Embed Size (px)
Citation preview

Breaking Up Prolonged SittingWith Standing or WalkingAttenuates the PostprandialMetabolic Response inPostmenopausal Women:A Randomized Acute StudyDiabetes Care 2016;39:130–138 | DOI: 10.2337/dc15-1240
OBJECTIVE
To determine whether breaking up prolonged sitting with short bouts of standingor walking improves postprandial markers of cardiometabolic health in women athigh risk of type 2 diabetes.
RESEARCH DESIGN AND METHODS
Twenty-two overweight/obese, dysglycemic, postmenopausal women (mean6 SDage 66.6 6 4.7 years) each participated in two of the following treatments:prolonged, unbroken sitting (7.5 h) or prolonged sitting broken up with eitherstanding or walking at a self-perceived light intensity (for 5 min every 30 min).Both allocation and treatment order were randomized. The incremental areaunder the curves (iAUCs) for glucose, insulin, nonesterified fatty acids (NEFA),and triglycerides were calculated for each treatment condition (mean 6 SEM).The following day, all participants underwent the 7.5-h sitting protocol.
RESULTS
Compared with a prolonged bout of sitting (iAUC 5.3 6 0.8 mmol/L · h), bothstanding (3.5 6 0.8 mmol/L · h) and walking (3.8 6 0.7 mmol/L · h) significantlyreduced the glucose iAUC (both P < 0.05). When compared with prolonged sitting(548.2 6 71.8 mU/L · h), insulin was also reduced for both activity conditions(standing, 437.26 73.5 mU/L · h; walking, 347.96 78.7 mU/L · h; both P < 0.05).Both standing (21.0 6 0.2 mmol/L · h) and walking (20.8 6 0.2 mmol/L · h)attenuated the suppression of NEFA compared with prolonged sitting (21.5 6 0.2mmol/L · h) (both P < 0.05). There was no significant effect on triglyceride iAUC. Theeffects on glucose (standing andwalking) and insulin (walkingonly) persisted into thefollowing day.
CONCLUSIONS
Breaking up prolonged sitting with 5-min bouts of standing or walking at a self-perceived light intensity reduced postprandial glucose, insulin, and NEFA responsesin women at high risk of type 2 diabetes. This simple, behavioral approach couldinform future public health interventions aimedat improving themetabolic profile ofpostmenopausal, dysglycemic women.
1Diabetes Research Centre, University of Leices-ter, Leicester, U.K.2National Institute for Health Research Leicester-Loughborough Diet, Lifestyle and Physical Activ-ity Biomedical Research Unit, Leicestershire, U.K.3National Institute for Health Research Collabo-rations for Leadership in Applied Health Re-search and Care, East Midlands, U.K.4Institute of Cardiovascular and Medical Sci-ences, University of Glasgow, Glasgow, U.K.5School of Sport, Exercise and Health Sciences,Loughborough University, Leicestershire, U.K.6Baker IDI Heart and Diabetes Institute, Mel-bourne, Victoria, Australia7Mary MacKillop Institute for Health Research,Australian Catholic University, Melbourne, Victo-ria, Australia
Corresponding author: Joseph Henson, [email protected].
Received 11 June 2015 and accepted 8 October2015.
Clinical trial reg. no. NCT02135172, clinicaltrials.gov.
This article contains Supplementary Data onlineat http://care.diabetesjournals.org/lookup/suppl/doi:10.2337/dc15-1240/-/DC1.
© 2016 by the American Diabetes Association.Readersmayuse this article as longas thework isproperly cited, the use is educational and not forprofit, and the work is not altered.
Joseph Henson,1,2 Melanie J. Davies,1,2
Danielle H. Bodicoat,1,2,3
Charlotte L. Edwardson,1,2
Jason M.R. Gill,4 David J. Stensel,2,5
Keith Tolfrey,2,5 David W. Dunstan,6,7
Kamlesh Khunti,1,3 and Thomas Yates1,2
130 Diabetes Care Volume 39, January 2016
IDF-ADATR
ANSLATIONALSYMPOSIUM

Sedentary behavior, now commonlyconceptualized as sitting during wakinghours with low energy expenditure (1),has recently emerged as an independentdeterminant of morbidity (particularlytype 2 diabetes) and mortality (2–4).Multiple observational studies havealso demonstrated a positive associa-tion between objectivelymeasured sed-entary time and markers of diabetesrisk, independent of the amount ofmoderate-to-vigorous physical activity(MVPA) undertaken (5–7). This suggeststhat sedentary behavior is likely to be adistinct risk factor for type 2 diabetesand a potential target for lifestyle inter-vention. This is important, as individualsat high risk of type 2 diabetes spend;70% of their waking time sedentary,with 25% in light activity and ,5%engaged in MVPA (6). Moreover, theinverse correlation between sedentarybehavior and MVPA is weak (7), furthersuggesting these are independent behav-iors. However, experimental data areneeded to determine whether a causalrelationship exists betweenmodificationsto sedentary time and metabolic health.Recently, experimental studies that
have broken up prolonged sitting withshort periods of light- or moderate-intensity activity have shown a reduc-tion in postprandial glucose and insulinconcentrations in both healthy andoverweight adults (8–11). These studiessuggest that important health-relatedmetabolic processes occur when indi-viduals transition from sitting to move-ment (light and moderate intensity).However, it is unclear whether movingfrom sitting to standing provides a suffi-cient stimulus to elicit metabolic benefits.While there is emerging evidence thatsustained bouts of standing may improveglucose regulation (12,13), it is not clearwhether breaking up prolonged sittingwith intermittent short bouts of standingimproves the metabolic health of individ-uals at high risk of chronic disease.Therefore, the aim of this study was to
establish whether breaking up prolongedsitting through frequent short bouts ofstanding or walking activity modulatespostprandial metabolic responses in indi-viduals at high risk of type 2 diabetes.
RESEARCH DESIGN AND METHODS
Study DesignA balanced incomplete block design wasused for this study (14). Such designs
have been used in pharmaceutical trialsand reduce participant burden whileminimizing the intrasubject effect, thusincreasing the sensitivity of the outcome(15,16). With this design, participantswere randomized to two of the threefollowing treatment conditions: 1) pro-longed, unbroken sitting (7.5 h); 2) pro-longed sitting broken up with standingfor 5 min every 30 min; or 3) prolongedsitting broken up with walking for 5 minevery 30 min (Supplementary Table 1).Regardless of the treatment conditioncarried out on day 1, all participants un-derwent the prolonged sitting protocolon day 2; thus, each treatment conditionwas carried out over 2 consecutive days.As an acute bout of physical activity mayenhance insulin sensitivity for up to 48 h(17), we used aminimumwashout periodof 7 days between each condition (themaximum washout was 22 days).
Participants attended five separatevisits to the Leicester Diabetes Centre,Leicester, U.K. Supplementary Fig. 1 de-scribes the studydesign.One to twoweeksafter an initial familiarization visit, partici-pants were randomized by an indepen-dent third party to one of six sequences,prepared by the study statistician prior torecruitment of the first participant(Supplementary Table 1).
Informed consent was obtained fromall eligible participants, and ethicsapproval was obtained from the North-ampton Research Ethics Committee.
ParticipantsA total of 34 participants were recruitedbetween January 2014 and October2014. Postmenopausal women at highrisk of developing type 2 diabetes wereidentified from studies previously con-ducted within the Leicester DiabetesCentre (18,19). This cohort was includedin order to negate the impact of hor-mone variations and because associa-tions between sedentary behavior andmarkers of cardiometabolic health havepreviously been shown to be stronger inwomen (20).
Eligibility criteria included the follow-ing: overweight or obese (BMI $27.5kg/m2 or $25 kg/m2 if South Asian),postmenopausal women (12 consecutivemonths without menstruation [21]),age 50–75 years with screen-detectedimpaired glucose regulation identifiedwithin the 12 months prior to the invita-tion letter being sent. Impaired glucose
regulation was defined as 2-h post-challenge glucose $7.8 mmol/L to,11.1 mmol/L after a standard oralglucose tolerance test (22) or HbA1c
between 5.7 and 6.4% (39–46 mmol/mol)inclusive (23). Exclusion criteria wereregular purposeful exercise ($150 minof objectively measured MVPA over atypical week), inability to communicatein spoken English, steroid use, knowntype 2 diabetes, or current use of hor-mone replacement medication.
In total, 30 participants were random-ized (Fig. 1). Causes of dropout betweenfamiliarization and randomization aredetailed in Fig. 1. A further eight individ-uals were excluded after randomization,due to cessation of the venous cannulaline, which resulted in,50% of data col-lection (n = 5), illness (n = 2), or a changein personal circumstance (n = 1). This left22 participants who were included inthe analysis. There were no significantdifferences inBMI, age, orHbA1c betweenthose who dropped out or were excludedand those who were included in thestudy.
Familiarization VisitBefore participating in the experimentalprotocol, all participants visited the Leices-ter Diabetes Centre for a familiarizationvisit where they provided informed con-sent. This allowed participants to becomeaccustomed to the walking speed andalso familiarize themselves with theBorg rating of perceived exertion (RPE)scale (24). A venous blood sample wasalso taken for HbA1c, lipid profile, andnonesterified fatty acid (NEFA) analysis.
Body mass (Tanita TBE 611; Tanita,West Drayton, U.K.), waist circumference(midpoint between the lower costalmargin and iliac crest), and heightwere measured to the nearest 0.1 kg,0.5 cm, and 0.5 cm, respectively.
Participants also wore an accelerom-eter (placed on the right anterior axil-lary line) for 7 days after familiarization(GT3X+;ActiGraph, Pensacola, FL) tomea-sure time spent engaged in sedentary,light physical activity, or MVPA underfree-living conditions.
Experimental Regimen OverviewParticipants were asked to record all foodand drink consumed the day before thefirst experimental condition. They werethen asked to replicate this diet beforesubsequent treatments. Participants werealso requested to avoid alcohol, caffeine,
care.diabetesjournals.org Henson and Associates 131

and any MVPA for 2 days prior to eachexperimental condition.Participants arrived at the laboratory
by car (0800 h) after a 10-h fast andhad a cannula fitted into an accessiblevein. A fasting blood sample (9 mL) wasthen taken (time point 21 h) for thequantification of glucose, insulin, NEFA,and triglycerides. Participants wereasked to sit quietly for 60 min, and afurther 9-mL blood sample was taken.A standardized mixed-meal breakfast(croissant, butter, cheese, double cream,skimmed milk, and a meal-replacementdrink [Complan;Nutricia Limited,Wiltshire,U.K.]) was consumed (0900 h; 0 h) provid-ing 0.66 g fat, 0.66 g carbohydrate, and0.4 g protein/kg bodymass (58% fat, 26%carbohydrate, and 16%protein). The timetaken to consume the meal (#15 min)was recorded and replicated in subse-quent conditions. Blood was sampledagain at 30, 60, 120, and 180 min post-prandially. Lunch, with a nutrient compo-sition identical to that of breakfast, wasconsumed at 1200 h, with blood samplesat 30, 60, 120, 180, and 210 min post-prandially. The research staff super-vised participants throughout eachstudy cycle to ensure full compliancewith the trial protocols. Participantsconsumed water ad libitum during thefirst of the experimental conditions and
were then asked to replicate the volumeingested in subsequent conditions.
Experimental Regimens: Day 1
Experimental Condition: Prolonged Sitting
(7.5 h)
During the prolonged sitting condition,walking and standing were restricted(lavatory visits were conducted via awheelchair). Participants sat in a desig-nated room equipped with a chair anddesk and access to books, magazines,and Internet services.
Experimental Condition: Sitting (Total
6.5 h) Plus Standing (Total 60 min)
This followed the same procedure as thesitting condition except that participantswere instructed to break their sitting timeby standing close to their chair for 5 minevery 30 min. Individuals were askedto stand in the same, fixed position.In total, individuals accumulated 12bouts (60 min) of standing.
Experimental Condition: Sitting (Total
6.5 h) Plus Walking (Total 60 min)
This was similar to the standing condi-tion, but sitting time was punctuatedwith 5-min bouts of walking at a self-perceived light intensity on a treadmill(Spazio Forma Folding Treadmill;TechnoGym U.K. Ltd., Bracknell, U.K.).During the first bout of walking, partici-pants were gradually taken up to a speed
that registered between 10 and 12 onthe Borg RPE scale (24), up to a maxi-mum of 4.0 km/h. This speed was fixedand replicated for all other intervals. Intotal, individuals accumulated 12 bouts(60 min) of walking.
The average treadmill speed duringthe walking condition was 3.0 km/h(range 1.5–4.0), with an average RPEscore of 10 (range 8–12).
Experimental Regimens: Day 2(Prolonged Sitting: 7.5 h)For determination of whether any acuteeffects of standing and walking persistedinto the next day, participants returnedto the laboratory (0800 h) after another10-h fast to undergo the prolonged sittingprotocol (including the same standard-ized meals and timings). They were askedto consume exactly the same meal as theprevious evening, while again avoidingalcohol, caffeine, and MVPA.
Sedentary Behavior, Physical Activity,and Posture DataParticipants were asked to wear an accel-erometer (GT3X+) and an activPAL3 pro-fessional physical activity monitor (PALTechnologies, Glasgow, Scotland) duringexperimental conditions and an acceler-ometer for 7 days before each experi-mental condition (Supplementary Fig. 1).
ActivPAL proprietary software (activPALProfessional V5.9.1.1) was used to createprocessed csv files.
For accelerometer data collected overeach 7-day period, nonwear time was de-fined as a minimum of 60 min of continu-ous zero counts, anddayswith at least 10hof wear time were considered valid (5,6).In order to be classed as valid, at least3 days were required (25). Freedson cutpoints were used to categorize activity in-tensity (26). Accelerometer data were an-alyzed using a bespoke tool (KineSoft,version 3.3.76; KineSoft, New Brunswick,Canada [www.kinesoft.org]).
Biochemical AnalysisPlasma glucose and serum triglycerideconcentrations were determined usingstandard enzymatic techniques withcommercially available kits (Beckman,High Wycombe, U.K.). The measurementof plasma NEFA involved a three-stagecolorimetric assay using a commerciallyavailable kit (RX monza; Randox Labora-tories, County Antrim, U.K.). Glucose, tri-glycerides, and NEFA were analyzed onthe day of collection.
Figure 1—Study CONSORT diagram.
132 Breaks in Sitting Time and Metabolic Risk Diabetes Care Volume 39, January 2016

Insulin samples underwent centrifuga-tion to separate plasma within 15 min ofcollection. Plasma was stored at 2808Cand analyzed at the end of data collec-tion using an enzyme immunoassay(Mercodia, Uppsala, Sweden). All mea-surements and analysis were undertakenby individuals blinded to experimentalcondition and independent of the scien-tific advisory team.
Sample SizeThe primary outcome was incrementalpostprandial area under the glucosecurve (iAUC) on day 1. Allowing for anintervention effect of a 20% change inglucose iAUC, a standardized differenceof 1 (where the SD is equivalent to theanticipated intervention effect), a within-person correlation of 0.3, 90%power, andan a of 0.025 (allowing for two primarycomparisons against control conditions),we estimated thatwewould require 12 par-ticipants for a complete three-treatment,three-period crossover design. Twice asmany participants were required for thethree-treatment, two-period balancedincomplete block design (27), and a20% dropout rate was allowed for;therefore, we aimed to recruit 30 partic-ipants with 24 needed to complete thetrial. Estimates were based on previousexperimental research (8) and with con-sideration given to the high-risk nature ofour cohort where a greater effect wasanticipated.
Statistical AnalysesIn line with best practice for acute studieswhere fasting physiology does not change,outcomes were calculated as iAUC ratherthan total AUC (28). Values were deter-mined using the trapezium rule and bysubtracting fasting levels from the overallpostprandial response.Participants were excluded if they had
.50%ofblood samplesmissing across anytreatment condition (n = 5). Missing out-comedata for remaining participantswereimputedusing a regressionmodelwith keypredictor variables (BMI, age, fasting val-ues, ethnicity, and treatment) for eachtime point and outcome. Imputation wasused to correct for verification bias (29).Across all experimental conditions, 11% ofdata values (378 of 3,472) were missingand imputed (Supplementary Table 2).On average, participants were missing amedian of 2 (interquartile range 1–4) val-ues across all experimental days and bio-chemical variables.
Multilevel mixed-effects linear regres-sion was used to look at the differencebetween groups in the continuous out-come measures (glucose, insulin, NEFA,triglycerides) allowing for repeated mea-surements from the same individuals.In these models, treatment was modeledas a fixed factor and participant as a ran-dom factor. The primary analysis involvedcomparing standing and walking againstthe control (prolonged sitting) condition.Tests between treatment conditions(standing vs. walking) were conductedfor exploratory purposes and form a sec-ondary outcome for the study.
All data were analyzed using STATA(version 13.0; StataCorp, College Sta-tion, TX). A P value of,0.05 was consid-ered statistically significant. Descriptivedata are reported as mean 6 SD unlessotherwise stated and as mean6 SEM inFigs. 2 and 3 and Supplementary Tables3–6.
In order to aid interpretation of theresults, a sensitivity analysis was con-ducted to investigate whether resultswere affected by analyzing the totalAUC (including fasting values). Further-more, we also investigated whetherfasting values differed between day 1and day 2 (Supplementary Table 7).
RESULTS
Anthropometric, biochemical, and demo-graphic information of the includedparticipants is displayed in Table 1.
Experimental Regimens: Day 1Biochemical results collected on day 1(for each experimental condition) arepresented in Fig. 2, with the corre-sponding numerical values displayedin Supplementary Table 3.
The mean glucose iAUC response was5.3 6 0.8 mmol/L z h in the prolongedsitting condition. Breaking sitting timewith 5 min of standing, every 30 min,reduced the glucose iAUC by 34%(3.5 6 0.8 mmol/L z h, P = 0.022) com-pared with prolonged sitting. Similarly,walking reduced the glucose iAUC by28% (3.8 6 0.7 mmol/L z h, P = 0.009)compared with prolonged sitting.
A similar pattern of results was ob-served for insulin and NEFA on day 1.The insulin iAUC was reduced by 20%(437.2 6 73.5 mU/L z h, P = 0.045)when sitting time was broken withstanding and by 37% (347.9 6 78.7mU/L z h, P = 0.008) when it was brokenwith walking compared with prolonged
sitting (548.26 71.8 mU/L z h). Breakingsitting time with standing attenuated thesuppression of the NEFA iAUC by 33%(21.06 0.2 mmol/L z h, P = 0.024) and withwalking by 47% (20.86 0.2 mmol/L z h,P = 0.003) compared with prolongedsitting (21.5 6 0.2 mmol/L z h).
There were no significant differ-ences between the standing and walk-ing conditions for any of these outcomes(glucose P = 0.717, insulin P = 0.376, NEFAP = 0.398).
Conversely, neither standing (6.2 60.8 mmol/L z h) nor walking (6.1 6 0.8mmol/L z h) significantly reduced thetriglyceride iAUC compared with thesitting condition (5.6 6 0.7 mmol/L z h)on day 1.
Experimental Regimens: Day 2(Prolonged Sitting: 7.5 h)Seventeen participants completed thesecond day owing to problems withintravenous cannulation. Biochemicalresults for day 2 are presented inFig. 3, with the corresponding numericalvalues displayed in SupplementaryTable 4.
Day 2 yielded a mean net glucoseresponse of 4.8 6 0.6 mmol/L z h if par-ticipants had undertaken the sittingcondition on day 1. Breaking sittingtime with standing on day 1 elicited aresponse of 3.9 6 0.8 mmol/L z h onday 2 (19% reduction in iAUC comparedwith sitting, P = 0.039). Similarly, walkingcarried out on day 1 reduced the glucoseiAUCby17%onday2 (4.060.7mmol/L z h,P = 0.027). There was no significantdifference between the standing andwalking conditions (P = 0.877).
The mean net insulin response was464.6 6 70.2 mU/L z h if participantshad undertaken the sitting conditionon day 1. The significant results forstanding on day 1 did not persist intothe second day (363.5 6 57.5 mU/L z h,P = 0.325). In contrast, results for walkingpersisted into day 2 (354.3657.3mU/L z h,P = 0.038). There was no significant differ-ence between the standing and walkingconditions (P = 0.529).
There was no difference in triglycerideresponse between the prolonged sitting(7.2 6 0.5 mmol/L z h) and standing(7.2 6 0.8 mmol/L z h, P = 0.603) con-ditions on day 2. Results for the walkingcondition (6.0 6 0.7 mmol/L z h, P =0.077) neared significance comparedwith prolonged sitting.
care.diabetesjournals.org Henson and Associates 133
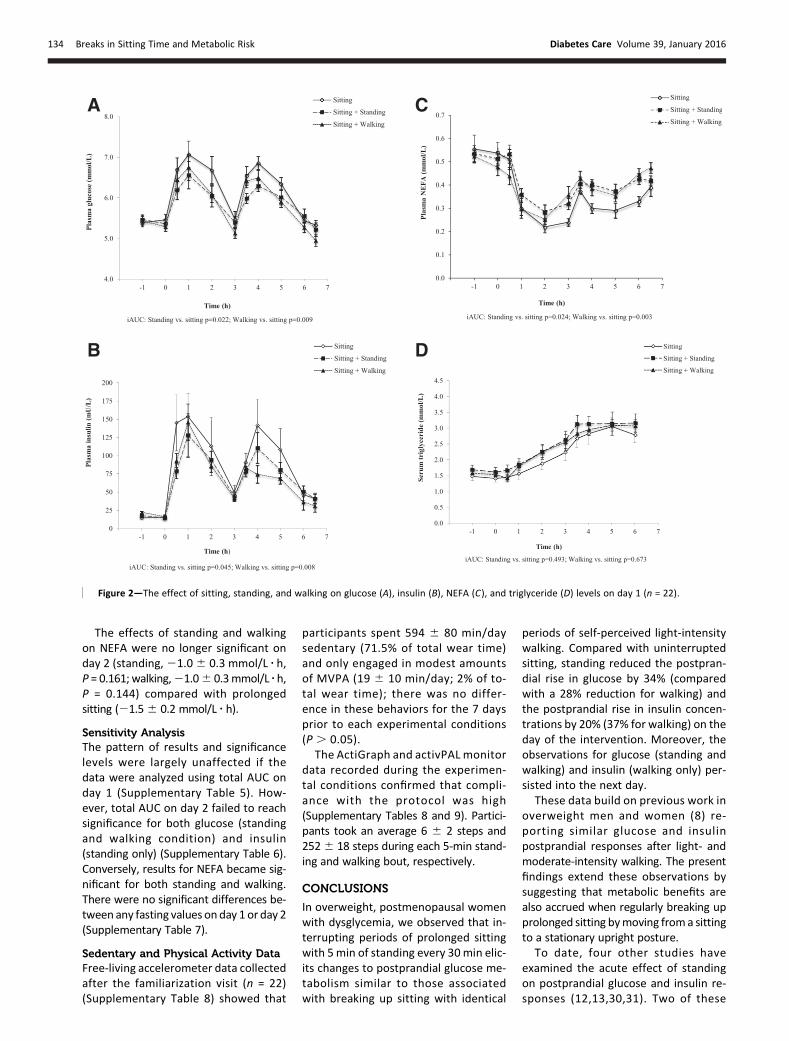
The effects of standing and walkingon NEFA were no longer significant onday 2 (standing,21.06 0.3 mmol/L z h,P = 0.161; walking,21.06 0.3mmol/L z h,P = 0.144) compared with prolongedsitting (21.56 0.2 mmol/L z h).
Sensitivity AnalysisThe pattern of results and significancelevels were largely unaffected if thedata were analyzed using total AUC onday 1 (Supplementary Table 5). How-ever, total AUC on day 2 failed to reachsignificance for both glucose (standingand walking condition) and insulin(standing only) (Supplementary Table 6).Conversely, results for NEFA became sig-nificant for both standing and walking.There were no significant differences be-tween any fasting values onday 1 or day 2(Supplementary Table 7).
Sedentary and Physical Activity DataFree-living accelerometer data collectedafter the familiarization visit (n = 22)(Supplementary Table 8) showed that
participants spent 594 6 80 min/daysedentary (71.5% of total wear time)and only engaged in modest amountsof MVPA (19 6 10 min/day; 2% of to-tal wear time); there was no differ-ence in these behaviors for the 7 daysprior to each experimental conditions(P . 0.05).
The ActiGraph and activPAL monitordata recorded during the experimen-tal conditions confirmed that compli-ance with the protocol was high(Supplementary Tables 8 and 9). Partici-pants took an average 6 6 2 steps and2526 18 steps during each 5-min stand-ing and walking bout, respectively.
CONCLUSIONS
In overweight, postmenopausal womenwith dysglycemia, we observed that in-terrupting periods of prolonged sittingwith 5min of standing every 30min elic-its changes to postprandial glucose me-tabolism similar to those associatedwith breaking up sitting with identical
periods of self-perceived light-intensitywalking. Compared with uninterruptedsitting, standing reduced the postpran-dial rise in glucose by 34% (comparedwith a 28% reduction for walking) andthe postprandial rise in insulin concen-trations by 20% (37% for walking) on theday of the intervention. Moreover, theobservations for glucose (standing andwalking) and insulin (walking only) per-sisted into the next day.
These data build on previous work inoverweight men and women (8) re-porting similar glucose and insulinpostprandial responses after light- andmoderate-intensity walking. The presentfindings extend these observations bysuggesting that metabolic benefits arealso accrued when regularly breaking upprolonged sitting bymoving froma sittingto a stationary upright posture.
To date, four other studies haveexamined the acute effect of standingon postprandial glucose and insulin re-sponses (12,13,30,31). Two of these
Figure 2—The effect of sitting, standing, and walking on glucose (A), insulin (B), NEFA (C), and triglyceride (D) levels on day 1 (n = 22).
134 Breaks in Sitting Time and Metabolic Risk Diabetes Care Volume 39, January 2016

found that breaking prolonged sittingwith regular standing breaks had noimpact on postprandial glucose (30,31)or insulin (30) in young healthy men.In contrast, alternating 30-min bouts ofsitting and standing throughout the dayhas been shown to significantly reducethe iAUC between trial conditions forpostprandial glucose (11% reductioncompared with prolonged sitting) (12).A nonrandomized office-based studyalso found that glucose levels werereduced by 43% following an afternoonof standing compared with seatedcomputer work (13). The fact that ourstudy reported effects that were to-ward the upper end of those reportedin previous studies, while using substan-tially smaller doses of standing, is likely tobe driven by differences in sample char-acteristics and potentially the increased
frequency in interruptions to prolongedsitting. Other studies have been con-ducted in groups that are broadly repre-sentative of the general population (age,50 years, BMI,30 kg/m2), whereas ourparticipants were older with existing dys-glycemia who represent those likely to bereferred into diabetes prevention path-ways. This is particularly importantgiven the prominence of national andinternational strategies highlightingthe need for identification and subse-quent referral of individuals at highrisk of type 2 diabetes (32,33).
Another novel finding was that reduc-tions in glucose and insulin responsesafter the breaking up of prolonged sit-ting were maintained into the secondobservation day. Glucose remained19% lower after the standing condi-tion and 17% lower after the walking
condition. Similarly, insulin remained24% lower after the walking condition.These findings are consistent with a pre-vious experimental study carried out inobese adults showing that a single boutof modest exercise (50% VO2 peak on astationary cycle ergometer) increased in-sulin sensitivity into the next day (11). Asimilar study also demonstrated thatthe morning after a prolonged bout ofsitting (17 h), participants exhibited asignificant reduction (39%) in whole-body insulin action compared with up-right light-intensity activity (10). Ourfindings indicate that an even loweractivity stimulus (e.g., standing) mayyield metabolic advantages for a mini-mum of 24 h.
The mechanisms underpinning theeffects of standing and walking on glu-cose and insulin levels require further
Figure 3—The effect of sitting, standing, andwalkingon glucose (A), insulin (B), NEFA (C), and triglyceride (D) levels onday 2 (n= 17).Mean6 SEMglucose,insulin, NEFA, and triglycerides on day 1 (Fig. 2A–D) and day 2 (A–D) measured over a 6.5-h period during the prolonged sitting, sitting and standing, andsitting and walking conditions. Standardized meals provided at 0 h and 3 h.
care.diabetesjournals.org Henson and Associates 135

elucidation. Acute and chronic light-intensity physical activity training studieshave consistently demonstrated im-provements in markers of glycemic con-trol in those with dysglycemia, withsimilar effects observed between light-and moderate-intensity exercise trainingregimes, when matched for total volume(34).However, it has not beenestablishedwhether the specific mechanisms in-volved in enhancing peripheral glucoseuptake that have been shown for MVPA,primarily through the translocation andturnover of GLUT4 (35), are observedwith walking at a self-perceived light in-tensity or standing.The attenuated postprandial suppres-
sion in plasma NEFA concentration ob-served on day 1 of this study for both thestanding and walking is likely to reflectan increase in the lipolysis of triglycer-ides stored in adipose tissue in order tosupply the working muscle. Moreover,the reduction of insulin in the standingand walking conditions suggests thatsuppression of lipolysis, driven by theantilipolytic properties of insulin (36),may have been reduced in these con-ditions. Previous studies have shownthat during low-intensity exercise, adi-pose tissue lipolysis increases four- to
fivefold above resting levels (37). Othershave also reported that lipolysis and mo-bilization of NEFA resulting from exerciseare related to, and may be enhanced by,hormonal changes, particularly increasedcatecholamines levels (38).
We found no change in the triglycer-ide iAUC for the standing and walkingconditions on either day 1 or day 2 ofthe experimental regimens. The nonsig-nificant results on day 1 are consistentwith previous studies that have shownno effect (9,12). Decreased triglyceridelevels were observed on day 2 afterthe walking condition, although thechanges were not statistically signifi-cant (17% reduction compared with sit-ting, P = 0.077). However, themagnitudeof the effect for walking on day 2 wasconsistent with previous studies demon-strating that walking (both intermittentand continuous) elicited reductions inthe postprandial triglyceride levelsthe following day (16–23% reduction).Our results corroborate with other find-ings suggesting that standing is not a suf-ficient stimulus to reduce postprandialtriglyceride levels (12,30).
This study has a number of strengths.Firstly, we studied postmenopausalwomen at high risk of type 2 diabetes,
so the findings are directly relevant forpublic health guidance and interventionsfor metabolic risk reduction. Secondly,this is the first study to directly comparethe effects of breaking up prolonged sit-ting with standing andwalking, demonstrat-ing that they both induce cardiometabolicbenefits.Moreover, by using a 2-day pro-tocol we were able to determine thatthe acute effects of standing and walk-ing persisted into the following day. Ourstudy also highlights the importanceof reporting both iAUC and total AUCin experimental studies that assessoutcomes over several days. Althoughresults on day 1 were unaffected bythe analysis method, there were smalldifferences in interpretation on day 2.Notwithstanding the nonsignificant dif-ferences in mean fasting levels on day 2,it is possible that the intervention condi-tions had a subtle effect on fasting path-ophysiology that subsequently influencedtotal AUC. As such, results should beinterpreted in relation to the methodused; for this study, the primary focuswas on the postprandial response (iAUC).Finally, all measurements were per-formed by the same team of trainedstaff, following identical standard op-erating procedures, and analysis wasconductedby individuals blinded to treat-ment allocation.
This study has several important lim-itations. Firstly, the acute nature of thetrial prohibits inferences about longer-term chronic effects. Secondly, the testmeals used were relatively high in fat(58% of total energy), and further stud-ies are needed to determine whetherthe findings persist when meals with amacronutrient composition more repre-sentative of dietary recommendationsare consumed. However, the macronu-trient composition of food was almostidentical to that which may be plausiblyconsumed by the general populationthrough a meal or as a snack. For exam-ple, based on an 80-kg individual, thestandardized meal used in this study isequivalent to 46 g brown bread, 6 g but-ter, 100 g bacon, and a 59-g chocolatebar (39). Studies have also indicated thatthe recommended daily intake of fat isoften exceeded by many adults (40). Wealso relied on participants to recordand standardize their own food intakethe day before and in between eachexperimental condition for practicalreasons; therefore, misreporting is
Table 1—Metabolic, demographic, and anthropometric characteristics at baselineand dietary and physical activity variables during the study (n = 22)
Baseline characteristicsAge (years) 66.6 6 4.7Current smoker 1 (4.5)BMI (kg/m2) 32.9 6 4.7Waist circumference (cm) 102 6 9.0Body mass (kg) 83.6 6 11.7Total cholesterol (mmol/L) 5.60 6 0.87Triglycerides (mmol/L) 2.17 6 0.86NEFA (mmol/L) 0.44 6 0.24HbA1c (%) 5.8 6 0.2HbA1c (mmol/mol) 40 6 2.3Fasting plasma glucose (mmol/L) 5.4 6 0.4Lipid-lowering medication 5 (22.7)b-Blockers 5 (22.7)ACE inhibitors 3 (13.6)EthnicityWhite European 20 (90.9)Black and minority ethnic 2 (9.1)
In-study characteristicsDietTotal energy intake (kcal/day) 1,717 6 234Total fat (energy %) 58 6 0.2Total carbohydrate (energy %) 26 6 0.1Total protein (energy %) 16 6 0.2
Walking speed (km/h) 3.0 (1.5–4.0)Borg RPE score 10 (8–12)
Data are mean 6 SD, n (%), or mean (range).
136 Breaks in Sitting Time and Metabolic Risk Diabetes Care Volume 39, January 2016

possible. Similarly, no physical activitydata were recorded between day 1 andday 2. Thirdly, the prolonged nature ofthe sitting condition may not reflecthabitual behavior for many individualswhere some standing or light move-ment would be expected over an 8 hperiod. Nonetheless, it was importantto initially establish a proof of conceptwhere standing and walking effects areobserved compared with a prolongedstandardized bout of sitting. Futurestudies should also focus on whetherthe effects observed in this study arereplicated under free-living scenarios.The reduced sample size (and subsequentunderpowered comparison), particularlypertaining to comparisons on day 2, in-creased the risk of a type 2 error andthus limits the conclusions that can bedrawn over the second day. Furthermore,the study was not designed to assessdifferences between the standing andwalking conditions, which were in-cluded as a secondary outcome. Finally,further research is needed to deter-mine whether the effects can be gener-alized to men and premenopausalwomen.In conclusion, this study demonstrates
that breaking up prolonged sitting with5-min bouts of standing or walking at aself-perceived light intensity reducespostprandial glucose, insulin, and NEFAresponses in postmenopausal women athigh risk of type 2 diabetes. This simple,behavioral approach could inform futurepublic health interventions aimed at im-proving the metabolic profile of dysglyce-mic individuals. Habitual standing andlight-intensity physical activity are behav-iorally more ubiquitous than MVPA andmay therefore provide appealing inter-ventional targets in the promotion ofmetabolic health. However, future behav-ioral intervention studies are needed toinvestigate themost effectivemethods ofreducing habitual sedentary behaviorwithin a prevention context and to assessgeneralizability beyond postmenopausalwomen.
Acknowledgments. The authors thank RosDowning, Steve Hartshorn, Carrie Wilson, TimSkelton, Hamid Mani, David Webb, Zin ZinHtike, Sarah Bunnewell, Jo Paul, Balu Webb,Helen Waller, and Ellen Edwardson for theirassistance throughout the study. A specialthank you must also go to all participantswho took the time to take part.
Funding. The research was supported by theNational Institute for Health Research (NIHR)Leicester-Loughborough Diet, Lifestyle andPhysical Activity Biomedical Research Unit,which is a partnership between UniversityHospitals of Leicester National Health ServiceTrust, Loughborough University, and theUniversity of Leicester; NIHR Collaborationsfor Leadership in Applied Health Research andCare, Leicestershire, Northamptonshire, andRutland (NIHR CLAHRC–LNR) and East Mid-lands (NIHR CLAHRC EM); and the Universityof Leicester Clinical Trials Unit.
The views expressed are those of the au-thors and not necessarily those of the NationalHealth Service, the NIHR, or the Department ofHealth.Duality of Interest.M.J.D., T.Y., and K.K. (Chair)aremembers of the National Institute for Healthand Care Excellence Public Health Guidance(PH38) Preventing type 2 diabetes: risk identifi-cation and interventions for individuals at highrisk. No other potential conflicts of interest rel-evant to this article were reported.Author Contributions. J.H., M.J.D., D.H.B.,C.L.E., J.M.R.G., D.J.S., K.T., D.W.D., K.K., andT.Y. made significant contributions to theconcept and subsequent design of the study,made substantial contributions to analysis andinterpretation, provided critical revision of themanuscript, and approved the final version ofthe manuscript. J.H. and T.Y. wrote the manu-script. J.H. supervised the study. J.H. is the guar-antorofthisworkand,assuch,hadfullaccess toallthe data in the study and takes responsibility forthe integrity of the data and the accuracy of thedata analysis.Prior Presentation. Parts of this study werepresented at the International Diabetes Fed-eration’s 2015 World Diabetes Congress, Van-couver, Canada, 30 November–4 December2015.
References1. Sedentary Behaviour Research Network. Let-ter to the editor: standardized use of the terms“sedentary” and “sedentary behaviours.” ApplPhysiol Nutr Metab 2012;37:540–5422. Wilmot EG, Edwardson CL, Achana FA, et al.Sedentary time in adults and the associationwith diabetes, cardiovascular disease anddeath: systematic review and meta-analysis.Diabetologia 2012;55:2895–29053. Biswas A, Oh PI, Faulkner GE, et al. Sedentarytime and its association with risk for diseaseincidence, mortality, and hospitalization inadults: a systematic review and meta-analysis.Ann Intern Med 2015;162:123–1324. Edwardson CL, Gorely T, Davies MJ, et al.Association of sedentary behaviour with meta-bolic syndrome: a meta-analysis. PLoS One2012;7:e349165. Healy GN, Matthews CE, Dunstan DW,Winkler EA, OwenN. Sedentary time and cardio-metabolic biomarkers in US adults: NHANES2003-06. Eur Heart J 2011;32:590–5976. Henson J, Yates T, Biddle SJ, et al. Associationsof objectively measured sedentary behaviour andphysical activity with markers of cardiometabolichealth. Diabetologia 2013;56:1012–10207. Healy GN, Wijndaele K, Dunstan DW, et al.Objectively measured sedentary time, physical
activity, and metabolic risk: the AustralianDiabetes, Obesity and Lifestyle Study (AusDiab).Diabetes Care 2008;31:369–3718. Dunstan DW, Kingwell BA, Larsen R, et al.Breaking up prolonged sitting reduces postpran-dial glucose and insulin responses. Diabetes Care2012;35:976–9839. Peddie MC, Bone JL, Rehrer NJ, Skeaff CM,Gray AR, Perry TL. Breaking prolonged sittingreduces postprandial glycemia in healthy, normal-weight adults: a randomized crossover trial. Am JClin Nutr 2013;98:358–36610. Stephens BR, Granados K, Zderic TW,Hamilton MT, Braun B. Effects of 1 day of in-activity on insulin action in healthy men andwomen: interaction with energy intake. Metab-olism 2011;60:941–94911. Newsom SA, Everett AC, Hinko A, HorowitzJF. A single session of low-intensity exercise issufficient to enhance insulin sensitivity into thenext day in obese adults. Diabetes Care 2013;36:2516–252212. Thorp AA, Kingwell BA, Sethi P, Hammond L,Owen N, Dunstan DW. Alternating bouts of sit-ting and standing attenuate postprandial glu-cose responses. Med Sci Sports Exerc 2014;46:2053–206113. Buckley JP, Mellor DD, Morris M, Joseph F.Standing-based office work shows encourag-ing signs of attenuating post-prandial glycae-mic excursion. Occup Environ Med 2014;71:109–11114. Senn SS. Incomplete block designs. In Cross-over Trials in Clinical Research. 2nd ed. West Sus-sex, England, John Wiley & Sons, 2003, p. 21115. Peng JZ, Denney WS, Musser BJ, et al.A semi-mechanistic model for the effects of anovel glucagon receptor antagonist on glucagonand the interaction between glucose, glucagon,and insulin applied to adaptive phase II design.AAPS J 2014;16:1259–127016. Henry RR, Mudaliar S, Ciaraldi TP, et al.Basal insulin peglispro demonstrates preferen-tial hepatic versus peripheral action relative toinsulin glargine in healthy subjects. DiabetesCare 2014;37:2609–261517. Mikines KJ, Sonne B, Farrell PA, Tronier B,Galbo H. Effect of physical exercise on sensitiv-ity and responsiveness to insulin in humans. AmJ Physiol 1988;254:E248–E25918. Yates T, Davies MJ, Henson J, et al. Walkingaway from type 2 diabetes: trial protocol of acluster randomised controlled trial evaluating astructured education programme in those athigh risk of developing type 2 diabetes. BMCFam Pract 2012;13:4619. Gray LJ, Khunti K, Williams S, et al.; Let’sPrevent Collaborators. Let’s prevent diabetes:study protocol for a cluster randomised con-trolled trial of an educational intervention in amulti-ethnic UK population with screen de-tected impaired glucose regulation. CardiovascDiabetol 2012;11:5620. Owen N, Healy GN, Matthews CE, DunstanDW. Too much sitting: the population healthscience of sedentary behavior. Exerc Sport SciRev 2010;38:105–11321. Tamimi RM, Hankinson SE, Chen WY,Rosner B, Colditz GA. Combined estrogen andtestosterone use and risk of breast cancer inpostmenopausal women. Arch Intern Med2006;166:1483–1489
care.diabetesjournals.org Henson and Associates 137

22. International Diabetes Federation. Definitionand diagnosis of diabetesmellitus and intermediatehyperglycaemia [article online], 2006. Availablefrom https://www.idf.org/webdata/docs/WHO_IDF_definition_diagnosis_of_diabetes.pdf.Accessed 6 March 201523. American Diabetes Association. Standardsof medical care in diabetesd2012. DiabetesCare 2012;35(Suppl. 1):S11–S6324. Borg GA. Psychophysical bases of perceivedexertion. Med Sci Sports Exerc 1982;14:377–38125. Trost SG, McIver KL, Pate RR. Conductingaccelerometer-based activity assessments infield-based research. Med Sci Sports Exerc2005;37(Suppl.):S531–S54326. Freedson PS, Melanson E, Sirard J. Calibra-tion of the computer science and applications,inc. accelerometer. Med Sci Sports Exerc 1998;30:777–78127. Senn SJ, Lillienthal J, Patalano F, Till D. Anincomplete blocks cross-over in asthma: A casestudy in collaboration. In Cross-over ClinicalTrials. Vollmar J, Hothorn LA, Eds. Stuttgart,Fischer, 1997, p. 3–2628. Le Floch JP, Escuyer P, Baudin E, Baudon D,Perlemuter L. Blood glucose area under thecurve. Methodological aspects. Diabetes Care1990;13:172–175
29. Janssen KJ, Donders AR, Harrell FE Jr, et al.Missing covariate data in medical research: to im-pute is better than to ignore. J Clin Epidemiol 2010;63:721–72730. Miyashita M, Park JH, Takahashi M, SuzukiK, Stensel D, Nakamura Y. Postprandial lipae-mia: effects of sitting, standing and walking inhealthy normolipidaemic humans. Int J SportsMed 2013;34:21–2731. Bailey DP, Locke CD. Breaking up prolongedsitting with light-intensity walking improves post-prandial glycemia, but breaking up sitting withstandingdoesnot. J SciMedSport 2015;18:294–29832. National Institute for Health and Care Ex-cellence. Preventing type 2 diabetes: risk iden-tification and interventions for individuals athigh risk [article online], 2012. Available fromhttps://www.nice.org.uk/guidance/ph38. Ac-cessed 24 February 201533. American Diabetes Association. Standards ofmedical care in diabetesd2015. Diabetes Care2015;38(Suppl. 1)S5–S8734. Hansen D, Dendale P, Jonkers RA, et al. Con-tinuous low- tomoderate-intensity exercise train-ing is as effective as moderate- to high-intensityexercise training at lowering blood HbA(1c) inobese type 2 diabetes patients. Diabetologia2009;52:1789–1797
35. Richter EA, Hargreaves M. Exercise, GLUT4,and skeletal muscle glucose uptake. Physiol Rev2013;93:993–101736. Karpe F, Dickmann JR, Frayn KN. Fattyacids, obesity, and insulin resistance: timefor a reevaluation. Diabetes 2011;60:2441–244937. Horowitz JF. Fatty acid mobilization fromadipose tissue during exercise. Trends Endocri-nol Metab 2003;14:386–39238. Henderson GC, Fattor JA, Horning MA,et al. Lipolysis and fatty acid metabolism inmen and women during the postexerciserecovery period. J Physiol 2007;584:963–98139. National Health Service. Calorie checker [In-ternet], 2014. Available from http://www.nhs.uk/LiveWell/weight-loss-guide/Pages/calorie-counting.aspx. Accessed 7 January 201540. Public Health England and the Food Stan-dards Agency. The National Diet and Nutritionsurvey data assesses the diet, nutrient intakeand nutritional status of the general populationin the UK [article online], 2014. Available fromhttps://www.gov.uk/government/uploads/system/uploads/attachment_data/file/310995/NDNS_Y1_to_4_UK_report.pdf. Accessed 7January 2015
138 Breaks in Sitting Time and Metabolic Risk Diabetes Care Volume 39, January 2016
![1860 February 2 ? Box 39, No. 130 - ASCSA · 10704 G . . . 1860 February 2 ? Box 39, No. 130 33002 G […] ? 1888 June 1 Vienna (Austria) Box 102, No. 246 ... 20540 Gazette d'Augsburg](https://img.dokumen.tips/doc/110x75/5c012dad09d3f20f068c4894/1860-february-2-box-39-no-130-10704-g-1860-february-2-box-39.jpg)




























