Embed Size (px)
Citation preview
MS THESIS - LONDON UNIVERSITY
THE EFFICACY AND SAFETY OF ADJUNCTIVE
INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING
THE LOCAL RECURRENCE RATE OF TUMOUR AFTER
RADICAL NECK DISSECTION
M.G.DILKES MB,BS., FRCSEd(GS), FRCS(Otol), FRCS(ORL)
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Acknowledgements
SUPERVISORS: PROFESSOR N.S.WILLIAMS AND MR P.MCKELVIE
FUNDING: THE CANCER RESEARCH CAMPAIGN
Other financial support: Scotia Pharmaceuticals
Physics support, experimental planning: Martin L. DeJode
Animal care, experimental support: Richard Rountree and staff
Histology: Alex Brown and staff
Technical support (vessel work): Steve G. Greenwald
Pharmacological analysis: Chung-Kee Lim and Andy Holroyd
Vessel microvascular anastomosis work: Sandra Simpkin
Fluorescence, general advice: Mike F. Grahn
Photosensitiser: Scotia Pharmaceuticals, Lederle Pharmaceuticals
Drug advice: Brenda Reynolds, Charles Stewart
Ultrasonic Doppler device: Linton Instruments2
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Laser devices: QuadraLogicTechnologies
Many thanks to the above - they made the project possible
3
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
INTRODUCTION PART 1
1:Squamous Cell Carcinoma of the Upper Aerodigestive
tract1a: Incidence 11-14
1b: Aetiology 15
1c: Histology 16
1d: Staging 17-21
1e: Treatment of HNSCC 22-23
1f: Cause of death 24
2: Metastatic Disease2a: Rate of distant metastasis 25-26
2b: Metastatic Neck Disease 27
2c: Incidence 28-29
2d: Prognosis - Neck Metastases 30
2e: Why Lymphatic spread? 31
2f: Treatment of metastatic neck disease. 32
2g: Recurrence after radical neck dissection 33-35
2h: Cause of local recurrence 36
2j: Surgery for metastatic neck disease
2j(i): Radical neck dissection 37-394
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
2j(ii): Conservative neck dissection 40-41
2k: Treatment of macroscopic residual disease 42
5
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
3: Radiotherapy3a: Introduction 43
3b: External Beam Radiotherapy 44-45
3c: Brachytherapy 46
3d: Efficacy of Radiotherapy 47
3e: Side Effects of radiotherapy 48-49
3f: Role of radiotherapy in neck malignancy 50
3g: Pre or Post operative radiotherapy? 51
6
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
INTRODUCTION PART II
4: Photodynamic Therapy4a: Development and Principles 52-54
4b: Photodynamic Therapy for Head and Neck cancer 55-56
4c: History of PDT for Head and Neck cancer 57-59
4d: Why do these advantages occur? 60-61
4e: Light for Photodynamic Therapy 62-65
4f: Potentiation of the Photodynamic effect 66-67
4g: Role of fluorescence in PDT 68-69
5: Chemistry of Photodynamic therapy5a: Drugs for Photodynamic Therapy 70
5b: Examples of first generation drugs 71-73
5c: Second generation Photosensitising Drugs 74-77
5d: Problems 78-79
6: Adjunctive Intraoperative Photodynamic Therapy
(AIOPDT)6a: Preclinical 80
6b: Clinical 80
7: Experimental Rationale 817a: Description 82
7b: First Stage - efficacy 83
7c: Second Stage - Safety Studies 83
7
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
7d: Third Stage - Clinical Study 83
7e: 6 consecutive preclinical experiments 84
8: Drugs, animals, Laser, Other equipment
8a: Photosensitising Drugs 85
8b: Anaesthetic Drugs 86
8c: Tumour 86-87
8d: Animals 88
8e: Lasers 88
9: Experiment 1 - Preclinical pharmacokinetic studies
of first and second generation photosensitising drugs
9a: Introduction 89-90
9b: Tumour 90
9c: Drug dose and analysis 91
9c(i): mTHPC analysis 92
9c(ii): Photofrin 2 analysis 93
9d: In-vivo validation 94
9e: Results 95-100
8
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
9f: Discussion 101-106
10: Experiment 2 - The efficacy of Adjunctive
Intraoperative Photodynamic Therapy in a rat
fibrosarcoma model with mTHPC10a: Description 107
10b: Tumour 107
10c: Photodynamic Therapy Parameters 108
10d: Preliminary studies 109
10d(i): Study 1 109
10d(ii): Study 2 110
10d(iii): Study 3 111-115
10e: Results 116-121
10f: Statistical Analysis 122
10g: Discussion 123-125
10h: Conclusion 125
11: Experiment 3 - Preclinical Photodynamic
Safety Studies on Arteries11a: Description 126-127
11b: PDT Details 127
11c: Drug 128
11d: Study Design 128-129
11e: Vessel Analysis 130-133
11f: Statistical analysis 1369
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
11g: Discussion 137-140
11h: Conclusion 141
12: Experiment 4: Acute phase effects of PDT on
arteries and veins12a: Description 142
12b: Chemical 142
12c: Measurement of flow 143-144
12d: Experimental technique 145-148
12e: Results 148-149
12f: Discussion 150-153
13: Experiment 5 - The effect of high intensity white
and filtered microscope light on the viability of
microvascular anastomoses in photosensitised rats13a: Description 154-156
13b: Plan 156
13c: Methodology
13c(i): Physics assessment 157
13c(ii): Safety study 157
13d: Drug 157
13e: Animals 158
13f: Operative technique 159
13g: Postoperative assessment 159
13h: Results 160-16510

THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
13I: Statistical analysis 166-168
13j: Discussion 169-172
11
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
14: Experiment 6 - Histological study of large
diameter arteries undergoing photodynamic therapy14a: Description 173
14b: Methodology 173
14c: Results 173
14d: Discussion 174
15: Adjunctive Intraoperative Photodynamic Therapy for
Head and Neck Cancer 175-177
15a: Method 178-183
15b: Results
15b(i): Case #1 184-185
15b(ii): Case #2 186
15b(iii): Case #3 187
15b(iv): Case #4 187
15c: Discussion 188
16: Conclusion 189
17: References 190-225
12
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
INTRODUCTION
1) Metastatic neck disease in Squamous Cell Carcinoma of the
Head and Neck
2) Photodynamic Therapy for Squamous Cell Carcinoma of the Head
and Neck
13
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
INTRODUCTION PART 1
Squamous Cell Carcinoma of the Upper Aerodigestive tract
1a: Incidence
These tumours are by far the most common malignant neoplasms of
the Head and Neck, excepting the skin. Those arising from the
upper aerodigestive tract account for 2.4% of all new cancers
presenting each year in men, and 0.7% of all new cancers in
women (see table 1). They tend to present in the 5th and 6th
decades of life, and are more common in men than women, although
the incidence in women is rising.
Head and Neck cancers account for around 4% of all cancer deaths
annually. The figures regarding incidence as a percentage of
total cancer cases, per site, are fairly similar in the Western
World (see tables 1 and 2), although geographical variance does
occur making tumours much more common in some areas than others
(see later).
To clarify descriptions in later tables, regarding the site of
primary tumours, ENT relates to any squamous cell carcinoma of
the Head and Neck (HNSCC) arising from the following described
areas. From the hard/soft palate junction, in a plane extending
down the anterior pillars of the fauces (which is the border of
the oral cavity and the oropharynx), extending caudally to the
end of the subglottic region of the larynx, and the
cricopharyngeal sphincter of the pharynx/oesophagus junction,
14
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
including the nose and nasopharynx. This is the anatomical
description of the ENT area as taken from Gray’s Anatomy.
Tumours arising anteriorly to the border between oropharynx and
oral cavity are described as oral cavity in origin. This area
extends to the vermilion border of the lip, where it meets the
skin. Other SCC's arising in the Head and Neck area will be from
ear, salivary gland or skin, and are not further discussed,
since the study aims at treating metastatic disease from HNSCC.
For the purposes of this Thesis, that means Oral Cavity and ENT
tumours as described above (although the treatment itself is
potentially applicable to all malignancy of the Head and neck).
There are three main surgical specialities dealing with this
disease, Ear, Nose and Throat (or Otolaryngology),
Oral/Maxillofacial, and Plastic surgeons, in order of number of
new cases seen per year. In the longer term it seems likely that
regional centres combining all three modalities in the same
therapeutic team, along with radiotherapy and support services
will treat the majority of cases, in accordance with Department
of Health Guidelines for cancer treatment (Calman-Hine Report,
1997).
15
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
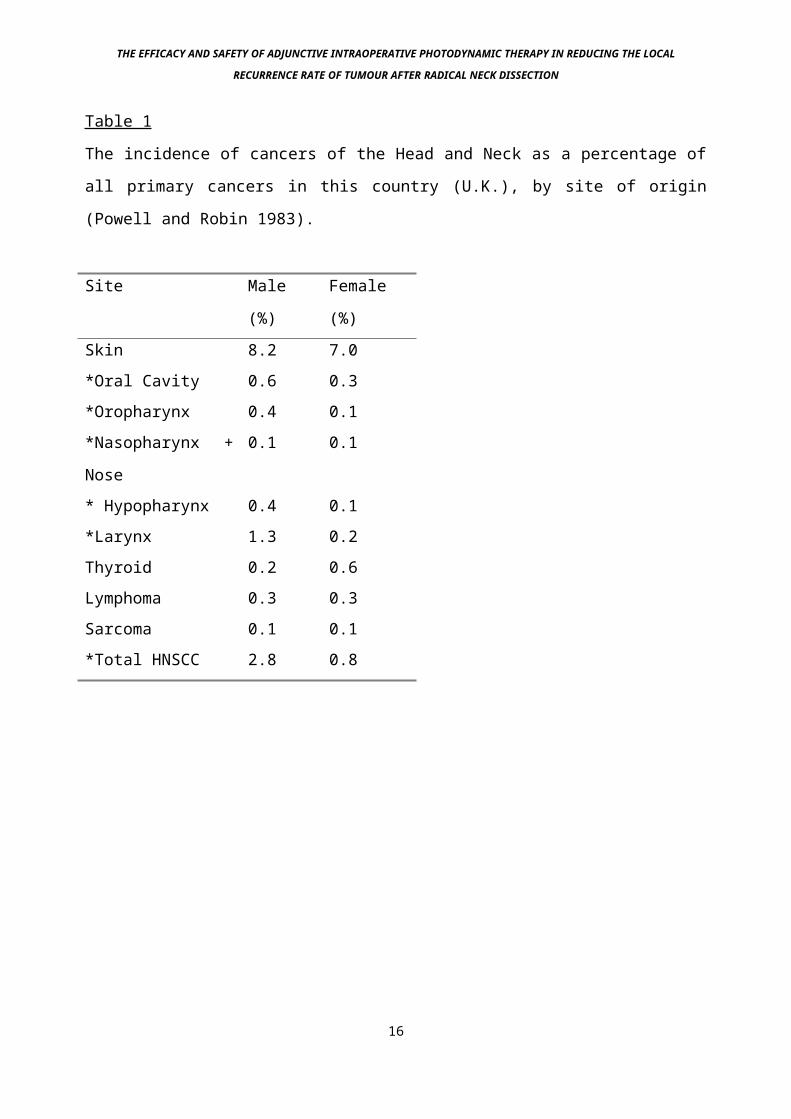
Table 1
The incidence of cancers of the Head and Neck as a percentage of
all primary cancers in this country (U.K.), by site of origin
(Powell and Robin 1983).
Site Male
(%)
Female
(%)Skin 8.2 7.0*Oral Cavity 0.6 0.3*Oropharynx 0.4 0.1*Nasopharynx +
Nose
0.1 0.1
* Hypopharynx 0.4 0.1*Larynx 1.3 0.2Thyroid 0.2 0.6Lymphoma 0.3 0.3Sarcoma 0.1 0.1*Total HNSCC 2.8 0.8
16
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
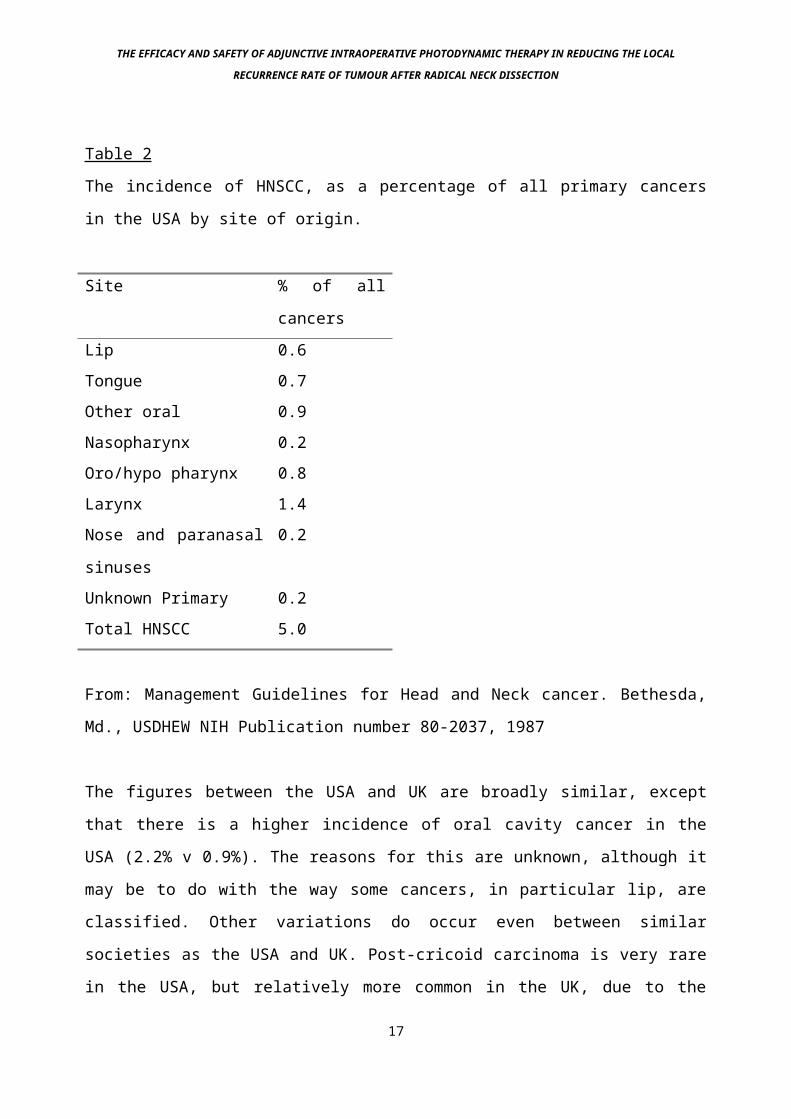
Table 2
The incidence of HNSCC, as a percentage of all primary cancers
in the USA by site of origin.
Site % of all
cancersLip 0.6Tongue 0.7Other oral 0.9Nasopharynx 0.2Oro/hypo pharynx 0.8Larynx 1.4Nose and paranasal
sinuses
0.2
Unknown Primary 0.2Total HNSCC 5.0
From: Management Guidelines for Head and Neck cancer. Bethesda,
Md., USDHEW NIH Publication number 80-2037, 1987
The figures between the USA and UK are broadly similar, except
that there is a higher incidence of oral cavity cancer in the
USA (2.2% v 0.9%). The reasons for this are unknown, although it
may be to do with the way some cancers, in particular lip, are
classified. Other variations do occur even between similar
societies as the USA and UK. Post-cricoid carcinoma is very rare
in the USA, but relatively more common in the UK, due to the
17

THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
incidence of post-cricoid webs from Patterson Kelly-Brown
Syndrome (Jacobs A. 1962).
18
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
1b: Aetiology
A number of factors have been implicated in the aetiology of SCC
of the upper aerodigestive tract (HNSCC). The most important of
these is cigarette smoking, with 90% of head and neck cancers
occurring in smokers (Johnston and Ballantyne 1977). This was
first noted in 1918 by Power, when he noted that in tongue
cancer, "tobacco was the greatest irritant". In the state of
Andrha Pradesh in India, the practice of reverse smoking,
whereby the lit end of the cigarette is inserted into the mouth,
causing a high level of smoke exposure to the oral cavity
epithelium, is associated with a very high incidence of oral
cavity SCC (Reddy and Rao 1957). The addition of significant
alcohol intake has a synergistic effect such that the risk of
developing HNSCC rises 3 times (Thompson 1989). Other, less
dominant aetiological associations have been identified (Vaughan
et al 1980), in particular, causes of chronic irrigation such as
poor dental hygiene, syphilis, candidaisis, erosive lichen
planus, iron deficiency anaemia and betel nut chewing. Patients
with the Acquired Immune Deficiency Syndrome (AIDS) also have a
higher incidence of this disease than the normal population.
The disease itself has a fairly uniform incidence rate
throughout the world, although certain areas, such as the Canton
province of Southeast China, have a very high incidence of one
tumour, in this case nasopharyngeal carcinoma, due to a mixture
of causative factors including genetic predisposition, a diet
including significant amounts of salted fish, and endemic
infection with the Epstein Barr virus (Wei et al 1992). The same19
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
is true of the Normandy region of France, where there is a high
incidence of oral cavity cancer, said to be due to excessive
amounts of alcohol consumed and the chain smoking of high tar
unfiltered cigarettes (Johnston and Ballantyne1977).
20
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
1c: Histology
The tumours originate from squamous epithelial cells lining the
upper aerodigestive tract. Their appearance may vary, from an
exophytic (verrucous) pattern, to an invasive pattern with
diffuse tissue infiltration and ulceration. The hallmark of
these tumours on pathological examination is the presence of
well formed desmosomal attachments and intracytoplasmic bundles
of keratin. Depending on the degree of expression of these
characteristics, the tumours can be classified into different
levels of differentiation from well differentiated to poorly
differentiated tumours. Those tumours that cannot be classified
in this way by light microscopy should be analysed by electron
microscopy and immunochemistry, since if they are of a squamous
cell origin, intracytoplasmic keratin will be found (Holm et al
1982). Poorly differentiated tumours behave in a more aggressive
manner than well differentiated tumours, although their alleged
higher replication rate that presumably causes their increased
aggression also makes them more sensitive to some forms of
treatment such as radiotherapy (Bauer H.C. 1974).
HNSCC often demonstrates signs of sequential change into overtly
malignant tumour. This is particularly true of the oropharynx
and oral cavity where progression from leukoplakia to
erythroplakia, carcinoma in situ and invasive carcinoma can be
closely monitored in at-risk groups, since it is a relatively
easy area to examine and biopsy. Progression in the degree of
dysplasia can be seen in these samples (Banoczy and Csiba 1976)
until frank malignancy occurs. Efforts have been made to attempt
to stop the progression into overt malignancy occurring, in21

THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
particular with the use of oral retinoid treatment (Shah J.P. et
al 1990).
22
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
1d: Staging
HNSCC is currently staged using the UICC/AJCC TNM (Tumour, Node,
Metastasis) classification system. This allows more accurate
auditing of results, and also meaningful comparison of results
from clinical trials. This method of staging is somewhat
artificial and rather subjective, but it is nonetheless a
universally accepted yardstick that needs to be retained until a
better method comes along.
See appendix 1 for a full description of current TNM staging.
Appendix 1
TNM staging of Head and Neck cancer.
Oral Cavity tumours:
Stage Description
TX Minimum requirements to assess tumour cannot be met
T0 No evidence of a primary tumour
TiS Carcinoma-in-situ
T1 Tumour diameter 2 cm or less
T2 Tumour diameter 2-4 cm
T3 Tumour diameter more than 4 cm
T4 Tumour with invasion of deeper structures, e.g. through
cortical bone, into deep muscle of tongue, skin.
23
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
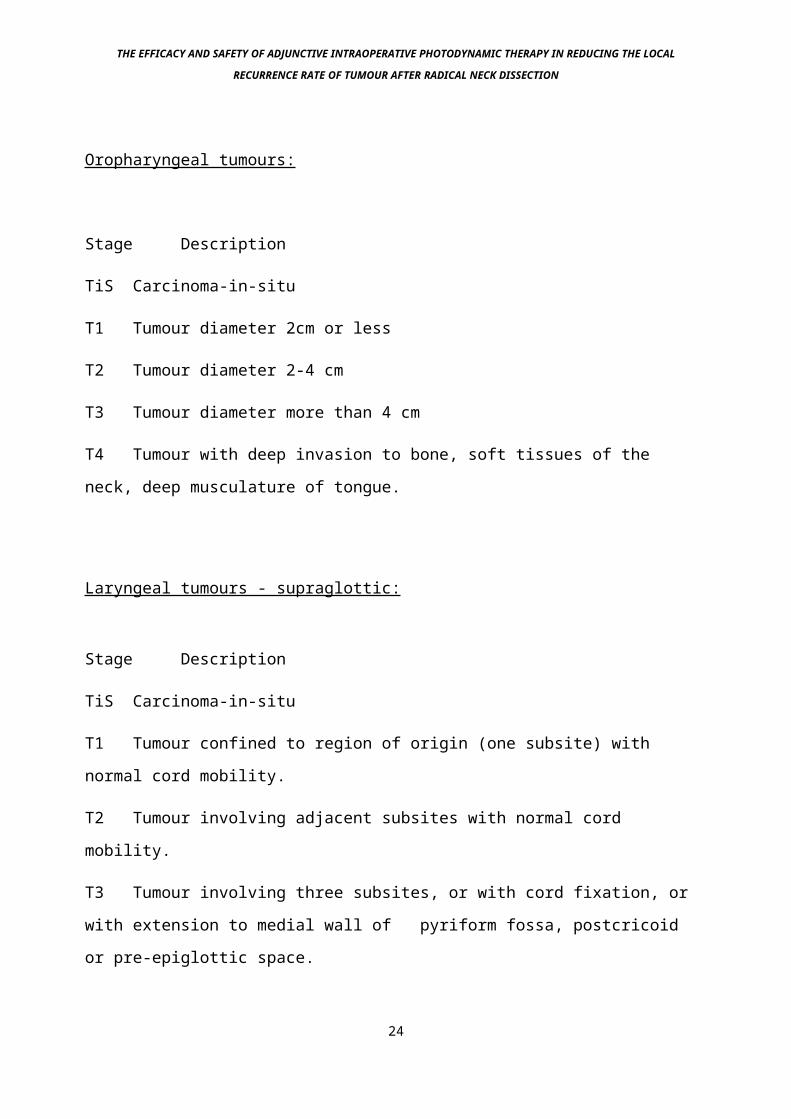
Oropharyngeal tumours:
Stage Description
TiS Carcinoma-in-situ
T1 Tumour diameter 2cm or less
T2 Tumour diameter 2-4 cm
T3 Tumour diameter more than 4 cm
T4 Tumour with deep invasion to bone, soft tissues of the
neck, deep musculature of tongue.
Laryngeal tumours - supraglottic:
Stage Description
TiS Carcinoma-in-situ
T1 Tumour confined to region of origin (one subsite) with
normal cord mobility.
T2 Tumour involving adjacent subsites with normal cord
mobility.
T3 Tumour involving three subsites, or with cord fixation, or
with extension to medial wall of pyriform fossa, postcricoid
or pre-epiglottic space.
24

THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
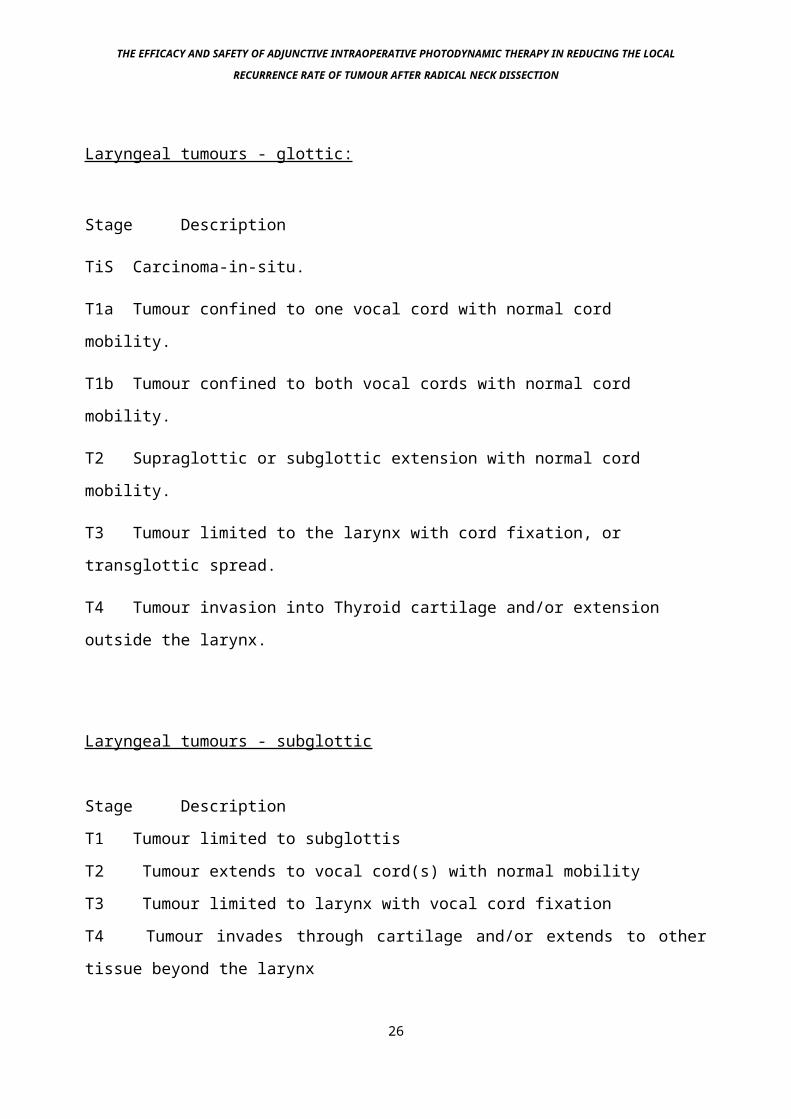
T4 Tumour extending beyond the larynx or to involve the
laryngeal cartilage.
25
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Laryngeal tumours - glottic:
Stage Description
TiS Carcinoma-in-situ.
T1a Tumour confined to one vocal cord with normal cord
mobility.
T1b Tumour confined to both vocal cords with normal cord
mobility.
T2 Supraglottic or subglottic extension with normal cord
mobility.
T3 Tumour limited to the larynx with cord fixation, or
transglottic spread.
T4 Tumour invasion into Thyroid cartilage and/or extension
outside the larynx.
Laryngeal tumours - subglottic
Stage Description
T1 Tumour limited to subglottis
T2 Tumour extends to vocal cord(s) with normal mobility
T3 Tumour limited to larynx with vocal cord fixation
T4 Tumour invades through cartilage and/or extends to other
tissue beyond the larynx
26
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
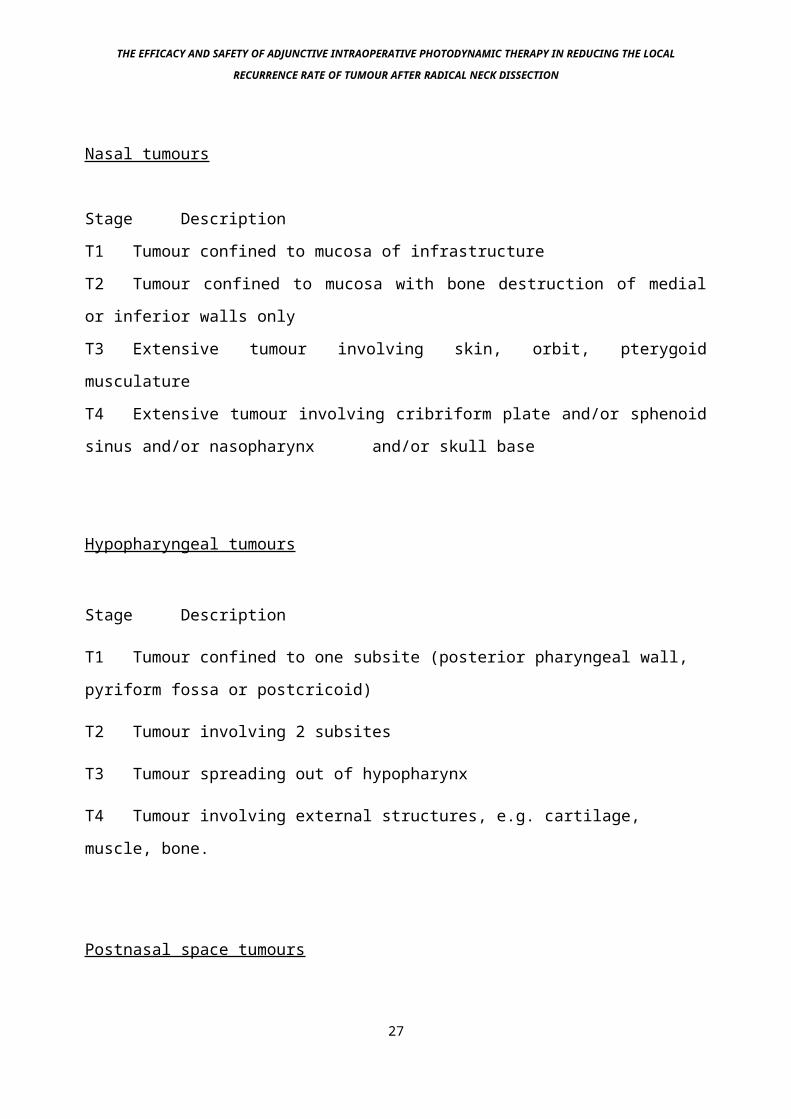
Nasal tumours
Stage Description
T1 Tumour confined to mucosa of infrastructure
T2 Tumour confined to mucosa with bone destruction of medial
or inferior walls only
T3 Extensive tumour involving skin, orbit, pterygoid
musculature
T4 Extensive tumour involving cribriform plate and/or sphenoid
sinus and/or nasopharynx and/or skull base
Hypopharyngeal tumours
Stage Description
T1 Tumour confined to one subsite (posterior pharyngeal wall,
pyriform fossa or postcricoid)
T2 Tumour involving 2 subsites
T3 Tumour spreading out of hypopharynx
T4 Tumour involving external structures, e.g. cartilage,
muscle, bone.
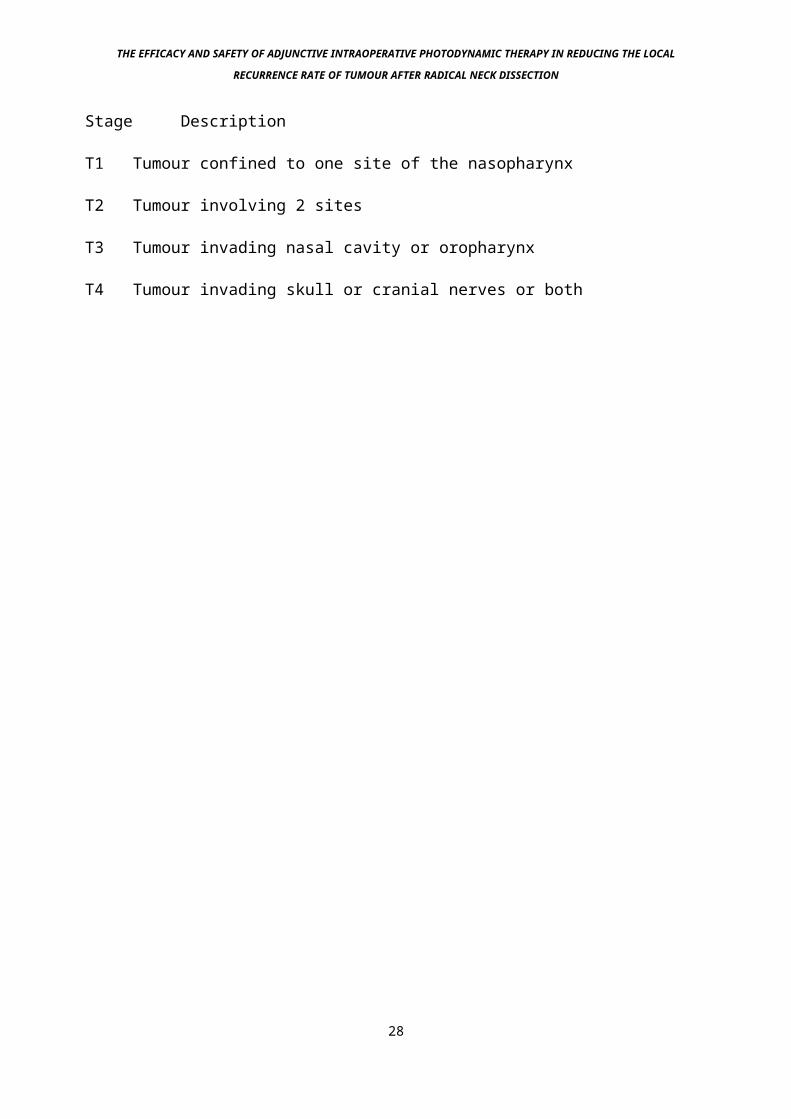
Postnasal space tumours
27
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Stage Description
T1 Tumour confined to one site of the nasopharynx
T2 Tumour involving 2 sites
T3 Tumour invading nasal cavity or oropharynx
T4 Tumour invading skull or cranial nerves or both
28
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
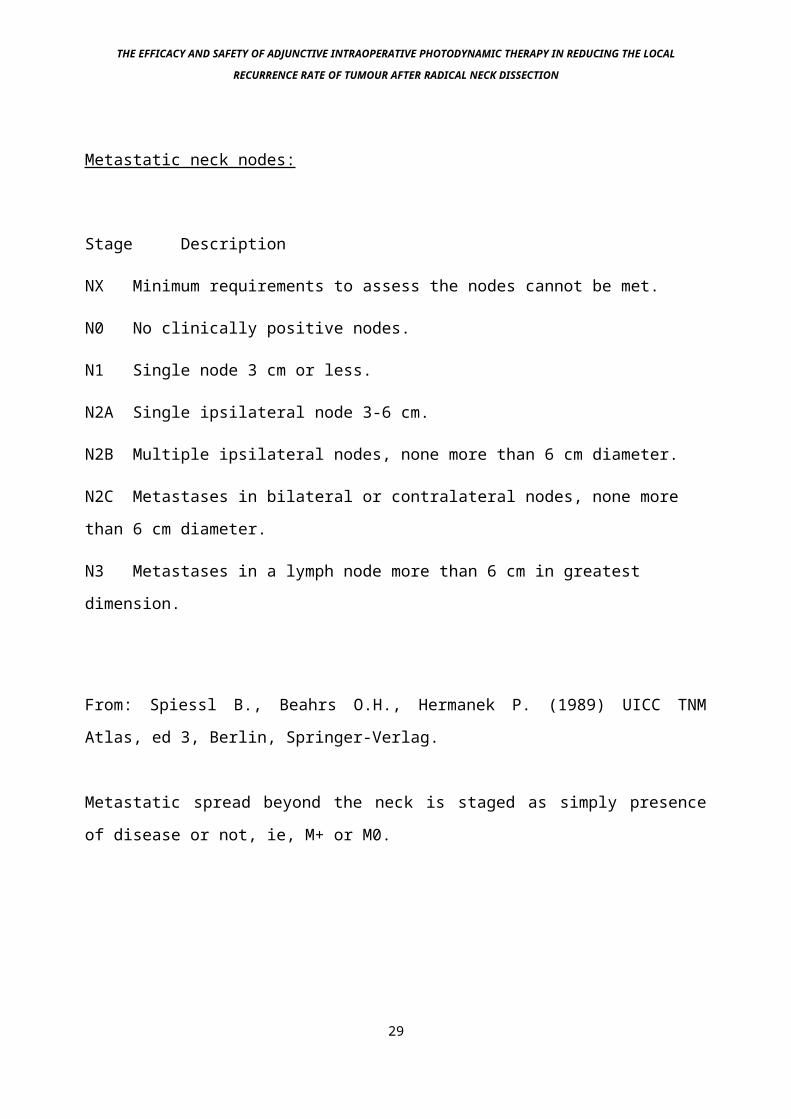
Metastatic neck nodes:
Stage Description
NX Minimum requirements to assess the nodes cannot be met.
N0 No clinically positive nodes.
N1 Single node 3 cm or less.
N2A Single ipsilateral node 3-6 cm.
N2B Multiple ipsilateral nodes, none more than 6 cm diameter.
N2C Metastases in bilateral or contralateral nodes, none more
than 6 cm diameter.
N3 Metastases in a lymph node more than 6 cm in greatest
dimension.
From: Spiessl B., Beahrs O.H., Hermanek P. (1989) UICC TNM
Atlas, ed 3, Berlin, Springer-Verlag.
Metastatic spread beyond the neck is staged as simply presence
of disease or not, ie, M+ or M0.
29
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
1e: Treatment of HNSCC
1ei: History of Treatment of HNSCC
Although laryngeal carcinoma represents only one part of the
spectrum of HNSCC, the history of the surgical treatment of this
condition represents an interesting and useful guide into how
management of all malignant disease of the Head and Neck
progressed. The treatment of laryngeal cancer was initially
developed during the latter half of the 19th century as
pathological diagnosis became possible and it was possible to
make the distinction between benign and malignant disease.
The decade from 1850 to 1860 marked a turning point in the
understanding of pathology of the upper aerodigestive tract.
This was due to the advent of indirect and direct laryngoscopy
which enabled accurate distinction of various laryngeal
abnormalities as described by Virchow in 1858. The technique of
indirect laryngoscopy was first effectively demonstrated by
Babington in 1829 in a presentation to the Hunterian Society of
London. His technique, using a tongue depressor combined with a
mirror and reflected sunlight was never generally accepted,
partly because it was a bulky and cumbersome piece of apparatus,
and partly because Babington never published his findings. It
was not until Manuel Garcia, the so-called "Father of
Laryngology" successfully presented and published work on
indirect laryngoscopy in 1855 that the technique properly caught
on. 30
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Following the successful introduction of indirect laryngoscopy,
laryngeal carcinoma was studied in some depth. Initially it was
thought that carcinoma intrinsic to the larynx was rare, but
studies by Semon, Chevalier Jackson, Tucker and Butlin (Thomson
1939) showed that the opposite was in fact true.
31
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
The surgical treatment of squamous cell carcinoma of the upper
aerodigestive tract was started in the latter part of the 19th
century. Initially, resections were performed either
endoscopically or via a laryngofissure (Buck 1853). However,
this technique involved piecemeal removal of tumour, with no
clear resection margins and consequently the results were poor
(Mackenzie, 1871). Billroth in 1874 performed the first
successful laryngectomy in Vienna (Billroth and Gussenbauer
1874). Although the treatment of Head and Neck cancer was
somewhat unfairly discredited during the infamous episode of
Morrel Mackenzie's treatment of Emperor Frederick the Third of
Germany (Stevenson 1946), the steady advancement of the
treatment of this disease has progressed gradually throughout
the 20th Century (Butlin 1909, Trotter 1913), particularly with
the advent of pedicled, axial and free flaps for the
reconstruction of large defects in the Head and Neck, enabling
increasingly wider resection margins, reducing the risk of local
recurrence. Despite these advances however, little has changed
in terms of survival rate from this disease over the past 20
years. This is due to a number of factors, one of which is the
fact that no successful new modality of treatment has been
introduced during this period - in particular, chemotherapy has
failed to make the expected advances in this area (Amrein 1991).
Other innovative techniques, such as the use of cryotherapy
(Holden and Mckelvie 1972) or isolated segmental perfusion with
chemotherapy, have not found a niche in the treatment of Head
and Neck cancer.32
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
1eii: Current Treatment
External beam radiotherapy and radical surgery applied singly or
in combination are the current mainstay of treatment (Jesse and
Lindberg 1975, Arrigada et al 1983). The overall outcome remains
almost unchanged over the past 30 years, despite many technical
advances as discussed. Age adjusted 5 year survival rates range
from as little as 10% for hypopharyngeal primary tumours, to 50%
+ for laryngeal tumours (Powell and Robin 1983). Prognosis is
largely determined by site and stage of tumour when discovered
(Vokes et al 1993). The best results have up to 90% 5 year
survival rate, whilst the same tumour, presenting later, has a
similar survival figure of less than 10% (Kumar et al 1987, Hong
et al 1990). Salvage surgery and radiotherapy after initial
“definitive” treatment has a depressingly low survival rate
(Zieske et al 1986).
33
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
1f: Cause of death
Studies of patients dying from head and neck cancer have shown
that approximately 30% of uncured patients have uncontrolled
disease at the primary site and about 70% have uncontrolled
local lymphatic or soft tissue spread. In these cases, the local
disease was usually directly implicated in the immediate cause
of death (Sloan and Goepfert 1991). About 25% of patients also
have distant metastases , although these tend to be incidental
findings at post-mortem rather than actual cause of death (see
later).
34
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
2: Metastatic Disease
2a: Rate of distant metastasis
Distant metastasis is defined as spread of tumour beyond its
site of origin and beyond the regional lymphatics for that site.
Crile was the first to look at the frequency of distant
metastases in patients with HNSCC at post mortem. Mentioning the
work of Hutchings (Crile 1923), a distant metastasis rate of 1%
of 4,500 cases was cited. In the same article, Crile said "The
collar of lymphatics about the neck forms an almost impossible
barrier through which tumour rarely penetrates and every portion
of this barrier is readily accessible to the surgeon".
On these rationale, it was difficult not to be enthusiastic
about Criles's operation (block dissection of the neck lymph
nodes - see later), since if local control could be achieved,
the major cause of death was removed, with potential cure being
therefore possible. Studies since then have shown a higher rate
of distant metastasis (see table 3), averaging at around 10% of
cases. As expected, when stage of primary tumour was noted along
with the presence or absence of distant metastases, an increase
in the rate of metastases occurred as the stage of the primary
increased (Merino et al 1977).
35
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
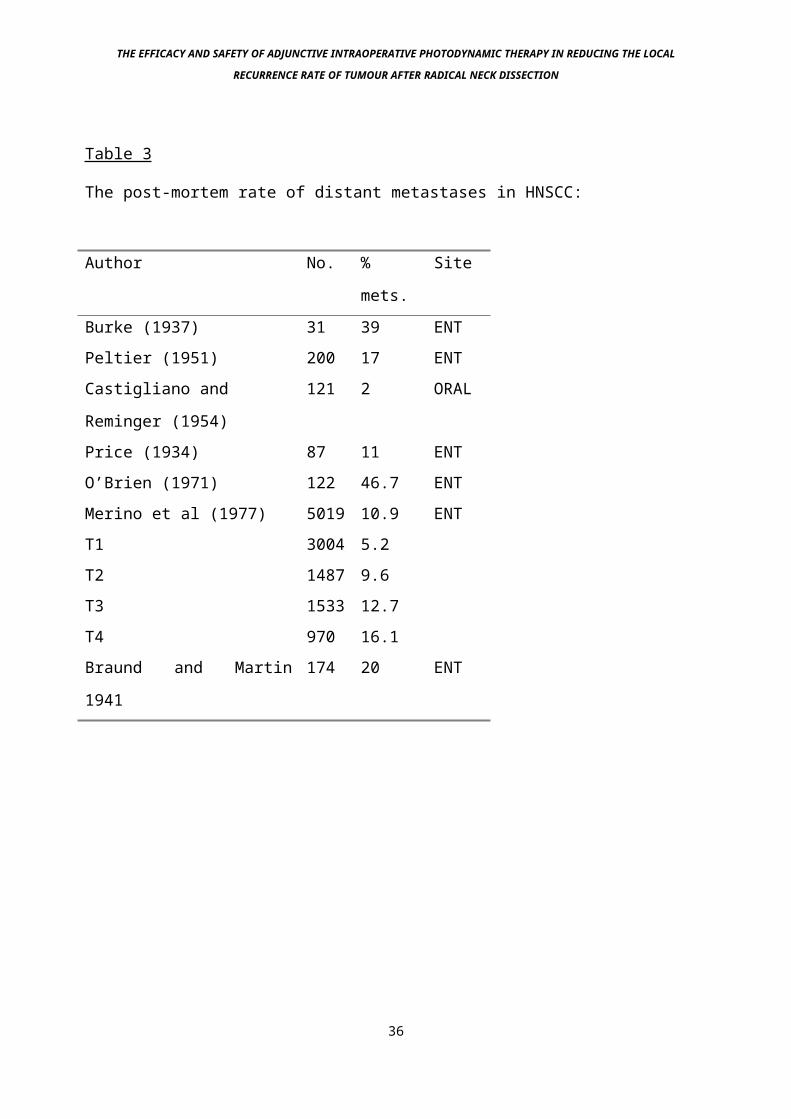
Table 3
The post-mortem rate of distant metastases in HNSCC:
Author No. %
mets.
Site
Burke (1937) 31 39 ENTPeltier (1951) 200 17 ENTCastigliano and
Reminger (1954)
121 2 ORAL
Price (1934) 87 11 ENTO’Brien (1971) 122 46.7 ENTMerino et al (1977) 5019 10.9 ENTT1 3004 5.2T2 1487 9.6T3 1533 12.7T4 970 16.1Braund and Martin
1941
174 20 ENT
36
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
2b: Metastatic neck disease
The phrase “metastatic neck disease” implies a malignant tumour
found in the neck that is a secondary deposit from a primary
tumour elsewhere, most commonly HNSCC that has spread into its
regional lymph nodes. Metastatic neck disease is staged
according to the Tumour, Node, Metastasis (TNM) UICC/AJCC system
- see above. Malignant tumours may arise denovo in the neck,
these are usually lymphoma (Jelliffe A.L. 1986), or perhaps
branchiogenic carcinoma from residual neck epithelial tissue
left during embryonic development (McCarthy and Turnbull 1981).
Occasionally malignant neck masses are found that have no
obvious primary site (Strasnick et al 1990). These are usually
undifferentiated or squamous carcinoma, and the most common site
of origin for them when it eventually makes itself known is the
postnasal space or tongue base. In situations where no obvious
primary is found these areas are investigated thoroughly and
treated prophyllactically. Secondary malignant disease in the
neck may also arise in the salivary or thyroid glands. In this
situation the tumour primary is usually distant, and spread
occurs in a blood bourn rather than lymphatic manner. Common
sites for primary tumours in this case include the lungs (Dilkes
and Birchall 1990) and stomach.
Cancer in the neck lymph glands therefore originates from one of
3 sources: as part of primary cancer of the lymph glands
(lymphoma), as part of widespread metastatic disease from
cancers elsewhere in the body, such as stomach or skin, or as
37
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
locoregional spread from a Head and Neck primary tumour, which
is usually Squamous Cell Carcinoma (SCC). The latter are by far
the most common source of malignant neck glands, and this study
is aimed at this area.
38
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
2c: Incidence
The incidence of metastatic spread of the primary tumour into
the neck lymph glands varies depending on the site and stage of
the primary tumour: see table 4. Some areas of the Head and Neck
have a much higher rate of metastasis into the neck than others,
this is presumably due to them having a richer network of
lymphatic channels than the lower rate areas. In particular the
supraglottis and tongue are known to have a rich supply of rich
lymphatic vessels. Size of the primary tumour also equates to a
higher incidence of neck metastases, presumably because the
bigger the tumour the longer it has been present, and therefore
if there is a certain “risk per year” of neck metastases, the
longer a tumour has been present, the more likely a lymph node
will be involved. This is generally accepted to be due to two
factors, increased intra-tumour pressure, and increased
likelyhood of lymphatic invasion. Therefore tumours that present
late, such as pyriform fossa or postnasal space carcinomas will
more often have an associated involved lymph node. When treating
the primary tumour, prophylactic treatment of the neck is
usually performed if the primary is at a high risk of neck
metastasis. This would be by either external beam irradiation or
neck dissection, or both.
39
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
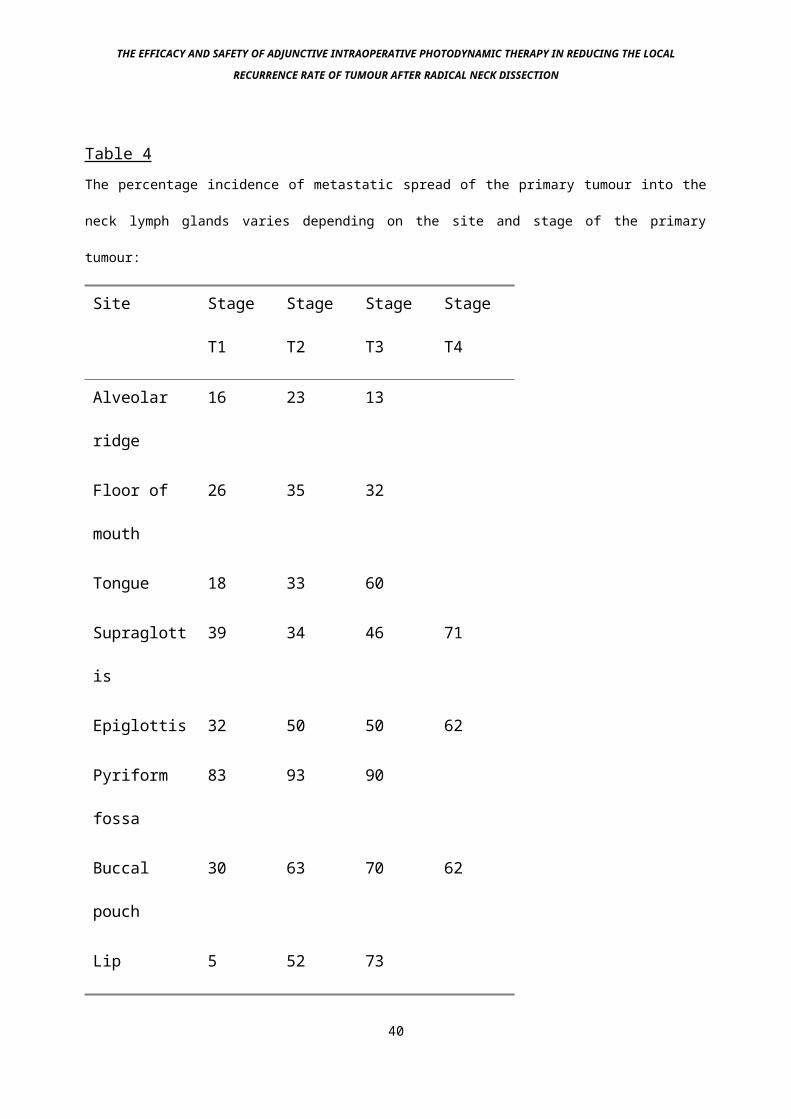
Table 4The percentage incidence of metastatic spread of the primary tumour into the
neck lymph glands varies depending on the site and stage of the primary
tumour:
Site Stage
T1
Stage
T2
Stage
T3
Stage
T4
Alveolar
ridge
16 23 13
Floor of
mouth
26 35 32
Tongue 18 33 60
Supraglott
is
39 34 46 71
Epiglottis 32 50 50 62
Pyriform
fossa
83 93 90
Buccal
pouch
30 63 70 62
Lip 5 52 73
40
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Data taken from: Mendelson et al, 1977, DeSanto et al 1977, Razack
et al 1978, Razack et al 1978, Joyce and McQuarrie 1976, Wurman et
al 1975.
41
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
2c: Prognosis with Neck Metastases
This study is aimed at metastatic squamous cell carcinoma from a
Head and Neck (HNSCC) primary site (definition of Head and Neck
cancer: any malignant tumour arising from the vermilion border
of the lips, down to the upper trachea and cricopharyngeal
sphincter, including the entire nasal area and middle ear,
excluding the orbit and brain). The presence of metastatic neck
disease in a patient with HNSCC significantly reduces the 5 year
survival rate (Snow et al 1982). There is an increased risk of
local recurrence at the primary site when lymphatic metastases
occur. Failure of local control following the treatment of
metastatic neck malignancy is a major cause of death in
patients with HNSCC, 5 year actuarial survival being around 5%
or less (Fletcher G.H 1973, Mendelsohn et al 1977, Pearlman
1979).
Following the successful treatment of the primary and the neck
metastasis, the patient has a reasonable chance of being cured
of his or her cancer (Jesse et al 1970, Shah and Tollefson 1974,
Mendelsohn et al 1976). This is because as mentioned previously
this form of tumour rarely metastasises widely (table 2). This
is unlike many other cancers such as breast cancer, which can be
relatively easily controlled locally by the simple excision of
the cancer mass, or mastectomy, but which often results in the
death of the patient from widespread metastases - this sort of
cancer is not as suitable for extra measures to be taken for
local control.
42
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
There is therefore a major advantage to patients with HNSCC if a
way of reducing the local recurrence rate after standard methods
of treatment can be devised. Local control of HNSCC is paramount
in improving mortality figures which have remained virtually
unchanged since the 1970’s, the time when the last major
advance, new reconstruction techniques allowing wider local
excision of tumours, was introduced.
43
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
2d: Why Lymphatic spread?
Spread of the primary tumour to the associated lymphatics is
more common in HNSCC than most other tumours for a number of
reasons: Firstly, it is postulated that the presence of dense
lymphatic tissue in Waldeyer's ring allows easy access of tumour
tissue to the lymphatic system. Secondly, the absence of a dense
subepithelial layer of collagen as compared to normal skin means
that tumours of the Head and Neck mucosa find penetration into
the lymphatic system easier. Thirdly, the frequent forced
movements of chewing, talking and swallowing probably help
propel tumour emboli into and along the lymphatic channels.
These actions can develop pressures of up to 100 mm Hg
(McQuarrie D.G. et al, 1986). These facts do not explain why the
tumours do not disseminate via the bloodstream - this tumour
specific factor is probably due to specific cellular
characteristics that are currently unrecognised.
44
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
2e: Treatment of metastatic neck disease.
The nineteenth century surgeons initially involved in the
treatment of HNSCC were aware that malignant diseases of the
upper aerodigestive tract metastasized to the cervical lymph
nodes. Initially, the finding of involved neck nodes would be an
indication of inoperability, rather as disseminated liver
involvement in colon cancer is regarded currently. In 1906
however, Crile published his results of treatment in 132 head
and neck cancers, with a reasonable degree of success in
removing the neck lymph glands en bloc, the first properly
described and followed up series that led to the operation of
block neck dissection. This technique of block dissection of
the neck nodes was further clarified and improved upon during
the pre World War 2 era, with increasingly good results being
achieved as added treatments such as antibiotics, blood
transfusion, inhalational anaesthetics through nasotracheal
tubes and improved physical health reduced the perioperative
mortality (Ward and Hendrick 1950). The greatest impetus in the
development of radical surgery for metastatic neck disease with
a primary tumour in the upper aerodigestive tract came in 1951
when Martin et al published an extensive series based on 30
years of experience with the treatment of HNSCC metastatic to
the neck nodes, advocating radical neck dissection in continuity
with resection of the primary tumour, and demonstrating very
impressive results.
45
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Following the publication of this paper, there was widespread
acceptance of the operation of radical primary tumour removal
with a block excision of involved nodes taken in continuity with
as wide a pedicle as possible connecting the lymph node
resection with the primary tumour. The role of radiotherapy in
any metastatic HNSCC tumour in the neck over 2cm diameter
appears to be essentially adjunctive to surgery, either given
preoperatively or postoperatively (Wizenburg et al 1972, Jesse
and Lindberg 1975, Leemans et al 1990).
46
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
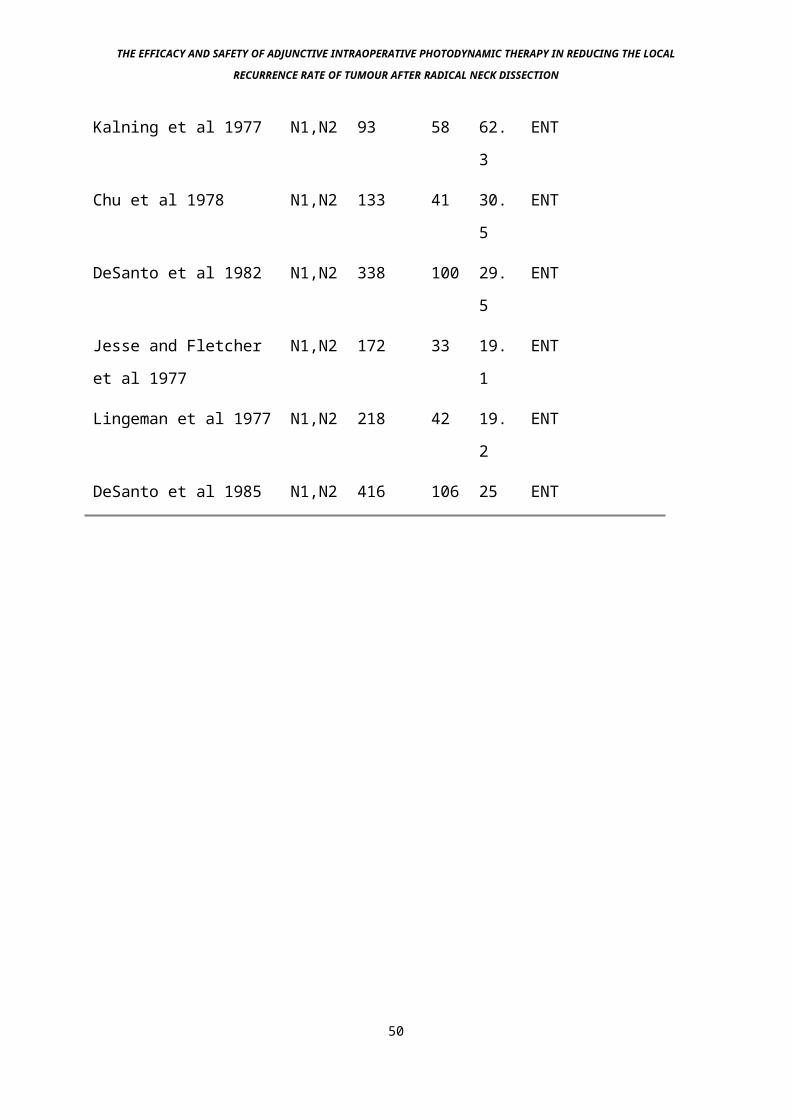
2f: Recurrence after radical neck dissection
Despite the advances mentioned above, the operation of radical
neck dissection does have an appreciable local recurrence rate
(see tables 5-7 inc). The rate of local recurrence in the neck
increases with:
1) Nodal stage (see tables)
2) Level of nodes involved (Spiro et al 1974, Kalnins et al
1977).
3) Presence of extra-capsular spread on histological analysis
(Johnson et al 1981).
At first glance, it might seem that the presence of
extracapsular spread would simply be a determinant of node size
and hence stage, and therefore not be an independent variable.
However, work by Annyas et al in 1979 showed that 23% of nodes
of less than 1cm diameter showed some degree of extracapsular
spread.
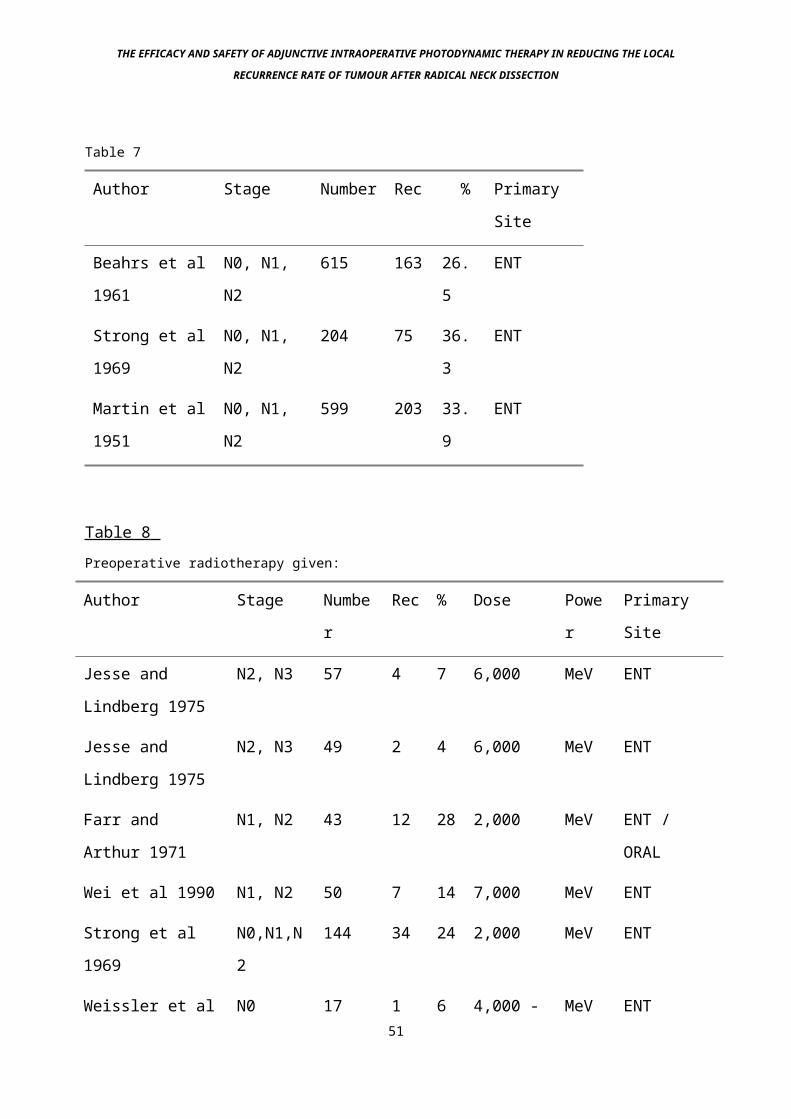
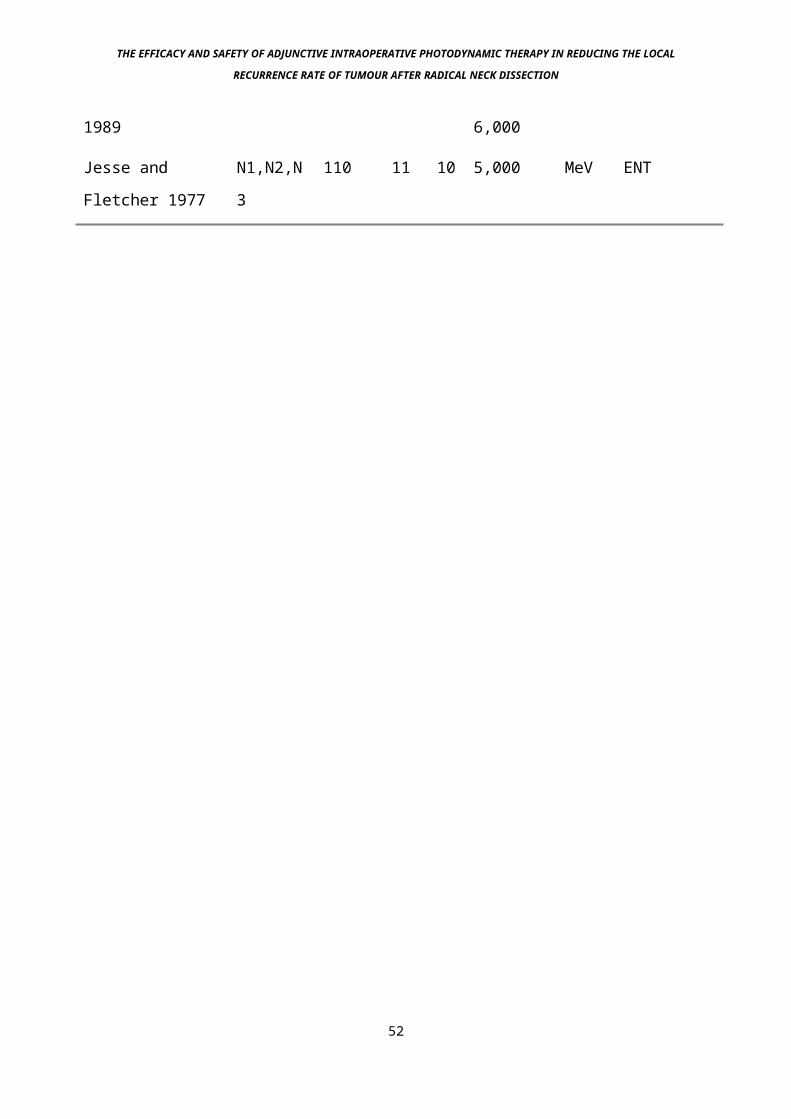
These figures show that on average there is a local recurrence
rate in the neck after radical neck dissection of around 30%
without pre or postoperative radiotherapy. This rate is
approximately halved by the addition of radiotherapy (table 8).
Since as previously stated, persistent neck disease is a major
cause of death in patients with HNSCC, there is clearly a place
for a successful adjunctive treatment during radical neck
dissection, to reduce the local recurrence rate. Data is not
47

THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
available on the presence or absence of extracapsular spread in
these cases or on the level of the involved nodes.
48
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
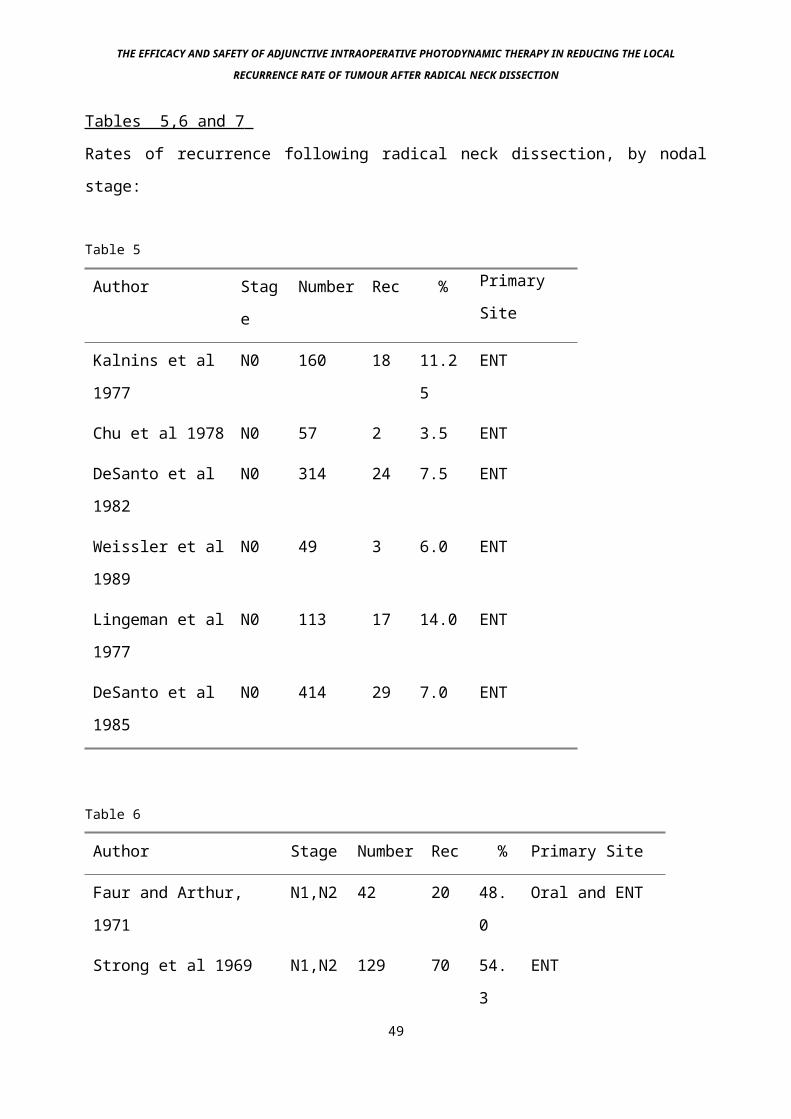
Tables 5,6 and 7
Rates of recurrence following radical neck dissection, by nodal
stage:
Table 5
Author Stag
e
Number Rec % Primary
Site
Kalnins et al
1977
N0 160 18 11.2
5
ENT
Chu et al 1978 N0 57 2 3.5 ENT
DeSanto et al
1982
N0 314 24 7.5 ENT
Weissler et al
1989
N0 49 3 6.0 ENT
Lingeman et al
1977
N0 113 17 14.0 ENT
DeSanto et al
1985
N0 414 29 7.0 ENT
Table 6
Author Stage Number Rec % Primary Site
Faur and Arthur,
1971
N1,N2 42 20 48.
0
Oral and ENT
Strong et al 1969 N1,N2 129 70 54.
3
ENT
49
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Kalning et al 1977 N1,N2 93 58 62.
3
ENT
Chu et al 1978 N1,N2 133 41 30.
5
ENT
DeSanto et al 1982 N1,N2 338 100 29.
5
ENT
Jesse and Fletcher
et al 1977
N1,N2 172 33 19.
1
ENT
Lingeman et al 1977 N1,N2 218 42 19.
2
ENT
DeSanto et al 1985 N1,N2 416 106 25 ENT
50
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Table 7
Author Stage Number Rec % Primary
Site
Beahrs et al
1961
N0, N1,
N2
615 163 26.
5
ENT
Strong et al
1969
N0, N1,
N2
204 75 36.
3
ENT
Martin et al
1951
N0, N1,
N2
599 203 33.
9
ENT
Table 8 Preoperative radiotherapy given:
Author Stage Numbe
r
Rec % Dose Powe
r
Primary
Site
Jesse and
Lindberg 1975
N2, N3 57 4 7 6,000 MeV ENT
Jesse and
Lindberg 1975
N2, N3 49 2 4 6,000 MeV ENT
Farr and
Arthur 1971
N1, N2 43 12 28 2,000 MeV ENT /
ORAL
Wei et al 1990 N1, N2 50 7 14 7,000 MeV ENT
Strong et al
1969
N0,N1,N
2
144 34 24 2,000 MeV ENT
Weissler et al N0 17 1 6 4,000 - MeV ENT51
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
1989 6,000
Jesse and
Fletcher 1977
N1,N2,N
3
110 11 10 5,000 MeV ENT
52
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
2g: Cause of local recurrence
The cause of local recurrence after radical neck dissection is
thought to be due to either the spillage of viable tumour cells
onto the surgical bed during the operation, or the incomplete
excision of all involved lymph nodes (Beahrs and Barber 1962).
An interesting study by Harris and Smith in 1960 demonstrated
viable tumour cells in washings taken from the operative bed
following macroscopically tumour-free head and neck surgery. The
presence of these cells however did not influence the rate of
local recurrence, this may be due to microscopic examination of
the washings missing tumour cells in those cases in which no
cells were seen.
It is interesting to speculate why patients with pathologically
confirmed N0 disease develop any recurrent cancer at all in the
neck as shown in the previous tables. This is most probably due
to the malignant cells being missed during pathological
examination. A pathologist scanning cut sections of a lymph node
would usually be able to detect one abnormal cell from among 100
normal cells, but he/she could not be expected to detect one
abnormal cell in 1000 normal cells. Since 1 gram of tissue
contains 1,000,000,000 cells, if there were one abnormal cell in
1000 missed, there could be 1,000,000 cells in that 1 gram node,
yet no pathologist would call that node positive (Ariyan et al
1977). Therefore, the only definitive report regarding a lymph
node dissection specimen is one reporting a positive finding. A
53

THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
negative report only gives a probability of being free of tumour
(Ariyan 1986).
54
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
2h Treatment of metastatic neck disease
2h(i) Radical neck dissection
Following initial work by Crile (1906), the technique of block
neck dissection was modified with time by many surgeons, most
notably Brown and McDowell (1944), Ward et al (1959) and Beahrs
et al (1955 and 1977). In time it came to be called a radical
neck dissection, as described by Martin (1951). This was because
he advocated a radical treatment for operable head and neck
cancers, and particularly stressed the importance of removing
the entire block of lymph nodes in the neck, in continuity with
the primary tumour if the operation was simultaneous. Martin
felt that there was no place for partial surgery in the
treatment of neck disease from a primary HNSCC tumour.
Prior to performing an isolated radical neck dissection it is
necessary to fully endoscope the patient, including bronchoscopy
and oesophagoscopy to assess for recurrence at the primary site
and the presence of synchronous primary tumours, both of which
significantly alter the treatment options (Gluckman 1979).
The incision made for the operation depends mainly on whether
the patient has had preoperative radiotherapy, and the surgeon's
own preference. Because the entire lateral neck area needs to be
exposed, an incision will be needed that allows both cranial and
caudal dissection along with anterior and posterior dissection.
This is best achieved using two incisions, an antero-posterior
arm joining a crania-caudal arm. The problem with any of the
incisions based on this premise is that there will be a junction
between the two arms, which will inevitably be a weak point55
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
that, in the event of poor healing due to radiotherapy, may
result in dehiscence. On its own that would be relatively minor.
However, once a radical neck dissection has been performed, the
carotid artery sits adjacent to the skin - any skin breakdown
could therefore expose the artery and lead to its potential
rupture due to chronic inflammation, with obvious consequences.
The prospects for poor healing and chronic inflammation are
enhanced by the presence of preoperative radiotherapy.
56
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Thus if two incisions that join are to be made after
radiotherapy, the junction should be posteriorly based, over the
anterior border of trapezius, minimising the risk of carotid
exposure if dehiscence occurs. Other options include using an s-
shaped incision or two separate anteroom-posterior incisions.
The s-shaped incision has problems with spontaneous dehiscence
of the anterior part of the lower curve due to poor vascularity
of this tip, and the twin incision (Macfee) makes the operation
technically more difficult. Both approaches also compromise a
full view of the neck.
For a non-irradiated neck a caudally curved anteroposterior
incision from mastoid tip to greater cornua of hyoid can be used
in conjunction with a lazy s-shaped caudal incision from the mid
point of the anteroposterior incision, into the supraclavicular
fossa. This gives the best exposure with a good cosmetic result
and little chance of skin flap non-viability. In the irradiated
neck, the previously mentioned posteriorly based incision is
safest, although some restriction of the anterior view is not
uncommon.
Once the skin flaps have been raised and sutured away from the
operative site in a sub-platysmal plane, the dissection can
begin. The key to the operation is to find the floor of the
resection, in the sub-omohyoid plane. There are many ways to do
this, such as by identifying the lower limits of the jugular
vein in the neck, ligating and dividing this, then working
posteriorly along the clavicle along the floor of the posterior
57
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
triangle sweeping all tissue postero-laterally until the
trapezius muscle is reached. The dissection can then be swept
superiorly along the anterior edge of the trapezius muscle in
the same subomohyoid plane, just superficial to the deep
investing layer of cervical fascia. At the cranial limit, the
dissection is turned anteriorly at the mastoid tip, so
identifying the upper limit of the jugular vein in the neck,
ligating and dividing this and continuing the dissection
anteriorly across the whole neck, including the submandibular
region. In order to reduce venous pressure during the procedure,
the internal jugular vein can be ligated at its cranial end
first, although there is a theoretical risk that this may allow
tumour emboli to pass down the vein during the first part of
surgery.
The common, internal and external carotid arteries and carotid
body are left behind in the bed of the operation, along with the
vagus, hypoglossal and phrenic nerves and the cervico-mandibular
trunk of the facial nerve. The rest of the bed is made up of the
deep investing layer of cervical fascia, and associated
musculature. The midline neck structures such as larynx and
pharynx are usually separated from the operative site by the
strap muscles, other than the omohyoid, unless they are being
removed in continuity. Other important structures in the bed of
the operation include the brachial plexus deep in the floor of
the posterior triangle, between Scalenus Anterior and Scalenus
Medius muscles.. This is usually not seen since it lies too
deep, and for the purposes of this study has not been deemed to
be significant. The parotid gland lies in the superior margin of58

THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
the operative site - this is useful since it protects the upper
3 branches of the facial nerve.
59
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
2h(ii): Conservative neck dissection
During a radical neck dissection, a number of important
structures such as the accessory nerve, sternocleidomastoid
muscle and internal jugular vein are removed. This is because
all the possible cancer bearing structures are required to be
removed. However, a number of other structures in the same
tissue plane are not removed, e.g. the common carotid artery,
the vagus nerve, the hypoglossal nerve and the phrenic nerve.
The reasons for not removing them are obvious - to do so would
cause an unacceptably high morbidity rate. It does raise the
question however, is it necessary to remove the other structures
mentioned? The aim of the operation is to completely remove the
tissue containing all the lymph nodes. The lateral spaces of the
neck, in which the major vessels and lymph nodes sit, are filled
with loose connective tissue. This tissue surrounds the lymph
nodes and is divided into compartments by a series of fascial
planes, although it is essentially one structure. These
compartments may be removed en bloc from other structures in the
neck such as the muscles and major neurovascular structures by
carefully dissecting them free, whilst keeping the whole block
of lymph nodes unviolated. This is the basis of the modified or
conservative neck dissection. The basic reason for developing
this procedure as an alternative to radical neck dissection was
because of the side effects of removing all the structures named
above (Bocca 1975).
60
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
The results of this technique have been encouraging (see table
8), although nodal staging data is not available in all the
cases in this table. Increasingly and particularly when treating
the node-negative neck in those patients with primary tumours
and a high likelihood of neck node metastasis, a conservative
neck dissection will be performed in continuity with resection
of the primary site as advocated by Martin. Additional
structures left behind in the bed of this operation above those
left after a standard radical neck dissection include the
sternocleidomastoid and omohyoid muscles, the internal jugular
vein, the accessory nerve and the transverse cervical vessels.
61
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
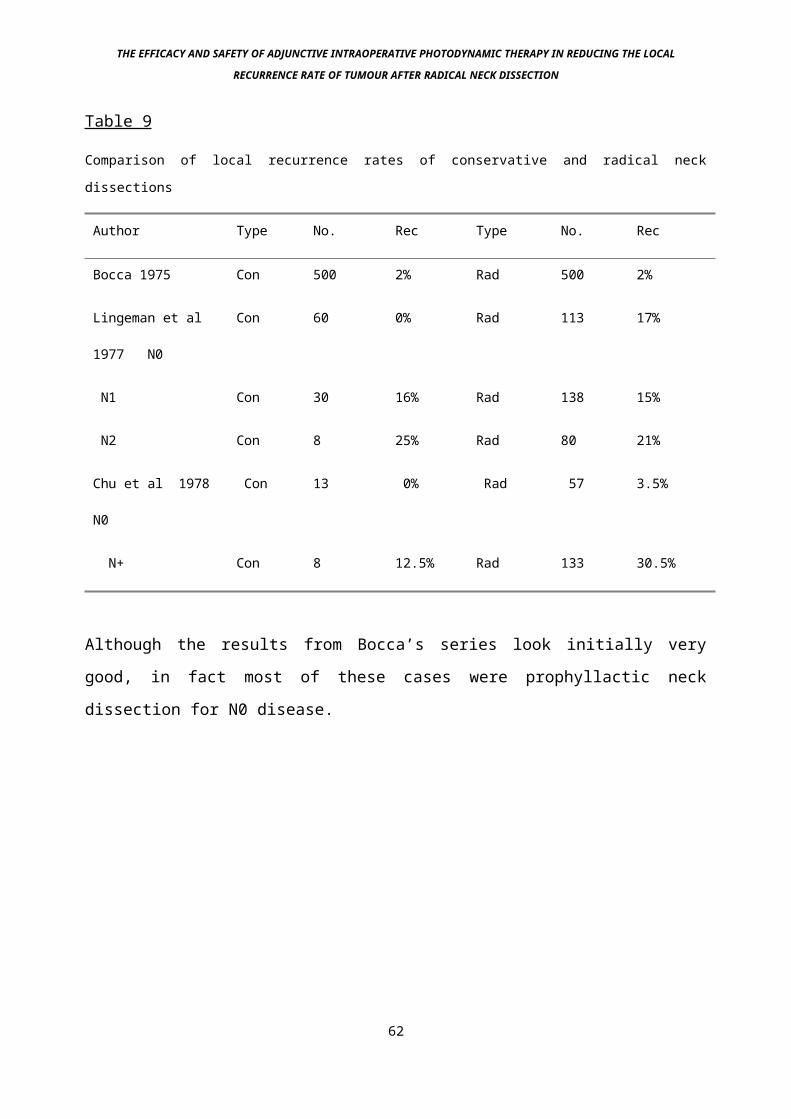
Table 9
Comparison of local recurrence rates of conservative and radical neck
dissections
Author Type No. Rec Type No. Rec
Bocca 1975 Con 500 2% Rad 500 2%
Lingeman et al
1977 N0
Con 60 0% Rad 113 17%
N1 Con 30 16% Rad 138 15%
N2 Con 8 25% Rad 80 21%
Chu et al 1978
N0
Con 13 0% Rad 57 3.5%
N+ Con 8 12.5% Rad 133 30.5%
Although the results from Bocca’s series look initially very
good, in fact most of these cases were prophyllactic neck
dissection for N0 disease.
62
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
2I: Treatment of macroscopic residual disease
Macroscopic disease may be left in the bed of a radical neck
dissection if it involves vital structures, in particular part
of the common or internal carotid arteries (Olcott et al 1981).
Normally such cases would be considered inoperable and radical
surgery not be performed. However, sometimes the extension of
the disease process is greater than initially thought
preoperatively, and such a situation will arise from time to
time. Thus “inoperable” tumours will be operated upon until it
is realised that the tumour is too advanced for the planned
surgery. In the event of macroscopic tumour invading the common
carotid artery, it may still be possible to remove the tumour if
it is only involving the adventitial tissues (Kennedy J.T. et al
1977). However, should it be deeper than this, the risks of
carotid rupture will be too high (Huvos et al 1973). In this
situation, the artery can be ligated and removed, or can be
bypassed and removed. Both of these procedures are associated
with very high morbidity (Biller et al 1988, McReady et al
1989, Moore and Baker 1955). It may be better to simply close up
once advanced disease is found and consider postoperative
chemotherapy or perhaps brachytherapy. In these situations
problems may still occur, since if the tumour is successfully
destroyed, spontaneous carotid rupture might still occur since
the tumour may make up the only viable arterial wall. For this
reason, PDT may cause exactly the same problem and its role in
this situation is unproven. If invasion of the carotid tree is
63
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
suspected, it is prudent to perform pre-operative digital
subtraction angiography.
Adjunctive intraoperative radiotherapy has been used with some
success, but the logistics of this make it virtually impossible
in the typical clinical situation (Freeman et al 1990).
64
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
3: Radiotherapy
3a: Introduction
Radiotherapy was first used in the treatment of cancer during
the early part of the twentieth century, radium and its
cytotoxic properties having first been discovered by Marie Curie
in 1898. The first treatments were for superficial lesions,
using orthovoltage (250-400 kilovolt (KV)) radiation, from
sources such as radium. Not only malignant but benign lesions
were treated, although since the discovery of radiotherapy
induced tumours, the practice of treating benign lesions has
been abandoned. The more modern radiotherapy equipment that has
been around for the last 50 years involves the use of radium and
cobalt sources of higher energy, along with linear accelerator X
rays, which can reach energies of up to 25 mega-electron volts
(MeV). Other forms of particle irradiation include neutrons and
protons, although these are still in the evaluatory stage.
The radiation energy used in routine clinical practice tends to
be gamma (particle derived from spontaneous emission from the
atom nucleus) or X (same particle, created artificially)
radiation.
The mode of action of radiotherapy is unsure. Its effect may be
explained by the fact that tumour and normal cells are
distinguished by the former's ability to proliferate
indefinitely. This is associated with a high rate of cell
turnover. Radiotherapy may have its effect because of its
ability to ionize and hence defunction DNA - the more rapidly a65
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
cell is dividing, the less time there is for DNA repair and
hence eventual loss of DNA function occurs, leading to cessation
of multiplication and cell death. Radiotherapy also causes the
formation of intracellular free radicals, such as singlet
oxygen, which are highly toxic and also cause cell death. The
true mode of action may well be a combination of both forms of
damage.
66
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
3b: External Beam Radiotherapy
As its name suggests, this form of radiotherapy is given from
outside the body, and is delivered by means of electromagnetic
radiation from one of several different sources. Initially these
sources were from relatively low voltage linear accelerators, or
shielded Cobalt isotopes. Once mega (million) voltage linear
accelerators had been created, the scope for treating larger and
less accessible tumours increased. This is for two reasons:
1) The absorption of electromagnetic radiation is exponential.
Therefore, the more energy a beam of particles has, the deeper
an effect will be seen in tissue.
2) A peculiar characteristic of megavoltage radiotherapy is its
skin sparing effect. Due to physical characteristics of
electromagnetic radiation beyond the scope of this chapter, a
surface sparing effect is seen. The maximum effect of this form
of radiation is therefore seen below the surface, the depth
below the surface being relative to the voltage applied to
produce the electromagnetic radiation. This allows toxic doses
of radiotherapy to structures below the skin, without killing
the skin itself.
67
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
The sources used for external beam radiotherapy in the Head and
Neck include:
Radium - low energies produced from this source treat
superficial depths only, therefore these machines are useful for
skin and lip cancer.
Cobalt 60 - a very commonly used source for Head and Neck
cancer. Gamma radiation of around 1.2 MeV produced from Cobalt
60 will penetrate most parts of the Head and Neck.
Linear Accelerators - very high energy particle are produced
from these machines, allowing deep penetration to most parts of
the body. Not so useful for Head and Neck cancer, although the
treatment of deep seated nodes or tumours can be effective with
these very high energy particles.
Electrons - electron beam radiotherapy is becoming increasingly
used for Head and Neck cancer. This is because it is associated
with rapid dose build up then equally rapid fall off after a
certain depth, depending on the energy of the electrons
produced. Therefore in those areas where a sharp fall off is
required, such as around the cervical spine or brain, they can
be very useful. However, little skin sparing is seen, so skin
68

THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
necrosis is possible at higher doses. For that reason it is
often used to 'top up' after photon radiation.
69
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
3c: Brachytherapy
This form of treatment involves the local treatment of tumours
from within, hence it is also called interstitial radiotherapy.
It involves the insertion of a radioactive device into or next
to the tumour to be treated, thus delivering a high dose of
radiation to the tumour, but little to surrounding normal
tissue, since sources producing low penetration beams are often
used, such as Beta radiation sources. This technique is
particularly useful for treating cavities, when a prosthesis
lined with radioactive material can be inserted next to the area
to be treated. The advantages of brachytherapy are maximised
when it is given following external beam radiotherapy, boosting
the usual treatment dose.
The most common form of brachytherapy is with radium needles.
These are inserted into the area to be treated and removed after
the correct dose has been given. However this can cause
excessive radiation exposure to medical and nursing personnel.
Other commonly used techniques include the administration of
radioactive iridium wire or seeds. The safest way to perform
brachytherapy is by the afterloading technique in which a tube
is inserted through the area to be treated followed by the later
mechanical passing of the wire or iridium containing device into
the tumour, with medical personnel observing safely from a
distance.
70
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
3d: Efficacy of Radiotherapy
Radiotherapy, whether external beam or brachytherapy, is often
effective against early squamous cell carcinoma, but often fails
when tumours present later than T2 stage, which often happens in
the Head and Neck area (Johansen et al 1990). In order to be
able to cure such a tumour, a number of criteria need to be
fulfilled.
1) Small tumour volume, so that a very high concentration of
energy can be achieved.
2) Minimal hypoxia within the tumours. This generally equates to
tumour size, since tumours grater than one centimetre diameter
will often have outgrown their blood supply, leading to central
hypoxia. The presence of oxygen is vital for the cytotoxic
effect of radiotherapy.
3) Easily accessible tumours allowing the use of more than one
field to treat the tumour site, minimizing normal tissue damage.
71
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
3e: Side Effects of radiotherapy
Radiotherapy, whether external beam or brachytherapy is
associated with not inconsiderable side effects, particularly
when given to the Head and Neck. The standard amount of
radiotherapy that is thought to be safe and tumoricidal is
around 6,000 rads. This has to be divided up into fractions,
usually daily on the premise that normal tissue, being normal,
can repair itself quicker than malignant tissue, being abnormal.
Thus in the 24 hours between doses, the normal tissue has
repaired, the malignant tissue has not. This lack of repair in
malignant tissue ends up with the tumour dying, as previously
mentioned. However, the amount of radiation to the cervical
spine has to be limited to 4000 rads, since any dose greater
than this has a high risk of causing inflammation and
irreversible damage to the spinal cord (transverse myelitis).
Because bone absorbs ionizing radiation strongly, there is a
risk of osteoradionecrosis if too much radiation is given to the
bone, giving great problems with dosimetry in the head and neck,
which has bone within most treatment portals.
The minor and major salivary glands are often irreversibly
damaged by radical radiotherapy with subsequent loss of saliva
secretion leading to xerostomia. Taste buds in the mouth are
often totally destroyed. During radiotherapy, an inflammatory
reaction develops in the mucous membranes of the upper
aerodigestive tract, leading to mucositis, an acutely painful
condition that may cause severe dysphagia, necessitating
nasogastric feeding for several weeks on occasion. 72
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Careful attention needs to be paid to the state of the teeth and
gums. Any disease of this area must first be eradicated prior to
radiotherapy, since there is a high risk of osteoradionecrosis
of the mandible and maxilla developing from such lesions during
radiotherapy. Skin care is also important, since the erythema
that almost always develops may be followed by moist
desquamation and breakdown during radiotherapy (Rao and Levitt
1986).
Radiotherapy may induce new malignancies to form in treated
tissue. These usually develop at least 10 years after treatment,
and the majority occur in connective tissue, being sarcomas or
fibrosarcomas on histology (Larson et al 1990).
Radiotherapy may also damage the major vessels of the neck. The
most important of these is the carotid tree. Damage to this set
of vessels includes rupture and stenosis, with an estimated 25%
of vessels being damaged as a direct sequel of treatment
(Elerding et al 1981). Radiotherapy may also cause carotid
artery thrombosis (Call et al 1990) and atherosclerosis (Glick
B., 1972, Hayward R.H., 1972)
Radiotherapy is cumulatively toxic, which means that once the
safe maximum dose of radiation has been given, no more can be
added if treatment fails (Anderson R.E., 1985).
73
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
3f: Role of radiotherapy in neck malignancy
There is debate as to if and when radiotherapy should be used
for metastatic neck disease from a Head and Neck primary. The
decision to go ahead rests on 3 main factors:
1) No previous radiotherapy to the proposed area of treatment
(most of the lateral neck). This usually excludes those patients
who have had radiotherapy to a primary pharyngeal or laryngeal
lesion.
2) Small node tumour volume - the larger the tumour the more
likely that hypoxic conditions within the tumour will occur,
greatly reducing the efficacy of the treatment, which depends
upon generation of oxygen-based free radicals for its effect on
DNA. The widely touted maximum tumour diameter for curative
radiotherapy is 2cm, although many institutions, particularly in
the U.K. would treat even larger metastases with curative
intent.
3) Disease at the primary site. If there is recurrence at the
primary site or within the upper aerodigestive tract, it is
often better to perform en bloc resection of both sites,
particularly if radiotherapy has been given to the primary site.
New cancers with associated neck nodes are often large in
volume, again despite a small neck node, en bloc resection would
be the treatment of choice.
74
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Radiotherapy is very useful in metastatic neck cancer when given
in conjunction with surgery, and can be given pre or post
surgery (Mantravadi et al 1983).
75
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
3g: Pre or Post operative radiotherapy?
Preoperative radiotherapy: The peripheral tumour that might be
close to surgical margins can be sterilised with preoperative
radiotherapy, preventing burst and spill of viable microscopic
tumour residue into the operative site. Preoperative
radiotherapy might also convert a non-resectable tumour into a
resectable one.
Postoperative radiotherapy: Radiotherapy can be given
postoperatively to kill off any microscopic tumour left behind
at surgery. This has the added advantage that more will be known
about the disease once the majority has been removed, such that
planning of the depth and site of radiotherapy will be more
accurate, and, depending on the specimen, whether radiotherapy
is needed at all. If the metastasis is of a very early, good
prognosis stage, radiotherapy could be held back in case of
further recurrence. Radiotherapy also reduces the rate and
efficacy of wound healing after surgery, and may therefore be
better given after surgery.
76
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
INTRODUCTION PART II
4: Photodynamic Therapy
4a: Development and Principles
Photodynamic therapy (PDT) as a principle has been around since
the early part of the 20th century. A photodynamic effect was
first described by Raab in 1900, when he reported the death of
Paramecia following the administration of a combination of
acridine and light, though not with either agent solely (Raab,
1900). This effect was first used on tumour cells in 1903, when a
combination of eosin and light was used to treat skin cancer (V
Tappeiner and Jesionek 1903) Further studies throughout the
earlier part of the 20th century began to define some of the
important concepts in this potential treatment, in particular
skin photosensitivity (Meyer-Betz 1913). The history of
Photodynamic Therapy’s development has been summarised by
Daniell and Hill in 1991.
PDT relies upon the fact that some chemically inert compounds
can be activated by light to produce locally toxic effects.
These chemical compounds are called photosensitisers, and the
locally toxic effect is largely due to singlet oxygen production
(Weishaupt et al 1976), a substance that is highly oxidative and
therefore destructive to adjacent biological structures
(Takemura et al 1991). The principle of light activation of
chemical compounds is not new, photosynthesis relies on just 77
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
such a principle, although the end result of activation with
photosynthesis is constructive rather than destructive as with
photodynamic therapy. Despite this, photosynthesis requires the
presence of orange and yellow pigments to quench spin-off
reactants that arise from photosynthesis.
Drugs that are activated by light tend to have ring structures
similar to that of porphrins, alteration of the configuration
of this ring is what makes one photosenstitising drug different
from another. Ring configurations can be changed to make
photosensitising drugs more efficient, more selective and, by
increasing the activating wavelength, more deeply effective (see
figure 1).
78
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
The Porphyrin ring structure has the ability to absorb light of
the correct energy, such that when absorption occurs, the drug
molecule is excited to a higher energy level. This can decay to
an intermediate product, then transfer its energy to oxygen –
resulting in the formation of singlet oxygen and at the same
time returning the photosensitiser to it’s ground state ready to
absorb another photon. Singlet oxygen is a highly reactive and
toxic species, which almost instantaneously oxidises any
adjacent structure (Bonnet 1994). If enough singlet oxygen is
created locally within a cell, this leads to cell death due to
overwhelming damage to vital intracellular organelles. Because
those photosensitisers in common use for PDT do not appear to
enter the nucleus, there is little risk of DNA damage and
potential carcinogenicity. This is because the half life of
singlet oxygen and its sheer reactivity would not lend enough
time for it to penetrate into the nucleus from the cytoplasm in
sufficient amounts to cause damage.
Some controversy exists over whether the main site of action is
intracellular as described above (Moan et al 1982, Pass et al
1991), or extracellular – i.e., vascular (Selman et al 1984,
Henderson et al 1984, Henderson et al 1985, Henderson and
Dougherty 1992). The latter relies on the fact that
microcirculatory damage undoubtedly occurs during PDT and that
this may lead to anoxic cell death. More likely, both
mechanisms have a part to play in the overall effect (Nelson et
al 1987, Bown 1990). Autoradiographic and microfluorescence
studies have certainly demonstrated significant levels of
intracellular drug, linked to vital cellular organelles when 79
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
comparing malignant and normal tissue (Gomer et al 1979,
Bugelski et al 1981), and benign diseased/normal tissue
(Shikowitz et al 1989).
When considering the treatment of malignant disease, it is
important to think about the potentially hazardous effects of
the treatment (Pope and Bown 1991), in particular whether the
treatment itself might extend the stage of the disease. This is
particularly true in the treatment of primary cancers, since
there is always a possibility that in curing the primary, cells
will be shed off into the lymphatics, causing metastases. With
photodynamic therapy being a non-traumatic, non-ablative
biostimulatory procedure, it seems very unlikely that this would
occur. Work by Gomer et al in 1987 helped support this.
Accurate dosimetry of light to the treated area is of obvious
importance, since a supra-threshold amount of light is needed
for tumour destruction. This is an area that may yield great
advantages in selective bleaching of photosensitiser, leading to
a very tumour specific effect (Potter et al 1987).
Photodynamic Therapy has been increasingly used over the past
20 years for the treatment of malignant disease, in particular
Head and Neck cancer (Gluckman J.L. 1991). Treatment has focused
on solid, visible tumours with the best results being achieved
with early disease (Monnier Ph. et al). Other main avenues for
exploration clinically have been skin (Lipson and Baldes 1961),
bladder (Kelly and Snell 1976), brain (Kaye 1987), bronchus
(Edell and Cortese 1987) and gastrointestinal tract (Bown 1990).
80
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
4b: Photodynamic Therapy for Head and Neck cancer
Photodynamic therapy has a potential to be particularly
beneficial for the treatment of Head and Neck cancer for two
main reasons - its ability to locally and non-thermally destroy
malignant tissue, and its selectivity for tumours above the
surrounding normal tissue. This leads to rapid healing with
retention of form and function, and minimal damage to
surrounding normal tissue. The two other mainstay treatments for
Head and Neck cancer, radical surgery and radiotherapy, do not
share this low morbidity outcome, both being associated with
major degrees of post-treatment morbidity (see Chapter 3). This
is particularly important in the Head and Neck, since loss of
functions such as speech, swallowing, smell, taste are a great
problem to patients, as are the poor cosmetic results of radical
surgery. The other main alternative to surgery or radiotherapy
in the Head and Neck, chemotherapy, has not been found to be
useful so far (Amrein P. 1991). Photodynamic therapy is also of
great value as an alternative treatment because once given, if
local recurrence occurs, the otherwise standard treatments of
radiotherapy or surgery can be given with no loss to the
patient. Indeed, PDT might be one day given to reduce the bulk
of tumours prior to standard treatments, rather like induction
chemotherapy. The rational for this is that both surgery and
radiotherapy work better with lower tumour mass. This is
particularly true of radiotherapy, the success of which is very
much volume-dependant, larger tumours having to some degree
outgrown their blood supply. This leads to an anoxic centre, 81
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
which will not respond. That is because radiotherapy relies on
the presence of oxygen for its effect, although PDT is also to
some degree limited by this (Henderson and Fingar 1989).
However, the reduction of tumour bulk remains an important
concept in cancer treatment and PDT may eventually find a role
in this.
The main role of PDT in Head and Neck cancer is with respect to
the primary treatment of early cancers, whether initial or
synchronous tumours (Gluckman 1991). These are generally defined
for the purposes of PDT and investigations into its efficacy as
those tumours with a maximum assessed depth of 5 mm, lateral
spread no greater than 3 cm, no regional or distant spread and
no involvement of deep structures.
82
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
4c: History of PDT for Head and Neck cancer
Following the first published clinical trial using PDT for
cancer (Kelly and Snell 1976), much interest was stirred among
those treating cancer throughout the body. For the reasons
mentioned above, PDT for Head and Neck cancer was particularly
attractive due to the major problems incurred when using
standard methods of treatment. The first mention of PDT being
used therapeutically in the Head and Neck area was in 1978
(Dougherty et al). The first cases treated were usually
palliative, the impressive initial results being independently
confirmed in a paper by Forbes et al in 1980. Dahlman et al in
1983 first reported a large series (20 patients, 26 tumours) in
which there was a complete response (defined as no evidence of
tumour at original site 30 days after treatment) in 5/14 locally
recurrent cancers treated. Keller et al in 1985 were the first
to use Photofrin 2 for the treatment of Head and Neck cancer,
their results in 31 cases again showing promising effect on
early cancers, although it was noted that large tumours and neck
tumours did not respond well. The role of PDT for palliation was
also felt to be encouraging (Schweizer et al 1993). Schuller et
al (1985) also produced a large series of patients, 24, in whom
necrosis of tumour was seen in all cases, with HpD. No mention
is made however of tumour staging or light dose, a problem that
has dogged meta-analysis of published work in PDT. The idea of
PDT being particularly useful for early Head and Neck cancer was
taken up by Gluckman in 1986, treating early tumours of the83
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
larynx, oral cavity and oropharynx with success. His
recommendations at the end of this article were 5 fold:
1) Because the anatomy of the Head and Neck lends itself to
visualisation down a rigid telescope, and because this often
involves closed-in access down a narrow endoscope, fibre-
delivered light for PDT is ideal in the Head and Neck area
generally.
2) Because of selective necrosis of tumour, large areas of
normal tissue could be safely irradiated, obviating the need for
on-table frozen sections of margins or suspicious areas.
3) Some procedures can be performed in an office setting,
reducing costs.
4) The treatment of field cancerisation or other large area
tumours is particularly appropriate with this treatment, with
optimal preservation of normal tissue.
5) No cumulative toxicity means recurrent lesions can be safely
re-treated, unlike radiotherapy.
A similar drug to Photofrin and HpD called Photosan 3 was also
reported to be effective particularly for skin tumours of the
Head and Neck region, by Feyh in 1990. A very large series was
produced from China in 1991 again showing excellent tumour
necrosis with no residual local tumour seen at 5 years follow up
with 34/72 complete remission cases achieved out of 114
treatments. These studies were backed up by other series during84
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
the 1980’s and early 1990’s using HpD or Photofrin, including
work by Biel, Schweizer, Grant, Carruth and Monnier (see table).
In all these series, a powerful tumour response to PDT has been
seen with the best results achieved with early disease.
At this stage, new drugs, called “second generation”
photosensitisers began to appear in the clinical field. These
compounds had been manufactured to try to amplify the beneficial
effects of PDT by looking at the chemical properties of
Haematoporphyrin, HpD, Photofrin etc., and picking target areas,
such as the ring structure, or side arm structure, and
continually test every variant as it came out, until more
powerful compounds were produced (Bonnet et al 1989(1)).Of the
second generation drugs, only 2 have currently been used in the
treatment of Head and Neck cancer (see below). These are meta-
Tetra(hydroxyphenyl)chlorin (FoscanR), and delta-Aminolaevulinic
acid (d-ALA). Results with the first drug have been very
encouraging for Head and Neck cancer (Dilkes et al 1994, 1995,
1996, Savary et al 1997). The second drug, d-ALA has been very
useful topically for early skin cancer or solar (actinic)
keratosis, but for more advanced Head and Neck malignancy it is
not powerful enough (Grant et al 1993). Table 9 briefly
summarises those cases available for scrutiny in the literature.
It was not possible to include tumour stage or success rates in
this table because in many cases that data is not adequately
described. This has been one of the failings of the development
of PDT, inadequate description of published data. However, in
all the cases mentioned, tumours treated were found to respond
at least partially to the effects of PDT.85
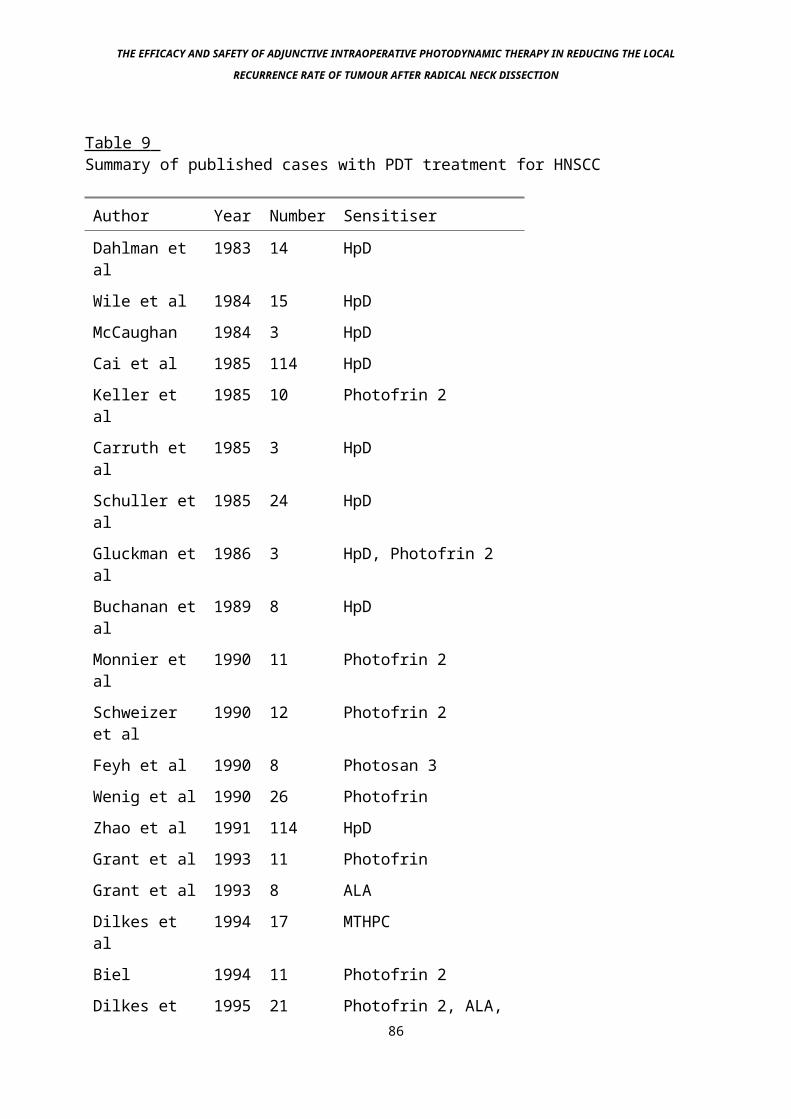
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Table 9 Summary of published cases with PDT treatment for HNSCC
Author Year Number Sensitiser
Dahlman et al
1983 14 HpD
Wile et al 1984 15 HpDMcCaughan 1984 3 HpDCai et al 1985 114 HpDKeller et al
1985 10 Photofrin 2
Carruth et al
1985 3 HpD
Schuller etal
1985 24 HpD
Gluckman etal
1986 3 HpD, Photofrin 2
Buchanan etal
1989 8 HpD
Monnier et al
1990 11 Photofrin 2
Schweizer et al
1990 12 Photofrin 2
Feyh et al 1990 8 Photosan 3Wenig et al 1990 26 PhotofrinZhao et al 1991 114 HpDGrant et al 1993 11 PhotofrinGrant et al 1993 8 ALADilkes et al
1994 17 MTHPC
Biel 1994 11 Photofrin 2Dilkes et 1995 21 Photofrin 2, ALA,
86
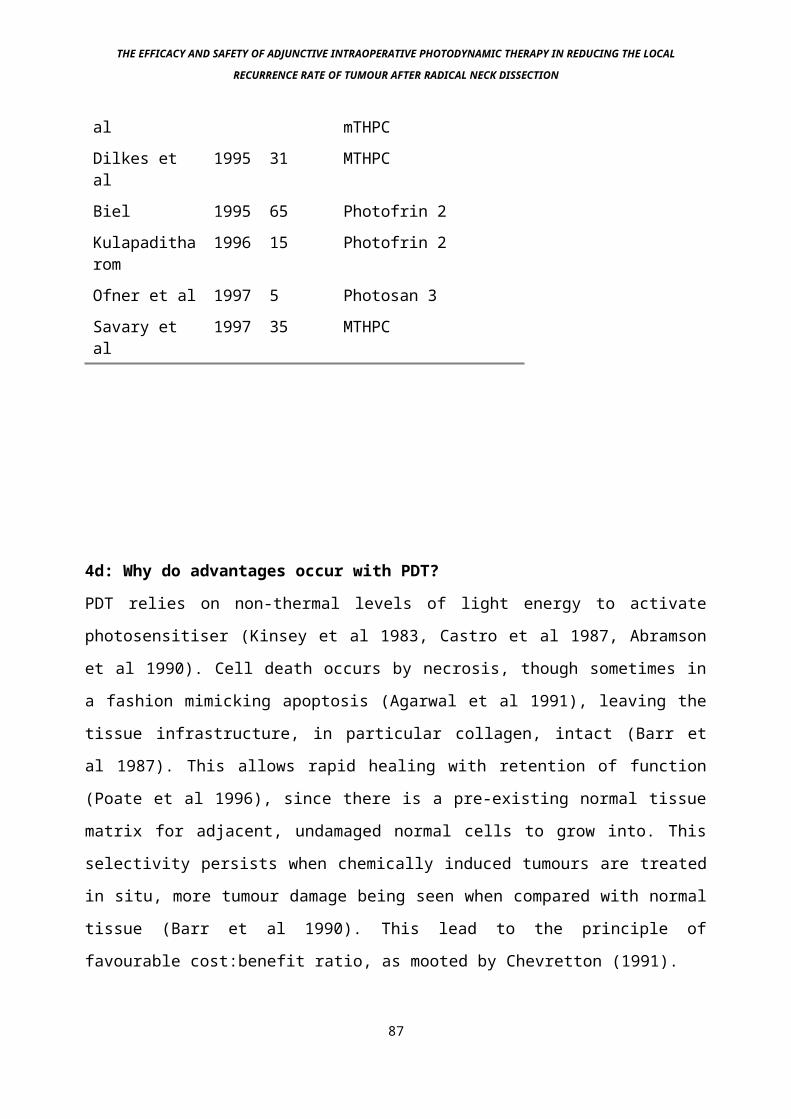
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
al mTHPCDilkes et al
1995 31 MTHPC
Biel 1995 65 Photofrin 2Kulapaditharom
1996 15 Photofrin 2
Ofner et al 1997 5 Photosan 3Savary et al
1997 35 MTHPC
4d: Why do advantages occur with PDT?
PDT relies on non-thermal levels of light energy to activate
photosensitiser (Kinsey et al 1983, Castro et al 1987, Abramson
et al 1990). Cell death occurs by necrosis, though sometimes in
a fashion mimicking apoptosis (Agarwal et al 1991), leaving the
tissue infrastructure, in particular collagen, intact (Barr et
al 1987). This allows rapid healing with retention of function
(Poate et al 1996), since there is a pre-existing normal tissue
matrix for adjacent, undamaged normal cells to grow into. This
selectivity persists when chemically induced tumours are treated
in situ, more tumour damage being seen when compared with normal
tissue (Barr et al 1990). This lead to the principle of
favourable cost:benefit ratio, as mooted by Chevretton (1991).
87
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Selectivity with respect to an increase in the amount of damage
sustained by tumour tissue when compared to normal tissue
undoubtedly occurs. It was first described by Policard in 1924
and nicely demonstrated by Figge and Weiland in 1948 and
Rasmussen-Taxdal et al in 1955. Selectivity appears to be true
of virtually all the photosensitising drugs tested since then
(Dougherty et al 1978, Peng et al 1991, Pass et al 1993). There
are at least 6 possible reasons why selectivity occurs (Lin C.W.
1990):
1) Because tumours have an increased affinity for
photochemicals such as Photofrin and HPD over normal tissue.
This may be due to enhanced uptake due to altered tumour
metabolism and leaking, abnormal vasculature (Fingar 1990) or
the upregulation of low density lipoprotein (LDL) receptors in
cancer cells (Kessel D., 1986). These effects may well be
mediated by prostaglandins or other local hormonal mediators
(Ben-Hur et al 1988, Henderson and Donovan 1989).
Photosensitisers tend to be lipophilic and therefore carried on
LDL.
2) The preferential tumour localisation of photosensitizers may
also be caused by special properties of tumour tissue, such as a
low pH (Wike-Hooley L. et al 1984.), the presence of large
numbers of macrophages (Eccles S.A. and Alexander P. 1974), a
high density of lipoprotein receptors , and a relatively large
amount of newly synthesised collagen (El-Far M.A. and Pimstone
N.R., 1985).
3) Tumour selectivity can also be achieved by applying a
treatment to which tumour tissue is more sensitive then88
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
surrounding normal tissue. Tumour cells generally seem to suffer
from a relative lack of nutrients and oxygen, due to their less
controlled and organised growth. This makes them more sensitive
to external or internal damage than normal tissue (West et al
1990). Since PDT may exert all or part of its effect due to
damage to the microcirculation supplying tissue, the relative
deficiency in tumour cells of vital nutrients and oxygen may
well cause them to be much more sensitive to this effect than
normal cells (West et al 1990, Ben-Hur and Orenstein 1991).
4) The larger than usual volume of interstitial space in tumours
may act as a reservoir for photosensitisers (Jain R.K. 1987).
5) Due to their altered metabolism, cancer cells may not clear
photosensitising drug as quickly as normally functioning cells,
again leading to a degree of selectivity with time.
6) Simply by aiming the light at tumours, hence sparing the
majority of surrounding normal tissue, a form of selectivity
will occur.
89
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
4e: Light for Photodynamic Therapy
The first light sources for clinical PDT were adapted arc lamps,
often slide projectors, passing through narrow band-width
filters (Lipson and Baldes 1960) to achieve relatively high
(hundreds of milliwatts per cm2) power outputs. However,
although useful for surface applications and diagnostic purposes
(Lipson et al 1961), filtered arc lamps were superseded as the
preferred light source for PDT by the advent of lasers of the
appropriate wavelength. The monochromatic nature of laser
radiation allowed maximal photosensitiser excitation, whilst the
directional properties of the laser emission permitted efficient
coupling of the light into single optical fibres, facilitating
treatment of relatively inaccessible sites, in particular the
Head and Neck region.
Light towards the infra red end of the visible spectrum is
beneficial for most indications of PDT. This is because maximal
penetration of tissue occurs at this wavelength as described by
Wan et al in 1981 on cadaveric tissue, then Anderson and Parrish
in 1982 on skin, and Wilson et al in 1985 on a selection of in vivo
and ex vivo tissue. This is summarised in figure 1. Work by Bown et
al (1986) confirmed these basic facts in an in-vivo model, using
two different photosensitising drugs. However because the energy
of each photon is inversely proportional to its wavelength,
eventually with increase in wavelength to the infra-red this
energy drops to such a level that they will not adequately
excite the photosenstitising drug to the triplet state - this
occurs at around 850 nm laser light wavelength (Moan 1990).90
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Therefore photosensitising drugs that act in this manner are
limited to activating wavelengths below 850 nm. Furthermore, as
the 850 nm level is reached, the generation of singlet oxygen
becomes an increasingly inefficient process, increasing
potential treatment times and removing one of the advantages of
the 2nd generation photosensitisers. Photosensitisers that
operate via type 1 mechanisms are not limited to this wavelength
region, and may be efficient up to 1270 nm wavelength, offering
maximal penetration through tissue. These compounds are not
currently available (Moan 1990). Light quanta above this
wavelength do not have the necessary energy to excite the
photosensitising drug up to its triplet state, the level that is
required in order to release the correct quantum of energy to
change the oxygen molecule on decay of the photosensitiser to
the ground state. So far lasers have been used that deliver
light in the 630 - 690 nanometre wavelength, although as new
photosensitising drugs are developed, these wavelengths will
move towards the 800nm range.
91
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Figure 1: The central curved line shows the transmittance of
light through tissue, peak transmission occurring at around 800
nm. The separate peaks are the absorption peaks of the different
groups of drugs. Of interest is the porphyrin peak in the blue
spectrum (400 nm), which is mimicked by most other
photosensitisers, especially mTHPC. This can be seen to be a
wavelength which is clinically not very useful due to low
penetration through tissue, but is responsible for a lot of the
sun-damage that occurs in exposed skin following systemic
delivery of photosensitising drugs.
92
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Currently used lasers have tended to be the gold vapour laser,
at 628 nm, used to activate Haematoporphyrin Derivative (HpD),
Photofrin 2, and amino-laevulinic acid (ALA), and the Copper
vapour or Argon Ion pumped dye lasers, able to cover the whole
range when used with a variety of dyes. The fact that these
systems produce either pulsed or continuous wave forms of laser
light does not seem to matter (Okunaka et al 1992). More
recently newer light sources have either made much more power
available (KTP-pumped dye laser) or been much cheaper and
portable than previous systems (Diode lasers and LED arrays:
Dilkes and DeJode 1995, DeJode and Dilkes 1995).
This all adds up to the need for a red light laser. The fact that
a variety of wavelengths are often required due to different drugs
being activated at different red peaks means that a tuneable laser
is far more advantageous for research purposes than a fixed
wavelength laser. Thus although the ruby and gold vapour lasers
produce red light of the correct physical characteristics for some
sensitisers, most PDT work is done with tuneable dye lasers,
giving the necessary degree of flexibility. A tuneable dye laser
relies on a higher energy pump laser driving a red light laser,
such as the Rhodamine dye laser.
The red light laser can be tuned to vary the wavelength of light
produced over most of the red spectrum, by means of a variable
light graticule. The pumping laser needs to produce photons of
higher relative energy than the eventual red light (one never gets
energy for nothing). This means that it has to be of a lower
93
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
wavelength. Thus green light lasers such as the Copper Vapour,
Argon Ion or KTP are used to pump most dye lasers.
The copper vapour or Argon Ion pumped dye lasers have therefore
been the mainstay of light production for PDT research. These are
bulky lasers, with high purchase and running costs. A full time
laser physicist is usually employed to run the lasers and perform
the necessary dosimetry prior to treatment. Because the tube
inside the copper vapour laser needs to heat up to 1500 degrees
Celsius to vaporise the copper prior to lasing, warm up times for
this laser are anything between 1 and 2 hours.
The Laserscope KTP pumped dye laser system is a major advance on
these earlier systems. As previously described it is a frequency
doubled Nd-YAG laser (KTP), which then pumps a Rhodamine Dye
laser. It is therefore a solid state system, with a setting up
time of perhaps 10 minutes. The control panel and light dosimetry
is computerised and with a little training, the operating
clinician can use it without technical support. Purchase costs
remain high however, although running costs are reduced over the
Copper Vapour/ Argon Ion lasers.
Recently, diode lasers of specific PDT wavelengths have been
produced by several different laser manufacturers worldwide. Only
a few have been used clinically, although it seems likely that by
the time this article is published, PDT Diode lasers will be
involved in full scale clinical treatments. The great advantage of
diode lasers for PDT is that they are so small (size of a small
suitcase) that they can be easily transported from centre to94
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
centre, enabling several different hospitals to use the same
system. They are also relatively cheap to purchase, and have
negligible running costs. The problem with them is that they are
of a fixed wavelength, so they will need to be replaced when
different sensitisers are used, and that in order to attain the
correct wavelength, the diodes have to be cooled – which can cause
problems in warm operating theatres / treatment areas.
The emergence of skin and oral cavity cancer as a target for PDT
has led to the re-consideration of non-laser light sources. This
is because fibre delivery is not necessary for treating these
areas. Development of narrow band filtered arc lap sources and
Light Emitting Diode arrays at a variety of wavelengths for the
treatment of malignancy in these areas has been possible (Dilkes
and DeJode 1995). Although the light produced is not
monochromatic, it is possible to almost exactly mimic the
absorption spectra of drugs like mTHPC and d-ALA in the red
spectrum. This is particularly true with the LED array, meaning
that although not all the light will maximally stimulate the drug,
the next best thing will happen – little of the light is wasted,
leading one assumes to a similar clinical effect although total
light dose may need to be increased (see figure superimposition of
LED output over red mTHPC peak). Early studies have borne this out
(DeJode and Dilkes 1995). The great advantages of these light
sources is that they are not only easily portable (with
development they might become powered by rechargeable batteries in
a torch-like package) but the costs are dramatically reduced. The
dosimetry and delivery of light with these sources should also be
95

THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
easy for a clinician to learn, again without the need for
technical support.
96
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
4f: Potentiation of the Photodynamic effect
As with any form of clinical treatment, efforts have been made
to increase the effect of PDT by either combining it with other
treatments or increasing the beneficial effects of its
environment. This has taken its shape in several different
forms:
Since PDT exerts its effect by the photoproduction of singlet
oxygen (Weishaupt et al 1976) and the production of this
substance depends on the concentration of oxygen in the tissue
treated (Moan J., and Sommer S., 1985) and the fact that PDT may
also cause a reduction in tissue oxygen concentration because of
its effect on the microcirculation, reducing vascularity,
particularly in tumours (Henderson B.W. 1990), it is possible
that by pulsing or chopping the delivered light and therefore
allowing tumour re-oxygenation between episodes of light
delivery, the effect of PDT may be enhanced (Foster et al 1991).
This principle may be taken one stage further by treating the
patient in a hyperbaric oxygen atmosphere (Jirsa et al 1991).
This is similar to ionising radiation with one major difference
- whereas the effect of ionising radiation is reduced when
oxygen is absent, there is no photodynamic effect at all in this
situation (Henderson and Dougherty 1992). Potentiation of the
photodynamic effect has also been tried with laser and other non
laser thermal devices, with limited success (Waldow et al 1987).
Photodynamic therapy has also been used in combination with
chemotherapy, a study by Nahabedian et al in 1988 combined
Cisplatin and Doxorubicin with PDT in a mouse tumour model, to97
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
reasonably good effect, particularly with Doxorubicin - a
finding that has been described elsewhere (Cowled et al 1987).
The role of PDT in combination with bioreductive drugs has also
been investigated - this was thought to be useful since these
compounds are essentially inactive unless present in conditions
of reduced oxygen supply. With PDT, the effect on the
microvasculature as described leads to hypoxia within the
treatment site (Reed et al 1989), with subsequent activation of
the bioreductive agent (Bremner et al 1994).
98
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Other drugs such as metoclopramide have also been shown to
potentiate the photodynamic effect in preclinical studies,
although no confirmation of this effect has been shown
clinically (Werning J.W. et al 1995). Linking photodynamic drugs
with carriers such as liposomes has been a way of both
increasing the stability and solubility of compounds in
physiological solution and also increasing their affinity for
tumours (Davis R.K. et al 1990), although despite considerable
investment being made in this area, there remains no firm
clinical evidence that this will prove to be advantageous.
The “magic bullet” scenario has been postulated by Donald et al
in 1991, linking photodynamic drugs with monoclonal antibodies,
sadly again no clinical work has yet been undertaken to confirm
or deny this postulate, although cell work has shown some very
impressive efficacy (Mew et al 1985).
99
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
4g: Role of fluorescence in PDT
Fluorescence was the first avenue down which PDT was explored in
the clinical field (Lipson and Baldes 1961). Its potential in
malignant disease was later confirmed by Gregorie et al in 1968.
The principal of this phenomenon is that certain compounds, such
as photosensitising agents, when stimulated by light of the
correct wavelength, will then re-emit light at a longer
wavelength, allowing this light to be detected independently of
the stimulating light. The property that most photosensitising
drugs seem to have, selectivity for malignant/altered tissue,
then allows that tissue to stand out from surrounding normal
tissue by means of its greater emittance of fluoresced light.
Therefore fluorescent imaging can be used to differentiate
malignant/premalignant tissue from normal tissue (Leonard and
Beck 1970). When applied to the skin, this is fairly easy, since
this area is easily accessible and background light is easy to
eliminate. However, when trying to perform fluorescent diagnosis
within the upper aerodigestive tract, a number of problems
occur:
- Stimulation and emission need to occur down a light carrying
fibre, rather than directly, since an endoscope needs to be
passed to access the area to be measured. This then means that
very low levels of light are obtained on emission, and often a
laser has to be used to stimulate the area. High technology is
needed to gather and amplify the emitted signal.
- Direct visualisation of the suspicious area is required, since
the area cannot be marked and treated later. This requires100
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
complex and expensive charge-coupled device (CCD) cameras to be
linked up to the fluorescence emittance pathway. This will allow
the suspicious areas to be visualised on a screen by the
surgeon, before immediate PDT is carried out (Mang et al 1993,
Monnier Ph. et al 1995).
If these expensive and time consuming problems are overcome,
fluorescence imaging can play an important role in both
diagnosis and monitoring of treatment (Braichotte et al 1996),
but currently due to the expense these facilities are available
in only a few centres worldwide. The drugs currently being
investigated for fluorescence diagnosis include d-ALA (Campbell
et al 1996), Photofrin 2 (Braichotte et al 1995) and mTHPC
(Braichotte et al 1995).
Our own efforts in this area have been related to using
fluorescence to determine the optimum drug-light interval for
best tumour response, unfortunately the tumour peak with
fluorescence may occur after peak photosensitiser concentration
in the tumour, when compared with the drug assayed tumour peak.
There is a variable gap between the two, giving us little added
information of use (Ansell J et al 1995, Grahn et al 1996).
PDT-induced fluorescence can also be used when studying the
cellular or tissue distribution of sensitising drug, which may
give vital information regarding the site of the PDT effect, in
particular whether there is any penetration of drug into the
nucleus, in which case the potential for mutagenesis arises.
Work so far suggests that this is not the case, although the
actual definite site of action remains unknown, it seems likely
to be cytoplasmic (Barr et al 1988).101
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
5: Chemistry of Photodynamic therapy
5a: Drugs for Photodynamic Therapy
In order to be useful as a photosensitiser for PDT, a drug must
have at least some and preferably all of the following
characteristics, as described by Moan (1990):
a) Selective uptake of sensitiser by tumour tissue.
b) Efficient photoactivation.
c) A maximum absorption peak well into the red spectrum of
light, allowing maximal tissue penetration.
d) Non-toxic in the dark.
e) Minimal/no skin sensitisation.
f) Have a constant composition and preferably be a pure single
substance.
Since the first description of the photodynamic effect by Raab
(1900), drugs used in PDT have evolved from impure compounds
with many disadvantages, to the stage whereby clinical PDT can
be performed scientifically and with a low risk of complications
(Gomer C.J. 1991). The majority of drugs developed have been
derived from the earlier, crude mixtures, all based on the basic
porphyrin ring structure (Bonnet et al 1989(2)).
Photosensitising drugs tend to be administered parenterally,
preferably intravenously for reliability of distribution (Perry
et al 1991). Much work continues on basic photochemistry to
achieve these goals (Lin C.W. 1991(2)). Virtually no resistance
to the Photodynamic effect has been seen clinically, although
preclinical work by Singh et al in 1991 did show some
resistance, particularly with multi-drug resistant cells.102
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
5b: Examples of first generation drugs
Haematoporphyrin
This compound is an impure derivative of haemoglobin, it was
first used clinically for PDT in the early part of the 20th
century. It was discovered in the 1940's to be preferentially
retained in malignant tissues, a major step for photodynamic
therapy (Auler and Banzer 1942, Figge et al 1948). It was well
recognised however that Haematoporphyrin was a crude, variable
mixture of numerous porphyrins (Schwartz et al 1955), and the
drug was quickly dropped in favour of more purified compounds as
they became available.
Haematoporphyrin Derivative (HpD), or Photofrin 1
This compound has been used extensively as a sensitiser in
clinical practice, with some promising results. Many early
principles of PDT have been established with this drug, although
its use has now been superseded by drugs derived from it. The
compound itself is a mixture of porphyrins with a peak of
activation in the red spectrum at 628 nm. It is prepared by the
alkaline hydrolysis of haematoporphyrin acetate(Lipson et al
1960). It was the first photosensitising drug to be used with
malignancy (Lipson et al 1961), although in this situation only
for photodetection. A further study in 1972 confirmed the
selectivity of HpD and restated its role in fluorescent
diagnosis (Sanderson et al 1972). Its cytotoxic potential was
initially described by Figge and Weiland in 1949, preclinical103
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
studies demonstrating its efficacy on tumour models were
convincing (Dougherty et al 1974), although it was not until
1976 (Kelly and Snell) that it was first shown to be effective
for potential cure against primary, early human cancer. Several
thousand patients, with malignancies from different parts of the
body have since been treated with the drug with generally
encouraging results. In particular, several of these studies
have looked at squamous cell carcinoma in the Head and Neck area
(Wenig at al 1990, Patrice et al 1990, Monnier et al 1990, Edell
and Cortese 1992, Ono et al 1992, Weiman and Fingar 1992). There
have been problems with the compound however, preventing its
widespread use. In particular, it remains a complex, variable
mixture of porphyrins that are derived from bovine blood and it
is largely uncharacterised (Dougherty et al 1984). It may have
a variable degree of activity depending on its batch and source.
Its peak absorption in the red spectrum being at 628 nm, gives
it only around 5mm depth of penetration in living tissue. It
also has a variable half life of around 19 days, leading to
prolonged skin sensitivity to light (Brown et al 1992).
104
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Photofrin 2
This is a compound derived from HPD (see above), and is the
first photosensitising drug to be licensed for clinical use,
this occurring in Canada in 1993, for in-situ bladder carcinoma.
Despite this, much preclinical work continues, attempting to
further determine the optimum parameters for treatment, still
unclear (Mukhtar et al 1991). Photofrin 2 is extracted from HpD
by gel exclusion chromatography, and is a purified fraction of
the photosensitising elements of HpD. It is also known as DHE
(Dihaemotoporphyrin Ether), or Polyporphyrin. It has been
characterised as an aggregated mixture of haematoporphyrin
molecules, linked together by ether and/or ester bonds. It has
been shown to selectively concentrate in malignant tissue, and
is maximally activated in the red spectrum by light at 630 nm.
There has been a considerable amount of work published regarding
the use of this drug in the treatment of Head and Neck cancer,
with generally encouraging results - see table 9. The dose of
light delivered is variable, most tumour work being carried out
at between 50 and 100 Joules/cm2 (Dougherty and Marcus 1992).
Being a slightly purified version of HpD, this compound suffers
with the same problems of impurity etc. (Byrne C.J. 1990) and
high unit drug dose linked with a long half life again lead to
problems with skin phototoxicity with over exposure from ambient
light (Dougherty 1990).
105
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
5c: Second generation Photosensitising Drugs
The limitations of HpD and Photofrin (Dougherty T.J. 1989) led
to the search for photosensitising drugs closer to the desired
qualities mentioned above for the ideal photosensitiser, and led
to the development of a new 2nd generation of synthetically
created drugs, based upon the original porphyrin ring and active
components of HpD, but markedly altered so that in some cases
there is little to recognise from the original (Berenbaum et al
1982, Berenbaum M.C. 1989).Such is the interest in these second
generation compounds that scientists have discovered potentially
non-photodynamic properties of compounds such as tin -
etiopurpurin and benzoporphyrin derivative, in which the drug
inhibits neointimal hyperplasia after balloon angioplasty
without light activation (Coates et al 1996).
Examples of second generation photosensitising drugs:
Chlorins
These compounds, (of which meta-TetraHydroxyPhenylChlorin
(mTHPC) is currently being clinically evaluated, Stewart J.C.M.
1994) were developed in order to increase the wavelength at
which a reasonable peak of sensitisation occurs. It was
synthesised from porphyrin by modifying the substitution pattern
of a basic form of the porphyrin molecule (Berenbaum et al
1986). Reduction of porphyrins with diimide gives the
corresponding Chlorin, hence reduction of
tetra(hydroxyphenyl)porphyrin, which had been shown in bioassay106
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
to have good tumour photosensitising properties, gives
tetra(hydroxyphenyl)chlorin (Bonnet et al 1989(1)). The meta-
and para- isomers showed good selectivity for tumours above
muscle and skin. When this large array of compounds was tested
for activity on a tumour model, one of the compounds with the
best all-round characteristics produced was meta-
TetraHydroxyPhenylChlorin, or m-THPC. This is a chemically and
isomerically pure compound at least 100 times more active mole
for mole than HpD, as assessed using tumour necrosis models
(Chevretton 1993). The drug appears to be far more tumour
selective than HpD, allowing equal clinical effect with reduced
normal tissue reaction (Ris H.B et al 1993(2)). Its activation
deeper into the red spectrum allows more depth of clinical
effect than Photofrin 2, with tumour necrosis up to 1cm deep
being seen in animal and human tumours (Ris H.B et al 1993 (1)).
The light dose given tends to be in the range 2.5-20 joules/cm2,
at 100-300mW/cm2 density (Dilkes et al 1996), leading to
treatment times of under 3 minutes for relatively small tumours,
and, depending on the light source used, also for adjunctive
work. This if in the order of 10 times less than with
Photofrin2. The accumulated evidence so far suggests that this
drug has the most potential for the treatment of Head and Neck
cancer, although the very fact that it is so powerful can lead
to dangerous skin toxicity and other side effects, such as
fistula formation (Bradley P.F. personal communication, Dilkes
et al 1996, Savary et al 1997)
107
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Phthalocyanines
These compounds are synthetic porphyrins, with high absorption
peaks in the red spectrum at around 680 nm wavelength (Ben Hur
and Rosenthal 1985, Chan et al 1986). They are chelated for
clinical use with a variety of metals, usually zinc or aluminium
(Selman et al 1986). They are thought to have less side effects
when compared to other photosensitizers, and also have a
powerful photodynamic effect with good tumour localisation
(Tralau et al 1987, Barr et al 1990). The activation deep into
the red spectrum made these drugs good candidates for PDT, by
increasing the potential depth of effect (Tralau 1987). There
have been problems however with stability of the drugs in
solution, with quantification of effect being difficult, and in
the fact that they dissolve poorly. Recently, combination with
liposomes has increased their solubility. Problems remain
however, particularly since high light doses (300 j/cm2) are
needed for effective treatment, leading to prolonged laser-on
time (Chan et al 1991).
Benzoporphyrin Derivative (BPD)
This compound is prepared from Protoporphyrin 9, an endogenously
produced photosensitising agent (see later under ALA). It has
similar properties to the Chlorin family of drugs, also
containing a reduced tetrapyrrhole ring. Its absorption peak is
at 692 nm, and it is very rapidly cleared from the body, leading
to reduced problems with skin photosensitivity (Wolford et al
1995). Little further is currently known about the drug, which108
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
is in preclinical (Jamieson et al 1993) and early clinical
evaluation in the USA (Nelson et al 1988), although currently
work seems to be concentrating on a role in the treatment of
ocular malignancy and other retinal diseases (Kim et al 1996).
109
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
ALA
delta - Aminolaevulinic acid (ALA) is a different form of
compound to the more classical photosensitizers. It acts by
being rapidly metabolised into an active photosensitising agent,
Protoporphyrin 9 (PP9) which is then slowly metabolised into
Haem (a rate limiting step) (Kennedy and Pottier 1992). It can
be delivered either systemically (orally) or topically, since
the ALA itself is a small, uncharged lipophilic molecule that
passes through cell membranes with relative ease, down a
concentration gradient. Active photosensitisation if given
systemically only occurs during a fairly short period of time
when PP9 levels are high and this dramatically reduces problems
with skin sensitisation since over a matter of a few hours the
PP9 is metabolised into Haem.. However due to its relative
inefficiency both in terms of depth of penetration and
efficiency compared to other drugs such as mTHPC it can only be
used to treat very superficial lesions such as early basal cell
carcinomas or premalignant conditions (Warloe et al 1992, Grant
et al 1993). The amount of light needed for a good clinical
effect appears to be circa 150 J/cm2, which increases the
treatment time compared to mTHPC, the fact that it is effective
topically is enough to make this a very exciting compound for
full scale clinical use, particularly on the skin (Svanberg K.
et al 1994).
110
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
5d: Problems
The major problem holding back PDT from more widespread use is
the fact that in almost all cases it involves the systemic
(usually intravenous to ensure good drug delivery) administration
of a photosensitising compound. Since the drugs are only ever
partially tumour specific (Dougherty et al 1990., Wooten et al
1988, Zalar et al 1977, Tralau et al 1986), drug will therefore
accumulate in normal tissue before being metabolised and removed
over a variable period of time. This causes two problems:
1) Photosensitizer in the skin and eye tissue will be activated by
light, including sunlight. Patients therefore need a prolonged
period (up to 2 months with the older sensitizers) of bright light
avoidance, necessitating the wearing of a hat, gloves and sun
glasses on top of normal wear when venturing outside, and making
sure that windows at home are shielded from direct sunlight (eg
with curtains) and that there are no light bulbs of greater than
60 watts output. Even at these light levels, patients are advised
that if they feel their skin tingling at light exposed areas, they
should reduce the ambient light levels. This is of particular
importance when considering that PDT was initially used for
palliation of advanced cancer in most cases, where being kept
indoors for the last few weeks of life was a major burden, and not
acceptable long term. The mechanism of skin phototoxicity is the
same as tumour destruction, namely the release of singlet oxygen
upon photoactivation of the drug (McLear and Hayden 1989). Manyak111
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
et al have also identified a role for a type 1 hypersensitivity
response, with mast cell degranulation and histamine release being
seen. Much work has been done trying to limit the photosensitive
effect on the skin whilst preserving it in the tumour, by the use
of singlet oxygen quenchers such as beta-carotenes (Mathews-Roth
1982) or N-acetylcysteine (Holdiness 1991), without much benefit.
To minimise the unwanted effects of skin photosensitivity, newer
drugs are being designed to have improved selectivity and a
shorter half life over the earlier compounds.
112
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
2) Photosensitizer in normal tissue around areas to be treated
will be activated by scattered light used for treatment. This will
cause local damage and pain over a period of around two weeks as
healing progresses. This can be minimised in areas where such
collateral damage may cause unwanted side effects, such as the
larynx or skin, by using adherent black gel that is liquid at room
temperature but adherent and gel-like at body temperature. This
means it can be painted onto the area to be masked, where it will
rapidly reach body temperature, and stick there until wiped away.
Other problems such as depth of penetration etc. are surmountable
by choosing cases to be treated correctly such that the depth of
the tumour to be treated is within the effective range of the
drug-light combination. No photosensitising drug has been reported
as being clinically toxic without photoactivation at normal
therapeutic doses. The second generation photosensitising drugs
have overcome most of the criticisms of earlier agents, in
particular they are now virtually 100% pure compounds that are
easily quantifiable, whereas before the haematoporphyrin
derivatives were an essentially unquantified mixture of active and
inactive compounds.
113
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
6: Adjunctive Intraoperative Photodynamic Therapy (AIOPDT)
6a: Preclinical
Since it has become quite clear that PDT is effective in
necrosing squamous cell carcinoma of the Head and Neck, the next
obvious role is in potentially mopping up the tumour residue at
radical resection that causes local recurrence, which is, as
previously described, a major cause of morbidity and mortality
following major Head and Neck cancer surgery. Several
preclinical studies have shown that adjunctive intraoperative
PDT (AIOPDT) significantly reduces the local recurrence of
tumour following macroscopically clear tumour removal (Davis et
al 1990, Abulafi et al 1995, van Hillsberg et al 1995). It is
postulated in these papers that AIOPDT destroys microscopic
tumour residue without causing significant damage to structures
in the operative bed, due to tumour selectivity of the drug, and
the rapid healing of damaged normal tissue, with the potential
for full retention of function. Thus following radical
(attempted curative) resection of cancer, prior to closing the
wound, treatment with PDT can be given to the operative bed to
reduce the chance of local recurrence of disease. PDT is known
to exert at least some, if not all its effect at the cellular
level (Gomer et al 1988), which is needed when considering
AIOPDT, since any effect relies on microscopic tumour
destruction, possibly that tumour which may be inadvertently
spilt at surgery, which is unlikely to have its own tumour
microvasculature as a PDT target (Henderson B.W. 1990). 114
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
6b: Clinical
Clinical studies are in progress looking at the efficacy of
AIOPDT in other parts of the body without the Head and Neck,
such as the colorectal (Allardice et al 1994, Abulafi et al
1993, Herrera-Ornelas et al 1986), neurosurgical (Muller and
Wilson 1995), thoracic (Ris et al 1991) and retroperitoneal
(Nambisan et al 1988) areas . No definitive data is currently
available, although recently published clinical studies in the
Head and Neck area suggest that this form of treatment has
definite potential (Dilkes et al 1995, Biel 1996).
In the face of evidence suggesting that the treatment is
potentially effective, the main question that needs to be
answered is the one regarding safety to other structures,
particularly vital ones, in the potential treatment bed.
115
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
EXPERIMENTAL RATIONALE
To explore the premise:-
Adjunctive Intraoperative Photodynamic Therapy using a 2nd
generation photosensitising drug is safe and effective for use
in Head and Neck Cancer
116
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
7: Experimental Rationale
7a: Description
When setting out to investigate the premise that adjunctive
intraoperative photodynamic therapy (AIOPDT) using the second
generation drug mTHPC was safe and effective, there were several
questions that needed answering. The decision was made to use
the new, virtually uncharacterised second generation Chlorin
photosensitiser meta-TetraHydroxyPhenylChlorin (mTHPC), because
having looked at all the drugs available, it was the one that
was closest to Moan’s ideal photosensitiser, being a pure
substance, readily soluble and stable in physiological solution,
with a high co-efficient of extinction deep into the red
spectrum (Berenbaum et al 1986). Given what was known about the
most widely explored photosensitising drug, Photofrin 2, it
seemed likely that this new drug would be more useful
clinically, with lower unit drug doses expected - reducing the
period of skin sensitivity to bright light, lowering light doses
needed for tumour necrosis (both of these due to the greater
efficiency (order of 200x) of mTHPC compared to Photofrin)
leading to shorter treatment times, deeper effective necrosis of
tumours since its activation peak in the red is significantly
further towards the infra-red, and the value of knowing exactly
what the active ingredient is, its purity and stability.
Not only were the basic tumour:normal tissue pharmacodyamics of
the drug not known, but the efficacy in the adjunctive
intraoperative situation of PDT also needed to be determined, 117
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
with respect to head and neck cancer since this had not been
tested before in any of the 3 previous AIOPDT preclinical
studies.
118
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
3 Stages to the experimental series were envisaged:
7b: First Stage - efficacy
Clearly there is no point in have a safe procedure that is
ineffective, so the first question to be answered was: does it
work, and at which PDT parameters?
Since the model clinical operation for this treatment is the
radical neck dissection for metastatic squamous cell carcinoma
of the Head and Neck (HNSCC), an animal tumour model was needed
that mimicked this tumour, and the pharmacodynamics of the new
photosensitiser evaluated on this model, compared to a first
generation photosensitiser to demonstrate the advantages of the
new drug (Experiment 1). The efficacy of AIOPDT would then be
tested in this model with the treatment optimised using data
from Experiment 1 (Experiment 2).
At this point, if the treatment was found to be ineffective, the
experimental series would be abandoned. If a statistically
significant positive result was achieved, the next stage of
experimentation would be performed.
7c: Second Stage - Safety Studies
The response to mTHPC PDT of those structures in the operative
bed deemed to be vital to the survival of the patient needed to
be determined . For the purposes of this experiment, this meant
the carotid arterial system, with delayed (histological
assessment, Experiment 3) and acute phase (doppler flow,
Experiment 4) studies. Further to this, the survival of 119
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
revascularised free flaps needed to be determined, since they
are a vascularly dependant structure often used during major
head and neck surgery, when a radical neck dissection might also
be performed (Experiment 5). Finally, a short study was
performed to confirm the results of the safety data in
experiment 3, on human sized vessels, namely the pig (Experiment
6), should the earlier study show a positive (no significant
damage) result.
7d: Third Stage - Clinical Study
Following the accumulation of satisfactory data (safe, effective
treatment) preliminary clinical studies were planned on patients
undergoing a radical neck dissection, initially in those thought
to have a high risk of local recur (Experiment 7).
120
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
7e: 6 consecutive preclinical experiments were therefore
performed:
Experiment 1: Determination of the correct PDT parameters for
mTHPC, in particular the drug-light interval. Comparison of
relative drug levels with Photofrin 2.
Title: Preclinical pharmacokinetic studies of first and second generation
photosensitising drugs
Experiment 2: Assessment of the efficacy of mTHPC PDT as an
adjunctive intraoperative therapy.
Title: The efficacy of Adjunctive Intraoperative Photodynamic Therapy with mTHPC in a
rat fibrosarcoma model
Experiment 3: Histological analysis of damage to arteries after
clinically appropriate PDT had been administered as in the
proposed clinical situation.
Title: Preclinical Photodynamic Safety Studies on Arteries
Experiment 4: Doppler flow studies of arteries and veins during
clinically appropriate PDT, as in the proposed clinical
situation.
Title: Acute phase effects of PDT on arteries and veins
Experiment 5: Analysis of survival of microvascular anastomises
in sensitised animals.
121
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Title: The effect of high intensity white and filtered microscope light on the viability
of microvascular anastomoses in photosensitised rats
Experiment 6: Confirmatory study on human sized arteries prior
to clinical study
Title: Histological study of large diameter arteries undergoing photodynamic
therapy
On finding positive results a 7th clinical experiment was performed
Experiment 7: Human studies.
Title: Adjunctive Intraoperative Photodynamic Therapy for Head and Neck Cancer
122
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
8: Drugs, animals, Laser, Other equipment
8a: Photosensitising Drugs: Photofrin 2 was obtained from
Lederle Pharmaceuticals, Gosport, Hants, U.K., as a gift and
stored as sterile dry powder in a fridge, protected from light.
The diluent used was 5% dextrose, to create solution of 5 mg/ml,
which was prepared fresh (within one hour of injection) in all
cases.
mTHPC (Temoporphyrin, Foscan) was obtained from Scotia
Pharmaceuticals, Guildford, U.K., as a gift. It was stored as a
sterile dry powder in a fridge, protected from light.
Solution for injection was made up within 1 hour of delivery, by
weighing the powder on a 7-place balance and reconstituting it
with its solvent (1g ethanol and 1g polyethylene glycol 400 made
up to 5 ml with sterile water for injection for mTHPC, 5%
dextrose for Photofrin 2) to achieve a final concentration of
0.5 mg/ml for mTHPC and 5 mg/ml for Photofrin 2. With both
compounds, meticulous attention was taken to ensure that the
drug had gone into solution. Invariably this meant 2 or 3
minutes of vigorous shaking, ensuring no residue was visible on
the bottom of the tube used for reconstitution. Care was taken
with both drugs to avoid exposure of the photosensitiser to
light during preparation and injection (see picture) to avoid
photobleaching active drug.
123
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
8b: Anaesthetic Drugs
Rat: Hypnorm (Janssen) - Fentanyl 0.315mg, Fluanisone 10mg, per
ml
Hypnovel (Roche) - Midazolam 5mg/ml
Sagatal (Rhone Merieux) - 60mg/ml pentobarbitone sodium
Atrocare (Animalcare Ltd) - Atropine Sulphate 0.6mg/kg
Pig: Halothane, Nitrous Oxide, Oxygen on an open circuit
(inhalational)
Euthesate (Willows Francis) - 20% Phenobarbitone
Drug Doses
Sedation rats - Hypnorm 0.2ml/kg i/p
General anaesthetic rats - premedicate Atropine sulphate
0.05mg/kg, then Hypnorm/Hypnovel mixture 1:1, 5mg/ml plus same
volume of water for injection, 2.7 ml/kg i/p. To extend the
period of anaesthesia additional doses of Hypnorm are given
(0.1ml/kg every 30 to 40 minutes).
Lethal injection rats - Sagatal 40mg/kg of freshly prepared 10%
solution of Sagatal and
n-saline i/p.
General anaesthetic pigs - Inhalational anaesthetic as above
Sedation pigs - Inhalational anaesthetic as above
124
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Lethal injection pigs - Inhalational anaesthetic as above
followed by Euthesate i/v 3.5ml/kg
8c: Tumour: The tumour model HSN fibrosarcoma was chosen because
it displays similar characteristics to Head and Neck Squamous
Cell Carcinoma (HNSCC), the eventual main clinical target. In
particular it is locally invasive see picture 1, non-
encapsulating, non-metastasising, hardy strain of tumour that
has been used before in PDT (Tralau C.J.,et al 1987). It is
available from the Chester-Beatty laboratories at The Royal
Marsden Hospital, Sutton, Surrey.
125

THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Picture 1: Tumour can be seen invading into surrounding muscle,
NOT encapsulating.
126
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
8d: Animals:
Chester-Beatty HSN adult rats of both sexes were obtained from
the National Institute for Medical Research, South Mimms,
Hertfordshire, U.K. These are a relatively cheap and hardy
strain of hooded rat, which bear the HSN Fibrosarcoma. The rats
were grown in free single sex cages with open access to food and
water, 5 animals per cage..
For other experiments not involving tumour, adult Wistar rats
were obtained from Charles River Ltd, and kept in free single
sex cages, 5 animals per cage with open access to food and
water.
Suckling pigs for the 6th experiment were obtained from Charles
River and kept in standard pens, food and drink given as per
home office regulations.
In all cases where photosensitising drug had been administered the animals were
kept in conditions of subdued lighting to prevent possible skin or retinal
phototoxicity.
8e: Laser:
Preclinical work - in all cases a copper vapour pumped (model Cu
15) tuneable Rhodamine dye laser was used. This was obtained
from and serviced by Oxford Lasers, Abingdon Rd., Oxford, U.K.
This produced adequate power for the preclinical work, when the
127
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
maximum light delivery rate necessitated less than 1.5 watts
from the fibre tip in all cases.
In the clinical work, a more powerful Cu20 pumped Rhodamine dye
laser was used (same supplier and maintenance), since demands
for power in adjunctive cases are higher. Some cases used the
KTP pumped Rhodamine dye laser (Laserscope, Raglan House,
Cwmbran, Wales, U.K.), which is the most powerful system
available for purchase, producing up to 7 watts of red light
from the fibre tip.
128
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
9: Experiment 1 - Preclinical pharmacokinetic studies of first
and second generation photosensitising drugs
The aim of this experiment was to compare the tissue
accumulation qualities of two photosensitising drugs in an
animal tumour model, to determine the optimum drug - light
interval for selectivity and efficacy with a view to future
preclinical and clinical studies. The pharmacological results
would then be corroborated by assessing depth of PDT induced
necrosis in the same tumour model.
9a: Introduction
There is evidence that malignant tumours preferentially retain
or take up photosensitising drugs when compared to normal
tissue. This was initially described by Policard in 1936, and
has been confirmed subsequently in virtually every study of
photosensitising drugs (Gomer 1991). For reasons outlined above,
it was decided to use the relatively unknown photosensitising
drug meta-(tetrahydroxyphenyl)chlorin (mTHPC) in this study
looking at the potential role of PDT in an adjunctive setting
for treatment after radical neck dissection and potentially
other major Head and Neck cancer procedures. The new second
generation photosensitising drugs are claimed to have this
property of selectivity enhanced over 1st generation compounds.
This experiment was therefore designed to compare the basic
pharmacokinetic properties of these typical first and second 129
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
generation photosensitising drugs using a suitable animal
tumour model (rat fibrosarcoma), skin, muscle and aorta as the
sampled sites.
130
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Meta-TetraHydroxyPhenylChlorin (mTHPC) is a good example of the
Chlorin group of second generation photosensitising drugs. which
are known to offer particular advantages over the most widely
used drug for PDT, Photofrin 2, which is a poorly characterised
mixture of esters and ethers of unknown relative molecular
weight and purity. The initial evaluatory work with mTHPC has
shown it to be particularly promising when compared with
Photofrin 2, both in terms of a high quantum yield of free
radicals, leading to lower drug and light doses, and also a high
absorption peak deep into the red spectrum at 652 nm (Berenbaum
et al 1986), giving more efficient tissue penetration than
Photofrin 2 at 630 nm. Preliminary studies had also shown that
tumour selectivity should be increased with this compound
( Bonnet et al 1989). This drug has been designed to fit in as
near as possible with the characteristics of an ideal
photosensitizer (Moan 1990) and although it is not ideal in
these respects, it does represent a considerable improvement on
the originally used clinical photosensitisers HpD and Photofrin
2.
9b: Tumour
Previous work had also shown the HSN Fibrosarcoma tumour to be
useful for measuring the clinical photodynamic effect, in terms
of depth of PDT - induced tumour necrosis (Tralau et al 1987).
Tumour was initially grown in cell culture, using cell culture
flasks containing 10% Foetal Calf serum in Dulbecco’s modified 131
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
egg medium, enhanced with 10% glutamine, Streptomycin,
Penicillin and Amphotericin B. Once confluence had been reached
as assessed on daily microscopy, the cells were split with
Trypsin, and divided into 10 new flasks prepared as before. Once
these had reached confluence, some cells were frozen in
dimethylsulphoxide and stored in liquid nitrogen, others were
injected into the flank areas of the HSN rats, approximately 2
x107 cells/ml of solution per injected area as measured using a
graticule, under Hypnorm sedation. 1 ml of solution was injected
into each area. Once a solid tumour had grown, live tumour was
maintained by passaging 1mm3 of viable (peripheral) tumour into a
fresh animal. This was then used as the method of tumour
preparation.
132
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
9c: Drug dose and analysis
In the clinical situation the dose of Photofrin used has
generally ranged from 1 to 5 mg/kg body weight. The dose used
in this experiment for adult rats was 20 mg/kg. The greater dose
in the rat as compared to the human is an extrapolation of the
smaller animal’s increased surface area to volume ratio which
equates to a higher metabolic rate and therefore increased
metabolism / excretion of drugs (Paxton J.W. 1995).
The dose of mTHPC, 1.0 mg/kg body weight was calculated on the
basis of some preliminary toxicology work, the levels used by
another investigator (Ris et al 1993) , and the initially
proposed and used human dose of 0.3 mg/kg body weight (Ris et al
1991), again extrapolated to take into account the higher
relative metabolic rate of small animals when compared to large
ones. Once tumour had reached approximately 1cm largest
diameter (after 7 to 10 days), the animal was weighed and an
intravenous injection of either mTHPC or Photofrin 2 was given,
at a dose of 1mg/kg and 20 mg/kg respectively. Based upon the
concentration of stock solution as described above, the volume
injected was between 0.7 and 1.0 ml, as measured using an
insulin syringe with 0.1 ml gradations. This could be performed
without the need for anaesthesia, the animal being held in a
restraining device, injecting into the tail vein (see picture
2). After injection, the animals were kept in conditions of
reduced lighting, no direct contact with light was allowed. 4
rats were sacrificed at each time interval, these were from 6
133
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
hours to 14 days in both the mTHPC and Photofrin groups. One
piece of viable tumour of approximately 0.5 cm3 was taken from
each animal and stored fresh at -80 degrees centigrade in a
separate container. At the same time, approximately 1cm3 samples
of shaved abdominal skin, gluteal muscle and thoracoabdominal
aorta (flushed with normal saline) were taken and stored in a
similar fashion (separately). Following the collection of all
the samples, they were sent for analysis.
134
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
9c(i): mTHPC analysis - performed by Dr C.K. Lim and associates
at the MRC Toxicology Unit, Carshalton, Surrey
Each specimen was thawed on reception and divided into 4
separate pieces, which were analysed separately. The final
figure for each piece of tissue is an average of the 4 levels.
The extraction of mTHPC was performed by High Performance Liquid
Chromatography (HPLC). A Hypersil (5 micron) column was used
with acetonitrile- 0.1% TFA as the mobile phase. The flow rate
was 1 ml/minute. A range of calibration curves was obtained with
standard concentrations of mTHPC before each set of assays. The
tissue to be assayed was homogenized in a medium containing 8
parts of methanol-Dimethylsulphoxide (4:1 v/v) containing para-
TetraHydroxyPhenylChlorin and 1 part water. 200-300mg of the
tissue was homogenized in 2ml of this medium in a Dounce
homogenizer. This was then centrifuged at 2,600g for 10 minutes.
400 microlitres of the supernatant was mixed with 200
microlitres of water and 200 microlitres of this solution was
injected into the HPLC column for measurement of relative
fluorescence (Wang et al 1993).
135
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
9c(ii): Photofrin 2 analysis - performed by Professor
S.B.Brown’s team at the Biochemistry Department of Leeds
University
Each specimen was thawed on reception and divided into 4
separate pieces, which were analysed separately. The final
figure for each piece of tissue is an average of the 4 levels.
The analysis of Photofrin 2 was performed by spectrophotometry.
Tumour and muscle were homogenised in HEPES/CTAB at pH 7.4,
using a Polytron homogeniser. Skin was digested overnight at 40
degrees Centigrade in 1.0 M Sodium Hydroxide solution. This was
then neutralised with phosphoric acid. Following this, 1 ml
samples of homogenate and blank buffer were taken in duplicate
and added to 5 ml of (4:1 ethyl acetate to glacial acetic acid).
After vigorous mixing the samples were centrifuged at 2,000g for
5 minutes to remove precipitated proteins. The supernatant was
removed to a clean tube and 4 ml of 1.0 M Hydrochloric acid
added and mixed. The upper organic phase was carefully removed
and discarded. The remaining aqueous phase was then incubated
for 30 minutes at 100 degrees Centigrade, in a water bath. This
was to convert ether and ester linked oligomers to monomeric
porphyrin. The fluorescence of these samples was recorded on a
Kontron SFM-25 spectrofluorometer exciting at a wavelength of
400 nm, emission being recorded at 596 nm . The fluorescence of
a standard solution of haematoporphyrin (50 ng/ml) was recorded
at the same time. This allows an apparent concentration of drug
to be calculated. The true concentration is greater because not
136
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
all the drug is hydrolysable in these conditions- hence the need
for a calibration, which was performed using 14C- labelled drug
injected into animals. Following a delay of a few hours, tissue
was then removed after killing the animal and the amount of drug
within the tissue was measured using a scintillation counter.
This then gave a “real” level, which was used to calibrate the
system (Vernon D.I. et al 1995).
137
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
9d: In-vivo validation
One the optimum DLI had been determined, a series of experiments
were planned to shown that peak levels of drug in tumour equated
to peak clinical effect. Tumours were grown to approximately 15
mm largest diameter as assessed by palpation and measured using
a steel ruler with 1 mm gradations. Photosensitising drug was
injected at times around the optimum DLI as determined from the
previous experiment - the tumour was exposed after the correct
time interval had passed, under a general anaesthetic of Hypnorm
and Midazolam. A standard light dose of 20 joules/square
centimetre (j/cm2) was given to a 1cm diameter spot on the
superficial surface of the tumour, at 100 milliwatts/cm2
(mW/cm2) using a microlens (Quadra Logic Technologies,
Vancouver, Canada). Laser light at 630 nm (Photofrin 2) or 652
nm (mTHPC) was used, being obtained from a Copper Vapour Laser
(Cu 15, Oxford Lasers, Abingdon Rd., Oxford, U.K.) pumping a
Rhodamine dye laser (Oxford Lasers). Following this the animal
was recovered. After a period of 72 hours had passed for tumour
necrosis to become established, the animals were re-
anaesthetised and given an intravenous injection via the tail
vein of Evans Blue dye (1ml 0.5% Evans Blue in 0.9% saline) to
facilitate identification of the necrotic border (necrotic
tissue is not perfused and therefore will not take up the dye).
The animals were killed 2 minutes later, and the tumours
removed. The tumours were then immediately serially sectioned
perpendicular to the surface of light delivery using a size 20
138
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
scalpel blade, and the depth of induced necrosis measured from
the surface into the tumour with a travelling microscope, the
average of the 3 largest measurements taken as the final
measurement.
139
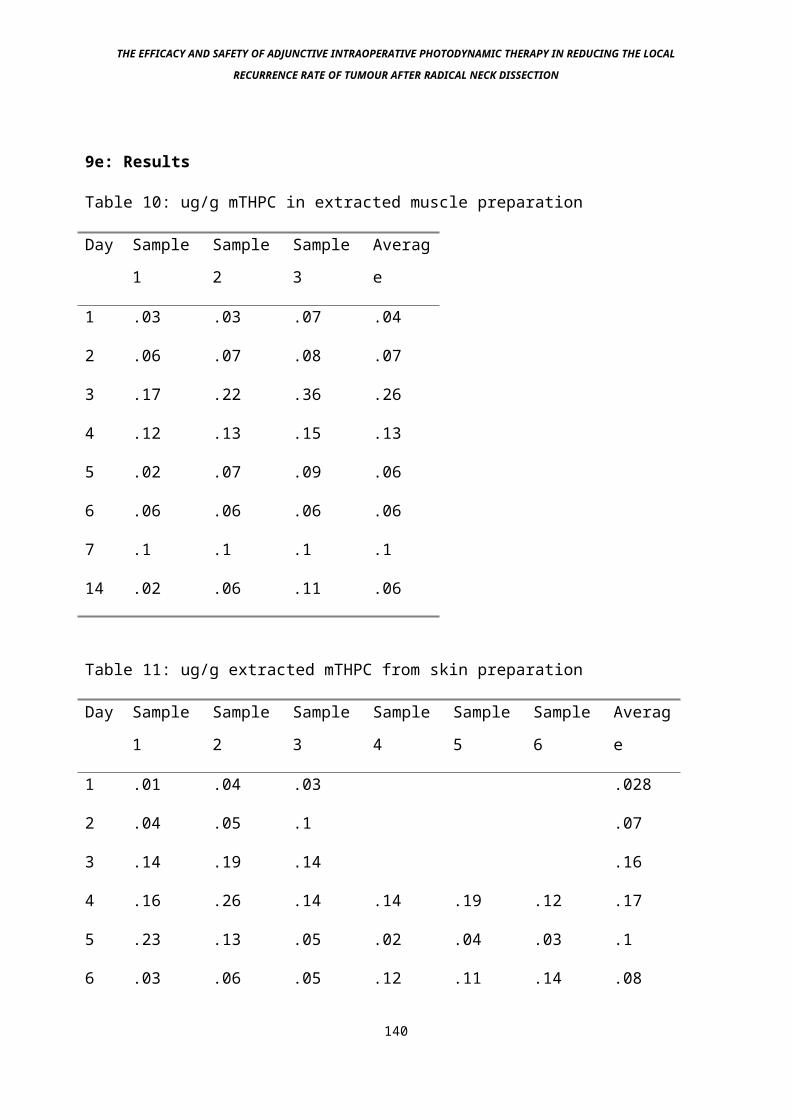
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
9e: Results
Table 10: ug/g mTHPC in extracted muscle preparation
Day Sample
1
Sample
2
Sample
3
Averag
e
1 .03 .03 .07 .04
2 .06 .07 .08 .07
3 .17 .22 .36 .26
4 .12 .13 .15 .13
5 .02 .07 .09 .06
6 .06 .06 .06 .06
7 .1 .1 .1 .1
14 .02 .06 .11 .06
Table 11: ug/g extracted mTHPC from skin preparation
Day Sample
1
Sample
2
Sample
3
Sample
4
Sample
5
Sample
6
Averag
e
1 .01 .04 .03 .028
2 .04 .05 .1 .07
3 .14 .19 .14 .16
4 .16 .26 .14 .14 .19 .12 .17
5 .23 .13 .05 .02 .04 .03 .1
6 .03 .06 .05 .12 .11 .14 .08
140
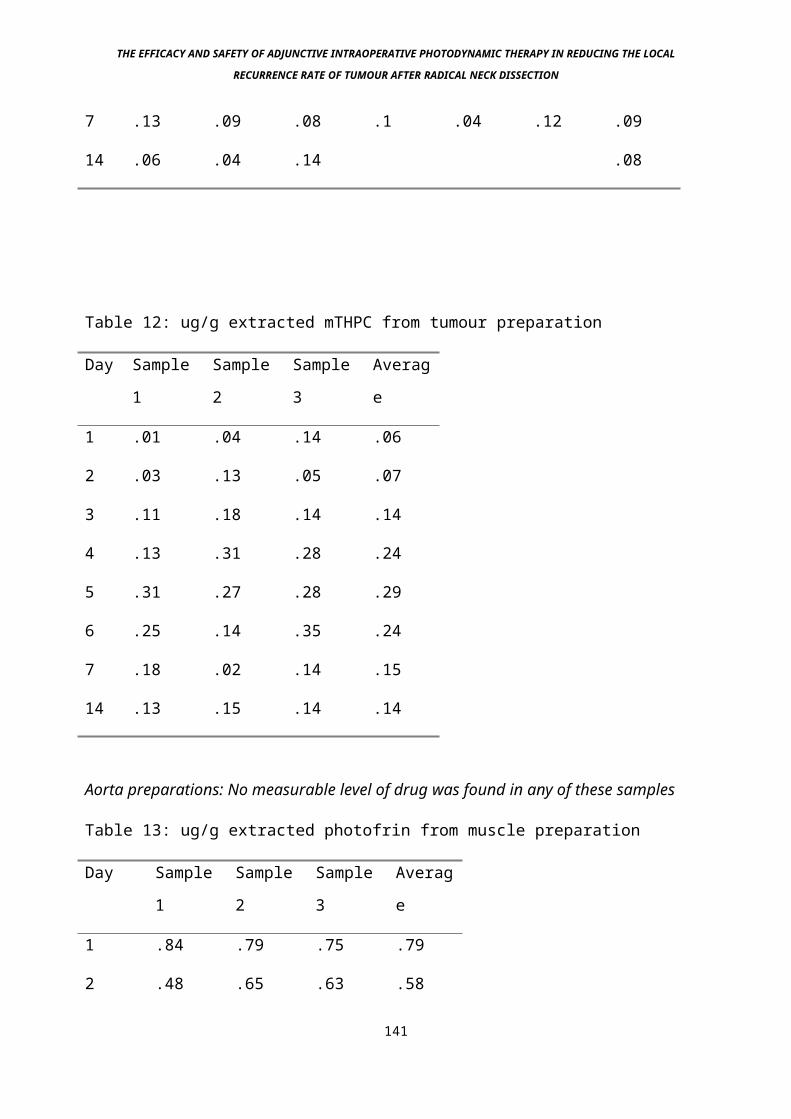
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
7 .13 .09 .08 .1 .04 .12 .09
14 .06 .04 .14 .08
Table 12: ug/g extracted mTHPC from tumour preparation
Day Sample
1
Sample
2
Sample
3
Averag
e
1 .01 .04 .14 .06
2 .03 .13 .05 .07
3 .11 .18 .14 .14
4 .13 .31 .28 .24
5 .31 .27 .28 .29
6 .25 .14 .35 .24
7 .18 .02 .14 .15
14 .13 .15 .14 .14
Aorta preparations: No measurable level of drug was found in any of these samples
Table 13: ug/g extracted photofrin from muscle preparation
Day Sample
1
Sample
2
Sample
3
Averag
e
1 .84 .79 .75 .79
2 .48 .65 .63 .58
141
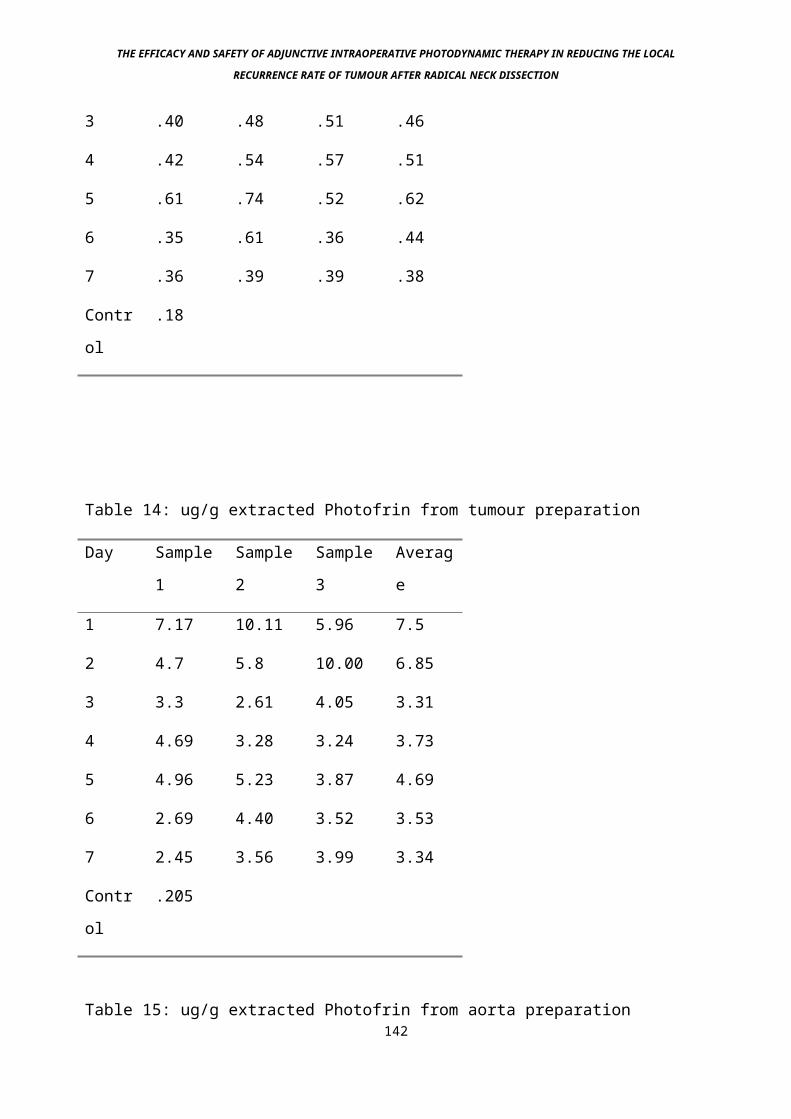
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
3 .40 .48 .51 .46
4 .42 .54 .57 .51
5 .61 .74 .52 .62
6 .35 .61 .36 .44
7 .36 .39 .39 .38
Contr
ol
.18
Table 14: ug/g extracted Photofrin from tumour preparation
Day Sample
1
Sample
2
Sample
3
Averag
e
1 7.17 10.11 5.96 7.5
2 4.7 5.8 10.00 6.85
3 3.3 2.61 4.05 3.31
4 4.69 3.28 3.24 3.73
5 4.96 5.23 3.87 4.69
6 2.69 4.40 3.52 3.53
7 2.45 3.56 3.99 3.34
Contr
ol
.205
Table 15: ug/g extracted Photofrin from aorta preparation142
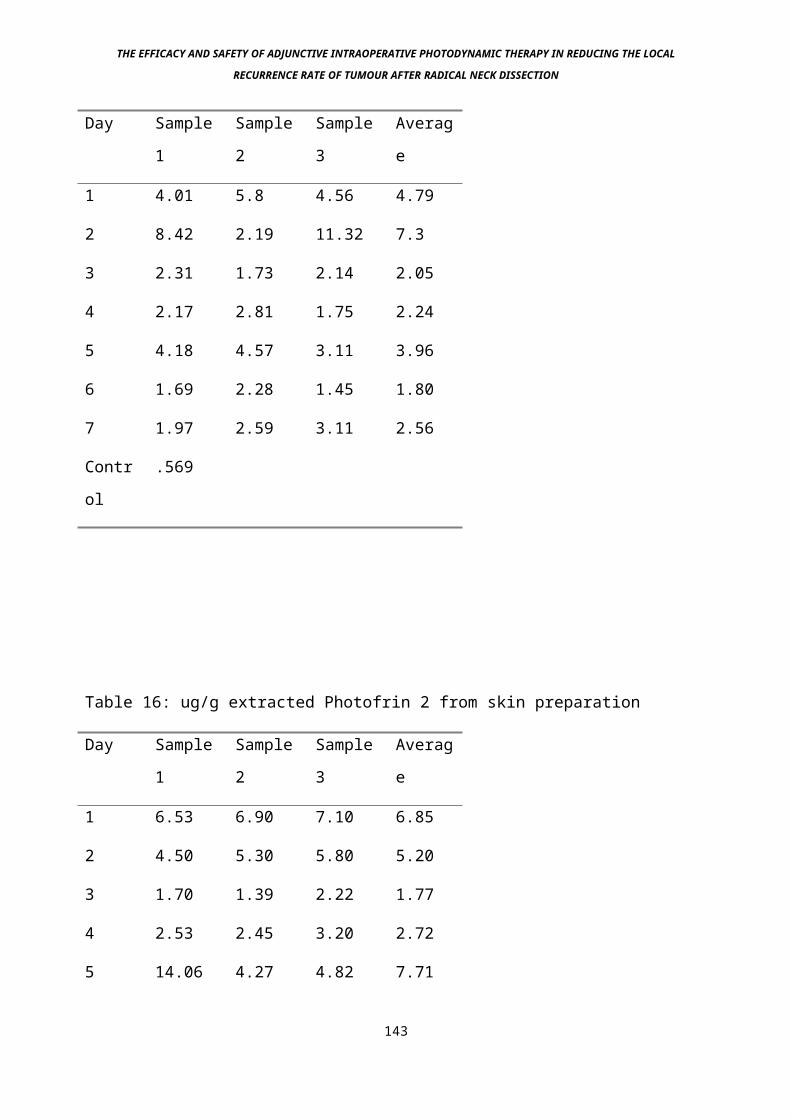
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Day Sample
1
Sample
2
Sample
3
Averag
e
1 4.01 5.8 4.56 4.79
2 8.42 2.19 11.32 7.3
3 2.31 1.73 2.14 2.05
4 2.17 2.81 1.75 2.24
5 4.18 4.57 3.11 3.96
6 1.69 2.28 1.45 1.80
7 1.97 2.59 3.11 2.56
Contr
ol
.569
Table 16: ug/g extracted Photofrin 2 from skin preparation
Day Sample
1
Sample
2
Sample
3
Averag
e
1 6.53 6.90 7.10 6.85
2 4.50 5.30 5.80 5.20
3 1.70 1.39 2.22 1.77
4 2.53 2.45 3.20 2.72
5 14.06 4.27 4.82 7.71
143
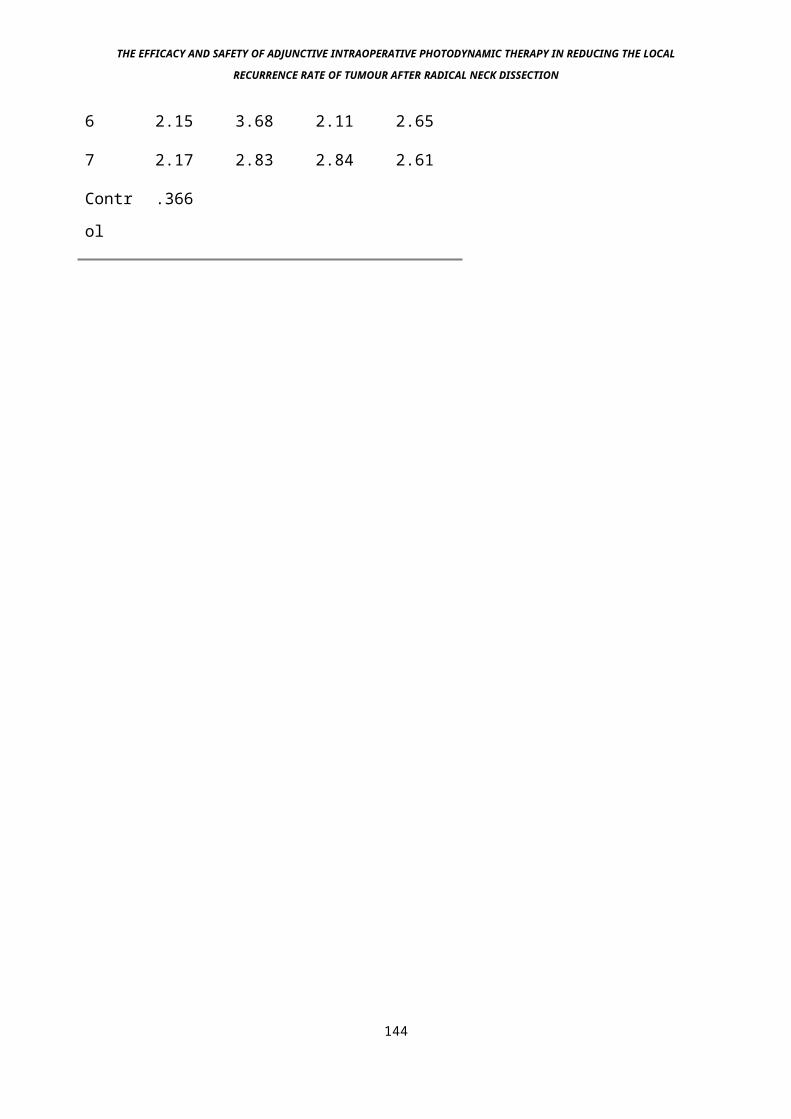
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
6 2.15 3.68 2.11 2.65
7 2.17 2.83 2.84 2.61
Contr
ol
.366
144
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Graph 1: Photofrin results summarised. Insignificant levels of
drug were found in control samples (diluent but no sensitiser
injected)
145
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Graph 2: mTHPC results summarised. No recordable drug was found
in the control samples (diluent but no sensitiser injected).
146
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
9f: Discussion
The main method of assay, namely an extraction procedure
followed by the measurement of resultant supernatant
fluorescence and comparing this with a standard solution is a
widely practised method of analysis of photosensitising drugs.
It is however an indirect process, and until better methods of
quantification and validation, such as measurement of emitted
radiation from isotope doped photosensitisers becomes widely
available (Whelpton R. et al 1996), it is essentially an
unproven process. It is possible that drugs are somehow changed
in the extraction process, or that fluorescence is not a
reliable indicator of amount of active photosensitising drug.
The best method of assay without doubt is a bioactivity assay,
in which the physiological effect, measured for example by depth
of necrosis in tissue, is measured and compared. In this case,
depth of necrosis with a standard light dose and intensity was
to be measured on a daily basis, comparing the two drugs with
their depth of effect at each time interval. This technique was
tried using our fibrosarcoma model. It was not successful mainly
because the predicted depth of necrosis using a clinically
relevant light and drug dose was at least 7 mm in tumour,
generally not optically very dense. Therefore, in order to treat
one surface and not get complete tumour necrosis, so that an
edge between live and necrosed tumour is visible (down to which
the measurement is taken from the incident beam surface), a
tumour at least 10 mm depth is needed, realistically 15 mm. At
this size, in our model HSN fibrosarcoma, central necrosis of
147
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
the tumour occurred, making any possible interpretation of PDT-
induced depth of necrosis meaningless, even when using Evans
Blue dye to optimise the distinction between live and dead
tumour. This problem can be circumvented by growing very small
tumours and treating with low levels of light and drug, but this
has little relation to the clinical doses used, and we have no
evidence that linear extrapolation of the obtained results would
be valid. Also, the percentage error of the measurements taken (
several, including drug to be injected, light dose and
intensity, and depth of necrosis) all increase as the size of
measurement decreases. Other methods of bioactivity assessment
include the treatment of tumours of known depth to induce
complete necrosis, ie, cure, or measure the reduction in tumour
volume (Orenstein et al 1996, Van Geel et al 1995). Thus if a 6
mm tumour is cured at a set parameter of light and drug doses,
but not cured at 7 mm, this gives a depth of effect of between 6
and 7 mm. On preceding and following days, only 5 mm of necrosis
may be obtained, eventually giving a full description of the PDT
kinetics with this model. However, the model is flawed by the
fact that it is very difficult to accurately measure the depth
of tumours prior to treatment, even if they are grown in the
skin and can be inverted - the thickness of the skin is a
variable that is difficult to predict, and since the tumours
need to be fairly small - around 7 mm diameter, this increases
the percentage error. Bioactivity measurement with tumours is
also flawed by the fact that the tumours are inevitably
transplanted from their original primary site and are therefore
unnatural. Other methods of assessment include surface blue 148
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
light fluorescence of tumours (Ansell et al 1995). We feel this
is potentially useful although not yet validated, and may be too
difficult to use clinically, particularly in the less accessible
regions of the head and neck.
The levels of Photofrin 2 in muscle show an initial peak at 24
H, followed by a gradual drop over 7 days, at which stage they
are 50% of their level at 24 hours. There is a small peak at 5
days which is mimicked in all the samples. This has not been
reported in other series, and may be real or artefactual. The
skin results show a very similar picture, although the peak at 5
days is more pronounced. In the fibrosarcoma results, there is
again a very similar drop off in levels, with peak tumour levels
occurring early, and being high only 6 hours after injection.
The peak at 5 days is much less pronounced. One possible reason
for this peak is that all 4 animals on day 5 were given an
incorrectly high amount of drug, although this seems unlikely
since all animals were weighed and injected with drug on the
same day, each cage of 4 animals being sacrificed on a different
day. When the average levels are compared (graph 1), it can be
seen that the best tumour to normal tissue ratio occurs within
the first 3 days. Muscle levels are very low when compared to
skin and tumour levels. Eventually at day 5, skin levels exceed
that of tumour, although favourable selectivity returns by day 6
and. 7. As far as treatment times go, at virtually any time
period between 1 and 7 days there is a highly favourable tumour
to muscle ratio, at its peak this reaches 8:1 (day 1). The peak
tumour to skin ratio occurs at day 3, and is 1.6:1, although at
day 2 it is not much lower, at 1.4:1, and drug levels in tumour 149
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
are that much higher. Thus if one was treating a fairly deep
tumour at the limits of adequate light penetration a drug-light
delay of 2 days would seem sensible, allowing for a fairly large
amount of normal tissue reaction. If a superficial tumour was
being treated, day 3 might be more suitable, because better
selectivity with less normal tissue reaction should occur there.
Other studies have shown these results to be broadly as
expected, and in most cases the clinical treatment times with
Photofrin 2 are between 1 and 2 days. The levels of mTHPC in
tissue show a marked difference to Photofrin 2. More analysis is
available on this drug because it was previously unknown, and
since given the advantages we knew it had over Photofrin 2, it
was likely to be used by us as a clinical agent. In all the
tissues where drug was assayable (muscle, skin and tumour)
initial levels were low. This went on for the first 48 hours.
After this however, levels rose rapidly in all tissue, with
muscle peaking at 3 days, skin between 3 and 4 days and tumour
at 5 days. Peak tumour to normal tissue ratios were 4.5:1 tumour
to muscle and 3:1 tumour to skin, both occurring at day 5, and
coinciding with the highest tumour levels. Fairly high tumour
levels and good selectivity also occurred at days 4 and 6. These
results can be seen clearly when the average levels are compared
(graph 2). Optimum treatment times for the tissues mentioned in
terms of selectivity and amount of drug in tumour therefore
occur at between 4 and 6 days.
150
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
These findings are in keeping with a previous study looking at
clinical effect with human mesothelioma grown in nude mice,
although in this study no difference was found in the levels of
assayed drug between tumour and normal tissue (Ris et al 1993),
a finding in distinct contrast with this study, and perhaps due
to the different tumour model used, the one in this study being
a natural rat tumour occurring in its tissue of origin, against
a human tumour grown in a mouse away from its site of origin.
Safety studies by another group looking at pancreas and
gastrointestinal tract also found normal tissue levels peak at
around 2 days, although in this case relatively high levels
remained until day 4 (Mlkvy et al 1996). The difference in the
pharmacokinetics of the two drugs raise interesting
possibilities. Clearly with Photofrin, the time immediately
after injection and up to 48 hours after that is when levels in
measured tissue are their highest, suggesting that the drug is
perhaps held in the vascular compartment, since immediate (6 H)
levels are very similar to 48 H levels. The lack of data on
plasma levels makes this difficult to prove however, and this
phenomenon may be simply a factor of drug entering tissue at the
same rate that it is cleared from the vascular compartment. With
mTHPC, there is little drug in tissue for the first 48 hours,
following which a rapid rise occurs. This suggests an active
uptake process, perhaps the long delay being due to enzyme
induction. The small amounts initially present may represent the
vascular component - the rest of the drug may be in another
compartment, such as fat. From here it will gradually be
depleted as active uptake processes occur in other tissue, with 151
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
plasma being the exchange medium. We presently have no data on
levels of drug in fat. Other studies have lent evidence that
gives weight to this theory, since initially as expected after
intravenous administration, plasma levels are very high. A rapid
fall off is seen over 6-12 hours, which is the stage we would
expect fat accumulation to occur.
The value of the undoubted pharmacological selectivity of these
drugs, in particular mTHPC has not been properly established.
Indeed, it is unclear as to whether assayed level of drug has
any bearing on resultant photodynamic effect, although common
sense suggests the two are directly related. Clearly if it were
to be true, then one could expect to find minimal normal tissue
damage around treated malignancy when using mTHPC, of great
benefit in areas such as the Head and Neck, skin and brain.
Studies have been performed that seem to validate this principal
(Berenbaum et al 1993), but not with this model or in a human
situation. The value of selectivity of effect can be taken one
step further. Theoretically it should be possible to bleach out
active drug from normal tissue at the same rate as tumour within
the same treatment, at a light intensity below the threshold of
PDT-induced damage.
152
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Given that there was more drug in tumour than normal tissue,
once all the drug in normal tissue has been photobleached, there
should be significant amounts of drug left in tumour (depending
on the degree of selectivity). At this stage the delivery rate
can be raised to above the putative threshold, and the tumour
necrosed with no damage to surrounding normal tissue, since no
drug is now present in that tissue. The levels of drug in the
tissue to be treated can be monitored by blue-,light
fluorescence, although this only gives a value for the
superficial tissue, the amount of bleaching deeper to this can
be calculated by extrapolation using a Monte-Carlo model (DeJode
M.L. personal communication). Once levels in normal tissue reach
minimal amounts, then is the time to raise the activating light
intensity to above threshold. This theory depends on there being
a measurable threshold of light intensity for PDT-induced damage
to occur. This must happen, since patients’ skin appears to be
undamaged by low levels of ambient light even when at the height
of photosensitisation. However, work in our Unit has not
currently been able to identify such a threshold, and it may be
at such a low level that is clinically non-useful.
The fact that no sensitiser was found in the arterial specimens
with either drug is due to either the amount of tissue being too
small to analyse, which the pharmacologists think is unlikely,
or because the total amount of drug present was too small to
analyse. This is encouraging when considering the effects of PDT
on vessels, although work by Grant et al (1994) shows that with
some drugs the endothelium is the site of photosensitiser
153
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
accumulation, and very small amount in such a delicate tissue
could still cause severe damage.
Another study has also compared mTHPC with Photofrin 2 and had
more success in assessing bioactivity when using a different
tumour model, RIF 1 (Van Geel I.P.J., et al 1995). They found
better efficacy and selectivity with mTHPC. Ma et al (1994) also
showed greater efficiency of light conversion into singlet
oxygen when comparing mTHPC with mTHPP and Photofrin 2. More
recently, Orenstein et al (1996) found that another Chlorin,
Chlorin E6 was more selective and more powerful than Photofrin 2
when using the Colo-26 tumour model.
154
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
In conclusion, this study showed that when measuring depth of
PDT induced necrosis from the surface with mTHPC as the
photosensitising drug, the HSN rat fibrosarcoma is not a
suitable model even when optimising the distinction between
normal and necrotic tissue with methylene blue administration.
Pharmacological selectivity was demonstrated with both drugs,
with unit drug doses of mTHPC being much lower due to its higher
efficiency. The optimum drug-light interval with mTHPC is
thought to be between 4 and 6 days post injection and between 1
and 2 days with Photofrin 2, for greatest selectivity and
effect. This study corroborates other evidence suggesting that
for mTHPC the optimum drug-light interval is 96 hours.
155
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
10: Experiment 2 - The efficacy of Adjunctive Intraoperative
Photodynamic Therapy in a rat fibrosarcoma model with mTHPC
10a: Description
Since PDT works at least partially at the cellular level, (Moan
et al 1982) it may also help to reduce the local recurrence rate
of tumours after surgical excision, by destroying microscopic
tumour residue. This experiment was designed to test this
hypothesis in an animal model. The aim of this study was to
determine whether the tumour model HSN fibrosarcoma, which bears
a close resemblance to our target clinical tumour, squamous cell
carcinoma of the Head and Neck , shows a statistically
significant reduction in local recurrence with the treatment
groups when compared with the control group. The experiment was
performed in such a manner that the operating and evaluating
surgeon (MGD) was blind to the treatment group each animal was
in. This had not been done in the previous studies, to our
knowledge. The other studies also used tumours that bore less
resemblance to the aggressively locally invasive fibrosarcoma
used here, which is similar in character to squamous cell
carcinoma of the Head and Neck.
10b: Tumour
The fibrosarcoma tumour HSN in Chester-Beatty hooded (CBH) rats
was used, as before.
Using a freshly killed donor animal with a tumour previously
inoculated, the tumour periphery (containing viable, non-156
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
necrotic cells) was excised. Small pieces of tumour
approximately 1mm x 1mm x 1mm were taken and implanted under
direct vision into the flank musculature of the adult CBH rats
under sedation with Midazolam. Either one or both flank areas
were inoculated. Following this the animals were recovered and
daily records made of the largest tumour dimension.
157
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
10c: Photodynamic Therapy Parameters
The drug dose of mTHPC used was 1.0 mg/kg body weight delivered
intravenously via the tail vein. mTHPC was obtained from Scotia
Pharmaceuticals, Guildford, U.K., as a gift. It was stored as a
sterile powder in a fridge, and reconstituted fresh with 1g
ethanol and 1g polyethylene glycol 400 made up to 5 ml with
sterile water for injection, to make up a solution of 0.5 mg/ml.
When reconstituting the drug for injection, meticulous attention
was taken to ensure that the drug had gone into solution.
Invariably this meant 2 or 3 minutes of vigorous shaking,
ensuring no residue was visible on the bottom of the tube used
for reconstitution.
The drug light interval was 96 hours, as Experiment 1 and other
studies have found this period of time to offer advantages in
terms of potential selectivity within tumour tissue when
compared to surrounding normal tissue whilst retaining excellent
anti-tumour activity (Ris et al 1993, Van Geel et al 1993). The
light dose given for photoactivation was 20 joules/square
centimetre (j/cm2) at an intensity of 100 milliwatts/cm2
(mW/cm2), wavelength 652 nm. These were parameters used in the
first studies with the mTHPC, with good necrosis of malignant
tissue seen (Ris et al 1991).
158
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
10d: Preliminary studies
The aims of the 2 preliminary studies were to determine:
1) What the feasible maximum size of the tumours was with
respect to maximising the recurrence rate of tumour after
surgery, without an unacceptably high mortality rate.
2) What the growth characteristics of the tumour were, in order
to predict the day at which tumours would reach the previously
determined optimum size.
10d(i): Study 1
Initial studies were performed to determine the optimum size of
tumour in terms of local recurrence rate after macroscopic
excision, and survival of the animal. This was necessary because
clearly the larger the tumour, the more likely it is to recur
locally due to inadequacy of excision, even if the margins are
macroscopically clear. However, resection of very large tumours
will result in a critical loss of fluid, and death of the
animal. Therefore we wanted to know what the safe maximum size
of the tumours was. Tumours were grown bilaterally until they
reached a size of 1cm, 2cm or 3cm largest diameter as measured
externally with the animal awake. At this stage a general
anaesthetic was administered, and both tumours removed locally,
but with full macroscopic clearance (ie no visible tumour left).
The skin was then closed and the animals recovered. Animals were
closely monitored postoperatively for signs of distress. If any
were shown the animals were immediately killed by a schedule 1
technique. Other animals succumbed shortly after surgery. All 159

THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
non-survivors were recorded. The survivors were killed 2 weeks
after surgery and the surgical sites examined for signs of local
recurrence, which was recorded.
160
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
10d(ii): Study 2
This was performed to determine the predictability of tumour
growth prior to photosensitisation. Once the optimum tumour size
had been determined, it was important to have an idea regarding
the growth rate of the tumour, since the decision had been taken
to sensitise 4 days prior to treatment. Clearly, a tumour
measured at the safe maximum size at injection would be
significantly above that size 96 hours later, given a doubling
time of x hours, where x is any number less than around 300. Ten
tumours were grown in 10 animals, the same way as above, but
unilaterally. Tumours were implanted on day zero. Alternate
daily measurements of the maximum tumour diameter were taken.
Measurements were taken with the animal awake using a steel
ruler with 1mm gradations. Once the tumour reached around 20mm
diameter (the chosen size for the 3rd experiment on the basis of
the first preliminary study), the animal was killed.
Once this data had been gathered, a blind, prospective
controlled study (Study 3) was performed to test the hypothesis
that AIOPDT with mTHPC reduces significantly local recurrence
after macroscopic surgical excision in the HSN rat fibrosarcoma
model:
161
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
10d(iii): Study 3
4 groups of 30 animals were included in the experiment. These
were:
1) Surgery and AIOPDT.
2) Surgery, mTHPC diluent and light only at the above parameters
(no drug).
3) Surgery and drug only
4) Surgery only.
Two independent tumours were grown in each animal, on the back,
to the left and right side of the midline, well separated
(picture 3), using the method described above. After 10 days,
the animals were admitted into one of the 4 treatment groups..
They were kept in cages of up to 5 animals each, cages were
coded according to the group each animal was in. Each cage was
coded following randomn selection by biological services staff.
Those animals due for drug injection (groups 1 and 2) were
weighed and injected intravenously via the tail vein with 1mg/kg
mTHPC that had been freshly prepared from powder. 4 days later a
general anaesthetic was administered to all animals and the
tumours exposed. The largest diameter measured. Any tumour of
20mm +/- 2mm largest diameter was included in the study and 162
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
resected so that no macroscopic tumour was left (picture 4).
Tumours beyond these criteria were not used. At that stage
animals due for light administration (groups 1 and 2) were
identified and 20 joules/cm2 of 652 nm laser light of 100
milliwatts/cm2 intensity was given. The light was produced by a
copper vapour laser pumping a rhodamine dye laser (Cu 15, Oxford
Lasers, Abingdon Rd., Oxford, U.K.). The light intensity was
measured using a photodetector linked to an integrating sphere,
and was delivered via a microlens (Quadra Logic Technologies,
Vancouver, Canada).
163
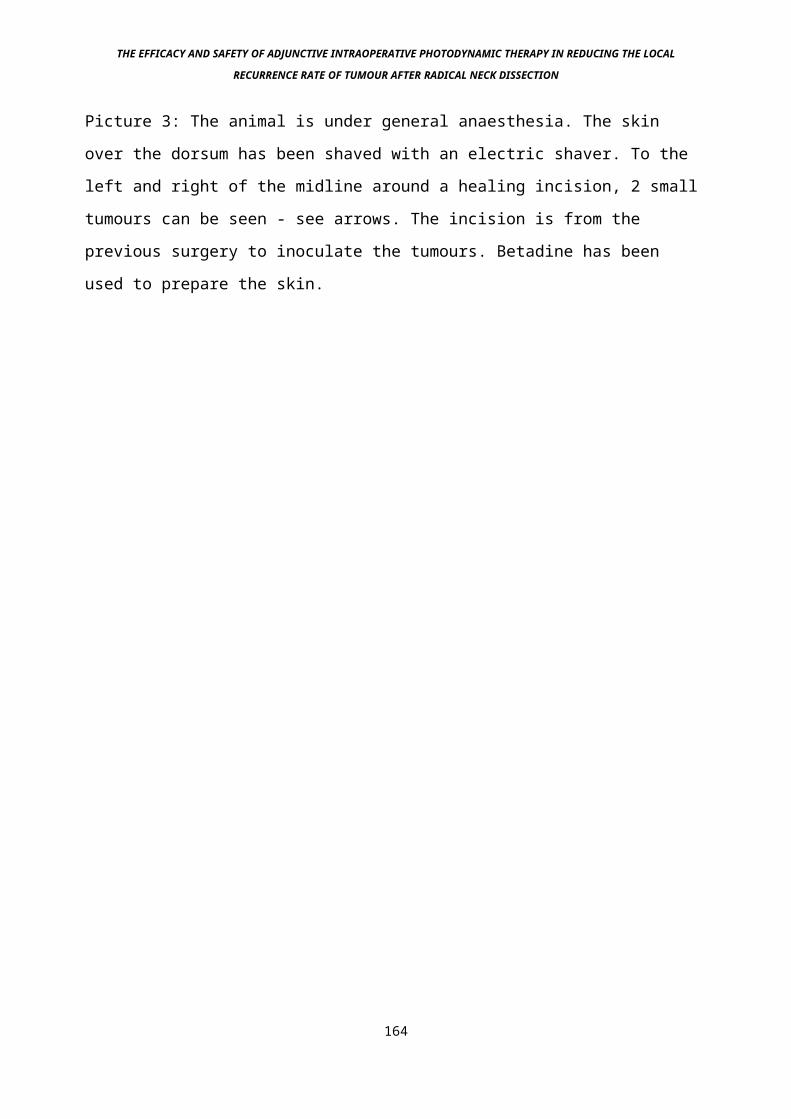
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Picture 3: The animal is under general anaesthesia. The skin
over the dorsum has been shaved with an electric shaver. To the
left and right of the midline around a healing incision, 2 small
tumours can be seen - see arrows. The incision is from the
previous surgery to inoculate the tumours. Betadine has been
used to prepare the skin.
164

THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Picture 4: At the end of the each day’s experimentation, the
tumours are collected and incinerated. The uniform nature of the
tumour growth can be seen from this picture.
165
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
In all cases a 2.5 cm diameter spot was used with the original
tumour site in the middle, giving a margin of normal tissue
treatment, which was 12.5 % of the original tumour size. The
light spot size was measured using a steel ruler with 1 mm
gradations. The microlens was held steady over the treatment
site by holding it with a clamp fixed to a retort stand.
Following this the skin was closed and the animals were
recovered. At this stage the rats were numbered by puncturing
and marking the ears with Evans Blue dye (Picture 5).
Postoperatively the animals were observed closely. Any animal in
distress was killed immediately and recorded. Any animal
succumbing to the effects of surgery was recorded.
Once obvious macroscopic and potentially distressing tumour
recurrence had occurred in one animal (the experimental end
point), all animals in the groups treated in that session were
killed. The flank areas were opened and examined for tumour
recurrence. Any suspicious areas that were not obviously tumour
were biopsied and sent for histological confirmation of the
result, otherwise the diagnosis of tumour recurrence was made by
sight alone. At this stage and during recording of the results
the examining surgeon was blind to the group the animals were
in, only the experiment had been completed were the codes broken
and the results recorded.
166

THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Picture 5: Ears being marked. The animals are recovered on a
heated mat to prevent hypothermia.
167
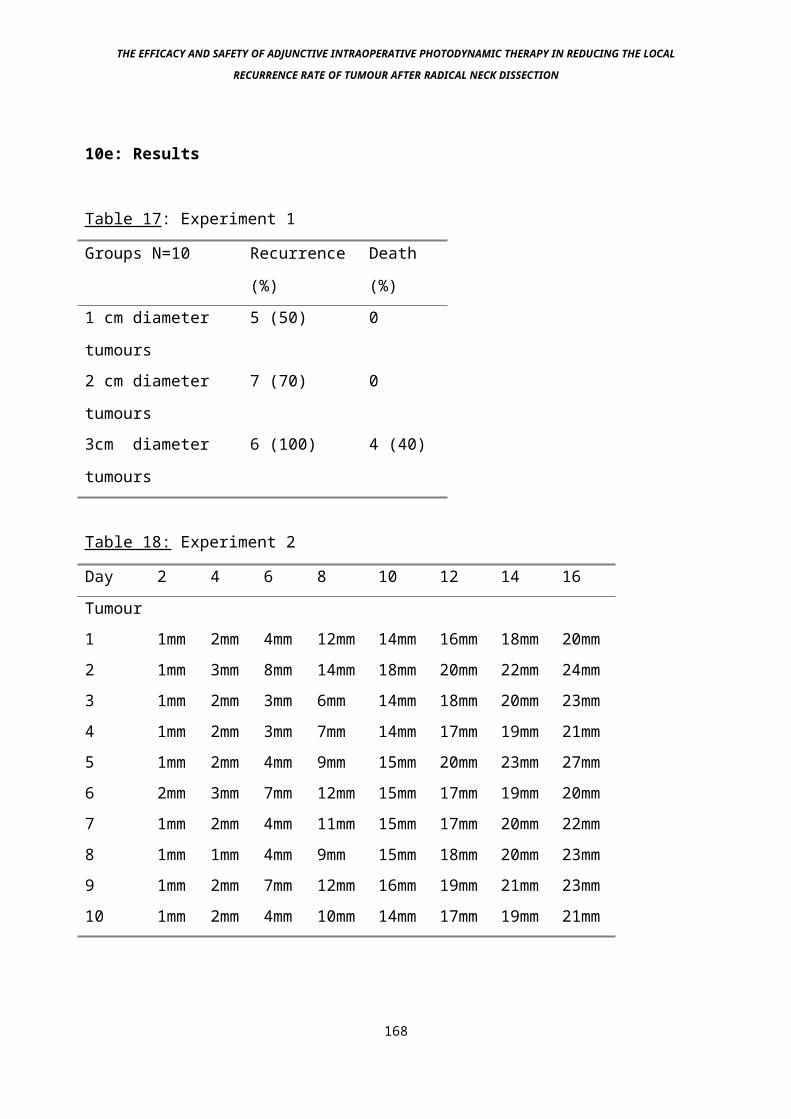
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
10e: Results
Table 17: Experiment 1
Groups N=10 Recurrence
(%)
Death
(%)1 cm diameter
tumours
5 (50) 0
2 cm diameter
tumours
7 (70) 0
3cm diameter
tumours
6 (100) 4 (40)
Table 18: Experiment 2
Day 2 4 6 8 10 12 14 16Tumour1 1mm 2mm 4mm 12mm 14mm 16mm 18mm 20mm2 1mm 3mm 8mm 14mm 18mm 20mm 22mm 24mm3 1mm 2mm 3mm 6mm 14mm 18mm 20mm 23mm4 1mm 2mm 3mm 7mm 14mm 17mm 19mm 21mm5 1mm 2mm 4mm 9mm 15mm 20mm 23mm 27mm6 2mm 3mm 7mm 12mm 15mm 17mm 19mm 20mm7 1mm 2mm 4mm 11mm 15mm 17mm 20mm 22mm8 1mm 1mm 4mm 9mm 15mm 18mm 20mm 23mm9 1mm 2mm 7mm 12mm 16mm 19mm 21mm 23mm10 1mm 2mm 4mm 10mm 14mm 17mm 19mm 21mm
168

THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Figure 2: Representation of tumour growth rate, obeying
Gompertzian dynamics
169
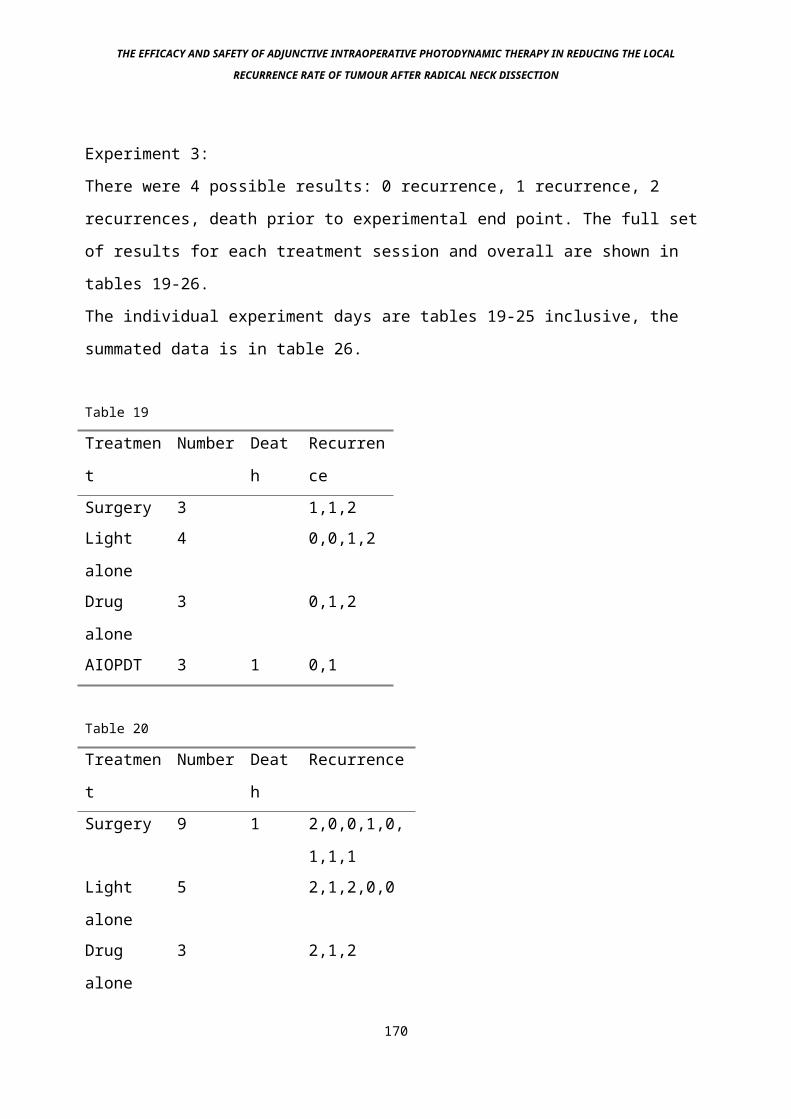
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Experiment 3:
There were 4 possible results: 0 recurrence, 1 recurrence, 2
recurrences, death prior to experimental end point. The full set
of results for each treatment session and overall are shown in
tables 19-26.
The individual experiment days are tables 19-25 inclusive, the
summated data is in table 26.
Table 19
Treatmen
t
Number Deat
h
Recurren
ceSurgery 3 1,1,2Light
alone
4 0,0,1,2
Drug
alone
3 0,1,2
AIOPDT 3 1 0,1
Table 20
Treatmen
t
Number Deat
h
Recurrence
Surgery 9 1 2,0,0,1,0,
1,1,1Light
alone
5 2,1,2,0,0
Drug
alone
3 2,1,2
170
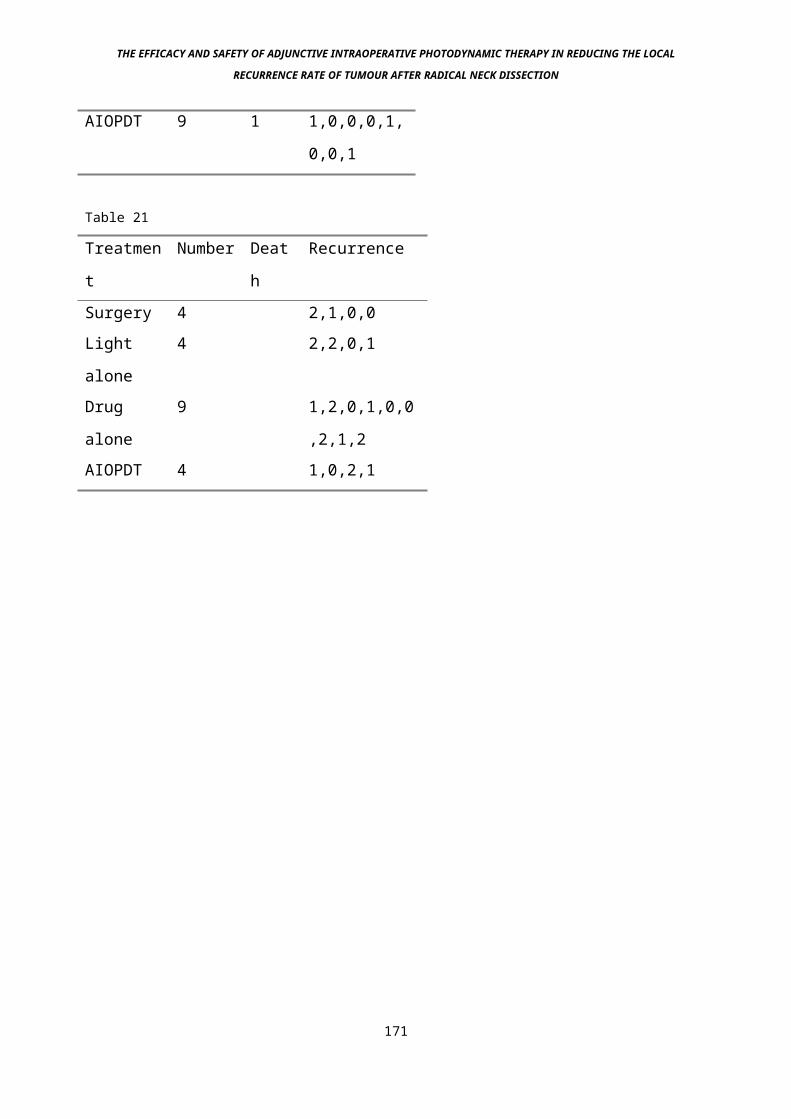
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
AIOPDT 9 1 1,0,0,0,1,
0,0,1
Table 21
Treatmen
t
Number Deat
h
Recurrence
Surgery 4 2,1,0,0Light
alone
4 2,2,0,1
Drug
alone
9 1,2,0,1,0,0
,2,1,2AIOPDT 4 1,0,2,1
171
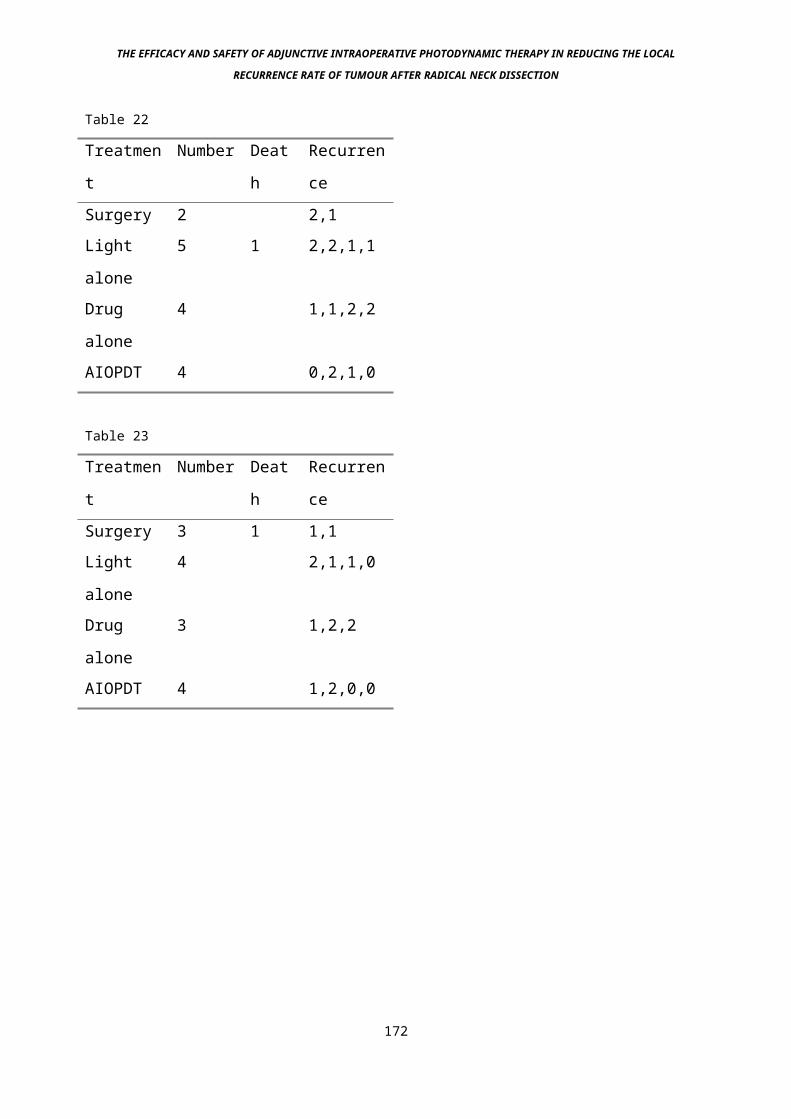
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Table 22
Treatmen
t
Number Deat
h
Recurren
ceSurgery 2 2,1Light
alone
5 1 2,2,1,1
Drug
alone
4 1,1,2,2
AIOPDT 4 0,2,1,0
Table 23
Treatmen
t
Number Deat
h
Recurren
ceSurgery 3 1 1,1Light
alone
4 2,1,1,0
Drug
alone
3 1,2,2
AIOPDT 4 1,2,0,0
172
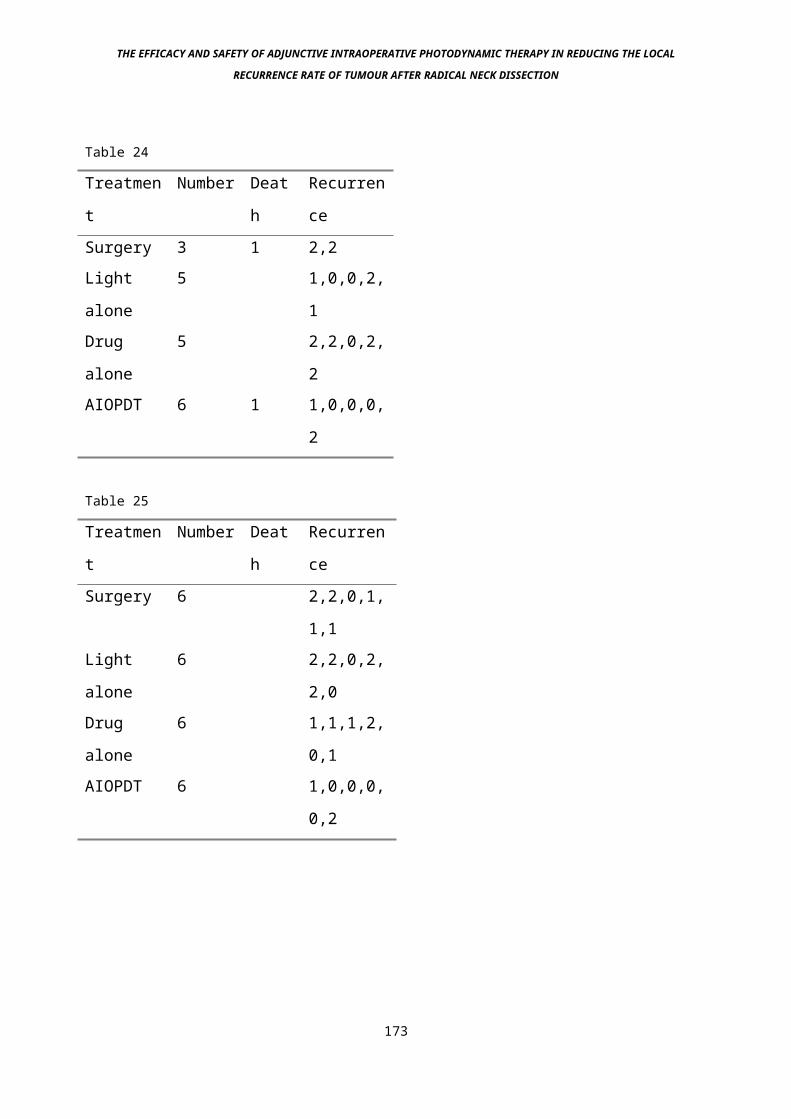
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Table 24
Treatmen
t
Number Deat
h
Recurren
ceSurgery 3 1 2,2Light
alone
5 1,0,0,2,
1Drug
alone
5 2,2,0,2,
2AIOPDT 6 1 1,0,0,0,
2
Table 25
Treatmen
t
Number Deat
h
Recurren
ceSurgery 6 2,2,0,1,
1,1Light
alone
6 2,2,0,2,
2,0Drug
alone
6 1,1,1,2,
0,1AIOPDT 6 1,0,0,0,
0,2
173
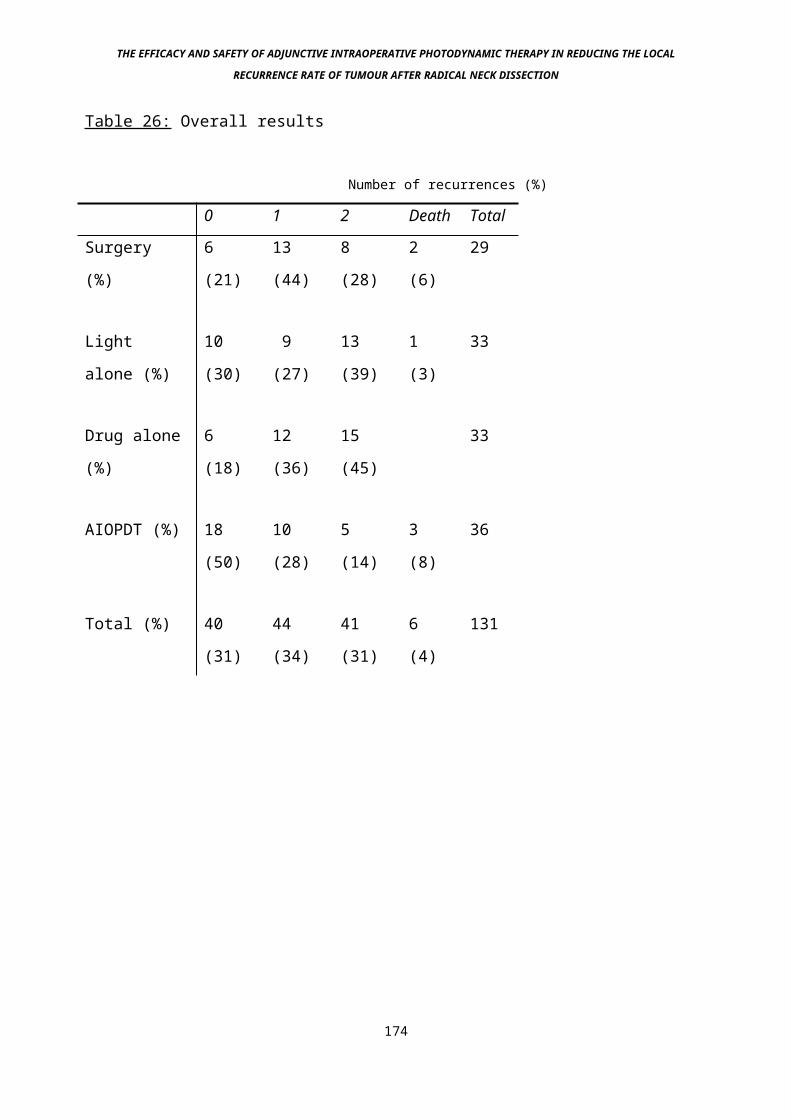
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Table 26: Overall results
Number of recurrences (%)
0 1 2 Death Total
Surgery
(%)
6
(21)
13
(44)
8
(28)
2
(6)
29
Light
alone (%)
10
(30)
9
(27)
13
(39)
1
(3)
33
Drug alone
(%)
6
(18)
12
(36)
15
(45)
33
AIOPDT (%) 18
(50)
10
(28)
5
(14)
3
(8)
36
Total (%) 40
(31)
44
(34)
41
(31)
6
(4)
131
174
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
10f: Statistical Analysis
A Kruskal-Wallis one way analysis of variance of ranks was used
to compare the 4 treatment groups (1st = Surgery alone, 2nd =
Light and surgery, 3rd = Drug and surgery, 4th = surgery and
AIOPDT). There were significant differences between the 4 groups
(p=0.01). Examination of the distribution of outcome in the 4
groups suggested that the first 3 groups had similar outcomes. A
Kruskal-Wallace anova test was used to compare these first 3
groups and found no significant difference (p=0.6). The 4th
group (surgery and AIOPDT) was then compared with these 3 groups
combined. The Kruskal-Wallace anova demonstrated a significant
difference (p=0.002). A rank transformation was also used on the
data, and a two-way analysis of variance on the ranks with the
factors “treatment group” and “day” was performed. There were no
significant differences between the 7 days on which the study
was performed (p=0.7).
175
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
10g: Discussion
Table 17 shows that the size of tumour removed is proportional
to the death rate following its removal. This is in keeping with
general mortality figures in surgery, in which size and stage at
surgery have a negative effect on outcome and perioperative
mortality. Size of tumour also influences the local recurrence
rate in a positive manner. Thus a compromise of perioperative
mortality against local recurrence was needed for this study.
The 2cm diameter tumours were chosen on that basis.
Table 18 and figure 2 show that tumours grow in a fairly uniform
manner after intramuscular inoculation of a standard sized
tumour piece. This it important because it allows the prediction
of when the tumour will be 2cm in largest diameter for the
experiment. This is particularly important in PDT
experimentation because of the 96 hour drug-light interval that
is needed before the experiment can begin.
Tables 19 – 25 show the individual experiment days. The
variation of numbers within the groups represents excluded
tumours that were outside the treatment parameters. As discussed
in the statistics section, there were no significant differences
between the groups.
The results (summarised in table 26) show a statistically
significant reduction in the local tumour recurrence rate with
the treatment group as compared to the control groups. Although
there were more deaths postoperatively in this group, this was
not a significant finding, and may just represent the relatively
small numbers tested. The control groups tested the hypothesis 176
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
that the drug and diluent is toxic to tumours without light
(drug only group), although even in this group there will have
been a mild photodynamic effect due to background theatre
illumination and theatre lights during the excision. However,
the total light dose given during the relatively short
(approximately 5 minutes) time that it took for excision of both
tumours is so low that this effect is unlikely to have been
significant. The control groups also tested the hypothesis that
the drug diluent is an active photosensitising agent (light and
diluent only group), although the hypothesis that 652 nm laser
light at non-thermal intensity could be cytotoxic was therefore
not independently tested. This is extremely unlikely however
since there are many publicly available lasers at around this
wavelength (laser light pointers) that have been shown to be
totally safe except when shone directly into the eyes. The fact
that there was no significant difference between any of the
control groups including the surgery alone suggests that these
hypotheses are invalid.
A study such as this is only valid if the principle that local
tumour recurrence is due to residual disease is agreed. There
are other theories regarding why tumours recur in the excision
bed, such as further metastases from the primary area, or new
primary disease growing in the tumour bed. Studies have shown
that after a macroscopically complete excision, if the tumour
bed is washed with cell growth medium and incubated in the
correct conditions for growth, viable tumour cells can be grown
(Harris and Smith 1960). These cells almost certainly come from
the excised tumour area, either due to "burst and spill" or 177
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
unwittingly cutting through tumour during the excision, and
contaminating the surgical instruments (Beahrs and Barber 1962).
What is not known is whether these are viable or not in the
clinical situation. Disease recurrence due to residual tumour
can also occur because of involvement of vital structures
rendering the tumour inoperable, or because tumour margins or
not clear due to the disease growing to the defined limits of
the operation (Olcott et al 1981). Other adjunctive
intraoperative methods have been tried in order to reduce the
local recurrence rate of tumour after Head and Neck surgery.
178
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Other intraoperative therapeutic methods include:
1) Intraoperative external beam radiotherapy, which was
logistically very difficult, time consuming and damaging to
the carotid artery (Freeman et al 1990).
2) Washing the tumour bed with cytotoxic agents, including
distilled, sterile water which has not been shown to be
effective, presumably because there is little penetration of
effect into the microscopic cracks and crevices on the tumour
bed where viable tumour clumps may lodge.
This tumour model bears a reasonable relationship to the
proposed clinical treatment, namely metastatic neck disease
treated by radical neck dissection. Neither are primary tumour
sites, the animal model being an implanted tumour graft, the
clinical model being a proliferating clump of tumour cells shed
from the primary site into lymphatic channels and caught in the
draining lymph glands. The main difference apart from site of
growth is in the fact that the clinical model lies in a lymph
gland, the animal model in normal surrounding muscle, although
this is important since the tumour is growing in its natural
environment, being a connective tissue tumour (Bown S.G. pers.
comm.). It thus is a more natural model than others used for
AIOPDT studies, such as neuroblastoma in muscle (Davis et al
1990) or adenocarcinoma in subcutaneous tissue (Abulafi et al
1994). However, by the time most secondary tumours in the neck
have been detected, they have reached a size of at least 1cm
diameter, and have usually destroyed the lymph node they lie in.179
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
The adjacent tissue to most of the lymph nodes in the neck is
mainly muscle, particularly in the lymph node bed, and fat,
which tends to lie superficially. Thus even in the human
situation, the tumour lies in close proximity to the muscle.
This is even more so following radical neck dissection, since
the superficial tissue (mainly fat, internal jugular vein and
the sternocleidomastoid muscle) and tumour is removed, the deep
musculature is left untouched. Thus the treatment site for
AIOPDT in both cases would be a muscle bed. The tumour type
used, HSN fibrosarcoma was also similar to the human model,
squamous cell carcinoma of the upper aerodigestive tract. This
is because it is a locally invasive, non-encapsulating tumour.
Clearly an encapsulating tumour would be easy to shell out with
little chance of local recurrence, whereas a tumour
microscopically invading into the surrounding tissue will recur
unless a wide block of apparently normal tissue is removed with
the specimen, which was not done in this case. The tumour was
removed very close to the main tumour lump, although macroscopic
clearance was complete in all cases. Therefore it is more likely
that microscopic tumour residue occurs, leading to a local
recurrence rate in the control groups of around 70%. The initial
studies on survival after excision also showed this - it would
have been useful to have had an even higher local recurrence
rate as occurred with the 3 cm diameter tumours, but the
postoperative mortality rate made this unacceptable.
The scope of procedures suitable for AIOPDT in surgery is much
greater than just radical neck dissection . It may also have a 180
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
role in general surgery (Herrera-Ornelas et al 1986, Nambisan
R.L. et al 1988, Abulafi et al 1993), neurosurgery (Muller and
Wilson 1995) and thoracic surgery (Ris et al 1993). Conservation
surgery in the neck, in vogue since it seems to reduce
postoperative morbidity (Bocca 1975) could be made safer by
treating those retained structures such as the accessory nerve
with PDT to mop up any residual tumour around such structures.
The fact that red light penetrates tissue significantly means
that structures such as the accessory nerve can be completely
treated by illuminating onto and through the nerve. The same may
be true of other vital structures in the neck such as the
carotid tree, although the fact that this is of quite large
diameter and filled with blood means that complete penetration
and treatment of the medial surface is unlikely to be effective.
Prior to clinical studies, safety work is therefore needed,
particularly regarding the effect of PDT on arterial structures.
10h: Conclusion
The scope of adjunctive intraoperative photodynamic therapy is
large, in the Head and Neck as well as other areas. This and
other studies have successfully demonstrated, to the
satisfaction of statisticians, the principle that treatment
reduces the local recurrence rate of tumour following
macroscopically clear excision to be true on a preclinical
basis.
181
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
11: Experiment 3 - Preclinical Photodynamic Safety Studies on
Arteries
11a: Description
The previous study has shown that adjunctive intraoperative
photodynamic therapy (AIOPDT) can significantly reduce the local
recurrence rate of malignant tumours after macroscopically clear
tumour removal. This has implications for most forms of cancer
surgery, but particularly those in which the local recurrence of
disease has a major impact on survival. One such operation is a
radical neck dissection for secondary spread of squamous cell
carcinoma of the upper aerodigestive tract. AIOPDT may be useful
to reduce the local recurrence rate after this operation. Before
AIOPDT could be safely transferred into the clinical sphere,
safety studies were necessary on vital structures that would be
in the photodynamic treatment area. For the operation of radical
neck dissection, this means the carotid tree, a structure whose
damage leads to grave consequences.
The operation of radical neck dissection, as described in the
introduction is a good example of a Head and Neck operation
that has a significant mortality if local recurrence occurs. It
involves the removal of a block of tissue from the side of the
neck, incorporating all of the surgically available lymph nodes 182
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
on that side. It is classically performed to treat secondary
spread of squamous cell carcinoma of the upper aerodigestive
tract into the lymph nodes on one side of the neck. All the
nodes are removed because it is not possible to know the extent
of spread prior to surgery, although retrospective studies have
suggested that this can usually be predicted. There is a very
high mortality rate due to local recurrence in this area when it
occurs (Pearlman 1979, DeSanto et al 1982). Therefore any
treatment that might reduce this figure is welcome.
Safety work was performed to assess the effect of AIOPDT on
vital structures that would be exposed to PDT in the tumour bed
of this operation, the most important of which is the carotid
tree, consisting of the common carotid artery and its terminal
branches, the internal and external carotid arteries.
183
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Other structures in the surgical bed include the vagus and
hypoglossal nerves and the carotid body. Since nervous tissue
has so far been found to be largely resistant to PDT (anecdotal,
unpublished observations in general), and since these structures
are not integral to the survival of the patient, they were not
studied in this experiment. The carotid vessels are vital
however, not least because if the carotid artery wall is
weakened with AIOPDT and it ruptures postoperatively, death due
to exsanguination is likely, as has happened following PDT
treatments to advanced Head and Neck cancers (Schuller et al
1985, Gluckman 1991), although there is a very definite
incidence of carotid artery rupture with this disease, so the
significance of this is not known. Also, the internal carotid
artery is often an "end artery", having little or no collateral
supply. Therefore if it clots off during PDT or stenoses at a
later date due to partial damage, the entire volume of tissue
supplied by the vessel might die. Since this vessel is the major
blood supply to the ipsilateral cerebrum, at the very least a
major cerebrovascular accident (CVA, stroke) can be expected.
11b: PDT Details
Previous studies had shown a suitable drug level for animal
experimentation to be 1.0 mg/kg body weight. The drug light
interval chosen was 96 hours, since again this seemed likely to
give a good tumour necrosis response with minimal normal tissue
damage, and was the DLI used in early and all subsequent
clinical investigation on Head and Neck cancer (Dilkes et al
1994). The light dose given ranged from 10 to 100 joules/cm2 184
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
(J/cm2), in order to potentially obtain a dose/damage curve and
predict safe levels of light, potentially useful if severe
damage was seen, 500 J/cm2 was given to the non-sensitised
control groups. The light delivery rate was kept at 300
milliwatts (mW)/cm2 and given via a microlens (Quadra Logic
Technologies, Vancouver, Canada) in all cases. The delivery rate
was higher than in previous studies because of the excessive
amount of time it would take to deliver the maximum light dose,
500 J/cm2 at the previously used parameter of 100 mW/cm2. The
light source used was an Oxford Lasers CU15 copper vapour laser
pumping a Rhodamine dye laser tuned to 652 nm. Light intensity
was continually checked using an integrating sphere and
radiometer.
185
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
11c: Drug
The drug mTHPC was obtained form Scotia Pharmaceuticals,
Guildford, Surrey, U.K. as a gift. It was supplied as dry,
sterile powder of 99.7% purity. When administered it was
dissolved immediately before use (within 1 hour) in its diluent.
Adult female ex-breeder Wistar rats were obtained from Charles
River Ltd. Drug was administered intravenously via the tail vein
using a standard restraining device. Once the animals had been
photosensitised, they were kept out of direct contact with
light, in darkened conditions.
11d: Study Design
The rat superficial femoral artery was chosen as the study
vessel. This structure is a continuation of the external Iliac
artery, arising where the common femoral artery gives off its
profunda vessels. It is easy to expose on the surface of the
adductor muscles in the floor of the femoral triangle, and lies
in a fibrous sheath also containing the femoral vein and nerve
(sensory only). Both (right and left) femoral vessels were
dissected free of surrounding structures under a general
anaesthetic of Hypnorm and Midazolam, using microsurgical
instruments and magnifying loupes where necessary. Prior to
light administration, a small piece of black blotting paper,
soaked in normal saline was gently manoeuvred under the vessel
to shield surrounding structures, making eventual postoperative
dissection easy, and avoiding serious damage to underlying 186
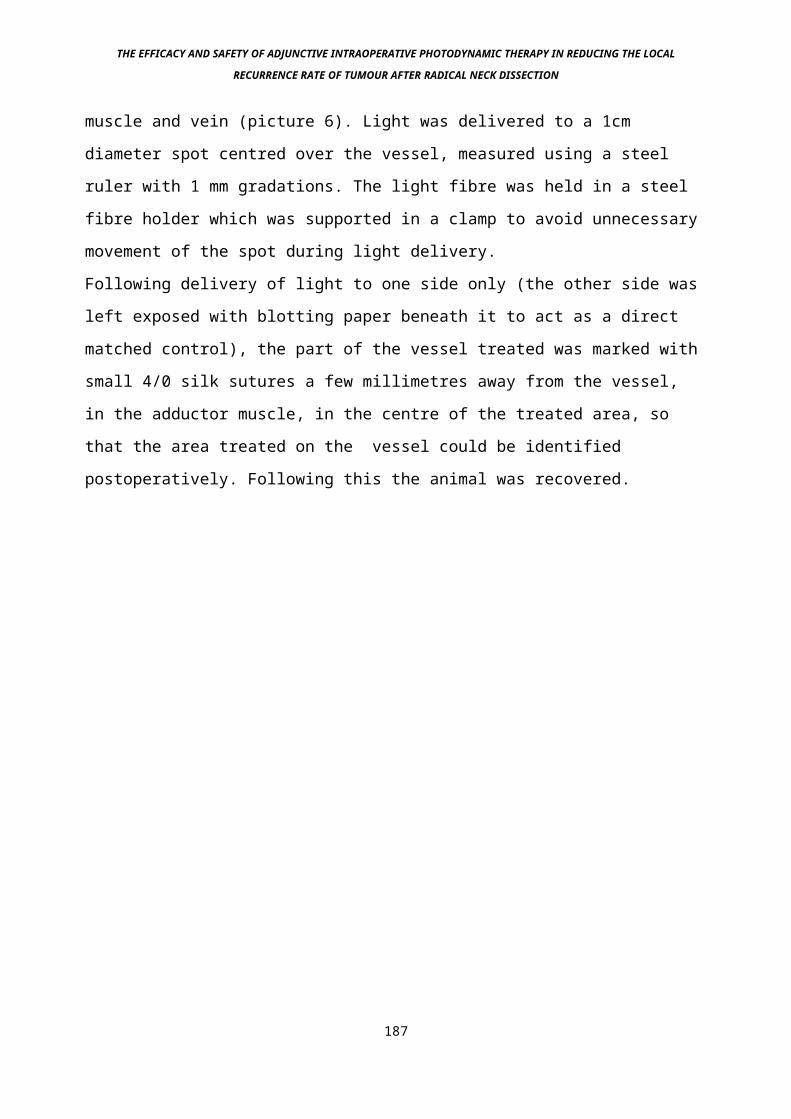
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
muscle and vein (picture 6). Light was delivered to a 1cm
diameter spot centred over the vessel, measured using a steel
ruler with 1 mm gradations. The light fibre was held in a steel
fibre holder which was supported in a clamp to avoid unnecessary
movement of the spot during light delivery.
Following delivery of light to one side only (the other side was
left exposed with blotting paper beneath it to act as a direct
matched control), the part of the vessel treated was marked with
small 4/0 silk sutures a few millimetres away from the vessel,
in the adductor muscle, in the centre of the treated area, so
that the area treated on the vessel could be identified
postoperatively. Following this the animal was recovered.
187
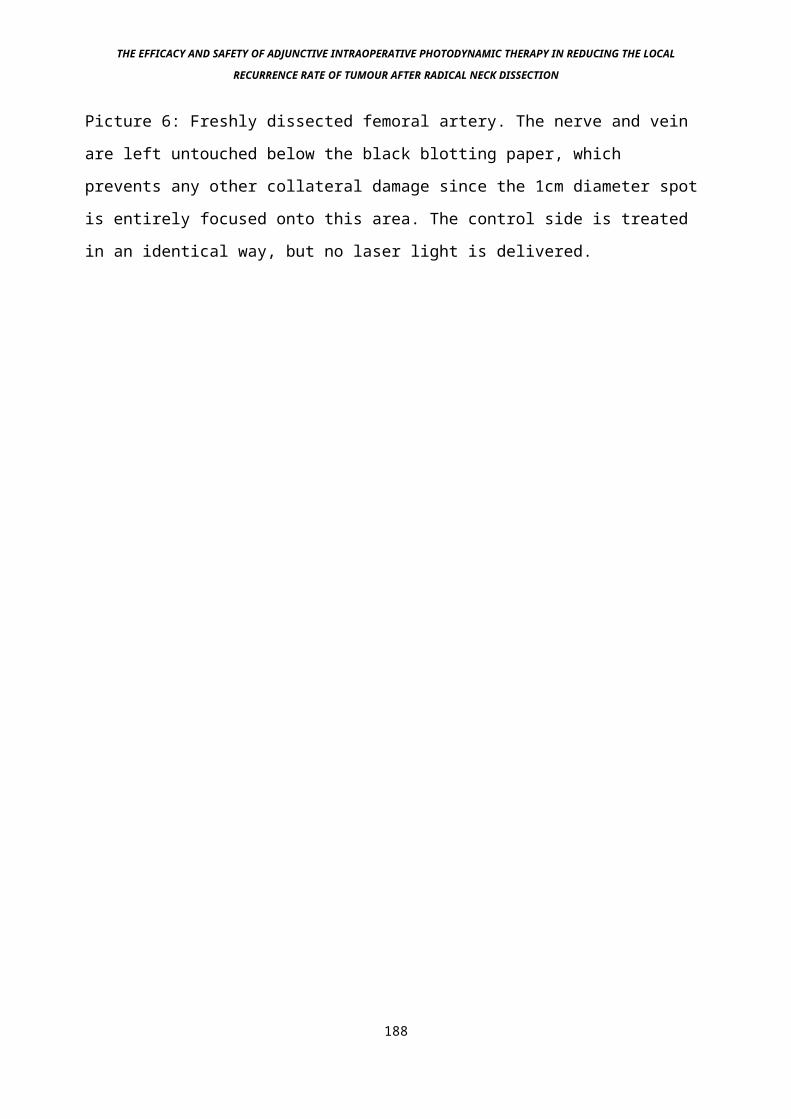
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Picture 6: Freshly dissected femoral artery. The nerve and vein
are left untouched below the black blotting paper, which
prevents any other collateral damage since the 1cm diameter spot
is entirely focused onto this area. The control side is treated
in an identical way, but no laser light is delivered.
188
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
11e: Vessel Analysis
After a time period of either 3 days, 14 days or 3 months from
treatment, the animals were given a further general anaesthetic.
The chest was opened via a thoraco-abdominal incision, and the
left ventricle of the heart identified. This was punctured using
a 23 gauge needle, and a standard sized cannula with a bulbous
tip was inserted into the ascending aorta. This was secured with
a silk tie placed below the bulbous tip (picture 7). Normal
saline at normal adult rat physiological pressure was then
perfused into the animal, drainage being obtained by an incision
into the right atrium of the heart. The reason for this was to
wash blood out of the system prior to perfusion, again at
physiological pressures, overnight with formol-saline to fix the
femoral arteries in their normal state. This allowed realistic
measurement of vessel lumen diameter and wall thickness.
Following overnight perfusion the femoral areas were dissected
and the femoral arteries removed, on the treated side a 2cm
length of vessel 1cm above and below the marking sutures was
taken (Picture 8). These were then mounted in paraffin blocks,
and cut using a microtome. The resultant slides were stained
with Haematoxylin and Eosin. Using a microscope fitted with a
CCD camera, images of the vessels were captured and measured on
a monitor using a Magiscanner. Three outside circumferences were
measured: lumen, media and adventitia (Picture 9). On each
animal analysed, there was control data from the contralateral
superficial femoral artery, with the ipsilateral side providing
data on PDT effects.189
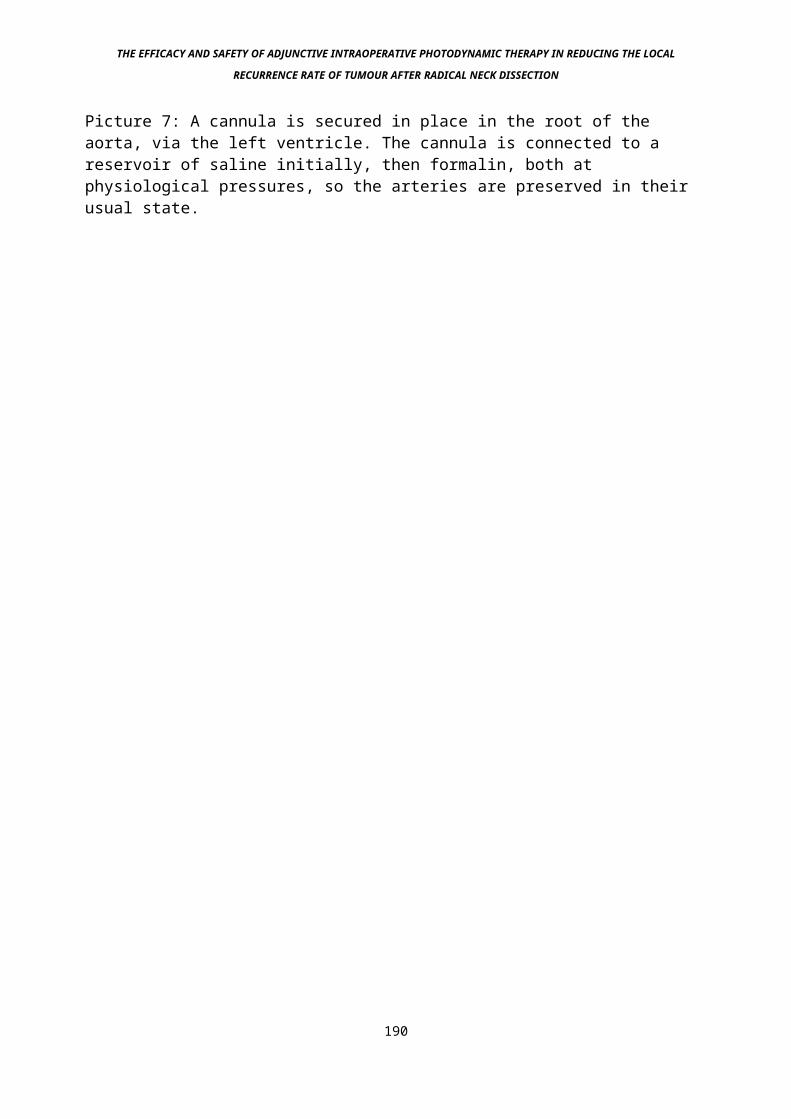
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Picture 7: A cannula is secured in place in the root of the aorta, via the left ventricle. The cannula is connected to a reservoir of saline initially, then formalin, both at physiological pressures, so the arteries are preserved in their usual state.
190
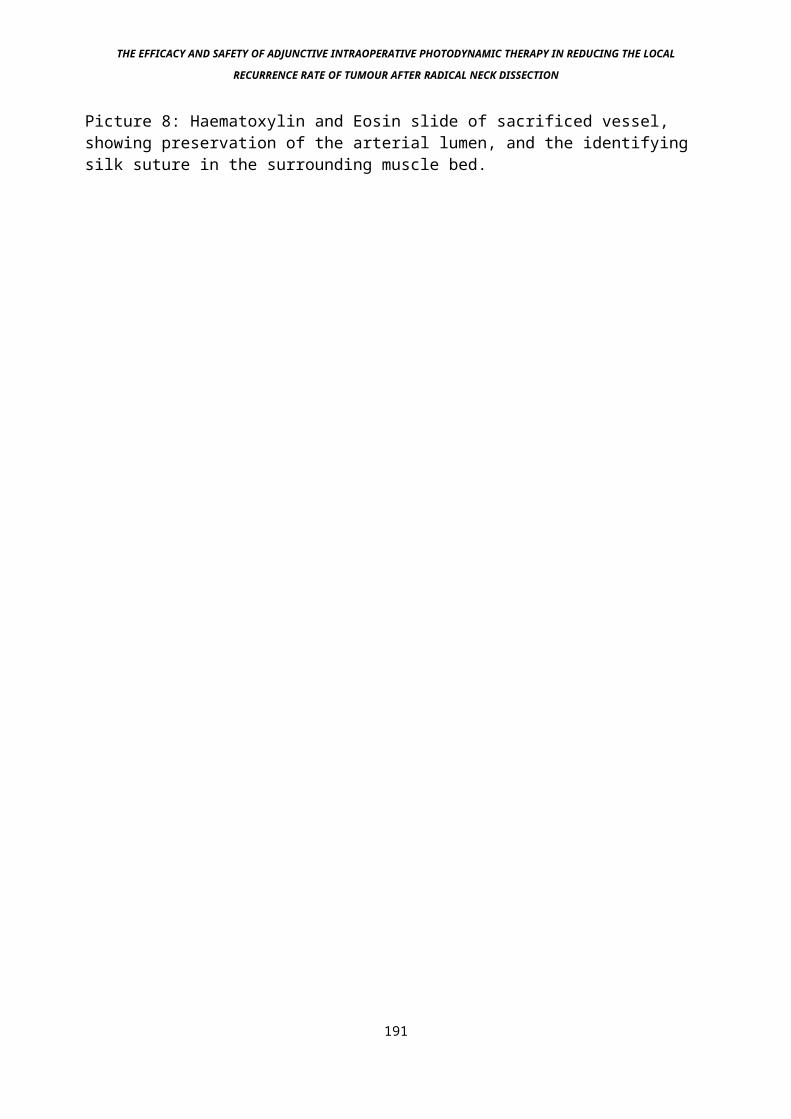
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Picture 8: Haematoxylin and Eosin slide of sacrificed vessel, showing preservation of the arterial lumen, and the identifying silk suture in the surrounding muscle bed.
191

THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Picture 9: Lines drawn around the areas to be measured with the magiscanner. From the calculated area (A- lumen, B- media, C - adventitia), the radii can be determined, and by subtraction, the average width of the three areas determined.
192
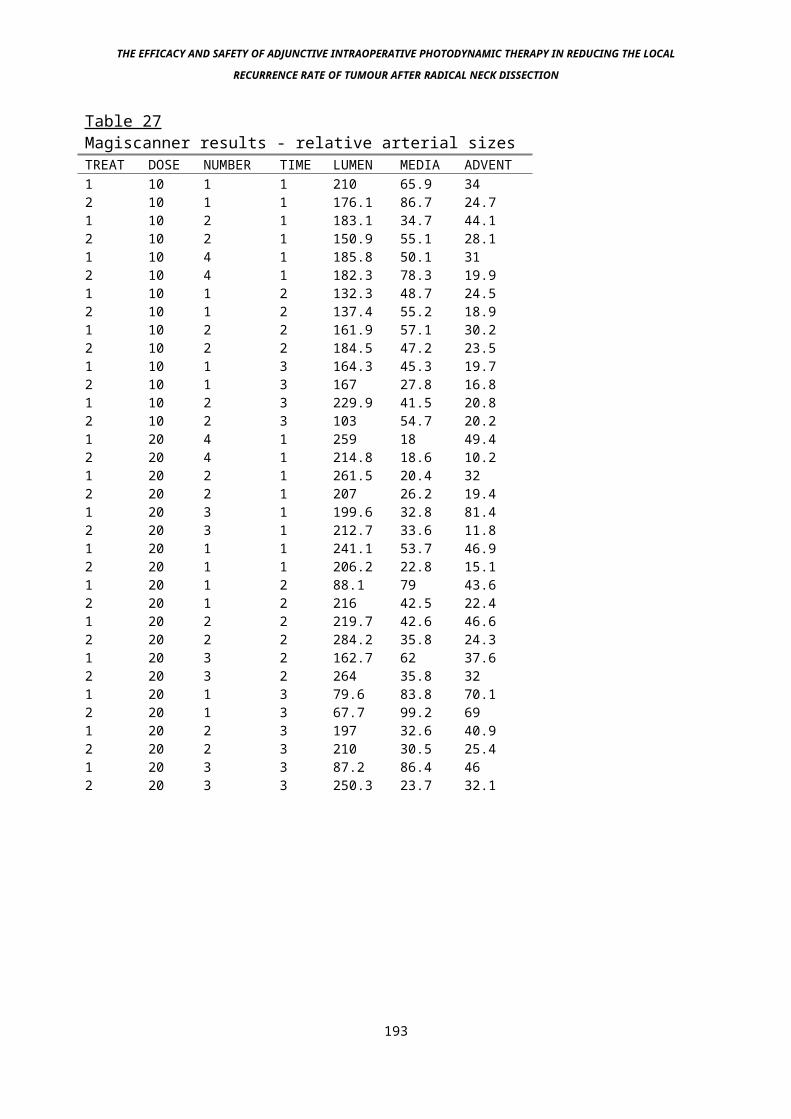
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Table 27Magiscanner results - relative arterial sizes TREAT DOSE NUMBER TIME LUMEN MEDIA ADVENT1 10 1 1 210 65.9 342 10 1 1 176.1 86.7 24.71 10 2 1 183.1 34.7 44.12 10 2 1 150.9 55.1 28.11 10 4 1 185.8 50.1 312 10 4 1 182.3 78.3 19.91 10 1 2 132.3 48.7 24.52 10 1 2 137.4 55.2 18.91 10 2 2 161.9 57.1 30.22 10 2 2 184.5 47.2 23.51 10 1 3 164.3 45.3 19.72 10 1 3 167 27.8 16.81 10 2 3 229.9 41.5 20.82 10 2 3 103 54.7 20.21 20 4 1 259 18 49.42 20 4 1 214.8 18.6 10.21 20 2 1 261.5 20.4 322 20 2 1 207 26.2 19.41 20 3 1 199.6 32.8 81.42 20 3 1 212.7 33.6 11.81 20 1 1 241.1 53.7 46.92 20 1 1 206.2 22.8 15.11 20 1 2 88.1 79 43.62 20 1 2 216 42.5 22.41 20 2 2 219.7 42.6 46.62 20 2 2 284.2 35.8 24.31 20 3 2 162.7 62 37.62 20 3 2 264 35.8 321 20 1 3 79.6 83.8 70.12 20 1 3 67.7 99.2 691 20 2 3 197 32.6 40.92 20 2 3 210 30.5 25.41 20 3 3 87.2 86.4 462 20 3 3 250.3 23.7 32.1
193
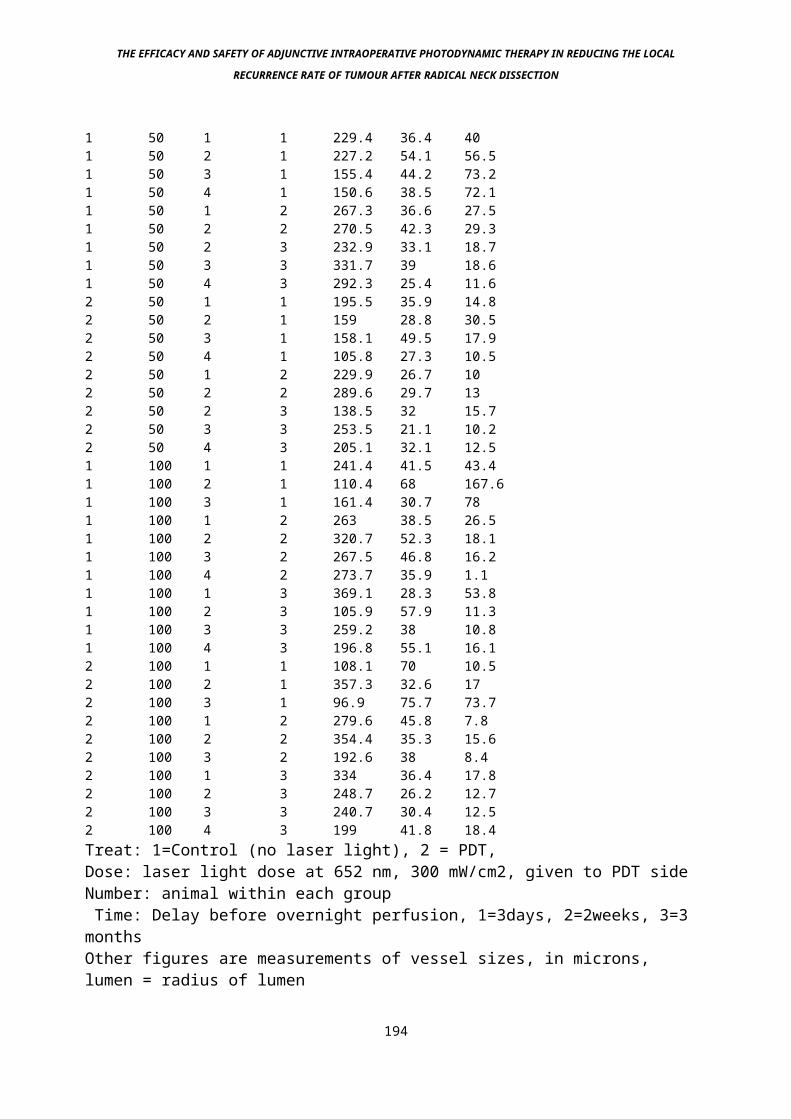
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
1 50 1 1 229.4 36.4 401 50 2 1 227.2 54.1 56.51 50 3 1 155.4 44.2 73.21 50 4 1 150.6 38.5 72.11 50 1 2 267.3 36.6 27.51 50 2 2 270.5 42.3 29.31 50 2 3 232.9 33.1 18.71 50 3 3 331.7 39 18.61 50 4 3 292.3 25.4 11.62 50 1 1 195.5 35.9 14.82 50 2 1 159 28.8 30.52 50 3 1 158.1 49.5 17.92 50 4 1 105.8 27.3 10.52 50 1 2 229.9 26.7 102 50 2 2 289.6 29.7 132 50 2 3 138.5 32 15.72 50 3 3 253.5 21.1 10.22 50 4 3 205.1 32.1 12.51 100 1 1 241.4 41.5 43.41 100 2 1 110.4 68 167.61 100 3 1 161.4 30.7 781 100 1 2 263 38.5 26.51 100 2 2 320.7 52.3 18.11 100 3 2 267.5 46.8 16.21 100 4 2 273.7 35.9 1.11 100 1 3 369.1 28.3 53.81 100 2 3 105.9 57.9 11.31 100 3 3 259.2 38 10.81 100 4 3 196.8 55.1 16.12 100 1 1 108.1 70 10.52 100 2 1 357.3 32.6 172 100 3 1 96.9 75.7 73.72 100 1 2 279.6 45.8 7.82 100 2 2 354.4 35.3 15.62 100 3 2 192.6 38 8.42 100 1 3 334 36.4 17.82 100 2 3 248.7 26.2 12.72 100 3 3 240.7 30.4 12.52 100 4 3 199 41.8 18.4Treat: 1=Control (no laser light), 2 = PDT,Dose: laser light dose at 652 nm, 300 mW/cm2, given to PDT sideNumber: animal within each group Time: Delay before overnight perfusion, 1=3days, 2=2weeks, 3=3 monthsOther figures are measurements of vessel sizes, in microns, lumen = radius of lumen
194
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Other non-sensitised controls (mTHPC diluent only) compared laser light at 500 J/cm 2 , 300 mW/cm 2 on one side, with no laser on the other. No significant differences were seen on Magiscanner analysis.
195
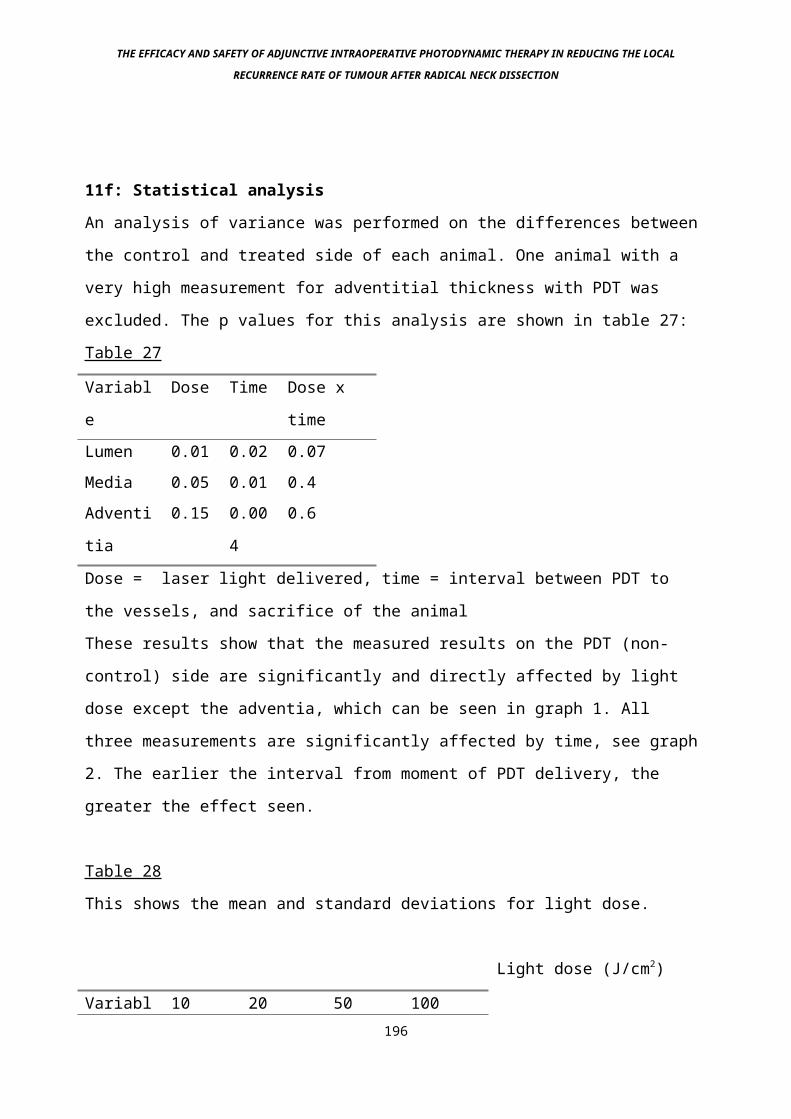
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
11f: Statistical analysis
An analysis of variance was performed on the differences between
the control and treated side of each animal. One animal with a
very high measurement for adventitial thickness with PDT was
excluded. The p values for this analysis are shown in table 27:
Table 27
Variabl
e
Dose Time Dose x
timeLumen 0.01 0.02 0.07Media 0.05 0.01 0.4Adventi
tia
0.15 0.00
4
0.6
Dose = laser light delivered, time = interval between PDT to
the vessels, and sacrifice of the animal
These results show that the measured results on the PDT (non-
control) side are significantly and directly affected by light
dose except the adventia, which can be seen in graph 1. All
three measurements are significantly affected by time, see graph
2. The earlier the interval from moment of PDT delivery, the
greater the effect seen.
Table 28
This shows the mean and standard deviations for light dose.
Light dose (J/cm2)
Variabl 10 20 50 100 196
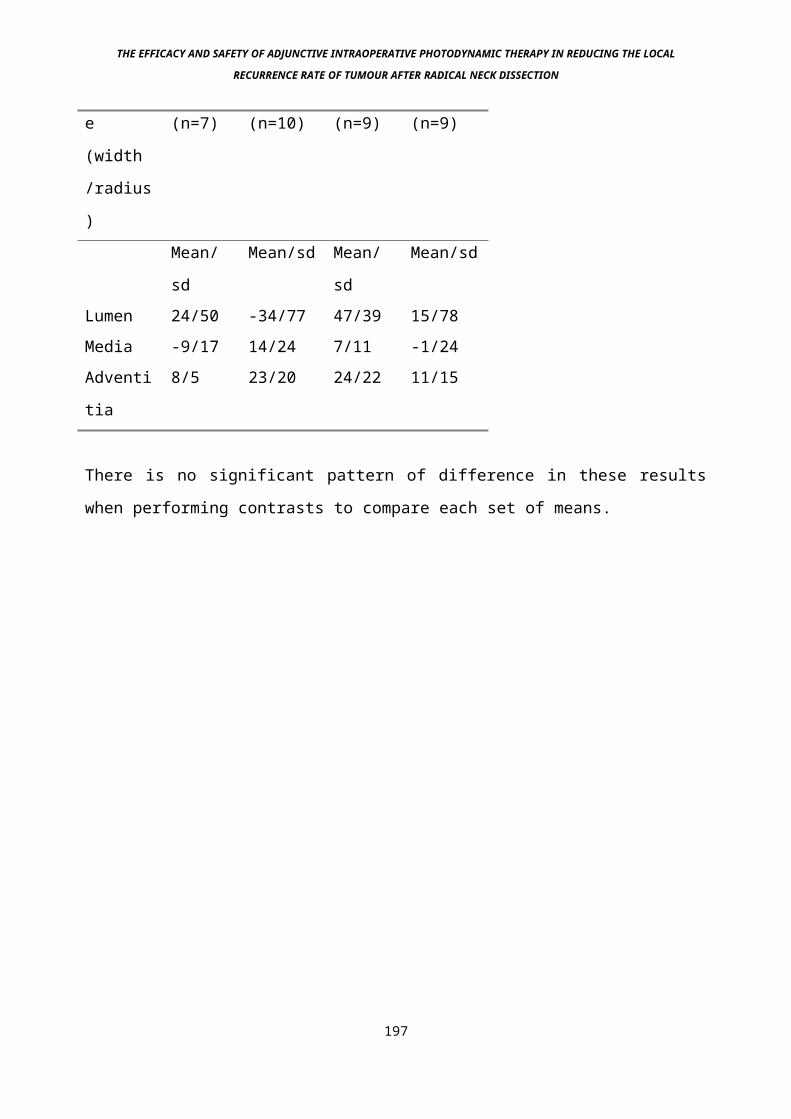
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
e
(width
/radius
)
(n=7) (n=10) (n=9) (n=9)
Mean/
sd
Mean/sd Mean/
sd
Mean/sd
Lumen 24/50 -34/77 47/39 15/78Media -9/17 14/24 7/11 -1/24Adventi
tia
8/5 23/20 24/22 11/15
There is no significant pattern of difference in these results
when performing contrasts to compare each set of means.
197
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
11g: Discussion
The main significant finding is that of substantial adventitial
oedema occurring in all the treatment groups 3 days after PDT,
when compared to the contralateral (control) side (Picture 10),
but no further significant damage to the media or intima. By the
time 2 weeks have passed this oedema is no longer present. Long
term stricture formation or dilatation of the treated vessel was
not noted 3 months post treatment, at which stage it would be
noticeable if present. This indicates that 96 hours post injection
of mTHPC, there is an insignificant amount of drug in the vessel
wall or endothelium, but still enough in the adventitia to cause
an effect, or that the endothelium and media are resistant to the
effects of PDT, a finding that has not been shown by those looking
specifically at this area (Sobeh M., pers. comm.). The fact that
no decrease in the vessel lumen size occurred in conjunction with
this is encouraging, since flow through the vessel should
therefore be maintained. The lack of endothelial damage is in
contrast to a similar study using different photosensitising
drugs, 5-Aminolaevulinic acid and aluminium phthalocyanine (Grant
et al 1994) . In this case almost total loss of endothelium was
seen in the early phase of the study, although full regeneration
eventually occurred, with no apparent adverse effects of this
damage, in particular no evidence of intravascular coagulation.
Total loss of all cells in the vessel wall also occurred in a
separate experiment (Dilkes M.G., unpublished data, see Picture
11) using Photofrin 2 20mg/kg, DLI 24 hours, light dose 100
J/cm2@100mW/cm2, with the control sides being unaffected, a major
factor in deciding which photosensitising drug to use in this198
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
series of experiments. Other studies have also looked at PDT for
the treatment of intravascular lesions, in particular atheroma
(Hsiang et al 1994) and neointimal hyperplasia (Nyamekye et al
1996). In both of these studies, light was delivered via the
endoluminal route in order to treat lesions of the vessel wall.
The results achieved were not particularly promising, which is
surprising since it is well known that vessel endothelium is the
site of at least part of the photodynamic effect, at least in
tumours (Henderson et al 1985). It may be that in these situations
the timing of the drug-light interval (DLI) is critical,
explaining the lack of damage seen in our study, although raising
questions therefore as to the potential efficacy of the treatment
if the microvascular effect has been lost. However, in over 100
clinical cases treated with mTHPC at a DLI of 96 hours as in this
experiment, excellent results have been seen in terms of tumour
response (Stewart J.C.M. 1996). It may be that with mTHPC the
vascular effect is of little consequence, tumour necrosis relying
much more on direct cell toxicity. Further studies looking at the
mechanical integrity of vessels following PDT showed that despite
full-thickness cell death (Orteu et al 1992), resistance to
bursting pressures was unaffected when compared to the control
side (Grant et al 1995).
Picture 10: Obvious damage is seen in the adventitial layer, but
no inflammation in the vessel wall, no endothelial damage, and no
relative compression of the lumen.
199
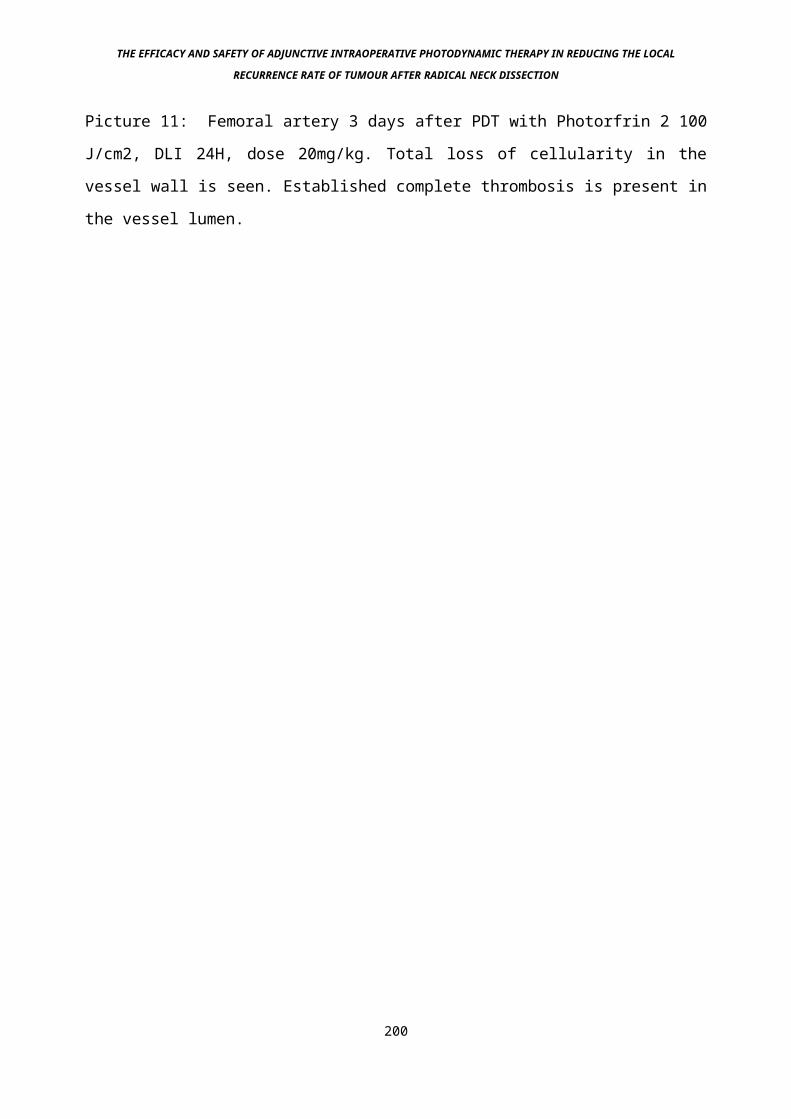
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Picture 11: Femoral artery 3 days after PDT with Photorfrin 2 100
J/cm2, DLI 24H, dose 20mg/kg. Total loss of cellularity in the
vessel wall is seen. Established complete thrombosis is present in
the vessel lumen.
200
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
This is presumably due to maintenance of the strength and function
of collagen in the vessel wall, a finding that has also been seen
in colonic mucosa (Barr et al 1987), and it is probably this
property that is the main cause of the much enhanced healing and
retention of function seen in clinical cases treated with PDT
(Poate et al 1996), an intact collagen matrix allowing the rapid
ingrowth and seeding of normal cells into the space vacated by
the tumour cells, which degenerate in a fashion somewhat
mimicking apoptosis (Agarwal et al 1991).
Studies into the clinical effect of PDT on coronary arteries using
another photosensitiser, Dihaematoporphyrin Ether showed that at
high light doses (>200J/cm2 ) 4/7 treated animals died within 48
hours, and again significant medial damage occurred. This study
also reported adventitial injury, although the exact nature of
this was unclear (Mackie et al 1991).
One reason for the lack of clinically significant damage in our
experiment could be explained by the fact that the drug was
inactive, or the laser incorrectly set-up. However, the fact that
obvious adventitial damage occurred (a definite photodynamic
effect as compared to the other side) means this cannot be so,
true selectivity has occurred between intima/media, and adventia.
The finding of significant adventitial oedema 3 days post
treatment is also interesting because the amount of damage shows a
direct relationship with the amount of light in J/cm2 delivered.
Although on the face of it this is not surprising, recent data
(M.L.DeJode et al 1996) looking at depth of necrosis in a liver
model, showed a plateau-ing of effect at around 40J/cm2, all
other parameters being the same as in this study. In this case201
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
there is a big jump in effect between 50J/cm2 and 100 J/cm2,
although if one very large result in both the treatment and
control groups in one animal is excluded, the trend is much less
pronounced, and in keeping with this other data that suggests the
plateau for effect is around 20 – 40 J/cm2. The difference in
level of plateau may also be due to different optical properties
of the tissues treated (vessels in this study, liver in the deJode
study).
The lack of damage in animals treated with light only, no drug,
demonstrates 2 points. One is that red light at 652 nm does not
have any directly negative effect on the vessels at this
intensity, the other is that the intensity of light used,
300mW/cm2, does not have any damaging thermal effect when surface
irradiance occurs even up to 500J/cm2 total light dose. This has
been confirmed using a microthermocouple by us (Dilkes et al
unpublished data) and others (Abramson et al 1990). Although some
photosensitising drugs have been shown to affect the intimal layer
of vessels without light activation (Coates et al 1996), no
significant change in the intima was seen in any part of the
study.
The use of ex-breeding adult rats was favourable because these
animals were fully mature - therefore any change in vessel size
over 3 months would not be due to growth of the animal.
202
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
11h: Conclusion
No significant damage has been seen in this experiment that might
be deleterious to the patient in a clinical situation. This is
relevant because the photodynamic therapy parameters in this
situation are the same as the parameters currently used for the
treatment of clinical tumours (Dilkes and DeJode 1994). Before
clinical trials on AIOPDT with mTHPC however, more data was needed
regarding the effects of PDT on vessels during PDT and
immediately after. This is because the first time point studied in
this case is 3 days, at which stage severe spasm may have
corrected, and thrombus in the vessel may have dispersed - if that
happens however, the short term effect of this on the carotid
artery for example would be disastrous. Also, data is needed
regarding the effects of PDT on larger vessels, although the
larger the vessel the less likely severe damage will be, since the
opposite side of the vessel to the incident surface will be that
much further away from the light, so intensity will be reduced.
203
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
12: Experiment 4: Acute phase effects of PDT on arteries and
veins
12a: Description
Adjunctive intraoperative photodynamic therapy is being
investigated for use in Head and Neck cancer. Although this and
previous studies have looked at the effects of PDT on vessels
that might be in the AIOPDT site, no study has looked at the
immediate effects of PDT on vessel flow, which has real clinical
significance. We have used an ultrasonic doppler probe to
investigate this problem in rats during and immediately after
PDT, and find no significant changes in arterial flow, but
significant reductions in venous flow rate, particularly in the
external jugular vein which goes into long term spasm.
Our main aim was to look at the role of AIOPDT on reducing the
local recurrence of tumours following radical neck dissection
for secondary spread of Head and Neck cancer. Structures in the
bed of this operation include the carotid arterial tree, and the
jugular vein if a conservative approach is used (Bocca et al
1975). There is currently no good data on the effect of PDT in
the short term, during and immediately after treatment. This is
of great importance clinically, since vessels may go into spasm
or thrombose during PDT, only to have returned to normal or
recanalised 3 days hence. During that period if major vessels
are occluded, serious and irreversible damage may have occurred
204
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
to the area supplied by that vessel. In the case of the carotid
tree, this could mean infarction of a large part of the brain.
12b: Chemical
The drug mTHPC was obtained form Scotia Pharmaceuticals,
Guildford, Surrey, U.K. as a gift. It was supplied as dry,
sterile powder of 99.7% purity. When administered it was
dissolved fresh (within 1 hour) in its diluent, to make up a
concentration of 0.5 mg/ml. Adult female ex-breeder Wistar rats
were obtained from Charles River Ltd. Drug was administered
intravenously via the tail vein using a standard restraining
device by experienced staff. 1.0 mg/kg body weight was given in
all cases except the light-only controls. Once the animals had
been photosensitised, they were kept out of direct contact with
light, in darkened conditions.
12c: Measurement of flow
The method of blood flow measurement chosen was with a
Transonic flowprobe (Linton Instruments, Stowmarket, Suffolk,
U.K.). This device uses two ultrasonic transducers pointing at a
fixed acoustic reflector (see figure 3), The time taken for
ultrasonic waves to pass between the two transducers is
measured, giving an accurate measure of transit time - which is
affected by the rate of flow in the vessel. By a subtraction
technique of integrated transit times the final measurement is
in volume of flow rather than velocity (Drost C.J. 1978). Using
a selection of flow probes it is possible to measure flow rate 205
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
in a number of different vessels. The Transonic Flowprobe and
meter was obtained on free long term loan from Linton
Instruments.
206

THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Figure 3
207
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
12d: Experimental technique
General anaesthesia was induced using the standard
intraperitoneal injection of a mixture of Hypnorm and Midazolam.
Because it was felt that depth of anaesthesia would directly
influence flow through vessels independent of any other
variables such as PDT, a steady state of anaesthesia was
desirable. This was achieved using an intravenous cannula placed
in the tail vein, attached to a syringe pump delivering a
continuous flow of Hypnorm and Midazolam.
The vessels to be examined were exposed using standard surgical
approaches (Picture 12). Magnifying surgical loupes and
microsurgical instruments were used to delicately free the
vessels from surrounding structures. Using a series of retort
stands and clamps the flowprobe was held in position around the
vessel, aqueous gel being used as the transmission medium (see
picture 13). Laser light at 652 nm wavelength was obtained from
a copper vapour laser pumping a Rhodamine dye laser (Cu15,
Oxford Lasers, Abingdon Rd., Oxford, U.K.), 100 mW/cm2
intensity, using a 1 cm diameter spot delivered via a
microlens. The vessel being in the middle of the spot in all
cases, the light fibre being held in a metal fibre-holder,
gripped again by clamps from a retort stand. With veins the
laser light was delivered distal to the probe, with arteries the
laser light was delivered proximally (with respect to the
heart).
Flow of blood through the vessels was recorded using a
continuous XY recorder (see picture 14) for a period of 5 208
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
minutes pre light delivery (baseline) and 15 minutes post light
delivery. Although the clinical dose of light was only 20 joules
per square centimetre (J/cm2), a total dose up to 250 J/cm2 was
given, in a continuous manner, to thoroughly evaluate any
changes induced at higher light doses.
209
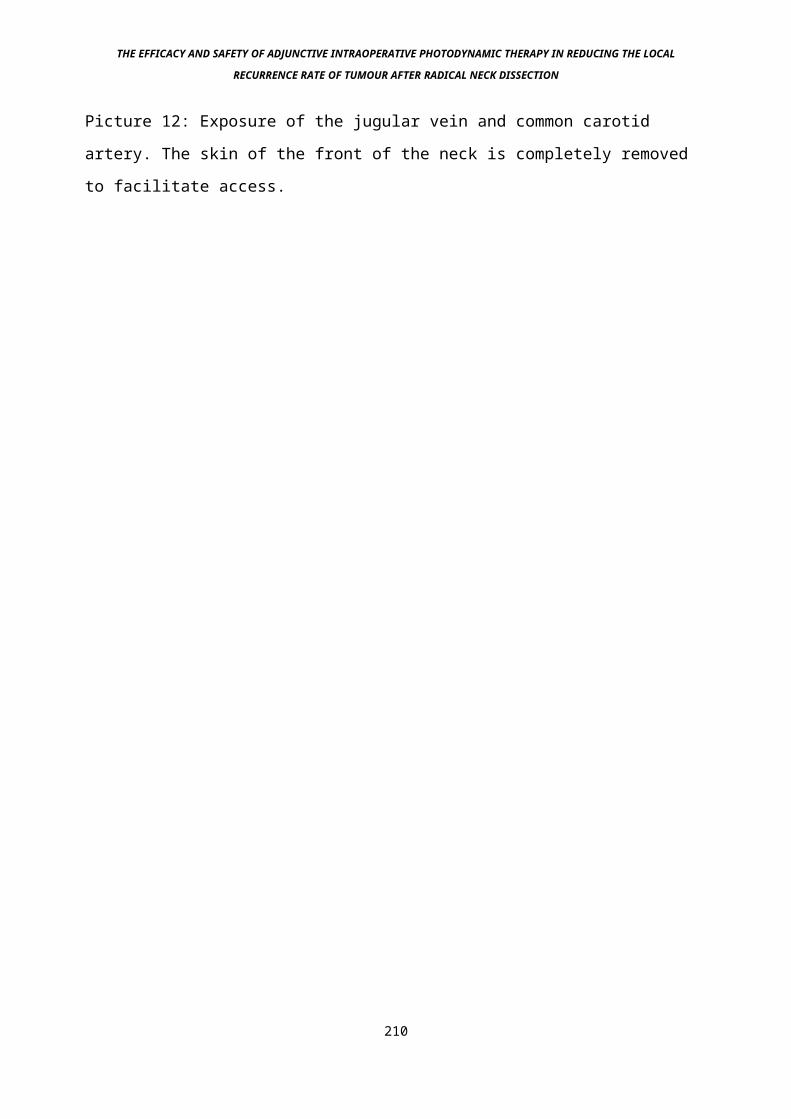
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Picture 12: Exposure of the jugular vein and common carotid
artery. The skin of the front of the neck is completely removed
to facilitate access.
210

THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Picture 13: Typical set-up during doppler flow measurements
211
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Only one vessel was examined per animal. When cases of vessel
spasm occurred, the vessel was bathed in Praxiline 10mg (0.5 ml
of 20mg/ml solution) to try to reverse this.
The following vessels were assessed: Jugular vein, common
carotid artery, abdominal aorta, common iliac artery and vein,
femoral artery and vein. Two of each vessel were measured with
PDT except in the case of the external jugular vein, in which 4
vessels were tested. One of each vessel was a control, except
with the external jugular vein in which there were 2 controls.
12e: Results
All animals tolerated the procedure successfully. The experiment
was sometimes dogged by air bubbles appearing in the gel around
the vessel, and satisfactory readings were not always possible,
despite the best efforts (Picture 14). The results obtained are
shown in graphs 3 and 4. They show that arteries do not appear
to be significantly affected by PDT when delivered in this
manner, but veins, and in particular the internal jugular vein,
do have a significant reduction in blood flow that is sustained
throughout the period of observation. Acute and irreversible
vessel spasm as occurred in the jugular veins was not helped by
Praxiline administration topically. It was not possible to get
accurate readings of aortic flow rate, probably because our flow
probe was too small to fit around the vessel. No significant
changes in flow occurred in any of the control animals.
212
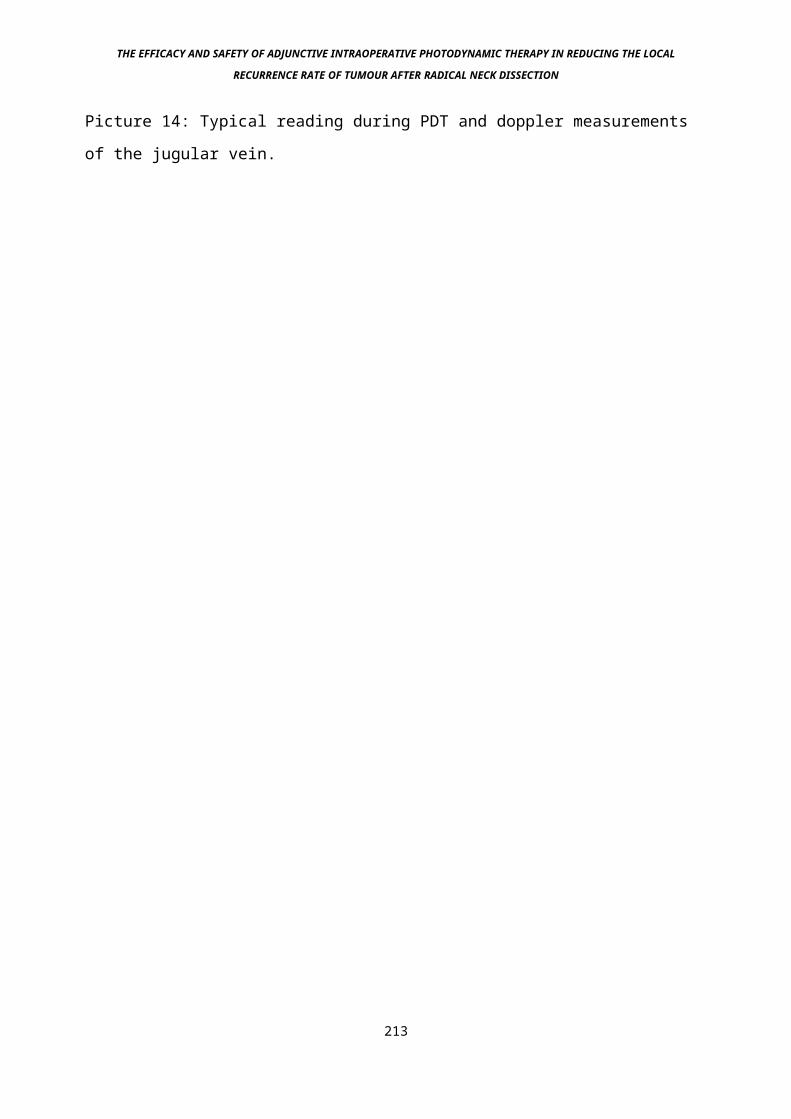
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Picture 14: Typical reading during PDT and doppler measurements
of the jugular vein.
213
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
12e: Discussion
The most striking result obtained was virtually complete
cessation of flow in the jugular veins tested in the PDT groups
(Graph 4). At the time of the procedure the vein was seen to go
into spasm which did not reverse during the entire procedure or
for 15 minutes after. The jugular vein is a structure noted for
its propensity to spasm, even with simple instrumentation, but
this was not seen in the control groups tested. More of these
vessels were studied because no major change in flow was seen in
any of the other vessels treated, although all the veins treated
did show some moderate reduction in flow rate. The use of
Praxilene, a powerful vasodilator which works topically did not
help. This finding has potentially major implications regarding
the role of AIOPDT in Head and Neck surgery, although not with
respect to the operation of radical neck dissection, where
temporary loss of a preserved internal jugular vein is of little
importance, unless perhaps the contralateral vein has already
been taken, or bilateral AIOPDT is planned. In this case there
may be a rise in intracranial pressure with potentially serious
side effects (Jones R.K. 1951, Marks et al 1990). However, the
size of the internal jugular vein in its normal state in the
adult human is much larger than that of a rat, and it is
possible that because of this only one half of the vessel wall,
on the irradiated surface side, will be stimulated by the PDT,
since significantly less light will pass through to the other
side, which is often separated from the lateral side by a lumen
of 1.75cm diameter filled with deoxygenated blood (Doktor et al 214
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
1996). However, in this case only a 1cm length of vessel was
treated, whereas in the clinical situation the entire length of
the internal jugular vein would be irradiated, some 15-20 cm.
The planned clinical light dose for AIOPDT would be the same as
that used in experiment 2, and in the treatment of early Head
and Neck cancer (Dilkes and DeJode, 1994), because since this is
effective in necrosing solid, visible tumours, it is assumed it
will also work on microscopic tumour residue. The light dose in
this situation is 20 J/cm2, at which stage little of the effect
had set in regarding spasm. From an initial average flow rate of
3.4 ml/minute, by the time 20 J/cm2 had been given, the average
flow had dropped to 2.7 ml/min, a 19% fall, which would not be
significant clinically. We did not wait however, after giving
the 20J/cm2 to see if further spasm occurred, although since
spasm occurs because of an irritative stimulus, we assume that
this is a linear, accumulative relationship, rather than due to
any possibly delayed effect.
215

THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Graph 3: CIV = Common iliac vein, CFA = Common femoral artery,
CIA = Common iliac artery, CCA = Common carotid artery.
216

THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Graph 4: IJV = Internal jugular vein.
217
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
The effect of PDT on veins might however be important in AIOPDT
for other Head and Neck operations. These would be operations
where vascularised free flaps of tissue are re-anastomosed with
local Head and Neck vessels to fill the holes created by radical
excision of tumours, as occurs increasingly commonly. In this
situation fairly small blood vessels are joined together, some
of only around 2 mm diameter. These would not be protected on
the non-irradiated side by blood, since when the vessels are
anastomosed they are empty, and besides which red light at 652
nm will adequately penetrate 2 mm of blood. Although the veins
and arteries to be anastomosed could be shielded from any laser
light at 652 nm used for the AIOPDT, when they are anastomosed a
microscope with very bright white light is needed to be able to
accurately appose and suture the edges of the vessels. This will
contain significant amounts of light that will activate
photosensitisers, with mTHPC this means blue and middle-far red.
Thus spasm could be induced in the veins of the anastomosis
(usually at least one artery and 2 veins are needed to ensure
survival of the graft), even though the internal jugular vein
would usually not be used for such a procedure. If persistent
venous spasm is induced, the graft will fail, with potentially
serious consequences for the patient.
More encouragingly, the arteries tested were all resistant to
all but minor variations in flow with PDT (Graph 3). In
particular the rat common carotid arteries tested showed no
significant variation in flow at all, up to 240 J/cm2 of light.
The control sides demonstrated that even at a relatively high
fluence rate of 300 mW/cm2, no damage due to heating occurred, 218
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
and it might be beneficial in the clinical situation to use
higher fluence rates to reduce treatment time once more powerful
laser systems are available, although there is some data, as yet
unpublished, to suggest that increased fluence rate decreases
the efficacy of the treatment (DeJode et al, in preparation
1997), presumably due to exhaustion of the oxygen supply for
PDT.
In summary, the ultrasonic flowprobe was a useful way of
measuring acute flow changes in vessels undergoing PDT. The
findings do not preclude clinical investigation of the role of
AIOPDT for the operation of radical neck dissection in which the
internal jugular vein is removed, but do raise questions about
the potential viability of free flaps if AIOPDT is used in other
cancer procedures.
219
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
13: Experiment 5 - The effect of high intensity white and
filtered microscope light on the viability of microvascular
anastomoses in photosensitised rats
13a: Description
The previous experiment has shown potentially serious damage to
small veins undergoing photodynamic therapy. This has
implications when PDT is planned in patients having a
simultaneous microvascular re-anastomosis of vessels during a
vascularised free flap reconstruction in surgery,. This is
because the high intensity white microscope light that is
necessary to illuminate the small vessels so that the very
accurate microscope controlled anastomosis can be created may
contain sufficient amounts of activating light to a damaging
photodynamic effect within the walls of the vessels being
anastomosed (Picture 15).
This is potentially a major problem, particularly in Head and
Neck cancer surgery where the use of microvascular anastomosis
for vascularised free flaps is increasing rapidly. Since the
late 1940’s small vessels anastomoses have been reliably
achieved (Johns T.W.P. 1947), and the procedure of free
microvascular transfer and re-anastomosis of tissue into local
blood supply is now a mainline method of reconstruction for
defects all over the body. This is particularly true in the Head
and Neck area where, following the radical resection of cancer, 220
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
these flaps offer better structure and versatility than
previously used flaps (Soutar et al 1983).
Following the previous experiment it seems that veins in
general and in particular the external jugular veins of the rat
were very sensitive to the effects of photodynamic therapy when
stimulated by red laser light at 652 nm and sensitised with
mTHPC, going into sustained spasm under PDT. The fact that veins
used in microvascular reconstruction are often of fairly small
diameter (like those in the rat) may mean that the brilliant
Xenon light source of operating microscopes might contain
enough activating light to damage venous anastomoses and cause
failure of the blood supply to free flaps, with their resultant
necrosis and high subsequent morbidity and mortality, should a
salivary fistula occur. Immediate excision of the failed graft
and its replacement is standard practice should necrosis occur.
221

THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Picture 15: Rat femoral artery held in an Acland clamp, under
conditions of magnification and brilliant, focused illumination
222
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
This aspect is particularly important when considering the
second generation photosensitising drugs such as mTHPC, which
have very high absorption peaks in the blue spectrum, which the
Xenon arc lamp sources such as the ones used in operating
microscopes tend to produce in significant amounts (see
diagram). They are also very efficient converters of light
energy into chemical energy (Bonnet 1995), so relatively small
amounts of activating light will cause significant amounts of
damage. Time interval between drug injection and light
administration might also be critical, since there is a well
known vascular effect in the first 6-12 hours sfter intravenous
administration of the drug, due to circulating photosensitiser,
and drug being taken up through the vessel wall into the
interstitial spaces. At 96 hours post injection however, minimal
levels of mTHPC are seen in vessels, as shown in experiment 1.
This might mean that anastomoses performed at the early stage
might fail, but those at a later stage might survive.
13b: Plan
The specific output of the Xenon lamp sources of standard
operating microscopes needed to be equated with the absorption
spectrum of the chosen photosensitising drug mTHPC. If
significant levels were found (>5j/cm2 in the red or blue
band)then it would be necessary to assess the viability of
microvascular anastomoses in sensitised and non-sensitised
animals, the non-sensitised group being a control group. All
other parameters would be kept exactly the same.223
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
The work was carried out at the Northwick Park Institute for
Medical Research, Surgical Research laboratories, Watford Road,
Harrow, Middlesex HA1 3UJ, with the assistance of Sandra
Simpkin, Senior Technician.
224
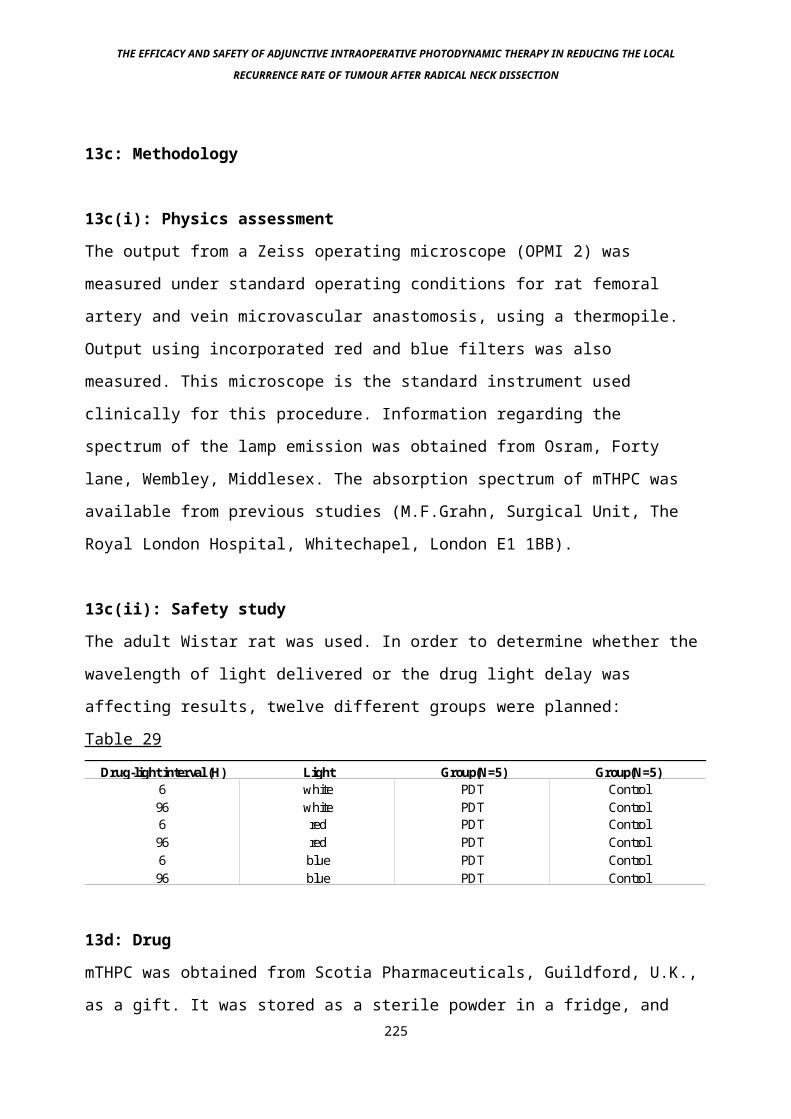
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
13c: Methodology
13c(i): Physics assessment
The output from a Zeiss operating microscope (OPMI 2) was
measured under standard operating conditions for rat femoral
artery and vein microvascular anastomosis, using a thermopile.
Output using incorporated red and blue filters was also
measured. This microscope is the standard instrument used
clinically for this procedure. Information regarding the
spectrum of the lamp emission was obtained from Osram, Forty
lane, Wembley, Middlesex. The absorption spectrum of mTHPC was
available from previous studies (M.F.Grahn, Surgical Unit, The
Royal London Hospital, Whitechapel, London E1 1BB).
13c(ii): Safety study
The adult Wistar rat was used. In order to determine whether the
wavelength of light delivered or the drug light delay was
affecting results, twelve different groups were planned:
Table 29
Drug-light interval (H) Light Group(N=5) Group(N=5)6 white PDT Control96 white PDT Control6 red PDT Control96 red PDT Control6 blue PDT Control96 blue PDT Control
13d: Drug
mTHPC was obtained from Scotia Pharmaceuticals, Guildford, U.K.,
as a gift. It was stored as a sterile powder in a fridge, and 225
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
reconstituted fresh with 1g ethanol and 1g polyethylene glycol
400 made up to 5 ml with sterile water for injection, to make up
a solution of 1.0 mg/ml. When reconstituting the drug for
injection, as usual meticulous attention was taken to ensure
that the drug had gone into solution. Invariably this meant 2 or
3 minutes of vigorous shaking, ensuring no residue was visible
on the bottom of the tube used for reconstitution.
13e: Animals
Male Sprague-Dawley rats in the weight range 450-600 grammes
were obtained from Charles River Ltd. (U.K.) and used
throughout. The experimental groups were given 1 mg/kg mTHPC and
0.5 ml of N-Saline via the lingual vein under Enflurane sedation
either 6H or 96H prior to microvascular anastomosis. The control
groups were given 1.0 ml N-Saline at the same time points. The
operation was performed under Hypnorm (intramuscular) and
Diazepam (intraperitoneal) anaesthesia.
The femoral triangle of the rat was exposed on one side. The
femoral artery and vein was dissected free from underlying
fascia and the profunda vessels were tied and divided.
A piece of plastic backing material was inserted under the
vessels (Picture 15) and a large damp swab was placed over the
surrounding tissue to protect the area from the potential
effects of the microscope light. This was in order to prevent
226
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
unnecessary collateral damage that might mask PDT induced damage
to the microvascular anastomosis, such as oedema, pain etc.
An ultrasonic doppler probe (Linton Instruments, Stowmarket,
Suffolk, U.K.) was used to objectively measure flow through the
vessels at 3 time points: On exposure, immediately post
anastomosis and after 80 minutes of microscope light exposure.
227
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
13f: Operative technique
The vessels were severed and then anastomosed using an ABB-1
Acland approximating clamp and 10/0 Ethilon (Ethicon Ltd)
sutures. Microscope light exposure was for 80 minutes in all
cases. The “white” light used was normal microscope light, “red”
and “blue” light was achieved by using filters set into
microscope filter holders. These were slotted into the
microscope so that the operating field was bathed in the
required light. The filters were RG-630 28mm x 3mm (red) and BG-
25 28mm x 3 mm (blue), both supplied by Schott. After 80 minutes
of light exposure the vessels were assessed for spasm and
patency, and their flow measured using the ultrasonic doppler.
13g: Postoperative assessment
The skin was closed and the animals recovered. Following this
they were closely observed for signs of anastomotic failure, in
particular leg swelling, footpad darkening, limping and general
condition. Close observation of the legs was carried out, in
order to detect any impending vascular insufficiency. Any animal
thought to be in difficulty was killed immediately and the
femoral area exposed to assess the state of the arterial and
venous anastomoses.
One week after the operation, the vessels were exposed and re-
assessed for patency and spasm in the surviving animals. The
flow rate was re-measured. The animals were killed and the
vessels were harvested and preserved in formol saline.,
228
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
13h: Results
Light source: Using the manufacturers data, the integral was
evaluated numerically between 350-720 nm, contributions beyond
these limits being negligible. The wavelength assessed was set
as 652 nm, the normal wavelength for mTHPC excitation. The
calculated value for the activation efficiency was 0.27.
The total focused output of the microscope was measured with the
thermopile as approximately 800 mW. Using a hot mirror to
eliminate infra red emission, the visible output 350-720 nm was
measured as approximately 500 mW.
The spot diameter was 6.8 cm, an area of 36cm2. This gave an
irradiance in the visible spectrum of 14 mW/cm2 of white light.
Typical operating time was set at 80 minutes, giving a total
light dose of 62J/cm2. In terms of photons absorbed (and
therefore photosensitiser activation) this is equivalent to
approximately 17J/cm2 of 652 nm light.
Through the RG630 longpass filter (Schott), the relative
activation of the lamp emission compared to monochromatic light
at 652 nm is 0.23. The power output using this filter was 170
mW, giving a red light dose of 23 J/cm2, equivalent to 5J/cm2 of
monochromatic 652 nm light for the 80 minute exposure.
The blue filtered light using the RG25 bandpass filter (Schott)
gave a relative activation figure of 0.55. The power output in
this spectrum was 30mW/cm2, giving a blue light dose of 4J/cm2
for the 80 minute exposure, equivalent to 2J/cm2 of 652nm red
light in terms of photon absorption. The results are displayed
in Graph 5.229

THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Graph 5
230
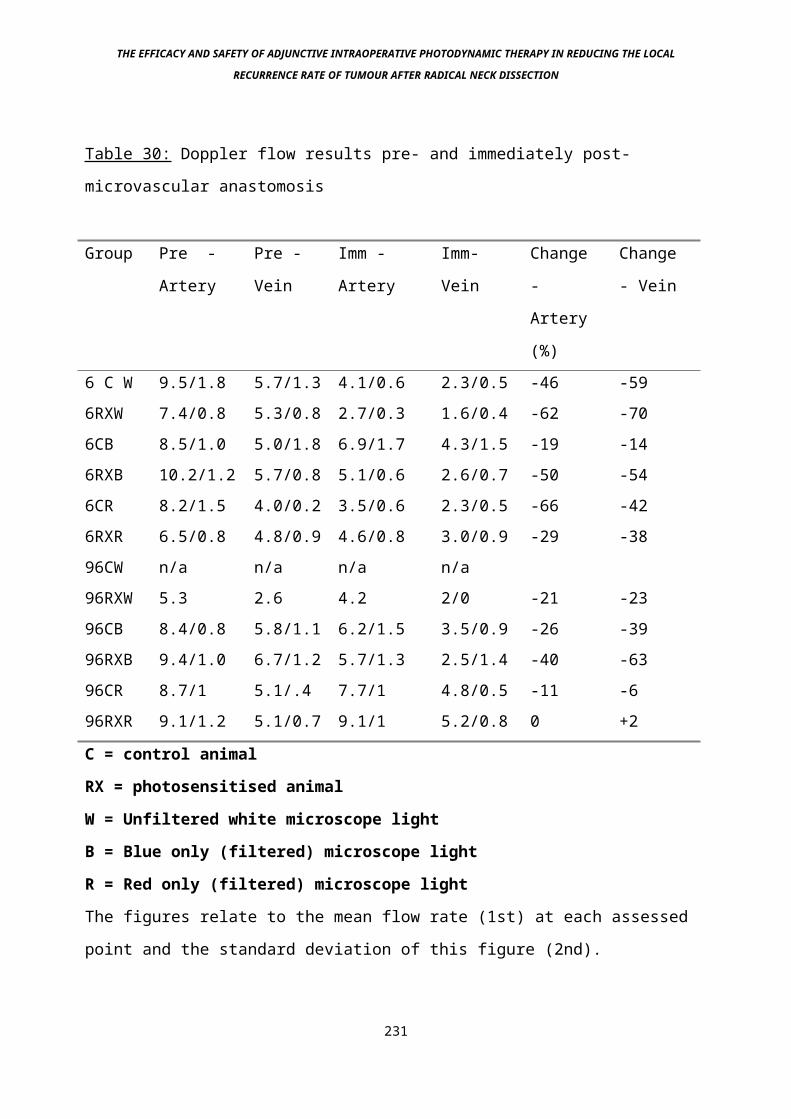
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Table 30: Doppler flow results pre- and immediately post-
microvascular anastomosis
Group Pre -
Artery
Pre -
Vein
Imm -
Artery
Imm-
Vein
Change
-
Artery
(%)
Change
- Vein
6 C W 9.5/1.8 5.7/1.3 4.1/0.6 2.3/0.5 -46 -596RXW 7.4/0.8 5.3/0.8 2.7/0.3 1.6/0.4 -62 -706CB 8.5/1.0 5.0/1.8 6.9/1.7 4.3/1.5 -19 -146RXB 10.2/1.2 5.7/0.8 5.1/0.6 2.6/0.7 -50 -546CR 8.2/1.5 4.0/0.2 3.5/0.6 2.3/0.5 -66 -426RXR 6.5/0.8 4.8/0.9 4.6/0.8 3.0/0.9 -29 -3896CW n/a n/a n/a n/a96RXW 5.3 2.6 4.2 2/0 -21 -2396CB 8.4/0.8 5.8/1.1 6.2/1.5 3.5/0.9 -26 -3996RXB 9.4/1.0 6.7/1.2 5.7/1.3 2.5/1.4 -40 -6396CR 8.7/1 5.1/.4 7.7/1 4.8/0.5 -11 -696RXR 9.1/1.2 5.1/0.7 9.1/1 5.2/0.8 0 +2
C = control animal
RX = photosensitised animal
W = Unfiltered white microscope light
B = Blue only (filtered) microscope light
R = Red only (filtered) microscope light
The figures relate to the mean flow rate (1st) at each assessed
point and the standard deviation of this figure (2nd).
231
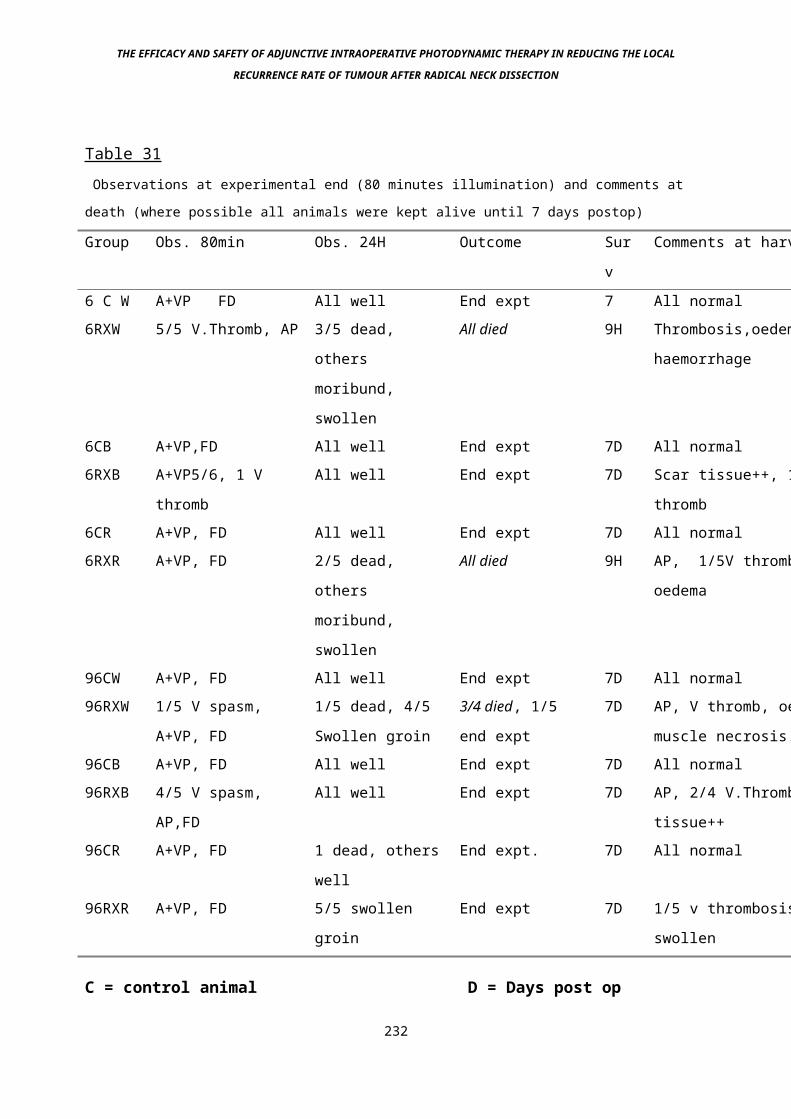
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Table 31 Observations at experimental end (80 minutes illumination) and comments at
death (where possible all animals were kept alive until 7 days postop)
Group Obs. 80min Obs. 24H Outcome Sur
v
Comments at harvest
6 C W A+VP FD All well End expt 7 All normal6RXW 5/5 V.Thromb, AP 3/5 dead,
others
moribund,
swollen
All died 9H Thrombosis,oedema,
haemorrhage
6CB A+VP,FD All well End expt 7D All normal6RXB A+VP5/6, 1 V
thromb
All well End expt 7D Scar tissue++, 1xV
thromb6CR A+VP, FD All well End expt 7D All normal6RXR A+VP, FD 2/5 dead,
others
moribund,
swollen
All died 9H AP, 1/5V thromb,
oedema
96CW A+VP, FD All well End expt 7D All normal96RXW 1/5 V spasm,
A+VP, FD
1/5 dead, 4/5
Swollen groin
3/4 died, 1/5
end expt
7D AP, V thromb, oedema,
muscle necrosis.96CB A+VP, FD All well End expt 7D All normal96RXB 4/5 V spasm,
AP,FD
All well End expt 7D AP, 2/4 V.Thromb, scar
tissue++96CR A+VP, FD 1 dead, others
well
End expt. 7D All normal
96RXR A+VP, FD 5/5 swollen
groin
End expt 7D 1/5 v thrombosis, all
swollen
C = control animal D = Days post op
232
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
RX = photosensitised animal H = Hours post op
W = Unfiltered white microscope light Thromb = Thrombosis
B = Blue only (filtered) microscope light V = vein
P = patent as assessed R = Red only (filtered)
microscope light
A = Artery FD = Fully dilated
233
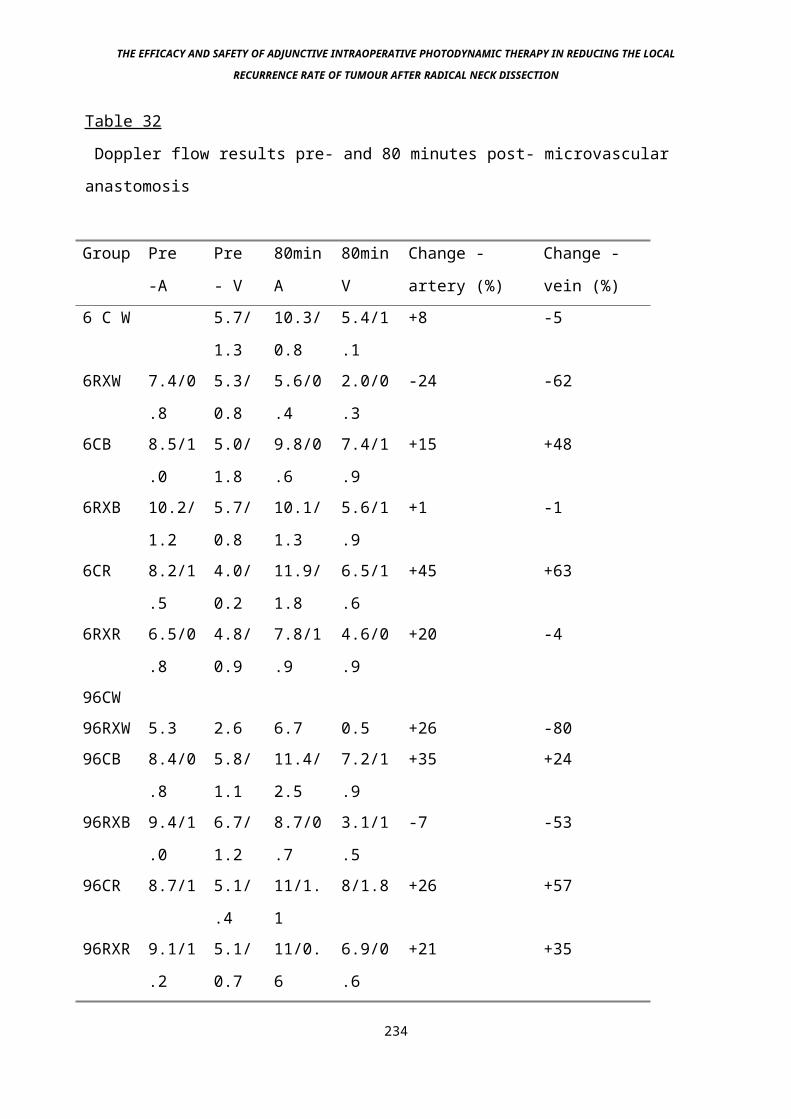
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Table 32
Doppler flow results pre- and 80 minutes post- microvascular
anastomosis
Group Pre
-A
Pre
- V
80min
A
80min
V
Change -
artery (%)
Change -
vein (%)6 C W 5.7/
1.3
10.3/
0.8
5.4/1
.1
+8 -5
6RXW 7.4/0
.8
5.3/
0.8
5.6/0
.4
2.0/0
.3
-24 -62
6CB 8.5/1
.0
5.0/
1.8
9.8/0
.6
7.4/1
.9
+15 +48
6RXB 10.2/
1.2
5.7/
0.8
10.1/
1.3
5.6/1
.9
+1 -1
6CR 8.2/1
.5
4.0/
0.2
11.9/
1.8
6.5/1
.6
+45 +63
6RXR 6.5/0
.8
4.8/
0.9
7.8/1
.9
4.6/0
.9
+20 -4
96CW96RXW 5.3 2.6 6.7 0.5 +26 -8096CB 8.4/0
.8
5.8/
1.1
11.4/
2.5
7.2/1
.9
+35 +24
96RXB 9.4/1
.0
6.7/
1.2
8.7/0
.7
3.1/1
.5
-7 -53
96CR 8.7/1 5.1/
.4
11/1.
1
8/1.8 +26 +57
96RXR 9.1/1
.2
5.1/
0.7
11/0.
6
6.9/0
.6
+21 +35
234
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
C = control animal
RX = photosensitised animal
W = Unfiltered white microscope light
B = Blue only (filtered) microscope light
R = Red only (filtered) microscope light
Numbers are (mean flow)/(standard deviation of results)
235
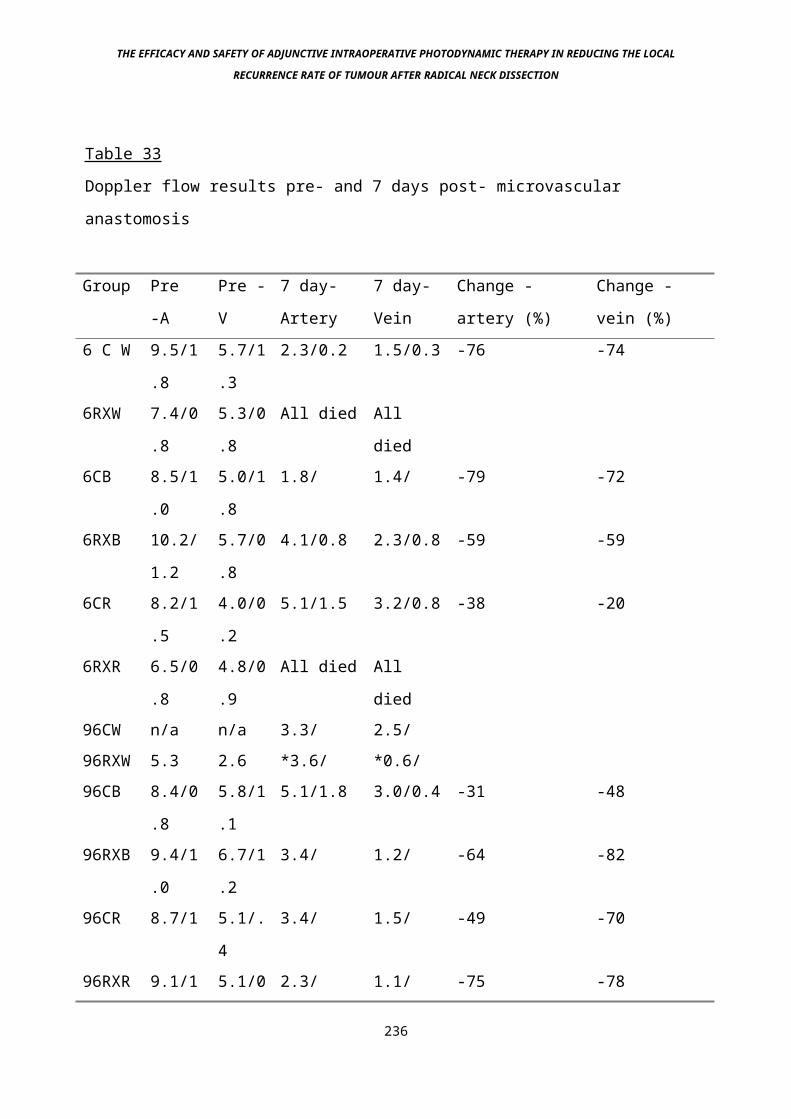
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Table 33
Doppler flow results pre- and 7 days post- microvascular
anastomosis
Group Pre
-A
Pre -
V
7 day-
Artery
7 day-
Vein
Change -
artery (%)
Change -
vein (%)6 C W 9.5/1
.8
5.7/1
.3
2.3/0.2 1.5/0.3 -76 -74
6RXW 7.4/0
.8
5.3/0
.8
All died All
died6CB 8.5/1
.0
5.0/1
.8
1.8/ 1.4/ -79 -72
6RXB 10.2/
1.2
5.7/0
.8
4.1/0.8 2.3/0.8 -59 -59
6CR 8.2/1
.5
4.0/0
.2
5.1/1.5 3.2/0.8 -38 -20
6RXR 6.5/0
.8
4.8/0
.9
All died All
died96CW n/a n/a 3.3/ 2.5/96RXW 5.3 2.6 *3.6/ *0.6/96CB 8.4/0
.8
5.8/1
.1
5.1/1.8 3.0/0.4 -31 -48
96RXB 9.4/1
.0
6.7/1
.2
3.4/ 1.2/ -64 -82
96CR 8.7/1 5.1/.
4
3.4/ 1.5/ -49 -70
96RXR 9.1/1 5.1/0 2.3/ 1.1/ -75 -78
236
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
.2 .7
* only one surviving animal
RX = photosensitised animal
W = Unfiltered white microscope light
B = Blue only (filtered) microscope light
C = control animal
R = Red only (filtered) microscope light
Numbers are (mean flow)/(standard deviation of results)
237
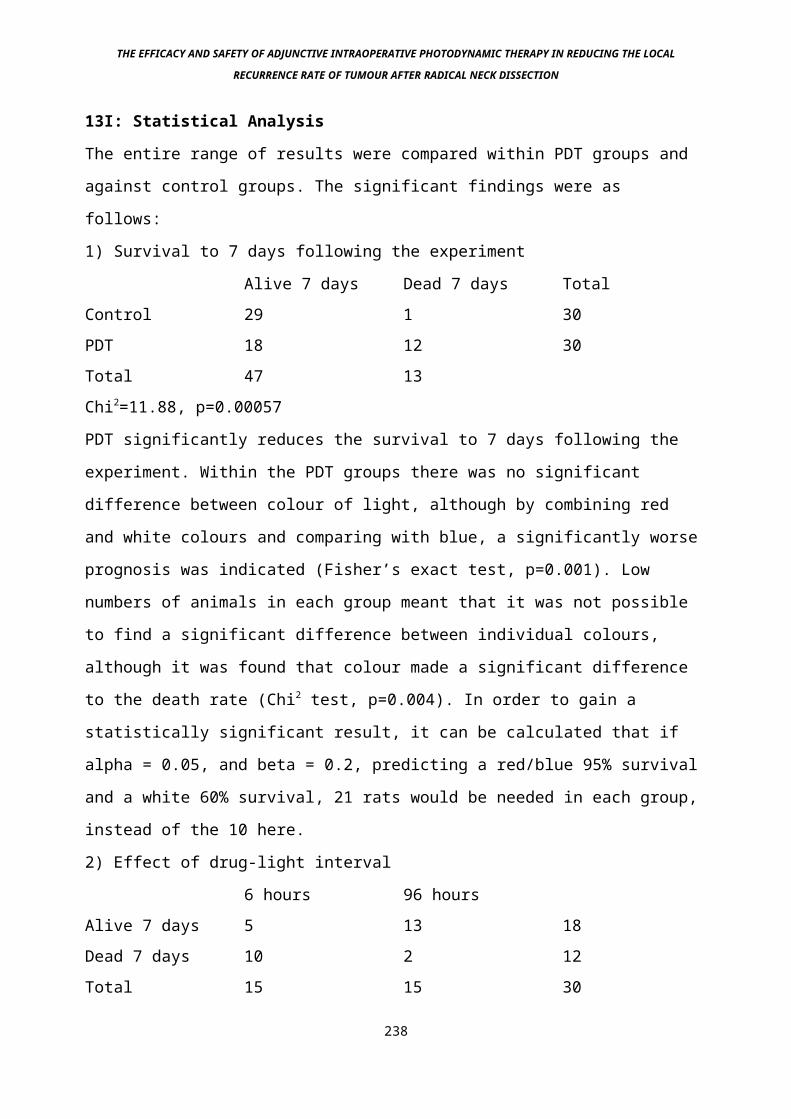
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
13I: Statistical Analysis
The entire range of results were compared within PDT groups and
against control groups. The significant findings were as
follows:
1) Survival to 7 days following the experiment
Alive 7 days Dead 7 days TotalControl 29 1 30PDT 18 12 30Total 47 13Chi2=11.88, p=0.00057
PDT significantly reduces the survival to 7 days following the
experiment. Within the PDT groups there was no significant
difference between colour of light, although by combining red
and white colours and comparing with blue, a significantly worse
prognosis was indicated (Fisher’s exact test, p=0.001). Low
numbers of animals in each group meant that it was not possible
to find a significant difference between individual colours,
although it was found that colour made a significant difference
to the death rate (Chi2 test, p=0.004). In order to gain a
statistically significant result, it can be calculated that if
alpha = 0.05, and beta = 0.2, predicting a red/blue 95% survival
and a white 60% survival, 21 rats would be needed in each group,
instead of the 10 here.
2) Effect of drug-light interval
6 hours 96 hoursAlive 7 days 5 13 18Dead 7 days 10 2 12Total 15 15 30
238
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Using a Fisher’s exact test the probability of the results being
randomly distributed is 0.008, ie the result is significant that
survival is decreased in the 6H group.
239
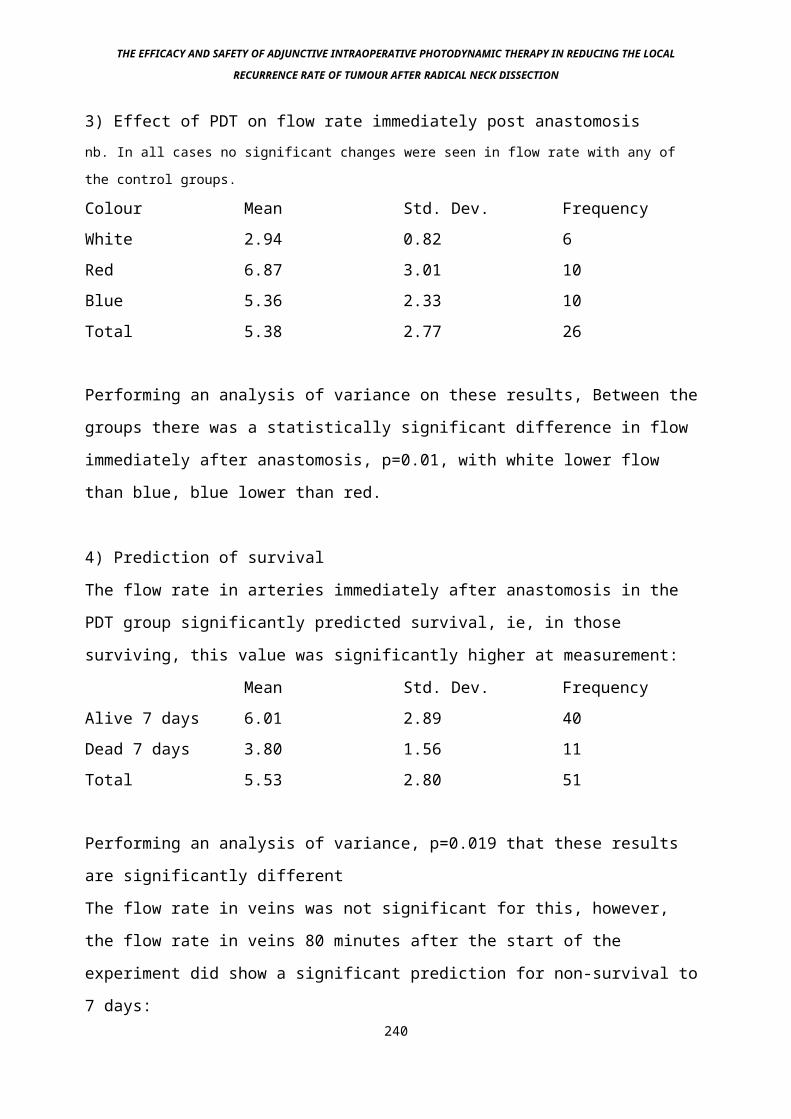
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
3) Effect of PDT on flow rate immediately post anastomosisnb. In all cases no significant changes were seen in flow rate with any of
the control groups.
Colour Mean Std. Dev. FrequencyWhite 2.94 0.82 6Red 6.87 3.01 10Blue 5.36 2.33 10Total 5.38 2.77 26
Performing an analysis of variance on these results, Between the
groups there was a statistically significant difference in flow
immediately after anastomosis, p=0.01, with white lower flow
than blue, blue lower than red.
4) Prediction of survival
The flow rate in arteries immediately after anastomosis in the
PDT group significantly predicted survival, ie, in those
surviving, this value was significantly higher at measurement:
Mean Std. Dev. FrequencyAlive 7 days 6.01 2.89 40Dead 7 days 3.80 1.56 11Total 5.53 2.80 51
Performing an analysis of variance, p=0.019 that these results
are significantly different
The flow rate in veins was not significant for this, however,
the flow rate in veins 80 minutes after the start of the
experiment did show a significant prediction for non-survival to
7 days:240
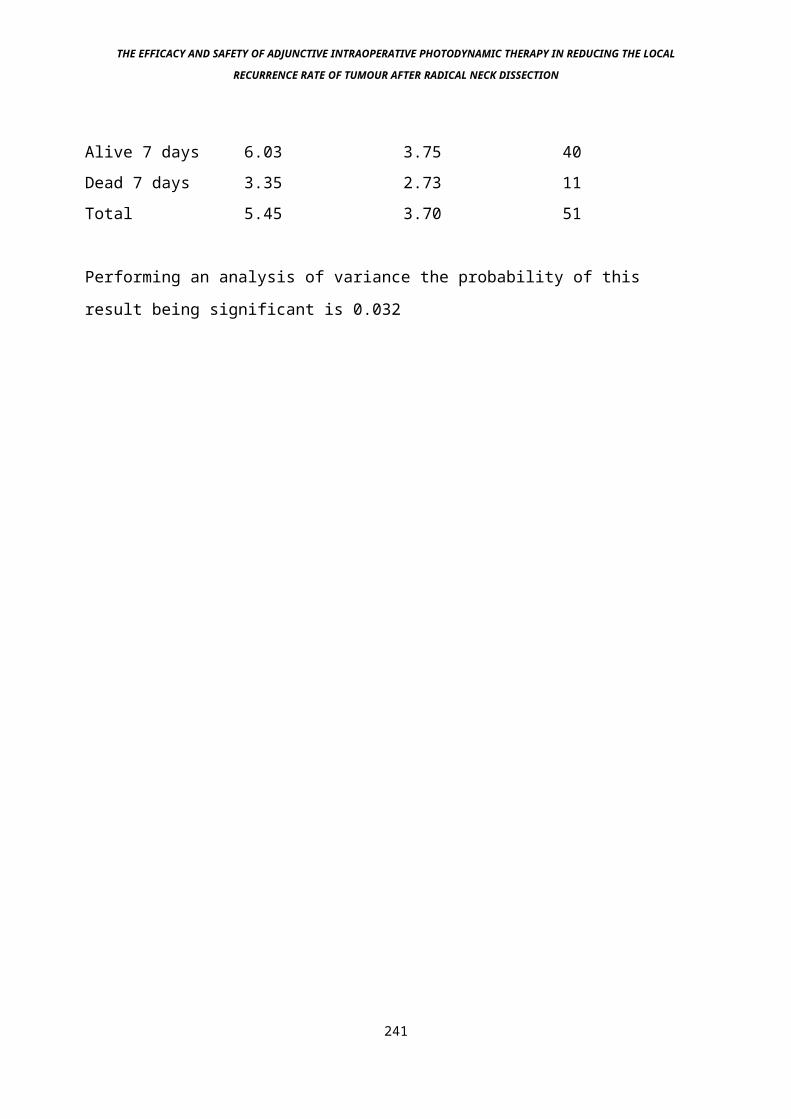
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Alive 7 days 6.03 3.75 40Dead 7 days 3.35 2.73 11Total 5.45 3.70 51
Performing an analysis of variance the probability of this
result being significant is 0.032
241

THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
The same is true for the arterial flow at 80 minutes:
Mean Std. Dev. FrequencyAlive 7 days 10.46 3.04 40Dead 7 days 6.91 3.11 11Total 9.69 3.36 51Performing an analysis of variance the probability of this
result being significant is 0.001
5) Effect of colour and drug-light interval on arterial flow
immediately after the anastomosis:
Anova test-
Partial
ss
df ms f p
Colour 34.89 2 17.44 3.88 0.036Time 35.26 1 35.26 7.85 0.01
Thus both colour and drug light interval have a significant
effect on this measurement, although using the same test, trying
to determine whether colour was important at both time
intervals, no significant difference was seen (Anova test,
p=0.06 for 6 hours, p=0.12 for 96 hours).
6) Effect of colour on flow immediately after anastomosis:
Oneway test- analysis of variance
ss df ms f pBetween
gps
58.92 2 29.46 4.21 0.02
242

THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Thus colour affects the flow through the anastomosis
significantly, white worse than red worse than blue
243
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
13J: Discussion
Little work has been done on the effect of clinic PDT on the
healing of reconstructed tissue following cancer surgery,
although there is evidence that abdominal bowel anastomoses are
not significantly damaged by PDT (Allardice 1992, Ansell 1996).
Work by Kubler et al in 1996 demonstrated damage to skin suture
lines in a pedicled myocutaneous flap reconstruction model. All
of these studies related to activating red or green light,
rather than the effects of ambient light. The previous study
(Experiment 4) has demonstrated the high sensitivity of small
veins to the effects of laser induced photodynamic therapy.
Usually they would be relatively unimportant, except in the
situation where they provide the sole drainage for a free flap
of skin with or without muscle and bone, as commonly used in the
reconstruction of Head and Neck defects following the excision
of malignancy. As previously stated, damage in this situation
could be catastrophic. Only one other study has mentioned the
use of free flaps such as these in sensitised patients (Biel
1996). This was using the drug Photofrin 2, no damage was
reported. No preclinical assessment such as in this study has
been carried out with any photosensitising drug, to our
knowledge.
Our own experiences with Photofrin on small vessels has however
shown significant damage 3 days postoperatively, at a light dose
of 100 J/cm2, 100 mW/cm2 irradiance (see previous experiments).
244
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
This was one of the reasons this entire series of experiments
has been mostly devoted to mTHPC.
However, the toxic effects of photofrin PDT on microvascular
anastomoses is mitigated by the fact that the net amount of
light given using a standard operating microscope is less than
20 J/cm2 in the red spectrum, as demonstrated in the first part
of this experiment. This is a small amount of light for an
inefficient photosensitiser such as Photofrin. We have not
however explored the effect of green light on microvascular
anastomoses, a part of the spectrum where there is a high
absorption peak for Photofrin, and where significant amounts of
activation may occur.
This study has instead concentrated on mTHPC, a powerful second
generation agent, for which 20 J/cm2 of activating red light is
a very significant dose, indeed, the therapeutic dose for Head
and Neck cancer treatments (Dilkes et al 1995).
245
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
In performing the assessment of amount of light in different
parts of the emitted spectrum of the microscope lamp, three
different levels were measured. The first, and most significant,
was the total amount of activating energy contained in the
unfiltered (except for infra-red) white microscope light. This
is the light that would be used in the clinical situation. On
linking the spectrum of the bulb with the action spectrum of
mTHPC, a relative activation efficiency can be calculated, in
the white light measurements this was the equivalent of 17 J/cm2
of monochromatic 652 nm red light for an 80 minute exposure, the
peak activating wavelength of mTHPC in the red spectrum. The 80
minute exposure relates to an approximate illumination time of
vessels undergoing microvascular anastomosis, and is the total
figure for vein and arterial anastomosis (40 minutes each). The
figure does not take into account other ambient operating light
that may also cause a damaging effect, particularly when raising
the flap prior to microvascular anastomosis.
The measurements were repeated using blue and red filters. This
was in order to assess the wavelength that was most critical in
causing damage to microvascular anastomoses in the next
experiment. As would be expected when light is being filtered
out, the relative activation figures were reduced in these
cases, down to 5J/cm2 for the red filter, 2 J/cm2 for the blue
filter.
The next part of the experiment was performed to assess the
sensitivity of the vessels in the microvascular anastomosis to
the effects of this light. Levels of mTHPC were undetectable in246
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
the abdominal aorta vessel of rats in the pharmacokimetic study
(experiment 1). No assessment was made of venous levels however,
where subsequent experimentation (Exp 4) showed significant
damage at higher light doses, although little effect at around
20 J/cm2. In these situation the drug-light interval was set at
96 hours, since this and other studies had shown this period of
time to be beneficial in terms of effect and selectivity (Exp.
1, Ris et al 1993). However, there is evidence to suggest that
high vascular levels occur in the first stages of
biodistribution following intravenous injection. This is
unsurprising since it is the vascular compartment of the
extracellular fluid that the drug is delivered to. This effect
falls off rapidly after the first 6 hours post-injection (Ronn
et al 1996). Two time points for the experiment were therefore
used, an early phase at 6 hours post injection, and a late stage
96 hours post injection. Control animals were selected at
randomn, and given an equivalent volume of drug diluent with no
sensitiser to prevent possible vascular overloading being an
independent variable. The 96 hour DLI was in keeping with
clinical studies, and the most critical time point, since this
is the stage at which vessels would be illuminated in the
clinical situation. The Linton Instruments doppler probe had
been used by us previously, and found to be a reliable method of
assessment of small vessel flow (exp 4). In this study it was
used for all cases, except early controls (96 hour DLI, white
light) when it was not available. The results comparing the pre-
and immediately post microvascular anastomoses show a fall in
measured blood flow in all groups. This is probably due to mild 247
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
stricturing of the vessels due to the anastomotic sutures. No
significant differences occurred between PDT with any of the
variables, and the controls. Once 80 minutes of total
illumination had occurred, an increase in blood flow was seen
when compared to the pre-anastomosis figures, for the control
(all groups) and arterial PDT groups. This is presumed to be
due to local and systemic inflammatory mediators causing vessel
dilatation, with some stretching of the anastomosis. The venous
PDT groups show a persistent fall in flow when compared to the
venous controls, a finding that is statistically WHAT??. The
effect is most pronounced in the white light groups, less in the
red and least in the blue filtered light groups. The range of
some of the results means statistical significance is not
reached for this effect, and this is due to the difficulty
maintaining a correct Doppler reading during the whole
experiment. The results comparing pre- and 7 days post
anastomosis are largely unimportant, since by this stage those
animals in whom a significant effect had been seen were dead.
The most clinically significant results were seen in the table
relating to observed findings, and death of animals. All of the
control animals survived to the experimental end point at 7 days
post anastomosis, when they were killed and the vessels
examined. In all these animals the vessels, anastomoses and
surrounding tissue were normal.
In the 6 hour DLI PDT group, damaging effects were seen in all
groups, the majority in the white light group, less in the red
light group and the least in the blue light group. In these
cases, observation at 80 minutes showed significant venous 248
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
thrombosis, with no arterial damage. 24 hours post anastomosis
the animals were re-assessed, further observation revealed
significant groin swelling particularly in the white light
group, 6/15 animals had already died. Post mortem examination
showed severe thrombosis, haemorrhage and oedema of the veins.
The arteries were undamaged. These findings were confirmed in
subsequent post mortems of those that survived beyond 24 hours.
249
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
In the 96 hour DLI PDT group, these findings were mirrored,
although the severity was less. Despite this only one of the
white light PDT group survived to 7 days postop, at post mortem
the venous anastomosis was thrombosed. Again in all cases the
arterial anastomosis was undamaged at post mortem, venous
thrombosis was present in 1/5 in the red light group and 2/5 in
the blue light group. In the situation where post mortem
examination at 7 days revealed venous thrombosis, collateral
circulation may have saved the animal.
Some attempt can be made to mask vessels from the effect of the
microscope light whilst they are not being anastomosed, for
example by hiding them behind moist black blotting paper. In
practice both vessels tend to be very close during surgery, and
this would be difficult to achieve. Although using filtered
light undoubtedly reduced the failure and damage rate of the
anastomoses, in practice performing surgery in these conditions
was difficult even in experienced hands, and was not felt to be
advisable in the clinical situation
250
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
14: Experiment 6 - Histological study of large diameter arteries
undergoing photodynamic therapy
14a: Description
This experiment was performed because the next experimental step
was to be human studies. Although the results of the arterial
studies had been convincing enough in rats, it was felt that
before human studies could be safely started, a human carotid
artery size vessel should be examined at the proposed human
drug, drug light interval, light dose and intensity for
confirmation of the safety seen in rats. The pig carotid artery
was chosen as the experimental target, since the pig has a
similar cardiac output to the adult human, around 5
litres/minute.
14b: Methodology
Suckling pigs of around 30 kg weight were used for the
experiment. They were injected with mTHPC 0.3 mg/kg
intravenously via an ear vein under sedation 96 hours prior to
PDT. After this they were kept in conditions of reduced
lighting. 96 hours later they were given a general anaesthetic
using halothane. The neck was opened on both sides. The carotid
artery was exposed after ligation of the external jugular vein,
division of the sternomastoid muscle and mobilisation of the
internal jugular vein. Black moist blotting paper was placed
medially to the vessel on both sides. One side was irradiated
with 20 j/cm2 red light at 652 nm wavelength, 100mW/cm2
intensity in 2 animals, the other side acted as a control. In 2 251
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
further animals the carotid vessels were emptied of blood by
holding the vessel between 2 rubber slings and milking the blood
out of the distal end using a vascular clamp. Light at the same
parameters as with the previous 2 animals was given unilaterally
on each animal. Following completion of the photodynamic
therapy, the area treated was marked with black silk sutures in
the muscle directly beneath the areas treated/exposed on both
sides. The skin was then closed and the animals recovered. 3
days later the animals were killed and the carotid vessels
removed for histological analysis.
14c: Results
No animal suffered unnecessarily as a consequence of the PDT to
its carotid artery. In particular there was no evidence of
cerebrovascular insufficiency. All animals were well prior to
the moment of death. The histological analysis revealed no
abnormal findings in PDT or control groups, in particular no
thrombosis or adventitial oedema was seen.
14d: Discussion
This study was performed to finalise safety work preclinically
prior to human studies. The 3 day time scale was chosen because
that is the point at which maximum damage had been seen in
experiment 3, where significant adventitial oedema had been
noted, although seemingly no compromise to blood flow occurred.
In this case there was no damage seen at all, on histological
analysis at this time point. This might be expected since the
vessel is 10x wider in diameter in the pig as compared to the 252
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
rat, thus it would be difficult for light to penetrate through
to the vessel wall opposite the light - incident surface.
Therefore any damage seen could be expected to be on the light
incident side only. In fact no damage was seen. This is in
contrast to a study performed in Switzerland on the same model,
which anecdotally (Altermatt H.B., pers. Comm. 1995) showed
internal carotid artery thrombosis at these PDT parameters,
particularly when the vessel was emptied of blood, as in this
study. Emptying the vessel of blood removes a significant part
of the light absorbing effect of the larger vessels, since
oxygenated haemoglobin is an important chromophore in the
absorption of light at this wavelength. Therefore it might be
expected that more damage occurs. The fact that no thrombosis
occurred in our experiment suggests that either we were not
adequately removing blood from the irradiated segment, or that
Altermatt and co. were over zealous in doing this, damaging the
intima so leading to thrombosis. The drug dose given, 0.3 mg/kg
was also significantly smaller than the 1.0 mg/kg given to the
rats. However, the rules of allometry suggest that this was a
fair relative dose (Paxton, 1995). The drug-light interval was
the same as in the rat study (96 hours). The light dose was 20
J/cm2, which equals the lowest level used in experiment 3,
although significant damage did still occur at that level in the
rats. Irradiance was the same in both studies (100 mW/cm2).
Other studies have looked at the effect of PDT using other
photosensitisers on larger vessels than rats. In particular,
work by Grant et al (1993) showed that the bursting pressure of
rabbit aorta’s was unaffected by PDT at time intervals up to 12 253
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
weeks post irradiation. Other safety studies, particularly
looking at PDT irradiation of the pig pelvis, showed no serious
damage to the common iliac vessels, although this was not
examined in depth (Allardice et al 1992).
254
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
15: Adjunctive Intraoperative Photodynamic Therapy for Head and
Neck Cancer
Having gained experience with the second generation
photosensitiser mTHPC on palliative and early cases of Head and
Neck cancer with very promising results, particularly with the
treatment of early malignancy (Pictures 16 and 17), we report
here our experience when using this treatment adjunctively, in 4
cases, further to the results of the previous 5 experiments. The
rationale and safety aspects are covered in the preceding
chapters.
255
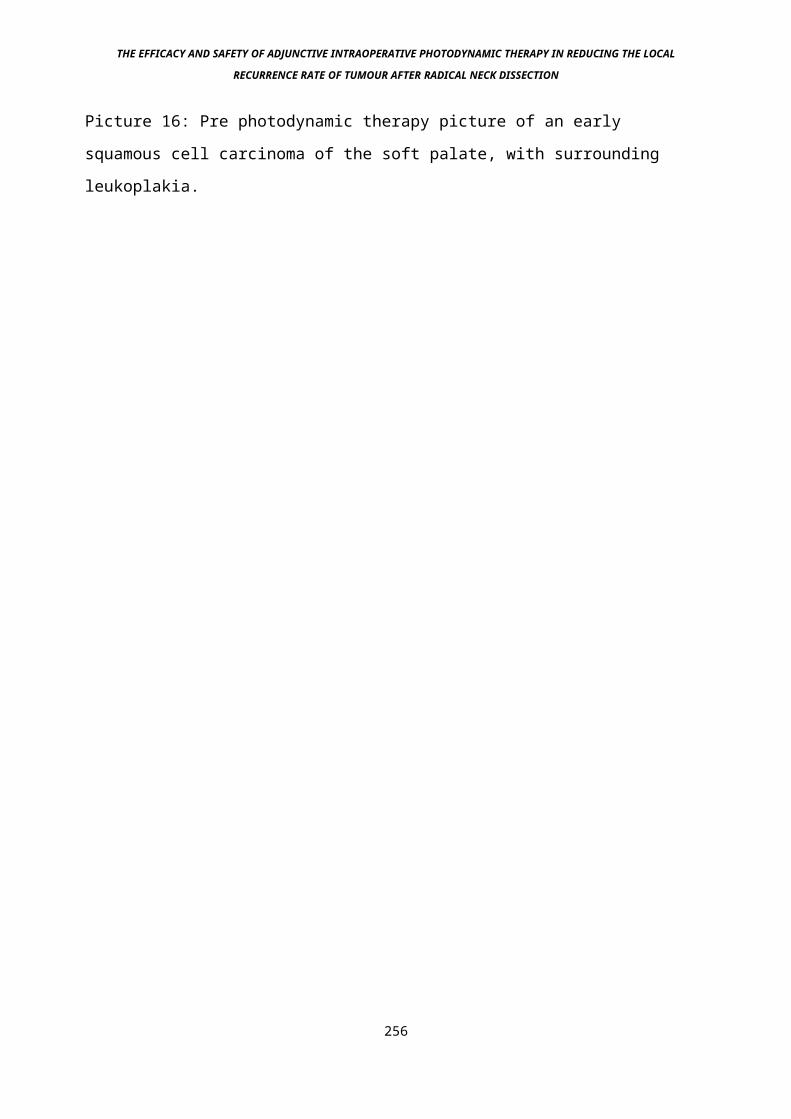
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Picture 16: Pre photodynamic therapy picture of an early
squamous cell carcinoma of the soft palate, with surrounding
leukoplakia.
256
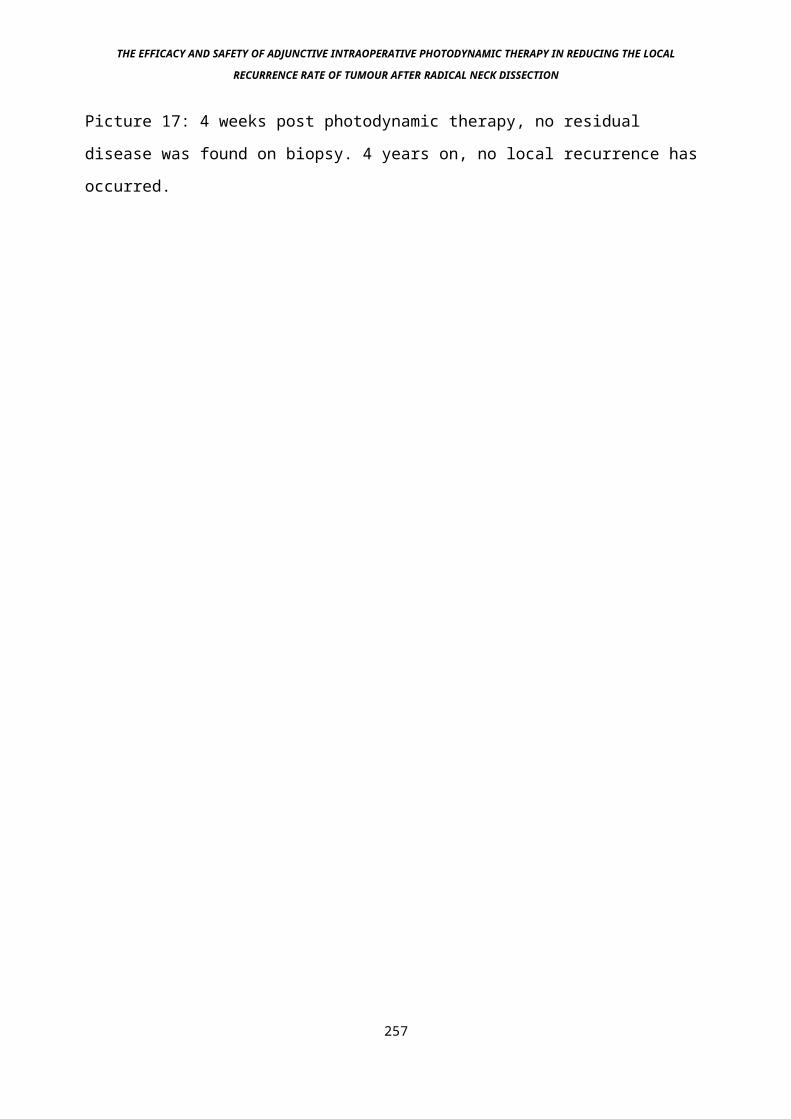
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Picture 17: 4 weeks post photodynamic therapy, no residual
disease was found on biopsy. 4 years on, no local recurrence has
occurred.
257
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
15a: Method
mTHPC (Temoporphyrin, Foscan) was obtained from Scotia
Pharmaceuticals, Guildford, U.K. It was stored as a sterile dry
powder in a fridge, protected from light. Solution for injection
was made up within 1 hour of delivery, by reconstituting the
powder with its solvent (1g ethanol and 1g polyethylene glycol
400 made up to 5 ml with sterile water for injection) to achieve
a final concentration of 4.0 mg/ml. The solution was filter-
sterilised as it was injected slowly over 5 minutes, a dose of
0.15 mg/kg body weight being given in all cases..
The drug-light interval was 96 hours in all cases, injection
therefore occurring 96 hours before the day of surgery. Patients
were fully consented regarding this additional treatment, and
particular care was taken to warn them regarding the risks of
exposure of the skin or eyes to direct sunlight for the first 4
weeks following drug injection, since to do this would risk a
serious photochemical skin burn. A full surgical resection of
the proposed site was performed, taking meticulous care to
ensure none of the patient’s skin was exposed to the operating
or theatre lights for a significant period of time. The skin
flaps were raised first, using ambient theatre light instead of
operating lights for illumination, and then folded back on
themselves, sutured in this position with 3/0 silk sutures, and
then covered by moist green cotton operating drapes, clipped to
the exposed edge. Betadine skin preparation was used prior to
surgery, its dark brown colour was felt to be helpful in further
absorbing ambient light during the initial phases of surgery 258
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
when skin would be exposed to operating theatre lights. The
pulse oximeter as routinely used by the anaesthetic staff was
not used for continuous monitoring, only on an “as required”
basis. This is because the red light emitted by these devices is
at around 630nm, and does activate the photosensitising drug
used here, mTHPC, albeit to a lesser extent than more commonly
used drugs such as Photofrin 2. Once the surgical resection was
complete, the patients were wheeled around to the laser room
still under general anaesthetic, if the Copper Vapour pumped dye
laser was used (Oxford Lasers, Abingdon Rd., Oxford, U.K.), or
treated in the operating theatre if the KTP pumped dye laser was
used (Laserscope, Raglan House, Cwmbran, Wales, U.K.). In order
to treat a uniform area, circular spots produced by the
microlens used (QLT, Vancouver, Canada) were converted to a
square of known area using a black anodised template (see
picture 18). Treated areas were marked with small dots of Evans
Blue dye to prevent missing out areas, and to make sure no over-
treatment occurred. Other methods of shielding treated and
untreated tissue included modifying a steridrape by cutting the
paper backing into uniform squares (Picture 19) and removing one
square at a time in a sequential manner, replacing each square
once the area underneath had been treated (Picture 20).
259

THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Picture 18: In order to prevent overlapping or under treatment,
the circular spot from the microlens is turned into a square
treatment area.
260

THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Picture 19: A steredrape is modified by sticking a grid of
squares over the irradiation site
261

THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Picture 20: Light is then delivered to the square with one area
removed, this is then re-applied and the next square treated
262
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Light at 652nm was delivered at 100 milliwatts/cm2 to a total
light dose of 20 joules/cm2 in all cases, over the entire
operative bed. We had previously found this to be an effective
level of light preclinically for AIOPDT and clinically for the
successful destruction of early malignant tumours of the Head
and Neck (Dilkes and DeJode 1994). The treatment time for each
spot was therefore 200 seconds. Using a 2cm x 2cm square (4cm2
area), the spot diameter was 2.8 cm. To treat the entire
operative bed of a radical neck dissection in this manner with
an area of approximately 200 cm2 would therefore take 10,000
seconds, just under 3 hours. In practice the more powerful laser
systems such as the KTP-pumped dye laser can treat up to 70 cm2
in one 200 second period, so the entire area can be treated in
600 seconds, 10 minutes. Thus the spot size is varied depending
on the output of the laser at 652 nm, and the area required to
treat. During PDT any structure deemed unsuitable for laser
light exposure can be masked using black absorbent gel (Black
stuff, Scotia Pharmaceuticals). For practical reasons in this
study this meant any exposed skin edge. Following completion of
photodynamic therapy, the usual drains were inserted, and skin
closure was completed with clips to save exposed skin from
ambient light damage, clips being quicker to insert than
sutures. During the in-patient period, standard precautions were
taken against sunlight exposure, the patient was not allowed
outside between 8 a.m. and 8 p.m., all light bulbs were replaced
with 60 watt bulbs, the windows were covered with black paper,
sellotaped to the glass. Baths and normal use of the toilet was
allowed, for up to 30 minutes per day. The same instructions 263
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
were given on discharge for 4 weeks post injection. At this
stage the patients were advised to place their hand in bright
light for several minutes. If tingling occurred, this meant
significant levels of sensitiser were still present, and the
patient was asked to wait 48 hours before trying this again.
264
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
14b: Results
14b(i): Case #1
A 55 year old man presented initially to another Hospital with
throat pain and difficulty swallowing. Full ENT examination
revealed a 3 cm x3 cm infiltrating mass in the tongue base,
subsequent pan-endoscopy showing this to be an isolated
squamous cell carcinoma, moderately differentiated, stage T3 N0
M0. Radical external beam radiotherapy was used to treat the
tumour, a dose of 2880 centigray (cGy) being given to both sides
of the neck and tumour, followed by a further 3000 cGy to the
tumour area alone. Routine follow up showed no symptoms or signs
of recurrent disease until, 12 months later, he developed a
painful mass deep in front of the right ear, with an associated
facial nerve palsy. At this stage he was transferred to our
Unit, where further pan-endoscopy showed no recurrence of tumour
at the primary site, but fine needle aspiration cytology of the
mass showed cells of squamous cell carcinoma. A radical
parotidectomy and neck dissection in continuity was performed,
AIOPDT was given to the upper half of the operative bed,
including the carotid bifurcation and tree. Facial reanimation
with temporalis fascia slings was performed by the plastic
surgeons. Postoperative progress was uneventful, he was
discharged home 7 days after surgery with no skin reaction from
PDT, drains having been removed at 48 and 72 hours, as per
usual. Six weeks after surgery, he died suddenly at home. A post
mortem revealed a massive pulmonary embolus from a pelvic deep
vein thrombosis that had been asymptomatic, a 3 cm x 3 cm
parotid gland node was found to be infiltrated with squamous 265
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
cell carcinoma. All other nodes in the specimen were clear. With
consent from the next of kin, both treated and untreated (right
and left respectively) carotid arteries were removed and
examined histologically with Haematoxylin + Eosin (routine), Van
Geesen (Collagen) and MSB (Fibrin) stains. No changes
attributable to PDT were found (see picture 21), although some
intimal hyperplasia and atheroma were noted on both sides,
thought to be due to age and previous radiotherapy.
266
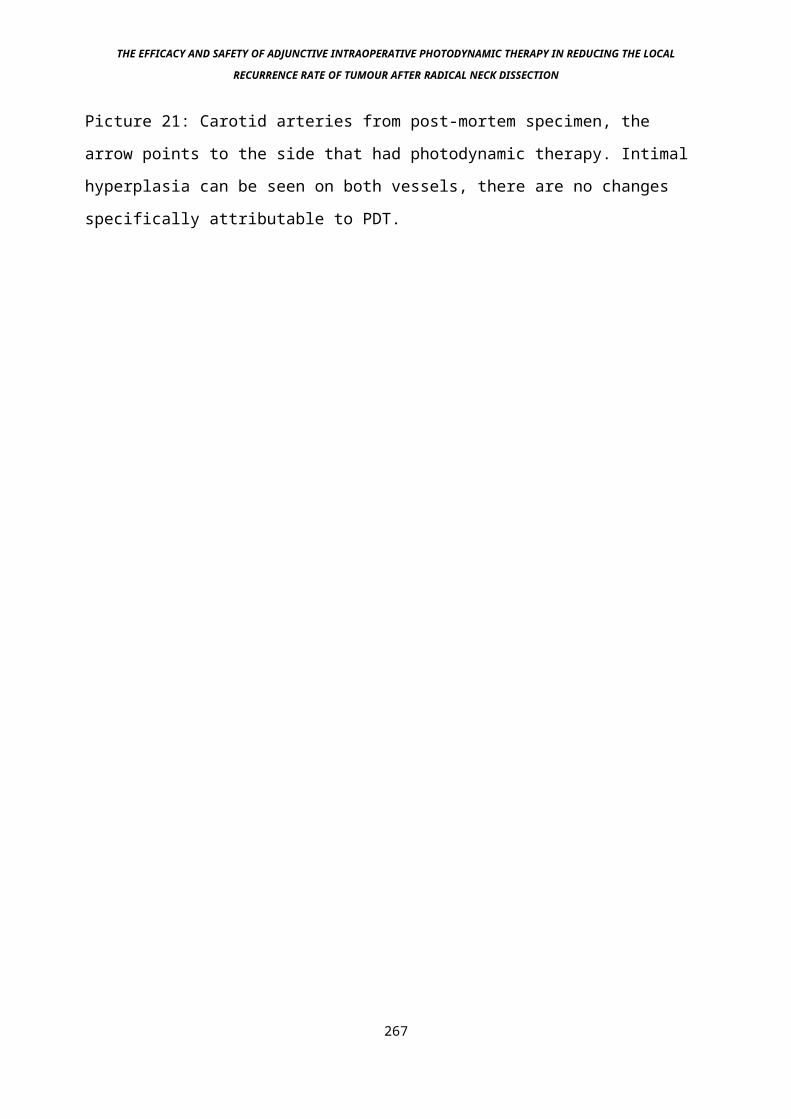
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Picture 21: Carotid arteries from post-mortem specimen, the
arrow points to the side that had photodynamic therapy. Intimal
hyperplasia can be seen on both vessels, there are no changes
specifically attributable to PDT.
267
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
14b(ii): Case #2
A 67 year old man presented with a 3 month history of a hoarse
voice. Indirect laryngoscopy revealed a keratinising lesion
confined to the mid-vocal cord on the left side. This was shown
at panendoscopy and biopsy to be a well differentiated squamous
cell carcinoma. Clinical and radiological staging was T1 N0 M0.
A course of radical radiotherapy was given, 5,500 cGy in 20
fractions over 4 weeks. Rapid regression of the tumour was noted
at monthly follow up. 10 months later he presented routinely
with an 8 x 6 cm hard mass arising from the mid-jugular area,
that had come up over the previous month. Needle aspiration and
panendoscopy revealed this to be a metastatic node from the
laryngeal primary, no further tumours being found. A radical
neck dissection was performed with AIOPDT given to the operative
bed, since clinical examination was suspicious of the tumour
involving the carotid tree. At operation this suspicion was
confirmed, tumour had to be peeled off the carotid artery below
the adventitial plane, with a high possibility of residual
tumour in the operative bed. Postoperatively no complications
specific to PDT were encountered. Less than 4 weeks after
surgery the skin on the treated side of the neck became
thickened and tender, biopsy showed carcinoma en cuirass.
Despite additional radiotherapy and chemotherapy the patient
died 2 months after this, from the effects of advanced disease.
268
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
14b(iii): Case #3
A 69 year old lady presented with a 2 year history of throat
discomfort. Indirect laryngoscopy revealed a 5 x 5 cm ulcerating
mass in the tongue base and vallecula. Panendoscopy and biopsy
showed this to be a moderately differentiated squamous cell
carcinoma, stage T3 N0 M0. This was treated with radical
radiotherapy, 2,500 cGy to neck and an extra 3,000 cGy to the
primary site. Check biopsy 2 months later showed persistent
tumour at the primary site, but no further spread. She turned
down a total laryngopharyngoglossectomy, but accepted a partial
laryngopharyngectomy with excision of the tongue base. AIOPDT
was given to the residual tongue resection margin. A radial
forearm free flap was revascularised locally and used to fill an
extensive anterior mucosal defect. Postoperatively a
pharyngocutaneous fistula developed, it was difficult to assess
the viability of the flap. No further adverse sequelae occurred
that might have been attributable to PDT. 6 weeks after surgery
a fatal carotid artery rupture occurred.
`
15b(iv): Case #4
A 39 year old man presented with a 4 week history of facial
pain, discharge into the roof of his mouth (antro-oral fistula),
and discharge onto the cheek skin (antro-cutaneous fistula).
Naso-endoscopy and biopsy revealed extensive polypoid disease
arising from the lateral nasal wall, shown on histology to be
poorly differentiated squamous cell carcinoma. Computerised
tomography scanning showed this tumour to have invaded the orbit269
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
and the pterygoid musculature. The clinical stage was T4 N0 M0.
Radical radiotherapy was given, 6,500 cGy to the whole area.
Biopsy 4 weeks after radiotherapy revealed persistent disease.
The was still no sign of metastasis. Radical surgery involving a
total maxillectomy, orbital exenteration and ethmoidectomy was
performed. 6 months after surgery tumour reappeared in the skin
near the nasomaxillary part of the incision. This was debulked
using the Nd-YAG and CO2 combination laser (Broomhead et al
1995), and the whole operative bed and lateral nose was treated
with AIOPDT. This area healed well, no complication due to PDT
occurred. Future tumour recurrence arose in the skull base which
was treated by additional radiotherapy, and chemotherapy. He
eventually died 6 months later of intracranial extension of the
disease.
15d: Discussion
No significant damage occurred that was attributable to PDT in
any case except number 3, when the microvascular anastomosis may
have been affected by the effects of white microscope light,
which we have shown to be possible in an animal model,
experiment 5 above. At this stage we do not recommend that
AIOPDT with mTHPC is attempted when a free flap is to undergo a
microvascular anastomosis. The results otherwise do not show
that tumour recurrence was reduced with AIOPDT, although in
cases 2,3 and 4 very advanced tumours were treated with a low 270
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
chance of long term survival (Sloan and Goepfert 1991). The
first case had no residual tumour in the site of treatment,
although only one node in the entire specimen was involved with
tumour, and local recurrence 6 weeks after treatment would be
unlikely in this situation anyway. The histological analysis of
the carotid arteries showed changes in keeping with age and
radiotherapy on both sides, no additional changes were seen on
the AIOPDT side. This was in keeping with the previous study
(experiment 3) in which short term (3 days) adventitial oedema
was seen in the femoral arteries, but no significant damage
occurred (Dilkes et al 1996b).
Local tumour recurrence after major head and neck surgery
depends on several factors, such as age and general condition of
the patient, site and extent of disease, pre or post operative
treatment with radiotherapy (Gilbert and Kagan 1974). When
considering the operation of radical neck dissection, the
incidence of local recurrence is further affected by the
presence of extracapsular spread of disease, and/or multiply
involved nodes (Snow et al 1982). The rate of local recurrence
in an N1 or N2 neck after radical neck dissection but without
radiotherapy is around 30% (DeSanto et al 1982). If local
recurrence occurs in a previously treated N+ neck, the salvage
rate is as low as 5% (Mendelsohn et al 1976). Therefore any
procedure that carries a reasonable expectation of increasing
this figure in a safe manner, is welcome. A prospective study is
needed with control (no AIOPDT) to show whether or not AIOPDT
is effective in the human situation.
271
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
16: Conclusion
This series of experiments has demonstrated the following facts:
mTHPC has a greater degree of tumour selectivity than Photofrin
2 when tested on the rat HSN Fibrosarcoma model, as measured
pharmacologically. The tumour necrosis validation was
unsuccessful. The peak drug-light interval for effect and
selectivity occurred between 96 and 144 hours post intravenous
injection.
The tumour model HSN Fibrosarcoma is a reliable and relatively
uniformly growing tumour with a doubling time of approximately
18 hours. PDT with mTHPC gives a statistically significant
reduction when compared to controls, in the local recurrence
rate after tumour excision and adjunctive intraoperative
delivery to the tumour bed, at an end point limited by
overwhelming tumour recurrence in each experimental series.
Safety studies at therapeutic levels used for adjunctive PDT,
and light doses above and below that showed no significant
damage to the femoral artery of rats, when compared to controls
(directly matched groups). Inconsequential adventitial oedema
occurred in the PDT groups only, 3 days post irradiation.
Ultrasonic Doppler blood flow measurements during and
immediately after PDT showed a significant reduction in flow
through veins, particularly the internal jugular vein, with no
effect on arteries or controls.
Measurement of the light output from operating microscopes used
for microvascular anastomosis showed significant relative
activation levels of light, particularly in unfiltered white272
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
light. This was found to cause severe compromise to the venous
anastomoses of sensitised rats both at 6 and 96 hours post drug
injection. No damage was seen in arteries, controls were
unaffected.
The pig common carotid artery was not affected by clinical doses
of PDT, even when emptied of blood.
Initial clinical studies have shown that adjunctive
intraoperative photodynamic therapy (AIOPDT) is safe for use in
the Head and Neck surgery performed without formal
reconstruction using tissue from elsewhere.
A prospective, controlled study is needed to assess the effect
of AIOPDT on a simple Head and Neck surgical model, where the
negative effects should be minimal. It is suggested that such a
model is the operation of radical neck dissection.
17: References
Abramson A.L., Levy A.S., and Hirschfield L.S. (1990) The
pathologic and thermal effects of gold vapour laser photodynamic
therapy on the larynx. Arch Otolaryngol Head and Neck Surg;
(116):687-691
Abulafi A.M., Allardice J.T. and Williams N.S. (1993) A phase 3
study on the effect of adjunctive intraoperative photodynamic
therapy in colorectal cancer: an interim report. Lasers Surg.
Med., Suppl.5:45
273
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Abulafi A.M., DeJode M., Allardice J.T., Ansell J., Rogers J. And
Williams N.S. (1995) Adjuvant intraoperative photodynamic therapy
in experimental colorectal cancer. Br. J. Surg.;82(2):178-81
Agarwal M.L., Clay M.E., Harvey E.J., Evans H.H., Atunez A.R. and
Oleinick N.L. (1991) Photodynamic therapy induced rapid cell death
by apoptosis in L5178Y mouse lymphoma cells. Cancer Res. ;51:5993-
5996
Allardice J.T., Abulafi A.M., Grahn M.F. and Williams N.S. (1994)
Adjuvant intraoperative photodynamic therapy for colorectal
cancer: a clinical study. Surgical Oncology;3(1):1-10
Amrein P. (1991) Current chemotherapy of Head and Neck cancer. J.
Oral and maxillofac. Surg.;49(8):864-870
Anderson R.E. (1985) Radiation injury. In: Kissane J.M., ed,
Anderson’s Pathology, St. Louis: CV Mosby Co.
Ansell J.K., DeJode M.L., Grahn M.F., Maudsley J. and Williams
N.S. (1995) Correlation of photodynamic effect with surface
fluorescence and drug assay. Lasers in Surgery and Medicine;
:41
Annyas A.A., Snow G.B. and van Slooten E.A. (1979) Prognostic
factors of neck node metastasis: Their impact on planning a
274
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
treatment regime. Read before the American Society of Head and
Neck Surgeons, New Orleans, Los Angeles, April 6th 1979.
Ariyan S., Krizek T.J. and Mitchell M.S. (1977) Identification
of squamous cell carcinoma of the head and neck by tissue
culture and immunological staining. Plast. Reconst. Surg;59:386
Ariyan S. (1986) Radical neck dissection. Surg. Clin. North
Am;66(1):133-148
Arrigada R., Eschwerge F., Cachin Y. and Richards J.M. (1983)
The value of combining radiotherapy with surgery in the
treatment of hypopharyngeal and laryngeal cancers.
Cancer;51:1819-1825
Auler H and Banzer G. (1943) Untersuchengen uber die rolle der
porphyrine be geschwulstkranken menschen und tieren.
Z.Krebsforsch.;53:65-68
Banoczy J, Csiba A (1976) Occurrence of epithelial dysphasia in
oral leukoplakia. Oral Surg Oral Med Oral Pathol 42:766-74
Barr H. Tralau C.J. Boulos P.B.,MacRobert A.J. Tilley R. and Bown
S.G.(1987) The contrasting mechanisms of collagen damage between
photodynamic therapy and thermal injury. Photochem.
Photobiol.;46:795-800
275
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Barr H. Tralau C.J. MacRobert A.J., Krasner N., Phillips D. And
Bown S.G. (1987) Photodynamic therapy in the normal rat colon
with Phthalocyanine sensitisation. Br. J. Cancer;56:111-8
Barr H., Tralau C.J., Boulos P., MacRobert A.J., Krasner N.,
Phillips D., and Bown S.G. (1990) Selective necrosis in
Dimethylhydrazine-induced rat colon tumours using phthalocyanine
photodynamic therapy. Gastroenterology;98:1532-1537
Barr H., Tralau C.J., MacRobert A,J., Morrison I., Philipps D.
and Bown S.G. (1988) Fluorescence photometric techniques for
determination of microscopic tissue distribution of
phthalocyanine photosensitizers for photodynamic therapy. Lasers
Med Sci;3:81-86
Bauer H.C. (1974) Varieties of squamous carcinoma: Biologic
behaviour. Front. Radiat. Ther. Oncol.;9:164
Beahrs O.H., Gassel J.D. and Hollingshead W.H. (1955) Technique
and surgical anatomy of radical neck dissection.
Am.J.Surg;;90:490-516
Beahrs O.H. and Barber K.W. (1962) The value of radical
dissection of structures of the neck in the management of
carcinoma of the lip, mouth and larynx. Arch. Surg;85:65-72
Beahrs O.H. (1971) Surgical anatomy and technique of radical
neck dissection. Surg. Clin. North Am;57:663-7000276
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Ben Hur E., Rosenthal I. (1985) The phthalocyanines: A new class
of mammalian cell photosensitisers with a potential for cancer
phototherapy. Int. J. Radiat. Biol.;47:145-
Ben-Hur E., Orenstein A. (1991) The endothelium and red blood
cells as potential targets in PDT-induced vascular stasis. Int. J.
Radiat. Biol.;60(1,2):293-301
Ben-Hur E., Heldman E., Crane S.W., and Rosenthal I.(1988)
Release of clotting factors from photosensitized endothelial
cells: a possible trigger for blood vessel occlusion by
photodynamic therapy. Febs Letts.;236(1)105-108
Berenbaum M.C., Bonnett R.R. and Scourides P.A. (1982) Inn vivo
biological activity of the components of haematoporpphyrin
derivative. Br. J. Cancer;45:571-
Berenbaum M.C., Akande S.L., Bonnet R., Kaur H., Ioannou S.,
White R.D. and Winfield U-J.(1986) meso-
Tetra(hydroxyphenyl)porphyrins, a new class of potent tumour
photosensitizers with favourable selectivity. Br J. Cancer 54:717-25
Berenbaum M.C. (1989) Comparison of haematoporphyrin derivatives
and new photosensitisers; in: Photosensitising Compounds: Their chemistry,
biology and clinical use. Ciba Foundation Symp 146. Chichester, Wiley,
33-277
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Berenbaum M.C., Bonnett R., Chevretton E.B., Akande-Adebakin
S.L. and ruston M (1993) Selectivity of meso-
tetrahydroxyphenylporphyrins and chlorins and of Photofrin 2 in
causing photodamage in tumour, skin, muscle and bladder. The
concept of cost-benefit in analysing the results. Lasers in
Medical Science;8:235-243
Meyer- Betz (1913) Untersuchengen uber die Biologische
(photodynamische) Wirkung des hamatoporphyrins und anderer
Derivative des Blut und Gallenfarbstoffs. Dtsch. Arch. Klin.
Med.;112:476-503
Biel M.A. (1994) Photodynamic therapy and the treatment of
neoplastic disease of the larynx. Laryngoscope 104:399-403
Biel M.A. (1995) Photodynamic therapy of Head and Neck cancers.
Semin. Surg. Oncol.;11(5):355-9
Biel MA (1996) Photodynamic therapy as an adjuvant
intraoperative treatment of recurrent head and neck carcinomas.
Arch Otolaryngol Head Neck ;122 (11):1261-5
Biller H.F., Urken M., Lawson W., and Haimov M. (1988) Carotid
artery resection and bypass for neck carcinoma. Laryngoscope
98:181-183
278
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Billroth T. and Gussenbauer C. (1874) Ulber die Erste durch
T.Billroth am Menschen ausgefuhrte Kehlkopf-Extirpation und die
Auswendung eines Kunstlichen Kehlkopfes. Arch. Clin. Chir;17:343-
Bocca E. (1975) Conservative neck dissection. Laryngoscope
85:1511-1515
Bonnet R., White R.D., Winfield U.J., Berenbaum M.C. (1989(1))
Hydroporphyrins of the mesotetra(hydroxyphenyl)porphyrin series
as tumour photosensitizers. Biochem J., 261:277-280
Bonnet R., Berenbaum M.C., (1989(2)) Porphyrins as
Photosensitizers. In: Photosensitizing compounds: their
Chemistry, Biology and Clinical use. Wiley, Chichester (CIBA
Foundation Symposium 146):40-59
Bonnet R. (1995) Photosensitisers of the Porphyrin and
Phthalocyanine series for Photodynamic Therapy. Chem. Soc.
Rev.;199:19-33
Bown S.G., Tralau C.J., Coleridge-Smith P.D., Akdemir D. and
Wieman T.J. (1986) Photodynamic Therapy with Porphyrin and
Phthalocyanine sensitisation: Quantitative studies in normal rat
liver. Br. J. Cancer 54:43-52
Bown S.G. (1990) Photodynamic Therapy to scientists and
clinicians - one world or two ? J. Photochem Photobiol. 6:(1-12).
279
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Braichotte D.R. Wagnieres G., Bays R. and Van den Burgh H. (1995
(1)) Clinical phartmacokinetic studies of photofrin by
fluorescence spectroscopy in the oral cavity, the esophagus and
the bronchi. Cancer;74:3113-17
Braichotte D.R., Savary J.F., Glanzmann T., Monnier P. and Van
Den Burgh H.E. (1995 (2)) Clinical pharmacokinetic studies of
tetra(meta-hydroxyphenyl)chlorin in squamous cell carcinoma by
fluorescence spectroscopy at 2 wavelengths. Int. J. Cancer;63:198-204
Braichotte D.R., Savary J.F., Monnier P. and Van Den Burgh H.E.
(1996) Optimising light dosimetry of early stage carcinomas of
the esophagus using fluorescence spectroscopy. Lasers Surg.
Med.;19(3):340-6
Braund R.R., and martin H.E. (1941) Distant metastases in cancer
of the upper respiratory and amliomentary tracts. Surg. Gynae
Obs.;73:63-71
Broomhead C.J., Dilkes M.G. and Monks P.S. (1995) Use of the
hayek Oascillator in failed fibreoptic intubation. Br. J.
Anaesthesia;74(6):720-721
Brown J.B. and McDowell F. (1944) Neck dissections for
metastatic carcinoma. Surg. Gynecol. Obstet;79:115-124
280
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Bremner J.C.M., Bradley J.K., Adams G.E., Naylor M.A., Sansom
J.M. and Stratford I.J. (1994) Comparing the antitumour effect
of several bioreductive drugs when used in combination with
photodynamic therapy (PDT). Int. J. Radiat. Oncol.;29(2):329-332
Buchanan R.B., Carruth J.A.S., McKenzie A.L. and Rhys-Williams
S. (1989) Photodynamic Therapy in the treatment of malignant
tumours of the skin and Head and Neck. Eur J. Surg. Oncol 15:400-406
Buck G., (1853) On the surgical treatment of morbid growths
within the larynx. Trans Am. Med. Assoc;6:509
Bugelski P.J., Porter C.W., Dougherty T.J. (1981)
Autoradiographic distribution of hematoporphyrin derivative in
normal and tumour tissue of the mouse. Canc. Res. 41:4606-4612
Burke E.M. (1937) Metastases in squamous cell cancer Am. J.
Cancer;30:493-503
Butlin H.T.(1909), "On early diagnosis of cancer of the tongue."
Br Med J.,1:462.
Byrne C.J., Marshallsay L.V. and Ward A.D. (1990) The
composition of Photofrin 2. J. Photochem Photobiol B. 6:13-27
Cai W.M., Yang Y., Zhang N.W. et al (1985) Photodynamic Therapy
in the management of cancer: An analysis of 114 cases, in:281
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Kessel D. (Ed) Methods in Porphyrin Photosensitisation, New
York, Plenum Press, p13-19
Call G.K., Bray P.F., Smoker W.R.K., Buys S.S. and Hayes J.K.
(1990) Carotid thrombosis following neck irradiation. Int. J.
Radiat. Oncol.;18:635-40
Campbell D.L., Gudgin-Dickson E.F., Forkert P.G., Pottier R.H.
and Kennedy J.C. (1996) Detection of early stages of
carcinogenesis in adenomas of murine lung by 5-aminolaevulinic
acid-induced protoporphyrin 1x fluorescence. Photochem
Photobiol.;64(4):676-82
Carruth J.A.S. and Mckenzie A.L. (1985) Preliminary report of a
pilot study of photoradiation therapy for the treatment of
superficial malignancies of the skin, head and neck. Eu. J.
Surg. Oncol;11:47-50
Castigliano S.C and Reminger C.J. (1954) Distant metastases from
carcinoma of the oral cavity. Am. J. Roentgol.;71:997-1006
Castro D.J., Saxton R.E., Fetterman H.R., Castro D.J., and Ward
P.H. (1987) Rhodamine 123 as a new photochemosensitizing agent
with the argon laser: "Nonthermal" and thermal effects on human
squamous carcinoma cells in vitro. Laryngoscope 97:554-561
Chan W.S., Svensen R., Phillips D. and Hart I.R. (1986) Cell
uptake, distributuion and response to aluminium chlorosulfonated282
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
phthalocyanine, a potential antitumour photosensitiser. Br. J.
Cancer.;53:255-
Chan W.S., West C.M.L., More J.V. and Hart I.R. (1991)
Phototoxic efficacy of sulphonated species of aluminium
phthalocyanine against cell monolayers, multicellular spheroids
and in vivo tumours. Br. J. Cancer 64:827-832
Chevretton E.B. (1991). MS Thesis, London University.
Chu W. and Strawitz J.G. (1978) Results in suprahyoid, modified
radical and standard radical neck dissections for metastatic
squamous cell carcinoma: recurrence and survival. Am. J.
Surg;136:512-515
Coates W.D. Jr., Currier J.W., Mejias Y., Narciso H.L. and faxon
D.P. (1996) Tin ethyl etiopurpurin significantly inhibits
vascular smooth muscle cell proliferation in vivo. Biochem. Cell
Biol.;74(3):325-31
Cowled P.A., Mackenzie L. and Forbes I.J. (1987) Pharmacological
modulation of photodynamic therapy with hematoporphyrin
derivative and light. Cancer Res.;47:971-974
Crile G.W. (1903) Tubage of the pharynx for facilitating the
administration of anaesthetics and preventing the inhalation of
blood in certain operations of the mouth and face. Ann.
Surg;37:859283
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Crile G.W. (1906), Excision of cancer of the head and neck with
special reference to the plan of dissection in 132 operations.
JAMA 47:1780.
Crile G.W. (1923) Cancer of jaws, tongue, cheek and lips. Surg.
Gynaecol. Obstet;36:159-184
Dahlman A., Wile A.G., Burns R.G., Mason R., Johnson F.M., and
Berns M.W. (1983) Laser Photoradiation Therapy of Cancer. Canc
Res. 43:430-434
Daniell M.D. and Hill J.S. (1991) A History of Photodynamic
Therapy. Aust. N.Z. J. Surg;61(5):340-348
284
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Davis R.K., Davis K., Straight R.C. and Warner M. (1988) Effects
of photosensitizer (haematoporphyrin derivative - HPD) and light
dose on vascular targets in the albino mouse ear. Laryngoscope
98:++++++++++++++++++++++++++++++++
Davis R.K., Straight R.C. and Keresati Z.G. Comparison of
photosensisiers in saline and liposomes for tumour photodynamic
therapy and skin phototoxicity. Laryngoscope;100:682-686
Davis R.K., Smith L.F., Thurgood R.F., Kereszti Z. and Straight
R.C. (1990(2)) Intraoperative Phototherapy (PDT) and surgical
resection in a mouse neuroblastoma model. Lasers Surgery Med. 10:275-
279
DeJode M.L., Dilkes M.G., Grahn M.F., Hart P.B. and Raven A.
(1995) New LED source for Photodynamic Therapy: Preclinical
study. Proc. S.P.I.E. 2629:299-305
DeJode M.L., McGilligan J.A., Dilkes M.G., Cameron I., Hart P.B.
and Grahn M.F. (1997) A comparison of novel light sources for
Photodynamic Therapy. Lasers in Medical Science;12(3): in press
DeSanto L.W., Lillie J.C. and Devine K.D. (1977) Cancers of the
larynx: supraglottic cancer. Surg. Clin. North Am;57:505-514
DeSanto L.W., Holt J.J., Beahrs O.H., O'Fallon W.M. (1982) Neck
Dissection: is it worthwhile? Laryngoscope;92:502-509285
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
DeSanto L.W., Holt J.J., Beahrs O.H., O'Fallon W.M. (1985). Neck
dissection and Combined therapy- Study of effectiveness. Arch Otol
111:368
Dilkes M.G. and Birchall M.A. (1990) Bilateral parotid
secondaries from primary bronchial carcinoid tumour.
J.L.O.;105(6):489-90
Dilkes M.G., DeJode M.L., Gardiner Q. and Kenyon G.S. (1995)
Photodynamic Therapy for Head and Neck cancer, 1 year's
experience. JLO;109(11):1072-76
Dilkes M.G. and DeJode M.L. (1994) meta-
Tetrahydroxyphenylchlorin mediated Photodynamic Therapy.
Experience and thoughts after 17 treatments. Proc. S.P.I.E. 2371:256-
261
Dilkes M.G. and DeJode M.L.(1995) Alternative Light Sources for
PDT (Abstract). In press, Lasers in Medical Science
Dilkes M.G., DeJode M.L., Rowntree-Taylor A., McGilligan J.A.,
Kenyon G.S. and McKelvie P. (1996) mTHPC Photodynamic therapy
for Head and Neck cancer. Lasers in Medical Science;11:23-29
Doktor B., So C.B., Saliken J.C. and Gray RR (1996) Ultrasound
monitoring in cannulation of the internal jugular vein: anatomic
and technical considerations. Can. Assoc. Radiol, J.;47(3):195-201286
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Donald P.J., Cardiff R.D., He D.E. and Kendall K. (1991)
Monoclonal antibody-porphyrin conjugate for head and neck
cancer: the possible magic bullet. Otolaryngol. Head Neck
Surg.;105(6):781-787
Dougherty T.J., Grindet G.B., Fiel R., Weishaupt K.R. and Boyle
D.G. Photoradiation therapy.2. Cure of animal tumours with
hematoporphyrin and light. J. Natl. Cancer Inst.;55(1):115-119
Dougherty T.J., Kaufman J.E., Goldfarb A., Weishaupt K.R., Boyle
D.G., Mittleman A. (1978) Photoradiation therapy for the
treatment of malignant tumours. Canc. Res.;38:2628-2635
Dougherty T.J., Potter W.R. and Weishaupt K.R. (1984) The
structure of the active component of haematoporphyrin
derivative. In: Porphyrins in tumour phototherapy, Andreoni &
Cubeddu. (Eds) p23, Plenum Press: New York
Dougherty T.J. (1989) Photodynamic Therapy- New approaches. Semin.
Surg. Oncol. 5:6-16
Dougherty T.J., Cooper M.T. and Mang T.S. (1990) Cutaneous
phototoxic occurences in patients receiving Photofrin. Lasers Surg
Med.;10:485-88
Dougherty T.J. and Marcus S.L. (1992) Photodynamic Therapy. Eur. J.
Cancer;28a(10):1734-1742287
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Drost C.J. (1978) Vessel diameter-independent volume flow
measurements using ultrasound. Proc. San Diego Biomedical
Symposium 17:299-302
Eccles S.A. and Alexander P. (1974), Macrophage content of
tumours in relation to metastatic spread and host immune
reaction. Nature 250:667-669
Edell E.S. and Cortese D.A. (1987) Bronchoscopic phototherapy
with hematoporphyrin Derivative for treatment of localized
bronchogenic carcinoma: A 5 year experience. Mayo Clin. Proc.;62:8-14
Edell E.S. and Cortese D.A. (1992) Photodynamic therapy in the
management of early superficial squamous cell carcinoma as an
alternative to surgical resection. Chest 102(5):1319-22
288
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Elerding S.C., Fernandez R.N., Grotta J.C., Lindberg R.D.,
Causay L.C., McMurtrey M.J. (1981) Carotid artery disease
following external cervical irradiation. Ann. Surg.;194(5):609-
615
El-Far M.A., and Pimstone N.R., (1985), The interaction of
tumour-localising porphyrins with collagen, elastin, gelatin,
fibrin and fibrinogen. Cell. Biochem. Function 3:115-9.
Farr H.W. and Arthur K. (1971) Epidermoid carcinoma of the mouth
and pharynx 1960-64. J.L.O;86:243-253
Feyh J. Goetz A., Muller W., Konigsberger R. and Kastenbauer E.
(1990) Photodynamic therapy in Head and Neck surgery. J. Photochem.
Photobiol. 7:353-358
Figge F.H.J and Weiland G.S (1948) The affinity of neoplastic,
embryonic and traumatised tissue for primary solid tumours in
pet cats and dogs. Anat. Rec.;100:659
Figge F.H.J and Weiland G.S. (1949) Studies on cancer detection
and therapy: the affinity of neoplastic, embryonic and
traymatised tissue for porphyrins and metalloporphyrins. Cancer
Res.;9:549
Fingar V.H., Wieman T.J., Doak K.W. (1990) Role of thromboxane
and prostacyclin release on photodynamic therapy induced tumour
destruction. Canc Res;50:2599-2603 289
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Fletcher G.H. (1972) Elective irradiation of subclinical disease
in cancers of the Head and Neck . Cancer ;29:1450-1454
Forbes I.J., Cowled P.A., Leong A.S.Y. (1980) Phototherapy of
human tumours using hmatoporphyrin derivative. Med. J. Aust.;2:489-
493
Foster T.H., Primavera M.C., Marder V.J., Hilf R., and Sporn
L.A. (1991). Photosensitized release of Von Willebrand Factor
from cultured human endothelial cells. Cancer Res 50:7765-7769
Freeman S.B., Hamaker R.C., Singer M.I., Pugh N., Garrett P. and
Ross D. (1990) Intraoperative radiotherapy of Head and Neck
cancer. Arch. Otolaryngol. Head Neck Surg.;116:165-168
Garcia M. (1855) Physiological observation on the human voice.
Proc. Roy. Soc. Lond; 7:399
Gilbert H and Kagan A.R. (1974) Recurrence patterns in squamous
cell carcinoma of the oral cavity, pharynx and larynx. J. Surg
Oncol.;6:357-380
Glick B. (1972) Bilateral carotid occlusive disease. Arch.
Pathol.;93:352-355
290
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Gluckman J.L. (1986) Photodynamic therapy for early squamous
cell cancer of the upper aerodigestive tract. Aust. N.Z. J.
Surg.;56:853-857
Gluckman J.L. (1979) Synchromous multiple primary lesions of the
upper aerodigestive system. Arch. Otolaryngol.;105:597-8
Gluckman J.L. (1991) Photodynamic Therapy for Head and Neck
Neoplasms. Otolaryngology Clinics of North America 24(6):1559-1567
Gluckman J.L. (1991) "Hematoporphyrin Photodynamic Therapy: Is
there truly a future in Head and Neck Oncology? Reflections on a
5 year experience." Laryngoscope. 101:36-41
Gomer C.J. (1991) Preclinical examination of first and second
generation photosensitizers used in photodynamic therapy.
Photochem. Photobiol 54(6) 1093-1107
Gomer C.J. Rucker N., and Murphree A.L. (1988) Preferential cell
photosensitivity following porphyrin photodynamic therapy. Canc.
Res. 40:4539-4542
Gomer C.J., Ferrario A., Murphree A.L. (1987) The effect of
localized porphyrin photodynamic therapy on the induction of
tumour metastasis. Br. J. Cancer;56:27-32
291
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Gomer C.J. and Dougherty T.J. (1979) Determination of (3H)- and
(14C)- hematoporphyrin derivative distribution in malignant and
normal tissue. Canc Res;39:146-151
Grahn M.F., DeJode M.L., Dilkes M.G., Ansell J.K., Onwu D.,
Maudsley J. And Williams N.S. (1996) Tissue photosensitiser
detection by low power remittance fluorimetery. Lasers in Medical
Science 12: In press
Grant W.E., Hopper C., Speight P.M., MacRobert A.J. and Bown
S.G. (1993) Photodynamic Therapy of malignant and premalignant
lesions in patients with "field cancerisation" of the oral
cavity. Journal of Laryngology and Otology 107:1140-1145
Grant W.E., Hopper C., MacRobert A.J., Speight P.M. and Bown
S.G. (1993) Photodynamic Therapy of Oral cancer:
photosensitisation with systemic aminolaevulinic acid. Lancet
342:147-148
Grant W.E , Speight P.M., MacRobert A.J., Hopper C. and Bown S.G
(1994) . Photodynamic therapy of normal rat arteries after
photosensitisation using disulphonated aluminium phthalocyanine
and 5-aminolaevulinic acid. Br.J.Cancer;70:72-78
Grant W.E., , Buonaccorsi G., Speight P.M., MacRobert A.J.,
Hopper C. And Bown S.G. (1995) The effect of photodynamic
therapy on the mechanical integrity of normal rabbit carotid
arteries. Laryngoscope;105:867-871292
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Gregorie H.B., Horger E.O., Ward J.L. et al. (1968)
Hematoporphyrin derivative fluorescence in malignant neoplasms.
Ann. Surg., 167:820
Harris A.H. and Smith R.R. (1960) Operative wound seeding with
tumour cells: its role in recurrences of head and neck cancer.
Ann.Surg;151(3):330-334
Hayward R.H. (1972) Atherosclerosis induced by radiation. Surg.
Clin. North Am.;52:359-366
Henderson B.W., Dougherty T.J. and Malone P.B. (1984) Studies on
the mechanism of tumour destruction by photoradiation therapy.
In: Doiron D.R., Gomer C.J. Eds. Porphyrin localisation and treatment of
tumours. New York: Alan R. Liss ; 604-12
Henderson B.W. and Fingar V.H. (1989) Oxygen limitation of
direct tumour cell killing during photodynamic tretament.
Photochem. Photobiol.;47:823-30
Henderson B.W. 1990. Probing the effects of photodynamic therapy
through in vivo-in vitro methods. In Photodynamic Therapy of
Neoplastic Disease (Edited by D.Kessel), Vol 1, p169-88. CRC
Press, Boca Raton, Ann Arbor, Boston.
293
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Henderson B.W., and Donovan J.M. (1989) Release of Prostaglandin
E2 from cells by Photodynamic Treatment in vivo. Canc Res.
49:6896-6900
Henderson B.W., Wadlow S.M., Mang T.S., Potter W.R., Malone
P.B., and Dougherty T.J. (1985) Tumour destruction and kinetics
of tumour cell death in two experimental mouse tumours following
photodynamic therapy. Canc. Res. 45:572-576
Henderson B.W and Dougherty T.J. (1992) How does photodynamic
therapy work? Photochem Photobiol 55(1):145-157
Herrera-Ornelas L., Petrilli N.J., Mittelman A. and Dougherty T.J.
(1986) Photodynamic therapy in patients with colorectal cancer.
Cancer;57:677-684
Holden H.B., McKelvie P. (1972) Cryosurgery in the treatment of
head and neck neoplasia. Brit. J. Surg;59(9):709-712
Holdiness M.R. (1991) Clinical pharmacokinetics of N-
Acetylcysteine. Clin. Pharmoacokinetics;20:123-134
Holm L E, Lundquist P G, Silversward C, Sobin A (1982)
Histological grading of malignancy in squamous cell carcinoma of
the oral tongue. Acta Otolaryngol 94:185-92
Hong A, Saunders M.I., Dische S., Grosch E., Fermont D., Ashford
R.F.U. and Maher E.J. (1990) An audit of Head and Neck cancer294
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
treatment in a regional centre for radiotherapy and oncology. Clin
Oncol 2:130-137
Hsiang Y.N., Crespo M.T., Machan L.S., Bower R.D. and Todd M.E.
(1994) Photodynamic therapy for atherosclerotic stenoses in
Yucatan miniswine. Can. J. Surg.;37(2):148-152
Huvos A.G., Leaming R.H. and Moore O.S. (1973)
Clinicopathological study of the resected carotid artery-
analysis of 64 cases. Am. J. Surg.;126:570-574
Jacobs A. (1962) Post-cricoid carcinoma in patients with
pernicious anaemia. Br. Med. J.;2:91-2
Jain R.K. (1987) Transport of molecules in the tumour
interstitium: a review. Cancer Res. 47:3039-3051
Jamieson C., Richter A. and Levy J.G. (1993) Efficacy of
Benzoporphyrin Derivative, a photosensitiser, in selective
destruction of leukaemia cells using murine tumour model. Exp.
Hematol. 21(5):629-34
Jelliffe A M (1986) Hodgkin’s disease and non-Hodgkin’s
lymphomas. In:Hope-Stone H F (ed) Radiotherapy in Clinical
Practice. London, Butterworths, pp.177-202
295
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Jesse R.H., Barklay H.T., Lindberg R.D. and Fletcher G.H. (1970)
Cancer of the oral cavity. Is elective neck dissection
beneficial? Am. J. Surg.120:505-508
Jesse R.H. and Lindberg R.D. (1975) The efficacy of combining
radiation therapy with a surgical procedure in patients with
cervical metastasis from squamous carcinoma of the oropharynx
and hypopharynx. Cancer;35:1163-1166
Jesse R.H. and Fletcher G.H. (1977) Treatment of the neck in
patients with squamous cell carcinoma of the head and neck.
Cancer;39:868-872
Jirsa M., Pouckova J., Dolezal J., Jospisil J. and Jirsa M.
(1991). Hyperbaric oxygen and photodynamic therapy i tumour
bearing nude mice. Eur J. Cancer 27:109.
Johansen L.V., Overgaard J., Overgaard M., Birkler N., Fisker A.
(1990) Squamous cell carcinoma of the oropharynx: An analysis of
213 consecutive patients scheduled for primary radiotherapy.
Laryngoscope;100:985-990
Johns T.W.P. (1947) A comparison of suture and non-suture
methods for anastomosis of veins. Surg. Gynae, Obst.;84:939-945
Johnson J.T., Barnes E.L., Myers E.M., Schramm V.L., Borochovitz
D. and Sigler B.A. (1981) The extracapsular spread of Tumours in
Cervical Node Metastasis. Arch Otolaryngol 107:725-729 296
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Johnston W.D. and Ballantyne A.J. (1977) Prognostic effect of
tobacco and alcohol use in patients with oral tongue cancer. Am.
J. Surg;134:444-447
Jones R.K. (1951) Increased intracranial pressure following
radical neck surgery. Arch. Surg. 63:599-603
Joyce L.G and McQuarrie D.G. (1976) Application of contemporary
reconstructive techniques in head and neck surgery for anterior
oral facial cancers. Surgery;80:373-378
Kaye A.H., Morstyn G. and Brownbill D. (1987) Adjuvant high dose
photoradiation therapy in the treatment of malignant glioma: A
phase 1-2 study. J. Neurosurg.;46:500-505
Keller G.S., Doiron D.R. and Fisher G.U. (1985) Photodynamic
Therapy in Otolaryngology- Head and Neck Surgery. Arch
Otol;111:758-761
Kelly J.F. and Snell M.E. (1976) Hematoporphyrin derivative: a
possible aid in the diagnosis and therapy of carcinoma of the
bladder. J. Urol. 115:150-151
Kalnins I.K., Leonard A.G., Sako K., Razack M.S. and Shedd D.P.
(1977) Correlation between prognosis and degree of lymph node
involvement in carcinoma of the oral cavity. Am. J. Surg;134:450-
454297
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Kennedy J.C. and Pottier R.H. (1992) Endogenous protoporphyrin
1X, a clinically useful photosensitiser for photodynamic
therapy. J. Photochem, Photobiol B:Biol 14(4):275-292
Kennedy J.T., Krause C.J. and Loevy S. (1977) The importance of
tumour attachment to the Carotid Artery. Arch Otolaryngol;103:70-73
Kessel D., (1986) , Porphyrin-lipoprotein association as a
factor in porphyrin localisation. Cancer Lett., 33,183-88.
Kim R.Y., Hu L.K., Foster B.S., Gragoudas E.S. and Young L.H.
(1996) Photodynamic therapy of pigmented choroidal melanomas of
greater than 3mm thickness. Opthalmology;103(12):2029-36
Kinsey J.H., Cortese D.A and Neel H.B. (1983) Thermal
considerations in murine tumour killing using hematoporphyrin
derivative phototherapy. Canc. Res.;43:1562-1567
Kubler A., Finley R.K. (3rd), Born I.A. and Mang T.S. (1996)
Effect of photodynamic therapy on the healing of a rat skin flap
and its implications for head and neck reconstructive surgery.
Lasers Surg. Med.;18(4):397-405
Kumar P.P., Good R.R., and Epstein B.E. (1987) Relationship of
dose to local control in advanced stage 3 and 4 head and neck
cancer treated by surgery and postoperative radiotherapy. Am. J.
Clin. Oncol.;10(3):240-242298
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Kulapaditharom B. and Boonkitticharoen V. (1996) Photodynamic
therapy in the treatment of head and neck cancers: a 2 year
experience. J. Med. Assoc. Thai.;79(4):229-35
Larsen D.L., Kroll S., Jaffe N., Serure A and Goepfert H. (1990)
Long term effects of radiotherapy in childhood and adolescence.
Am. J. Surg.;160:348-51
Leonard J.R., and Beck W.L. (1970) Hematoporphyrin fluorescence:
an aid in diagnosis of malignant neoplasms. Laryngoscope++++++++++
+++++++++
Lin C.W. (1991) Selective localisation of photosensisitsers in
tumors: a review of the phenomenon and possible mechanisms. In:
Photodynamic therapy of neoplastic disease. Boca Raton, Fla: CRC press;
1990:79-101
Lin C.W. (1991) Photodynamic Therapy of Malignant Tumours -
Recent Developments. Cancer Cells;3(11):437-444
299
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Lingeman R.E., Helmus C., Stephens R. and Ulm J. (1977) Neck
dissection: radical or conservative. Ann. Otol;86:737-744
Lipson R.L. and Baldes E.J. (1960). The photodynamic properties
of a particular hematoporphyrin derivative. Arch Dermatol;82:508
Lipson R.L, Baldes E.J. and Olsen A.M. (1961) Haematoporphyrin
Derivative: a possible new aid for endoscopic detection of
malignant disease. J. Thoracic. Cadiovasc. Surg.;42:623-629
Luo Y., Chang C.K. and Kessel D. (1996) Rapid initiation of
apoptosis by photodynamic therapy. Photochem Photobiol
(USA);63(4):528-34
Ma L., Moan J. and Berg K. Evaluation of a new photosensitiser
meso-tetra-hydroxyphenyl-chlorin for use in photodynamic
therapy: a comparison of its photobiological properties with
those of two other photosensitisers. Int. J. Cancer, 57:883-888
(1994)
Mackenzie M. (1871) Essay on growths of the larynx. J.& A.
Churchill, London.
Mackie R.W.Jr., Vincent G.M., Fox J., Orme E.C., Hammond E.H.,
Chang-Zong C. and Johnson M.D. (1991) In Vivo canine coronary
artery laser irradiation: Photodynamic therapy using
300
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
dihaematoporphyrin Ether and 632nm laser. A safety and dose-
response relationship study. Lasers Surgery Med. 11(6):535-544
Mang T.S., McGinnis C., Liebow C., Nseyo U.O., Crean D.H. and
Dougherty T.J. (1993) Fluorescence detection of tumours. Early
diagnosis of microscopic lesions in preclinical studies.
Cancer;71(1):269-76
Mantravardi R.V.P., Skolnik E.M., Haas R.E. and Applebaum E.L.
(1983) Patterns of cancer recurrence in the postoperatively
irradiated neck. Arch. Otolaryngol;109:753-756
Manyak M.J., Smith P.D., Harrington F.S., Steinberg S.M.
Glatstein E. and Russo G. (1988) Protection against
dihaematoporphyrin photosensitivity. Photochem. Photobiol.;47:823-
850
Marks S.C., Jaques D.A., Hirata R.M. and Saunders J.R. (1990)
Blindness following bilateral radical neck dissection. Head Neck
Surg.;12:342-345
Martin H., Del Valle B., Ehrlich H., and Cahan W.G. (1951) Neck
Dissection. Cancer ;4:441-499
McCarthy S A, Turnbull F M (1981) The controversy of
branchchogenic carcinoma. Arch Otolaryngol 107:570-2
301
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
McCaughan J.S. (1984) Photoradiation of malignant tumors
presensitized with haematoporphyrin derivative. In: Porphyrin
localisation and treatment of tumors, Pubs. Alan R. Liss Inc.
McLear W.P and Hayden N.I. (1989) Prevebntion of cutaneous
phototoxicity in photodynamic therapy. Am. J. Otolaryngol.;10:92-98
McQuarrie D.G., Adams G.L. and Rao Y. (1986) Cervical
lymphatics:Decisions and Variations in managing existing or
potential cervical lymph node metastases. In:Head and Neck
Cancer. Eds. McQuarrie D.G., Adams G.L., Shons A.R. and Browne
G.A. Year Book Medical Publishers Inc. Chicago;145-177
McReady R.A., Miller S.k., Hamaker R.C., Singer M.I., and Herod
G.T. (1989) What is the role of carotid arterial resection in
the management of advanced cervical cancer? J. Vasc. Surg. 10:274-80
Mendelsohn B.C., Woods J.E., and Beahrs O.H. (1976) Neck
dissection in the treatment of carcinoma of the anterior two
thirds of the tongue. Surg. Gynecol. Obstet. ;143:75-80
Mendelson B.C., Hodgkinson D.J. and Wood J.E. (1977) Cancer of
the oral cavity. Surg. Clin. North Am;57:585-596
Merino O.R., Lindberg R.D. and Fletcher G.H. (1977) Analysis of
distant metastases from squamous cell carcinoma of the upper
respiratory and digestive tracts. Cancer;40:145-151302
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Mew D., Lum V., Wat C.K., Towers G.H.N., Sun C-H.C., Walter
R.J., Wright W., Berns M.W., Levy J.G. (1985) Ability of
specific monoclonal antibodies and conventional antisera
conjugated to hematoporphyrin to label and kill selected cell
lines subsequent to light activation.: Canc. Res. 45;4380-4386
McCaughan J.S. (1984) Photoradiation of malignant tumours
presensitized with Hematoporphyrin Derivative. In: Porphyrin
Localisation and Treatment of Tumours, Alan R.Liss Publisher.
P805-827
Mlkvy P., Messman H., Pauer M., Stewart J.C., Millson C.,
Macrobert A.J. and Bown S.G. (1996) Distribution and
photodynamic effects of meso-tetrahydroxyphenylchlorin (mTHPC)
in the pancreas and adjacent tissues in the Syrian golden
hamster. Br J. Cancer 73(12):`1473-1479
Moan J., and Sommer S., (1985), Oxygen dependence of the
photosensitizing effect of Haematoporphyrin derivative in NHIK
3025 cells. Cancer lett 14:291-6
Moan J., Johannessen J.V., Christensen T., Esperick T. and
McGhie J.B. (1982) Porphyrin sensitized photoinactivation of
human cells in vitro. Am. J. Path.;109:184
Moan J. (1990) Properties for optimal PDT sensitisers. J. Photochem
Photobiol 5(3-4):521-4303
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Monnier Ph., Savary M., Fontolliet Ch., Wagnieres G., Chatelain
A., Cornaz P., Depeursinghe Ch. and Van Den Burgh H. (1990)
Photodetection and Photodynamic Therapy of "Early SCC of the
pharynx, oesophagus and tracheobronchial tree." Lasers in Medical
Science 5:149-169
Moore O., and Baker H.W. (1955) Carotid artery ligation in
surgery of the Head and Neck. Cancer 8(4) 712-726
Mukhtar H., Agarwal R., Athar M., Lewen R.L., Elmets C.A. and
Bickers D.R. (1991) Photodynamic Therapy of murine skin tumours
using Photofrin2. Photodermatol., Photoimmunol., Photomed;8(4):169-75
Muller P.J. and Wilson B.C. (1995) Photodynamic therapy for
recurrent supratentorial gliomas. Semin. Surg. Oncol.;11(5):346-
354
Nahabedian M.Y., Cohen R.A., Contino M.F., Terem T.M., Wright
W.H., Berns M.W., Wile A.G. (1988) Combination cytotoxic
chemotherapy with cisplatin or doxorubicin and photodynamic
therapy in murine tumours. J.Natl.Cancer.Inst.;80(10):739-743
304
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Nambisan R.N., Kararkousis C.P.,. Holyoke E.D. and Dougherty
T.J. (1988) Intraoperative photodynamic therapy for
retroperitoneal sarcomas. Cancer;61:1248-1252
Nelson J.S., Liaw L-H., and Berns M.W. (1987) Tumour destruction
in Photodynamic therapy. Photochem. Photobiol 46(5):829-835
Nelson J.S., Liaw L-H., Orenstein A., Roberts W.G., and Berns
M.W. (1988) Mechanism of tumour destruction following
photodynamic therapy with Hematoporphyrin derivative , chlorin
and Phthalocyanine. J.Natl Cancer Inst.;80(20):1599-1605
Nyamekye I., Buonaccorsi G., McEwan J., MacRobert A., Bown S. And
Bishop C. (1996) Inhibition of intimal hyperplasia in balloon
injured arteries with adjunctive phthalocyanine sensitised
photodynamic therapy. Eur. J. Endovasc. Surg.;11(1):19-28
O'Brien P.H., Carlso R., Steubner E.A. and Stalet C.T. (1971)
Distant metastases in epidermoid cell carcinoma of the head and
neck. Cancer;27:304-307
Ofner J.G., Bartl B., Konig S. And Thumfart W.F. (1996)
Photodynamic therapy in selected cases at the ENT Clinic,
Innsbruck, Austria. Photochem. Photobiol B (Switz);36(2):185-7
Okunaka T., Kato H., Konaka C., Sakai H., Kawabe H. and Aizawa K
(1992) A comparison between argon-dye and excimer-dye laser for
305
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
photodynamic effect in transplanted mouse tumour. Jpn.J. Cancer
Res.;83(2):226-231
Olcott C., Fee W.E., Enzmann D.R. and Mehigan J.T. (1981)
Planned approach to malignant invasion of the Carotid Artery Am.
J. Surg .;142:123-127
306
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Orenstein A., Kostenich G., Roitman L., Shechtman Y., Kopolovic
Y., Ehrenberg B. and Malik Z. (1996) A comparative study of
tissue distribution and photodynamic therapy selectivity of
chlorin E6, Photofrin 2 and ALA-induced protoporphyrin 9 in a
colon carcinoma model. Br. J. Cancer 73:937-944)
Orteu P., LaMuraglia G.M., Roberts W.G., Flotte T.J. and Hasan
T. (1992) Photodynamic therapy of arteries. A novel approach for
treatment of experimental intimal hyperplasia. Circulation; 85:1189-
1196
Pass H.I., Evans S., Matthews W.A., Perry R., Venzon D., Roth
J.A. and Smith P. (1991) Photodynamic therapy of oncogene
transformed cells. J.Thorac Cardiovasc Surg;101:795-9
Pass H.I. (1993) Photodynamic therapy in clinical oncology:
mechanisms and clinical use. J. Natl Cancer Inst 85:443-456
Patrice T., Foultier M.T. and Yactayo S. (1990) Endoscopic
photodynamic therapy with hematoporphyrin derivative in
gastroenterology. J. Photochem Photobiol B;6:157-165
Paxton J.W. (1995) The allometric approach for interspecies
scaling of pharmacokinetics and toxicity of anti-cancer drugs.
Clin. Exp. Pharmocol. Physiol.;22:851-854
307
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Pearlman N.W. (1979) Treatment outcome in recurrent Head and
Neck cancer. Arch. Surg.;114:39-42
Peltier L.F., Thomas L.B., Crawford T.H., Barclay M.B. and
Kremer A.J. (1951) The incidence of distant metastases among
patients dying of Head and Neck cancer. Surgery;30:827-833
Peng Q., Moan J., Kongshaug M., Evensen J.F., Anholt H. and
Rimington C. Sensitizer for photodynamic therapy of cancer: a
comparison of the tissue distribution of Photofrin 2 and
Aluminium Phthalocyanine tetrasulfonate in nude mice bearing a
human malignant tumour. Int. J. Cancer;48:258-264
Perry R.R., Smith P.D., Evans S. and Pass H.I. (1991)
Intravenous vs Intraperitoneal sensitizer: Implications for
intraperitoneal photodynamic therapy. Photochem.
Photobiol;53(3):335-340
Policard A. (1924) Etudes sur les aspects offert par des tumeurs
experimentales examinees a al lumiere de Wood.
C.R.Soc.Biol.;91:1423-8
Poate T.W.J., Dilkes M.G. and Kenyon G.S. (1996) Use of
photodynamic therapy for the treatment of squamous cell
carcinoma of the soft palate. Br. J. Oral and maxillofacial
surgery;34:66-68
308
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Pope A.J, Bown S.G. (1991) The morphological and functional
changes in rat bladder following photodynamic therapy with
pthalocyanine photosensitization. J.Urol.;145:1064-70
Potter W.R., Mang T.S. and Dougherty T.J. (1987) The Theory of
photodynamic therapy dosimetry: consequences of photodestruction
of sensitizer. Photochem Photobiol +++++++++++++++++++++++++
Powell R. and Robin P.E. (1983) Cancer of the head and neck: the
present state. In: Head and Neck Cancer, Eds. P. Rhys-Evans,
P.E.Robin and J.W.L. Fielding, p3-16, Tunbridge Wells press,
Castle House Publications.
Power D. (1918) On cancer of the tongue. Br.J.Surg;6:336
Price L. (1934) Metastases in squamous cancer Am. J. Cancer;22:1-16
Raab O. (1900) Uber die Wirkung Fluorescierenden Stoffe auf
Infusorien . Z.Biol;39:524-46
Rao Y. and Levitt S. (1986) General Principles of radiation
therapy for Head and Neck malignancy. In: Head and Neck Cancer, Eds
McQuarrie D.G., Adams G.L., Shons A.R. and Brown G.A., Year Book
Medical Publishers, Chicago 126-128
Razack M.S., Silapasvang S., Sako K. et al (1978) Significance
of the site and nodal metastases in squamous cell carcinoma of
the epiglottis. Am. J. Surg;136:520-24309
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Razack M.S., Sako K. and Kalnins I. (1978) Squamous cell
carcinoma of the pyriform sinus. Head Neck Surg;1:31-34
Razmussen-Taxdal D.S., Ward G.E. and Figge F.H. (1955).
Fluorescence of human lymphatic and cancer tissue following high
doses of intravenous haematoporphyrin. Cancer;8:78-81
Reddy D.G. and Rao U.K. (1957) Cancer of the mouth in coastal
Andhra due to smoking cigars with the burning end inside the
mouth. Ind. J. Med;11:791
Reed M.W.R., Mullins A.P., Anderson G.L., Miller F.N. and Wieman
T.J. (1989) The effect of photodynamic therapy on tumour
oxygenation. Surgery;106:94-9
Ris H-B, Altermatt H.J., Inderbitzi R., Hess R., Nachbur B.,
Stewart J.C.M., Wang Q., Lim C.K., Bonnett R., Berenbaum M.C.
and Althaus U. (1991) Photodynamic therapy with Chlorins for
diffuse malignant mesothelioma: initial clinical results. Br. J.
Cancer 64(6):1116-1120
Ris H-B., Altermatt H.J., Nachbur B., Stewart J.C.M., Wang Q.,
Lim C.K., Bonnett R. and Althaus U. (1993) Effect of drug-light
interval on photodynamic therapy with meta-
tetrahydroxyphenylchlorin in malignant mesothelioma. Int. J. Cancer
53:141-146
310
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Ris H-B., Altermatt H.J., Stewart J.C.M., Schaffner T., Wang Q.,
Lim C.K., Bonnett R. and Althaus U. (1993) Photodynamic therapy
with m-THPC in vivo optimisation of the therapeutic index. Int. J.
Cancer 55:245-249
Sanderson D.R., Fontana R.S. and Lipson R.L. Haematoporphyrin as
a diagnostic tool. A preliminary report of new techniques.
Cancer;30:1368
Savary J.F., Monnier P., Fontolliet C., Mizeret J., Wagnieres
G., Braichotte D. and Van den Bergh H. (1997) Photodynamic
therapy for early squamous cell carcinomas of the esophagus,
bronchi and mouth with m-Tetra(hydroxyphenyl)chlorin. Arch Otol
Head and Neck Surg.;123:162-88
Schuller D.E., McCaughan J.S., Rock R.P. (1985) Photodynamic
Therapy in Head and Neck Cancer. Arch Otol 111:351-355
Selman S.H., Kreimer-Bernbaum M., Klaunig J.E., Goldblatt P.J.,
Kreck R.W. and Britton S.. (1984) Blood flow in transplantable
bladder tumours treated with Hematoporphyrin Derivative and
light.
Selman S.H., Kreimer-Birnbaum M., Chaudhuri K., Garbo G.M.,
Seaman D.A., Keck R., Ben-Hur E., and Rosenthal I.(1986)
Photodynamic treatment of transplantable bladder tumours in
rodents after pretreatment with chloraluminium
tetrasulfophthalocyanine. J.Urol.;136:141-145311
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Schweizer V.G. (1990) Photodynamic Therapy for -related
mucocutaneous Kaposi's sarcoma. Otolaryngology Head and Neck Surgery
102(6):639-649
Schweizer V.G. Bologna S. and Batra S.K. (1993) Photodynamic
Therapy for treatment of esophageal cancer: a preliminary
report. Laryngoscope 103:669-703
Shah J.P. Cendon R.A., Farr H.W. (1977) Carcinoma of the oral
cavity - factors affecting treatment failure at the primary site
and neck. Am. J. Surg.;132:504-7
Shah J.P. (1990) Patterns of cervical lymph node metastasis from
squamous carcinoma of the upper aerodigestive tract. Am. J. Surg.
160:405-9
Shikowitz M.J., Galli R., Bandyopadhyay D., Hoory S. (1989)
Biodistribution of Indium 111-labelled dihematoporphyrin ether
in papillomas and body tissues. Arch Otolaryngol. Head Neck Surg.
115:845-847
Singh G., Wilson B.C., Sharkey S.M., Browman G.P. and Deschamps
P. (1991) Resistance to photodynamic therapy in radiation
induced fibrosarcoma-1 and chinese hamster ovary-multi-drug
resistant cells in vitro. Photochem. Photobiol.;54(2):307-312
312
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Sloan D., Goepfert H., (1991) Conventional Therapy of Head and
Neck cancer. In: Hematology/Oncology Clinics of North America, Ed. Vokes
E.V. W.B.Saunders Inc, Philadelphia.5:601-626
Soutar D.S., Scheker L.R., Tanner N.S.B. and McGregor I.A.
(1983) The radial forearm flap: a versatile method for intra-
oral reconstruction. Br. J. Plast. Surg.;36:1-
Spiro R.H., Alfonso A.E., Farr H.W. and Strong E.W. (1974)
Cervical node metastases from epidermoid carcinoma of the Oral
cavity and oropharynx. Am.J.Surg;128:562-567
Stevenson R.S. (1946) Morell Mackenzie, The story of a Victorian
Tragedy. William Heinemann, London
Stewart J.C.M.(1994) meta-tetra(hydroxyphenyl)-chlorin (mTHPC):
a second generation photosensitiser for photodynamic therapy: a
review. In: New approaches to cancer treatment. Unsaturated
lipids and ohotodynamic therapy., D.F.Horrobin Ed., Edinburgh:
Churchill Livingstone p109-120
Strasnick B, Moore D M, Abemayor E, Julliard G, Fu Y S (1990)
Occult primary tumors. The management of isolated submandibular
lymph node metastases. Arch Otolaryngol Head Neck Surgery
116:173-6
313
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Strong E. (1969) Preoperative radiation and radical neck
dissection. Surg. Clin. North Am;49(2)271-276
Svanberg K, Andersson T. and Killander D (1992) Photodynamic
therapy of human skin malignancies and laser-induced
fluorescence diagnostics utilizing Photofrin and d-amino-
laevulinic acid. In. Photodynamic therapy and Biomedical lasers. Spinelli
P., Dal Fante M., Marchesini R. (Eds). Exerpta Medica, London
436-440
Svanberg K., Andersson T., Killander D., Wang I., Stenram U.,
Andersson-Engels S., Berg R., Johanssen J. and Svanberg S.
(1994) Photodynamic therapy of non-melanoma malignant tumours
of the skin using topical delta-amino levulinic acid
sesitisation and laser irradiation. Br. J. Dermatol.;130(6):743-51
Takemura T., Ohta N., Nakajima S., and Sakata I. (1991). The
mechanism of photosensitization in photodynamic therapy:
phosphorescence behaviour of porphyrin derivatives in saline
solution containing human serum albumin. Photochem Photobiol
54(5):683-88
Thompson L.W. (1989) Head and Neck Cancer: Early detection.
Semin. Surg. Oncol;5(3):168-75
Thomson S.C. (1939) The history of cancer of the larynx. J.
Laryngol. Otol;54:61
314
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Tralau C.J., MacRobert A.J., Coleridge-Smith P.D., Barr H., and
Bown S.G. (1987) Photodynamic Therapy with phthalocyanine
sensitisation: quantitative studies in a transplantable rat
fibrosarcoma. Br J. Cancer 55:389-395
Tralau C.J., Young A.R., Walker N.P.J., Vernon D.I., MacRobert
A.J., Brown S.B. and Bown S.G. Mouse skin photosensitivity with
dihaematoporphyrin ether (DHE) and aluminium sulphonated
phthalocyanine (AISPc): a comparative study. Photochem
Photobiol;49(3):305-312
Trotter W., (1913) Operative treatment of malignant disease of
the mouth and pharynx. Lancet 1:1075
Van Geel I.P.J., Oppelaar H., Oussoren Y.G., Van Der Valk M.A.
and Stewart F.A (1995) Photosensitising efficacy of mTHPC-PDT
compared to Photofrin-PDT in the RIF1 mouse tumour and normal
skin. Int. J. Cancer 60(3):388-394
Van Hillegersberg R., Hekking-Weijma J.M., Wilson J.H.,
Edixhoven-Bosdijk A. and Kort W.J. (1995) Adjuvant
intraoperative photodynamic therapy diminishes the rate of local
recurrence in a rat mammary tumour model. Br. J.
Cancer;71(4):733-737
Vaughan C.W., Homburger F., Shapshay S.M., Soto E. And Bernfield
P. (1980) Carcinogenesis of the upper aerodigestive tract.
Otolaryngol. Cli. North Am.;13:405-12315
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Vernon D.I., Holroyd J.A., Stribbling S.M. and Brown S.B. (1995)
The quantitative determination of Photofrin and
Polyhaematoporphyrin in plasma: pitfalls and inaccuracies. J.
Photochem. Photobiol B 27(3):209-17
Virchow R.L.K. (1858) Die Cellular Pathologie in Ihren
Begrundung auf Physiologische und Pathologische Gewebelhre A.
Hirschwald, Berlin 1858
Vokes E.E., Weischelbaum R.R., Lippman S.M. and Hong W.K. (1993)
Head and Neck Cancer. New England Journal of Medicine 328(3):184-194
Von Tappenier H. and Jesionek A. (1903) Therapeutische Versuche
mit fluorescierenden Stoffen. Munch. Med. Wochenschr;47:2042-4
Waldow S.M., Henderson B.W., Dougherty T.J. (1987) Hyperthermic
potentiation of photodynamic therapy employing Photofrin I and
II Comparison of results using 3 animal tumour models. Lasers
Surgery Med. 7(1):12-22
Wan S., Parrish J.A., Anderson R.R. and Madden M. (1981)
Transmittance of non ionizing radiation in human tissue.
Photochem Photobiol.;34:679-681
Wang Q., Ris H.B., Ris H.B., Altermatt H.J., Reynolds B.,
Stewart J.C., Bonnett R. and Lim C.K. (1993) Determination of316
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
5,10,15,20 tetra-(m-Hydroxyphenyl)chlorin in human plasma by
high performance liquid chromatography. Biomedical
Chromatography;7(1):45-7
Ward G.E. and Hendrick J.W. Tumours of the Head and Neck.
Williams and Wilkins Co., Baltimore.
Ward G.E., Edgerton M.T., Chambers R.G. and McKee D.M. (1959)
Cancer of the oral cavity and pharynx and results of treatment
by means of a composite operation (in continuity with radical
neck dissection). Ann.Surg;150:202-220
Weishaupt K.R., Gomer C.J. and Dougherty T.J. (1976)
Identification of singlet oxygen as the cytotoxic agent in
photoinactivation of a murine tumour. Canc. Res.36:2326-2329
Weissler M.C., Weigel M.T., Rosenmann J.G., and Silver J.R.
(1989) Treatment of the clinically negative neck in advanced
cancer of the head and neck. Arch Otolaryngol Head Neck Surg.
115(6):691-694
Wei W.I., Lam K.H., Ho C.M., Shame J.S.T and Lau S.K. (1990)
Efficacy of radical neck dissection for the control of cervical
metastasis after radiotherapy for nasopharyngeal carcinoma. Am. J.
Surg;160(4):439-442
317
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Wei W.I., Ho C.M., Wong M.P., Ng W.F., Lau S.K. and Lam K.H.
(1992) Pathological basis of surgery in the management of
postradiotherapy cervical metastasis in nasopharyngeal
carcinoma. Arch. Otolaryngol. Head Neck Surg. 118(9):923-929
Weiman T.J. and Fingar V.H. (1992) Photodynamic Therapy. Surgical
Clin. North. Am,.;72:609-622
Wenig B.L., Kurtzman D.M. and Grossweiner L. (1990)
Photodynamic Therapy in the treatment of sqyuamous cell
carcinoma of the Head and Neck. Arch. Otolaryngol. Head and Neck
Surg.;116:1267-1270
Werning J.W., Stepnock D.W., Jafri A., Megerian C.A., Antunez
A.R. and Zaidi S.I. (1995) Metoclopramide enhances the effect of
photodynamic therapy on xenografted human squamous cell
carcinoma of the head and neck. Arch Otol. Head and Neck
Surg.;121(7):783-9
West C.M., West D.C., Kumar S., and Moore J.V. (1990) A
comparison of the sensitivity to photodynamic treatment of
endothelial and tumour cells in different proliferative states.
Int. J. Radiat. Biol.;58(1):145-156
Whelpton R., Michael-Titus A., Jamdar R.P., Abdillah K. and
Grahn M.F. (1996) Distribution and excretion of radiolabelled
temoporphyrin in a murine tumour model. Photochemistry and
Photobiology; 63(6):885-891318
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
Wike-Hooley L., Haveman J., and Reinhold H.S., (1984), The
relevance of tumour Ph to the treatment of malignant disease.
Radiother Oncol.,2:343-366
Wilson B.C., Jeeves W.P. and Lowe D.M. (1985) In vivo and post
mortem measurements of the attenuation spectra of light in
mammalian tissues. Photochem. Photobiol.;42(2):153-162
Wizenburg M.J., Bloedorn F.G., Weiner S. and Gracia J. (1972)
Treatment of lymph node metastases in head and neck cancer. A
radiotherapeutic approach. Cancer;29:1455-1462
Wolford S.T., Novicki D.L. and Kelly B. (1995) Comparative skin
phototoxicity in mice with two photosensirtising drugs:
benzoporphyrin derivative monoacid ring A and porfimer sodium
(Photofrin). Fundam. Appl. Toxicol;25(1):52-6
Wooten R.S. Smith K.C., Ahlquist D.A., Muller S.A., Balm R.K.
(1988) Prospective study of cutaneous phototoxicity after
systemic hematoporphyrin derivative. Lasers Surg. Med.;8(3):294-300
Wurman L.H., Adams G.L. and Myerhoff W.L. (1975) Carcinoma of
the lip. Am.J.Surg;130:470-474
Zalar G.L., Pho-Fitzpatrick M., Krohn D.L., Jacobs R. and Harber
L.C. (1977) Induction of drug photosensitisation in man after
319
THE EFFICACY AND SAFETY OF ADJUNCTIVE INTRAOPERATIVE PHOTODYNAMIC THERAPY IN REDUCING THE LOCAL
RECURRENCE RATE OF TUMOUR AFTER RADICAL NECK DISSECTION
parenteral exposure to haematoporphyrin. Arch. Dermatol.;113:1392-
1397
Zhao F.Y., Zhang K.H., Jiang F., and Wu M.J. (1991) Photodynamic
Therapy for Treatment of cancers in Oral and Maxillofacial
regions: a long term follow up study in 72 complete remission
cases. Lasers in Medical Science 6:201204
Zieske L.A., Johnson J.T., Myers E.N., and Thearle P.B. (1986)
Squamous Cell Carcinoma with positive margins-Surgery and
Postoperative irradiation. Arch Otol Head Neck Surg.;112(8):863-6
320





























