Embed Size (px)
Citation preview

Managing a large scale accident/incident
investigation
ICAO Accident/Incident Investigation Workshop
Oficina Regional NACC de la OACI – Mexico City
4 June 2013
Recurrent Questions
What happened?
Have you found the recorders?
Who collaborates and how?
Will the investigation be long?
Whose fault is it?
Why did it happen?
What could have
been done to prevent
this accident?

� More than ever, abide by it:� Investigations must be conducted in a timely manner with the sole
objective of drawing safety lessons;
� The State conducting the investigation must associate with the investigation other States, in particular the States of Manufacture, Design, Registry and Operation of the aircraft;
�Investigators must be independent and cannot receive instructions from any authority;
�If a judicial investigation takes place in parallel with the safety investigation, it must not impede the due course of the safety investigation;
�Only the authority conducting the investigation can provide information on the investigation. Its report must be made public.
�While respecting the sovereignty of each ICAO contracting state, an accident and its lessons learned belong to the international aviation community.
Annex 13

State of
Occurrence
State of
Design
State of
Registry
State of the
Operator
State of
Manufacture
International Organization of a Safety Investigation

International Organization of a Safety Investigation
State of
Occurrence
State of
Design
Designer
State of
Registry
Owner
State of the
OperatorOperator
State of
Manufacture
Manufacturer

Technical
adviser
Technical
adviser
Technical
adviser
Example
EASA BEA(France)
US NTSB(Acc. Rep.)
DGAC
UK AAIB
(Acc. Rep.)
Accident on 23 July 2011 at Paris-CDG airport
to the Boeing 737-300 registered G-CELD operated by Jet2.com
State of Occurrence
State of Manufacture(and Design)
State of the Operator (and Registry)

Part IOrganization and
Planning
Part IIProcedures and
Checklists
Part III
Investigation
Part IV
Reporting
ICAO Doc 9756

� Working groups:
Organization
-Wreckage-Structure-Basic systems-Engines-Maintenance
-Flight recorders-Flight qualities/ Performance-Complex systems
-Flight ops-Weather-Air navigation-Survival aspects
AIRCRAFT SYSTEMS OPERATIONS HUMAN PERFORMANCE
IIC
Deputy IIC

�Site access� Airport closed due to the accident
� Uncertainty on the location of the accident
� Remoteness of the area
� Security issues
Challenges
� Independence and competence
�Relations between Justice and Safety investigations
� Investigating human and organizational factors
�Consultation and publication of final reports
�Communication and media coverage
�Cost of sea searches and recovery
�Training
Challenges

Case Study
Safety Investigation
into the accident to the Airbus A330,
Air France flight 447, June 1, 2009

� 228 victims
� 32 nationalities
� 23-month search for
wreckage*
� 3-year investigation
� 32 millions €
Circumstances

���� BEA (France) in charge of the safety investigation
with participation of
���� CENIPA (Brazil)
���� NTSB (USA)
���� BFU (Germany)
���� AAIB (UK)
���� ANAC (Senegal)
and
� 10 countries as Observers (China,Hungary, Ireland, Italy, Korea,
Lebanon, Morocco,Norway, Russia, Switzerland).
Organization of the Safety Investigation

Floating Debris

Undersea Search Operations
Divers
Totally
encapsulated suit
standard ROV
Specialized ROV -
Submarine
????
around 2 km
Plateau continental
Plaine abyssale
Limited pingerrange
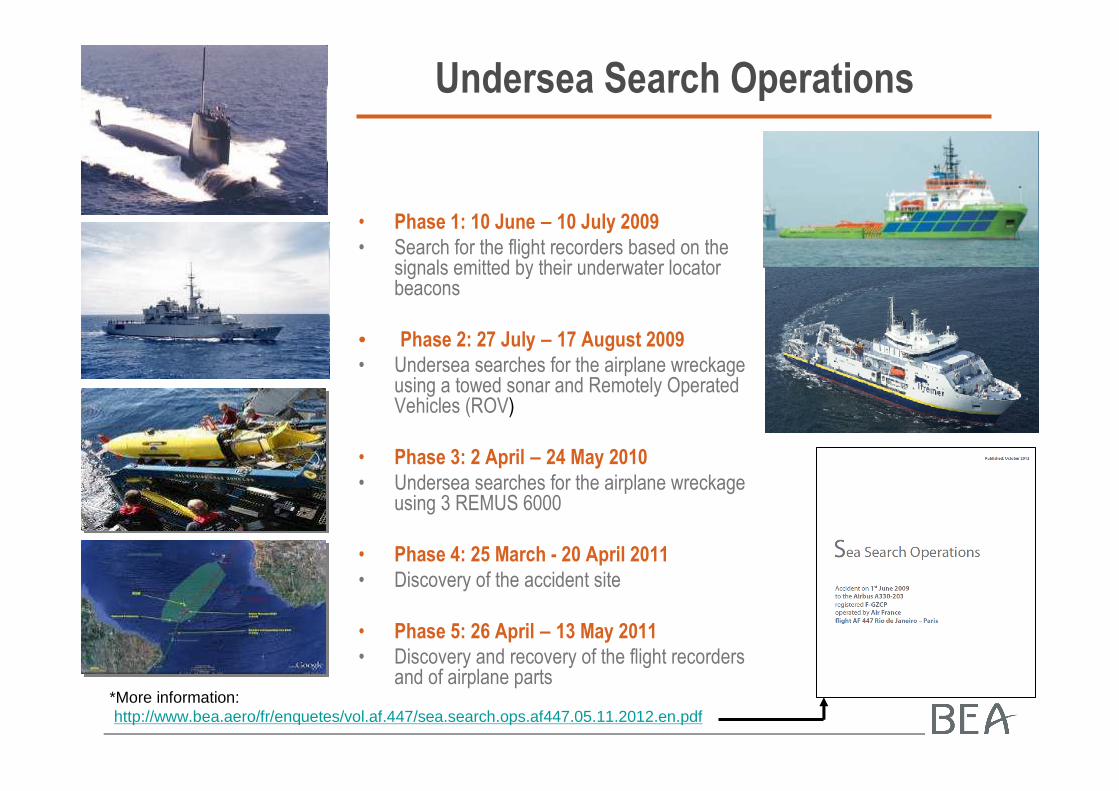
Undersea Search Operations
• Phase 1: 10 June – 10 July 2009
• Search for the flight recorders based on the signals emitted by their underwater locator beacons
• Phase 2: 27 July – 17 August 2009
• Undersea searches for the airplane wreckage using a towed sonar and Remotely Operated Vehicles (ROV)
• Phase 3: 2 April – 24 May 2010
• Undersea searches for the airplane wreckage using 3 REMUS 6000
• Phase 4: 25 March - 20 April 2011
• Discovery of the accident site
• Phase 5: 26 April – 13 May 2011
• Discovery and recovery of the flight recorders and of airplane parts
*More information:http://www.bea.aero/fr/enquetes/vol.af.447/sea.search.ops.af447.05.11.2012.en.pdf

1 and 3 May 2011: Discovery of the FDR & CVR

Recorders readout

History of flight

Flight Path
22 h 29
01 h 49

BEA animation
� Based on data from flight recorders
� For educational or training purpose only
� Not all parameters that were displayed to the crew are shown here
AOA and Stall Warning threshold
Warnings
Significant CVR events or comments
Flight path

1 2 34 5 6
7
Part 1
Part 2 Part 3
���� Part 1: from the beginning of the CVR
recording until the disconnection of the
autopilot
���� Part 2: from the disconnection of the
autopilot to the triggering of the stall warning
���� Part 3: from the triggering of the stall
warning to the end of the flight

1 Cruise at FL 350 and Mach 0.82
Part 1

A few minutes after ORARO: heading change of 12 degrees to the left2
Part 1

Main findings - Part 1
�The composition of the crew was in accordance with the operator’s procedures.
�There was an implicit designation of a pilot as relief Captain.
�There is no regulatory CRM training for a crew made up of two copilots in a situation with a relief Captain.

1 2 34 5 6
7
Phase 1
Part 3
Part 2

Soon after AP disconnection: roll and nose-up inputs by the PF, the
airplane began to climb3
Part 2

Altitude 36,000 ft - vertical speed reached max value of +6,900 ft/min4
Part 2

Frozen Pitot

Speed displayed on the PFDs

Main findings - Part 2
�Unreliable airspeed situation �difficulty to have a correct situation awareness following a situation
with unreliable airspeed
�lack of appropriate response to unreliable airspeed situation
�observed response of the crew not specific nor isolated
�poor training to unreliable airspeed situations
�Insufficient basic airmanship
�CRM �loss of coordination due to stress and when faced to a
misunderstood situation.
�inaccurate communications
�Ergonomic �numerous messages displayed by ECAM
�no specific ECAM message that could help the crew to identify the situation
�FD still engaged

1 2 34 5 6
7
Part 1
Part 2
Part 3

Altitude 37,500 ft, Mach 0.68 and angle of attack 5°°°° => triggering of the stall warning5
Part 3

Stall warning in alternate law
AOA

Flight Enveloppe

Altitude 35,800 ft, vertical speed -9,000 ft/min, N1 around 102%
Part 3
6

Altitude 10,000 ft, nose-up pitch: 12 °°°°, angle of attack > 40°°°°, vertical speed: -12,000
ft/min
Part 3
7

End of flight, nose-up pitch: 16°°°°, roll 5°°°° left, vertical speed: -10,900 ft/min
Part 3
Main findings - Part 3
�The speed displayed
�on the left PFD was incorrect for 29 seconds,
�that of the speed on the ISIS for 54 seconds
�and the speed displayed on the right PFD for 61 seconds
at most
�The angle of attack is the parameter that allows the stall
warning to be triggered; if the angle of attack values become
invalid, the warning stops
�By design, when the measured speed values are lower than
60 kt, the measured angle of attack values are invalidated.
�The aeroplane’s angle of attack is not directly displayed to
the pilots
�Neither of the pilots formally identified the stall situation

Sequence of events leading to the accident

1. The temporary inconsistency between the measured
speeds, likely following the obstruction of the Pitot probes
by ice crystals

Pitot probes

Speed measurement system architecture

1. The temporary inconsistency between the measured
speeds, likely following the obstruction of the Pitot probes
by ice crystals
Ice Crystals
Pressionmesurée
Measured
Pressure
⇒⇒⇒⇒ autopilot disconnection and reconfiguration to alternate law

2. Inappropriate control inputs destabilizing the flight path

3. The lack of any link, by the crew, between the loss of displayed airspeed information and the appropriate procedure

4. The late identification of the deviation from the flight path by
the PNF and insufficient correction applied by the PF

5. The crew not identifying the approach to stall, their lack of
immediate response and the exit from the flight envelope
6. The crew’s failure to diagnose the stall situation and
consequently a lack of inputs that would have made
recovery possible
AOA

These events can be explained by the
combination of these associated factors:
� The feedback mechanisms of all of those involved
� To identify the repeated non-application of the loss of
airspeed information procedure and to remedy this,
� To ensure that the risk model for crews in cruise included
icing of the Pitot probes and its consequences;
These events can be explained by the
combination of these associated factors:
� An absence of training, at high altitude, in manual
aeroplane handling and the procedure relating to
speed indication anomalies

These events can be explained by the combination of these associated factors:
� Task-sharing weakened by
� Incomprehension of the situation when the autopilot disconnection occurred,
� Poor management of the startle effect that generated a highly charged emotional factor for the two copilots;
� Lack of a clear display in the cockpit of the airspeed inconsistencies identified by the computers

These events can be explained by the combination of these associated factors:
� The crew not taking into account the stall warning, which could have been due to:� A failure to identify the aural warning, due to low exposure time in training to stall
phenomena, stall warnings and buffet,
� The appearance at the beginning of the event of transient warnings that could be considered as spurious,
� The absence of any visual information to confirm the approach-to-stall after the loss of the limit speeds,
� The possible confusion with an overspeed situation in which buffet is also considered as a symptom,
� Flight Director indications that may led the crew to believe that their actions were appropriate, even though they were not,
� The difficulty in recognizing and understanding the implications of a reconfiguration in alternate law with no angle of attack protection.

Safety Recommendations

41 Safety Recommendations
� Interim Report n°2: 6
� Interim Report n°3: 10
� Final Report: 25
6
26
13
13
1
0
5
10
15
20
25
30
DGAC AESA OACI Aut. Brésil FAA Aut. SénégalSenegalEASA Brazil FAAICAODGAC

Safety Recommendations
� Certification (2)� Meteorological
� AOA indicator
� Operations and Initial and Recurrent Training of Pilots (11)� Manual aircraft handling
� Reconfiguration law and associated protections
� Relief captain
� Managing crew resources and surprise
� Instructor training
� Improvement of flight simulators and scenarios

Safety Recommendations
� Ergonomics (6)
� FD appearance / disappearance
� Warning vs Triggering of specific monitoring
� Stall warning
� Operational and Technical Feedback (2)
� Feedback process from in-service events
� Oversight of the Operator (2)
Safety Recommendations
� Search and Rescue Operations (6)� Coordination
� Organization of SAR in France
� Air Traffic Control (2)� Use of ADS-C and ADS-B
� Link ground / aeroplane
� Flight Recorders and Transmission of Flight Data (10)� Flight parameters transmission
� ULB
� Recorded parameters
� Image Recorder

� Public reports:� 3 interim reports (July 2, 2009;
December 17, 2009; July 29, 2011)
� final report (July 5, 2012)
� More at: http://www.bea.aero/en/enquetes/flight.af.447.php
More Information






























