Embed Size (px)
Citation preview


2
1. Multi-Sector Service Accountability Agreements (MSAA) Governance Structure
2. Context
3. Community Accountability Planning Submission (CAPS)
a) Changes to the 2018/19 CAPS
b) CAPS Narrative Completion
c) CAPS Narrative Submission
d) Additional Resources
e) CAPS Demo
f) Completing the Submission for 2019/20
4. 2019/20 MSAA Schedules Overview
5. 2019/20 MSAA Indicators Overview
6. CAPS & MSAA Schedules Timelines

3
Comprehensive Consultation through Multiple Tables
MSAA Advisory Committee
MSAA Indicators Work Group
MSAA Planning & Schedules
Work Group
SRI Reporting Forms
Work Group
MSAA Legal Counsel Support: LHIN Legal Services Branch
MSAA Secretariat Support: Health Shared Services Ontario
Local MSAA Implementation: MSAA LHIN Leads
4
The MSAA Advisory Committee is working toward a new three-year agreement
effective from April 1, 2019 to March 31, 2022.
To support this new agreement the MSAA indicators and schedules have been
refreshed and updated:
• A (Description of Services)
• B (Service Plan)
• C (Reports)
• D (Directive Guidelines and Policies)
• E (Performance) (MSAA Indicator Work Group)
• F (Project Funding Template)
• G (Compliance)
* Note: Final approval from the CEO Council is upcoming and changes may occur.

5

6
Removed four Functional Centres (FC) that changed to Account Headers effective
April 1, 2018:
• 72 5 10 40 COM Clinics/Programs – Therapy Clinic
• 72 5 10 50 COM Clinics/Programs – Chronic Disease Clinic
• 72 5 50 45 COM Health Prom/Educ. & Com Dev – Personal Health and Wellness
• 72 5 50 35 COM Health Prom/Educ. & Com Dev – COM Chronic Disease Education,
Awareness and Prevention
Added six FCs (two New, four Previously reported in one of the FCs above that became
Account Headers in April 2018):
New
• 72 5 10 50 50 Clinics/Programs – Chronic Disease – Cardiac Rehabilitation Clinic
• 72 5 50 45 05 Personal Health and Wellness – General
Existing in Ontario Healthcare Reporting Standards (New to CAPS reporting)
• 72 5 50 45 10 Personal Health and Wellness – Mental Wellness, Personal Health Practices
and Coping Skills
• 72 5 50 45 20 Personal Health and Wellness – Oral Health
• 72 5 50 45 30 Personal Health and Wellness – Healthy Child
• 72 5 50 45 40 Personal Health and Wellness – Youth Development
7
Edit Checks Added
• On the Service Selection Screen when a Functional Centre (FC) is selected it must have a
corresponding Transfer Payment Business Entity (TPBE) selected to identify the program
funding to which the service applies.
• If a provider does not select a FC on the Service Selection screen, but completes planned
amounts on the Act Summary screen for that FC, an error will be flagged.
Financial and Service Activity Reporting Pages
• Added columns for Budget for 2020/21 and 2021/22.
- These columns are not locked but do populate from the input into the Budget 2019/20
column E.
• Variance calculations have been added for each line to highlight changes between the
2018/19 CAPS budget (original) and the 2019/20 CAPS budget (proposed).
• The HSP-specific view on the Activity Page now has two options:
- Show the HSP-specific Functional Centres that they have selected along with the
“Mandatory” services.
- Show the HSP-specific Functional Centres that they have selected along with all of the
service lines. This option is available where changes to the Mandatory lines have
occurred after the report was finalized.
8
Main Menu
• Added a calculation in Column F that flags any Changes to the budget from 2018/19
CAPS.
• The “Verify Edit Checks” link will show an to the left of the link when there are
any outstanding edit checks that have not been resolved on the Edits worksheet.
• Colour-coded the links to differentiate between General, Financial, and Activity.
• Moved the Financial Summary link to the top of the Financial list.
9
The CAPS Narrative has been redesigned to accommodate more detailed collection of
data relating to the services provided by Health Service Providers by sub-region:
• Instructions for completion are contained in the new
CAPS Narrative Guide 2019/20.
• The information provided in the CAPS Narrative will not be included in the final
MSAA.
• Supporting education documents are provided on the Central East LHIN website at:
http://www.centraleastlhin.on.ca/forhsps/SAA%20Resources.aspx

10
The CAPS Narrative should be submitted with the CAPS on the Self Reporting
Initiative (SRI) under the “Additional Documents” tab.
The CAPS Narrative should accompany the CAPS. The due date is
November 16, 2018.

11
The 2018/19 CAPS Completion Guide contains important information to assist HSPs
in completing the CAPS process. HSPs should refer to the Completion Guide when
completing the 2019/20 CAPS.
The CAPS Guidelines have been updated for 2019/20 to provide additional information
when completing the CAPS.
The CAPS Narrative file (CAPS Narrative – 2019/22) is available to download on the
Central East LHIN site at:
http://www.centraleastlhin.on.ca/forhsps/SAA%20Resources.aspx.
12
The new CAPS narrative has two recorded training webinars:
• HSP completion webinar: https://ali.health.gov.on.ca/p32lkvnvizc/
• The CAPS recorded webinar that mirrors the written completion guide:
https://ali.health.gov.on.ca/p9eiv0i80rc/
Detailed step-by-step training is available in the CAPS Completion Guide located on the
Central East LHIN website at:
http://www.centraleastlhin.on.ca/forhsps/SAA%20Resources.aspx

13

14
Schedule Title Description
A A1. Description of Services
A2. Population & Geography
Describes the services delivered by the
HSP and the HSP’s client populations
and geography served
B B1. Total LHIN Funding Service
Plan
B2. Clinical Activity – Summary
Describes the financial and statistical
status of the HSP
C Reports Identifies and sets due dates for HSP
reporting
D Directives, Guidelines, Policies &
Standards
Identifies applicable MOHLTC policies

15
Schedule Title Description
E 1. Core Indicators Identifies indicators, standards and local
performance requirements 2a. Clinical Activity Detail
2b. CHC Sector Specific
Indicators
2c. CMH&A Sector Specific
Indicators
2d. CSS Sector Specific
Indicators
3a. Local Indicators &
Obligations
F Project Funding Agreement
Template
Template used for funding projects that are
distinct from anything else; a unique project
that has nothing to do with the existing services
within the SAA
G Declaration of Compliance Form completed by the HSP Board of Directors
to declare that the HSP has complied with the
terms of the Agreement

16
Schedule Change Rationale
A • Removed and incorporated into a separate
CAPS Narrative
• The information captured is used for LHIN
planning and not relevant to accountability
B • B1: Total LHIN Funding - added
applicable dates for 2019/20
• Updated to reflect 2019/20
• B2: Clinical Activity Summary – removed • The information is redundant as it is a
summary of other information collected
C - CHC • Added applicable reporting dates for
2019/20
• Updated to reflect applicable 2019/20
reporting periods
• Added Community Engagement and
Integration Activities Reporting
• Was added to the MSAA template in 2018/19
C - CMHA • Added applicable reporting dates for
2019/20
• Updated to reflect applicable 2019/20
reporting periods
• Added Community Engagement and
Integration Activities Reporting
• Was added to the MSAA template in 2018/19
• Removed due dates for the Common Data
Set for Community Mental Health
Services (CDS-MH)
• The ministry has deferred the submission of
CDS-MH data starting in fiscal year 2018/19.
See footnote note in schedule.

17
Schedule Change Rationale
C - CMHA
& CSS
• Added applicable reporting dates for
2019/20
• Updated to reflect applicable 2019/20
reporting periods
• Added Community Engagement and
Integration Activities Reporting
• Was added to the MSAA template in
2018/19
C - CSS • Added applicable reporting dates for
2019/20
• Updated to reflect applicable 2019/20
reporting periods
• Added Community Engagement and
Integration Activities Reporting
• Was added to the MSAA template in
2018/19
D - CHC • Added additional directives, polices
and guidelines
• Relevant to sector
D - CMHA
& CSS
• Added additional directives, polices
and guidelines
• Relevant to sector
D - CSS • Added additional directives, polices
and guidelines
• Relevant to sector

18
Schedule Change Rationale
D - CMHA • Added additional directives, polices
and guidelines
• Relevant to sector
E • See indicator slides
F • No change • Section 11 of the Public Sector
Compensation Restraint to Protect
Public Services Act, 2010 is still
applicable
G • Added applicable period • Updated to reflect the applicable
period

19

20
• The work group will be completing an in-depth review of the indicators, technical
specifications, and target setting guidelines.
• It aims to deliver a slate of meaningful and measurable indicators that reflect the
patients’ continuum of care, promotes patient-centred discussions among all the
sectors, and in which each sector can recognize its contribution.
• Recognizing that the work will go beyond the deadlines for the usual refresh
process, the group has expanded its work plan and will continue working through
the remainder of the fiscal year.

21
• A technical specification (tech spec) document is developed each year. The tech spec
specifies indicator definitions, calculations, reporting periods, and other technical
information.
• The work group will update the tech spec to more clearly describe and define the
indicators, and will add a section that identifies the CAPS location for ease of
reference.

22
• A target setting document is developed each year that provides performance target
and corridor setting methodology to guide consistency and commonality across the
LHINs and health service providers (HSP) when establishing targets.
• The performance target and corridor-setting guideline accompanies the indicator
technical specification document.
Note: Performance targets and corridors are established for performance indicators
only.
23
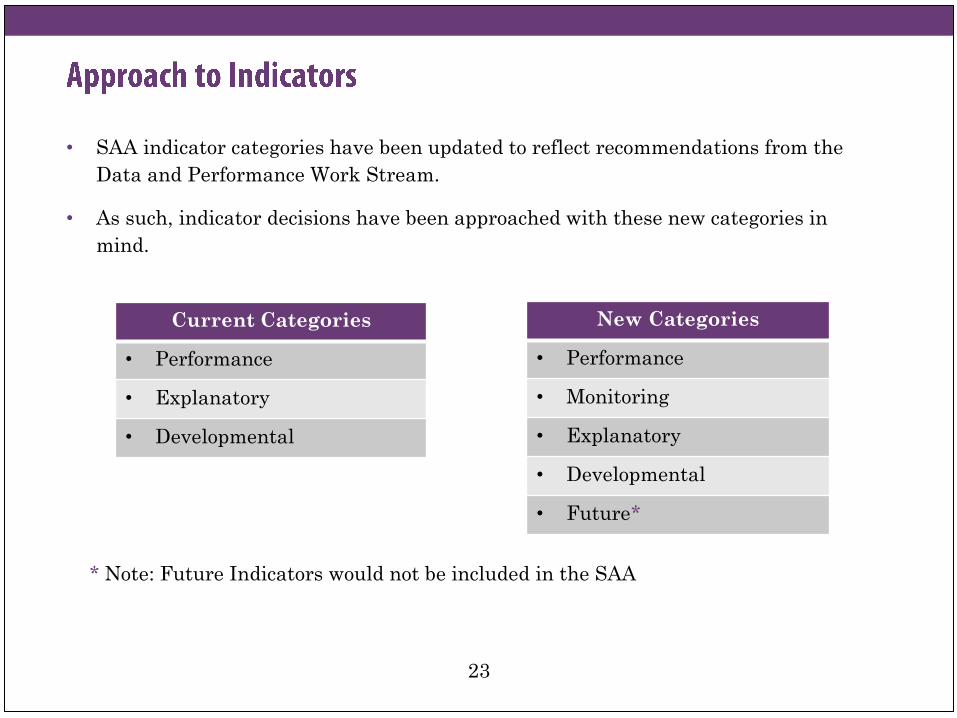
• SAA indicator categories have been updated to reflect recommendations from the
Data and Performance Work Stream.
• As such, indicator decisions have been approached with these new categories in
mind.
Current Categories
• Performance
• Explanatory
• Developmental
New Categories
• Performance
• Monitoring
• Explanatory
• Developmental
• Future*
* Note: Future Indicators would not be included in the SAA

24

25
• Renewed LHIN mandates (based on Patients First)
• Desire for refreshed 2018/19 Ministry/LHIN Accountability Agreement (MLAA) and
SAA indicators
• Need for greater alignment between MLAA and SAAs
• The Institute for Healthcare Improvement’s Triple Aim Framework

26
Core Indicators:
• Performance
• Monitoring
• Explanatory
Community Health Centres (CHC) Indicators:
• Performance
• Explanatory
• Developmental
Community Support Services (CSS) Indicators:
• Explanatory
• Developmental
Community Mental Health & Addiction (CMHA) Indicators:
• Explanatory
• Developmental
27
• Fund type 2 balanced budget
• Proportion of budget spent on administration
• Variance forecast to actual expenditures (moved to Monitoring)
• Percentage total margin
• Service activity by functional centre
• Variance forecast to actual units of service (moved to Monitoring)

28
• Number of Individuals Served (by functional centre) (name changed from Number
of individuals served)
• ALC Rate (moved to ‘Monitoring’)

29
• Variance forecast to actual expenditures (moved from Performance)
• Variance forecast to actual units of service (moved from Performance)
• ALC Rate (moved from Performance)
30
• Cost per unit of service (by functional centre)
• Cost per individual serviced (by program/service/functional centre)
• Client experience
• Percentage of Alternative Level of Care (ALC) days

31
• Number of persons waiting for service (by functional centre)

32
• Average number of days waited for first service (by functional centre)

33
• Cervical cancer screening
• Colorectal Screening rate
• Inter-professional diabetes care rate
• Influenza vaccination rate
• Breast cancer screening rate
• Retention Rate (for Nurse Practitioners and General Practitioners)
• Access to primary care
34
• Client satisfaction – Access
• Clinical support staff per primary care provider
• Interpretation
• Exam rooms per primary care provider
• New grads/new staff
• Non-Primary Care activities

35
• Number of new patients
• Number of registered clients
• Specialized care
• Supervision of students
• Third next available appointment (3NAA)
• Non-insured clients
• Travel time (NEW) – This indicator calculates the percentage of total time General
Practitioners, Nurse Practitioners, Physician Assistant, Registered Nurses, and
Registered Practical Nurses spent travelling for the purpose of direct service
delivery to clients.
• High-risk urban population (NEW) – This indicator identifies Community Health
Centres who provide services to a high-risk urban population.
36
• CHC clients hospitalized for Ambulatory Care Sensitive Conditions (ACSC)

37
• Repeat unscheduled emergency visits within 30 days (for mental health and
substance abuse conditions)
• Average number of days waited from referral/application to initial assessment
complete
• Average number of days waited from initial assessment complete to service
initiation

38
• Ontario Common Assessment of Need (OCAN)
39
• Ontario Perception of Care (OPOC) Tool for MHA (NEW)

40
• Strategic Alignment: The proposed LHIN-specific obligation* reflects the system
perspective and important goals or aspects of the regional or local health system. It
aligns with one or more provincial and/or LHIN system imperatives, and with one
or more health system outcome objectives.
• Focus on Integration: The proposed LHIN-specific obligation* enables greater
integration within and across health sectors at the sub-region or LHIN level, with
an emphasis on seamless transitions in care for patients.
• Focus on Improvement: The proposed LHIN-specific obligation* focuses on
matters related to system outcomes, provider-specific performance, and quality
improvement.
* Note: The proposed LHIN-specific obligation is distinct from existing requirements
and accountabilities.

41
Activity Target Dates Responsible
CAPS Launch in SRI for HSPs October 1, 2018 LHIN
CAPS 60 Day Issuance Notice to HSPs October 4, 2018 LHIN
Completed CAPS refresh submitted through SRI to LHINs
* PRELIMINARY October 4 – November 16, 2018 HSP
Send MSAA LHSIA Notices to HSPs Fall 2018 LHIN
LHIN review of CAPS refresh, consultations on MSAA
refresh indicators, population of Schedules, and final MSAA
Schedule amendments
November 19, 2018 –
January 15, 2019 LHIN and HSP
LHIN Boards to endorse MSAA Template (2/3 majority
required) December 1 – 31, 2018 LHIN
LHIN Analysis, Final Negotiations of Indicator Targets, and
final version of CAPS, if necessary * FINAL January 15, 2019 LHIN and HSP
HSP Board approves CAPS January 1 – 31, 2019 HSP
Final MSAA template and Schedules sent to Community
HSPs for Board approval February 1 - 28, 2019 LHIN
HSP-signed MSAA returned to the LHIN March 1 – March 15, 2019 HSP
LHIN Board approval of MSAA with final negotiated
schedules March 31, 2019 LHIN
2019-2022 MSAA takes effect April 1, 2019

42
If you have any questions, please contact:
• George Jacob – Senior Analyst, Contract Management, Performance and
Accountability
905-427-5497 (ext. 3264)
• Pauline Rahaman – Senior Analyst, Finance and Risk Management
905-427-5497 (ext. 3223)





























