Embed Size (px)
Citation preview
e-Referral Service Paper Switch-Off Pioneer Project - Lessons LearnedSherwood Hospitals NHS Foundation Trust, Mansfield and Ashfield CCG and Newark and Sherwood CCGJune 2017 V 1.0
1.0Introduction
The NHS Standard Contract1 states that, “With effect from 1 October 2018, the Provider need not accept (and will not be paid for any first outpatient attendance resulting from) referrals by GPs to Consultant-led acute outpatient services made other than through the NHS e-Referral Service.”.
To ensure that commissioners and providers have adequate time to make the necessary process changes to reach a position of 100% e-RS utilisation by October 2018, a national Paper Switch Off (PSO) Programme has been established to provide direct support to trusts in effecting these changes.
The PSO pioneer project between Mansfield and Ashfield (M&A) and Newark and Sherwood (N&S) CCGs and Sherwood Hospitals NHS Foundation Trust (SFH) aims to:
build on the strong e-RS utilisation between the provider and CCGs, which was over 90% when the PSO project commenced deliver full PSO status i.e., 100% e-RS utilisation by 30th April 2017. This was delivered, with a pilot period running through May
(and June due to the unforeseen national cyber-attack) enable lessons to be documented and shared to support other providers to achieve PSO
This document summarises key learning from the pioneer project and shares artefacts that were used in its delivery.
Note: “Going live” with paper switch-off means that the provider will return any paper referrals received to the original referrer without taking any further action.
1 Service condition 6.2A of the NHS Standard Contract 2017/18 and 2018/19 (full length)
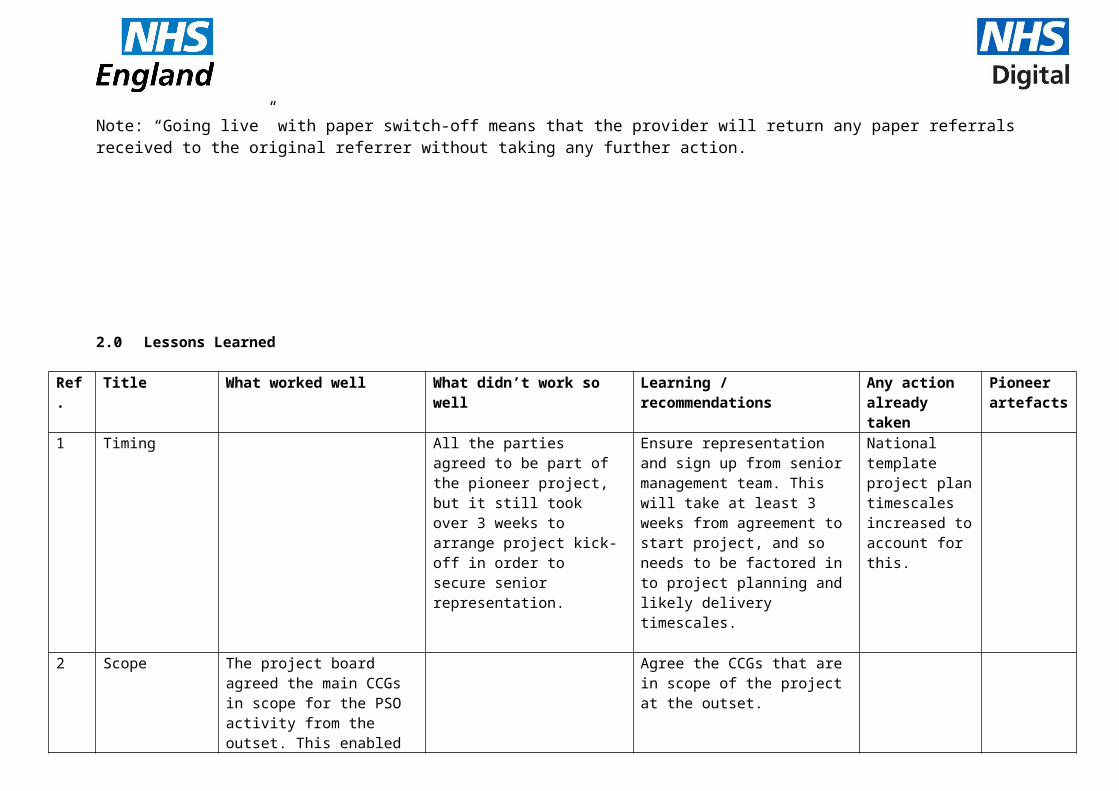
2.0 Lessons Learned
Ref. Title What worked well What didn’t work so well Learning / recommendations Any action already taken
Pioneer artefacts
1 Timing All the parties agreed to be part of the pioneer project, but it still took over 3 weeks to arrange project kick-off in order to secure senior representation.
Ensure representation and sign up from senior management team. This will take at least 3 weeks from agreement to start project, and so needs to be factored in to project planning and likely delivery timescales.
National template project plan timescales increased to account for this.
2 Scope The project board agreed the main CCGs in scope for the PSO activity from the outset. This enabled communications and processes to be focussed.
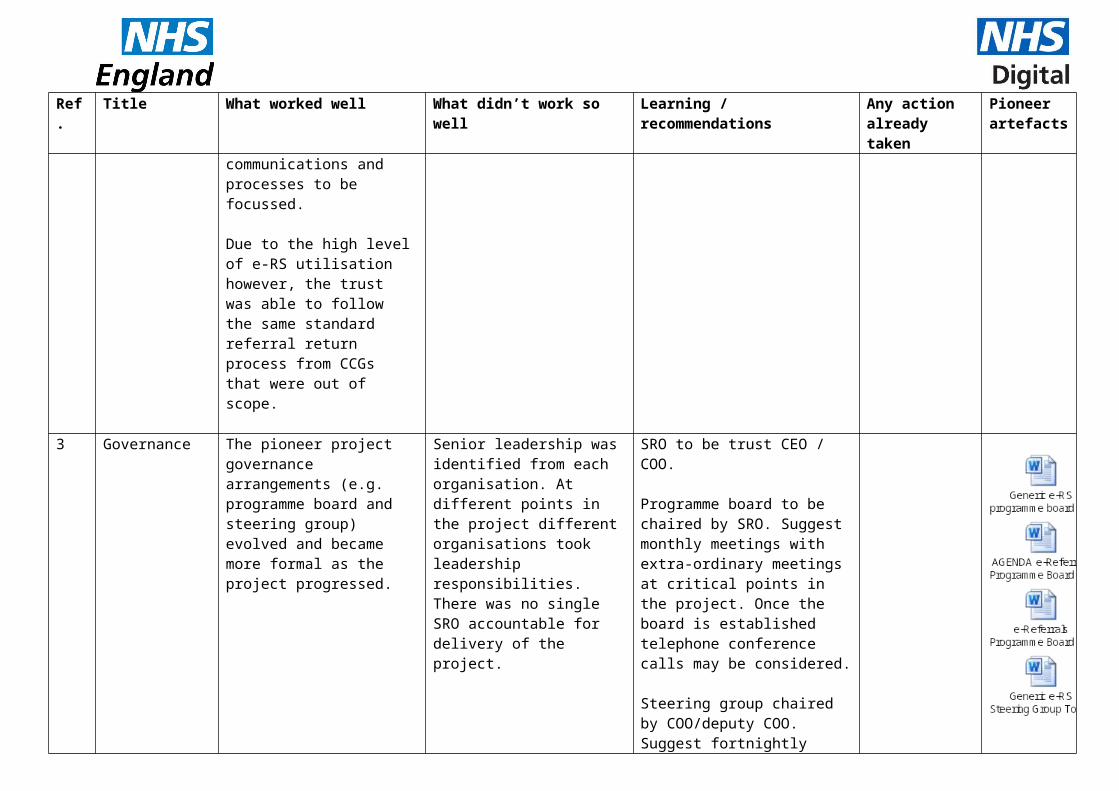
Due to the high level of e-RS utilisation however, the trust was able to follow the same standard referral return process from CCGs that were out of scope.
Agree the CCGs that are in scope of the project at the outset.
3 Governance The pioneer project governance arrangements (e.g. programme board and steering group) evolved and became more formal as the project progressed.
Senior leadership was identified from each organisation. At different points in the project different organisations took leadership responsibilities. There was no single SRO accountable for delivery of the project.
SRO to be trust CEO / COO.
Programme board to be chaired by SRO. Suggest monthly meetings with extra-ordinary meetings at critical points in the project. Once the board is established telephone conference calls may be considered.
Ref. Title What worked well What didn’t work so well Learning / recommendations Any action already taken
Pioneer artefacts
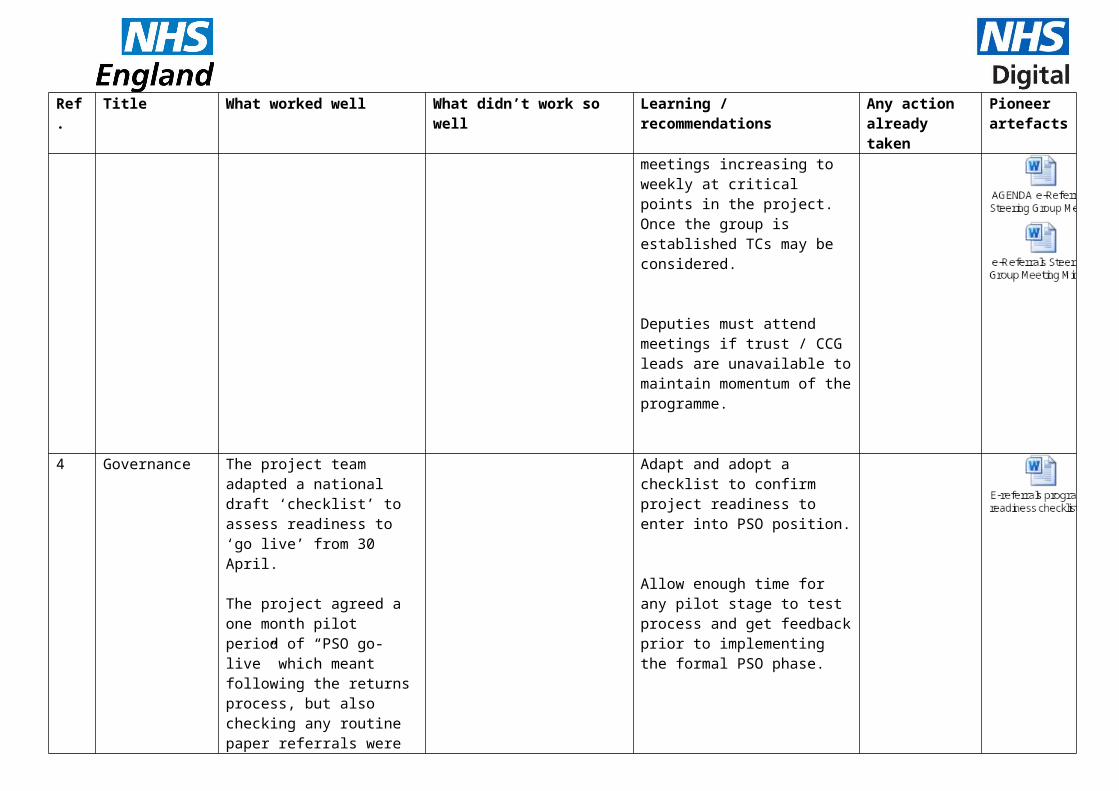
Steering group chaired by COO/deputy COO. Suggest fortnightly meetings increasing to weekly at critical points in the project. Once the group is established TCs may be considered.
Deputies must attend meetings if trust / CCG leads are unavailable to maintain momentum of the programme.
4 Governance The project team adapted a national draft ‘checklist’ to assess readiness to ‘go live’ from 30 April.
The project agreed a one month pilot period of “PSO go-live” which meant following the returns process, but also checking any routine paper referrals were followed up with an e-RS referral. This check will NOT be done in formal BAU.
Adapt and adopt a checklist to confirm project readiness to enter into PSO position.
Allow enough time for any pilot stage to test process and get feedback prior to implementing the formal PSO phase.
5 Project plan/risk log
The DCO pulled together a project plan and risk log after the data phase of the project when wider actions were clearer.
Develop a detailed project plan and risk log early on in the project and continually review.
Ref. Title What worked well What didn’t work so well Learning / recommendations Any action already taken
Pioneer artefacts
6 Performance reporting
The national e-RS utilisation data has an approximate 8 week lag. For this reason, the project team developed a local performance report which could be produced weekly to demonstrate performance improvement in almost ‘real time’. The local performance report solely used the SF-PAS data, as it clearly identified e-RS and non-e-RS referrals received from each of the GP practices.
Develop a local performance report to demonstrate weekly changes in performance as a result of project activities.
For SFH this was relatively easy to do, given the small numbers of paper referrals already occurring, but if considering PSO and returning referrals with lower utilisation, this will be more labour intensive and so resource impact needs to be considered.
7 Data reporting Data reporting was supported through dedicated allocation and effective management and analysis by the provider booking manager.
Assign dedicated time for data reporting and analysis to identify any specific areas for improvement.
8 Data reporting In preparation, the project team agreed early on to communicate to GPs what types of referral MUST be sent via e-RS, and what would be excluded.Note: PSO exclusions might not be exclusions to the MAR, eg. emergency clinics.
Agree list of exclusions with CCG at earliest possible stage prior to go live pilot phaseReview this on a regular basis in line with new services
This task has been added to action plan in the development phase.
Ref. Title What worked well What didn’t work so well Learning / recommendations Any action already taken
Pioneer artefacts
9 Data quality review
Initial discussions during the project initiation phase focussed on data quality and project reporting to determine not only whether there were any data and reporting discrepancies, but also assist to identify the paper referrals still being sent to the trust.
Strat data reporting ASAP, this can be done before the formal project start.
Paper switch-off projects with a utilisation baseline of 80% and above, which will be starting full paper switch-off processes should focus on data and reporting quality as a first priority and at the initial phase of the project.
All other projects should undertake data and referral reporting analyses (MAR and e-RS data) at an early stage of the project to correct any discrepancies and determine the base-line and necessary process for accurate reporting for the paper switch-off project duration. However, this is in conjunction with all other project objects and should not be the sole focus.
10 Data quality review
We compared the booking data from e-RS against the corresponding booking data extracted from the SF-PAS. This was very time consuming and all it achieved was identification of data inconsistencies which led to us focussing on one data source as already reported.
Identify areas of data inconsistency in order to demonstrate margin of error on data reporting for monitoring ongoing PSO position, but don’t go into too much detail. MAR data needs to be accurate and that should be used as the guide. The key is to ensure that the information on e-RS needs
Ref. Title What worked well What didn’t work so well Learning / recommendations Any action already taken
Pioneer artefacts
to be correct, and if it is not on e-RS but should be, then get it on.
Trust Performance/ Information Team are included in the PSO project, at least to support the initial data analysis.
11 Baseline e-RS position/ Preparation
The trust had high usage of e-RS prior to the commencement of programme and good relationships had been built by central support officers with GP’s to support usage of e-RS
Ensure that high usage of e-RS is in place prior to commencing the final PSO stage. One way of achieving high utilisation is to ensure there are good relationships between the provider and GP practices.
12 Baseline e-RS position/ Preparation
DOS is regularly reviewed and updated prior to commencement of programme.This is done at least once a year; services that change work with consultants and the whole of the central booking team (3wte).
Ensure that DOS is reviewed continually & prior to commencing the final PSO stage. NHS Digital has produced a template to support this. It can be downloaded from: http://content.digital.nhs.uk/media/23489/CQUIN-Template/xls/e-RS_CQUIN_Template_Feb_17.xlsx
Paper referrals received into clinics which are available on e-RS maybe due to GP/practice education or certain sub-specialities or specialist conditions not being easily found. GP education, support and communications can
This is accounted for the in CQUIN, and also covered in template project plan.
Ref. Title What worked well What didn’t work so well Learning / recommendations Any action already taken
Pioneer artefacts
address these areas.
13 Baseline e-RS position/ Preparation
A review was undertaken of clinic set ups. This identified clinics that were not
consultant-led, but had been set up as consultant-led clinics.
paper referrals were coming into the trust through other routes than the central process.
Review clinic set ups as part of the project – if not before- as well as communicating the PSO project to all clinics to enable joint working and the identification of current process gaps.
This may require an ad-hoc report to be created, usually for a recent month, and is dependent on NHS trust and PAS. The report should identify; All referrals received and
booked via e-RS. The UBRN (e-RS/unique booking reference number) and the e-RS service ID booked into should be identified.
For referrals received via all other sources (email, fax etc.), the PAS clinic code should be identified.
Where paper referrals are received into PAS clinics, the project team need to identify whether the clinic is mapped to and can be referred to via e-RS or not. Referrals will only be received via paper if the service is not available to the GP/practice on e-RS.
This is covered as a task in the template project plan.
Ref. Title What worked well What didn’t work so well Learning / recommendations Any action already taken
Pioneer artefacts
14 New operating processes / Access policies
SFH and the CCGs developed new operating processes for the handling of referrals from 30 April to 31 May (transitional processes during pilot period) and 1 June onwards (post transition processes). These were signed off by the medical director of SFH and David Ainsworth (clinical rep. at the CCGs).
This process was supported by having the centralised booking team as a resource for GP’s to email or telephone with any queries.
In the pilot “switch-off” phase, the trust kept the paper referral in order to keep track that the referral still got made, and it matched up to one through e-RS.
The main reason identified for paper referrals continuing was due to high locum workforce but GPs try to refer back to them. GPs also report they feel more “confident” with the referral on paper. Key message for anything critical – use e-RS and then for anything urgent
It took longer than expected to get appropriate clinical/executive staff to sign-off changes to policy and process.
There was a need to secure a comprehensive list of GP email addresses for rejection process and this took longer than expected to obtain.
Allow sufficient time to ensure governance processes are agreed and signed off by CCG and trust governance leads i.e. algorithm, rejection process.
Develop and agree local operating processes regarding actions should any paper referrals be received following PSO “go-live” and ensure these are approved by clinical representatives at both the provider and CCG.
Communicate these to all GP practices.
Keep track of paper referrals following “switch off” to identify any specific GP practices which require further communication.
Communicate and reassure practices that referrals are not higher priority/seen quicker/less likely to be missed if they are on paper. If they have any concerns the e-RS referral would be missed, advise practices to still use e-RS and follow up on the phone/email to team.
.
Ref. Title What worked well What didn’t work so well Learning / recommendations Any action already taken
Pioneer artefacts
follow up on the phone/email to team.
15 New operating processes / access policies
It was not possible to achieve approval of the revised trust access policy by both trust board and CCG governing body before ‘go live’. Only relatively minor words changed but due to the review process being only every 3 months, plus the number of committees, this takes significantly longer. (Although this was not business critical for ‘go live’ in this particular situation as changes were minor).
Revise and approve trust access policy prior to “going live” with PSO status. This needs to be right at the start of process due to all the approvals.
National project plan revised to ensure this at the start.
16 CCG communications
The CCG used a number of channels to reach practices, ie. weekly newsletter, direct telephone conversation, clinical exec committee.
Some FAQ’s were also developed and shared based on GP practice queries
Ensure that GP practices are communicated to early on in the project, regularly, and also consider direct communication to ensure they are aware of the revised process.
Use as many different kinds of communication as possible to ensure coverage – bulletins might not be read by all (which was evident when CCG followed up with phone call)
Added to implementation pack
17 ‘Go live’ decision
Written approval from the trust COO and CCG director lead meant that the programme board approval to
The time taken for this approval was longer than anticipated.
Formal written approval should be sought from the trust COO and CCG director lead before recommending ‘go live’ to the
Ref. Title What worked well What didn’t work so well Learning / recommendations Any action already taken
Pioneer artefacts
“go-live” was less contentious.
Kick-off meeting agreed the approach to making the go-live decision.
programme board for final decision to return paper referrals, i.e., PSO status.The time taken to get this approval should be factored into planning.
18 Ongoing reporting following PSO
The trust and CCGs agreed ongoing reporting activities following PSO to ensure any slips in performance are identified and can be rectified immediately.
Trusts’ PAS data should be utilised to report and monitor referrals received via e-RS and received via paper. Any reporting should be aligned to what is included in the MAR, to ensure only consultant-led referrals are included in the reporting and all other referrals, including agreed exclusions are not included.
Monthly e-RS reports that NHS Digital publishes (http://content.digital.nhs.uk/referrals/reports) including monthly ASI reports, monthly e-RS utilisation and daily booking reports to be analysed every month.
Internal e-RS applications reports and extracts are available within the e-RS professional application to support additional analysis of referrals and bookings made via e-RS. There is more information
Ref. Title What worked well What didn’t work so well Learning / recommendations Any action already taken
Pioneer artefacts
on the NHS Digital website -http://content.digital.nhs.uk/applicationextracts
Trust agreed to provide CCG with ongoing data set from PAS to enable the CCG to continually address concerns with practices but to also include with other reporting formats.
19 Contingency plan
Contingency process for when e-RS is not available is already written into the SFT Health economy contingency plan. Within one week of going live with the pilot phase, there was a national cyber-attack. This affected the trust and CCGs systems, so they were unable to make and receive e-RS referrals. The contingency plan was invoked and worked well to ensure referrals continued to be made and received.
e-RS contingency process should be detailed in the trust/health economies contingency plan.
3.0 Next steps to Lessons Learnt
This report covers stage one of the approach to sharing lessons from the Sherwood Forest PSO project.
Stage Two will involve an interview with the trust and CCGs focussing on their wider e-RS performance, and more innovative and interactive communications channels for sharing and communicating the information. This could include lessons learnt WebEx, short video clips or a case study.
Stage three will incorporate other trusts and projects that have demonstrated significant improvement in e-RS utilisation over the last year and how they achieved improvement.




























