Embed Size (px)
Citation preview

Carolina Population CenterUniversity of North Carolina
at Chapel Hill123 W. Franklin StreetChapel Hill, NC 27516Phone: 919-966-7482Fax: [email protected]
www.cpc.unc.edu/measure
Collaborating Partners:
Macro International Inc.11785 Beltsville Drive
Suite 300Calverton, MD 20705-3119
Phone: 301-572-0200Fax: 301-572-0999
John Snow Research and Training Institute
1616 N. Ft. Myer Drive11th Floor
Arlington, VA 22209Phone: 703-528-7474
Fax: [email protected]
Tulane University1440 Canal Street
Suite 2200New Orleans, LA 70112
Phone: 504-584-3655Fax: 504-584-3653
Funding Agency:
Center for Population, Health and Nutrition
U.S. Agency for International Development
Washington, DC 20523-3600Phone: 202-712-4959
WP-03-72
Understanding Perceptions of HIV Risk amongAdolescents in KwaZulu-Natal
Kate Macintyre, Naomi Rutenberg, Lisanne Brown, Ali Karim
October 2003

������
The research upon which this paper is based was sponsored by the MEASURE Evaluation Project withsupport from the United States Agency for International Development (USAID) under Contract No.HRN-A-00-97-00018-00.
The working paper series is made possible by support from USAID under the terms of CooperativeAgreement HRN-A-00-97-00018-00. The opinions expressed are those of the authors, and do notnecessarily reflect the views of USAID.
The working papers in this series are produced by the MEASURE Evaluation Project in order to speedthe dissemination of information from research studies. Most working papers currently are under reviewor are awaiting journal publication at a later date. Reprints of published papers are substituted forpreliminary versions as they become available. The working papers are distributed as received from theauthors. Adjustments are made to a standard format with no further editing.
A listing and copies of working papers published to date may be obtained from the MEASUREEvaluation Project at the address listed on the back cover.
Other MEASURE Evaluation Working Papers
WP-03-71 Contrasting Primary School Outcomes of Paternal and Maternal Orphans in Manicaland, Zimbabwe: HIV/AIDS and Weaknesses in the Extended Family System (Constance Nyamukapa, Simon Gregson)
WP-03-70 The Impacts of Decentralization on Health Behaviors in Uganda (Paul Hutchinson, John Akin, Freddie Ssengooba)
WP-03-69 How and When Should One Control for Endogenity Biases? Part I: The Impact of a Possibly Endogenous Explanatory Variable on a Continuous Outcome (Gustavo Angeles,David K. Guilkey, Thomas A. Mroz)
WP-03-68 The role of user charges and structural attributes of quality on the use of maternal health services in Morocco (David R. Hotchkiss, Katherine Krasovec, M. Driss Zine-Eddine El-Idrissi, Erin Eckert, Ali Mehryar Karim)
WP-03-67 Association of mass media exposure on family planning attitudes and practices in Uganda (N. Gupta, C. Katende, R. Bessinger )
WP-03-66 Multi-media campaign exposure effects on knowledge and use of condoms for STI and HIV/AIDS prevention in Uganda (R. Bessinger, C. Katende, and N. Gupta)
WP-03-65 The Social Side of Service Accessibility (B. Entwisle, A. Weinberg, R.R. Rindfuss, and K. Faust)
WP-03-64 Comparative Analysis of Program Effort for Family Planning, Maternal Health, and HIV/AIDS, 30 Developing Countries (J.A. Ross)
WP-03-63 Assessment of a Capture-Recapture Method for Estimating the Size of the Female Sex Worker Population in Bulawayo, Zimbabwe (S.S. Weir, D. Wilson, P.J. Smith, V.J. Schoenbach, J.C. Thomas, P.R. Lamptey, and J.T Boerma)
WP-02-62 Socioeconomic Status, Permanent Income, and Fertility: A Latent Variable Approach (K.A. Bollen, J.L. Glanville, and G. Stecklov)
WP-02-61 The Effect of Facility Characteristics on Choice of Family Planning Facility in Rural Tanzania (S. Chen, D. K. Guilkey)
WP-02-60 Health Program Effects on Individual Use of Services (Amy O. Tsui, Festus Ukwuani, David Guilkey, and Gustavo Angeles)
WP-02-59 Health Facility Characteristics and the Decision to Seek Care (E. Jensen, J. Stewart)
WP-02-58 HIV impact on mother and child mortality in rural Tanzania (Japheth Ng'weshemi, Mark Urassa, Raphael Isingo, Gabriel Mwaluko, Ngalula J, J Ties Boerma, Marston M, Basia Zaba)
WP-02-57 Secretive females or swaggering males? An assessment of the quality of sexual
partnership reporting in rural Tanzania (Soori Nnko, J Ties Boerma, Mark Urassa, Gabriel Mwaluko, Basia Zaba)
WP-02-56 Understanding the Uneven Spread of HIV within Africa: Comparative Study of Biological, Behavioral and Contextual Factors in Rural Populations in Tanzania and Zimbabwe (J Ties Boerma, Constance Nyamukapa, Mark Urassa, Simon Gregson)
WP-02-55 Assessment of the Roll Back Malaria Monitoring and Evaluation System (Kate Macintyre, Erin Eckert, Amara Robinson)
WP-02-54 Measuring Family Planning Sustainability at the Outcome and Program Levels (Rob
Stephenson, Amy Ong Tsui, Rodney Knight)
WP-02-53 An Assessment of the Quality of National Child Immunization Coverage Estimates in Population-based Surveys (Jennifer Brown, Roeland Monasch, George Bicego, Anthony Burton, and J. Ties Boerma)
WP-02-52 Determinants of Contraceptive Method Choice in Rural Tanzania between 1991 and 1999 (Susan Chen and David K. Guilkey)
WP-02-51 Estimation of levels and trends in age at first sex from surveys using survival analysis(Basia Zaba, Ties Boerma, Elizabeth Pisani, Nahum Baptiste)
WP-02-50 The Impact of Community Level Variables on Individual Level Outcomes: TheoreticalResults and Demographic Applications (Gustavo Angeles, David K. Guilkey andThomas A. Mroz)
WP-02-49 The Impact of a Reproductive Health Project Interventions on Contraceptive Use in Uganda (Katende C, Gupta N, Bessinger )
WP-02-48 Decentralization in Tanzania: the View of District Health Management Teams (PaulHutchinson)
WP-02-47 Community effects on the risk of HIV infection in rural Tanzania (Shelah S. Bloom,Mark Urassa, Raphael Isingo, Japheth Ng�weshemi, J. Ties Boerma)
WP-02-46 The Determinants of Fertility in Rural Peru: Program Effects in the Early Years of theNational Family Planning Program (Gustavo Angeles, David K. Guilkey and Thomas A.Mroz)
WP-02-45 Cost and Efficiency of Reproductive Health Service Provision at the Facility Level inParaguay (Gustavo Angeles, Ruben Gaete and John F. Stewart)
WP-02-44 Decentralization, Allocative Efficiency and Health Service Outcomes in the Philippines(J. Brad Schwartz , David K. Guilkey and Rachel Racelis)
WP-01-43 Changes in Use of Health Services During Indonesia's Economic Crisis (ElizabethFrankenberg, Bondan Sikoki, Wayan Suriastini, Duncan Thomas)
WP-01-42 Contraceptive Use in a Changing Service Environment: Evidence from the First Year ofIndonesia�s Economic Crisis (Elizabeth Frankenberg, Bondan Sikoki, Wayan Suriastini,DuncanThomas)
WP-01-41 Access as a Factor in Differential Contraceptive Use between Mayans and Ladinos inGuatemala (Eric Seiber and Jane T. Bertrand)
WP-01-40 Dimensions of Ratings of Maternal and Neonatal Health Services: A Factor Analysis(Rodolfo A. Bulatao and John A. Ross)
WP-01-39 Do Health Services Reduce Maternal Mortality? Evidence from Ratings of MaternalHealth Programs (Rudolfo A. Bulatao and John A. Ross)
WP-01-38 Economic Status Proxies in Studies of Fertility in Developing Countries: Does theMeasure Matter? (Kenneth A. Bollen, Jennifer L. Glanville, and Guy Stecklov)
WP-01-37 A Pilot Study of a Rapid Assessment Method to Identify Areas for AIDSPrevention in Cape Town, South Africa (Sharon S. Weir, Chelsea Morroni, NicolCoetzee, John Spencer, and J. Ties Boerma)
WP-01-36 Decentralization and Local Government Health Expenditures in the Phillippines (J. BradSchwartz, Rachel Racelis, and David K. Guilkey)
WP-01-35 Decentralization and Government Provision of Public Goods: The Public Health Sectorin Uganda (John Akin, Paul Hutchinson and Koleman Strumpf)
WP-01-34 Appropriate Methods for Analyzing the Effect of Method Choice on ContraceptiveDiscontinuation (Fiona Steele and Siân L. Curtis)
WP-01-33 A Simple Guide to Using Multilevel Models for the Evaluation of Program Impacts(Gustavo Angeles and Thomas A.Mroz)
WP-01-32 The Effect of Structural Characteristics on Family Planning Program Performance inCôte d�Ivoire and Nigeria (Dominic Mancini, Guy Stecklov and John F. Stewart)
WP-01-31 Socio-Demographic Context of the AIDS Epidemic in a Rural Area in Tanzania with aFocus on People�s Mobility and Marriage (J. Ties Boerma, Mark Urassa, Soori Nnko,Japheth Ng�weshemi, Raphael Isingo, Basia Zaba, and Gabriel Mwaluko)
WP-01-30 A Meta-Analysis of the Impact of Family Planning Programs on Fertility Preferences,Contraceptive Method Choice and Fertility (Gustavo Angeles, Jason Dietrich, DavidGuilkey, Dominic Mancini, Thomas Mroz, Amy Tsui and Feng Yu Zhang)
WP-01-29 Evaluation of Midwifery Care: A Case Study of Rural Guatemala (Noreen Goldman andDana A. Glei)
WP-01-28 Effort Scores for Family Planning Programs: An Alternative Approach (John A. Rossand Katharine Cooper-Arnold)

WP-00-27 Monitoring Quality of Care in Family Planning Programs: A Comparison of Observationand Client Exit Interviews (Ruth E. Bessinger and Jane T. Bertrand)
WP-00-26 Rating Maternal and Neonatal Health Programs in Developing Countries (Rodolfo A.Bulatao and John A. Ross)
WP-00-25 Abortion and Contraceptive Use in Turkey (Pinar Senlet, Jill Mathis, Siân L. Curtis, andHan Raggers)
WP-00-24 Contraceptive Dynamics among the Mayan Population of Guatemala: 1978-1998 (JaneT. Bertrand, Eric Seiber and Gabriela Escudero)
WP-00-23 Skewed Method Mix: a Measure of Quality in Family Planning Programs (Jane T.Bertrand, Janet Rice, Tara M. Sullivan & James Shelton)
WP-00-21 The Impact of Health Facilities on Child Health (Eric R. Jensen and John F. Stewart)
WP-00-20 Effort Indices for National Family Planning Programs, 1999 Cycle (John Ross and JohnStover)
WP-00-19 Evaluating Malaria Interventions in Africa: A Review and Assessment of RecentResearch (Thom Eisele, Kate Macintyre, Erin Eckert, John Beier, and Gerard Killeen)
WP-00-18 Monitoring the AIDS epidemic using HIV prevalence data among young womenattending antenatal clinics: prospects and problems (Basia Zaba, Ties Boerma andRichard White)
WP-99-17 Framework for the Evaluation of National AIDS Programmes (Ties Boerma, ElizabethPisani, Bernhard Schwartländer, Thierry Mertens)
WP-99-16 National trends in AIDS knowledge and sexual behaviour in Zambia 1996-98 (CharlesBanda, Shelah S. Bloom, Gloria Songolo, Samantha Mulendema, Amy E. Cunningham,J. Ties Boerma)
WP-99-15 The Determinants of Contraceptive Discontinuation in Northern India: A MultilevelAnalysis of Calendar Data (Fengyu Zhang, Amy O. Tsui, C. M. Suchindran)
WP-99-14 Does Contraceptive Discontinuation Matter?: Quality of Care and FertilityConsequences (Ann Blanc, Siân Curtis, Trevor Croft)
WP-99-13 Socioeconomic Status and Class in Studies of Fertility and Health in DevelopingCountries (Kenneth A. Bollen, Jennifer L. Glanville, Guy Stecklov)
WP-99-12 Monitoring and Evaluation Indicators Reported by Cooperating Agencies in the FamilyPlanning Services and Communication, Management and Training Divisions of theUSAID Office of Population (Catherine Elkins)
WP-98-11 Household Health Expenditures in Morocco: Implications for Health Care Reform(David R. Hotchkiss, Zine Eddine el Idriss, Jilali Hazim, and Amparo Gordillo)

WP-98-10 Report of a Technical Meeting on the Use of Lot Quality Assurance Sampling (LQAS) inPolio Eradication Programs
WP-98-09 How Well Do Perceptions of Family Planning Service Quality Correspond to ObjectiveMeasures? Evidence from Tanzania (Ilene S. Speizer)
WP-98-08 Family Planning Program Effects on Contraceptive Use in Morocco, 1992-1995 (DavidR. Hotchkiss)
WP-98-07 Do Family Planning Service Providers in Tanzania Unnecessarily Restrict Access toContraceptive Methods? (Ilene S. Speizer)
WP-98-06 Contraceptive Intentions and Subsequent Use: Family Planning Program Effects inMorocco (Robert J. Magnani)
WP-98-05 Estimating the Health Impact of Industry Infant Food Marketing Practices in thePhilippines (John F. Stewart)
WP-98-03 Testing Indicators for Use in Monitoring Interventions to Improve Women's NutritionalStatus (Linda Adair)
WP-98-02 Obstacles to Quality of Care in Family Planning and Reproductive Health Services inTanzania (Lisa Richey)
WP-98-01 Family Planning, Maternal/Child Health, and Sexually-Transmitted Diseases inTanzania: Multivariate Results using Data from the 1996 Demographic and HealthSurvey and Service Availability Survey (Jason Dietrich)
MEASURE Evaluation 1
Understanding Perceptions of HIV Risk among Adolescents in KwaZulu-Natal
October 2003
Kate Macintyre1
Naomi Rutenberg2,
Lisanne Brown1,
Ali Karim1
Running head: Understanding Perceptions of HIV Risk among Adolescents in KwaZulu-Natal
Kate Macintyre – Corresponding author 1 Department of International Health and Development, School of Public Health and Tropical Medicine, Tulane University, 1440 Canal Street, Suite 2200, New Orleans, LA 70115 Tel. 504 588 5185 Fax. 504 584 3653 [email protected]
2 The Population Council, 4301 Connecticut Ave, Suite 280, NW Washington DC 20008

MEASURE Evaluation 2
Understanding Perceptions of HIV Risk among Adolescents in KwaZulu-Natal
Abstract
Risk perception has been theorized to be an important antecedent for adopting protective
behavior. It is a key construct of research applying the Health Belief Model and other behavior
change models. In relation to HIV, risk perception is an indicator of perceived susceptibility to
infection, a measure of one’s understanding of AIDS transmission as well as willingness to
consider behavioral changes. However, there remains much we do not know about what drives
risk perception, especially among youth. This study identifies factors that influence the
calculation of HIV risk perception among a group of adolescents in South Africa. Data, collected
in 1999 from 2,716 adolescents aged 14-22, are used to explore factors predicting risk
perception. Logistic regression models suggest connectedness to parents and community for
males and females, self-efficacy to use a condom among males and living in a household with a
chronically ill member for females are associated with HIV risk perception. We conclude that a
greater understanding of the connection of adolescents to their communities and adults in their
lives is needed, and ways in which programs can alter the environments in which adolescents
form opinions, make choices, and act should be incorporated into program design.
Key words: HIV/AIDS, adolescent health, risk reduction, perception of risk
MEASURE Evaluation 3
Understanding Perceptions of HIV Risk among Adolescents in KwaZulu-Natal Introduction This paper examines the determinants of perception of risk among adolescents and young people
who are living through one of the most severe HIV epidemics globally. South African youth are
incredibly vulnerable to HIV infection. Recent population-based survey data from 2002 indicate
about 9.0% of 15-24 year-olds nationally (12.0% of females and 6.1% of males) and 8.3% in Kwa
Zulu-Natal (KZN) are infected (Mandela Foundation, 2002). These rates are already very high,
and the sexual behavior of this group over the next few years will help determine the trajectory of
the epidemic in the coming decades. Public health programmers urgently need better
understanding of the dynamics of how adolescents decide who to have sex with and whether to
use condoms or not, and perceptions of risk is believed to be one important element of this set of
dynamics.
Public health, including epidemiology, health education and other applied sciences, has
looked at individual risk from a number of perspectives. These have included the social-
psychological perspective on the one hand and sociological/anthropological perspectives on the
other. The social-psychological discipline has been most influential through the theory of
cognizance (how individuals process information) and the sociological and anthropological
perspectives have influenced public health programs in respect to the debates around what
constitutes the individuals situation within our, so-called, “risk society.” These two perspectives
are discussed below to help develop models that can be tested to explain factors that influence
adolescents’ conceptual understanding of their own risk, in relation to HIV.
This is a complex area of research, with numerous contradictory theses and hypotheses.
Public health programming has traditionally walked a delicate tightrope between multiple
disciplinary perspectives, drawing on the social–psychological perspectives for the theories
behind health education and individual responses to information cues, and using sociology to
augment the psychological explanations for behavior. These frameworks have particularly
influenced those in the socio-demographic field of inquiry to look at more structural impacts on
MEASURE Evaluation 4
behavior. Anthropological models have influenced the way public health researchers understand
the influence of cultural norms and responsibilities on individual behavior.
Cognitive theory, a highly orthodox and popular approach in social psychology, centers
around a view of individuals as active processors of information, and that the effect of any
stimulus, or information, depends on how it is categorized and interpreted by the perceiver (Eiser,
1986). Further, this interpretation depends on both attributes of the stimulus, and on prior
expectations and standards of comparison. One of the core elements of the cognitive approach,
is the recognition that although human beings are decision makers (extraordinaire) they are not
necessarily rational decision-makers, and that they can bring all sorts of assumptions, historical
experience and ideology to this decision making. This is partly acknowledgement of the myriad
biases that enter when incorrect information is at hand, but it also derives from other forces that
play important roles in how information is processed. The influence of group norms, community-
wide myths, and collective experience has increasingly been incorporated into the cognition
theoretical frameworks. This has been important for the field of adolescent reproductive health,
though little empirical data has been available to test any of these theories.
We know factual knowledge alone, in the context of AIDS, does not appear to change
behavior. In fact, many studies have concluded that no significant relationship exists between
sexual knowledge and safe sex (Farmer and Kim, 1991, Sobo, 1995, Macintyre et al., 2001a).
But if knowledge of the facts of HIV transmission plays little obvious role in increasing the
likelihood of safe sex, what does? Researchers began in the 1980s to ask about the stage that
comes between knowledge and action, which is perception of individual risk (e.g., Prohaska et al.,
1990).
Perception of risk is a key determinant in the Health Belief Model (HBM) (Janz and
Becker, 1984) and the theory of reasoned action (Ajzen and Fishein, 1980), both of which have
been often used in AIDS risk reduction programs (Prohaska et al., 1990). The argument is that
people use condoms (or have only one partner or postpone sexual initiation) if they think the
costs of the potential illness (the negative consequences) outweigh the costs of buying condoms,
overcoming reluctance to wear a condom, and demanding that it be used every time. Many of
MEASURE Evaluation 5
these models that are based on rational, logical thought processes, also acknowledge that
emotion (self-efficacy and self-esteem) may have a mediating effect on the risk perception, but
few have examined the mechanisms behind emotion (Sobo, 1995).
Very low perception of risk, even in relatively high prevalence situations has been
reported in a number of settings. For example, in Ethiopia, Sahlu et al. (1999) found that only
17% of men and 2% of women, despite high and correct knowledge of HIV transmission,
acknowledged that they were at any risk of HIV. In Tanzania two recent studies have reported
increases in perception of high risk among young men and women in Dar Es Salaam, though
they still underestimate their own risk relative to data from the national surveillance system. Of
the Tanzanian students interviewed, 25% felt that they were at personal risk of having HIV.
Meanwhile, 41% thought their friends were at great risk (Maswanya et al., 1999). In Zambia,
Magnani et al. (2001) report that although 52% of the young people interviewed in a cross-
sectional study knew someone with AIDS, most of the younger group of adolescents did not think
they were at risk of getting AIDS. MacPhail and Campbell (2001) report that almost 70% of the
young South African men they spoke to said there was “no chance of their becoming infected or
that they didn’t know whether or not they were personally vulnerable.” Conversely, a Gambian
study in a low prevalence area found that the adolescents considered that they were the most at
risk group in the country for HIV (Miles et al., 2001), and that this group seemed to overestimate
their risk. Intense public media attention and health education programs may lead to teens over-
estimating their risk.
“Optimistic” bias is a central theoretical issues for adolescent research on perception of
risk (Eiser, 1986). Optimistic bias theory (which is part of the cognitive approach in social
psychology) says that many people think along the lines of “AIDS/STDs/pregnancy/cancer etc…
can’t happen to me” with a consequence that many systematically underestimate their risk in
comparison to the real risk. The hypothesized determinants of this bias towards under-estimation
of risk may include the difficulty in realizing that an illness that may affect you in later years needs
to be actively prevented today, and therefore it is treated as a very distant possibility. A second
potential factor underlying underestimation of risk is the general notion of adolescent
MEASURE Evaluation 6
invulnerability. Adolescents tend to undervalue their own risk, certainly when they compare
themselves with adults, but even in comparison to their peers.
Third, admitting to being at risk of HIV means, in many people’s minds, admitting to place
oneself in the category of a stigmatized person. AIDS in South Africa (as elsewhere) carries
enormous stigma, related to both the fear of dying and death and the long held association of
AIDS with homosexuals and prostitution. Homosexuality among many sectors of South African
society is virtually a taboo notion, while prostitution is associated both with poverty and
immorality. None of these categories are enticing, especially to adolescents still unsure of their
identity. Thus, to perceive oneself as high-risk the individual adolescent has to either overcome
the thought and image of the stigmas or perhaps to have had some other over-riding shock,
perhaps through personally knowing someone who has died of the disease.
Only a few studies have focused on the possible influences of peers and parents on the
accuracy of individual risk perception, although Edem and Harvey (1995) discuss the influence of
family through the discussions about HIV and the use of condoms. Van Landingham (1995)
shows the potential for peer influence and especially peer group norms on whether individuals
condone the use of condoms or not. There is a growing body of literature that shows the relative
connectedness of adolescents to their schools, their peers and their families (not in that order)
may be important protective factors, and thus operate as suppressors of risk. However, Magnani
et al., (2001) have recently demonstrated a weaker than expected association between
adolescents’ sexual risk-taking behavior and their connection to parents. Magnani’s study was
conducted in Zambia, and the authors hypothesize that adolescents growing up in Lusaka may
be extraordinarily affected, due to the high prevalence of HIV and AIDS, to disruption within and
among households, thus dampening the protective effect of connections in the household.
The influence of experience and personal knowledge of someone with HIV/AIDS is also
thought to influence risk perception, and has been studied in a number of different settings using
different methods. The notion behind this experiential theory is that AIDS does not become real,
or denial is preferable, including denial of risk, until one witnesses someone ill or dying of AIDS.
In 1995, Sweat et al. (1995) reported that young Thai men had very high fears of HIV, yet low
MEASURE Evaluation 7
perception of their own risk of acquiring the disease. In focus groups, individuals said that their
perception was low because they “had never known anyone with AIDS,” and because “prostitutes
[that they had visited] had health certificates” (Sweat et al., 1995). Bosga et al. (1995) report that
men who engaged in risky behavior did not perceive their behavior as such, unless they had
known someone who was ill or who had died from AIDS. In South Africa, MacPhail and Campbell
(2001) report conflicting views of HIV risk among young people about the level of HIV infection in
the community of Khutsong, a township outside the mining town of Carltonville. Some of their
respondents thought AIDS “is not common here” (said by a 20-25 year old woman). This in a
context of very high infection rates, with one survey (Williams et al., 1999) suggesting over 40%
of South African young adults (20-25) may be infected. In the same study, other respondents
agreed that AIDS was a threat to the community, with more women than men agreeing with this
sentiment. Some commented that personal experience with AIDS was “forcing people to
acknowledge that it really exists.” Finally, a cross national comparative study of men’s behaviors
in Zambia, Uganda and Kenya found that a lower level of risky behavior, controlling for all other
factors, was associated with the respondent having personally known someone who had died of
AIDS (Macintyre et al., 2001a).
But regarding perception of risk as an outcome opens one up to the charge of having a
recursive model. This has often been discussed in relation to the HBM. For example,
Montgomery et al. (1989) gives several examples where the expected association between
perception of risk and relatively safe sexual practices is found; i.e., that the higher the perception
of risk the more likely condoms are being used. But Havanon et al. (1992) argue that men who
were engaging in risky sexual behavior were aware of the risks involved and acknowledged they
were at high risk; i.e., that the higher the perception of risk, the more likely the men were not
using condoms. Other examples come from studies of intravenous drug users in the U.S. who
are reported to use their knowledge of the prevalence of HIV in their neighborhoods to predict
their perception of their own risk (Valle et al., 1999). One study among adolescents in the US
(Ellen et al., 1996) describes the determinants of perception of risk as including past condom use,
as well as number of lifetime partners, and a belief that the adolescent would prevent STDs and
MEASURE Evaluation 8
could also recognize someone with an STD. And young sexually active Nigerians who perceive
themselves as being at high risk of testing positive to HIV, were also more likely to have never
used condoms (Edem and Harvey, 1995).
The influence of the social context and environment on individual perception of risk has
been the concern of sociological and anthropological debates for many years. The concept of the
relationship between modernity and risk is currently a major theme within sociological theoretical
thinking. Theorists such as Douglas, Giddens, Arendt, Beck and Foucault have emphasized the
need to look outside the individual to the structural influences that surround us as individuals in
order to judge the varied influence of risk, including the perception of risk, on our behavior and
social relations. This tradition has influenced the theoretical thinking around adolescent
reproductive health for several years (DiClemente, 2000), and on HIV prevention tactics for about
a decade (Sweat et al., 1995 and Coates, 1997). Meanwhile, empirical studies in the U.S. have
begun to test structural and environmental relationships to adolescent behavior, mostly in relation
to the risk and protective factors framework (see Resnick et al., 1997; Jessor et al. 1998).
However, much less has been done to test these distal factors in developing country contexts
(Magnani et al., 2002; Macintyre et al., 2001b).
Much of the focus of the risk and protective factors framework emphasizes the
importance of “connectedness.” This has ranged from connection to peers, to school and to
family members. It is hypothesized that having higher levels of connectedness provides the
adolescents with protection from harms, provides positive role models, and is indicative of access
to other development assets (money, work, opportunities for extra curriculum activities etc.). The
important variables have ranged from the standard socioeconomic and education related
variables at the household level, to measures of how well the adolescent is linked to their family,
and does he/she have a close relationship with a parent or parent-figure, an older sibling or close
family relation with whom they can discuss reproductive health matters including AIDS.
The community or environmental variables that have emerged as possibly important
predictors include factors related to the physical environment that lead to perceptions of safety for
the community members including young people (Sampson et al., 1997; Cohen et al., 2000).
MEASURE Evaluation 9
These have been measured using a rating of the cleanliness of the neighborhood, as well as how
the municipality or bureaucracy functions in relation to rubbish collection, waste water
management and provision of water for the inhabitants of the area. All of these measures are
interpreted as possible, measurable associations between individual’s perception of risk and the
likelihood that he or she will act in risky ways. A well-ordered environment, often associated with
higher socio-economic strata, may well co-exist with and perhaps even influence the perception
that individuals within this community are at low risk for everything negative (including HIV).
Conversely, a disordered and violent environment may also co-vary with a perception that
members of that community are at high risk for everything, including HIV. Communal levels of
the perception of risk for the general population within a specific community may well influence
(through gossip or through the talk of leaders) individuals to see themselves at a particular level
of low or high risk.
In sum, the picture is a mixed one, with some adolescents appearing to view the fact that
they have never or rarely use condoms as indicative that they are at high risk of becoming or
being HIV positive, while others may perceive themselves at high risk (in general) and therefore
use condoms out of fear of contracting the disease. The calculus of risk is clearly complex, and
drawing definite conclusions from this review of a few studies is unwise (see also Poppen and
Reisen, 1997).
The premise underlying “safe sex” programs is that most individuals are assumed to want
to avoid serious disease—so the determinants are the perceived probabilities (and
consequences) and the perceived costs and benefits of a risk reduction strategy. However, this
premise also assumes that individuals have full knowledge of both these costs and the benefits of
this strategy. What are the probabilities and estimates that go into the calculation of risk?
Presumably, they include: the past history of their current partner in terms of STDs, their own past
history and their former partners’ histories, where these partners have come from and their area
of residence, whether any of them have also been exposed through other channels (e.g., drugs or
blood transfusion), etc. Are young people’s prior experiences, for example, with a STD, make it
MEASURE Evaluation 10
more likely that they may subsequently place them selves in a high-risk group? Do friends
influence each other?
Teenagers and young adults in South Africa are being forced to calculate this risk and
then to operate within a very difficult, and rapidly changing environment. One writer offers a very
pessimistic idea in relation to AIDS-risk when she says “accurate perceptions of AIDS risk [may
be] beyond our cognitive capabilities” (Sobo, 1995). We take a different view—that researchers
must try to disentangle the determinants and impact of perceptions of risk in order to use the
information to help adolescents calculate the costs and benefits of a risk reduction strategy and
offer them support and services to act on it. To this end, we employ multi-level models to identify
the individual, social and environmental factors that influence the calculation of risk by
adolescents living in the heart of the AIDS epidemic in South Africa using data from the study
Transitions to Adulthood in the Context of AIDS in South Africa (Rutenberg et al., 2001).
Data and Methods
The study Transitions to Adulthood in the Context of AIDS in South Africa was carried out in
KwaZulu-Natal in 1999. KwaZulu-Natal (KZN) is situated on the east coast along the Indian
Ocean, and with a population of 8.4 million is the most populous province in South Africa. The
province is approximately 45% urban and includes Durban, the largest port and third largest city
in the country. Just under one-quarter of the country’s black population resides in the province.
KZN has one of the highest levels of HIV in the country; with HIV prevalence among all antenatal
care attendees (the site of national surveillance system for HIV) at 34% in 2001 (South African
Department of Health, 2002). While the data from the population-based survey reported earlier
(Mandela Foundation, 2002) that showed youth in KZN as having a prevalence of about 8.3% is
slightly less alarming than the surveillance data, there is nevertheless one of the worst
generalized epidemics among youth going on in KZN at the moment.
For this study, two districts in KZN—Durban Metro and Mtunzini—were purposely
selected in order to encompass urban, transitional and rural regional variation within the province.
Within these districts, sample households (i.e., households with at least one resident 14-22 years
MEASURE Evaluation 11
of age) were chosen using a modified stratified, multi-stage cluster sampling approach often
referred to as the “segmentation method” (Turner et al., 1996). Prior to fieldwork, Census
Enumeration Areas (EA) were stratified into race categories (African, Indian, White) based upon
their majority composition. EAs were allocated to racial categories proportionally to their
representation in the population in the two districts. In the first stage of sample selection, 118
EAs were chosen from a sampling frame consisting of all EAs in the two districts using a
systematic-random sampling procedure with probability-proportional-to-size (PPS). At the second
stage, EAs were divided by field supervisors into approximately equal sized segments of about 50
households based upon a “quick count” of households undertaken as a preliminary field
operation. One segment was then selected randomly and interviewers attempted to obtain the
information sought from all households and youth within that segment, visiting households up to
three times. The data collection teams were composed of male and female Africans, Indians and
Whites in proportion to the distribution in the sample. Interviews were conducted by a field
worker of the same race and gender as the respondent.
All households in the selected EAs with one or more adolescents between the ages of 14
and 22 were eligible. Within sample households, two separate individual structured
questionnaires were administered. First, a household questionnaire was administered to an adult
(age 18 or over) in the household. For the most part this adult was a parent or other adult relative
(e.g., grandparent, aunt). When an adult was not available, the interviewer discontinued with the
household and returned at a later time when an adult was said to be available. The interview
solicited information on numbers and background characteristics of usual residents of the
household, household assets and expenditures (as indicators of socioeconomic position), living
conditions (e.g., building material, number of rooms), economic shocks (e.g., death in the family,
loss of job, abandonment or divorce), expenditure, government assistance, and knowledge of and
attitudes toward selected adolescent sexual-reproductive health issues.
Based on the roster of residents obtained in the household interview, all youth aged 14-
22 were eligible for interview. These interviews covered the background characteristics of the
respondents, education history, work experience, exposure to school-based life skills programs,
MEASURE Evaluation 12
sexual relationships, contraceptive and condom knowledge, attitudes and use, knowledge and
perception of HIV risk, connectedness to school, family and community, alcohol and drug use,
and reproductive history.
Interviewers obtained informed consent for both household and youth interviews. For
youth under the age of 16, parental consent was also obtained. Attempts were made to ensure
privacy by conducting the interviews in a separate room when possible or even going outside.
Respondents did not receive any compensation for their time. Interviews were face-to-face and
responses were recorded on paper and then subsequently entered into a database.
Data collection resulted in 1,974 household and 3,052 individual interviews with
adolescents aged 14-22. The interviews were conducted in 113 sample EAs during September
and October 1999. A separate community survey was conducted six months after the adolescent
and household interviews (May 2000) in the same 113 EAs. For this study, a community was
defined by the administrative boundaries of the EA. Two complementary methods were used.
First, data was gathered through observation: where interviewers, using a structured checklist,
assessed the presence and quality of physical infrastructures, community maintenance and
general observable cleanliness of those structures.
Second, data were collected using a street intercept module where interviews were
conducted with people living in the community. Respondents were recruited at several central
locations in the community, such as in shopping centers, bus stops, or along busy streets.
Interviewers were conducted with 40 respondents living in the EA, of which half were male and
half female and half between the ages of 14 and 30 years and half above age 30 in order to
obtain information from older and younger community members. The EA boundaries were
described to the respondents to establish their eligibility to participate and to define for them the
area to which questions were referring. Questions on the perceived levels of crime and safety
were asked. Also, the perception of HIV risk and attitudes toward people living with AIDS were
assessed.
Teams of six pairs (four African, one Asian and one White pair) were trained for the
community surveys. Training included discussion of the outcomes of the household and

MEASURE Evaluation 13
individual adolescent surveys, followed by the purpose of the community study and the
methodologies to be employed, specifically interview and observation techniques. Pilot testing
was conducted to ensure that common definitions of items be observed. Each team was
assigned a number of communities and each member of the team went to collect the data
(observation and street intercept) separately. Two to three days were allocated for each EA.
Findings and experiences from each team were compared; differences in perceptions and
definitions of observed items were discussed and consensus achieved. Two external quality
controllers visited six other areas each and reported only minor adjustments to the schedules.
Finally, as each team returned from the field, they debriefed with the research team who probed
and "interviewed" the interviewers, supplementing the maps and making adjustments to the
schedules where necessary. Although these street intercept surveys were only quasi-random, a
post hoc analysis matching various variables across the household, individual and community
surveys suggest that the individuals interviewed in the street intercept module were similar in
characteristics such as socio-economic, education levels, knowledge and attitude regarding HIV,
and other variables available across the three surveys. Moreover, data from the two community
modules were analyzed at the EA level, which were randomly selected. Therefore, the street
intercept data was aggregated at the community/EA level.
Variable Measurement
The dependent variable is whether the adolescent perceives himself or herself at no risk or at any
risk based on his or her response to the following question: Do you think you have no risk, a
small risk, a moderate or a great risk of getting the AIDS virus in the next 12 months? Overall,
76% of the respondents said they were at no risk, while 24% said they were at some risk of
getting the AIDS virus—13% reported they were at a small risk, 4% reported a moderate risk, and
7% said they were at great risk.
The classification of risk behavior is based on responses to questions about whether the
respondent had ever had sex, used condoms, and the number of sexual partners in the past 12
months. Respondents were classified as having low-risk behavior if they had never had sex, had

MEASURE Evaluation 14
not had sex in the past year, or had no more than one partner during the past 12 months and
always used condom with that partner. Respondents were considered to have high-risk behavior
if they had two or more partners in the past 12 months or had one partner and inconsistent
condom use. The decision to use a dichotomous categorical variable for risk behavior was based
on previous research (Cantania et al., 1990) and sample size available.
We tested a number of variables which we hypothesized are related to risk perception
based on an extensive literature review of adolescent risk taking and community level impacts on
adolescent behavior. Individual level variables include age, race, and residence (Durban metro
or Mtunzini). We also include reported confidence in using a condom (the self-efficacy index),
connectedness to a parent, knowledge of someone who has died of HIV/AIDS, willingness to
have a person living with HIV/AIDS as a friend, thinks those who are HIV positive should remain
in school, connectedness to neighborhood (has friends in the neighborhood), has experienced
forced sex (females only), and whether the individual reported any STD symptoms in the past 12
months (either gender). The household-level variables in the model are whether a household
member was chronically ill in the last 12 months and whether HIV/AIDS was discussed often at
home. Community-level social and economic environmental measures include the percentage of
the community with paved roads, the perceived safety in the community, and the percent of
adolescents in the neighborhood who are enrolled in school. The measure of adult perception of
the degree of HIV risk in the community is based on the proportion of those over 30 who think
youth in their neighborhood are at high risk of AIDS. We also asked all community informants if
they knew of someone in their community who had died of AIDS.
Analysis
We used logistic regression to examine factors that predict risk perception. A methodological
challenge is to understand the relationship between risk perception and risky behavior, as it could
be in either direction. This is especially problematic when using cross-sectional data, because
one cannot tell whether perceived susceptibility causes behavioral change, or merely reflects an
understanding of the risks that that individual is taking. In order to try to approach this problem

MEASURE Evaluation 15
from a slightly different angle, we control for behavioral risk by dividing our sample of adolescents
into high and lower risk takers based on their reported sexual behavior and examine risk
perception within each group. Previous analyses of this population of adolescents have
underscored the sharp gender difference in HIV risk behaviors (Macintyre et al., 2001b;
Rutenberg et al., 2000). We continue our detection of gender-specific influences by running
separate models for males and females. STATA 7 was used to analyze the data. Its functions
using “logit macros” can control for hierarchical multi-level models and cluster sampling designs
were employed at all relevant stages. Weights were applied at all relevant levels—i.e., individual,
household and community level. It should be noted however that these data are relevant only to
the two districts—Durban Metro and Mtunzini magisterial district—that were purposely selected at
the outset of the survey. Generalizing results to adolescent behavior and risk perception beyond
these regions is incorrect.
Results
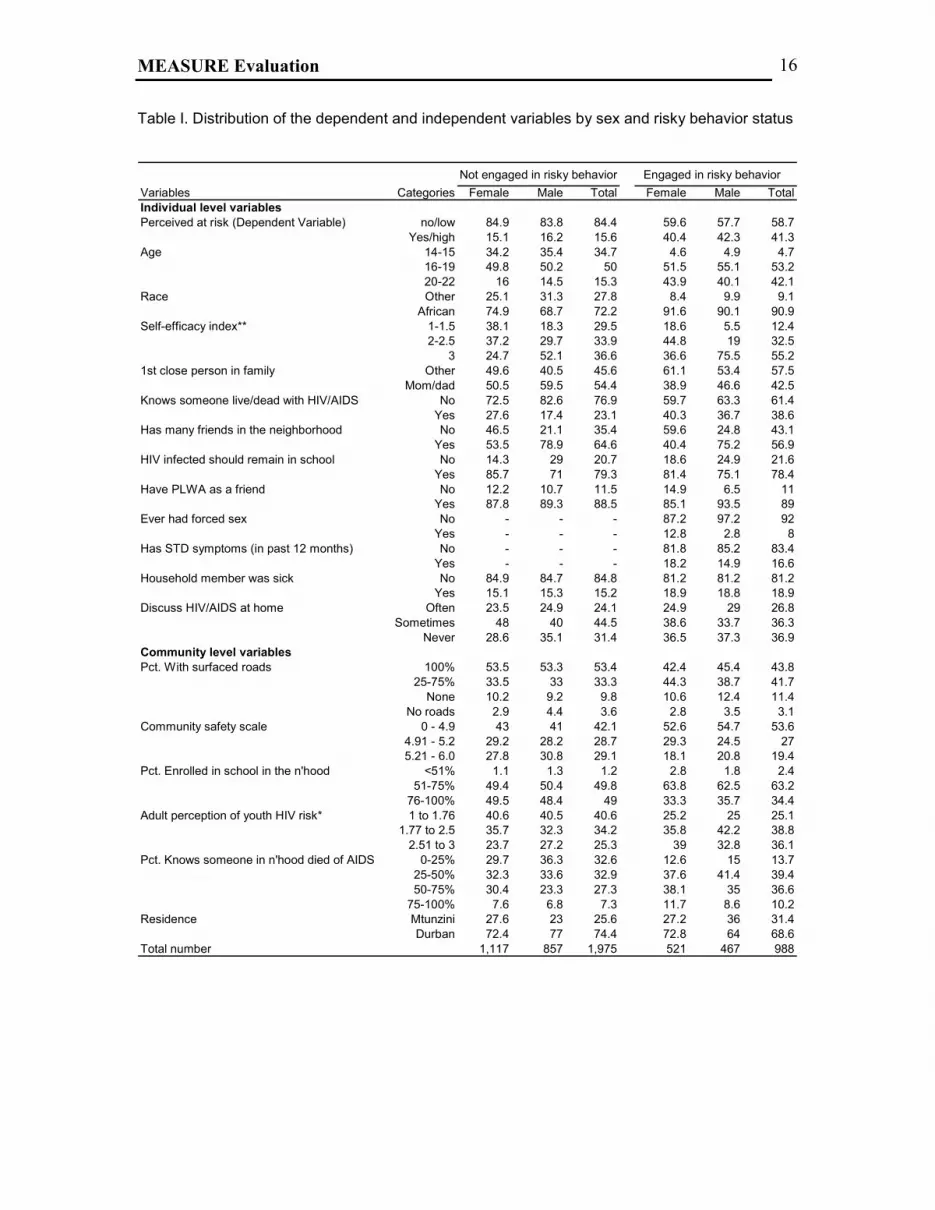
Distributions of the dependent and independent variables across gender and by their reported
risky behaviors are shown in Table I. The table is divided by the self report of whether the
adolescent reported recent risk behavior. Respondents were considered to have high risk
behavior if they had two or more partners in the past 12 months or had one partner and
inconsistent condom use, otherwise they were classified as engaging in low risk behavior. We
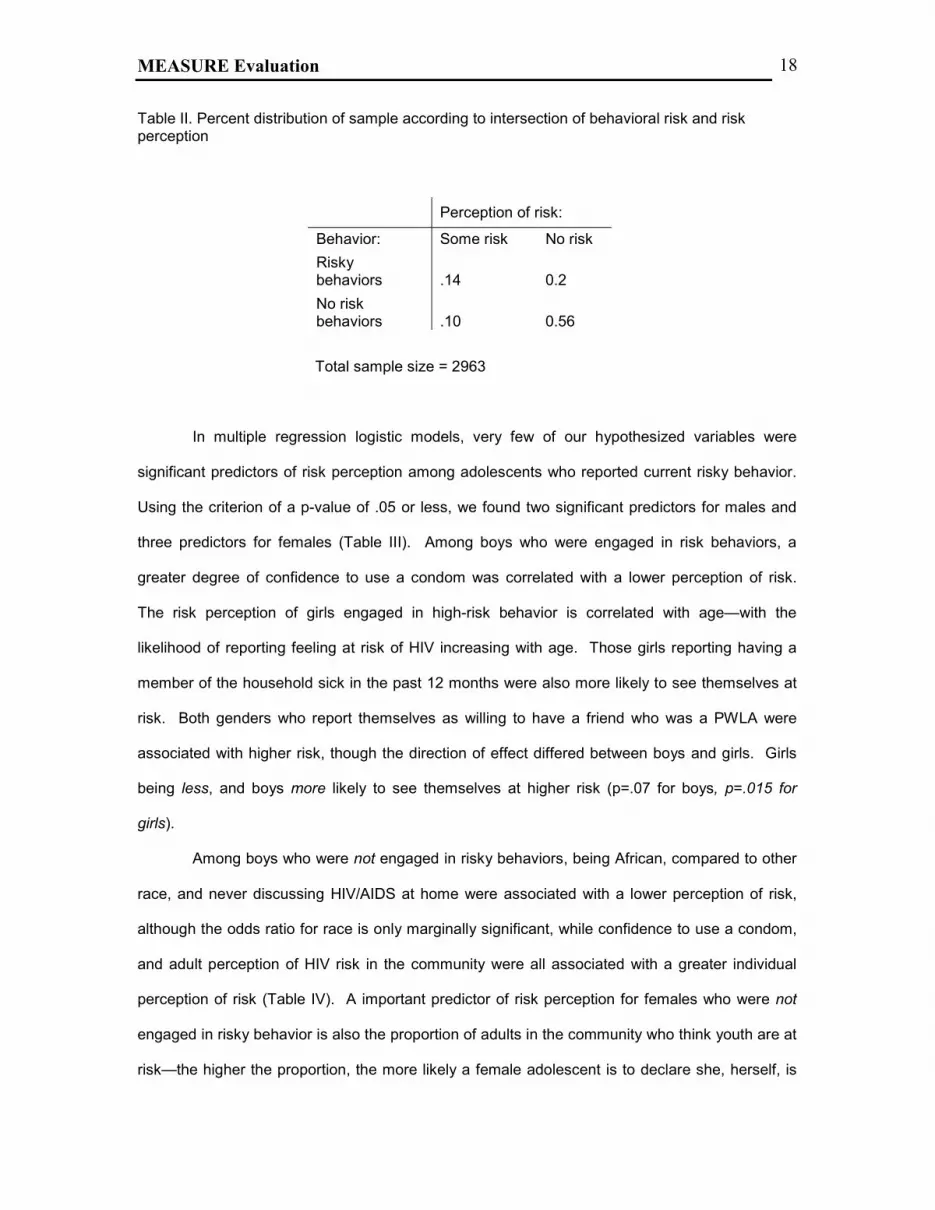
next examined risky behavior by risk perception in order to consider four categories of adolescent
HIV behavior risk (Table II). The first category we consider as “highly vulnerable,” i.e.,
respondents with high-risk behaviors but no perception that they are at risk of HIV infection. This
accounts for 20% of our sample. The majority of this group said that they believed they were not
at risk because they were abstinent (17%), had only one sexual partner (26%), or always used
condoms (30%). However, this is inconsistent with their reported behavior. We view these
adolescents as a priority for programs concerned with addressing adolescents’ vulnerability to
HIV because their denial and lack of recognition of their risk means that they likely
MEASURE Evaluation 16
Table I. Distribution of the dependent and independent variables by sex and risky behavior status
Not engaged in risky behavior Engaged in risky behaviorVariables Categories Female Male Total Female Male TotalIndividual level variablesPerceived at risk (Dependent Variable) no/low 84.9 83.8 84.4 59.6 57.7 58.7 Yes/high 15.1 16.2 15.6 40.4 42.3 41.3Age 14-15 34.2 35.4 34.7 4.6 4.9 4.7 16-19 49.8 50.2 50 51.5 55.1 53.2 20-22 16 14.5 15.3 43.9 40.1 42.1Race Other 25.1 31.3 27.8 8.4 9.9 9.1 African 74.9 68.7 72.2 91.6 90.1 90.9Self-efficacy index** 1-1.5 38.1 18.3 29.5 18.6 5.5 12.4 2-2.5 37.2 29.7 33.9 44.8 19 32.5 3 24.7 52.1 36.6 36.6 75.5 55.21st close person in family Other 49.6 40.5 45.6 61.1 53.4 57.5 Mom/dad 50.5 59.5 54.4 38.9 46.6 42.5Knows someone live/dead with HIV/AIDS No 72.5 82.6 76.9 59.7 63.3 61.4 Yes 27.6 17.4 23.1 40.3 36.7 38.6Has many friends in the neighborhood No 46.5 21.1 35.4 59.6 24.8 43.1 Yes 53.5 78.9 64.6 40.4 75.2 56.9HIV infected should remain in school No 14.3 29 20.7 18.6 24.9 21.6 Yes 85.7 71 79.3 81.4 75.1 78.4Have PLWA as a friend No 12.2 10.7 11.5 14.9 6.5 11 Yes 87.8 89.3 88.5 85.1 93.5 89Ever had forced sex No - - - 87.2 97.2 92 Yes - - - 12.8 2.8 8Has STD symptoms (in past 12 months) No - - - 81.8 85.2 83.4 Yes - - - 18.2 14.9 16.6Household member was sick No 84.9 84.7 84.8 81.2 81.2 81.2 Yes 15.1 15.3 15.2 18.9 18.8 18.9Discuss HIV/AIDS at home Often 23.5 24.9 24.1 24.9 29 26.8 Sometimes 48 40 44.5 38.6 33.7 36.3 Never 28.6 35.1 31.4 36.5 37.3 36.9Community level variablesPct. With surfaced roads 100% 53.5 53.3 53.4 42.4 45.4 43.8 25-75% 33.5 33 33.3 44.3 38.7 41.7 None 10.2 9.2 9.8 10.6 12.4 11.4 No roads 2.9 4.4 3.6 2.8 3.5 3.1Community safety scale 0 - 4.9 43 41 42.1 52.6 54.7 53.6 4.91 - 5.2 29.2 28.2 28.7 29.3 24.5 27 5.21 - 6.0 27.8 30.8 29.1 18.1 20.8 19.4Pct. Enrolled in school in the n'hood <51% 1.1 1.3 1.2 2.8 1.8 2.4 51-75% 49.4 50.4 49.8 63.8 62.5 63.2 76-100% 49.5 48.4 49 33.3 35.7 34.4Adult perception of youth HIV risk* 1 to 1.76 40.6 40.5 40.6 25.2 25 25.1 1.77 to 2.5 35.7 32.3 34.2 35.8 42.2 38.8 2.51 to 3 23.7 27.2 25.3 39 32.8 36.1Pct. Knows someone in n'hood died of AIDS 0-25% 29.7 36.3 32.6 12.6 15 13.7 25-50% 32.3 33.6 32.9 37.6 41.4 39.4 50-75% 30.4 23.3 27.3 38.1 35 36.6 75-100% 7.6 6.8 7.3 11.7 8.6 10.2Residence Mtunzini 27.6 23 25.6 27.2 36 31.4 Durban 72.4 77 74.4 72.8 64 68.6Total number 1,117 857 1,975 521 467 988

MEASURE Evaluation 17
perceive current program messages about HIV and behavior change as personally irrelevant.
We believe that understanding who is in this group and the reasons they believe they are not at
risk is a high priority in order to develop messages that do resonate with this vulnerable group
and are effective in eliciting behavior change. These issues are explored in the multivariate
analysis described below.
The second category is comprised of adolescents who are at risk and recognize they are
at risk, which accounts for 14% of our sample. Nearly half of this group reported being at risk
because they had unprotected sex (30%) or because they have multiple partners (18%).
According to classic health belief and AIDS risk reduction models, because these adolescents
recognize their risk factors they should be predisposed to interventions and support that help
them behave safely.
The third group is the “worried well”; they believe they are at risk but currently report no
risk behaviors. These account for 10% of the sampled youth. It may be that they are concerned
because of the generalized HIV/AIDS epidemic in South Africa or because they perceive their
immediate environment as risky, e.g., know someone who is infected with HIV or observe
considerable peer pressure or coercion to have unprotected sex. It may be they have recently
changed their behavior and lowered their personal risk because of their concerns. Indeed, 35%
of respondents in this group reported abstinence as their reason for feeling at risk when in fact
they may have meant that because they felt susceptible to HIV they were abstaining from sex.
Adolescents are also concerned about the risk of HIV transmission if a road or sports accident
was to occur, that is, that they would be exposed to HIV infected blood from another injured
person or while receiving first aid treatment.
The fourth group, the majority of adolescents—56%, is those who have no risk factors
nor do they perceive they are at risk. Three-quarters of these adolescents are not yet sexually
active; they may view themselves too young for sex, the opportunity for sex may not yet have
presented itself or they have deliberately postponed sexual initiation to reduce their HIV risk.
MEASURE Evaluation 18
Table II. Percent distribution of sample according to intersection of behavioral risk and risk perception
Perception of risk:
Behavior: Some risk No risk Risky behaviors .14 0.2 No risk behaviors .10 0.56
Total sample size = 2963
In multiple regression logistic models, very few of our hypothesized variables were
significant predictors of risk perception among adolescents who reported current risky behavior.
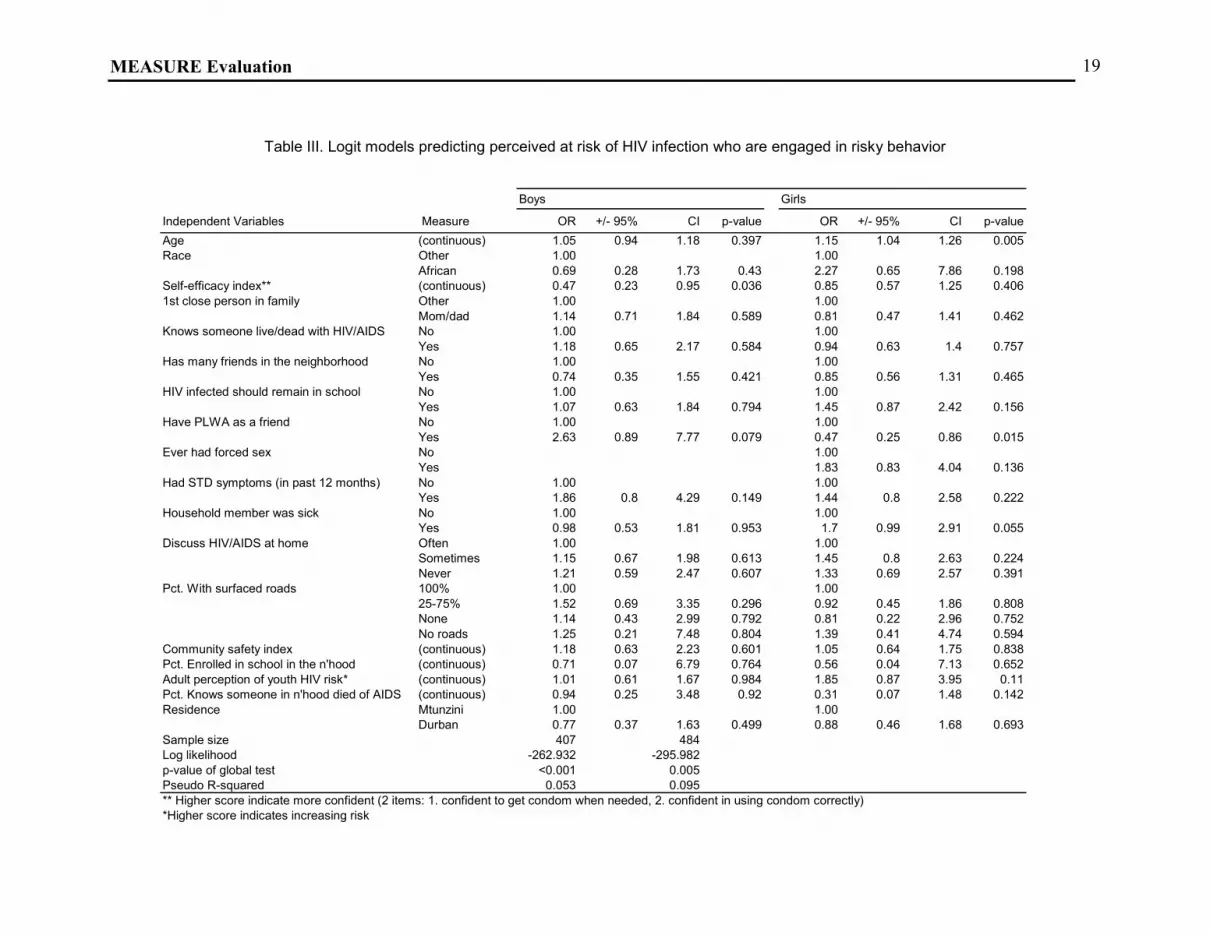
Using the criterion of a p-value of .05 or less, we found two significant predictors for males and
three predictors for females (Table III). Among boys who were engaged in risk behaviors, a
greater degree of confidence to use a condom was correlated with a lower perception of risk.
The risk perception of girls engaged in high-risk behavior is correlated with age—with the
likelihood of reporting feeling at risk of HIV increasing with age. Those girls reporting having a
member of the household sick in the past 12 months were also more likely to see themselves at
risk. Both genders who report themselves as willing to have a friend who was a PWLA were
associated with higher risk, though the direction of effect differed between boys and girls. Girls
being less, and boys more likely to see themselves at higher risk (p=.07 for boys, p=.015 for
girls).
Among boys who were not engaged in risky behaviors, being African, compared to other
race, and never discussing HIV/AIDS at home were associated with a lower perception of risk,
although the odds ratio for race is only marginally significant, while confidence to use a condom,
and adult perception of HIV risk in the community were all associated with a greater individual
perception of risk (Table IV). A important predictor of risk perception for females who were not
engaged in risky behavior is also the proportion of adults in the community who think youth are at
risk—the higher the proportion, the more likely a female adolescent is to declare she, herself, is
MEASURE Evaluation 19
Table III. Logit models predicting perceived at risk of HIV infection who are engaged in risky behavior
Boys Girls
Independent Variables Measure OR +/- 95% CI p-value OR +/- 95% CI p-valueAge (continuous) 1.05 0.94 1.18 0.397 1.15 1.04 1.26 0.005Race Other 1.00 1.00
African 0.69 0.28 1.73 0.43 2.27 0.65 7.86 0.198Self-efficacy index** (continuous) 0.47 0.23 0.95 0.036 0.85 0.57 1.25 0.4061st close person in family Other 1.00 1.00
Mom/dad 1.14 0.71 1.84 0.589 0.81 0.47 1.41 0.462Knows someone live/dead with HIV/AIDS No 1.00 1.00
Yes 1.18 0.65 2.17 0.584 0.94 0.63 1.4 0.757Has many friends in the neighborhood No 1.00 1.00
Yes 0.74 0.35 1.55 0.421 0.85 0.56 1.31 0.465HIV infected should remain in school No 1.00 1.00
Yes 1.07 0.63 1.84 0.794 1.45 0.87 2.42 0.156Have PLWA as a friend No 1.00 1.00
Yes 2.63 0.89 7.77 0.079 0.47 0.25 0.86 0.015Ever had forced sex No 1.00
Yes 1.83 0.83 4.04 0.136Had STD symptoms (in past 12 months) No 1.00 1.00
Yes 1.86 0.8 4.29 0.149 1.44 0.8 2.58 0.222Household member was sick No 1.00 1.00
Yes 0.98 0.53 1.81 0.953 1.7 0.99 2.91 0.055Discuss HIV/AIDS at home Often 1.00 1.00
Sometimes 1.15 0.67 1.98 0.613 1.45 0.8 2.63 0.224Never 1.21 0.59 2.47 0.607 1.33 0.69 2.57 0.391
Pct. With surfaced roads 100% 1.00 1.00 25-75% 1.52 0.69 3.35 0.296 0.92 0.45 1.86 0.808 None 1.14 0.43 2.99 0.792 0.81 0.22 2.96 0.752 No roads 1.25 0.21 7.48 0.804 1.39 0.41 4.74 0.594Community safety index (continuous) 1.18 0.63 2.23 0.601 1.05 0.64 1.75 0.838Pct. Enrolled in school in the n'hood (continuous) 0.71 0.07 6.79 0.764 0.56 0.04 7.13 0.652Adult perception of youth HIV risk* (continuous) 1.01 0.61 1.67 0.984 1.85 0.87 3.95 0.11Pct. Knows someone in n'hood died of AIDS (continuous) 0.94 0.25 3.48 0.92 0.31 0.07 1.48 0.142Residence Mtunzini 1.00 1.00
Durban 0.77 0.37 1.63 0.499 0.88 0.46 1.68 0.693Sample size 407 484Log likelihood -262.932 -295.982p-value of global test <0.001 0.005Pseudo R-squared 0.053 0.095** Higher score indicate more confident (2 items: 1. confident to get condom when needed, 2. confident in using condom correctly)*Higher score indicates increasing risk

MEASURE Evaluation 20
Table IV. Logit model predicting perceived at risk of HIV infection who are not engaged in risky behavior
Boys Girls
Independent variables Measure OR +/- 95% CI p-value OR +/- 95% CI p-valueAge (continuous) 1.08 0.92 1.26 0.334 1.09 1.00 1.18 0.064Race Other 1.00 1.00
African 0.43 0.16 1.16 0.096 0.43 0.13 1.48 0.182Self-efficacy index** (continuous) 2.02 1.4 2.91 <0.001 1.05 0.79 1.41 0.7351st close person in family Other 1.00 1.00
Mom/dad 0.81 0.5 1.31 0.389 0.58 0.42 0.8 0.001Knows someone live/dead with HIV/AIDS No 1.00 1.00
Yes 0.92 0.56 1.5 0.731 1.32 0.8 2.17 0.28Has many friends in the neighborhood No 1.00 1.00
Yes 0.59 0.24 1.46 0.256 0.94 0.64 1.37 0.743HIV infected should remain in school No 1.00 1.00
Yes 0.71 0.43 1.16 0.168 1.45 0.71 2.97 0.308Have PLWA as a friend No 1.00 1.00
Yes 0.93 0.24 3.58 0.91 1.23 0.41 3.73 0.709Household member was sick No 1.00 1.00
Yes 1.15 0.66 2.03 0.619 2.21 1.43 3.41 <0.001Discuss HIV/AIDS at home Often 1.00 1.00
Sometimes 0.93 0.53 1.62 0.799 2.5 1.38 4.53 0.002Never 0.57 0.34 0.96 0.033 1.31 0.63 2.75 0.47
Pct. With surfaced roads 100% 1.00 1.00 25-75% 1.11 0.6 2.05 0.736 1.18 0.53 2.62 0.678 None 1.55 0.46 5.25 0.484 0.36 0.07 1.82 0.218 No roads 0.42 0.11 1.57 0.198 0.7 0.12 4 0.685Community safety index (continuous) 0.82 0.58 1.15 0.241 1.21 0.4 3.67 0.734Pct. Enrolled in school in the n'hood (continuous) 0.37 0.02 7.25 0.511 0.72 0.04 12.02 0.816Adult perception of youth HIV risk* (continuous) 2.24 1.4 3.58 0.001 4.57 2.15 9.74 <0.001Pct. Knows someone in n'hood died of AIDS (continuous) 1.23 0.26 5.73 0.794 0.48 0.06 3.55 0.471Residence Mtunzini 1.00 1.00
Durban 6.99 1.94 25.2 0.003 0.67 0.32 1.41 0.286Sample size 814 1,011Log likelihood -314.735 -372.172p-value of global test <0.001 <0.001Pseudo R-squared 0.126 0.138** Higher score indicate more confident (2 items: 1. confident to get condom when needed, 2. confident in using condom correctly)*Higher score indicates increasing risk
MEASURE Evaluation 21
at risk. Females were more likely to report perception of high risk if they are older and if they
report sometimes discussing HIV at home compared to those who discussed it often and if there
had been a chronically ill household member in the past 12 months. Females were less likely to
think they were at risk if they named their mother or father as the family member they felt closest
to. Finally, residence inside the Durban metro area, compared to the more rural Mtunzini area is
a powerful predictor of boys, not engaged in high-risk behaviors, to perceive themselves at high
risk for HIV.
Discussion
South Africans are living in the midst of a terrifying epidemic. The year these data were
collected, 1999, was still relatively early in terms of how visible the epidemic was in the country.
Yet, we know from the surveillance data that this age group of 14-22 is a vital sub population at
tremendous risk of acquiring the virus. Many of the adolescents we interviewed know this fact,
but translating this first into a perception of being personally at high risk and then of altering their
own behavior require significant changes. For consistent protection there must be accurate
knowledge and extremely high access to STD treatment and condoms. For total protection there
must be abstinence from sex. Compounding all this are two other major factors; stigma against
AIDS, which may well extend into a range of behaviors that illustrate denial and fear, and the
well-established notion in developmental psychology of the feeling of invulnerability amongst
youth. Optimistic bias and stigma may reinforce each other in a complex syndrome that directly
affects young people’s calculus of their own risk. This paper only begins to examine these
factors. Much more information is required for programs to be able to help youth in South Africa
navigate this epidemic.
The results of the present analysis suggest that connectedness to parents and
community seem to play a significant role in some adolescents’ perception of their own risk.
However, feeling connected appears to have very different effects for females compared to
males. Parents seem to play an important role in helping girls feel safe by supporting them to
resist peer pressure to engage in unsafe sex or by controlling their activities and friendships so as
MEASURE Evaluation 22
to reduce the opportunities for harm. The converse, less family and community oversight, is
associated with lower risk perception for boys. It may be that in this setting, the risk and sexual
health of boys are relatively ignored compared to girls and boys are more likely to be ignorant of
or to be in denial of their own risk.
Further evidence for the importance of adult influences may be seen in the strong
positive relationship between adult perception of HIV risk from those adults (over 30) interviewed
in the street intercept community surveys, and the adolescents’ own perceptions, especially
among those who do not seem to be practicing such high-risk behavior. The strong correlation
reveals a high degree of concordance between the perceptions of adults and adolescents in
these communities. The effects of this factor are particularly large for girls, suggesting that they
may be more sensitive or more responsive to what is said in the community than boys. Another
interpretation may be that boys and girls are being given very different messages at home. For
example, girls may be being encouraged to abstain, use condoms, etc., while boys may still in
some communities have less information, or be being encouraged to have more than one
girlfriend. Other research has also identified this important gendered division in South African
communities (Varga, 1997, Varga, 1998, LeClerc-Madlala, 1997).
A number of findings reinforce how much adolescent males and females differ in factors
associated with their perception of risk. The fact that boys who are willing to have a friend who is
a PLHA are more likely to see themselves at high risk, but girls are less likely may reflect
considerable differences in the denial of illness between the genders, or it may be an artifact of
our data, i.e. that very few boys or girls said they were unwilling to have a friend who is living with
HIV or AIDS. The large coefficient predicting that boys or men living in Durban, but classified as
not at risk, are nearly seven times more likely to see themselves at high risk is an important
result. The fact that residence doesn’t appear to make a difference for girls is also important,
suggesting either that the messages of risk are being heard equally by all girls, or that boys in
Mtunzini are more likely to be in denial about their own risk.
Further, in the males not engaged in risky behavior, boys with a higher score on the self-
efficacy index in how to use a condom are significantly less likely to see themselves at high risk.
MEASURE Evaluation 23
In other words, boys who are confident in how to obtain and use a condom feel protected from
risk. However, the direction is reversed for boys who are not at risk—confidence to use a
condom is associated with a greater perception of risk; it may be that a sense of vulnerability has
spurred some boys to become adept at using this form of protection. Self efficacy in condoms
does not appear associated with risk perception in these models for girls, which probably reflects
the well established gender/power imbalance over the inability of girls to dictate condom use if
their partners are reluctant or inexperienced (Varga, 1997).
Among girls who do not report risk behaviors, living in a household with a chronically ill
member—some proportion of whom probably are affected by AIDS—seems to increase their
sense of being at risk of HIV. Adolescent females are much more likely than adolescent males to
shoulder the burden of care of an ill family member and this closeness to AIDS or another chronic
illness increases the feeling of vulnerability.
Some of the factors suggested by the literature as potentially affecting risk perception
had no relationship to reported risk in our models. For example, having experienced STD
symptoms in the past 12 months—a clear marker of high-risk behavior—had no impact on risk
perception. One reason for this is that we had a very small sample of youth reporting having
experienced an STD. Our measure of social proximity through HIV/AIDS experience—
“personally knowing someone infected with or who has died of HIV”—which we expected to act
as a predictor of risk, failed. However, because of the stigma associated with AIDS, it may also
be that the variable measuring the proximity of the epidemic through the presence of a chronically
ill member of the household is capturing this impact of the epidemic, at least for girls.
Our models did poorly in predicting risk perception among adolescents, particularly male
youth, engaged in risk behaviors. It may be that many of these adolescents are in denial or
overly optimistic about their risk and thus their reporting is not easily explained by our conceptual
models which relied on measures of knowledge, self-efficacy, and household and community
influences and supports. Moreover, admitting to being at risk of HIV means, in many people’s
minds, admitting to place oneself in the category of a stigmatized person (Malcolm et al., 1998,
UNAIDS 2000a, UNAIDS 2000b). AIDS, as acknowledged earlier, carries enormous stigma,
MEASURE Evaluation 24
related to both the fear of death and the long-held association of AIDS with sinful or illegal
behaviors. Homosexuality among many sectors of South African society is virtually a taboo
notion, while prostitution is associated both with poverty and immorality. None of these
categories are enticing, especially to adolescents still unsure of their identity. Thus, in order to
perceive oneself in a high-risk category the individual adolescent has to either overcome the
thought and image of the stigmas or perhaps to have had some other overriding shock (presence
of a household member who is chronically ill, for example).
Risk perception may also be influenced by one’s faith in oneself to predict who is a risky
partner (Dodoo and Adomako, 2002). Thus the poor predictive power of the model may be due
to omitted (and unavailable) variables for whether respondents believe they can predict who is
infected with HIV and whether their sexual partners have characteristics which are associated
with a lesser or greater likelihood of being HIV infected (e.g., look healthy or ill, fat or thin, stick to
one partner or have multiple sexual partners). The variables we included in our models, which
are not specific to a particular partnership, better predict a more generalized sense of risk for
adolescents not currently engaged in risk behaviors, most of whom are not currently in a sexual
partnership.
We hope that the results of this analysis will inform future behavior change programs in at
least two ways. First, a greater understanding of the connection of adolescents to their
communities, and to the adults in their households should be incorporated into program design.
Greater efforts could be made to involve parents and other significant adults that surround them
in the youth programs, not in a didactic role but in ways that support adolescents to examine their
own behavior, make positive changes and protect themselves. Youth programming has widely
recognized the role for peer educators but we are now beginning to increase our knowledge base
about an effective role for adult mentors. Second, the results should remind program planners
that an emphasis on the provision of information and even skills building has limits to how much it
can help an adolescent change his or her behavior. Programs must also explore how they can
alter the environments in which adolescents form opinions, make choices, and act.

MEASURE Evaluation 25
Acknowledgements
This research was made possible through support provided by the U. S. Agency for International
Development (USAID) through the HORIZONS Project (under the terms of Co-operative
agreement No. HRN-A-00-97-00012-00), the FOCUS on Young Adults Program (Co-operative
agreement No. CCP-3-73-A00-6002-00), the MEASURE Evaluation Project (Co-operative
agreement HRN-A-00-97-00018-00), and by a Rockefeller Foundation grant to the Population
Council’s Policy Research Division. The opinions expressed herein are those of the authors and
do not necessarily reflect the views of the U.S. Agency for International Development or the
Rockefeller Foundation.

MEASURE Evaluation 26
References
Abt Associates Inc--South Africa. (2000). The impending catastrophe: A Resource book on the
emerging HIV/AIDS epidemic in South Africa. Johannesburg: Report by Love Life
Programme.
Ajzen, I., and Fishbein, M. (1980). Understanding Attitudes and Predicting Social Behavior. New
Jersey: Englewood Cliffs.
Bosga, M.B., de Wit, J.B., de Vroome, E.M., Houweling, H., Schop, W., and Sandfort, T.G.
(1995). Differences in perception of risk for HIV infection with steady and non-steady
partners among homosexual men. AIDS Education & Prevention, Apr, 7(2), 103-15.
Brown, L., Macintyre, K., Stavrou, S., Kehus, C., Karim, A., and Robinson, A. (2001). Measuring
community effects on adolescent reproductive health in Kwa-Zulu Natal, South Africa.
Paper presented at the Population Association of America annual meeting, Washington
DC.
Catania, J., Kegeles, S., and Coates, T. (1990). Towards an understanding of risk behavior: an
AIDS Risk Reduction Model (ARRM). Health Education Quarterly, 17(1), 53-72.
Coates TJ 1997 Reducing high risk HIV behaviors: An overview of effective approaches. NIH
Consensus Development Conference, February 1997.
Cohen, B., and Trussell, J., editors. (1980). Preventing and Mitigating AIDS in Sub-Saharan
Africa. Washington DC: National Research Council.
Cohen, D., Spear, S., Scribner, R., Kissinger, P., Mason, K., and Wilden, J. (2000). “Broken
Windows” and the Risk of Gonorrhea. American Journal of Public Health, 90(2), 230-236. DiClemente, R. (2000). Expanding the scope of HIV prevention of adolescents: beyond individual
level interventions. Journal of Adolescent Health, 26, 377-378.
Dodoo, F., and Adomako, A. (2002). AIDS–related knowledge and behavior among married
Kenya men: A behavioral paradox? Journal of Health and Human Services
Administration, 24(2), 197-231. In Press.
Edem, C.U., and Harvey, S.M. (1995). Use of health belief model to predict condom use among
university students in Nigeria. International Journal of Community Health Education,
15(1), 3-14.
Eiser, R, 1986, Social Psychology: Attitudes, cognition and social behavior, CUP
Ellen, J.M., Boyer, C.B., Tschann, J.M., and Shaffer, M. (1996). Adolescents’ perceived risk for
STDS and HIV infection. Journal of Adolescent Health, 18, 177-181.
Farmer, P. (1991). Anthropology, accountability and the Prevention of AIDS. Journal of Sex
Research, 28(2), 203-221.
Havanon, N., Knodel, J., and Bennett, T. (1992). Sexual networking in a Provincial Thai setting.
Bangkok: AIDSCAP, Monograph series paper no 1.

MEASURE Evaluation 27
Janz N and M Becker 1984 The Health Belief Model: A decade later. Health Education Quarterly
11 (1) 1-47.Jessor, R. (1998). New Perspectives on adolescent risk behavior. United
Kingdom: Cambridge University Press.
Jessor R, MS Turbin, FM Costa, 1998, Risk and Protection in successful outcomes among
disadvantaged adolescents. Applied Development Science 2, 194-208
King, R. (1999). Sexual Behavioural Change for HIV: Where have theories taken us? Geneva:
UNAIDS.
LeClerc-Madlala S. (1997) Infect one, infect all: psychosocial response and impact of the AIDS
epidemic on Zulu youth in South Africa. Medical Anthropology 17, 363-380.
Macintyre, K., Brown, L., and Sosler, S. (2001a). It is not what you know , but who you knew:
AIDS Mortality and Behavior Change in Africa. Aids Prevention and Education, 13(2),
160-174.
Macintyre, K., Rutenberg, N., Brown, B., Magnani, R., Manzini, N., and Stavros, S. (2001b).
Social Disorganization and Condom Use among Adolescents in South Africa. Poster
presentation at the annual meeting of the Population Association of America, Washington
DC. MacPhail, C., and Campbell, C. (2001). ‘I Think Condoms Are Good but, aai, I Hate Those
Things': Condom Use among Adolescents and Young People in a Southern African
Township, June, 52(11), 1613-27.
Magnani, R.J., Karim, A., Weiss, L., Bond, K., Lemba, M., and Morgan, G. (2001). Reproductive
Health risk and protective factors among youth in Lusaka, Zambia. Journal of Adolescent
Research, 30, 76-86.
Malcolm, A.et al. (1998). HIV-related stigmatization and discrimination: Its forms and contexts.
Critical Public Health, 8(4), 347-370
Mandela Foundation/HSRC. South African National HIV Prevalence, Behavioural Risks and Mass
Media: Household Survey 2002. Cape Town: Human Sciences Research Council, 2002.
Maswanya, E.S., Moji, K., Horiguchi, I., Nagata, K., Aoyagi, K., Honda, S., and Takemoto, T.
(1999). Knowledge, risk perception of AIDS and reported sexual behavior among
students in secondary schools and colleges in Tanzania. Health Education Research,
14(2), 185-96
Montgomery, S.B., Joseph, J.G., Becker, M.H., Ostrow, D.G., Kessler, R.C., and Kirscht, J.P.
(1989). The Health Belief Model in understanding compliance with preventive
recommendations for AIDS: how useful? Aids Education and Prevention, 1(4), 303-23.
Parker, R., Easton, D., and Klein, C.H. (2000). Structural barriers and facilitators in HIV
prevention: a review of international research. AIDS, 14(Suppl 1), S22-S32.
Poppen, P., and Reisen, C.A. (1997). Perception of Risk and sexual self-protective behavior: A
methodological critique. AIDS Education and Prevention, 9, 373-90.
MEASURE Evaluation 28
Prohaska TR, G Albrecht, A Levy, N Sugrue, JH Kim, 1990, Determinants of self-perceived risk
for AIDS. Journal of Health and Social Behavior, 31(4) 384-94.
Resnick MD, P Bearman, RW Blum, 1997, Protecting adolescents from hard, JAMA 1997;
278:823-32
Rutenberg, N., Kaufman, C., Macintyre, K., Brown, L., Karim, A., and Kehus-Alons, C. (2000).
Pregnant or positive: Adolescent childbearing and HIV risk in South Africa. Paper
presented at the annual meeting of the Population Association of America, Los Angeles,
CA. Month
Rutenberg, N., Dallimore, A., and Kaufman, C. (2001). Transitions to Adulthood in the Context of
AIDS in South Africa: Report of Wave I. Washington DC: Horizons/Population Council.
Sahlu, T., Kassa, E., Agonafer, T., Tsegaye, A., Rinke de Wit, T., Gebremariam, H., Doorly, R.,
Spijkerman, I., and Fontanet, A.L. (1993). Sexual behaviors, perception of risk of HIV
infection and factors associated with attending HIV post-test counseling in Ethiopia.
AIDS, 13(10), 1263-72.
Sampson, R., Raudenbush, S., and Earls, F. (1997). Neighborhoods and Violent Crime: A
Multilevel Study of Collective Efficacy. Science, 277(5328), 918-924.
Sobo, E.J. (1995). Choosing Unsafe Sex, Aids-risk denial among disadvantaged women. Univ. of
Philadelphia.
South African Department of Health (2002). National HIV and Syphilis Sero-Prevalence Survey of
Women Attending Public Antenatal Clinics in South Africa: Summary Report. Available at:
. (downloaded 6/24/02).
Sweat, M.D., and Denison, J.A.. (1995). Reducing high-risk HIV incidence in developing countries
with structural and environmental interventions. AIDS, 9(Suppl A), S251-7.
Sweat, M.D., Nopkesorn, T., Mastro, T.D., Sangkharomya, S., MacQueen, K., Pokapanichwong,
W., Sawaengdee, Y., and Weniger, B.G . (1995). Aids awareness among a cohort of
young Thai men: exposure to information, level of knowledge and perception of risk. Aids
Care, 7(5), 573-91.
Turner, AG, Magnani, RJ, Shuaib, M.1996. “A not quite as quick alternative to the expanded
programme on immunization (EPI) cluster survey design.” International Journal of
Epidemiology. 25: 198-203.
UNAIDS. (2000a). AIDS Epidemic Update. Geneva: UNAIDS/00.44E.
UNAIDS. (2000b). HIV and AIDS-related stigmatization, discrimination and denial: forms,
contexts and determinants. UNAIDS Best Practice Collection. Geneva: UNAIDS/00.16E.
Valle, M., Levey, J., and Fax, S. (1999). Self-perception of risk for HIV among action IDU and
their at-risk sex and needle partners. Proceedings of the National HIV Prevention
Conference: Atlanta, GA.

MEASURE Evaluation 29
VanLandingham, M.J., Suprasert, S., Grandjean, N., and Sittitrai, W. (1995). Two views of risky
sexual practices among northern Thai males: the Health Belief Model and the Theory of
Reasoned Action. Journal of Health & Social Behavior. Jun 36(2), 195-212.
Varga, C. (1997) Sexual decision making and negotiation in the midst of AIDS: youth in
KwaZulu-Natal, South Africa, Health Transition Review, supplement 3 to Vol. 7, 45-67.
Varga, C. (1999) South African young people’s sexual dynamics: implications for behavioural
responses to HIV/AIDS, Resistances to Behavioural Change to Reduce HIV/AIDS
Infection, 1999, 13-34.





























