Embed Size (px)
Citation preview

Lumbar Disk Herniation

35 and 45 years age
Risk factor – Smoking sedentary work motor vehicle driving
Sciatica, characterized by pain radiating down the leg in
Pathophysiology
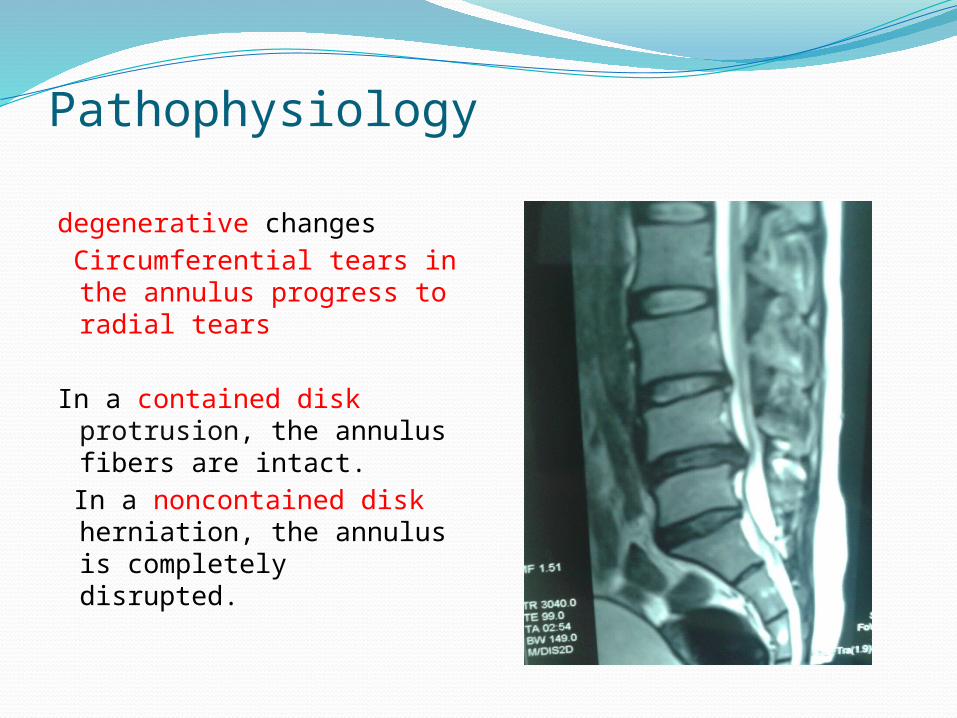
degenerative changes Circumferential tears in
the annulus progress to radial tears
In a contained disk protrusion, the annulus fibers are intact.
In a noncontained disk herniation, the annulus is completely disrupted.
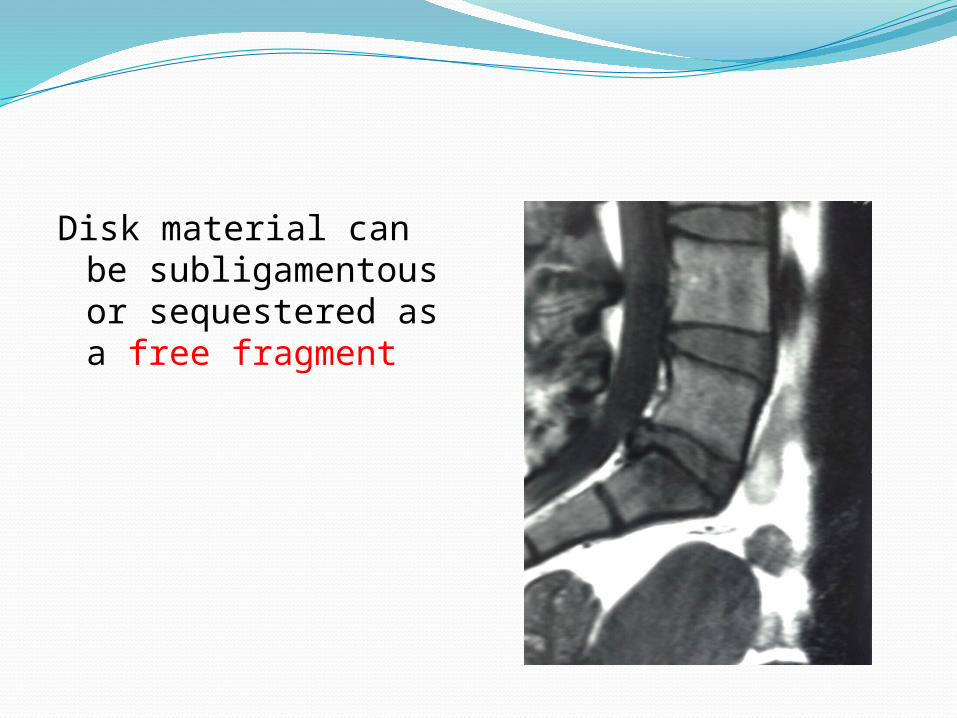
Disk material can be subligamentous or sequestered as a free fragment

Cause of pain;direct pressure on the nerve root breakdown products from a degenerated
nucleus pulposus autoimmune reaction
hydration of the disk;90% during childhood 70% by the sixth decade

Clinical FindingsSymptoms and Signs
The typical sciatica is commonly preceded by back pain for a period of days or weeks.
compression of nerve fibers in the outer layers of the annulus
rupture of the disk material into the spinal canal

dominating symptom is pain, patients often present with a sciatic list

The mobility of the lumbar spine is diminished more in flexion than in extension

Coughing, sneezing, or a voluntary Valsalva maneuver commonly aggravates the radiating pain.
90% at L4-L5
Paracentral disk herniations typically affect the traversing nerve root at the affected level, whereas lateral and foraminal herniations affect the exiting nerve root at the above level.
Disc at L3-L4
pain and numbness in the L4 dermatome
Quadriceps Weakness
patella tendon reflex -depressed or absent

Disc at L4-L5
Numbness - L5 dermatome weakness of the foot and toe dorsiflexors.

Disc at L5-S1
numbness or pain in the S1 dermatomeweak plantarflexion of the footloss of the Achilles tendon reflex

straight leg–raising test Pain in leg on elevationpositive in 98%
cross-Lasègue sign (pain radiating to the affected leg when the contralateral leg is elevated) is positive in 20%.
For lesions involving the L3 or L4 nerve root, the
femoral nerve stretch test should be applied.

Imaging Studies
MRI is the study of choice for diagnosis of a herniated disk.
Because 28% of asymptomatic patients show a disk herniation on MRI, it is important to correlate the level of spinal involvement with the peripheral nerve deficit.

disk extrusion at the L5/S1 disk level

Grading system for the assessment of lumbar disc degeneration. Sagittal T2-weighted images show the different degrees of disk degeneration

sequestrateddisk at the L3/4
level

Diskogram showing posterior annular
defect at L4-5
Differential Diagnosisrenal disease or a tumor of the uterus or bladder
Hip disorders, including trochanteric bursitis and coxarthrosis, must be ruled out.
The presence of incontinence, perianal numbness, and bilateral leg pain associated with numbness suggests a cauda equina syndrome and requires immediate surgical attention.
Treatment
goal of treatment is to return the patient to normal activities as quickly as possible
Unnecessary surgery should be avoided

Conservative Treatment
Two days of bed rest followed by a good physical therapy significant alleviation of symptoms within 2 or 3 weeks
Analgesics and nonsteroidal
epidural corticosteroids is successful in decreasing the acute sciatic pain

Surgical TreatmentApproximately 10% of patients with lumbar
disk herniation ultimately require surgery.
Surgery is recommended if the sciatica is severe and disabling and tension signs are positive, if symptoms persist without improvement for longer than 1 month, or consistent with nerve root compromise.
When a standard diskectomy is used, the overall success rate is 85%, and 95% of the patients with successful surgery return to work.
Microdiskectomy minimizes the dissection and has an equally high success rate.
Newer techniques using muscle-splitting approaches and small tubular retractors require even less soft-tissue violation than microdiskectomy.
Postoperative discomfort is minimized and speed of recovery is maximized.
Risks of surgery include dural tear, wrong-level exploration, hemorrhage, infection, and nerve deficit.

In cases of contained disk protrusion, percutaneous automated diskectomy or chemonucleolysis may be considered.