Embed Size (px)
Citation preview

Too much, too little, too late: Abnormal uterine bleeding
JodySteinauer,MD,MASJuly,2015
The Questions
• Toomuch(&tooearlyortoolate)– Differentialandapproachtowork‐up
– Doessheneedanendometrialbiopsy(EMB)?
– Doessheneedanultrasound?
– HowdoIstopperi‐menopausalbleeding?
– Isn’titduetothefibroids?
• Toofast:She’shemorrhaging—whatdoIdo?
• Toolittle:Aquickreviewofamenorrhea

Case 1
A46yo G3P2T1reportsherperiodshavebecomeincreasinglyirregularandheavyoverthelast6‐8months.Sometimestheycome2timespermonthandsometimesthereare2monthsbetween.LMP2monthsago.Shebleeds10dayswithclotsandfrequentlybleedsthroughpadstoherclothes.Sheoccasionallyhashotflashes.Shealsohasdiabetesandisobese.
1. Whattermdescribeshersymptoms?
2. Physiologically,whatcausesthistypeofbleedingpattern?
3. Whatisthedifferential?
1. FSH2. Testosterone&DHEAS3. Serumbeta‐HCG4. Transvaginal Ultrasound(TVUS)5. EndometrialBiopsy(EMB)
Q1: In addition to a urine pregnancy test and TSH, which of the following is the most appropriate test to obtain at this time?

Terminology: What is abnormal?
• Normal:Cycle=28days+‐ 7d(21‐35);Length=2‐7days;Heaviness=self‐defined
• Toolittlebleeding:amenorrheaoroligomenorrhea
• Toomuchbleeding:Menorrhagia(regulartimingbutheavy(accordingtopatient)ORlongflow(>7days)
• Irregularbleeding:Metrorrhagia,intermenstrual orpost‐coitalbleeding
• IrregularandExcessive:Menometrorrhagia
• Preferredtermfornon‐pregnantbleedingissues=AbnormalUterineBleeding(AUB)– Avoid“DUB”‐ dysfunctionaluterinebleeding.
Pathophysiology: Anovulatory Bleeding
Bricks&MortarEstrogen=Bricks,buildendometrium
Progesterone(P)=Mortar,stabilizes,onlyhavePifovulate
Normalmenses:WithdrawalofPcauseswalltofalldown,allatonce(orderlybleed)
Anovulation: NoPsowhenwallgrowstootall,itfalls.Itisheavywhenwallistall.Brickscanalsofallintermittently&incompletely–irregularly,irregular

Differential: AUBStep 1: Pregnant?
Pregnant
• Ectopic• SpontaneousAbortion• ThreatenedAbortion• MolarPregnancy• Trauma• Somenon‐pregnantcauses
NotPregnant• Anovulation***• Anatomic/structural**• Neoplastic*• Infectious• Iatrogenic• Non‐gynecologic
* = Most likely for this patient
PCOS Hypo/HyperThyroid
Anorexia/Over‐exercise
menopause
Peri‐menarche/Peri‐menopause
Physiologic Hyperandrogenic CNS Iatrogenic
Obesity
Causes of Anovulation

Reference: Causes of Anovulation
Pregnancy*Peri‐menarche+Peri‐menopause+Breast‐feeding*Obesity(viainsulineffectinovary)+
PCOS+Adult‐onsetcongenitaladrenalhyperplasia+
Pituitary adenoma (prolactin-secreting)*
Neuroleptic agents (via increased prolactin)*
Hypo or hyper thyroid (* or +)
Hypothalamic (stress, anorexia)*
LevonorgestrelIUD#Progestininjection*#Progestinimplant#Combinedhormonalcontraception#
*Typicallyamenorrhea#Typicallyspotting/lightirregularbleeding+Typicallyirregularheavybleeding(q1.5‐6mos)
Physiologic Hyperandrogenic CNS Iatrogenic
Reference: AUB Differential
Uterus:Myoma,polyp,adenomyosis,atrophy
Cervix:polyp,atrophy,trauma
Vagina:atrophy,trauma
Uterus:Hyperplasia,cancer
Cervix:Dysplasia,cancer
Ovary:hormoneproducingtumor
Uterus:Endometritis,PID
Cervix:Cervicitis
Vagina:Vaginitis(eg Trich)
Coagulopathy(vWD),severerenalorliverdz,GIorGUsource
Non-Gynecologic
Infectious
Neoplastic
Anatomic
Hormonal
Not Pregnant
Anovulation
Not Pregnant

Initial Work‐up: Menometrorrhagia
• Always:Urinepregnancy
• Usually:TSH
• Maybe:Hct,r/ocoagulopathy
• Maybe:EMB(EndometrialBiopsy)
• Maybebutlater:TransvaginalUltrasound
• Usuallynotnecessary:FSH,LH,Testosterone,Estradiol
Does she need an EMB?
EndometrialCancerFacts• 4thmostcommoncancerinwomen;averageage61but25%occurinpremenopause
• 10%ofpost‐menopausalwomenwithbleedinghavecancer
• Presentsatearlystagewithbleeding;rareintheabsenceofbleeding.Vastmajorityeffectivelytreatedwithsimplehysterectomy
• Riskfactor=Increasedestrogen(longh/oanovulatione.g.PCOS,obesity).Protective=smoking,OCP’s

The Problem
• Irregularbleedingiscommon
• Endometrialcancerisrelativelycommon
• Riskpredictionmodelsarenotuseful
• LittleevidencetoguideusregardingwhentodoEMB
• ACOGguidelines(expertopinion)recommendbiopsyinMANYwomen
ACOG, July 2012
ACOGPracticeBulletin128,DiagnosisofAUBinReproductive‐AgedWomen

Perimenopause
• Averages4years
•12%suddenlystopmenstruating
•18%havelonger,heaviermenses
•70%haveshort,irregularmenses
ShouldwethereforeperformEMB onallbut12%of
women?
The Evidence…
• Oneprospectivecohortstudyof1000womentotestlessaggressiveEMBClinicalPathway
• AlleligibleforbiopsyusingACOGguidelines.Onlybiopsiedthosethatwerepost‐menopausalorhadatleast1riskfactor(n=570)
• Nocancers/hyperplasiain2yrs f/uinthosethatweren’tbiopsied.(under‐poweredtoanswerthisquestion)
Dunn,JReprodMed. 2001Sep;46(9):831‐4

A Rational Approach to EMB
• Naturalhistory:Endometrialcancertakesmanyyearstodevelopprogressingfromnoatypia toatypia priortoinvasion.Wehavetimetodetectit.
• Bleedingpatterncues:Cancer&hyperplasiapresentmostcommonlywithmenometrorrhagia,sometimeswithintermenstrual bleeding.Rarelywithregularly‐timedmenses.
• Progestins (IUD,progestin‐onlypill)havebeenshowntotreathyperplasiaandcancer.
A Rational Approach to EMB
Post‐Menopause:ALLwomenWITHANY BLEEDING(except4‐6monthsafterstartingHRT)
Recentonsetirregularbleeding: Considertreatingfirstandifbleedingnormalizes,noneedEMB
>50: Allwomenwithrecurrent,irregular bleeding(considernotdoingifperiodslightandspacingout)
45‐50: Recurrentirregularbleedingplus>1riskfactorOR>6mosmenometrorrhagia
<45:Longhistory(>2yr?>5yr?)ofuntreatedanovulatory bleeding(eg PCOS)

Otherreasons:Papwithatypicalglandularcellsorendometrialcells(ie ifpapnotdoneattimeofmenses).
EMB isnotperfectlysensitivesofurtherevaluationmandatoryif:
1.PersistentAUB afternegativeEMB
2.PersistentAUB after3‐6monthsofmedicaltherapy
A Rational Approach to EMB (cont’d)
Do all women with AUB need an ultrasound?
AlthoughTVUS isthebestimagingchoiceforpelvicpathology(ie betterthanMRI,CT)….• 80%withheavymenstrualbleedinghavenoanatomicpathology
• Incidentalfindingssuchasfunctionalovariancystsandsmallfibroids(~50%)areoftenfoundleadingtoanxietyandunnecessarytreatments
• SO….treatfirst,TVUS iftreatmentfails
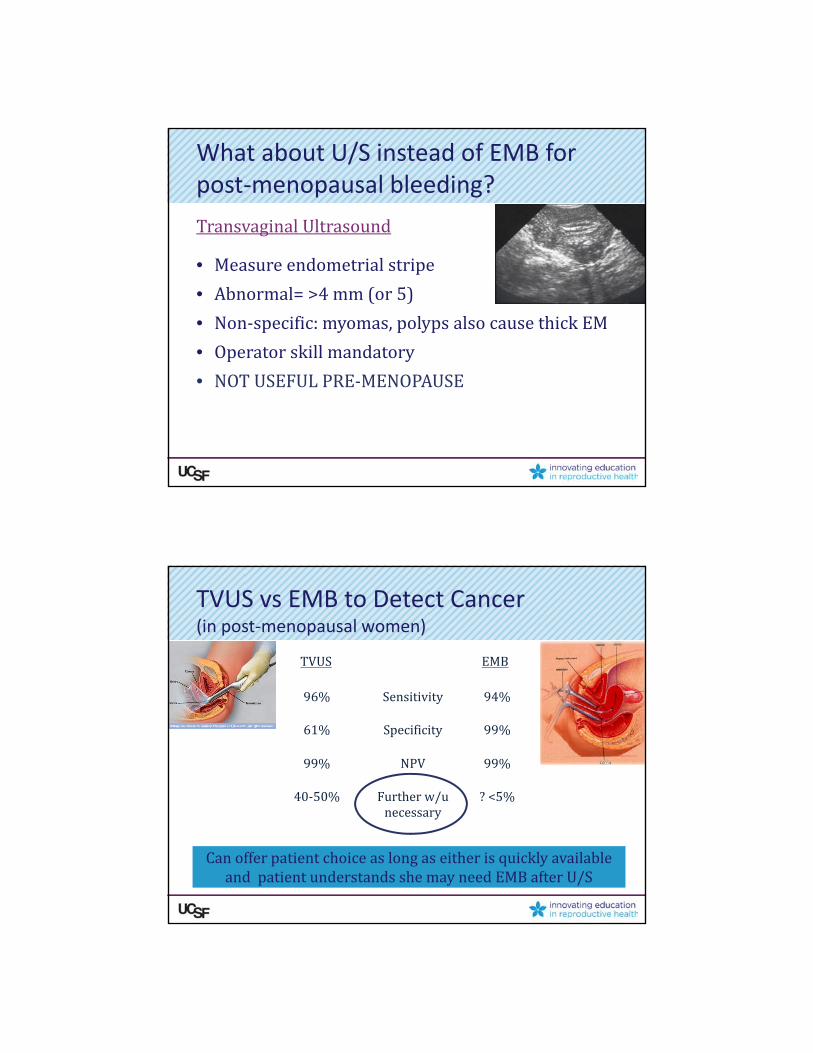
What about U/S instead of EMB for post‐menopausal bleeding?
Transvaginal Ultrasound
• Measureendometrialstripe
• Abnormal=>4mm(or5)
• Non‐specific:myomas,polypsalsocausethickEM
• Operatorskillmandatory
• NOTUSEFULPRE‐MENOPAUSE
TVUS EMB
96% Sensitivity 94%
61% Specificity 99%
99% NPV 99%
40‐50% Furtherw/unecessary
?<5%
CanofferpatientchoiceaslongaseitherisquicklyavailableandpatientunderstandsshemayneedEMBafterU/S
TVUS vs EMB to Detect Cancer (in post‐menopausal women)

Q1: In addition to a urine pregnancy test and TSH, which of the following is the most appropriate test to order at this time?
1. FSH2. Testosterone&DHEAS3. Serumbeta‐HCG4. Transvaginal
Ultrasound5. EndometrialBiopsy
A46yo G3P2T1reportsherperiodshavebecomeincreasinglyirregularandheavyoverthelast6‐8months.Sometimestheycome2timespermonthandsometimesthereare2monthsbetween.LMP2monthsago.Shebleeds10dayswithclotsandfrequentlybleedsthroughpadstoherclothes.Sheoccasionallyhashotflashes.Shealsohasdiabetesandisobese.
EMB=“Disordered Proliferative”. How do I stop the bleeding?
MedicalNSAID’sTransexamic AcidOralE+PE+Ppatch,ringHRT(lowerdoseE+P)HRTpatchOralProgestinProgestinIUDIMProgestinGnRH agonist
SurgicalEndometrialablation
(D&C/Hysteroscopy)
Hysterectomy(failedmedicalmanagement)
Disorderedproliferative=Anovulation

Non‐hormonal Treatment: NSAID’s
• 5daysaroundtheclock(eg 600mgtid)
• ManydosagesandtypesproveneffectiveinmultipleRCT’s todecreaseblding by~40%
• Usealoneorwithothertherapies
DON’TFORGETNSAIDs!
First Line Hormonal Treatments
• Firstchoice:Levonorgestrel IUD– >80%reductioninbloodloss,decreasedcramping,prevents/treatshyperplasia,highlyeffectivebirthcontrol
– Veryfewcontraindicationstousing– Bloodlossandsatisfactioncomparabletoablation,satisfactioncomparabletohyst.
• 2nd choice:combinedcontraceptives(pill,patch,ring)orprogestininjection– Proventodecreaseirregularperi‐menopausalbleeding– Anytypeok,20mcgpreferredforwomen>40– Estrogencontraindications:smokers>35,HTN,complicatedDM,multipleRFforCAD,h/oDVT,migraines

Second Line Hormonal Options
• CyclicProgestins:– LesseffectivethanNSAID’sandLevo IUD– 21‐daytherapymoreeffectivethan10‐daybutpoorlytolerated
• HT(post‐menopausaldosing):– MoredifficulttogaincyclecontrolcomparedwithOCP– SamecontraindicationsasCombinedHormonalContraception
Transexamic Acid
• Anti‐fibrinolytic;availableinEuropeformanyyears‐availableinUS2011
• Expensive$170percycle
• InRCT’s,moreeffectivethanNSAID,cyclicprovera.– LesseffectivethanMirena.ImprovesQOLby80%by3rdcycle
• Dose:2tabstid for5days(3900mg)
• Risks:TheoreticriskofVTE.Noincreaseinlargestudies.ContraindicatedinthosewithhistoryoforriskfactorsforVTE.UnknownifsafeinconjunctionwithCHC.
• Sideeffects:Minimal

Surgical Treatments
• D&C,Hysteroscopy:– Notreallyatreatment.Temporaryreductioninbleeding.Diagnostic,notcurative(exceptifpolypremoved).
• EndometrialAblation– Reducesbutdoesn’teliminatemenses– ~25%repeatablationorhyst in5years– Mustruleoutcancerfirst– Can’tbedonein>12weekuteriorforwomenwhowantfertility
Perimenopausal/AnovulatoryBleeding: Summary
R/opregnancy,thyroiddz
EMBifmeetscriteria
Treatfirstasifanovulatory bleeding:– NSAID’s+– Hormones(Levo IUD,CHC,DMPA)
Ifpersists:– U/Stocheckforanatomiccauses(andEMBifnotalreadydone)
– Discusssurgicaloptionsforbleedingrefractorytomedicalmanagement.

Case 2: Is it the fibroids?
SamehistoryasCase1exceptshehasfibroids….
A46yo G2P2womanpresentsstatingthatherfibroidsarecausingirregularbleeding.
Shehasaknownfibroiduterusandcomplainsofincreasinglyirregularandheavyperiods.Sometimestheycome2timespermonthandsometimesthereare2monthsbetween.LMP 2monthsago.Shebleeds10dayswithclotsandfrequentlybleedsthroughpadstoherclothes.Sheoccasionallyhashotflashes.Shealsohasdiabetesandisobese.
Onexam,heruterusis16weekssizeandirregular.
Fibroids…...
• Verycommon 80%ofhysterectomyspecimens(doneforanyreason)and~75%haveonU/Satage50.
• 2‐3foldhigherincidenceinblackwomen
• About50%areasymptomatic
• Growslowlyuntilmenopauseandthendecreaseby~50%(canstillcausebleedingpost‐menopause)

Fibroid Symptoms
• Bleeding– Usuallynormal ormenorrhagia(heavybutregular).Fibroidsstretchendometrium=moreblding
– Occasionallymenometrorrhagiaifsubmucous orintracavitary(Fibroidsdistortendometriumsoitcan’teverbestable=constantblding)
• Pressure(notpain)• Dysmenorrhea
Heavy,irregularbleeding
NoeffectHeavy,regularbleeding
Is the bleeding due to the fibroids?
• Fibroidsarecommoninlater40s• Anovulationiscommoninlater40s• Theincreasedbleedingseenwithfibroidsistypicallyduetoincreasedvolumeordistortionoftheendometrium
• Therefore:Decreasetheamountofendometriumbytreatingasanovulatory bleeding.Thisoftenworks.

AUB with Known Fibroids: Work‐up and Treatment
• R/ocancer(using“rationalemb algorithm”andpregnancy(don’tblamefibroidsforthebleeding)
• NSAID’sandhormones
• Ifnobetter,blamethefibroids!
• +/‐ Lupron‐‐asabridgetomenopauseorpre‐optoshrinktoobtainlessinvasiverouteofhysterectomy
• Surgicaltherapies(hysteroscopic resectionif<3cm,myomectomy,hysterectomy,UAE)
Hysterectomy
• Veryhighpatientsatisfaction(90%)(higherthanablation)
• Improvedqualityoflife,sexualsatisfactionanddecreasedpain
• Increasedlongtermrisksofprolapse,incontinence

Uterine Artery Embolization
• Benefits:40%decreaseinsize,75‐90%improvedbleeding
• Unknown:Willtheyre‐grow?In5yrf/uofRCT,25%hadhysterectomy
• Notfor:womenwhowantfertility• A“major”non‐surgicalprocedure:
– Requireshospitalizationforpaincontrol,– ~2weekstoreturntofullactivities(duetopainandfever)
– Risks:emergenthyst (1‐2%),5%expelmyoma throughcervix,40%havefever
Case 3… Too Fast
41yearoldwomanpresentswithdizzinessandheavyvaginalbleedingfor2weeksstraight.
Priortothis,occasionalirregularperiodsbutnothinglikethis!
Hemoglobin=9

Acute Menorrhagia Treatment
ABC’sandStopthebleeding!• ConsiderEDfortransfusion• Estrogen—2‐4OCPs(30‐35mcgE2)
– Increasesfibrinogen,factorsV,IX,plateletaggregation.“Covers”denudedareasinuterus
– OralaseffectiveasIV(souseoral)
• Givewithanti‐emetic• SmallRCTsuggestshigh‐doseprovera maybeeffectiveas
well,20mgtid• Ifnoteffective,options:D&C,Foleybulbtamponade,
emergencyhysterectomy
OCP Taper
• Don’twanttogive2‐4OCP’s perdayandthenstopsuddenlyb/cwillhavelargewithdrawalbleed
• Taper:4x4days,3x4days,2x4daysthen1 perdayfor1‐2months(66‐96pillsrequired).
• Instructnottotakeplacebosandgiveatleast3packsofpillsatonce.
• Givewithanti‐emetic,splitbid(i.e.2bidratherthan4allatonce)

What about too little bleeding?
Sevenquestionsinevaluationof2° amenorrhea
1. Pregnant?2. Excessivehairgrowthoracne? PCOS3. Overweight? Obesity‐inducedanovulation4. Breastsecretions? Hyperprolactinemia5. Verythin,over‐exercise,stress? Functional
hypothalamicamenorrhea6. Hotflashes? Prematureovarianfailure7. Pregnantrecentlycomplicatedwithinfectionoruterine
surgery(D&C)? Asherman’s syndrome
Size of words reflects frequency.
WORK‐UP: Amenorrhea
• Always:– Urinepregnancytest.
– IfNeg:TSH&PLN
• Ifhotflashes:– FSH
• Ifhirsute/obese:
– Usuallynofurthertestingneeded.(Ifdeepvoiceorclitoromegaly:testosterone.Iffamilyhistoryhirsutism oronsetatpuberty:17OH‐P)

Reference: Progestin Challenge Test
• Progestinchallengetest:(10mgProverax10days)– Bleedingafterconfirmsendogenousestrogenispresent
– Distinguisheshypothalamicamenorrhea(nobleedingorjustspots)fromPCOS(fullwithdrawalbleed)
• Estrogenchallengetest:(Premarin 2.5mgqd x3wksthenProverax10days)distinguisheshypothalamicamenorrhea(fullwithdrawalbleed)fromAsherman’s (nobleedingorjustspots)
Amenorrhea Treatment
1. PCOS Protecttheendometrium!(fromhyperplasiaduetounopposedE2) combinedcontraceptives,DMPA,LNGIUD
2. Obesityinducedanovulation same
3. Hyperprolactinemia duetomicroadenoma OCPsornothing,Bromocriptine ifdesirespregnancyortotreatsxs
4. Functionalhypothalamicamenorrhea‐‐ protectthebones!(fromlackofE2) estrogen‐containingcontraceptives
5. Prematureovarianfailure same
6. Asherman’s syndrome Hysteroscopy

Conclusions
• Diagnosis:consideranovulationeveninwomenwithfibroids.
• Work‐up:Alwaysruleoutpregnancy.Usually:TSH,PLN,?HCT,?EMB,TVUSifinitialtreatmentfails.
• Treatment:allbleedingtreatedsimilarly;NSAID’splushormones.Considerothercausesandtreatmentsifthisdoesn’twork.Preventhyperplasiawithprogestin‐dominanthormones.
• Persistentabnormalbleedingrequirescontinuedwork‐upevenifEMBand/orultrasoundarenegative.





























