-
8/2/2019 Pyelonephritis (Final Case)
1/59
PYELONEPHRITISGROUP 1
-
8/2/2019 Pyelonephritis (Final Case)
2/59
I. INTRODUCTION
The diagnosis of a urinary tract infection (UTI) istypically
confirmed on the basis of a certain numberof microorganisms in the
urinary system, althoughmanifestation may begin with many fewer
organisms. The infectious process usually affectsthe bladder,
but the uretrhra, ureters, and kidneymay be involved.
-
8/2/2019 Pyelonephritis (Final Case)
3/59
Urinary tract infection (UTI) is one of the mostcommon infection
treated by primary careproviders, untreated, it has the potential
for seriousconsequence, such as pyelonephritis and
bacteremia. On rare occasions, complication of UTIcan lead
death. Cystisis is the most common typesof UTI.
-
8/2/2019 Pyelonephritis (Final Case)
4/59
DEFINITION:
CYSTITIS
Inflammation of the urinary bladder
s/sx:
Pressure in lower pelvis Painful urination (dysuria)
Frequent urination(polyuria)
Abnormal urine color(cloudy)
Foul odor of urine
-
8/2/2019 Pyelonephritis (Final Case)
5/59
-URETHRITIS
inflammation of the urethra.
s/sx:
Dysuria
Painful urination
-URETERITIS
Inflammation of the ureter.
s/sx:
Renal colic
Fever
Blood in the urine
-
8/2/2019 Pyelonephritis (Final Case)
6/59
PYELONEPHRITIS
Inflammation of renalpelvis.
s/sx:
Acutely ill with chills andfever
High fever and chills
Leukocytosis
Bacteriuria
Dysuria
Flank pain
CVA tenderness
Nausea
Foul smelling urine
-
8/2/2019 Pyelonephritis (Final Case)
7/59
CAUSES:
Pyelonephritis is caused by Escherichia coli this isa type of
bacteria that normally in the largeintestine. However, any physical
obstruction to theflow of urine, such as structural
abnormality,
bladder tumor, strictures, kidney stone or anenlarged prostrate
or backflow (reflux) of urine fromthe bladder into the ureters may
causepyelonephritis
-
8/2/2019 Pyelonephritis (Final Case)
8/59
PREVALENCE RATE:
EPIDEMIOLOGY:
-Pyelonephritis is very common, with 12-13 casesannually per
10,000 populations in women and 3-4cases per 10,000 in men. Young
women are mostlikely to be affected, traditionally affecting
sexualactivity in that age group. Infants and the elderly arealso
at increase risk, reflecting anatomical changesand hormonal
status.
-
8/2/2019 Pyelonephritis (Final Case)
9/59
6 years of age;
Boys: 1.8% Girls: 6.6%
5-7% Female febrile infant (8 weeks of age)
1% School-age children 1-3% Girl between 1-5 years of age
0.003% School age boys
-
8/2/2019 Pyelonephritis (Final Case)
10/59
DIAGNOSIS:
The presence of nitrite and leukocyte (white bloodcell) on a
urine dipstick test in patients with typicalsymptoms are sufficient
for the diagnosis ofpyelonephritis, and are an indication for
empirical
treatment. Formal diagnosis is with culture of theurine blood
cultures may be needed if the source ofthe infection is initially
doubtful.
-
8/2/2019 Pyelonephritis (Final Case)
11/59
II.NURSING HISTORY
PATIENTS PROFILE
Name: Ms. Yuri
Age:21
Sex: Female
Address: P2 Dubinan west Santiago city Nationality: Filipino
Civil status: Single
Religion: Roman Catholic
Occupation: Office secretary
Date admitted: 3/4/2011 Time admitted: 8:10am
Admitting diagnosis: UTI, Pyelonephritis
Chief complaint: Right lower quadrant and radiatingflank pain
since Saturday February 26, 2011.
-
8/2/2019 Pyelonephritis (Final Case)
12/59
B. HISTORY OF PRESENT ILLNESS
The day PTA, the patient complained of back painand couldnt
stand alone because she felt dizzy andradiating flank pain in night
lower quadrant of theabdomen and general also complaining for
body
malaise and painful urination.
-
8/2/2019 Pyelonephritis (Final Case)
13/59
PAST MEDICAL HISTORY
The patient has been hospitalized when shewas in 4th yr. high
school due to bronchitis
FAMILY HISTORYThe patient verbalized that her father had
also
suffered urinary tract infection.
-
8/2/2019 Pyelonephritis (Final Case)
14/59
E. GORDONS FUNCTIONAL PATTERN
HEALTH PERCEPTION
BEFORE CONFINEMENT:
-The patient stated that she consider herself healthybecause she
cannot feel something unusual.
DURING CONFINEMENT:-She stated that shes already unhealthy
because she can
feel pain
NUTRITION
BEFORE CONFINEMENT:
-The patient seldom drink water and sometimes not at all.Shes
also fun in eating sweets and salty foods.
DURING CONFINEMENT:
-On her first day of confinement the ROD ordered DAT.
-
8/2/2019 Pyelonephritis (Final Case)
15/59
ELIMINATION PATTERN
PRIOR CONFINEMENT
-The patient usually voids for 1-2 times a day. The color ofher
urine was dark yellow. However, 1 day PTA shecomplained of pain
upon urination in the pain scale 7
that causes her to void in small quantities. DURING
CONFINEMENT
-She voids 2-4 times a day in normal quantities and slightpain
upon urination
ACTIVITY
BEFORE CONFINEMENT:-The patient can go to work and stayed at the
office from
7-5 pm can do activity daily living.
DURING CONFINEMENT:
-The patient appears weak to go the bathroom.
-
8/2/2019 Pyelonephritis (Final Case)
16/59
SLEEP/REST PATTERN:
BEFORE CONFINEMENT:
-Her usual sleeping pattern was 6-8 hours daily.
DURING CONFINEMENT:-She is able to sleep 8-10 hours and an hour
of snaps
in the afternoon
COGNITIVE PERCEPTUAL PATTERN
-The patient can read and write and her sensesfunctions well.
The decision for the benefit of thepatient always comes from her.
However, at timesshe asks for assistance her family.
-
8/2/2019 Pyelonephritis (Final Case)
17/59
-
8/2/2019 Pyelonephritis (Final Case)
18/59
SEXUAL PATTERN:
-The client is single
COPING STRESS TOLERANCE
-She asks for assistance from her mother in terms of
making decision to avoid stress. She managed herproblem through
praying.
VALUES AND BELIEF PATTERNS
BEFORE CONFINEMENT:
-She said she attends Sunday masses regularly but herrecent
confinement hinders her practice.
DURING CONFINEMENT:
-During hospitalization, she prays to GOD to bless her andher
family with good health.
-
8/2/2019 Pyelonephritis (Final Case)
19/59
III.PHYSICAL EXAMINATION
March 4, 2011
General appearance:
The patient looks weak and irritable, complainingpain at the
right lower quadrant and radiating flank
pain, (+) guarding and facial grimace and palelooking with
excessive sweating.
Vital Sign:
BP: 100/70 mmHg
Temperature: 38.3 RR: 25 cpm
PR: 89 bpm
Parts Technique Abnormal Analysis
-
8/2/2019 Pyelonephritis (Final Case)
20/59
Parts Technique Abnormal Analysis
Hair
Head
Face
Eyes
Ears
Mouth
Neck
Lungs
Abdomen
Extremities
Upper: Nail
Skin
Lower: Nail
Skin
Inspection
Inspection
Inspection
Palpation
Inspection
Inspection
Palpation
Inspection
Inspection
Palpation
Inspection
Palpation
Percussion
AuscultationInspection
Palpation
Percussion
Auscultation
Inspection
Inspection
Palpation
Inspection
Palpation
Inspection
Palpation
Inspection
Palpation
Weak looking and facial
grimace
pale, and with eye bags
Dry mouth, pale, cracked and
dry lips.
Shivers
Pale
Dry
Pale
Pale
As body response to pain
Due to inadequate sleep
As body response to fever and
fluid loss of the body
Due to fever
Response of the body to
Inflammation
Due to fever
Response of the body to
inflammation
Due to fever
-
8/2/2019 Pyelonephritis (Final Case)
21/59
MARCH 5, 2011
General appearance: the patient looks pale andweak.
Vital sign: BP: 100/80mmHg
Temperature: 37.5
RR: 19 cpm
PR: 87 bpm
Parts Technique Abnormal Analysis
-
8/2/2019 Pyelonephritis (Final Case)
22/59
q y
Hair
Head
Face
Eyes
Ears
Mouth
Neck
Lungs
Abdomen
ExtremitiesUpper: Nail
Skin
Lower: Nail
Skin
Inspection
Inspection
Palpation
Inspection
Palpation
Inspection
Inspection
Palpation
Inspection
Inspection
Palpation
Inspection
Palpation
Percussion
Auscultation
Inspection
Palpation
Percussion
Auscultation
InspectionInspection
Palpation
Inspection
Palpation
Inspection
Palpation
Inspection
Palpation
Weak looking
Pale and with eye bags
Cracked and dry lips
Pale
Dry
Pale
Dry
Due to uncomfortable feeling
Due to inflammation andinadequate sleep
Due to fever and fluid loss of
the body
Response of the body toinflammation
Response of the body to
inflammation
-
8/2/2019 Pyelonephritis (Final Case)
23/59
IV.LABORATORY RESULTS
URANALYSIS NORMAL VALUES RESULTS ANALYSIS
COLOR Amber Dark yellow Urine becomes over
concentrated with waste that
makes urine dark yellow
TRANSPARENCY Clear Turbid The presence of bacteria,
increase WBC and RBC that
cause her urine turns to turbid
SPECIFIC GRAVITY 1.010 - 1.025 1.015
PH 4.5 8.0 Alkaline
PROTEIN 6 8 g/d (+) 2 Due to infection, medications,
and physical stress
SUGAR 65 99 mg/dl (-)
A. MARCH 4, 2011
-
8/2/2019 Pyelonephritis (Final Case)
24/59
URANALYSIS NORMAL VALUES RESULTS ANALYSIS
WBC 5000 10000/mm3 TNTC Due to her body response to
invasion, they provide
components of coagulation,
transportation and complement
production during acute
infection.
RBC 4.2 5.4 mil/mm3 12 15
AMORPHUS URATES Moderate
EPITHELIAL CELLS Moderate
BACTERIA Many Due to infection
-
8/2/2019 Pyelonephritis (Final Case)
25/59
HEMATOLOGIC REPORT
Complete Blood Count Normal Values Results
Hemoglobin 110 160 g/d 139
Hemotocrit 34-47 41.5
White Cell Count 5-10x10 9 23.6
Segmenters 50-65% 93
Lymphocytes 25-35% 4.2
Eosinophils 1-3%
2.8
Monocytes 3-7%
Platelet count 150-450 X 10 9 24
A. MARCH 4, 2011
-
8/2/2019 Pyelonephritis (Final Case)
26/59
V.REVIEW SYSTEM
-ANATOMY OF URINARY SYSTEM
The urinary system consist of two kidneys, twoureters, the
urinary bladder, and the urethra. A largevolume of blood flows
through the kidneys, which
removes substances from the blood to form urine.The urine
contains excess water and ion metabolicwastes such as urine and
toxic substancesconsumed with food. The urine produce by the
kidneys flows through the ureters to the urinarybladder, where
it is stored until it is eliminatedthrough the urethra.
-
8/2/2019 Pyelonephritis (Final Case)
27/59
FUNCTIONS OF THE URINARY SYSTEM
KIDNEYS:
The major functions of the urinary system areperformed by the
kidneys, and the kidneys play thefollowing essential roles in
controlling the
composition and volume of body fluids.
1. Excretion. The kidneys are the major excretoryorgans of the
body. They remove waste products,many of with are toxic from the
blood.
-
8/2/2019 Pyelonephritis (Final Case)
28/59
The kidneys control blood volume by regulating thevolume of
urine produced.
3. The kidneys help regulate the concentration ofmajor ions in
the body fluid.
4. The kidneys help regulate the pH of the fluids.
5. The kidneys regulate the concentration of redblood cell in
the blood.
6. The kidneys participate with the skin, and liver,invitamin D
synthyesis.
-
8/2/2019 Pyelonephritis (Final Case)
29/59
URINARY BLADDER is a hollow muscularcontainer that lies in the
pelvic cavity just posteriorto the pubic symphisis. It functions to
store urine,and its size depends on the quality of urine
present.
URETHRA is a tube that exist the urinary bladderinfection and
anteriorly the triangle-shape portion ofthe urinary bladder located
between the opening ofthe ureters and the opening of the urethra is
called
the trigone. The urethra carries urine from theurinary bladder
to the outside of the body.
-
8/2/2019 Pyelonephritis (Final Case)
30/59
KIDNEY are been shape organs, each about thesize of a tightly
clenched fist. They lie in theposterior abdominal wall, behind the
peritoneum,with one kidney on either side of the vertebral
column.
-
8/2/2019 Pyelonephritis (Final Case)
31/59
OUTER KIDNEY
Hilium (opening)-where the renal artery and nervesenter and
where the renal vein and ureter exit thekidney.
Renal artery-branch off the abdominal aorta and
abdominal aorta and enter the kidneys. They giverise to several
branches.
Renal vein-are veins that drain the kidney. Theycorrect the
kidney to the inferior vena cava.
-
8/2/2019 Pyelonephritis (Final Case)
32/59
Renal pelvis-is the funnel-like dilated proximal partof the
ureter in the kidney. In humans, the renalpelvis is the point of
convergence of two or threemajor calyces.
URETER-are muscular tubes that proper urine fromthe kidneys to
the urinary bladder.
-
8/2/2019 Pyelonephritis (Final Case)
33/59
INNER KIDNEY
Cortex-is the outer part of the substance or thekidney, composed
mainly of glomeruli andconvulated tubules.
Renal pyramid -the conical masses composing the
medullary substance of the kidney.
Major calyces -in the kidney, surrounds the apex ofthe
malphighian pyramids. Urine formed in thekidney passes through a
papilla at the apex into a
minor calyx then into the major calyx beforepassing through the
renal pelvis into the ureter. Afusion of minor calyx.
-
8/2/2019 Pyelonephritis (Final Case)
34/59
Renal artery-brach off the abdominal aorta andenter the
kidneys.
Minor calyces -the cup-shape dilation of theintrarenal ureter,
into which a single papilla of a
multiple-lobe kidney protrudes.
Nephron -is the basic structure and functional unitof the
kidney. Its chief function is to regulate theconcentration of water
and soluble substance like
sodium salts by filtering the blood, reabsorbed whatis needed
and excreting the rest of urine.
-
8/2/2019 Pyelonephritis (Final Case)
35/59
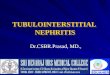
NORMAL KIDNEYS AND PARTS
-
8/2/2019 Pyelonephritis (Final Case)
36/59
-
8/2/2019 Pyelonephritis (Final Case)
37/59
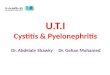
PYELONEPHRITIS
-
8/2/2019 Pyelonephritis (Final Case)
38/59
URINE FLOW Urine is produced by the processes of filtration,
reabsorption
and secretion.
FILTRATION
The renal filtrate passes from the glomerulus into Bowmans
capsule and contains no blood cells and few blood proteinsthen
filtration pressure is responsible for filtrate formation.
REABSORPTION
About 99% of the filtrate volume is reabsorbed, 1% becomesurine.
Proteins, amino acids, glucose, fructose, sodium,potassium, calcium
are among the substances reabsorbed.
About 65%of the filtrate volume is reabsorbed in the
proximaltubule and collecting ducts.
SECRETIONS
Hydrogen ions same by-products of metabolism, and somedrugs are
actively secreted into the nephron.
-
8/2/2019 Pyelonephritis (Final Case)
39/59
B. PATHOPHYSIOLOGY
PYELONEPHRITIS
Precipitatingfactor:
Immunocompromise patientLifestyleMisconceptionwith regard
toproper hygiene
care
Etiology:
Attachment ofEschericha colibacteria in the
urethra
Predisposing
factor:AgeGenderHealthproblem
-
8/2/2019 Pyelonephritis (Final Case)
40/59
B. PATHOPHYSIOLOGY
Proliferation of bacteria in the urethra
Urethritis
Urethrovesical reflux
-
8/2/2019 Pyelonephritis (Final Case)
41/59
-
8/2/2019 Pyelonephritis (Final Case)
42/59
B. PATHOPHYSIOLOGY
Introduction of bacteria to the Ureter
Inflammation of the Ureter
Ureteritis
-
8/2/2019 Pyelonephritis (Final Case)
43/59
B. PATHOPHYSIOLOGY
Infection ascends to the kidneys
Pyelonephritis
Activation of theimmune response
GeneralBody
Malaise
Nauseaandvomiting
Dysuria
Colic
-
8/2/2019 Pyelonephritis (Final Case)
44/59
B. PATHOPHYSIOLOGY
Release ofpyrogens from
bacteria
Release ofprostaglandins E2
Elevation of thebody thermostat bythe hypothalamus
Flankpain
-
8/2/2019 Pyelonephritis (Final Case)
45/59
B. PATHOPHYSIOLOGY
Vasoconstriction
Shivers
Fever
-
8/2/2019 Pyelonephritis (Final Case)
46/59
VII. NURSING CARE PLAN
March 4, 2011
-
8/2/2019 Pyelonephritis (Final Case)
47/59
ASSESSMENT DIAGNOSIS PLANNING INTERVENTION RATIONALE
EVALUATION
SUBJECTIVE:
Giniginaw ako
as verbalized by
the patient.
OBJECTIVE:
-Warm to touch
flush face teary
eyes shivering
-TEMP: 38.3c
-chills
Alteration in
thermoregulator:
hyperthermia r/t
bodys response
against invading
pyrogens 2 to
UTI.
After 30 minutes
of continuous
nursing
intervention the
patient will be
able to stabilized
body
temperature in
normal
range.from 38.3-
37.5 c
Monitor v/s
Wrap in warm
blankets extra
clothing and
check clothing.
Provide warm
liquids if the
client can
swallow
Close the
window and
doors and turns
the light on.
Turn off electric
fan and aircon if
necessary
Provide extra
pillow beside thepatient
Administer
paracetamol as
prescribed by the
ROD
-For base line
data
-To provide warm
and comfort.
-To elevate the
body
temperature
After 30 minutes
of continuous
nursing
intervention the
patient was able
to stabilized body
temperature
from 38.3 to 37.2
c
-GOAL MET-
March 4, 2011
-
8/2/2019 Pyelonephritis (Final Case)
48/59
ASSESSMENT DIAGNOSIS PLANNING INTERVENTION RATIONALE
EVALUATION
SUBJECTIVE:
Masakit tang
tagiliran ko
hanggang likod ko.
As verbalized by thepatient.
OBJECTIVE:
Facial grimace
guarding irritable
body weakness pale
-Pain scale:8/10
Acute pain r/t an
inflammatory
process in the
kidney.
After 30 minutes or
1 hour of giving
appropriate
intervention, the
patient will be ableto alleviate pain.
Monitor v/s and
record
Perform a
comprehensive
assessment of painseverity(0-10 scale)
Encourage
verbalization of
feelings about pain
Provide quit
environment
comfort measures
like back rubEncourage
adequate rest period
Keep comfortable.
-For baseline data
-For baseline data
-Help determine
possibility of
underlying condition-To prevent fatigue
-To provide non
pharmacologic pain
management
-To prevent fatigue
-For quick recovery
After 30 minutes or
1 hour of giving
appropriate
intervention, the
patient was able toelevate pain.
-GOAL MET-
March 4, 2011
-
8/2/2019 Pyelonephritis (Final Case)
49/59
ASSESSMENT DIAGNOSIS PLANNING INTERVENTION RATIONALE
EVALUATION
SUBJECTIVE:
Nagsusuka akoas
verbalized by the
patient.
OBJECTIVE:-Pale
-weak looking
-dry skin and lips
-restlessness
(+)vomit for 3 times
Risk for deficient
fluid volume r/t
nausea and
vomiting secondary
to dehydration.
After 30 minutes to
1 hour the patient
will be able to
maintain fluid
balance.
Monitor v/s
Monitor I and O
balance, being
aware of altered
intake outputEncourage the
client to increase
fluid intake at least
6-8 glasses a day.
Review
appropriate use of
medication
Give hard candies
-For baseline data
-To ensure accurate
picture of fluid
status
-To maintain fluidand electrolytes
balance
- To have potential
for causing of
exacerbating
Dehydration.
-To lessen the
stimulation of saliva
that enduses
vomiting
After 30 minutes to
1 hour the patient
was able to
maintain fluid
balance.-GOAL MET-
March 4, 2011
-
8/2/2019 Pyelonephritis (Final Case)
50/59
ASESSMENT DIAGNOSIS PLANNING INTERVENTION RATIONALE
EVALUATION
OBJECTIVE:
-Small frequent
urination with pain-PAIN SCALE:7/10
-WBC:
TNTC
-DYSURIA
-Urine analysis:
-COLOR: Dark
yellow
TRANSPARENCY:Tur
bid
-S.G.:1.015
-PH: Alkaline
-PROTINE: +2
SUGAR: -
RBC:12-15
Impaired urinary
elimination r/t
inflammation of
bladder mucosa
Within 8 hours of
nursing intervention
the patient
verbalizeunderstanding of
condition and
techniques to
prevent urinary
tract infection (UTI)
Monitor v/s
Encourage fluid
intake at least 8-10
glasses a dayDiscuss possible
dietary restriction
base on individual
symptoms.
Discuss proper
genitalia cleansing
and using of
feminine wash
Monitor and
assess urine output
-For baseline data
-To help maintain
renal function,
prevent infectionand urinary stones
-To help elevate the
present condition
-To let the patient
understand the said
topics
-For base line data,
for any particular
changes
Within 8 hours of
nursing intervention
the patient
verbalizedunderstanding of
condition and
techniques to
prevent urinary
tract infection (UTI).
-GOAL MET-
March 5, 2011
-
8/2/2019 Pyelonephritis (Final Case)
51/59
ASESSMENT DIAGNOSIS PLANNING INTERVENTION RATIONALE
EVALUATION
SUBJECTIVE:
Nanghihina ako as
verbalized by the
patientOBJECTIVE:
-Decrease range of
motion
-weak looking
-pale
-irritable
-slowed movement
Impaired physical
mobility r/t
decrease muscle
strength secondaryto fatigue
After 2-3 hours of
nursing intervention
the patient will able
to increase strengthand function of
compensatory body
parts.
Establish rapport
Assess nutritional
status and clients
report of energywith monitor v/s
Provide comfort
measures such as
therapeutic touch
Encourage the
patient to eat
nutritious food
which is rich in
vitamin c such as
orange fruits,
malunggay.
Identify energy
conserving
techniques for ADLs
Schedule activitieswith adequate rest
periods during the
day.
Provide safety
measures
-To gain trust and
cooperation
-For baseline data
-To provide comfort-To promote well
being and maximize
energy production
-To limits fatigue,
Maximize
participation.
-To relive fatigue
-To prevent falling
After 2-3 hours of
nursing intervention
the patient was able
to increase strengthand function of
compensatory body
parts.
-GOAL MET-
-
8/2/2019 Pyelonephritis (Final Case)
52/59
VIII. DRUG STUDY
DRUG(CLASSIFICATON)
INDICATION ACTION ADVERSE EFFECT CONTRAINDICATION NSG.
CONSIDERATION
-
8/2/2019 Pyelonephritis (Final Case)
53/59
CEFUROXIME
Brand name : Ceftin
(Anti-infectives)
750mg IV
For Urinary tract
infection
Second-generation
cephalosporin that
inhibits cell-wall
synthesis promoting
osmotic instability;usually bactericidal.
CV: Phlebitis
GI: nausea, vomiting,
diarrhea
Other:
hypersensitivityreaction
Contraindicated in
patients
hypersensitive to
drug and other
Cephalosporins. Usecautiously in the
patients
hypersensitivity to
penicillin because of
possibility of cross-
sensitivity with other
beta-lactam
antibiotics.
Before giving
ask patient if
she has
allergies to
penicillins orcephalosporin.
Obtain
sensitivity test
before giving
the first dose.
If large doses
are given,
therapy is
prolonged or
patient is at
risk, monitor
patient for sign
and symptoms
of infection.
Look-alike-sound alike:
Dont confuse
drug with other
Cephalosporins
that alike
DRUG(CLASSIFICATON)
INDICATION ACTION ADVERSE EFFECT CONTRAINDICATION
NSG. CONSIDERATION
-
8/2/2019 Pyelonephritis (Final Case)
54/59
GENTAMICIN
(Anti-infectives)
80mg IV
Serious
infections
caused by
sensitive strains
of
pseudomonas
aeruginosa,
Escherichia coli,
Proteus,
Klebsiella or
Staphylococcus
Inhibits protein
synthesis by
binding directly
to the 30s
ribosomal
subunits;
bactericidal.
CNS: fever,
headache,,
lethargy,confusion,
dizziness
CV:Hypotension
Respiratory: Apnea
GI: vomiting, nausea
Skin: rash
Contraindicated in
patients
hypersensitivity to
drug or other
aminoglycosides.
Use cautiously in
neonates, infants,
elder patients with
impaired renal
function or
neuromuscular
disorders.
Obtain sensitivity tests before
giving first dose.
Evaluate patients hearing
before and during therapy.
Notify and during therapy.
Notify prescriber if patients
complain tinnitus, vertigo,
hearing loss.
Weight patient and review
renal function studies before
therapy begins.
Obtain blood peak gentamicin
level 30 minutes after IV
infusion finishes.
Monitor renal function
Watch for s/sx of
superinfection
Therapy usually continues for
7-10days. If no response occurs
in 3-5days, stop therapy and
obtain new specimen forculture and sensitivity.
DRUG
(CLASSIFICATON)
INDICATION ACTION ADVERSE EFFECT CONTRAINDICATI
ON
NSG.
CONSIDERATION
-
8/2/2019 Pyelonephritis (Final Case)
55/59
(CLASSIFICATON) ON CONSIDERATION
METOCLOPRAMID
E
(antiemetics)
1amp IV
To prevent or
reduce nausea
and vomiting
Stimulates
motility of
upper GI tract,
in cases lower
esophageal
sphincter tone,
and blocks
dopamine
receptors at
the
chemoreceptortrigger zone.
CNS: fatigue,
anxiety
CV: Hypotension
GI: nausea, bowel
disorders,
diarrhea
GU: urinary
frequency,
incontinence
Skin: rash
Contraindicated
in patients
hypersensitivity
to drug.
Contraindicated
in patients for
whom
stimulation of GI
motility might be
dangerous (those
withhemorrhage,
obstruction or
perforation)
Monitor bowel
sounds.
Safety and
effectiveness of
drug havent
been established
for therapy
lasting longer
than 12 weeks.
Alert: use 25mg
diphenhydramine IV counteract
extrapyramidal
adverse effects
from high doses.
DRUG(CLASSIFICATON)
INDICATION ACTION ADVERSE EFFECT CONTRAINDICATION
NSG. CONSIDERATION
-
8/2/2019 Pyelonephritis (Final Case)
56/59
KETOROLAC
Brand name: Toradol
(non steroidal anti-
inflammatory drugs)
1amp IV
Short-term
management of
moderately
severe, acute
pain for single
dose treatment.
May inhibit
prostaglandin
synthesis, to
produce anti-
inflammatory,
analgesic and anti-pyretics.
CNS: dizziness,
headache
GI: vomitin,
flatulence
Skin: rash
Other: pain atinjection site.
Contraindicated in
patients
hypersensitivity to
drug and in those
with advanced renal
impairment andthose at risk for
renal impairment
depletion or at risk
of bleeding.
Contraindicated as
prophylactic
analgesic before
major surgery or
intraoperatively
when hemostatic is
critical; and in
patients currently
receiving aspirin, an
NSAID or pronecid.
Alert. The maximum
combined duration
of parenteral and
oral therapy is 5
days.
Dont give drugsepidurally or
intrathecally because
of alcohol content.
NSAIDs may mask
the s/sx of infection
because of their
antipyretic and
inflammatory
actions.
Serious GI toxicity,
including peptic
ulcers and bleeding,
can occur in patient
taking NSAIDs,
despite lack ofsymptoms.
Look-alike-sound
alike: dont confuse
Toradol with Tegretol
or Foradil
DRUG(CLASSIFICATON)
INDICATION ACTION ADVERSE EFFECT CONTRAINDICATION
NSG.CONSIDERATION
-
8/2/2019 Pyelonephritis (Final Case)
57/59
Calcium Carbonate
Brand name:
Contylan
(antacid and
antiflatulent)
Used for acute
hypocalcemiaa,
electrolyte
depletion,
cardiac arrest,
hyperkalemiaand
hypermagnesia.
Used in chronic
hypocalcemia,
calcium
deficiency, and
as an antacid.
Used treatment
of
hyperphosphat
emia
Calcium is essential
for function, integrity
of nervous, muscular
and skeletal systems.
It plays an important
role in normal cardiacand renal function,
respiration blood
coagulation, cell
membrane and
capillary
permeability. It
assists in regulating
the release and
storage of
neurotransmitters
and hormones.
Calcium neutralizes
or reduces gastric
acid production.
CNS: headache
CV: Hypotension
GI: nausea, vomiting
GU: difficult or
painful urination
Skin: flushing,warmth, rash,
redness, sweating
Other: burning
sensation at injection
site
No contraindicated
had notify.
Assess bp, ECG
reading, renal
function.
Give syrup
diluted in juice
or water. Chew chewable
tablet well
before
swallowing.
Monitor for sign
of
hypercalcemia.
DRUG INDICATION ACTION ADVERSE EFFECT CONTRAINDICATIO NSG.
CONSIDERATION
-
8/2/2019 Pyelonephritis (Final Case)
58/59
N
PARACETAMOL
Classification:
-Therapeutics:
Antipyretics, non
opioid analgesics
Mild pain and
fever
Inhibits to synthesis
of prostaglandins
that serve as
medicines of pairs
and fever primarily
in the CNS has no
significant anti-
inflammatory
properties or G.I
toxicity
GI: hepatic failure,
hepatoxicity
GV: Renal failure(high
doses/chronic use)
HEMAT: neutropehia.
Fancy topenia,
Leukopenia
DERM: rash, urticaria
Previous
hypersensitivity
products
containing alcohol,
aspartame,
sacharin, sugar or
tartrazine should
be avoided in
patients who have
hypersensitivity or
intolerance to
these compound.
Assess overall
health status and
alcohol usage
before
administering
paracetamol
patients who are
malnourished or
chronically abuse
alcohol are at
higher risks of
developing
hepatotoxicity With chronic use
of usual doses of
drugs.
Assess amount
frequently and
type of drugs taken
in patients self
medicating,
especially with
over the counter
drugs prolonged
use of paracetamol
increase the risk of
adverse renal
effects.
Assess fever: Note
-
8/2/2019 Pyelonephritis (Final Case)
59/59
END OF CASE
PRESENTATIONTHANK YOU!
GROUP 1 (GROUP BULILIT & BAGTIT!)