Embed Size (px)
Citation preview

© Copyright 2003 Cardinal Health, Inc. or one of its subsidiaries. All rights reserved.
PET in PET in Colorectal CancerColorectal Cancer
Early detection of diseaseEarly detection of diseasePrecise Staging of Disease ProgressionPrecise Staging of Disease Progression
Accurate Assessment of TherapyAccurate Assessment of Therapy

© Copyright 2003 Cardinal Health, Inc. or one of its subsidiaries. All rights reserved.
Colorectal CancerColorectal Cancer
• Over 150,000 new colorectal cancers/yr, the second most common killer after lung cancer.
• A Malignant transformation of a polyp
• TNM staging is used to plan and assess therapy
• Complete surgical resection is generally required for a cure
• Resection of limited metastatic disease yields improved survival, unlike many cancers

© Copyright 2003 Cardinal Health, Inc. or one of its subsidiaries. All rights reserved.
Colorectal Cancer IndicationsColorectal Cancer Indications
• Diagnosis
• Staging
• Restaging

© Copyright 2003 Cardinal Health, Inc. or one of its subsidiaries. All rights reserved.
Diagnosing Colorectal CancerDiagnosing Colorectal Cancer
History • 54 YOF • Right Upper Quadrant
abdominal pain• CT reveals hepatic metastases
without known primary
PET Findings• 3 Hyper-metabolic foci in the
liver and 1 in the Left Upper Quadrant
Outcome • Splenic flexure colon cancer
and 3 liver mets resected
primary
mets

© Copyright 2003 Cardinal Health, Inc. or one of its subsidiaries. All rights reserved.
PET in Colorectal CancerPET in Colorectal Cancer
• Diagnosis
• Staging
• Restaging

© Copyright 2003 Cardinal Health, Inc. or one of its subsidiaries. All rights reserved.
Staging Colorectal CancerStaging Colorectal Cancer
History • 63 YOM • Large rectal cancer via pre-op evaluation• CT suggest invaded lymph nodes near
the primary
PET Findings• Rectal, multiple pelvic, right inguinal,
and liver abnormalities
Outcome • Aggressive chemotherapy followed by
pelvic XRT• Followed by successful AP (rectal) and
liver resection
Large solitary met

© Copyright 2003 Cardinal Health, Inc. or one of its subsidiaries. All rights reserved.
Pre-operative Staging of Pre-operative Staging of Primary Colorectal CarcinomaPrimary Colorectal Carcinoma
• Study of 48 colorectal cancer patients
• Pre-op PET results compared to results at surgery and follow up
PET CT Liver Mets Detected 88% 38%
• 4 liver mets were detected by PET, but ignored at time of initial surgery.
Presence of mets was confirmed >3 months after surgery
Abdel-Nabi Radiology 1998; 206:755.
© Copyright 2003 Cardinal Health, Inc. or one of its subsidiaries. All rights reserved.
PET in Colorectal CancerPET in Colorectal Cancer
• Diagnosis
• Staging
• Restaging Detecting recurrence
Staging recurrence
Assessing therapy

© Copyright 2003 Cardinal Health, Inc. or one of its subsidiaries. All rights reserved.
Detecting RecurrenceDetecting Recurrence
History • 60 YOM • Colon cancer 2 years ago • Rising CEA• Negative CT findings
PET Findings• Retroperitoneal abnormality
Outcome • Nodal metastasis resected to
confirm PET findings• Adjuvant chemotherapy

© Copyright 2003 Cardinal Health, Inc. or one of its subsidiaries. All rights reserved.
Staging RecurrenceStaging Recurrence
History • 56 YOF • Rectal cancer 14 months ago• Persistently elevated CEA (never
really dropped)
PET Findings• Single liver abnormality
Outcome • Liver met resection• No recurrence
© Copyright 2003 Cardinal Health, Inc. or one of its subsidiaries. All rights reserved.
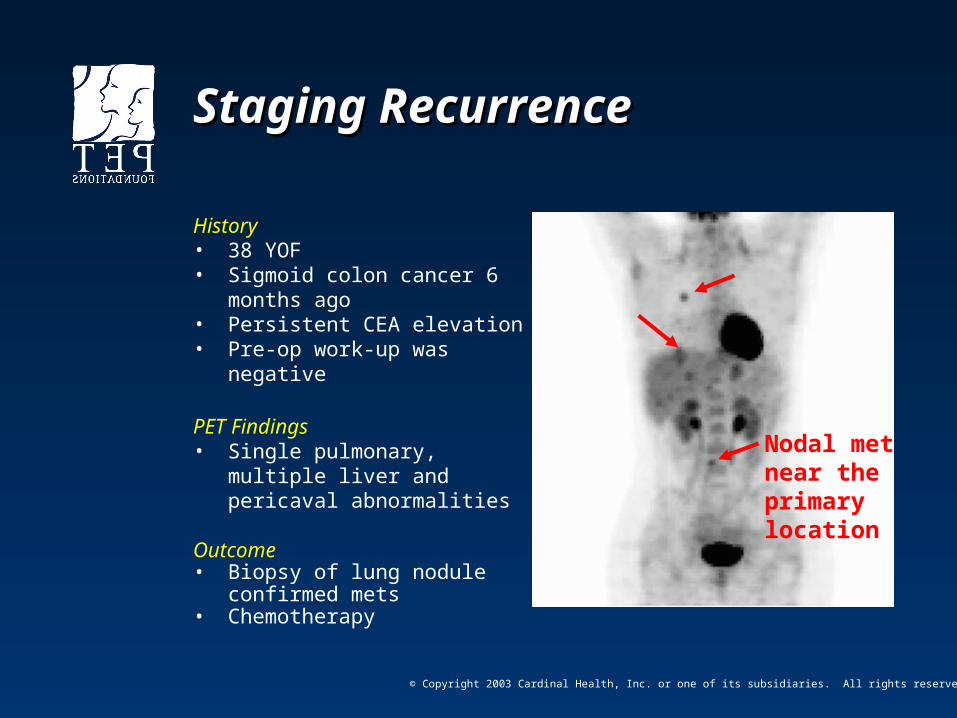
Staging RecurrenceStaging Recurrence
History • 38 YOF • Sigmoid colon cancer 6 months
ago• Persistent CEA elevation• Pre-op work-up was negative
PET Findings• Single pulmonary, multiple liver
and pericaval abnormalities
Outcome • Biopsy of lung nodule confirmed
mets• Chemotherapy
Nodal met near the primary location

© Copyright 2003 Cardinal Health, Inc. or one of its subsidiaries. All rights reserved.
Detecting Recurrence in Patients Detecting Recurrence in Patients with Increasing CEA Levels with Increasing CEA Levels
• Prospective study of 28 colorectal cancer patients
• PET was compared to 2nd look surgery results
• PET predicted correctly
PET Un-resectable Disease90% Resectable Disease 81%
Libutti SK Ann Surg Onc 2001;8:779

© Copyright 2003 Cardinal Health, Inc. or one of its subsidiaries. All rights reserved.
Why PET?Why PET?
• Recurrent and metastatic colorectal cancer is common (35% within 2 years)
• Early detection of localized disease is possible with PET , when the disease is still resectable
• PET helps avoid surgery in patients with multi-focal and extra-hepatic metastases

© Copyright 2003 Cardinal Health, Inc. or one of its subsidiaries. All rights reserved.
PET in Colorectal CancerPET in Colorectal Cancer
• PET accurately detects local, hepatic and extra-hepatic disease
• PET is superior to all imaging modalities in the restaging of colorectal cancer
• Difficult patient management problems can be solved with the unique information PET provides













![[PPT]What is t,n,m staging and summary staging? Staging for... · Web viewWhat are we discussing? What is AJCC Staging Purpose of staging General rules for clinical and pathological](https://img.dokumen.tips/doc/110x75/5b1cc7cc7f8b9a8c5a8ba42e/pptwhat-is-tnm-staging-and-summary-staging-staging-for-web-viewwhat.jpg)















