Embed Size (px)
Citation preview

Clinical biochemistry
The hypothalamus andpituitary gland

GENERAL PRINCIPLES OFENDOCRINEDIAGNOSISA hormone can be defined as a substance secreted
by an endocrine gland that is transported in theblood, therebyregulating the function of another tissue(s). Ex.GH,T4,INSULIN and rout of secretion fromglands. • Conversely, trophic hormones from the
pituitary gland stimulate target endocrineglands to synthesize and secrete further

Endocrine glands may secrete excessive ordeficient amounts of hormone. Abnormalities of target glands may beprimary or secondary to dysfunction of thecontrolling mechanism, usually located inthe hypothalamus or anterior pituitarygland.
Hormone secretion may varyHormone secretion may vary

It is also important to know about the assay’s performance,as sometimes heterophilic interfering antibodies may cross-react with various hormones, as can certainimmunoglobulins, for example macroprolactin If the resultsof preliminary tests are definitely abnormal, this may beprimary or secondary to a disorder of one of the controllingmechanisms. if the results be equivocal when considered together withthe clinical findings, so-called ‘dynamic’ tests should becarried out.

dynamic’ testsSuppression tests are used mainly for thedifferential diagnosis of excessive hormonesecretion.The substance (or an analogue) that normallysuppresses secretion by negative feedback isadministered and the response is measured. Failure to suppress implies that secretion is notunder normal feedback control (autonomoussecretion).

Stimulation tests are used mainly for the differentialdiagnosis of deficient hormone secretion. The trophic hormone that normally stimulatessecretion is administered and the response ismeasured. A normal response excludes an abnormality of thetarget gland, whereas failure to respond confirms it.

HYPOTHALAMUS ANDPITUITARY
GLANDThere are two lobes of pituitary gland anteriorand posterior lobes.both depend on hormones synthesized in thehypothalamus for normal function. The hypothalamus also has extensive neuralconnections with the rest of the brain.stress and some psychological disorders affectthe secretion of pituitary hormones and of thehormones from other endocrine glands

Control of posterior pituitary hormonesTwo structurally similar peptide hormones,antidiuretic hormone (ADH) –– and oxytocin, aresynthesized inthe hypothalamus and transported to pituitary stalkattached to specific carrier proteins – neurophysins.Then stored in the posterior pituitary gland and arereleased into the bloodstream under hypothalamiccontrol, together with neurophysin.Neurophysin has no apparent biological function andis rapidly cleared from plasma.


Antidiuretic hormone (arginine vasopressin) ismainly synthesized in the supraoptic nuclei of thehypothalamus and enhances water reabsorption fromthe collecting ducts in the kidneys . Oxytocin is synthesized in the paraventricular nucleiof the hypothalamus. It controls the ejection of milkfrom the lactating breast and may have a role ininitiating uterine contractions, It may be used therapeutically to induce labour.

Anterior pituitary hormones
There is no direct neural connection between thehypothalamus and the anterior pituitary gland.The hypothalamus synthesizes small molecules(regulating hormones or factors) that are carriedto the cells of the anterior pituitary lobe by thehypothalamic portal system. This network of capillary loops, which, afterpassing down the pituitary stalk, divide into asecond capillary network in the anterior pituitarygland, from where hypothalamic hormones
The cells of the anterior pituitary lobe canbeclassified simply by their stainingreactions as acidophils,basophils or chromophobes.Acidophils are of two cell types:lactotrophs, which secrete prolactin,somatotrophs, which secrete GH(somatotrophin).
These hormones, which are simple
Basophils secretehormones thataffect otherendocrine glands.The hypothalamiccontrol is mainly
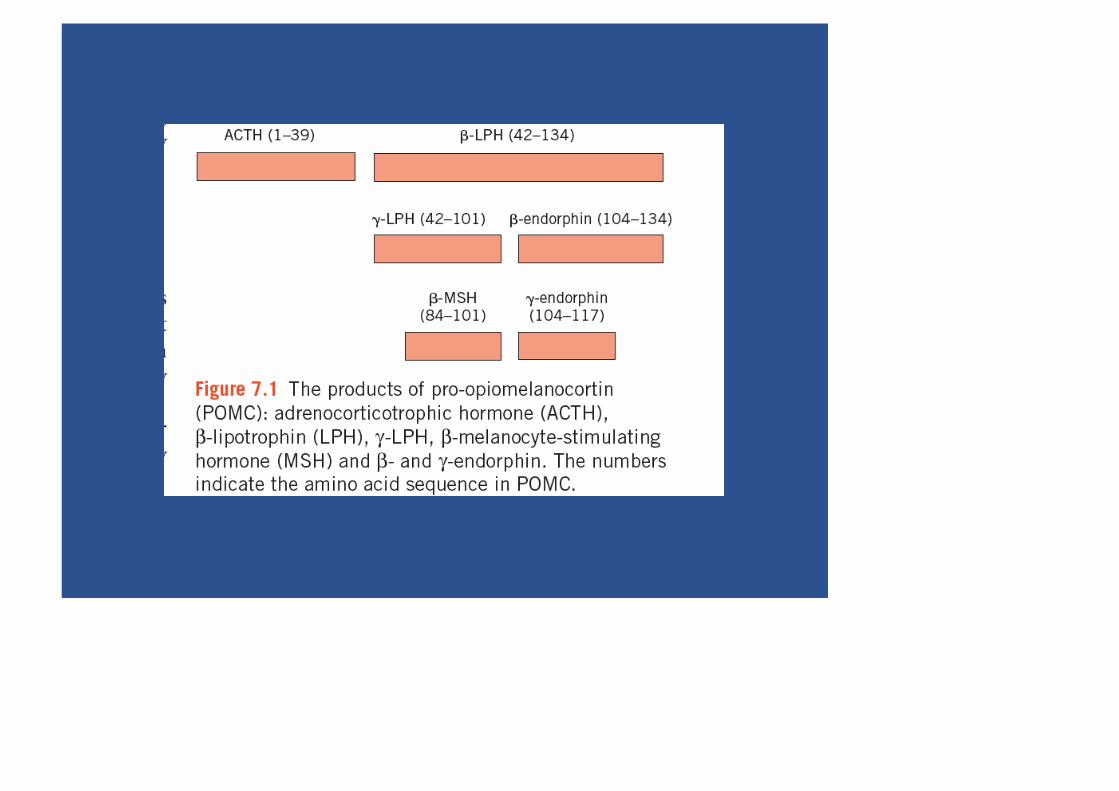
Part of the molecule has melanocyte-stimulatingactivity, and high circulating concentrations ofACTH are often associated with pigmentation. β-Lipotrophin is inactive until rapidly convertedto endorphins. These are neurotransmitters whichbecause they have opiate-like effects, helpcontrol pain

. Gonadotrophs secrete the gonadotrophins,folliclestimulating hormone (FSH) and luteinizinghormone (LH), which act on the gonads.Thyrotrophs secrete TSH (thyrotrophin), which actson the thyroid gland. These hormones are structurally similar glycoproteinsconsisting of two subunits, α and β. The α -subunit iscommon to all three hormones; the β -subunit isimportant for receptor recognition.Chromophobes, once thought to be inactive, docontain secretory granules.


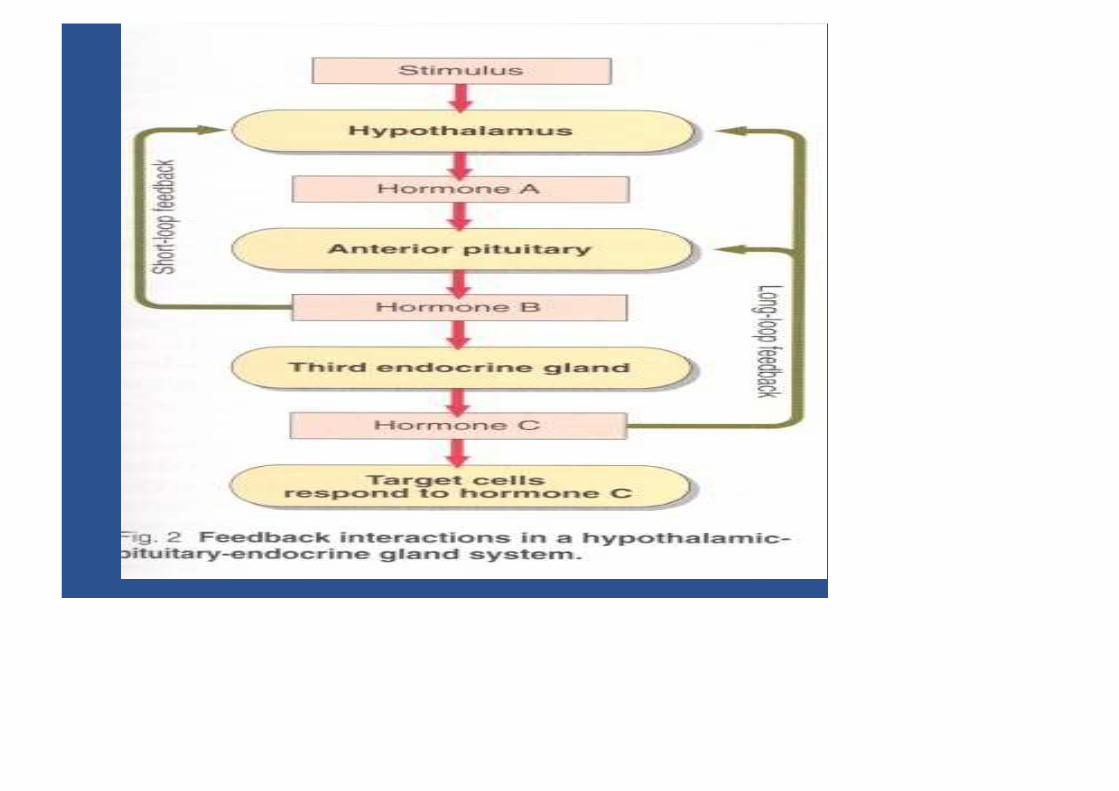
Extra hypothalamic neural stimuli modify, and attimes over-ride, other control mechanisms.Physical or emotional stress and mental illnessmay give similar findings to, and evenprecipitate, endocrine disease.The stress caused by insulin-inducedhypoglycaemia is used to test anterior pituitaryfunction.Stress may also stimulate the secretion of ADHfrom the posterior pituitary.
Feedback control is mediated by theconcentrations ofcirculating target-cell hormones; a risingconcentrationusually suppresses trophic hormone secretion. This negative feedback may directly suppresshypothalamic hormone secretion or may modifyits effect on pituitary cells (long feedback loop).The secretion of hypothalamic hormones may

2-Inherent rhythms: hypothalamic, andconsequentlypituitary, hormones are released intermittently,eitherin pulses or in a regular circadian rhythm. Disturbances of such rhythms may be ofdiagnostic value. 3-Drugs may also stimulate or block the actionof neurotransmitters, such as catecholamines,acetylcholine and serotonin, and influence the

• Certain neuroleptic drugs, such aschlorpromazine and haloperidol, interfere withthe action of dopamine. This results in reducedGH secretion
(reduced effect of releasing factor) and increasedprolactin secretion (reduced inhibition). • Bromocriptine, which has a dopamine-like
action, and levodopa, which is converted todopamine, have the opposite effect in normalsubjects.
• Bromocriptine causes a paradoxicalsuppression of excessive GH secretion in

Evaluation of anterior pituitaryfunction
The diagnosis of suspected hypopituitarism isbest excluded by the direct measurement ofpituitary hormones after stimulation or bydemonstrating target gland hyposecretion afterthe administration of the relevant trophichormone.
However, prolonged hypopituitarism may resultin secondary failure of the target gland withdiminished response to stimulation.Laboratory tests establish only the presence orabsence of hypopituitarism, and the cause mustbe sought by other clinical means such asradiological imaging
DISORDERS OF ANTERIORPITUITARY
HORMONE SECRETIONThe main clinical syndromes associated withexcessive or deficient anterior pituitary hormonesecretion are shown in Table 7.1.Excessive secretion usually involves a singlehormone, but deficiencies are often multiple.However, many pituitary tumours are non-secretory and may present clinically with eyesigns or headaches.


Growth hormoneGrowth hormone secretion from the anteriorpituitary gland is mainly controlled byhypothalamic GH releasing hormone (GHRH).After synthesis by the hypothalamus, this istransported via the hypothalamic portal system tothe somatotrophs of the anterior pituitary.Secretion of GHRH, and therefore of GH, ispulsatile, occurring about seven or eight times aday, usually associated with:

• exercise,• onset of deep sleep,• in response to the falling plasma glucose
concentration about an hour after meals. At other times, plasma concentrations are usuallyvery low or undetectable, especially in children. Growth hormone release is inhibited in anegative feedback pathway by another
Somatostatin is found not only in thehypothalamus and elsewhere in the brain, butalso in the gastrointestinal tract and pancreaticislet cells, where it inhibits the secretion of manygastrointestinal hormones. Insulin like growth factor 1 (IGF-1) acts byfeedback to inhibit GHRH action.
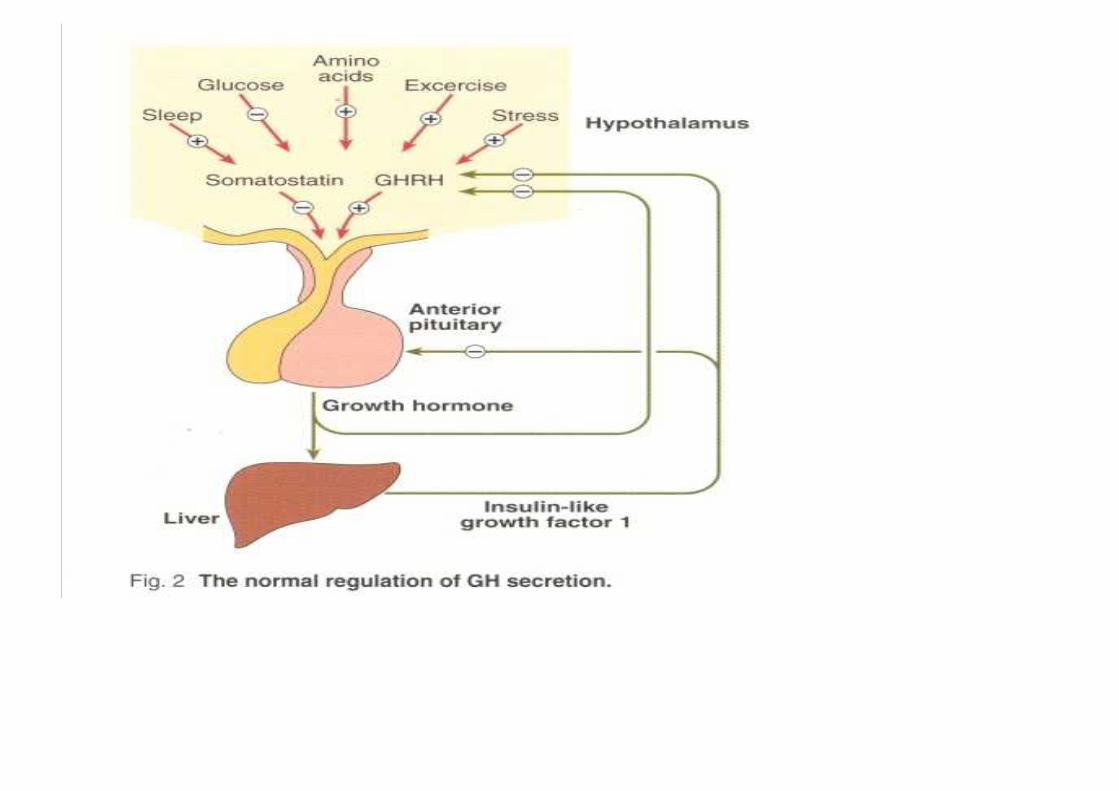

Growth hormone secretion may be stimulatedby:• stress, one cause of which is hypoglycaemia,• glucagon,• some amino acids, for example arginine,• drugs such as levodopa and clonidine.All these stimuli have been used to assess GHsecretory capacity, which may also be impairedin obese patients, in hypothyroidism andhypogonadism, in some cases of Cushing’ssyndrome and in patients receiving large doses of
Actions of growth hormoneaction is primarily mediated by IGFs,polypeptides that are synthesized in manytissues, where they act locally.Plasma concentrations of one of these, IGF-1(also known as somatomedin C), correlate withGH secretion.Carbohydrate metabolism is affected by GH: GHantagonizes the insulin-mediated cell uptake ofglucose,and excess secretion may produce glucoseintolerance.Fat metabolism is stimulated by GH: lipolysis is
The production of IGF-1 is also influenced byotherfactors, the most important of which isnutritional status.In undernutrition, plasma concentrations arelow, whereas GH concentrations are elevated,suggesting that plasma IGF-1 may influence GHsecretion by negative feedback.Other factors, such as adequate nutrition and T4,are also needed for normal growth.

Growth hormone excess: gigantismand acromegaly
Growth hormone excess causes gigantism duringchildhood and acromegaly in adults.Most patients with GH excess have acidophiladenomas of the anterior pituitary gland, whichmay be secondary to excessive hypothalamicstimulation.Rarely, malignant tumours may release GH orGHRH.

• Acromegaly is sometimes one of themanifestations of multiple endocrine neoplasia(MEN).
• The clinical manifestations of GH excessdepend on whether the condition developsbefore or after fusion of the bony epiphyses.
• Gigantism is caused by excess GH secretion inchildhood before fusion of the epiphysealplates, which may be delayed byaccompanying hypogonadism.
• Heights of up to about 2 metres may be
The features of acromegaly mayinclude the following;
• An increase in the bulk of bone and soft tissueswith enlargement of, for example, the hands,tongue, jaw and heart.
Changes in facial appearance , due to theincreasing size of the jaw and sinuses;Excessive hair growth, hyperhidrosis andsebaceous gland secretion are common.

• Menstrual disturbances are common infemales.
• Impaired glucose tolerance is present inabout25 per cent of patients, about half ofwhom develop symptomatic diabetes mellitus.In most cases the pancreas can secrete enoughinsulin to overcome the antagonistic
• Hyperphosphataemia, hypercalcaemia and
hypertriglyceridaemia may also be present.• Many of these features are due to the action of
IGF-1, which acts as a general growth factor.• Compression of the optic chiasma may cause
visual field defects such as bitemporalhemianopsia.

• If destruction of the gland progresses, other
anterior pituitary hormones such as ACTH,LH, FSH and TSH may become deficient .
• Plasma prolactin concentrations may,however, be raised as prolactin differs from allother pituitary hormones in its method ofcontrol.
• Secretion is inhibited, not stimulated, bydopamine; therefore, impairment ofhypothalamic control causeshyperprolactinaemia.
Diagnosis• The diagnosis of GH excess is suggested by the
clinical presentation, biochemical tests andradiological findings of the pituitary.
• Magnetic resonance imaging (MRI) is more
sensitive than computerized tomography (CT)scanning.
• Random GH measurements are often not
diagnostic owing to episodic secretion and a

• The diagnosis is confirmed by demonstrating a
raised plasma GH concentration that is notsuppressed by a rise in plasma glucoseconcentration.
• In normal subjects, plasma GH concentrationsfall to very low levels – to below 1 mg/L aftera 75 g oral glucose load.
• In acromegaly, the secretion of GH isautonomous and this fall may not occur or beonly slight, or there may even be a paradoxicalrise.
• Growth hormone secretion is inhibited by

Glucose suppression test forsuspected acromegaly
• ProcedureAfter an overnight fast,insert IV canula, After atleast 30 min why?, take basal samples for plasmaglucose and GH estimation.The patient should drink 75 g of glucosedissolved in about 300 mL of water, or anequivalent glucose load.Take samples for glucose and GH assays at 30,60, 90 and 120 min after the glucose load hasbeen taken.

interpretation
In normal subjects, plasma GH concentrationsfall to undetectable levels.Although failure to suppress suggestsacromegaly or gigantism, it may be found insome patients with severe liver or renal disease,in heroin addicts or in those taking levodopa. The plasma glucose concentrations maydemonstrate impaired glucose tolerance ordiabetes mellitus in acromegaly.• If acromegaly is confirmed, it is wise to
•• Plasma IGF-1 has a long half-life and may be
used in screening for acromegaly. • Plasma concentrations correlate with the
activity of the disease.• Measurement of the plasma concentrations of
GH, or of IGF-1, may be used to monitor theefficacy of treatment.
• Remember that pregnancy increases IGF-1concentration, and starvation, obesity anddiabetes mellitus decrease it.

• Insulin-like growth-factor-binding protein-3 is
the main binding protein for IGF-1 and itsconcentration is also increased in acromegaly.
• Sometimes plasma GHRH concentrations areuseful and can be raised where there is anectopic source or may be suppressed inpituitary disease.
• Computerized tomography or MRI bodyscanning may help to find an ectopic source ofGH or GHRH.
Treatment
• 1-surgery to remove the adenoma,• 2-medical therapy, usually with either
bromocriptine or cabergoline (dopaminereceptor agonists)
• or somatostatin analogues (somatostatin itselfhas too short a half-life for effectivetherapeutic use).
• Octreotide or lanreotide, which bind tosomatostatin receptors, can be used orpegvisomant (GH receptor antagonist).
• 3-Radiation therapy.

Growth hormone deficiency• In adults, GH deficiency may cause clinical
symptoms, such as tiredness, dyslipidaemiaand increased cardiovascular disease.
• Growth hormone deficiency can cause shortstature in children.
• It is important to investigate children withreduced growth rate to identify those who maybenefit from recombinant human GHreplacement treatment.
• Isolated GH deficiency is most commonlysecondary to idiopathic deficiency ofhypothalamic GHRH.
Diagnosis• It is, important to exclude hypothyroidism,
chronic diseases and malabsorption states,poor nutritional state and failure to thrive.
• Clinical examination should assess for obvioussyndromes, pubertal status, bone age, growthor growth velocity .
• Karyotyping may be indicated if achromosomal disorder such as Turner’ssyndrome (45,X0) is suspected.
• There is a physiological reduction in GHsecretion at the end of pre-puberty. Thus, inchildren with bone age more than 10 years,
• Plasma GH concentrations in normal childrenare often low and assays under basalconditions rarely exclude the diagnosis.
• A low plasma IGF-1 concentration may be auseful screening test.
• Urinary GH excretion, either in 24-hcollections or timed overnight, may offer arelatively safe screening test.
• If blood is taken at a time when
physiologically high concentrations are
• If GH deficiency is not excluded by the above
measurements, it is necessary to perform oneor more stimulation tests.
• The response of GH to insulin may be themost reliable to detect GH deficiency, but it isnot without the risk of fatal hypoglycaemia.
• Glucagon could also be used as an alternative(see Glucagon stimulation test of thehypothalamus–pituitary axis).
• A GH absolute response of greater than 20mU/L (7 µg/L) makes GH deficiency unlikely.
• Other such stimuli include arginine, clonidine
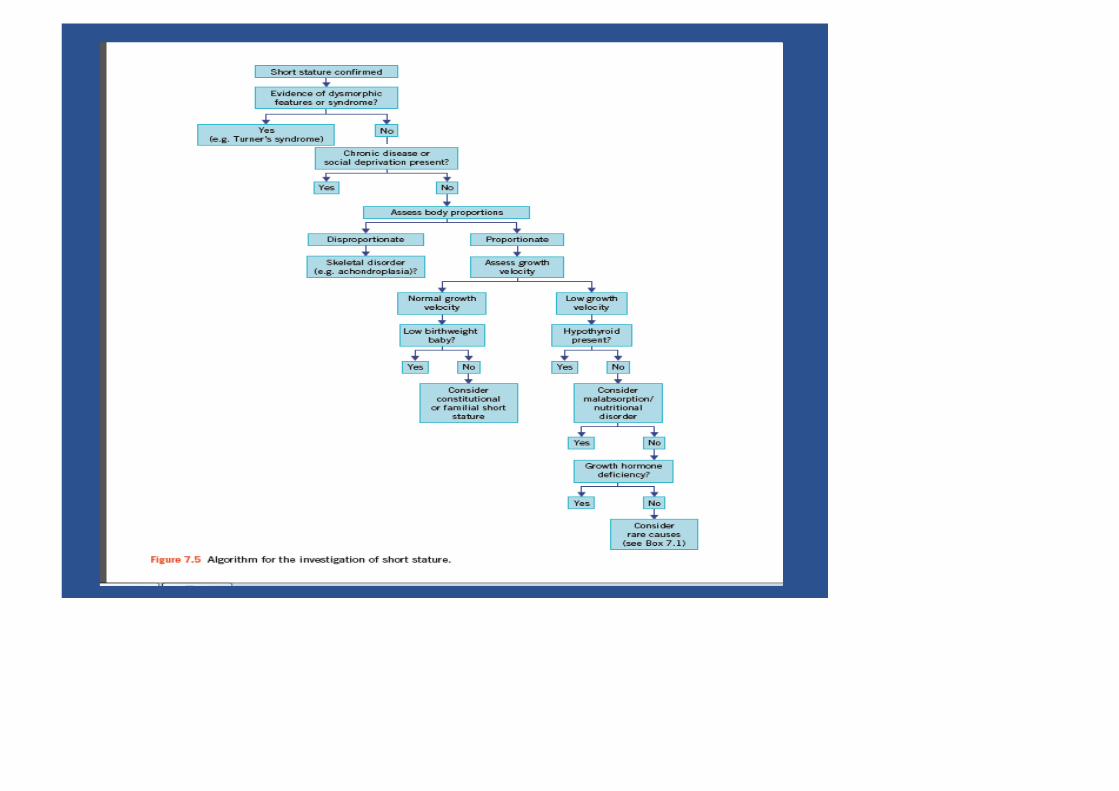
• Figureshows an algorithmfor the investigationof short stature.
DISORDERS OF POSTERIORPITUITARY
HORMONE SECRETION• Disorders of the posterior pituitary are rarecompared with those of the anterior pituitary.
• Deficiency of ADH in diabetes insipidus maypresent as polyuria.
• In the syndrome of inappropriate ADH,hyponatraemia due to water excess occurs.

HYPOPITUITARISM
• Hypopituitarism is a syndrome of deficiency ofpituitary hormone production that may resultfrom disorders of the hypothalamus, pituitaryor surrounding structures.
• Clinical features of deficiency are usually
absent until about 70 % of the gland has beendestroyed, unless there is associatedhyperprolactinaemia, when amenorrhoea andinfertility may be early symptoms.
• Panhypopituitarism alludes to the involvement




• Panhypopituitarism with the full clinical
picture described below is uncommon.• Suspicion of anterior pituitary hypofunction
usually arises in patients presenting withvarious features such as clinical andradiological evidence of a pituitary or localizedbrain tumour,
• hypogonadism, adrenocortical insufficiency,short stature caused by GH deficiency, andhypothyroidism.
• Gonadotrophins are often the first to decreasein hypopituitarism and it is unusual for the

Consequences of pituitaryhormonedeficiencies• Progressive pituitary damage usually presents
with evidence of deficiencies ofgonadotrophins and GH.
• Plasma ACTH and/or TSH concentrations
may remain normal, or become deficientmonths or even years later.

The clinical and biochemical consequences of thetarget-gland failure include the following:
• Growth retardation in children This may bedue to deficiency of GH; deficiency of TSH,and therefore of thyroid hormone, maycontribute.
• Secondary hypogonadism This is due togonadotrophin deficiency, presenting asamenorrhoea, infertility and atrophy ofsecondary sexual characteristics with loss ofaxillary and pubic hair and impotence or lossof libido. Puberty is delayed in children.
• Secondary adrenocortical hypofunction
• However, cortisol is needed for normal freewater excretion, and consequently there maybe a dilutional hyponatraemia due to cortisoldeficiency.
• Cortisol is also necessary for the maintenanceof normal blood pressure. Hypotension may beassociated with ACTH deficiency.
• Cortisol and/or GH deficiency may causeincreased insulin sensitivity with fastinghypoglycaemia.
• Secondary hypothyroidism (TSH deficiency)This may sometimes be clinicallyindistinguishable from primaryhypothyroidism.
• Prolactin deficiency Associated with failure tolactate, this may occur after post-partumpituitary infarction (Sheehan’s syndrome).
• However, in hypopituitarism due to a tumour,plasma prolactin concentrations are oftenraised and may cause galactorrhoea (secretionof breast fluid).

Pituitary tumours
• The clinical presentation of pituitary tumoursdepends on the type of cells involved and onthe size of the tumour (microadenomas lessthan 10 mm and macroadenomas more than 10mm).
• Tumours of secretory cells may produce theclinical effects of excess hormone secretion:
• excess prolactin causes infertility,amenorrhoea and varying degrees ofgalactorrhoea .
• excess GH causes acromegaly or gigantism,
• Non-secreting tumours are difficult to diagnoseusing biochemical tests, although thecombined pituitary stimulation test mayindicate subclinical impairment of function.
• Hyperprolactinaemia, which may beasymptomatic, is a valuable biochemicalmarker of the presence of a pituitary tumour.
• Prolactin may be secreted by the tumour cellsor by unaffected lactotrophs if tumour growthinterferes with the normal inhibition ofprolactin secretion

Investigation of suspectedhypopituitarism
• Deficiency of pituitary hormones causeshypofunction of the target endocrine glands.
• Investigation aims to confirm such deficiency,to exclude disease of the target gland and thento test pituitary hormone secretion aftermaximal stimulation of the gland.
• Measurement should be made of the plasmaconcentrations of:
• LH, FSH and oestradiol (female) ortestosterone (male),
• total or free T4 and TSH,
• If the plasma concentration of the target glandhormone is low and the concentration oftrophic hormone is raised, the affected targetgland should be investigated.
• Conversely, if the plasma concentrations ofboth the target gland and trophic hormones arelow or low-normal, consider a pituitarystimulation test .
• Investigation of the pituitary region usingradiological techniques such as CT or MRIscanning may help elucidate a cause of the

Insulin tolerance or insulinstimulation test
• This test is potentially dangerous and must bedone under direct medical supervision due tosevere hypoglycaemia and the test should becarried out only in specialist units byexperienced staff.
• It is contraindicated in the following patientgroups: the elderly, patients with ischaemicheart disease, epilepsy or severepanhypopituitarism, and patients in whomplasma cortisol at 09.00 h is less than 100nmol/L.

• A resting electrocardiogram should be normal.• Hypothyroidism should be treated before hand
as this can impair the cortisol and GHresponses.
• However, note that treatment with thyroxinecan precipitate an adrenal crisis in suchpatients and thus corticosteroid replacement isalso necessary.
• Indications of the insulin stimulation test mayinclude:
• assessment of GH in growth deficiency,

Procedure• After an overnight fast, fter at least 30 min,
take basal samples at time 0 min for cortisol,GH and glucose.
• Inject soluble insulin in a dose sufficient tolower plasma glucose concentrations to lessthan 2.5 mmol/L and evoke symptomatichypoglycaemia.
• The recommended dose of insulin must beadjusted for the patient’s body weight and forthe suspected clinical condition under

Interpretation
• Interpretation is not possible if hypoglycaemiais not attained, and the dose of insulin cancautiously be repeated if this is not attained inthe 45-min blood sample.
• If hypoglycaemia has been adequate, plasmacortisol concentrations should rise by morethan 200 nmol/L and exceed 580 nmol/L, andan adequate GH response occurs with anabsolute response of greater than 20 mU/L (7µg/L).
• In Cushing’s syndrome, neither plasma

Glucagon stimulation test of thehypothalamus–pituitary axis• This test is useful if the insulin hypoglycaemic
test is contraindicated.• However, it is essential that the test is carried
out in a specialist unit by experienced staff.• The basic principle is that glucagon stimulates
GH and ACTH release probably via ahypothalamic route.
• The test is contraindicated if there is severeadrenal failure, for example if cortisol at 09.00h is less than 100 nmol/L or inhypothyroidism.

• Procedure• Patients should fast overnight, although they
can drink water.• For adults, 1 mg of glucagon is injected
subcutaneously at 09.00 h.• Blood samples are taken at 0, 90, 120, 150,
180, 210 and 240 min for cortisol and GH.
• Interpretation• Plasma cortisol should normally rise by at least
200 nmol/L to more than 580 nmol/L, and anadequate GH response occurs with an absoluteresponse of greater than 20 mU/L (7 µg/L).

• Treatment of hypopituitarism• This consists of specific therapy depending on
its cause and may include surgical removal ofa large adenoma.
• If the ACTH axis is impaired, it is essential toprescribe a glucocorticoid, for examplehydrocortisone in the acute situation orprednisolone for maintenance.
• Secondary hypothyroidism will need thyroidreplacement. Adrenal replacement shouldprecede T4 therapy to avoid an Addisonian






























