neglect
Listening to seniors and their caregivers
Intervening when you suspect elder abuse
Educating others about how to recognize andreport elder abuse
Latihan Kesadaran Diri: Intensitas marah Bayangkan situasi ini:

8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 89/90
y g
Anda pulang telat setelah belajar di perpustakaan untuk ujian semester
dan Anda merasa lelah. Saat berjalan ke rumah, tanpa disadari seorang
anak remaja yang mengendarai sepeda motor menabrak Anda. Seperti apakah emosi yang anda rasakan saat itu? Hal apa sajakah yang
mempengaruhi intensitas marah yang anda rasakan?
- Rasa nyeri yang anda rasakan saat tertabrak?
- Keadaan tubuh anda yang lelah? - Kenyataan bahwa anda belum sempat makan malam?
- Seorang anak remaja yang tidak sengaja menabrak anda?
- Rasa stres akan menghadapi ujian?
Jika situasi yang sama terjadi pada saat tubuh anda tidak lelah, dalamkeadaan tenang, tidak mengalami beban pikiran, apakah perasaan dan
intensitas marahnya akan sama?
8/12/2019 5. psikogeroB11
http://slidepdf.com/reader/full/5-psikogerob11 90/90
―We need to meet all kinds of people so that we
can find ourselves. Young people need olderpeople just as older people need young people in
order to become more themselves and more
human. That humanizing process will teach usthat there is a child behind the mask of each
older face, just as there is already an older
person behind the mask of each young face.‖
– Leo. E. Missinne (1990)






![Rachmaninov 3rd Piano Concerto [First Movement] · PDF file53-g e5 = 5 !5 = 5 5 5 5 5 4 5 5 =5 5 = 5e5 5 5 5 5 5 5 5e5 5 5!55 5 5 5 5 5e5 5 5 5 5 5 5! 5 $3e55 5 5: 5 5 5 55 5e 55 5](https://img.dokumen.tips/doc/110x75/5a78944a7f8b9a1f128d15db/rachmaninov-3rd-piano-concerto-first-movement-53-g-e5-5-5-5-5-5-5-5-4-5.jpg)



![[XLS] · Web view4.95. 4.95. 5. 5. 5. 5. 5. 5. 4.95. 5. 5. 4.95. 4.95. 5. 4.95. 5. 5. 4.95. 4.95. 5. 5. 5. 5. 5. 5. 4.95. 5. 4.95. 4.95. 4.95. 4.95. 5. 5. 4.95. 4.95. 5. 5. 4.95](https://img.dokumen.tips/doc/110x75/5ba3371b09d3f2cc2e8da3f6/xls-web-view495-495-5-5-5-5-5-5-495-5-5-495-495-5-495.jpg)

















