Embed Size (px)
Citation preview

1

2
1. To understand JNC-7 guidelines that are pertinent to our practice.
2. To appreciate the importance and impact of ALLHAT as it relates to a cost effective approach to controlling hypertension.
3. To underscore the role of lifestyle changes in managing hypertension and how to influence patient behavior in this regard.

3
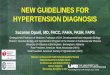
Not at Goal Blood Pressure (<140/90 mmHg)
Initial Drug Choices
Drug(s) for the compelling indications
Other antihypertensive drugs (diuretics, ACEI, ARB, BB, CCB)
as needed.
With Compelling Indications
Lifestyle Modifications
Stage 2 Hypertension (SBP >160 or DBP >100 mmHg)
2-drug combination for most (usually thiazide-type diuretic and
ACEI, or ARB, or BB, or CCB)
Stage 1 Hypertension(SBP 140–159 or DBP 90–99 mmHg)
Thiazide-type diuretics for most. May consider ACEI, ARB, BB, CCB,
or combination.
Without Compelling Indications
Not at Goal Blood Pressure
Optimize dosages or add additional drugs until goal blood pressure is achieved.
Consider consultation with hypertension specialist.

4
First, let’s focus on initial drug choices. For patients who need medication to help control their blood pressure, specific recommendations are:1.Thiazide-type diuretics should be initial drug therapy for most, either alone or combined with other drug classes. If SBP is >20 mmHg above goal or DBP is >10 mm Hg above goal, initiate therapy with two agents. 2.Patients already on antihypertensive medication whose BP is not controlled should have dosages increased or medications added until both SBP and DBP are under control.3.Most patients will require two or more antihypertensive drugs to achieve goal BP.
Talking points about previous slide

5
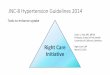
Diuretics
ACE Inhibitors & ARBS
Calcium Channel Blockers
Can add: Spironolactone, α-blockers, alternative CCBs, vasodilators,
β-blockers, central agents, and/or reserpine

6
The cornerstones of initial hypertension treatment can be depicted in the form of a triad where Diuretics as a class should be viewed at the top in terms of being the first choice for single drug therapy. However, each of the other cornerstones are also considered reasonable initial choices if there is a problem with diuretic therapy. In addition, the cornerstones may be combined with each other before adding what is highlighted in the box in the middle of the triangle.
Talking points about previous slide

Red
ucti
on in
SB
P (
mm
Hg)
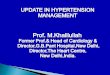
Carter BL, Ernst ME, Cohen JD. Hypertension 2004;43:4-9.
50 mg HCTZ approximates 25 to 37.5 mg chlorthalidone
7

8
The previous slide illustrates the dose response curve for HCTZ and chlorthalidone. The dose response curve for BP lowering with these drugs is clearly linear up to well above 50 mg/day. However, at every point of the dose response curve you can see that Chlorthalidone is clearly more potent than HCTZ in BP reduction.
With chlorthalidone, potassium-wasting tends to be more prominent when compared dose-for-dose with HCTZ. Therefore, dosing of 12.5-25 mg is viewed as a compromise between antihypertensive efficacy and potassium-wasting.
Talking points about previous slide

Volume Distribution
Relative Potency*
Oral Bioavail
Onset (h)
Peak (h)
Half-life (h)
Duration (h)
HCTZ 3-4 L/kg
40% protein bound
1 ~70% 2 4-6 6-9 (single dose)8-15 (long-term
dosing)
12 (single dose)16-24(long-term
dosing)
Chlorthalidone 3-13 L/kg
75% protein bound
98% distribution
into RBC
1 ~65% 2-3 2-6 40(single dose)45-60(long-term
dosing)
24-48(single dose)48-72(long-term
dosing)
Indapamide 20 ~93% 1-2 <2 14 Up to 36
Carter BL, Ernst ME, Cohen JD. Hypertension 2004;43:4-9.. 9

10
In the previous slide, the key point in comparing hydrochlorothiazide to chlorthalidone is that chlorthalidone has a duration of action that is 2 to 3 times longer than that of HCTZ . This fact is what contributes to the higher potency of chlorthalidone when compared to HCTZ.
Talking points about previous slide

• Duration of action of generic oral clonidine is short (T1/2 = 7-11 hrs) requiring TID dosing.
• Clonidine patches are expensive.
• Guanfacine (Tenex) though little used has been around since the 1970’s and FDA-approved in the mid 1980’s.Pharmacodynamically identical to clonidine, but its
12-23 hour half-life allows true once-a-day dosing.
1-3 mg once-a-day is comparable to clonidine 0.1-0.3 mg TID.
Side effect profile is similar to clonidine.
11

• Hydralazine 50-100 BIDRequires sympatholytic and diuretic in regimen
Higher doses raise risk of drug-SLE (arthritis, pericardial effusion, renal disease is rare)
Useful in women on top of CCBs to reduce minoxidil need
• Spironolactone 25-100 mg/dayUseful in resistant HTN, especially with sleep apneaAdverse effects:
Gynecomastia and other antiandrogen effectsHyperkalemia, especially with RAASI, beta blockers, DM,
CKDEplerenone good substitute, but more expensive and
contraindicated in CKD
12

Compelling Indications for Specific Drug Classes
BB, beta blocker; ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker;CCB, calcium channel blocker; AA, aldosterone antagonist; HF, Heart Failure;MI, myocardial infarction; CAD, coronary artery disease; DM, diabetes mellitus Modified from JNC 7. JAMA. 2003;289:2560-2572.
Heart Failure
Post MI
CAD risk
Diabetes Mellitus
Renal disease
Recurrent strokeprevention
BB
ACEI
ARB
CCB
AADiuretic

14
For patients with certain conditions co-morbid with hypertension, there are compelling indications for specific drug choices that provide dual benefit for the patient.
Talking points about previous slide

• β-blockers are clearly indicated in hypertensives with Heart Failure, Coronary Heart Disease, and when needed for additional BP treatment
• Current clinical outcome data base does not support prescribing β-blockers as initial treatment over THZ/CCB/RASI
• It is not clear whether newer β-blockers (e.g. carvedilol and nebivolol) should be considered differently without hard clinical outcome data?
15

• Diuretic (and sympatholytic if HR > 70) will be added to vasodilator for BP control
• Furosemide is the diuretic of choice if eGFR < 35 ml/min/1.73 m2
Note: The combination of diltiazem and a beta blocker presents significant risk of heart block and heart failure.
16

• ACEIs/ARBs should be considered first in patients (including Blacks) with nephropathy (especially with proteinuria) and/or heart failure.
• Available data suggest that RAS inhibitors are less effective in lowering BP in Black hypertensives in the absence of adequate doses of a diuretic or CCB (and in preventing clinical outcomes).
• ACEI also carry increased of angioedema, especially in Blacks.
• In the absence of heart failure or CKD, particularly in Black hypertensives, beta blockers, ACEIs, and ARBs should be prescribed only in combination with adequate doses of thiazide-type diuretics or calcium channel blockers.
17

• The ACCORD study, which ended in 2009, tested treatment approaches to determine the best ways to decrease the high rate of major CVD events – heart attack, stroke or death from CVD – among type 2 diabetics who had high risk of having a CVD event, like heart attack or stroke.
• One of the arms of ACCORD looked at intensive lowering of BP (<120/80) compared to standard BP treatment (<140/90).
• ACCORD demonstrated that standard BP treatment was just as good as intensive treatment in hypertensive diabetics with respect to cardiovascular outcomes.
18

AntihypertensiveTrial Design• Randomized, double-blind, clinical trial of 42,418 participants with
high blood pressure comparing 4 commonly-used antihypertensives.
• ALLHAT investigated whether there was a difference in fatal CHD & nonfatal MI among patients randomized to CCB, ACEI, or alpha-blocker compared to a diuretic.
• ALLHAT also examined differences in secondary endpoints, including:
– All-cause mortality, stroke, combined CHD (primary outcome, coronary revascularization, hospitalized angina)
– combined CVD (combined CHD, stroke, other treated angina, HF [fatal, hospitalized, or treated non-hospitalized], and peripheral arterial disease)
– renal endpoints, and cancer19

Baseline Follow-upN 42,418 Known alive 82%Mean SBP/DBP 146 / 84 Confirmed dead 15%Mean age, y 67 Lost / refused 3%Black, % 36 Person-years
(% obs/exp)99%
Women, % 47
Current smoking % 22
History of CHD, % 26
Type 2 diabetes, % 36
On antihypertensive treatment, % 92
20

21
The ALLHAT cohort had a mean baseline blood pressure of 146/84 mm Hg. The mean age was 67 years; 36% were Black, 47% were women, 22% were current cigarette smokers, 26% had a history of CHD, and 36% were diabetic. 92% were on antihypertensive medications at entry.
Talking points about previous slide

22
BP Results by Treatment Group
Compared to chlorthalidone:
SBP significantly higher in the amlodipine group (~1 mm Hg) and the lisinopril group (~2 mm Hg).
Compared to chlorthalidone:
DBP significantly lower in the amlodipine group (~1 mm Hg), similar in the lisinopril group.
ALLHAT

23
Illustrated in the two graphs is that blood pressure results demonstrate that:
1.Chlorthalidone, amlodipine, and lisinopril all lowered BP from baseline levels.
2.Chlorthalidone was best in lowering systolic BP.
3.Amlodipine was best in lowering diastolic BP.
Talking points about previous slide

24
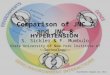
Amlodipine / Chlorthalidone Lisinopril / Chlorthalidone
CHD 0.98 (0.91, 1.08) 0.99 (0.91, 1.08)
Death 0.96 (0.89, 1.02) 1.00 (0.94, 1.08)
CCHD 1.00 (0.94, 1.07) 1.05 (0.98, 1.11)
Stroke 0.93 (0.82, 1.06) 1.15 (1.02, 1.30)
CCVD 1.04 (0.99, 1.09) 1.10 (1.05, 1.16)
HF1.38 (1.25, 1.52) 1.19 (1.07, 1.31)
Summary of CV OutcomesRelative Risks and 95% CIALLHAT

25
As you can see on the previous slide, for the primary endpoint of fatal CHD and nonfatal MI, these drugs did not differ from one another. Thus the older drug class, diuretics, was not shown to be inferior to the newer classes. Similarly, in all secondary endpoints, chlorthalidone was unsurpassed, and, in fact when one looks at heart failure, chlorthalidone was clearly better than the newer classes.
Talking points about previous slide

Results were consistent across age, race, gender, and baseline diabetes subgroups, except: Stroke
Black L/C RR (95% CI) = 1.40 (1.17 – 1.68) Non-Black L/C RR (95% CI) = 1.00 (0.85 – 1.17)
Combined CVD Black L/C RR (95% CI) = 1.19 (1.09 – 1.30) Non-Black L/C RR (95% CI) = 1.06 (1.00 – 1.13)
26
ALLHAT

27
The results were consistent across age, race, gender and baseline diabetes subgroups, except that the results were even more compelling for Black patients.
Talking points about previous slide

28
ALLHAT results can have a major impact on the nation’s medication expenditures. Diuretic use declined from 56% to 27% of
antihypertensive prescriptions during the period between1982 and 1992.
There could have been $3.1 billion in savings in the estimated cost to society for antihypertensive drugs had the prescription pattern not changed from the 1982 level of prescribing diuretics.
ALLHAT

29
ALLHAT addressed the question of whether “newer types of antihypertensive agents, which are currently more costly, are as good as or better than diuretics in reducing CHD incidence and progression.” The result that the diuretic did at least as good and, in some cases, better than the newer drugs, is good news for patients, because the high cost of medication may be a barrier to treatment for some. Given that thiazide diuretics are inexpensive, there is no reason for high blood pressure to go untreated.
Talking points about previous slide

30
Not at Goal Blood Pressure (<140/90 mmHg)
Initial Drug Choices
Drug(s) for the compelling indications
Other antihypertensive drugs (diuretics, ACEI, ARB, BB, CCB)
as needed.
With Compelling Indications
Lifestyle Modifications
Stage 2 Hypertension (SBP >160 or DBP >100 mmHg)
2-drug combination for most (usually thiazide-type diuretic and
ACEI, or ARB, or BB, or CCB)
Stage 1 Hypertension(SBP 140–159 or DBP 90–99 mmHg)
Thiazide-type diuretics for most. May consider ACEI, ARB, BB, CCB,
or combination.
Without Compelling Indications
Not at Goal Blood Pressure
Optimize dosages or add additional drugs until goal blood pressure is achieved.
Consider consultation with hypertension specialist.

31
A key point in showing the JNC-7 treatment algorithm again in this presentation is that Patient Lifestyle Modifications is at the top of the algorithm.
Talking points about previous slide

32
• Most patients will experience better control if they modify their diet and improve their exercise.
• We should always advise our hypertensive patients about the role of lifestyle modification; and, believe it or not, sometimes it works!
• During F/U visits we should check both the BP and our patients’ lifestyle change efforts.
• It is not uncommon that our lifestyle counseling is limited to simple advice and admonishment because of time limitations.
• Nevertheless, lifestyle modification remains perched at the top of the JNC-7 algorithm and must not be taken lightly in treating our hypertensive patients.

Modification Approximate SBP reduction
Weight reduction 5-20 mmHg / 10 kg weight loss
Adopt DASH eating plan 8-14 mmHg
Dietary sodium reduction 2-8 mmHg
Physical activity 4-9 mmHg
Moderation of alcohol consumption
2-4 mmHg
33
Lifestyle Modifications

Keys to Influencing Lifestyle Modification
34
• There is evidence to suggest that brief behavioral modification counseling aimed at matching messages to the patient’s readiness to change and eliciting the patient’s own motivation to change can move the patient along a continuum of change or behavioral modification.
• Any movement on the part of the patient towards readiness to change should be considered a success.

35
• Permission: Ask the patient for permission to talk about lifestyle change and get preference for beginning with diet or exercise
• Interest: Ask the patient about readiness to change – How interested are you on a scale of 1-10. Ask why they are not a lower number – to elicit a motivational statement from the patient.
• Confidence: Ask how sure they are that they can do the behavior – again ask why not a lower number
• Match a message to interest and confidence
Influencing Lifestyle Modification What to Do: PICM

36
For low interest – “Would you be willing to think about reasons to begin diet/exercise and talk with me again next time?” Reinforce
For low confidence – “Would you be willing to monitor your activity/diet, think about a plan and visit with me again about this?” Give monitoring tools. Reinforce.
For high interest and confidence - Get commitment. Refer to dietitian, give diet plan, and/or assess plan for exercise.

37
In just a couple of minutes of interaction your goals must be limited. You want to move the patient along to change – not cause him to dig his heels in. To match a message, of course you have to hear what the patient is telling you.The first thing to do is to elicit change statements from the patient. If someone has just told you that they are a five on a scale from one to ten, ask “you are a five -- why are you not a three or a two? …… What would it take for you to be a 6 or a 7?”This is not a measurement technique – it is a technique for drawing out the patient’s own motivation.
Talking points about previous 2 slides

Summary
38
We should focus on BP control efforts for both Systolic and Diastolic to get the BP below 140/90 mm Hg.
We are urged to follow the JNC-7 treatment guidelines.
We should use a thiazide-type diuretic as the first line of attack against hypertension and in combination with other agents for uncontrolled hypertension.
Learning from ALLHAT, sometimes CHEAPER is BETTER.
We must make a renewed effort to encourage lifestyle changes in the management of hypertension.

Tools
39
For use with hypertensive patients:
• The DASH Eating Plan is very meaningful for our patients which is accessible on CD and at NHLBI.ORG) or can be found at the following link (http://neonproviders.com/nutrition.aspx)
• Brief behavioral counseling steps and patient monitoring tools
• Keep a copy of the JNC-7 recommendations handy or can be found at the following link (http://neonproviders.com/adultmedicine.aspx)