Embed Size (px)
Citation preview

(see figure 9) may be focal or widely distributed throughout the renal parenchyma.
CT abdomen is the gold stand-ard for diagnosis and may be valu-able in differentiating between this condition and others, for example, a renal cell carcinoma. Manage-ment options include a conservative approach or surgical intervention based on the patient’s individual condition. Antimicrobial therapy is always required.
PROGNOSISMOST PATIENTS can be managed as outpatients, despite the significant morbidity and mortality associated with acute pyelonephritis. A recent study in Hong Kong reported a mor-tality of 7.4% and that male gender, age over 65, impaired renal func-tion or the presence of disseminated intravascular coagulation was asso-ciated with a higher mortality.1 This study emphasises the significant impact of pyelonephritis, which is compounded if there is not appropri-ate and prompt management.
THE FUTUREAS ANTIMICROBIAL use becomes more widespread in the commu-nity, we are seeing increasing num-bers of resistant organisms. Further research is required to assess local and regional resistance patterns, which will facilitate prompt diagno-ses and the use of appropriate anti-microbial therapy.
A recent systematic review in the UK assessed the clinical efficacy and safety of IV antibiotics. The authors concluded there was a need for high-quality clinical trials into the oral antibiotic treatment of pyelone-phritis, with more consistent designs and reporting of outcomes.14
A SA study investigated the link between increasing temperatures and renal conditions.
They concluded that due to cli-mate change, an increased frequency of renal disease, including urolithia-sis, acute kidney injury and urinary tract infections is predicted.19 This is a potential area for further research.
CASE STUDIESCase study one RITA, 26, presents to her GP with a three-day history of dysuria and uri-nary frequency. This is the second episode of these symptoms in the past three weeks. Rita was woken that morning by right-sided flank pain, which is causing her some con-cern. She noted marked sweating overnight and anorexia since lunch-time the previous day.
She has no significant past medi-cal history, family history of kidney disease or regular medications. Rita is a non-smoker and denies any alco-hol consumption.
She is sexually active and has an IUD in place. Her last menstruation was four weeks ago and her cycle is regular. Her only allergy is to bees.
On examination, Rita has a HR of 80, BP 118/74, saturation of 99% and temperature of 37.6°C. Her abdomen is soft with mild tenderness of the right renal angle and right flank, and no signs of peritonism.
The rest of the examination is unremarkable.
Urine dipstick is positive for leukocytes and nitrites only. This sample is sent for formal urine microscopy and culture STI
31 MAY 2019 ausdoc.com.au22 HOW TO TREAT: PYELONEPHRITIS
PAGE 24
No
No
No
Yes
Yes
Yes
Yes
Yes
No
No
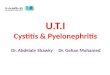
Acute pyelonephritis
Indication for initial genitourninary imaging?New eGFR decrease to ≤40mL per minuteKnown or suspected urolithiasisUrine pH≥7.0
Clinical indication for immediate hospital admission?Sepsis or septic shockFragile conditionImmunocompromiseUnstable or severe coexisting conditionsTenuous psychosocial situationNo suitable oral antibiotic option
Imaging shows need for drainage procedure?
Indication for ED or observation unit stay?Clinically significant hypovolemiaModerately illNausea or vomiting
Treat initially in ED or observation unitIV antibioticsFluidsMedications for symptom relief
Admit to hospitalDrainage, if indicated by imagingIV antibioticsIV fluidsICU, if sepsis or septic shock is presentMedications for symptom relief
Discharge to home with oral antibiotic(with or without initial supplemental dose of suitable long-acting, broad-spectrum agent)
Persisting indication for admission after ED or observation unit stay?Ongoing nausea or vomitingOngoing need for hydrationOngoing hemodynamic instabilityPatient too ill or unwilling to go home
Figure 7. Suggested management of acute pyelonephritis in adults.
SOU
RCE: 13
Figure 8. Bilateral emphysematous pyelonephritis evidence on CT abdomen .
HTT_017_024_31MAY19.indd 22 5/22/19 11:34 AM










![Suresh K. Bhavnani*, Bryant Dang, Varun Kilaru, Maria … account for approximately 70% of infant mor-tality and morbidity resulting in high personal and finan-cial costs [1]. For](https://img.dokumen.tips/doc/110x75/5ab347ea7f8b9abc2f8e82ea/suresh-k-bhavnani-bryant-dang-varun-kilaru-maria-account-for-approximately.jpg)




![a arXiv:1612.08012v2 [cs.CV] 5 Jan 2017 · computed tomography (CT) reduced lung cancer mor-tality after 7 years by 20% in comparison to screening with chest radiography (Aberle et](https://img.dokumen.tips/doc/110x75/601c88b2327db6329c4c6020/a-arxiv161208012v2-cscv-5-jan-2017-computed-tomography-ct-reduced-lung-cancer.jpg)