Embed Size (px)
Citation preview
Interesting case (Esophageal achalasia) A 7-month-old female infant with chronic vomiting
27 กนยายน 2556
พญ.อมรพรรณ แกนสาร
สถาบนกมารเวช
โรงพยาบาล สมตเวช สขมวท
ทารกเพศหญง อาย 7 เดอน สญชาต โอมาน
CC: อาเจยนทกวนมา 4 เดอน PI: ทารกเรมอาเจยนตงแตอาย 3 เดอน อาเจยนหลงกนนม 5-10 นาท มอาการทกวนและทกครงทกน ไอกอนอาเจยน บางครงกไมไอ กนนมแมอยางเดยว ยงไมไดเรมใหอาหารตามวย น าหนกลด 1 กโลกรม ใน 1 เดอน ตงแตอาย 5 เดอน ตองนอน รพ. ดวยเรอง ปอดอกเสบ 3 ครง ปจจบนตองพนยา ventolin NB 2 ครงตอวนทกวน ยงมอาการอาเจยนอยทกวนและทกมอหลงกนนม
PH: เกดครบก าหนด น าหนกแรกเกด 2.6 กโลกรม ไมมปญหาหลงเกด กอนอาย 3 เดอน กนนมไดปกตด ไมมอาเจยน
FH: พอ เปน หอบหด
Physical examination: Marasmic appearance, BW 5 kg (<P3), length 66 cm (P50), HC 39 cm, SpO2 97% in room air Vital signs: BT 36.8oC, PR 100/min, RR 40/min, BP 90/60 mmHg HEENT: no pallor, no icteric sclerae Heart: normal S1& S2, no murmur Lungs: occasional rhonchi, no wheezing, no chest retraction Abdomen: no distension, active bowel sound, soft, no hepatosplenomegaly Extremities: no rash Neurological exam: within normal limit
Pthaiga
stro.o
rg
Problem lists: 1. Chronic vomiting 2. Failure to thrive / PEM 3. Recurrent pneumonia 4. Chronic lung disease
Differential diagnosis:
• Gastroesophagel reflux disease with stricture
• Pharyngeal incoordination / TE fistula
• Eosinophilic gastroenteritis
• Esophageal / gastric obstruction
• Hypertrophic pyloric stenosis (very unlikely, onset is too late)
• Gastric malrotation
• Cow milk protein allergy / food allergy
• Motility disorder: achalasia, esophageal dysmotility, pseudo-achalasia
• Neurological disorder
• Metabolic disorder
Investigations:
• CBC: Hct 36%, WBC 10,580/ cu mm (N 23, L 66, E 3%), Plt 335,000/ cu mm
• Na 138, K 4.5, Cl 101, CO2 21 mEq/L
• Blood sugar 85 mg/dL; AST 30, ALT 26 IU/L
• TB/DB 0.6/0.2 mg/dL, serum albumin 4.3 g/dL
• Calcium 10, phosphorus 5.8 mg/dL
• Amylase 48 U/L; BUN 8, Cr 0.3 mg/dL
• IgE for cow milk : class II (0.70-3.50 kU/I)
• Abdominal ultrasound : normal Pthaiga
stro.o
rg
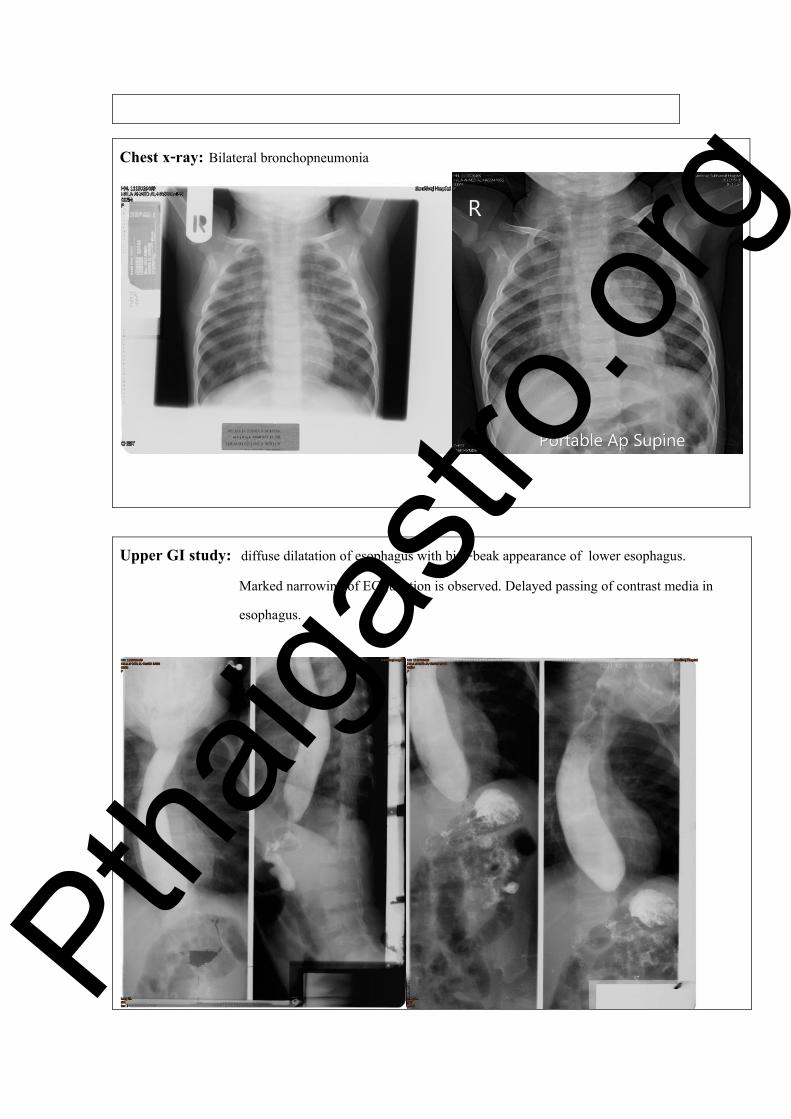
Chest x-ray: Bilateral bronchopneumonia
Upper GI study: diffuse dilatation of esophagus with bird-beak appearance of lower esophagus. Marked narrowing of EG junction is observed. Delayed passing of contrast media in esophagus.
Pthaiga
stro.o
rg

จากผล work up เพมเตม เหลอ differential diagnosis: • Achalasia • GERD with stricture • Eosinophilic esophagitis • Pseudo-achalsia
Diseases associated with achalasia-like motility:
• Malignancy
• Chagas disease
• Amyloidosis
• Sarcoidosis
• Neurofibromatosis
• Eosinophilic gastroenteritis
• Multiple endocrine neoplasia, type 2B
• Juvenile Sjögren syndrome with achalasia and gastric hypersecretion
• Chronic idiopathic intestinal pseudo-obstruction
• Anderson-Fabry disease
Gastroscopy: Esophagus : moderate retained white fluid (milk) from upper to lower esophagus, no fistula EG-junction : mild dilatation of distal esophagus, endoscope (8.8 mm) can be passed with a little bit force and minimal tear, but no active bleeding
Pthaiga
stro.o
rg

Stomach : normal mucosa
Duodenal bulb : multiple small lymphoid hyperplasia
Ptha
igastr
o.org

Pathology result: Glycogenic acanthosis, no organism or inflammatory cell infiltration seen
Final diagnosis is Achalasia
หลงจากสองกลอง ผปวยไมอาเจยนอก ดดนมไดด อาจเปนจากทตอนสองกลองม partial dilatation ไดปรกษาศลยกรรมเดกเรองการผาตด Heller myotomy แตมารดาปฎเสธเพราะเหนวาทารกไมอาเจยนแลว ไดแนะน ามารดาวา มโอกาสทจะมอาการกลบมาเปนซ าอก ถามอาการมาอกแนะน าใหผาตด หรอท า esophageal dilatation
สวนอาการทางปอดไดปรกษากมารแพทยโรคทางเดนหายใจ ใหพนยา รกษาแบบ chronic lung disease
นอกจากนไดปรกษากมารแพทยตอมไรทอ เนองจาก โรค achalasia ในเดกอาจจะพบรวมกบ
Allgrove syndrome (4 “A” syndrome) ไดแก 1. achalasia 2. alacrima (รองไหไมมน าตา) 3. autonomic disturbance และ 4. ACTH (corticotropin) insensitivity ซงท าใหเกด adrenal insufficiency จะม hyperpigmentation และ low serum cortisol แตจะม normal serum electrolytes เพราะไมมผลกบ aldosterone ซงผปวยรายนมผล serum electrolytes ปกต กมารแพทยตอมไรทอแนะน าวา ผปวยรองไหมน าตา คงนกถง Allgrove syndrome นอย ยงไมตอง ตรวจ ACTH stimulation test ใหตดตามดอาการ Progression ชวง 1 เดอน (อาย 7 เดอน) หลงจากสองกลอง ทารกกนได ไมอาเจยนเลย น าหนกเรมขน เมออาย 8 เดอน เรมมอาการอาเจยนอก เกอบทกมอ ไดแนะน ามารดาวา การท า esophageal dilatation ไมไดหายขาด อาจจะมอาการกลบมาใหมไดอก ตองท าหลายครง มารดาจงตดสนใจใหผาตด Heller myotomy หลงผาตดไมมภาวะแทรกซอน ไมมอาเจยน กนได น าหนกขนด Ptha
igastr
o.org

Achalasia
ค าวา achalasia มาจากภาษากรกทแปลวา ไมคลายตว เปน primary motor disorder ทม absence of peristalsis in distal esophagus จาก smooth muscle และม incomplete relaxation of the lower esophageal sphincter (LES) ท าใหมอาการเหมอน esophageal obstruction จดเปน functional obstruction โดยมการรายงานผปวยรายแรกในป ค.ศ.1674 โดย Sir Thomas Willis และไดมการตงชอโรควา “achalasia” ในป ค.ศ. 1927 โดย Hurst การศกษาจากตางประเทศพบอบตการณของโรค ประมาณ 0.1:100,000 คน (England . Wales study) ความชก 10.8 : 100,000 คน สวนใหญจะวนจฉยขณะอาย 7-15 ป พบในเดกอายนอยกวา 15ป ประมาณ 3-5% พบนอยมากในทารก
Pathophysiology:
• ม degeneration of Auerbach’s myenteric plexus
• จ านวน myenteric ganglion cells ลดลง หรอ อาจมจ านวนปกต แตม myenteric fibrosis
• loss of intrinsic inhibitory enteric neurons
• ผลท าใหมการไมสมดลระหวาง excitatory and inhibitory input ท าใหม ineffective esophageal peristalsis และ incomplete LES relaxation
Etiology:
Primary (idiopathic) ไมทราบสาเหตชดเจน Secondary Chagas disease สาเหตจากเชอ Trypanosoma cruzi
(พบบอยใน South และ Central America) เบาหวาน มะเรงบางชนด Many hypotheses:
• โรคตดเชอจากไวรสบางชนด เชน measles, HSV-1, VZV
• สาเหตทางพนธกรรม เชน อาจพบรวมกบโรคทางพนธกรรมบางโรค เชน Trisomy 21, Hirschsprung disease, Allgrove syndrome, familial dysautonomia
• สาเหตจาก autoimmunity Ptha
igastr
o.org

จากการส ารวจผปวย 175 รายในป 1994 พบวา มอาการขณะเปนทารกประมาณ 18% แตสามารถวนจฉยขณะเปนทารกไดเพยง 6%
Clinical manifestations in infant:
• Vomiting (62.5%)
• Failure to thrive (75%)
• Recurrent aspiration pneumonia (50%)
Clinical manifestations in children:
• Vomiting (80%)
• Dysphagia (75%)
• Weight loss (64%)
• Chest pain and odynophagia (45%)
• Respiratory symptoms (44%)
• Failure to thrive (31%)
• Choking and food regurgitation (21%)
Diagnosis of achalasia
• History: มประวตและอาการทท าใหคดถงโรค achalasia เชน อาเจยน กลนล าบาก เปนปอดอกเสบบอยๆ เลยงไมโต ส าลกอาหาร
• Chest x-ray : ม widening of mediastinum , air- fluid level in lower chest, double mediastinal stripe
• Barium swallowing : diagnostic accuracy 95%; dilated distal esophagus, bird’s beak-like, sigmoid shape, fluoroscope: absent / delayed persistalsis
• Gastroscopy ดงจะกลาวตอไป
• Esophageal manometry Ptha
igastr
o.org

Endoscopic findings in achalasia:
• Retained food in dilated esophagus without mechanical obstruction
• Tight EG junction (difficult to distend with air insufflation) but can pass scope to stomach with little force
• Esophageal mucosa : normal
• Inflammation, ulceration : irritation caused by retained food or pills
• Esophageal stasis predisposed to candida infection (adherent whitish plaques on the mucosa surface)
• Normal endoscopic finding dose not rule out achlasia Conventional esophageal manometry: PPV 96%, specificity 98%, sensitivity 100% จะพบลกษณะดงน
1. Elevated resting LES (> 45 mmHg) 2. Incomplete LES relaxation after a swallow 3. Aperistalsis in the smooth muscle portion of the body of the esophagus
Milner-Fenwick, Inc. at AGA.1-800-432-8433
การท า esophageal manometryไมสามารถแยก primary (idiopathic) achalasia จาก pseudo-achalasia ดงนนถงแมวาผล esophageal manometry จะเขาไดกบ achalasia กควรทจะท า gastroscopy เพอการวนจฉยแยกจาก pseudo-achalasia Ptha
igastr
o.org

High resolution esophageal manometry: สามารถใชแยก subtype ของ esophageal achalasia ได การแยก subtype จะชวยบอก prognosis ของโรคไดโดยการรกษาจะไดผลดทสดใน type II และจะไดผลนอยทสดใน type III
Original figure modified from this publication. Pandolfino JE, Kwiatek MA, Nealis T, et al. Achalasia: a new clinically relevant classification by high-resolution manometry. Gastroenterology 2008; 135:1526. ตารางการเปรยบเทยบเกณฑการวนจฉย achalasia โดยใช conventional หรอ high resolution manometry
Ptha
igastr
o.org
Treatment of achalasia:
• Chronic condition without cure
• Current treatment aim decreasing the resting pressure in LES Goals of treatment:
• Relieve patients’ symptoms
• Improve esophageal emptying
• Prevent further dilation of the esophagus Treatment of choice is still debated:
• Pharmacological therapy
• Botulinum toxin injection
• Pneumatic dilatation
• Temporary self-expanding metalic stent (case report of a 12-year-old patient)
• Peroral endoscopic myotomy (POEM)
• Surgical myotomy Pharmacological Therapy:
• ยากลมทใช ไดแก nitrates, calcium channel blockers และ phosphodiesterase inhibitors ท าใหเกด relaxation of smooth muscle of LES เชน isosorbide dinitrate patch, nifedipine
• ผลการรกษา variable success 53-87%
• ผลขางเคยงจากการรกษา 30% เชน nitrate ท าใหเกด headache, hypotension
และ Ca channel blocker ท าใหเกด peripheral edema และ frequently associated
with tachyphylaxis
• มกใชเปนการรกษาชวคราวกอนทจะท า definitive therapy Ptha
igastr
o.org

Botulinum toxin injection:
• ใช botulinum toxin ซงเปน potent pre-synaptic inhibitor of acetylcholine release
from nerve endings
• ฉดท LES จะท าใหเพม LES smooth muscle tone ผลรวมท าใหมการลดลงของ LES pressure
• ต าแหนงทฉด ฉดเหนอ squamo-columnar junction อยางนอย 4 quadrants
• ผลของการรกษา 80%
• ผลการรกษาจะลดลงตามเวลา ไดผล 70% ท 3 เดอน 53% ท 6 เดอน และ ลดเหลอ 41% เมอเวลาผานไปมากกวา 12 เดอน
Pneumatic dilatation:
• การท า graded pneumatic dilatation เพอใหมการฉกขาดของ muscle fiber
• ขนาด balloon size 18-35 mm (ถาไมมอาจใช CRE balloon ขนาด 18, 19, 20 mm หรอใช pneumatic balloon ขนาด 30, 35 mm)
• ผลการรกษา 1 เดอนแรก และยงคงไดผลใน 2 ปแรก เทากบ 85%
• ผลการรกษาจะลดลงตามเวลา ไดผล 74% ท 6 เดอน 68% ท 12 เดอน และ 58% ท 3 ป โดย 1/3 จะมอาการกลบเปนซ าและตองการการรกษาอกใน 4-6 ป
• ผลแทรกซอนทอาจเกดขนไดแก perforation (1.6%), heart burn (15-35%)
• ถาท าการ dilatation > 3 ครงแลวยงมอาการอย แนะน าใหผาตด Ptha
igastr
o.org

รป แสดงการท า pneumatic dilatation และ อปกรณ จาก เวปไซด
Surgical myotomy
• ผาตดท า Heller myotomy with partial fundoplication
• การท าแบบ laparoscopic ดกวา transabdominal และ trans abdominal ดกวาแบบtransthoracic
• ไดผลดใน achalasia type I มากกวา type II
• ผลการรกษา 1 เดอนแรก และยงคงไดผลใน 2 ปแรก เทากบ 90%
• ภาวะแทรกซอนทอาจเกดขน ไดแก GERD (9%), perforation, pneumothorax, bleeding, phrenic nerve paralysis, infection, herniation of stomach
• ภาวะแทรกซอนทอาจเกดขนไดในระยะยาว ไดแก persistent dysphagia, GERD Ptha
igastr
o.org
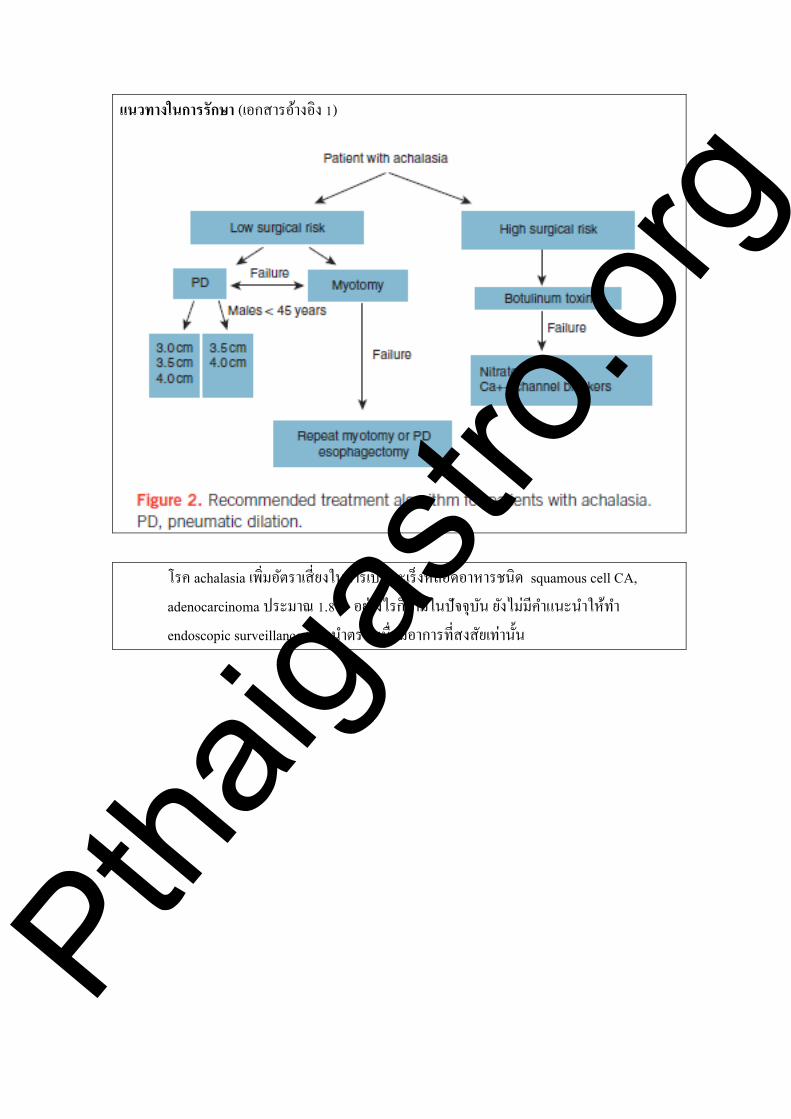
แนวทางในการรกษา (เอกสารอางอง 1)
โรค achalasia เพมอตราเสยงในการเปนมะเรงหลอดอาหารชนด squamous cell CA, adenocarcinoma ประมาณ 1.8% อยางไรกตามในปจจบน ยงไมมค าแนะน าใหท า endoscopic surveillance แนะน าตรวจเมอมอาการทสงสยเทานน
Ptha
igastr
o.org

เอกสารอางอง 1. Vaezi MF, Pandolfino JE, Vela MF. ACG clinical guideline: diagnosis and management
of achalasia. Am J Gastroenterol 2013; 108(8): 1238. 2. Reynolds JC, Parkman HP. Achalasia. Gastroenterol Clin North Am1989; 18: 223-55. 3. Sadowski DC, et al. Achalasia: incidence, prevalence and survival. A population-based
study. Neurogastroenterol Motil 2010; 22(9): 256-61. 4. Mayberry JF, Mayell MJ. Epidemiological study of achalasia in children. Gut 1988; 29(1):
90-3. 5. Holloway RH, Dodds WJ, Helm JF, et al. Integrity of cholinergic innervation to the lower
esophageal sphincter in achalasia. Gastroenterology 1986; 90: 924-9 6. Campos GM, Vittinghoff E, Rabl C, Takata M, et al. Endoscopic and surgical treatments
for achalasia: a systematic review and meta-analysis. Ann Surg2009 Jan; 249(1): 45-57. 7. Boeckxstaens GE, Annese V, des Varannes SB et al. Pneumatic dilation versus
laparoscopic Heller's myotomy for idiopathic achalasia. N Engl J Med 2011; 364(19):1807 8. Zendehdel K, Nyrén O, Edberg A, Ye W. Risk of esophageal adenocarcinoma in achalasia
patients, a retrospective cohort study in Sweden. Am J Gastroenterol 2011; 106(1): 57. 9. Yaşar NAZLIGÜL, Mehmet ASLAN2, Ramazan ESEN, et al. Benign glycogenic
acanthosis lesions of the esophagus. Turk J Gastroenterol 2012; 23 (3): 199-202 10. Hamza AF, Awad HA , Hussein O. Achalasia in Children. Dilatation or Surgery? Eur J Pediatr Surg 1999; 9(5): 299-302 11. Upadhyaya VD, Gangopadhyaya AN, Gupta DK, et al. Esophageal achalasia of unknown
etiology in infants. World J Pediatr 2008; 4(1): 63-5.
Pthaiga
stro.o
rg




























