Embed Size (px)
Citation preview

CiSEClinics in Shoulder and Elbow
Official Journal of Korean Shoulder and Elbow Society
Aims and Scope
Clinics in Shoulder and Elbow (Clin Shoulder Elb, CiSE; pISSN: 1226-9344, eISSN: 2288-8721) is an in-ternational, peer-reviewed journal and the official journal of Korean Shoulder and Elbow Society. It was first launched in 1998. It is published quarterly in the last day of March, June, September, and Decem-ber, with articles in English. The purpose of CiSE are: first, to contribute in the management and education of shoulder and elbow topics; second, to share latest scientific informations among international societies; and finally, to pro-mote communications on shoulder/elbow problems and patient care. It can cover all fields of clinical and basic researches in shoulder and elbow. CiSE published papers on basic and clinical researches, focusing on areas such as the etiology and epi-demiology, biomechanics and pathogenesis, management and surgery, complication and prognosis for disease of shoulder and elbow. The manuscripts in the following categories will be submitted: such as original articles, case reports, invited review articles, editorials and letters to the editor. All submissions are processed on line (www.cisejournal.org). The publication is determined by the editiors and peer re-viewers, who are experts in their specific fields of shoulder and elbow.Articles published in this journal can be obtained from the official web site of CiSE (www.cisejournal.org) as contents, abstracts and full text PDF files. Clinics in Shoulder and Elbow is indexed/tracked/covered by Korea Citation Index (KCI), KoreaMed, CrossRef, and Google Scholar.For subscription, submission, or any other information, please contact the editorial office below.
Clinics in Shoulder and Elbow Department of Orthopedic Surgery, Samsung Medical Center, Sungkyunkwan University, 81 Irwon-ro, Gangnam-gu, Seoul 135-710, Korea Tel: +82-2-3410-3509 / 3501, Fax: +82-2-3410-0061E-mail: [email protected]
Copyright © 2014 by Korean Shoulder and Elbow Society. All rights reserved.Articles published in CiSE are open-access, distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by-nc/3.0), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.This journal was supported by the Korean Federation of Science and Technology Societies (KOFST) Grant funded by
the Korean Government.
Volume 17 Number 2 (June, 2014)
Printed on June 25, 2014 Published on June 30, 2014Publisher Hyung-Bin Park Editor-in-Chief Sung-Jae KimPublished by Korean Shoulder and Elbow SocietyDepartment of Orthopedic Surgery, Seoul National University Bundang Hospital, 82 Gumi-ro 173beon-gil, Bundang-gu, Seongnam 463-707, KoreaTel: +82-10-9607-1397, Fax: +82-31-787-4087, E-mail: [email protected] by MEDrang Inc.8-17, WorldCupbuk-ro 5ga-gil, Mapo-gu, Seoul 121-841, KoreaTel: +82-2-325-2093, Fax: +82-2-325-2095E-mail: [email protected]
pISSN 1226-9344 • eISSN 2288-8721 • www.cisejournal.org
Editor-in-ChiefSung-Jae Kim
Editorial Board Kerem BilselLuciano BiglianiChih-Hwa ChenChul-Hyun ChoNam-Su ChoSung Wook ChoiYong-Min ChunMoustafa Ismail Ibrahim ElsayedDarren FriedmanMichael HantesChunyan JiangIn-Ho JeonChris H. JoKyung-Cheon KimSang-Hun KoWilliam LevineAndri Maruli Tua LubisEdward McFarlandTeruhisa MihataTomoyuki MochizukiYoung Lae MoonHyung-Bin ParkYong Girl RheeJoong-Bae SeoHyun-Seok SongW. Jaap WillemsYeo-Seung Yoon
Assistant EditorJae Chul Yoo
Manuscript EditorHyun Jung Kwon
Editorial Board
This paper meets the requirements of KS X ISO 9706, ISO 9706-1994 and ANSI/NISO Z39.48-1992 (Permanence of Paper).

CiSEClinics in Shoulder and Elbow
Editorial
49 For the Future of Clinics in Shoulder and ElbowSung-Jae Kim
Original Articles
50 Short-term Low-dose Oral Corticosteroid Therapy of Impingement Syndrome of the Shoulder: A Comparison of the Clinical Outcomes to Intra-articular Corticosteroid InjectionYoung Bok Kim, Young Chang Kim, Ji Wan Kim, Sang Jin Lee, Sang Won Lee, Hong Joon Choi, Dong Hyun Lee, Joo Young Kim
57 The Effect of Different Starting Periods of Passive Exercise on the Clinical Outcome of Arthroscopic Rotator Cuff RepairYoung-Woong Back, Suk-Kee Tae, Min-Kyu Kim, Oh-Jin Kwon
64 Changes in Matrix Metalloproteinase and Tissue Inhibitors of Metalloproteinase in Patients with Rotator Cuff TearsOh-Soo Kwon, Young-Yul Kim, Ji Yoon Ha, Han Bit Kang
68 Reverse Total Shoulder Arthroplasty: Early Outcome and Complication ReportYong-Bok Park, Sung-Weon Jung, Ho-Young Ryu, Jin-Ho Hong, Sang-Hoon Chae, Kyoung-Bin Min, Jae-Chul Yoo
Case Reports
77 Unusual Migration of Kirschner’s Wire into Intervertebral Foramen after Lateral Clavicle Fracture Fixation - A Case ReportJin-Ho Lee, Jae-Yoon Chung, Myung-Sun Kim
80 Tuberculous Tenosynovitis of the Elbow - A Case ReportChi-Hun Oh, Jung-Ho Park, Jung-Wook Kim
Review Articles
84 Animal Experiments Using Rotator CuffSeok Won Chung, Sae Hoon Kim, Joo Han Oh
91 Partial Thickness Rotator Cuff TearsSang-Jin Shin, Myeong-Jae Seo
Volume 17 • Number 2 • June, 2014

For the Future of Clinics in Shoulder and Elbow
Sung-Jae Kim
Arthroscopy and Joint Research Institute, Department of Orthopaedic Surgery, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea
Since its inauguration in 1993, the Korean Shoulder and Elbow Society (KSES) has showed remarkable growth for the last two decades. Although the history of shoulder and elbow surgery is relatively short in Korea, KSES has become a world-class society of shoulder and elbow surgery, comparable to those of Japan and other western countries. I believe that KSES is now one of the most promising orthopaedics societies and such development is all due to the active research and excellent presentation of our mem-bers.
KSES has actively held the annual meeting of shoulder and elbow surgery, related symposiums, and live surgeries and it certainly serves as an exemplary model to other societies in Korea. Especially, Clinics in Shoulder and Elbow (CiSE) has steadily developed into one of the leading orthopaedics journals in Korea; it is all due to active participation and research of our members.
Keeping pace with its recent development, the recent decision to switch CiSE into an English journal is timely and future-orient-ed for globalization of KSES and its further growth. I wish the transition can serve as a stepping point of being registered in the SCI journal list.
Furthermore, I believe that hosting the International Congress of Shoulder & Elbow Surgery in 2016 in Jeju Island will raise the status of KSES to a higher level. I wish its great success and active participation of our members.
It is not much to say that my career as a (shoulder and elbow) surgeon has developed together with the growth of KSES. I wish further development of KSES in upcoming years, including being registered in the SCI journal list and holding many symposiums with world-class scholars.
Once again, I congratulate the transition of the Journal of the Korean Shoulder and Elbow Society to an English journal.
CiSEClinics in Shoulder and Elbow
Copyright © 2014 Korean Shoulder and Elbow Society. All Rights Reserved.This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
pISSN 1226-9344eISSN 2288-8721
EDITORIAL
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014http://dx.doi.org/10.5397/cise.2014.17.2.49
Correspondence to: Sung-Jae KimArthroscopy and Joint Research Institute, Department of Orthopaedic Surgery, Severance Hospital, Yonsei University College of Medicine, 50-1 Yonsei-ro, Seodaemun-gu, Seoul 120-749, KoreaTel: +82-2-2228-5679, Fax: +82-2-363-6248, E-mail: [email protected]
Financial support: None. Conflict of interests: None.

Short-term Low-dose Oral Corticosteroid Therapy of Impingement Syndrome of the Shoulder: A Comparison of the Clinical Outcomes to Intra-articular Corticosteroid Injection
Young Bok Kim, Young Chang Kim, Ji Wan Kim, Sang Jin Lee, Sang Won Lee, Hong Joon Choi, Dong Hyun Lee, Joo Young Kim1
Department of Orthopedic Surgery, Inje University Haeundae Paik Hospital, 1Inje University Busan Paik Hospital, Busan, Korea
Background: To assess the clinical outcomes of short-term oral corticosteroid therapy for impingement syndrome of the shoulder and determine whether it can be substituted as an alternative to the intra-articular injection.Methods: The clinical outcomes of the 173 patients, the oral steroid group (n=88) and the injection group (n=85), were measured at 3 weeks, 2, 4, and 6 months postoperatively. The clinical outcomes were assessed by measuring the the University of California at Los Angeles (UCLA) score, visual analog scale (VAS) and range of motion (ROM) at every follow-up. Any complications and recurrence rate were noted. A relationship between the treatment outcomes and factors such as demographic factors, clinical symptoms and radiograph-ic findings were determined.Results: No difference was observed in VAS and UCLA scores between the two groups, but forward flexion and internal rotation of ROM were significantly improved in the injection group at the 2nd and 4th postoperative month (p < 0.05). At 6th postoperative month, recurrence rate of symptoms was 26% in the oral steroid group and 22% in the injection group. No major adverse effects were observed. When the clinical outcomes of the oral steroid group were compared to either demographic, clinical symptoms, or radio-graphic findings, UCLA score was found to be significantly low (p < 0.05) in patients with joint stiffness and UCLA score, whereas VAS score was significantly improved in patients with night pain (p < 0.05).Conclusions: Short-term low-dose oral corticosteroid therapy of impingement syndrome showed comparable clinical outcomes to intra-articular injection without any remarkable adverse effects. Low-dose oral steroids can be regarded as a partial alternative to intra-articular injection for the initial therapy of impingement syndrome of the shoulder.(Clin Shoulder Elb 2014;17(2):50-56)
Key Words: Shoulder; Impingement syndrome; Intra-articular steroid injection; Oral corticosteroid
Introduction
Impingement syndrome of the shoulder was first differenti-ated as a separate clinical condition in 1972 by Neer. Within 30 years, it has become the most commonly diagnosed type of impingement syndrome of shoulder. The criteria for diagnosis and treatment methods of impingement syndrome have been debated for many years, but the general consensus is to conser-
vatively manage at an early stage. Irrespective of the pathology, the success rate of conservative treatment was shown to be around 70%.1-3) Conservative treatment comprise of stabilizing the shoulder and controlling shoulder pain, in parallel with reha-bilitation courses. Exploiting the window for rehabilitation is criti-cal at the early stage of treatment in order to decrease clinical symptoms such as shoulder pain.4-7) Various ways to control pain include physiotherapy, use of nonsteroidal anti-inflammatory
CiSEClinics in Shoulder and Elbow
Copyright © 2014 Korean Shoulder and Elbow Society. All Rights Reserved.This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
pISSN 1226-9344eISSN 2288-8721
ORIGINAL ARTICLE
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014http://dx.doi.org/10.5397/cise.2014.17.2.50
Received August 23, 2013. Revised May 23, 2014. Accepted May 24, 2014.
Correspondence to: Young Bok KimDepartment of Orthopedic Surgery, Inje University Haeundae Paik Hospital, 875 Haeun-daero, Haeundae-gu, Busan 612-896, KoreaTel: +82-51-797-0611, Fax: +82-51-797-0991, E-mail: [email protected]
Financial support: None. Conflict of interests: None.

Low-dose Oral Corticosteroid Therapy of Impingement Syndrome of the ShoulderYoung Bok Kim, et al.
www.cisejournal.org 51
drugs (NSAIDs), and intra-articular injections, but of these the anti-inflammatory methods of the latter two are usually used. NSAIDs are generally used, and an exemplary benefit is pain relief even at a low blood concentration. However, limitations of NSAIDs are that its anti-inflammatory effects exerts only at steady state plasma concentration, which is achieved in about 1−2 weeks. This means the time taken to control the clinical symptoms would take at least 4 weeks, thus requiring a relatively long duration of drug administration.8) This long-term use often leads to gastrointestinal side-effects, adrenal insufficiency, and other drug-related complications9) that make the rate of patient compliance low.
Intra-articular injection is the most common method of ad-ministration and despite advantages such as fast resolving of pain and improved range of motion (ROM), as with other drug therapy, it does not resolve the diseases completely.10) Other limitations include, the need for technical specialty, steroid flares after injection, and fatal complications such as infections.11-13) The authors propose oral corticosteroids as an alternative for its speed and strength of effect and its bioability as a non-invasive oral administration.14) Not only are these benefits make oral cor-ticosteroids a promising alternative, it requires no technical spe-cialty for administration nor is it associated with complications. Thus, to test the applicability of oral corticosteroids in addressing the initial inflammatory response of impingement syndrome, the clinical stability and outcomes, potential problems and limita-tions, and factors influencing treatment were assessed.
Use of oral corticosteroids as medication is widespread, espe-cially for musculoskeletal disorders such as rheumatoid arthritis. Although a few reports have described the efficacy of oral corti-costeroid therapy on adhesive capsulitis,15-18) so far there is none reporting the efficacy of oral corticosteroids on impingement syndrome. In comparison, systemic exposure of steroids can be expected to modulate various immunological and inflammatory responses, and improve shoulder pain. Thus, we investigated the efficacy of short-term oral corticosteroids, as an intermediate of NSAIDs and intra-articular injections, on impingement syn-drome.
Methods
Between June 2010 and December 2011, of the 1,227 patients who were suspected of impingement syndrome, 244 patients who had contracted the condition within 9 months, showed a one-sided symptomatic shoulder, and had a trivial medical history were included in the study. The mean age of pa-tients was 56.4 years (range, 39−73 years), and ratio of sex was 95 males to 149 females.
The diagnosis of impingement syndrome was made when the patient complained of shoulder pain during motion or rest-ing and when there was a clear positive result for Neer sign,
Hawkins-Kennedy impingement sign, and painful arc sign by a single orthopedic surgeon.19) Several exclusion criteria were placed in our study to exclude the possibility of misdiagnosis of an impingement syndrome in the case where additional tests were required to differentiate an impingement syndrome. Patients with stiffness were included; however, patients with when less than 90o forward flexion, or even with more than 90° forward flexion but with tethering at end of motion at passive movement were excluded from the study to rule out patients with adhesive capsulitis corresponding to Neviaser stage 2 and 3.20) Patients shown to have calcific deposits, degenerative ar-thritis, or humeral head spurs through plain radiography of the anteroposterior and axillary views at internal and external rota-tions of the shoulders were excluded as well. Further, ultrasound imaging was taken on all patients by one expert and patients shown to have anatomical lesions such as full-thickness rotator cuff tears, partial rotator cuff tears according to the Ellman’s clas-sification,21) biceps lesion or dislocation were excluded. Although diabetic patients were included in the study, those diagnosed with a diabetic foot, diabetic retinopathy, diabetic kidney dis-ease, or those with uncontrolled glycemic levels were excluded. Lastly, those who were already on steroids, or had tuberculosis or acute/chronic infectious diseases were excluded after ques-tioning.
ROM included the forward flexion, external rotation at 90o abduction, external rotation at neutral position, using a protrac-tor, with the patient at supine position. The internal rotation was noted at the highest vertebra, and these values were fitted into the Mallon system22) to give a total shoulder internal rotation. Neutral position was set to 0o, umbilicus to 20o, anterior superior iliac spine to 30o, buttocks to 45o, sacrum to 80o, L5 to 85o, and for all values above 2o was added for every vertebra. All patients were questioned and physical tests were performed, the scores of which were standardized using the University of California at Los Angeles (UCLA) shoulder rating scale. To analyze complica-tions, the weight of each patient was taken during their visit the outpatient department. The patients were questioned on their level of pain, function, and satisfaction, whereas physical tests for active forward flexion and strength of forward flexion were per-formed. These results were standardized into the UCLA score. The visual analogue scale (VAS) was used to assess subjectively the patient’s current level of pain in comparison to the worst pain experienced by the patient. The current study randomly di-vided the patients into either the oral steroid group (n = 125/75 females, 50 males) and the injection group (n = 119/74 females, 45 males) using coin flipping. The oral steroid group included 18 diabetic patients, whereas the injection group included 16. The oral steroid group was prescribed 2 mg of Triamcinolone twice a day to take 30 minutes after breakfast and dinner for 3 weeks, and a reduced volume thereafter of 1 mg Triamcinolone for a further week. The injection group was injected once with

52 www.cisejournal.org
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014
40 mg/ml of Triamcinolone dissolved in 10 ml of saline solu-tion through the posterior portal under the ultrasound guide.23) From 3 weeks of the start of medication, both groups were administered with NSAID (Meloxicam 7.5 mg twice daily) for 8 weeks. Simultaneous to the start of the oral therapy or the injec-tion therapy, a proton pump inhibitor (Omeprazole 10 mg) was administered for around 3 months until the end of the duration of NSAID administration. Concomitant to the initiation of drug therapy, stretching and shrugging exercises of the shoulder were begun using a door pulley, and from the 8th week, a Thera-band was also used for the rotator cuff strengthening exercise. All patients were instructed to exercise both sides of the shoulder equally 2−3 times a day for a total of 40−60 minutes.
The 173 patients with a high compliance and were able to participate in a 6 month follow-up study were divided into either the oral steroid group (n = 88) or the intra-articular injec-tion group (n = 85). The changes in UCLA score, VAS score, ROM was assessed at 3 week, 2, 4, and 6 month follow-up. Any drug side-effects24) were noted and recurrence rate were ana-lyzed.
To measure weight gain as one side-effect of the drug, we measured the weight of the patients pre-therapy and through-out the 4 week therapy. A weight gain of more than 1 kg was considered significant and other short-term complications of steroid medication such as gastrointestinal dysfunction (upper abdominal discomfort or pain), infection (fever or chilling), skin problems such as acne, muscle soreness, increase in intraocular pressure (ophthalmalgia or impaired visual acuity) were also in-vestigating by questioning the patient. To discriminate potential adrenal insufficiency, experience of symptoms such as headache, dizziness, nausea vomiting, or sweating was noted. In case of diabetic patients, any loss of glycemic control or hyperglycemia was noted down, and also maximal glucose level was noted.
Other clinical variables analyzed were whether abrupt cessa-tion of oral steroids led to worsening of pain in the oral steroid group, or whether worsening of pain was felt between 3−5 days after the injection was performed in the injection group. The condition was considered to have recurred if the final VAS score was the same or only one stage higher than the initial VAS score, or if the final UCLA score was below or within 20 points higher of the initial UCLA score. The recurrence rate of the patients who were nonresponsive to treatment or had failed remission of symptoms was also determined.
To determine factors associated with the clinical outcomes of oral steroid group were separated demographically. The oral steroid group was divided into sex considering that activity and muscle strength of shoulder would differ between the sexes and this may have an influence on the therapy outcome. As well as sex, since level of activity and disease pathology may differ between age, the oral steroid group was also divided into either below age 40 or above age 40. We made an assump-
tion that the extent of clearance of inflammation and changes will depend on the duration of contraction of the syndrome. Arbitrarily, we set the time of contraction as either more than 6 months prior to or within 6 months of commencement of therapy. To take into consideration the possible effect of joint stiffness on the biomechanics of the joint, the patients were also divided into either stiff or not stiff group by defining a stiff joint as forward flexion of less than 120o or if any one of 3 ROM of rotation was less than half of the contralateral side. Further, to as-sess the influence of the severity of infection on the outcome of therapy, patients were divided into whether they had night pain that disrupted sleep cycle or not. To assess the effect of drug treatment on mechanical impingement, plain radiographs was taken and examined. Using the radiographic data, the patients were divided into those with a normal acromion and those with either an acromion that was deviated from its normal contour or subacromial congruity that was disrupted by a spur. An associa-tion of various demographic, clinical, factors of these two groups with the improvements in the UCLA score (final UCLA − initial UCLA) and VAS score (initial VAS − final VAS) were compared.
Data entry and analysis were done using IBM SPSS Statistics software ver. 20.0 (IBM CO., Armonk, NY, USA) and p value < 0.05 was considered significant.
Results
We found that in general VAS scores was lower in the injec-tion group (n = 85) than the oral steroid group (n = 88) and injection group (n = 85) in the 3 week, 2, 4, 6 month follow (Fig. 1). Although the difference between the groups was statistically insignificant, we found in both groups a greater than 50% de-crease in pain at 6 month final follow-up. The changes in UCLA score were statistically insignificant between the two groups over the entire follow-up (Fig. 2). A statistically significant difference in terms of the ROM between the two groups was seen initially.
Fig. 1. This graph shows the average change of visual analogue scale (VAS) score between oral medication group and intra-articular injection group. No statistically significant difference was seen.

Low-dose Oral Corticosteroid Therapy of Impingement Syndrome of the ShoulderYoung Bok Kim, et al.
www.cisejournal.org 53
The forward flexion (t-test, p = 0.007) and the internal rotation (t-test, p = 0.4) at 2 month follow-up were better in patients of the injection group (n = 25) with joint stiffness than the oral
steroids group (n = 28) with joint stiffness, and this statistically significant was still seen at 4 month follow-up for forward flexion (t-test, p = 0.02) and internal rotation (t-test, p = 0.02); how-ever, it was no longer seen at the final follow-up (Fig. 3).
We assessed side-effects of drugs and postoperative compli-cations between the two groups. In the oral steroids groups, we found an average weight gain of 2.3 kg/8 weeks in 5 patients, upper abdominal discomfort and pain in 11, loss of glucose control in 4 of the 18 diabetic patients 18, hot flushing in 1, en-hanced appetite in 4. But none of these patients had side-effects or complications severe enough to stop the drug administration altogether. In the injection group, we found an average weight gain of 1.4 kg/8 weeks in 3 patients, upper abdominal discom-fort in 2, steroid flare after injection in 9, enhanced appetite in 2, and hyperglycemia in 5 of the 16 diabetic patients. In neither of the two patient groups, none were seen to have complica-tion such as focalized or systemic infections or drug withdrawal symptoms such as adrenal insufficiency.
The total recurrences and non-compliant patients were 26% in the oral steroids group (23/88) and 22% in the injection group
Fig. 2. This graph shows the average change of University of California at Los Angeles (UCLA) score between oral medication group and intra-articular injection group. No statistically significant difference was seen.
Fig. 3. This graph shows progress of range of motion (ROM) in stiff patients. Forward flexion (A) and internal rotation (B) of ROM are significantly improved more in the injection group. (C) External rotation at side. (D) External rotation at 90o abduction.
54 www.cisejournal.org
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014
(19/85) at the final follow-up.Patients in the oral steroid group (n = 88) were subdivided
within various demographic, clinical, and radiographic catego-ries that were thought possible to influence the treatment out-come of the oral therapy. We determined whether each factor were associated with changes in UCLA score (final UCLA−initial UCLA), improvement in VAS (initial VAS−final VAS) at the final follow up.
In terms of demographic factors, sex did not influence the improvement in the UCLA and VAS scores when these scores were compared between men (n = 37) and women (n = 51) in the oral steroids group. Likewise, age (below or over 40) did not influence the clinical outcomes.
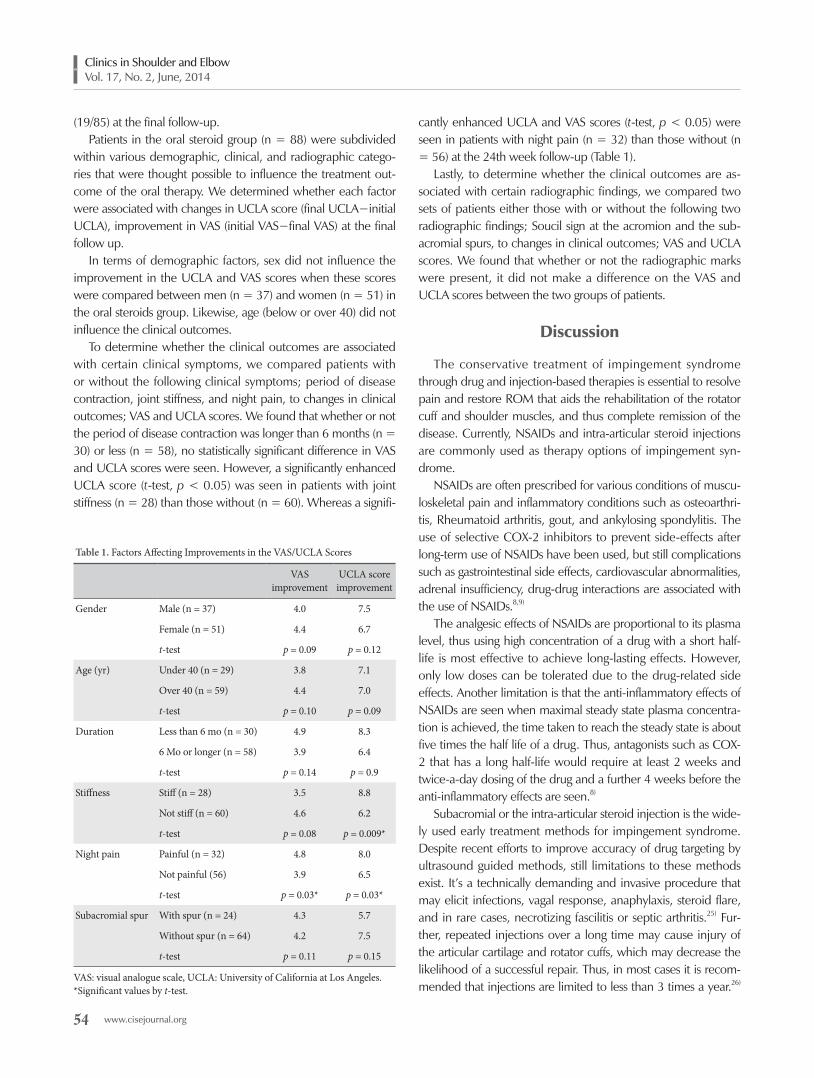
To determine whether the clinical outcomes are associated with certain clinical symptoms, we compared patients with or without the following clinical symptoms; period of disease contraction, joint stiffness, and night pain, to changes in clinical outcomes; VAS and UCLA scores. We found that whether or not the period of disease contraction was longer than 6 months (n = 30) or less (n = 58), no statistically significant difference in VAS and UCLA scores were seen. However, a significantly enhanced UCLA score (t-test, p < 0.05) was seen in patients with joint stiffness (n = 28) than those without (n = 60). Whereas a signifi-
cantly enhanced UCLA and VAS scores (t-test, p < 0.05) were seen in patients with night pain (n = 32) than those without (n = 56) at the 24th week follow-up (Table 1).
Lastly, to determine whether the clinical outcomes are as-sociated with certain radiographic findings, we compared two sets of patients either those with or without the following two radiographic findings; Soucil sign at the acromion and the sub-acromial spurs, to changes in clinical outcomes; VAS and UCLA scores. We found that whether or not the radiographic marks were present, it did not make a difference on the VAS and UCLA scores between the two groups of patients.
Discussion
The conservative treatment of impingement syndrome through drug and injection-based therapies is essential to resolve pain and restore ROM that aids the rehabilitation of the rotator cuff and shoulder muscles, and thus complete remission of the disease. Currently, NSAIDs and intra-articular steroid injections are commonly used as therapy options of impingement syn-drome.
NSAIDs are often prescribed for various conditions of muscu-loskeletal pain and inflammatory conditions such as osteoarthri-tis, Rheumatoid arthritis, gout, and ankylosing spondylitis. The use of selective COX-2 inhibitors to prevent side-effects after long-term use of NSAIDs have been used, but still complications such as gastrointestinal side effects, cardiovascular abnormalities, adrenal insufficiency, drug-drug interactions are associated with the use of NSAIDs.8,9)
The analgesic effects of NSAIDs are proportional to its plasma level, thus using high concentration of a drug with a short half-life is most effective to achieve long-lasting effects. However, only low doses can be tolerated due to the drug-related side effects. Another limitation is that the anti-inflammatory effects of NSAIDs are seen when maximal steady state plasma concentra-tion is achieved, the time taken to reach the steady state is about five times the half life of a drug. Thus, antagonists such as COX-2 that has a long half-life would require at least 2 weeks and twice-a-day dosing of the drug and a further 4 weeks before the anti-inflammatory effects are seen.8)
Subacromial or the intra-articular steroid injection is the wide-ly used early treatment methods for impingement syndrome. Despite recent efforts to improve accuracy of drug targeting by ultrasound guided methods, still limitations to these methods exist. It’s a technically demanding and invasive procedure that may elicit infections, vagal response, anaphylaxis, steroid flare, and in rare cases, necrotizing fascilitis or septic arthritis.25) Fur-ther, repeated injections over a long time may cause injury of the articular cartilage and rotator cuffs, which may decrease the likelihood of a successful repair. Thus, in most cases it is recom-mended that injections are limited to less than 3 times a year.26)
Table 1. Factors Affecting Improvements in the VAS/UCLA Scores
VAS improvement
UCLA score improvement
Gender Male (n = 37) 4.0 7.5
Female (n = 51) 4.4 6.7
t-test p = 0.09 p = 0.12
Age (yr) Under 40 (n = 29) 3.8 7.1
Over 40 (n = 59) 4.4 7.0
t-test p = 0.10 p = 0.09
Duration Less than 6 mo (n = 30) 4.9 8.3
6 Mo or longer (n = 58) 3.9 6.4
t-test p = 0.14 p = 0.9
Stiffness Stiff (n = 28) 3.5 8.8
Not stiff (n = 60) 4.6 6.2
t-test p = 0.08 p = 0.009*
Night pain Painful (n = 32) 4.8 8.0
Not painful (56) 3.9 6.5
t-test p = 0.03* p = 0.03*
Subacromial spur With spur (n = 24) 4.3 5.7
Without spur (n = 64) 4.2 7.5
t-test p = 0.11 p = 0.15
VAS: visual analogue scale, UCLA: University of California at Los Angeles.*Significant values by t-test.

Low-dose Oral Corticosteroid Therapy of Impingement Syndrome of the ShoulderYoung Bok Kim, et al.
www.cisejournal.org 55
NSAIDs and intra-articular steroid injection are widely used for impingement syndrome and other acute and chronic musculo-skeletal diseases, but although the former is a safe option its po-tency is weak, whereas the latter has an extremely potent effect but its associated side-effects limit its use.
For decades, the treatment of frozen shouder have used high dose of oral steroids. We investigated short-term low-dose oral steroids as a possible therapy for impingement syndrome for two major reasons. First, its anti-inflammatory effects are greater than NSAIDs and it does not require the technical expertise of ad-ministration and also eliminates the related risks of the invasive procedures. We compared the clinical outcomes of oral steroids and intra-articular injections, and further determined possible factors that influence the clinical outcomes in oral steroid use, and thereby assess what possible indicators there are for oral ste-roids. Historically, potency comparable to the potency of pred-nisolone 5−10 mg/day is considered as a low-dose and the au-thors considered duration of 4 weeks as short-term. In this study, we administered triamcinolone 4 mg/day to patients, which has the same potency as prednisolone, for 4 weeks.
Irrespective of the route of administration, the major concerns of exogenous steroids are Cushing syndrome or drug side-effects such as hypothalamic-pituitary-adrenal (HPA) axis inhibition. The likelihood of such complication surfacing increases when exogenous steroids are taken for more than 6−12 months, and in general, the incidence of complications is proportional to the average drug volume and duration. In a large-scale study where corticosteroids to a potency equaling the potency of mean 16 ± 14 mg/day of prednisolone was given for over 60 days, the most common side-effect associated with drug administration was weight-gain (70%), which was followed by bruising and thin-ning of the skin, and insommia. The most fatal side-effects were cataracts (15%) and bone fractures (12%).13) Low-dose steroid use of over 2 years was associated with mean 4−8% increase in weight-gain, and use of over 90 days showed a statistically signif-icant association with weight-gain.27) Although these side-effects should not be dismissed even when small doses of steroids are administered, many side-effects seen from high-dose therapies have been unnecessarily connected to low-dose therapy despite a very small likelihood of manifesting.27) Including the weight loss period, during the period of 4 weeks of drug administration, the authors found trivial weight-gain and gastrointestinal dysfunc-tion in a small portion of patients. No other complications were noted.
The benefits of short-term low-dose oral steroids were lower than the benefits of the intra-articular injections. The mean ex-tent of pain-relief was shown to be lower through the period of the treatment, and especially, if drug dose was lowered or ceased, the tendency for the pain to resurface was greater in the oral steroid group. Further, improvement in ROM was lower for the oral steroid group than the injection group. Although all
mean clinical results were slightly lower than the injection group, it did not influence the patients’ ability to follow the rehabilita-tion program and also there were no statistically significant dif-ferences between the two groups across the whole study.
Factors associated with more improvement in the clinical outcome within the oral steroid group was seen in the patients with night pain and joint stiffness. However, rather than to say these factors are indicators for oral steroid medication per say, these findings probably result from an emphasized improvement in patients with these factors who were more symptomatic and had a capacity to improve from inflammatory state and stiffness.
In this study, we found that there were no statistically signifi-cant differences in the clinical outcomes we assessed between the oral corticosteroid therapy and intra-articular steroid injec-tion. Although, we found that all mean clinical outcomes were higher in the injection group than the oral steroid group across the whole follow-up, we believe that the oral steroid therapy can partially substitute the injection method to treat the early phase of impingement syndrome without mechanical injury of the rotator cuff, which is not associated with other underlying conditions.
Our study determined the efficacy of short-term low-dose oral corticosteroids in therapy of impingement syndrome, and assessed for associated complications. We compared the clini-cal outcomes to those of NSAIDs and injection therapies to see whether oral steroids can be substituted as a replacement. However, a limitation to our study is that the changes in clini-cal factors relating to the HPA axis such as plasma cortisol level, electrolyte level, glycemic levels were not looked into. Another limitation is that volume and dose-response relationships of oral steroids were not analyzed. Thus, further studies are required to address these issues.
Conclusion
Using short-term oral corticosteroids as an anti-inflammatory treatment for impingement syndrome of the shoulder show clini-cal outcomes comparable to those of intra-articular injection, es-pecially in terms of pain control. Oral corticosteroids don’t have remarkable complications or side effects. Although the beneficial effects are less obvious in patients with combined joint stiffness, all in all short term oral corticosteroids can be considered as a partial alternative of intra-articular injections for impingement syndrome in which inflammatory pain is the main clinical symp-tom.
References
1. Almekinders LC. Impingement syndrome. Clin Sports Med. 2001;20(3):491-504.
2. Morrison DS, Frogameni AD, Woodworth P. Non-operative
56 www.cisejournal.org
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014
treatment of subacromial impingement syndrome. J Bone Joint Surg Am. 1997;79(5):732-7.
3. Bartolozzi A, Andreychik D, Ahmad S. Determinants of out-come in the treatment of rotator cuff disease. Clin Orthop Relat Res. 1994;(308):90-7.
4. Goldberg SS, Bigliani LU. Shoulder impingement revisited: advanced concepts of pathomechanics and treatment. Instr Course Lect. 2006;55:17-27.
5. Williams GR Jr, Rockwood CA Jr, Bigliani LU, Iannotti JP, Stan-wood W. Rotator cuff tears: why do we repair them? J Bone Joint Surg Am. 2004;86-A(12):2764-76.
6. Cummins CA, Sasso LM, Nicholson D. Impingement syn-drome: temporal outcomes of nonoperative treatment. J Shoulder Elbow Surg. 2009;18(2):172-7.
7. Cakmak A. Conservative treatment of subacromial impinge-ment syndrome. Acta Orthop Traumatol Turc. 2003;37 Suppl 1:112-8.
8. Kaplan B, Swain RA. NSAIDs. Are there any differences? Arch Fam Med. 1993;2(11):1167-74.
9. Ong CK, Lirk P, Tan CH, Seymour RA. An evidence-based up-date on nonsteroidal anti-inflammatory drugs. Clin Med Res. 2007;5(1):19-34.
10. Green S, Buchbinder R, Hetrick S. Physiotherapy inter-ventions for shoulder pain. Cochrane Database Syst Rev. 2003;(2):CD004258.
11. von Essen R, Savolainen HA. Bacterial infection following intra-articular injection. A brief review. Scand J Rheumatol. 1989;18(1):7-12.
12. Kumar N, Newman RJ. Complications of intra- and peri-articu-lar steroid injections. Br J Gen Pract. 1999;49(443):465-6.
13. Curtis JR, Westfall AO, Allison J, et al. Population-based assess-ment of adverse events associated with long-term glucocorti-coid use. Arthritis Rheum. 2006;55(3):420-6.
14. Czock D, Keller F, Rasche FM, Häussler U. Pharmacokinetics and pharmacodynamics of systemically administered glucocor-ticoids. Clin Pharmacokinet. 2005;44(1):61-98.
15. Blockey NJ, Wright JK, Kellgren JH. Oral cortisone therapy in periarthritis of the shoulder; a controlled trial. Br Med J. 1954;1(4877):1455-7.
16. Buchbinder R, Hoving JL, Green S, Hall S, Forbes A, Nash P. Short course prednisolone for adhesive capsulitis (frozen
shoulder or stiff painful shoulder): a randomised, double blind, placebo controlled trial. Ann Rheum Dis. 2004;63(11):1460-9.
17. Widiastuti-Samekto M, Sianturi GP. Frozen shoulder syn-drome: comparison of oral route corticosteroid and intra-artic-ular corticosteroid injection. Med J Malaysia. 2004;59(3):312-6.
18. Lorbach O, Anagnostakos K, Scherf C, Seil R, Kohn D, Pape D. Nonoperative management of adhesive capsulitis of the shoul-der: oral cortisone application versus intra-articular cortisone injections. J Shoulder Elbow Surg. 2010;19(2):172-9.
19. Park HB, Yokota A, Gill HS, El Rassi G, McFarland EG. Di-agnostic accuracy of clinical tests for the different degrees of subacromial impingement syndrome. J Bone Joint Surg Am. 2005;87(7):1446-55.
20. Neviaser RJ, Neviaser TJ. The frozen shoulder. Diagnosis and management. Clin Orthop Relat Res. 1987;(223):59-64.
21. Ellman H. Diagnosis and treatment of incomplete rotator cuff tears. Clin Orthop Relat Res. 1990;(254):64-74.
22. Mallon WJ, Herring CL, Sallay PI, Moorman CT, Crim JR. Use of vertebral levels to measure presumed internal rotation at the shoulder: a radiographic analysis. J Shoulder Elbow Surg. 1996;5(4):299-306.
23. Buchbinder R, Green S, Youd JM. Corticosteroid injec-tions for shoulder pain. Cochrane Database Syst Rev. 2003;(1):CD004016.
24. van der Goes MC, Jacobs JW, Boers M, et al. Monitoring adverse events of low-dose glucocorticoid therapy: EULAR recommendations for clinical trials and daily practice. Ann Rheum Dis. 2010;69(11):1913-9.
25. Hopper JM, Carter SR. Anaphylaxis after intra-articular injec-tion of bupivacaine and methylprednisolone. J Bone Joint Surg Br. 1993;75(3):505-6.
26. Watson M. Major ruptures of the rotator cuff. The re-sults of surgical repair in 89 patients. J Bone Joint Surg Br. 1985;67(4):618-24.
27. Da Silva JA, Jacobs JW, Kirwan JR, et al. Safety of low dose glucocorticoid treatment in rheumatoid arthritis: pub-lished evidence and prospective trial data. Ann Rheum Dis. 2006;65(3):285-93.

The Effect of Different Starting Periods of Passive Exercise on the Clinical Outcome of Arthroscopic Rotator Cuff Repair
Young-Woong Back, Suk-Kee Tae, Min-Kyu Kim, Oh-Jin Kwon
Department of Orthopaedic Surgery, Dongguk University Ilsan Hospital, Goyang, Korea
Background: To compare the effect of different starting periods of rehabilitative exercise (early or delayed passive exercise) on the rate of retear and other clinical outcomes after the arthroscopic repair of the rotator cuff.Methods: In total, 103 patients who underwent arthroscopic repair of the rotator cuff were included in the study. Determined at 2 weeks post-operation, patients who were incapable of passive forward elevation greater than 90˚ were allotted to the early exercise group (group I: 79 patients; 42 males, 37 females), whilst those capable were allotted to the delayed exercise group (group II: 24 pa-tients; 14 males, 10 females). The group I started passive exercise, i.e. stretching, within 2 weeks of operation, whilst group II started within 6 weeks. The results were compared on average 15.8 months (11-49 months) post-operation using the passive range of motion, the Visual Analog Scale (VAS) pain score, and the University of California at Los Angeles (UCLA) and Constant scores. Stiffness was de-fined as passive forward elevation or external rotation of less than 30˚ compared to the contralateral side. Follow-up magnetic resonance imaging (MRI) was carried out on average 1 year post-operation and the rate of retear was compared with Sugaya’s criteria.Results: There were no differences between the two groups in gender, age, smoking, presence of diabetes, arm dominance, period of tear unattended, pre-operative range of motion, shape and size of tear, degree of tendon retraction, and tendon quality. There were no significant differences in clinical outcomes. Whilst stiffness was more frequent in group II (p-value 0.03), retear was more frequent in group I (p-value 0.028) according to the MRI follow-up.Conclusions: During rehabilitation after the arthroscopic repair of the rotator cuff, the delay of passive exercise seems to decrease the rate of retear but increase the risk of stiffness.(Clin Shoulder Elb 2014;17(2):57-63)
Key Words: Shoulder; Rotator cuff repair; Immobilization; Rehabilitation; Stiffness
Introduction
Arthroscopic surgery is widely carried out for the repair of the rotator cuff.1-3) However, retear after surgery is common, ranging from a rate of 25%4) up to 94%5) as observed by many research-ers and in clinical studies.6,7) There are several factors, biological and environmental, contributing to the retear of the rotator cuff. The biological factors include the patient’s age,6) the size of the tear,8) period of tear unattended,9) and the health and genetic disposition of the patient.10,11) The environmental factors include the patient’s working conditions, the rehabilitative exercise undertaken, the use of nonsteroidal anti-inflammatory drugs,
smoking, etc.12-14)
In the past, doctors have recommended the delayed passive exercise in order to lower the rate of retear. However, the con-sequent prolonged period of stabilization have led to a higher rate of stiffness.15-17) To counter this, early passive exercise was pursued,18) but the starting period of rehabilitative passive exer-cise that harbors the minimal risk of both retear and stiffness is still controversial. For instance, Parsons et al.19) favors the delayed passive exercise on the grounds that a prolonged stabilization period of 6 weeks is beneficial for repair and also reduces the risk of stiffness.
Thus, our study aims to identify whether delayed passive ex-
CiSEClinics in Shoulder and Elbow
Copyright © 2014 Korean Shoulder and Elbow Society. All Rights Reserved.This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
pISSN 1226-9344eISSN 2288-8721
ORIGINAL ARTICLE
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014http://dx.doi.org/10.5397/cise.2014.17.2.57
Received October 25, 2013. Revised January 20, 2014. Accepted March 7, 2014.
Correspondence to: Suk-Kee TaeDepartment of Orthopaedic Surgery, Dongguk University Ilsan Hospital, 27 Dongguk-ro, Ilsandong-gu, Goyang 410-773, KoreaTel: +82-31-961-7310, Fax: +82-31-961-7312, E-mail: [email protected]
Financial support: None. Conflict of interests: None.

58 www.cisejournal.org
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014
ercise indeed reduces the rate of retear and increases the rate of stiffness after the arthroscopic repair of the rotator cuff.
Methods
Subject of StudyFrom January 2005 to May 2012, 243 patients underwent
arthroscopic repair of the full-thick tear in the supraspinatus or infraspinatus. Of these, 43 patients with the following co-morbidities were excluded; fracture, history of previous shoulder surgery, severe degeneration of the glenohumeral joint, inflam-matory disease or infection, calcifying tendinitis (in which stiff-ness is common after surgery20)), superior labral tear from ante-rior to posterior (SLAP) tear, and/or Bankart tear. The remaining 200 patients were followed-up 1 year after surgery, and of these, 155 patients were included in the post-operative magnetic resonance imaging (MRI). Surgery was undertaken by the same surgeon. Patients were anaesthetized and checked for the range of motion. If rotation beyond 130˚ was possible, manipulation was carried out before arthroscopic repair. The size of the rota-tor cuff tear and the length of the retraction were measured using a probe. The measurement was carried out after marginal debridement of the affected tendon. Further 52 patients were excluded; in accordance with the measurements, 41 patients with a rotator cuff tear smaller than 1.5 cm and 11 patients who underwent incomplete repair were also excluded. Data of the remaining 103 patients were analyzed for the study (Fig. 1).
Patients were visited between 1-2 weeks post-operation in order to be allotted into the two groups. Patients who were ca-
pable of passive forward elevation greater than 90˚ were allot-ted to the delayed exercise group. Here, the risk of stiffness due to prolonged stabilization was deemed low. Patients incapable of this elevation were allotted to the early exercise group. The early exercise group (group I: 79 patients; 42 males, 37 females; aver-age age 58.5 years, range 29-77 years) started passive stretching exercise within 2 weeks post-operation, whilst the late exercise group (group II: 24 patients; 14 males, 10 females; average age 60.1 years, range 50-72 years) started at 6 weeks post-operation.
Method of AssessmentThe results of the two groups were analyzed using both clini-
cal and radiologic assessments. Clinical assessments were carried out before the surgery, and 12 months post-operation using University of California at Los Angeles (UCLA) score,21) Constant score,22) and Visual Analogue Scale (VAS) pain scores. Radiologic assessments were also carried out at 12 months post-operation using MRI to identify retear. The definition of stiffness in the context of the shoulder joint is based on the decreased ability of passive forward elevation and external rotation, but not on abduction internal rotation. Specifically, stiffness is defined as passive forward elevation or external rotation of less than 30˚ compared to the contralateral side. Retear was assessed against the Sugaya’s criteria23) during the follow-up MRI scan by the surgeon and one other orthopedic specialist. Grade 4 or 5 were classed as retear (Fig. 2), but otherwise (grade 1, 2, 3) classed as no retear (Fig. 3). Furthermore, the risk factors of retear were compared between the two groups. The risk factors include; gender, age, presence of diabetes, smoking, arm dominance,
Fig. 1. Patient selection algorithm. MRI, magnetic resonance imaging.

The Effect of Starting Periods of Passive Exercise after Arthroscopic Rotator Cuff RepairYoung-Woong Back, et al.
www.cisejournal.org 59
period of tear unattended, pre-operative range of motion, size and shape of tear, tendon quality, degree of tendon retraction, duration of operation, start period of rehabilitative passive exer-cise (within 2 weeks or 6 weeks post-operation), and the degree of pre-operative fatty degeneration in rotator cuff as assessed by the global fatty degeneration index (GFDI)24) obtained by MRI. The GFDI is the average of the degrees of fatty degeneration, obtained by Goutallier’s classficiation,24) in the 3 muscles that meet at the Scapular Y-shape. Observed in the sagittal oblique view, the Scapular Y-shape is where the spine and the scapular body meets. The size of tear was classified according to the DeOrio and Cofield criteria.25)
Surgery Procedure and Rehabilitation ProgramThe following arthroscopic procedures were used; single-row
repair, double-row repair, or suture-bridge technique. Eighty-six patients (78.9%) underwent acromioplasty. To control for the possible effect of the tendon quality on retear, the quality of the torn tendon was recorded by the subjective assessment of the surgeon during the operation. Using a probe, the thicknesses of
the frontal, central and rear side of the torn tendon were mea-sured. The mean values were then classed as follows; above 10 mm as good (16 patients, 14.7%), between 5-10 mm as aver-age (83 patients, 76.1%), and below 5 mm as poor (83 patients, 76.1%). Tendons, regardless of their thickness, that were torn easily when pulled with a grasper were also classed as poor.
All patients were given a stabilization brace to support the rotator cuff after the operation. Also, they were given advice to actively move their hands, wrists and elbow joints right after the operation. At 1-2 weeks post-operation, patients were followed-up to check passive forward elevation. Patients capable of el-evation greater than 90˚ maintained the stabilizer for 4 weeks (until 6 weeks post-operation) without passive or active exercise. Patients incapable of this degree of elevation also maintained the stabilizer for the same period but were immediately started on passive pendulum motion exercise in which the pendulum motion was increased progressively. This progressive increase in motion was within a range that did not cause pain and was car-ried out for one minute, 3 to 5 times a day.
At 6 weeks post-operation, stabilizers were removed regard-
Fig. 2. (A) Preoperative T2-weighted coronal magnetic resonance image shows rotator cuff tear. (B) One-year postoperative magnetic resonance image shows retear of the supra-spinatus tendon.
Fig. 3. (A) Preoperative T2-weighted coronal magnetic resonance image shows rotator cuff tear. (B) One-year postoperative magnetic resonance image shows healed rotator cuff.

60 www.cisejournal.org
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014
less of the state of stiffness. At this point, the following exercises were started on the affected arm; pendulum motion exercise, passive elevation exercise, and passive external rotation exercise using the T-bar. The effectiveness of the passive forward eleva-tion and external rotation exercises were maximized by repeat-ing the following sequence 10-20 times; holding the maximal position (i.e., the greatest angle of motion) for 10 seconds fol-lowed by relaxation for 5 seconds. The exercises took 5-10 minutes to complete and were repeated 3-6 times a day. Next, at 3 months post-operation, exercises to strengthen the rotator cuff and the periscapular muscles were started. To strengthen the rotator cuff, active internal and external rotation exercises were carried out using Theraband products (Breg Inc., Carlsbad, CA, USA). Band resistance was chosen at a slight difficulty ac-
cording to the patient’s capability after 10 pulls. Resistance was increased if patients felt no difficulty even after 15 pulls. The exercises were carried out twice a day with 5 repeats each time. To strengthen the periscapular muscles, shoulder hunching and standing wall push-ups were carried out. Further, at 4 months post-operation, deltoid muscle strengthening exercises were started, and finally at 6 months post-operation all exercises and activities were allowed to pre-operative levels.
Statistical AnalysisStatistical data were analyzed by SPSS for windows release
ver. 17.0 (SPSS Inc., Chicago, IL, USA), and statistical signifi-cance was considered as p-value <0.05. The Fisher’s exact test was used to assess the correlation between the size of tear and
Table 1. Patient Demographics and Clinical Features
Early exercise group Delayed exercise group p-value
Age (yr) 58.51 ± 9.72 (39-77) 60.08 ± 7.02 (50-72) 0.462*
Gender (n) 0.656†
Male 42 14
Female 37 10
Diabetes mellitus (n) 6 3 0.456†
Smoking (n) 11 3 0.859†
Op. side: dominant (n) 17 9 0.114†
Preop. duration of symptom (mo) 16.1 ± 5.74 (1-46) 15.4 ± 6.61 (2-57) 0.223*
Preop. PFE (˚) 152.5 ± 17.05 (90-180) 149.16 ± 24.83 (50-180) 0.483*
Preop. PER (˚) 52.17 ± 11.16 (20-70) 48.25 ± 8.75 (30-60) 0.252*
Postop. PFE (˚) 154.3 ± 14.95 (60-170) 153.95 ± 16.21 (105-180) 0.84*
Postop. PER (˚) 48.67 ± 11.37 (10-70) 49.17 ± 9.28 (30-70) 0.90*
Size of tear (cm) 2.24 ± 0.96 (1-6) 2.51 ± 0.95 (1.5-5) 0.23*
Retraction (cm) 1.93 ± 0.67 (1-4) 1.98 ± 0.52 (1-3) 0.72*
Duration of surgery (min) 137.25 ± 21.31 (89-182) 151.47 ± 17.2 (92-178) 0.562*
Quality of tendon (n) 0.715†
Good 7 2
Fair 61 17
Poor 11 5
Shape of tear (n) 0.067†
Crescent 41 11
U-shape 12 2
L-shape 14 10
Reverse L-shape 12 1
GFDI 1.04 ± 0.53 1.10 ± 0.58 0.659†
Values are presented as mean ± standard deviation (range) or number only. Op.: operative, Preop.: preoperative, Postop.: postoperative, PFE: passive forward elevation, PER: passive external rotation, GFDI: Global Fatty Degeneration In-dex.*Independent t-test, †chi-square test.

The Effect of Starting Periods of Passive Exercise after Arthroscopic Rotator Cuff RepairYoung-Woong Back, et al.
www.cisejournal.org 61
subsequent retear. The paired t-test was used to compare func-tional outcome before and after operation. The chi-square test was used to compare the rate of retear and of stiffness between the two groups and an independent t-test was used to compare functional outcome. To assess the variables that might have an effect on the results, the chi-square and independent t-tests were used.
Results
Patient DemographicsGroup I and II had no significant differences (p>0.05, Table
1) in the following variables; gender, age, presence of diabe-tes, smoking, arm dominance, period of tear unattended, pre-operative range of motion, size of tear, tendon quality, degree of tendon retraction, duration of operation, and GFDI as assessed by pre-operative MRI.
Clinical OutcomesAll clinical assessments, including the pain score, and UCLA
and Constant scores, showed a statistically significant improve-ment at one year post-operation. The pain score improved from an average of 6.2 to 1.2, the UCLA score from 17.2 to 31.9 and the Constant score from 42.1 to 70.1 (Table 2).
A difference between the 2 groups in the pain scores and clinical tests exists but is statistically insignificant. For each group, the pain scores were 1.13 and 0.9 (p=0.09), respectively, and the Constant scores were 69.8 and 72.5 (p=0.18), respectively.
All clinical and pain tests indicate an improved outcome in the delayed exercise group. However, the differences are small and statistically insignificant (Table 3).
Rate of Retear and Rate of StiffnessOf the 38 patients with retear, most had improved pain
scores and clinical outcomes compared to pre-operation. Of these, 7 retear patients expressed discomfort in daily activities and consequently, one patient underwent corrective surgery. Retear was more common in group I, whilst stiffness was more common in group II. The rate of retear is significantly greater in the group I than in group II (43%, 34 out of 79 patients vs. 16.7%, 4 out 24 patients) (p=0.028) (Table 4). The rate of stiff-ness is significantly greater in group II than in group I (20.8%, 5 out of 24 vs. 5.1%, 4 out of 79 patients) (p=0.03) (Table 4).
Discussion
The ultimate aim of the repair of the rotator cuff is to main-tain the integrity of the repaired rotator cuff, thus relieving pain and recovering its original function. Of the various risk factors for retear, post-operative rehabilitation is the most obvious vari-able that can be intervened by doctors. However, rehabilitative method and starting period must be chosen appropriately since it coincides with the possibility of post-operative occurrence of stiffness. In fact, stiffness is the most common complication after the repair of the rotator cuff by open surgery.17,18,26) Accordingly, early rehabilitative exercises were emphasized in the past,18,27) and Raab et al.28) argued for the positive effects of early exer-cises upon pain reduction and recovery of the range of motion. Conversely, the negative effects of early exercise on recovery have also been noted.4) A number of authors have argued for a prolonged stabilization period, i.e. delayed exercise, after the arthroscopic repair of the rotator cuff,19,29) but admitted the risk of consequent complications such as a reduced range of mo-tion and the increased rate of stiffness. In fact, Brislin et al.16) reports a rate of stiffness at 8.6% (23 out of 268 patients) after
Table 2. Clinical Outcomes after Arthroscopic Rotator Cuff Repair Exclud-ing Small Size Tear (103 cases)
Preoperative Postoperative (at 1 year) p-value*
Clinical outcomes
VAS pain score 6.2 1.2 0.028
UCLA score 17.2 31.9 0.003
Constant score 42.1 70.1 0.000
VAS: Visual Analog Scale, UCLA: University of California at Los Angeles. *Paired t-test.
Table 3. Comparison Analysis of Clinical Outcomes at Postoperative One Year Follow-up Period between Early and Delayed Exercise Groups
Early exercise group Delayed exercise group p-value*
Clinical outcomes
VAS pain score 1.1 0.9 0.12
UCLA score 32.5 33.0 0.09
Constant score 69.8 72.5 0.18
VAS: Visual Analog Scale, UCLA: University of California at Los Angeles.*Independent t-test.
Table 4. The Rate of Retear and the Incidence of Stiffness between Early and Delayed Exercise Groups
Early exercise group
Delayed exercise group p-value*
The rate of retear
Retear 34 (43.0%) 4 (16.7%) 0.028
Intact 45 20
The incidence of stiffness
Stiffness 4 (5.1%) 5 (20.8%) 0.03
Intact 75 19
*Chi-square test.

62 www.cisejournal.org
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014
the arthroscopic repair of the rotator cuff. In a study of a similar context, Kim et al.30) investigated the starting period of passive exercise in the repair of rotator cuffs with small- and medium-sized tears. In contrast to our study, they reported no differences between the different starting periods on the rate of retear or on the range of motion. However, it is important to note that we have excluded, unlike Kim et al.,30) small-sized tears because the rate of retear is generally low in this category. Thus, our study of the repair of rotator cuffs with medium-size or above tears, indicates that delayed passive exercise may reduce the rate of retear. The delayed exercise group had better range of motion at right after surgery, but had significantly higher rates of stiffness at the one year follow-up than the early exercise group. Although the early and delayed exercise groups did not differ in average degree of motion range, delayed exercise seems to be correlated with the occurrence of stiffness.
In accordance with our results, we recommend the delay of passive exercise to reduce the risk of retear after the repair of the rotator cuff with tear of medium size or above. This is recommended in most cases, but in some cases, other protocol is needed, because stiffness is anticipated in particular patients. These patients, characterized by slow recovery of range of mo-tion, should be identified through careful observation of the range of motion in numerous follow-ups and started on early passive exercise to reduce the risk of stiffness.
What is different in our study is the definition of stiffness. In previous studies, such as in the delayed exercise study by Par-sons et al.,19) stiffness was defined as forward elevation below 100˚ or external rotation below 30˚. Our reason for newly de-fining stiffness is two-fold. Firstly, the range of motion fluctuates markedly between individuals and second, forward elevation greater than 100˚ can also negatively impact on daily activities.
The first limitation of this study is the small sample size. The risk of retear increases as the size of the tear increases. The num-ber of large and massive tears was 15 in the early group and 6 in the delayed group, and only 1 case of retear was observed in the delayed group. The second limitation is how the presence of retear or stiffness was judged. There is risk of subjective bias depending on the observer as well as selection bias. The third limitation is the learning curve effect of the surgeon. The study includes operations that have been carried out between 2008 and 2012, and thus the skill of the surgeon may have improved across the years. A majority of the delayed exercise group has had surgery after 2010, and therefore we cannot eliminate the possible learning curve effect on the lower rate of retear in this group. Finally, various repair methods were used to repair the rotator cuff tear; single-row repair, double-row repair, or com-bination techniques. We did not include suture technique as a variable in our study because of numerous reports that it does not affect the post-operative range of motion or risk of retear. However, we feel that the various use of techniques poses as a
possible limitation.
Conclusion
The delay of passive exercise after the arthroscopic repair of the rotator cuff may reduce the risk of retear, but increase the risk of stiffness in some patients. Thus, the appropriate starting period of passive exercise should consider the possible occur-rence of joint stiffness through careful observation of the range of motion by numerous follow-ups.
References
1. Bennett WF. Arthroscopic repair of massive rotator cuff tears: a prospective cohort with 2- to 4-year follow-up. Arthroscopy. 2003;19(4):380-90.
2. Brox JI, Gjengedal E, Uppheim G, et al. Arthroscopic surgery versus supervised exercises in patients with rotator cuff disease (stage II impingement syndrome): a prospective, randomized, controlled study in 125 patients with a 2 1/2-year follow-up. J Shoulder Elbow Surg. 1999;8(2):102-11.
3. Snyder SJ, Pachelli AF, Del Pizzo W, Friedman MJ, Ferkel RD, Pattee G. Partial thickness rotator cuff tears: results of ar-throscopic treatment. Arthroscopy. 1991;7(1):1-7.
4. Boileau P, Brassart N, Watkinson DJ, Carles M, Hatzidakis AM, Krishnan SG. Arthroscopic repair of full-thickness tears of the supraspinatus: does the tendon really heal? J Bone Joint Surg Am. 2005;87(6):1229-40.
5. Galatz LM, Ball CM, Teefey SA, Middleton WD, Yamaguchi K. The outcome and repair integrity of completely arthroscopi-cally repaired large and massive rotator cuff tears. J Bone Joint Surg Am. 2004;86-A(2):219-24.
6. Gazielly DF, Gleyze P, Montagnon C. Functional and anatomi-cal results after rotator cuff repair. Clin Orthop Relat Res. 1994;(304):43-53.
7. Gerber C, Fuchs B, Hodler J. The results of repair of massive tears of the rotator cuff. J Bone Joint Surg Am. 2000;82(4):505-15.
8. Wu XL, Briggs L, Murrell GA. Intraoperative determinants of rotator cuff repair integrity: an analysis of 500 consecutive re-pairs. Am J Sports Med. 2012;40(12):2771-6.
9. Chun JM, Song JS, Sohn DW. Clinical outcome and causative factor in patients of structural failure after rotator cuff repair. J Korean Shoulder Elbow Soc. 2008;11(1):29-36.
10. Gwilym SE, Watkins B, Cooper CD, et al. Genetic influences in the progression of tears of the rotator cuff. J Bone Joint Surg Br. 2009;91(7):915-7.
11. Tashjian RZ, Farnham JM, Albright FS, Teerlink CC, Cannon-Albright LA. Evidence for an inherited predisposition contrib-uting to the risk for rotator cuff disease. J Bone Joint Surg Am. 2009;91(5):1136-42.

The Effect of Starting Periods of Passive Exercise after Arthroscopic Rotator Cuff RepairYoung-Woong Back, et al.
www.cisejournal.org 63
12. Baumgarten KM, Gerlach D, Galatz LM, et al. Cigarette smok-ing increases the risk for rotator cuff tears. Clin Orthop Relat Res. 2010;468(6):1534-41.
13. Cohen DB, Kawamura S, Ehteshami JR, Rodeo SA. Indometh-acin and celecoxib impair rotator cuff tendon-to-bone healing. Am J Sports Med. 2006;34(3):362-9.
14. Galatz LM, Silva MJ, Rothermich SY, Zaegel MA, Havlioglu N, Thomopoulos S. Nicotine delays tendon-to-bone healing in a rat shoulder model. J Bone Joint Surg Am. 2006;88(9):2027-34.
15. Koo SS, Burkhart SS. Rehabilitation following arthroscopic ro-tator cuff repair. Clin Sports Med. 2010;29(2):203-11.
16. Brislin KJ, Field LD, Savoie FH 3rd. Complications after ar-throscopic rotator cuff repair. Arthroscopy. 2007;23(2):124-8.
17. Tauro JC. Stiffness and rotator cuff tears: incidence, ar-throscopic findings, and treatment results. Arthroscopy. 2006;22(6):581-6.
18. Mansat P, Cofield RH, Kersten TE, Rowland CM. Complications of rotator cuff repair. Orthop Clin North Am. 1997;28(2):205-13.
19. Parsons BO, Gruson KI, Chen DD, Harrison AK, Gladstone J, Flatow EL. Does slower rehabilitation after arthroscopic rotator cuff repair lead to long-term stiffness? J Shoulder Elbow Surg. 2010;19(7):1034-9.
20. Huberty DP, Schoolfield JD, Brady PC, Vadala AP, Arrigoni P, Burkhart SS. Incidence and treatment of postoperative stiff-ness following arthroscopic rotator cuff repair. Arthroscopy. 2009;25(8):880-90.
21. Ellman H, Hanker G, Bayer M. Repair of the rotator cuff. End-result study of factors influencing reconstruction. J Bone Joint Surg Am. 1986;68(8):1136-44.
22. Constant CR, Murley AH. A clinical method of func-tional assessment of the shoulder. Clin Orthop Relat Res. 1987;(214):160-4.
23. Sugaya H, Maeda K, Matsuki K, Moriishi J. Repair integrity and functional outcome after arthroscopic double-row rotator cuff repair. A prospective outcome study. J Bone Joint Surg Am. 2007;89(5):953-60.
24. Goutallier D, Postel JM, Gleyze P, Leguilloux P, Van Driessche S. Influence of cuff muscle fatty degeneration on anatomic and functional outcomes after simple suture of full-thickness tears. J Shoulder Elbow Surg. 2003;12(6):550-4.
25. DeOrio JK, Cofield RH. Results of a second attempt at surgi-cal repair of a failed initial rotator-cuff repair. J Bone Joint Surg Am. 1984;66(4):563-7.
26. Norberg FB, Field LD, Savoie FH 3rd. Repair of the rotator cuff. Mini-open and arthroscopic repairs. Clin Sports Med. 2000;19(1):77-99.
27. Mormino MA, Gross RM, McCarthy JA. Captured shoul-der: a complication of rotator cuff surgery. Arthroscopy. 1996;12(4):457-61.
28. Raab MG, Rzeszutko D, O’Connor W, Greatting MD. Early results of continuous passive motion after rotator cuff repair: a prospective, randomized, blinded, controlled study. Am J Or-thop (Belle Mead NJ). 1996;25(3):214-20.
29. Trenerry K, Walton JR, Murrell GA. Prevention of shoul-der stiffness after rotator cuff repair. Clin Orthop Relat Res. 2005;(430):94-9.
30. Kim YS, Chung SW, Kim JY, Ok JH, Park I, Oh JH. Is early pas-sive motion exercise necessary after arthroscopic rotator cuff repair? Am J Sports Med. 2012;40(4):815-21.

Changes in Matrix Metalloproteinase and Tissue Inhibitors of Metalloproteinase in Patients with Rotator Cuff Tears
Oh-Soo Kwon, Young-Yul Kim, Ji Yoon Ha, Han Bit Kang
Department of Orthopedic Surgery, The Catholic University of Korea, Daejeon St. Mary’s Hospital, Daejeon, Korea
Background: The purpose of this study was to determine whether in patients with rotator cuff tears a correlation exists between mo-lecular changes and clinical parameters such as age, duration of symptom, range of motion, and tear size. Molecular changes of matrix metalloproteinase (MMP) and tissue inhibitor of metalloproteinase (TIMP) were assessed by measuring messenger RNA (mRNA) levels of the two proteins. Methods: The rotator cuff tissue from was obtained from the edge of a torn tendon revealed after debridement by a motorized shaver. Using the sample of rotator cuff tissue, the reverse transcription polymerase chain reaction was performed to quantify MMP-2 and TIMP-2 mRNA expression. To determine whether mRNA levels and the clinical variables, such as age, defect size, range of motion (ROM) of shoulder, and duration of symptoms, show any correlation, Spearman’s correlation coefficients were used to test for significant differ-ences. Results: There was an inverse correlation between the mRNA levels of MMP-2 and TIMP-2 from the torn rotator cuff tendons regardless of the clinical variables. However, comparison of mRNA levels versus clinical parameters such as age, defect size, range of motion and duration of symptoms revealed a number of findings. We found a significant correlation between age and mRNA levels of MMP-2 from torn cuffs (r = 0.513, p = 0.021). Further, we found a significant correlation between defect size in the full thickness tears and mRNA levels of MMP-2 (r = 0.454, p = 0.045). Conversely, no significant association between mRNA levels of MMP-2 and ROM or duration of symptom was found. Conclusions: Our results suggest that both MMP-2 and TIMP-2 may be involved in the disease process of rotator cuff tears. Although the level of mRNA expression of MMP-2 and TMP-2 remain constant in torn rotator cuffs irrespective of the clinical variables, their levels may be influenced by age and defect size, which could account to change in tendon degradation and the healing process. (Clin Shoulder Elb 2014;17(2):64-67)
Key Words: Rotator cuff; Matrix metalloproteinase; Tissue inhibitor of metalloproteinase, Polymerase chain reaction
Introduction
Rotator cuff tears are common cause of pain in the shoulder joints.1) The rotator cuff is responsible for the dynamics stabil-ity of the shoulder joint and receives considerable stress during shoulder exercises. Rotator cuff tears manifest as pain in the shoulder joint that cause suboptimal function. The debilitating changes in rotator cuffs range from being a reversible tendini-tis to forming a tear across all levels of the rotator cuff. Natural
healing of rotator cuff tears without surgical intervention is dif-ficult, which is why open or arthroscopic repairs have been implemented and have been shown to give clinically successful outcomes.2-4) Despite a high rate of clinical success in the repairs in rotator cuff, studies that look at the biomolecular or histologi-cal patterns in the degenerative changes such as decrease in cell count, disorganization of fibrous tissue, formation of granulation tissue, glycosaminoglycan infiltration, changes in fibrocartilage, and calcification were noted that would eventually lead to
CiSEClinics in Shoulder and Elbow
Copyright © 2014 Korean Shoulder and Elbow Society. All Rights Reserved.This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
pISSN 1226-9344eISSN 2288-8721
ORIGINAL ARTICLE
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014http://dx.doi.org/10.5397/cise.2014.17.2.64
Received February 25, 2014. Revised March 20, 2014. Accepted April 30, 2014.
Correspondence to: Oh-Soo KwonDepartment of Orthopedic Surgery, The Catholic University of Korea, Daejeon St. Mary’s Hospital, 64 Daeheung-ro, Jung-gu, Daejeon 301-723, KoreaTel: +82-42-220-9248, Fax: +82-42-221-4120, E-mail: [email protected]
Financial support: None. Conflict of interests: None.

Changes in MMP and TIMP in Rotator Cuff TearsOh-Soo Kwon, et al.
www.cisejournal.org 65
complete tears. However, studies that look into the molecular mechanisms behind these changes are sparse.
Matrix metalloproteinase (MMP) is a biological enzyme that mediate breakdown of polypeptides, of which around 20 types are known so far. MMP is a zinc dependent endopeptidase that is essential to break down extracellular matrix components. The ability of MMP to regulate the extracellular medium contributes to local infiltration, vascularization, metastasis of tumor cells etc. MMP is classified according to the type of substrates they target. For example, MMP-1, -8, -13 are primary collagenases, and MMP-3, -10, -11 are streptolysins that target a broader range of substrates. The endogenous inhibitor of MMP is tissue inhibitor matrix metalloproteinase (TIMP). As an inhibitor that can inhibit the action of all known types of MMPs, any defects in TIMP expression, formation, and recycling, may lead to degenerative conditions such as rheumatoid arthritis. Other molecular func-tions of TIMPs exist, but in rotator cuff tears, the concentration of TIMP-3 has been apoptosis.5,6)
Of these, MMP-2 is an enzyme that can break down sub-stances such as gelatin at a fast rate, and its activity is essential for collagen breakdown in soft tissues. Animal studies that had used shoulder muscles to study the regenerative process have found increased expression of MMP-2 during the recovery period of the rotator cuff. Further, an increase in MMP-13 and IL-1b was proposed as a possible biomarker of an imminent rotator cuff tear.6,7) As such, this study aimed to look whether the expression of MMP and the expression of TIMP, the enzyme that inhibits MMP expression, are associated with clinical variables, such as age, duration of symptom, range of motion, and tear size in pa-tients with rotator cuff tears.
Methods
Tissues were obtained from each patient once consent was given and all consent forms were filled out by the patient. All procedures relating to human tissue sampling were approved by the human ethics review committee of The Catholic University of Korea, Daejeon St. Mary’s Hospital. Of the 20 rotator cuff tear patients, 13 had complete tears and 7 had partial tears. The tissues were obtained during the arthroscopic repair. The rela-tive ratio of male to female was 12:8. The mean age of patients was 59 years (range, 39−76 years), and the average duration of symptoms was 10 months (range, 3−24 months). Further, for patients with complete rotator cuff tears a probe with 1 mm in-crements was used to measure the defect size, and the average defect size was measured as 439 mm2 (range, 150−600 mm2).
The tissue were collected during arthroscopic debridement and stored in a -70oC freezer. For the quantification of mes-senger RNA (mRNA), primers against MMP-2, TIMP-2, MMP-9, and TIMP-1 were created (See Table 1 for primer sequences) and the reverse transcription polymerase chain reaction (RT-PCR) was performed. In brief, total RNA was extracted from the tissue using the Trizol kit (Invitrogen, Carlsbad, CA, USA). Then, complementary DNA (cDNA) was produced using the extracted RNA (2 mg) as template by reverse transcription using the Super-script system from Invitrogen. The conditions for RT-PCR were as follows; denaturation step for 3 min at 94oC, primer anneal-ing step for 1 min at 65oC, and extension step for 1 min at 72oC. The number of PCR cycle used was 35 cycles. To check for PCR products, electrophoresis at 70 V for 90 min was performed on all products on 1.5% agarose gels. The relative density of each band was measured using the Image J program (NIH, Bethesda, MD, USA).
Spearman correlation coefficients were calculated by SPSS program ver. 12.0 (SPSS Inc., Chicago, IL, USA) to determine correlation between the clinical variables (age, defect size, range of motion [ROM] of shoulder, and duration of symptoms) and
Table 1. The Sequence of Primers Used in the Experiment
Primer Sequences
MMP-2 (199 bp) Forward Reverse
5'-GGCCCTGTCACTCCGAGAT-3' 5'-GGCATCCAGGTTATCGGGGA-3'
TIMP-2 (400 bp) Forward Reverse
5'-GGCGTTTTGCAATGCAGATGTAG-3' 5'-CACAGGAGCCGTCACTTCTCTTG-3'
TIMP-1 (400 bp) Forward Reverse
5'-GCGGATCCAGCGCCCAGAGAGACAC-3' 5'-TTAAGCTTCCACTCCGGGCAGGATT-3'
MMP-9 (247 bp) Forward Reverse
5'-CACTGTCCACCCCTCAGAGC-3' 5'-GCCACTTGTCGGCGATAAGG-3'
GAPDH (200 bp) Forward Reverse
5'-TAAAGGGCATCCGGGCTACACT-3' 5'-TTACTCCTTGGAGGCCATGTAGG-3'
MMP: matrix metalloproteinase, TIMP: tissue inhibitor of metalloproteinase, GAPDH: glyceraldehyde 3-phosphate dehydrogenase.
Fig. 1. Electrophoresis of polymerase chain reaction products show bands at sizes ~370 bp and ~400 bp that represent expression of MMP-2 and TIMP-2, respectively. MMP: matrix metalloproteinase, TIMP: tissue inhibitor of metal-loproteinase, M: marker.

66 www.cisejournal.org
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014
mRNA levels. The level of significance was set at p < 0.05.
Results
We found that the MMP-2 and TIMP-2 were expressed in all patients irrespective of the clinical variables, and that the mRNA levels of MMP-2 and TIMP-2 were inversely proportional (Fig. 1, 2). The mRNA transcripts of MMP-9 and TIMP-1 were not ex-pressed in most samples, and similarly the mRNA level of TIMP-2 was expressed in very low amounts (Fig. 3). A correlation analysis of the expression level of the two mRNA transcripts with age, defect size, ROM and duration of symptoms showed that, the expression of MMP-2 mRNA is significantly correlated to age and defect size (r = 0.513, p = 0.021), but not ROM or dura-tion of symptoms (Table 2).
Discussion
MMP is important for tissue regeneration, and even though the exact mechanism is unknown, the overexpression of MMP
in muscle during tissue regeneration is thought to elicit lesions, especially under stress-induced conditions.8) Conversely, TIMP is involved in counteracting stress conditions. Further, MMP modu-lates expression of collagen and other extracellular matrix com-ponents important for the rotator cuff tear recovery process.8) Previous report has shown that in response to acute lesions, the rotator cuffs respond by switching the gene expression of type 1 collagen to type 3 collagen, and MMP has been shown to be involved in such regenerative processes.9,10)
MMP requires zinc as a cofactor for its enzymatic activity. MMP is known to be involved in both normal and pathophysi-ological processes, such as degeneration or regeneration, involv-ing proteolysis and peptide formation inside the tissue and in the extracellular matrix space. For example, MMP-2 is a key factor required for the efficient breaks down collagen. Imbalance of collagen reconstruction is attributed to changes in MMP and TIMP levels. A decrease in MMP-3 and stromelysin-1, increase and/or decrease in MMP-2 (gelatinase A), and changes in mRNA levels of MMP-1, -9 and -13 TIMP 2−4 was seen in some stud-ies. A study using rabbit showed that MMP-2 and TIMP-1 are expressed in both damaged and regenerated tissue, thereby highlighting their possible role in recovery of a damaged supra-spinatous. Similarly, in a different study, changes in mRNA con-centration of MMP-13 also indicated the possible role of these
Fig. 2. An inverse correlation between MMP-2 (A) and TIMP-2 (B) in torn rotator cuffs. MMP: matrix metalloproteinase, TIMP: tissue inhibitor of metallopro-teinase.
Fig. 3. Expression of MMP-9 and TIMP-1 demonstrates a less remarkable pattern compared to MMP-2. MMP: matrix metalloproteinase, TIMP: tissue inhibitor of metalloproteinase, M: marker.
Table 2. Correlation between mRNA Levels and Clinical Variables
Variable Correlation coefficient*
Age 0.513
Duration of symptoms -0.613
Tear size 0.454
Range of motion (forward flexion) 0.009
*By Spearman’s correlation.

Changes in MMP and TIMP in Rotator Cuff TearsOh-Soo Kwon, et al.
www.cisejournal.org 67
enzymes in the recovery process.10-12)
Select studies have shown that in degeneration or in tendon lesions, the mRNA expression level of MMP is inversely corre-lated to that of TIMP. However, Choi et al.13) reported that MMP-2 expression is not only seen in tendons of surgically excised tissue but also in regenerated tissue. Other studies,14,15) have also shown increased expression of MMP-2 and MMP-9 in synovium tissue. Such studies have assessed mRNA expression, but did not analyze a possible relationship between mRNA levels and clini-cal variables, as in our study. Lakemeier et al.11) found that whilst the position and size of the rotator cuff tear influences that biol-ogy of MMPs, the concentration of MMP-1 and MMP-9 at the articular surface of a partial tear is significantly greater than at the surface of the synovium. Prospective studies that similarly assess changes in the clinical variables that are correlated with changes in the biomarkers of rotator cuff tears. Factors that inhibit MMP have been assessed previously, but results had shown that drug or mechanical induction of changes in MMP was found to cause a varied influence on recovery.
Limitations to this studies came from only obtaining a small sample volume, not being able to obtain healthy tissue for ethi-cal reasons, thus any correlations we could make could not be compared in the context of an undamaged tissue.
Conclusion
Therefore, our results show that despite a constant expression of MMP-2 and TIMP-1 in damaged tissue, their expression is un-related to any clinical variable we tested. Our findings show that the mRNA levels of MMP-2 and TIMP-1 may be influenced by age and defect size. Thus, prospective studies into how changes in mRNA levels of MMP-2 and TIMP-1 may contribute to the pathophysiology of rotator cuff tears should be addressed, if any.
References
1. Murrell GA, Walton JR. Diagnosis of rotator cuff tears. Lancet. 2001;357(9258):769-70.
2. Cofield RH, Parvizi J, Hoffmeyer PJ, Lanzer WL, Ilstrup DM, Rowland CM. Surgical repair of chronic rotator cuff tears. A prospective long-term study. J Bone Joint Surg Am. 2001;83-A(1):71-7.
3. Hattrup SJ. Rotator cuff repair: relevance of patient age. J Shoulder Elbow Surg. 1995;4(2):95-100.
4. Jensen KL, Williams GR Jr, Russell IJ, Rockwood CA Jr. Rotator
cuff tear arthropathy. J Bone Joint Surg Am. 1999;81(9):1312-24.
5. Tetlow LC, Adlam DJ, Woolley DE. Matrix metalloproteinase and proinflammatory cytokine production by chondrocytes of human osteoarthritic cartilage: associations with degenerative changes. Arthritis Rheum. 2001;44(3):585-94.
6. Yoshihara Y, Nakamura H, Obata K, et al. Matrix metallopro-teinases and tissue inhibitors of metalloproteinases in synovial fluids from patients with rheumatoid arthritis or osteoarthritis. Ann Rheum Dis. 2000;59(6):455-61.
7. Dalton S, Cawston TE, Riley GP, Bayley IJ, Hazleman BL. Hu-man shoulder tendon biopsy samples in organ culture produce procollagenase and tissue inhibitor of metalloproteinases. Ann Rheum Dis. 1995;54(7):571-7.
8. Bedi A, Kovacevic D, Hettrich C, et al. The effect of matrix me-talloproteinase inhibition on tendon-to-bone healing in a rota-tor cuff repair model. J Shoulder Elbow Surg. 2010;19(3):384-91.
9. Lo IK, Marchuk LL, Hollinshead R, Hart DA, Frank CB. Matrix metalloproteinase and tissue inhibitor of matrix metallopro-teinase mRNA levels are specifically altered in torn rotator cuff tendons. Am J Sports Med. 2004;32(5):1223-9.
10. Riley GP, Curry V, DeGroot J, et al. Matrix metalloproteinase activities and their relationship with collagen remodelling in tendon pathology. Matrix Biol. 2002;21(2):185-95.
11. Lakemeier S, Braun J, Efe T, et al. Expression of matrix metallo-proteinases 1, 3, and 9 in differing extents of tendon retraction in the torn rotator cuff. Knee Surg Sports Traumatol Arthrosc. 2011;19(10):1760-5.
12. Thornton GM, Shao X, Chung M, et al. Changes in mechanical loading lead to tendonspecific alterations in MMP and TIMP expression: influence of stress deprivation and intermittent cy-clic hydrostatic compression on rat supraspinatus and Achilles tendons. Br J Sports Med. 2010;44(10):698-703.
13. Choi HR, Kondo S, Hirose K, Ishiguro N, Hasegawa Y, Iwata H. Expression and enzymatic activity of MMP-2 during heal-ing process of the acute supraspinatus tendon tear in rabbits. J Orthop Res. 2002;20(5):927-33.
14. Ritty TM, Herzog J. Tendon cells produce gelatinases in response to type I collagen attachment. J Orthop Res. 2003;21(3):442-50.
15. Castagna A, Cesari E, Gigante A, Conti M, Garofalo R. Metal-loproteases and their inhibitors are altered in both torn and in-tact rotator cuff tendons. Musculoskelet Surg. 2013;97 Suppl 1:39-47.

Reverse Total Shoulder Arthroplasty: Early Outcome and Complication Report
Yong-Bok Park, Sung-Weon Jung1, Ho-Young Ryu, Jin-Ho Hong, Sang-Hoon Chae, Kyoung-Bin Min2, Jae-Chul Yoo
Department of Orthopaedic Surgery, Samsung Medical Center, Seoul, 1Department of Orthopaedic Surgery, Samsung Changwon Hospital, Changwon, 2Sports Medicine Center, Samsung Medical Center, Seoul, Sungkyunkwan University School of Medicine, Korea
Background: Recently, reverse total shoulder arthroplasty (RTSA) has been accepted as a main treatment option in irreparable massive rotator cuff tear with cuff arthropathy. The purpose of this study was to evaluate the early complication incidence and the preliminary clinical results of RTSAs performed in single institute.Methods: Fifty-seven RTSAs (56 patients) were performed between April 2011 and March 2013. The indications for RTSA were cuff tear arthropathy and irreparable massive rotator cuff tear with or without pseudoparalysis. Exclusion criteria were revision, preoperative infec-tions and fractures. At final follow-up, 45 shoulders were enrolled. Mean follow-up duration was 12.5 months (range, 6−27 months). The mean age at the time of surgery was 73.6 years (range, 58−87 years). All the patients were functionally accessed via Constant score, American Shoulder and Elbow Surgeons (ASES) score, pain and functional visual analogue scale (VAS) scores and active range of motion. Complications were documented as major and minor. Major complications include fractures, infections, dislocations, nerve palsies, asep-tic loosening of humeral or glenoid components, or glenoid screw problems. Minor complications include radiographic scapular notch-ing, hematomas, heterotopic ossification, algodystrophy, intraoperative dislocations, intraoperative cement extravasation, or radiographic lucent lines of the glenoid.Results: The mean Constant score increased from 31.4 to 53.8 (p < 0.001). The pain and functional VAS scores improved (5.2 to 2.7, p < 0.001, 4.0 to 6.7, p < 0.001) and active forward flexion improved from 96.9° to 125.6° (p = 0.011). One or more complications oc-curred in 16 (35.6%) of 45 shoulders, with one failure (2.2%) resulting in the removal of implants by late infection. The single most com-mon complication was scapular notching (9 [20%]). There were 4 (8.9%) axillary nerve palsies postoperatively (n=3: transient n. palsy, n=1: Symptom existed at 11 months postoperatively but improving).Conclusions: In a sort term follow-up, RTSA provided substantial gain in overall function. Most common early complications were scap-ular notching and postoperative neuropathy. Although overall early complication rate was as high as reported by several authors, most of the complications can be observable without compromise to patients’ clinical outcome. Long term follow-up is required to clarify the clinical result and overall complication rate.(Clin Shoulder Elb 2014;17(2):68-76)
Key Words: Shoulder; Arthroplasty; Reverse; Early outcome; Complication
Introduction
Reverse total shoulder arthroplasty (RTSA) has been devel-oped to salvage the glenohumeral articulation damaged by infection, arthritis, or trauma.1,2) Unfortunately, its initial design resulted in high complication and failure.3,4) Now with marked
changes in its design because of Grammont contribution in the late 1980’s, the clinical outcome of RTSA has improved.5,6) Reverse design moved the center of rotation (COR) distally and medially in comparison to the native glenohumeral articulation.7) The change in glenohumeral COR improves deltoid function and decreases glenoid implant-bone interface stresses and loos-
CiSEClinics in Shoulder and Elbow
Copyright © 2014 Korean Shoulder and Elbow Society. All Rights Reserved.This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
pISSN 1226-9344eISSN 2288-8721
ORIGINAL ARTICLE
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014http://dx.doi.org/10.5397/cise.2014.17.2.68
Received March 31, 2014. Revised May 26, 2014. Accepted June 3, 2014.
Correspondence to: Jae-Chul YooDepartment of Orthopaedic Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul 135-710, KoreaTel: +82-2-3410-3501, Fax: +82-2-3410-0061, E-mail: [email protected], [email protected]
Financial support: None. Conflict of interests: None.

Reverse Total Shoulder ArthroplastyYong-Bok Park, et al.
www.cisejournal.org 69
ening. Moreover, it significantly improves the function of patients with painful pseudoparalysis secondary to a massive irreparable rotator cuff tear.2,5) Furthermore, because of recent advances in implant technology and surgical techniques, marked improve-ment in clinical scores, subjective patient satisfaction, complica-tions, and failure rates has been achieved.1)
However, even with recent advancement, studies report wide variable clinical outcomes and complication rates reached to 75%.8,9) Moreover, it is still considered as having much more complication rate than conventional total shoulder arthro-plasty.3,4) Furthermore, their clinical outcomes seem to have much more variance because of many factors such as expanded indications (cuff arthropathy, fracture or infection sequelae, and massive tear),5,6) quality of remaining external rotators, bone quality, and so forth. Therefore, our early clinical results and complication rate with modern RTSAs were questionable.
The purpose of the study was to evaluate the early com-plication based preliminary clinical result of RTSAs performed by single surgeon in single institute. Our hypotheses were; (1) observed complication of RTSA would be similar to published rates, and (2) although the complication rate is high, most would be treated successfully without much compromise to the clinical outcome.
Methods
Patients SelectionThis preliminary report is a retrospective review of 57s’ con-
secutive RTSAs performed between April 2011 and March 2013 by one surgeon at a single institution. The indications were cuff arthropathy and massive irreparable rotator cuff tear with or without pseudoparalysis. We considered irreparable rotator cuff tear as chronic rotator cuff tears, severe atrophy of supraspina-tus/infraspinatus muscle, with Goutallier grade four for supraspi-natus and 3/4 for infraspinatus.10) Prior conservative treatment failed for all the patients. The exclusion criteria were insufficient follow-up period (at least six months), revision surgery, preop-erative infection history, preoperative neurologic injury, and worker’s compensation cases. Of the 57 shoulders, 12 cases were excluded (two follow-up loss, four insufficient follow-up period, and one incomplete axillary nerve palsy preoperatively because of shoulder dislocation, four patients with pre-operative infection history, and one patient with traffic accident just after the surgery).
Forty-five shoulders were finally enrolled in this retrospective study, which was conducted after obtaining approval from the institutional review board at our institution (IRB no. 2014-01-108). The mean age at the time of surgery was 73.6 ± 6.1 years (range, 58−87 years). The dominant shoulder was involved in 30 patients (66.6%), and one patients had bilateral surgery. Ce-mented and cementless stems were inserted in 21 and 24 shoul-
ders, respectively. The mean follow-up duration was 12.5 ± 5.6 months (range, 6−27 months). According to Hamada-Walch classification, degrees of glenohumeral arthritis in our series were classified as stage 1−3 in 18 shoulders and stage 4−5 in 27 (Table 1).11,12)
Six patients had previous operations: Of these patients, 4 patients had rotator cuff repair because of rotator cuff tear. An-other one patient had rotator cuff repair only because of massive rotator cuff tear and concomitant Bankart lesion with instability. Moreover, the other one patient had arthroscopic Bankart repair because of recurrent dislocation with Bankart lesion. There were no patients who had more than two operations on same side of the surgery. Fourteen patients had previous intra-articular injec-tion more than once and 31 patients had no previous injection history before RTSA.
Clinical and Radiologic EvaluationA clinical and radiologic assessment consisting of a structured
interview, clinical examination, photographic documentation, and radiographic observation were performed preoperatively and postoperatively in each clinical visit. All the patients were functionally accessed via Constant score,13) American Shoulder and Elbow Surgeons (ASES) score,14) Korean Shoulder Scoring System,15) pain and functional visual analog scale (VAS) score, and active range of motion (including forward flexion, external
Table 1. Preoperative Demography
Variable Data
Age (yr) 73.6 ± 6.1 (58–87)
Gender (male:female) 9:36
Involved side (left:right) 14:31
Dominant arm 30 (66.6)
Stem (cemented:non-cement) 21:24
Mean follow-up duration (mo) 12.5 ± 5.6 (6–27)
Staging of massive rotator cuff tears*
Grade 1 2 (4.4)
Grade 2 11 (24.4)
Grade 3 5 (11.1)
Grade 4a 10 (22.2)
Grade 4b 7 (15.6)
Grade 5 10 (22.2)
Values are presented as mean ± standard deviation (range), number, or num-ber (%).*In accordance with Hamada-Walch classification.Grade 1: AHI ≥6 mm, Grade 2: AHI <6 mm, Grade 3: AHI <6 mm with ac-etabularization, Grade 4a: glenohumeral arthritis without acetabularization, Grade 4b: glenohumeral arthritis with acetabularization, Grade 5: collapse of humeral head, ‘‘cuff tear arthropathy”.AHI: acromiohumeral distance.

70 www.cisejournal.org
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014
rotation with the arm at the side, and internal rotation behind the back). Standardized anteroposterior, glenohumeral antero-posterior, axillary lateral, and scapular lateral and 30 degree cau-dal tilted view was obtained preoperatively and postoperatively.
Zumstein et al.8) classified an intraoperative or postoperative event under problem and complication which were likely to affect the patient’s final outcome or not. Problem is a type of complication, we classified problems and complications to mi-nor and major complications, respectively. Major complications include fractures, infections, dislocations, nerve palsies, aseptic loosening of humeral or glenoid components, modular stem or polyethylene disassociations, or glenoid screw problems. Minor complications include scapular notching, hematomas, hetero-topic ossifications, algodystrophy, phlebitis, intraoperative dislo-cations, cement extravasation, or radiographic lucent lines of the glenoid.
Surgical TechniqueAll procedure was performed by a single senior author (J.C.Y.).
Three types of Grammont-style RTSA prosthesis were used dur-ing this period (Aequalis Reverse system type II; Tonier, Mont-bonnot, France) (n = 23), Trabecular metal reverse shoulder system (Zimmer, Warsaw, IN, USA) (n = 7), Versa-dial system: standard adaptor (Biomet, Warsaw, IN, USA) (n = 15). If the bone stock of glenoid was not favorable for fixation due to os-teoporosis or deformation of glenoid, we chose Versa-dial sys-tem which has central screw for glenoid plate fixation. And the others were used randomly according to surgeon’s preference. All the patients were operated on the beach-chair position. The
10−15 cm sized deltopectoral approach was used. The superior portion of the pectoralis major tendon and the coraco-acromial ligament was incised for better exposure. The subscapularis tendon was detached from the subscapularis footprint with tag-ging sutures. Humeral head cutting was performed with 0−20° retroversion according to patient’s natural retroversion and de-pending on the implant system. After the head cutting, the gle-noid baseplate fixation was followed according to the company instrumentation manual. Glenoid base plate was placed slightly inferior to glenoid center with 10° inferior tilting in all the cases. The size of the base plate was determined with available glenoid bone stock and surgeon’s preference, usually the smallest diam-eter baseplate. In all the cases, 36 mm sized glenosphere was used. Using Kirschner wire, 4−5 holes were made on anterior proximal humeral cortex for fixation of subscapularis tendon. Then, the humeral component was placed. After the insertion of trial implant, appropriate tension was determined for the case when the joint was not easily dislocated subjectively. The sub-scapularis tendon was repaired via transosseous sutures in most of the cases. Incised superior portion of pectoralis major muscle was repaired. A soft tissue biceps tenodesis was also performed when in the presence of the tendon. All incisions were closed over one or two suction drain.
Postoperative RehabilitationPostoperatively, the shoulder was immobilized with 30o ab-
duction brace for four weeks. During this period, the sling was kept for all times except for hygiene and changing clothes. Pas-sive range of motion was initiated after removal of hemovac at
Table 2. Any Details of Complications and Treatment according to Complications
Complication No. Detail and Treatment
Major complication
Postoperative neuropathy 4 n=3: transient, fully recovered within 6 months; n=1: symptom existed at 11 months’ postoperatively, follow-up is ongoing.
Infection 1 Late infection at 20 months postoperatively: Implant removal and PROSTALAC insertion was performed.
Minor complication
Periprosthetic fracture 1 Slip down, type B (The Wright and Cofield classification, Copyright Mayo Foundation)
Acromial fracture 1 Spontaneous fracture: Open reduction and internal fixation using Plate and Screw performed
Scapular notching 9 n=8 : grade 1, n=1 : grade 2
Radiolucent line on glenoid 2
Heterotopic ossification 2
Instability-related symptom 1 Discomfort with “weird sound” during range of motion. There was no pain, apprehension and sign of subluxation.
Limited range of motion
Ext. rotation difficulty 6 n=4: external rotation difficulties only; n=3: internal rotation difficulties only; n=2: external and internal difficulties
Int. rotation difficulty 5
PROSTALAC: prosthesis with antibiotic-loaded acrylic cement.

Reverse Total Shoulder ArthroplastyYong-Bok Park, et al.
www.cisejournal.org 71
postoperative 2 or 3 days. Active forward elevation was not per-mitted to protect the subscapularis repair if they had one. After four weeks, the sling was removed and tolerable active assisted passive range of motion was allowed for 4−6 weeks, and fol-lowed by active strengthening exercises.
Statistical AnalysisComparisons of preoperative and postoperative clinical scores
were performed using the paired t-tests or Wilcoxon signed rank test. Subgroup analysis between group A (patients with compli-cations) and group B (patients without complications) were con-ducted with the Mann-Whitney U-test. All statistical analysis was performed using the IBM SPSS Statistics 20.0 software (IBM-SPSS, Armonk, NY, USA). The significance level of p-value was set at 0.05.
Results
ComplicationOne or more complications occured for 16 out of the 45
RTSAs (35.6%) and are listed in Table 2. Minor and major com-plications occurred in 13 (28.9%) and seven (15.6%) patients, respectively, and four patients had major and minor complica-tions simultaneously.
Scapular notching was single most common complication and was graded by the Nerot-Sirveaux grading system.16) Nine (20%) scapular notching were observed with eight of grade 1, and one of grade 2. However, no further complication including implant loosening was found (Fig. 1).
There were four nerve palsies existed postoperatively, and three out of which had transient axillary nerve palsies and fully recovered in sensation and function within six months. One patient still had nerve symptoms (deltoid wasting, and discom-fort at forward elevation); however, he showed improvement at postoperative 11 months (forward flexion: 150°, abduction 130°, ASES score: 75, Constant score: 71, pain VAS: 0) (Fig. 2). No glenoid and humeral component loosening occurred; however, radiographic lucent lines of the glenoid can be seen in two cases (Fig. 3). One periprosthetic humeral fracture occurred after slip down from the front door at postoperative one month, and was treated with open reduction and internal fixation with a long locking plate (Fig. 4). One acromial fracture was devel-oped spontaneously at postoperative six months (Fig. 5), and considered to be a fatigue fracture. Surgery was not performed, because the fracture site was peripheral and most part of the deltoid insertion was preserved. At 15 months’ follow-up on this patient, active forward elevation was 130°, abduction was 80° and pain VAS score was five. Late infection was occurred in one
Fig. 1. Grade II scapular notching was noted at postoperative 15 months (white arrow).
Fig. 2. The patient with axillary nerve neuropathy. Deltoid muscle wasting in involved side was noted at postoperative 11 months.
Fig. 3. Radiolucent line near glenoid component was noted at postoperative 18 months (white arrow).

72 www.cisejournal.org
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014
Fig. 4. (A) Periprosthetic fracture was oc-curred in one patient due to slip down at 1 month postoperatively. (B) The patient had open reduction and internal fixation using plate and screws.
Fig. 5. Spontaneous acromial fracture was occurred in one shoulder after surgery. (A) Preoperative X-ray: Superiorly migrated humerus. (B) At 3 months post-operatively: Humerus was moved inferiorly. (C) At 6 months postoperatively: Acromial fracture was noted. (D) At 9 months postoperatively: Callus was formed around acromion. (E) At 15 months postoperatively.

Reverse Total Shoulder ArthroplastyYong-Bok Park, et al.
www.cisejournal.org 73
case. Glenoid loosening was observed on six months’ follow-up X-ray. Moreover, functional score and range of motion (ROM) were suddenly declined during five months from postoperative six to 11 months. Pain, mild redness, heatness, high erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) were observed at 20 months’ follow-up (Fig. 6). This patient recently received the prosthesis removal with antibiotics-mixed cement spacer insertion. Two cases of heterotopic ossification occurred on infra-glenoid neck area (Fig. 7). One patient complained discomfort with click and metallic sound during range of mo-tion, which the patient claims as “weird sound in the case of the prosthesis moving”. There was no pain, apprehension and sign of subluxation.
Hematomas, phlebitis, intraoperative cement extravasation problem, dislocation, modular stem or polyethylene disassocia-
tions, and glenoid screw dislocation problems were not ob-served.
Early Clinical OutcomesAfter excluding two patients (the patient who underwent re-
moval of the prosthesis because of late infection, and the patient with periprosthetic fracture), overall functional scores were im-proved. However, the range of improvement in SST, pain VAS, and functional VAS scores were not marked. In terms of ROM, forward elevation was substantially increased (96.9° to 125.6°, p = 0.011); however, abduction, external rotation and internal ro-tation were not significantly different. Nine patients complained
Table 3. Preoperative and Postoperative Clinical Scores
Parameter Preoperative scores Postoperative scores p-value
Constant score 31.4 ± 15.9 53.8 ± 11.3 <0.001
ASES 33.3 ± 16.0 60.6 ± 14.0 <0.001
SST 3.0 ± 1.9 5.3 ± 1.9 <0.001
KSS 39.6 ± 19.7 60.3 ± 13.1 <0.001
pVAS 5.2 ± 2.8 2.7 ± 1.6 <0.001
fVAS 4.0 ± 2.6 6.7 ± 1.6 <0.001
Range of motion (°)
Forward elevation 96.9 ± 39.4 125.6 ± 16.5 0.011
Abduction 77.0 ± 54.2 73.3 ± 26.0 0.709
External rotation 26.7 ± 18.6 27.6 ± 12.25 0.737
Internal rotation T11 T12–L1 0.067
Values are presented as mean ± standard deviation. ASES: American Shoulder and Elbow Surgeons score, SST: simple shoulder test, KSS: Korean Shoulder Scoring System, pVAS: pain visual analog scale score, fVAS: functional visual analog scale score.
Table 4. Clinical Score Comparison of Patients with or without Complica-tions
Parameter Group A Group B p-value
Constant Preoperative 27.6 ± 14.3 28.9 ± 17.0 0.751
Postoperative 53.0 ± 10.5 53.6 ± 11.2 0.678
ASES Preoperative 32.5 ± 17.8 28.4 ± 14.7 0.555
Postoperative 62.6 ± 13.4 61.6 ± 12.9 0.957
SST Preoperative 4.1 ± 2.9 3.3 ± 2.3 0.530
Postoperative 5.0 ± 1.8 5.5 ± 2.4 0.512
KSS Preoperative 39.3 ± 19.6 39.1 ± 19.9 0.895
Postoperative 63.4 ± 13.4 63.6 ± 12.3 0.986
pVAS Preoperative 4.7 ± 2.6 5.2 ± 3.0 0.598
Postoperative 3.2 ± 1.4 3.1 ± 1.7 0.986
fVAS Preoperative 4.2 ± 3.0 3.7 ± 2.1 0.831
Postoperative 6.5 ± 1.6 6.9 ± 1.7 0.503
Values are presented as mean ± standard deviation. Group A: the patients who had one or more complications, Group B: the pa-tients who had not any complications, ASES: American Shoulder and Elbow Surgeons score, SST: simple shoulder test, KSS: Korean Shoulder Scoring Sys-tem, pVAS: pain visual analog scale score, fVAS: functional visual analog scale score.
Fig. 6. The late infection was occurred in one patient. (A) Glenoid loosening was observed on 6 months’ follow up x-ray. And functional score and range of motion were suddenly de-clined during 5 months from postoperative 6 month to 11 months. (B) Glenoid loosening was progressed. Pain, mild redness, heatness, high erythrocyte sedimentation rate and C-reactive protein were observed at 20 months’ follow-up.

74 www.cisejournal.org
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014
internal or external rotation difficulties (three with internal rota-tion difficulties only, four with external rotation difficulties only, and two with internal and external difficulties). Of total six pa-tients who had external rotation difficulties, three patients could not at all rotate the arm externally (three with external rotation 0°, three with external rotation 0−20°). The preoperative and post-operative results are listed in Table 3. Table 4 lists sub-analysis of the patient with one or more complications (group A) and those with no complications (group B). No statistical differences in functional scores between groups A and B was observed.
Discussion
One or more complications occurred in 16 patients out of the 45 RTSAs (35.6%). Our complication rate is lower than pre-vious series, with rates reported as high as 68%.9) Minor and ma-jor complications were 13(28.9 %) and 7(15.6%), respectively. Out of seven patients with major complication, two patients un-derwent surgical treatment similar to other studies where minor complications occurred more frequently and most of the major complication were treated conservatively.8,16,17) Dislocation after RTSA was not as common as previously reported.
In our study, the incidence and severity of scapular notch-ing (9 [20%]) was lower than previously reported (range, 44−96%).6,18,19) However, the incidence and severity could be increased with time, the longer follow up is required to clarify the definite result. The clinical significance of scapular notching is still a matter of debate. Some studies declared that scapular notching is associated with glenoid component loosening16,20) and has negative effect on clinical outcomes.16,21) The largest and most comprehensive study on the subject reported no clini-cal effect and only one case of progressive notching leading to
glenoid component loosening at 114 months postoperatively.22) Factors associated with the development of scapular notch-ing include prosthetic design, surgical approach, positioning of the glenosphere and body mass index (BMI).21,23) Among these parameters, lateralization of COR and inferior placement of glenosphere are associated with low rates of inferior scapular notching, improved shoulder rotation, no prosthetic instability and improved shoulder contour.24)
Internal and external rotation difficulties are other problems of Grammont-type RTSAs. In our study, the mean external and internal rotations were 27.6 ± 12.2° and ~T12–L1, respectively. Nine patients complained for internal or external rotation diffi-culties after the operation (three with internal rotation difficulties only, four with external rotation difficulties only, and two with both difficulties). Grammont-type RTSA system (lowering the hu-merus and medialization of the COR at the glenoid component) has the dual advantage of tensioning the deltoid muscle to in-crease its functional strength, and decreasing mechanical torque at the glenoid component, thus avoiding glenoid loosening.2,19) However, because of the medialization of COR, posterior del-toid component for external rotation and anterior component for internal rotation were decreased. Therefore, internal and external rotation difficulties occurred frequently.2) Moreover, reduced rotational moment arms in the conjunction with the decrease in origin-to-insertion distance can cause impaired ex-ternal and internal rotation.25) Postoperative external rotation dif-ficulty is a cause of patient’s dissatisfaction. Therefore, if patient has severe external rotation lagging and insufficient teres minor muscle, surgeon should anticipate patient’s dissatisfaction and explain it to the patient before surgery. If operated arm is domi-nant side, at least T10−L1 of internal rotation is essential for hygiene. For this reason, less degree of retroversion is favorable. Lateralization of COR improve tension of the remaining rotator cuff muscles.8) And increased anterior and posterior recruitment can restore active internal and external rotation.17) However, the lateralization of COR can increase shear force on glenoid component, resulting in acceleration of glenoid loosening is of theoretical concern. Some controversies exist on this issue. Vi-rani et al.26) declared no difference in glenoid loosening between standard RTSA and RTSA of 10 mm lateralized COR. However, Boileau et al.24) declared that bony lateralization has mechani-cal advantage compared to metallic lateralization,6,25) improving shoulder rotation, and no prosthetic instability. More studies are necessary to confirm this issue.
There was wide variation in the rates of postoperative hema-toma between studies (1−21%).20,27) Probably because some authors only included hematomas as a complication if there was a need for a reoperation,5) whereas others included all hemato-mas, even if no re-intervention was needed.28) Our study did not have any known hematoma problems.
Neurologic complications occurred in four cases (8.9%). All
Fig. 7. Heterotopic ossification was noted at 11 months follow-up postopera-tively (white arrow).

Reverse Total Shoulder ArthroplastyYong-Bok Park, et al.
www.cisejournal.org 75
the cases were related to axillary nerve. Three of these were transient and one has neurologic symptom such as (Deltoid muscle wasting and difficulty in forward elevation at postopera-tive 11 months’ follow-up). However, the symptoms were im-proving and more follow-up is needed. This patient’s Hamada-Walch stage was 4a. After superiorly migrated humerus reduced, traction injury might have occurred in this patients resulting in higher than previously reported (0−12.2%).8,29) Neurologic com-plications may be attributed to intraoperative traction, manipu-lation of the arm, retractor placement, or relative lengthening of arm. In a systemic review of 782 cases reported by Zumstein et al.8), nine neurologic complications were reported including axillary (two cases), radial (six cases) and musculocutaneous (one case) nerve palsies.
One (2.2%) acromial fracture occurred spontaneously and was treated with conservative management. It was considered to be a fatigue fracture because of deltoid over-tension after the reduction of superior migrated humerus preoperatively (Fig. 5). This result is similar to the previously reported one (0−6.9%).5,8,16)
Postoperative instablility, a major complication, can result in poor functional outcome and pain. Postoperative instability has been reported in a range 2.4% to 31%.3) In our study, one patient complained of instability-related symptom. This patient complains weird sound and uncomfortable feeling without pain while elevating arm forward at near 90° and rotating arm inter-nally. There was no objective sign of impingement, subluxation and dislocation. We are not sure why we didn’t have any dis-tinctive dislocations. Maybe we are putting our implant too tight instead of too loose. However, we feel that it is more worrisome putting the prosthesis too tight than loose making the shoulder joint to be in the risk of acromion fracture or transient nerve pal-sies.
This study has several limitations. First, our follow-up is too short to make definitive estimation of the clinical outcome. Pre-vious studies with long term follow up have shown increased complication rates with time.8,18) Second, our small series pre-clude statistical analysis according to implant systems. A larger sample size will clarify the clinical result and provide greater precision for complication rate. Third, surgeon’s factor is always there; therefore, our complication rate will decrease and clini-cal outcome will improve with accumulation. Several studies reported the learning curve for the RTSA and the complication rate tends to decrease after some numbers of operations.9,18) Therefore, our result may show the clinical outcome and com-plication incidence in early phase of the first 50 surgeries of single surgeon.
Conclusion
In short term follow-up, RTSA provided substantial gain in overall function. Most common early complications were
scapular notching and postoperative neuropathy. Although over-all early complication rate was as high as reported by several authors, most of the complications can be observable without compromise to patients’ clinical outcome. Long term follow-up is required to clarify the clinical result and overall complication rate.
References
1. Wall B, Nové-Josserand L, O’Connor DP, Edwards TB, Walch G. Reverse total shoulder arthroplasty: a review of results accord-ing to etiology. J Bone Joint Surg Am. 2007;89(7):1476-85S.
2. Boileau P, Watkinson DJ, Hatzidakis AM, Balg F. Grammont re-verse prosthesis: design, rationale, and biomechanics. J Shoul-der Elbow Surg. 2005;14(1 Suppl S):147S-61.
3. Cheung E, Willis M, Walker M, Clark R, Frankle MA. Compli-cations in reverse total shoulder arthroplasty. J Am Acad Or-thop Surg. 2011;19(7):439-49.
4. De Wilde LF, Audenaert EA, Berghs BM. Shoulder prostheses treating cuff tear arthropathy: a comparative biomechanical study. J Orthop Res. 2004;22(6):1222-30.
5. Boileau P, Watkinson D, Hatzidakis AM, Hovorka I. Neer Award 2005: The Grammont reverse shoulder prosthesis: results in cuff tear arthritis, fracture sequelae, and revision ar-throplasty. J Shoulder Elbow Surg. 2006;15(5):527-40.
6. Gerber C, Pennington SD, Nyffeler RW. Reverse total shoulder arthroplasty. J Am Acad Orthop Surg. 2009;17(5):284-95.
7. Grammont P, Trouilloud P, Laffay J, Deries X. Concept study and realization of a new total shoulder prosthesis. Rhumatolo-gie. 1987;39:407-18.
8. Zumstein MA, Pinedo M, Old J, Boileau P. Problems, compli-cations, reoperations, and revisions in reverse total shoulder arthroplasty: a systematic review. J Shoulder Elbow Surg. 2011;20(1):146-57.
9. Wierks C, Skolasky RL, Ji JH, McFarland EG. Reverse total shoulder replacement: intraoperative and early postoperative complications. Clin Orthop Relat Res. 2009;467(1):225-34.
10. Goutallier D, Postel JM, Bernageau J, Lavau L, Voisin MC. Fatty muscle degeneration in cuff ruptures. Pre- and postoperative evaluation by CT scan. Clin Orthop Relat Res. 1994;(304):78-83.
11. Hamada K, Fukuda H, Mikasa M, Kobayashi Y. Roentgeno-graphic findings in massive rotator cuff tears. A long-term ob-servation. Clin Orthop Relat Res. 1990;(254):92-6.
12. Walch G, Edwards TB, Boulahia A, Nové-Josserand L, Ney-ton L, Szabo I. Arthroscopic tenotomy of the long head of the biceps in the treatment of rotator cuff tears: clinical and radiographic results of 307 cases. J Shoulder Elbow Surg. 2005;14(3):238-46.
13. Constant CR, Murley AH. A clinical method of func-tional assessment of the shoulder. Clin Orthop Relat Res.

76 www.cisejournal.org
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014
1987;(214):160-4.14. Richards RR, An KN, Bigliani LU, et al. A standardized method
for the assessment of shoulder function. J Shoulder Elbow Surg. 1994;3(6):347-52.
15. Tae SK, Rhee YG, Park TS, et al. The development and vali-dation of an appraisal method for rotator cuff disorders: the Korean Shoulder Scoring System. J Shoulder Elbow Surg. 2009;18(5):689-96.
16. Sirveaux F, Favard L, Oudet D, Huquet D, Walch G, Molé D. Grammont inverted total shoulder arthroplasty in the treat-ment of glenohumeral osteoarthritis with massive rupture of the cuff. Results of a multicentre study of 80 shoulders. J Bone Joint Surg Br. 2004;86(3):388-95.
17. Frankle M, Siegal S, Pupello D, Saleem A, Mighell M, Vasey M. The Reverse Shoulder Prosthesis for glenohumeral arthritis as-sociated with severe rotator cuff deficiency. A minimum two-year follow-up study of sixty patients. J Bone Joint Surg Am. 2005;87(8):1697-705.
18. Groh GI, Groh GM. Complications rates, reoperation rates, and the learning curve in reverse shoulder arthroplasty. J Shoulder Elbow Surg. 2014;23(3):388-94.
19. Nyffeler RW, Werner CM, Simmen BR, Gerber C. Analysis of a retrieved delta III total shoulder prosthesis. J Bone Joint Surg Br. 2004;86(8):1187-91.
20. Boulahia A, Edwards TB, Walch G, Baratta RV. Early results of a reverse design prosthesis in the treatment of arthritis of the shoulder in elderly patients with a large rotator cuff tear. Or-thopedics. 2002;25(2):129-33.
21. Simovitch RW, Zumstein MA, Lohri E, Helmy N, Gerber C. Predictors of scapular notching in patients managed with the Delta III reverse total shoulder replacement. J Bone Joint Surg Am. 2007;89(3):588-600.
22. Lévigne C, Boileau P, Favard L, et al. Scapular notching in reverse shoulder arthroplasty. J Shoulder Elbow Surg. 2008;17(6):925-35.
23. Falaise V, Levigne C, Favard L; SOFEC. Scapular notching in reverse shoulder arthroplasties: the influence of gleno-metaphyseal angle. Orthop Traumatol Surg Res. 2011;97(6 Suppl):S131-7.
24. Boileau P, Moineau G, Roussanne Y, O’Shea K. Bony in-creased-offset reversed shoulder arthroplasty: minimizing scapular impingement while maximizing glenoid fixation. Clin Orthop Relat Res. 2011;469(9):2558-67.
25. Herrmann S, König C, Heller M, Perka C, Greiner S. Reverse shoulder arthroplasty leads to significant biomechanical chang-es in the remaining rotator cuff. J Orthop Surg Res. 2011;6:42.
26. Virani NA, Harman M, Li K, Levy J, Pupello DR, Frankle MA. In vitro and finite element analysis of glenoid bone/baseplate interaction in the reverse shoulder design. J Shoulder Elbow Surg. 2008;17(3):509-21.
27. Levy JC, Virani N, Pupello D, Frankle M. Use of the reverse shoulder prosthesis for the treatment of failed hemiarthroplasty in patients with glenohumeral arthritis and rotator cuff defi-ciency. J Bone Joint Surg Br. 2007;89(2):189-95.
28. Werner CM, Steinmann PA, Gilbart M, Gerber C. Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunc-tion with the Delta III reverse-ball-and-socket total shoulder prosthesis. J Bone Joint Surg Am. 2005;87(7):1476-86.
29. Bufquin T, Hersan A, Hubert L, Massin P. Reverse shoulder arthroplasty for the treatment of three- and four-part fractures of the proximal humerus in the elderly: a prospective review of 43 cases with a short-term follow-up. J Bone Joint Surg Br. 2007;89(4):516-20.

Unusual Migration of Kirschner’s Wire into Intervertebral Foramen after Lateral Clavicle Fracture Fixation - A Case Report
Jin-Ho Lee, Jae-Yoon Chung, Myung-Sun Kim
Department of Orthopaedic Surgery, Chonnam National University College of Medicine, Gwangju, Korea
The migration of metallic devices such as Kirschner’s wire (K-wire) from the shoulder is a well-recognized and significant complication of operation, the wire ending up in the lungs, the heart, the esophagus, the aorta or the subclavian artery. However, spinal migration is very rare. We report the case of a 72-year-old female patient with K-wire migration into the C7-T1 intervertebral foramen, 2 months after sur-gery for a lateral end fracture of left clavicle.(Clin Shoulder Elb 2014;17(2):77-79)
Key Words: Clavicle; Lateral end fracture; Kirschner’s wire; Spinal migration
Kirschner’s wires (K-wires) are used commonly in various or-thopaedic surgical fixations. Especially, that is often used around the shoulder girdle for fixation of displaced fractures and dislo-cated joints to ensure adequate stabilization. The use of K-wire fixation is often complicated by component migration, especially when employed about the shoulder girdle. There are many re-ports of migrations of the chest, vessels and muscles by K-wires in the literature, but cases of interspinal migration are extremely rare. We report the case of a woman who was interspinal migra-tion of K-wire after fixation for the lateral clavicle end fracture.
Case Report
A 72-year-old wound was fall down in April 2008, and sus-tained a fracture of the left clavicle end (Neer type II). For which she underwent stabilization of the fracture by two K-wires and tension band wiring at other hospital (Fig. 1). The regular follow-up was done every 2 week. About 7 weeks post-operatively, the patient was developed a radiating pain on left arm while walking or shoulder motion. At routine follow-up 8 weeks post-operatively, radiologic examination revealed that the wire migra-
CiSEClinics in Shoulder and Elbow
Copyright © 2014 Korean Shoulder and Elbow Society. All Rights Reserved.This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
pISSN 1226-9344eISSN 2288-8721
CASE REPORT
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014http://dx.doi.org/10.5397/cise.2014.17.2.77
Received February 21, 2014. Revised March 27, 2014. Accepted April 7, 2014.
Correspondence to: Myung-Sun KimDepartment of Orthopedic Surgery, Chonnam National University College of Medicine, 42 Jebong-ro, Dong-gu, Gwangju 501-757, KoreaTel: +82-62-227-1640, Fax: +82-62-225-7794, E-mail: [email protected]
Financial support: None. Conflict of interests: None.
Fig. 1. Anteroposterior radiograph of left shoulder. Preoperative (A) and postoperative (B) radiograph shows left distal clavicle frac-ture and internal fixation state with K-wire.

78 www.cisejournal.org
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014
tion. Roentgenogram of the cervical spine showed a movement of one of the two pins, which one wire migrated into C7-T1 intervertebral foramen (Fig. 2). A computed tomography scan of the cervical spine revealed that the dislocated K-wire had pen-etrated through the left intervertebral foramen of C7-T1 (Fig. 3). At that time we done emergency operation. The transverse inci-sion over the left clavicle and through the sternocleidomastoid muscle was opened. The K-wire was pulled out successfully un-der image intensifier (Fig. 4). After a few days, she did not have neurologic symptoms anymore.
On the last checked X-ray, at the former fracture site, a bony union was found (Fig. 5). Two months post-operatively, the pa-tient continues to do well.
Discussion
K-wire, either alone or in conjunction with a tension band wire, are very frequently used by trauma surgeon for trauma surgery to hold the unstable fractures. Benign thin, tubular and
unthreaded wires have strong tendency to migrate back along the path of their insertion. Antegrade migration of K-wire is rath-er uncommon. Furthermore, most of antegrade pin migration remains poorly reported because of the sensitive and litigious nature of the problem.1)
Case of K-wire migration were first reported by Mazet2) in 1943, and then, K-wire have been reported to migrate to heart, thorax, mediastinum, abdominal wall, spleen, and spinal canal etc.3-8)
Interestingly, all types of migrations have been reported, es-pecially with use in the shoulder region. The mechanism is still obscure, but in theory, factors as the great freedom of shoulder movements containing muscle action, the breathing movements, the gravitational force and the regional bony re-absorption are probably involved.1,7,9) In our case, maybe the great freedom of shoulder movement due to patient’s incooperation and the regional bony re-absorption contributed to the migration of the
Fig. 2. Plain radiograph shows the migration of one wire.
Fig. 3. On computed tomography scans, the K-wire located in C7-T1 inter-vertebral foramen.
Fig. 5. Last follow-up radiograph shows the bone union of left clavicle.
Fig. 4. Photograph shows about 6 cm sized metallic device.

Migration of K-wire into Intervertebral ForamenJin-Ho Lee, et al.
www.cisejournal.org 79
K-wire. Also, as the far cortex was already drilled, the wire faced minimal resistance to migration.
Like this case, in 1986, Conzen and Sollmann10) described a case that complained radiating pain in the C6 and C7 derma-tome after interspinal migration of a K-wire after clavicle fracture. They mentioned that follow-up X-rays should be taken every 2 or 4 weeks until the pins are removed in order to avoid legal problem.
We think that the orthopaedic surgeons should take care when they fix the fracture with metallic wires especially in the shoulder region. For example, the complication can be avoided through using a threaded pin for the shoulder surgery, bending the external end of the pin and choosing a correct diameter of the K-wire. Also, patients with a K-wire osteosynthesis should be followed regularly with radiographs every 2 or 4 weeks. And if necessary, until K-wires are removed, arm movement should be restricted to elevation.
References
1. Lyons FA, Rockwood CA Jr. Migration of pins used in opera-tions on the shoulder. J Bone Joint Surg Am. 1990;72(8):1262-7.
2. Mazet R. Migration of a Kirschner-wire from the shoulder
region into the lung. Report of two cases. J Bone Joint Surg. 1943;25(2):477-83.
3. Anić D, Brida V, Jelić I, Orlić D. The cardiac migration of a Kirschner wire. A case report. Tex Heart Inst J. 1997;24(4):359-61.
4. Chou NS, Wu MH, Chan CS, Lai WW, Lin MY. Intratho-racic migration of Kirschner wires. J Formos Med Assoc. 1994;93(11-12):974-6.
5. Demaria R, Picard E, Bodino M, et al. Migration of a clavicu-lar bone wire acutely perforating the ascending aorta. Presse Med. 1998;27(21):1013.
6. Brade A, Hippe P. Migration of Kirschner wire following osteo-syntheses of the hip (author’s transl). Z Orthop Ihre Grenzgeb. 1981;119(1):80-4.
7. Rajesh PB, Nair KK. Unusual migration of a Kirschner wire. Eur J Cardiothorac Surg. 1991;5(3):164.
8. Regel JP, Pospiech J, Aalders TA, Ruchholtz S. Intraspinal migra-tion of a Kirschner wire 3 months after clavicular fracture fixa-tion. Neurosurg Rev. 2002;25(1-2):110-2.
9. Kumar P, Godbole R, Rees GM, Sarkar P. Intrathoracic migra-tion of a Kirschner wire. J R Soc Med. 2002;95(4):198-9.
10. Conzen M, Sollmann H. Displacement of materials in the cer-vical spinal canal following clavicular fixation as a late compli-cation. Unfallchirurg. 1986;89(1):47-8.
Tuberculous Tenosynovitis of the Elbow - A Case Report
Chi-Hun Oh, Jung-Ho Park, Jung-Wook Kim
Department of Orthopedic Surgery, Korea University Ansan Hospital, Korea University College of Medicine, Ansan, Korea
A 29-year-old man visited our clinic owing to a persistent swelling in the anterior part of the left elbow joint that began one year ago. Through magnetic resonance imaging (MRI), we observed tenosynovitis with multiple rice bodies, and so we performed an excisional biopsy and tenosynovectomy. Through pathology and culture tests, we identified tuberculosis in the tissue biopsy that we harvested in-traoperatively. Following the anti-tuberculosis medication relieved the patient’s symptoms without recurrence. Since tuberculosis of the elbow occurs only rarely, and the symptoms mimic those of rheumatoid synovitis or of non-specific chronic synovitis, early diagnosis and appropriate treatment are often delayed. The authors report this rare case of tuberculous tenosynovitis of the elbow with a review of the relevant literature.(Clin Shoulder Elb 2014;17(2):80-83)
Key Words: Elbow; Tuberculous tenosynovitis; Tenosynovectomy; Anti-tuberculosis medication
Recently, the improvements in the level of nutrition and hygiene, as well as the developments in anti-tuberculosis drugs have led to the decline of tuberculous arthritis and tenosynovitis. Musculoskeletal tuberculosis comprises less than 5% of all tuber-culosis cases, and are often restricted to the spine and weight bearing joints.1) Those that occur in the elbow joint comprises 2−5% of all osetoarticular tuberculosis cases.2) Osetoarticular tuberculosis is reported often, but tuberculosis tenosynovitis is extremely rare. Thus in this paper, the authors report the obser-vation of a 29-year-old man with tuberculosis tenosynovitis in the left elbow joint with a review of the relevant literature.
Case Report
A 29-year-old man visited our clinic owing to discomfiture from swelling in the anterior part of the left elbow joint that be-gan one year ago. The patient did not have a history of external trauma, but reported that the swelling occurred after a blood donation one year ago, and that he received acupuncture in the said area on numerous occasions thereafter. At the time of visit, a physical examination of the patient showed no clinical symp-toms, such as fever or weight loss, apart from the localized swell-
ing in the anterior part of the left elbow joint. Both active and passive range of movement of the elbow was normal, apart from the presence slight discomfiture. Bone tenderness, temperature changes, or Tinel’s sign were not observed.
The basic radiologic test was normal apart from the swell-ing in soft tissue of the anterior part of the elbow. The magnetic resonance imaging (MRI) showed a mass of exudate surrounding the forearm biceps tendon with marked extension to the distal part of the radial tuberosity. Furthermore, proton density weight-ed images and fat suppressed T2-weighted images showed mul-tiple low signal rice bodies (Fig. 1) within the mass lesion. Whilst, the basic radiologic test of the chest and respiratory function test were normal, the sputum cytology and culture tests were both negative. Blood tests were normal.
Tenosynovectomy was carried out in the anterior part of the elbow joint under the assumption that a tuberculous tenosynovi-tis in the bicep tendon was present. During the operation, it was observed that the tendon sheath in the distal part of the biceps tendon had thickened, and a cyst of synovial lining tissue had formed around the biceps anchor. During the operation, many rice bodies were observed when the synovial lining cyst of the granulation tissue was opened (Fig. 2). A wide-range tenosyno-
CiSEClinics in Shoulder and Elbow
Copyright © 2014 Korean Shoulder and Elbow Society. All Rights Reserved.This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
pISSN 1226-9344eISSN 2288-8721
CASE REPORT
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014http://dx.doi.org/10.5397/cise.2014.17.2.80
Received August 16, 2013. Revised April 8, 2014. Accepted April 9, 2014.
Correspondence to: Jung-Ho ParkDepartment of Orthopedic Surgery, Korea University Ansan Hospital, 123 Jeokgeum-ro, Danwon-gu, Ansan 425-707, KoreaTel: +82-31-412-5040 -, Fax: +82-31-439-3852, E-mail: [email protected]
Financial support: None. Conflict of interests: None.

Tuberculous Tenosynovitis of the ElbowChi-Hun Oh, et al.
www.cisejournal.org 81
vectomy and debridement was carried out, during which tissue biopsy was obtained for pathological and microbiological tests. In the pathological test, staining of the tendon sheath and the
multiple rice bodies with hematoxylin-eosin showed localized caseation necrosis and chronic caseating granulomatous inflam-mation (Fig. 3). Real-time polymerase chain reaction (PCR) and Periodic Acid Schiff staining of the Mycobacterium tuberculosis-infected tissue showed a negative result, but Acid-fast staining showed a positive result. Immediately, the patient was started on anti-tuberculosis medication composed of 2 months of qua-druple therapy (isoniazid, rifampin, Ethambutol, pyrazinamide), followed by 7 months of triple therapy that excludes pyrazin-amide. After surgery, the incision area from the operation healed normally, and at two weeks, the suture stitch was removed after which early joint exercise was started. Follow-up via outpatient visits are being carried out at each following month after surgery. Even at 10 months after surgery, there was no recurrence or degeneration of condition. At the final follow-up, the elbow and wrist joint functions were normal, indicated by a normal range of motion and muscle strength.
Discussion
Tuberculous tenosynovitis is a relatively rare disease. At the
Fig. 1. (A) The proton density-weighted sagittal image shows a mass surrounding the biceps tendon that extends to the distal part of the radial tuberosity. (B) The T2-weighted axial image shows multiple low signal rice bodies within the mass lesion.
Fig. 2. In operation, many rice bodies were observed in the synovial lining cyst of the granulation tissue.
Fig. 3. A Langerhans cell is surrounded by lymphocytes and epithelioid cells in hematoxylin-eosin staining. Chronic caseating granulomatous inflamma-tion is also seen (×200).

82 www.cisejournal.org
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014
early stages it occurs progressively without clear symptoms, dur-ing which swelling and inflammatory changes in the tendon sheath forms gradually, followed by symptoms such as pain and restriction in joint movement. Due to such characteristics of the disease, early diagnosis followed by the appropriate treatment is critical.3)
In the Republic of Korea, osetoarticular tuberculosis in the elbow joint and tuberculous tenosynovitis in the flexor tendon of the wrist joint have been reported,4,5) but tuberculous tenosyno-vitis in the elbow joint is yet to be reported. One exception is in foreign literature where Asaka et al.6) have reported one case of tuberculous tenosynovitis in the elbow.
The area of the body most susceptible to tuberculous teno-synovitis is the wrist joint, in which the flexor tendon is twice as more susceptible than the extensor tendon.7) The clinical symptom is the gradual development of a swelling that is most commonly painless but can sometimes be painful and restrict joint movement. Though uncommon, numbness and muscle weakness have also been noted. On the other hand, infection of the respiratory system and other musculoskeletal infections are rare co-morbidities, as are whole-body fevers and weight loss.7) Furthermore, the symptoms are also similar to symptoms of rheumatoid arthritis and non-specific chronic tenosynovitis. Therefore, delay of diagnosis is common as is the start of appro-priate treatment.3)
The diagnosis of tuberculous tenosynovitis is carried out via the positive culture test of the bacteria. The rate of diagnosis from a culture test varies depending on the form of clinical specimen used. Testing on joint fluid gives a diagnosis rate of less than 50%, whilst a biopsy sample of the tendon sheath obtained from surgery gives a rate greater than 90%.8) A biopsy sample is also helpful in that a further pathology test may be carried out to differentiate conventional granulomas or the presence of acid fast bacilli via Acid-fast staining. However, bacterial culture tests take at least 6 weeks during which the diagnostic rate of Acid-fast staining falls and cannot differentiate well from atypi-cal mycobacterial infections. Therefore, a clinical diagnosis of tuberculosis is crucial. Bush and Schneider3) suggest two clinical situations in which tuberculous tenosynovitis should be strongly suspected. First, through a physical examination, is the presence of a progressive, painless tenosynovitis with either an abnormal basic radiologic screening of the chest or a history of mycobac-terium tuberculosis infection or exposure. Second, through a surgical examination, is whether the tenosynovitis has a relatively widespread area and a severe adherence, and in particular when multiple rice bodies are also present. Furthermore, MRI are recommended through which the presence of multiple rice bodies can be confirmed. If such clinical observations are observed together, tuberculosis must be strongly suspected and anti-tuberculosis medication must be started on as soon as pos-sible.
The most effective treatment of tuberculous tenosynovitis is when thorough tenosynovectomy and anti-tuberculosis chemo-therapy is carried out in parallel.3) Mycobacterium tuberculosis infected tissue undergoes necrosis, which has a negative impact on blood flow. Therefore, the injection of anti-tuberculosis drug alone is insufficient for complete recovery, and surgical treat-ment alone also has high rates of recurrence. Boyes9) reported a recovery rate of 70% when surgery is carried out alone, whilst a 15% recurrence rate is seen when chemotherapy is carried out in parallel. However, these recurrences were recovered with conservative treatment. The injection of anti-tuberculosis drugs are recommended for at least 9 months, which generally com-prises of, 2 months of quadruple therapy (isoniazid, rifampin, Ethambutol, pyrazinamide) followed by at least 4 months of triple therapy that excludes pyrazinamide.
In musculoskeletal infections, the infection spreads from other tuberculosis-infected organs, such as the lungs and the lymph nodes, from which the mycobacterium tuberculosis travels through blood to invade the subchondral bone or the tubular bone. In some cases, infection occurs by the invasion of the synovial sheaths or via direct inoculation.10) In our study, we suspect that infection may have occurred via needles used in acupuncture, which the patient received after the occurrence of a swelling that formed since donating blood one year ago. However, in order to elucidate a causal relationship further epi-demiological investigation is required.
The frequency of tuberculosis tenosynovitis is very low, but it could be the cause of a painless swelling in elbow joints of certain patients. Further, if history of an intralesional injection is present or the patient does not respond to appropriate treat-ment, the possibility of tuberculosis tenosynovitis must be con-sidered during diagnosis.
References
1. Alvarez S, McCabe WR. Extrapulmonary tuberculosis revisited: a review of experience at Boston City and other hospitals. Medicine (Baltimore). 1984;63(1):25-55.
2. Dhillon MS, Goel A, Prabhakar S, Aggarwal S, Bachhal V. Tu-berculosis of the elbow: A clinicoradiological analysis. Indian J Orthop. 2012;46(2):200-5.
3. Bush DC, Schneider LH. Tuberculosis of the hand and wrist. J Hand Surg Am. 1984;9(3):391-8.
4. Moon MS, Bae TY, Kim JB, Chon JG. Cystic tuberculosis in olecranon, mimicking the bone tumor: A case report. J Korean Shoulder Elbow Soc. 2008;11(2):193-5.
5. Jung JM, Kim JO, Yun YH, et al. Tenosynovectomy for chronic flexor tenosynovitis at the wrist. J Korean Soc Surg Hand. 2004;9(2):83-8.
6. Asaka T, Takizawa Y, Kariya T, et al. Tuberculous tenosynovitis in the elbow joint. Intern Med. 1996;35(2):162-5.

Tuberculous Tenosynovitis of the ElbowChi-Hun Oh, et al.
www.cisejournal.org 83
7. Lee KE. Tuberculosis presenting as carpal tunnel syndrome. J Hand Surg Am. 1985;10(2):242-5.
8. Andersson MI, Willcox PA. Tuberculous tenosynovitis and car-pal tunnel syndrome as a presentation of HIV disease. J Infect. 1999;39(3):240-1.
9. Boyes JH. Bunnell’s surgery of the hand. 5th ed. Philadelphia: J. B. Lippincott Co; 1970. 632.
10. Watts HG, Lifeso RM. Tuberculosis of bones and joints. J Bone Joint Surg Am. 1996;78(2):288-98.

Animal Experiments Using Rotator Cuff
Seok Won Chung, Sae Hoon Kim1, Joo Han Oh2
Department of Orthopaedic Surgery, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Department of Orthopaedic Surgery, 1Seoul National University Hospital, Seoul, 2Seoul National University Bundang Hospital, Seongnam, Seoul National University College of Medicine, Korea
In conducting animal studies using rotator cuff, researchers should select the appropriate types of animals and experimental models. This should also be followed by complete understanding of the selected experimental animals as well as the methods for evaluating the results. Thus, researchers could minimize errors and failure in conducting animal experimental studies. Further, this will provide a basis of establishing new idea and theory about rotator cuff diseases.(Clin Shoulder Elb 2014;17(2):84-90)
Key Words: Animal; Rotator cuff
Introduction
An animal study is an intermediate one between the labora-tory and clinical studies. From the view point that it is conducted prior to clinical studies, it is commonly referred to as pre-clinical study. An animal study is one of the methods for evaluating new theory or treatment modalities on a whole-body scale in a well-controlled, consistent environment. It is probable that clinical studies can be conducted or clinical applications can be rejected based on the results of animal studies. Conversely, animal stud-ies are also conducted to interpret the results of clinical study or to clarify the relevant mechanisms. In conducting animal studies, researchers should determine the study objectives, the type of experimental animals in creating a certain type of animal models and the methods for evaluating the results. In this article, we dis-cuss the actual procedure of animal studies based on the above viewpoints in conducting animal studies using rotator cuff (Fig. 1).
Main Subjects
Study ObjectivesThe subject matters of studies using animal rotator cuff can
be classified into the following:
(1) Etiology(2) Surgical technique(3) Rehabilitation(4) The effects of prosthesis and reinforcing materials
CiSEClinics in Shoulder and Elbow
Copyright © 2014 Korean Shoulder and Elbow Society. All Rights Reserved.This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
pISSN 1226-9344eISSN 2288-8721
REVIEW ARTICLE
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014http://dx.doi.org/10.5397/cise.2014.17.2.84
Received May 5, 2014. Revised June 3, 2014. Accepted June 9, 2014.
Correspondence to: Joo Han OhDepartment of Orthopaedic Surgery, Seoul National University Bundang Hospital, Seoul National University College of Medicine, 166 Goomi-ro, Bundang-gu, Seongnam 463-707, KoreaTel: +82-31-787-7197, Fax: +82-31-787-4056, E-mail: [email protected]
Financial support: None. Conflict of interests: None.
Fig. 1. Flowchart for the process of animal studies using rotator cuff.

Animal Experiments Using Rotator CuffSeok Won Chung, et al.
www.cisejournal.org 85
(5) The effects of cellular or biological additives(6) Alternative or adjuvant treatment modalities(7) The actions of local and systemic factorsThe etiologies of diseases occurring in the rotator cuff may
include age-related impingement syndrome,1) muscle atrophy and fatty degeneration,2) the functions of tendon, cartilaginous changes after the onset of rotator cuff tear, shoulder stiffness, and the effects on the adjacent anatomical structures such as the long head of biceps tendon. In addition, researchers may also con-sider such matters as the difference depending on the location of rotator cuff tears, the optimal timing of surgery, and postop-erative changes in the bone strength. As the surgical technique, researchers may compare between various types of suturing methods,3) the appropriate sites for the insertion of anchor, the adjustment of pressure and tension for sutures, and the prepara-tion methods for the footprint. With regard to the rehabilitation, researchers may consider the effects of exercise and immobili-zation after operation.4) Moreover, subject matters may also in-clude the difference depending on the types of anchor and the effects of various patch grafts on the tendon-to-bone healing.5) Furthermore, researchers may also consider the effects of various growth factors,6) stem cells7) or platelet-rich plasma.8) Besides, the effects diabetes,9) smoking,10) hypercholesterolemia,11) para-thyroid hormone,12) vitamin D,13) various types of nonsteroidal anti-inflammatory drugs14) and steroids,15) botulinum toxin,16) local anesthetics,17) low intensity pulsed ultrasound18) or extra-corporeal shock wave may also be of interest to readers. Once researchers have determined the subject matter of the study, they should consider the anatomical sites that they should evalu-ate. In conducting studies about rotator cuff, the anatomical sites would be muscle, bone or tendon-to-bone junction.19) In studies about the muscles, researchers would evaluate changes in the muscle fiber, muscle atrophy or fatty degeneration.7) In studies about tendon, researches would evaluate the maturity of col-lagen fiber and the characteristics of tenocytes and fibroblasts.20) In studies about the bone, researchers would evaluate changes in the bone mineral density and the degree of the expression of osteoblasts and chondroblasts.21) In particular, the tendon-to-bone junction is a region of interest in studies about rotator cuff, for which researchers would evaluate the types, orientation and continuity of collagen fibers, the degree of fibrocartilage and ten-sile strength.8)
The Selection of Experimental AnimalsIn conducting studies about rotator cuff, researchers use such
experimental animals as rats,2) rabbits,7) dogs,22) lambs,5) goats23) and monkeys.24)
Firstly, rats are characterized by morphological findings that the supraspinatus tendon passes below the arch, which is simi-lar to those of humans.1) They are the most frequently used to create an animal experimental model because they are cheap
and a large number of animals are available for experimental procedures. In particular, the etiology of various types of rota-tor cuff diseases has been elucidated in an animal experimental model using rats.25) Due to the presence of various molecular markers, they can be easily used for molecular biological tests.19) However, their rotator cuff is of small size. This may make it dif-ficult to perform surgery and assessment. Moreover, they exhibit an excellent profile of regeneration. It is therefore probable that it would be difficult to analyze the results of the experiment due to spontaneous recovery after the onset of rotator cuff tear.
Secondly, rabbits are also advantageous in that they are cheap and can be easily bred. In particular, the natural course of fatty degeneration has been clarified in the literature.26) Therefore, they can be easily applied to studies about fatty degeneration. They are also disadvantageous; however, in that the shoulder joint is a weight-bearing one and the supraspinatus tendon and its adjacent structures are different from those of humans.27) This has led to the development of an animal experimental model using the subscapularis tendon below the coracoid process, for which studies have been conducted in a limited scope.27) But there are some problems due to the deep location and severe degree of retraction.
Thirdly, large sized experimental animals, such as dogs, lambs and goats, are also used to create an animal experimental model of rotator cuff tear. In Korea, however, lambs cannot be used for such studies because of breeding problems. As the large sized animals walk on four feet, their mobility is limited as compared with humans in that their shoulder joint is a weight-bearing one and they perform only extension and flexion. Studies using the rotator cuff of large sized animals have been mainly conducted using the infraspinatus tendon.22) The size of infraspinatus ten-don in dogs is as approximately half as humans.28) Mongrel dogs are not too expensive and they can be easily supplied. There-fore, they can be considered as experimental animals for rotator cuff model. The size and shape of the infraspinatus tendon in goats are very similar to those of humans.5) Thus, they can be easily used for animal experiments simulating surgical proce-dures using implant materials in humans. In addition, they also have a similar profile of biomechanical properties.29) This makes them to be an appropriate model for biomechanical studies. But it is difficult to breed them. Typically, goats as well as dogs are disadvantageous in that the anatomical characteristics of their rotator cuff are quite different from those of humans. In particu-lar, their shoulder joint is characterized by a lack of the clavicle, the prematurity of acromion and coracoid process, the discrete presence of infraspinatus tendon as an extraarticular structure outside of the bursa.29) These features are different from humans. In addition, due to a lack of species-specific probes or reagents, it would be difficult to perform molecular biological tests using goats or dogs (Table 1).29)
Finally, monkeys can also be used to create an animal experi-

86 www.cisejournal.org
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014
mental model for rotator cuff.24) Due to such problems as the complex legal procedure for experiments, high cost, breeding and ethical issue, they are not available for experimental studies about rotator cuff at the moment in Korea.
Selection of Animal Experimental Models Using Rotator Cuff
Depending on surgical sites, animal experimental models us-ing rotator cuff can be a rat model of supraspinatus tendon,20) a rabbit model of subscapularis tendon7) and a large-animal model of infraspinatus tendon.5) It is a matter of course that a rabbit model of supraspinatus or infraspinatus tendon and large-animal models of supraspinatus tendon using dogs or goats are also available. In this section, however, we’ll discuss representative animal experimental models of rotator cuff for each experimen-tal animal.
A rat model of supraspinatus model is a representative one which used the most frequently to examine rotator cuff using experimental animals. As described above, there is a similarity in the adjacent environment to the supraspinatus tendon between rats and humans.1) Therefore, etiologies of diseases that occur in the rotator cuff have been well investigated in a rat model. Using the rat model, nearly all types of researches are possible includ-ing the elucidation of the relevant molecular biological mecha-nism to various rotator cuff diseases.
Rabbit models of subscapularis tendon are created based on the similarity in the anatomical characteristics between the subscapularis tendon complex constrained by subcoracoid bony tunnel and the coracobrachialis muscle in rabbits and
the supraspinatus tendon complex constrained by subacromial bony tunnel and the coracoacromial ligament in humans.27) In addition, the shape of the lesser tubercle where the subscapu-laris tendon is inserted in rabbits shows similar characteristics to that of the greater tubercle where the supraspinatus tendon is inserted in humans.29) The size of the lesser tubercle in rabbits is approximately 1/4 of the greater tubercle in humans.29) To date, however, only a small number of studies have been conducted probably due to the complexity of the surgical procedures com-ing from a small tendinous portion of the rabbit subscapularis, a significant retraction of the torn subscapualaris, and a difficulty in exposure.
Nearly all the studies about rotator cuff in dogs and goats have been conducted using the infraspinatus tendon.23) An ac-cess can be easily made for experimental animals placed in a lateral decubitus position. Particularly in goats, the size and biomechanical properties of the infraspinatus tendon are very close to those of humans.29) Therefore, they are frequently used to create an experimental model for the purposes of evaluating the biomechanical effects of implants or augmenting materials as well as surgical technique. But the infraspinatus tendon is an extraarticular structure that is present outside of the bursa and its anatomical structure is different from that of human.29) This limits the interpretability of the results of biological repair. In addition, there are no molecular markers for molecular biological stud-ies.29) Most of the dogs and goats are used to assess the results of biomechanical studies.
Most of rotator cuff diseases are chronic ones accompanied by the degenerative changes. It can therefore be inferred that an
Table 1. Characteristics of Animal Experimental Models of Rotator Cuff
Rat/mouse Rabbit Dog or goat
Advantage Comparable anatomy to humanWidely available InexpensiveLowest demandLarge number is possible
Appropriate for the investigation of fibrofatty infiltration
Relatively inexpensiveLow demand
Close to human sizeUse of standard techniqueAppropriate for the investigation of
biomechanical properties
Disadvantage Small sizeSignificant fatty infiltration in only with
nerve transection High healing potential
Weight bearing jointSubscapularis model
Limited movement directionWeight bearing jointDifferent anatomy from humanInfraspinatus modelExpensiveHigh demand
Research aim Tendon-to-bone healingPathomechanism (age-related degeneration,
intrinsic and extrinsic injury)Molecular pathwayRehabilitationEffect of cells and biologic additiveEffect of systemic factor
Tendon-to-bone healingMuscular changeEffect of cells and biologic additive Effect of scaffold augmentation
Tendon-to-bone healingMechanical strength Repair techniqueEffect of scaffold augmentation
Price 10,000 KRW/animal 50,000 KRW/animal 400,000 or 1,000,000 KRW/animal
KRW: Korean won.

Animal Experiments Using Rotator CuffSeok Won Chung, et al.
www.cisejournal.org 87
animal experimental model of rotator cuff, reflecting the chronic diseases, would be more useful to simulate the clinical setting. After substantial periods of time after the resection of the rota-tor cuff, chronic animal models can be created. We also have experiences about creating a chronic animal model by leaving the torn tendon for six weeks and enclosing that with the use of penrose drain for the prevention of the adhesion to the adjacent tissue following the dissection of the subscapularis and supraspi-natus tendon in rabbits.8)
In addition, an impingement model has been established to induce the intrinsic or extrinsic impingement.25) To induce the intrinsic impingement, inflammatory responses are triggered using injections of collagenase.1) To induce the extrinsic impinge-ment, animal experimental models have been created in such a manner that the Achilles tendon is placed under the acromion1) or bone graft is performed.30)
Other animal models of rotator cuff may include an overuse model where experimental animals are induced to run on a treadmill for the purposes of triggering the occurrence of repeat-ed microtears and degenerative changes,31) an immobilization model where the plaster cast is applied to the shoulder joint32) and a denervation model where the fatty degeneration of the rotator cuff is induced through the dissection of the suprascapu-lar nerve.33)
But if there is a lack of the established animal experimental models that are appropriate for the subject matters, research-ers would create a new model. It can be stated that it would provide a basis of various types of further researches if there are any chances that researchers create a new animal experimental model. This would be of great significance.
As described here, after selecting experimental animals and the relevant models based on their subject matters, researchers would perform surgical operations or other procedures. Then, they would perform experimental procedures to evaluate the results after certain periods of time.
Methods for Evaluating the ResultsMethods for evaluating the results of animal studies may in-
clude gross appearance, biomechanical evaluation, histological evaluation, immunohistochemical evaluation and radiological evaluation. In particular, biomechanical and histological tests are essential for assessing the results of animal experimental studies.
On gross examination, researchers evaluate the detachment of rotator cuff from the bone, the degree muscle atrophy, the color or the weight of muscles, and the thickness and width of rotator cuff tendon.7,26) Moreover, researchers may also mea-sure the contact pressure and area by placing the pressure film between the rotator cuff tendon and the bone and performing various types of suturing.34)
A biomechanical test is a tensile testing where researchers as-sess the solidity of tendon-to-bone healing with the traction of
rotator cuff tendon inserted in the bone. In the biomechanical test, researchers are required to use instruments for fixing the humerus and tendon and pulling the tendon from the bone. Instruments for fixing the humerus and tendon are commonly designed by researchers. According to a review of literatures, various types of these instruments have been designed and then used for animal experimental studies.35,36) As the factors that are measured on biomechanical test, there are mode of failure and various parameters derived from the stress-strain curve or load relaxation curve. The mode of failure means the specific sites where the failure occurred, which may include the avulsion of the humerus, the insertion sites, the parenchyma of the tendon and the fixation sites of clamp.37) As a whole, the rupture at the parenchyma of the tendon is referred to as stronger tendon-to-bone healing.8) Various parameters on both the stress-strain curve and load relaxation curve may also be used. It can be stat-ed, however, that load to failure is the most important indicator of the strength of tendon-to-bone healing.7) In addition, it would be mandatory to measure the load to failure, which is essential for performing the biomechanical test.
A histopathologic examination is a laboratory process where various types of staining methods are performed. It is com-monly encountered that the tissue sectioning, fixation, paraffin-embedding, staining and slide preparation are performed with the help of the department of pathology or reference laborato-ries. Thus, the selection of the specific staining method rather than the tissue preparation would be more important. Staining methods for animal experimental studies about rotator cuff include hematoxylin and eosin staining for examination of the overall morphology and density of the cells,38) Oil Red O and osmium tetroxide staining for examination of the adipose tissue in the muscles,39) Masson’s trichrome staining and Picrosirius red for examination of the connective tissue and collagen fibers,40) Safranin O staining and Toluidine blue staining for examination of cartilages based on proteoglycan-positive staining properties16) and Verhoeff-van Gieson staining for examination of elastic fi-ber. These staining methods are used to examine the muscles, tendons, bone and cartilage, tendon-to-bone insertion site, and graft materials. Basically, the cellularity, vascularity and inflamma-tion rates are checked. In addition, the muscle fibers, connective tissue and adipose tissue in the muscle, and the organization and maturation of the collagen fibers as well as fibroblasts and tenocytes in the tendon are examined using the above staining methods for the muscle and tendon. At the junction between the tendon and the bone, staining methods are used to assess the orientation and the continuity of the collagen fibers between tendon and bone, the fibrocartilage, and the degree of the granulation tissue formation. Moreover, the staining methods for the cartilage are used to assess the surface irregularity, the degree of staining property and that of the maintenance of tidemark. In addition, the formation of new bone, the organization of and

88 www.cisejournal.org
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014
the connectivity to graft materials and the degree of the absorp-tion of graft materials can be assessed. The arrangement of col-lagen fibers can be accurately on confocal microscopy and po-larized light microscopy although it can also be examined using conventional types of light microscopy.41) Both semi-quantitative and quantitative methods can be used for the evaluation. As a whole, however, semi-quantitative methods are used. It is also probable that such imaging software as the Image J software or Photoshop software may be used for quantitative analyses.41) In general, the cellularity is measured as the number of cells per unit area and the shape of the cells is given 1 point as it becomes close to the round shape (0 to 1 point).38) In the assess-ment of the muscle tissue, the size of muscle fibers is measured based on the distribution of actual measurements of their width and area.42) In addition, the degree of the muscle atrophy and the deposition of adipose cells are evaluated using semi-quanti-tative methods based on a 4- (no/a few/some/many) or 5-point scale (no/minimal/mild/moderate/severe).7) Furthermore, semi-quantitative methods can also be considered to evaluate the tendon-to-bone junction based on the relevant grading system.8) This may also be accompanied by the use of conventional scor-ing system such as the Movin score and Bonar score43) or tendon maturation score.44)
Immunohistochemical and fluorescent staining methods are used to confirm the presence of specific materials that are present in the tissues or cells with the use of antigen-antibody reaction.20) That is, they are based on the methods for detecting antigens by labeling antibodies with a specific type of materi-als. Representative markers include fluorescent dye or enzymes such as peroxidase. Examinations are routinely done using light microscopy or epifluorescence microscopy. To date, various types of markers have been established in rats and rabbits.42) The results are evaluated based on the degree of the expression of target proteins. The accurate sites of the expression of target pro-teins in the tissues can be identified compared with the Western blotting or polymerase chain reaction (PCR). Immunohistochem-ical and fluorescent staining methods as well as Western blotting or PCR are also advantages that the molecular pathways can be clarified.45)
Radiological methods include micro-computed tomogra-phy,46) magnetic resonance imaging47) and ultrasonography,48) by which researchers can evaluate the degree of fatty degeneration, muscle atrophy, tendon-to-bone healing, and alterations in the thickness of cartilage.46-48)
In addition to these, there are also methods based on electro-physiology, such as electromyography, where active electrodes are placed in the target muscle and reference electrodes are placed in the tendons that are adjacent to the sites of bone inser-tion.49) Then, the electrical activity of the target muscle is evalu-ated with the stimulation of nerves innervating the target muscle at the supramaximal intensity.49) These methods are character-
ized by the functional assessment rather than the morphological one.
The assessment can be done at the single time point, but it may also be done at more than two time points. It would be desirable; however, to perform the assessment at more than two time points, which is essential for analyzing time-dependent changes. According to a review of literatures, assessments have been performed until 16 weeks in rats or rabbits and 26 weeks in dogs, lambs or goats.50,51)
Conclusion
In conducting animal studies using rotator cuff, researchers should select the appropriate types of animals and experimental models. This should also be followed by complete understand-ing of the selected experimental animals as well as the methods for evaluating the results. Thus, researchers could minimize er-rors and failure in conducting animal experimental studies. Fur-ther, this will provide a basis of establishing new idea and theory about rotator cuff diseases.
References
1. Soslowsky LJ, Carpenter JE, DeBano CM, Banerji I, Moalli MR. Development and use of an animal model for investigations on rotator cuff disease. J Shoulder Elbow Surg. 1996;5(5):383-92.
2. Plate JF, Pace LA, Seyler TM, et al. Age-related changes af-fect rat rotator cuff muscle function. J Shoulder Elbow Surg. 2014;23(1):91-8.
3. Gerber C, Schneeberger AG, Perren SM, Nyffeler RW. Experi-mental rotator cuff repair. A preliminary study. J Bone Joint Surg Am. 1999;81(9):1281-90.
4. Jelinsky SA, Lake SP, Archambault JM, Soslowsky LJ. Gene expression in rat supraspinatus tendon recovers from overuse with rest. Clin Orthop Relat Res. 2008;466(7):1612-7.
5. Nicholson GP, Breur GJ, Van Sickle D, Yao JQ, Kim J, Blanchard CR. Evaluation of a cross-linked acellular porcine dermal patch for rotator cuff repair augmentation in an ovine model. J Shoulder Elbow Surg. 2007;16(5 Suppl):S184-90.
6. Rodeo SA, Potter HG, Kawamura S, Turner AS, Kim HJ, Atkin-son BL. Biologic augmentation of rotator cuff tendon-healing with use of a mixture of osteoinductive growth factors. J Bone Joint Surg Am. 2007;89(11):2485-97.
7. Oh JH, Chung SW, Kim SH, Chung JY, Kim JY. 2013 Neer Award: Effect of the adipose-derived stem cell for the im-provement of fatty degeneration and rotator cuff healing in rabbit model. J Shoulder Elbow Surg. 2014;23(4):445-55.
8. Chung SW, Song BW, Kim YH, Park KU, Oh JH. Effect of plate-let-rich plasma and porcine dermal collagen graft augmenta-tion for rotator cuff healing in a rabbit model. Am J Sports

Animal Experiments Using Rotator CuffSeok Won Chung, et al.
www.cisejournal.org 89
Med. 2013;41(12):2909-18. 9. Bedi A, Fox AJ, Harris PE, et al. Diabetes mellitus impairs
tendon-bone healing after rotator cuff repair. J Shoulder Elbow Surg. 2010;19(7):978-88.
10. Ichinose R, Sano H, Kishimoto KN, Sakamoto N, Sato M, Itoi E. Alteration of the material properties of the normal supraspina-tus tendon by nicotine treatment in a rat model. Acta Orthop. 2010;81(5):634-8.
11. Beason DP, Tucker JJ, Lee CS, Edelstein L, Abboud JA, Sos-lowsky LJ. Rat rotator cuff tendon-to-bone healing properties are adversely affected by hypercholesterolemia. J Shoulder Elbow Surg. 2014;23(6):867-72.
12. Hettrich CM, Beamer BS, Bedi A, et al. The effect of rhPTH on the healing of tendon to bone in a rat model. J Orthop Res. 2012;30(5):769-74.
13. Angeline ME, Ma R, Pascual-Garrido C, et al. Effect of diet-induced vitamin D deficiency on rotator cuff healing in a rat model. Am J Sports Med. 2014;42(1):27-34.
14. Cohen DB, Kawamura S, Ehteshami JR, Rodeo SA. Indometh-acin and celecoxib impair rotator cuff tendon-to-bone healing. Am J Sports Med. 2006;34(3):362-9.
15. Papaspiliopoulos A, Papaparaskeva K, Papadopoulou E, Fer-oussis J, Papalois A, Zoubos A. The effect of local use of nan-drolone decanoate on rotator cuff repair in rabbits. J Invest Surg. 2010;23(4):204-7.
16. Ficklscherer A, Hartl TK, Scharf M, et al. Effects of selective pa-ralysis of the supraspinatus muscle using botulinum neurotoxin a in rotator cuff healing in rats. J Orthop Res. 2013;31(5):716-23.
17. Rao AJ, Johnston TR, Harris AH, Smith RL, Costouros JG. Inhi-bition of chondrocyte and synovial cell death after exposure to commonly used anesthetics: chondrocyte apoptosis after anesthetics. Am J Sports Med. 2014;42(1):50-8.
18. Nagura I, Kokubu T, Niikura T, et al. I-4. The effect of low-intensity pulsed ultrasound (LIPUS) on human rotator cuff de-rived cells. J Orthop Trauma. 2014;28(6):S3.
19. Edelstein L, Thomas SJ, Soslowsky LJ. Rotator cuff tears: what have we learned from animal models? J Musculoskelet Neuro-nal Interact. 2011;11(2):150-62.
20. Yokota A, Gimbel JA, Williams GR, Soslowsky LJ. Supraspinatus tendon composition remains altered long after tendon detach-ment. J Shoulder Elbow Surg. 2005;14(1 Suppl S):72S-8.
21. Wopenka B, Kent A, Pasteris JD, Yoon Y, Thomopoulos S. The tendon-to-bone transition of the rotator cuff: a preliminary Ra-man spectroscopic study documenting the gradual mineraliza-tion across the insertion in rat tissue samples. Appl Spectrosc. 2008;62(12):1285-94.
22. Adams JE, Zobitz ME, Reach JS Jr, An KN, Steinmann SP. Rota-tor cuff repair using an acellular dermal matrix graft: an in vivo study in a canine model. Arthroscopy. 2006;22(7):700-9.
23. MacGillivray JD, Fealy S, Terry MA, Koh JL, Nixon AJ, Warren
RF. Biomechanical evaluation of a rotator cuff defect model augmented with a bioresorbable scaffold in goats. J Shoulder Elbow Surg. 2006;15(5):639-44.
24. Sonnabend DH, Howlett CR, Young AA. Histological evalu-ation of repair of the rotator cuff in a primate model. J Bone Joint Surg Br. 2010;92(4):586-94.
25. Soslowsky LJ, Thomopoulos S, Esmail A, et al. Rotator cuff tendinosis in an animal model: role of extrinsic and overuse factors. Ann Biomed Eng. 2002;30(8):1057-63.
26. Trudel G, Ryan SE, Rakhra K, Uhthoff HK. Extra- and intramus-cular fat accumulation early after rabbit supraspinatus tendon division: depiction with CT. Radiology. 2010;255(2):434-41.
27. Gupta R, Lee TQ. Contributions of the different rabbit models to our understanding of rotator cuff pathology. J Shoulder El-bow Surg. 2007;16(5 Suppl):S149-57.
28. Derwin KA, Baker AR, Codsi MJ, Iannotti JP. Assessment of the canine model of rotator cuff injury and repair. J Shoulder El-bow Surg. 2007;16(5 Suppl):S140-8.
29. Longo UG, Forriol F, Campi S, Maffulli N, Denaro V. Animal models for translational research on shoulder pathologies: from bench to bedside. Sports Med Arthrosc. 2011;19(3):184-93.
30. Schneeberger AG, Nyffeler RW, Gerber C. Structural changes of the rotator cuff caused by experimental subacromial im-pingement in the rat. J Shoulder Elbow Surg. 1998;7(4):375-80.
31. Soslowsky LJ, Thomopoulos S, Tun S, et al. Neer Award 1999. Overuse activity injures the supraspinatus tendon in an animal model: a histologic and biomechanical study. J Shoulder Elbow Surg. 2000;9(2):79-84.
32. Zhang S, Li H, Tao H, et al. Delayed early passive motion is harmless to shoulder rotator cuff healing in a rabbit model. Am J Sports Med. 2013;41(8):1885-92.
33. Kim HM, Galatz LM, Lim C, Havlioglu N, Thomopoulos S. The effect of tear size and nerve injury on rotator cuff muscle fatty degeneration in a rodent animal model. J Shoulder Elbow Surg. 2012;21(7):847-58.
34. Ostrander RV 3rd, McKinney BI. Evaluation of footprint con-tact area and pressure using a triple-row modification of the suture-bridge technique for rotator cuff repair. J Shoulder El-bow Surg. 2012;21(10):1406-12.
35. Bisbinas I, Magnissalis E, Gigis I, Beslikas T, Hatzokos I, Christo-foridis I. Rotator cuff repair: a biomechanical ex vivo ovine study. Proc Inst Mech Eng H. 2013;227(5):560-70.
36. Quigley RJ, Gupta A, Oh JH, et al. Biomechanical comparison of single-row, double-row, and transosseous-equivalent repair techniques after healing in an animal rotator cuff tear model. J Orthop Res. 2013;31(8):1254-60.
37. Levy DM, Saifi C, Perri JL, Zhang R, Gardner TR, Ahmad CS. Rotator cuff repair augmentation with local autogenous bone marrow via humeral cannulation in a rat model. J Shoulder

90 www.cisejournal.org
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014
Elbow Surg. 2013;22(9):1256-64. 38. Reuther KE, Thomas SJ, Tucker JJ, et al. Disruption of the
anterior-posterior rotator cuff force balance alters joint func-tion and leads to joint damage in a rat model. J Orthop Res. 2014;32(5):638-44.
39. Joshi SK, Liu X, Samagh SP, et al. mTOR regulates fatty infiltra-tion through SREBP-1 and PPARγ after a combined massive ro-tator cuff tear and suprascapular nerve injury in rats. J Orthop Res. 2013;31(5):724-30.
40. Loeffler BJ, Scannell BP, Peindl RD, et al. Cell-based tissue en-gineering augments tendon-to-bone healing in a rat supraspi-natus model. J Orthop Res. 2013;31(3):407-12.
41. Uezono K, Ide J, Tokunaga T, Sakamoto H, Okamoto N, Mizuta H. Effect of immobilization on rotator cuff reconstruc-tion with acellular dermal matrix grafts in an animal model. J Shoulder Elbow Surg. 2013;22(9):1290-7.
42. Peltz CD, Hsu JE, Zgonis MH, Trasolini NA, Glaser DL, So-slowsky LJ. Intra-articular changes precede extra-articular changes in the biceps tendon after rotator cuff tears in a rat model. J Shoulder Elbow Surg. 2012;21(7):873-81.
43. Buchmann S, Sandmann GH, Walz L, et al. Refixation of the supraspinatus tendon in a rat model--influence of continuous growth factor application on tendon structure. J Orthop Res. 2013;31(2):300-5.
44. Yokoya S, Mochizuki Y, Natsu K, Omae H, Nagata Y, Ochi M. Rotator cuff regeneration using a bioabsorbable material with
bone marrow-derived mesenchymal stem cells in a rabbit model. Am J Sports Med. 2012;40(6):1259-68.
45. Liu X, Joshi SK, Samagh SP, et al. Evaluation of Akt/mTOR ac-tivity in muscle atrophy after rotator cuff tears in a rat model. J Orthop Res. 2012;30(9):1440-6.
46. Cadet ER, Vorys GC, Rahman R, et al. Improving bone density at the rotator cuff footprint increases supraspinatus tendon fail-ure stress in a rat model. J Orthop Res. 2010;28(3):308-14.
47. Samagh SP, Kramer EJ, Melkus G, et al. MRI quantification of fatty infiltration and muscle atrophy in a mouse model of rota-tor cuff tears. J Orthop Res. 2013;31(3):421-6.
48. Reuther KE, Sarver JJ, Schultz SM, et al. Glenoid cartilage mechanical properties decrease after rotator cuff tears in a rat model. J Orthop Res. 2012;30(9):1435-9.
49. Mannava S, Plate JF, Whitlock PW, et al. Evaluation of in vivo rotator cuff muscle function after acute and chronic detach-ment of the supraspinatus tendon: an experimental study in an animal model. J Bone Joint Surg Am. 2011;93(18):1702-11.
50. Inui A, Kokubu T, Mifune Y, et al. Regeneration of rotator cuff tear using electrospun poly(d,l-Lactide-Co-Glycolide) scaffolds in a rabbit model. Arthroscopy. 2012;28(12):1790-9.
51. Baums MH, Spahn G, Buchhorn GH, Schultz W, Hofmann L, Klinger HM. Biomechanical and magnetic resonance imaging evaluation of a single- and double-row rotator cuff repair in an in vivo sheep model. Arthroscopy. 2012;28(6):769-77.

Partial Thickness Rotator Cuff Tears
Sang-Jin Shin, Myeong-Jae Seo
Department of Orthopaedic Surgery, Ewha Womans University School of Medicine, Seoul, Korea
Partial-thickness rotator cuff tear (PTRCT) is not single disease entity but one phase of disease spectrum. Symptoms of PTRCT vary from being asymptomatic to severe pain leading to deterioration in quality of life. Pathogenesis of degenerative PTRCT is multifactorial. Whereas articular sided PTRCT is usually caused by internal causes, both internal and external causes have important role in bursal sided PTRCT. A detailed history, clinical examination and magnetic resonance angiography are used in the diagnosis of PTRCT. Treatment of PTRCT is chosen based on age, demands of patients, causes and depth of tear. In most patients, non-operative treatment should be initi-ated. Whereas debridement can be done for less than 6 mm of articular sided PTRCT and in less than 3 mm of bursal sided PTRCT, re-pair techniques should be considered for higher grade PTRCT than that. Although the effect of acromioplasty is not clear, acromioplasty may be performed when the extrinsic causes appear to be the cause of tear. Either transtendon repair technique or repair after tear completion provided satisfactory clinical outcomes in treatment of articular sided PTRCT.(Clin Shoulder Elb 2014;17(2):91-100)
Key Words: Rotator cuff; Partial thickness tear; Articular side; Bursal side
Introduction
Partial-thickness rotator cuff tear (PTRCT) have been recog-nized as an asymptomatic consequence of the ageing process.1,2) However, after recent advances in basic science, imaging mo-dalities and treatment techniques, PTRCT is now recognized as a part of disease spectrum and not as a single entity. This spectrum of rotator cuff disease ranges from rotator cuff edema, inflam-matory tendinitis and rotator cuff fibrosis progressing to partial or full-thickness tears. PTRCT is not rare and its prevalence is even expected to increase with a rise in geriatric population.1,3) In this review the diagnosis, classification, treatment options, surgical indications, surgical techniques and its outcomes with regard to PTRCT will be discussed.
Incidence
The reported incidence of PTRCT is 13−32% in cadaveric studies.4,5) An in vivo study using magnetic resonance imaging (MRI) in asymptomatic population reported the overall preva-
lence of PTRCT as 20% and that of PTRCT in the patients aged older than 60 years as 26%.3) Ultrasonography studies demon-strated that the prevalence of PTRCT was 17% in the asymp-tomatic volunteers, and 7% in the symptomatic patients.6) The prevalence of articular sided tears is 2−3 times more than that of bursal side.4) Although the incidence of PTRCT increases with age,7) it may not be necessarily associated with symptoms.
Natural History
The natural history of PRTCT has not been clearly identi-fied; several studies have reported tear progression with time and age.8,9) In a study on progression of tears on arthroscopic examination in 40 patients, the tear size increased in 4 (10%) patients, progressed to the full-thickness tear in 11 (28%) pa-tients, reduced in 4 (10%) patients and the tear healed in 4 (10%) patients.9) Even though a few studies have reported the potential for spontaneous healing of torn cuff tendons, most studies have shown that the torn tendon is less likely to heal spontaneous-ly.10-13) In histologic studies no evidence of active healing of torn
CiSEClinics in Shoulder and Elbow
Copyright © 2014 Korean Shoulder and Elbow Society. All Rights Reserved.This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
pISSN 1226-9344eISSN 2288-8721
REVIEW ARTICLE
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014http://dx.doi.org/10.5397/cise.2014.17.2.91
Received May 9, 2014. Revised June 10, 2014. Accepted June 11, 2014.
Correspondence to: Sang-Jin ShinDepartment of Orthopaedic Surgery, Ewha Womans University Mokdong Hospital, 1072 Anyangcheon-ro, Yangcheon-gu, Seoul 158-710, KoreaTel: +82-2-2650-5143, Fax: +82-2-2642-0349, E-mail: [email protected]
Financial support: None. Conflict of interests: None.

92 www.cisejournal.org
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014
end of the tendon and a rounded proximal stump, retracted and avascular appearance of cuff stump was reported.14) All these findings supported limited potential for spontaneous healing of PTRCT. In an immunohistochemical study, some chemical me-diators such as interleukin-1b, cathepsin D, and matrix metal-loprotease-1 were found to be increased with the macrophages and multinucleated giant cells present in the injured supraspina-tus tendon and reparatory granulation tissue.12) They may con-tribute to the rotator cuff injury by weakening the insertion site.
Classification
PTRCT can be classified into articular sided tear (Fig. 1A), bursal sided tear (Fig. 1B), intratendinous tear and combined type tear. Ellman15) further classified PTRCT based on the loca-tion of tear (A: articular, B: bursal, C: intratendinous) and on the depth of tear (grade 1: <3 mm, grade 2: 3−6 mm, grade 3: >6 mm) (Table 1). Synder et al16) coined the term “partial articular sided tendon avulsion” for PTRCT on the articular sided. He also described a classification of partial tears based on the location of the tear (articular, bursal, total) and severity of the tear (grade 1−4). Conway17) described articular sided partial tear accompa-nying intratendinous tear as partial articular tears with intraten-dinous extension. Recently, Habermeyer et al.18) pointed out the limitation of the classification of Snyder et al.16) and Ellman15) and proposed a new classification based on 2-dimensional sagittal and longitudinal extension of the tear.
Pathogenesis
The injury mechanisms of articular sided and bursal sided PTRCT are different because of the difference in vascularity, biomechanical and histological characteristics. A critical zone of avascularity close to the insertion of the supraspinatus tendon into the humeral head19) and its histological correlation with the site of rotator cuff degeneration has been described.20) This sparse vascular distribution was found mainly on the articu-
lar sided which was a significant factor in the pathogenesis of degenerative rotator cuff tears. A cadaveric study showed the histological and biomechanical differences between bursal sided and articular sided tendon layer.21) This difference could make articular sided tendon layer more vulnerable to tear than bursal sided tendon layer.
Etiology of PTRCT can be classified into intrinsic, extrinsic and traumatic causes. Intrinsic causes include age related meta-bolic and vascular changes which can lead to degenerative tear, and differential shear stress which leads to intratendinous tears especially in the throwing arthlete.22,23) Extrinsic causes include subacromial impingement, inflammatory bursitis and internal impingement. A spur of undersurface of acromion was always associated with a rotator cuff tear; however, the converse was not always true.22) In an animal model, the undersurface of the acromion of test group of rats was thickened with plate like bony transplants to cause impingement. As compared to control group which did not have any rotator cuff tears, the test group demon-strated bursal sided tears. This demonstrates the role of external source of impingement as a cause of bursal sided tears.24) Al-though the pathogenesis of rotator cuff tear is controversial, it is likely that both intrinsic and extrinsic causes are associated with the pathogenesis of PTRCT.
Diagnosis
Clinical PresentationThe symptoms of PTRCT are variable depending on con-
comitant disease. The most common symptoms are pain and
Table 1. Ellman’s Classification of Partial-thickness Rotator Cuff Tear
Location Grade
A: Articular surface 1: <3 mm deep
B: Bursal surface 2: 3–6 mm deep
C: Interstitial 3: >6 mm deep
Fig. 1. (A) Arthroscopic view of articular sided partial-thickness rotator cuff tear. (B) Arthroscopic view of bursal sided partial-thickness rotator cuff tear.

Partial Thickness Rotator Cuff TearsSang-Jin Shin and Myeong-Jae Seo
www.cisejournal.org 93
stiffness of the shoulder joint. Pain is usually severe at night and aggravated by overhead elevation of the arm. Patients may com-plain of weakness of the upper arm. In a previous study, 74% of the patients with PTRCT felt more than moderate pain, whereas only 50% of those with the full thickness rotator cuff tear (FTRCT) did.4) The level of substance P which is a pain mediator in the subacromial bursa was higher in PTRCT patients than in the FTRCT patients.25) Bursal sided PTRCT are more painful than articular sided partial tears due to more inflammatory mediator like interleukin-1b, interleukin-1 receptor agonists in subacro-mial space than that in the intra articular space.
PTRCT is more likely to lead to stiffness of affected shoulder than FTRCT. The tear of 1/3 or 2/3 of the thickness of supraspi-natus tendon had little effect on force transmission and hence usually does not present with weakness in abduction.26) A partial tear of rotator cuff tendon can lead to localized strain concentra-tion in the adjacent area of tendon.27) This strain concentration may be cause of the more severe pain in PTRCT. In PTRCT, although, mechanical force transmission may be preserved, ten-sion concentration on the normal fiber during abduction may contribute to shoulder pain and stiffenss.28)
Physical ExaminationThe clinical diagnosis of PTRCT is based on an integrated as-
sessment based on detailed history taking, physical examination and the radiologic results. Visual inspection of muscles around shoulder joint is performed to detect muscle atrophy or asym-metry as compared to unaffected side. Range of shoulder mo-tion including active and passive motion, and muscle power during forward flexion, abduction, adduction, external rotation and internal rotation should be examined. Tests like sulcus sign, apprehension test and relocation test are useful for evaluation of accompanying shoulder instability. Biceps tendon lesions which can be associated with rotator cuff lesion should be examined with tests for biceps lesion like O’Brien test. Cervical spondylosis is an important differential diagnosis and the tenderness, range
of motion of cervical spine should be examined. Provocative tests such as Spurling maneuver are very useful for discrimina-tion. After ruling out other differential diagnoses, the symptoms which arise from FTRCT are evaluated. The symptoms of rotator cuff tear can be divided into the inflammatory symptoms and the mechanical symptoms. Inflammatory symptoms include pain, painful arc and impingement sign. Mechanical symptoms and signs include muscle power weakness, muscle atrophy, crepitus and drop arm sign. The final differential diagnosis of PTRCT based on the physical examination is difficult, because the symptoms of the PTRCT are atypical and similar to those of impingement syndrome without rotator cuff tear and small FTRCT. For reasons mentioned above, PTRCT was identified by chance when arthroscopic surgery was performed in patients with impingement syndrome.
Radiologic EvaluationA variety of radiologic modalities are used to diagnose PTRCT
currently. In the past, arthrography and bursography have been used as the primary imaging modalities for rotator cuff tear. Due to their low sensitivity (15−83%) and specificity (25−67%) and availability of better methods these modalities are rarely used now.29-31)
Ultrasonography and MRI have become the gold standard for diagnosis of rotator cuff tear. A mixed hyperechoic/hypoechoic focus in the supraspinatus tendon has a sensitivity of 93%, speci-ficity of 94%, positive predictive value of 82%, and negative pre-dictive value of 98% of diagnosing a PTRCT.32) A ‘focal heteroge-neous hypoechogenicity’ has a sensitivity of 95%, specificity of 90%, positive predictive value of 97%, negative predictive value of 94%, and accuracy of 94% of detecting a PTRCT.33) The limi-tation of ultrasonography is the accuracy rate depends on the experience and the skill of the examiner in spite of its relatively low cost, good patient tolerance and reported high accuracy rate.
PTRCT on the MRI has increased signal intensity and ab-
Fig. 2. (A) Articular sided partial-thickness rotator cuff tear on magnetic resonance imaging (MRI) scan. (B) Interstitial partial-thickness rotator cuff tear on MRI scan. (C) Bursal sided partial-thickness rotator cuff tear on MRI scan.

94 www.cisejournal.org
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014
normal morphology without discontinuity on T1 images and increased signal intensity with focal defect on T2 images (Fig. 2).7) PTRCT can be differentiated from tendinosis based on MRI im-age because tendinosis showed high signal intensity on T1 and Proton images but low signal intensity on T2 image. Ultrasonog-raphy and MRI have been shown to have comparable accuracy for identifying and measuring the size of PTRCT and FTRCT.34)
MRI and ultrasonography have been reported to be less useful for PTRCT than for FTRCT.35) The accuracy of MRI and ultra-sonography for PTRCT is 73% and 70% respectively, whereas that for FTRCT it was 95% and 88% respectively. The authors emphasized that in the hands of well trained and experienced orthopedic surgeon utility of ultrasonography is comparable to MRI. MRI helps to evaluate the remainder of the shoulder anat-omy however is relatively costly. With the introduction of the magnetic resonance angiography (MRA), a recent study reported sensitivity of 84%, specificity of 96%, positive predictive value of 93%, and overall accuracy of 91% for diagnosis of PTRCT.36) MRA is the most sensitive and specific technique for diagnosing PTRCT. Ultrasonography and MRI are comparable in both sensi-tivity and specificity.37)
Treatment
Non-operative TreatmentThe treatment options depend on the causes of tear, the
location of tear and the symptoms and activities of patients. Management is initiated with rest, activity modification and non-steroidal ant-inflammatory drugs. Pain relief due to reduction in
inflammation is expected with this treatment. For patient with stiff shoulder, after pain relief, physical therapy and exercises to recover the range of motion should be initiated. Subacromial or intra-articular corticosteroid injections have certain benefits for pain relief. As patients recover range of motion, strengthening exercises for periscapular muscles should be initiated. There are no standardized, long-term follow up studies evaluating the clini-cal outcomes of patients with PTRCT treated non-operatively. Although available studies indicate that PTRCT progress with time, it is possible for patients to improve symptomatically with non-operative treatment. Non-operative treatment can usually be continued for more than 6 months with satisfactory clinical outcomes. However, non-operative treatment is less effective in treatment of bursal sided PTRCT.29,38)
Operative TreatmentWith symptom aggravation or failure of conservative treat-
ment for a reasonable period of time, operative treatment can be considered. Although the timing of operation is variable it is usually after trial of non-operative treatment for 3−6 months and no more than 1 year. Operative treatment depends on the severity of symptoms, degree of improvement with non-oper-ative treatment and the demands of patients. Various options include debridement, acromioplasty, repair and combination of these techniques using arthroscope or mini incision. Choice of treatment is determined based on the location and the depth of tear (Fig. 3). However, there are times when visual inspec-tion of the field does not reveal the exact site of PTRCT. Fukuda color test can be used during mini open approach.39) It is done
Fig. 3. Treatment algorithm for partial-thickness rotator cuff tear.

Partial Thickness Rotator Cuff TearsSang-Jin Shin and Myeong-Jae Seo
www.cisejournal.org 95
by checking for dyed cuff tendon region after injecting indigo carmine or the methylene blue into the glenohumeral joint and taking the shoulder through its range of movement. When using arthroscopic approach, suture marking technique and bubble sign are used. The bubble sign is demonstrated by directing nor-mal saline into the suspicious lesion. In the operative field, the tear size can be measured using a variety of tools like the probe, tip of shaver and special ruler for arthroscopic approach. The tear should be debrided first with a shaver to define the extent of the tear. For bursal sided tear, the extent is determined from the edge of intact margins in the anteroposterior plane and from the footprint to the torn edge in the coronal plane. For the artic-ular sided tear, the extent is measured from lateral margin of the articular surface to the torn edge of the tendon and the distance between the torn tendon edges in the anteroposterior plane.
DebridementBursal or articular sided PTRCT of grade 1 and articular sided
PTRCT of grade 2 can be treated by debridement with or with-out acromioplasty. Debridement stimulates healing as it not only removes inflammatory cells and mediators, but also decreases the mechanical irritation in the subacromial space and glenohu-meral joint. In addition, it helps to evaluate the exact depth of the tear site to plan additional procedures if needed. In patients with PTRCT treated by debridement, 89% had good or excellent outcomes at minimum 5 years follow up.40) In another study41) addressing elite overhead throwers, most of patients could re-turn to competitive professional pitching after debridement. However, 55% of patients could return to their previous level of competitive sports.
AcromioplastyWhen clinical signs or subacromial osteophytes suggestive of
subacromial impingement are found after sufficient bursectomy, acromioplasty can be done for bursal sided PTRCT. The purpose of this technique is to remove osteophytes, flatten the acromion undersurface and clear the subacromial space for the rotator cuff to glide. Satisfactory results in 15 out of 16 patients with bursal sided PTRCT treated by acromioplasty in 5 years follow up have been reported.42) The exact role of acromioplasty is not clear as no significant difference in outcomes have been described be-tween arthroscopic bursectomy alone and arthroscopic bursec-tomy with acromioplasty.43)
Acromioplasty with DebridementA study comparing the bursectomy alone with bursectomy
and acromioplasty in PTRCT patient described satisfactory re-sults in 84% patients with no significant difference in results be-tween the two procedures.16) Weber44) presented results of study comparing open acromioplasty and repair with arthroscopic acromioplasty and debridement for 65 patients with grade 3
of PTRCT. At 7 years follow, the mean UCLA scores in articu-lar sided PTRCT was 31.6 for open repair group and 22.7 for arthroscopic debridement group, and for bursal sided PTRCT it was 33.0 and 13.6 respectively. It was concluded that grade 3 PTRCT should be treated with arthroscopic acromioplasty and repair. Park et al.45) compared results of 13 patients with bursal sided PTRCT with that of 24 patients with articular sided PTRCT treated with acromioplasty and debridement. Although outcomes were better in patients with bursal sided PTRCT, there were no significant difference between groups, and both groups showed excellent results at 6 months postoperatively. Patients with grade 2 bursal sided PTRCT have shown higher failure rates (38%) than articular sided grade 2 of PTRCT (5%) when treated with acromioplasty and debridement at minimum 2 years fol-low up.46) The outcomes of acromioplasty and debridement for athletes less than 40 years old are related with the cause of the tear and symptom period. Whereas, acute traumatic PTRCT of athletes showed good results in 86% patients, chronic PTRCT of athletes showed good results in only 66% patients.47)
On the basis of the literature, grade 1 and grade 2 articular sided PTRCT can be treated by arthroscopic debridement alone, whereas grade 3 PTRCT should be repaired. For bursal sided PTRCT, only grade 1 PTRCT can be treated by debridement with or without acromioplasty, whereas grade 2 and grade 3 bursal sided tear should be repaired. As the effects of acromio-plasty alone are not clear, it can be performed with debridement based on the morphology of acromion.
Repair
Repair of PTRCT is dependent on the depth of tear. Tear depth more than 50% of entire tendon thickness, grade 3 articu-lar sided PTRCT and more than grade 2 of bursal sided PTRCT is considered as indications for repair. The indications for tear completion and repair technique are when the tear is almost through the complete tendon thickness with only a small rem-nant of tissue remaining after debridement and there is a tear on the corresponding side of the tear, that is, when a bursal surface tear is accompanied by an articular surface tear in the same ten-don at the same location and vice versa. When the other side of tendon is intact and tendon viability at the tear site is relatively favorable, the transtendon repair technique for articular sided PTRCT48) or small-window technique49) for bursal-sided PTRCT are used.
Bursal Sided PTRCTTraditionally for bursal sided PTRCT, tear completion and re-
pair technique had been used. This technique in PTRCT showed significant improvement in the VAS and American Shoulder and Elbow Surgeons (ASES) scores in PTRCT.47) The functional out-comes of tear completion and repair technique for bursal sided

96 www.cisejournal.org
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014
PTRCT is comparable or superior when compared with that of articular sided PTRCT.50) However, tear completion and repair technique damages the normal rotator cuff tissue, can alter the normal anatomy of footprint and cause tension mismatch. Yoo et al.49) described small-window technique to help preserve the remnant rotator cuff tendon with minimum tissue damage for bursal sided PTRCT.
Surgical techniqueAny repair technique for bursal-sided PTRCT (Fig. 4A) is to
preserve the remaining tendon on the articular sided. After a conservative debridement, the flaps of torn tendon are defined. A small window is made in the articular sided tendon remnant. A suture anchor is inserted on the medial margin of the foot-print. Sutures are then passed through the anterior and posterior flaps of the torn tendon remnant using a direct suture passing in-strument. If the central portion of the torn portion is inadequate or does not come to the footprint, the suture is passed to include the intact tendon through the small window. This is done by
passing the suture passing instrument through the same window. The sutures are then tied sequentially to reduce the torn edge to the footprint. Then lateral suture anchors are inserted to com-plete suture bridge technique (Fig. 4B).
Articular Sided PTRCT
1. Tear completion and repair technique in articular sided PTRCTThe tear completion and repair technique has shown satis-
factory clinical outcomes and high levels of patient satisfaction. Good functional outcome and healing rates after arthroscopic repair using tear completion and repair technique for 41 patients with grade 3 PTRCT have been reported. At the final follow up, healed rotator cuff repair was seen in 88% patients on ultraso-nography and 93% patients were satisfied with the results. The authors described that this technique allows better access to the tendon footprint and the removal of degenerative tissues.47,51) However, this technique sacrifices the intact bursal sided rotator
Fig. 4. (A) Bursal sided partial-thickness rotator cuff tear (PTRCT) as seen through the posterior portal. (B) Bursal sided PTRCT repaired by suture bridge technique.
Fig. 5. Various methods to measure the depth of articular sided partial-thickness rotator cuff tear during the arthroscpic procedure. (A) Shaver tip. (B) Calibrated probe. (C) 90o angled ruler.

Partial Thickness Rotator Cuff TearsSang-Jin Shin and Myeong-Jae Seo
www.cisejournal.org 97
cuff tendon and has the risks of non-anatomic restoration of the tendon footprint and of changing the normal biomechanics.
Surgical techniqueWhen tear completion and repair technique is used for artic-
ular sided PTRCT, after careful debridement of the tear site, the depth of tear should be identified using a shaver (Fig. 5A), a cali-brated probe (Fig. 5B) or a arthroscopic ruler (Fig. 5C). To locate the corresponding bursal sided cuff, a spinal needle is used to pass a no. 1 polydioxanone (PDS) suture as a marker (Fig. 6A). After changing the position of arthroscope to the subacromial space, the corresponding bursal sided cuff which is marked with PDS suture can be identified. (Fig. 6B). Tear completion is ac-complished using meniscal knife (Fig. 7), shaver or arthroscopic punch. However, preservation of bursal sided tendon as much as possible is important to reduce retear rate. Thereafter con-ventional cuff repair technique using the suture anchor can be
done.
2. Transtendon technique in articular sided PTRCTSome prefer the transtendon repair technique, because using
this technique the intact bursal sided of the tendon is preserved and the rotator cuff footprint is restored more anatomically. Re-cently, a long term study demonstrated significantly better func-tional and clinical outcomes with no complications using this technique.52)
In a prospective study, Shin53) compared clinical outcomes between patients treated using two different techniques and obtained satisfactory functional improvements and pain relief re-gardless of the repair technique. The tear completion and repair technique showed less postoperative morbidity, however tendon integrity after repair is of concern. On the other hand, the trans-tendon repair technique produced good tendon integrity after surgery; however, slower functional recovery was identified. In the transtendon repair technique, the restoration of retracted articular cuff layer on original footprint may cause bunching up of the bursal layer of the cuff and thus result in imbalance in ten-sion. This non-physiologic tension may lead to residual shoulder discomfort54) or shoulder siffness.55) For these reasons, various modifications of transtendon repair techniques have been intro-duced to prevent tendon overstrain.56-59)
Surgical techniqueAfter a conservative debridement the torn cuff edges and
the footprint are defined. The arthroscope is placed in the gle-nohumeral joint through the posterior portal. A spinal needle is inserted percutaneously along the lateral edge of the acromion through the musculotendinous junction of the rotator cuff onto the lateral articular margin of the footprint. The spinal needle acts as a guide to locate the proper position of the suture anchor. Using a small skin incision, a suture anchor is inserted percuta-neously across the rotator cuff tendon to the center of footprint parallel to the path of the spinal needle. If the size of the tear
Fig. 6. (A) To locate the corresponding bursal sided cuff, a spinal needle is used to pass a no. 1 polydioxanone (PDS) suture as a marker. (B) After changing the position of arthroscope to the subacromial space, the corresponding bursal sided cuff which is marked with PDS suture can be identified.
Fig. 7. Tear completion is accomplished using meniscal knife to preserve bur-sal sided tendon as much as possible.

98 www.cisejournal.org
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014
is more than 1.5 cm, then two anchors are usually needed-one anteriorly and the other posteriorly. All the suture limbs are pulled through the anterior portal intra-articularly. A spinal nee-dle is inserted percutaneously medial to the free edge of the torn tendon and a PDS suture is passed through the spinal needle to be retrieved through the anterior portal. Using the shuttle relay technique, the PDS suture is substituted for the suture limb of the suture anchor (Fig. 8A). Then the suture limb of the suture anchor which penetrated the rotator cuff can be seen outside of the skin through the puncture wound of the spinal needle. The same procedure can be repeated for the remaining suture limbs of the suture anchor from posterior to anterior. After changing the position of arthroscope to the subacromial space, all suture limbs in the subacromial space are retrieved through the lateral portal and tied on the bursal sided of the rotator cuff tendon to compress the torn edge of the tendon on the footprint (Fig. 8B).
Conclusions
PTRCT is not single disease entity but one phase of disease spectrum. Symptoms of PTRCT vary from being asymptomatic to severe pain leading to deterioration in quality of life. Patho-genesis of degenerative PTRCT is multifactorial. A detailed his-tory, clinical examination and MR arthrography are used in the diagnosis of PTRCT. Treatment of PTRCT is chosen based on age, demands of patients, causes and depth of tear. In most patients, non-operative treatment should be initiated. Whereas debride-ment can be done for less than 6 mm of articular sided PTRCT and in less than 3 mm of bursal sided PTRCT, repair techniques are considered for higher grade PTRCT and who failed con-servative treatment at least 3 months. Although the effect of acromioplasty is not clear, acromioplasty may be performed when the extrinsic causes appear to be the cause of tear. Either transtendon repair technique or repair after tear completion provides satisfactory clinical outcomes in treatment of articular
sided PTRCT.
References
1. Milgrom C, Schaffler M, Gilbert S, van Holsbeeck M. Rotator-cuff changes in asymptomatic adults. The effect of age, hand dominance and gender. J Bone Joint Surg Br. 1995;77(2):296-8.
2. Meyer AW. Further evidences of attrition in the human body. Am J Anat. 1924;34(1):241-67.
3. Sher JS, Uribe JW, Posada A, Murphy BJ, Zlatkin MB. Abnor-mal findings on magnetic resonance images of asymptomatic shoulders. J Bone Joint Surg Am. 1995;77(1):10-5.
4. Fukuda H. Partial-thickness rotator cuff tears: a modern view on Codman’s classic. J Shoulder Elbow Surg. 2000;9(2):163-8.
5. Löhr JF, Uhthoff HK. Epidemiology and pathophysiology of ro-tator cuff tears. Orthopade. 2007;36(9):788-95.
6. Singisetti K, Hinsche A. Shoulder ultrasonography versus ar-throscopy for the detection of rotator cuff tears: analysis of er-rors. J Orthop Surg (Hong Kong). 2011;19(1):76-9.
7. Finnan RP, Crosby LA. Partial-thickness rotator cuff tears. J Shoulder Elbow Surg. 2010;19(4):609-16.
8. Hamada K, Tomonaga A, Gotoh M, Yamakawa H, Fukuda H. Intrinsic healing capacity and tearing process of torn supraspi-natus tendons: in situ hybridization study of alpha 1 (I) procol-lagen mRNA. J Orthop Res. 1997;15(1):24-32.
9. Yamanaka K, Matsumoto T. The joint side tear of the rotator cuff. A followup study by arthrography. Clin Orthop Relat Res. 1994;(304):68-73.
10. Hirose K, Kondo S, Choi HR, Mishima S, Iwata H, Ishiguro N. Spontaneous healing process of a supraspinatus tendon tear in rabbits. Arch Orthop Trauma Surg. 2004;124(6):374-7.
11. Carpenter JE, Thomopoulos S, Flanagan CL, DeBano CM, Soslowsky LJ. Rotator cuff defect healing: a biomechanical and histologic analysis in an animal model. J Shoulder Elbow Surg.
Fig. 8. Transtendon technique in articular sided partial-thickness rotator cuff tear. (A) The limb of the polydioxanone (PDS) suture which passed medial to the free edge of the torn tendon is pulled through the anterior portal. In subacromial space, the limb of the PDS suture penetrated the intact bursal sided cuff layer. The four suture limbs of the suture anchor substituted the PDS sutures by shuttle relay technique consecutively. (B) All the su-ture limbs of the suture anchor were tied on the bursal sided cuff surface.

Partial Thickness Rotator Cuff TearsSang-Jin Shin and Myeong-Jae Seo
www.cisejournal.org 99
1998;7(6):599-605.12. Gotoh M, Hamada K, Yamakawa H, Tomonaga A, Inoue A,
Fukuda H. Significance of granulation tissue in torn supraspi-natus insertions: an immunohistochemical study with antibod-ies against interleukin-1 beta, cathepsin D, and matrix metal-loprotease-1. J Orthop Res. 1997;15(1):33-9.
13. Fukuda H, Hamada K, Yamanaka K. Pathology and pathogen-esis of bursal-side rotator cuff tears viewed from en bloc histo-logic sections. Clin Orthop Relat Res. 1990;(254):75-80.
14. Wolff AB, Sethi P, Sutton KM, Covey AS, Magit DP, Medvecky M. Partial-thickness rotator cuff tears. J Am Acad Orthop Surg. 2006;14(13):715-25.
15. Ellman H. Diagnosis and treatment of incomplete rotator cuff tears. Clin Orthop Relat Res. 1990;(254):64-74.
16. Snyder SJ, Pachelli AF, Del Pizzo W, Friedman MJ, Ferkel RD, Pattee G. Partial thickness rotator cuff tears: results of ar-throscopic treatment. Arthroscopy. 1991;7(1):1-7.
17. Conway JE. Arthroscopic repair of partial-thickness rotator cuff tears and SLAP lesions in professional baseball players. Orthop Clin North Am. 2001;32(3):443-56.
18. Habermeyer P, Krieter C, Tang KL, Lichtenberg S, Magosch P. A new arthroscopic classification of articular-sided supraspinatus footprint lesions: a prospective comparison with Snyder’s and Ellman’s classification. J Shoulder Elbow Surg. 2008;17(6):909-13.
19. Lohr JF, Uhthoff HK. The microvascular pattern of the supra-spinatus tendon. Clin Orthop Relat Res. 1990;(254):35-8.
20. Rathbun JB, Macnab I. The microvascular pattern of the rota-tor cuff. J Bone Joint Surg Br. 1970;52(3):540-53.
21. Nakajima T, Rokuuma N, Hamada K, Tomatsu T, Fukuda H. Histologic and biomechanical characteristics of the supraspina-tus tendon: Reference to rotator cuff tearing. J Shoulder Elbow Surg. 1994;3(2):79-87.
22. Ozaki J, Fujimoto S, Nakagawa Y, Masuhara K, Tamai S. Tears of the rotator cuff of the shoulder associated with pathologi-cal changes in the acromion. A study in cadavera. J Bone Joint Surg Am. 1988;70(8):1224-30.
23. Mazoué CG, Andrews JR. Repair of full-thickness rotator cuff tears in professional baseball players. Am J Sports Med. 2006;34(2):182-9.
24. Schneeberger AG, Nyffeler RW, Gerber C. Structural changes of the rotator cuff caused by experimental subacromial im-pingement in the rat. J Shoulder Elbow Surg. 1998;7(4):375-80.
25. Gotoh M, Hamada K, Yamakawa H, Inoue A, Fukuda H. In-creased substance P in subacromial bursa and shoulder pain in rotator cuff diseases. J Orthop Res. 1998;16(5):618-21.
26. Halder AM, O’Driscoll SW, Heers G, et al. Biomechanical comparison of effects of supraspinatus tendon detachments, tendon defects, and muscle retractions. J Bone Joint Surg Am. 2002;84-A(5):780-5.
27. Frisch KE, Marcu D, Baer G, Thelen DG, Vanderby Jr R. The influence of partial and full thickness tears on infraspinatus tendon strain patterns. J Biomech Eng. 2014. In press, avail-able on doi: 10.1115/1.4026643.
28. Bey MJ, Ramsey ML, Soslowsky LJ. Intratendinous strain fields of the supraspinatus tendon: effect of a surgically cre-ated articular-surface rotator cuff tear. J Shoulder Elbow Surg. 2002;11(6):562-9.
29. Fukuda H, Mikasa M, Yamanaka K. Incomplete thickness rota-tor cuff tears diagnosed by subacromial bursography. Clin Or-thop Relat Res. 1987;(223):51-8.
30. Gartsman GM, Milne JC. Articular surface partial-thickness ro-tator cuff tears. J Shoulder Elbow Surg. 1995;4(6):409-15.
31. Itoi E, Tabata S. Incomplete rotator cuff tears. Results of opera-tive treatment. Clin Orthop Relat Res. 1992;(284):128-35.
32. van Holsbeeck MT, Kolowich PA, Eyler WR, et al. US depic-tion of partial-thickness tear of the rotator cuff. Radiology. 1995;197(2):443-6.
33. Yen CH, Chiou HJ, Chou YH, et al. Six surgery-correlated sonographic signs for rotator cuff tears: emphasis on partial-thickness tear. Clin Imaging. 2004;28(1):69-76.
34. Teefey SA, Rubin DA, Middleton WD, Hildebolt CF, Leibold RA, Yamaguchi K. Detection and quantification of rotator cuff tears. Comparison of ultrasonographic, magnetic resonance imaging, and arthroscopic findings in seventy-one consecutive cases. J Bone Joint Surg Am. 2004;86-A(4):708-16.
35. Iannotti JP, Ciccone J, Buss DD, et al. Accuracy of office-based ultrasonography of the shoulder for the diagnosis of rotator cuff tears. J Bone Joint Surg Am. 2005;87(6):1305-11.
36. Meister K, Thesing J, Montgomery WJ, Indelicato PA, Walczak S, Fontenot W. MR arthrography of partial thickness tears of the undersurface of the rotator cuff: an arthroscopic correla-tion. Skeletal Radiol. 2004;33(3):136-41.
37. de Jesus JO, Parker L, Frangos AJ, Nazarian LN. Accuracy of MRI, MR arthrography, and ultrasound in the diagnosis of rotator cuff tears: a meta-analysis. AJR Am J Roentgenol. 2009;192(6):1701-7.
38. Hawkins RH, Dunlop R. Nonoperative treatment of rotator cuff tears. Clin Orthop Relat Res. 1995;(321):178-88.
39. Fukuda H, Mikasa M, Ogawa K, Yamanaka K, Hamada K. “The color test”: An intraoperative staining test for joint-side rotator cuff tearing and its extension. J Shoulder Elbow Surg. 1992;1(2):86-90.
40. Budoff JE, Nirschl RP, Guidi EJ. Débridement of partial-thick-ness tears of the rotator cuff without acromioplasty. Long-term follow-up and review of the literature. J Bone Joint Surg Am. 1998;80(5):733-48.
41. Reynolds SB, Dugas JR, Cain EL, McMichael CS, Andrews JR. Débridement of small partial-thickness rotator cuff tears in elite overhead throwers. Clin Orthop Relat Res. 2008;466(3):614-21.

100 www.cisejournal.org
Clinics in Shoulder and Elbow Vol. 17, No. 2, June, 2014
42. Neer CS 2nd. Anterior acromioplasty for the chronic impinge-ment syndrome in the shoulder: a preliminary report. J Bone Joint Surg Am. 1972;54(1):41-50.
43. Donigan JA, Wolf BR. Arthroscopic subacromial decompres-sion: acromioplasty versus bursectomy alone--does it really matter? A systematic review. Iowa Orthop J. 2011;31:121-6.
44. Weber SC. Arthroscopic debridement and acromioplasty versus mini-open repair in the treatment of significant partial-thickness rotator cuff tears. Arthroscopy. 1999;15(2):126-31.
45. Park JY, Yoo MJ, Kim MH. Comparison of surgical outcome between bursal and articular partial thickness rotator cuff tears. Orthopedics. 2003;26(4):387-90; discussion 90.
46. Cordasco FA, Backer M, Craig EV, Klein D, Warren RF. The partial-thickness rotator cuff tear: is acromioplasty without re-pair sufficient? Am J Sports Med. 2002;30(2):257-60.
47. Kamath G, Galatz LM, Keener JD, Teefey S, Middleton W, Yamaguchi K. Tendon integrity and functional outcome after arthroscopic repair of high-grade partial-thickness supraspina-tus tears. J Bone Joint Surg Am. 2009;91(5):1055-62.
48. Lo IK, Burkhart SS. Transtendon arthroscopic repair of partial-thickness, articular surface tears of the rotator cuff. Arthros-copy. 2004;20(2):214-20.
49. Yoo JC, Ahn JH, Lee SH, Kim JH. Arthroscopic full-layer re-pair of bursal-side partial-thickness rotator cuff tears: a small-window technique. Arthroscopy. 2007;23(8):903.e1-4.
50. Kim KC, Shin HD, Cha SM, Park JY. Repair integrity and func-tional outcome after arthroscopic conversion to a full-thickness rotator cuff tear: articular- versus bursal-side partial tears. Am J Sports Med. 2014;42(2):451-6.
51. Deutsch A. Arthroscopic repair of partial-thickness tears of the
rotator cuff. J Shoulder Elbow Surg. 2007;16(2):193-201. 52. Stuart KD, Karzel RP, Ganjianpour M, Snyder SJ. Long-term
outcome for arthroscopic repair of partial articular-sided su-praspinatus tendon avulsion. Arthroscopy. 2013;29(5):818-23.
53. Shin SJ. A comparison of 2 repair techniques for partial-thickness articular-sided rotator cuff tears. Arthroscopy. 2012;28(1):25-33.
54. Castagna A, Delle Rose G, Conti M, Snyder SJ, Borroni M, Garofalo R. Predictive factors of subtle residual shoulder symp-toms after transtendinous arthroscopic cuff repair: a clinical study. Am J Sports Med. 2009;37(1):103-8.
55. Huberty DP, Schoolfield JD, Brady PC, Vadala AP, Arrigoni P, Burkhart SS. Incidence and treatment of postoperative stiff-ness following arthroscopic rotator cuff repair. Arthroscopy. 2009;25(8):880-90.
56. Seo YJ, Yoo YS, Kim DY, Noh KC, Shetty NS, Lee JH. Trans-tendon arthroscopic repair for partial-thickness articular side tears of the rotator cuff. Knee Surg Sports Traumatol Arthrosc. 2011;19(10):1755-9.
57. Brockmeier SF, Dodson CC, Gamradt SC, Coleman SH, Altchek DW. Arthroscopic intratendinous repair of the delami-nated partial-thickness rotator cuff tear in overhead athletes. Arthroscopy. 2008;24(8):961-5.
58. Ide J, Maeda S, Takagi K. Arthroscopic transtendon repair of partial-thickness articular-side tears of the rotator cuff: anatom-ical and clinical study. Am J Sports Med. 2005;33(11):1672-9.
59. Waibl B, Buess E. Partial-thickness articular surface supraspi-natus tears: a new transtendon suture technique. Arthroscopy. 2005;21(3):376-81.

CiSEClinics in Shoulder and Elbow
Instructions to Authors
1. AIMS AND SCOPE
CiSE is an international, peer-reviewed journal and the of-ficial journal of Korean Shoulder and Elbow Society. It was first launched in 1998. It is published quarterly in the last day of March, June, September, and December, with articles in English.
The purpose of CiSE are, first to contribute in the manage-ment and education of shoulder and elbow topics, second, to share latest scientific informations among international societ-ies, and finally to promote communications on shoulder/elbow problems and patient care. It can cover all fields of clinical and basic researches in shoulder and elbow.
2. LANGUAGE
All manuscripts should be written in English.
3. PEER REVIEW
The papers will be peer-reviewed by two accredited experts in the shoulder and elbow with one additional review by promi-nent member from our editorial board. The Editor-in-Chief is re-sponsible for final decisions regarding the acceptance of a peer-reviewed paper.
4. RESEARCH AND PUBLICATION ETHICS
A. Conflict of Interest
Authors of manuscripts must disclose any potential conflicts of interest at the time of submission. Statements on conflict of interest have no influence on the editorial decision to publish.
B. Research Approval
All manuscripts dealing with human subjects must include a statement that subjects provided informed consent and that the study was approved by an institutional review board. All manu-scripts containing animal experiments must include a statement that the study has been approved by an animal utilization com-mittee or a similar committee.
Any research that involves a clinical trial should be regis tered with a primary national clinical trial registration site such as http://ncrc.cdc.go.kr, or other sites accredited by the WHO or the International Committee of Medical Journal Editors.
C. Policy on Duplicate Publication
Submitted manuscripts must not have been previously pub-lished or be under consideration for publication elsewhere. Redundant or duplicate publication of a paper may be consid-ered acceptable under specific circumstances according to the Uniform Requirements for Manuscripts Submitted to Biomedical
Journals (http://www.icmje.org/icmje.pdf). For policies on research and publication ethics not stated in
the instructions, the ‘Good publication Practice Guidelines for Medical Journals (http://kamje.or.kr/publishing_ethics.html)’ or ‘Guidelines on good publication (http://www.publicationethics.org.uk/guidelines)’ can be applied.
5. SUBMISSION OF MANUSCRIPT
A. Online Submission
• Manuscript submission is only available through the on-line manuscript submission center at http://www.cisejournal.org.
• All manuscripts should be submitted as MS-Word files, and will be converted into PDF files on site. Authors should check converted files before final submission.
B. Financial Disclosure and Copyright Transfer
All authors must download and sign a copy of the journal’s “Financial Disclosure and Copyright Transfer” form, which is available on-line on the submission page. The completed form should be submitted at the time of manuscript submission.
6. PREPARATION OF MANUSCRIPT
Authors are required to submit their manuscripts after reading the following instructions. Any manuscript that does not conform to the following requirements will be considered inappropriate and may be returned.
A. General Requirements
• Manuscripts must be submitted as MS-WORD files. • Text Style - Double space your manuscript. - 10-point font - Times New Roman is preferred. - Use continuous line numbering. - Type text flush left. Do not justify the right margin of your
manuscript. - Enter only one space after punctuation. - Use two hard returns at the end of each paragraph (i.e., one
blank line should appear between paragraphs). - Use two hard returns between headings and text.• All pages and manuscript text with line should be num bered
sequentially, starting from the abstract. Do not restart number-ing in each page instead do a continuous numbering to the final page.
• To facilitate blind peer review, the manuscript must not con-tain the name of any author or institution.
• Measurements should be presented in accordance with the International System of Units (SI).
Enacted from June 1, 2009, Revised on December 31, 2010; June 1, 2013; March 1, 2014 ; May 13, 2014

CiSEClinics in Shoulder and Elbow
Instructions to Authors
• Abbreviations should be minimized. When necessary, spell out the full term the first time it appears in the text, add the abbreviation in parentheses, and use the abbreviation there-after.
• To cite a reference with an author in the text, insert the au-thor’s surname only and the citation number in superscript. e.g., Brown1)
For a reference with two authors, list both names in the ci-tation. e.g., Brown and Copper2) For a reference with three or more authors, use ‘et al.’, e.g., Brown et al.3) The end of a sentence should be indicated by a citation number, not by a period or a comma. e.g., described.3) not as described3).
• If two or more citation numbers are required, separate numbers with a comma (,) or a dash (-). e.g., Boyes1-3) Chap-man1,2,7)
B. Title Page
The title page should contain the full title of the paper, the names of the authors and of the institutions, and institu tional addresses. If authors are at different institutions, first present the institution where most of the work was carried out, and indicate individual departments and institutions by inserting a superscript letter immediately after the author’s name, and the same letter in front of the appropriate institution. The name, address, e-mail address, telephone, and fax number of the corresponding au-thor should be placed in the lower portion of the title page. The title should be expressed briefly, clearly, and concisely.
C. Abstract
Each paper should start with an abstract not exceeding 250 words. The abstract should state the background, methods, re-sults, and conclusions in each paragraph in a brief and coherent manner. Relevant numerical data should be included. Under the abstract, keywords should be inserted (maximum 5 words). Authors are recommended to use the MeSH database to find Medical Subject Heading Terms at http://www.nlm.nih.gov/mesh/meshhome.html. The abstract should be structured into the following sections.1) Background: The rationale, importance, or objective of
the study should be described briefly and concisely in one to two sentences. The objective should be consistent with that stated in the Introduction.
2) Methods: The procedures conducted to achieve the study objective should be described in detail, together with relevant details concerning how data were obtained and analyzed and how research bias was adjusted.
3) Results: The most important study results and analysis should be presented in a logical manner with specific ex-perimental data.
4) Conclusions: The conclusions derived from the results should be described in one to two sentences, and must
match the study objective.
D. Introduction
State the background or problem that led to the initiation of the study. Introduction is not a book review, rather it is best when the authors bring out controversies which create interest. Lead systematically to the hypothesis of the study, and finally, to a restatement of the study objective, which should match that in the Abstract. Do not include conclusions in the Introduction.
E. Methods
Describe the study design (prospective or retrospective, inclu-sion and exclusion criteria, duration of the study) and the study population (demographics, length of follow-up). Explanations of the experimental methods should be concise, but yet enable replication by a qualified investigator.
F. Results
This section should include detailed reports on the data ob-tained during the study. All data in the text must be presented in a consistent manner throughout the manuscript. All issues which the authors brought up in the method section need to be in re-sult section. Also it is preferred that data to be in figures or table rather than long list of numbers. Instead, numbers should be in tables or figures with key comment on the findings.
G. Discussion
The first paragraph of the discussion should deal with the key point in this study. Do not start by article review or general comment on the study topic. In the Discussion, data should be interpreted to dem on strate whether they affirm or refute the original hypothesis. Discuss elements related to the purpose of the study and present the rationales that support the conclu-sion drawn by referring to relevant literature. Discussion needs some comparison of similar papers published previously, and discuss why your study is different or similar from those papers. Care should be taken to avoid information obtained from books, historical facts, and irrelevant information. A discussion of study weaknesses and limitations should be in-cluded in the last paragraph of the discussion.
H. Conclusion
Here you must briefly state your new (or verified) view of the problem you outlined in the Introduction. Take special care to draw your conclusions only from your results. Check that your conclusions are firmly supported by your data. And, most importantly, do not make concluding statements that lie beyond the scope of your study, or unnecessary statements such as “further studies are warranted.” The conclusions in the text must match those in the abstract.

CiSEClinics in Shoulder and Elbow
Instructions to Authors
I. Acknowledgements
All persons who have made substantial contributions, but who have not met the criteria for authorship, should be acknowl-edged here. All sources of funding for the study should be stated here explicitly.
J. References
• The number of references is recommended to 30 for origi-nal article and 10 for case report and technical note.
• The references should be numbered according to the cita-tion order in the text (not alphabetically).
• All references must be cited in the text.• Non-published findings and personal communications
should not be included in the list of references.• References to journal articles should conform to the journal
title abbreviations used in the Index Medicus.• List names of all authors when six or fewer. When seven or
more, list only the first three names and add et al.• Authors should be listed by surname followed by initials.• Examples of references are as follows:
1) Journal article1. Cho NS, Lee BG, Rhee YG. Radiologic course of the calcific
deposits in calcific tendinitis of the shoulder: Does the initial radiologic aspect affect the final results? J Shoulder Elbow Surg. 2010;19(2):267-72.
2. Bhatia S, Frank RM, Ghodadra NS, et al. The outcomes and surgi-cal techniques of the latarjet procedure. Arthroscopy. 2014;30(2): 227-35.
2) Supplement1. Swen JW, Van Der Zwaal P, Thomassen BJW, et al. Clinical out-
come in all-arthroscopic versus mini-open rotator cuff repair in small- to medium-sized tears: a randomized controlled trial in 100 patients. Arthroscopy. 2013;29(10) Suppl:e44.
3) Book1. Iannotti JP, Williams Jr GR. Disorders of the shoulder: diagnosis
& management. 2nd ed. Philadelphia: Lippincott Williams & Wilkins; 2007. 66-80.
4) Book chapter1. Provencher MP, LeClere LE, Van Thiel GS, et al. Posterior
instability of the shoulder. In: Angelo RL, Esch JC, Ryu RKN, eds. AANA advanced arthroscopy the shoulder. Philadelphia: Saunders; 2010. 115-23.
5) Article in Press 1. Shin SJ. A comparison of 2 repair techniques for partial-
thickness articular-sided rotator cuff tears. Arthroscopy. In press, available on 17 October 2011. doi: 10.1016/j.arthro.
2011.07.005.
• For more on references, refer to the NLM Style Guide for Authors, Editors, and Publishers.
K. Tables
• Tables should be numbered sequentially with Arabic nu-merals and given a brief title. Use capital letters for the first letter of each word in the title, except articles, prepositions, and conjunctions.
• Tables should be numbered in the order in which they are mentioned in the text.
• If an abbreviation is used in a table, it should be defined in a footnote below the table.
• The symbols should be used in the following order: *, †, ‡, §,∥, ¶, **, ††, ‡‡. Each symbol must be defined in a foot-note.
• Tables should be understandable and self-explanatory, with-out references to the text.
L. Figure Legends
• Illustrations should be numbered in the order in which they are mentioned in the text (e.g., Fig. 1).
• Each illustration should have a brief and specific legend, which should be listed on a separate manuscript page after references.
• Staining techniques used should be described. Pho tomicro-graphs with no inset scale should have the mag nification of the print in the legend.
M. Illustrations
• Papers containing unclear photographic prints may be re-jected.
• Each figure should be prepared in a separate file (e.g., Fig 1.jpg).
• The name of an image file should match the figure number, such as Fig 1.eps. If a figure contains two or more photo-graphs, they should be assigned an Arabic numeral followed by letters in the English alphabet. Example: Fig 1A, Fig 1B
• Submit illustrations on-line in JPEG, GIF or PPT format. Do not embed images into the text file.
Figures may be halftone photographs or black on white line drawings. Color images will be accepted only when essen-tial. Remove any writing that could identify a patient.
• If a manuscript is accepted for publication, the journal will request high quality figures in TIFF or EPS format. When us-ing a digital camera, set the resolution to a minimum of 300 ppi (pixels per inch), and set the size of the image to 5 × 7 in (127 × 178 mm). Color and grayscale images, such as ra-diographs, must have a minimum resolution of 300 dpi, and line art drawings must have a minimum resolution of 1200 dpi.
• Any illustrations previously published should be accompa-nied by the written consent of the copyright holder.

CiSEClinics in Shoulder and Elbow
Instructions to Authors
7. OTHER TYPES OF MANUSCRIPTS
All other types of manuscripts should meet the above-men-tioned requirements.
A. Review Articles
Review articles should focus on a specific topic. Publi cation of these articles will be decided upon by the Edi torial Board.
B. Case Reports
Authors are warned that these have a high rejection rate.• Abstract: The Abstract should not exceed 200 words, and
must be written as one unstructured paragraph. In other words, Introduction, Materials and Methods, Results, and Conclusions must not be paragraphed in the Abstract.
• Introduction: The reason for reporting the case should be stated in a clear and cohesive manner. It is not necessary to use the word “Introduction.”
• Case Report: This section should include relevant elements, such as, patient history and treatment.
• Discussion: Discussion should focus on the case and perti-nent literature.
• References: References to recommended not to exceed 10.
C. Technical Notes
Technical notes should not exceed 1,500 words. The ab stract should be an unstructured summary not exceeding 150 words. The body of these manuscripts should consist of Introduction, Technique, Discussion, References, and Figures/Figure legends and tables (if applicable). References should not exceed 10. A maximum of 3 figures and 1 table are allowed.
D. Current Concepts
An article that deals with most current trends and controver-sies of a single topic in shoulder and elbow. Authors are recom-mended to update all the knowledge to most recent studies and researches.
E. Systemic Review
An article that examines published material on a clearly de-scribed subject in a systematic way. There must be a description of how the evidence on this topic was tracked down, from what sources and with what inclusion and exclusion criteria.
F. Meta-analysis
A systematic overview of studies that pools results of two or more studies to obtain an overall answer to a question or inter-est. Summarizes quantitatively the evidence regarding a treat-ment, procedure, or association.
G. Letters to the Editor
The journal welcomes readers’ comments on articles pub-lished recently in the journal or orthopedic topics of interest.
H. By Invitation: Editorial
Editorials are invited by the editors and should be com-mentaries on articles published recently in the journal. Editorial topics could include active areas of research, fresh insights, and debates in the field of orthopedic surgery. Editorials should not exceed 1,000 words, excluding references, tables, and figures.
I. By Invitation: Concise Review
This is short version of systemic review requested to submit in the journal by the Editorial board. Usually, previous papers re-garding such topic were published by the main author(s).
J. Special Reports/Expert Opinions
Special reports and expert opinions (Level V studies) of various topics in shoulder and elbow can be submitted. They are limited to 2,700 words excluding references, tables, and figures.
8. STANDARDS FOR REPORTING
For the specific study design, such as randomized con trol study, study of diagnostic accuracy, meta-analysis, ob servational study and non-randomized study, it is recom mended for authors to follow the reporting guide lines listed in the following table.
CONSORT (Consolidated Standards of Reporting Trials)
http://www.consort-statement.org/
STARD (Standards for Reporting of Diagnostic Accuracy)
http://www.stard-state-ment.org/
PRISMA (Preferred Reporting Items of Systematic Reviews and Meta- Analyses)
http://www.prisma-statement.org
STROBE (Strengthening the Report-ing of Observational studies in epidemiology)
http://www.strobe-statement.org/
MOOSE (Meta-analysis of Observa-tional Studies in Epidemiology)
http://www.consort-statement.org/mod_product/uploads/MOOSE%20State-ment%202000.pdf

CiSEClinics in Shoulder and Elbow
Instructions to Authors
Editorial Office Contact InformationClinics in Shoulder and Elbow Department of Orthopedic Surgery, Samsung Medical Center, Sungkyunkwan University, 81 Irwon-ro, Gangnam-gu, Seoul 135-710, Korea Tel: +82-2-3410-3509 / 3501, Fax: +82-2-3410-0061E-mail: [email protected]
9. AUTHOR’S CHECKLIST
□Manuscript in MS-WORD (.doc) format.
□ Double-spaced typing with 10-point font.
□ Sequence of title page, abstract and keywords, introduc tion, methods, results, discussion, conclusion, acknowledgements, references, tables, and figure legends. All pages and manuscript text with line should be numbered sequen tially, starting from the abstract.
□ Title page with article title, authors’ full name(s) and affiliation(s), address for correspondence (including telephone number, e-mail address, and fax number), running title (less than 10 words), and acknowledge ments, if any.
□ Abstract in structured format up to 250 words for origin al articles and in unstructured format up to 200 words for case reports. Keywords (up to 5) from the MeSH list of Index Medicus.
□ All table and figure numbers are found in the text.
□ Figures as separate files, in JPG, GIF, or PPT format.
□ References listed in proper format. All references listed in the reference section are cited in the text and vice versa.
□ Covering letter signed by the corresponding author.
The submission of this journal is free of charge. For submission, subscription, or any other information, please contact the Editorial office.All the figures will be printed in black and white (free of charge), unless requested to be in colors. The ad-ditional cost for color figures might be charged to the authors.

CiSEClinics in Shoulder and Elbow
Copyright Transfer Agreement Form
Clinics in Shoulder and Elbow requires a formal written Copyright Transfer Form of the author(s) for each article published. We therefore ask you to complete and return this form, retaining a copy for your records. Your cooperation is essential and appreciated. Publication cannot proceed without a signed copy of this agreement. If the manuscript is not published in Clinics in Shoulder and El-bow, this agreement shall be null and void.
Copyright Transfer Agreement. I/we have read and agreed with the terms and conditions stated on this page of this agree-ment. I/we hereby confirm the transfer of all copyrights in and relating to the manuscript, in all forms and media of expression now known or developed in the future, including reprints, translations, photographic reproductions, microform, electronic form (offline, online) or any other reproductions of similar nature, to Korean Shoulder and Elbow Society, effective from the date stated below. I/we acknowledge that Korean Shoulder and Elbow Society are relying on this agreement in publishing the manuscript.
Manuscript Title:
Manuscript Number (if applicable):
Date:
All authors appearing in manuscript should be signed in order.
Print Name Signature

CiSEClinics in Shoulder and Elbow
Ethical Policies Check Lists
Please check the below questions.
1. SponsorshipI certify that I had full access to all of the data in this study and I take responsibility for the integrity of the data and the accuracy of
the data analysis. ☐ Yes ☐ No
2. Affirmation of OriginalityI certify that, except to the extent expressly credited to others in the text of the Manuscript: the entire Manuscript is an original cre-
ation of the Authors; and none of the material in the Manuscript has been published previously, is included in another manuscript, or is currently under consideration for publication elsewhere. I also certify that this Manuscript has not been accepted for publication elsewhere, and that I have not assigned, licensed, or otherwise transferred any right or interest in the Manuscript to anyone. More-over, should Korean Shoulder and Elbow Society Institute or the editors of Clinics in Shoulder and Elbow request the data upon which the Manuscript is based, I shall produce them. ☐ Yes ☐ No
3. Institutional Review Board/Animal Care Committee ApprovalI certify that my institution has approved the protocol for any investigation involving humans or animals and that all experimenta-
tion was conducted in conformity with ethical and humane principles of research. ☐ Yes ☐ No
4. Authorship ResponsibilityI certify that I have participated sufficiently in the intellectual content, the analysis of data, if applicable, and the writing of the Man-
uscript, to take public responsibility for it. I have reviewed the final version of the Manuscript, believe it represents valid work, and ap-prove it for publication. ☐ Yes ☐ No
5. Financial DisclosureI have included on the title page of the manuscript any financial arrangements (eg., employment, consultancies, honoraria, stock
ownership or options, expert testimony, grants/patents received, or royalties) that I have with a company whose product figures prom-inently in the submitted manuscript or with a company making a competing product. If no relevant conflicts of interest exist for an author, I’ve stated as such. ☐ Yes ☐ No
6. Funding Sources I certify that all funding sources supporting the work are acknowledged on the title page. ☐ Yes ☐ No
Print Name Signature





























