-
Intern. J. Neuroscience, 116:11251138, 2006Copyright C 2006
Informa HealthcareISSN: 0020-7454 / 1543-5245 onlineDOI:
10.1080/00207450500513922
EFFECTS OF SLEEP DEPRIVATION ON LATERALVISUAL ATTENTION
ATHENA P. KENDALLMARY A. KAUTZWalter Reed Army Institute of
ResearchSilver Spring, Maryland, USA
MICHAEL B. RUSSOUnited States Army Aeromedical Research
LaboratoryFort Rucker, Alabama, USA
WILLIAM D. S. KILLGOREWalter Reed Army Institute of
ResearchSilver Spring, Maryland, USA
Sleep loss temporarily impairs vigilance and sustained
attention. Because thesecognitive abilities are believed to be
mediated predominantly by the right cerebralhemisphere, this
article hypothesized that continuous sleep deprivation resultsin a
greater frequency of inattention errors within the left versus
right visualfields. Twenty-one participants were assessed several
times each day during a40-h period of sustained wakefulness and
following a night of recovery sleep.At each assessment,
participants engaged in a continuous serial addition task
whilesimultaneously monitoring a 150 visual field for brief
intermittent flashes of light.Overall, omission errors were most
common in the leftmost peripheral field for
Received 9 June 2005.The views expressed in this article are
those of the authors and do not reflect the official policy
or position of the Department of the Army, the Department of
Defense, the U.S. Government, orany of the institutions with which
the authors are affiliated.
Address correspondence and reprint requests to MAJ William D. S.
Killgore, Ph.D.,Department of Behavioral Biology, Division of
Psychiatry and Neuroscience, Walter ReedArmy Institute of Research,
503 Robert Grant Avenue, Silver Spring, MD 20910, USA.
E-mail:[email protected]
1125
-
1126 A. P. KENDALL ET AL.
all sessions, and did not show any evidence of a shift in
laterality as a functionof sleep deprivation. Relative to rested
baseline and postrecovery conditions, sleepdeprivation resulted in
a global increase in omission errors across all visual locationsand
a general decline in serial addition performance. These findings
argue againstthe hypothesis that sleep deprivation produces
lateralized deficits in attention andsuggest instead that deficits
in visual attention produced by sleep deprivation areglobal and
bilateral in nature.
Keywords attention, cognition, laterality, right-hemisphere,
sleep deprivation,vigilance, visual field, visual perception
Normal, healthy individuals need adequate sleep for optimal
cognitivefunctioning (Himashree et al., 2002). Without adequate
sleep, humansshow reduced alertness (Penetar et al., 1993) and
impairments in cognitiveperformance (Thomas et al., 2000, 2003).
Prolonged sleep deprivation isassociated with decrements in
elementary cognitive abilities such as vigilanceand sustained
attention (Doran et al., 2001; Wesensten et al., 2004), as wellas
impairments in complex, higher-order cognitive processes such as
verbalfluency, logical thought, decision making, and creativity
(Harrison & Horne,1997, 1999, 2000). In occupational settings
such as aviation, air traffic control,and sustained military
operations where constant vigilance is a necessity,extended periods
of sleep loss have been associated with catastrophic
accidents(Mitler et al., 1988) and may have been a factor in some
friendly fire incidents(Belenky et al., 1994). Studies of
sleep-deprived individuals show that errorsattention begin to
emerge by 19 h of continuous wakefulness (Russo et al.,2004) and
cognitive performance declines at a rate of approximately 25%
foreach 24-h period of wakefulness (Belenky et al., 1994).
Sleep deprivation produces global decreases in cerebral
metabolism andblood flow, with the greatest declines evident in
those regions critical for higherorder cognitive processes (Thomas
et al., 2000). These regions, the heteromodalassociation cortices,
are associated with attention, vigilance, and complexcognitive
processing, and reductions in activity within these regions
areassociated with decrements in these higher-order cognitive
process (Mesulam,1999). As a global blood flow and metabolic
activity decline during prolongedperiods without sleep, the brain
appears to compensate by recruiting cognitiveresources from nearby
brain regions within the prefrontal and parietal corticesin order
to maintain cognitive performance at acceptable levels (Drummondet
al., 2001). Some evidence suggests that these compensatory
activities maybe particularly prominent within the right cerebral
hemisphere (Drummondet al., 2001). Consistent with these reports,
other studies suggest that cognitive
-
SLEEP DEPRIVATION & VISUAL ATTENTION 1127
processes mediated by the right hemisphere are more adversely
affected bysleep deprivation than those mediated by the left
(Johnsen et al., 2004; Pallesenet al., 2004).
Neuropsychological evidence suggests that the right cerebral
hemisphere isdominant for attentional processes (Heilman & Van
Den Abell, 1980; Mapstoneet al., 2003). Much of the evidence
supporting the dominance of the righthemisphere in attention comes
from studies of patients with unilateral braindamage (Heilman &
Van Den Abell, 1980; Weintraub & Mesulam, 1987).Lesions to the
right cerebral hemisphere are more likely to produce
contralateralhemispatial neglect than similar lesions to the left
hemisphere (Behrmann et al.,2004; Mapstone et al., 2003, Mesulam,
1999). Further evidence supporting theprominent role of the right
hemisphere in attentional processing comes fromseveral functional
neuroimaging studies that reveal greater right hemisphereactivity
in response to tasks requiring allocation of spatial attention
(Fink et al.,2001; Macaluso et al., 2001). The accumulating
evidence suggests that the leftcerebral hemisphere allocates its
attentional processing predominantly towardthe contralateral (i.e.,
right) hemispace, whereas the right hemisphere appearsto distribute
attentional processing more equally between both hemispaces, andis
therefore considered dominant for attention (Mesulam, 1999).
Consequently,the phenomenon of contralesional neglect occurs nearly
exclusively followinglesions to the right hemisphere.
Given the apparently greater role of the right hemisphere in
attentionalprocessing and the preliminary evidence that the
cognitive processes mediatedby the right hemisphere may be more
sensitive to the detrimental effects of sleepdeprivation, it was
hypothesized that prolonged sleep loss results in greaterimpairment
of right hemisphere visual attention mechanisms oriented towardthe
contralateral (i.e., left) perceptual hemispace. Participants were
assessedseveral times each day while remaining awake for 40 h.
During each 15-mintesting session, participants monitored a 150 arc
of lateral visual space forperiodic occurrences of brief flashes of
light while simultaneously performinga continuous serial addition
task.
METHODSubjectsTwenty-one active duty military personnel (9
females; 12 males; M age = 28.2,SD = 5.5) participated in the
study. Volunteers were recruited through word ofmouth and flyers
posted at the Walter Reed Army Institute of Research. Visual
-
1128 A. P. KENDALL ET AL.
acuity was assessed prior to entry with a standard Snellen
Chart. Screeningcriteria required distant acuity of 20/20 and near
acuity of 20/25 withoutrefractive correction or from +1.00 D.S. to
3.00 D.S. with correction to20/20. All participants were in good
physical health, had no evidence of acurrent sleep disorder, and
were free of any history of neurologic, psychiatric, orserious
medical condition, as determined by the study physician. All
potentialvolunteers consented to a urine drug screen and were
excluded if there wasany evidence of use of illegal substances or
stimulants. Volunteers were alsoexcluded if they regularly consumed
more than 300 mg of caffeine per day.Financial compensation was
provided for participation in the study and allprocedures were
conducted in accordance with the requirements of the HumanUse
Committee at Walter Reed Army Institute of Research and the
SurgeonGenerals Human Subjects Research Review Board.
ApparatusIn order to assess divided attention capacities,
participants were required toengage in two demanding attentional
tasks simultaneously. Attention to visualstimuli within the lateral
visual field was assessed with the Choice VisualPerception Task
(CVPT). The CVPT consists of a horizontal U-shaped barfitted with
11 light-emitting diodes (LEDs) located at 15 increments aroundthe
arc (see Figure 1). The arc was placed at eye level and the center
diode waslocated 18 inches from the bridge of the nose of the
participant. RemainingLEDs were located in the left and right
visual fields at 15 intervals (i.e.,L75, L60, L45, L30, L15, C,
R15, R30, R45, R60, and R75). The task wasperformed against a black
backdrop and ambient room light was maintained atapproximately 5
foot candles to ensure uniform visibility of the stimuli. A
chinrest was used to stabilize head movement and volunteers were
instructed tomaintain visual fixation on a focal point presented on
a laptop computer. Eachstimulus appeared for 250 ms, with an
interstimulus interval varying from 3.50to 15.25 s for each trial.
Fifteen variations of visual stimuli were presentedrandomly 10
times for a total of 150 stimulus presentations for each trial.Each
administration of the CVPT lasted 15 min. For single LED
presentations,responses were made via a keypad with buttons for
left, center, and right,corresponding to the location of the
stimulus.
Double simultaneous stimuli were also presented on 40 trials.
Thesepresentations always included the center stimulus (C) and an
additional stimuluslocated within the left or right peripheral
field (i.e., C+L75, C+L60, C+R60,and C+R75). During presentations
of double simultaneous stimuli, responses
-
SLEEP DEPRIVATION & VISUAL ATTENTION 1129
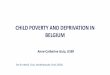
Figure 1. An example of a participant engaged in the Choice
Visual Perception Task (CVPT) andSerial Addition Test (SAT). The
SAT was presented on a laptop computer placed in front of
theparticipant. The CVPT apparatus includes a laterally placed
U-shaped bar with light emitting diodesplaced at 15-degree
intervals around a 150 degree arc of the visual field. Participants
completedthe SAT continuously while monitoring the CVPT for
intermittent light flashes.
were made by pressing the two corresponding buttons
simultaneously (e.g.,center and right keys). All volunteers were
instructed to use their right-handfor the keypad response,
regardless of reported handedness. Hits, misses, andresponse
omissions were recorded for each stimulus presentation.
In conjunction with continuous monitoring of the light locations
of theCVPT, participants were required to sustain continuous
performance on a SerialAddition Task (SAT). During the SAT,
participants were required mentallyto add sequences of single digit
numbers that were presented on the screenand then vocally report
the answers for each trial. During each sequence, anumber from 0 to
9 would appear on the screen for 750 ms, which would beimmediately
replaced by a plus-sign (+) for 750 ms, then a second
number,followed by an equal sign ( = ). At the presentation of the
equal sign, theparticipant would vocally report the sum of the
preceding two digits. The
-
1130 A. P. KENDALL ET AL.
SAT stimuli were presented three inches below the center LED on
a 15-inch(diagonal) computer screen placed immediately below the
CVPT. The targetstimuli were presented in 72-point bolded Tahoma
font at a screen resolutionof 1024 768 pixels. Participants were
required to continuously engage inthe SAT while simultaneously
monitoring the CVPT for periodic stimulusoccurrences.
Design and ProcedureEach study run was conducted over two
consecutive weeks. On the first day(Monday) of the baseline phase,
volunteers reported to the sleep laboratoryat approximately 0945.
Each volunteer was fitted with an actigraph watch,given a sleep log
to record their daily sleep habits, and reminded to abstainfrom
caffeine, alcohol, and tobacco products. On that same day, the
volunteerswere trained on a battery of neuropsychological tests and
the CVPT-SAT.Baseline testing concluded at approximately 1130. The
residential phase beganthe following week.
Volunteers arrived at the sleep laboratory at 0800 to begin the
residentialphase. The residential phase involved a second baseline
testing session, 40 hof sleep deprivation, 9 h of recovery sleep,
and a postrecovery sleep testingsession. On day 1 (Monday),
subjects completed CVPT-SAT at 2-h intervalsto provide a second
rested baseline measure. Starting at 24:00 (midnight)volunteers
received 8 h time in bed. The 40 h sleep deprivation period
beganwhen participants awakened at 0800 on day 2 (Tuesday).
Volunteers remainedawake until 2400 (midnight) on Day 3
(Wednesday). Throughout the course ofthe sleep deprivation period,
the CVPT-SAT was administered at 2-h intervals.After the 40 h sleep
deprivation period was concluded, each volunteer received9 h of
time in bed to obtain recovery sleep. On Thurs (day 4)
volunteerswere awakened at 0900, were retested twice on the
CVPT-SAT, debriefed, andreleased from the study at 18:00. Each
CVPT-SAT administration lasted for 15min.
Data AnalysisTo control for the effects of circadian influences,
data were averaged andcompared across blocks of time encompassing
the same time periods eachday (i.e., 1500, 1700, and 1900). For
each trial, the number of single anddouble stimulus response
omissions was calculated and averaged across trialsfor each
session. Similarly, the percentage correct for each trial of the
serial
-
SLEEP DEPRIVATION & VISUAL ATTENTION 1131
addition task was calculated and averaged across trials for each
session. Datawere analyzed using repeated measures analysis of
variance, with Greenhouse-Geisser corrections for lack of
sphericity. Stimulus location within the visualfield (11 locations)
and testing session (4 sessions) were entered as repeatedmeasures
variables. The criterion for significance was set at = .05.
Becausea greater number of errors were hypothesized within the
leftmost peripheralfield as a consequence of sleep deprivation, the
authors conducted plannedcomparisons between the number of errors
at the leftmost peripheral location(L75) versus the central (C) and
rightmost peripheral (R75) sites, with =.05, uncorrected. Post hoc
comparisons were conducted using a Bonferronicorrection to = .05
for experiment-wise error rate.
RESULTS AND DISCUSSIONAccumulating evidence suggests that sleep
deprivation affects lateralizedprocessing of stimuli (Iskra-Golec,
2001), and may be particularly disruptive tocognitive and
perceptual processes that involve the right hemisphere (Johnsenet
al., 2002; Pallesen et al., 2004). It was predicted, therefore,
that sleep depri-vation is associated with a general decline in
alertness and attention to visualstimuli and that these deficits
would be most evident within the left peripheralvisual field. There
was a significant main effect of session, (F3,60 = 45.18, p