Embed Size (px)
Citation preview

1
Chapter 3 CNS Gross Anatomy
Chris RordenUniversity of South CarolinaNorman J. Arnold School of Public HealthDepartment of Communication Sciences and DisordersUniversity of South Carolina

2
Key Objective
To be able to identify the level of the CNS by recognizing the landmarks in transverse, horizontal, and coronal sections– Brain, brainstem, spinal cord– Requires practice and drill– Use book, atlases and software – Look for shape, size, location and proximity to
other features.

3
Easy to spot changes
Pyramidal Tract Changes– Cortical + Subcortical
Ventricular Changes– All levels – including fourth ventricle and brainstem– Changes in shape of brainstem and spinal cord
4
Crucial anatomy
Horizontal and Coronal Views– Pyramidal Tracts– Cerebellum– Thalamus– Internal Capsule– Basal Ganglia
PutamenGlobus PallidusCaudate Nucleus
–Hippocampus
–Fornix
–Ventricles
–Corpus Callosum
–Optic tract
–Insula
5
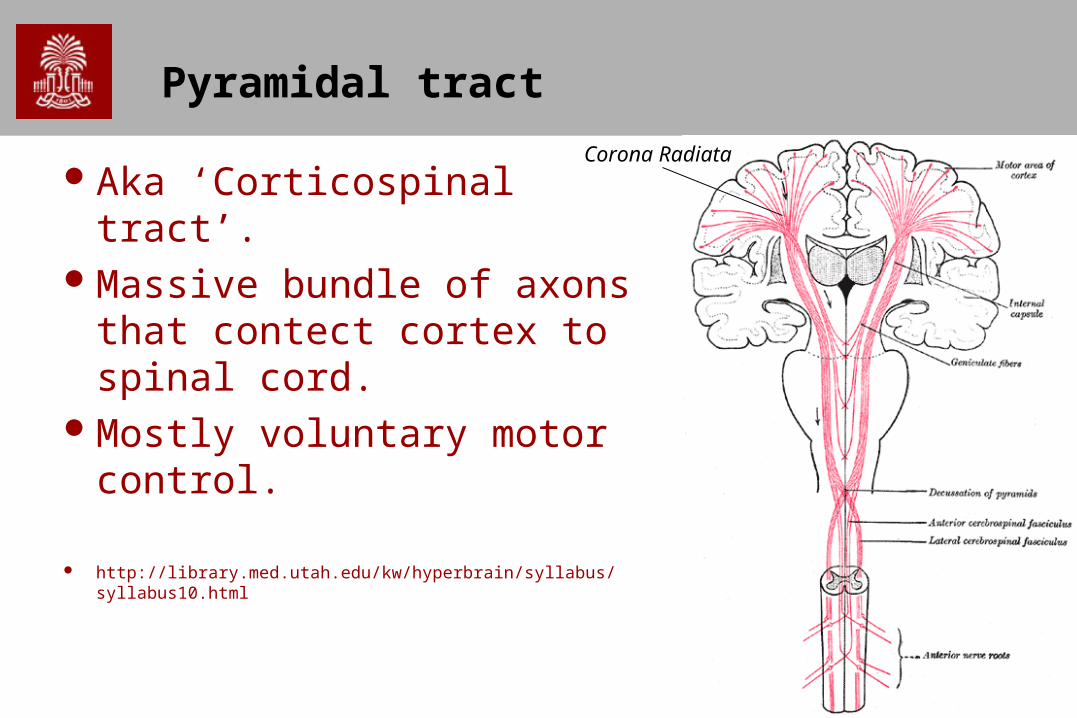
Pyramidal tract
Aka ‘Corticospinal tract’.Massive bundle of axons that
contect cortex to spinal cord.Mostly voluntary motor
control.
http://library.med.utah.edu/kw/hyperbrain/syllabus/syllabus10.html
Corona Radiata

6
Primary Motor Cortex
M1 is principle origin for pyramidal tract.– Spatial organization (homunculus)
M1: movement
S1: sensation
7
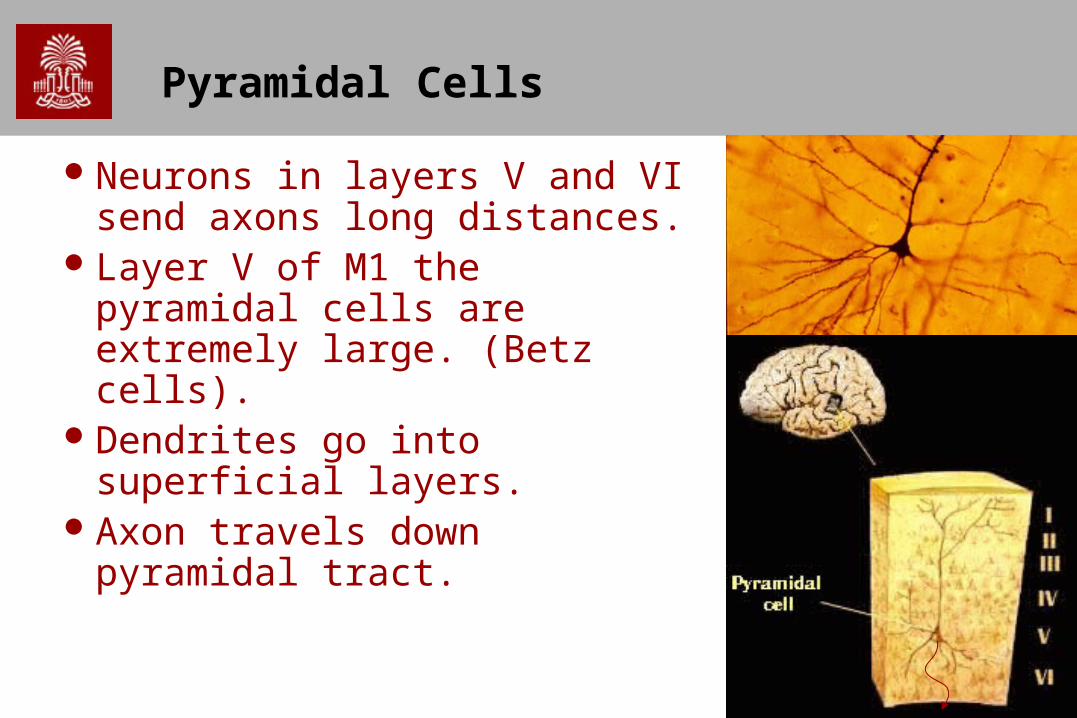
Pyramidal Cells
Neurons in layers V and VI send axons long distances.
Layer V of M1 the pyramidal cells are extremely large. (Betz cells).
Dendrites go into superficial layers.
Axon travels down pyramidal tract.

8
Corona Radiata
Near the motor cortex, we refer to the fibers of the pyramidal tract as being in the ‘corona radiata’.
9
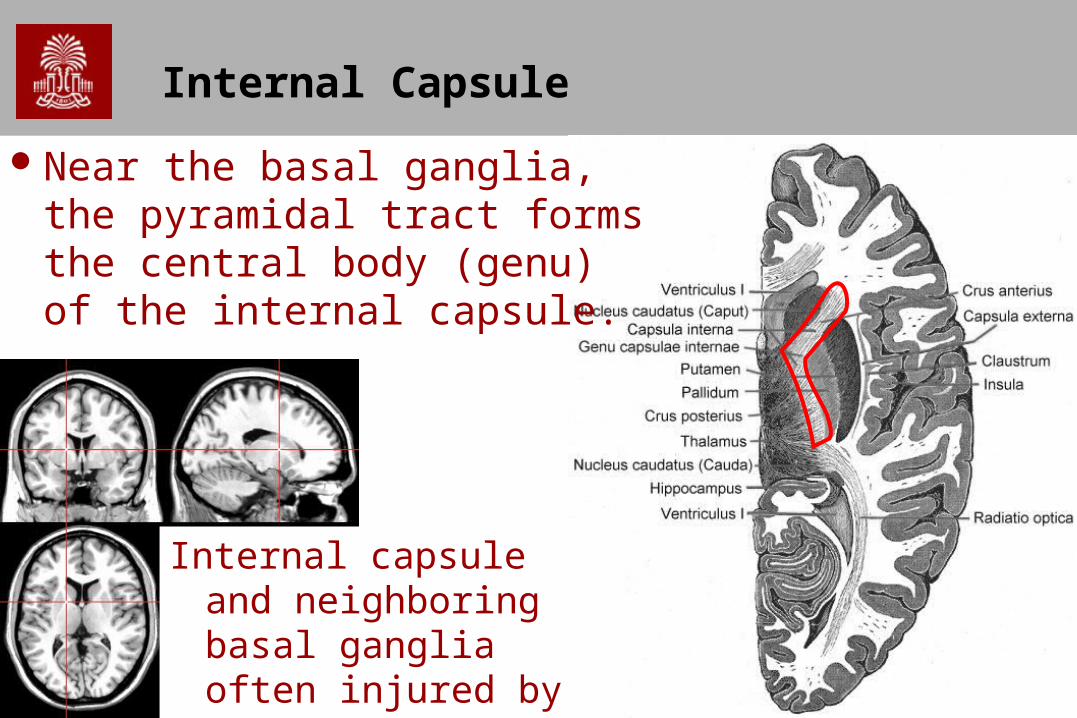
Internal Capsule
Near the basal ganglia, the pyramidal tract forms the central body (genu) of the internal capsule.
Internal capsule and neighboring basal ganglia often injured by small strokes.

10
Peduncles
A
P
Pes Pedunculi (part of Cerebral peduncle)
AP

11
Motor Fibers in the Pons
Corticospinal Tract
A
A
P

12
Motor Fibers in the Medulla
Pyramidal Tract
A
A
P
13
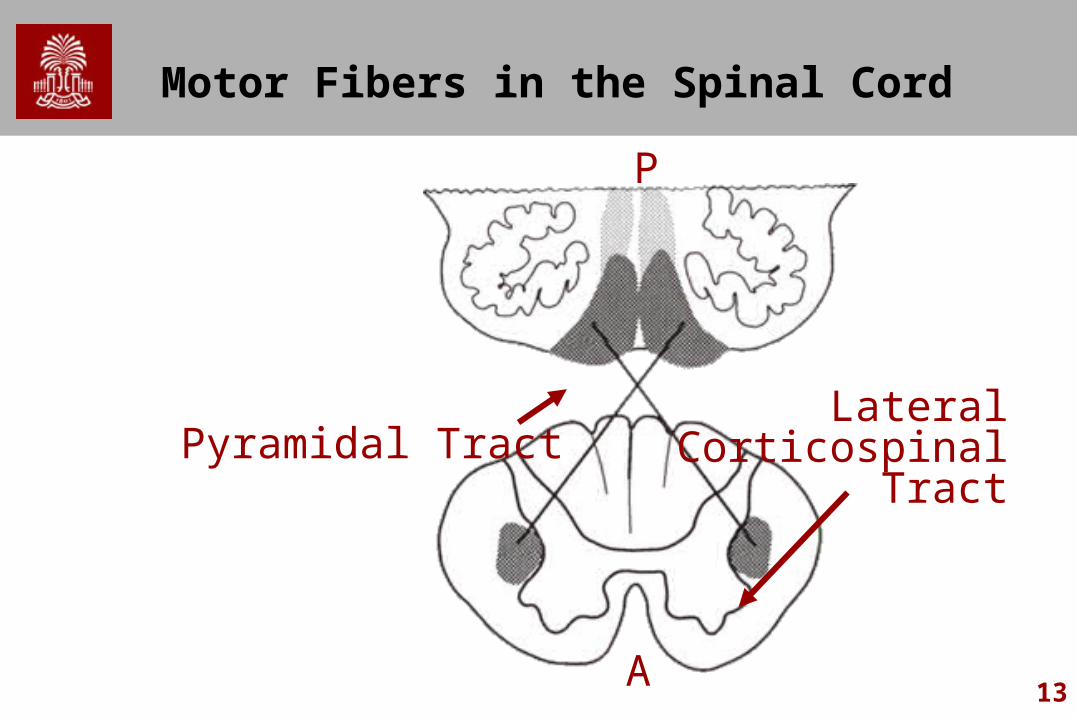
Motor Fibers in the Spinal Cord
Pyramidal TractLateral
CorticospinalTract
A
P

14
CSF
Lateral Ventricles
Third Ventricle
Cerebral Aqueduct
Fourth Ventricle

15
Ventricles

16
Sections of the Brain
Note whether views are – Axial (Horizontal) Views – Coronal Views– Less need for familiarity with sagittal view
Look for relationships and shapes of structures

17
Cerebellum
Heavily folded appearance – huge number of neurons.

18
Thalamus
Difficult to see on MRI scan – similar contrast to nearby white matter
Major portion of diencephalon

19
Thalamus
Sensory information is relayed to the cortex via the thalamus.
Auditory, somatic, visceral, gustatory and vision (but not smell) each have dedicated nuclei in thalamus.
Not just relaying information: thalamic nuclei have reciprocal connections with cortex. Regulates level of awareness - damaged can lead to coma.
20
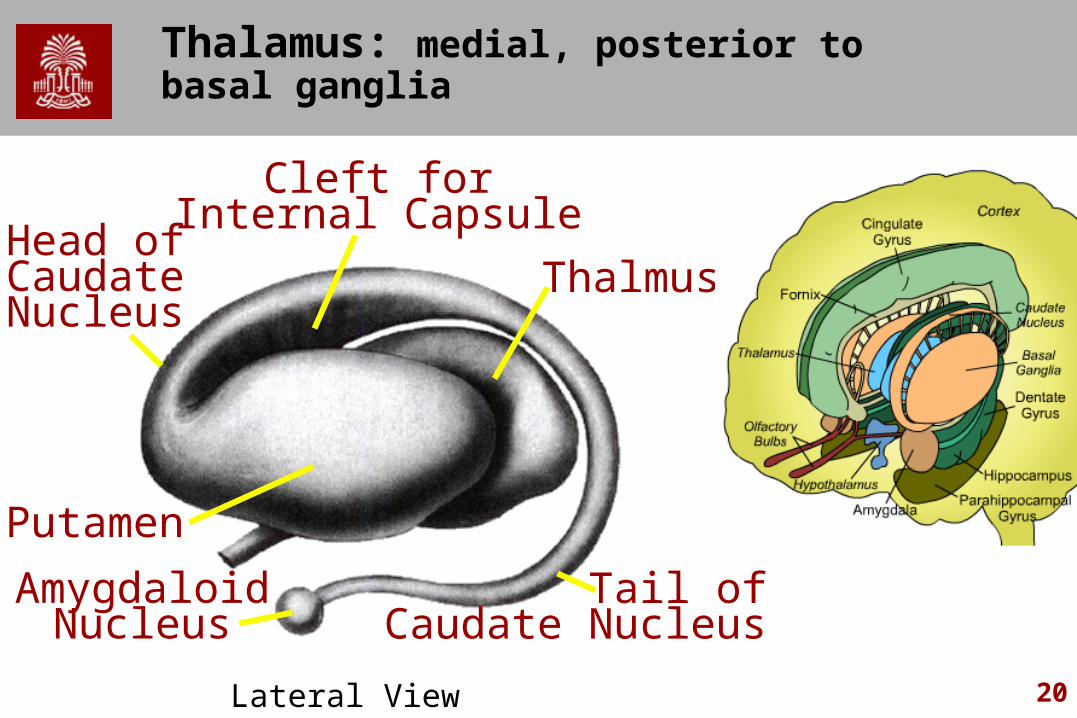
Thalamus: medial, posterior to basal ganglia
Cleft forInternal Capsule
Head ofCaudateNucleus
Thalmus
Putamen
AmygdaloidNucleus
Tail ofCaudate Nucleus
Lateral View

21
Thalamus
Not seen on the more anterior coronal slices.

22
Basal Ganglia
Basal Ganglia (CN+Putamen referred to as striatum)– Caudate nucleus near lateral ventricle– Putamen (yellow): superficial– Globus pallidus (green): deep– Nucleus accumbens: (not shown – junction of CN and Putamen)
Function: initiating action. Involved with parkinson disease. Also involved with motivation, addiction.

23
Basal Ganglia
Coronal slices
24
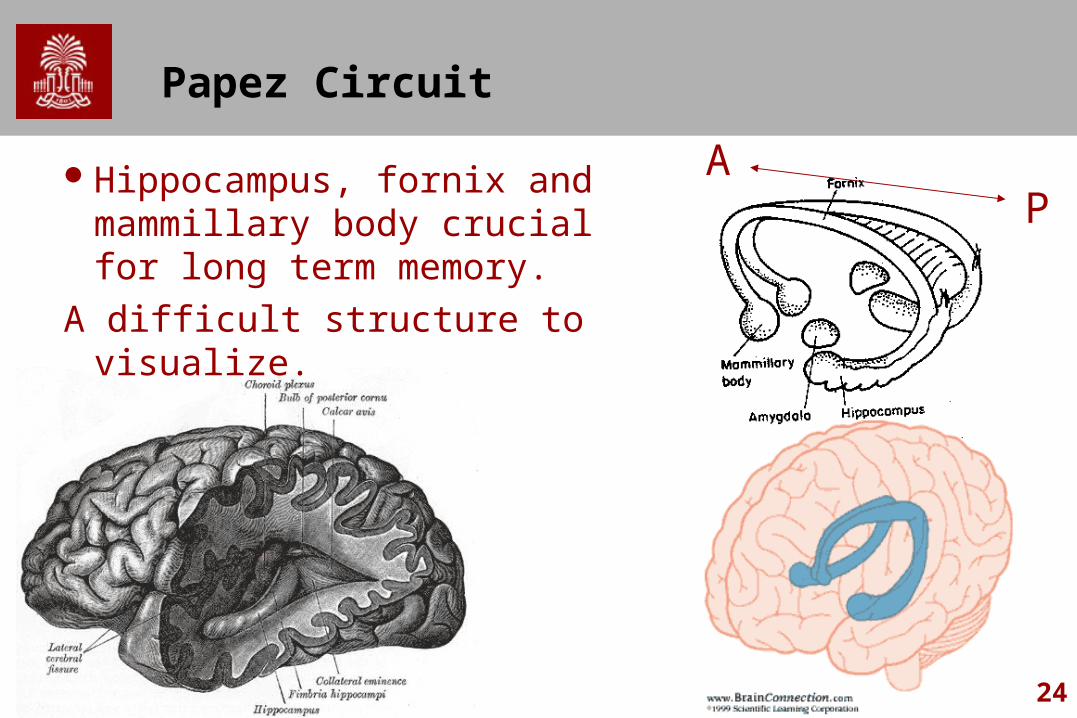
Papez Circuit
Hippocampus, fornix and mammillary body crucial for long term memory.
A difficult structure to visualize.
PA
25
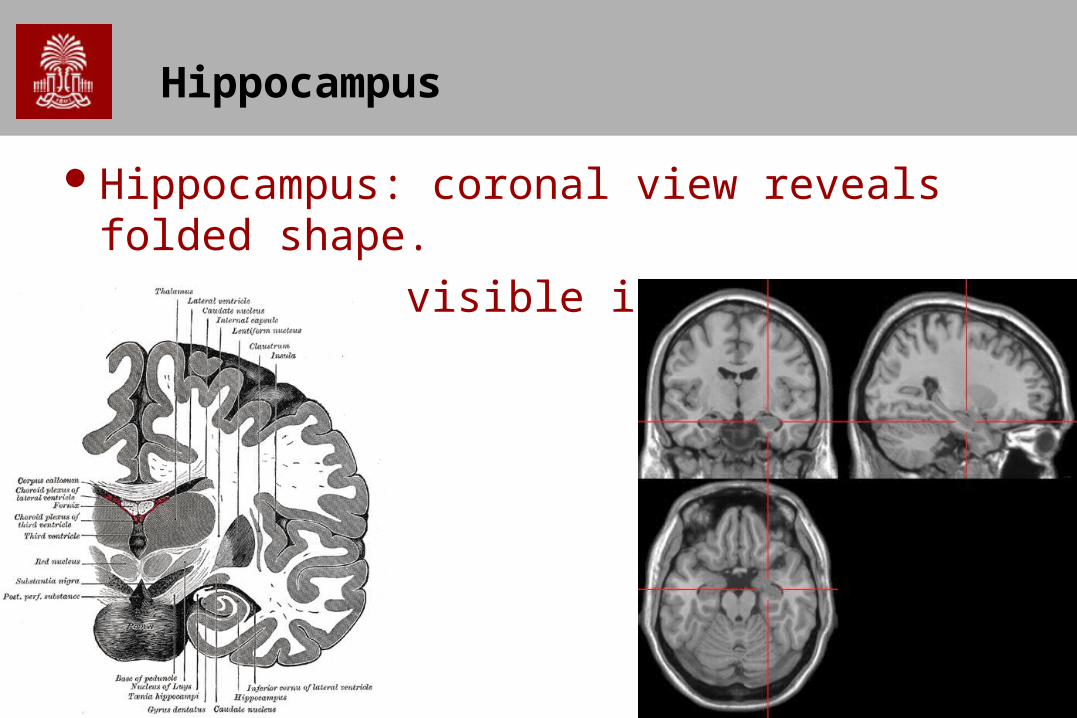
Hippocampus
Hippocampus: coronal view reveals folded shape.Fornix also visible in this view.

26
Corpus Callosum
Massive white matter bundle that connects the two hemispheres

27
Corpus Callosum
Sometimes surgically severed to treat epilepsy– ‘Split brain patients’ – Connections mostly homotopic

28
The optic tract
Lesions at different locations lead to different forms of visual field cuts.
Important diagnostic tool to infer brain injury.
LateralGeniculate Nucleus (Thalamus) V1 Primary Visual Cortex

29
Visual Defects
Field defects reveal anatomical injury
A. Monocular blindness
B. Monocular quadrantanopia
C. Bitemporal hemianopia
D. Homonymous hemianopia
E. Upper quadrantanopia
F. Lower quadrantanopia
G. Homonymous hemianopia
30
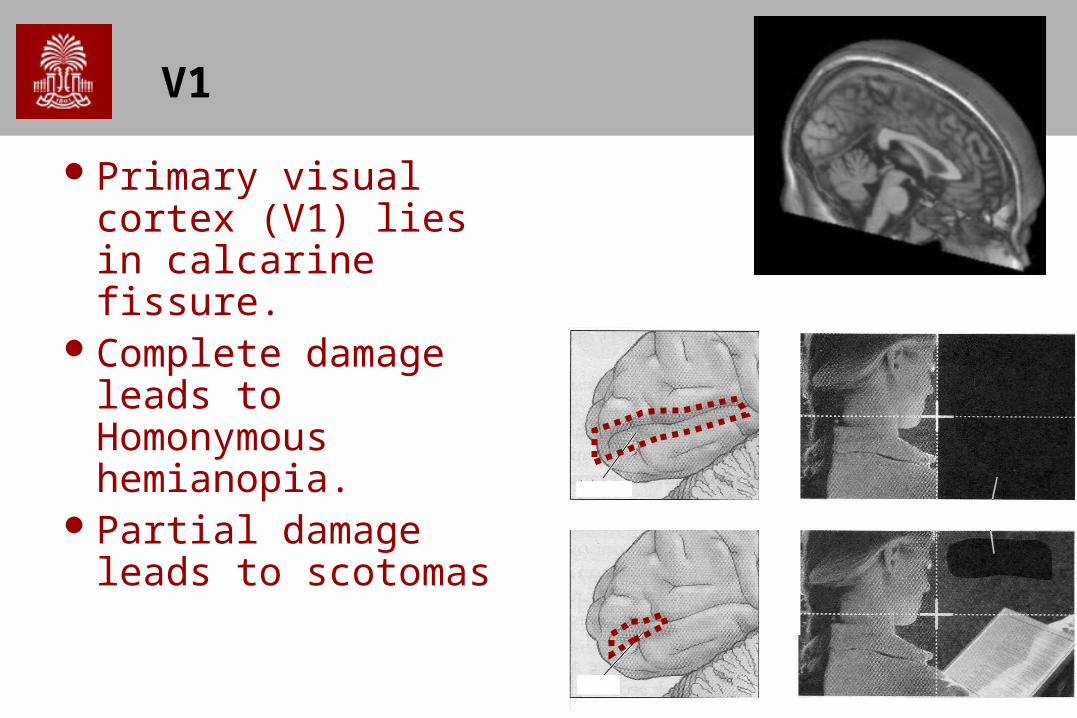
V1
Primary visual cortex (V1) lies in calcarine fissure.
Complete damage leads to Homonymous hemianopia.
Partial damage leads to scotomas

31
V1 – retinotopic mapping
V1 is retinotopic: distorted spatial map of visual scene
Fovea has massively over represented.

Insular Cortex
Insula: below the portions of the frontal, temporal, and parietal lobes

Insular Cortex
Sometimes referred to as Insular Lobe Operculum (lids) separate the insula and the
superficial cortex. Temporal Operculum
(inferior bank) Parietal Operculum
(posterior+superior) Frontal Operculum
(anterior+superior)





























