Embed Size (px)
Citation preview
2
Resilience and Transitions from Dementia Caregiving
Joseph E. Gaugler, Ph.D.Assistant Professor
Center on Aging, Center for Gerontological NursingThe University of Minnesota
April 20, 2006

Acknowledgements
Collaborators
• Robert L. Kane, M.D., Minnesota Chair in Long-Term Care and Aging, University of Minnesota
• Robert Newcomer, Ph.D., Professor, Department of Social and Behavioral Science and Institute for Health and Aging, The University of San Francisco
Funding Support
• The Alzheimer’s Association, NIRG-2249
• Health Care Financing Administration, 509-89-0069
Background
Resilience as a concept• Child development and developmental psychopathology
• Processes that may encompass resilience (Masten et al., 1990; Wyman et al., 1999)
– Positive outcomes despite negative circumstance; resilience as “overcoming the odds”
– Sustained competence of positive development while facing continual threat or stress: resilience as “stress resistance”
– Recovery from negative life experience or trauma: resilience as “recovery”
Resilience in aging

Resilience in Dementia Caregiving
Cross-sectional vs. longitudinal research
• The “wear and tear hypothesis”
Uplifts and rewards of dementia caregiving
Small-scale descriptive reports of resilience (Garity, 1997; Ross et al., 2003)

Conceptual Model
Conceptual overlap of resilience with similar constructs
Resilience in dementia caregiving as “stress resilience”
Research question and hypothesis What factors are associated with resilience among dementia
caregivers?
Dementia caregivers who indicate low resilience at baseline will be less likely to remain in their caregiving roles when compared to the high resilience group.
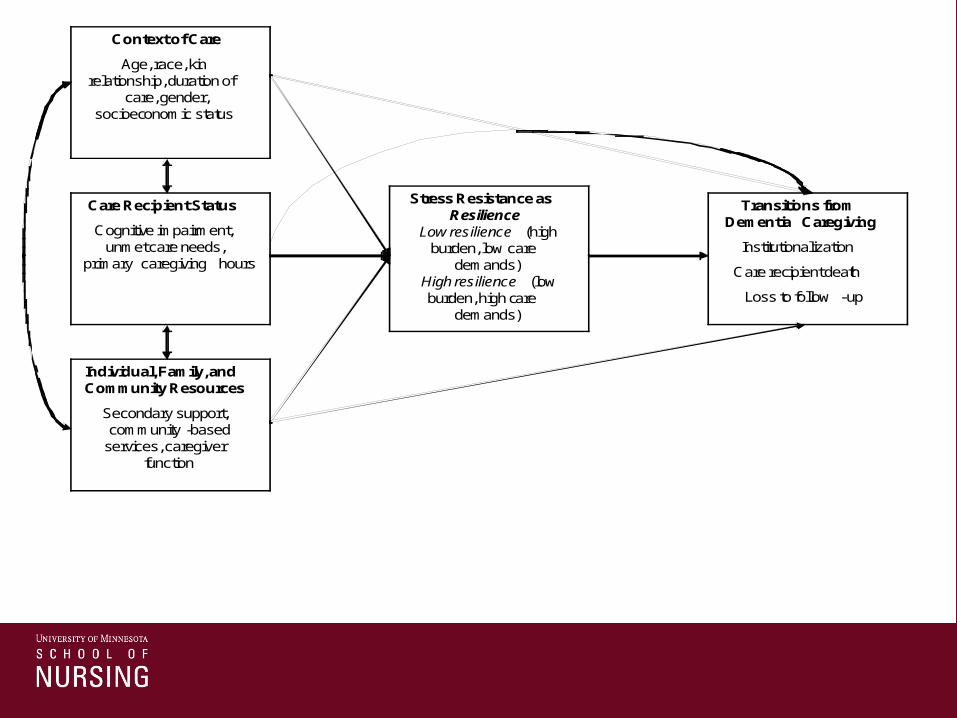
Individual, Family, and Community Resources
Secondary support, community -based
services, caregiver function
Care Recipient Status
Cognitive impairment, unmet care needs,
primary caregiving hours
Context of Care
Age, race, kin relationship, duration of
care, gender, socioeconomic status
Stress Resistance as Resilience
Low resilience (high burden, low care
demands) High resilience (low burden, high care
demands)
Transitions from Dementia Caregiving
Institutionalization
Care recipient death
Loss to follow -up
Methods
Medicare Alzheimer’s Disease Demonstration
Measures: Resilience• Burden
• Care Demands
• Construction of resilience measure– High resilience vs. low resilience
Measures: Covariates• Context of care
• Care recipient function and cognitive status
• Resources
Analysis• Correlates of resilience: Logistic regression
• Resilience as a predictor of transitions from dementia caregiving: Multinomial logistic regression
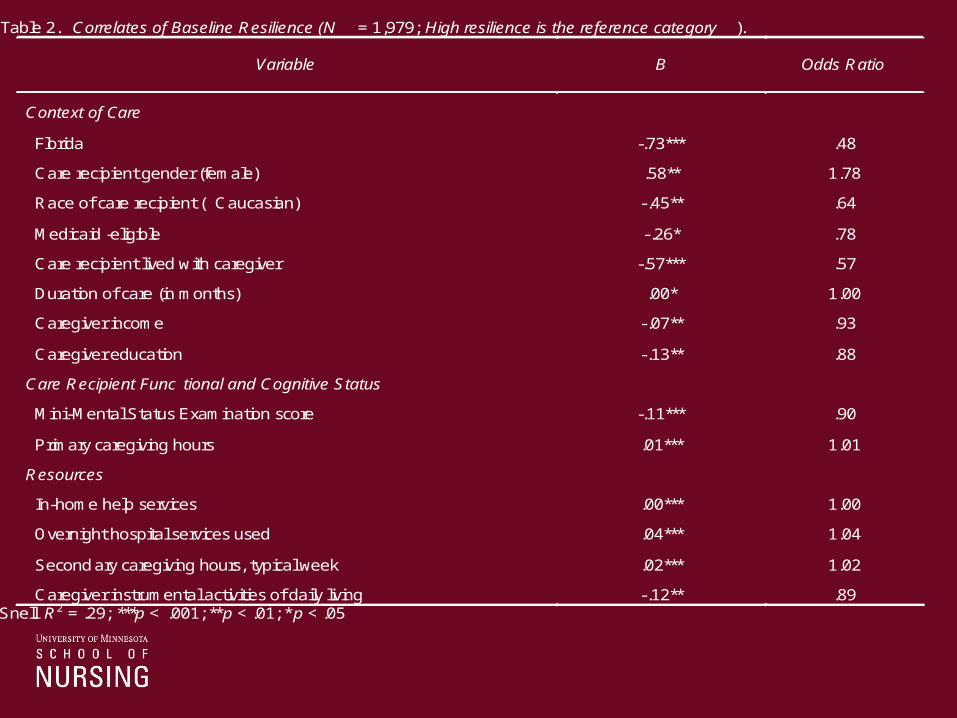
Table 2. Correlates of Baseline Resilience (N = 1,979; High resilience is the reference category ).
Variable
B
Odds Ratio
Context of Care
Florida -.73*** .48
Care recipient gender (female) .58** 1.78
Race of care recipient ( Caucasian) -.45** .64
Medicaid -eligible -.26* .78
Care recipient lived with caregiver -.57*** .57
Duration of care (in months) .00* 1.00
Caregiver income -.07** .93
Caregiver education -.13** .88
Care Recipient Func tional and Cognitive Status
Mini-Mental Status Examination score -.11*** .90
Primary caregiving hours .01*** 1.01
Resources
In-home help services .00*** 1.00
Overnight hospital services used .04*** 1.04
Second ary caregiving hours, typical week .02*** 1.02
Caregiver instrumental activities of daily living -.12** .89 Cox and Snell R2 = .29; ***p < .001; **p < .01; * p < .05

Effects of Baseline Resilience (N = 1,979) and Change in Resilience (N = 1556) on Transitions
Variable
Baseline Resilience
Change in Resilience
Death NH
LTFU
Death
NH
LTFU
Resilience Baseline resilience (low re silience)
.62** 1.87*** 1.77* - - -
Change in resilience a Stability -low resilience
- - - 2.46* .43* .34
High resilience -low care demand/low burden
- - - 11.52*** 1.36 4.14**
Low resilience -low care d emand/low burden
- - - 10.42*** 3.31*** 8.90***
NOTE: *** p < .01; ** p < .01; * p < .05 aHigh resilience -low resilience is the reference category Cox and Snell pseudo R2 = .28 and .33 for baseline resilience and change in resilience models, respective ly

Discussion
Care recipient function and sociodemographic context associated with resilience
Complex effects of baseline resilience
• Low resilience as predictive of institutionalization and loss to follow-up
• Low resilience negatively associated with care recipient death
Complex effects of change in resilience
• Anticipation of the termination of at-home care
Implications
Limitations
Capturing heterogeneity of dementia caregivers
• A typology approach
Assessment strategies
Incorporation of intrinsic dimensions of resilience





























