Embed Size (px)
Citation preview
"TO CORRELATE CLINICORADIOLOGICAL CHARACTERISTICS
OF BRONCHIECTASIS WITH PULMONARY HYPERTENSION"
DISSERTATION SUBMITTED TO
THE TAMIL NADU Dr. M.G.R MEDICAL UNIVERSITY, CHENNAI
IN PARTIAL FULFILLMENT OF THE REGULATIONS FOR THE
AWARD OF DEGREE OF M.D IN RESPIRATORY MEDICINE
BY
Dr.NAJMA MUHAMMED.K
GUIDE : DR.K.ANUPAMA MURTHY
DEPARTMENT OF RESPIRATORY MEDICINE
PSG INSTITUTE OF MEDICAL SCIENCES AND RESEARCH
PEELAMEDU, COIMBATORE – 641004
TAMILNADU, INDIA
"TO CORRELATE CLINICORADIOLOGICAL CHARACTERISTICS
OF BRONCHIECTASIS WITH PULMONARY HYPERTENSION"
DISSERTATION SUBMITTED TO
THE TAMIL NADU Dr. M.G.R MEDICAL UNIVERSITY, CHENNAI
IN PARTIAL FULFILLMENT OF THE REGULATIONS FOR THE
AWARD OF DEGREE OF M.D IN RESPIRATORY MEDICINE
BY
Dr.NAJMA MUHAMMED.K
GUIDE : DR.K.ANUPAMA MURTHY
DEPARTMENT OF RESPIRATORY MEDICINE
PSG INSTITUTE OF MEDICAL SCIENCES AND RESEARCH
PEELAMEDU, COIMBATORE – 641004
TAMILNADU, INDIA
"TO CORRELATE CLINICORADIOLOGICAL CHARACTERISTICS
OF BRONCHIECTASIS WITH PULMONARY HYPERTENSION"
DISSERTATION SUBMITTED TO
THE TAMIL NADU Dr. M.G.R MEDICAL UNIVERSITY, CHENNAI
IN PARTIAL FULFILLMENT OF THE REGULATIONS FOR THE
AWARD OF DEGREE OF M.D IN RESPIRATORY MEDICINE.
BY
Dr.NAJMA MUHAMMED.K
GUIDE : DR.K.ANUPAMA MURTHY
DEPARTMENT OF RESPIRATORY MEDICINE
PSG INSTITIUTE OF MEDICAL SCIENCES AND RESEASRCH
PEELAMEDU, COIMBATORE – 641004
TAMILNADU, INDIA
CERTIFICATE
This is to certify that the thesis entitled “TO CORRELATE
CLINICORADIOLOGICAL CHARACTERISTICS OF BRONCHIECTASIS
WITH PULMONARY HYPERTENSION” is a bonafide work of
DR.NAJMA MUHAMMED.K done under the guidance and supervision of
DR.ANUPAMA MURTHY MD(CHEST) in the Department of PSG Institute
of Medical Sciences and Research, Coimbatore in fulfilment of the regulations
of Dr.MGR Medical University for award of M.D .Degree in Tuberculosis and
Respiratory Diseases.
DR.K.ANUPAMA MURTHY
Professor & Head
Department of Respiratory Medicine
DR.RAMALINGAM
DEAN
DECLARATION
I hereby declare that this study dissertation entitled “TO CORRELATE
CLINICORADIOLOGICAL CHARACTERISTICS OF BRONCHIECTASIS
WITH PULMONARY HYPERTENSION” was prepared by me under the direct
guidance and supervision of Professor of Respiratory Medicine,
DR.K.ANUPAMA MURTHY, MD (CHEST),PSG Institute of Medical
Sciences & Research, Coimbatore.
This dissertation is submitted to the Tamil Nadu Dr.MGR Medical
University in fulfilment of the University regulations for the award of M.D.
Degree in Tuberculosis and Respiratory Diseases. This dissertation has not
been submitted for the award of any other Degree or Diploma.
DR.NAJMA MUHAMMED.K
CERTIFICATE BY GUIDE
This to certify that the thesis entitled “TO CORRELATE
CLINICORADIOLOGICAL CHARACTERISTICS OF BRONCHIECTASIS
WITH PULMONARY HYPERTENSION” is a bonafide work of
DR.NAJMA MUHAMMED done under my direct guidance and supervision in
the Department of Respiratory medicine, PSG Institute of Medical Sciences
and Research, Coimbatore in fulfilment of the regulations of DR.MGR Medical
University for the award of M.D .Degree in Tuberculosis and Chest Diseases.
DR.K.ANUPAMA MURTHY
Professor & Head
Department of Respiratory Medicine
ACKNOWLEDGEMENT
I shall forever remain indebted to my beloved teachers,
Dr.K.Anupama Murthy, Dr.Karthikeyan Ramaraju for their constant valuable
inputs guidance, patients support without which thesis would have been
impossible
A special mention to the Radiology and Cardiology departments for
their unyielding support and providing a good number of cases for this study. I
take this opportunity to thank all the above mentioned departments
Finally I thank all my patients, who cooperated at every step and
provided me the opportunity to conduct the study.
Thank you
Dr.Najma Muhammed.K
PLAGIARISM CERTIFICATE
This is to certify that this dissertation work titled “ TO
CORRELATE CLINICORADIOLOGICAL CHARACTERISTICS OF
BRONCHIECTASIS WITH PULMONARY HYPERTENSION” of the
candidate Dr. Najma Muhammed. K with registration number
201527151 for the award of MD in the branch of RESPIRATORY
MEDICINE. I personally verified the urkund.com website for the
purpose of Plagiarism check. I found that the uploaded thesis file
contains introduction to conclusion pages and result shows 7% of
plagiarism in the dissertation.
Signature of the guide

CONTENTS
SL.NO CONTENTS PAGE NO
1 INTRODUCTION 1-12
2 AIMS AND OBJECTIVES 13
3 MATERIALS AND METHODS 14-16
4 REVIEW OF LITERATURE 17-51
5 RESULTS 52-62
6 DISCUSSION 63-74
7 SUMMARY 75
8 LIMITATION 76
9 CONCLUSION 77
10 BIBLIOGRAPHY
11 ANNEXURE
I) ABBREVIATIONS
II) CONSENT FORM
III) PATIENTS INFORMATION FORM
IV) MASTER CHART
1
INTRODUCTION
Bronchiectasis is one of the most prevalent morbidity in any community
leading to recurrent lower respiratory tract infections. Bronchiectasis means
abnormal and permanent dilation of medium sized subsegmental bronchi from
fourth to ninth generations. First described by Laennec in 1819,Later by Sir
William Osler,late by 1800 and futher defined by Reid in 1950.Bronchiectasis
usually associated with mucosal thickening, mucus plugging and avariable
degree of hyperinflation of lung. Bronchiectasis is associated with common
and rare disease, which impact of muciliary clearance and immunity. Mucus
clearance and local defence mechanisms aganist microorganisms are important
in preventing recurrent pulmonary infection.Repeated infection causes damage
and impedes the clearance of mucus.The airway dilatation and impairement of
mucociliary clearance increases suspectibility for repeated infection in
lungs,resulting in chronic infection.The abnormal airway anatomy ,chronic
infection and mucus retension result in decline in respiratory function.
Bronchiectasis may be congenital or acquired. Pathogenesis has not
been well defined. The combination of a microbial insult and defect in host
defence may result in persistent bronchial infection and inflammation which
leads to further structures to prolonged infection,result in lung damage. Other
pathogenesis includes obstructive either intraluminal or extraluminal,
inflammatory conditions, immunological changes.Autoimmune disease also
have some association in pathogenesis of bronchiectasis. The prevalence of
2
bronchiectasis is 5-7 times greater in persons over 55years of age. In Indian
adult it is third commonest non –tubercular respiratory disease with the
incidence of 71per lakh.
PULMONARY HYPERTENSION
Pulmonary Hypertension is a common complication in chronic lung
disease. Most revised classification of pulmonary hypertension,chronic lung
disease or conditions with alveolar hypoxia are included in WHO Group III of
PH –related disease. In this category of chronic lung disease of a mixed
obstructive and restrictive pattern,which includes chronic bronchiectasis, cystic
fibrosis and syndrome characterized by combination of pulmonary fibrosis and
emphysema ,in which the prevalence of PH is almost 50%. Prevelance in India
of bronchiectasis with pulmonary hypertension 1% in occupational airway
disease,15% in Chronic obstructive pulmonary disease,2% in Obliterative
bronchiolitis.Global prevalence in bronchiectasis of pulmonary hypertension is
7-12%.
Alveolar hypoxia is major factor for pulmonary vasoconstriction.
Endothelial level is one of the most important leading pathway for
development of PH in chronic lung disease. Alveolar hypoventilation increases
acute pulmonary vasoconstriction and vasodilation causes physiological shunt.
Hypoxia causes pulmonary vasoconstriction leads to increase pulmonary
vascular resistance. Vasoconstriction is achieved through activation of
3
vasoconstrictor pathway or inactivation of a vasodilator pathway, or through
the effects of hypoxia on vascular smooth muscle.
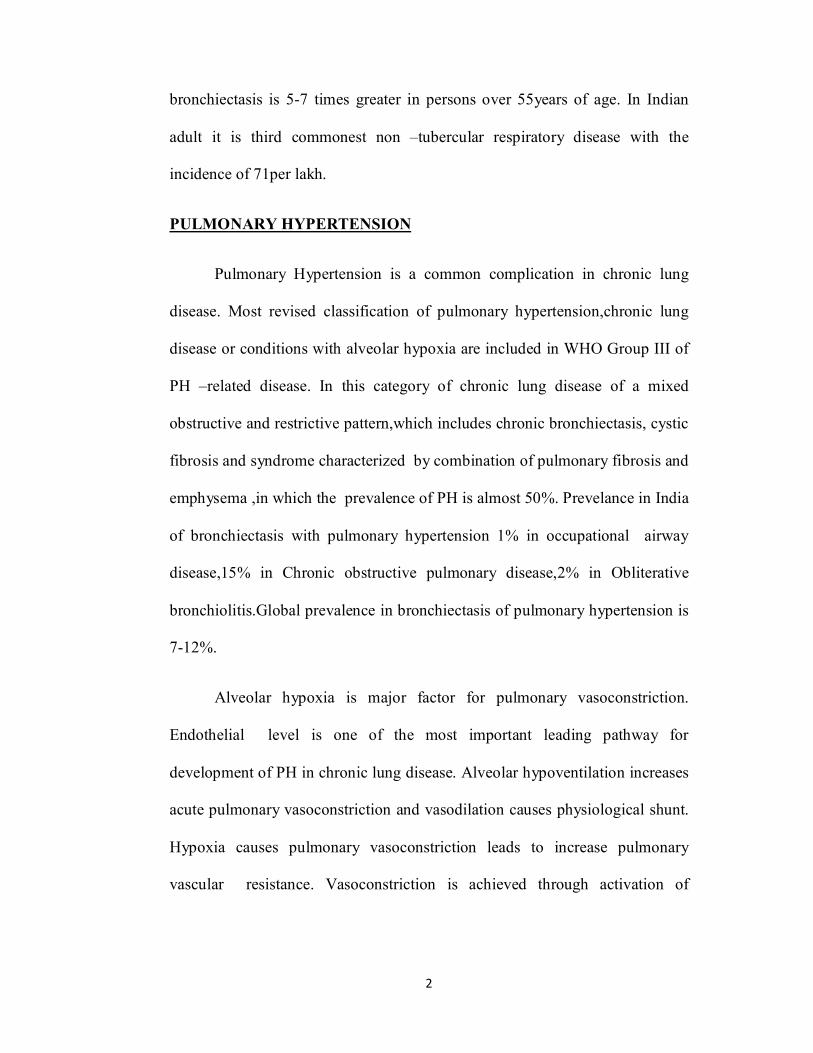
Figure : 1 Chest radiograph showing markedly dilated pulmonary arteries
(arrows).
4
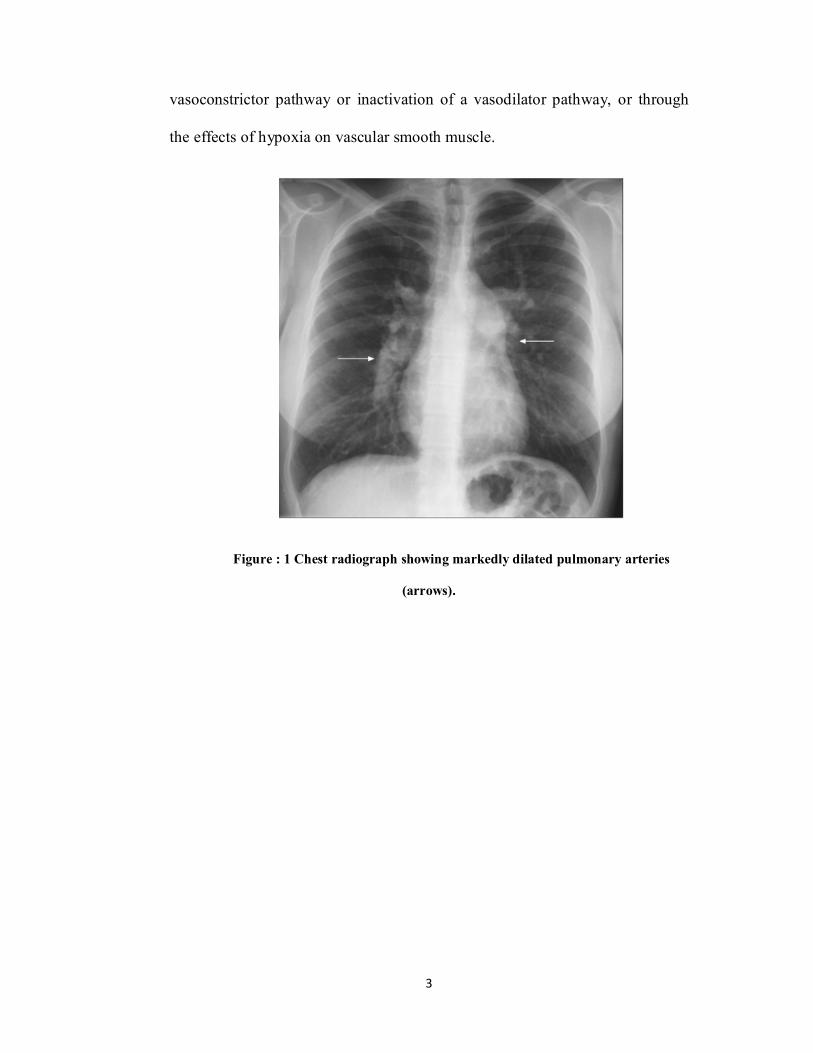
Figure 2 : Contrast-enhanced computed tomography of the chest of a patient with
pulmonary arterial hypertension associated with congenital heart disease (large atrial
septal defect). Massive dilatation of the pulmonary arterial trunk and branches (#). The
ratio of the diameter of aorta (Ao) to the diameter of main pulmonary artery
(PA) is >1.5.
5
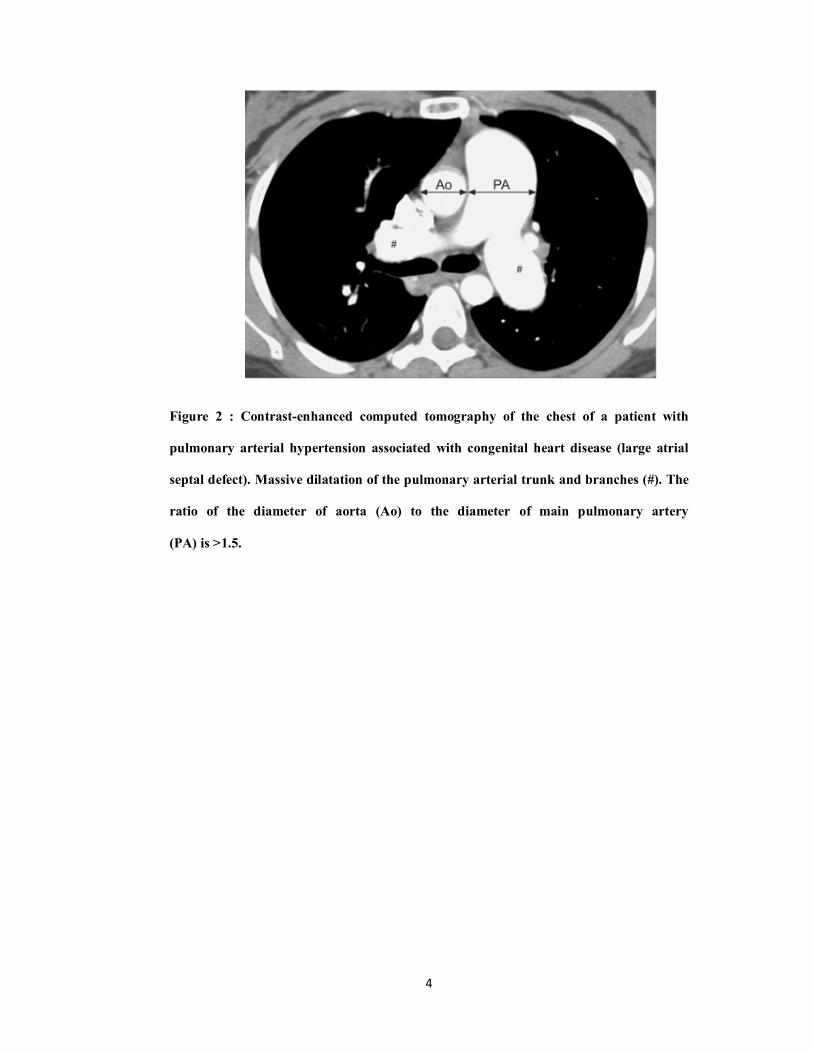
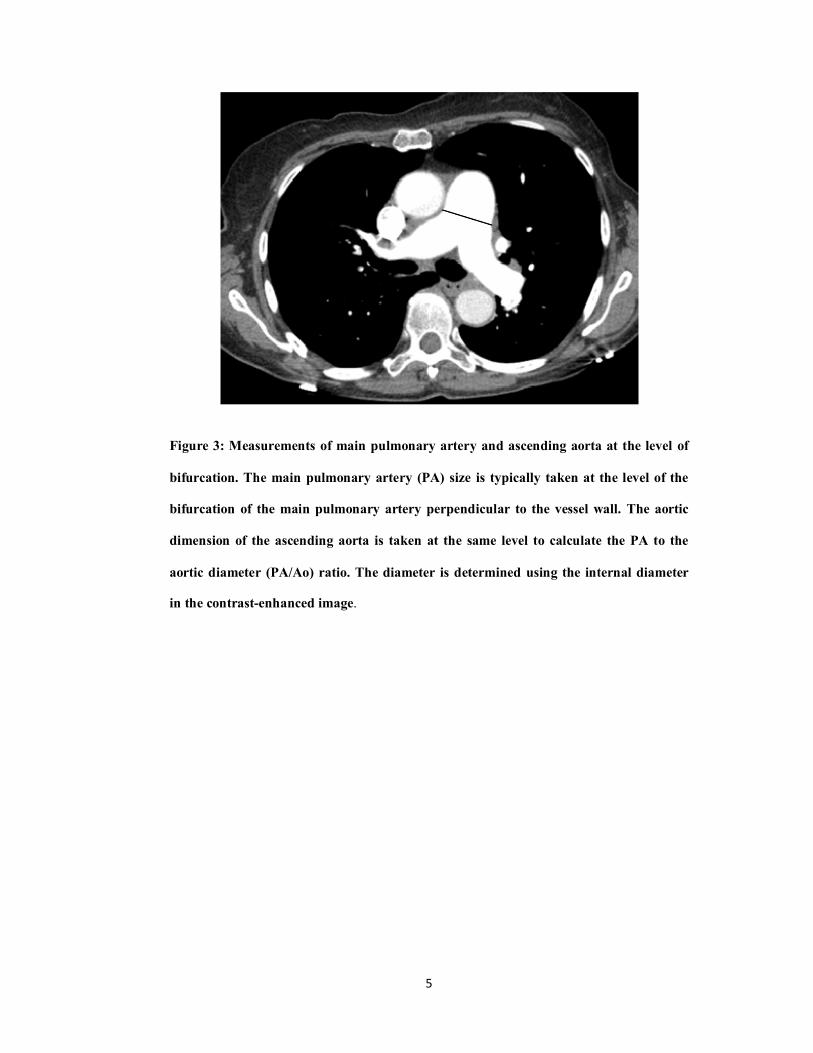
Figure 3: Measurements of main pulmonary artery and ascending aorta at the level of
bifurcation. The main pulmonary artery (PA) size is typically taken at the level of the
bifurcation of the main pulmonary artery perpendicular to the vessel wall. The aortic
dimension of the ascending aorta is taken at the same level to calculate the PA to the
aortic diameter (PA/Ao) ratio. The diameter is determined using the internal diameter
in the contrast-enhanced image.
6
Chest radiography is not sensitive for the diagnosis of airway disease.In
most severe cases of patients with bronchiectasis,as dilation of large airways
which can be visualized . High –resolution computed tomography is more
sensitive test than chest radiography and is useful in diagnosis of airway
disease. The test is considered as gold standard for diagnosing bronchiectasis.
Greater variance in section thickness compared to HRCT sections obtained
only at 10mm intervals,leads to improve the detection of bronchiectasis. HRCT
technique compromises scanning for apex to base with 1-2mm cuts at 10mm
intervals.
Common finding in bronchiectasis include bronchial wall
thickening,centrilobular nodules mosaic attenuation by air trapping. Following
tomographic criteria are used for diagnosis of CT bronchiectasis
1) Bronchial internal diameter larger than 1.5times the diameter of adjacent
pulmonary artery
2) Bronchial visualization in the periphery 1-2cm from the paritel pleura
7
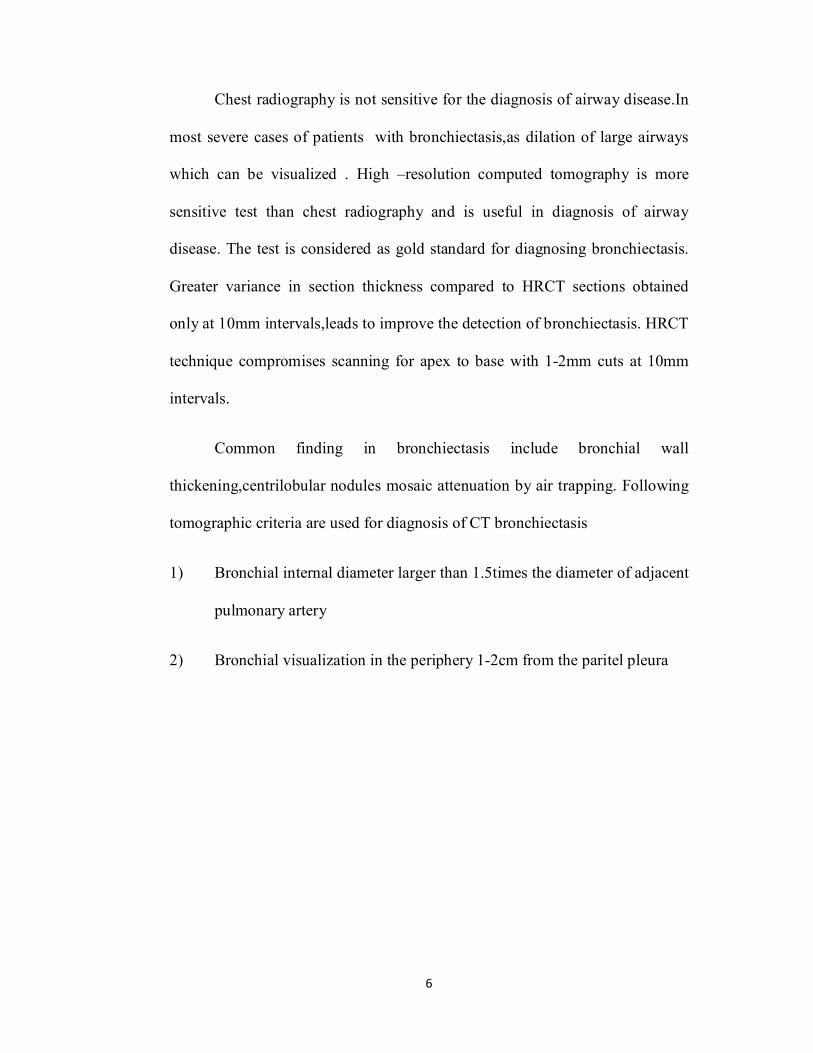
Figure 4: shows normal lung (right), bronchiectasis lung (left)
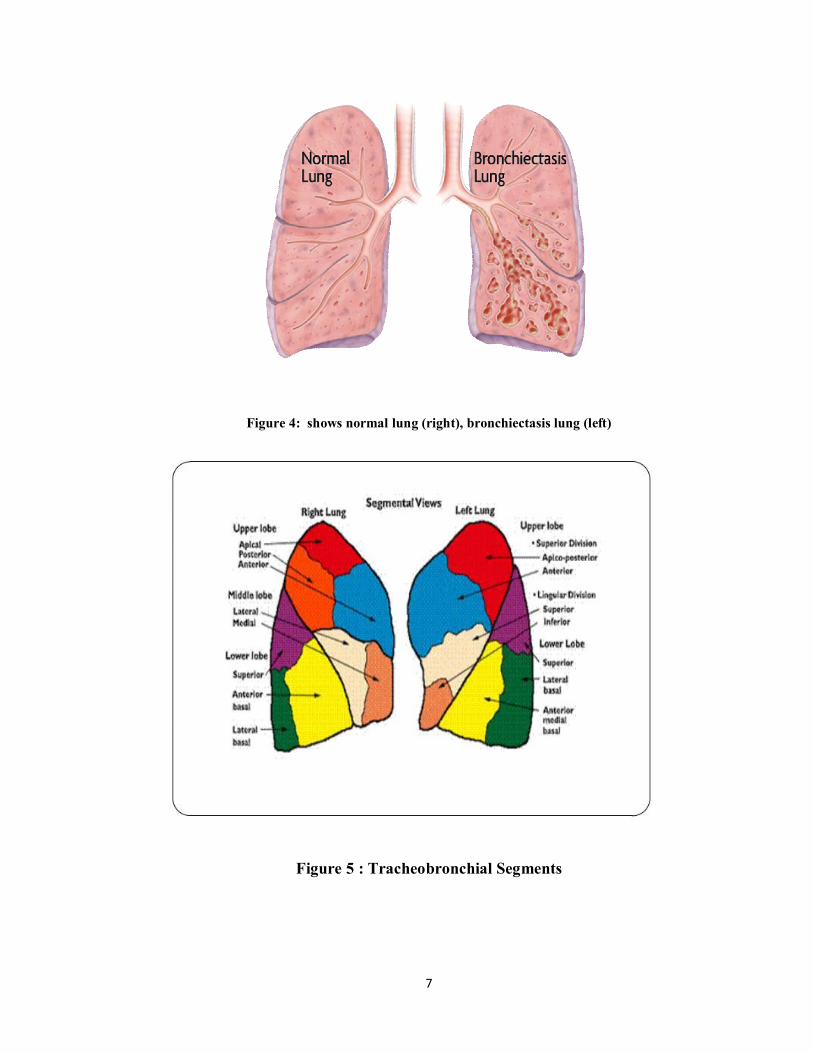
Figure 5 : Tracheobronchial Segments
8
TRACHEOBRONCHIAL TREE ANATOMY
Trachea divides into right- and left- primary main bronchi.
Each further divides into lobar bronchi which in turn give rise to segmental
bronchi - supply air to bronchopulmonary segments.
Segmental bronchi divide dichotomously, eventually giving rise to terminal
bronchioles which further terminates into respiratory bronchioles.
Originating from each respiratory bronchioles are 2-11 alveolar ducts leading
to the alveolar sacs which are extended as a group of alveoli.
Airway becomes progressively narrower, shorter and more numerous, and
Cross sectional area, enlarges.
Areas of tracheobronchial tree furthest from the trachea are collectively called
the "distal respiratory tree"
RIGHT MAIN BRONCHUS :
The right main bronchus is 2 cm long on average and has an internal diameter
of 10-16 mm. This is slightly larger than the diameter of the left main
bronchus.
The bronchus intermedius of the right bronchial tree is actually quite short ,
extending for 1.0-2.5 cm until its anterior wall extends into and becomes the
middle lobe bronchus. Its posterior wall extends into and becomes the right
lower lobe bronchus.
9
Volume loss caused by pleural effusion, atelectasis, elevated right
hemidiaphragm, as well as traction or torsion from a fibrotic or scarred upper
lobe often cause shortening of this bronchus.
The RIGHT UPPER LOBE BRONCHUS Right upper lobe bronchus divides into
a. The apical bronchus
b. The anterior bronchus
c. The posterior bronchus
Distally just beyond the bronchus intermedius, another division occurs into :
The middle lobe bronchus with its anterior direction, dividing into
a) medial and b) lateral segmental bronchus
RIGHT LOWER LOBE BRONCHUS
The right lower lobe bronchus divides immediately into
a) Superior segmental bronchus (just across from the right middle
lobebronchus), and
b) Medial basal segmental bronchus a bit more distally and along its
medial wall.
10
Finally dividing into three lower lobe bronchi
(Three musketeers):
c) Antero-basal
d) Latero-basal
e).Postero-basal
LEFT MAIN BRONCHUS
The left main bronchus is usually 4-5cm long (Right. 2cm long). Its lumen is
narrower and relatively horizontal. The usual length of the left
lower lobe bronchus beyond the origin of the superior segmental bronchus is
1cm.
Divides into upper and lower lobe bronchus.
Left upper lobe bronchus divides into apicoposterior and anterior.
Lingular – supr division, inferior division.
Left Lower lobe bronchus divides into apical,anterior basal, posterior basal,
lateral basal segments.
11
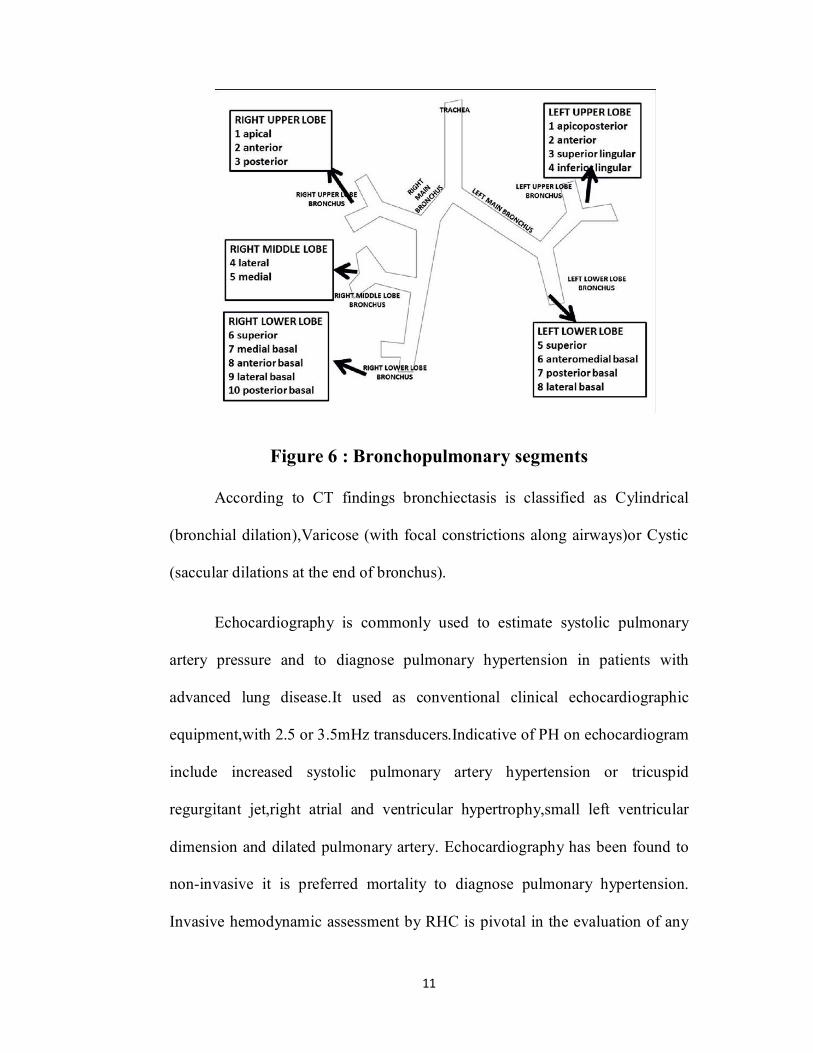
Figure 6 : Bronchopulmonary segments
According to CT findings bronchiectasis is classified as Cylindrical
(bronchial dilation),Varicose (with focal constrictions along airways)or Cystic
(saccular dilations at the end of bronchus).
Echocardiography is commonly used to estimate systolic pulmonary
artery pressure and to diagnose pulmonary hypertension in patients with
advanced lung disease.It used as conventional clinical echocardiographic
equipment,with 2.5 or 3.5mHz transducers.Indicative of PH on echocardiogram
include increased systolic pulmonary artery hypertension or tricuspid
regurgitant jet,right atrial and ventricular hypertrophy,small left ventricular
dimension and dilated pulmonary artery. Echocardiography has been found to
non-invasive it is preferred mortality to diagnose pulmonary hypertension.
Invasive hemodynamic assessment by RHC is pivotal in the evaluation of any
12
patient with suspected PAH. Right –Heart catherization is typically performed
after the non invasive testing for PH.
Physiological parameters such as pulmonary function test that are
characteristic of an obstructive disorder, confirming initial involvement of
small airways. With progression of disease, a mixed functional disorder or a
restrictive disorder can be found due to progressive destruction of pulmonary
parenchyma that is characterised by recurrent infectious exacerbations and
massive destruction of the small airways. 6-minute walk test enabling the
evaluation of the degree of respiratory discomfort, in terms of determination of
subjective rates according to the perfection of individual. This a vertical scale
to quatify from 0-10 in which 0 represents no symptoms, and 10 represents
maximum symptoms and providing an providing individual measurement of
the density of the exercise.
In conclusion high –resolution CT scan can be used for diagnosis extend
of involvement of segments of bronchiectasis. So predictors of clinical,
physiological and radiological correlation in patients with bronchiectasis will
help to determine predictors of pulmonary hypertension.
13
AIMS & OBJECTIVES
To correlate clinicoradiological characteristics of bronchiectasis with
pulmonary hypertension
OBJECTIVE
Primary Objective
To correlate clinicoradiological profile of bronchiectasis
Secondary Objective
To correlate clinicoradiological profile of bronchiectasis with severity of
pulmonary hypertension
To correlate clinicoradiological profile with physiological charecteristics of
bronchiectasis
14
MATERIALS AND METHODS
The study aim to correlate the clinicoradiological parameters of
bronchiectasis,and to assess the severity of exercise capacity and Pulmonary
Artery Hypertension in these patients.Clinical and radiological predictors will
facilitate futher understanding of pulmonary atery hypertension and thereby
affect treatment outcomes.
Study type
Prospective cross-sectional study
Study Duration
12months
Study Locale
PSG Institute of Medical Sciences and Research
Study Method
Convenience Sampling
Sample Size
40subjects
15
Inclusion Criteria
Age 18 to 65 years
Cases of Bronchiectasis diagnosed based on clinico radiological profile
Willing to participate in the study adhering to its protocol
Exclusion Criteria
Patients not having acute exacerbation or active infection
Patients with Primary PulmonaryHypertension(PPH)
Patients with pulmonary hypertension attributable to primary causes other than
bronchiectasis
Mental status not competent enough to consent for the study in the study
adhering to its protocol
16
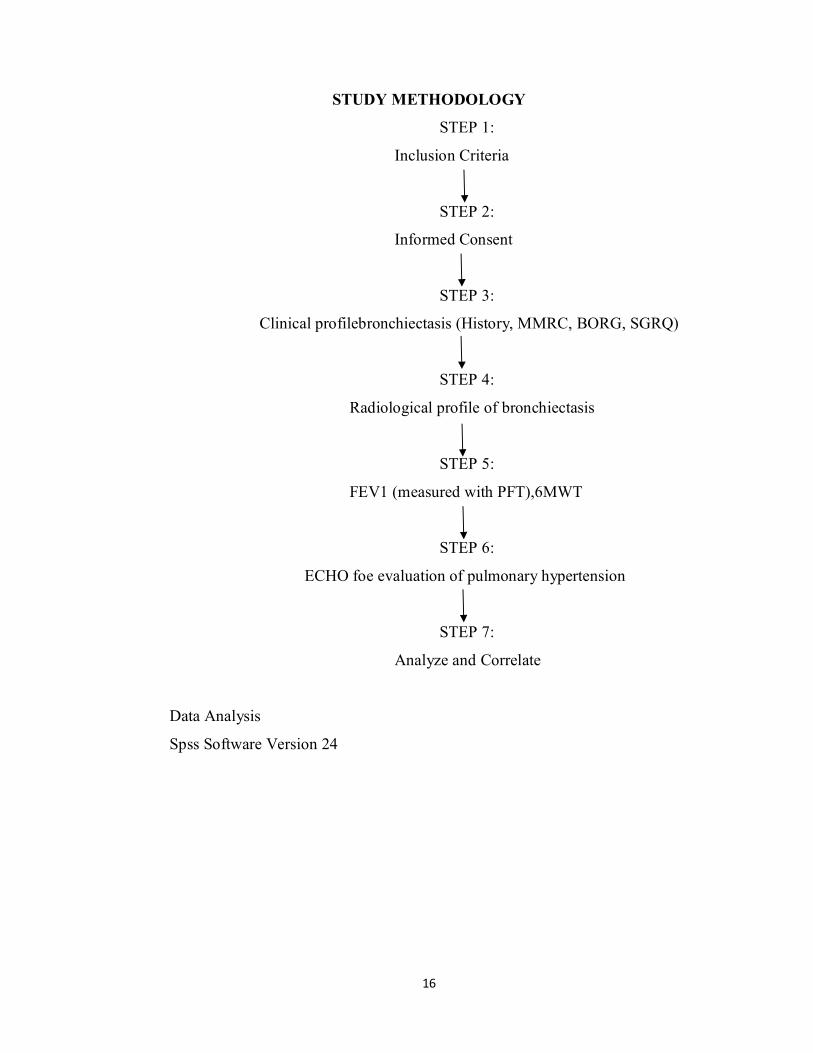
STUDY METHODOLOGY
STEP 1:
Inclusion Criteria
STEP 2:
Informed Consent
STEP 3:
Clinical profilebronchiectasis (History, MMRC, BORG, SGRQ)
STEP 4:
Radiological profile of bronchiectasis
STEP 5:
FEV1 (measured with PFT),6MWT
STEP 6:
ECHO foe evaluation of pulmonary hypertension
STEP 7:
Analyze and Correlate
Data Analysis
Spss Software Version 24
17
REVIEW OF LITERATURE
Bronchiectasis is an important cause of respiratory morbidity but it has
generally a low profile. As it is a heterogeneous condition with a large number
of predisposing factors, long clinical history, the pathogenesis has not been
well defined. Bronchiectasis is defined as permanent and abnormal dilatation of
bronchi(1).In 1953,1.3 cases of bronchiectasis were reported in Bedford, a
similar prevalence of 1.5 cases per 1000 was found from the chest radiographs
obtained from routine miniature chest radiographs obtained from England and
Wales in 1956 during tuberculosis eradication campaign. It is described as
common in developing nations, but there is a lack of data on the actual
prevalence. Generally ,bronchiectasis appears to be more common in females,
with approximately two -thirds of patients in studies.
Most studies of bronchiectasis pathology were performed between 1920
and 1960,when there was readily available access to surgical and post mortem
tissue. Bronchiectasis was characteristed by dilatation of subsegmental airways,
which were tortuous, inflamed and obstructed by secretions. There was
generally damage to the bronchioles, often with associated fibrosis and
parenchymal destruction. The vascular supply to affected areas was derived
mainly from hypertrophy of bronchial arteries and their anastomoses with
pulmonary arteries.
18
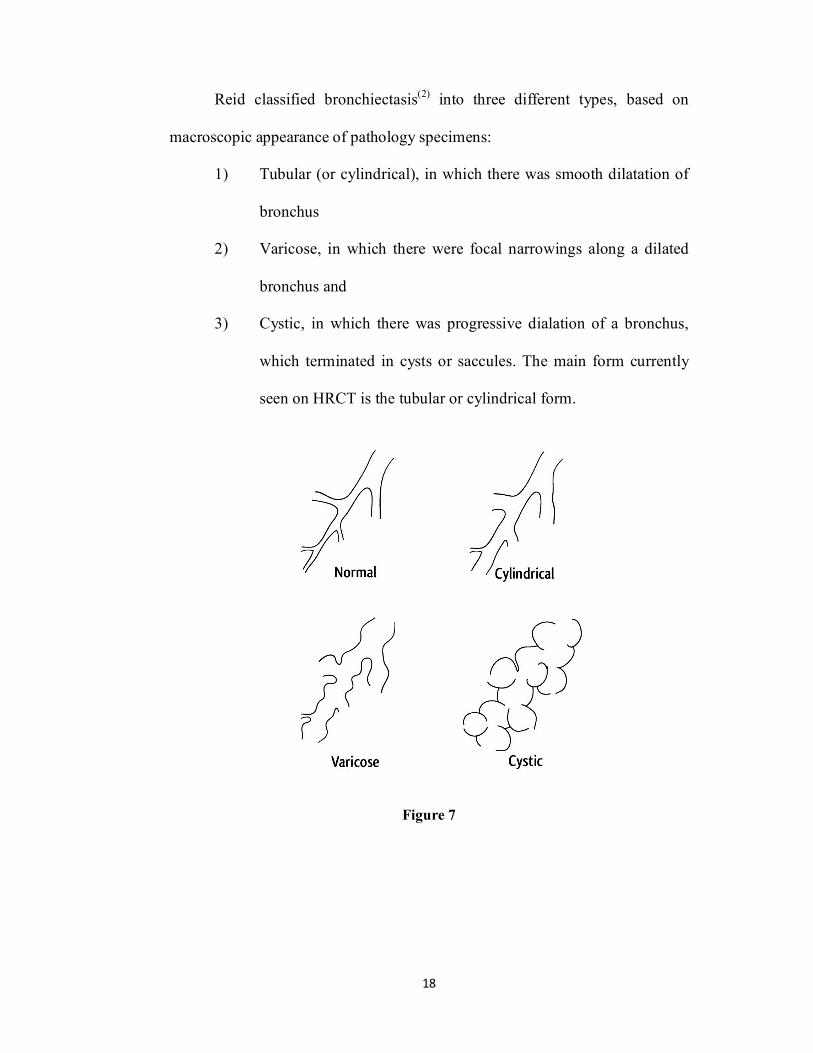
Reid classified bronchiectasis(2) into three different types, based on
macroscopic appearance of pathology specimens:
1) Tubular (or cylindrical), in which there was smooth dilatation of
bronchus
2) Varicose, in which there were focal narrowings along a dilated
bronchus and
3) Cystic, in which there was progressive dialation of a bronchus,
which terminated in cysts or saccules. The main form currently
seen on HRCT is the tubular or cylindrical form.
Figure 7
19
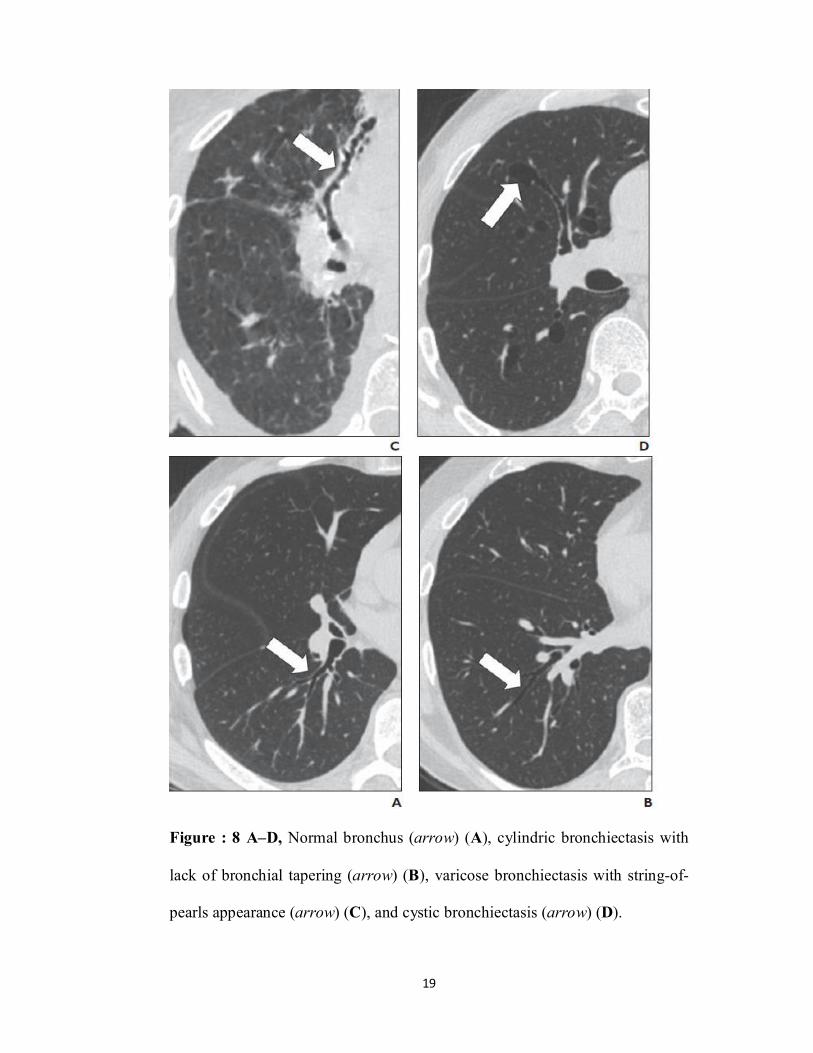
Figure : 8 A–D, Normal bronchus (arrow) (A), cylindric bronchiectasis with
lack of bronchial tapering (arrow) (B), varicose bronchiectasis with string-of-
pearls appearance (arrow) (C), and cystic bronchiectasis (arrow) (D).
20
Most definitive pathology study was performed by Whitwell(3) in a
study “pathology and pathogenesis” in 1952 also described . He studied 200
operative lung samples from patients with bronchiectasis. He described the
bronchial wall to be infiltrated with inflammatory cells. Ciliated epithelium
was often replaced with squamous or columnar epithelium. The elastin layer
was deficient or absent and, in more severe cases, there was destruction of
muscle and cartilage, theses changes were responsible for bronchodilation.
He described three main forms of bronchiectasis:
1) Follicular 2) Saccular 3) Atelectactic.
1) Follicular bronchiectasis is acquired, it forms in presence of numerous
lymphoid follicles situated in thickened,usually cylindrically dialated
bronchial walls.
2) Saccular bronchiectasis characterised by presence of macroscopically
visible thin walled, saccular bronchial dilations.
3) Atelectatic bronchiectasis , it was predominantly right-sided with
follicular and saccular bronchiectasis, which involved the left lung
more commonly.
.
21
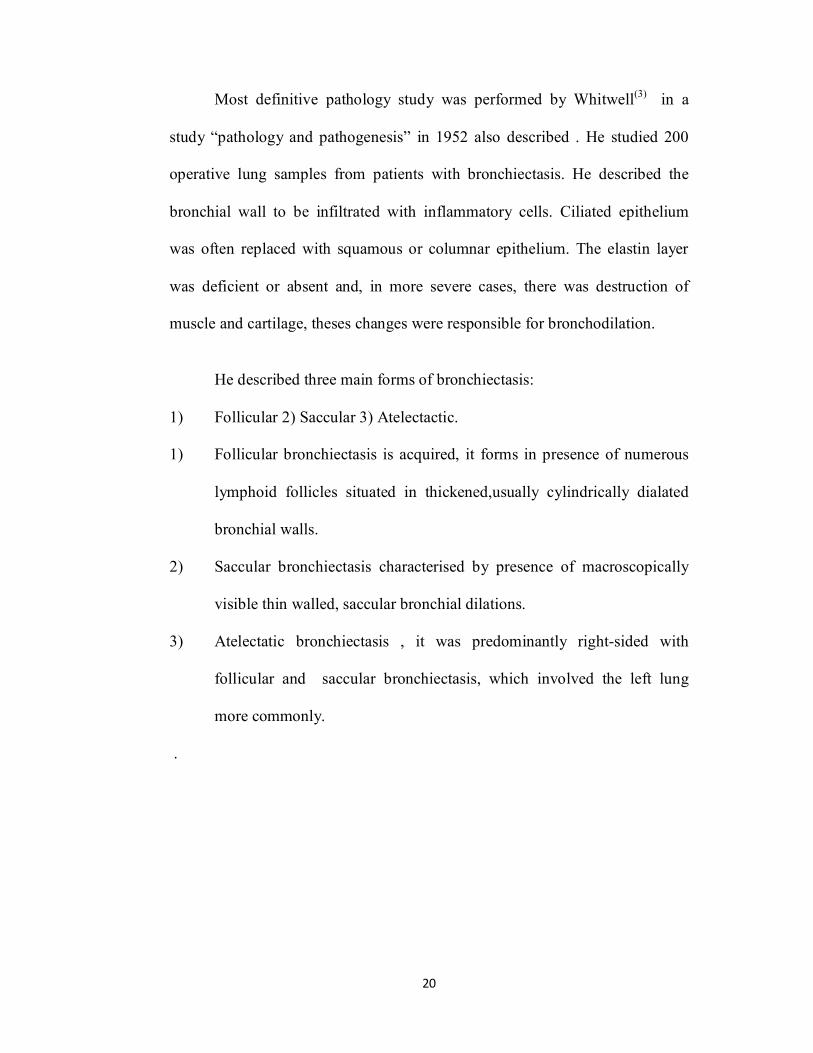
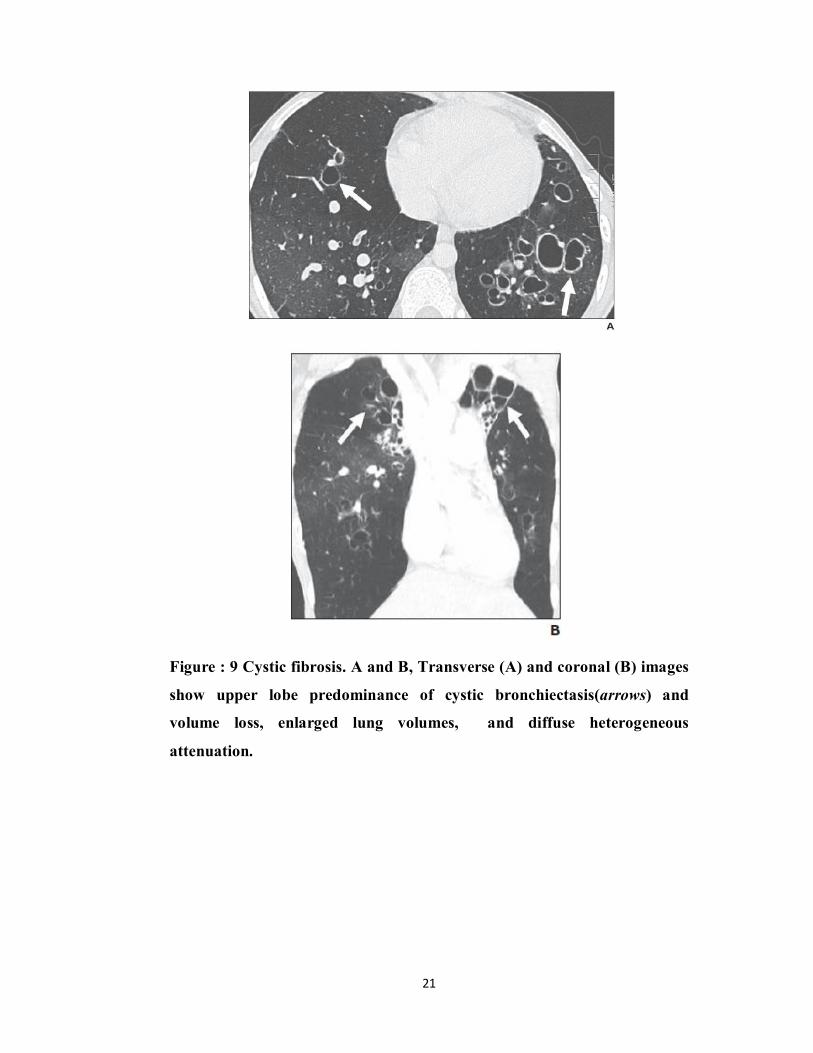
Figure : 9 Cystic fibrosis. A and B, Transverse (A) and coronal (B) images
show upper lobe predominance of cystic bronchiectasis(arrows) and
volume loss, enlarged lung volumes, and diffuse heterogeneous
attenuation.
22
Pathophysiology of Bronchiectasis
The dominant feature of bronchiectasis is airway inflammation in
association with bacterial infection. It has generally been thought that the
inflammation is secondary to unclearing infection. The “vicious cycle
hypothesis” was proposed by Cole at al(4) explain the development of
bronchiectasis. It compromised mucociliary clearance, allowing infection and
colonisation of the respiratory tract. Bacteria caused inflammation, which
damaged the respiratory tract, leading to more bacterial proliferation and more
inflammation or damage. Thus ongoing cycle developed which caused
progressive destruction of the lung. The current view is that a combination of
microbial insult and defect in host defence allow establishment of persistent
bronchial infection.
23
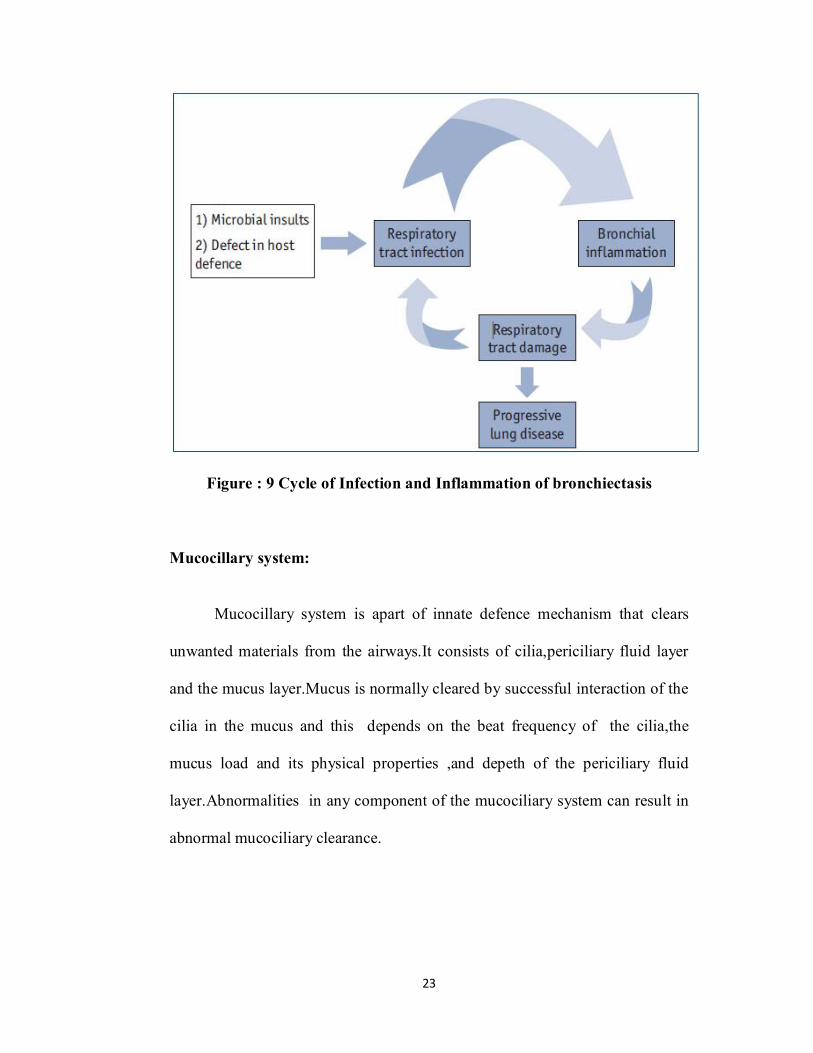
Figure : 9 Cycle of Infection and Inflammation of bronchiectasis
Mucocillary system:
Mucocillary system is apart of innate defence mechanism that clears
unwanted materials from the airways.It consists of cilia,periciliary fluid layer
and the mucus layer.Mucus is normally cleared by successful interaction of the
cilia in the mucus and this depends on the beat frequency of the cilia,the
mucus load and its physical properties ,and depeth of the periciliary fluid
layer.Abnormalities in any component of the mucociliary system can result in
abnormal mucociliary clearance.
24
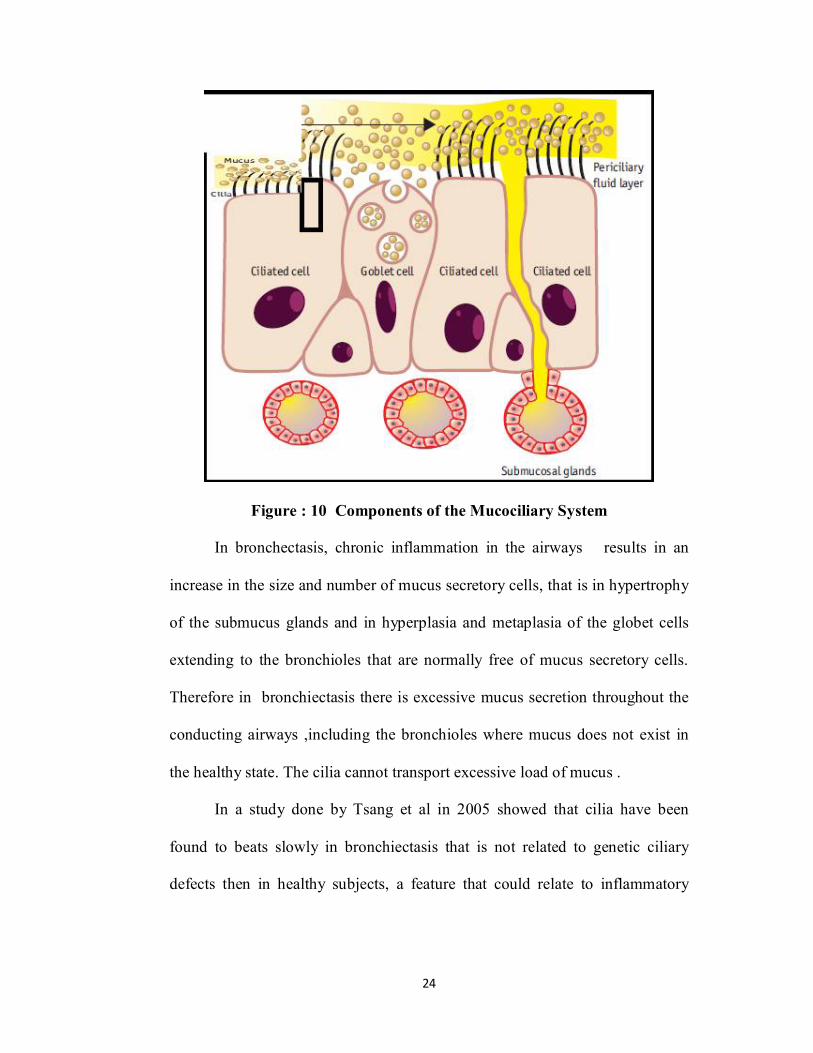
Figure : 10 Components of the Mucociliary System
In bronchectasis, chronic inflammation in the airways results in an
increase in the size and number of mucus secretory cells, that is in hypertrophy
of the submucus glands and in hyperplasia and metaplasia of the globet cells
extending to the bronchioles that are normally free of mucus secretory cells.
Therefore in bronchiectasis there is excessive mucus secretion throughout the
conducting airways ,including the bronchioles where mucus does not exist in
the healthy state. The cilia cannot transport excessive load of mucus .
In a study done by Tsang et al in 2005 showed that cilia have been
found to beats slowly in bronchiectasis that is not related to genetic ciliary
defects then in healthy subjects, a feature that could relate to inflammatory
25
products such as neutrophil elastase or to bacterial products especially in those
colonized with pseudomonas.
Mucus in bronchiectasis can be highly viscoelastic and adhesive. These
physical properties are greatly influenced by the hydration at the airway
surface. Then the secreted mucus volume is excessive as bronchiectasis there
is an imbalance between mucins and available water. Daviskas et al and
Boucher et al studies showed that dehydration of airway mucus in
bronchiectasis is evident when the percentage of solids in sputum is greater
than the normal 2-3% .The increase in the percentage of solids in the mucus of
bronchiectasis patients in addition to causing impairement to its transport can
potentially inhibit the motility of neutrophilis within the mucus and thus their
ability to kill bacteria. When the solids where increased from normal 2.5% to
6.5%,neutrophilis failed to kill bacteria.
The increased production of mucus in bronchiectasis together with the
impairement of the mucociliary system leads to accumulation of mucus,
chronic cough, mucus plug formation, airway obstruction, bacterial
colonization and infections that fails to resolve completely. In bronchiectasis
,the failure of mucociliary system to transport mucus most likely relates to the
abnormal load of mucus and the abnormal physical properties of the mucus
rather that to the cilia or their movement being abnormal, except in patients
with genetic ciliary defects. When the mucociliary system fails cough becomes
a every important mechanism for clearing mucus. Cough become compromised
26
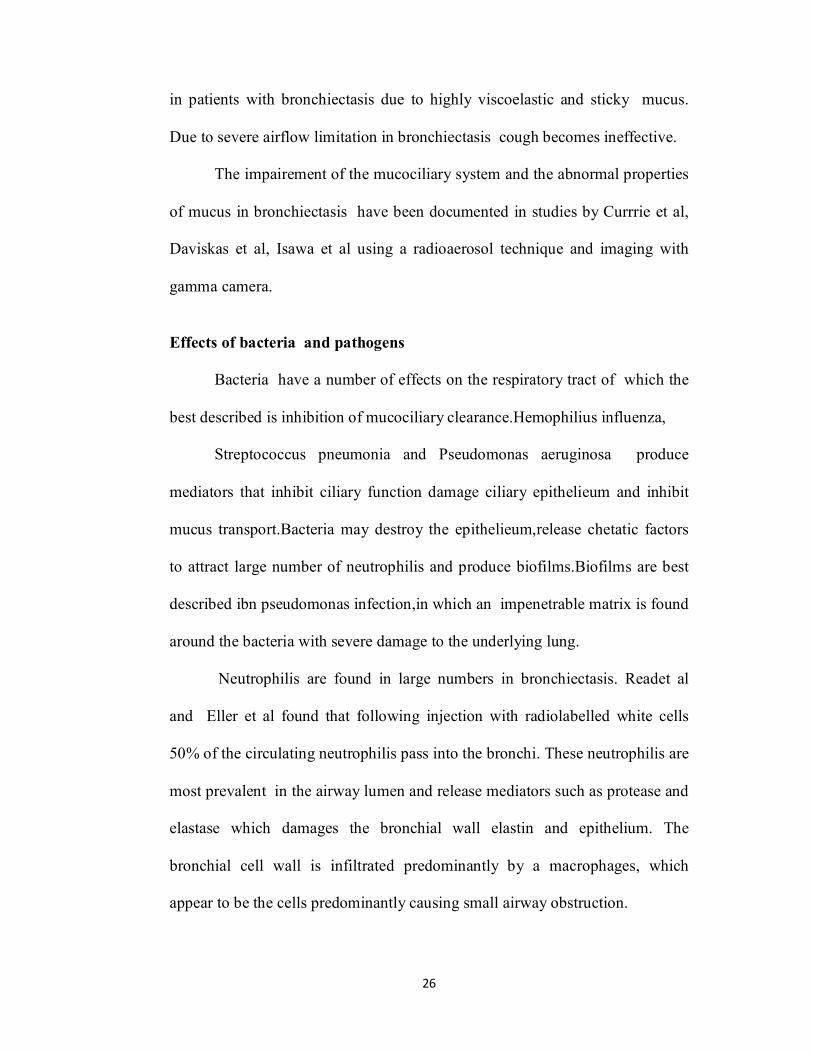
in patients with bronchiectasis due to highly viscoelastic and sticky mucus.
Due to severe airflow limitation in bronchiectasis cough becomes ineffective.
The impairement of the mucociliary system and the abnormal properties
of mucus in bronchiectasis have been documented in studies by Currrie et al,
Daviskas et al, Isawa et al using a radioaerosol technique and imaging with
gamma camera.
Effects of bacteria and pathogens
Bacteria have a number of effects on the respiratory tract of which the
best described is inhibition of mucociliary clearance.Hemophilius influenza,
Streptococcus pneumonia and Pseudomonas aeruginosa produce
mediators that inhibit ciliary function damage ciliary epithelieum and inhibit
mucus transport.Bacteria may destroy the epithelieum,release chetatic factors
to attract large number of neutrophilis and produce biofilms.Biofilms are best
described ibn pseudomonas infection,in which an impenetrable matrix is found
around the bacteria with severe damage to the underlying lung.
Neutrophilis are found in large numbers in bronchiectasis. Readet al
and Eller et al found that following injection with radiolabelled white cells
50% of the circulating neutrophilis pass into the bronchi. These neutrophilis are
most prevalent in the airway lumen and release mediators such as protease and
elastase which damages the bronchial wall elastin and epithelium. The
bronchial cell wall is infiltrated predominantly by a macrophages, which
appear to be the cells predominantly causing small airway obstruction.
27
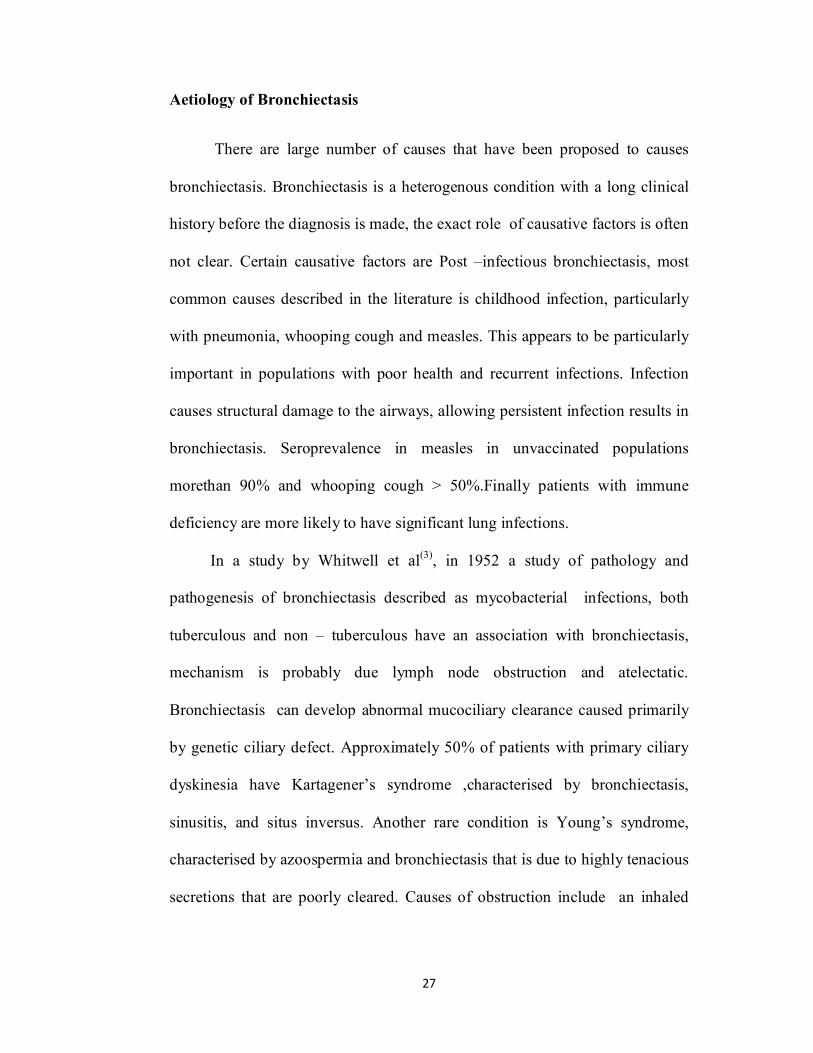
Aetiology of Bronchiectasis
There are large number of causes that have been proposed to causes
bronchiectasis. Bronchiectasis is a heterogenous condition with a long clinical
history before the diagnosis is made, the exact role of causative factors is often
not clear. Certain causative factors are Post –infectious bronchiectasis, most
common causes described in the literature is childhood infection, particularly
with pneumonia, whooping cough and measles. This appears to be particularly
important in populations with poor health and recurrent infections. Infection
causes structural damage to the airways, allowing persistent infection results in
bronchiectasis. Seroprevalence in measles in unvaccinated populations
morethan 90% and whooping cough > 50%.Finally patients with immune
deficiency are more likely to have significant lung infections.
In a study by Whitwell et al(3), in 1952 a study of pathology and
pathogenesis of bronchiectasis described as mycobacterial infections, both
tuberculous and non – tuberculous have an association with bronchiectasis,
mechanism is probably due lymph node obstruction and atelectatic.
Bronchiectasis can develop abnormal mucociliary clearance caused primarily
by genetic ciliary defect. Approximately 50% of patients with primary ciliary
dyskinesia have Kartagener’s syndrome ,characterised by bronchiectasis,
sinusitis, and situs inversus. Another rare condition is Young’s syndrome,
characterised by azoospermia and bronchiectasis that is due to highly tenacious
secretions that are poorly cleared. Causes of obstruction include an inhaled
28
foreign body, slow growing tumour and twisting of an airway after lobar
resection.
In a study in described by Currie et al (6) in 1987 “Impaired
tracheobronchial clearance in bronchiectasis in studied retained that sputum
can contribute to obstruction which leads to an important role in bronchiectasis.
Immune dysfunction associated with bronchiectasis including HIV,
hypogammaglobulinaemia, type I major histocompatibility complex. Therefore
,malnutrition and socioeconomic factors may play a role in precipitating
immune dysfunction.
In a study Silva et al(41) in 1989,highlighted that othercauses strongly
associated with bronchiectasis such as Rheumatoid arthritis, Sjogrens
syndrome, Churg –Strauss syndrome and inflammatory bowel disease.
In a cohort study by Parr et al(38) in 2000,74 subjects with α1-Antitrypsin
deficiency that 70 subjects had evidence of radiological bronchiectasis and 20
had the syndrome of clinical bronchiectasis.
Microbiology of bronchiectasis
The microbiology of bronchiectasis is complex , with multiple
potential pathogens. The pattern of isolates varies between different
institutions. Previous studies have shown that the two major pathogens found
are H.Influenza,and P.aeruginosa .Other important pathogens include
Moxarella catarrhalis, S.pneumoniae,non –tuberculous mycobacteria and
Aspergillus species. A consistent finding is that, despite the presence of
purulent sputum,30-40% of specimens will fail to grow any pathogens.
29
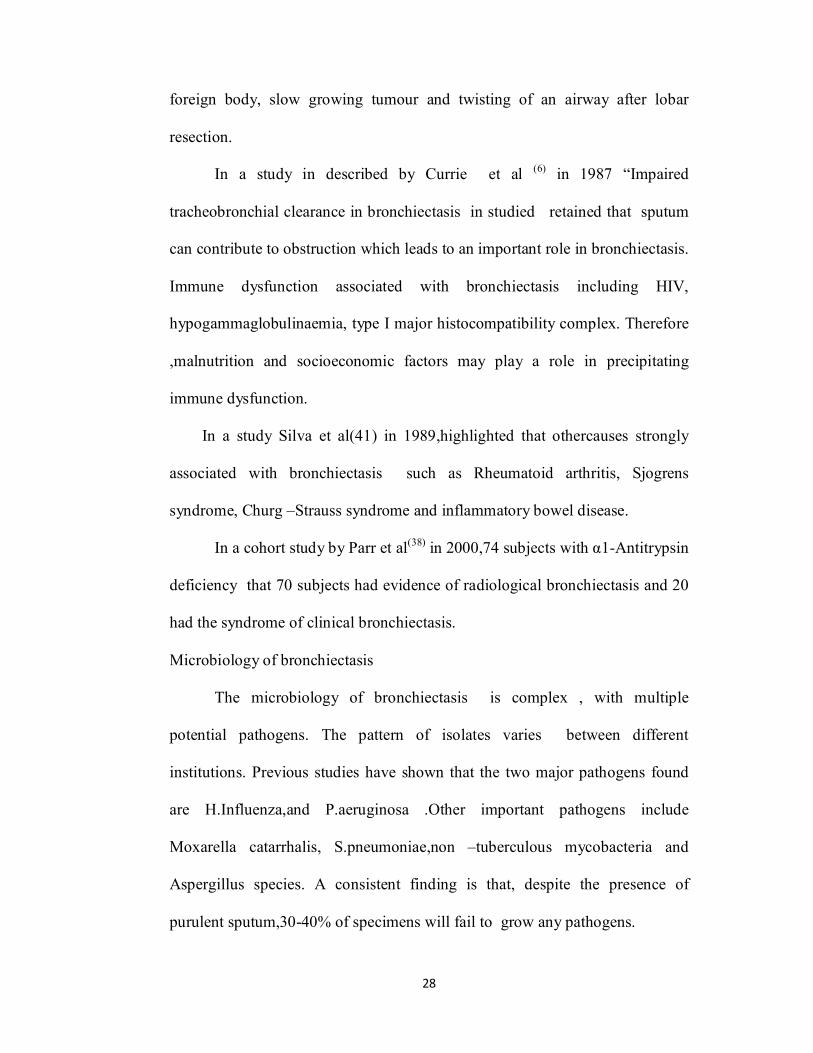
As bronchiectasis progresses there appears to be a change in bacterial flora.
Subjects with mild disease usually have no pathogens isolated, while subjects
with moderate disease most commonly have H.Influenzae.In most severe
disease ,P.aeruginiosa is the dominant pathogen.
Assessment of bronchiectasis based on
Clinical features:
Severity of clinicopathologic events varies widely in patients with
bronchiectasis. Patients have exacerbations, with chronic sputum production
other symptoms include hemoptysis, especially during exacerbations and
breathlessness, characterized by mild to moderate airflow obstruction, lethargy
and reduced health status.
Clinical signs
Finger digital clubbing recognized as a sign of chronic suppurative lung
disease.Studies reports that prevalence of clubbing 1- 2%.Overall, suggests that
finger clubbing is now seen only in minority of patients with non –CF
bronchiectasis.Other clinical finding in bronchiectasis is coarse
crackles,reported upto 73% of patients in more recent studies.
30
Assessment of Functional status with physiological parameters
Bronchiectasis is chronic respiratory condition,characterised by cough
and sputum production together with physical fatigue and reduced exercise
tolerance.It causes diminished exercise capacity include dyspnea secondary to
dynamic hyperinflation,altered respiratory mechanics and decreased skeletal
muscle bulk.However ,there have been limited evaluation of physical function
in patients with bronchiectasis and influence on respiratory disease severity
and extent of disease on exercise capacity is notknown.
6-Minute Walk test
It is widely used to measure of functional status, as well as a predictor of
prognosis(32).With the clinical application suggested that simple measurement
reflected on the pulmonary and functional status of patients with
bronchiectasis,evaluation of the 6MWT in population has been limited.
A study done by Lee at al(33) in 2008,clinical determinants of the 6-Minute
Walk test in bronchiectasis provides a valuable information of the functional
status in a group of patients with mild to moderate bronchiectasis and also
indicates dynamic hyperinflation and increased work of breathing are
responsible of disease.In this study evidence of airflow obstruction measured
by using FEV1 and FVC associated 6minute walk test.
31
Pulmonary Functional Test
Patients with bronchiectasis generally have mild to moderate airflow
obstruction.Both adults and children have been shown to develop
progressively worsening airflow obstruction. Hogg et al have studied small
airways obstruction found the factor most associated with obstruction was the
presence of lymphoid follicles, which were similar.Airway reversibility may
also be common in bronchiectasis.Murpghy et al and Pang et al found
significant airway reversibility in 40% of subjects and two other studies found
a 30% and 69% of reversibility in bronchiectasis.
Functional impairement in bronchiectasis is related to the extent of lung
damage as determined by the number of bronchopulmonary segments involved.
Measurements of ventilatory capacity and lung volumes with
bronchographically proven bronchiectasis showed that airways obstruction is
constantly ventilatory defect.
Another smaller series shown that 71% of 34 patients with
bronchiectasis had airflow limitations in FEV1/forced vital capacity ratio is less
than 65%.
The findings showed that the presence of infection/inflammation was
associated with increased airways obstruction. In a study done by Taylor et
al,in 2010 about 204 patients showed that degree of airflow limitation has
been correlated positively with both the duration of symptoms and extent of
disease on CT examination. Reversibility of airflow limitation may present in
bronchiectasis.Lung function tests have diagnostic value in bronchiectasis but
32
are useful in measuring the extent of impairement and demonstrating
occasional response to bronchodilators or other treatments.The simple and
highly reproducible tests, such as FEV1 and FVC are also clinically useful and
reliable
MODIFIED BORG Dyspnea scale
This scale is an aid for the 6-minute walk test enabling the evaluation of the
degree of respiratory discomfort,in terms of determination of subjective rates
according to the perfection of individual.This a vertical scale to quatify from 0-
10 in which 0 represents no symptoms,and 10 represents maximum symptoms
and providing an providing individual measurement of the density of the
exercise.
Martinez gracia et al in 2000 in their study suggested an independent
impact of BORG score in assessing the lung extent in bronchiectasis.
33
Imaging in Bronchiectasis
Chest radiography is often the first imaging modality used to
investigate patients with suspected bronchiectasis(9)
Plain chest radiography
Radiographs are insensitive as a diagnostic tool for bronchiectasis,
and suggest the diagnosis in lessthan 50% of cases in studies. Plain chest
radiographic features have been described by Simon et al(1) in 1978,which
include :
Evidence of dilated bronchi
Ring Shadows: produced by dilated bronchi seen ‘end-on’.It may be
small, numerous widespread, sometimes referred as honeycomb lung. Larger
ring shadows
(0.5-2cm diameter) which contain fluid levels, formed by retained mucopus.
They may be localized or widespread, giving the radiographic appearance of
cystic lung.
Parrallel Lines: are produced by dilated bronchi viewed ‘side-on’. It is
fine parallel, air-contaning , hairline opacities. Tramline: there walls been
thickened rather than hairline, more numerous or crowded together, indicating
lobar shrinkage.
Solid tubular opacities: bronchi contain mucopus which may seen as
solid tubular, looking like a scaled –down column of tooth –paste. Gloved
34
finger shadow’s tangentially produce glove tending to have a rounded end,
representing a large dilated bronchus containing mucopus.
Bronchography
It was for many years for the investigation of choice, for confirming
bronchiectasis. Technique involves instillation of liquid contrast medium into
tracheobronchial tree, under general or local anaesthesia. Aqueous or oily
propyliodone was commonly used. Affected parts of lungs showed areas of
bronchial dilatation, described as cylindrical, fusiform, saccular. Changes seen
are found commonly in left lung and are bilateral in about one-third of cases.
Nowadays, bronchography is regarded as obsolete in most centres, HRCT
having been to be more satisfactory.
Computed tomography scanning with high resolution
It should be used to diagnose bronchiectasis as technique demonstrates the
airways in higher detail than standard computed tomography scanning. In a
study done by Naidich et al(9) and Mcguinness et al(10) ,in 1982 and 2002 have
established the use of standard criteria for diagnosis of bronchiectasis.
Most specific features are :
a) Internal diameter of a bronchus is wider than its adjacent pulmonary artery
b) Failure of bronchi to taper, and
c) Visualisation of the bronchi in outer 1-2cm of lung fields.
Less specific features include mucosal wall thickening, crowding of
bronchi and mucus impaction. Lobes most commonly involved in
bronchiectasis are lowerlobes.
35
High resolution computed tomography
It has become the investigation of choice in bronchiectasis. Earlier studies CT
was used for non- invasive and safe, this technique is used as alternative to
bronchography in the diagnosis of bronchiectasis. These showed that
conventional CT was less sensitive for diagnosing bronchiectasis than
bronchography ,the sensitivities for 10-mm slices at 20 mm intervals .Cooke
and colleagues found that conventional CT diagnosed bronchiectasis in 71% of
45 bronchiectatic lobes, sensitivity 71%,indicates that this form of CT cannot
be used to ruleout bronchiectasis. Development of thin section HRCT changed
this so that sensitivities increased to 82-97%. Recommended HRCT technique
comprises scanning from apex to base with 1-2mm cuts at 10mm intervals.
HRCT criteria for diagnosing bronchiectasis are bronchial dilatation,
and bronchial wall thickening. A bronchus is taken to be dilated if its internal
diameter is greater than that of pulmonary artery branch, measurements being
conventionally made in short axis of both the bronchus and the vessel.
Bronchial wall thickening is present if the thickness of the wall is at least equal
to the diameter of adjacent pulmonary artery branch. The occurence of
bronchial wall thickening prior to the development of bronchial dilatation is
described in patients with hypogammglobulinaemia. Air trapping on expiration
has been demonstrated as areas of increased transradiancy in patients with
severe bronchiectasis. Scanning during inspiration and expiration may
distinguish between an area of bronchiectasis and emphysematous blebs,or
bullae.
36
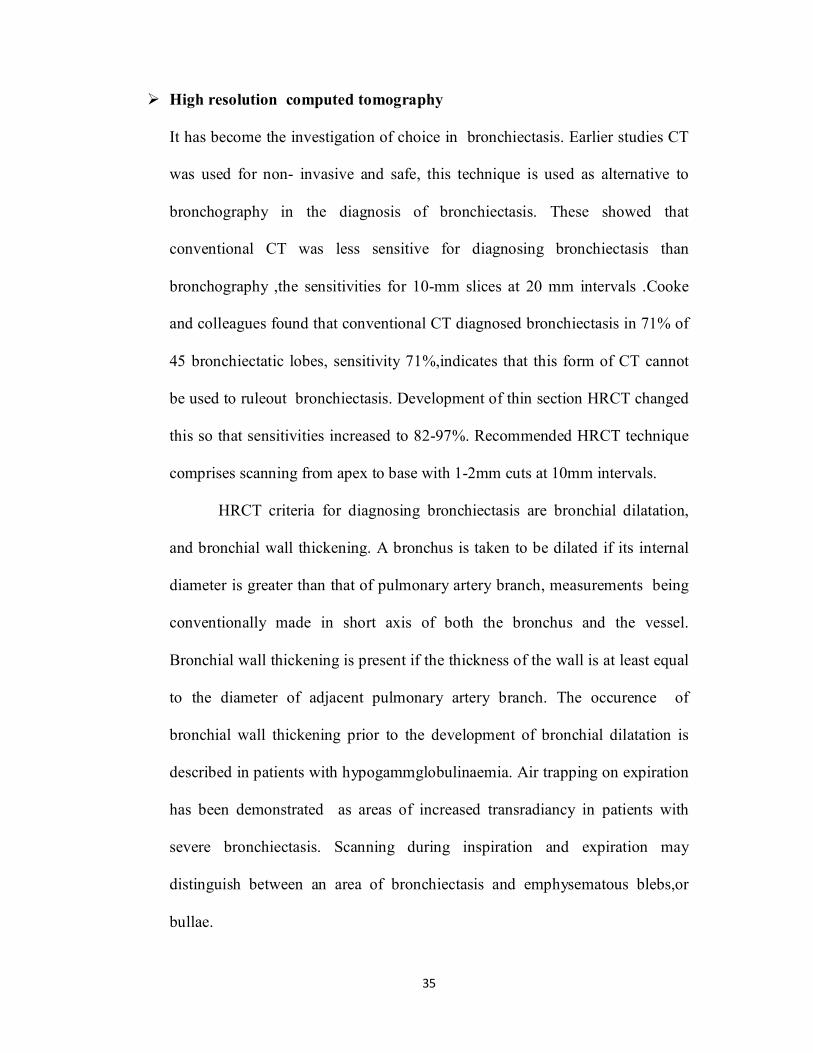
Most commonly involved in bronchiectasis are lowerlobes usually multiple
lobes are involved. HRCT has been found to have greater sensitivity than spiral
CT when applied to patients in whom bronchiectasis is suspected.
Figure : 11 shows signet ring sign seen in bronchiectasis
37
Treatment of Bronchiectasis
Antimicrobial therapy is required once a acute exacerbation is identified
.Patients who relapse quickly or frequently (>3times in 1year)with mucoid or
mucopurulent sputum are usually managed with short course of appropriate
antibiotics ,may also need longer term preventive therapy. Patients with
chronic purulent sputum usually require higher antibiotics and also need of
long term nebulised antibiotic therapy.
Prophylactic Therapy
Macrolides are the most common antimicrobials used in clinical practise.
Azithromycin twice weekly for 6months,has shown positive results, with
reduced 24-hour sputum volume and reduced number of exacerbations.
Postural Drainage
Physiotherapy ,including postural drainage of chest secretions,has been
regarded for many years is the mainstay in treatment of
bronchiectasis.Postural drainage has been shown in the short term to
increase rates of mucociliary clearance and to increase the expectoration of
sputum,in patients whose secretions are copious.It has also been found to
improve airway function .
Vaccination
In routine practises patients with bronchiectasis are vaccinated aganist
influenza. Evidence is minimal regarding the pneumococcal vaccine, 23 valent
pneumococcal vaccine as routine management in adults with bronchiectasis.
38
Surgical Treatment
Surgical treatment plays only a small role in management of bronchiectasis.
Surgery is indicated in the patients whose significantly disabled by persistent
sputum production, recurrent infective exacerbations or haemoptysis despite all
reasonable medical measures having been taken over a period of at least
12months.The disease should be confirmed radiologically, should be
sufficiently localized to one lung or to part of one lung to enable curative
resection and residual lung should be suffienctly healthy in terms of measured
lung function.
39
PULMONARY ARTERY HYPERTENSION
Pulmonary hypertension(28) is a rare, pathologically complex disease
characterized by a progressive increase in pulmonary arterial pressure
associated with variable degrees of pulmonary vascular remodelling,
vasoconstriction, and thrombosis. These changes leads to increased
pulmonary vascular resistance, and with right-sided heart failure and death.PH
is defined as an increase in mean pulmonary arterial pressure > 25mmHg at rest
assessed by right heart catherisation. Pulmonary hypertension is a common
complication in chronic lung disease which included in alveolar hypoxia in
WHO group III of PH-related disease.PH is a haemodynamic
pathophysiological state that can be found in multiple conditions.
The clinical classification of Pulmonary Hypertension has gone through
a series of changes the first version was proposed in 1973 by WHO. Evian -
Venice classification proposed in 1998-2003 on PAH. This is classified into
five groups according to pathological, patho physiological and therapeutic
characteristics. During Fourth World Symposium on PH held in 2008 in Dana
Point, new classification was derived.
40
Classification:
Updated Clinical Classification of Pulmonary Hypertension(28) :
1. Pulmonary arterial hypertension
1.1 Idiopathic PAH
1.2 Heritable :
1.2.1 Bone morphogenetic protein receptor type II(BMPR2)
1.2.2 ALK-1, endoglin
1.2.3 Unknown
1.3 Drug or toxin –induced
1.4 Associated with:
1.4.1 Connective Tissue Diseases
1.4.2 Human Immunodeficiency virus (HIV) infection
1.4.3 Portal hypertension
1.4.4 Congenital heart diseases
1.4.5 Schitosomiasis
1.4.6 Chronic haemolytic anemia
1.5 Persistent pulmonary hypertension of newborn
41
1. Pulmonary venocclussive disease and/pulmonary capillary
hemangiomatosis
2 . Pulmonary hypertension due to left- sided heart disease
3. Pulmonary hypertension due to lung disease and / hypoxia
4. Chronic thromboembolic pulmonary hypertension (CTEPH)
5. Pulmonary hypertension with multifactorial mechanisms
Normal pulmonary arteries have thin medial layer of circular muscle ,
with thickness less than 5% of diameter of vessel. Under physiological
condition pulmonary circulation is characterised by variable intimal
hyperplasia, medial hypertrophy, adventitial proliferation, and fibrosis that
occur in close proximity to plexiform lesions. These lesions results from
intimal proliferation and progresses from a cellular to a fibrotic lesion with
advancing disease. As the vascular pathology progresses, pulmonary vascular
resistance increases and pulmonary artery rises, in order to maintain cardiac
output. So as right ventricle is able to compensate for resistance, the pressure
continues to increases as the pulmonary vascular resistance increases. When
contractile reserve of the right ventricle is exhausted, right ventricular systolic
failure ensures. Various degrees on right ventricular diastolic dysfunction also
present in PH. A combination of reduced right ventricular output and diastolic
dysfunction resulting in impairing left ventricular filling and leads in
42
hemodynamic deterioration. Inflammation associated with underlying lung
disease is responsible for development of PH in hypoxic states.
Group 3: Pulmonary hypertension due to Lung Disease and /or Hypoxia
Pulmonary hypertension associated with disorders of the respiratory system or
hypoxemia is a category of PH that is caused mainly by inadequate
oxygenation of pulmonary arterial blood result of either parenchymal lung
disease, impaired control of breathing or residence at high altitude. Pulmonary
arterial pressure is modest and survival depends on the severity of the
pulmonary disease, rather than on the severity of the associated hypertension.
Pathophysiology
Pulmonary hypertension in the setting of chronic respiratory disease leads to
increased pulmonary vascular resistance when pulmonary artery wedge
pressure is normal. Increased pulmonary vascular resistance is usually
secondary to effects of hypoxia and destruction of the vascular bed in lung
parenchyma. While acute hypoxia leads to pulmonary vasoconstriction in the
small pre-capillary arteries, chronic hypoxemia results in pulmonary vascular
remodelling including medial hypertrophy and intimial proliferation of distal
pulmonary arteries. Additional it includes mechanical stress secondary to
hyperinflation, loss of capillaries, inflammation and endothelin –derived
vasoconstriction – vasodilator imbalance.
Moreover, significant number of lung disease and severe PH, other co-
morbidities may contribute pathogenesis of PH, such as left ventricular
43
diastolic dysfunction or chronic thromboembolic pulmonary hypertension.
Genetic factors may also play an important role for developing PH.
Mechanism of Pulmonary hypertension in Bronchiectasis
Alveolar hypoxia is a stimulus for pulmonary vasoconstriction. Most
important pathways leading to pulmonary hypertension is endothelial level in
chronic lung diseases. Alveolar hypoventilation precipitates acute pulmonary
vasoconstriction in some parts of lungs and vasodilation which causes
physiological shunt. Studies by Sylvester et al 2009,showed that
vasoconstriction is achieved through vasoconstrictor pathway or inactivation of
a vasodilator pathway, through the effects of hypoxia on vascular smooth
muscle.Studies by Jing et al ,2009in rats,exposed to hypoxia suggest that
hypoxia exposed arterioles develop smooth muscles in the walls of non
muscular pre capillary blood vessels which persist after the removal of the
stimulus and contributes to on going pulmonary hypertension.
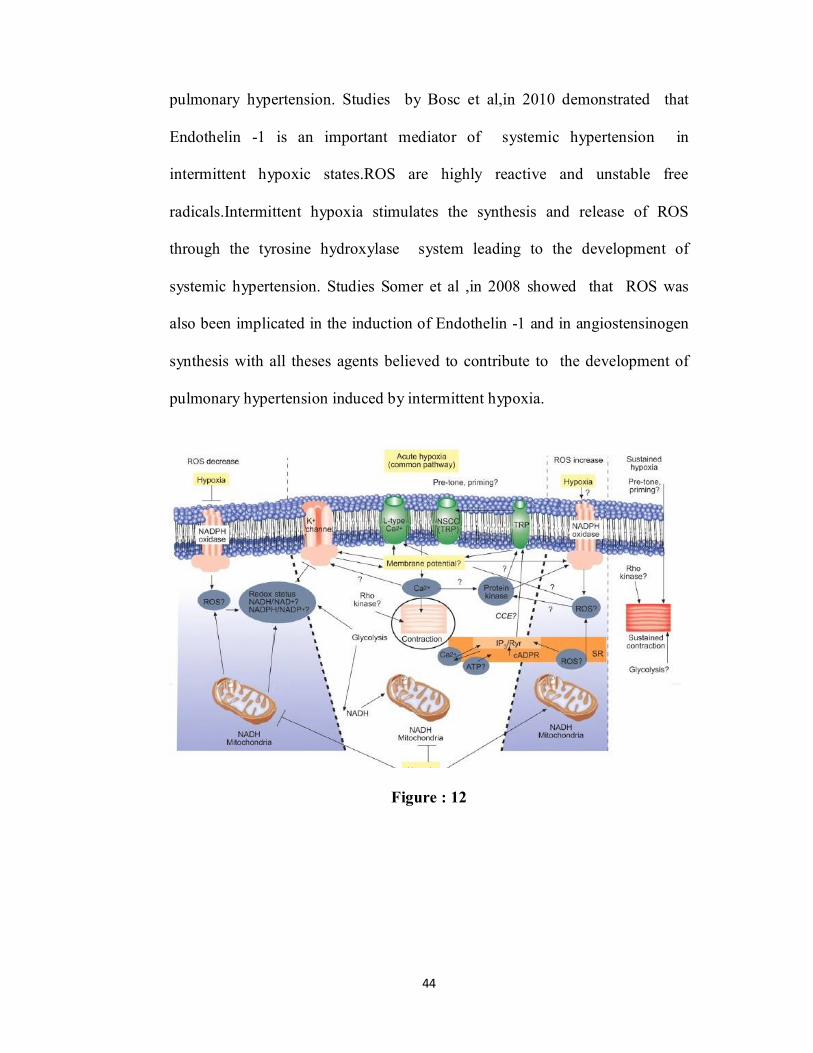
Development of pulmonary hypertension may result in both
intermittent and chronic. The effector pathway suggested L-type calcium
channels, non –specific cation channels and voltage –dependent potassium
channels, whereas mitochondria and nicotinamide adenine dinucleotide
phosphate oxidase described as oxygen sensors. Reactive oxygen species,
redox couples and adenosine monophoshate – activated kinases are the
mediators of hypoxic pulmonary vasoconstriction. Endothelin -1 pathway,
nitric oxide pathway, and reactive oxygen species helps for development of
44
pulmonary hypertension. Studies by Bosc et al,in 2010 demonstrated that
Endothelin -1 is an important mediator of systemic hypertension in
intermittent hypoxic states.ROS are highly reactive and unstable free
radicals.Intermittent hypoxia stimulates the synthesis and release of ROS
through the tyrosine hydroxylase system leading to the development of
systemic hypertension. Studies Somer et al ,in 2008 showed that ROS was
also been implicated in the induction of Endothelin -1 and in angiostensinogen
synthesis with all theses agents believed to contribute to the development of
pulmonary hypertension induced by intermittent hypoxia.
Figure : 12
45
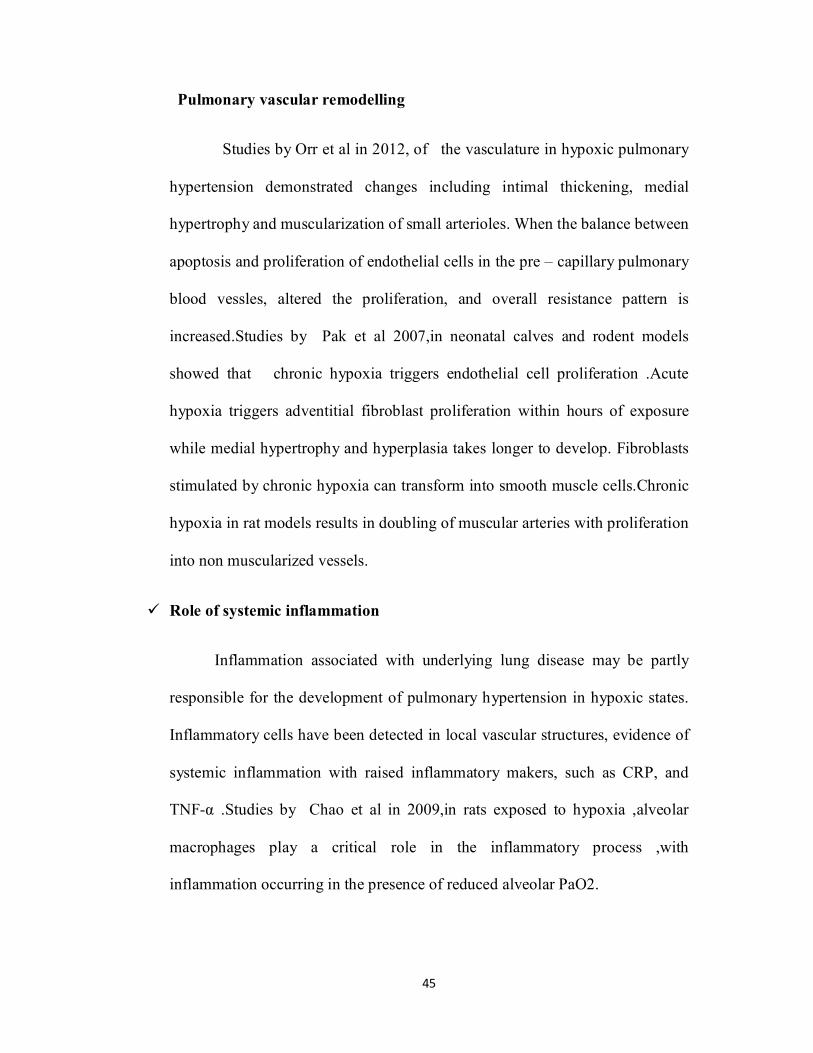
Pulmonary vascular remodelling
Studies by Orr et al in 2012, of the vasculature in hypoxic pulmonary
hypertension demonstrated changes including intimal thickening, medial
hypertrophy and muscularization of small arterioles. When the balance between
apoptosis and proliferation of endothelial cells in the pre – capillary pulmonary
blood vessles, altered the proliferation, and overall resistance pattern is
increased.Studies by Pak et al 2007,in neonatal calves and rodent models
showed that chronic hypoxia triggers endothelial cell proliferation .Acute
hypoxia triggers adventitial fibroblast proliferation within hours of exposure
while medial hypertrophy and hyperplasia takes longer to develop. Fibroblasts
stimulated by chronic hypoxia can transform into smooth muscle cells.Chronic
hypoxia in rat models results in doubling of muscular arteries with proliferation
into non muscularized vessels.
Role of systemic inflammation
Inflammation associated with underlying lung disease may be partly
responsible for the development of pulmonary hypertension in hypoxic states.
Inflammatory cells have been detected in local vascular structures, evidence of
systemic inflammation with raised inflammatory makers, such as CRP, and
TNF-α .Studies by Chao et al in 2009,in rats exposed to hypoxia ,alveolar
macrophages play a critical role in the inflammatory process ,with
inflammation occurring in the presence of reduced alveolar PaO2.
46
Diagnosis of Pulmonary Hypertension
The evaluation process with suspects PH requires a series of
investigations confirm the diagnosis, clarify the clinical group of PH to
evaluate functional and hemodynamic impairment.
Clinical presentation
Symptoms includes breathlessness, fatigue, weakness, angina and syncope.
Physical signs of PAH include left parasternal lift second heart sound,
pansystolic murmur of tricuspid regurgitation. Lung sounds are usually normal.
Right –Heart catheterization
Invasive hemodynamic assessment by RHC is pivotal in the evaluation of any
patient with suspected PAH. Right –Heart catherization is typically performed
after the non invasive testing for PH. In RHC essential measurements include:
o Oxygen saturation
o Right atrial pressure
o Pulmonary artery pressure
o Left sided filling pressure
o Cardiac index/Cardiac output
o Systolic blood pressure
o Heart rate
o Response to acute vasodilators
47
In recent study of 94 patients with bronchiectasis,31 patients (32.9%)had
PH,defined as systolic Pulmonary artery pressure of ≥40mmHg on Doppler
echocardiography100.Significant correlation was obseverd between right
ventricular dimensions and systolic pulmonary artery pressure(r=0.74)while
RV dimension were inversely related to PaO2 values(r=0.37).
Chest radiograph
In 90% of patients with PAH the chest radiograph is abnormal at time of
diagnosis. Findings include loss of peripheral blood vessels. Right atrium and
ventricle enlargement more seen in advanced cases. Chest radiograph allows
associated moderate –to – severe lung disease, or pulmonary venous
hypertension due to left heart disease. The degree of PH in any given patient
doesnot correlate with extent of radiographic abnormalities.
Pulmonary Function Tests
This testing is a necessary part of initial evalutation of all patients with
pulmonary hypertension, to exclude or characterised the underlying airway or
parenchymal lung disease. Patients with PAH usually have decreased lung
diffusion capacity for carbon monoxide and mild to moderate reduction of lung
volumes. A decrease in lung volume together with a decrease in diffusion
capacity for carbon dioxide tension, may indicate pulmonary hypertension.
48
Echocardiography
Doppler echocardiography should performed as a noninvasive
screening test to detect elevated pulmonary artery pressure. It provides an
estimation of right ventricular function and pulmonary artery pressure and can
reveal other underlying cardiac abnormalities. Signs indicative of pulmonary
hypertension on echocardiogram include increased pulmonary artery
hypertension or tricuspid regurgitant jet, right atrial and ventricular
hypertrophy, flattening of intraventricular septum, small left ventricular
dimension and dilated pulmonary artery. Echocardiography is useful in disease
progression, removing the need for repeated pulmonary artery
catheterizations.
Patients with suspected pulmonary hypertension, right-sided heart
catheterization is required to confirm the presence of PH, to establish the
specific diagnosis, and to determine the severity and prognosis of pulmonary
hypertension. It also can be used to evaluate for vasoreactivity and guide
therapy. A acute response to a vasodilator is defined as a fall in pulmonary
artery hypertension of at least 10mm Hg to 40mm Hg or less, with an
increased or unchanged cardiac output. Eysmann et al(30) proven that right
heart catherization is required to perform presence of PH, for diagnosing
purposes.
In a study conducted by Abdulaziz et al(20) in 2008 found that systolic
pulmonary artery pressure was higher in cystic bronchiectasis with right and
left ventricular dysfunction.
49
Study showed correlation between HRCT score and SPAP and FEV%.It
showed SPAP could be a predictor of future pulmonary hypertension .Patient
with cystic bronchiectasis have significantly higher impairement of pulmonary
physiology as compared with cylindrical bronchiectasis patients.
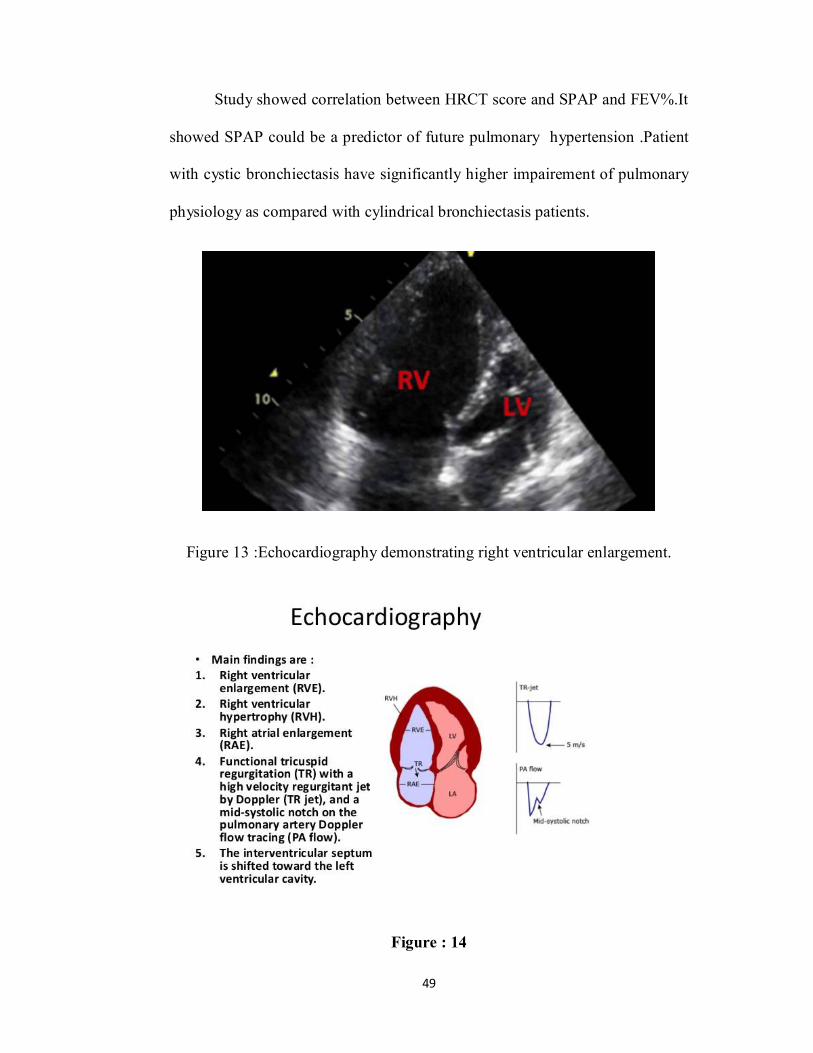
Figure 13 :Echocardiography demonstrating right ventricular enlargement.
Figure : 14
50
Approach to therapy
Treatment goals for patients with pulmonary hypertension include
reduction in clinical signs, and symptoms and improvement in exercise
tolerance, hemodynamics, and quality of life, with decreased need for
hospitalization and longer survival. Long term oxygen administration has been
shown partially to reduce the progression of pulmonary hypertension.
Phosphodiesterase Type -5 Inhibitors
Pulmonary vasodilating effects of nitric oxide are mediated through
cGMP.Nitric oxide activates guanylate cyclise,which increases cGMP
production.Cyclic GMP causes vasorelaxation,but effects are attenuated by
rapid degradation of cGMP by phoshodiesterase.Sildenafil and Tadalafil inhibit
phosphodiesterase type 5,thus enhancing relaxation and growth inhibition of
vascular smooth muscle cells..both have demonstrated improvement in exercise
capacity and functional class.
Endothelin Receptor Antagonists
Endothelin -1 is a potent vasoconstrictor and smooth muscle mitogen, that is
over expressed in the plasma and lung tissue of patients with pulmonary
hypertension.
o Bosentan is a oral nonselective endothelin receptor antagonist,
o Ambrisentan is a oral selective endothelin type A receptor antagonist, both of
these agents have been shown to improve exercise capacity, functional class,
and time to clinical worsening.
51
Prostanoids
Prostacylin is a potent vasodilator and inhibitor of platelet activation and
smooth muscle proliferation. Three prostanoids have been shown to improve
exercise capacity, quality of life, hemodynamics are epoprostenol,treprostinil,
and iloprost.
Thus the above mentioned studies shows that alveolar hypoxia in
bronchiectasis is a potent stimulus for pulmonary vasoconstriction was leading
to the development of pulmonary artery hypertension and bronchiectasis
patients with pulmonary hypertension have worse survival than bronchiectasis
subjects without pulmonary hypertension.Studies also found that extent and
severity of bronchiectasis correlated strongly with severity of airflow
obstruction. Clinical determinants of the 6-Minute Walk test in bronchiectasis
provides a valuable information of the functional status in a group of patients
with mild to moderate bronchiectasis and also indicates dynamic hyperinflation
and increased work of breathing are responsible of disease.
52
RESULTS
We present our study results under following description
1. Distribution of study variables
2. Comparison of the variables within the study population
3. Correlation of variables in the study population
DISTRIBUTION OF VARIABLES IN STUDY POPULATION
A total of 40 patients were recruited for the study. In that 19 patients were
cystic, 11 were cylindrical and 10 were varicose. Out of 40 patients 17 were
male (42.5%) and 23 were female (57.5%). The mean age group of the study
was 45-55 years. The average age was 5510 years. Among the study
population 13 patients had history of smoking and 2 patients had history of
alcohol intake.
Socio-demographic details N=40
Age 5510 years
Gender Male
Female
17 (42.5%) 23(57.5%)
BMI Male
Female
22 24
53
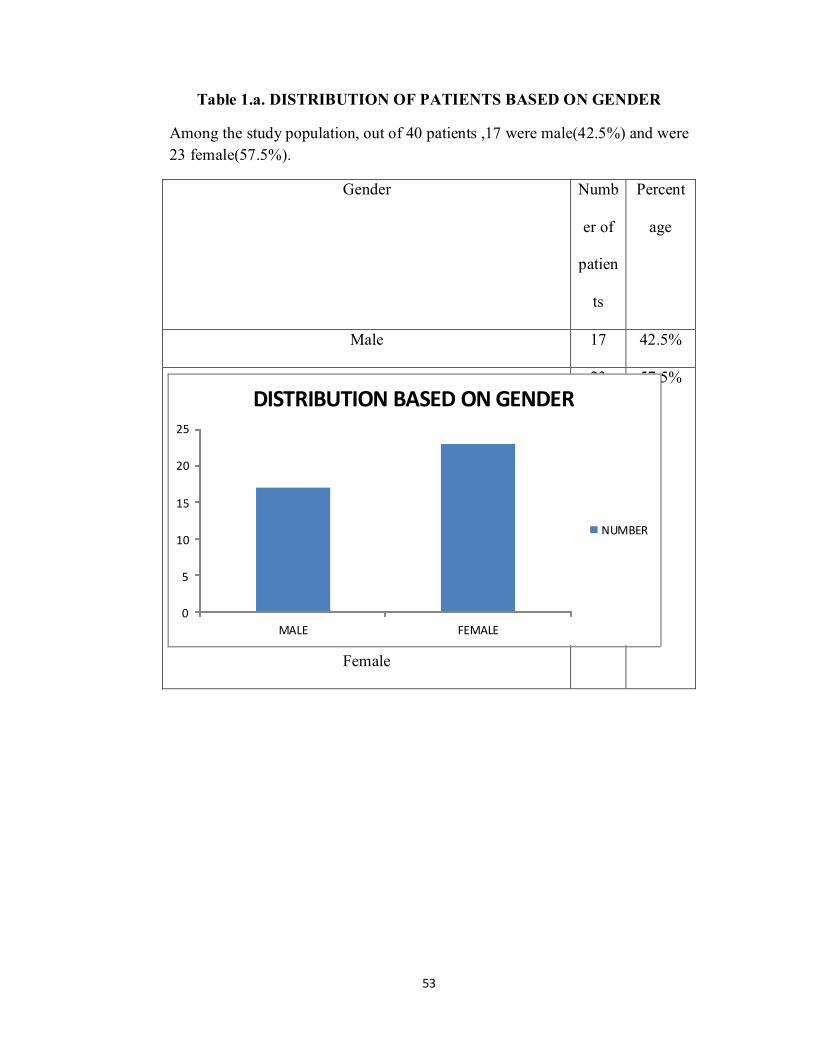
Table 1.a. DISTRIBUTION OF PATIENTS BASED ON GENDER
Among the study population, out of 40 patients ,17 were male(42.5%) and were 23 female(57.5%).
Gender Numb
er of
patien
ts
Percent
age
Male 17 42.5%
Female
23 57.5%
0
5
10
15
20
25
MALE FEMALE
DISTRIBUTION BASED ON GENDER
NUMBER
54
Table 1.b. DISTRIBUTION OF PATIENTS BASED ON AGE
Among 40 patients, most of the patients in the age group of 40 to 60 year old.
The mean age of the study population was 5510 years. Distribution of patients
in the age group of less than 40 years and more than 40 years as given below.
Age group Number of patients Percentage
<40 6 15%
40-60 20 50%
>60 14 35%
TABLE 1.c. DISTRIBUTION OF PATIENTS BASED ON BMI
Among 40 patients the average BMI was 23.6 kg/m2. The mean BMI of male
patients was 22 kg/ m2 and for female it was 24 kg/m2. There was no
significant correlation between the BMI and extent of bronchiectasis.
BMI(mean)
Male 22
Female 24
55
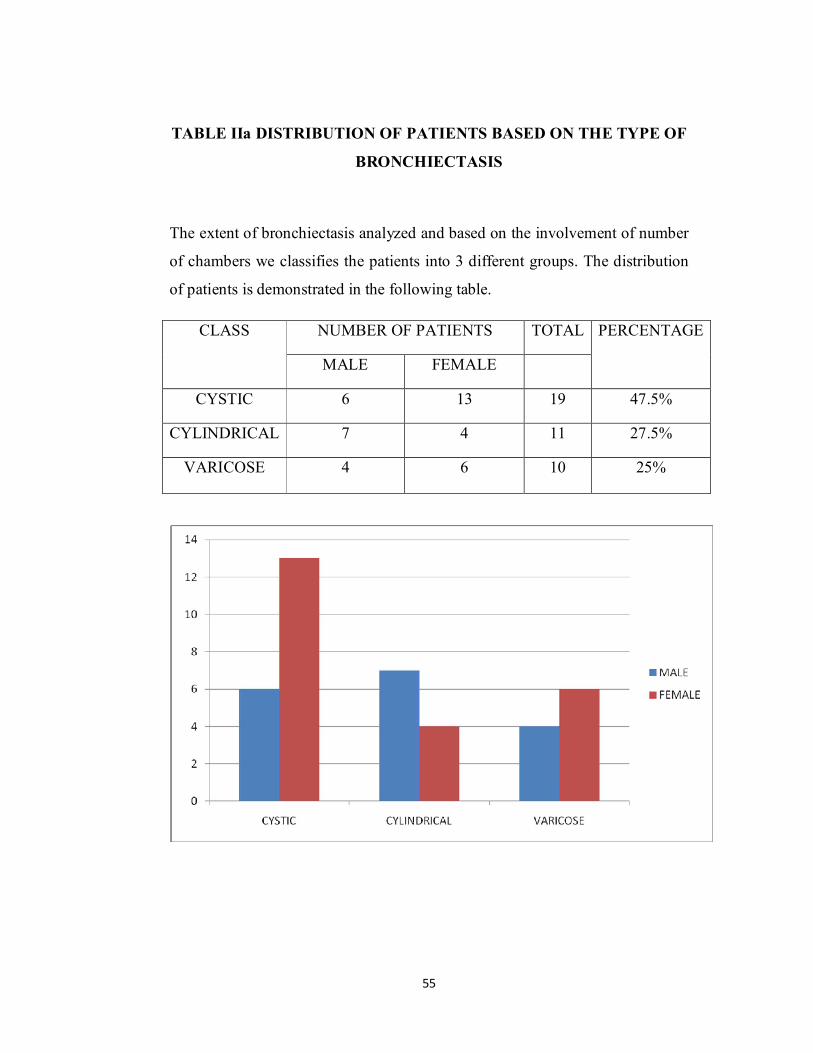
TABLE IIa DISTRIBUTION OF PATIENTS BASED ON THE TYPE OF
BRONCHIECTASIS
The extent of bronchiectasis analyzed and based on the involvement of number
of chambers we classifies the patients into 3 different groups. The distribution
of patients is demonstrated in the following table.
CLASS NUMBER OF PATIENTS TOTAL PERCENTAGE
MALE FEMALE
CYSTIC 6 13 19 47.5%
CYLINDRICAL 7 4 11 27.5%
VARICOSE 4 6 10 25%
56
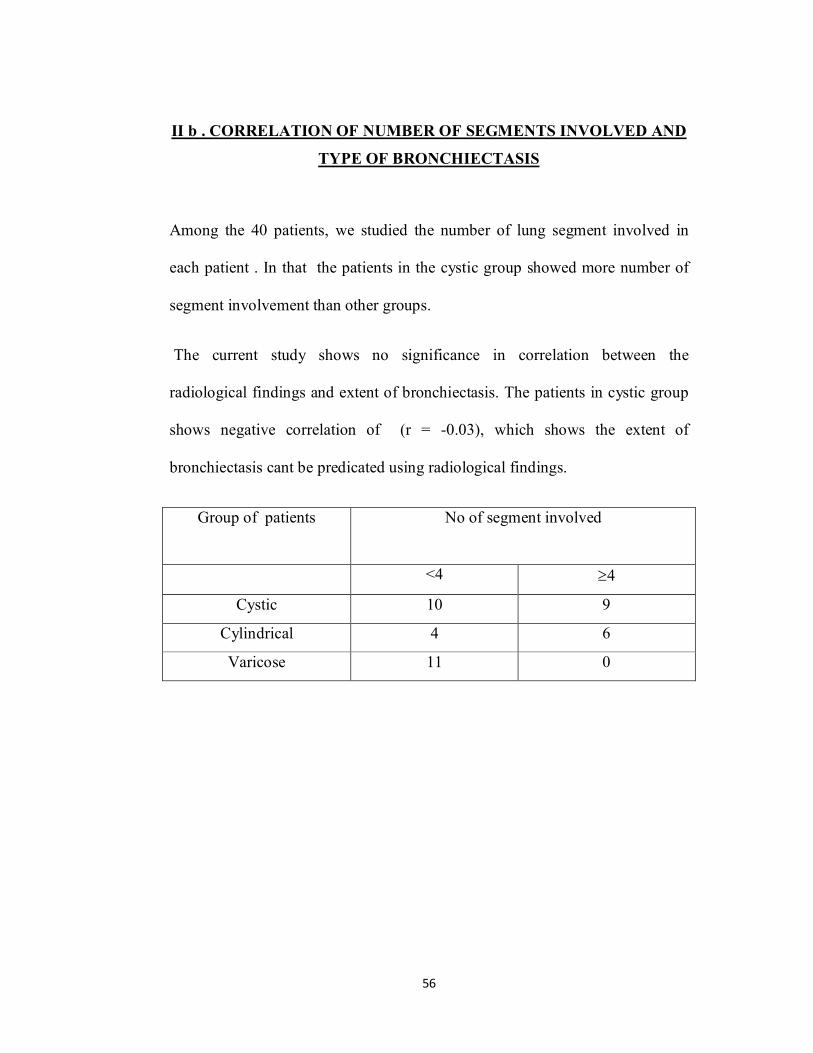
II b . CORRELATION OF NUMBER OF SEGMENTS INVOLVED AND
TYPE OF BRONCHIECTASIS
Among the 40 patients, we studied the number of lung segment involved in
each patient . In that the patients in the cystic group showed more number of
segment involvement than other groups.
The current study shows no significance in correlation between the
radiological findings and extent of bronchiectasis. The patients in cystic group
shows negative correlation of (r = -0.03), which shows the extent of
bronchiectasis cant be predicated using radiological findings.
Group of patients No of segment involved
<4 4
Cystic 10 9
Cylindrical 4 6
Varicose 11 0
57
II c .CORRELATION OF HRCT SCORE WITH TYPE OF
BROCHIECTASIS
The HRCT score done based 3 parameters
Bronchial dilation
Mucus thickness
Bronchial thickness
Among the parameters bronchial thickness was rare among the study
population. Most of the patient had high HRCT score.
The patients in cystic group shows significant correlation with the HRCT
findings (r=0.23) and extent of bronchiectasis. The positive correlation of
HRCT score was statistically significant only in cystic group compared to
others.
58
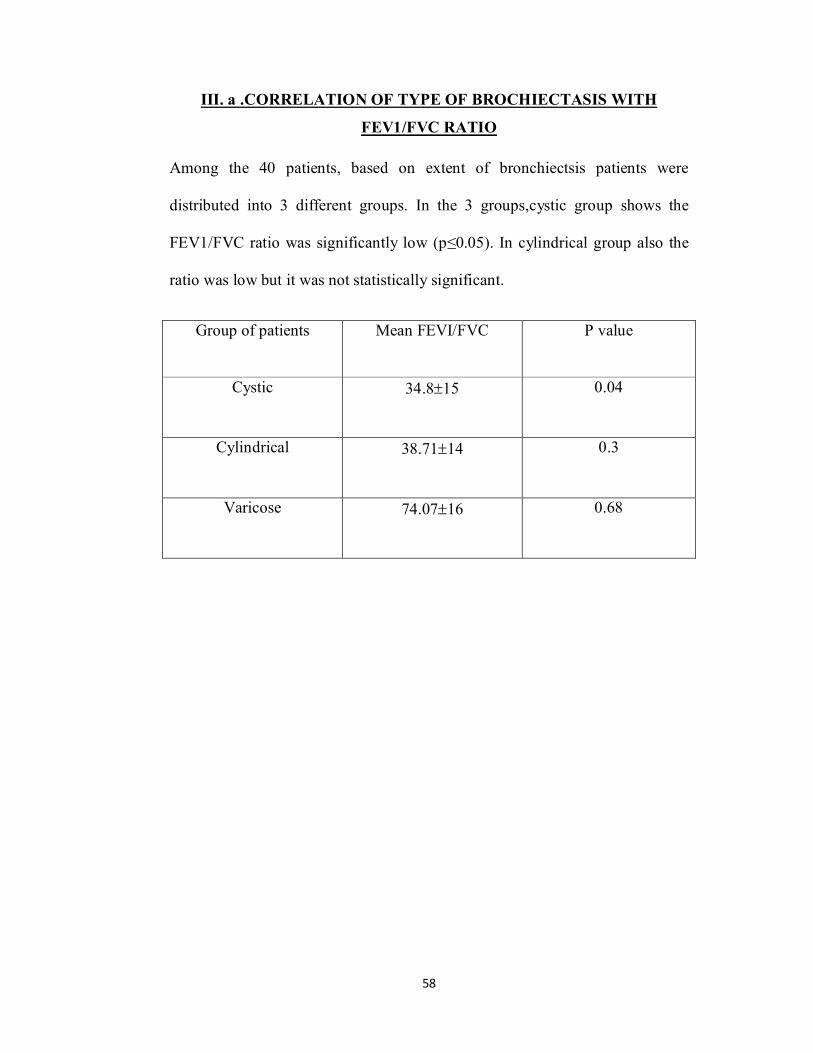
III. a .CORRELATION OF TYPE OF BROCHIECTASIS WITH
FEV1/FVC RATIO
Among the 40 patients, based on extent of bronchiectsis patients were
distributed into 3 different groups. In the 3 groups,cystic group shows the
FEV1/FVC ratio was significantly low (p≤0.05). In cylindrical group also the
ratio was low but it was not statistically significant.
Group of patients Mean FEVI/FVC P value
Cystic 34.815 0.04
Cylindrical 38.7114 0.3
Varicose 74.0716 0.68
59
III.b. CORRELATION OF 6 MINUTE WALK TEST AND FEV1/FEC IN
STUDY POPULATION
In our study we observed a significant correlation between the 6 minute walk
test and the pulmonary function test. Patients with altered PFT shows low score
in six minute walk test .There was a positive correlation (r=0.25) in the study
population with significant alteration in the FEV1/FVC . The 6 minute walk
test was found to be useful in patients with bronchiectasis in predicting the
severity.
According to the walking distance the patients were scored based on the
following criteria
Distance Score
>350 0
250-349 1
150-249 2
≤149 3
We consider walking distance more than 400m as normal. Among the study
population a total of 11 patients got score 3 , 5 got 2 , 7 got a score of 1 and 17
got score zero. There was no patient covered a walking distance of 400 m
among the study participants. The significant correlation of FEV1/FVC ratio
with 6 minute walk test shows p value (p<0.01)
60
III.c. CORRELATION OF MODIFIED MEDICAL RESEARCH
COUNCIL DYSPNEA SCALE (MMRC) WITH TYPE OF
BRONCHIECTASIS
Among the study population while correlating the MMRC score , there was
more patients coming under MMRC score of 2 . The patients in cystic group
showed a high MMRC score as compared to the cylindrical but it was not
statistically significant (p=0.8). the mean MMRC score in the study population
was 2.
III.d. CORRELATION OF MODIFIED BORG DYSPNEA SCALE
SCORE (BORG) WITH TYPE OF BRONCHIECTASIS
Among the study population while correlating the BORG score there was more
patients coming under the score of 4 . In the current study there was no
significant correlation between the BORG score and extent of bronchiectasis
(p=0.98). The mean score of the entire study population was 4.
61
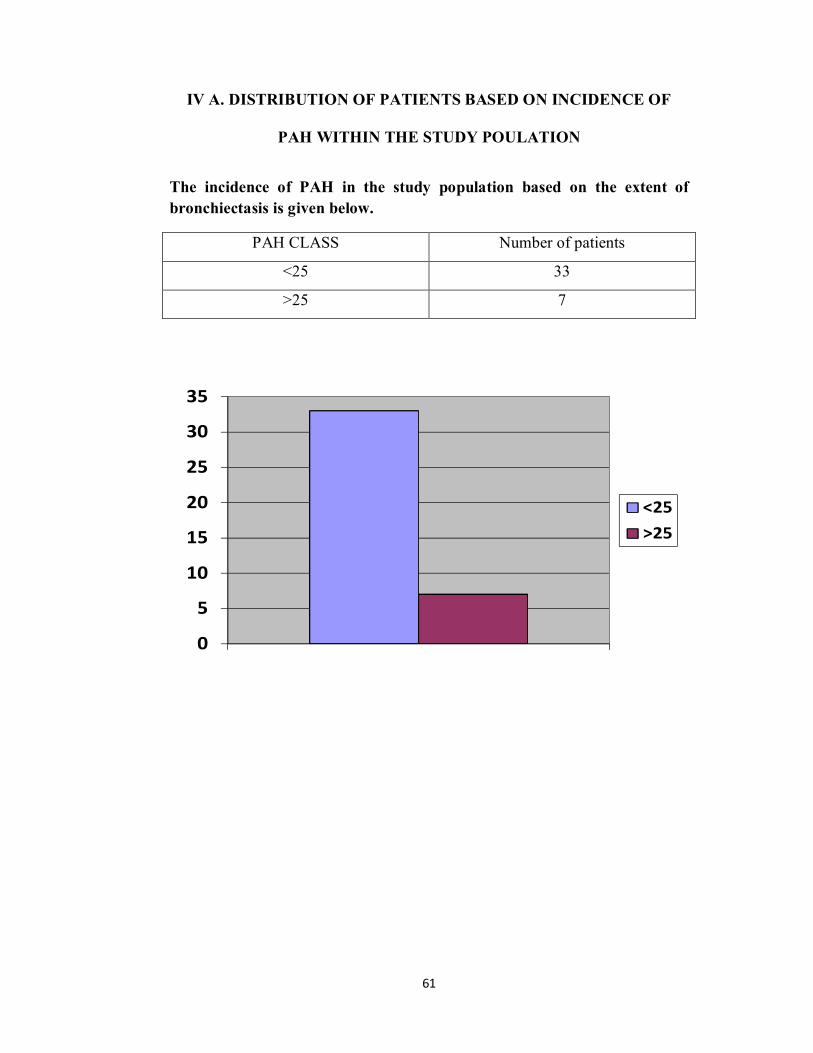
IV A. DISTRIBUTION OF PATIENTS BASED ON INCIDENCE OF
PAH WITHIN THE STUDY POULATION
The incidence of PAH in the study population based on the extent of bronchiectasis is given below.
PAH CLASS Number of patients
<25 33
>25 7
0
5
10
15
20
25
30
35
<25>25
62
IV B .CORRELATION OF TYPE OF BRONCHIECTASIS WITH
PULMONARY ARTERY HYPERTENSION
In the current study we found few patients with significant high incidence of
PAH , mostly in the cystic group. But while comparing with the other groups it
was not statistically significant and shows no correlation in the cylindrical
group of patients (p=0.9). The extent of bronchiectasis may be affected by
pulmonary artery hypertension in cystic group of patients (r=0.07).
IV C.CORRLATION OF HRCT SCORE AND SEVERITY OF
PULMONARY ARTERY HYPERTENSION
In our study we analyzed that pulmonary hypertension seen commonly in
advanced bronchiectasis , particularly cystic disease than other 2 groups. On
analyzing our study found that there is no significant correlation between
HRCT score with incidence of pulmonary hypertension.
63
DISCUSSION
The important findings in our study were as follows
1. Correlate clinicoradiological characteristics of bronchiectasis with pulmonary
hypertension
2. To correlate clinicoradiological profile of bronchiectasis with severity of
pulmonary hypertension and physiological characteristics of bronchiectasis
Bronchiectasis is most prevalent morbidity in community with lower
respiratory tract infection. When they are impaired due to repeated infection
causes damage which impedes the clearance of mucus.
The aim of our study was to evaluate the clinicoradiological parameters of
bronchiectasis and to assess the severity of exercise capacity and pulmonary
artery hypertension in the patients. Clinical and radiological predictors will
facilitate further understanding of pulmonary artery hypertension and thereby
affect prognosis. We found that the predictors like (Clinical,
physiological,radiological) in patients of bronchiectasis who can develop
pulmonary hypertension.
SOCIODEMOGRAPHIC CHARACTERS
In our study 40 subjects were recruited in which 23 were female and 17 were
male with a mean age of 55±10 years. According to the epidemiological
studies the prevalence of bronchiectasis in india is 8.4% in the age group of 18-
65 years.
64
The current study was to analyse the correlation of variables in the study
population with extent of bronchiectasis. The variables were 1) FEV1/FVC 2)
HRCT 3) 6 Minute Walk Test 4) PAH 5) Modified Medical Research Council
Dyspnea Scale score 6) Modified BORG dyspnea scale score.
Based on the extent of bronchiectasis the patients were classified into 3
different groups. Which are cystic, cylindrical and varicose bronchiectasis.
Among the 3 groups 19 patients were in the cystic group ,11 were in the
cylindrical and 10 were in the varicose group. Cystic class of patients shows
more significant correlation with the variables than the other 2 groups.
The socio- demographic details were analysed and there was no significant
difference in the extent of bronchiectasis according to age or gender. The
average BMI was 22.47±5 and it was significantly correlated .
Singleton et al 87 patients found no statistical correlation between BMI and
bronchiectasis of patients. Ellis et al(36) in study conducted amongst 187
patients with bronchiectasis also found no significant correlation between BMI
and study groups.Similary no studies till date have proven the role of BMI in
assessing patients with bronchiectasis and correlating its significance in the
same.
Assessing the significance of smoking and alcohol intake in our study it was
found that,14 were smokers in 40 patients which was not statistically
significant with (p =0.443).Similarly alcohol intake while amongst the 40
65
patients had 5 patient had a history of alcohol intake. No significant correlation
was found between alcohol intake and study groups (p= 0.332).
Lindskog et al in 72 patients also reported similar findings that there was no
positive correlation between smoking and alcohol and the study groups.
Similarly no study has analyzed the relation between these parameters and
bronchiectasis. No significant correlation was found between alcohol intake
and study groups with( p = 0.327)
Cole et al (41)also reported similar findings that there was no positive
correlation between smoking and alcohol and study groups.Similarly no study
has analysed the relation between these parameters. Thus concluding that on
individual basis smoking and alcohol had no significance in differentiating
bronchiectasis and their presence could not be taken as a reliable indicator.
On analysing the symptomatology and nature of bronchiectasis, our study
found that 40 patients with breathlessness was seen in 25 patients(69.2%)cough
in 20 patients(46.2%),chest pain in 4 patients(30.8%) and hemoptysis 9
patients(2%).Correlating the symptomatology with bronchiectasis it was found
that symptomatology had no positive statistical significance.However all the
above mentioned studies concluded that symptomatology was inconclusive .
On analyzing haematological variables in our study,it was found that for
bronchiectasis group the mean values for haemoglobin (12.25 + 2.12),TLC
(9435+2234) , ESR (28.85+25.85)had no statistical significance in
differentiating bronchiectasis.There was no positive correlation between the
66
study groups on determining the haematological variables as was evidenced by
our study(P= 0.30).
Similar findings were noted by Perry et al(38) studied in 400 patients. Thus it
was proved that analysis of haematological parameters had no significant
impact on bronchiectasis. There was no study suggesting the haematological
variables have any effect in determining bronchiectasis.
CORRELATION OF NUMBER OF SEGMENTS INVOLVED AND
TYPE OF BRONCHIECTASIS
Among the 40 patients, most of the patient from cystic group showed more
number of segment involvement than other groups. There are 16 patients had
involvement of 3 segments and 3 had more than 4 segments involvement.
The current study shows no significance in correlation between the
radiological findings and extent of bronchiectasis. The patients in cystic group
shows negative correlation of (r = -0.03), which shows the extent of
bronchiectasis cant be predicated using radiological findings.
Mehmet A. Habesoglu et al in his study “Effect of radiological extent and
severity of bronchiectasis on pulmonary function” proved there is no
morphologic changes associated with bronchiectasis with lung function in
patients. He studied 71 patients, in that only 2 patient showed significant
radiological changes which was not significant.
67
CORRELATION OF HRCT SCORE WITH TYPE OF
BROCHIECTASIS
In our study the correlation between HRCT score and extent of bronchiectasis
showed significant correlation the cystic group of patients. The patients in
cystic group shows significant correlation with the HRCT findings (r=0.23) and
extent of bronchiectasis. The positive correlation of HRCT score was
statistically significant only in cystic group compared to others.
Gaik C. Ooi et al in his study “High-resolution ct quantification of
bronchiectasis: clinical and functional correlation” studied 60 patients in which
all patient underwent high resolution CT . This study establishes a link between
morphologic high-resolution CT parameters and clinical activity and emphasize
the role of bronchial wall thickening in patients with bronchiectasis.
68
CORRELATION OF TYPE OF BRONCHIECTASIS WITH
PULMONARY FUNCTION TEST (FEV1/FVC)
Among the 40 patients in the current study we observed a significant
correlation between the FEV1/ FVC and extent of bronchiectasis (p<0.05).
Patients were in cystic group those showed significant correlation with the
pulmonary function test while compared to cylindrical group.
The cystic group patient showed the significance with a p value of (P<0.05).our
study suggests that the severity of bronchiectasis can be predicated using the
pulmonary function tests.
Abdullaziz et al in the study “HRCT score in bronchiectasis: correlation with
pulmonary function with tests and pulmonary artery pressure” concluded that
there is a significantly lower FEV1/FVC in the cystic patients with a P value of
( p<0.0001).the mean of FEV1 and FVC % compared in cystic and cylindrical
group which shows significant difference in the mean values. In this study the
FEV1/FVC suggested as a diagnostic tool for bronchiectasis.
69
CORRELATION OF 6 MINUTE WALK TEST AND FEV1/FEC IN
STUDY POPULATION
In our study we analysed the significance of 6 minute walk test in correlation
with bronchiectasis. If the patients have significant PFT alteration , those
patients showed lowest score in 6 minute walk test.
The 6 minute walk test was found to be useful in patients with bronchiectasis in
predicting the severity. There is a positive correlation (r=0.25) between these
two factors in the entire study population and it was statistically significant
(p<0.01) .6 MWT is widely used to measure the functional status, used as
predictor in respiratory conditions.
In a study Lee et al in his study “ clinical determinants of the six minute walk
test in bronchiectasis” suggested that evidence of expiratory flow limitation,
which indicates dynamic hyperinflation and increased work of breathing are
responsible of disease. In this study evidence of airflow obstruction measured
by using FEV1 and FVC associated 6 minute walk test.
Jenkins et al in his study Six-minute walk test in pulmonary rehabilitation: do
all patients need a practice test?proven that Respiratory diagnosis influences
the magnitude of the learning effect for the 6MWT. The findings support the
recommendation of a practice 6MWT at baseline assessment in order to
provide an accurate measure of the effects of rehabilitation on 6MWD.
70
CORRELATION OF MODIFIED MEDICAL RESEARCH COUNCIL
DYSPNEA
SCALE (MMRC) WITH TYPE OF BRONCHIECTASIS
Among the study population while correlating the MMRC score there was
more patients coming under MMRC score of 2 . The patients in cystic group
showed a high MMRC score as compared to the cylindrical but it was not
statistically significant (p=0.8). the mean MMRC score in the study population
was 2.
There was studies suggesting that there is significant correlation between
MMRC and pulmonary function in obese patients. There was no study
supporting this correlation in stable bronchiectasis. In the current study MMRC
score was not showing any significant benefit in assessing the extent of
bronchiectasis.
71
CORRELATION OF MODIFIED BORG DYSPNEA SCALE SCORE
(BORG) WITH TYPE OF BRONCHIECTASIS
Among the study population while correlating the BORG score there was more
patients coming under the score of 4 . In the current study there was no
significant correlation between the BORG score and extent of bronchiectasis
(p=0.98). The mean score of the entire study population was 4.
Martinez gracia et al (n= 56) in their study “Dissociation of lung function,
dyspnea ratings and pulmonary extension in bronchiectasis” suggesting an
independent impact of BORG score in assessing the lung extent in
bronchiectasis.
72
CORRLATION OF HRCT SCORE WITH SEVERITY OF
PULMONARY ARTERY HYPERTENSION
In our study we analysed that pulmonary hypertension seen commonly in
advanced bronchiectasis ,particularly cystic disease. On analyzing our study
found that there is no significant correlation between HRCT score with
incidence of pulmonary hypertension.
Alzeer et al in his study “ right and left ventricular function and pulmonary
artery pressure in patient with bronchiectasis” 109 patients reported that 32.9%
of stable patients with bronchiectasis had pulmonary hypertension was higher
in cystic bronchiectasis with concomitant right and left ventricular
dysfunction.In this study SPAP was positively correlated with HRCT
score(r=0.23)Moreover high HRCT score not only reflects lung damage in
these patients,but it can also be associated with pulmonary hypertension.
Helbich et al, in his study “ evaluation of CT findings in cystic fibrosis”
reported similar findings that are correlated with score of all patients
(n=107).It has statistically significant positive relationship between the scores
and SPAP for all patients (p=<0.05)mean global score (8.67+ 2.9) for patients
whose SPAP value <40mmHg .
Abdullaziz et al (20) were in 94 patients ;62 were cystic and 32 were
cylindrical with mean age of 53.4+ 17.5 SD years. Forced vital capacity and
Forced expiratory volume 1 second (FEV1%)were lower in cystic
patients(p<0.0001)as compared with cylindrical patients.
73
David et al(16) in a study conducted in 261 patients with significant
bronchiectasis, it was found that score and extent of bronchiectasis have
comparison, but according to the other scores bronchial thickening
significantly decreased in studies. Silverman et al found in cystic disease were
found to have significantly higher HRCT score with other scores. Atilla et
al(41) in study conducted amongst 97 with patients with HRCT score is
increased in cystic type when comparing to other significant scores of HRCT.
74
CORRELATION TYPE OF BRONCHIECTASIS WITH PULMONARY
HYPERTENSION
In our study we analysed the incidence of systolic pulmonary artery pressure
was high in the study population .CT signs in bronchiectasis patients with
pulmonary hypertension showed enlarged of pulmonary artery. Some patients
with cystic bronchiectasis shows PAH but there was no significant correlation
between PAH and extent of bronchiectaisis in the current study. The correlation
coefficient showed positive correlation (r=0.07) but was not statistically
significant (p=0.9).
Devaraj et al , in his study “ pulmonary hypertension in patients with
bronchiectasis: prognostic significance of CT signs”studied on 91 patients
analysed that enlargement of pulmonary artery hypertension showed a highly
prognostic indicator in evaluation of patients with bronchiectasis.
Abdullaziz et al found that systolic pulmonary artery pressure was higher in
cystic bronchiectasis with right and left ventricular dysfunction.Study showed a
correlation between HRCT score and systolic pulmonary artery
hypertension.SPAP could be a predictor of future pulmonary hypertension.
In a study Hassan et al mentioned that right ventricular diameter was
significantly greater in cystic bronchiectasis and was positively correlated with
pulmonary hypertension. Study concluded that cystic bronchiectasis is
associated with more severe lung function impairment.
75
SUMMARY
In our study we included 40 patients in that 17 were male and 23
were female. The variables used in the study were age, gender, BMI, the HRCT
findings, pulmonary artery hypertension, 6 minute walk test, pulmonary
function test, MMRC score and BORG score.Among the 40 patients we
distributed the patients based on 3 different groups cystic, cylindrical and
varicose. We analysed sociodemographic variables found in bronchiectasis
There was a significant correlation between the pulmonary
function test and extent of bronchiectasis with (p<0.05)pulmonary
hypertension.As we compared to the other groups in cystic group the
correlation was more significant. Also the pulmonary function tests shows
significant positive correlation with HRCT score and 6 minute walk test.There
was a significant correlation between 6 minute walk test with extent of
bronchiectasis (r=0.25).There was no significant correlation between the extent
of involvement and pulmonary artery hypertension with extent of
bronchiectasis. Also the MMRC score and BORG score was not proved to be
an effective tool in assessing the extent of bronchiectasis.
76
LIMITATIONS
1. HRCT is the gold standard for diagnosing bronchiectasis, there is no
significant correlation between HRCT score and incidence of pulmonary
hypertension.
2.The gold standard for diagnosing pulmonary artery hypertension is Right –
heart catherisation, but in our study the severity of PAH was assessed by
Echocardiography,because Right heart-catherisation was invasive.
4. Eventhough six minute walk test was found to be useful in patients with
bronchiectasis in predicting the severity ,the test was difficult in patients with
severe pulmonary hypertension.
4.Sample size was less.
77
CONCLUSION
1. The patient with cystic bronchiectasis are develop pulmary artery hypertension
and MMRC score was higher in cystic group.
2. Pulmonary function test (FEV1/FVC and post FVC) has good significant
correlation and thereby it shows a strong predictor of Pulmonary hypertension.
3. 6Minute Walk Test (<400Mts) has good significant correlation.
4. Simple bedside and outpatient test like 6minute walk test/ Pulmonary Function
test can help to predict onset of pulmonary hypertension in bronchiectasis.
However further study need to be increase the sample size and use of Bio-
Markers.
BIBLIOGRAPHY
1. CROFTONS AND DOUGLAS’S Textbook of Respiratory Diseases /5th
Edition/Chapter 28/pg;794-828
2. Reid L.Reduction in bronchial subdivisions in bronchiectasis.Thorax
1950;223-247
3. Whitwell.F .A study of the pathology and pathogenesis of
bronchiectasis.Thorax 1952:7:
4. Nictora MB,Rivera M,Dale AM et al,Clinical ,pathophysiologic,and
microbiologic characterization of bronchiectasis in an aging cohort.Chest
1995;108:955-961
5. Field .E.Bronchiectasis :a long term followup of medical and surgical cases
from childhood.Arch Dis child 1961;36: 587-603
6. Currie DC,Cooke JC,Morgan AD,et al.Interpretation of bronchograms and
chest radiographs in patients with chronic sputum production.Thorax
1987;42: 278-284
7. Weycker D,Edelsberg J,Oster G, et al. Prevalence and economic burden of
bronchiectasis.Clinical Pulm Medicine 2005,4:205-209
8. Barker AF. Bronchiectasis.N Engl J Med 2002; 346:1383-1393
9. Naidich DP,McCauley DI, Khouri NF,et al. Computed tomography of
bronchiectasis.J Comput Assist Tomogr 1982; 6: 437-444
10. Naidich DP, McGuinness G, CT of Airways disease and
bronchiectasis.Radiol Clin North Am 2002; 40: 1-19
11. Clinical Respiratory Medicine, Stephen G.Spiro , Gerard A.Silvestri,Alvar
Agusti ,4th Edition.Pg:580-587,710-721.
12. Loukides S,BourosD, Papatheodorou G et al, Relationship with Cellular
composition in induced sputum,spirometery and extent and severity of
disease. Chest 2002;121: 81-87
13. King PT,Holdsworth SR,Freezer NJ,et al.Outcome in adult bronchiectasis.J
Chron Obstruct Pulmon Dis 2005;2: 27-34
14 .King P,Holdsworth S, Freezer N ,et al.Bronchiectasis .Intern Med J 2006;36:
729- 737.
15. Murray and Nadel’s –Textbook of Respiratory disease /5th Edition/Vol : 1/pg
1023 - 1046
16. David A. Lynch, John Newell, Valerie Hale et al,Correlation of CT findings
with Clinical evalauation in 261 patients with symptomatic Bronchiectasis
AJR:173:53-58 ,July 1999
17. R.E.Sheehan,A.U.Wells,S.J Copley. A Comparison of serial computed
tomography and functional change in bronchiectasis.Eur Respir J.2002;
20:581-587
18. Mehmet Gencer,Erkan Ceylan,Remzi Yilmaz.Impact of bronchiectasis on
right and left ventricular functions.Respiratory medicine (2006)100, 1933-
1943
19 .Paul T.King, Stephen R ,Holdswort, Nicholas J.Freezer, Elmer Villanueva,
Peter W.Holmes et al,Characterisation of the Onset and presenting clinical
features of adult Bronchiectasis..Respiratory Medicine (2006)100,2183-2189
20. Abdulaziz H.Alzeer HRCT Score in bronchiectasis: Correlation with
Pulmonary function tests and pulmonary artery pressure,Annals of
Thoracic medicine –Vol -3 Issue 3,July- September 2008
21 . Anand Devaraj,Athol U Wells,Mark G Meister, Pulmonary Hypertension in
Patients with bronchiectasis. Prognostic significance of CT sigh.AJR
2011;196:1300-1304
22 . Mehmet Ali,Aylin Ozsancak and Fusun Oner .Clinical ,Radiologic,and
Functional evaluation of 304 patients with bronchiectasis.Amm Thorac
Med .2008 Jul-Sep ;3(3)82-86
23. Wafaa Ali Hassan,Ibraheem Shalan,Hythan Abd Allah. Role of a diagnostic
triad in bronchiectasis 29 March 2015.Egyptian Journal of Chest Disease and
Tuberculosis
24. Bethany Milliron ,Travis S.Henry,Srihari ,Brent P.Little et al,Bronchiectasis :
Mechanisms and Imaging Clues of Associated Common and uncommon
Disease,Vol;35,1-20
25. Serpil Ocal,Oytun Portakal,Arshan Ocal,Ahmet Ugur Demir,Arzu Topeli
,Lutfi Coplu et al ,Elsevier Article , Factors associated with pulmonary
hypertension and long –term survival in bronchiectasis subjects
.Respiratory medicine 119(2016)109-114
26. Enid Silverman, Linda Ebright ,Marianne Kwiatkowski et al, Current
Management of bronchiectasis :Review and 3 case studies,Vol.32 Heart
Lung (R) 2003; 59- 64
27. H R Roberts, A U Wells, D G Milne,P.J Cole et al,Airflow Obstruction in
bronchiectasis : Correlation between Computed tomography features and
Pulmonary function Tests,Thorax 2000; 55:198-204
28. N.Galie,M.M Hoeper,M.Humbert,A.Torbicki et al, Guidelines for diagnosis
and Treatment of pulmonary hypertension .European Heart Journal 2009;
30:2493-2537
29. Dimitar Sajkov,Bliegh Mupunga,Jeffrey J.Bowden and Nikolai et al,
Pulmonary hypertension in Chronic Lung disease and / or Hypoxia 2013
Chapter 2
30. Eysmann SB,Palevsky HI,Reichek N,et al,Two –dimensional and Doppler –
echocardiographic and Cardiac catherization correlates of survival in primary
pulmonary hypertension .Circulation 1989;80:353-360
31. Raymond RJ,hinderliter AL ,Willis PW, et al.Echocardiographic predictors of
adverse outcomes in primary pulmonary hypertension.J.AM Coll Cardiol
2002;39:1214-1219
32. Herve P,Humbert m,Sitbon O,et al. Pathobiology of Pulmonary
hypertension;The role of platelets and thrombosis.Clin Chest med 2001;22:
451- 458
32. Miyamoto S,Nagaya N,Satoh T et al,Clinical correlates and Prognostic
significance of Six –minute walk test in patients with primary pulmonary
hypertension.comparison with cardiopulmonary exercise testing. Am J,
Respir Crit Care Med 2000;161: 487-492
33. A.L.Lee,B.M .Button ,S.Ellis,A.E.Holland et al,Clinical determinants of the 6-
Minute Walk Test in bronchiectasis, 2009 Respiratory Medicine,103:780-785.
34. Chang AB,Grimwood K, Mulholland EK et al.Bronchiectasis in indigenous
children in remote communities.Med J Aust 2002;177: 200-204
35. Singleton R,,Morris A,Redding G ,et al.Bronchiectasis causes and clinical
courses.Pediatr Pulmonol 2000;29:182-187
36. Ellis DA,Thornley PE,Wightman AJ et al.Present outlook in bronchiectasis :
clinical and social study and review of factors influencing prognosis.Thorax
1981; 36:659- 664
37. Lindskog G,Hubbell D An analysis of 215 cases of
bronchiectasis,1955;100:643-650
38. Perry K,King D. Bronchiectasis a study of prognosis based on a follow up of
400 patients Am Rev Tuberc 1940;41:531-548
39. Hogg JC, Chu F, Utokaparch S, et al. The nature of small-airway obstruction
in chronic lung disease. N Engl J Med2004; 350:2645,2653
40. King PT,Holdsworth S,Farmer MW,et al.Characterisation of onset and
presentating clinical features of adult bronchiectasis.Respir Med 2006 ;100:
2183-2189
41. Orr R,Smith,L .J &Cuttica, M.J.Pulmonary Hypertension in advanced chronic
obstruction pulmonary disease.Curr Opin Pulm Med2012,18(2),138-143
42. Xu,X-Q & Jing ,Z- c.High altitude pulmonary hypertension .Eur Respir Rev
2009,18 (111),13-17.
43. Sylvester, J.T,Shimoda,L.A,Aaronson,P.I & Ward,J.PHypoxicPulmonary
vasoconstriction Physiol Rev(2012).92(1).367-520
44.. Bosc L.V,Resta.T,Walker,B, & Kanagy,N.L.Mechanisms of intermittent
hypoxia induced hypertension .J Cell Mol med (2010)
45. Sommer .N,Dietrich, A,Schermuly, R.T,Ghofrani,H.A, Gudermann,
T,Schulz,R,et al.Regulation of hypoxic pulmonary vasoconstriction: Basic
mechanisms.Eur Respir.J (2008) 32 (6),1639-1651
ANNEXURES
PFT - Pulmonary function Test
HRCT - High Resolution Computed Tomography
PAH - Pulmonary Artery Hypertension
FVC - Forced vital capacity
FEV1 - Forced Expiratory volume at 1 second
MMRC - Modified Medical Research Council
BORG - BORG Dyspnea scale
6MWT - Six minute Walk test
PSG Institute of Medical Science and Research, Coimbatore Institutional Human Ethics Committee
INFORMED CONSENT FORMAT FOR STUDENT RESEARCH PROJECTS I NAJMA MUHAMMED.K MD(Respiratory Medicine) 2015 batch PG student of the PSG Institute of Medical Sciences & Research (PSG IMS&R), I am carrying out a study on the topic To Correlate Clinicoradiological Characteristics of Bronchiectasis With Pulmonary Hypertension. as part of my student research project being carried out under the aegis of the Department of Respiratory Medicine My /Our research guide is : Dr.Anupama Murthy.K Designation : Professor and Head,
Department of respiratory Medicne The justification for this study is: COPD occurs worldwide,but it is a major health problem principally in societies where smoking is common.Its incidence is on the rise and WHO estimates that by 2020 it will be the 5th most prevalent disease worldwide and 3rd most common cause of death.COPD is a systemic disease with various extrapulmonary manifestations of which cardiac complication forms the leading cause of mortality and morbidity.so by early assessment of cardiac function by echocardiography, which is one of the best non invasive tests, prompt management can be initiated and helps in monitoring the patient. The aims of this study are: To correlate clinicoradiological characteristics of
bronchiectasis with pulmonary hypertension and to correlate the spirometric findings
with echocardiographic changes.
Sample size : 40. Respondents are (population group & age group): ____________________. Location : Department of Respiratory Medicine, PSG-IMSR. We request you to kindly cooperate with us in this study. We propose collect background information and other relevant details related to this study. We will be carrying out (strike off items that are not applicable): Initial interview (specify approximate duration):_ 10 minutes.
Health education sessions: Number of sessions: _ ONE. Approximate duration of each session: _ 10 minutes. Clinical examination (Specify details and purpose): YES, General and system wise examination as a part of routine work up. Echocardiogram : To assess pulmonary hypertension 6MWT Pulmonary Function Test : To determine physiological parameters BORG Scale,MMRC Blood sample collection : NA Specify purpose, discomfort likely to be felt and side effects, if any: Medication given, if any, duration, side effects, purpose, benefits: Final interview (specify approximate duration):_________ mts. If photograph is taken, purpose: Benefits from this study, if any: How the results will be used: If you are uncomfortable in answering any of our questions during the course of the interview / biological sample collection, you have the right to withdraw from the interview / study at anytime. You have the freedom to withdraw from the study at any point of time. Kindly be assured that your refusal to participate or withdrawal at any stage, if you so decide, will not result in any form of compromise or discrimination in the services offered. You will continue to have access to the regular services offered to a patient. You will NOT be paid any remuneration for the time you spend with us for this interview / study. The information provided by you will be kept in strict confidence. Under no circumstances shall we reveal the identity of the respondent or their families to anyone. The information that we collect shall be used for approved research purposes only. Consent: The above information regarding the study, has been read by me/ read to me, and has been explained to me by the student investigators from the PSG IMS&R. Having understood the same, I hereby give my consent to them to interview me. I affixing my signature / left thumb impression to indicate my consent and willingness to cooperate in this study. Respondent ID: _________. Signature / Left thumb impression of the Respondent. Signature of the Interviewer with date
Thesis Project
Title : Clinico Radiological Correlation of Bronchiectasis with Pulmonary Hypertension
Department of Respiratory medicine
PSG IMSR
Case Record Form
Name: ………………………………………. Informant: …………………………............
Age / sex: …………………………………… CRC. No : ………………………………….
Father’s / Husband’s name: …………………………………………………………………………...
Address: ……………………………………... Height: …………. Weight: ……………....
………………………………………………... BMI: ………………………………………
………………………………………………... PSG OP No: ________________________
Marital status: Married Unmarried Widow/widower
No. of family members: …………………… Adults ………. Children ……… (< 12 years)
Dwelling {lived for most part (>70%) of the subject’s life} Urban / Rural/High altitude
Education : Illiterate Read & write
Primary school High school
Higher secondary Graduate
Postgraduate Professional / Fellow / Doctorate
Occupation : employed unemployed retired housewife
Present : ………………………………………………… Duration : …………………
Past : (1) ………………………………………… Duration : …………………
(2) ………………………………………... Duration : …………………
Total monthly family income: ………………………
What is your contribution to total monthly family income? …………………… %
Socioeconomic status(Modified prasad’s classification):
Personal History :
Diet: vegetarian / mixed
If mixed diet how frequently you take animal food?
Daily / weekly / fortnightly / monthly / occasional
Smoking: Yes / No ( presence of regular smoking for at least one year and / or smoked at
least 100 cigarettes / beedies / others in his / her lifetime)
If yes, beedi/ cigarette/ hukka /others
No of beedies / cigarettes per day ………………………….
Age at started …………………………………………………
If ex-smoker, when stopped …………………………………
Alcohol : Yes / No
If yes, Quantity ……………………ml
Frequency ……………………
If stopped when …………………………..
Other informations : Drugs / narcotics abuse
Tobacco / pan chewing
Sexual promiscuity
Disease specific details : Bronchiectasis/Pulmonary Hypertension
Primary Symptoms:
Cough……………………………………………………………………….
Sputum(colour,quantity,foul smelling)……………………………………..
Breathlessness……………………………………………………………….
Hemoptysis…………………………………………………………………..
Chest Pain…………………………………………………………………….
Fever………………………………………………………………………….
Wheeze………………………………………………………………………..
Other symptoms:
Upper respiratory symptoms…………………………………………………..
Weight loss…………………………………………………………………….
Growth retardation…………………………………………………………….
Gastrointestinal symptoms……………………………………………………..
Infertility………………………………………………………………………..
History suggestive of asthma……………………………………………………
Details(Age,Duration,Family history)………………………………………….. …………………………………………………………………………………..
……………………………………………………………………………………
Type of medications Inhaled/Dry powered
In ABPA – h/o oral steroids
h/o high inhaled steroids
Treatment Details
Duration of respiratory symptoms suggestive of bronchiectasis
When was the diagnosis established with HRCT
Are you on any treatment for respiratory symptoms ?............Yes/No
If yes………………………………………………………………………
Treatment Details:
Medical Treatment:
Antibiotic’s used………..…..YES/NO
If yes duration & frequency……………………………………………………………………………
Bronchodilators- Inhaled/Oral &Duration……………………………………………………………..
Mucolytics………………………………………………………………………………………………Steroids used…………………..YES/NO
Postural drainage………………………………………………………………………………………..
Vaccination……………………………………………………………………………………………..
Pulmonary vasodilators used …….YES/NO
If yes details…………………………………………………………………………………………….
Oxygen therapy…………………YES/NO
If yes short burst or LTOT
Surgical Treatment……………...YES/NO
If yes give details ………………………………………………………………………………………
Details of exacerbation for bronchiectasis:
No. of ED visits for an acute exacerbation in the past one year (both PSG and GP clinics / hospitals)
( In the past one year, have you ever received emergency injectables / nebulized bronchodilators for your respiratory illness, in emergency departments of any hospitals / GP clinics? )
No ED visit ≤ 5 ED visits (…………..) >5 ED visits (………....)
No. of hospitalizations:
mm / yy
Reason
duration
ICU stay
Mech vent
Remarks
Past history / Co-existing illness:
Infection - Tuberculosis /Measles/Bacterial/Viral/Retroviral……………………………….. …………… Congential Disease………………………………………………………………………………………….. Lung Disease –COPD/ILD/Sleep disorder/Developmental abnormalities………………………………. Allergic Rhinitis/Sinusitis………………………………………………………………………………… Congenital heart disease /LVD/Valvular heart disease/Hypertension GERD / Acid peptic disease………………………………………………………………………………… Diabetes mellitus……………………………………………………………………………………………. Hypo/hyperthyroidism……………………………………………………………………………………… Other endocrine disorders…………………………………………………………………………………... Connective tissue disorder……………………………………………………………………………. Metabolic disorder…………………………………………………………………………………………….. Cerebro vascular diseases…………………………………………………………………………………... Kidney diseases……………………………………………………………………………………………... Obstetric history / Gynecological illnesses…………………………………………………………........... Surgical illnesses .………………………………………………………………………………………… Congenital anomalies……………………………………………………………………………………….. Others………………………………………………………………………………………………………..
Family History: (mention relationship where relevant)
Atopic diseases……………………………………………………………………………………………... Hypertension………………………………………………………………………………………………... Diabetes mellitus……………………………………………………………………………………………. Hypo/hyperthyroidism……………………………………………………………………………………… Other endocrine disorders…………………………………………………………………………………... Lung diseases ………………………………………………………………………………………………. Heart diseases……………………………………………………………………………………………….. Kidney diseases……………………………………………………………………………………………... Obstetric history / Gynaecological illnesses…………………………………………………………........... Surgical illnesses……………………………………………………………………………………………. Congenital anomalies………………………………………………………………………………………
Congenital disease – Cystic fibrosis/ Kartagener’s/ Young’s/
Hypogammaglobulenemia………………………………………………………………………
Alpha1antitrypsindeficiency………………………………………………………………………….
Others……………………………………………………………………………………… Malignancy………………………………………………………. Foreign body aspiration/Inhalation of toxic fumes………………………………………………………. Infertility…………………………………………………………………………………… Others………………………………………………………………………………………………………..
Physical examination
1. Vitals:
Pulse rate: …………………….. Respiratory rate: …………………….
B.P.: …………………………. Temperature: ………………………..
O2 saturation: ………………...
2. General examination:
Built Pallor cyanosis clubbing JVP Edema Lymph nodes
3. Respiratory system:
4. Cardiovascular System:
5. Others system
INVESTIGATIONS:
Hemogram Hb
TC DC
Platelet ESR
Sr.Urea Sr.Creatine
Urine Routine
X-ray chest PA view:
Normal /Abnormal
Unilateral/Bilateral
Zone Involved
Upper Mid Lower
Appearance Tooth paste Tramline FingerGlove Sign Honeycomb
Pulmonary function test:
Spirometry: prebronchodilator postbronchodilator
FVC
FEV1
FEV1/ FVC
ECHO EF RA /RV dilation RVSP
Others
HRCT Lungs Lobe involved upper middle Lower
Type
Unilateral /Lateral
Bronchial dilation
Associated features:

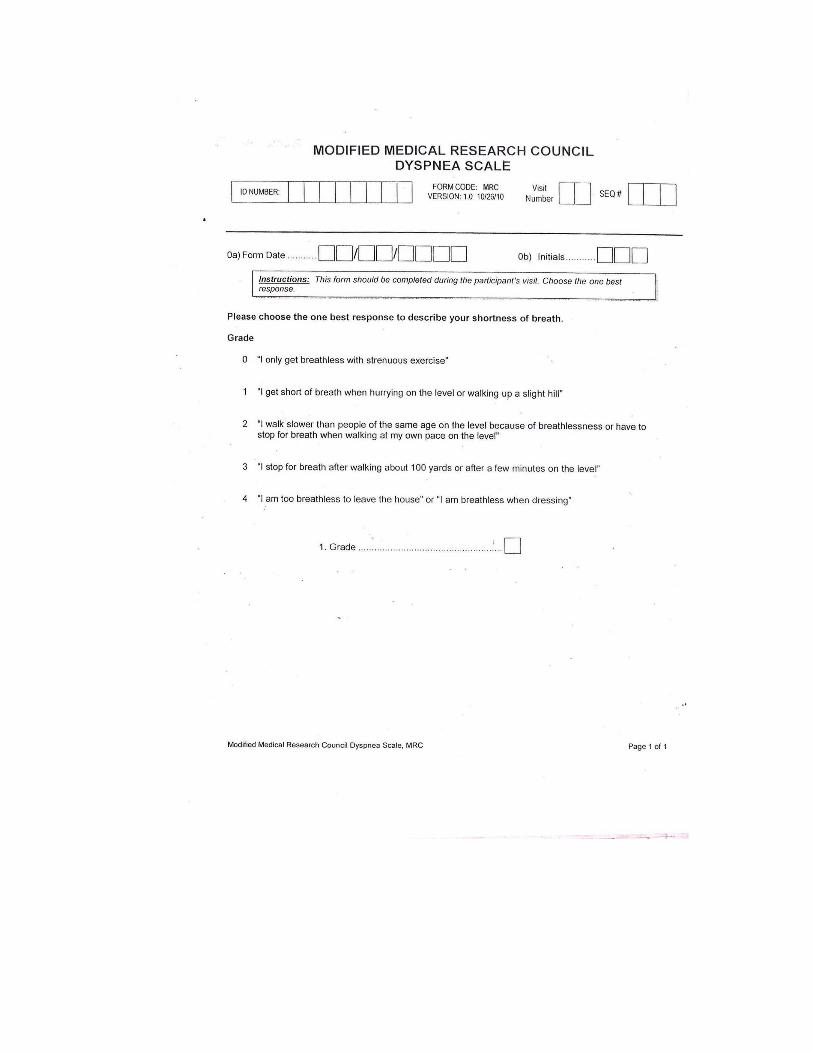
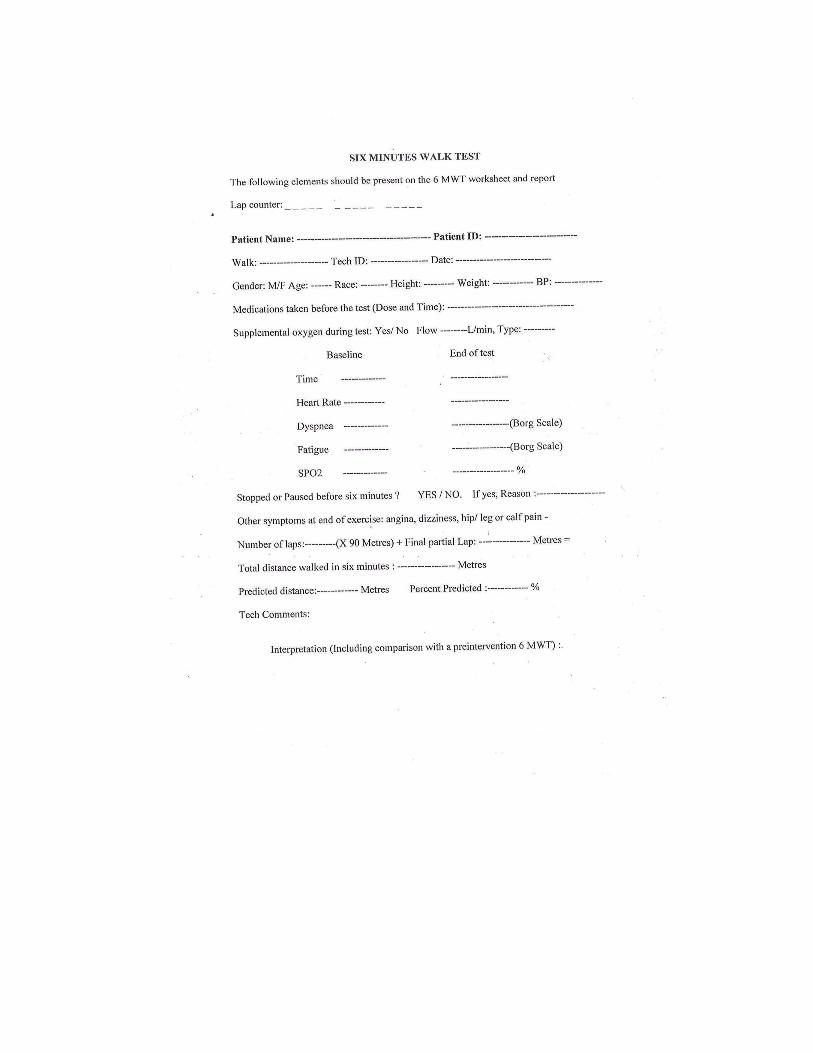
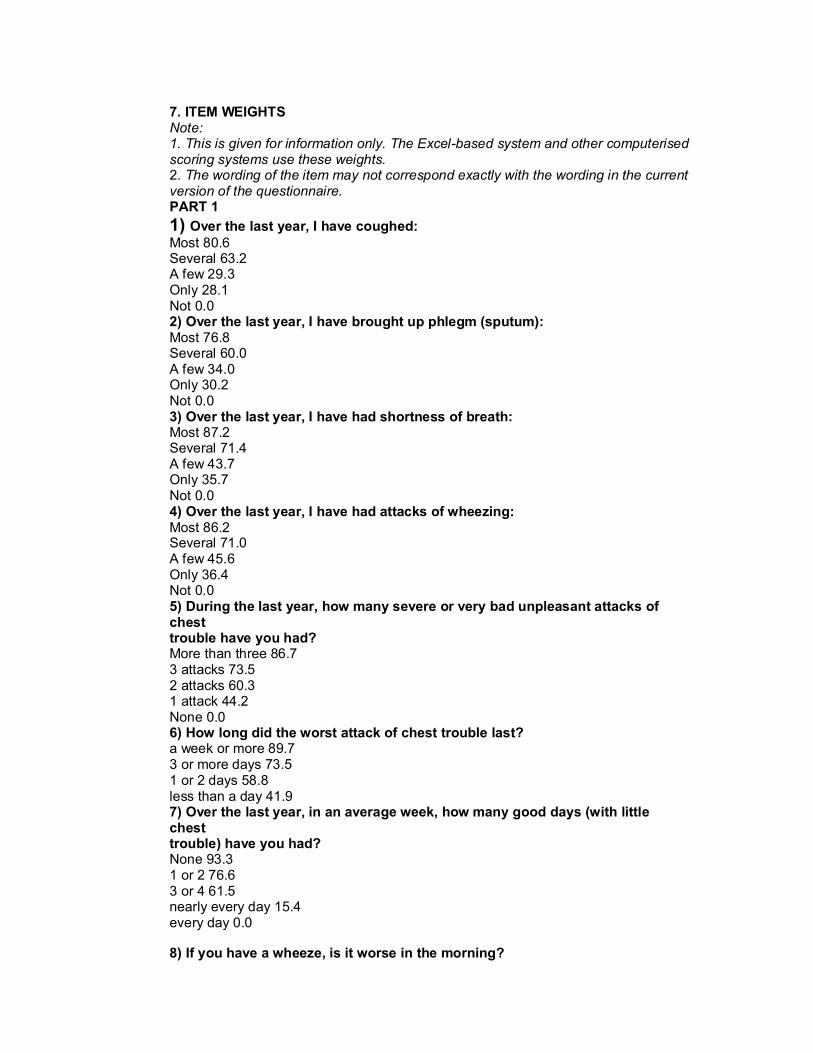
7. ITEM WEIGHTS Note: 1. This is given for information only. The Excel-based system and other computerised scoring systems use these weights. 2. The wording of the item may not correspond exactly with the wording in the current version of the questionnaire. PART 1 1) Over the last year, I have coughed: Most 80.6 Several 63.2 A few 29.3 Only 28.1 Not 0.0 2) Over the last year, I have brought up phlegm (sputum): Most 76.8 Several 60.0 A few 34.0 Only 30.2 Not 0.0 3) Over the last year, I have had shortness of breath: Most 87.2 Several 71.4 A few 43.7 Only 35.7 Not 0.0 4) Over the last year, I have had attacks of wheezing: Most 86.2 Several 71.0 A few 45.6 Only 36.4 Not 0.0 5) During the last year, how many severe or very bad unpleasant attacks of chest trouble have you had? More than three 86.7 3 attacks 73.5 2 attacks 60.3 1 attack 44.2 None 0.0 6) How long did the worst attack of chest trouble last? a week or more 89.7 3 or more days 73.5 1 or 2 days 58.8 less than a day 41.9 7) Over the last year, in an average week, how many good days (with little chest trouble) have you had? None 93.3 1 or 2 76.6 3 or 4 61.5 nearly every day 15.4 every day 0.0
8) If you have a wheeze, is it worse in the morning?
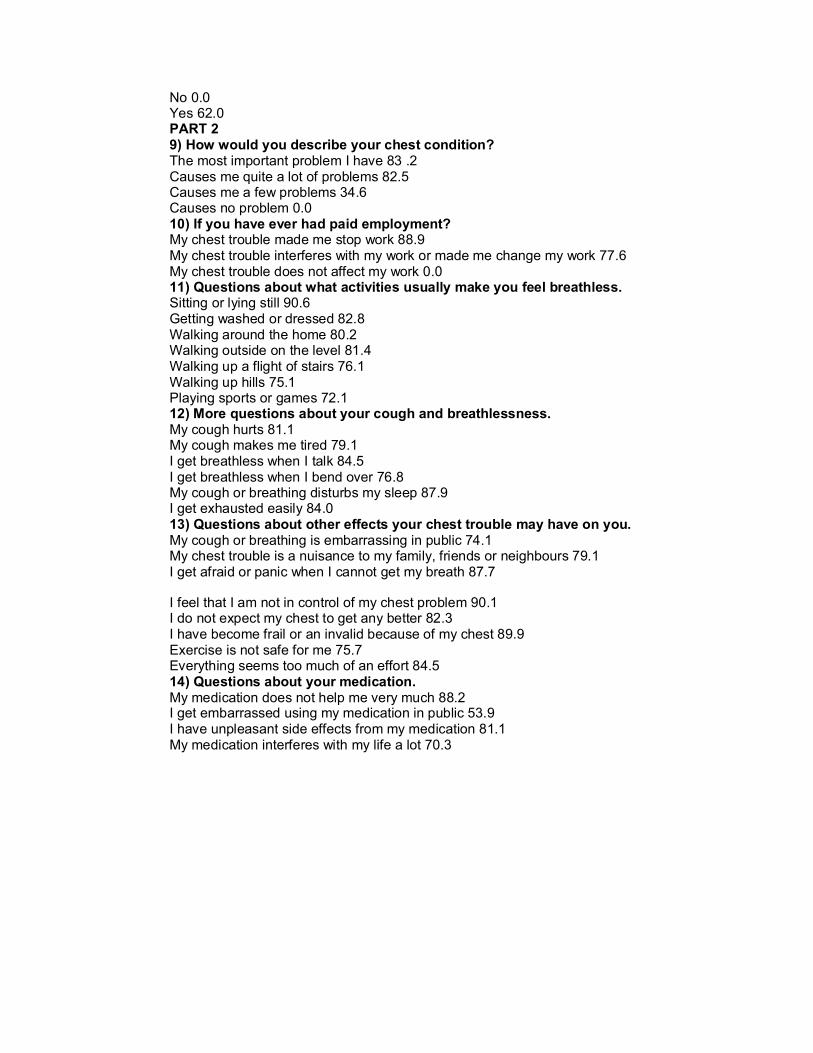
No 0.0 Yes 62.0 PART 2 9) How would you describe your chest condition? The most important problem I have 83 .2 Causes me quite a lot of problems 82.5 Causes me a few problems 34.6 Causes no problem 0.0 10) If you have ever had paid employment? My chest trouble made me stop work 88.9 My chest trouble interferes with my work or made me change my work 77.6 My chest trouble does not affect my work 0.0 11) Questions about what activities usually make you feel breathless. Sitting or lying still 90.6 Getting washed or dressed 82.8 Walking around the home 80.2 Walking outside on the level 81.4 Walking up a flight of stairs 76.1 Walking up hills 75.1 Playing sports or games 72.1 12) More questions about your cough and breathlessness. My cough hurts 81.1 My cough makes me tired 79.1 I get breathless when I talk 84.5 I get breathless when I bend over 76.8 My cough or breathing disturbs my sleep 87.9 I get exhausted easily 84.0 13) Questions about other effects your chest trouble may have on you. My cough or breathing is embarrassing in public 74.1 My chest trouble is a nuisance to my family, friends or neighbours 79.1 I get afraid or panic when I cannot get my breath 87.7
I feel that I am not in control of my chest problem 90.1 I do not expect my chest to get any better 82.3 I have become frail or an invalid because of my chest 89.9 Exercise is not safe for me 75.7 Everything seems too much of an effort 84.5 14) Questions about your medication. My medication does not help me very much 88.2 I get embarrassed using my medication in public 53.9 I have unpleasant side effects from my medication 81.1 My medication interferes with my life a lot 70.3
15) Questions about how activities may be affected by your breathing. I take a long time to get washed or dressed 74.2 I cannot take a bath or shower, or I take a long time 81.0 I walk more slowly than other people, or I stop for rests 71.7 Jobs such as housework take a long time, or I have to stop for rests 70.6 If I walk up one flight of stairs, I have to go slowly or stop 71.6 If I hurry or walk fast, I have to stop or slow down 72.3 My breathing makes it difficult to do things such as walk up hills, carry things up stairs, light gardening such as weeding, dance, play bowls or play golf 74.5 My breathing makes it difficult to do things such as carry heavy loads, dig the garden or shovel snow, jog or walk at 5 miles per hour, play tennis or swim 71.4 My breathing makes it difficult to do things such as very heavy manual work, run, cycle, swim fast or play competitive sports 63.5
16) We would like to know how your chest trouble usually affects your daily life. I cannot play sports or games 64.8 I cannot go out for entertainment or recreation 79.8 I cannot go out of the house to do the shopping 81.0 I cannot do housework 79.1 I cannot move far from my bed or chair 94.0 17) Tick the statement which you think best describes how your chest affects you. It does not stop me doing anything I would like to do 0.0 It stops me doing one or two things I would like to do 42.0 It stops me doing most of the things I would like to do 84.2 It stops me doing everything I would like to do 96.7
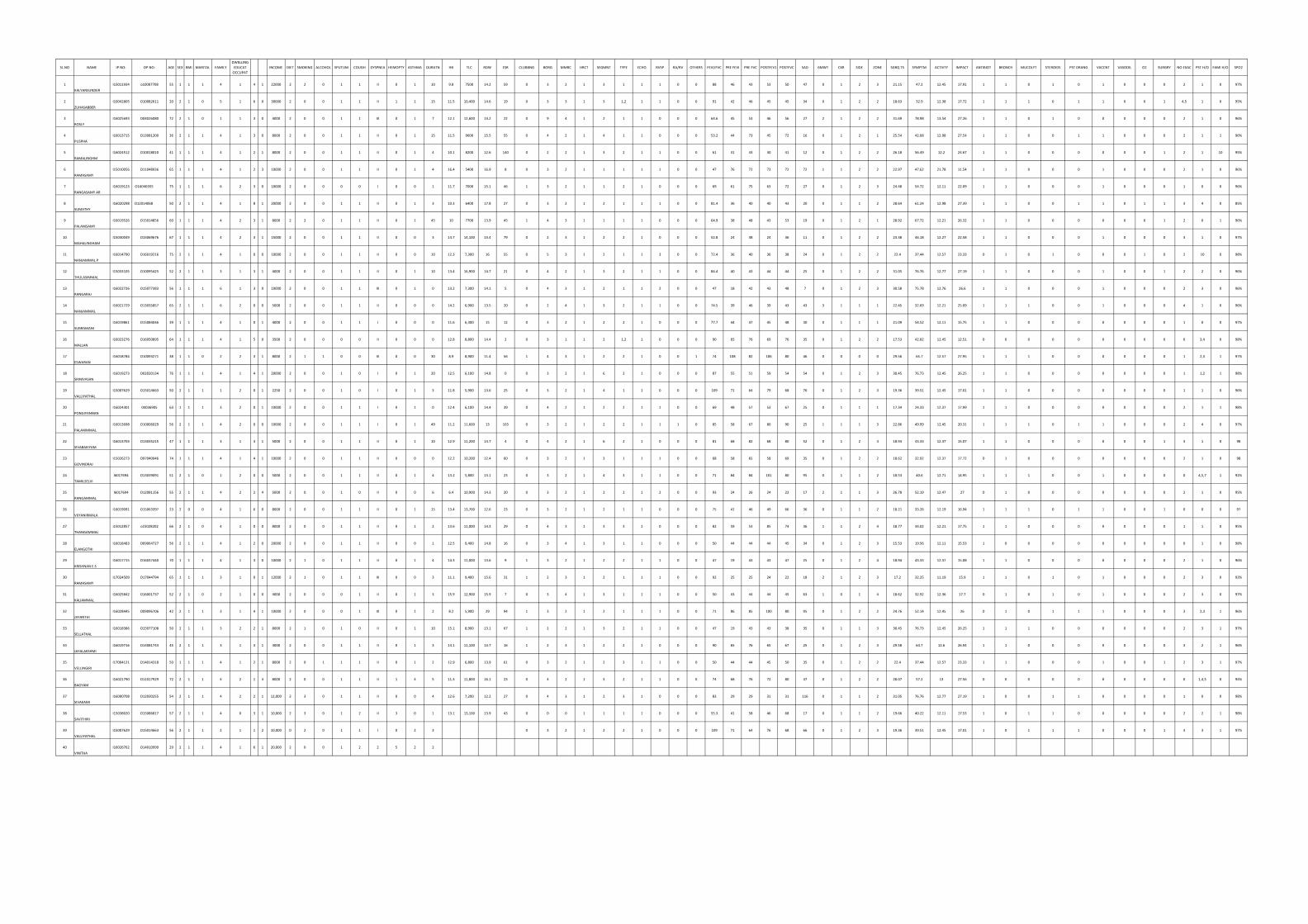
SL.NO NAME IP NO: OP NO: AGE SEX BMI MARITAL FAMILYDWELLING
EDUCAT OCCUPAT
INCOME DIET SMOKING ALCOHOL SPUTUM COUGH DYSPNEA HEMOPTY ASTHMA DURATN HB TLC RDW ESR CLUBBNG BORG MMRC HRCT SEGMNT TYPE ECHO RVSP RA/RV OTHERS FEVI/FVC PRE FEVI PRE FVC POSTFEV1 POSTFVC SAD 6MWT CXR SIDE ZONE SGRQ TS SYMPTM ACTIVTY IMPACT ANTIBIOT BRONCH MUCOLYT STEROIDS PST DRANG VACCNT VASODIL O2 SURGRY NO EXAC PST H/O FAMI H/O SPO2
1KALYANSUNDER
I15011934 o10007708 55 1 1 1 4 1 4 1 22000 2 2 0 1 1 II 0 1 10 9.8 7500 14.2 59 0 3 2 1 3 1 1 1 0 0 88 46 43 53 50 47 0 1 2 3 21.15 47.2 12.45 17.91 1 1 0 1 0 1 0 0 0 2 1 0 97%
2ZUHASABBER
I10042805 O10082611 20 2 1 0 5 1 6 0 30000 2 0 0 1 1 II 1 1 15 11.5 10,400 14.6 19 0 3 3 1 3 1,2 1 1 0 0 91 42 46 45 45 34 0 1 2 2 18.63 32.9 12.38 17.72 1 1 1 0 1 1 0 0 1 4,5 1 0 95%
3ROSLY
I16025693 O04026080 72 2 1 0 1 1 3 0 4000 2 0 0 1 1 III 0 1 7 12.1 12,600 14.2 22 0 9 4 1 2 1 1 0 0 0 64.6 45 53 46 56 27 2 1 2 2 31.69 78.98 13.54 27.26 1 1 0 1 0 0 0 0 0 2 1 0 96%
4PUSPHA
I16013715 O13081200 36 2 1 1 4 1 3 0 8000 2 0 0 1 1 II 0 1 15 11.5 9600 15.5 55 0 4 2 1 4 1 1 0 0 0 53.2 44 73 45 72 16 0 1 2 1 25.54 42.08 12.98 27.54 1 1 0 0 1 1 0 0 0 2 1 1 96%
5RAMALINGHM
I16024512 O10018010 41 1 1 1 4 1 2 1 8000 2 0 0 1 1 II 0 1 4 10.1 8200 12.6 140 0 2 2 1 3 2 1 1 0 0 61 31 43 30 41 12 0 1 2 2 26.18 56.49 12.2 24.67 1 1 0 0 0 0 0 0 1 2 1 10 95%
6RAMASAMY
I15010056 O11048936 65 1 1 1 4 1 2 3 10000 2 0 0 1 1 II 0 1 4 16.4 5400 16.9 8 0 3 2 1 1 1 1 1 0 0 47 76 72 73 72 72 1 1 2 2 22.97 47.62 21.78 11.54 1 1 0 0 0 1 0 0 0 2 1 0 96%
7RANGASAMY AR
I16019123 O16040355 75 1 1 1 6 2 3 0 10000 2 0 0 0 0 I 0 0 1 11.7 7000 15.1 46 1 3 2 1 1 2 1 0 0 0 69 61 75 63 72 27 0 1 2 3 24.48 54.72 12.11 22.09 1 1 0 0 0 1 0 0 0 1 0 0 96%
8SUMATHY
I16020298 O12014068 50 2 1 1 4 1 8 1 20000 2 0 0 1 1 II 0 1 3 10.3 6400 17.8 27 0 3 2 1 2 1 1 1 0 0 81.4 36 40 40 43 20 0 1 1 2 28.64 61.24 12.98 27.39 1 1 0 0 1 1 0 1 1 3 4 0 85%
9PALANISAMY
I16019526 O15014856 60 1 1 1 4 2 3 1 8000 2 2 0 1 1 II 0 1 45 10 7700 13.9 45 1 4 3 1 1 1 1 0 0 0 64.9 38 48 43 53 19 0 1 2 1 28.92 67.72 12.21 26.32 1 1 0 0 0 0 0 0 1 2 0 1 96%
10MAHALINGHAM
I15030049 O15069676 67 1 1 1 4 2 3 1 15000 2 0 0 1 1 II 0 0 3 14.7 14,100 13.4 79 0 2 3 1 2 2 1 0 0 0 52.8 24 38 24 36 11 0 1 2 2 23.38 46.18 12.27 22.58 1 1 0 0 0 1 0 0 0 3 1 0 97%
11NANJAMMAL P
I16014790 O16019216 75 2 1 1 4 1 0 0 10000 2 0 0 1 1 II 0 0 10 12.3 7,300 16 55 0 5 3 1 2 1 1 3 0 0 72.4 36 40 36 38 24 0 1 2 2 22.4 37.44 12.57 23.33 0 1 0 1 0 0 0 1 0 2 10 0 98%
12THULASIMMAL
I15033105 O10095425 52 2 1 1 3 1 3 1 4000 2 0 0 1 1 II 0 1 10 13.4 16,900 14.7 21 0 4 2 1 3 2 1 1 0 0 84.4 40 43 44 44 25 0 1 2 2 31.05 76.76 12.77 27.19 1 1 0 0 0 1 0 0 1 2 2 0 96%
13RANGARAJ
I16022726 O15077383 56 1 1 1 6 1 3 0 10000 2 0 0 1 1 III 0 1 0 13.2 7,300 14.1 5 0 4 3 1 2 1 1 2 0 0 47 18 42 43 48 7 0 1 2 3 30.58 75.78 12.76 26.6 1 1 0 0 0 1 0 0 0 2 3 0 96%
14NANJAMMAL
I16021729 O13035857 65 2 1 1 6 2 0 0 5000 2 0 0 1 1 II 0 0 0 14.2 6,900 13.5 20 0 2 4 1 3 2 1 1 0 0 74.5 39 46 39 43 43 3 1 1 1 22.45 32.69 12.21 25.09 1 1 1 0 0 1 0 0 0 4 1 0 96%
15SUBRAMANI
I16019861 O15084046 39 1 1 1 4 1 0 1 4000 2 0 0 1 1 I 0 0 0 11.6 6,300 15 12 0 3 2 1 2 2 1 0 0 0 77.7 44 47 45 48 30 0 1 1 1 21.09 54.52 12.11 15.75 1 1 0 0 0 0 0 0 0 1 0 0 97%
16MALLAN
I16023276 O16050895 64 1 1 1 4 1 5 0 3500 2 0 0 0 0 II 0 0 0 12.8 8,800 14.4 2 0 3 1 1 2 1,2 1 0 0 0 90 65 76 69 76 35 0 1 2 2 17.53 42.82 12.45 12.51 0 0 0 0 0 0 0 0 0 0 3,4 0 98%
17ESWARAN
I16018784 O10093271 38 1 1 0 2 2 3 1 8000 2 1 1 0 0 III 0 0 30 8.9 8,900 11.4 56 1 4 3 1 2 2 1 0 0 1 74 108 82 106 80 46 0 0 0 0 29.56 65.7 12.57 27.95 1 1 1 0 0 0 0 0 0 1 2,3 1 97%
18SRINIVASAN
I16019273 O02020134 76 1 1 1 4 1 4 1 20000 2 0 0 1 0 I 0 1 20 12.5 6,100 14.8 0 0 3 2 1 6 2 1 0 0 0 87 55 51 59 54 54 0 1 2 3 30.45 76.73 12.45 26.25 1 1 0 0 0 0 0 0 0 1 1,2 1 98%
19VALLIYATHAL
I15007629 O15014663 50 2 1 1 1 2 0 1 2250 2 0 0 1 0 I 0 1 3 11.8 5,900 13.6 25 0 3 2 1 4 1 1 0 0 0 109 71 64 79 68 76 0 1 2 3 19.36 39.51 12.45 17.01 1 1 0 0 0 0 0 0 0 1 1 0 96%
20PONGIYANNAN
I16024301 0II036905 63 1 1 1 3 2 0 1 10000 2 0 0 1 1 I 0 1 0 12.4 6,100 14.4 39 0 4 2 1 2 2 1 1 0 0 69 48 57 53 67 25 0 1 1 1 17.34 24.33 12.37 17.99 1 1 0 0 0 0 0 0 0 2 1 1 98%
21PALANIMMAL
I16013698 O10006029 56 2 1 1 4 2 0 0 10000 2 0 0 1 1 I 0 1 49 11.2 11,600 13 103 0 3 2 1 2 2 1 1 1 0 85 58 67 80 90 25 1 1 1 3 22.86 49.99 12.45 20.31 1 1 1 0 1 1 0 0 0 2 4 0 97%
22SIVABAKIYAM
I16013703 O13035215 47 1 1 1 3 1 3 1 5000 2 0 0 1 1 II 0 1 10 12.9 11,200 14.7 4 0 4 2 1 6 2 1 0 0 0 81 68 82 68 80 52 0 1 2 4 18.94 43.33 12.37 15.07 1 1 0 0 0 0 0 0 1 3 1 0 98
23GOVINDRAJ
I15026273 O97040946 74 1 1 1 4 1 4 1 10000 2 0 0 1 1 II 0 0 0 12.2 10,200 12.4 60 0 3 2 1 3 1 1 1 0 0 68 58 65 58 69 35 0 1 2 2 18.62 32.92 12.37 17.72 0 1 0 0 0 0 0 0 0 2 1 0 98
24TAMILSELVI
I6017694 O13039091 51 2 1 0 1 2 0 0 5000 2 0 0 1 1 II 0 1 4 13.2 5,800 13.1 23 0 3 2 1 4 3 1 1 0 0 71 84 84 101 80 95 0 1 1 2 18.53 40.6 12.71 14.95 1 1 1 0 0 1 0 0 0 0 4,5,7 1 92%
25RANGAMMAL
I6017694 O12081156 55 2 1 1 4 2 2 4 5000 2 0 0 1 0 II 0 0 6 6.4 10,900 14.3 20 0 3 2 1 2 2 1 2 0 0 93 24 26 24 22 17 2 1 1 3 26.78 52.19 12.47 27 0 1 0 0 0 0 0 0 0 2 1 0 95%
26VIJYANIRMALA
i16019091 O15063397 23 2 0 0 4 1 6 0 8000 2 0 0 1 1 II 0 1 15 13.4 13,700 12.6 23 0 3 2 1 2 1 1 0 0 0 75 41 46 49 66 36 0 1 1 2 18.21 33.26 12.19 16.94 1 1 1 0 1 1 0 0 1 0 0 0 97
27THANGAMMAL
i15012857 o15028202 66 2 1 0 4 1 0 0 8000 2 0 0 1 1 II 0 1 2 13.6 11,000 14.3 29 0 4 3 1 3 3 1 0 0 0 82 59 53 85 74 36 1 1 2 4 18.77 34.02 12.21 17.75 1 1 0 0 0 0 0 0 0 1 1 0 95%
28ELANGOTHI
I16018483 O09064727 56 2 1 1 4 1 2 0 20000 2 0 0 1 1 II 0 0 1 12.5 9,400 14.8 16 0 3 4 1 3 1 1 0 0 0 50 44 44 44 45 34 0 1 2 3 15.53 19.56 12.11 15.53 1 0 0 0 0 0 0 0 0 0 1 0 98%
29KRISHNAN E.S
I16017715 O16037440 70 1 1 1 4 1 3 0 10000 2 1 0 1 1 II 0 1 4 14.3 11,000 13.6 9 1 3 2 1 2 2 1 1 0 0 47 19 43 43 47 25 0 1 2 4 18.94 43.33 12.37 15.08 1 1 0 0 0 0 0 0 0 2 1 0 96%
30RAMASAMY
I17024509 O17044794 65 1 1 1 3 1 0 1 12000 2 1 0 1 1 III 0 0 3 11.1 9,400 15.6 31 1 2 3 1 2 1 1 1 0 0 92 25 25 24 22 18 2 1 2 3 17.2 32.25 11.19 15.9 1 1 0 1 0 1 0 0 0 2 3 0 93%
31KALIAMMAL
I16025842 O16001737 52 2 1 0 2 1 0 0 4000 2 0 0 0 1 II 0 1 3 15.9 12,900 15.9 7 0 3 4 1 3 1 1 1 0 0 50 43 44 44 45 63 1 0 1 4 18.62 32.92 12.36 17.7 0 1 0 1 0 1 0 0 0 2 3 0 97%
32JAYANTHI
I16028445 O09096706 42 2 1 1 3 1 4 1 10000 2 0 0 0 1 III 0 1 2 8.2 5,900 29 94 1 3 2 1 2 1 1 1 0 0 71 86 85 100 80 95 0 1 2 2 24.76 52.14 12.45 26 0 1 0 1 1 1 0 0 0 3 2,3 1 96%
33SELLATHAL
I16018386 O15077108 50 2 1 1 3 2 2 1 8000 2 1 0 1 0 II 0 1 10 15.1 8,900 13.1 67 1 2 2 1 3 2 1 1 0 0 47 19 43 43 38 35 0 1 1 3 30.45 76.73 12.45 26.25 1 1 1 0 0 0 0 0 0 2 3 1 97%
34JAYALAKSHMI
I16019716 O14081743 45 2 1 1 3 1 3 1 4000 2 0 0 1 1 II 0 1 3 14.1 11,100 13.7 16 1 2 3 1 2 2 1 0 0 0 90 65 76 65 67 25 0 1 2 3 29.58 64.7 12.6 26.94 1 1 0 0 0 0 0 0 0 3 2 1 96%
35VELLINGIRI
I17004121 O14014318 50 1 1 1 4 1 2 1 8000 2 0 1 1 1 II 0 1 2 12.9 6,800 13.9 61 0 3 2 1 2 3 1 1 0 0 50 44 44 45 50 35 0 1 2 2 22.4 37.44 12.57 23.33 1 1 0 0 0 1 0 0 1 2 3 1 97%
36BAGYAM
I16021790 O11017929 72 2 1 1 4 2 1 4 8000 2 0 0 1 1 II 1 4 5 11.3 11,800 16.1 23 0 4 2 1 3 2 1 1 0 0 74 68 76 72 80 47 0 1 2 2 28.07 57.2 13 27.56 0 0 0 0 0 0 0 0 0 0 1,4,5 0 94%
37SIVAKAMI
I16000708 O12030255 54 2 1 1 4 2 2 1 12,000 2 3 0 1 1 II 0 0 4 12.6 7,200 12.2 27 0 4 3 1 2 3 1 0 0 0 83 29 29 31 31 116 0 1 1 2 31.05 76.76 12.77 27.19 1 0 0 1 1 0 0 0 0 1 0 0 98%
38SAVITHIRI
I15038020 O15086817 57 2 1 1 4 0 3 1 10,000 2 3 0 1 2 II 3 0 1 13.1 13,100 13.9 43 0 0 0 1 1 1 1 0 0 0 55.3 41 58 46 68 17 0 1 1 2 19.66 40.22 12.11 17.53 1 0 1 1 0 0 0 0 0 2 2 1 98%
39VALLIYATHAL
I15007629 O15014663 56 2 1 1 2 1 1 2 10,000 0 2 0 1 1 I 0 2 3 0 3 2 1 2 2 1 0 0 0 109 71 64 76 68 66 0 1 2 3 19.36 39.51 12.45 17.01 1 0 1 1 1 0 0 0 1 3 3 1 97%
40VINITHA
I16026762 O14010999 29 2 1 1 4 1 6 1 20,000 2 0 0 1 2 2 5 2 2





























