Embed Size (px)
Citation preview

Controversial Suboptimal diagnostic testing Transmitted by Ixodes ticks
◦ May also transmit Babesia and Anaplasma Variable disease presentation
◦ Cutaneous◦ Cardiac◦ Rheumatologic◦ Neurologic
Treatment is longer than for other spirochetal illnesses

1883 – Buchwald, degenerative skin d/o 1902 – Herxheimer, ACA 1909 – Afzelius, EM rash post tick bite described 1913 – Lipschutz, ECM rash described 1921 – Afzelius case reports, associates Ixodes
ticks 1930 Hellerstrom, links EM and lymphocytic
meningitis 1941 – Bannwarth, lymphocytic
meningoradiculitis 1946 – Svartz, PCN for ACA

1948 – Lenhoff, spirochetes on EM 1950 – Hellerstrom, ECM with meningitis
treated with PCN 1955 – Binder, 355 cases of ECM treated
with PCN 1968 – Scrimenti, first case of EM in US
reported 1975 – Murray (Lyme resident) reports
cases in relatives and friends in area 1975 – Steere identifies cases as “Lyme
arthritis”
1997 – Steere, defines more complete case description (cardiac, rheum, neuro)
1980 – Steere, rx with PCN or tetracycline 1982 – Burgdorfer, discovers spirochetes in
blood, CSF, skin lesions of Lyme patients 1997 – genome sequenced 1999 – vaccine marketed

Borrelia burgdorferi has has at least 132 functional genes (c/w about 22 for T pallidum)
Most plasmids of any bacteria identified to date
Antigenic variation/quorum sensing to evade immune response
Dormancy? Cyst structures form in vitro





Ixodes scapularis (east and midwest)
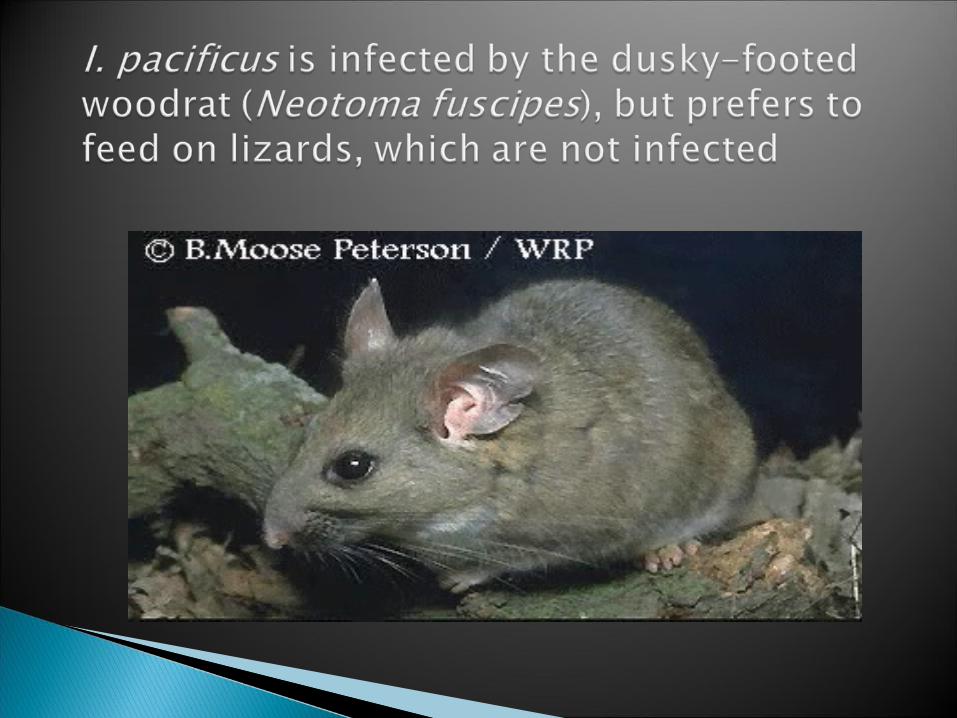
Ixodes pacificus (west)
Deer / blacklegged tick,
Ixodes scapularis
Western blacklegged tick (Ixodes pacificus)


From left to right: The deer tick (Ixodes scapularis) adult female,
adult male, nymph, and larva on a centimeter scale.




Most common tick-borne disease in US and Europe.
Affects 50 nations worldwide
Nymphal ticks are primarily responsible for Lyme transmission to humans.
Tick must feed for ~ 48 hours and become engorged before risk of transmission becomes substantial.
Risk of infection after a deer tick bite in a highly endemic area is ~1.4%.

Obtaining Lyme serology at the time of tick bite is not recommended.
Prophylactic one time use of 200 mg doxy can be considered if:◦ 20% or more of local ticks are Bb+ (this is generally true in East
only)◦ The patient presents within 72 hours of Ixodes bite◦ The tick was attached for 36 hours or more.◦ No contraindication to doxy
Analysis of ticks to determine whether they are infected is not recommended.

Early local infection◦ Skin - EM◦ CNS
Early disseminated infection◦ Skin
Multifocal EM Lymphocytoma cutis (Europe)
◦ Heart Heart block
◦ Musculoskeletal◦ Nervous System◦ Ocular
Conjunctivitis Late stage infection
◦ Skin◦ Musculoskeletal
Oligoarticular arthritis◦ Nervous system◦ Eye
uveitis

EM:◦Erythema migrans appears 3-30 (usually
7-10) days after tick bite, commonly on thigh, groin, axilla.
◦EM recognized in 70% of patients with objective evidence of B. burgdorferi infection.
◦Early symptoms may include fever, malaise, headache, myalgias, arthralgias, meningismus.

Erythema migrans◦ Clinical diagnosis – testing not indicated◦ Annular or macular◦ History of tick bite in only 25% of cases◦ Location: Skin/folds and creases◦ By definition at least 5 cm in size (controversial)◦ Lesions may grow 2-3 cm/day◦ Multiple EM reflective of disseminated disease
(hematogenous)



Multiple EM 3-5 weeks after tick bite.
Cranial nerve palsies (especially facial nerve—can be bilateral).
Aseptic meningitis.
Carditis 5% (AV block).
Myalgias, arthralgias, headache, fatigue.
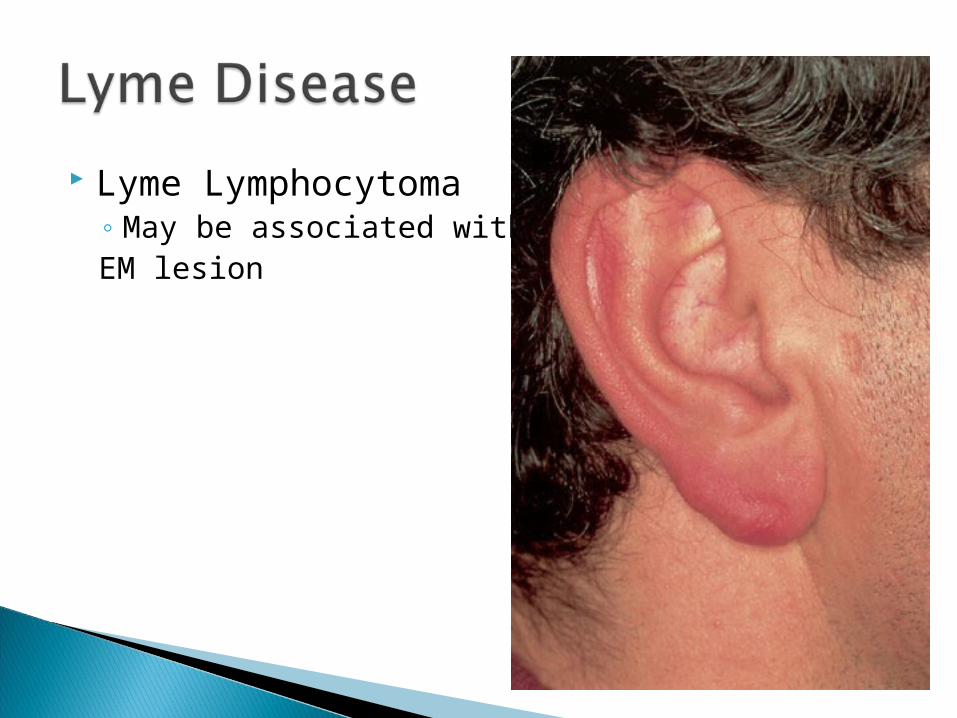
Lyme Lymphocytoma◦ May be associated withEM lesion

80% of untreated patients will develop some manifestation of late disease
Arthritis (mono- or oligoarticular, affecting large joints, especially the knee).
Encephalitis/encephalopathy. Polyradiculopathy.

Early local infection (<30 days)◦ EM with CNS seeding (HA, stiff neck, cognitive
difficulties)◦ Flu like syndrome with CNS seeding
Early disseminated infection (<3 mo)◦ Aseptic meningitis◦ Meningoencephalitis (acute cerebellar ataxia,
acute myelitis)◦ Cranial nerve palsy (facial)◦ Acute painful radiculoneuritis

Late persistent infection (>3 mo)◦ Encephalopathy◦ Chronic axonal polyradiculoneuropathy◦ Chronic encephalomyelitis

4-10% of Lyme Disease patients develop carditis
AV block◦ 40% Wenkebach◦ 50% complete
Myocardial involvement

Emerges in 60% of untreated EM within 6 months average
Intermittent attacks Asymmetrical Usually large joints especially the knees May involve the TMJ

No formal definition: persistent (predominantly neurologic) subjective symptoms that date to initial Lyme disease illness
Most likely heterogeneous and multifactorial causes involved◦ Persistent infection◦ Post infectious immune/inflammatory syndrome◦ Co infection◦ Reinfection◦ Fixed deficits◦ Alternative diagnosis◦ Hypochondriasis
Most patients do not respond to antibiotics Medical Clinics of NA 2002;86(2)

Erythema migrans is the only manifestation of Lyme sufficiently diagnostic to be clinically diagnosed without lab testing
Serology (ELISA)◦ Only 30-40% of patients with EM have a positive
serology.◦ IgM antibodies appear in 3-4 weeks, may persist
despite treatment.◦ IgG antibodies appear in 6-8 weeks, usually
remain detectable for many years.◦ 2-4 weeks after acute reaction 70-80% are
positive Western blot
◦ Indicated for positive or equivocal ELISA.◦ IgM is only diagnostic within the first month of
illness.

Up-To-Date 2004

False positive◦ Other spirochete (syphilis)◦ Cross reaction with other bacterial heat shock
protein (RMSF, Ehrlichia)◦ RA◦ SLE◦ Mononucleosis

IFA: At least as sensitive and specific as the ELISA
Immune assays of CSF◦ ELISA

TEST SENSITIVITY SPECIFICITY
ELISA/IFA (early) 59% 93%
ELISA/IFA (late) 95% 81%
ELISA/IFA + WB (early + late)
50-75% 99-100%
Cultivation◦ Barbour-Stoenner-Kelly (BSK) broth medium◦ Sensitive for detection of early-phase infection
(EM)◦ Limited value for detection of infection during late
stages◦ Very few places can do this◦ Skin biopsy or blood taken within first 2-3 weeks
of infection

Histology◦ Numbers of B. burgdorferi in tissues is low◦ Very hard to find on specimens◦ Silver stain
PCR◦ Limited places are able to do this◦ Urine PCR is available but there is insufficient
evidence of its accuracy, predictive value, or its significance
◦ Unclear of benefit of this test

Early localized◦ Doxycycline 100 bid or amoxicillin 500 tid or
Cefuroxime 500 mg po bid x 14-21 days.
Early disseminated◦ Isolated facial nerve palsy/mild carditis:
doxy/amoxicillin.◦ Meningitis/severe carditis: ceftriaxone 2gm qd x
14-28 days.
Late disease◦ Arthritis: doxycycline or amoxicillin or ceftrixaone
or IV PCN x 28 days.◦ Recurrent arthritis: ceftriaxone.◦ CNS disease: ceftriaxone or IV PCN.◦ Facial palsy alone: oral meds may be enough

Cardiac◦ 1st degree AV block: oral meds◦ High degree AV block: Ceftriaxone for 14-21 days
or IV PCN for 28 days































