Embed Size (px)
Citation preview
ªï∑ ’Ë 26 ©∫ —∫∑ ’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2548 ∫∑∫√√≥“∏ ‘°“√: Unplaned Extubationœ 75
ªí≠À“¢Õß°“√∂Õ¥∑àՙ૬À“¬„®‚¥¬‰¡àµ—Èß„® ‡ªìπªí≠À“∑’Ë “¡“√∂ –∑âÕπ∂÷ߧÿ≥¿“æ¢Õß°“√√—°…“欓∫“≈„πÀÕÕ¿‘∫“≈ºŸâªÉ«¬«‘°ƒµ‰¥â1,2 ´÷ËßÕ—µ√“°“√∂Õ¥∑ àՙ૬À“¬„®‚¥¬‰¡àµ— Èß„®π — Èπ æ∫‰¥â√ âÕ¬≈– 3-16 ”À√ —∫ª√–‡∑»„π‡Õ‡™’¬Õ“§‡π¬åπ—Èπ¡’Õÿ∫—µ‘°“√≥åª√–¡“≥√âÕ¬≈–
8.7-22.53,4 °“√»÷°…“¥—ß°≈ à“«¢â“ßµâπ‰¥â√«∫√«¡∂ ÷ßªí®®—¬‡ ’ˬߵàÕ°“√∂Õ¥∑àÕ (µ“√“ß∑’Ë1) ·π«∑“ß°“√·°â ‰¢(µ“√“ß∑ ’ Ë 2) ·≈–·π«‚π â¡¢ÕߺŸâªÉ«¬∑ ’ ËÕ“®µâÕß„ à∑ àՙ૬À“¬„®Õ’° (µ“√“ß∑’Ë 3)
«“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫—¥«‘°ƒµThai Journal of TuberculosisChest Diseases and Critical Care
UNPLANNED EXTUBATION : AN UNWANTEDEVENT THAT WE CANNOT DENY
∫∑∫√√≥“∏‘°“√
µ“√“ß 3 ·π«‚πâ¡¢ÕߺŸâªÉ«¬∑’ËÕ“®µâÕß„ à∑àՙ૬À“¬„®
Higher pre-extubation FiO2 (FiO2 > 50%) lower PaO2/FiO2 ratio < 200 )3,6,7,8
Higher ventilatory requirements7
Higher APACHE II score3
Type of mechanical ventilatory support (full ventilatory support)9
“‡Àµÿ¢Õß°“√„ à∑àÕ®“°‚√§ pneumonia10
µ“√“ß∑’Ë 1 ªí®®—¬‡ ’ˬߵàÕ°“√∂Õ¥∑àՙ૬À“¬„®
®”π«π欓∫“≈‰¡à‡æ’¬ßæÕ4
Anxiety, insufficient sedation5
History of previous unplanned extubation2
µ“√“ß∑’Ë 2 ·π«∑“ß°“√·°â ‰¢
ªí≠À“ ·π«∑“ß°“√·°â‰¢
ª√ —∫®”π«π 欓∫“≈: ºŸ âªÉ«¬ „Àâ‡À¡“– ¡®—¥°“√»÷°…“µàÕ‡π◊ËÕ߇æ ◊ËÕ‡æ‘Ë¡æŸπ∑ —°…–4
ª√–‡¡‘π‚¥¬„™â motor activity assessmentscales (MAAS)5 ·≈–ª√ —∫¬“„Àâ‡À¡“– ¡∑” CQI ‚¥¬¡ÿàß∑’Ë ®—¥¡“µ√∞“π¢Õß°“√∑”ß“π,‡æ‘Ë¡∑ —°…–„π¥â“π°“√ ◊ ËÕ “√·≈–§—¥°√ÕߺŸâªÉ«¬∑’Ë¡’ªí®®—¬‡ ’ˬ߷≈–„Àâ°“√‡ΩÑ“√–«—ßÕ¬à“ß„°≈♑¥1
®”π«π欓∫“≈‰¡à‡æ’¬ßæÕ
ºŸâªÉ«¬ anxiety
√—∫‰«âµ’æ‘¡æ凡 ◊ËÕ«—π∑’Ë 1 ‡¡…“¬π 2548

76 Õ¥‘»√ «ß…“ «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
°“√¥Ÿ·≈ºŸ ⪠ɫ¬„πÀÕÕ¿‘∫“≈ºŸ ⪠ɫ¬« ‘°ƒµ„πª√–‡∑»‰∑¬ °Á¥”‡π ‘πµ“¡¡“µ√∞“π “°≈·≈–æ∫ºŸâªÉ«¬∑ ’ Ë∂Õ¥∑ àՙ૬À“¬„®‚¥¬‰¡àµ—Èß„®Õ¬Ÿà∫ àÕ¬§√ — Èß ·µà¬—߉¡à¡’°“√»÷°…“·≈–√“¬ß“π‡ªìπ∑’Ë™—¥‡®π ‡ªìπ∑’Ëπ à“¬‘π¥’∑’Ë πäÕµ‡µ™–«—≤π«√√≥“ ·≈–§≥–11 ‰¥â∑”°“√»÷°…“·≈–√“¬ß“πÕÿ∫ —µ‘°“√≥ å∑ ’ ˇ°‘¥¢÷Èπ æ√ âÕ¡∑ — È߉¥â«‘‡§√“–Àå∂ ÷ßªí®®—¬‡ ’ ˬ߷≈–ªí®®—¬∑ ’ ˙૬∫ àß™’È∂ ÷ß°“√µâÕß„ à∑ àՙ૬À“¬„®´È” °“√»÷°…“π’Èæ∫«à“Õ—µ√“°“√‡°‘¥¿“«–∑’Ë∂Õ¥∑ àՙ૬À“¬„®‚¥¬‰¡àµ—Èß„®Õ¬Ÿà∑’Ë√ âÕ¬≈– 4.9 ´÷ËßÕ¬Ÿà„π‡°≥±å∑’Ëæ∫‰¥âµ“¡¡“µ√∞“π ·≈–ªí®®—¬‡ ’ ˬßÀ≈ —°∑ ’ Ëæ∫§ ◊Õ√–¥—∫§«“¡√ Ÿ â ÷°µ—«∑ ’ ˇ√ ‘ Ë¡‡Õ–Õ–«ÿà𫓬 (motor activityassessment scales √–¥—∫ 4-6) √ à«¡°—∫‰¥â√—∫¬“ ß∫ª√– “∑‰¡à‡æ’¬ßæÕ ¢âÕ¡Ÿ≈¥—ß°≈ à“«π ’ È “¡“√∂π”¡“ª√–¬ÿ°µå„™â°—∫ºŸ âªÉ«¬„πª√–‡∑» √«¡∑ — Èߙ૬„Àâ°“√æ—≤π“§ÿ≥¿“æ°“√∫√ ‘°“√·≈–¡“µ√°“√¥Ÿ·≈ºŸâªÉ«¬„À⥒¢÷Èπ1,2 πÕ°®“°π ’ Ȭ—ßæ∫ºŸâªÉ«¬∑ ’ Ë¡’ minute v entilation Ÿß (>10 ≈ ‘µ√/π“∑ ’) ®–¡’·π«‚π â¡∑ ’ ˵âÕß°≈ —∫¡“„ à∑ àՙ૬À“¬„®Õ’° ¥—ßπ — Èπ∫∑§«“¡π ’ È®÷ß “¡“√∂π”¡“ª√ —∫„™âµ“¡ ∂“π°“√≥å„π·µà≈–∑’Ë ‰¥â ·µà ‘Ëß∑’ËÕ“®µâÕߧ”π÷ß√ à«¡§ ◊Õ Õ—µ√“ à«π¢Õß·æ∑¬å·≈–欓∫“≈µàÕºŸâªÉ«¬ √«¡∑ — Èß∑ —°…–„π°“√¥Ÿ·≈∑ ’ Ë·µ°µà“߉ª °“√𔉪ª√–¬ÿ°µå„™â®√ ‘ß®÷ߧ«√‡°Á∫¢âÕ¡Ÿ≈‡æ ◊ ËÕ‡ª√ ’¬∫‡∑ ’¬∫«à“ ºŸâªÉ«¬„π°“√¥Ÿ·≈¢Õ߇√“π — Èπ¡’Õÿ∫ —µ‘°“√≥ 凰‘¥¢÷ Èπ„π™à«ß„¥¢Õß«—π ´÷ Ëß “¡“√∂ –∑ âÕπªí≠À“„π¥â“π∫ ÿ§≈“°√‰¥â ®÷ß®–∑”„Àâ°“√æ—≤π“§ÿ≥¿“懰‘¥¢÷Èπ‰¥â®√‘ß
Õ¥‘»√ «ß…“ æ.∫.°ÕßÕ“¬ÿ√°√√¡
«‘∑¬“≈—¬·æ∑¬»“ µ√åæ√–¡ß°ÿƇ°≈â“
‡Õ° “√Õâ“ßÕ‘ß1. Chiang AA, Lee KC, Lee JC, et al. Effectiveness of a
continuous quality improvement program aiming toreduce unplanned extubation: a prospective study.Intensive Care Med 1996; 22:1269-1271.
2. Maguire G P, De Lorenzo LJ, Moggio RA, et al.Unplanned extubation in the intensive care unit:a quality-of-care concern. Crit Care Nurs Q 1994;17:40-47.
3. Phoa LL, Pek WY, Syap W, et al. Unplanned extuba-tion: a local experience. Singapore Med J 2002; 43:504-508.
4. Yeh SH, Lee LN, Ho TH, et al. Implications of nursingcare in the occurrence and consequences of unplannedextubation in adult intensive care units. Int J NursStud 2004;41:255-262.
5. Devlin JW, Boleski G, Mlynarek M, et al. Motor activ-ity assessment scale: A valid and reliable sedationscale for use with mechanically ventilated patients inan adult surgical intensive care unit. Crit Care Med1999;27:1271-1275.
6. Chevron V, Menard JF, Richard JC, et al. Unplannedextubation: risk factors of development and predictivecriteria for reintubation. Crit Care Med 1998; 26:1049-1053.
7. Whelan J, Simpson SQ, Levy H, et al. Unplannedextubation. Predictors of successful termination of me-chanical ventilatory support. Chest 1994; 105:1808-1812.
8. Razek T, Gracias V, Sullivan D, et al. Assessing theneed for reintubation: a prospective evaluation of un-planned endotracheal extubation. J Trauma 2000.48:466-469.
9. Betbese AJ, Perez M, Bak E, et al. A prospectivestudy of unplanned endotracheal extubation inintensive care unit patients. Crit Care Med 1998;26:1180-1186.
10. Chen CZ, Chu YC, Lee CH, et al. Factors predictingreintubation after unplanned extubation. J Formos MedAssoc. 2002;101: 542-546.
11. Techawattanawanna N, Sittipunt C, Wongtim S,Udompanich V and Kawkitinarong K. Unplannedextubation in medical ICU. Thai J Tuberc Chest DisCrit Care 2548;26:89-100.
ªï∑’Ë 26 ©∫—∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2548 Therapeutic approach to septic shock 77
Septic shock ‡ªìπ¿“«–«‘°ƒµ∑’Ë¡’§«“¡ ”§—≠ ¡’Õÿ∫—µ‘°“√≥å Ÿß·≈–¡’Õ—µ√“µ“¬ Ÿß ·æ∑¬å·≈–∑’¡®–µâÕß„Àâ°“√√—°…“‚¥¬‡√Á«·≈–§√∫∂â«π„πª√–‡¥Áπµà“ßÊ ∑’Ë ”§—≠§◊Õ„À⬓ªØ‘™’«π–·≈–°”®—¥·À≈àß°“√µ‘¥‡™◊ÈÕ √ —°…“ª√–§—∫-ª√–§Õß„À⺟âªÉ«¬√Õ¥™’«‘µ (intensive life support)·≈–„™â¬“À√◊Õ “√∑’ˉª¬—∫¬—Èß inflammatory pathway „πseptic shock º≈°“√√—°…“®–¥’À√◊Õ‰¡à ¢÷ÈπÕ¬Ÿà°—∫«à“∑’¡¡’§«“¡√ Ÿ âæ ◊ Èπ∞“π‡°’Ë¬«°—∫欓∏ ‘ √ ’√«‘∑¬“ 欓∏ ‘«‘∑¬“¢Õß‚√§ °“√¥”‡π ‘π‚√§ °“√√ —°…“ µ≈Õ¥®π°“√ª√–‡¡‘π·≈–‡Ω Ñ“√–«—ߺ≈¢Õß°“√√ —°…“Õ¬à“ß∂ Ÿ°µâÕß ∫∑§«“¡π ’ È®–§√Õ∫§≈ÿ¡ª√–‡¥Áπ¥—ß°≈à“«‚¥¬‡πâπ„πª√–‡¥Áπ intensivelife support ·≈–¡’«—µ∂ ÿª√– ߧå„Àâ·æ∑¬å„Àâ°“√√ —°…“ºŸâªÉ«¬°≈ÿà¡π’ÈÕ¬à“ß∂Ÿ°µâÕß ·≈–¡’ª√– ‘∑∏‘º≈°“√√—°…“ Ÿß ÿ¥
§«“¡√Ÿâ‡∫◊ÈÕßµâπ‡°’Ë¬«°—∫ septic shock§”®”°—¥§«“¡1
Septic shock ‡ªìπ¿“«–™ÁÕ§∑ ’ˇ°‘¥®“° systemicinflammatory response ¢Õß√ à“ß°“¬Õ—π‡ªìπº≈¡“®“°°“√µ‘¥‡™◊ÈÕ√ÿπ·√ßÀ√◊Õ°“√¡’ inflammatory foci
®“° Consensus conference √–À«à“ß Ameri-can College of Chest Physician ·≈– Society ofCritical Care Medicine „πªï 1992 ‰¥â¡’°“√°”Àπ¥»—æ∑åÀ≈“¬§”∑ ’ˇ°’ˬ«¢âÕß°—∫°≈ÿà¡‚√§π ’È ¥—ßπ’È
Systemic inflammatory response syndrome(SIRS) ‡ªìπ¿“«–∑’˺ŸâªÉ«¬¡’°“√Õ—°‡ ∫·æ√à°√–®“¬∑—Ë« ʉª„π√ à“ß°“¬ (widespread inflammation) ‚¥¬¡’ “‡Àµÿ®“°°“√µ‘¥‡™◊ÈÕ À√◊Õ inflammatory stimuli Õ ◊Ëπʇ™àπ µ—∫ÕàÕπÕ—°‡ ∫ °“√∫“¥‡®Á∫√ ÿπ·√ß burns œ≈œ „π°“√«‘π‘®©—¬¿“«– SIRS ºŸâªÉ«¬®–µâÕß¡’Õ“°“√∑“ߧ≈‘π‘°¥—ßµàÕ‰ªπ’ÈÕ¬à“ßπâÕ¬ 2 ¢âÕ ‚¥¬°“√«‘π‘®©—¬‚¥¬„™âÕ“°“√∑“ߧ≈ ‘π ‘°π ’ È „™â ‰¥â‡©æ“–ºŸâªÉ«¬ºŸâ„À≠ à‡∑ à“π — Èπ ‰¡à “¡“√∂π”¡“„™â„πºŸâªÉ«¬‡¥Á°
1. Õÿ≥À¿Ÿ¡‘°“¬ ¡“°°«à“ 38oC À√◊ÕπâÕ¬°«à“ 36oC2. Õ—µ√“‡µâπ¢ÕßÀ—«„® ¡“°°«à“ 90 §√—Èß/ π“∑’3. Õ—µ√“°“√À“¬„®¡“°°«à“ 20 §√ — Èß/π“∑ ’ À√◊Õ
PaCO2 πâÕ¬°«à“ 32 ¡¡. ª√Õ∑4. ‡¡Á¥‡≈◊Õ¥¢“« 12,000 ‡´≈≈å/≈∫.¡¡. À√◊ÕπâÕ¬
°«à“ 4,000 ‡´≈≈ å/≈∫.¡¡.À√◊Õ¡’‡¡Á¥‡≈◊Õ¥¢“«™π‘¥ bandform ¡“°°«à“ 10%
Sepsis ®÷߇ªìπ à«πÀπ÷ËߢÕß ¿“«–SIRS §◊Õ®”°—¥‡©æ“–„π°≈ ÿà¡∑ ’Ë¡’°“√µ‘¥‡™ ◊ÈÕ‡ªì𠓇Àµÿ
Severe sepsis ‡ªìπ ¿“«– sepsis ∑ ’Ë¡’ Õ«—¬«–µà“ßÊ∑”ß“πº‘¥ª√°µ‘ (organ dysfunction) ¡’‡≈◊Õ¥‰ª‡≈ ’ ȬßÕ«—¬«–µà“ßÊ≈¥≈ß (hypoperfusion) À√◊Õ¡’§«“¡¥—π‚≈À‘µµË” (hypotension) „πºŸâªÉ«¬°≈ÿà¡π’È ·æ∑¬åÕ“®æ∫≈—°…≥–∑“ߧ≈‘π‘°‡™àπ lactic acidosis ªí “«–ÕÕ°πâÕ¬ À√◊Õ¡’√–¥—∫§«“¡√ Ÿâ µ‘‡ª≈’ˬπ·ª≈ß ‡ªìπµâπ
THERAPEUTIC APPROACH TO SEPTIC SHOCK
«“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫—¥«‘°ƒµThai Journal of TuberculosisChest Diseases and Critical Care
‰™¬√ —µπ å ‡æ‘Ë¡æ‘°ÿ≈ æ.∫.«√°“√ «‘‰≈™π¡å æ.∫.
“¢“«‘™“‡«™∫”∫ —¥«‘°ƒµ ¿“§«‘™“Õ“¬ÿ√»“ µ√å §≥–·æ∑¬»“ µ√ 廑√ ‘√“™æ¬“∫“≈
√—∫‰«âµ’æ‘¡æ凡◊ËÕ«—π∑’Ë 18 惻®‘°“¬π 2547
∫∑§«“¡æ‘‡»…
78 ‰™¬√—µπå ‡æ‘Ë¡æ‘°ÿ≈ ·≈– «√°“√ «‘‰≈™π¡å «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫—¥«‘°ƒµ
Septic shock ‡ªìπ¿“«– sepsis ∑ ’˺ŸâªÉ«¬¬—ߧߡ’§«“¡¥—π‚≈À‘µµË”·¡â ‰¥â√ —∫°“√√ —°…“¥â«¬ “√π È”®πæՇ撬߷≈ â« ·≈–¬—ß¡’À≈ —°∞“π∑ ’ Ë∫ àß™’È«à“¡’‡≈◊Õ¥‰ª‡≈ ’ ȬßÕ«—¬«–µà“ßÊ≈¥≈ß (hypoperfusion) ‡™àπ lactic acido-sis ªí “«–ÕÕ°πâÕ¬ À√◊Õ¡’√–¥—∫§«“¡√Ÿâ µ‘‡ª≈’ˬπ·ª≈ߺŸâªÉ«¬∑ ’ Ë ‰¥â√ —∫¬“°√–µÿâπÀ—«„®·≈–¬“∫ ’∫À≈Õ¥‡≈◊Õ¥Õ“®¡’§«“¡¥—π‡≈◊Õ¥‡ªìπª√°µ‘¢≥–∑’Ë¡’ hypoperfusion
欓∏‘°”‡π‘¥·≈–欓∏ ‘ √’√«‘∑¬“2,3
欓∏ ‘°”‡π‘¥¢Õß¿“«– septic shock „πªí®®ÿ∫—π¬—߉¡à‡ªìπ∑ ’ Ë∑√“∫§√∫∂ â«π ·µàÀ≈ —°∞“π„πºŸâªÉ«¬·≈–„π —µ«å∑¥≈Õßæ∫«à“ °“√µ‘¥‡™◊ÈÕÀ√◊Õ inflammatory foci „π√à“ß°“¬ºŸâªÉ«¬®–°√–µÿâπ immune cells (macrophage,dendritic cells ·≈– neutrophil) „Àâ¡’°“√µÕ∫ πÕß ºà“πCD 4 cells ∑ —Èß„π≈—°…≥–°“√Õ—°‡ ∫ (inflammation re-sponse, Th1) ·≈–°“√µâ“π°“√Õ—°‡ ∫ (anti inflamma-tory response À√◊Õ anergy, Th2) „π à«π¢Õßinflammatory response ®–‡°‘¥¢÷Èπ‚¥¬ cytokinesµà“ß Ê ∑’Ë ”§—≠§◊Õ monocyte, neutrophil ·≈– endot-helial cell „ÀâÀ≈—Ëß mediators µà“ßÊ ∑ ’Ë ”§—≠§◊Õ tumornecrotic factor (TNF) interleukin-1(IL-1) ®“°¢âÕ¡Ÿ≈„πªí®®ÿ∫ —π‡™ ◊ ËÕ«à“ TNF ·≈– IL-1 π ’ È®–‰ª°√–µÿ âπ°“√ √â“ß·≈–°“√À≈—Ëß cytokines µà“ßÊ ‡™àπ TNF, IL-1,IL-2 œ≈œ °√–µÿâπ complement pathways, coagula-tion system, platelet activating factors œ≈œ àߺ≈„Àâ¡’ inflammatory response ∑—Ë«Ê „π√ à“ß°“¬
”À√—∫ anti-inflammatory response ®– àߺ≈„À⺟âªÉ«¬¡’¿“«– anergy À√◊Õ immunosuppressivestate ‰¡à “¡“√∂°”®—¥ infection ·≈–¡’§«“¡‡ ’ ˬߵàÕnosocomial infection ´÷Ëß≈ —°…≥–¥—ß°≈ à“«®–æ∫‰¥â‡¡◊ËÕºŸâªÉ«¬¡’¿“«– sepsis ‰ª™à«ßÀπ÷Ëß
systemic inflammation ·≈–§«“¡º‘¥ª√°µ‘∑’ˇ°‘¥¢÷Èππ ’ È¡’º≈µàÕ°“√∑”ß“π¢Õ߇´≈≈ åµà“ßÊ ∑”„ÀâÕ«—¬«–µà“ßÊ∑”Àπâ“∑ ’ˇ ’¬‰ª à«π°“√‡ ◊ËÕ¡Àπ â“∑’Ë¢Õß√–∫∫‰À≈‡«’¬π‡≈◊Õ¥‡°‘¥®“°§«“¡º‘¥ª°µ‘µ—Èß·µà√–¥—∫‡´≈≈å microcircu-lation ‡™àπ vasodilatation, vasoconstriction ·≈–
vascular leakage ·≈– myocardial depression àߺ≈‚¥¬¿“æ√«¡„Àâ¡’§«“¡º‘¥ª°µ‘À√◊Õ‡°‘¥¿“«– ç™ÁÕ§é
§«“¡º‘¥ª°µ‘¢Õß°“√‰À≈‡«’¬π‡≈◊Õ¥„π√–¥—∫®ÿ≈¿“§(microcirculation)4
systemic inflammation ®–∑”„Àâ°“√‰À≈‡«’¬π‡≈◊Õ¥„π√–¥—∫‡π◊ ÈÕ‡¬ ◊ ËÕ®–º‘¥ª√°µ‘ ‡°‘¥ vasodilatation·≈– vasoconstriction5 „π microvascular bed ¿“«–disseminated intravascular coagulation6 ÷Ë߇°‘¥®“°°“√°√–µÿâπ coagulation cascade Õ“®∑”„À⇰‘¥ micro-thombosis ∑”„Àâ°“√‰À≈‡«’¬π‡≈◊Õ¥„π√–¥—∫‡π◊ÈÕ‡¬◊ËÕ ≈¥≈ß à«π欓∏‘ ¿“æ¢Õß endothelium π—Èπæ∫«à“ mi-crovascular permeability ‡æ‘Ë¡¢÷Èπ àߺ≈„Àâ¡’°“√‡ ’¬ “√πÈ”„πÀ≈Õ¥‡≈◊Õ¥·≈–°“√∫«¡πÈ”µ“¡Õ«—¬«–µà“ßÊ7-10
‡™àπ ªÕ¥ ‰µ º‘«Àπ—ß·≈–°≈â“¡‡π◊ÈÕ À—«„® ·≈– ¡Õß πÕ°®“°π ’ Ȭ —ßæ∫À≈ —°∞“π¢Õß ar teriolarvasoconstriction ·≈– vasodilatation „π°≈ â“¡‡π◊ÈÕ≈“¬·≈–„πÕ«—¬«–Õ◊ËπÊ Õ’°¥â«¬
„π·ßà¢Õß red blood cells ¡’°“√»÷°…“∑—Èß„π§π·≈– —µ«å∑¥≈Õß11 ∑ ’ Ë· ¥ß«à“ red cell deformability®–≈¥≈ß®“°¿“«– acidosis, mediators µà“ßÊ ·≈–®“°white cell àߺ≈„À⇡Á¥‡≈◊Õ¥·¥ß‰À≈ºà“πÀ≈Õ¥‡≈◊Õ¥ΩÕ¬≈”∫“°¢÷Èπ Õ“®Õÿ¥µ—π„πÀ≈Õ¥‡≈◊Õ¥ΩÕ¬ À√◊Õ‡°‘¥arteriovenous shunting º≈∑’˵“¡¡“§◊Õ ‡π◊ÈÕ‡¬◊ËÕ®–‰¥âÕÕ°´‘‡®π·≈– “√Õ“À“√≈¥≈ßÀ√◊ÕÕ“®‡°‘¥ hemolysis à«π white blood cell ®–‰À≈‡«’¬π„π microcircula-tion ¢Õß —µ«å∑¥≈Õß∑ ’ Ë ‰¥â√ —∫ endotoxin ®–‰¡à –¥«°‡æ√“– cell ®–‡°“–µ‘¥°—∫ endothelium ·≈–¡’°“√À≈—Ëßenzyme º≈µ“¡¡“§ ◊Õ °“√Õÿ¥°—Èπ¢ÕßÀ≈Õ¥‡≈◊Õ¥·≈–permeability ‡æ‘Ë¡¢÷Èπ
Cytopathic hypoxia12
°“√∑’ˇ´≈≈åµà“ßÊ ¡’°“√∑”ß“π≈¥≈ßÀ√◊ÕÀ¬ÿ¥∑”ß“π„π¿“«– septic shock ¡‘‰¥â‡°‘¥®“°°“√¡’ tissue perfu-sion ≈¥≈ß·µàÕ¬à“߇¥’¬« ‡æ√“–®“°°“√µ√«®»æºŸâªÉ«¬∑ ’ ˇ ’¬™’«‘µ®“° septic shock ®–‰¡àæ∫‡´≈≈ 嵓¬„πÕ«—¬«–∑’ˇ ◊ËÕ¡ ¿“æÀ√◊ÕÀ¬ÿ¥∑”ß“π ‡™àπ „π‰µ¢ÕߺŸâªÉ«¬
ªï∑’Ë 26 ©∫—∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2548 Therapeutic approach to septic shock 79
∑ ’ Ë¡’‰µ«“¬®“° sepsis ∫“ß√“¬°Á‰¡àæ∫≈ —°…≥– cellnecrosis ™—¥‡®π ‡™◊ËÕ«à“ organ failure „πºŸâªÉ«¬°≈ÿà¡π’ÈÕ∏‘∫“¬‰¥â‚¥¬°≈‰° cellular hibernation À√◊Õ cellularstunning À√◊Õ‡√’¬°«à“ çcytopathic hypoxiaé „π¿“«–π’ȇ´≈≈åµà“ßʉ¡à “¡“√∂¡’ aerobic respiration ‰¥â ‡π◊ËÕß®“°¡’°“√∑”ß“π¢Õß mitochondria ‡ ’¬‰ª®“° “‡ÀµÿÀ≈“¬Õ¬à“ß ∑’Ë ”§—≠§◊Õ ¡’ cellular store ¢Õß NAD/NADH+≈¥≈ß®“°°“√°√–µÿâπ enzyme poly (ADP-ribose)polymerase (PARP-1) „π¿“«– sepsis
§«“¡º‘¥ª°µ‘¢Õß√–∫∫‰À≈‡«’¬π‡≈◊Õ¥‚¥¬√«¡2,3
septic shock ‡ªìπ¿“«–™ÁÕ§∑’ËÕ¬Ÿà„π°≈ÿà¡ distribu-tive shock °≈à“«§◊Õ ™ÁÕ§∑’Ë¡’°“√≈¥≈ߢÕß systemicvascular resistance ·≈– maldistribution ¢Õß bloodflow Õ—π‡°‘¥®“° generalized vasodilatation ·≈– vas-cular leakage ©–π — Èπ„π√–¬–‡√ ‘ Ë¡µâπ ºŸâªÉ«¬®–¡’¿“«–hypovolemia ·µàÀ≈ —ß®“°‰¥â√ —∫ “√π È”®πæՇ撬߷≈ â«®–æ∫ hemodynamic profile ∑’˪√–°Õ∫¥â«¬ systemicvascular resistance (SVR) ∑ ’ ˵˔√ à«¡°—∫ cardiacoutput ∑ ’˪√°µ‘À√◊Õ Ÿß¢÷Èπ systemic vascular resis-tance ∑ ’˵˔≈ß
§à“ cardiac output ∑ ’ ˇæ‘Ë¡¢÷Èππ ’ È¡‘‰¥â Ÿß¡“°æÕ∑ ’ Ë®–‡ªìπª√–‚¬™π å„π¿“«–™ÁÕ§ ‡π◊ ËÕß®“° systemicinflammation ¡’º≈‚¥¬µ√ßµàÕ°≈ â“¡‡π◊ ÈÕÀ—«„® ∑”„Àâ°“√∫’∫µ—« (ejection fraction) ¢Õß ventricle ∑ —Èß 2 ¢â“ß≈¥≈ß left ventricle ®–¢¬“¬µ—« (dilate) ·≈– compli-ance ®–≈¥≈ß
Õ“°“√∑“ߧ≈‘π‘°1,2
ª√–°Õ∫¥â«¬ ‰¢â, Àπ“« —Ëπ, ™’æ®√‡√ Á«, À“¬„®‡√Á«§«“¡¥—π‡≈◊Õ¥µË”≈ß √–¥—∫§«“¡√Ÿâ ÷°≈¥≈ß √à«¡°—∫Õ“°“√·≈–Õ“°“√· ¥ß¢Õß°“√µ‘¥‡™ ◊ ÈÕ„π·µà≈–Õ«—¬«– Õ“°“√∑“ß√–∫∫À—«„®·≈–‰À≈‡«’¬π‡≈◊Õ¥ „π√–¬–·√°®–‡ªìπ≈ —°…≥– warm shock µ“¡æ¬“∏ ‘ √ ’√«‘∑¬“∑ ’ Ë°≈ à“«¡“¢â“ßµâπ·≈ â« ·µà„πºŸâªÉ«¬∫“ß√“¬Õ“®¡’Õ“°“√¢Õß coldshock µ—Èß·µà‡√ ‘ Ë¡µâπ Õ“°“√µà“ßÊ ®–¥’¢÷Èπ„π 24-96™—Ë«‚¡ß„πºŸâªÉ«¬∑ ’ ˵Õ∫ πÕßµàÕ°“√√ —°…“ „πºŸâªÉ«¬∑ ’ Ë¡’Õ“°“√Àπ —°Õ“®æ∫¿“«–™ÁÕ§√ ÿπ·√ß√ à«¡°—∫Õ“°“√¢Õßprogressive organ dysfunction Õ“®¡’„π√–¬–‡√ ‘ Ë¡·√°‰¥â ·≈–®–𔉪 Ÿà multiple organ failure
„πºŸâªÉ«¬∫“ß°≈ ÿ ࡪ√–®”µ—«Õ¬Ÿà‡¥‘¡ ‡™àπ ¥ ◊ Ë¡ ÿ√“‡√◊ÈÕ√—ß, ‡∫“À«“π §π™√“ ‡¥Á°·√°‡°‘¥, ‚√§µ—∫·¢Áß ‰µ«“¬‡√◊ ÈÕ√ —ß, lymphoma, leukemia, neutropenic ·≈–malnutrition ·≈–ºŸâªÉ«¬∑ ’ˉ¥â√—∫ corticosteroid ¡“‡ªìπ‡«≈“π“π Õ“®‰¡à¡’‰¢â ·≈–Õ“°“√¢Õß°“√µ‘¥‡™◊ÈÕ™—¥‡®π∫“ß√“¬Õ“®¡’Õ“°“√‡≈Á°πâÕ¬ ‡™àπ ¡’ hyperventilation,÷¡≈ß ∑“πÕ“À“√‰¥âπâÕ¬ §≈◊Ëπ‰ âÕ“‡®’¬πÀ√◊ÕÕÿ≥À¿Ÿ¡‘°“¬
‡ª≈ ’Ë¬π‰ª (∫“ß√“¬Õ“®¡’ hypothermia) ·æ∑¬åºŸâ√—°…“®–µâÕßπ ÷°∂ ÷ß¿“«–π ’ È „πºŸâªÉ«¬∑ ’ Ë¡’ ‚√§·≈–§«“¡‡ ’ ˬߥ—ß°≈à“«
©–π — Èπ°“√ª√–‡¡ ‘πºŸ âª É«¬Õ¬à“ß≈–‡Õ ’¬¥·≈–√–¡—¥√–«—ß®–™à«¬„Àâ·æ∑¬å«‘π‘®©—¬¿“«– septic shock√«¡∑ — Èß«‘π ‘®©—¬°“√µ‘¥‡™ ◊ ÈÕÀ√◊Õ¿“«–∑ ’ ˇªìπµâπ‡Àµÿ‰¥â °“√µ√«®æ∫≈—°…≥–®”‡æ“–µà“ß Ê ®–™à«¬„π°“√«‘π‘®©—¬ ‡™àπstellate hemorrhagic skin lesion √à«¡°—∫ meningealsign „π meningococemia À√◊Õ eschar „π scrubtyphus ‡ªìπµâπ
°“√«‘π ‘®©—¬®“°Õ“°“√∑“ߧ≈‘π‘°·≈–§”®”°—¥§«“¡¢â“ßµâπ °“√
«‘π ‘®©—¬«à“ºŸâªÉ«¬¡’¿“«– septic shock Õ“»—¬Õ“°“√·≈–Õ“°“√· ¥ß¢Õß¿“«– shock ·≈–À≈ —°∞“π¢ÕßSIRS √à«¡°—∫À≈—°∞“π¢Õß°“√µ‘¥‡™◊ÈÕ„π√à“ß°“¬ ªí≠À“∑ ’ Ë·æ∑¬åæ∫Õ¬Ÿà‡ ¡Õ§ ◊Õ°“√À“À≈ —°∞“π¬ ◊π¬—π«à“ºŸâªÉ«¬¡’°“√µ‘¥‡™◊ÈÕÕ¬Ÿà®√‘ß À“µ”·Àπàß∑’Ë¡’°“√µ‘¥‡™◊ÈÕ ·≈–·ª≈º≈°“√µ√«®∑“ßÀâÕߪؑ∫—µ‘°“√µà“ßÊ
‚¥¬∑—Ë«‰ª ºŸâªÉ«¬∑’Ë¡’Õ“°“√‡¢â“°—π‰¥â°—∫¿“«–¥—ß°≈à“«·æ∑¬å§«√‡°Á∫µ—«Õ¬à“ߢÕ߇≈◊Õ¥ ÀπÕß À√◊Õ “√§—¥À≈ —Ëß®“°Õ«—¬«–∑ ’ ˵‘¥‡™ ◊ ÈÕ „π°“√∑”°“√‡æ“–‡™ ◊ ÈÕ®“°‡≈◊Õ¥·æ∑¬å§«√‡°Á∫µ—«Õ¬à“ß 2-3 §√ —Èß„π∑’˵à“ßÊ °—π ·µà∂⓺ŸâªÉ«¬¡’Õ“°“√√ÿπ·√ßÕ“®‡®“–‡≈◊Õ¥®“°À≈“¬ Ê ∑’Ë„π‡«≈“‡¥’¬«°—π
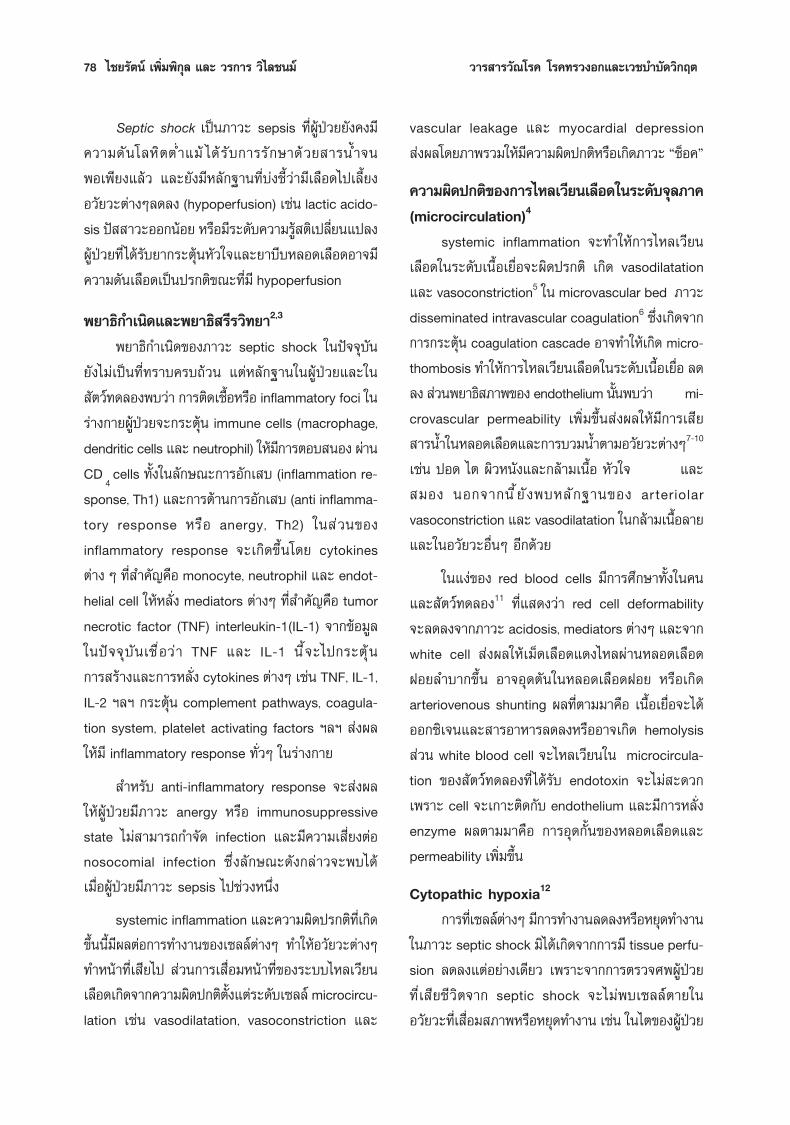
·π«∑“ß°“√ªØ‘∫ —µ‘√ —°…“‰¥â· ¥ß„π·ºπ¿“æ∑ ’ Ë 1®“°¢âÕ¡Ÿ≈¢ÕßÀÕºŸâªÉ«¬ ‰Õ ´’ ¬Ÿ ¿“§«‘™“Õ“¬ÿ√»“ µ√ å‚√ß欓∫“≈»‘√ ‘√“™ æ∫«à“ ºŸâªÉ«¬„π°≈ÿà¡π’È à«π„À≠à‡ªìπºŸâªÉ«¬∑’Ë¡’Õ“°“√ sepsis syndrome À√◊Õ septic shockÀ√◊Õ¡’ multiple organ dysfunction syndrome (MODS)®“°°“√µ‘¥‡™◊ÈÕ„πÕ«—¬«–µà“ßÊ ∑’Ë·æ∑¬å “¡“√∂µ√«®æ∫‰¥â
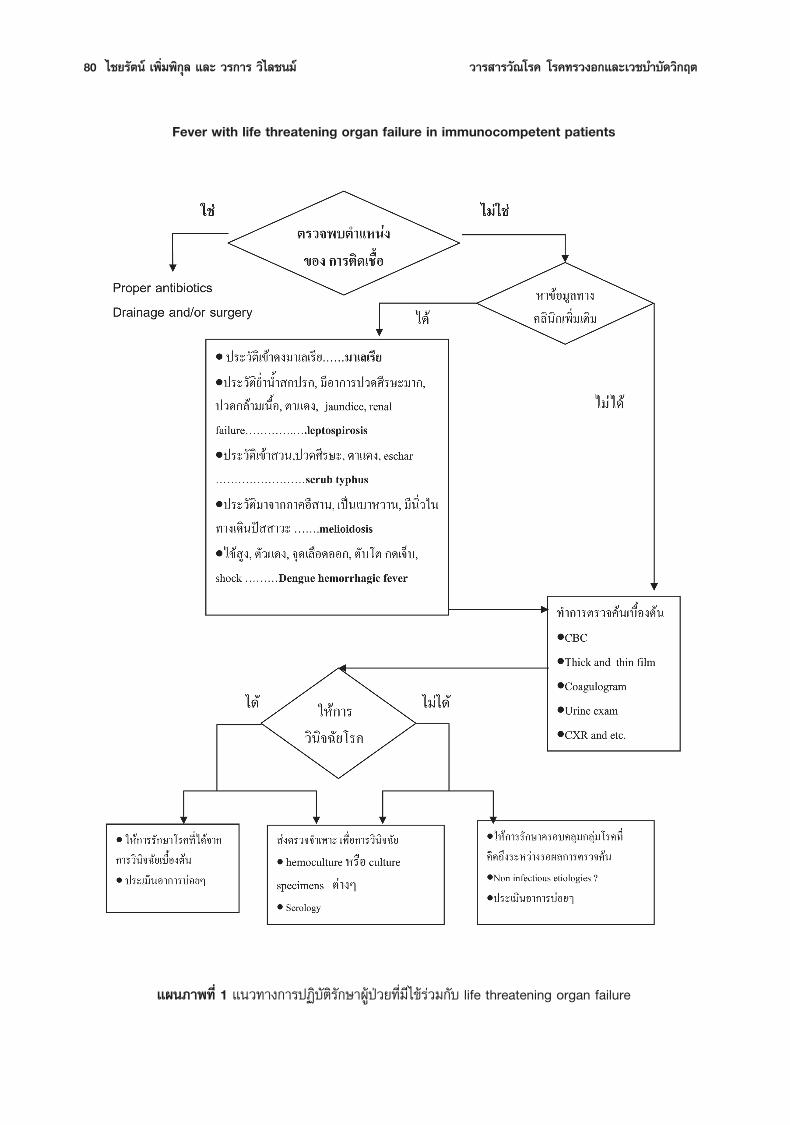
80 ‰™¬√—µπå ‡æ‘Ë¡æ‘°ÿ≈ ·≈– «√°“√ «‘‰≈™π¡å «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫—¥«‘°ƒµ
Fever with life threatening organ failure in immunocompetent patients
·ºπ¿“æ∑’Ë 1 ·π«∑“ß°“√ªØ‘∫—µ‘√—°…“ºŸâªÉ«¬∑’Ë¡’‰¢â√à«¡°—∫ life threatening organ failure
ªï∑’Ë 26 ©∫—∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2548 Therapeutic approach to septic shock 81
‡™àπ urinary tract infection, biliary tract infectionœ≈œ ”À√—∫ºŸâªÉ«¬∑’Ë·æ∑¬åµ√«®‰¡àæ∫µ”·Àπàß∑’Ë¡’°“√µ‘¥‡™ ◊ ÈÕ·≈–¡’Õ“°“√√ ÿπ·√ß·æ∑¬å§«√À“¢âÕ¡Ÿ≈∑“ߧ≈ ‘π ‘°‡æ‘Ë¡‡µ‘¡‡æ ◊ Ëՙ૬®”°—¥«ß¢Õß°“√«‘π ‘®©—¬‚√§„Àâ·§∫≈ßµ—«Õ¬à“ߢÕß‚√§„π°≈ÿà¡π’È ‰¥â·°à systemic infection µà“ßʇ™àπ Salmonellosis À√◊Õ disseminated infection Õ◊ËπÊ°≈ ÿ à¡‚√§‡¢µ√ âÕπÀ≈“¬‚√§®–Õ¬Ÿà„π°≈ ÿ à¡π ’ È ©–π — Èπ ºŸâªÉ«¬∑’Ë¡’ª√–«—µ‘‡¢â“ªÉ“À√◊Õ¡“®“°∫√‘‡«≥∑’Ë¡’°“√µ‘¥‡™◊ÈÕ¡“‡≈‡√’¬ª√–«—µ‘‡¢â“ «π À√◊Õª√–«—µ‘‰ª¬Ë”À√◊Õ≈ ÿ¬π È”∑ à«¡ °ÁÕ“®™à«¬ π—∫ πÿπ°“√«‘π ‘®©—¬‚√§ malaria, scrub typhusÀ√◊Õ leptospirosis µ“¡≈”¥—∫ ª√–«—µ‘‚√§‡∫“À«“πÀ√◊Õª√–«—µ ‘°“√¡’π ‘ Ë«„π∑“߇¥‘πªí “«– ®–™à«¬ π —∫ π ÿπ°“√µ‘¥‡™ ◊ ÈÕ Burkholderia pseudomallei à«πª√–«—µ‘‚√§π ’ ȺŸ âªÉ«¬‡ªìπÕ¬Ÿà‡¥‘¡√«¡∑ — Èß°“√√ —°…“∑ ’ ˺ŸâªÉ«¬‰¥â√ —∫®–∫Õ°¿“«–∑“ß¿Ÿ¡‘§ÿâ¡°—π¢ÕߺŸâªÉ«¬‰¥â ‡™àπª√–«—µ‘‚√§¿Ÿ¡‘§ÿ â¡°—π∫°æ√ àÕß ª√–«—µ‘‰¥â√ —∫ steroidÀ√◊Õ‡§¡’∫”∫—¥ ‡ªìπµâπ
°“√µ√«®√à“ß°“¬°Á¡’§«“¡ ”§—≠ ‡æ√“–„π∫“ß°√≥’ºŸâªÉ«¬Õ“®¡’Õ“°“√· ¥ß∑’ˇªìπ≈—°…≥–®”‡æ“–¢Õß‚√§ ‡™àπeschar „π scrub typhus µàÕ¡π È”‡À≈◊Õß‚µÕ“®æ∫‰¥â„π«—≥‚√§, melioidosis À√◊Õ scrub typhus Õ“°“√meningeal irritation À√◊Õ°“√µ√«®æ∫≈ —°…≥–¢Õßπ È”‰¢ —πÀ≈—ß∑’ˇ¢â“°—π‰¥â°—∫ aseptic meningitis Õ“®æ∫‰¥â„π scrub typhus À√◊Õ leptospirosis °“√µ√«®æ∫µ—∫‚µæ∫‰¥â„πÀ≈“¬‚√§ ‡™àπ Dengue hemorrhagic fever,scrub typhus, leptospirosis ∂ â“æ∫√ à«¡°—∫®ÿ¥‡≈◊Õ¥ÕÕ°®–‡æ‘Ë¡πÈ”Àπ—°¢Õß Dengue hemorrhagic fever „Àâ¡“°¢÷Èπ ºŸâ∑ ’ Ë¡’¢âÕ¡Ÿ≈∑“ߧ≈ ‘π ‘°‡¢â“°—π‰¥â°—∫‚√§µà“ßÊÕ“®∑”„Àâ·æ∑¬å„Àâ°“√«‘π ‘®©—¬‡∫◊ ÈÕßµâπ‰¥âßà“¬¢÷Èπ ·≈–„Àâ°“√√—°…“‡∫◊ÈÕßµâπ‰¥â∑—π∑ à«ß∑’
„π¢≥–‡¥’¬«°—π ·æ∑¬å§«√∑”°“√µ√«®§âπ‡æ◊ËÕ„À≥Ⱃ√«‘π‘®©—¬∑ ’Ë·πàπÕπ (specific diagnosis) Õ’°¥â«¬„πºŸâ∑ ’ Ë ‰¡à¡’¢âÕ¡Ÿ≈∑“ߧ≈ ‘π ‘°∑ ’ Ë®”‡æ“–µàÕ‚√§„¥ ·æ∑¬å§«√∑”°“√µ√«®§âπ„π‚√§∑ ’ Ë ß —¬ ´÷Ëß°“√µ√«®‡À≈ à“π ’ È®–„™â‡«≈“π“π°«à“®–‰¥âº≈ ·æ∑¬å®–µâÕß„Àâ°“√√ —°…“‡∫◊ÈÕßµâπ∑’˧√Õ∫§≈ÿ¡°≈ÿà¡‚√§∑’ËÕ“®‡ªìπ‰ª‰¥â ‡™àπ‡¡◊ËÕ ß —¬
«à“ºŸâªÉ«¬Õ“®‡ªìπ septic shock ®“° Burkholderiapseudomallei À√◊ÕÕ“®‡ªìπ severe leptospirosis ·æ∑¬å§«√„À⬓∑ ’˧√Õ∫§≈ ÿ¡°“√µ‘¥‡™ ◊ÈÕ∑—Èß ÕßÕ¬à“ß ‡ªìπµâπ
πÕ°®“°π’È„πºŸâªÉ«¬∑’ˉ¡à¡’¢âÕ¡Ÿ≈ π—∫ πÿπ‚√§µ‘¥‡™◊ÈÕ„¥Ê ·æ∑¬å§«√¡Õß„Àâ°«â“ß«à“ºŸâªÉ«¬¡’‰¢â·≈–Õ“°“√∑ ’ Ë√ ÿπ·√ß®“°°“√µ‘¥‡™ ◊ ÈÕ®√ ‘ßÀ√◊Õ‰¡à ‡æ√“–„π∫“ß°√≥ ’°“√‰¥â√ —∫ “√æ‘… °“√¡’ metabolic illness ∫“ßÕ¬à“߇™àπ thyroid storm ¿“«– pancreatitis √«¡∑ —Èß¡–‡√Áß∫“ß™π ‘¥ Õ“®∑”„À⺟âªÉ«¬¡’‰¢â·≈– multiple organdysfunction ‰¥â‡™àπ°—π
„π°“√§âπÀ“¢âÕ¡Ÿ≈∑“ߧ≈ ‘π ‘°π — Èπ ·æ∑¬å®–µâÕß∂“¡ª√–«—µ‘ ·≈–µ√«®√ à“ß°“¬Õ¬à“ß∂’Ë∂â«π ‡™àπ·æ∑¬å®–‰¡à “¡“√∂µ√«®æ∫ eschar ‰¥â‡≈¬∂Ⓣ¡à‰¥â ß —¬ ·≈–∑”°“√µ√«®∫√ ‘‡«≥¢“Àπ’∫ perineal area ·≈– glutealcleft ‡ªìπµâπ à«π°“√ à߇≈◊Õ¥À√◊Õµ—«Õ¬à“ßÕ ◊ ËπÊ ‡æ ◊ ËÕ∑”°“√µ√«®π—Èπ ·æ∑¬å®–µâÕß√ Ÿâ®—°«‘∏’µ√«®∑ ’Ë„™â §«“¡‰«·≈–§«“¡®”‡æ“–µàÕ«‘∏ ’π — Èπ Ê µ—«Õ¬à“߇™àπ °“√µ√«®Weil-Felix test ”À√ —∫ scrub typhus π — È𠇪ìπ∑ ’ Ë∑√“∫°—π‚¥¬∑ — Ë«‰ª«à“ ¡’§«“¡‰«·≈–§«“¡®”‡æ“–µË”´÷Ëß„πªí®®ÿ∫ —π °“√µ√«®‚¥¬„™â«‘∏ ’ indirect immuno-fluorescent antibody ®–¡’ª√– ‘∑∏ ‘¿“æ‡Àπ◊Õ°«à“πÕ°®“°π’È·æ∑¬å§«√µ√–Àπ—°∂÷ß§à“„™â®à“¬ ®”π«π§√—Èß∑’Ë àßµ√«® ·≈–√–¬–‡«≈“∑ ’Ë√Õº≈°“√µ√«®Õ’°¥â«¬
°“√√—°…“À≈—°°“√√—°…“ª√–°Õ∫¥â«¬ à«π ”§—≠ 3 Õ¬à“ß
§◊Õ 1) °“√°”®—¥‡™◊ÈÕ·≈–·À≈àßµ‘¥‡™◊ÈÕ 2) „Àâ intensivelife support ·≈– 3) 欓¬“¡ neutralize toxin ·≈–ª√ —∫ host inflammatory response
°“√„À⬓ªØ‘™’«π–·≈–°“√°”®—¥·À≈àßµ‘¥‡™◊ÈÕ·æ∑¬å§«√„À⬓ªØ‘™’«π–∑ —π∑ ’ À≈ —ß®“°‰¥â‡°Á∫
µ—«Õ¬à“߇≈◊Õ¥ body fluid À√◊Õ exudate ∑ ’Ë ß —¬«à“‡ªìπ·À≈ àßµ‘¥‡™ ◊ ÈÕ„πºŸâªÉ«¬ septic shock °“√‡°Á∫µ—«Õ¬à“ßhemoculture §«√‡®“–‡≈◊Õ¥Õ¬à“ßπâÕ¬®“° 2 ·À≈àß
°“√„À⬓ªØ‘™’«π–∑’ˇÀ¡“– ¡Õ¬à“ß√«¥‡√Á«„π√–¬–
82 ‰™¬√—µπå ‡æ‘Ë¡æ‘°ÿ≈ ·≈– «√°“√ «‘‰≈™π¡å «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫—¥«‘°ƒµ
·√°¢Õß septic shock ®–∑”„ÀâÕ—µ√“√Õ¥‡æ‘Ë¡¢÷ Èπ°“√∑√“∫¢âÕ¡Ÿ≈¢ÕߺŸâªÉ«¬Õ¬à“ß≈–‡Õ’¬¥√«¡∑ — Èß·À≈ àßµ‘¥‡™◊ÈÕ ·≈–°“√µ√«®¬âÕ¡µ—«Õ¬à“ßµà“ß Ê ®“°ºŸâªÉ«¬ (‡™àπgramûs stain, AFB œ≈œ ) ®–∑”„Àâ°“√µ—¥ ‘π°“√„À⬓ßà“¬¢÷È𠬓∑ ’ Ë „Àâ„π™à«ß·√°®–µâÕߧ√Õ∫§≈ ÿ¡‡™ ◊ ÈÕ∑ ’ ˇªìπ‰ª‰¥â„π¢≥–π — ÈπÊ ·≈–‡¡ ◊ ËÕº≈°“√‡æ“–‡™ ◊ ÈÕµà“ß Ê °≈ —∫¡“·≈ â« §«√ª√ —∫¬“„À⇪ìπ™π ‘¥∑ ’ Ë®”‡æ“–µàÕ‡™ ◊ ÈÕπ — Èπ „πºŸâªÉ«¬∑ ’ Ë·æ∑¬å‰¡à “¡“√∂∫Õ°·À≈ àß°“√µ‘¥‡™ ◊ ÈÕ·≈–™π ‘¥¢Õ߇™◊ÈÕ‰¥â ‡™àπ „πºŸâªÉ«¬∑’Ë¡’¿“«– febrile neutropenia·æ∑¬å§«√„À⬓∑ ’ ˧√Õ∫§≈ ÿ¡‡™ ◊ ÈÕ∑ ÿ°™π ‘¥°àÕπ √“¬≈–‡Õ’¬¥¢Õß°“√„™â¬“ªØ‘™’«π–®–‰¡à°≈à“«„π∫∑§«“¡π ’È
Intensive life support®ÿ¥ª√– ß§å ‡æ◊ËÕª√–§—∫ª√–§Õß„À⺟âªÉ«¬√Õ¥™’«‘µ
‚¥¬„ÀâÕ«—¬«–µà“ß Ê ‡ ◊ËÕ¡ ¿“æπ âÕ¬∑’Ë ÿ¥ „π™à«ß·√° Êæ√ âÕ¡‰ª°—∫°“√√ —°…“®”‡æ“– § ◊Õ ¬“ªØ‘™’«π– ·≈–°”®—¥·À≈àßµ‘¥‡™◊ÈÕ ‡π◊ËÕß®“° inflammatory response∑’Ë√ÿπ·√ߢÕß√à“ß°“¬∑”„ÀâÕ«—¬«–µà“ßÊ ∑”Àπ â“∑’˺‘¥ª°µ‘‰ª¥—ß∑ ’ Ë ‰¥â°≈ à“«¡“·≈ â« ºŸâªÉ«¬∑ ’ Ë ‰¥â√ —∫°“√√ —°…“®πæâπ®“°¿“«–™ÁÕ§Õ¬à“ß√«¥‡√Á«∑’ËÀâÕß©ÿ°‡©‘π‚¥¬°“√„Àâ “√πÈ”¬“°√–µÿ âπÀ—«„®·≈–¬“∫ ’∫À≈Õ¥‡≈◊Õ¥ µ≈Õ¥®π°“√„Àâ‡≈◊Õ¥‡¡ ◊ ËÕ¡’¢âÕ∫ àß™’È ‡æ ◊ ËÕ„Àâ tissue perfusion °≈ —∫‡ªìπª°µ‘‚¥¬‡√ Á«®–¡’Õ—µ√“√Õ¥ Ÿß°«à“°≈ ÿ à¡∑ ’ Ë ‰¥â√ —∫°“√√—°…“µ“¡ª√°µ‘∑’ËÀÕºŸâªÉ«¬Àπ—°13
ºŸâªÉ«¬∑ ’ Ë ‰¥â√ —∫°“√√ —°…“‡∫◊ ÈÕßµâπ®π “¡“√∂‡§≈◊ ËÕπ¬â“¬‰¥â·≈ â« §«√‰¥â√ —∫°“√√ —°…“„πÀÕºŸâªÉ«¬Àπ —° ¡’°“√»÷°…“æ∫«à“ºŸâªÉ«¬∑ ’ Ë ‰¥â√ —∫°“√√ —°…“„πÀÕºŸâªÉ«¬Àπ —°∑ ’ Ë¡’∫ ÿ§≈“°√ª√–®”µ≈Õ¥‡«≈“·≈–‡§√◊ ËÕß¡ ◊Õ‡Ω Ñ“√–«—ßµà“ßÊ®–¡’Õ—µ√“√Õ¥¡“°°«à“ºŸâªÉ«¬„πÀÕºŸâªÉ«¬ “¡—≠
Hemodynamic management and monitoring14
ºŸâªÉ«¬§«√‰¥â√—∫°“√¥Ÿ·≈√—°…“„πÀÕºŸâªÉ«¬Àπ—° ´÷Ëß¡’°“√‡ΩÑ“√–«—ßÕ“°“√∑“ߧ≈‘π‘° vital signs ¡’°“√µ√«®continuous EKG ‡π◊ ËÕß®“°ºŸ âªÉ«¬¡’§«“¡‡ ’ ˬߵàÕ
À—«„®‡µâπº‘¥®—ßÀ«–®“°‚√§À√◊Õ¬“°√–µÿâπÀ—«„®∑’Ë„Àâ ·≈–§«√ª√–‡¡‘π intake output „π·µà≈–™—Ë«‚¡ß ·≈–°“√ª√–‡¡‘π intravascular volume ¥â«¬ CVP ‡ªìπÕ¬à“ßπâÕ¬ à«π°“√‡ΩÑ“√–«—ߥ⫬ pulmonary artery catheter·≈– intraarterial catheter „π ∂“π∑’Ë∑’Ë∑”‰¥â®–¡’ª√–‚¬™πå„πºŸâªÉ«¬∑ ’ Ë¡’§«“¡¥—π‡≈◊Õ¥µË”À√◊Õ°”≈ —߇ª≈ ’ ˬπ·ª≈ß∂ ÷ß·¡â«à“¢âÕ¡Ÿ≈∑ ’ Ë¡’Õ¬Ÿ à „πªí®®ÿ∫ —π‰¡à “¡“√∂æ‘ Ÿ®π å ‰¥â«à“°“√‡Ω Ñ“√–«—ߥ—ß°≈ à“«®–∑”„ÀâÕ—µ√“√Õ¥ºŸâªÉ«¬ Ÿß¢÷Èπ16
·µà·æ∑¬å®–ª√ —∫°“√„Àâ “√π È” µ—¥ ‘π°“√„À⬓°√–µÿâπÀ—«„®·≈–∫’∫À≈Õ¥‡≈◊Õ¥‰¥âßà“¬¢÷Èπ‚¥¬Õ“»—¬§à“ pulmonarycapillary wedge pressure (PCWP), cardiac output·≈– continuous BP µ≈Õ¥®π “¡“√∂§”π«≥ systemicvascular resistance (SVR) ·≈–¥Ÿ¥‡≈◊Õ¥„π pulmonaryartery ‰ªµ√«® mixed venous blood gas ‰¥â
„π°“√„™â§à“ CVP „π°“√ª√–‡¡‘π intravascularvolume ·æ∑¬åºŸâ√ —°…“®–µâÕß√–¡—¥√–«—ßªí®®—¬∑ ’ Ë∑”„ÀâCVP Ÿß‡°‘πª√°µ‘ ‡™àπ ºŸâªÉ«¬∑ ’ Ë¡’§«“¡¥—π„π™àÕߪեÀ√◊Õ™àÕß∑âÕß Ÿß ·µà„π∑’Ëʉ¡à “¡“√∂„ à “¬ «π pulmo-nary ‰¥â °“√„ à “¬ CVP Õ“®™à«¬„π°“√∑” fluidchallenge ∂ â“∑”Õ¬à“ß√–¡—¥√–«—ß
®ÿ¥À¡“¬„π°“√√ —°…“ (Goal of therapy)14
∑’Ë ”§—≠§◊Õ°“√®—¥°“√„Àâ tissue perfusion À√◊Õtissue oxygenation °≈ —∫¡“‡ªìπª√°µ‘ ∑ —π∑ ’∑ ’ Ë«‘π ‘®©—¬¿“«–™ÁÕ§‰¥â ‚¥¬°“√„Àâ “√π È”·≈–°“√„™â¬“°√–µÿâπÀ—«„®·≈–¬“∫’∫À≈Õ¥‡≈◊Õ¥‡¡◊ËÕ¡’¢âÕ∫àß™’È °“√ª√–‡¡‘π«à“tissue perfusion °≈—∫¡“‡ªìπª√°µ‘·≈â« ‚¥¬„™â vital sign,organ blood flow ·≈–°“√µ‘¥µ“¡ tissue oxygenation¥—ßπ’È
Mean arterial pressure ¡“°°«à“ 65 ¡¡.ª√Õ∑ CVP 8-12 ´¡.πÈ” (12-15 ´¡.πÈ” „πºŸâªÉ«¬∑’Ë¡’
§«“¡¥—π„π™àÕߪե Ÿß) ®”π«πªí “«–¡“°°«à“ 0.5 ¡≈./°°./™—Ë«‚¡ß Central venous (superior vena cava) or
mixed venous oxygen saturation 70%(∂â“∑”°“√µ√«®‰¥â)
ªï∑’Ë 26 ©∫—∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2548 Therapeutic approach to septic shock 83
°“√„Àâ “√π È” (fluid therapy)°“√„Àâ “√π È”·≈–¬“°√–µÿâπÀ—«„®∫ ’∫À≈Õ¥‡≈◊Õ¥
¡’§«“¡ ”§—≠‡∑ à“‡∑ ’¬¡°—∫°“√„Àâ antibiotics „π¿“«–septic shock ·æ∑¬å§«√‡√ ‘ Ë¡„Àâ “√π È”‡ªìπÕ—π¥—∫·√°‚¥¬‡√ Á« ‡π◊ ËÕß®“°ºŸâªÉ«¬¡’°“√¢“¥ “√π Ȕլà“ß¡“°®“°æ¬“∏ ‘ √ ’√«‘∑¬“¥—ß∑ ’ Ë ‰¥â°≈ à“«¡“¢â“ßµâπ ™π ‘¥¢Õß “√π È”‰¡à«à“®–‡ªìπ crystalloid À√◊Õ colloid ®–‰¡à¡’º≈µàÕÕ—µ√“°“√√Õ¥Õ¬à“ß™—¥‡®π„πºŸâªÉ«¬∑ — Ë«‰ª ¢âÕ¥’¢Õß “√colloid §◊Õ®–§ßÕ¬Ÿà„πÀ≈Õ¥‡≈◊Õ¥‰¥âπ“π°«à“ ·≈–∑”„Àâ·√ߥ—π‡≈◊Õ¥°≈ —∫¡“‡ªìπª√°µ‘‰¥â‡√ Á«°«à“·µà¢âÕ‡ ’¬§ ◊Õ√“§“·æß·≈– synthetic colloid ∫“ß™π ‘¥Õ“®∑”„À⇰‘¥°“√·æâ√ÿπ·√ßÀ√◊Õ√∫°«π°“√·¢Áßµ—«¢Õ߇≈◊Õ¥ à«πhuman albumin π — Èπ ∂ ÷ß·¡â«à“®–¡’°“√»÷°…“Àπ ÷ Ëß∑ ’ Ë· ¥ß«à“º≈°“√√—°…“Õ“®®–¥’°«à“°“√„Àâ crystalloid15 ·µà‰¡à¡’π —¬ ”§—≠∑“ß ∂ ‘µ‘ à«π¢âÕ‡ ’¬§ ◊ÕÕ“®¡’‡™ ◊ ÈÕ‚√§∑ ’ ˵‘¥µàÕÀ√◊Õ‡°‘¥°“√·æâÕ¬à“ß√ ÿπ·√߉¥â
Õ—µ√“°“√„Àâ “√πÈ”¡’§«“¡ ”§—≠¡“° §«√‡√‘Ë¡„Àâ “√πÈ”„πÕ—µ√“‡√Á« ‡™àπ 500-1,000 ¡≈. ¢Õß crystalloid§√ ÷ Ëß™— Ë«‚¡ßÀ√◊Õ„Àâ “√ colloid 300-500 ¡≈. „π15 π“∑ ’∂ ÷ß 1 ™—Ë«‚¡ß ·≈ â«·µà ¿“æ¢ÕߺŸâªÉ«¬·≈–‚√§∑“ß√–∫∫À—«„®À√◊Õ‰À≈‡«’¬π‡≈◊Õ¥∑ ’ Ë¡’Õ¬Ÿà‡¥‘¡·≈–„Àâ´È”‚¥¬°“√ª√–‡¡‘𧫓¡¥—π‚≈À‘µ ·≈–§à“ CVP (fluidchallenge) √ à«¡°—∫°“√ª√–‡¡‘π®”π«πªí “«–µàÕ™—Ë«‚¡ß‡æ◊ËÕ¥Ÿ«à“ organ perfusion °≈—∫¡“‡ªìπª°µ‘·≈â«À√◊Õ‰¡à
„π°√≥ ’∑ ’ Ë„Àâ°“√√ —°…“„π™à«ßµâπ®π§«“¡¥—π‚≈À‘µ·≈– tissue perfusion °≈—∫¡“‡ªìπª°µ‘·≈â« ºŸâ√—°…“®–µâÕߧ”π÷ß∂÷ß continuing leakage ´÷Ë߬—ߧߡ’Õ¬Ÿà„π™à«ß24 ™—Ë«‚¡ß (À√◊Õπ“π°«à“„π°√≥ ’∑’Ë·À≈àß°“√µ‘¥‡™◊ÈÕÀ√◊Õµ—«‡™◊ÈÕ‰¡à‰¥â√—∫¬“ªØ‘™’«π–‰¡à∂Ÿ°°”®—¥∑’ˇÀ¡“– ¡) °“√„Àâmaintenance fluid ∑’ˇÀ¡“– ¡®÷ß¡’§«“¡ ”§—≠·≈–µâÕß
§Õ¬‡Ω Ñ“ª√–‡¡‘π∫ àÕ¬Ê „π™à«ßπ ’ È ¡‘©–π — ÈπºŸâªÉ«¬Õ“®¡’prolonged tissue hypoxia ‡°‘¥ multiorgan dysfunc-tion ‰¥â
°“√„™â inotropic drugs ·≈– vasopressors14
„π°√≥ ’∑ ’ ˵√«®æ∫«à“ª√ ‘¡“≥ “√π È”„πÀ≈Õ¥‡≈◊Õ¥¢ÕߺŸâªÉ«¬‡æ’¬ßæÕ·≈ â« ·µàºŸ âªÉ«¬¬—ßÕ¬Ÿà„π¿“«–™ÁÕ§·æ∑¬å§«√‡√ ‘ Ë¡„À⬓°√–µÿâπÀ—«„®‚¥¬µ—¥ ‘π°“√„™â¬“µ“¡hemodynamic profile ·≈–ƒ∑∏ ‘ Ï¢Õ߬“ ‚¥¬∑ — Ë«‰ª¡’ºŸâ·π–π”„Àâ„™â dopamine À√◊Õ norepinephrine ‡ªì𬓇√‘Ë¡µâπ ‚¥¬ dopamine ¢π“¥µË” Ê (1-5 ¡§.°./°°./π“∑ ’) ®–ÕÕ°ƒ∑∏ ‘ χªìπ inotropic ‡æ‘Ë¡§«“¡¥—π‡≈◊Õ¥¢π“¥¢Õß dopamine Õ“®ª√ —∫¢÷Èπ‰ª‰¥â∂ ÷ß 20 ¡§.°./°°./π“∑ ’ ´÷ Ëß„π¢π“¥∑ ’ Ë Ÿßπ ’ È¬“®–¡’ƒ∑∏ ‘ ÏÀ¥À≈Õ¥‡≈◊Õ¥dopamine ∑”„ÀâÀ—«„®‡µâπ‡√ Á«·≈–Õ“®∑”„ÀâÀ—«„®‡µâπº‘¥®—ßÀ«–‰¥â à«π norepinephrine ÕÕ°ƒ∑∏ ‘Ï∫ ’∫À≈Õ¥‡≈◊Õ¥ ∑”„ÀâÕ—µ√“‡µâπ¢ÕßÀ—«„®·≈– stroke volume‡æ‘Ë¡¢÷Èπ‰¡à¡“°
„πºŸâªÉ«¬∑ ’ Ë¡’ cardiac dysfunction Õ¬à“ß¡“°¡’ cardiac output µË”·≈– SVR Ÿß ·æ∑¬å§«√„À⬓°√–µÿâπ β adrenergic receptor √ à«¡°—∫ vasocon-strictor ºŸâªÉ«¬∑’ˉ¡àµÕ∫ πÕßµàÕ norepinepherine ·≈–dopamine §«√‡ª≈ ’ Ë¬π¡“„™â dobutamine √ à«¡°—∫norepinepherine À√◊Õ dopamine ‡æ’¬ßÕ¬à“߇¥’¬«À√◊Õ„™â adrenaline °“√„™â¬“∑’Ë¡’ƒ∑∏‘Ï¢¬“¬À≈Õ¥‡≈◊Õ¥‡æ’¬ßÕ¬à“߇¥’¬«Õ“®°àÕ„À⇰‘¥º≈‡ ’¬Õ¬à“ß¡“°„π°√≥’π’È
„π°√≥ ’∑ ’ ˺ŸâªÉ«¬¬—ߧߡ’§«“¡¥—π‚≈À‘µµË” ∂ ÷ß·¡â«à“®–„™â¬“„π¢π“¥ Ÿß ÿ¥·≈â«Õ“®‡ª≈’ˬπ‡ªìπ epinephrine‡æ√“–Õ“®∑”„À⧫“¡¥—π‡≈◊Õ¥‡æ‘Ë¡‰¥â®√ ‘ß ·µà®–∑”„Àâ‡≈◊Õ¥‰ª‡≈’ȬßÕ«—¬«–¿“¬„π≈¥≈ß17
84 ‰™¬√—µπå ‡æ‘Ë¡æ‘°ÿ≈ ·≈– «√°“√ «‘‰≈™π¡å «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫—¥«‘°ƒµ
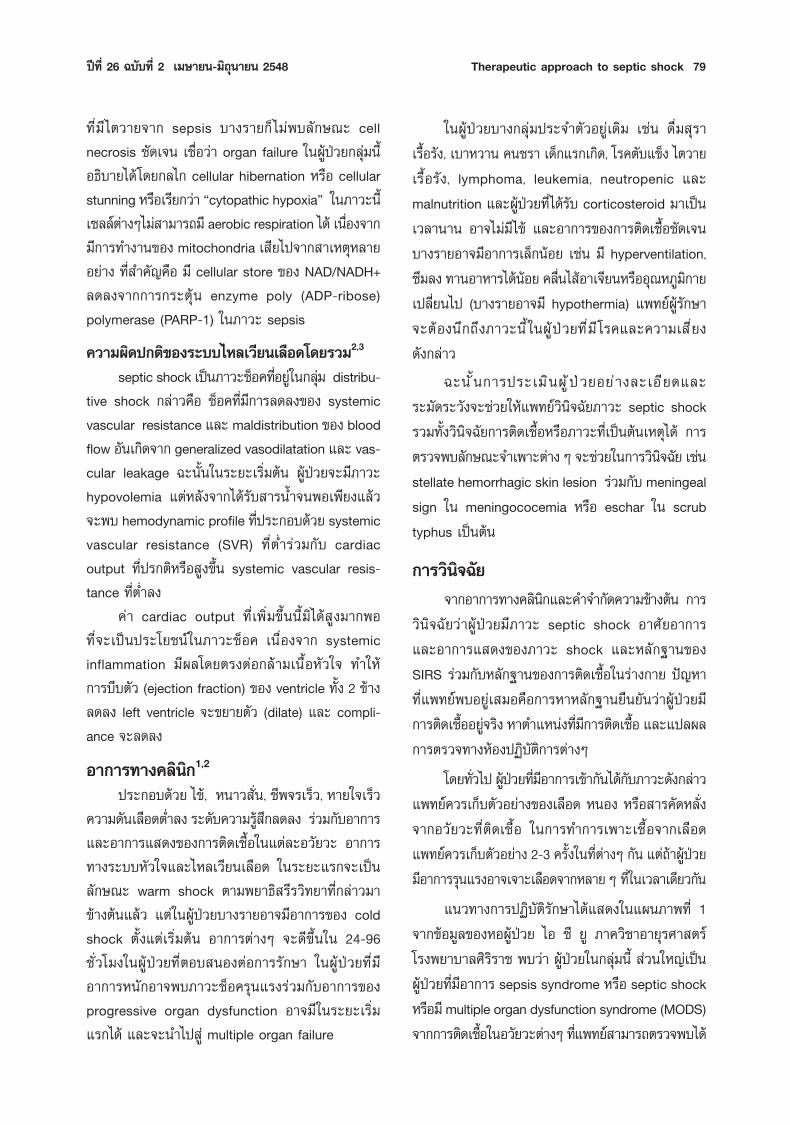
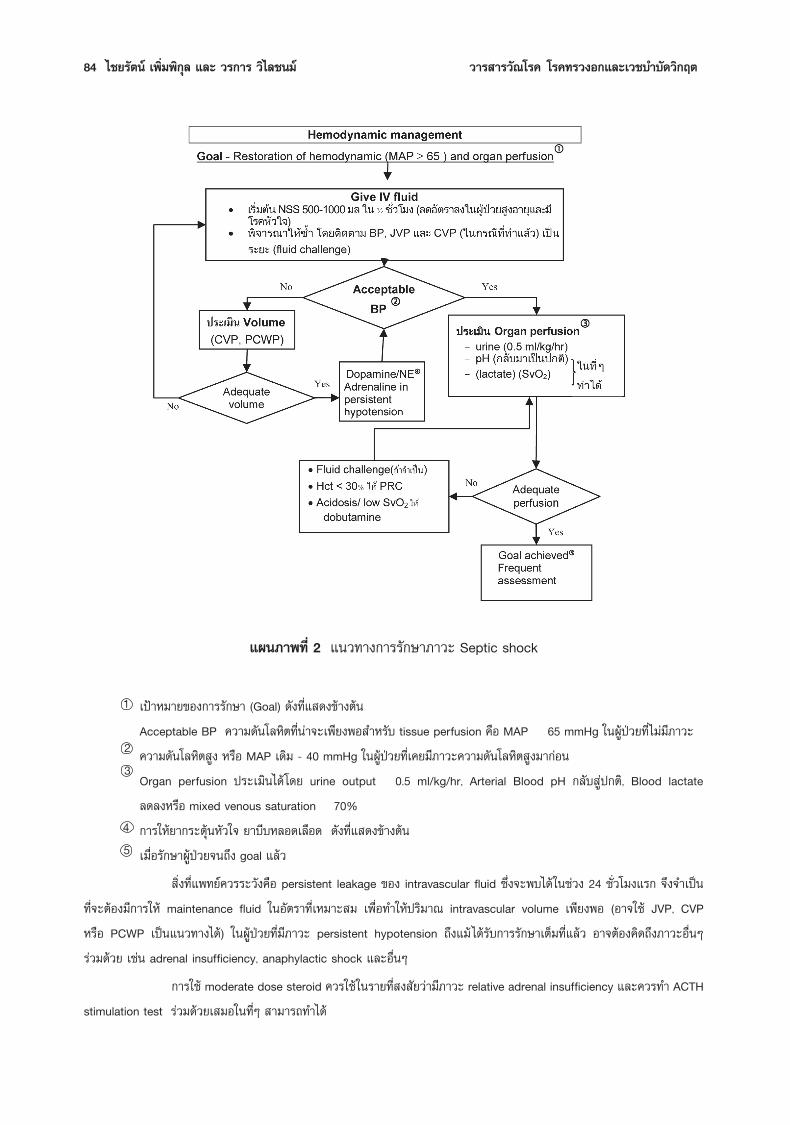
·ºπ¿“æ∑’Ë 2 ·π«∑“ß°“√√—°…“¿“«– Septic shock
‡ªÑ“À¡“¬¢Õß°“√√ —°…“ (Goal) ¥—ß∑’Ë· ¥ß¢â“ßµâπAcceptable BP §«“¡¥—π‚≈À‘µ∑’Ëπà“®–‡æ’¬ßæÕ ”À√—∫ tissue perfusion § ◊Õ MAP 65 mmHg „πºŸâªÉ«¬∑’Ë ‰¡à¡’¿“«–§«“¡¥—π‚≈À‘µ Ÿß À√◊Õ MAP ‡¥‘¡ - 40 mmHg „πºŸâªÉ«¬∑ ’ˇ§¬¡’¿“«–§«“¡¥—π‚≈À‘µ Ÿß¡“°àÕπOrgan perfusion ª√–‡¡‘π‰¥â‚¥¬ urine output 0.5 ml/kg/hr, Arterial Blood pH °≈ —∫ Ÿ રµ‘, Blood lactate≈¥≈ßÀ√◊Õ mixed venous saturation 70%°“√„À⬓°√–µÿâπÀ—«„® ¬“∫’∫À≈Õ¥‡≈◊Õ¥ ¥—ß∑’Ë· ¥ß¢â“ßµâπ‡¡◊ËÕ√—°…“ºŸâªÉ«¬®π∂÷ß goal ·≈â«
‘Ëß∑’Ë·æ∑¬å§«√√–«—ߧ◊Õ persistent leakage ¢Õß intravascular fluid ´÷Ëß®–æ∫‰¥â„π™à«ß 24 ™—Ë«‚¡ß·√° ®÷ß®”‡ªìπ∑ ’ Ë®–µâÕß¡’°“√„Àâ maintenance fluid „πÕ—µ√“∑ ’ ˇÀ¡“– ¡ ‡æ ◊ ËÕ∑”„Àâª√ ‘¡“≥ intravascular volume ‡æ’¬ßæÕ (Õ“®„™â JVP, CVPÀ√◊Õ PCWP ‡ªìπ·π«∑“߉¥â) „πºŸâªÉ«¬∑ ’ Ë¡’¿“«– persistent hypotension ∂ ÷ß·¡â ‰¥â√ —∫°“√√ —°…“‡µÁ¡∑ ’ Ë·≈ â« Õ“®µâÕߧ‘¥∂ ÷ß¿“«–Õ ◊ ËπÊ√à«¡¥â«¬ ‡™àπ adrenal insufficiency, anaphylactic shock ·≈–Õ◊ËπÊ
°“√„™â moderate dose steroid §«√„™â„π√“¬∑’Ë ß —¬«à“¡’¿“«– relative adrenal insufficiency ·≈–§«√∑” ACTHstimulation test √ à«¡¥â«¬‡ ¡Õ„π∑’ËÊ “¡“√∂∑”‰¥â
1
23
45

ªï∑’Ë 26 ©∫—∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2548 Therapeutic approach to septic shock 85
„π√–¬– 10 ªï∑’Ë·≈â«¡’ºŸâ°≈à“«∂÷ß°“√‡æ‘Ë¡ oxygendelivery „π√–¥—∫∑’Ë Ÿß‡°‘πª°µ‘ (supranormal level) ‚¥¬°“√„™â “√π È”À√◊Õ dopamine ‡π◊ ËÕß®“°¡’§«“¡‡™ ◊ ËÕ«à“oxygen consumption ∑’Ë≈¥≈ß„π¿“«– sepsis “¡“√∂®–‡æ‘Ë¡‰¥â‡¡ ◊ ËÕ‡æ‘Ë¡ oxygen delivery ·µà°“√»÷°…“ „π√–¬–À≈ —ßæ∫«à“Õ—µ√“µ“¬‰¡à‡ª≈ ’ ˬπ·ª≈ß18 ©–π — Èπ°“√„Àâ supranormal oxygen delivery ®–‰¡à¡’¢âÕ∫àß™’È„π¢≥–π’È
°“√ª√–‡¡‘πº≈°“√√ —°…“ §«√„™âÕ“°“√∑“ߧ≈ ‘π ‘°‡™àπ vital signs, ·≈–µ‘¥µ“¡ signs ¢Õßhypoperfusion‡™àπ urine output ( ÷Ëߧ«√®–¡“°°«à“ 0.5 ¡°./°°./™¡.),consciousness level œ≈œ À√◊ÕÕ“®µ‘¥µ“¡§à“ pH ®“°blood gas À√◊Õ§à“ lactate „π ∂“π∑ ’Ë∑’Ë∑”‰¥â
‚¥¬¿“æ√«¡¢Õß°“√„Àâ hemodynamic support·æ∑¬åºŸâ√—°…“µâÕß optimize tissue oxygenation ‚¥¬ª√—∫ preload „ÀâæÕ‡À¡“–·≈–„™â inotropes „π¢π“¥æÕ¥’∑ ’ Ë ‰¡à√∫°«πª√ ‘¡“≥‡≈◊Õ¥∑ ’ Ë®–‰ª‡≈ ’ È¬ß splanchnicorgan
·π«∑“ß°“√„Àâ hemodynamic support ‰¥â √ÿª‰«â„π·ºπ¿“æ∑ ’Ë 2
Pulmonary supportºŸâªÉ«¬‡°◊Õ∫∑ ÿ°√“¬®–¡’ acute lung injury À√◊Õ
ARDS ®“°°≈‰°¢Õß septic shock ·≈–„π∫“ß√“¬Õ“®¡’°“√µ‘¥‡™ ◊ ÈÕ∑ ’ ˪եµ—Èß·µà‡√ ‘ Ë¡µâπ °“√·≈°‡ª≈ ’ ˬπ°ä“´∑ ’˪ե®–‡ ’¬‰ª®“° shunting perfusion compli-ance ¢Õ߇π◊ ÈÕªÕ¥°Á®–‡ ’¬‰ª®“°æ¬“∏ ‘ ¿“æ∑ ’ ˇ°‘¥¢÷Èπairway resistance °Á®–‡æ‘Ë¡¢÷Èπ ∑”„À⺟âªÉ«¬µâÕßÕÕ°·√ßÀ“¬„®‡æ‘Ë¡¢÷Èπ ∑ — ÈßÀ¡¥π ’ È√ à«¡°—∫¿“«– hypercatabolicstate Õ“®∑”„À⺟âªÉ«¬¡’¿“«–À“¬„®«“¬‰¥âßà“¬¢÷Èπ ·æ∑¬å§«√„ÀâÕÕ°´‘‡®π„π√“¬∑ ’ ËÀ“¬„®‰¥â‡Õß „πºŸ âªÉ«¬∑ ’ Ë¡’Õ“°“√¢Õß respiratory failure §«√‰¥â√—∫°“√™à«¬À“¬„®‡æ◊ËÕ≈¥ respiratory load ·≈–∑”„Àâ oxygenation ¥’¢÷Èπ
«‘∏ ’°“√™à«¬À“¬„®„πºŸâªÉ«¬∑’Ë¡’ acute lung injuryÀ√◊Õ ARDS ®“°¿“«– septic shock °Á‡ªìπ‡™àπ‡¥’¬«°—∫ARDS14 ®“° “‡ÀµÿÕ◊ËπÊ °≈à“«§◊Õ „™âª√‘¡“µ√≈¡À“¬„®µË”(6-8 ¡≈./°°.) „™â PEEP „πºŸâªÉ«¬∑ÿ°√“¬‡æ ◊ËÕ‡æ‘Ë¡ lungcompliance ‡æ‘Ë¡ oxygenation ·≈–≈¥ end tidal
collapse ‚¥¬‡√ ‘Ë¡®“° 5-8 ´¡.πÈ” ª√—∫µ“¡§à“ PaO2,compliance ‚¥¬®ÿ¥À¡“¬°“√√ —°…“∑ ’ ˵âÕß°“√ PaO2∑ ’ ËæÕ‡À¡“– (PaO2>60 ¡¡.ª√Õ∑) À√◊Õ oxygensaturation ≥ 90% ‚¥¬„™â§«“¡‡¢â¡¢âπ¢ÕßÕÕ°´‘‡®π(FiO2) < 0.6 ·≈–√–«—ß¡‘„Àâ plateau airway pressure‡°‘π 35 ´¡. πÈ” °“√„™â PEEP „π¢π“¥ Ÿß„πºŸâªÉ«¬∑’Ë¡’septic shock induced ARDS §«√√–¡—¥√–«—ß ‡æ√“–PEEP Õ“®≈¥ cardiac output àߺ≈„Àâ oxygendelivery ≈¥≈ß À√◊Õ‡°‘¥ pressure complication ¢÷Èπ‰¥â
°“√™à«¬À“¬„®‚¥¬ noninvasive ventilator ∂÷ß·¡â®–¡’¢âÕ∫àß™’È„πÀ≈“¬¿“«– ·µà‰¡à·π–π”„Àâ„™â„π°√≥’π’È
Renal support°“√∑’Ë¡’‡≈◊Õ¥∑’ˉª‡≈’Ȭ߉µ≈¥≈ß„π septic shock ‡ªìπ
ªí®®—¬ ”§—≠∑ ’ Ë∑”„ÀâÀπ â“∑ ’ Ë¢Õ߉µ‡ ◊ ËÕ¡≈ß ·µàº≈‚¥¬µ√ߢÕß sepsis § ◊Õ systemic arterial vasodilatation àߺ≈„Àâ¡’°“√‡æ‘Ë¡¢÷Èπ¢Õß arginine vasopressin ´÷Ëß àߺ≈„Àâ rennin angiotensin-aldosterone system∂Ÿ°°√–µÿâπ ‡°‘¥ renal vasoconstriction ∑”„Àâ‡≈◊Õ¥‰ª‡≈’Ȭ߉µ≈¥≈ß ¡’ salt ·≈– water retention ‡æ‘Ë¡¢÷Èπ19
„π°“√√—°…“·æ∑¬å§«√·°â‰¢¿“«–™ÁÕ§‚¥¬‡√Á« ‚¥¬°“√„Àâ “√πÈ” °“√¥Ÿ·≈√–¥—∫πÈ”µ“≈‰¡à„À⠟߇°‘π·≈–µ‘¥µ“¡¢âÕ∫ àß™’È¢Õß renal replacement therapy ·≈–√ ’∫∑”‡¡ ◊ ËÕ¡’¢âÕ∫ àß™’È®–∑”„À⺟âªÉ«¬√Õ¥™’«‘µ‰¥â¡“°¢÷Èπ19 °“√„™âdopamine „π¢π“¥µË” (renal dose, 2-4 ¡§.°./°°./π“∑ ’) ‡æ ◊ ËÕÀ«—ß«à“®–‡æ‘Ë¡‡≈◊Õ¥‰ª‡≈ ’ Ȭ߉µ·≈–≈¥ renalcomplication π —Èπ„πªí®®ÿ∫—π‡™◊ËÕ«à“‰¡à‰¥âº≈·≈–‰¡à¡’°“√»÷°…“∑’ˇªìπ¡“µ√∞“π„¥Ê ∑’Ë π—∫ πÿπ°“√„™â«‘∏’¥—ß°≈à“«°“√§«∫§ÿ¡√–¥—∫π È”µ“≈
„πªí®®ÿ∫ —π¡’°“√»÷°…“∑ ’ Ë· ¥ß«à“°“√§«∫§ÿ¡√–¥—∫πÈ”µ“≈ºŸâªÉ«¬À≈—ßºà“µ—¥„ÀâÕ¬Ÿà„π√–¥—∫ 80-110 ¡≈/¥≈ ¥â«¬insulin infusion ®–≈¥Õ—µ√“µ“¬‰¥â20 ·µàºŸâªÉ«¬µâÕ߉¥â√—∫°“√ª√–‡¡‘π√–¥—∫π È”µ“≈Õ¬à“ß ¡Ë”‡ ¡Õ·≈–„°≈ ♑¥‡æ√“–Õ“®¡’√–¥—∫πÈ”µ“≈µË”®π‡°‘¥Õ—πµ√“¬‰¥â °“√»÷°…“¢âÕ¡Ÿ≈µàÕ¡“æ∫«à“ºŸ âªÉ«¬°≈ ÿ à¡∑ ’ Ë¡’√–¥—∫π È”µ“≈µË”°«à“150 ¡°/¥≈ ¬—ߧߡ’Õ—µ√“µ“¬µË”°«à“ºŸâªÉ«¬∑’Ë¡’πÈ”µ“≈ Ÿß©–π—Èπ‡¡◊ËÕÕ“»—¬º≈°“√»÷°…“¥—ß°≈à“« ·æ∑¬å§«√§«∫§ÿ¡√–¥—∫πÈ”µ“≈„ÀâµË”°«à“ 150 ¡°./¥≈. ‡ªìπÕ¬à“ßπâÕ¬ ‡æ◊ËÕ

86 ‰™¬√—µπå ‡æ‘Ë¡æ‘°ÿ≈ ·≈– «√°“√ «‘‰≈™π¡å «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫—¥«‘°ƒµ
≈¥Õ—µ√“µ“¬·≈–À≈’°‡≈’ˬߢâÕ·∑√° âÕπ®“°°“√„Àâ insu-lin ¡“°‡°‘π
°“√„™â corticosteroid„π™à«ß 20-30 ªï∑ ’ ˺à“π¡“π ’ È¡’¢âÕ∂°‡∂ ’¬ß°—π¡“°
‡°’ˬ«°—∫°“√„Àâ steroid „πºŸâªÉ«¬ septic shock „π·ßà¢Õß anti-inflammatory agent ‚¥¬¡’°“√»÷°…“∑ ’ Ë π—∫ πÿπ·≈–§—¥§â“π ‚¥¬‡©æ“–Õ¬à“߬‘Ëß°“√„™â steroid„π¢π“¥ ŸßÊ21 ·µà®“°°“√»÷°…“Àπâ“∑’Ë¢ÕßµàÕ¡À¡«°‰µ¢ÕߺŸâªÉ«¬„π¿“«–π ’ Èæ∫«à“ ∫“ß√“¬¡’°“√µÕ∫ πÕßµàÕ¿“«– stress ≈¥≈ߧ◊Õ¡’√–¥—∫ cortisol À≈—ß°“√°√–µÿâππâÕ¬°«à“∑ ’˧«√ ®÷ß¡’°“√»÷°…“°“√„™â corticosteroid „π¢π“¥π âÕ¬ Ê ‡æ ◊ ËÕ∑¥·∑π°“√∑”ß“π¢ÕßµàÕ¡À¡«°‰µ∑’Ë≈¥≈ß °“√»÷°…“‚¥¬ Annane ·≈–§≥–22 „™â hydro-cortisone „π¢π“¥ 50 ¡°. ∑“ßÀ≈Õ¥‡≈◊Õ¥¥” ∑ ÿ°6 ™—Ë«‚¡ß√ à«¡°—∫ fludocortisone 50 ¡§.°./«—𠇪ìπ‡«≈“ 7 «—π„πºŸâªÉ«¬∑ ’ Ë¡’¿“«–™ÁÕ§∑ ’ Ë ‰¡àµÕ∫ πÕßµàÕ¬“°√–µÿâπÀ—«„®·≈–¬“∫ ’∫À≈Õ¥‡≈◊Õ¥®–≈¥Õ—µ√“µ“¬·≈–°“√„™â¬“¥—ß°≈à“«≈ß
¢âÕ‡ πÕ·π–®“°ºŸâ‡™’ˬ«™“≠∑—Ë«‰ª § ◊Õ „™â hydro-cortisone „π¢π“¥¥—ß°≈ à“« (Õ“®√ à«¡°—∫ fludocor-tisone) „πºŸâªÉ«¬∑’Ë¡’≈—°…≥–¢â“ßµâπ‡ªìπ‡«≈“ 7 «—π À≈—ß®“°∑ ’Ë ‰¥â∑” ACTH stimulation test ·≈ â« („π∑ ’ËÊ ∑”‰¥â)∂⓺≈‡≈◊Õ¥ºŸâªÉ«¬´÷Ëß°≈—∫¡“°àÕπ 7 «—π ‰¡à· ¥ß≈—°…≥–¢Õß adrenal insufficiency (baseline cortisol level< 15 ¡§.°./¥≈. À√◊Õ √–¥—∫√–À«à“ß 15 - 34 ¡§.°./¥≈.·µà√–¥—∫ cortisol À≈ —ß°√–µÿâπ Ÿß¢÷Èπ < 9 ¡§.°./¥≈.)°Á„ÀâÀ¬ÿ¥¬“‰ª23,14
°“√„ÀâÕ“À“√14
°“√„ÀâÕ“À“√∑ ’ ËæÕ‡À¡“–¡’§«“¡ ”§—≠∑ — Èß„π·ßà°“√√ —°…“·≈–°“√ªÑÕß°—π¿“«– sepsis ‚¥¬∑ — Ë«‰ª «‘∏ ’°“√„Àâ enteral nutrition ‡ªìπ«‘∏’∑’ˇÀ¡“– ¡∑ ’Ë ÿ¥ ·µà„π°√≥’∑ ’˺ŸâªÉ«¬‰¡à “¡“√∂√ —∫ enteral nutrition ‰¥â §«√„Àâparenteral nutrition ‚¥¬°”Àπ¥„Àâ ‰¥âæ≈—ßß“π 25-30Kcal/°°./«—π ´÷Ëߪ√–°Õ∫¥â«¬‚ª√µ’π 1.3-2.0 °./°°./«—π·≈–„Àâ glucose 30-70% ¢Õß total non-proteincalories ‚¥¬√ —°…“√–¥—∫π È”µ“≈„π‡≈◊Õ¥„ÀâµË”°«à“
225 ¡°./¥≈. „Àâ lipids 15-30% ¢Õß total non-protein calories°“√„™â Antiinflammatory substance
¡’°“√»÷°…“∑’ËÕ¬Ÿà„π¢—Èπ∑¥≈Õß®”π«π¡“°∑’Ë欓¬“¡≈¥ inflammatory response ¢Õß√ à“ß°“¬ ‡™àπ °“√„™â¬“‡æ◊ËÕ neutralize toxins µà“ß Ê ‡™àπ antiendotoxinsantibody, core lipolysaccharide antibody œ≈œ À√◊Õ°“√ª√—∫ host mediators ‚¥¬°“√„™â antibody TNF24
IL-1 PAF C5A œ≈œ µ≈Õ¥®π°“√„™â antithrombin III¬—߉¡à¡’¬“µ—«„¥¡’ª√– ‘∑∏ ‘¿“æ‡æ’¬ßæÕ„π°“√√ —°…“ºŸ ⪠ɫ¬‡≈¬ ¡’¬“∫“ßµ—«Õ“®∑”„ÀâÕ—µ√“µ“¬‡æ‘ Ë¡¢÷ Èπ„πªí®®ÿ∫ —π¡’¬“™π ‘¥‡¥’¬«∑ ’ Ë¡’º≈„π°“√√ —°…“Õ¬à“ß™—¥‡®π§◊Õ°“√„™â recombinant human activated protein C
¢âÕ¡Ÿ≈®“°°“√»÷°…“æ∫«à“√–¥—∫ protein C „π‡≈◊Õ¥¢ÕߺŸâªÉ«¬ septic shock ®–π âÕ¬°«à“ª°µ‘·≈–°“√„Àâ recombinant activated protein C „πºŸâªÉ«¬°≈ÿà¡∑’Ë¡’Õ“°“√√ÿπ·√ß (APACHE II score ¡“°°«à“ 25) ®–≈¥Õ—µ√“µ“¬‰¥âÕ¬à“ß¡’π—¬ ”§—≠25 ‚¥¬Õ—µ√“µ“¬ ≥ «—π∑’Ë 28À≈ —ß°“√√ —°…“„π°≈ ÿ à¡∑ ’ Ë ‰¥â√ —∫¬“ ·≈–°≈ ÿ à¡∑ ’ Ë ‰¡à‰¥â√ —∫¬“=24.7% ·≈– 30.8% µ“¡≈”¥—∫ P < 0.005 ·≈– abso-lute risk of death reduction = 6.1% ¿“«– seriousbleeding side effect æ∫‰¥â¡“°°«à“°≈ÿà¡ control ·µà‰¡àµà“ß°—πÕ¬à“ß¡’π—¬ ”§—≠∑“ß ∂ ‘µ‘ (P = 0.06)
ºŸâ‡™’ˬ«™“≠‚¥¬∑ — Ë«‰ª·π–π”„Àâ„™â recombinanthuman activated protein C „πºŸâªÉ«¬∑’Ë¡’Õ“°“√√ÿπ·√ß(APACHE II score ¡“°°«à“ 25) ‚¥¬µâÕß√–«—ߪí≠À“‡≈◊Õ¥ÕÕ°º‘¥ª√°µ‘ ·≈–µâÕß·πà„®‡√◊ËÕß§à“„™â®à“¬ √ ÿª
Septic shock ‡ªìπ¿“«–«‘°ƒµ∑ ’ Ë¡’§«“¡ ”§—≠·≈–æ∫∫ àÕ¬„πÀÕºŸâªÉ«¬Àπ —° ∫∑§«“¡¢â“ßµâπ‰¥â°≈ à“«‚¥¬¬àÕ∂ ÷ß°≈‰°°“√‡°‘¥‚√§Õ—π𔉪 Ÿ ৫“¡‡¢â“„®„π°“√ªØ‘∫ —µ‘√ —°…“ ´÷Ëß®–µâÕߧ√Õ∫§≈ ÿ¡∑ — Èß°“√°”®—¥·À≈ àß°“√µ‘¥‡™ ◊ ÈÕÀ√◊ÕÕ—°‡ ∫√«¡∑ — Èß°“√ª√–§—∫ª√–§ÕßÕ«—¬«–µà“ß Ê „ÀâÕ¬Ÿà√Õ¥„π™à«ß«‘°ƒµ„πÀÕºŸâªÉ«¬Àπ—° §«“¡‡¢â“„®„π ‘Ëßµà“ßÊ ®– àߺ≈„ÀâÕ—µ√“√Õ¥¢ÕߺŸâªÉ«¬ Ÿß¢÷Èπ ¡’¿“«–·∑√°´âÕπ≈¥≈ß ‡«≈“„π°“√Õ¬Ÿà„π‚√ß欓∫“≈ — Èπ≈ß·≈–≈¥§à“„™â®à“¬

ªï∑’Ë 26 ©∫—∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2548 Therapeutic approach to septic shock 87
‡Õ° “√Õâ“ßÕ‘ß1. ACCP/SCCM Consensus Conference: definition for
sepsis and organ failure and guideline for the use ofinnovative therapies in sepsis: Chest 1992;101:1644- 1655.
2. Natanson C, Hoffman WD and Parillo JE. Septic shockand multiple organ failure. In: Parillo JE, Bone R.C.(eds). Critical Care Medicine. Principle of diagnosisand management. Missouri: Mosby Year Book, Inc.1995:355-373.
3. Heumann D and Glauser MP. Pathogenesis of sepsis.Science& Medicine November/ December 1994;1:28-37.
4. Hotclkiss RS and Karl IE. The pathophysiology andtreatment of sepsis. N Eng J Med 2003; 348:138-150.
5. Backer DD, Creteur J, Preiser JC, Dubois MJ andVincent JL. Microvascular blood flow is altered inpatients with sepsis. Am J Respir Crit Care Med2002;166:98-104.
6. Colman RW. Disseminated intravascular coagulationclue to sepsis. Semin Hemetol 1994;3 (suppl):10-17.
7. Chien S, Sinclair DG, Dellenback RK, et al. Effect ofendotoxin on capillary permeability to macromolecules.Am J Physiol 1964; 207:518-522.
8. Lam C, Tyml K and Marlin C. Microvascular perfusionis impaired in a rat model of sepsis. J Clin Invest1994:94:2077-2083.
9. Rai DK, Gupta LP and Singh RH. A study of micro-circulation in endotoxin shock. Surg Gynecol Obstet1974;139:11-16.
10. Sehutzer K-M, Larsson A, Risberg B, et al. Lungprotein leakage in feline septic shock. Am J RespirDis 1993;147:1380-1385.
11. Todd JC III and Moll HL. Sepsis-induced alterationsin the erythrocyte membrane. Am Surg 1994;60:954-957.
12. Fink MP. Bench to bedside review: Cytopathichypoxia. Critical care 2002;6:491-499.
13. Rivers E, Nyugen B, Havstad S et al. Early goaldirected therapy in the treatment of severe sepsisand septic shock. New Eng J Med 2001;345:1368-1377.
14. Dellinger RP, Carlet JM, Masur H. et al. Surviving
sepsis campaign guidelines for management ofsevere sepsis and septic shock. Intensive Care Med2004;30:536-555.
15. The SAFE Study Investigators. A compassionof albumin and saline for fluid resuscitation inthe intensive care unit. N Eng J Med 2004;350:2247-2256.
16. Bellomo R and Pinsky MR. Invasive hemodynamicmonitoring. In: Tinker J, Browne RG and Sibbald WJ.(eds) Critical Care: standard, audit and ethics. NewYork. Oxford University Press Inc. 1996:82-104.
17. Hellmann AM, Reinhart K, Bredle D et al. Epinephrineimpairs splanchnic perfusion in septic shock. CritCare Med 1997;25:399-404.
18. Aha I, Esteban A, Lorente JA, et al. A randomizedand controlled trial of the effect of treatment aimedat maximizing oxygen delivery in patients with severesepsis or septic shock. Chest 1999;115:453-461.
19. Schrier RW and Wang W. Mechanisms of disease:Acute renal failure and sepsis. N Eng J Med 2004;351:159-169.
20. Berghe G van der, Wontess P, Weekers F, et al.Intensive insulin therapy in the critically ill patients.N Engl J Med 2001;345:1359-1367.
21. Cronin L, Cook DJ, Carlet J, et.al. Corticosteroid treat-ment for sepsis: A critical appraisal and meta-analysisof the literature. Crit Care Med 1995; 23: 1430-1439.
22. Annane E, Sebille V, Charpentier C et al. Effectof treatment with low dose of hydrocortisone andfludocortisone on mortality in patients with septic shock.JAMA 2002;288:862-871.
23. Cooper MS and Stewart PM. Current concepts: corti-costeroid insufficiency in acutely ill patients. N Eng JMed 2003;348:727-734.
24. Edward A, Antonio A, Guillermo G, et al. Double-blindrandomized controlled trial of monoclonal antibody tohuman tumour necrosis factor in treatment of septicshock. Lancet 1998;351:929-933.
25. Bernard GR, Vincent JL, Laterre PF, et al. Recombi-nant human protein C Worldwide Evaluation in SevereSepsis (PROWESS) study group. Efficacy and safetyof recombinant human activated protein C for severesepsis. N Eng J Med 2001;344:699-709.
ªï∑ ’Ë 26 ©∫ —∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2548 Unplanned Extubation in Medical ICU 89
Abstract:Objective: To investigate incidence, clinical characteristics, and outcomes of unplanned extubation(UE) in medical intensive care unit in King Chulalongkorn Memorial Hospital during June 1st, 2002to January 31st, 2003.Research Design: A descriptive study.Methods: All intubated medical ICU patients who underwent unplanned removal of endotracheal tubewas enrolled to this study. Clinical characteristics, sedation scores to evaluate sedation adequacy andoutcomes of unplanned extubation were collected.Results: 471 patients were intubated in medical ICU during an eight-month study. 23 unplannedextubations (4.9%) in 21 patients have been documented. The majority of unplanned extubated cases(16 of 23, 69.6 %) occurred in the first 48 hours after intubations. There was no significant differencein extubations between shifts of work of medical personnel. The motor activity assessment scales(MAAS) were equal to 4 to 6 (çRestless and Cooperativeé to çDangerously Agitatedé) in the majority(17 of 23, 73.9 %) of UE, however, only one (5.9%) of them was sedated, and nine (58.8%) of themwere restrained. The ventilation assessment scales (VAS) were from A to B (çComfortableé to çMildlyDistressé) in most (21 of 23, 91.3%) of self-extubated patients. Reintubations were required in 12episodes (52.2 %), mostly in 1 hour after extubation. There was no serious adverse event attributedto unplanned extubation. No significant difference in age, gender distribution, diagnosis, and durationof intubation between the reintubated and non-reintubated group was observed. Of the respiratorysupport modes and parameters studied, the mean pre-extubation ventilator-delivered minute ventilation
UNPLANNED EXTUBATION IN MEDICAL ICUNorth Techawattanawanna M.D.*
Chanchai Sittipunt M.D.**Somkiat Wongtim M.D. ** Visit Udompanich M.D. **
Kamon Kawkitinarong M.D.**
*King Chulalongkorn Memorial Hospital, Bangkok 10330.**Division of Pulmonary and Critical Care Medicine, Department of Medicine, Chulalongkorn University.
Received for publication 1 November, 2004
«“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫—¥«‘°ƒµThai Journal of TuberculosisChest Diseases and Critical Care

90 North Techawattanawanna et al. «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
was significantly higher in reintubated group (11.1 L/min) than in non-reintubated group (4.0 L/min,p-value = 0.027).Conclusion: Unplanned extubation accounts for 4.9% in intubated medical ICU patients, mostlyoccurred in the first 48 hours after intubations. Lack of sedation in agitated patients is one ofpredisposing factors of unplanned extubation. Motor activity assessment scale (MAAS) may be usedas a predictor of unplanned extubation and need to be evaluated. Patients who required reintubationshave higher preextubation ventilatory assistance than patients in successfully extubated group.
∫∑§—¥¬àÕ πäÕµ ‡µ™–«—≤π«√√≥“*, ©—𙓬 ‘∑∏‘æ—π∏å **, ¡‡°’¬√µ‘ «ß…å∑ ‘¡ **, «‘»‘…Æå Õÿ¥¡æ“≥ ‘™¬å ** ·≈– °¡≈·°â«°‘µ‘≥√ߧå**. °“√∂Õ¥∑àՙ૬À“¬„®‚¥¬‰¡àµ—Èß„®„πÀÕºŸâªÉ«¬«‘°ƒµ∑“ßÕ“¬ÿ√°√√¡ «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫—¥«‘°ƒµ 2548;26:89-100.*‚√ß欓∫“≈®ÿÓ≈ß°√≥å **Àπ૬‚√§√–∫∫°“√À“¬„®·≈–‡«™∫”∫—¥«‘°ƒµ ¿“§«‘™“Õ“¬ÿ√»“ µ√å §≥–·æ∑¬»“ µ√å®ÿÓ≈ß°√≥å¡À“«‘∑¬“≈—¬«—µ∂ÿª√– ß§å ‡æ◊ËÕ»÷°…“‡°’ˬ«°—∫ Õÿ∫—µ‘°“√≥ å ≈—°…≥–∑“ߧ≈ ‘π‘° ·≈–º≈∑’˵“¡¡“ ¢Õß°“√∂Õ¥∑àՙ૬À“¬„®‚¥¬‰¡àµ—Èß„® „πÀÕºŸâªÉ«¬«‘°ƒµ∑“ßÕ“¬ÿ√°√√¡„π‚√ß欓∫“≈®ÿÓ≈ß°√≥å√–À«à“߇¥◊Õπ ¡‘∂ÿπ“¬π æ.». 2545 ∂÷߇¥ ◊Õπ¡°√“§¡ æ.». 2546√Ÿª·∫∫°“√«‘®—¬ °“√»÷°…“·∫∫‰ª¢â“ßÀπ â“‚¥¬°“√∫√√¬“¬«‘∏ ’¥”‡π ‘π°“√«‘®—¬‰¥â√«∫√«¡¢âÕ¡Ÿ≈®“°ºŸâªÉ«¬„πÀÕºŸâªÉ«¬«‘°ƒµ∑“ßÕ“¬ÿ√°√√¡∑ ÿ°√“¬∑ ’ Ë¡’°“√∂Õ¥∑ àՙ૬À“¬„®‚¥¬‰¡à‰¥â¡’°“√«“ß·ºπ¡“°àÕπ √«¡∑ — Èß„™â°“√„À⧖·ππ‡æ ◊ ËÕª√–‡¡‘𧫓¡µâÕß°“√¬“§≈“¬ª√– “∑ ·≈–º≈∑ ’ ˵“¡¡“®“°°“√∂Õ¥∑àՙ૬À“¬„®º≈°“√»÷°…“ ºŸâªÉ«¬ 471 √“¬∑’Ë ‰¥â√ —∫°“√„ à∑àՙ૬À“¬„®„πÀÕºŸâªÉ«¬«‘°ƒµ∑“ßÕ“¬ÿ√°√√¡„π™à«ß∑ ’Ë∑”°“√»÷°…“8 ‡¥ ◊Õπæ∫«à“¡’ºŸâªÉ«¬ 21 √“¬¡’°“√∂Õ¥∑ àՙ૬À“¬„®‚¥¬‰¡à‰¥âµ—Èß„® 23 §√ — Èߧ‘¥‡ªìπ√ â âÕ¬≈– 4.9 à«π„À≠ à16 „π 23 §√—Èß (√ âÕ¬≈– 69.6) ‡°‘¥¢÷Èπ„π 48 ™—Ë«‚¡ß·√°À≈—ß„ à∑àՙ૬À“¬„® ”À√—∫‡«≈“∑ ’Ë¡’°“√∂Õ¥∑àՙ૬À“¬„®·∫∫‰¡àµ—Èß„®π — Èπ ‰¡àæ∫§«“¡·µ°µà“ßÕ¬à“ß¡’π —¬ ”§—≠√–À«à“ß·µà≈–√Õ∫¢Õß°“√∑”ß“π¢Õß∫ ÿ§≈“°√∑“ß°“√·æ∑¬å ®“°°“√„™â Motor activity assessment scales (MAAS) æ∫«à“¡’§à“µ—Èß·µà 4 ∂÷ß 6 ´÷ËßÀ¡“¬∂÷ß√–¥—∫§«“¡√ Ÿ â ÷°µ—«∑ ’ Ë°√–«π°√–«“¬·µà¬—ß„À⧫“¡√ à«¡¡ ◊Õ¥’ ‰ª®π∂ ÷ß°≈ ÿ à¡∑ ’ Ë¡’§«“¡°√–«π°√–«“¬¡“°®πÕ“®‡ªìπÕ—πµ√“¬‰¥â 17 „π 23 §√—ÈßÀ√◊Õ§‘¥‡ªìπ√âÕ¬≈– 73.9 ¢Õß°“√∂Õ¥∑àՙ૬À“¬„®·∫∫‰¡àµ—Èß„® Õ¬à“߉√°Áµ“¡æ∫«à“¡’‡æ’¬ß 1 √“¬‡∑à“π—Èπ„π°≈ ÿà¡π ’È∑’Ë ‰¥â√—∫°“√„À⬓‡æ◊ËÕ∫√√‡∑“§«“¡°√–«π°√–«“¬ ·≈– ¡’ 9 √“¬∑ ’ˉ¥â√—∫°“√¡—¥‡æ◊ËÕªÑÕß°—πÕ—πµ√“¬∑’ËÕ“®‡°‘¥¢÷Èπ‰¥â®“°§«“¡°√–«π°√–«“¬ ”À√—∫°“√„™â ventilation assessment scales (VAS)æ∫«à“¡’§à“®“° A ∂ ÷ß B ´÷ËßÀ¡“¬∂ ÷ß Õ¬ŸàÕ¬à“ß ∫“¬∂÷ß√–¥—∫∑ ’Ë¡’§«“¡‰¡à ∫“¬‡≈Á°πâÕ¬„π 21 ®“° 23 §√ —ÈߢÕß°“√∂Õ¥∑ àÕÀ“¬„®‡Õß (√ âÕ¬≈– 91.3) „π 23 §√ —Èß∑ ’Ë∂Õ¥∑àՙ૬À“¬„®‡Õßπ—Èπ ¡’ 12 §√ —Èß À√◊Õ√âÕ¬≈– 52.2 ∑’˵âÕ߉¥â√ —∫°“√„ à∑ àՙ૬À“¬„®°≈ —∫‡¢â“‰ª„À¡à´÷Ëß à«π¡“°µâÕß„ à„π 1 ™—Ë«‚¡ßÀ≈ —ß°“√∂Õ¥∑ àՙ૬À“¬„® ‰¡àæ∫º≈‡ ’¬√ ÿπ·√ß®“°°“√∂Õ¥∑ àՙ૬À“¬„®·∫∫‰¡àµ—Èß„® „π°≈ ÿ à¡∑ ’ ˵âÕß„ à∑ àՙ૬À“¬„®°≈ —∫‡¢â“‰ª„À¡à ·≈–°≈ ÿ à¡∑ ’ Ë “¡“√∂À“¬„®‰¥â‡ÕßÀ≈ —ß®“°∂Õ¥∑ àՙ૬À“¬„®π — Èπ æ∫«à“¡’§«“¡·µ°µà“ߪ√–°“√‡¥’¬«§ ◊Õª√ ‘¡“≥Õ“°“»„πÀπ ÷ Ëßπ“∑ ’∑ ’ ˇ§√◊ ËÕߙ૬À“¬„®™à«ß°àÕπ°“√∂Õ¥∑ àՙ૬À“¬„®¡’§à“ Ÿß°«à“Õ¬à“ß¡’π —¬ ”§—≠„π°≈ ÿ à¡∑ ’ ˵âÕ߉¥â√ —∫°“√„ à∑ àՙ૬

ªï∑ ’Ë 26 ©∫ —∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2548 Unplanned Extubation in Medical ICU 91
À“¬„®°≈—∫‡¢â“‰ª„À¡à§◊Õ ‡©≈ ’ˬ 11.1 ≈‘µ√µàÕπ“∑’‡∑’¬∫°—∫ 4.0 ≈‘µ√µàÕπ“∑’ (p ‡∑ à“°—∫ 0.027) ‰¡àæ∫§«“¡·µ°µà“ß„π¥â“πÕ“¬ÿ ‡æ» °“√«‘π‘®©—¬‚√§∑’ˇªì𠓇Àµÿ¢Õß°“√„ à∑àՙ૬À“¬„® ™à«ß‡«≈“∑’ˉ¥â√—∫°“√„ à∑àՙ૬À“¬„®¡“°àÕπ„π√–À«à“ß Õß°≈ÿà¡π ’È √ ÿª æ∫°“√∂Õ¥∑ àՙ૬À“¬„®‚¥¬‰¡àµ—Èß„® √âÕ¬≈– 4.9 à«π„À≠à‡°‘¥¢÷Èπ„π 48 ™—Ë«‚¡ß·√°À≈—ß„ à∑àՙ૬À“¬„®°“√¢“¥°“√„À⬓§≈“¬ª√– “∑„πºŸâªÉ«¬∑ ’Ë°√–«π°√–«“¬ Õ“®‡ªì𠓇ÀµÿÀπ÷Ëß °“√„™â Motor activity assess-ment scale (MAAS) Õ“®™à«¬∑”𓬰“√∂Õ¥∑ àՙ૬À“¬„®·∫∫‰¡àµ—Èß„®‰¥â´÷ËßµâÕß°“√°“√»÷°…“‡æ‘Ë¡‡µ‘¡ æ∫ºŸâªÉ«¬∑ ’ ˵âÕß„ à∑ àՙ૬À“¬„®°≈ —∫‡¢â“‰ª„À¡à √ âÕ¬≈– 52.2 ·≈–„π°≈ ÿ à¡π ’ ȵâÕß°“√°“√™à«¬‡À≈◊Õ®“°‡§√◊ ËÕߙ૬À“¬„®°àÕπ∂Õ¥∑àՙ૬À“¬„®¡“°°«à“°≈ÿà¡∑’ˉ¡àµâÕß„ à∑àՙ૬À“¬„®°≈—∫‡¢â“‰ª„À¡à
IntroductionUnplanned extubation (UE) is a major com-
plication of translaryngeal intubation occurring in3% to 16% of mechanically ventilated patients 1-11.Recent studies have clearly shown its impact onduration of mechanical ventilation, length of ICUand hospital stay, and need for chronic care, butnot on mortality 11. Factors contributing to this eventare multifactorial and not well clarified in adult pa-tients.
Patients in ICU face several unpleasant prob-lems from severe diseases and therapeutic inter-ventions. Agitated patients tend to have morechances of UE than normal. Sedation has beenaccepted as one of important methods to alleviateanxieties and difficulties in ICU patients. The motoractivity assessment scale (MAAS) has recently beenshown as a valid and reliable scoring system toassess levels of distress and consciousness andto evaluate adequate sedation in ICU setting12.Because most patients in ICU need ventilatory sup-port, some parameters such as high respiratoryrate, high airway pressure and frequent cough maybe helpful signs reflecting patient-ventilatorasynchrony or other discomforts in ventilatedpatients which may result in UE. Although the ven-
tilation-adjusted motor activity assessment scale(VA-MAAS) or ventilation assessment scale (VAS),have been used for more accuracy (13-15), its ben-efit over MAAS have not been clearly studied.
We prospectively studied incidence, clinicalcharacteristics, and outcome of UE in medical ICUin King Chulalongkorn Memorial Hospital, atertiary care university hospital. Two assessmentscales, MAAS and VAS, were applied for evalua-tion of adequacy of sedation in these patients.
MethodsKing Chulalongkorn Memorial Hospital is a
university hospital with 1400 beds. Of these, 358beds are in medical department. Two medical ICUsare an 8-bed closed unit each with the similarfacilities and criteria of admission. More than 80per cent of the patients need intubation and venti-latory assistance. Nursing care in both ICUs wasprovided by registered nurses experienced in ICUcare. Physicians, consisting of first-year residents,senior residents, attending staff physicians andattending pulmonologists, work as a team of24-hour coverage medical ICU care.
From June 1, 2002 to January 31, 2003, allmedical ICU patients who were intubated morethan 12 hours and had unplanned removal of
92 North Techawattanawanna et al. «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
endotracheal tube in medical ICU in KingChulalongkorn Memorial Hospital were includedin this study.
Endotracheal tubes were secured with clothadhesive tape, using the recommended çheadhalteré technique. Sedation was prescribed by at-tending physician based on individual judgement.Restraints were used as necessary by the nursingstaff after patient relativesû informed consent.Decisions regarding intubation, ventilatory support,weaning and extubation were based on standardmedical indication.
Unplanned extubation (UE) was defined aspatient’s extubation that could be done by thepatient himself (deliberately or accidentally) oraccidentally by members of the nursing andmedical staffs during procedures at the bedsideor transportation. Unplanned extubations weresubdivided into failure and success groups basedon whether or not reintubation was requiredwithin 72 hrs of extubation.
Data collectionA standard form detailing pertinent data sur-
rounding each UE case was completed byresearcher. Data included:
1. Clinical characteristics such as age, gen-der, diagnosis, duration of intubation, and outcomeof each patient.
2. Onset and nature of UE, MAAS, VAS,sedation, restraint, ventilatorûs settings, adverseevents related with UE, and reintubation. The MAASand VAS used was detailed in Table 1 and 2.Ethics
All medical treatment and nursing cares werejudged as indicated by physicians and nursing staffs.Patientsû consents were performed at the time ofadmission in all cases.
Statistical AnalysisUnpaired t-test and Chi-Square test were used
for evaluation of statistical difference between twocompared groups.
Do not move or response to noxious stimulusOpen eyes or raise eyebrows or turn head ormove limbs towards noxious stimulusOpen eyes or raise eyebrows or turn head ormove limbs when touched or calledConscious ,no stimulus is required to elicitmovement and follow commandsConscious ,no stimulus is required to elicitmovement and follow commands but picking atsheets or tubes or uncovering himselfDo not consistently follow commands andattempting to sit up or move limbs out of bedDo not follow any commands and attempting tosit up or thrashing side to side or trying to climbout of bed
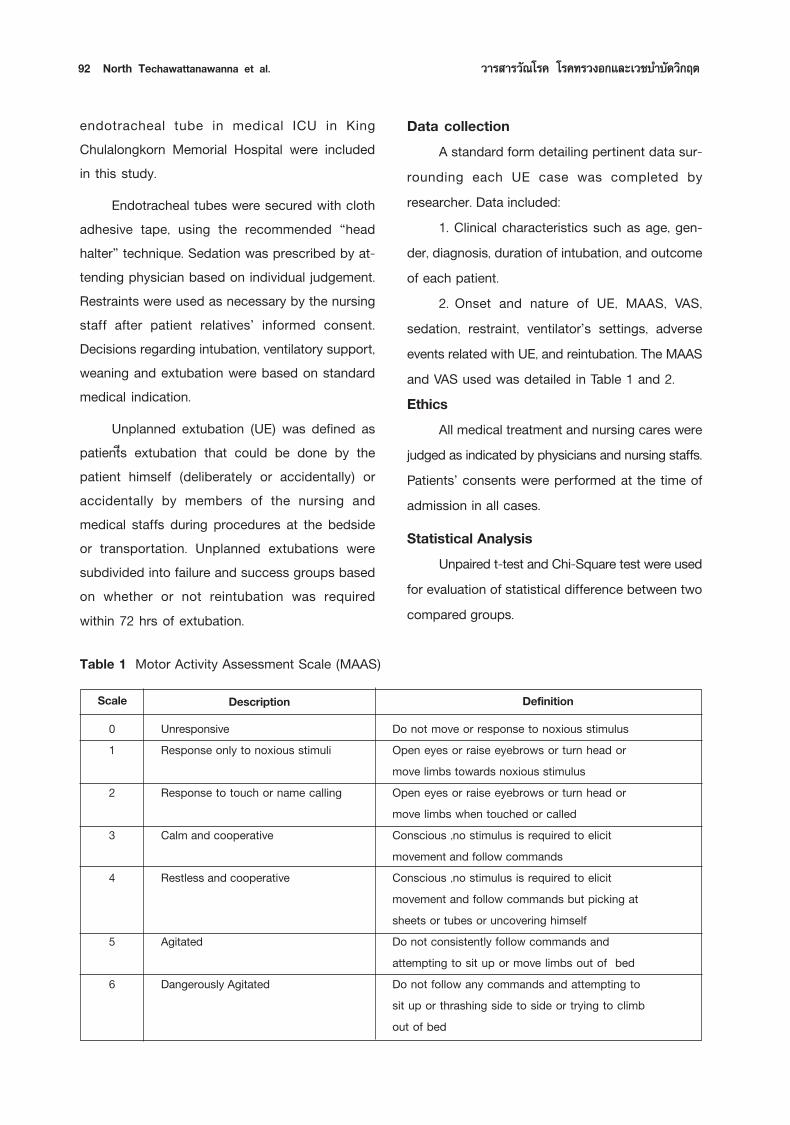
Table 1 Motor Activity Assessment Scale (MAAS)
DefinitionScale DescriptionUnresponsiveResponse only to noxious stimuli
Response to touch or name calling
Calm and cooperative
Restless and cooperative
Agitated
Dangerously Agitated
01
2
3
4
5
6
ªï∑ ’Ë 26 ©∫ —∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2548 Unplanned Extubation in Medical ICU 93
Table 2 Ventilation Assessment Scale (VAS)
Minimal coughing ,comfortable respiratory rate, rare high airway pres-sure or rate alarms, tolerable to any movement or stimulationCoughing, having high respiratory rate when stimulated but easily settledwith removal of stimulationFrequent episodes of coughing, or competing with the respirator, orhaving high respiratory rate or high airway pressure alarmsProlonged coughing, difficult to control ventilation or deliver adequatetidal volume
DefinitionScale Description
Comfortable
Mildly distress
Moderately distress
Markedly distress
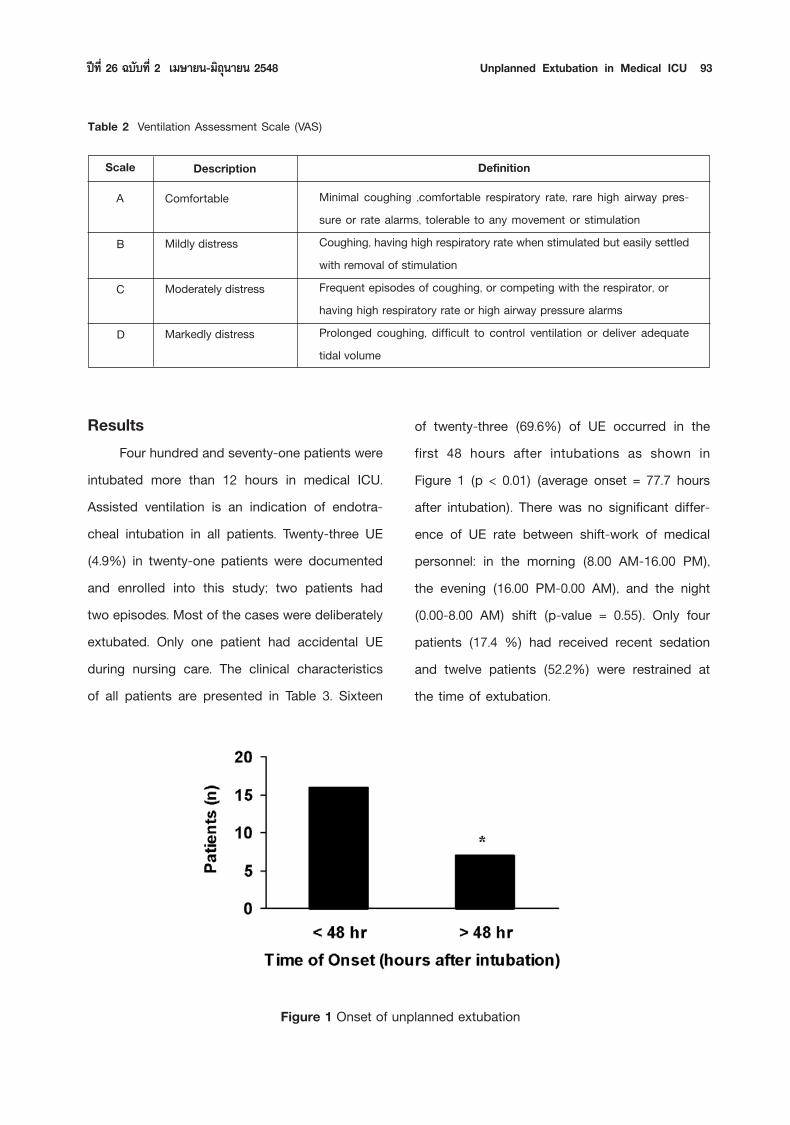
ResultsFour hundred and seventy-one patients were
intubated more than 12 hours in medical ICU.Assisted ventilation is an indication of endotra-cheal intubation in all patients. Twenty-three UE(4.9%) in twenty-one patients were documentedand enrolled into this study; two patients hadtwo episodes. Most of the cases were deliberatelyextubated. Only one patient had accidental UEduring nursing care. The clinical characteristicsof all patients are presented in Table 3. Sixteen
Figure 1 Onset of unplanned extubation
of twenty-three (69.6%) of UE occurred in thefirst 48 hours after intubations as shown inFigure 1 (p < 0.01) (average onset = 77.7 hoursafter intubation). There was no significant differ-ence of UE rate between shift-work of medicalpersonnel: in the morning (8.00 AM-16.00 PM),the evening (16.00 PM-0.00 AM), and the night(0.00-8.00 AM) shift (p-value = 0.55). Only fourpatients (17.4 %) had received recent sedationand twelve patients (52.2%) were restrained atthe time of extubation.
A
B
C
D
94 North Techawattanawanna et al. «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
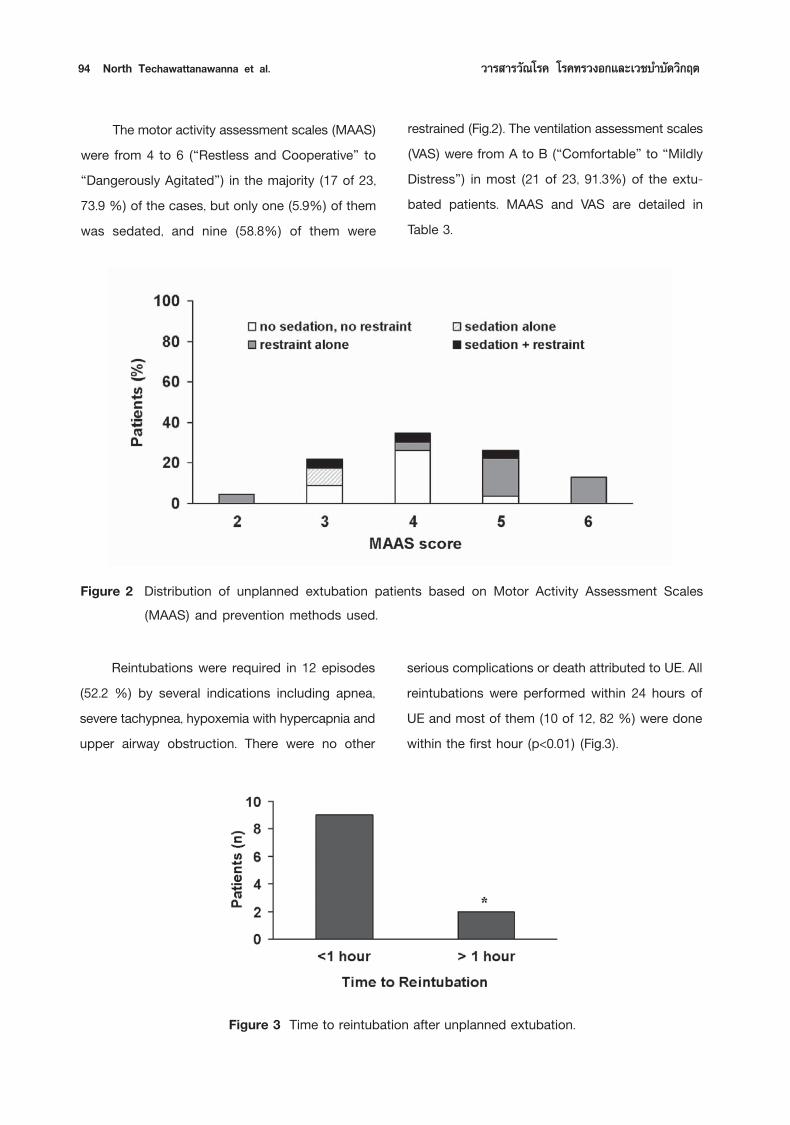
Figure 2 Distribution of unplanned extubation patients based on Motor Activity Assessment Scales(MAAS) and prevention methods used.
Figure 3 Time to reintubation after unplanned extubation.
Reintubations were required in 12 episodes(52.2 %) by several indications including apnea,severe tachypnea, hypoxemia with hypercapnia andupper airway obstruction. There were no other
serious complications or death attributed to UE. Allreintubations were performed within 24 hours ofUE and most of them (10 of 12, 82 %) were donewithin the first hour (p<0.01) (Fig.3).
The motor activity assessment scales (MAAS)were from 4 to 6 (çRestless and Cooperativeé toçDangerously Agitatedé) in the majority (17 of 23,73.9 %) of the cases, but only one (5.9%) of themwas sedated, and nine (58.8%) of them were
restrained (Fig.2). The ventilation assessment scales(VAS) were from A to B (çComfortableé to çMildlyDistressé) in most (21 of 23, 91.3%) of the extu-bated patients. MAAS and VAS are detailed inTable 3.
ªï∑ ’Ë 26 ©∫ —∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2548 Unplanned Extubation in Medical ICU 95
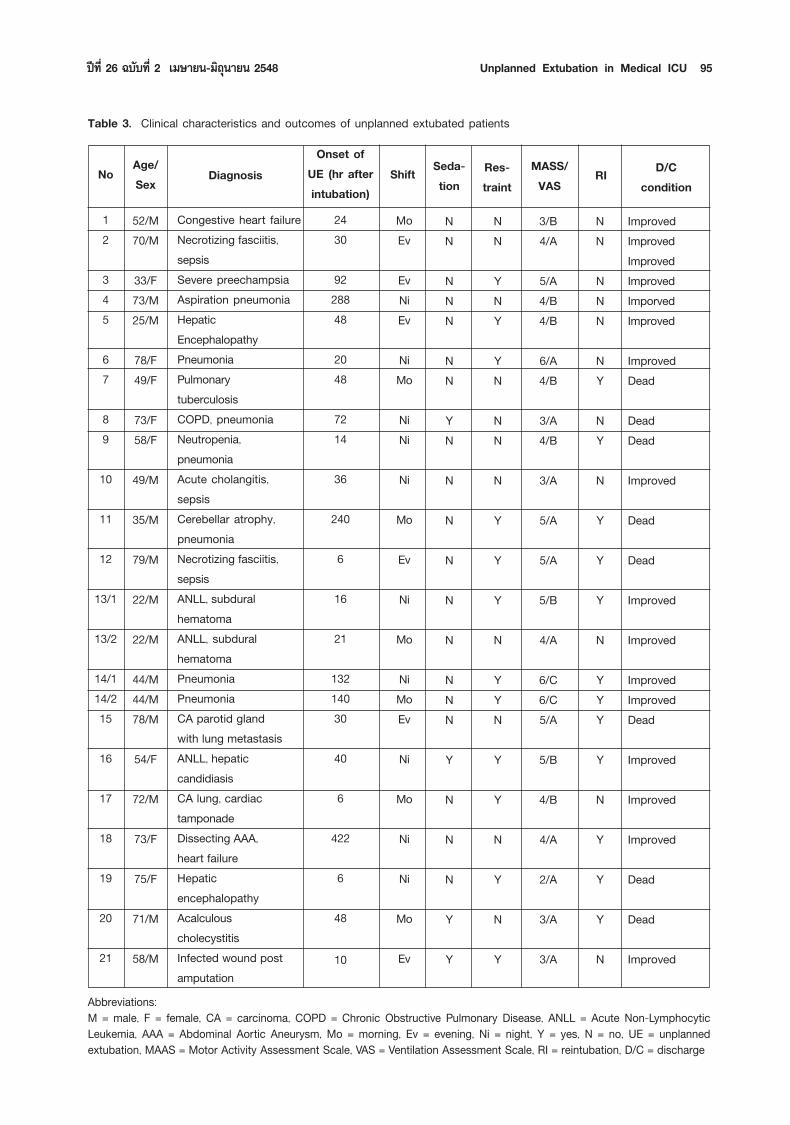
Table 3. Clinical characteristics and outcomes of unplanned extubated patients
12
345
67
89
10
11
12
13/1
13/2
14/114/215
16
17
18
19
20
21
52/M70/M
33/F73/M25/M
78/F49/F
73/F58/F
49/M
35/M
79/M
22/M
22/M
44/M44/M78/M
54/F
72/M
73/F
75/F
71/M
58/M
Congestive heart failureNecrotizing fasciitis,sepsisSevere preechampsiaAspiration pneumoniaHepaticEncephalopathyPneumoniaPulmonarytuberculosisCOPD, pneumoniaNeutropenia,pneumoniaAcute cholangitis,sepsisCerebellar atrophy,pneumoniaNecrotizing fasciitis,sepsisANLL, subduralhematomaANLL, subduralhematomaPneumoniaPneumoniaCA parotid glandwith lung metastasisANLL, hepaticcandidiasisCA lung, cardiactamponadeDissecting AAA,heart failureHepaticencephalopathyAcalculouscholecystitisInfected wound postamputation
2430
9228848
2048
7214
36
240
6
16
21
13214030
40
6
422
6
48
10
MoEv
EvNiEv
NiMo
NiNi
Ni
Mo
Ev
Ni
Mo
NiMoEv
Ni
Mo
Ni
Ni
Mo
Ev
NN
NNN
NN
YN
N
N
N
N
N
NNN
Y
N
N
N
Y
Y
NN
YNY
YN
NN
N
Y
Y
Y
N
YYN
Y
Y
N
Y
N
Y
3/B4/A
5/A4/B4/B
6/A4/B
3/A4/B
3/A
5/A
5/A
5/B
4/A
6/C6/C5/A
5/B
4/B
4/A
2/A
3/A
3/A
NN
NNN
NY
NY
N
Y
Y
Y
N
YYY
Y
N
Y
Y
Y
N
ImprovedImprovedImprovedImprovedImporvedImproved
ImprovedDead
DeadDead
Improved
Dead
Dead
Improved
Improved
ImprovedImprovedDead
Improved
Improved
Improved
Dead
Dead
Improved
Abbreviations:M = male, F = female, CA = carcinoma, COPD = Chronic Obstructive Pulmonary Disease, ANLL = Acute Non-LymphocyticLeukemia, AAA = Abdominal Aortic Aneurysm, Mo = morning, Ev = evening, Ni = night, Y = yes, N = no, UE = unplannedextubation, MAAS = Motor Activity Assessment Scale, VAS = Ventilation Assessment Scale, RI = reintubation, D/C = discharge
No Age/Sex Diagnosis
Onset ofUE (hr afterintubation)
Shift Seda-tion
Res-traint
MASS/VAS RI D/C
condition
96 North Techawattanawanna et al. «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
No.
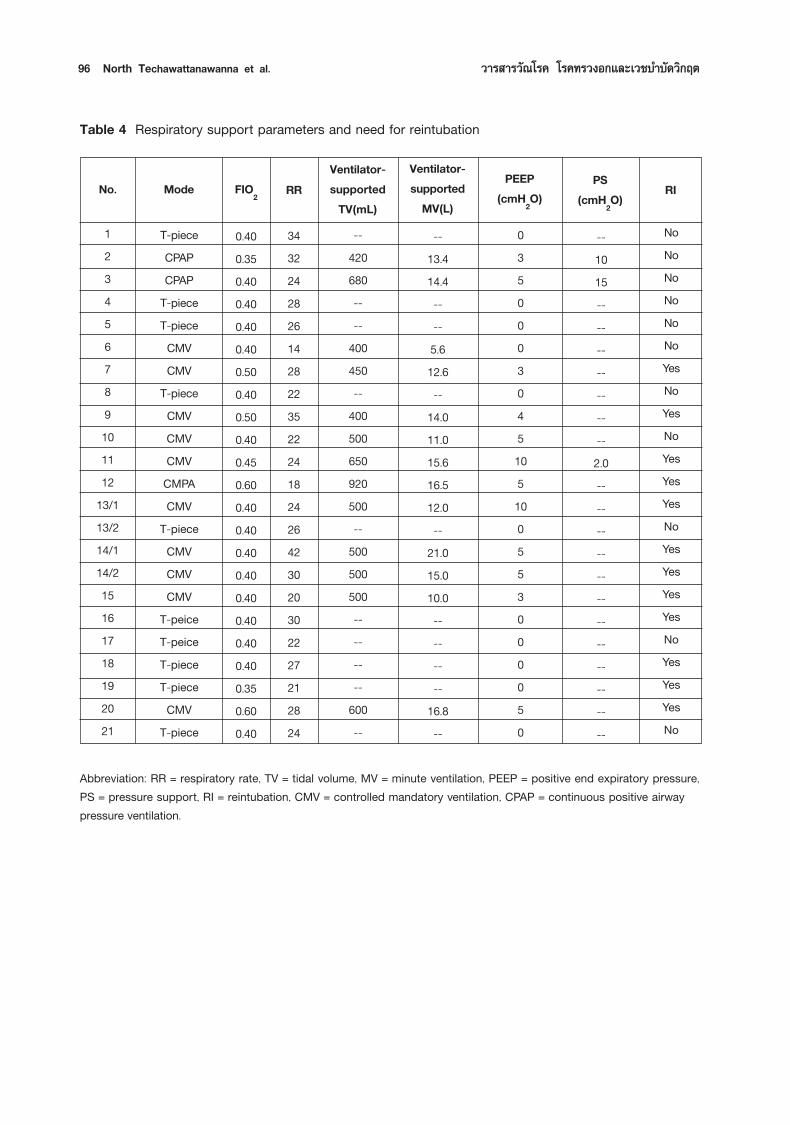
Table 4 Respiratory support parameters and need for reintubation
Mode FIO2 RRVentilator-supportedTV(mL)
Ventilator-supported
MV(L)
PEEP(cmH2O)
PS(cmH2O) RI
123456789101112
13/113/214/114/215161718192021
T-pieceCPAPCPAP
T-pieceT-pieceCMVCMV
T-pieceCMVCMVCMVCMPACMV
T-pieceCMVCMVCMV
T-peiceT-peiceT-pieceT-pieceCMV
T-piece
3432242826142822352224182426423020302227212824
0.400.350.400.400.400.400.500.400.500.400.450.600.400.400.400.400.400.400.400.400.350.600.40
--420680----
400450--
400500650920500--
500500500--------
600--
--13.414.4----5.612.6--
14.011.015.616.512.0--
21.015.010.0--------
16.8--
0350003045105100553000050
--1015--------------2.0------------------------
NoNoNoNoNoNoYesNoYesNoYesYesYesNoYesYesYesYesNoYesYesYesNo
Abbreviation: RR = respiratory rate, TV = tidal volume, MV = minute ventilation, PEEP = positive end expiratory pressure,PS = pressure support, RI = reintubation, CMV = controlled mandatory ventilation, CPAP = continuous positive airwaypressure ventilation.
ªï∑ ’Ë 26 ©∫ —∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2548 Unplanned Extubation in Medical ICU 97
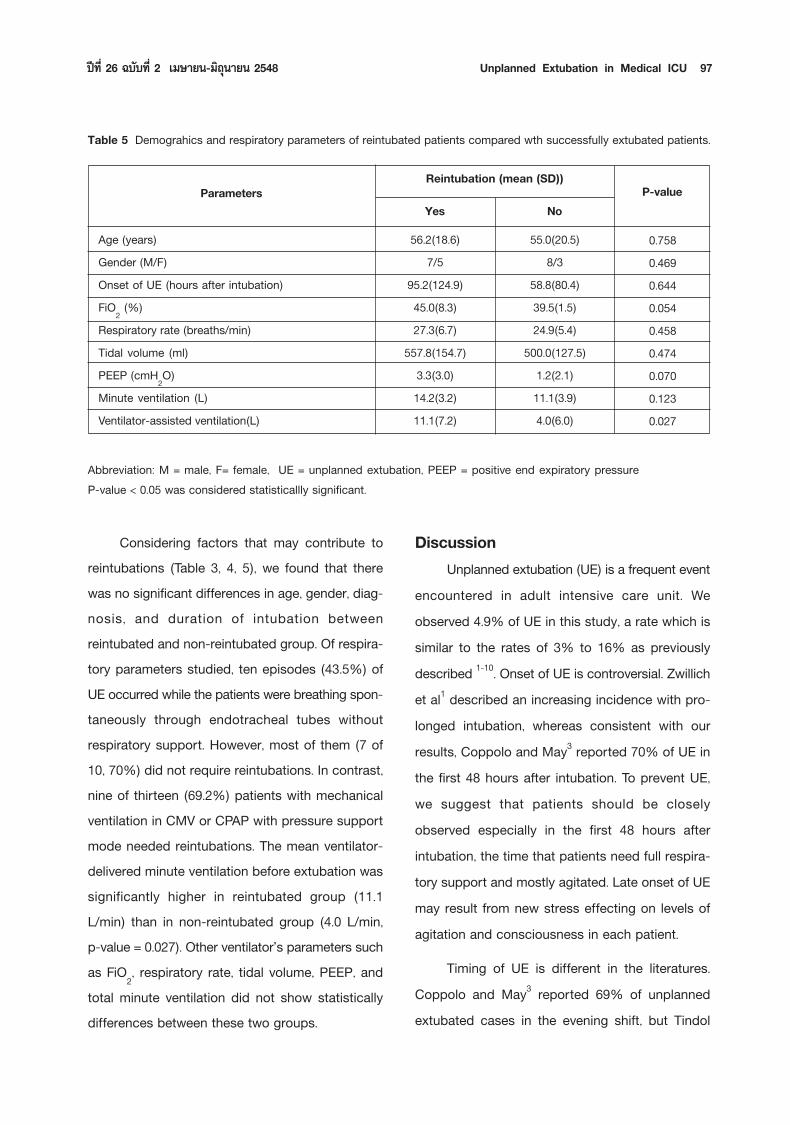
Table 5 Demograhics and respiratory parameters of reintubated patients compared wth successfully extubated patients.
Reintubation (mean (SD))Parameters
YesAge (years)Gender (M/F)Onset of UE (hours after intubation)FiO2 (%)Respiratory rate (breaths/min)Tidal volume (ml)PEEP (cmH2O)Minute ventilation (L)Ventilator-assisted ventilation(L)
NoP-value
0.7580.4690.6440.0540.4580.4740.0700.1230.027
56.2(18.6)7/5
95.2(124.9)45.0(8.3)27.3(6.7)
557.8(154.7)3.3(3.0)14.2(3.2)11.1(7.2)
55.0(20.5)8/3
58.8(80.4)39.5(1.5)24.9(5.4)
500.0(127.5)1.2(2.1)11.1(3.9)4.0(6.0)
Abbreviation: M = male, F= female, UE = unplanned extubation, PEEP = positive end expiratory pressureP-value < 0.05 was considered statisticallly significant.
DiscussionUnplanned extubation (UE) is a frequent event
encountered in adult intensive care unit. Weobserved 4.9% of UE in this study, a rate which issimilar to the rates of 3% to 16% as previouslydescribed 1-10. Onset of UE is controversial. Zwillichet al1 described an increasing incidence with pro-longed intubation, whereas consistent with ourresults, Coppolo and May3 reported 70% of UE inthe first 48 hours after intubation. To prevent UE,we suggest that patients should be closelyobserved especially in the first 48 hours afterintubation, the time that patients need full respira-tory support and mostly agitated. Late onset of UEmay result from new stress effecting on levels ofagitation and consciousness in each patient.
Timing of UE is different in the literatures.Coppolo and May3 reported 69% of unplannedextubated cases in the evening shift, but Tindol
Considering factors that may contribute toreintubations (Table 3, 4, 5), we found that therewas no significant differences in age, gender, diag-nosis, and duration of intubation betweenreintubated and non-reintubated group. Of respira-tory parameters studied, ten episodes (43.5%) ofUE occurred while the patients were breathing spon-taneously through endotracheal tubes withoutrespiratory support. However, most of them (7 of10, 70%) did not require reintubations. In contrast,nine of thirteen (69.2%) patients with mechanicalventilation in CMV or CPAP with pressure supportmode needed reintubations. The mean ventilator-delivered minute ventilation before extubation wassignificantly higher in reintubated group (11.1L/min) than in non-reintubated group (4.0 L/min,p-value = 0.027). Other ventilatorûs parameters suchas FiO2, respiratory rate, tidal volume, PEEP, andtotal minute ventilation did not show statisticallydifferences between these two groups.

98 North Techawattanawanna et al. «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
et al7 found that the morning shift, while physi-cians are making rounds, families are visiting, andnew orders are being carried out-activities thatlead to increased distractions for the staff, hadthe highest incidence. Our results showed nosignificant difference between shifts suggestingthat timing of extubation events may dependon patientsû condition, different hospitalûs workschedule and interfering circumstances.
Although factors contributing in UE are still indebate, we hypothesized that inadequate seda-tion plays an important role. Correlation of themotor activity assessment scale (MAAS) and UErevealed that majority (17 of 23, 73.9 %) of thecases occurred when the patients were restlessor agitated, but only one (5.9%) of them wassedated, and nine (58.8%) of them were restrained.It may be considered that sedation in our ICU maybe overlooked in some cases. Inadequate sedationin agitated patients is one of predisposing factorsfor UE4 and may place critically ill patients in dan-ger of self-injury10,16. In contrast, adequate seda-tion and analgesia delivered by continuous infu-sion may prevent UE in alert, intubated patient17.In some studies, it has been suggested thatrestrained, agitated patients who extubated them-selves should have been attached more securely7,18,
however, determined patients are often able toextubate themselves even when they are stronglyrestrained3. Adequate intravenous sedation shouldbe used to control harmful agitation in criticalcare19,20, however, oversedation may prolong wean-ing and intubation. Monitoring and adjusting dos-ages of sedation is crucial to balance its appro-priateness. Additionally, high percentage of restraintin agitated patient could result from contraindications
of sedation in some diseases such as hepaticencepahalopathy, neurological diseases that con-sciousness needs to be closely observed. In othercases, sedation should be considered beforerestraint in prevention of harm in agitated patients.
Ventilation assessment scale (VAS) has beendescribed as a good scoring system used inventilator-assisted patients. However, we found thatVAS is not sensitive enough to evaluate adequacyof sedation or predict UE. Additionally, two eventsthat have çCé from VAS scoring have MAAS scoreequals to 6 reflecting that VAS did not increasebenefits of MAAS in our study (Table 3). We sug-gest that MAAS scoring system should be used asa predictor of UE in medical ICU, which need to beevaluated in the larger population.
Although UE did not affect mortality in ICUpatients, it could result in serious complications3, 21, 22.
We observed immediate laryngeal complications in1 of 23 events. Cautious clinical evaluation canoften avoid immediate reintubation of extubatedpatient1,3,6, but reintubation remains necessary in31% to 78% of the patient3,7. In our series,reintubations were required in 52.2 % after UEwith indications including apnea, tachypnea,hypoxemia, hypercapnia and upper airway obstruc-tion. Patients who had successfully UE implydelayed planned extubation and stress the impor-tance of weaning protocol in ICU.
We found that preextubation ventilatory sup-port is the sole factor associated with reintubation.Most of UE that occurred during spontaneousbreathing through endotracheal tubes did notrequire reintubations. In contrast, most of UE caseswith preextubation ventilatory support by controlled

ªï∑ ’Ë 26 ©∫ —∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2548 Unplanned Extubation in Medical ICU 99
mandatory ventilation (CMV) or pressure supportventilation (PSV) needed reintubations. Reintubatedgroup has higher mean preextubation ventilator-delivered minute ventilation than non-reintubatedgroup (11.1, 4.0 L respectively, p-value = 0.027). Ofthe predictors of successful termination of ventila-tory support, Whelan et al6 reported significantlyhigher preextubation FiO2 and ventilator-deliveredminute ventilation in patients who requirereintubation than successfully-extubated patients.Chenûs work23 supported indirectly that respiratoryfailure caused by pneumonia is the most importantpredictor of reintubation. Although our studies didnot show the difference of preextubation FiO2between these two groups, the p-value is nearlysignificant (p = 0.054). In addition to the need ofCMV, Jayamanne and coworkers24 noted thatmultisystem failure and altered mental status alsohave strong association with reintubation. Due tovarious factors contributing to reintubation, Listelloet al5 later developed seven parameters to deter-mine the likelihood of reintubation in self-extubatedpatient.
In conclusion, we reported 4.9% of UE inmedical ICU patients. Outcome of UE is good.Reintubations were required in half of the cases,and associated with degrees of ventilatory supportbefore extubation documented by ventilator-deliv-ered minute ventilation. Lack of sedation in agi-tated patients is one of the predisposing factorsfor UE, which may be predicted by the motoractivity assessment scale (MAAS). To solve thisproblem, an action plan consisting of educationand awareness of risks associated with UE, stan-dard protocols for weaning and sedation in ICUshould be developed based on individual ICU with
cooperation of all medical personnel25. Survey ofUE could be used as one of parameters evaluat-ing quality of ICU cares.
References1. Zwillich CW, Pierson DJ, Creagh CE, Sutton FD, Schatz
E and Petty TL. Complications of assisted ventilation:a prospective study of 354 consecutive episodes.Am J Med 1974;57:161-170.
2. Stauffer JL, Olson DE and Petty TL. Complicationsand consequences of endotracheal intubation andtracheotomy. A prospective study of 150 critically illadult patients. Am J Med 1981;70:65-76.
3. Coppolo DP and May JJ. Self-extubations: A12-month experience. Chest 1990; 98:165-169.
4. Vassal T, Anh NGD, Gabillet JM, Guidet B, StaikowskyF and Offenstadt G. Prospective evaluation of self-extubations in a medical intensive care unit. IntensiveCare Med 1993;19:340-342.
5. Listelo D and Sessler CN. Unplanned extubation: clinicalpredictors for reintubation. Chest 1994; 105:1496-1503.
6. Whelan J, Simpson SQ and Levy H. Unplannedextubation. Predictors of successful termination ofmechanical ventilatory support. Chest 1994;105:1808-1812.
7. Tindol GA Jr, DiBenedetto RJ and Kosciuk L.Unplanned extubations. Chest 1994; 105:1804-1807.
8. Chevron V, Menard JF, Richard JC, Girault C, Leroy Jand Bonmarrchand G. Unplanned extubation: riskfactors of development and predictive criteria forreintubation. Crit Care Med 1998;26:1049-1053.
9. Betbese AJ, Perez M, Bak E, Rialp G and ManceboJ. A prospective study of unplanned endotrachealextubation in intensive care unit patients. Crit CareMed 1998;26:1180-1186.
10. Boulain T. Unplanned extubations in the adult inten-sive care unit: A prospective multicenter study. Am JRespir Crit Care Med 1998;157:1131-1137.
11. Epstein SK, Nevins ML and Chung J. Effect ofunplanned extubation on outcome of mechanical

100 North Techawattanawanna et al. «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
ventilation. Am J Respir Crit Care Med 2000;161:1912-1916.
12. Devlin JW, Boleski G, Mlynarek M, et al. Motor activ-ity assessment scale: A valid and reliable sedationscale for use with mechanically ventilated patients inan adult surgical intensive care unit. Crit Care Med1999; 27: 1271-1275.
13. Clemmer TP, Wallace JC, Spuhler VJ, Bailey PP andDevlin JW. Origins of the motor activity assessmentscore: a multi-institutional process. Crit Care Med2000;28:3124.
14. De Jonghe B, Cook D, Appere-De-Vecchi C, GuyattG, Meade M and Outin H. Using and understandingsedation scoring systems: a systematic review.Intensive Care Med 2000;26:275-285.
15. Carrasco G. Instruments for monitoring intensive careunit sedation. Crit Care 2000;4:217-225.
16. Powers J. A sedation protocol for preventing patientself-extubation. Dimens Crit Care Nurs 1999;18:30-34.
17. Balon JA. Common factors of spontaneous self-extu-bation in a critical care setting. Int J Trauma Nurs2001;7:93-99.
18. Branstetter RD, Khawaja IT and Bartky E. Self-extu-bation. Chest 1991;99:1319-1320.
19. Windsor D, Ward B, Albrant D, Roma M, Trask Aand Rainey T. Reduction of unintentional extubationsamong agitated ICU patients: an algorithm for seda-tion (abstract). Crit Care Med 1995;23: A46.
20. Ramsay MAE, Savege TM, Simpson BRJ and GoodwinR. Controlled sedation with alpharealone-alphadalone.BMJ 1974;2:656-659.
21. Rashkin MC and Davis T. Acute complications ofendotracheal intubation: relationship to reintubation,route, urgency, and duration. Chest 1986;89:165-167.
22. Blanc VF and Tremblay NAG. The complications oftracheal intubation: a new classification with a reviewof literature. Anesth Analg 1974;53:202-213.
23. Chen CZ, Chu YC, Lee CH, Chen CW, Chang HYand Hsiue TR. Factors predicting reintubation afterunplanned extubation. J Formos Med Assoc.2002;101:542-546.
24. Jayamanne D, Nandipati R and Patel D. Self-extuba-tion: a prospective study. (abstract) Chest 1998;94(Suppl.1): 3S.
25. Maguire GP, DeLorenzo LJ and Moggio RA. Unplannedextubation in the intensive care unit: a quality-of-careconcern. Crit Care Nurs Q 1994;17:40-47.
ªï∑ ’Ë 26 ©∫ —∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2548 Perception of Exertional Dyspnea, Pulmonary Functionœ 101
PERCEPTION OF EXERTIONAL DYSPNEA,PULMONARY FUNCTION AND EXERCISE
TOLERANCE IN THAI PATIENTS WITH CHRONICOBSTRUCTIVE PULMONARY DISEASE
Natpatou Sanguanwongse M.D.
Department of Medicine, Bamrasnaradura Institute, Nonthaburi
«“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫—¥«‘°ƒµThai Journal of TuberculosisChest Diseases and Critical Care
Abstract :Study Objectives: 1. To find the pulmonary function parameters that could predict the exercisetolerance in both subjective and objective evidence 2. To verify the correlation between the changeof pulmonary function and the perception of exertional dyspnea as well as the work at the level ofmaximal exertional dyspnea. 3. To assess whether the pulmonary function is really worsening duringexertional dyspnea.Design: The cross-sectional study.Patients and Method: Fifteen patients with stable COPD and functional and class I-II, wererecruited. The spirometry, lung volume and capacity studies were performed before and after theexercise. An incremental symptom-limited exercise test was performed by using an electrical brakedcycle ergometer. The degree of exertional dyspnea was evaluated by using the modified Borg scaleat the baseline. A visual analog scale was used to measure the change of dyspnea after exercise.Results: It w as found that some baseline pulmonary function parameters correlated with evidenceof exertional dyspnea. Additionally, baseline FEV1 had not only the best significant negative corre-lation with perceptional dyspneic symptom but also had the best significant positive correlation withexercise tolerance. After the patients felt exertional dyspneic, there was significant worsening in FEV1.
Received for publication January 21, 2005
102 Natpatou Sanguanwongse «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
INTRODUCTIONThe perception of dyspnea varies consider-
ably among COPD patients with similar degreesof airflow limitation.1,2 It was postulated that anincreased central output with ineffective inspira-tory muscle response3-6 and the development ofdynamic hyperinflation (DH)7,8 contributed to thecause of exertional dyspnea. The relationshipbetween the resting pulmonary function and exer-cise tolerance had been extensively studied in thisgroup of patients.9,13 In most previous studies,they found loose association between maximalexercise capacity (Wmax) and Forced expiratoryvolume in one second (FEV1), Forced vital capac-ity (FVC) or even Diffusing lung capacity (DLCO).9,11
Conclusion: FEV1 might be used as the predictor of exercise tolerance in patients with COPD.When the patients felt exertional dyspneic, there would be a real change in FEV1. The suggestionof an inhaled bronchodilator as needed based on symptom should thus be reasonable.∫∑§—¥¬àÕ : π“Ææ∏ Ÿ ß«π«ß»å. §«“¡√ Ÿ â ÷°‡Àπ◊ ËÕ¬‡¡ ◊ ËÕÕÕ°°”≈ —ß°“¬, ¡√√∂¿“æªÕ¥·≈–°“√∑πµàÕ°“√ÕÕ°°”≈—ß°“¬„πºŸâªÉ«¬‚√§ªÕ¥Õÿ¥°—Èπ‡√◊ÈÕ√—߉∑¬. «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫—¥«‘°ƒµ 2548;26:101-109.¿“§«‘™“Õ“¬ÿ√»“ µ√ å ∂“∫ —π∫”√“»π√“¥Ÿ√ ππ∑∫ ÿ√’«—µ∂ÿª√– ߧå 1. ‡æ ◊ ËÕÀ“«‘∏ ’µ√«® ¡√√∂¿“æªÕ¥∑ ’ Ë “¡“√∂欓°√≥ å°“√∑πµàÕ°“√ÕÕ°°”≈ —ß°“¬„πºŸâªÉ«¬‚√§ªÕ¥Õÿ¥°—Èπ‡√◊ÈÕ√—ß 2. ‡æ ◊ ËÕÀ“§«“¡ —¡æ—π∏ å¢Õß°“√‡ª≈ ’ ˬπ·ª≈ß ¡√√∂¿“æªÕ¥ §«“¡√ Ÿ â ÷°‡Àπ◊ ËÕ¬‡¡ ◊ ËÕÕÕ°°”≈ —ß·≈–ß“π∑ ’ Ë∑”¢≥–∑ ’ ˇÀπ◊ ËÕ¬¡“°∑ ’ Ë ÿ¥ 3. ‡æ ◊ ËÕæ‘ Ÿ®π å«à“¢≥–∑ ’ Ë√ Ÿ â ÷°‡Àπ◊ ËÕ¬‡¡ ◊ ËÕÕÕ°°”≈ —ßπ — Èπ ¡√√∂¿“æªÕ¥·¬à≈ß®√‘ßÀ√◊Õ‰¡à«‘∏’°“√»÷°…“ ‡ªìπ·∫∫ cross sectional study ºŸâªÉ«¬‡ªìπ‚√§ªÕ¥Õÿ¥°—Èπ‡√◊ÈÕ√—ß√ ÿπ·√ß√–¬–∑ ’Ë 1 ·≈– 2 ∑ ’ˉ¡à¡’Õ“°“√°”‡√ ‘∫ 11 √“¬ ∑ ÿ°√“¬‰¥â√—∫°“√µ√«® ‰ª‚√‡¡µ√ ’¬å ª√ ‘¡“µ√ §«“¡®ÿ¢Õߪե°àÕπ·≈–À≈—ßÕÕ°°”≈—ß°“¬(„™â‡§√◊ËÕß electrical braked cycle ergometer) √–¥—∫°“√‡Àπ◊ËÕ¬°àÕπÕÕ°°”≈—ß«—¥¥â«¬ modified Borg scale√–¥—∫°“√‡ª≈’ˬπ·ª≈ߧ«“¡‡Àπ◊ËÕ¬À≈—ß°“√ÕÕ°°”≈—ß°“¬«—¥¥â«¬ Visual analog scaleº≈°“√»÷°…“ æ∫«à“ ¡√√∂¿“æªÕ¥‚¥¬‡©æ“– FEV1 °àÕπ°“√»÷°…“ —¡æ—π∏ å°—∫Õ“°“√‡Àπ◊ ËÕ¬‡¡ ◊ ËÕÕÕ°°”≈ —ß°“√µ√«® ¡√√∂¿“æªÕ¥‚¥¬‡©æ“– FEV1 —¡æ—π∏凪ìπ —¥ à«π°≈—∫°—∫§«“¡√Ÿâ ÷°‡Àπ◊ËÕ¬‡¡◊ËÕÕÕ°°”≈—ß°“¬·≈–‡ªìπ —¥ à«π‚¥¬µ√ß°—∫°“√∑π∑“πµàÕ°“√ÕÕ°°”≈ —ß æ∫«à“‡¡◊ËÕºŸâªÉ«¬√Ÿâ ÷°‡Àπ◊ËÕ¬¡“°¢÷Èπ®–¡’ FEV1 ≈¥πâÕ¬≈ß √ÿª ‡™◊ËÕ«à“ FEV1 ®–‡ªìπµ—«æ¬“°√≥ 姫“¡∑π∑“πµàÕ°“√ÕÕ°°”≈—ß°“¬„πºŸâªÉ«¬ COPD ·≈–°“√„À⬓¢¬“¬À≈Õ¥≈¡‡¡◊ËÕºŸâªÉ«¬√ Ÿâ ÷°‡Àπ◊ËÕ¬ π —Èπ¡’‡Àµÿº≈‡æ’¬ßæÕ
Recently, it has been shown that indicesrelated to dynamic hyperinflation, such as inspira-tory capacity (IC), are more closely relatedto exercise tolerance than FEV1.
12,13 With COPDpatients tidal volume (VT) during exercise increasesonly at the expense of the inspiratory reservevolume (IRV); thus the maximal VT during exercise(VT max) should depend mostly on the magnitudeof resting IC. Since Wmax is related to VT max,there should be a close association of Wmax andIC.7,14
The inhaled bronchodilator reduces exerciseDH and improves inspiratory pressure reserve andneuroventilator coupling. So the change in DH and

ªï∑ ’Ë 26 ©∫ —∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2548 Perception of Exertional Dyspnea, Pulmonary Functionœ 103
neuroventilatory coupling may be the maindeterminants in reducing breathlessness7. However,the inhaled bronchodilator is usually prescribed;as needed, therefore, the frequency and dosageof the inhaled bronchodilator may be directlyrelated to the perception both of the dyspneicsymptom and the level of symptom relief affordedby the medication. To our knowledge, the correla-tion between the perception of exertional dyspneaand the baseline pulmonary function or even thechange of pulmonary function after exertionaldyspnea have never been investigated in Thaipatients with COPD.
The goals of this study are, firstly, to find thepulmonary function parameters that could predictthe exercise tolerance in the patients with COPDand, secondly, to verify the correlation betweenthe change of pulmonary function after exerciseand the perception of exertional dyspnea, as wellas the work at the level of maximal exertionaldyspnea, as exercise tolerance.
Materials and MethodsSubjects
Fifteen Thai male COPD patients, with func-tional class I-II according to the New York HeartAssociation function Classification were recruited.The diagnosis was made according to GOLD guide-lines15. All patients had previously attended theCOPD clinic at Siriraj Hospital and had beenreceiving the optimal medical therapy for at least8 weeks before being enrolled. Their clinical andfunctional classes were stable at the time of thestudy, i.e., there were no exacerbation, no changein the dosage of bronchodilator medication and nosignificant change in spirometric values during the
preceding 8 weeks. All patients had stopped smok-ing for at least 6 months before the study. Nonewas participating in a respiratory training programnor was receiving home oxygen therapy or homenoninvasive mechanical ventilation. All of themagreed to participate in the study and signed theinformed consent form.
The patients were excluded if they hadevidence of asthma, other concomitant lungdiseases, cardiovascular diseases, peripheralvascular diseases, neuromuscular diseases, mus-culoskeletal disorders or other disabling condi-tions that would interfere with the tests. The studywas also stopped if the patients were unable tocooperate, or had oxygen desaturation of less than80% in room air during exercise.
MethodsPulmonary function tests
Each patient underwent pulmonary functionstudies, including the spirometry and lung volumewith capacity study, both before and after exer-cise. All pulmonary function tests were measuredthree times (using spirometer: Sensor-Medics Vmax229; Yorba Linda, CA). The acceptance of spiro-metric data was made according to the AmericanThoracic Society standard15. Absolute lung volumewas measured with the nitrogen washout method(Sensor-Medics Vmax 229: Yorba Linda, CA).The reference values from the reference spiro-metric values for healthy lifetime nonsmokersin Thailand17 were used. Because there was nocurrent equation for predicting normal spirometricIC value, a predicted normal value for IC wascalculated as predicted TLC minus predicted FRC.Oxygen saturation was indirectly measured usingspulse oxymeter (BCI international 3301; Waukesha,Wisconsin).

104 Natpatou Sanguanwongse «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
Perception of exertional dyspneaSymptom severity was assessed using two
scales: a modified Borg scale18 and a visual ana-log scale (VAS).19 The modified Borg scale wasbaseline evaluated before the exercise. The VASwas used after the exertional dyspnea to rate anychanges in their sensation compared with theirbaseline states.
The modified Borg scale is from 0 to 10; thesubject was instructed that 0 represented no dys-pneic sensation at all and that 10 represented themost severe dyspneic sensation that they couldimagine. The VAS was an interval scale, which wasanchored at one end by ùvery much betterû and atthe other end by ùvery much worseû. The middle ofthe scale was marked with the phrase ùno changeû.The VAS was 20 cm. in length and a value in cm.was measured from the ùno changeû point to thepoint marked by the subject on the scale.
Exercise studyAn incremental symptom-limited exercise test
was performed using an electrical braked cycleergometer (Sensor medics: Yorba Linda, CA).Subjects were cycled at the rate of 50-60 revolu-tion-min-1 (rmp), with the external power startedat 60% of target work rate ( = (53.76* measuredFEV1) -11.07) 20 for 5 minutes and then increasedthe work rate 10% each minute until their maxi-mal work rate was called as ùWfinalû and the totalwork load (Wtotal) was calculated as the sum ofthe work rate at each step of exercise (fromstart to finish) multiplied at each step.
Nevertheless, if the patient stopped the exer-cise because of leg fatigue or other causes other
than exertional dyspnea, he then would beexcluded from the study.
Statistical analysisData were presented as mean ± S.D. The
conventional level of statistical significance (p < 0.05)was used for all analyses. The association betweenWfinal, Wtotal or VAS (dependent variables) and thebaseline Borg scale, the resting pulmonary func-tion, and the change of pulmonary function afterexertional dyspnea (independent variables) weredetermined using Pearsonûs correlation co-efficiencyanalysis. The best-value was selected as thestrongest significant contributor.
ResultsFifteen patients from the COPD clinic of the
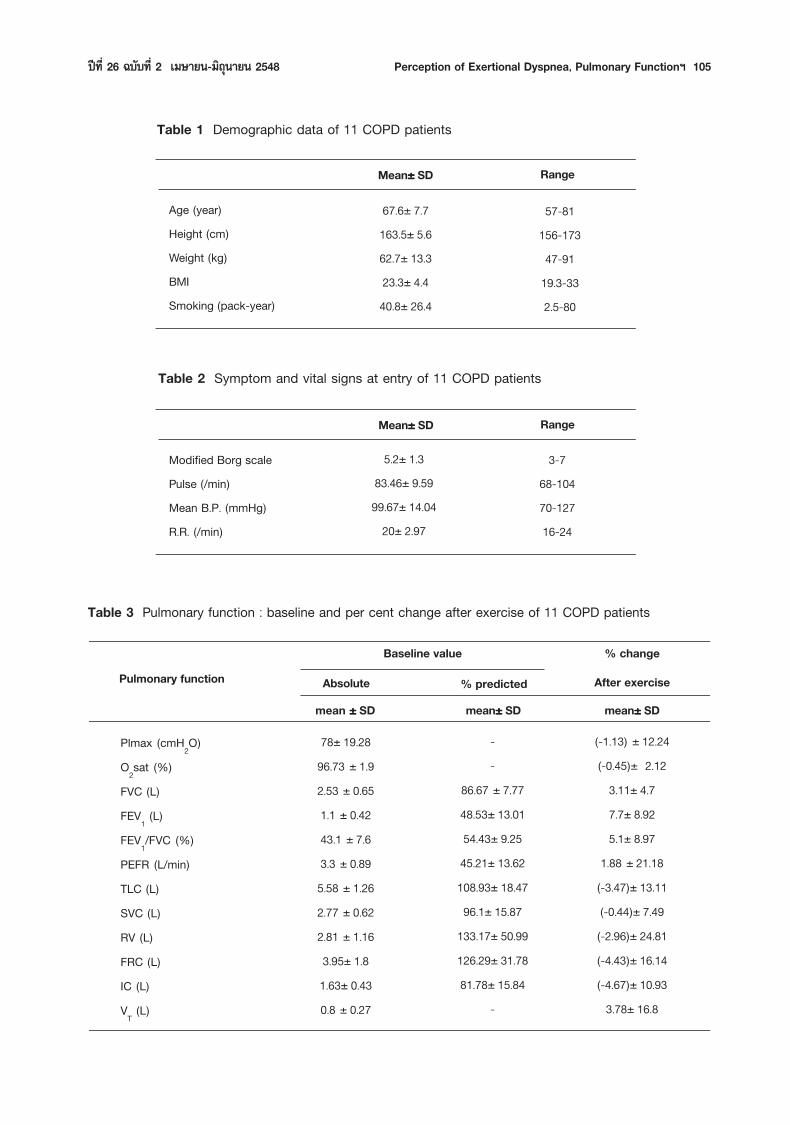
Division of Respiratory Disease and Tuberculosis,Department of Medicine, Faculty of Medicine SirirajHospital, were recruited; four patients were excluded,ie, two patients were not able to complete thepulmonary function test and two patients stoppedthe exercise due to leg fatigue. Only 11 patientsûdata were analyzed. The patientsû demographic data,baseline modified Borg scale and baseline pulmo-nary function are shown in Table 1 to 3. The meanage was 67.6 year with appropriate mean BMI(23.3) and all had normal mean baseline vitalsigns. The baseline Borg scale ranged from 3 to 7.The mean FEV1 was 48.53% predicted and themean FEV1/FVC ratio was 54.43% predicted. Mostpatients had lung hyperinflation as reflected byhigh RV (mean 133% predicted) and high TLC(mean 108.93% predicted). The mean PImax was78 cm H2O. None had hypoxemia at rest orafter exercise.
ªï∑ ’Ë 26 ©∫ —∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2548 Perception of Exertional Dyspnea, Pulmonary Functionœ 105
Mean±±±±± SD Range
Age (year)Height (cm)Weight (kg)BMISmoking (pack-year)
67.6± 7.7163.5± 5.662.7± 13.323.3± 4.440.8± 26.4
57-81156-17347-9119.3-332.5-80
Mean±±±±± SD Range
Modified Borg scalePulse (/min)Mean B.P. (mmHg)R.R. (/min)
5.2± 1.383.46± 9.5999.67± 14.04
20± 2.97
3-768-10470-12716-24
Plmax (cmH2O)O2sat (%)FVC (L)FEV1 (L)FEV1/FVC (%)PEFR (L/min)TLC (L)SVC (L)RV (L)FRC (L)IC (L)VT (L)
Pulmonary functionBaseline value
Table 2 Symptom and vital signs at entry of 11 COPD patients
Table 1 Demographic data of 11 COPD patients
Table 3 Pulmonary function : baseline and per cent change after exercise of 11 COPD patients
% change
After exercisemean±±±±± SD
(-1.13) ± 12.24(-0.45)± 2.12
3.11± 4.77.7± 8.925.1± 8.97
1.88 ± 21.18(-3.47)± 13.11(-0.44)± 7.49(-2.96)± 24.81(-4.43)± 16.14(-4.67)± 10.93
3.78± 16.8
% predictedmean±±±±± SD
--
86.67 ± 7.7748.53± 13.0154.43± 9.2545.21± 13.62108.93± 18.4796.1± 15.87
133.17± 50.99126.29± 31.7881.78± 15.84
-
78± 19.2896.73 ± 1.92.53 ± 0.651.1 ± 0.4243.1 ± 7.63.3 ± 0.895.58 ± 1.262.77 ± 0.622.81 ± 1.163.95± 1.81.63± 0.430.8 ± 0.27
Absolutemean ±±±±± SD
106 Natpatou Sanguanwongse «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
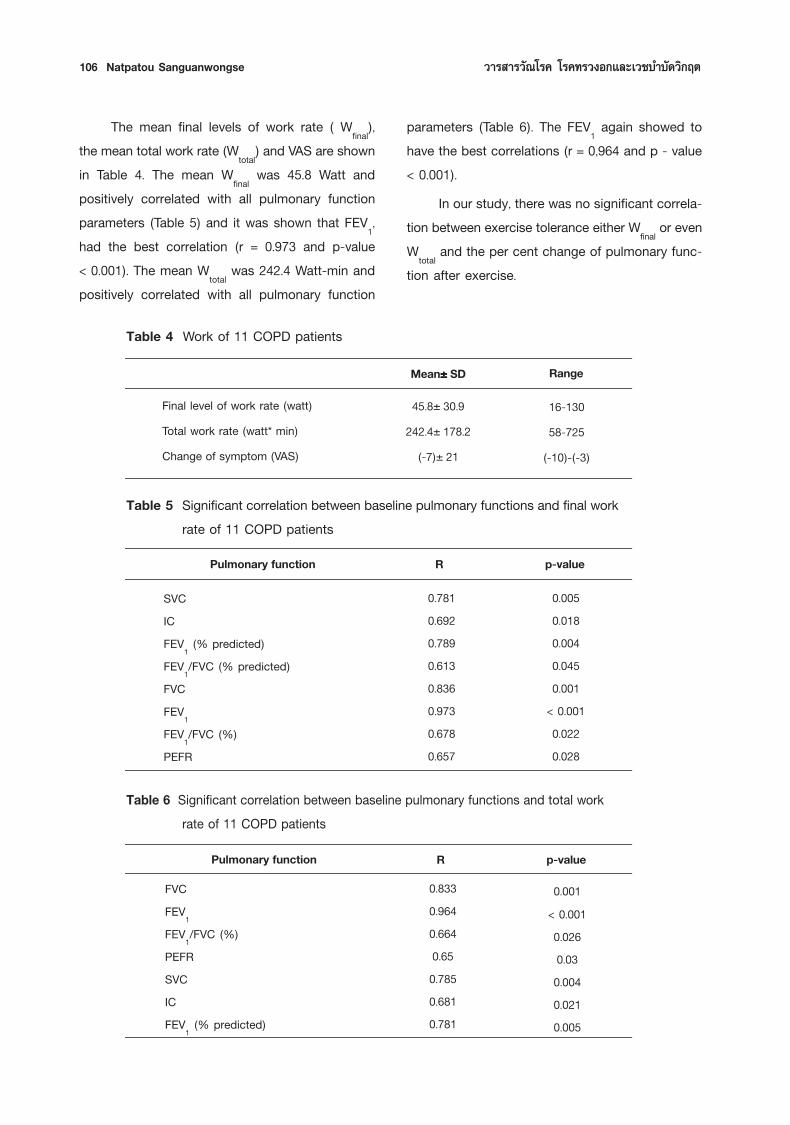
The mean final levels of work rate ( Wfinal),the mean total work rate (Wtotal) and VAS are shownin Table 4. The mean Wfinal was 45.8 Watt andpositively correlated with all pulmonary functionparameters (Table 5) and it was shown that FEV1,had the best correlation (r = 0.973 and p-value< 0.001). The mean Wtotal was 242.4 Watt-min andpositively correlated with all pulmonary function
parameters (Table 6). The FEV1 again showed tohave the best correlations (r = 0,964 and p - value< 0.001).
In our study, there was no significant correla-tion between exercise tolerance either Wfinal or evenWtotal and the per cent change of pulmonary func-tion after exercise.
p-valueRPulmonary function
Mean±±±±± SD Range
p-valueRPulmonary function
SVCICFEV1 (% predicted)FEV1/FVC (% predicted)FVCFEV1FEV1/FVC (%)PEFR
0.7810.6920.7890.6130.8360.9730.6780.657
0.0050.0180.0040.0450.001
< 0.0010.0220.028
FVCFEV1FEV1/FVC (%)PEFRSVCICFEV1 (% predicted)
0.8330.9640.6640.650.7850.6810.781
0.001< 0.0010.0260.030.0040.0210.005
Table 6 Significant correlation between baseline pulmonary functions and total workrate of 11 COPD patients
Table 4 Work of 11 COPD patients
Table 5 Significant correlation between baseline pulmonary functions and final workrate of 11 COPD patients
Final level of work rate (watt)Total work rate (watt* min)Change of symptom (VAS)
45.8± 30.9242.4± 178.2
(-7)± 21
16-13058-725
(-10)-(-3)

ªï∑ ’Ë 26 ©∫ —∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2548 Perception of Exertional Dyspnea, Pulmonary Functionœ 107
DISCUSSIONThe main findings of the presented study were
as follows: 1). Some baseline pulmonary functionparameters had correlation with measures ofexertional dyspnea. Baseline FEV1 had not only thebest significant negative correlation with percep-tional dyspneic symptom (r = -0.698, p = 0.017)but also the best significant positive correlationwith exercise tolerance (r = 0.973, p < 0.001). 2.)After the patients felt exertional dyspnea, it wassignificantly worse in FEV1 (r = 0.824, p = 0.002).
Although we found a significant correlationbetween perceptional dyspnea and baseline FEV1(negative correlation) and also a correlationbetween exercise tolerance and baseline FEV1(positive correlation), more subjects were neededto calculate a predictive equation using multipleregression analysis for practical implications.
The presented data also confirmed the find-ing of Calson et al11, that FEV1 was the best pre-dictor in all baseline pulmonary function param-eters with exercise tolerance in patients with COPD(r = 0.70). However, Murariu et al12 found that therewere 3 baseline pulmonary function parameters thatcorrelated with exercise tolerance: IC (r = 0.81,p = < 0.001), FVC (r = 0.64, p = < 0.001), FEV1(r = 0.54, p < 0.01). In addition, Diaz et al21 alsofound that the baseline IC still showed the bestcorrelation to exercise tolerance (r = 0.75, p < 0.0001).Compared to our study, although IC was signifi-cantly correlated with exercise tolerance (r = 0.692,p = 0.018), it was not one of the most significantdeterminants. However, there were many explana-tions such as, in the Murariu study, the patientswere both COPD and asthmatic and they also hadless severe disease (mean FEV1% predicted =
The VAS, which was rated after exercise,ranged from 3 to 10 (mean = 7) in the ùvery muchworseû end and negatively correlated with only 2parameters (Table 7); i.e: FEV1 ( both absolutevalues and % predicted) and FEV1/FVC ratio (bothabsolute values and % predicted). However, FEV1
revealed the best correlation (r = -0.698 andp-value = 0.017). Regarding the change of pulmo-nary function, there was a positive correlationbetween per cent change or FEV1 and VAS.(r = 0.824 and p- value = 0.002).
Table 7 Significant correlation between baseline pulmonary functions and changeof symptom (VAS) of 11 COPD patients
p-value
0.0360.0170.0260.0270.002
R
-0.633-0.698-0.634-0.6610.824
FEV1FEV1 (% predicted)FEV1/FVC (%)FEV1 /FVC (% change)FEV1 (% change)
Pulmonary

108 Natpatou Sanguanwongse «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
68± 21) than the patients in our study (mean FEV1% predicted = 48.53± 13.01). The study designswere also different. In the Diaz study, the demo-graphic data was similar to our study, thus IC wasshown the same degree of correlation. However,the correlation of exercise tolerance with FEV1 wasnot reported.
Considering the perception of exertional dys-pnea, Martin et al22 demonstrated a correlationbetween the change of the Borg scale and thechange of IC (r=0.49, p=0.00001). In our study, wechose VAS to represent the perception of exertionaldyspnea; and there was also the difference in studydesign.
The limitations of our study was: 1) smallpopulation, (only patients in FC I-II) 2) We usedan electrical braked cycle ergometer that mighthave represented the real daily activities of samepeople and the target for exercise was subjectiveby perception of exertional dyspnea, so the indi-vidual final work rate might not be the real maxi-mal work rate. 3) In real life, beyond FEV1, therewere other factors that might have contributed tothe exertional dyspnea i.e. respiratory musclestrength, deconditioning, individual difference inthe perception of symptoms.
The clinical implications of our study shows,firstly, that the FEV1 was one of the predictors toestimate the exercise tolerance of COPD patientsand, secondly, that the exertional dyspnea wascorrelated to the changed FEV1 which was theobjective evidence of increasing airway obstruc-tion. Therefore the suggestion of an inhaled bron-chodilator as needed based on symptoms mightbe reasonable. However, further study is necessaryto prove the benefit of the inhaled bronchodilatorin symptom relief by improving pulmonary function.
AcknowledgementThe author is grateful to Professor Khun Nanta
Maranetra for her valuable contributions and wouldlike to thank Mr. Chana Naruman for his technicalassistance as well as Mrs. Amolwan Dechapol fortyping the manuscript.
References1. Mahler DA and Harver A. A factor analysis of dysp-
nea ratings, respiratory muscle strength, and lung func-tion in patients with chronic obstructive pulmonarydisease. Am Rev Respir Dis 1992;145:467-470.
2. Wegner R, Jorres RA, Kinsted DK, et al. Factor analysisof exercise capacity, dyspnoea ratings and lungfunction in patients with severe COPD. Eur Respir1994;7:725- 729.
3. Dodd DS, Brancatisano T and Engel LA. Chest wallmechanics during exercise in patients with severechronic airflow obstruction, Am Rew Respir Dis 1984;126:33-38.
4. Hamillton AL, Killian KJ, Summers E, et al. Musclestrength, symptom intensity, and exercise capacity inpatients with cardio-respiratory disorders. Am J RespirCrit Care Med 1995:152;2021-2031.
5. Montes de Oca M and Rassulo J. Cell BR. Respira-tory muscle and cardiopulmonary function duringexercise in very severe COPD. Am J Respir Crit CareMed 1996;154;1284-1289.
6. Marin JM, Montes de Oca M, Rassulo J, et al. Venti-latory drive at rest and perception of exertionaldyspnea in severe COPD. Chest 1999;115:1293-1300.
7. Belman MJ, Botnick WC and Shin JW. Inhaledbronchodilators reduce dynamic hyperinflationduring exercise in patients with chronic obstructivepulmonary disease. Am J Respir Crit Care Med 1996;153:967-975.
8. OûDonnell DE and Webb KA. Exertional breathless-ness in patients with chronic airflow limitation:the role of lung hyperinflation. Am Rev Respir Dis1993:148;1351-1357.
ªï∑ ’Ë 26 ©∫ —∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2548 Perception of Exertional Dyspnea, Pulmonary Functionœ 109
9. Gilbet R, Keighley J and Auchincloss JH. Disability inpatients with chronic obstructive pulmonary disease.Am Rev Respir Dis 1964:90;383-394.
10. Jones NI, Jones G and Edwards RHT. Exercisetolerance in chronic airway obstruction. Am RevRespir Dis 1971:130;477-491.
11. Carison DJ, Ries AL and Kaplan RM. Predictingmaximal exercise tolerance in patients with COPD.Chest 1991:100;307-311.
12. Nurariu C, Ghezo H, Milic-Emili J et al. Exerciselimitation in obstructive lung disease. Chest 1998:114;965-968.
13. Bauerle O, Chrusch CA and Younes M. Mechanismby which COPD affects exercise tolerance. Am JRespir Crit Care Med 1998:157:57-58.
14. Koulouris NG, Dimopoulou l, Valta P, et al. Detectionof expiratory flow limitation during exercise in COPDpatients. J Appl Physio 1997:82;723-731.
15. Pauwels RA, Buist AS, Calverley PM, et al. Globalstrategy for the diagnosis, management, and preven-tion of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic ObstructivePulmonary Disease (GOLD) Workshop Summary.Am J Respir Crit Care Med 2001:163;1256-1276.
16. American Thoracic Society. Standardization ofspirometry. Am J Respir Crit Care Med 1995:152;1107-1136.
17. Dejsomritrutai W, Nana A, Maranetra KN, et al.Reference spirometric values for healthy lifetimenonsmokers in Thailand. J Med Assoc Thai 2000:83;457-465.
18. Simon PM, Schwartzsrein RM, Weiss JW, et al.Distinguishable sensations of breathlessness inducedin normal volunteers. Am Rev Respir Dis 1989:140;1021-1027.
19. Lewis RA, Lewis MN and Tattersfield AE. Asthmainduced by suggestion: is it due to airway cooling?Am Rev Respir Dis 1984;129:691-695.
20. American Thoracic Society. Guidelines for methacho-line and exercise challenges testing-1999. Am RespirCrit Care Med 2000: 161;309-329.
21. Diaz O, Villafrance C, Ghezzo H, et al. Role of inspira-tory capacity on exercise tolerance in COPD patientswith and without tidal expiratory flow limitation atrest. Eur Respir J 2000:16;169-175.
22. Martin JM, Carrizo SJ, Gascon M, et al. Inspiratorycapacity, dynamic hyperinflation, breathlessness, andexercise performance during the 6-minute -walk testin chronic obstructive pulmonary disease. Am J RespirCrit Care Med 2001:163;1395-1399.
ªï∑’Ë 26 ©∫ —∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2548 Controlling multidrug-resistant tuberculosis œ 111
The emergence and spread of multidrug-resistant tuberculosis (MDR-TB) could threatenglobal TB control. The treatment of patients withMDR-TB is prolonged, expensive and oftenunsuccessful. Many experts assert that standardTB control prevents the emergence of MDR-TBin a cost-effective way. Others argue that it isunethical to abandon patients with MDR-TB andmaintain that, if untreated, MDR-TB strains willbecome dominant and undermine TB controlin future generations. These arguments are ofparticular consequence in settings where resourcesare scarce. While additional evidence would helpto define the right point between efficiency andequity, we propose a preliminary rational frame-work for addressing the problem of MDR-TB invarious circumstances.
Genesis and magnitude of multidrug-resistant TB1
Treatment with only one effective drug,because of inappropriate prescription or poor
adherence, suppresses the growth of organismssusceptible to it but permits the multiplication ofisolated strains with spontaneous drug-resistancemutations. This phenomenon is called acquired drugresistance. Subsequent transmission leads to TBdisease in new patients which is drug-resistantat the outset, a phenomenon known as primaryresistance. Independent, cumulative events resultin MDR-TB, defined as resistance to at least iso-niazid and rifampicin. Both the creation and thetransmission of drug resistance contribute to itsincidence.
Resistance to TB drugs emerged soon aftertheir introduction 50 years ago. A survey con-ducted by the International Union Against Tuber-culosis and Lung Disease in 17 countries duringthe late 1950s found primary resistance of 3.7%for streptomycin, 3% for isoniazid, and 1% forboth drugs together. Clinical outcomes were poorerwith dual resistance (analogous to MDR-TBtoday), but the problem was deemed unimportant
«“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫—¥«‘°ƒµThai Journal of TuberculosisChest Diseases and Critical Care
CONTROLLING MULTIDRUG-RESISTANTTUBERCULOSIS AND ACCESS TO EXPENSIVE
DRUGS: A RATIONAL FRAMEWORKAttapon Cheepsattayakorn M.D., FACP, FCCP
10th Zonal Tuberculosis and Chest Disease Center, 10th Office of Disease Prevention and Control,Department of Disease Control, Ministry of Public Health, Thailand
Received for publication November 24, 2004
112 Attapon Cheepsattayakorn «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
because it accounted for only a small proportionof treatment failures. Furthermore, clinical trialsdemonstrated that standard treatment withoutroutine baseline testing for drug susceptibilityproduced outcomes similar to those obtainedwhere such testing was applied and individual-ized treatment was given. The introduction ofrifampicin in the early 1970s brought about am-bulatory short-course chemotherapy, a regimenof three or four drugs including rifampicin for atleast the first two months, given over six to ninemonths. This reinforced hopes for the eliminationof TB.
By the early 1990s the incidence of TB hadincreased in the USA, following reductions in con-trol programmes associated with the HIV epidemic,growing poverty, and homelessness. Poor adher-ence to recommended treatment regimens bydoctors and patients fostered high levels of MDR-TB. MDR-TB came to widespread attention withthe occurrence of nosocomial and prison outbreaks.High case-fatality rates and cases of MDR-TBamong health care workers and others led to anincrease in public concern. WHO declared TB aglobal emergency in 1993, focusing on developingcountries where 95% of cased occurred.
Although MDR-TB was one of many concernsin global TB control, there were no data on themagnitude of the problem. For this reason, WHOand the International Union Against Tuberculosisand Lung Disease began the Global Project onAnti- tuberculosis Drug Resistance Surveillancein 1994. A network of supranational referencelaboratories provided quality control for drug sus-ceptibility-testing. It emerged that the prevalenceof multidrug resistance among new patientswas generally low, the median value being 1%,
especially in Africa. However, several hot spots,i.e. countries or regions where the prevalence ofmultidrug resistance among new TB patientsexceeded 3%, were identified, particularly in theformer Soviet Union. Drug resistance was found inall 72 countries surveyed by 2000.
International response to growingproblem of multidrug-resistant TB1
Because of the low prevalence of multidrug-resistance in most countries, WHO stressed basicTB control as the priority for the prevention ofMDR-TB in low-income countries. The world bodydid not advocate treatment against MDR-TB ona large scale but recommended that individualpatients with MDR-TB be referred to clinicalexperts. The reasons for these recommendationsincluded: i) uncertainties about the risk posedby MDR-TB and the rapidity of its spread; ii) thehigh costs and poor results of treatment inpatients with chronic MDR-TB before the 1990s;and iii) the potential diversion of resources toMDR-TB instead of expanding the DOTS strategy(the TB control strategy recommended by WHOand the International Union Against Tuberculosisand Lung Disease).
The scenario changed in the second half ofthe 1990s. In Now York City, individualized che-motherapy based on drug susceptibility-testingbecame nearly as effective in new patients withMDR-TB as in those with drug-susceptible TB andthe number of MDR-TB cases decreased by morethan 90% during the decade. The relatively largenumber of cased in rich countries made second-line drugs (amikacin, kanamycin, capreomycin,cycloserine, para-aminosalicylic acid (PAS),ethionamide, and the fluoroquinolones) more avail-able and affordable. Yet questions remained about
ªï∑’Ë 26 ©∫ —∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2548 Controlling multidrug-resistant tuberculosis œ 113
which interventions had led to New York Cityûssuccess, and about the need, feasibility and cost-effectiveness of this approach in countries withfewer resources.
A pilot project involving community-basedtreatment of MDR-TB in northern Lima, Peru, chal-lenged the status quo: it was shown that it waspossible to cure MDR-TB on an out-patient basisin a country where TB was endemic. Advocated ofindividualized treatment for the control of MDR-TBargued that empirical short-course chemotherapyregimens could amplify the problem of MDR-TB inpatients already infected with strains resistant toone or more drugs. The human rights of patientsdying with MDR-TB in Russian prisons were high-lighted. The spectre of an explosive, transnationalepidemic of MDR-TB was raised, and the price ofinaction became a subject of intense debate.
In 1999, WHO created a working group onçDOTS-Plus for multidrug-resistant tuberculosisé toaddress the management of MDR-TB underprogramme conditions. This initiative seeks to as-sess the feasibility and cost-effectiveness of treat-ing MDR-TB in low-income and middle-incomecountries. Several pilot projects, using differentmanagement and therapeutic strategies, areunder way. DOTS-Plus has already successfullynegotiated a 90% price reduction for selectedprojects with the pharmaceutical industry.
Significance of multidrug-resistant TB1
MDR-TB is still infrequent in most countries.Its global prevalence in new patients remainsbelow 2%, decades after the introduction oftuberculosis drugs. Increases, although rapid in out-break settings with immunocompromised people,e.g. those affected by AIDS or malnutrition,
have generally been gradual. On the other hand,in hot spots in Eastern Europe and elsewhere thelevels of MDR-TB are alarming.
While some strains of MDR-TB have causedlarge outbreaks, recent analyses based onmolecular epidemiology suggest that they are, onaverage, less infectious than drug-susceptibleorganisms.Genetic mutations that confer a sur-vival advantage in the presence of an environ-mental factor may become a functional burdenin the absence of such selective pressure. Theselection factor for MDR-TB is inadequate drugtreatment, which is prevented by directly observedtherapy. Thus, even in the absence of widespreadtreatment of MDR-TB, the prevalence of thelatter does not necessarily increase.
After TB control was strengthened inNew York City the number of MDR-TB cases fellmuch faster than the total number of TB cased.Similarly, during the 1960s in Kolin, then inCzechoslovakia, the number of chronic casesfell ten times faster than new TB cases. Whilesecond-line drugs were used in those instances,strains that were virtually pan-resistant alsodisappeared and declines in MDR-TB wereachieved with standard short-course chemotherapy.With DOTS in place, curing MDR-TB appearsto accelerate such trends, with a time-limitedincrease in costs.
Globally, an estimated 20% of patients withTB default or fail to respond to therapy but lessthan 2% have MDR-TB. The vast majority ofpatients who are not successfully treated do nothave MDR-TB, even in hot spots, indicatingfailure to ensure that drugs are taken properly.This represents inadequacy in the implementation
114 Attapon Cheepsattayakorn «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
of basic DOTS programmes more than failure inthe drugs themselves.
Furthermore, a poorly functioning programmecan create MDR-TB much faster than it can betreated, even if unlimited resources are available.MDR-TB results from poor TB management, i.e.inadequate drug treatment followed by lapses ininfection control, and its prevalence is up to tentimes higher in previously treated patients than innew patients. The highest priority in stopping MDR-TB must therefore be its prevention. The estab-lishment of DOTS programmes has been shownto reduce the development of MDR-TB in addi-tion to cutting TB mortality by 70%.
The programme benefits of treatment againstMDR-TB are being evaluated. The costs aresubstantial. Such treatment requires the adminis-tration of drugs that are more toxic and lesseffective and are given for at least three timesas long and at 100 times the cost of basic short-course chemotherapy regimens TB control pro-grammes could spend over 30% of their budgetson less 3% of their cases. Cost-effectivenessanalyses are needed before treatment againstMDR-TB is implemented in national programmes.
Susceptibility-testing for second-line anti-TBdrugs has not been standardized and has yet tobe systematically evaluated for individual clinicalmanagement in developing countries. In a com-munity with a true prevalence of MDR-TB of 3%,a laboratory with an average drug susceptibility-testing specificity for rifampicin of 98% and asensitivity of 96% would report a prevalence of4.8%, but one-third of patients reported as havingMDR-TB would not have it. Widespread testingand treatment of MDR-TB might subject somepatients without it to unnecessary expense andtoxicity.
The DOTS strategy, developed and field-tested during the 1970s and 1980s, was notdesigned to cure patients with MDR-TB, espe-cially those with chronic disease. However, DOTScan prevent MDR-TB from becoming a seriousproblem in a population. This has been demon-strated in Benin, Cuba, the Czech Republic, andKenya, where MDR-TB is virtually non-existent.It is also possible that DOTS can reduce MDR-TBonce it has occurred; in Burkina Faso, Hong Kong(China), Chile, Sierra Leone, and Uruguay,MDR-TB is rare and decreasing.
Worldwide, less than one-third of patientswith TB are treated in DOTS programmes. At most,half the estimate number of patients with TB areofficially detected and barely 60% of these com-plete treatment. From a global public health per-spective, therefore, the top priority should be theexpansion of DOTS. In individual countries or partsof countries, however, additional strategies maybe appropriate. In settings where there are largeoutbreaks of MDR-TB an intensive approach,including infection control, is essential.
Rational strategy for controllingmultidrug-resistant TB1
On the basis of data from the WHO/Interna-tional Union Against Tuberculosis and LungDisease surveillance project, groups countriesaccording to the proportion of TB patients com-pleting treatment successfully and the level ofMDR-TB among previously untreated patients.Specific cut-points for what constitutes good clini-cal outcomes and high levels of MDR-TB havenot been empirically validated. The resulting matrixprovides a reasonable framework for decidingwhether to implement treatment against MDR-TB.Since approximately 70% of new cases of MDR-
ªï∑’Ë 26 ©∫ —∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2548 Controlling multidrug-resistant tuberculosis œ 115
TB occur in only 10 countries a global strategycould emerge while individual countries takeappropriate action.
Countries in which the treatment success rate.i.e. the proportion of new patients who completethe scheduled treatment whether bacteriologicalcure is documented or not, is less than 70%should give top priority to the introduction orimprovement of the DOTS programme. Second-linedrugs should not be widely available in suchsettings. Similarly, in countries with multidrugresistance levels below 1.5% the treatment ofMDR-TB is not a priority, although it could beundertaken on individual clinical grounds withappropriate laboratory support. This categorywould include most African countries, where it ismore important to expand DOTS and to considerinterventions to limit the impact of HIV on TB.
Almost no country with treatment successabove 85% has a rate of primary MDR-TB above5%. Countries in quadranth with intermediatelevels of multidrug resistance and achieving morethan 85% treatment success, generally countrieswhere DOTS has been well implemented in recentyears, are prime locations for DOTS-Plus pro-grammes. A good laboratory and directly observedtherapy are essential for the avoidance of patientmisclassification and the selection of resistanceto second-line drugs. In these few countries,resource mobilization and international assistancefor the treatment of MDR-TB is justified.
Resource-rich countries would generallyoffer treatment for patients with MDR-TB. Inresource-poor countries, where national pro-grammes can barely afford DOTS, nongovern-mental organization could provide assistance in
the implementation and evaluation of DOTS-Pluspilot projects.
The hot spots with multidrug resistancelevels above 5% represent international public healthemergencies. The countries concerned cannotadminister individualized treatment against MDR-TB without creating even more drug resistance.If a programme cannot deliver two to four non-toxic drugs for six to nine months after sputumsmear microscopy has been performed, thedelivery of five to eight drugs that are often toxinfor 18-30 months with culture and first-line andsecond-line drug susceptibility-testing is nearlyimpossible. Such settings require a completeoverhaul of control activities and outbreak controloperations, and coordinated, intensive and sustainedinternational assistance.
The importance of infection control practicesshould be emphasized. Outbreaks in crowdedsettings such as hospitals, shelters or prisons,particularly among immuno-compromised indi-viduals (with AIDS or malnutrition), are a commondenominator in MDR-TB hot spots. Ending suchoutbreaks was vital in turning the tide of MDR-TBin New York City and Milan. No single interventioncan control MDR-TB but the various tools avail-able should be applied wisely: firstly, good DOTSand infection control; then second-line drug treat-ment. The interval between the two depends onthe local context and resources.
TB control and access to second-linedrugs: better model needed1
Pablos-Me @ndez et al rightly point out thatmultidrug-resistant tuberculosis (MDR-TB) is nota major pandemic. However, as drug-susceptibleTB is a worldwide problem, the first priority for

116 Attapon Cheepsattayakorn «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
national TB programmes should be the imple-mentation or expansion of the DOTS strategy,MDR-TB is in most cases a sign of poor programmeperformance, although there may be highlyvirulent strains spreading rapidly. A weak nationalprogramme can do more harm than good ifits main focus is the widespread introduction ofsecond-line drugs to manage this problem.
To tackle MDR-TB Pablos-Me @ndez et al.propose a matrix based on two variables: treat-ment success for new TB cases, and prevalenceof primary MDR-TB. They propose that the use ofsecond-line drugs should be limited to countrieswhich belong in specified quadrants according tothese two variables. We find it questionable thatthe management of an MDR-TB, or any otherdisease, should be based on only two variables.We live in a world in which the control of illnesscalls for modern multidisciplinary approaches.We will come back to this point.
The proposal of Pablos-Me @ndez et al isdifficult to accept for at least two reasons. Firstly,more than two variables are needed to decide ifa country should treat MDR-TB. For instance, acountry may score well on treatment success, havea low number of primary MDR-TB cases but stillhave a high number of treatment failure cases(a variable not taken into account in the proposedmodel), which are likely to have MDR. Such acountry may need to implement management ofMDR-TB as well as DOTS, regardless of its levelof primary MDR and treatment success. Further-more, treatment success could be a very mislead-ing variable since it is the result of cure plus treat-ment completion. There are some examples ofpoor national TB programmes having high rates
of success upon completion of treatment but lowcure rates.
Secondly, do we really need cut-off pointsto manage a disease? On what basis can wechoose 5% and not, say, 3% for MDR prevalence,or 70% and not, say, 60% for treatment success?No biological, statistical or epidemiological reasonis given for choosing such cut-off points. A straight-forward indication of the point at which to startmanagement of MDR-TB could be helpful, butthe issue is not that simple, and other mattersneed to be carefully looked at when taking sucha decision. The assertion that DOTS can reduceMDR-TB has not been fully proved, although it isclear that short-course chemotherapy can preventMDR-TB. Countries that have reduced MDR-TBhave also used second-line drugs and it is notclear to what extent the use of both first-line andsecond-line drugs have contributed to reducingMDR-TB. It is also well known that short-coursechemotherapy, one of the pillars of DOTS, onlycures an unacceptable low fraction of MDR-TB.
The approach suggested by Pablos-Me@ndezet al needs rethinking. First of all, any model formanaging MDR-TB must recognize that such adecision has to be made by the countries con-cerned. It will depend on several national factors,including the resources available, the epidemio-logical profile, the status of TB control, and ethicaland humanitarian issues. Certainly an economicthreshold is likely to exist. A country choosingwhether to manage MDR-TB may benefit from acomprehensive multidisciplinary assessment of itssituation, in order to decide if such drugs areneeded or not. If the decision to go ahead is made,the path to follow should be a strategy that in-

ªï∑’Ë 26 ©∫ —∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2548 Controlling multidrug-resistant tuberculosis œ 117
cludes−but is not limited to−DOTS to reducetransmission of MDR M. tuberculosis strains.
The international community needs to pur-sue a feasible and cost-effective strategy to man-age MDR-TB, which enables countries to offer acure to patients. Although current evidence is lim-ited, there are indications that treatment of MDRin resource-limited setting with strong TB controlprogrammes may be feasible and cost-effective.This information can benefit patients even insetting where MDR-TB rates are below or abovethe threshold proposed by Pablos-Me @ndez et al.
First requirement for control of multi-drug-resistant TB: realism1
The primary cause of an uncontrolled andincreasing TB epidemic worldwide is the neglect ofTB control programmes. This neglect is evidencedby lack of political support, scarce financialresources, and little or no leadership. Successfulprogrammes in both industrialized and developingcountries indicate that a DOTS strategy preventsmultidrug-resistant tuberculosis (MDR-TB). Thetimely and appropriate diagnosis and treatment ofnew and previously-treated TB patients is thefocus in DOTS. As Pablos-Me@ndez et al. suggest,a DOTS-Plus strategy is needed to control MDR-TB only after the DOTS programme has beenestablished and is being adequately implemented.
However, besides the epidemiological andoperative factors involved in implementing aDOTS-Plus strategy, there is an internationaldebate about the ethics and humanism involved.To deny treatment to patients with MDR-TB is toviolate their human rights. Experience in Peruindicates the need for sustained and long-termefforts in preventing the emergence of MDR-TB
with a DOTS strategy. Only then does it becomepossible to treat MDR-TB by applying a DOTS-Plus strategy in the context of an efficient,sustainable and comprehensive TB controlprogramme.
The major area of controversy in applying aDOTS-Plus strategy is about the use of standard-ized or individualized regimens to treat MDR-TBin countries with limited resources. In high incomecountries with a low incidence of TB and suffi-cient financial, technical and human resources,MDR-TB treatment with individualized regimens isbased on drug susceptibility tests. The feasibilityof using this approach in low-or medium-incomecountries has not been assessed. The options forusing standardized or individualized regimens forMDR-TB in these countries should be examinedin pilot projects. These should obtain comparabledata and have the following aims: to develop anevidence-based approach; to design and imple-ment the most appropriate strategy according tothe epidemiology and operational conditions ineach country; and to be subject to rigorous evalu-ation by international standards. A DOTS-Plus strat-egy should also be based on national and inter-national technical assistance to tackle MDR-TB.
The major components for the implementa-tion of a DOTS-Plus strategy would then be: (i)an efficient, effective and integrated TB controlprogramme; (ii) first-line and second-line anti-TBdrugs provided free of charge to each patient withMDR-TB; (iii) drug susceptibility tests for first-lineand second-line anti-TB drugs, not charged tothe patients; (iv) appropriately designed regimensfor MDR-TB, standardized or individualized; (v) areporting system for data management, monitor-ing and evaluation of individual and aggregated
118 Attapon Cheepsattayakorn «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
data on MDR-TB cases; (vi) community-basedstrategies, with the participation of local govern-ments in order to enhance adherence to theregimens; and (vii) the adequate training andorganization of health professionals responsiblefor the care of MDR-TB patients.
Countrywide public health and political com-mitment to sustaining the DOTS strategy remainsthe most important element for implementingDOTS-Plus strategies. In reality it may be the onlymeans of achieving MDR-TB control.
Multidrug-resistant TB-unexaminedcosts and complexities1
Pablos-Me @ndez et al touch on many prob-lems that have to be considered carefully beforeeven the first steps towards comprehensive con-trol of multidrug-resistant tuberculosis (MDR-TB)can be contemplated. I will mention only three ofthese, and only very briefly.
The first is the administration of second-linedrugs, once they have been obtained. Such slightexperience as currently exists in cohort treatmentof MDR-TB comes mainly from relatively controlledsituations. In these places it has been possible tomarshal the resources needed to ensure compli-ance over the long period of treatment and themanagement of its manifold side-effects. Even inan urban situation such as Lima, Peru, the cost ofestablishing the basis for ambulatory care wasenormous, and those arrangements cannot yet becontemplated for the rural areas.
As the authors point out, case-holding andcompliance are the major difficulties in first-lineDOTS programmes and a potent cause ofMDR-TB. Yet few of the situations which might
qualify as MDR sites on the authorsû matrix haveanything like the support mechanisms in placeto ensure an effective control programme. Also,control must, presumable, imply legislative regu-lation of the drug supply.
A second issue is how countries, until nowsupposedly not exposed to heavy burdens ofMDR-TB, discover they have problems. Manycountries, especially in sub-Saharan Africa, havemanaged to institute effective DOTS programmeson the basis of microscopy alone. Few haveculture facilities for the majority of patients, letalone the quality control mechanisms to maintaintheir performance. In these countries, the outcomeçtreatment failureé tends to play a much smallerrole than elsewhere, and it is rarely subjected tofurther investigation. To set up culture facilitiesin order to investigate and treat MDR-TB wouldentail costs that few of these countries couldcontemplate.
A third difficulty, common to all too manyWHO papers, is to base statements about a wholecountry on findings from a small, often atypical,model area. Yet the difference between a special,usually heavily funded, trial area and the rest of acountry is often greater than differences betweencountries. With suitable caveats, such mattersare not of great importance in a summary paperexcept that they may inhibit discussion of thepotential for disease control in isolated circum-stances such as prisons, displaced personsû campsetc. Such sites may meet criteria for MDR-TBcontrol which exist nowhere else in the countryand they should be considered eligible, even inisolation.

ªï∑’Ë 26 ©∫ —∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2548 Controlling multidrug-resistant tuberculosis œ 119
These thoughts are proffered only as anaddendum to what seems to me a very useful andwell-written paper.
DOTS-Plus in the Philippines, a high-burden country: funds needed1
Multidrug-resistant tuberculosis (MDR-TB) isa global problem requiring a global solution. Thearticle of Pablos-Me @ndez et al provides a rationalframework for finding such a solution.
The Philippines is ranked No.7 on the listof 22 high-burden countries for TB DOTS wasintroduced at the public health centres only in 1992,and treatment success was 87% (J. Lagahid onthe DOTS strategy at the Department of Health,Personal communication). MDR-TB is estimatedto be present in 1.5% of new cases, although aprecise assessment still has to be made. Theserates would put the Philippines in the çfé categoryon the matrix of Pablos-Me@ndez et al for ratio-nalizing the control of MDR-TB. Here MDR-TBtreatment is not seen as a priority of the nationalTB control service, but to be allowed in specializedcentres with appropriate laboratory support andhelp from nongovernmental organizations.
Only a third of the patients who seek medicalcare for TB in the Philippines are treated at apublic health centre. The majority are treated byprivate practitioners. The Makati Medical Center,a tertiary referral private hospital, established aDOTS Clinic in 1999 in the spirit of private-publiccollaboration in TB control. Re-treatment casesin this clinic steadily increased, and now accountfor 44% of the patients enrolled. Treatmentsuccess in two cohorts analyses showed a declinefrom 85.3% in the first year to 68.2% in the
second, with a corresponding increase in failurerates from 5.6% to 10.3%. All the failures wereMDR-TB among the re-treatment cases. Treatmentfor these MDR-TB cases, in spite of logisticalconstraints, was called for clinical, public health,and socioeconomic reasons.
The transmissibility of MDR-TB, contraryto previously held beliefs, is equal to that of pan-susceptible strains. Most of our patients livein poverty, under the most adverse conditions,characterized by heavy population density andmalnutrition. To leave them untreated would pro-long the period of their contagiousness andincrease the number of MDR-TB cases amongthe highly susceptible malnourished membersof their community.
Despite severely limited resources, outpatienttreatment was made possible for 117 patientswith MDR-TB through the DOTS-Plus pilotproject. Support was provided by the national TBprogramme of the Department of Health, thePhilippines Charity Sweepstakes, and the localgovernment unit. Results so far have beenencouraging, with a 75% preliminary estimate ofcure and likely cute, and 9.1% failure or likelyfailure, and a default rate of 7.7%. Patients whoare household heads and have responded to therapyhave gone back to work and are now gainfullyemployed.
DOTS expansion in the country, whichincludes harnessing the private sector to theprogramme, remains the priority, as this shouldput a stop to the generation of more MDR-TB.However, with a large segment of the populationvery susceptible owing to malnutrition and crowd-ing, treatment for MDR-TB should also be

120 Attapon Cheepsattayakorn «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
pursued, in a well-supervised fashion as practisedat the Makati Medical Centerûs DOTS-Plus pilotproject. An epidemiological study of the extentof MDR-TB in the country is urgently needed,to determine whether the Philippines should beregarded as a hot spot fuelling a global pandemic.If it is, funds for DOTS-Plus are urgently needed.
Examining assumptions aboutmultidrug-resistant TB control1
The first assumption−that strains of MDR-TBçare, on average, less infectiousé−is not supportedby the literature. The cluster studies referencedfound that drug-susceptible TB was more likely tooccur in clusters than drug-resistant TB. None-theless, other such studies have identified MDR-TB as a risk factor for clustering. Similarly, mul-tiple observational reports describe the widespreaddissemination of MDR clones from the W-strainfamily. Other groups have also raised questionsabout the interpretability of cluster studies forinference. Finally, longitudinal epidemiologicalstudies of TB transmission among householdcontacts have failed to support this finding.
A second assumption that DOTS çcanreduce MDR-TB once it has occurredé is sup-ported only by examples of falling MDR-TB rates:no evidence has causally linked the use of DOTSalone to observed declines. In fact, the claim thatDOTS can reduce rates of MDR-TB is not sup-ported by the growing body of evidence thatpatients with MDR-TB have poor outcomes withshort-course chemotherapy. New York City is citedas an example of successful control, yet thissuccess was achieved through comprehensiveinterventions that included massive investmentsin infrastructure, infection control, improved case
detection, and treatment of active cases ofMDR-TB.
The third assumption−that çthe need tointroduce second-line therapy should be deter-mined by countrywide statistics on treatment suc-cess rates and the proportion of all cases causedby MDR strainsé−may result in dangerous policydecisions. The authors suggest an arbitrary thresh-old for their çrationalé framework; however, theynote that çspecific cut-points for ... good clinicaloutcomes and high levels of MDR-TB have notbeen empirically validated.é Because MDR-TBoutbreaks are focal, countrywide averages mayunderestimate the seriousness of the problem.Additionally, focal outbreaks present an opportu-nity to develop a control strategy before theMDR-TB rates compromise the efficacy of DOTSprogrammes.
Lastly, it is assumed that to prioritize DOTSexpansion çmost national TB programmes do notneed to introduce second-line anti-TB therapyé.Poor outcomes of DOTS re-treatment regimensdocumented in patients who fail their initial roundof short-course chemotherapy, however, raise animportant ethical challenge to this assertion. As aresult, WHO must now make a decision aboutwhether or not to recommend second-line drugsas part of standard re-treatment regimens for allDOTS programmes.
DOTS expansion is the first priority in globalTB control, but it is short-sighted to concludethat the latter can be achieved without effectivestrategies to treat and control MDR-TB. Ratherthan pit DOTS expansion against MDR-TB therapy,the task at hand is to obtain dramatically increasedfunds for comprehensive global TB control.With the new Global Fund to Fight AIDS, TB and

ªï∑’Ë 26 ©∫ —∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2548 Controlling multidrug-resistant tuberculosis œ 121
Malaria, these resources may soon be forthcom-ing. We would argue that now, to deny accessto effective treatment for those already sick onthe grounds that resources are scarce would beirrational or worse.
Management of Tuberculosis Caused byDrug-resistant Organisms2
Tubercle bacilli are continually undergoingspontaneous mutation that create resistance toindividual antituberculosis drugs. However, thefrequency of these single mutations is sufficientlylow that with appropriate combination chemotherapythat is reliably ingested, clinically significant resis-tance will not develop. Most commonly the devel-opment of acquired drug resistance occurs whenthere is a large bacillary population, such asin pulmonary cavities, when an inadequatedrug regimen is prescribed (inappropriate drugs,insufficient dosage) or when there is a combinedfailure of both the patient and the provider toensure that an adequate regimen is taken.Rarely, malabsorption of one or more antitubercu-losis drugs may account for acquired resistance.Drug resistance is much more likely to occur incavitary pulmonary tuberculosis because of theimmense number of rapidly multiplying bacilli inthe cavity(ies). During extended or repeatedtreatment, resistance to multiple agents may evolve.Patients with acquired drug resistance maytransmit their strains to others who, if theydevelop tuberculosis, will have primary drug resis-tance.
Drug resistance in a patient with newlydiagnosed tuberculosis may be suspected onthe basis of historical (previous treatment) orepidemiologic information (contact with a known
drug-resistant case or coming from a regionin which drug resistance is common). In suchsituations it is prudent to employ an empiricallyexpanded regiment, as described previously,especially if the patient is seriously ill (Table 1).
Drug resistance can be proven only by drug-susceptibility testing performed in a competentlaboratory (Table 2). The steps taken when resis-tance is shown to be present are of critical impor-tance. Patients harboring strains of M. tuberculo-sis resistant to both INH and RIF (MDR) are athigh risk for treatment failure and further acquiredresistance; they must be referred immediatelyto a specialist or consultation obtained fromspecialized treatment centers. Patients with strainsresistant to RIF alone have a better prognosisthan MDR cases, but also are at increased riskfor failure and additional resistance. Thus, theirmanagement should also be subject to specialscrutiny.
Definitive randomized or controlled studieshave not been performed among patients withthe various patterns of drug resistance. In theabsence of ideal evidence, practices in thetreatment of patients are based on a mixtureof general principles, extrapolations and expertopinion. The WHO and IUATLD have formulatedstandard algorithmic regimens for the managementof treatment failure or chronic cases, largely basedon the principles listed below, as well as onexpert opinion. This approach is best suited toregions without in vitro susceptibility testingcapacity and access to the full array of retreatmentmedications, but it is not appropriate for industrial-ized nations with more ample resources.
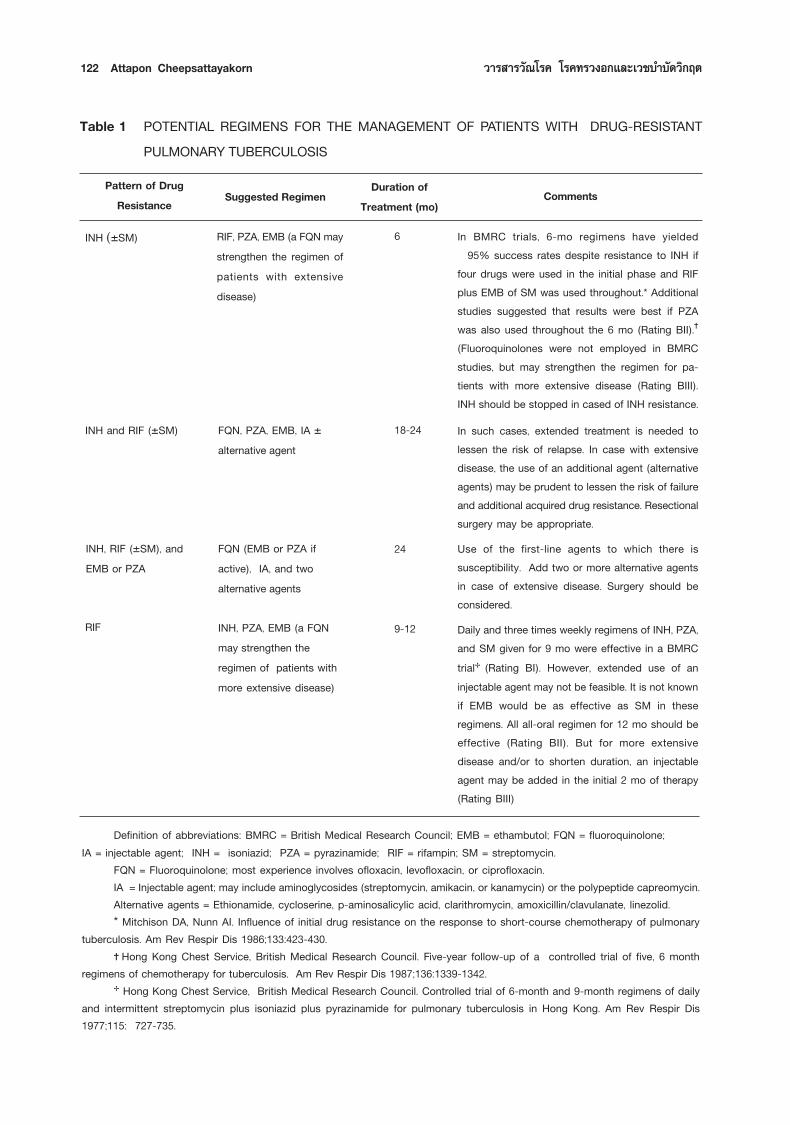
122 Attapon Cheepsattayakorn «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
In BMRC trials, 6-mo regimens have yielded 95% success rates despite resistance to INH if
four drugs were used in the initial phase and RIFplus EMB of SM was used throughout.* Additionalstudies suggested that results were best if PZAwas also used throughout the 6 mo (Rating BII).(Fluoroquinolones were not employed in BMRCstudies, but may strengthen the regimen for pa-tients with more extensive disease (Rating BIII).INH should be stopped in cased of INH resistance.
In such cases, extended treatment is needed tolessen the risk of relapse. In case with extensivedisease, the use of an additional agent (alternativeagents) may be prudent to lessen the risk of failureand additional acquired drug resistance. Resectionalsurgery may be appropriate.Use of the first-line agents to which there issusceptibility. Add two or more alternative agentsin case of extensive disease. Surgery should beconsidered.Daily and three times weekly regimens of INH, PZA,and SM given for 9 mo were effective in a BMRCtrial (Rating BI). However, extended use of aninjectable agent may not be feasible. It is not knownif EMB would be as effective as SM in theseregimens. All all-oral regimen for 12 mo should beeffective (Rating BII). But for more extensivedisease and/or to shorten duration, an injectableagent may be added in the initial 2 mo of therapy(Rating BIII)
Table 1 POTENTIAL REGIMENS FOR THE MANAGEMENT OF PATIENTS WITH DRUG-RESISTANTPULMONARY TUBERCULOSIS
Definition of abbreviations: BMRC = British Medical Research Council; EMB = ethambutol; FQN = fluoroquinolone;IA = injectable agent; INH = isoniazid; PZA = pyrazinamide; RIF = rifampin; SM = streptomycin.
FQN = Fluoroquinolone; most experience involves ofloxacin, levofloxacin, or ciprofloxacin.IA = Injectable agent; may include aminoglycosides (streptomycin, amikacin, or kanamycin) or the polypeptide capreomycin.Alternative agents = Ethionamide, cycloserine, p-aminosalicylic acid, clarithromycin, amoxicillin/clavulanate, linezolid.* Mitchison DA, Nunn AI. Influence of initial drug resistance on the response to short-course chemotherapy of pulmonary
tuberculosis. Am Rev Respir Dis 1986;133:423-430. Hong Kong Chest Service, British Medical Research Council. Five-year follow-up of a controlled trial of five, 6 month
regimens of chemotherapy for tuberculosis. Am Rev Respir Dis 1987;136:1339-1342. Hong Kong Chest Service, British Medical Research Council. Controlled trial of 6-month and 9-month regimens of daily
and intermittent streptomycin plus isoniazid plus pyrazinamide for pulmonary tuberculosis in Hong Kong. Am Rev Respir Dis1977;115: 727-735.
CommentsPattern of DrugResistance Suggested Regimen Duration of
Treatment (mo)
FQN (EMB or PZA ifactive), IA, and twoalternative agents
INH, RIF (±SM), andEMB or PZA
6
18-24
24
9-12
RIF, PZA, EMB (a FQN maystrengthen the regimen ofpatients with extensivedisease)
INH (±SM)
FQN, PZA, EMB, IA ±alternative agent
INH and RIF (±SM)
INH, PZA, EMB (a FQNmay strengthen theregimen of patients withmore extensive disease)
RIF
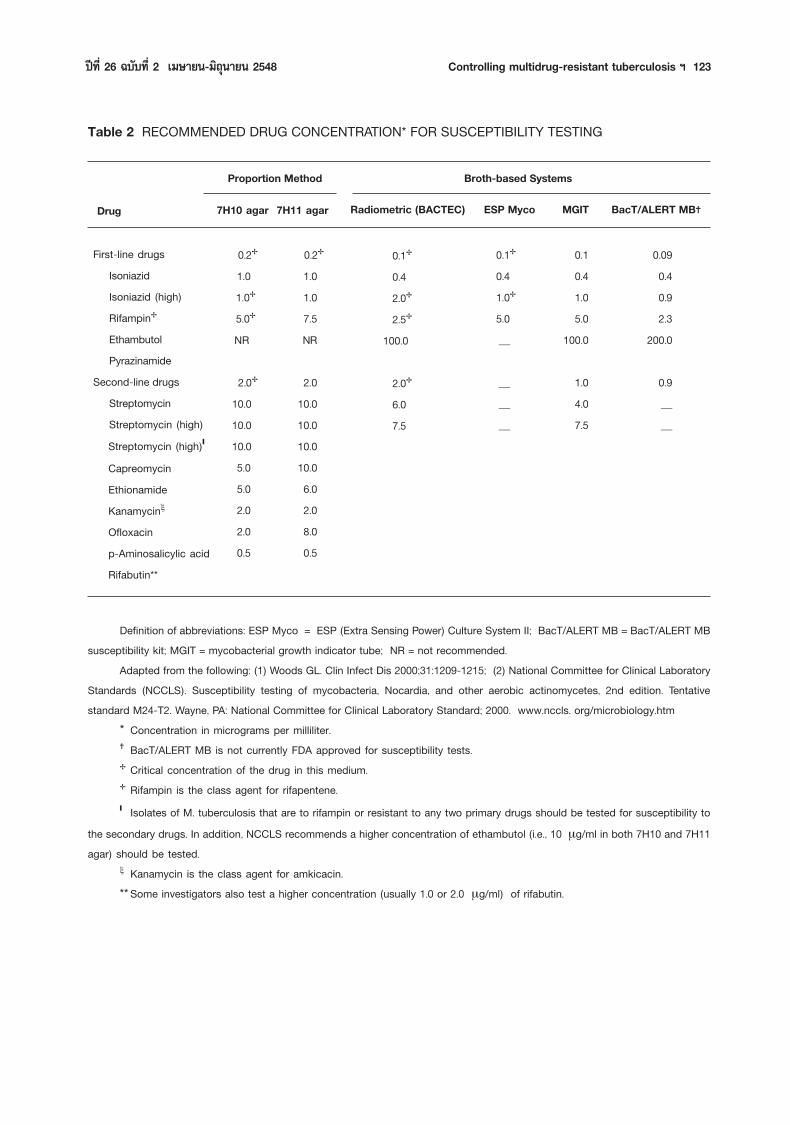
ªï∑’Ë 26 ©∫ —∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2548 Controlling multidrug-resistant tuberculosis œ 123
Definition of abbreviations: ESP Myco = ESP (Extra Sensing Power) Culture System II; BacT/ALERT MB = BacT/ALERT MBsusceptibility kit; MGIT = mycobacterial growth indicator tube; NR = not recommended.
Adapted from the following: (1) Woods GL. Clin Infect Dis 2000;31:1209-1215; (2) National Committee for Clinical LaboratoryStandards (NCCLS). Susceptibility testing of mycobacteria, Nocardia, and other aerobic actinomycetes, 2nd edition. Tentativestandard M24-T2. Wayne, PA: National Committee for Clinical Laboratory Standard; 2000. www.nccls. org/microbiology.htm
* Concentration in micrograms per milliliter. BacT/ALERT MB is not currently FDA approved for susceptibility tests. Critical concentration of the drug in this medium. Rifampin is the class agent for rifapentene. Isolates of M. tuberculosis that are to rifampin or resistant to any two primary drugs should be tested for susceptibility to
the secondary drugs. In addition, NCCLS recommends a higher concentration of ethambutol (i.e., 10 µg/ml in both 7H10 and 7H11agar) should be tested.
ξ Kanamycin is the class agent for amkicacin.** Some investigators also test a higher concentration (usually 1.0 or 2.0 µg/ml) of rifabutin.
Table 2 RECOMMENDED DRUG CONCENTRATION* FOR SUSCEPTIBILITY TESTING
Proportion Method Broth-based Systems
Drug 7H10 agar 7H11 agar Radiometric (BACTEC) ESP Myco MGIT BacT/ALERT MB
0.2 1.0
1.0 5.0NR
2.010.010.010.0 5.0 5.0 2.0 2.0 0.5
0.10.41.05.0
100.0
1.04.07.5
0.090.40.92.3
200.0
0.9__
First-line drugsIsoniazidIsoniazid (high)RifampinEthambutolPyrazinamide
Second-line drugsStreptomycinStreptomycin (high)Streptomycin (high)
CapreomycinEthionamideKanamycinξ
Ofloxacinp-Aminosalicylic acidRifabutin**
1.01.07.5NR
2.010.010.010.010.06.02.08.00.5
0.2 0.10.42.02.5
2.06.07.5
100.0
0.10.41.05.0_
___
124 Attapon Cheepsattayakorn «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
Guidelines for management of patients withtuberculosis caused by drug-resistant organismsare based on the following guidelines, all of whichare rated A III :
A Single new drug should never be addedto a failing regimen.
When initiating or revising therapy, alwaysattempt to employ at least three previ-ously unused drugs to which there is invitro susceptibility. One of these shouldbe an injectable agent.
Do not limit the regimen to three agents ifother previously unused drugs that are likelyto be active are available. In patients withMDR organisms in whom there is resis-tance to first-line agents in addition to INHand RIF, regimens employing four to sixmedications appear to be associated withbetter results.
Patients should receive either hospital-based or domiciliary DOT. The implica-tions of treatment failure and furtheracquired resistance are such that thesecases should receive highest priority forDOT.
Intermittent therapy should not be used intreating tuberculosis caused by drug-resistant organisms, except perhaps forinjectable agents after an initial period (usu-ally 2-3 months) of daily therapy.
The use of drugs to which there is dem-onstrated in vitro resistance is not encour-aged because there is little or no efficacyof these drugs (assuming the test resultsare accurate), and usually, alternative medi-cations are available. However, the clini-cal significance and effectiveness of the
use of INH in the setting of low-level INHresistance is unclear. It should be notedthat the use of INH was associated withbetter survival rates in patients with thestrain-W variety of MDR M. tuberculosisthat was susceptible to higher concentra-tions of INH.
Resistance to RIF is associated in nearlyall instances with cross-resistance torifabutin and rifapentine. Rare strains withRIF resistance retain susceptibility torifabutin; this is associated with uncom-mon mutations of the RNA-polymeraselocus in the bacillus. However, unlessin vitro susceptibility to rifabutin is demon-strated, this agent should not be employedin cases with RIF resistance. Cross-resis-tance between RIF and rifapentineappears almost universal.
There is no cross-resistance between SMand the other injectable agents: amikacin,kanamycin, and capreomycin (althoughresistance to all may occur as indepen-dent events); however, cross-resistancebetween amikacin and kanamycin is uni-versal. Simultaneous use of two injectableagents is not recommended due to theabsence of proof of efficacy and potentialamplification of drug toxicity.
Determination of resistance to PZA is tech-nically problematic and, thus, is not madein many laboratories. However, resistanceto PZA is uncommon in the absence ofresistance to other first-line drugs. Ifmonoresistance to PZA is observed, con-sideration must be given to the possibilitythat the etiologic agent is M. bovis, not

ªï∑’Ë 26 ©∫ —∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2548 Controlling multidrug-resistant tuberculosis œ 125
M. tuberculosis (M. bovis is genotypicallyresistant to PZA and is not distinguishedfrom M tuberculosis by nucleic acidhybridization-probe assays that are com-monly used for identification).
Table 1 Contains regimens suggested for usein patients with various patterns of drug-resistanttuberculosis.
A 6-month regimen of isoniazid, rifampin,pyrazinamide, and either ethambutol or strepto-mycin has been demonstrated to be effective forthe treatment of TB resistant only to isoniazid.When resistance to isoniazid is documentedduring the recommended initial four-drug therapy,the regimen should be adjusted by discontinuingisoniazid and continuing the other three drugs forthe entire 6 months of therapy. TB resistant onlyto isoniazid may also be treated with rifampin andethambutol for 12 months.3
When isoniazid resistance is documented inthe 9-month regimen without pyrazinamide, iso-niazid should be discontinued. If ethambutol wasincluded in the initial regimen, treatment withrifampin and ethambutol should be continued fora minimum of 12 months. If ethambutol was notincluded initially, susceptibility tests should berepeated, isoniazid should be discontinued, andtwo other drugs, to which the isolate is suscep-tible (e.g., ethambutol and streptomycin), shouldbe added. The regimen can be adjusted when theresults of the susceptibility tests become avail-able.3
Multidrug-resistant TB (i.e., TB resistant toat least isoniazid and rifampin) presents difficulttreatment problems. Treatment must be individu-alized and based on the patientûs medicationhistory and susceptibility studies.3
Unfortunately, adequate data are not avail-able on the effectiveness of various regimens andthe necessary duration of treatment for patientswith organisms resistant to both isoniazidand rifampin. Moreover, many of these patientsalso have resistance to other first-line drugs(e.g., ethambutol and streptomycin) when drugresistance is discovered. Because of the pooroutcome in such cases, it is preferable to give atleast three new drugs to which the organism issusceptible. This regimen should be continueduntil culture conversion is documented, followedby at least 12 months of two-drug therapy. Often,a total of 24 months of therapy is given empiri-cally. Some experts recommend that at least18-24 months of three-drug therapy be givenafter culture conversion. MDR TB should be treatedusing a daily regimen under direct observation(DOT). Intermittent administration of medicationsis not possible in treatment of MDR TB.3
Clinicians who are unfamiliar with the treat-ment of drug-resistant TB should seek expertconsultation. Because second-line drugs can causeserious adverse reactions, patients taking thesedrugs should be monitored closely throughoutthe course of treatment. The role of agents suchas the quinolone derivatives and amikacin in thetreatment of multidrug-resistant disease is not wellcharacterized, although these drugs are commonlybeing used in such cases. Surgery may offerconsiderable benefit and a significantly improvedcure rate for patients who have multidrug-resistant TB if the bulk of disease can be resected.However, drug therapy is usually required tosterilize the remaining disease.3

126 Attapon Cheepsattayakorn «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
ConclusionAt present, most national TB programmes
do not need to introduce second-line anti-TBtherapy in order to control the disease. Access,in this case, is a secondary question. First-lineDOTS remains one of the most cost-effective ofall public health strategies. Relatively simple,standardized short-course chemotherapy regimenscan cure more than 90% of new TB patientsand prevent transmission of the disease.
The emergence and spread of MDR-TBis a symptom of poor programme performance.In the absence of an effective TB control
TB treatment for HIV-Positive Patientswith Drug-Resistant TB3
TB disease resistant to isoniazid only. Thetreatment regimen should generally consist of arifamycin (rifampin or rifabutin), pyrazinamide,and ethambutol for the duration of treatment.Because the development of acquired rifamycinresistance would result in MDR TB, cliniciansshould carefully supervise and manage TBtreatment for these patients.
TB disease resistant to rifampin only.The 9-month treatment regimen should generallyconsist of an initial 2-month phase of isoniazid,streptomycin, pyrazinamide, and ethambutol. Thesecond phase of treatment should consist ofisoniazid, streptomycin, and pyrazinamide admin-istered for 7 months. Because the developmentof acquired isoniazid resistance would result inMDR TB, clinicians should carefully supervise andmanage TB treatment for these patients.
Multidrug-resistant TB (resistant to bothisoniazid and rifampin). These patients should bemanaged by or in consultation with physiciansexperienced in the management of MDR TB. Mostdrug regimens currently used to treat MDR TBinclude an aminoglycoside (e.g., streptomycin,kanamycin, amikacin) or capreomycin, and a fluoroquinolone, along with other agents to which theorganism is sensitive. The recommended durationof treatment for MDR TB in HIV-positive patientsis 24 months after culture conversion, and post-treatment follow-up visits to monitor for TBrelapse should be conducted every 4 months for24 months. Because of the serious personal andpublic health concerns associated with MDR TB,health departments should always use DOT for
these patients and take whatever steps are neededto ensure their adherence to the treatment regi-men.
Role of Surgery in MDR Tuberculosis2
The role of resectional surgery in the man-agement of patients with extensive pulmonary MDRtuberculosis has not been established in random-ized studies. In one series, patients with severedrug resistance (on average, having resistance tomore than 5 drugs) appeared to benefit from theresection of cavitary or badly damaged lungtissue when compared with historical controls.In contrast, other clinicians have reported patientswith drug resistance having similar cure rateswithout surgery. The disparity in these reports maybe due to long-standing disease with extensivefibrosis in the former group. If surgery is to bedone, it should be performed by and experiencedsurgeon after the patient has received severalmonths of intensive chemotherapy. Even withsuccessful resection, 12-24 additional months ofchemotherapy, using drugs to which there isdemonstrated susceptibility, should be given.
ªï∑’Ë 26 ©∫ —∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2548 Controlling multidrug-resistant tuberculosis œ 127
programme, a narrow focus on MDR-TB therapycould, paradoxically, make a bad situation worse.In countries where TB is endemic, resources spentcuring a single case of MDR-TB could be used totreat 100 new TB patients. Many lives could thusbe saved and the development of new MDR-TBcases could be reduced. This would be funda-mentally in keeping with human rights and publichealth principles. Drug resistance is ubiquitous,but primary MDR-TB is still infrequent afterdecades of drug treatment. However, the severalhot spots that have emerged require urgentattention.
The framework that we propose for dealingwith MDR-TB highlights important differences invarious programmes. Countries differ not only intheir resources but also in matters of epidemiol-ogy and health care. The differences may deter-mine which strategy is most appropriate for pre-venting and controlling TB and MDR-TB. Formalmodelling and cost-effectiveness analyses areneeded in order to refine the framework, as isresearch on the transmissibility and overall impactof MDR-TB under programme conditions. As arecent paper put it, çthe future may not be sodarké.
The DOTS-Plus initiative has led to dramaticreductions in the prices of second-line drugs. Pilotprojects around the world have qualified forimplementation and can be expected to provide
important guidance on the evidence-basedexpansion of treatment against MDR-TB. Asfunds are allocated for the treatment of MDR-TBin hot spots it is essential to increase humanand financial resources for the expansion ofDOTS worldwide. The top priority should continueto be the improvement of basic treatment pro-grammes in order to prevent the emergence ofMDR-TB. For treatment to be undertaken on alarge scale it is important to reduce further thecost of second-line drugs, implement outbreakcontrol, maintain surveillance, improve diagnostictesting, and develop new anti-TB drugs. Onlya comprehensive approach, tailored to localconditions, can be expected to prevent a globalepidemic of MDR-TB.
Reference1. World Health Organization. Control of Multidrug-
Resistant Tuberculosis. Bulletin of the World HealthOrganization, 2002;80:490-498.
2 American Thoracic Society. Management of Tubercu-losis Caused by Drug-resistant Organisms. AmericanJournal of Respiratory and Critical Care Medicine 2003;167:655-657.
3. Core Curriculum on Tuberculosis: What the clinicianshould know. 4th ed. U.S. Department of Health andHuman Services, Centers for Disease Control andPrevention, National Center for HIV, STD, and TBPrevention and Division of Tuberculosis Elimination,2000;75-76.





























