Embed Size (px)
Citation preview
The role of photodynamic therapy „PDT… physicsTimothy C. Zhua� and Jarod C. FinlayDepartment of Radiation Oncology, University of Pennsylvania, Philadelphia, Pennsylvania 19104
�Received 14 April 2008; revised 7 May 2008; accepted for publication 8 May 2008;published 16 June 2008�
Photodynamic therapy �PDT� is an emerging treatment modality that employs the photochemicalinteraction of three components: light, photosensitizer, and oxygen. Tremendous progress has beenmade in the last 2 decades in new technical development of all components as well as understand-ing of the biophysical mechanism of PDT. The authors will review the current state of art in PDTresearch, with an emphasis in PDT physics. They foresee a merge of current separate areas ofresearch in light production and delivery, PDT dosimetry, multimodality imaging, new photosensi-tizer development, and PDT biology into interdisciplinary combination of two to three areas. Ulti-mately, they strongly believe that all these categories of research will be linked to develop anintegrated model for real-time dosimetry and treatment planning based on biologicalresponse. © 2008 American Association of Physicists in Medicine. �DOI: 10.1118/1.2937440�
Key words: PDT, spectroscopy, implicit dosimetry, explicit dosimetry, dynamic process
I. INTRODUCTION
Photodynamic therapy �PDT� is an emerging cancer treat-ment modality based on the interaction of light, a photosen-sitizing drug, and oxygen.1 PDT has been approved by theU.S. Food and Drug Administration for the treatment of mi-croinvasive lung cancer, obstructing lung cancer, and ob-structing esophageal cancer, as well as for premalignant ac-tinic keratosis and age-related macular degeneration. Studieshave shown some efficacy in the treatment of a variety ofmalignant and premalignant conditions including head andneck cancer,2,3 lung cancer,4–6 mesothelioma,7 Barrett’sesophagus,8,9 prostate,10–12 and brain tumors.9,13–15 Unlike ra-diation therapy, PDT uses nonionizing radiation and can beadministered repeatedly without cumulative long-term com-plications since it does not appear to target DNA.
There has been tremendous progress made in the last 2decades in new technologies and in understanding of thebasic biophysical mechanisms of PDT. The most importantquestion to be answered is: “What determines PDT efficacyfor a particular patient, photosensitizer, and treatment proto-col?” Answering this question will require a unified under-standing of the interactions of the three basic components:light, photosensitizer, and tissue oxygenation. We have cat-egorized the current basic research in PDT into five areas: �1�light sources, light transport, and light delivery in tissue; �2�PDT dosimetry; �3� optical and anatomic imaging; �4� newphotosensitizers; and �5� PDT biology. Among these, the de-velopment of new photosensitizers and PDT biology is tra-ditionally considered outside of the realm of PDT physicsand will only be briefly described for completeness. All fiveareas are linked by a quantitative understanding of the dy-namic processes involved in the photochemical interactionthat drives PDT. In the next section, we will describe these
areas separately.3127 Med. Phys. 35 „7…, July 2008 0094-2405/2008/35„7…/3
II. THE PROBLEMS IN CLINICAL PDT
II.A. Modeling the dynamic process of PDT
Photodynamic therapy is inherently a dynamic process.There are three principal components: photosensitizer, light,and oxygen, all of which interact on time scales relevant to asingle treatment. The distribution of light is determined bythe light source characteristics and the tissue optical proper-ties. The tissue optical properties, in turn, are influenced bythe concentration of photosensitizer and the concentrationand oxygenation of the blood. The distribution of oxygen isaltered by the photodynamic process, which consumes oxy-gen. Finally, the distribution of photosensitizer may changeas a result of photobleaching, the photodynamic destructionof the photosensitizer itself. To account for these interac-tions, a dynamic model of the photodynamic process is re-quired.
At the most fundamental level, the photodynamic processdepends on the photosensitizer molecule itself. Figure 1shows the energy level, or Jablonski, diagram for a typicaltype-II photosensitizer. The photochemical reaction is initi-ated by the absorption of a photon of light by a photosensi-tizer molecule in its ground state �S0�, promoting it to anexcited state �S1�. Both this state and the ground state arespectroscopic singlet states. One essential property of a goodphotosensitizer is a high intersystem crossing �ISC� yield,i.e., a high probability of transition from S1 to an excitedtriplet state �T1�. In the T1 state, the photosensitizer cantransfer energy to molecular oxygen �3O2�, exciting it to itshighly reactive singlet state �1O2�. The details of this energytransfer process are beyond the scope of this article but havebeen an area of active study.16
Two approaches have been used to study PDT dynamics.First, a microscopic model takes into account diffusion ofoxygen and photosensitizer from blood vessels and can de-termine the singlet oxygen concentration in cells microscopi-
cally. Foster et al. were the first to propose such a quantita-3127127/10/$23.00 © 2008 Am. Assoc. Phys. Med.

3128 T. C. Zhu and J. C. Finlay: PDT physics 3128
tive model and to verify its results in multicell tumorspheroid models.17,18 These models demonstrate that thedominant effect of the fluence rate in photodynamic therapyarises because the photochemical process itself consumesoxygen. If the rate of photochemical oxygen consumption isgreater than the rate at which oxygen can be resupplied bythe vasculature or ambient medium, an induction of transienthypoxia by PDT can result. This effect has been modeledtheoretically and has been demonstrated in cell spheroids,17
animals,19 and human tissues,20 and continues to be an areaof active research.21 A second, macroscopic model has alsobeen developed.22,23 This is an empirical model that does nottake into account the actual oxygen and photosensitizer dif-fusion processes microscopically but instead approximatesthem with simpler functions. It does, however, explicitly ac-count for the larger-scale spatial variation in fluence ratebased on the diffusion approximation. This model provides aquantity �reacted singlet oxygen� that can be used directly forclinical PDT dosimetry, and that relates directly to the three-dimensional distribution of photosensitizers, light fluencerate, and a mean tissue oxygenation distribution.22,23
II.B. Current areas of basic PDT research
II.B.1. Light source, transport, and delivery
PDT became popular after the invention of the laser,which allowed the production of monochromatic light thatcould be easily coupled into optical fibers. The wavelengthof light used for PDT is typically in the wavelength rangebetween 600–800 nm, the so called “therapeutic window.”24
In this wavelength range, the energy of each photon �h�� ishigh enough ��1.5 eV� to excite the photosensitizer and yetis low enough so that the light has sufficient penetration intothe tissue. Early lasers were based on either argon gas lasers�488 and 514.5 nm� or frequency doubled Nd:yttrium-aluminun-garnet solid state lasers �532 nm�, which werethen used to pump a dye laser to produce light in the desiredwavelength range. With the development of the diode laser,
S1
S0
T11O2
3O2Sensitizer
Photonabsorption
Energytransfer tooxygen
ISC
Oxygen
FIG. 1. Energy level diagram for a typical type II photosensitizer and oxy-gen. The sensitizer in its ground state �S0� absorbs a photon of light and isexcited to its first singlet state �S1�. It spontaneously decays to its excitedtriplet state �T1� via ISC. From T1, energy is transferred to ground statemolecular oxygen �3O2�, creating reactive singlet oxygen �1O2�.
the laser source has become portable and a turn-key opera-
Medical Physics, Vol. 35, No. 7, July 2008
tion. Development of more powerful and cheaper lasersources, e.g., fiber lasers, which couple more efficiently intooptical fiber, is an active area of research.
The invention of optical fiber allowed light to be directedeasily to deliver irradiation to desired regions without therequirement of a straight light path and is another enabler ofPDT. Currently, most PDT procedures are performed withoptical fibers. By attaching diffuse scattering tips of variousgeometrical shapes at the exit end of the fiber, point, linear,and planar light sources can be produced.25 Further develop-ment in light delivery devices that produce a light field withvarious geometrical shapes and in power distribution modu-lation that covers a larger area and has higher power is stillan active area of research.
Light distributions can be modeled using the diffusionapproximation to radiative transport.26 The finite-elementmethod is commonly used to solve the diffusion equation27
in an optically heterogeneous medium with arbitrary geom-etry. Various boundary conditions are used to describe vari-ous tissue-tissue, tissue-air, and tissue-water interfaces.26,28
However, the solution is often inaccurate in regions withouta sufficient number of multiple scattering �near the lightsource or nonscattering medium�. In these regions MonteCarlo simulation provides more accurate results but is muchslower.29 Active research is on going to solve the Boltzmannequation of light transport directly to provide accurate resultwhile improve the speed of calculation.26,30
II.B.2. PDT dosimetry
Three general strategies have been developed for dosim-etry based on the cumulative dose of singlet oxygen, whichis presumed to be predictive of tissue damage. Explicit do-simetry refers to the prediction of singlet oxygen dose on thebasis of measurable quantities that contribute to the photo-dynamic effect.31 The quantities of interest are typically thedistributions of light, photosensitizer, and oxygen. The dis-tributions of photosensitizer and oxygenation can be mea-sured via optical spectroscopy, as described above. In currentclinical practice, however, the quantity most straightforwardto measure is the light dose. Flat photodiode detectors havebeen used to measure the incident irradiance at the tissuesurface in intraoperative PDT.32 These measurements, how-ever, may not accurately reflect the fluence rate in the tissueitself because they neglect contribution of backscatteredlight. Detectors based on optical fibers overcome this prob-lem by collecting light isotropically.33 The effect on the mea-sured fluence rate is significant.34 Because these probes col-lect light via multiple scattering, the interface between thescattering tip and the surrounding medium can change thesensitivity of the detector by as much as a factor of 2, requir-ing careful calibration.35
Because complete explicit dosimetry requires measure-ment of three different parameters, it is inherently challeng-ing. Two alternatives have been suggested that require mea-surement of only a single parameter. Direct dosimetry relieson the detection of singlet oxygen itself, either through its
own phosphorescence emission or via singlet-oxygen-
3129 T. C. Zhu and J. C. Finlay: PDT physics 3129
sensitive chromophores. Implicit dosimetry31 uses a quan-tity such as fluorescence photobleaching of the photosensi-tizer, which is indirectly predictive of the production ofsinglet oxygen. Strategies for direct and implicit dosimetryare under development and will be discussed in later sec-tions.
II.B.3. Anatomic and optical imaging
The most commonly used medical imaging modalities in-clude ultrasound, computer tomography �CT�, magneticresonance, magnetic resonance spectroscopy, single photonemission computer tomography, and positron emission to-mography �PET�. The first three modalities produce excellentanatomical images, while the latter three provide functionalinformation �e.g., oxygen perfusion or tissue metabolism� atthe expense of image resolution. Diffuse optical tomography�DOT� is a viable new biomedical imaging modality.36 Thistechnique images the absorption and scattering properties ofbiological tissues and has been explored as a diagnosis toolin breast,37–42 brain,43,44 and bones and joints.45 Some pre-liminary attempts have been made to perform DOT forprostate.46–49 DOT at the treatment wavelength can be usedas input to calculate light fluence rate distribution for PDT.In addition, it provides access to a variety of physiologicalparameters that cannot otherwise be measured easily. An-other modality, optical coherence tomography �OCT� usescoherent light to obtain high resolution images. However,OCT is rarely used in PDT because of the limitation of pen-etration depth ��1 mm�.50
Most image reconstruction of DOT is based on solvingthe inverse problem for the diffusion equation.27 This is anill-posed problem because of the strong scattering in the tur-bid medium. As a result, the image resolution of DOT islimited when compared with other imaging modalities, suchas magnetic resonance imaging �MRI� or CT. The use ofspectroscopic information and/or a priori anatomic informa-tion is common to provide additional constraint to producereliable DOT reconstruction. Interested readers can find moreinformation from some excellent review articles.51,52
The concept of absorption and fluorescence spectroscopyas a modality for the diagnosis of disease dates back severaldecades.53 In recent years, the potential for spectroscopy todiagnose cancer54 and to monitor the progress of cancertreatment55 has been increasingly appreciated. In addition toits role in diagnosis, spectroscopy is particularly applicableto PDT in determining the local drug and oxygenconcentrations.56
Photodynamic therapy can cause changes in the concen-tration and oxygenation of blood in tissue both directly,through photochemical oxygen consumption, and indirectly,through effects on the vasculature and general physiologicalresponses. The monitoring of these responses may, therefore,be predictive of treatment outcome. For oxygen monitoring,the difference in absorption spectra between oxy- and deoxy-hemoglobin is used to determine the hemoglobin oxygensaturation, i.e., the fraction of total hemoglobin that is in its
oxygenated state. This quantity can be related to the oxygenMedical Physics, Vol. 35, No. 7, July 2008
concentration in the blood using the Hill curve.57 This mea-surement does not directly measure the concentration of oxy-gen in the tissue itself, however, it is possible to model therelationship between the vascular and tissue oxygenation.This concept has been investigated in animal models inwhich the blood flow and/or oxygenation were monitoredand changes correlated with outcome.58,59
II.B.4. New photosensitizers
Various photosensitizing drugs have been developed. Thefirst-generation photosensitizer, hematoporphyrin derivative,is a mixture of porphyrin monomers and oligomers that ispartially purified to produce the commercially availableproduct, porfimer sodium, marketed under the tradenamePhotofrin®. Photofrin® was approved for treatment of earlystage lung cancer in 1998 and for Barrett’s esophagus in2003. The clinical applicability of Photofrin® has been lim-ited by two factors. First, its absorption peak occurs at tooshort a wavelength �630 nm� to allow deep penetration intissue. Second, administration of Photofrin® results in cuta-neous photosensitivity lasting up to 6 weeks. These limita-tions have inspired the development of a second generationof photosensitizers with longer-wavelength absorption peaksand more rapid clearance from skin. Among these was ben-zoporphyrin derivative monoacid A �BPD-MA�, or vertepor-fin. In preclinical trials, it was observed that verteporfin pref-erentially targeted neovasculature. This selectivity has beenexploited for the treatment of choroidal neovascularization�CNV�, an abnormal growth of vessels in the retina associ-ated with age-related macular degeneration �AMD�, the lead-ing cause of blindness in the developed world. Verteporfinwas approved in the U.S. under the tradename Visudyne forCNV treatment in 2000. Tetra �m-hydroxyphenyl� chlorin�mTHPC, Foscan®� is another second generation photosen-sitizer, a pure synthetic chlorin compound, which is activatedby 652 nm light.60 The major advantages of mTHPC are ashort duration of skin photosensitivity �15 days�, a highquantum yield for singlet oxygen, and depth of tumor necro-sis of up to 10 mm in preclinical models.61 mTHPC has beenused for treatment of pleural mesothelioma,7 head-and-neckcancers,62,63 esophagus,64,65 prostate,10,66 pancreas,67 arthriticjoints,68 and skin cancers69 and was approved in Europe forPDT of head-and-neck and varieties of other tumors in 2001.
Another development of note is the prodrug�-aminolevulinic acid �ALA�. Unlike other PDT drugs, ALAitself is not a photosensitizer. When taken up by cells, how-ever, it is converted by a naturally occurring biosyntheticprocess into the photosensitizer protoporphyrin IX �PpIX�.ALA can be applied topically, and was approved by the FDAin 1999 for the treatment of actinic keratosis �AK�. Table Isummaries several of the more widely used photosensitizerscurrently available.
II.B.5. PDT biology
From the point of view of biological response, PDT isfundamentally different from other cancer therapies. Unlike
ionizing radiation, PDT achieves its cytotoxic effects prima-
3130 T. C. Zhu and J. C. Finlay: PDT physics 3130
rily though damage to targets other than DNA. The specificsubcellular targets damaged by PDT depend on the photosen-sitizer’s localization within the cell, which varies amongphotosensitizers and cell lines. Different types of damage canlead to different mechanisms of cell death. Damage to mito-chondria in particular can lead to apoptosis even at relativelylow light doses.70 Recently, the role of autophagic cell deathin PDT has been increasingly recognized.71 In addition to thevariation among photosensitizers in their subcellular targets,there is considerable variability in the macroscopic targetingof photosensitizers. Photosensitizers that are retained in thevasculature can destroy tumors via vascular damage ratherthan direct cell killing. Some photosensitizers may act asvascular agents at short times after injection and at high flu-ence rates, where only the vasculature is sufficiently oxygen-ated, and produce direct cell kill at low fluence rates and
TABLE I. An incomplete list of photosensitizers currently undergoing human
Photosensitizer Trade name Approval
Porfimer sodium Photofrin 1998, 2003 �FDA�ALA-PpIX Levulan Keratastick 1999 �FDA�Methyl aminolevulate-PpIX Metvix 2004 �FDA�Hexyl aminolevulate-PpIX Hexvix 2005 �EU�BPD-MA Verteporfin, Visudyne 2000 �FDA�mTHPC Foscan Phase I trials, 2001 �
Motexafin Lutetium MLu, Lutex, Lutrin Phase I trialsPd-bacteriopheophorbide Tookad Phase I trialsTaloporfin sodium�mono-L-aspartyl chlorin e6�
LS11 Phase I and II trials
Silicon pthalocyanine 4 PC-4 Phase I trials
Real-timand treatmbased o
res
Light Dosimetrywith Feedback
Explicit and,Implicit
Dosimetry,SOLD
ComplexDosimetry withFeedback,
Real-time TPS
PMBresim
Light Delivery Dosimetry Im
FIG. 2. Diagram illustrating the progress of PDT development from a set ofbiologists, chemists, physicists, and engineers. The second row illustrates th
The third row illustrates the future research direction and the fourth row is the ultMedical Physics, Vol. 35, No. 7, July 2008
long times after injection.72 An additional level of complex-ity arises from the fact that the response to PDT is not con-fined to the cells where the singlet oxygen is deposited butcan involve physiological73 and immunological74,75 re-sponses as well.
III. CURRENT DEVELOPMENTS
Much of the research in the early decades of PDT and itsrelated fields proceeded in five almost independent areas, asillustrated in the top row of Fig. 2. The problems associatedwith light source and light delivery system development, do-simetry, and optical imaging were treated as physics prob-lems, while photosensitizer development and PDT biologywere treated as problems of chemistry and biology, respec-tively. In recent years, however, the most promising ad-
ical trials.
Excitation�nm�
Drug-lightinterval
Clearancetime Sites
630 48–150 h 4–6 weeks Lung, Barrett’s esophagus405, 635 14–18 h �2 days AK405, 635 3 h �2 days AK
405 1–3 h �2 days Detection of bladder tumors689 15 min 5 days CNV652 48–110 h 15 days Head and neck, prostate, pancreas,
esophagus, mesothelioma732 3 h Prostate, atherosclerosis762 �30 min �2 h Prostate664 1 h CNV, liver and colorectal metastasis
672 24–36 h Skin
simetryplanninglogicale
BiomarkersMolecularBeacons
TargetedPhotosensitizer,
Photo-immunotherapy
se-iveg
BiologicalResponseImaging
g PDTBiology
PhotosensitizerDevelopment
arate fields �top row� to a collaborative effort unifying the contributions ofent state of art of research and represents integration of two separate fields.
clin
EU�
e doentn biopons
, doponsagin
agin
dispe curr
imate integration of all disparate fields. See text for a complete description.

3131 T. C. Zhu and J. C. Finlay: PDT physics 3131
vances have come out of interdisciplinary collaborationsamong these areas. The systems and strategies currently inpreclinical and clinical trials are examples of suchcollaborations.
III.A. Light dosimetry with real-time feedback
It is very difficult to assess the efficacy and toxicity of anytreatment in a clinical trial without a rigorous quantitativemeasurement of the treatment given. One reason that radio-therapy has become an accepted locoregional therapy is thatthe dose to tissues has been quantified accurately and cura-tive doses can be delivered safely. In our current clinicaltrials, we deliver a dose of light to the treatment sites basedupon measurements made from implanted isotropic lightdetectors.34,76 These detectors allow us to prescribe the lightdose based upon actual measurements in the prostate ratherthan the output of the laser. This dosimetric approach alsoensures that the same amount of light energy �as measuredby the isotropic detectors� is deposited uniformly in the pros-tate within each cohort of patients as a specific dose level.
The measurement of light fluence in vivo is necessary butnot sufficient to optimize the light fluence distribution. Opti-mization of the light fluence depends upon accurate calcula-tion of the light fluence rate in the entire prostate volume,which in turn requires accurate characterization of the in vivoprostate optical properties as input. Many studies have beenconducted to determine the in vivo optical properties of hu-man prostate.77–79 These light fluence measurements showthat the optical properties of the prostate vary substantiallywithin a prostate gland as well as among separate prostateglands. The optical properties of prostate tissue may alsovary over time during a PDT procedure.
The state of the art for prostate PDT uses only in vivolight fluence rate monitoring to determine the light fluenceusing equal weight of linear light sources. This is not suffi-cient since light fluence at only selected points are known.Integrating ultrasound imaging and the PDT dose calculationengine into the PDT delivery system, with input of tissueoptical properties and drug uptake, will allow the clinician tooptimize the weight of each light-delivery fiber, and thusimprove the light fluence distribution in the prostate gland.Adequate treatment planning often uses various optimizationengines to optimize the distribution of light sourceintensities.
III.B. Implicit dosimetry and dosimetric imaging
The most commonly cited example of implicit dosimetryis fluorescence photobleaching. Wilson31 suggested that thephotobleaching of the photosensitizer, if moderated by thesame mechanism as the photodynamic effect, could indicatethe extent of damage. The theoretical basis for quantitativeimplicit dosimetry using fluorescence photobleaching wasformalized by Georgakoudi et al.18 for the case of multicelltumor spheroids. Fluorescence photobleaching has been usedin animal models to investigate the fluence-rate dependenceof photodynamic therapy80–82 and has been shown to corre-
83
late with visible skin damage. A device for skin PDT do-Medical Physics, Vol. 35, No. 7, July 2008
simetry using photobleaching has been developed for use inclinical trials84 and work to extend the spheroid models torealistic tissues is ongoing.85
Fluorescence photobleaching is relatively inexpensive andstraightforward to implement, however, its quantitative inter-pretation involves several challenges. First, fluorescencemeasurement in vivo must always account for the confound-ing effects of light scattering and absorption. Second, thevalidity of the relationship between fluorescence pho-tobleaching and reacted singlet oxygen dose assumes that thephotobleaching is mediated primarily by singlet oxygen re-action with the photosensitizer. There is experimental evi-dence to suggest that other bleaching mechanisms may beimportant for the commonly used photosensitizersPhotofrin®82 and ALA-induced PpIX,86 and the in vivo pho-tobleaching of mTHPC exhibits features that are not readilyinterpretable.81 Care should therefore be exercised in usingphotobleaching as a dose metric.
Two methods have been developed for the detection ofsinglet oxygen itself. Qin et al. have demonstrated achemoluminescent compound that emits light in the presenceof singlet oxygen.87 The translation of this technology intopatients will require the development of a nontoxic, singlet-oxygen-specific chemoluminescent probe that distributesuniformly in tissue.
Direct measurement of singlet oxygen can be accom-plished via detection of its 1270 nm phosphorescence emis-sion, a technique known as singlet oxygen luminescence do-simetry �SOLD�.88 Detection of this signal presentssignificant technical challenges due to the long wavelengthof the emission and the weak signal. Jarvi et al.88 have de-veloped a system based on a photomultiplier tube capable ofdetecting the long-wavelength emission of singlet oxygen.The emission is stimulated by a pulsed laser at the treatmentwavelength, and a time-resolved measurement of the emittedsignal allows determination of the singlet oxygen lifetime inthe system being measured. An additional challenge is theinterpretation of the singlet oxygen phosphorescence signal.The phosphorescence emission arises from a transition ofoxygen from its singlet state to its ground state. This processtherefore competes with the reaction of singlet oxygen withcellular and extracellular substrates. This leads to an increasein phosphorescence emission in conditions where substratesfor singlet oxygen are not plentiful. To differentiate betweenthe cellular signal corresponding to PDT effect and the ex-tracellular signal, the time-resolved emission signal can be fitas a sum of signals with different lifetimes.
III.C. Biomarkers and molecular beacons
Because the goal of PDT is ultimately to deliver the op-timal treatment to the tumor, the idea of using noninvasivedetection and imaging to determine the status of tumor cellsat the molecular level is very attractive. This concept hasdriven the development of molecular beacons, molecules thattarget specific molecular pathways that can be imaged using,for instance, near-infrared fluorescence. Steflova et al. have
developed a series of molecular beacons whose fluorescence
3132 T. C. Zhu and J. C. Finlay: PDT physics 3132
is quenched in their latent state and restored under the actionof specific cellular processes of interest.89 Because these bea-cons target specific molecules, it is likely that they will betumor-type specific, however, the variety of cellular pro-cesses that can potentially be imaged using this approachmakes it very promising. Molecular beacons are a subset ofthe general category of cancer biomarkers, molecules whichallow imaging of specific biological processes via variousmodalities including MRI, PET,90 and optical imaging.
III.D. Enhancement and targeting of photosensitizers
Several researchers have developed methods for enhanc-ing the ability of a photosensitizer to target tumors. Onestrategy to accomplish this is to optimize the timing the ad-ministration of light to coincide with the desired distributionof the photosensitizer.72 This approach has been used to tar-get vasculature by applying light while the photosensitizer isin circulation, for the treatment of AMD using Vertepofin andthe prostate using Tookad.12 In cases where the rate of pro-duction of singlet oxygen is limited by the vascular resupplyof oxygen, changes in the light fluence rate can change thedistribution of deposited singlet oxygen, with higher fluencerates leading to preferential targeting of vascular-adjacent tis-sue. Thus, the combination of drug-light interval and fluencerate can be adjusted to enhance the treatment of the desiredtissue type.
A more direct approach to photosensitizer targeting is theconjugation of the photosensitizer to a tumor-selective mol-ecule or particle.91 The last 2 decades have seen tremendousprogress in the development of tumor-targeted therapeuticand imaging agents for cancer in general.92,93 These innova-tions will continue to inform the development of new photo-sensitizers targeted to specific tumor types.
Recent research has shown PDT induced increases ofVEGF, MMPs, and/or COX-2 in tumor microenvironmentthat cause resistance to standard treatment. As a result, com-bination of therapy that suppresses these growth factors hasbeen proposed to enhance the therapeutic efficacy of PDT.C225, a monoclonal antibody that inhibits the receptor ty-rosine kinase activity of EGFR, has been shown to enhancethe PDT treatment in ovarian cancer.94,95 Other combinedmodalities seek to target treatment-induced angiogenesisand/or inflammation to enhance the effectiveness of PDT.96
IV. FUTURE DEVELOPMENTS ANDPREDICTIONS
We predict that future developments in PDT will continuethe trend toward interdisciplinary work and the inclusion ofmore technologies and subfields, such as imaging, noveldrug design, and biological modeling into the treatment plan-ning and dosimetry processes. Below are a few predictions offuture PDT physics research directions:
IV.A. Light sources: Faster, cheaper, larger, smaller
A significant driver in the development of new light
sources has been the advent of inexpensive, reliable diodeMedical Physics, Vol. 35, No. 7, July 2008
lasers and light-emitting diodes. Diode light sources havealready been made small enough to be implantable.97 Wepredict that this trend will continue, with future light sourcesbecoming ever smaller, cheaper, and more efficient. On theother hand, the increases in efficiency of these light sourceswill also lead to lasers with greater total power output, al-lowing the treatment of larger volumes of tissue using asingle source.
Simple increases in power are not the only advances wecan expect from future light sources. New delivery systemswill incorporate mechanisms to deliver a light distributioncustomizable to each patient’s treatment plan. In our group,we have developed a computer-controlled attenuator systemfor prostate PDT designed to adjust the intensities of up to 16implanted interstitial diffusing fibers independently and inreal time.98 Lilge et al. have investigated optical diffusingfibers whose emission profiles along the fiber axis can becustomized to deliver much more complex light distributionsthan conventional diffusers.99,100 We expect further develop-ments in this direction to allow more and more precise con-trol of the in vivo light distribution during PDT.
IV.B. Real-time oxygen monitoring
While it has long been recognized that oxygenation of thetarget tissue is essential to PDT, measurements of oxygen-ation are now starting to be implemented in preclinical andclinical trials. We anticipate that future clinical protocols in-volving real-time dosimetry will also include real-time oxy-gen monitoring, both to prevent PDT-induced hypoxia and totake advantage of the predictive value of PDT-inducedchanges in blood flow and hemoglobin oxygen saturation.58
The monitoring of hemoglobin saturation and blood flow hasbeen demonstrated in clinical trials.101 The translation ofmeasurements of hemoglobin oxygenation into a determina-tion of the cellular oxygen concentration requires a model ofoxygen diffusion and consumption. The development of suchmodels is ongoing and will inform future dosimetrydevelopments.85
An alternative to hemoglobin monitoring is the use oftime-resolved SOLD measurements. A sufficiently sophisti-cated analysis of the time dependence of the SOLD signalallows determination of the photosensitizer triplet lifetime,which is related to the local oxygen concentration. Hence,SOLD has the potential to provide both a measure of reactedsinglet oxygen dose and a measure of the molecular oxygenconcentration at the point of singlet oxygen generation.88
This approach has the additional advantage from the point ofview of explicit dosimetry of providing an intermediate veri-fication of the triplet lifetime predicted by the dosimetricmodel.
IV.C. Multifunctional, multimodality photosensitizers
Another area of active research in photodynamic therapyis the development of photosensitizers and photosensitizerdelivery systems that enhance the functionality of thephotosensitizer.102 For instance, a photosensitizer may be
linked to a fluorescent molecule to enhance its delectability
3133 T. C. Zhu and J. C. Finlay: PDT physics 3133
under fluorescence imaging.103 Pandey et al.104 have pro-posed combining photosensitizers with contrast agents foroptical, MRI and PET imaging, allowing image-guided PDTtreatment. Zheng et al. have combined the “molecular bea-con” concept with a photosensitizer to produce photody-namic molecular beacons.105 These molecules exhibitquenching that suppresses their production of 1O2 in theirlatent state. They can be activated by interaction with atumor-specific molecular marker, in this case the matrix met-alloproteinase MMP-7. The clinical implementation of strat-egies such as these has the potential to dramatically improvethe targeting of the photosensitizer to the tumor. An essentialcomponent of any targeting strategy will be the ability toverify the targeting of the drug to the desired target. Thedistribution of the photosensitizer can be determined opti-cally using fluorescence or absorption imaging. In addition,detailed models of the distributions and kinetics of light,photosensitizer, and oxygen will provide a quantitative rela-tionship between the microscopic distribution and photo-chemical properties of the drug and the macroscopically ob-served treatment response.106 In cases where the drug isactivated by an endogenous agent, the results will be predict-able only using such sophisticated models.
IV.D. Treatment planning integrated with dosimetry,imaging, and light delivery devices to allowadaptive treatment
The integration of dosimetry systems with multimodalityimaging �anatomic and DOT� and light delivery devices intoan integrated system has drawn great interest recently. Sev-eral groups are developing integrated systems to control lightdelivery, real-time light monitoring, and volumetric light flu-ence calculation. The group in Lund, Sweden is developing amultiple channel system of point sources that can be used aseither light sources or detectors.107 A personal computer con-trols the position and duration of the point sources to opti-mize light fluence distribution. Another group in Toronto,Canada has commercialized a four-channel light source withcomputerized power control in each channel. Our group hasdeveloped an integrated system that incorporates PDT do-simetry that include light fluence rate at multiple points,108 athree-dimensional map of optical properties,46 drug concen-tration distribution,56 and tissue oxygenation.98 A kernel-based algorithm was developed to calculate light fluence ratedistribution in the optically heterogeneous prostate gland,109
which, coupled with an optimization engine allows optimi-zation of light source powers to achieve a uniform light flu-ence distribution.110,98 This area of research will evolve intoa totally computerized delivery, monitoring, and dosimetrysystem for real-time feedback control.
IV.E. New dosimetry quantities based on modeling ofthe dynamic system
The current state of art in PDT dosimetry is to explicitlydetermine the quantity PDT dose, defined as the number ofphotons absorbed by photosensitizing drug per gram of
111
tissue. While this quantity takes into account the consump-Medical Physics, Vol. 35, No. 7, July 2008
tion of photosensitizer, it does not consider the effect of tis-sue oxygenation on the quantum yield of oxidative radicals.Thus, it is only applicable in cases where ample oxygen sup-plies exist. It is anticipated that new dosimetry quantitiesbased on reacted singlet oxygen �1O2�rx, e.g., a product ofsinglet oxygen quantum yield and PDT dose, can be used toaccount for kinetics of the oxygen consumption during PDTprocess.23 Foster et al. have determined most of fundamentalparameters necessary for microscopic model of the oxygenconsumption during PDT.18,82,106,112 However, when apply-ing models developed in the microscopic scale to a macro-scopic environment, the values of many parameters maychange, and many parameters may be observable only in thevolume average, so extensive study will be required to deter-mine the values for each specific photosensitizer.
IV.F. Physiological effects of PDT will be exploited todevelop systemic therapy
The ability of PDT to elicit an immune response has beenrecognized for some time.75 The past decade has seen dra-matic progress in our understanding of the mechanisms ofPDT-induced immune response.74,113 In addition it has beendemonstrated that PDT can be used to generate vaccinesagainst specific tumor types.114,115 This strategy is particu-larly attractive for the treatment of cancer, where it is likelythat PDT will be used in combination with radiation andchemotherapy, both of which can have immunosuppressiveeffects.
As the details of the mechanisms of the immune responseare better understood, it is likely that new photosensitizersand delivery mechanisms will be developed for the expresspurpose of enhancing the immunological response and/ormoderate treatment induced angiogenesis and inflammation.Furthermore, the parameters which optimize immune re-sponse to PDT will be different from those that maximizesinglet oxygen dose or direct cell killing.116 Therefore, therewill be an increasing need for the incorporation of these ef-fects into PDT treatment planning and dosimetry. We predictthat PDT vaccines will find a use as an adjuvant therapy,even in cases where the tumor location or geometry pre-cludes conventional PDT as a primary treatment. In thesecases, it may be possible to perform PDT on ex vivo tissue orcell cultures, in which case the problems of light propagationand tumor physiology are greatly simplified, allowing a levelof treatment optimization not feasible in vivo.
V. CONCLUSIONS
We have predicted that PDT research will increasinglyrely on combinations of widely varied fields, leading to moreand more sophisticated treatment protocols. It is tempting toassume that such therapies will become so complex that theycan only be modeled empirically, and that the role of physicswill diminish. However, the history of PDT research demon-strates that many advances in the field are made not byavoiding the complexity of the problem but by embracing it.As we exploit our growing knowledge of the underlying pho-
tochemistry, biology, and physiology of PDT to develop new
3134 T. C. Zhu and J. C. Finlay: PDT physics 3134
and better treatments, it will be more important than ever tounderstand and optimize those treatment parameters overwhich we have direct control. In the future, as in the past, itwill be the understanding of the physics of PDT that willallow us to take advantage of our scientific understandingand translate it into improved clinical treatments.
ACKNOWLEDGMENTS
This work is supported by the National Institute of Health�NIH� Grant Nos. P01 CA87971 and R01 CA109456.
a�Electronic mail: [email protected]. J. Dougherty, C. J. Gomer, B. W. Henderson, G. Jori, D. Kessel, M.Korbelik, J. Moan, and Q. Peng, “Photodynamic therapy,” J. Natl. CancerInst. 90, 889–905 �1998�.
2M. A. Biel, “Photodynamic therapy and the treatment of head and neckcancers,” J. Clin. Laser Med. Surg. 14, 239–244 �1996�.
3W. E. Grant, P. M. Speight, C. Hopper, and S. G. Bown, “Photodynamictherapy: an effective, but non-selective treatment for superficial cancersof the oral cavity,” Int. J. Cancer 71, 937–942 �1997�.
4J. S. Friedberg, R. Mick, J. P. Steveson, T. Zhu, T. M. Busch, D. Shin, D.Smith, M. Culligan, A. Dimofte, E. Glatstein, and S. M. Hahn, “A phaseII trial of pleural photodynamic therapy �PDT� and surgery for patientswith non-small cell lung cancer �NSCLC� with pleural spread,” J. Clin.Oncol. 22, 2192–2201 �2004�.
5T. L. Moskal, T. J. Dougherty, J. D. Urschel, J. G. Antkowiak, A. M.Regal, D. L. Driscoll, and H. Takita, “Operation and photodynamictherapy for pleural mesothelioma: 6-year follow-up,” Ann. Thorac. Surg.66, 1128–1133 �1998�.
6H. I. Pass et al., “Intrapleural photodynamic therapy: Results of a phase Itrial,” Ann. Surg. Oncol. 1, 28–37 �1994�.
7J. S. Friedberg, R. Mick, J. Stevenson, J. Metz, T. Zhu, J. Buyske, D. H.Sterman, H. I. Pass, E. Glatstein, and S. M. Hahn, “A phase I study ofFoscan-mediated photodynamic therapy and surgery in patients with me-sothelioma,” Ann. Thorac. Surg. 75, 952–959 �2003�.
8R. Ackroyd, N. J. Brown, M. F. Davis, T. J. Stephenson, S. L. Marcus, C.J. Stoddard, A. G. Johnson, and M. W. Reed, “Photodynamic therapy fordysplastic Barrett’s esophagus: A prospective, double blind, randomised,placebo controlled trial,” Gut 47, 612–617 �2000�.
9M. Panjehpour, B. F. Overholt, J. M. Haydek, and S. G. Lee, “Results ofphotodynamic therapy for ablation of dysplasia and early cancer in Bar-rett’s esophagus and effect of oral steroids on stricture formation,” Am. J.Gastroenterol. 95, 2177–2184 �2000�.
10T. R. Nathan, D. E. Whitelaw, S. C. Chang, W. R. Lees, P. M. Ripley, H.Payne, L. Jones, M. C. Parkinson, M. Emberton, A. R. Gillams, A. R.Mundy, and S. G. Browen, “Photodynamic therapy for prostate cancerrecurrence after radiotherapy: A phase I study,” J. Urol. 168, 1427–1432�2002�.
11D. Stripp, R. Mick, T. C. Zhu, R. Whittington, D. Smith, A. Dimofte, J. C.Finlay, J. Miles, T. M. Busch, D. Shin, A. Kachur, Z. Tochner, S. B.Malkowicz, E. Glatstein, and S. M. Hahn, “Phase I trial of MotexfinLutetium-mediated interstitial photodynamic therapy in patients with lo-cally recurrent prostate cancer,” Proc. SPIE 5315, 88–99 �2004�.
12R. A. Weersink, A. Bogaards, M. Gertner, S. R. Davidson, K. Zhang, G.Netchev, J. Trachtenberg, and B. C. Wilson, “Techniques for delivery andmonitoring of TOOKAD �WST09�-mediated photodynamic therapy ofthe prostate: clinical experience and practicalities,” J. Photochem. Photo-biol. B 79, 211–222 �2005�.
13M. A. Rosenthal, B. Kayar, J. S. Hill, D. J. Morgan, R. L. Nation, S. S.Stylli, R. L. Basser, S. Uren, H. Geldard, M. D. Green, S. B. Kahl, and A.H. Kaye, “Phase I and pharmacokinetic study of photodynamic therapyfor high-grade gliomas using a noval boronated porphyrin,” J. Clin. On-col. 19, 519–524 �2001�.
14T. T. Goodell and P. J. Muller, “Photodynamic therapy: A novel treatmentfor primary brain malignancy,” J. Neurosci. Nurs. 33, 296–300 �2001�.
15A. Bogaards, A. Varma, K. Zhang, D. Zach, S. K. Bisland, E. H.Moriyama, L. Lilge, P. J. Muller, and B. C. Wilson, “Fluorescence image-guided brain tumour resection with adjuvant metronomic photodynamic
therapy: Pre-clinical model and technology development,” Photochem.Medical Physics, Vol. 35, No. 7, July 2008
Photobiol. Sci. 4, 438–442 �2005�.16M. J. Paterson, O. Christiansen, F. Jensen, and P. R. Ogilby, “Overview of
theoretical and computational methods applied to the oxygen-organicmolecule photosystem,” Photochem. Photobiol. 82, 1136–1160 �2006�.
17T. H. Foster, D. F. Hartley, M. G. Nichols, and R. Hilf, “Fluence rateeffects in photodynamic therapy of multicell tumor spheroids,” CancerRes. 53, 1249–1254 �1993�.
18I. Georgakoudi, M. G. Nichols, and T. H. Foster, “The mechanism ofPhotofrin photobleaching and its consequences for photodynamic dosim-etry,” Photochem. Photobiol. 65, 135–144 �1997�.
19S. L. Gibson, K. R. VanDerMeid, R. S. Murant, R. F. Raubertas, and R.Hilf, “Effects of various photoradiation regimens on the antitumor effi-cacy of photodynamic therapy for R3230AC mammary carcnimoas,”Cancer Res. 50, 7236–7241 �1990�.
20B. W. Henderson, T. M. Busch, L. A. Vaughan, N. P. Frawley, D. Babich,T. A. Sosa, J. D. Zollo, A. S. Dee, M. T. Cooper, D. A. Bellnier, W. R.Greco, and A. R. Oseroff, “Photofrin photodynamic therapy can signifi-cantly deplete or preserve oxygenation in human basal cell carcinomasduring treatment, depending on fluence rate,” Cancer Res. 60, 525–529�2000�.
21B. W. Henderson, T. M. Busch, and J. W. Snyder, “Fluence rate as amodulator of PDT mechanisms,” Lasers Surg. Med. 38, 489–493 �2006�.
22X. H. Hu, Y. Feng, J. Q. Lu, R. R. Allison, R. E. Cuenca, G. H. Downie,and C. H. Sibata, “Modeling of a type II photofrin-mediated photody-namic therapy process in a heterogeneous tissue phantom,” Photochem.Photobiol. 81, 1460–1468 �2005�.
23T. C. Zhu, J. C. Finlay, X. Zhou, and J. Li, “Macroscopic modeling of thesinglet oxygen production during PDT,” Proc. SPIE 6427, 642708–642720�2007�.
24B. C. Wilson and M. S. Patterson, in Photodynamic Therapy of Neoplas-tic Disease, edited by D. Kessel �CRC Press, Boca Raton, 1990�, Vol. 1,pp. 129–144.
25P. R. Almond, Photodynamic Therapy Equipment and Dosimetry �Ameri-can Institute of Physics, Woodbury, NY, 1992�.
26A. Ishimaru, Wave Propagation and Scattering in Random Media �IEEE,New York, 1997�.
27W. Cong, L. V. Wang, and G. Wang, “Formulation of photon diffusionfrom spherical bioluminescent sources in an infinite homogeneous me-dium,” Biomed. Eng. Online 3, 12 �2004�.
28R. C. Haskell, L. O. Svaasand, T.-T. Tsay, T.-C. Feng, M. S. McAdams,and B. J. Tromberg, “Boundary conditions for the diffusion equation inradiative transfer,” J. Opt. Soc. Am. A 11, 2727–2741 �1994�.
29L. Wang, S. L. Jacques, and L. Zheng, “MCML-Monte Carlo modeling oflight transport in multi-layered tissues,” Comput. Methods ProgramsBiomed. 47, 131–146 �1995�.
30J. J. Duderstadt and W. R. Martin, Transport Theory �Wiley, New York,1979�.
31B. C. Wilson, M. S. Patterson, and L. Lilge, “Implicit and explicit dosim-etry in photodynamic therapy: A new paradigm,” Lasers Med. Sci. 12,182–199 �1997�.
32S. K. Hendren, S. M. Hahn, F. R. Spitz, T. W. Bauer, S. C. Rubin, T. Zhu,E. Glatstein, and D. L. Fraker, “Phase II trial of debulking surgery andphotodynamic therapy for disseminated intraperitoneal tumors,” Ann.Surg. Oncol. 8, 65–71 �2001�.
33J. P. Marijnissen and W. M. Star, “Performance of isotropic light dosim-etry probes based on scattering bulbs in turbid media,” Phys. Med. Biol.47, 2049–2058 �2002�.
34T. G. Vulcan, T. C. Zhu, C. E. Rodriguez, A. Hsi, D. L. Fraker, P. Baas,L. H. Murrer, W. M. Star, E. Glatstein, A. G. Yodh, and S. M. Hahn,“Comparison between isotropic and nonisotropic dosimetry systems dur-ing intraperitoneal photodynamic therapy,” Lasers Surg. Med. 26, 292–301 �2000�.
35J. P. Marijnissen and W. M. Star, “Calibration of isotropic light dosimetryprobes based on scattering bulbs in clear media,” Phys. Med. Biol. 41,1191–1208 �1996�.
36A. H. Hielscher, A. Y. Bluestone, G. S. Abdoulaey, A. D. Klose, J.Lasker, M. Stewart, U. Netz, and J. Beuthan, “Near-infrared diffuse op-tical tomography,” Dis. Markers 18, 313–337 �2002�.
37A. Li, E. L. Miller, M. E. Kilmer, T. J. Brukilacchio, T. Chaves, J. Stott,Q. Zhang, T. Wu, M. Chorlton, R. H. Moore, D. B. Kopans, and D. A.Boas, “Tomographic optical breast imaging guided by three-dimensionalmammography,” Appl. Opt. 42, 5181–5190 �2003�.
38
J. P. Culver, R. Choe, M. J. Holboke, L. Zubkov, T. Durduran, A. Slemp,
3135 T. C. Zhu and J. C. Finlay: PDT physics 3135
V. Ntziachristos, B. Chance, and A. G. Yodh, “Three-dimensional diffuseoptical tomography in the parallel plane transmission geometry: Evalua-tion of a hybrid frequency domain/continuous wave clinical system forbreast imaging,” Med. Phys. 30, 235–247 �2003�.
39M. J. Holboke, B. J. Tromberg, X. Li, N. Shah, J. Fishkin, D. Kidney, J.Butler, B. Chance, and A. G. Yodh, “Three-dimensional diffuse opticalmammography with ultrasound localization in a human subject,” J.Biomed. Opt. 5, 237–247 �2000�.
40S. Srinivasan, B. W. Pogue, S. Jiang, H. Dehghani, C. Kogel, S. Soho, J.J. Gibson, T. D. Tosteson, S. P. Poplack, and K. D. Paulsen, “In vivohemoglobin and water concentrations, oxygen saturation, and scatteringestimates from near-infrared breast tomography using spectral reconstruc-tion,” Acad. Radiol. 13, 195–202 �2006�.
41B. Brooksby, S. Jiang, H. Dehghani, B. W. Pogue, K. D. Paulsen, J.Weaver, C. Kogel, and S. P. Poplack, “Combining near-infrared tomog-raphy and magnetic resonance imaging to study in vivo breast tissue:implementation of a Laplacian-type regularization to incorporate mag-netic resonance structure,” J. Biomed. Opt. 10, 051504–051514�2005�.
42B. W. Pogue, S. P. Poplack, T. O. McBride, W. A. Wells, K. S. Osterman,U. L. Osterberg, and K. D. Paulsen, “Quantitative hemoglobin tomogra-phy with diffuse near-infrared spectroscopy: Pilot results in the breast,”Radiology 218, 261–266 �2001�.
43J. P. Culver, A. M. Siegel, J. J. Stott, and D. A. Boas, “Volumetric diffuseoptical tomography of brain activity,” Opt. Lett. 28, 2061–2063 �2003�.
44J. P. Culver, T. Durduran, D. Furuya, C. Cheung, J. H. Greenberg, and A.G. Yodh, “Diffuse optical tomography of cerebral blood flow, oxygen-ation, and metabolism in rat during focal ischemia,” J. Cereb. Blood FlowMetab. 23, 911–924 �2003�.
45Y. Xu, N. Iftimia, H. Jiang, L. L. Key, and M. B. Bolster, “Three-dimensional diffuse optical tomography of bones and joints,” J. Biomed.Opt. 7, 88–92 �2002�.
46T. C. Zhu and J. C. Finlay, “Prostate PDT dosimetry,” PhotodiagnosisPhotodynamic Therapy 3, 234–246 �2006�.
47X. Zhou, T. C. Zhu, J. C. Finlay, J. Li, A. Dimofte, and S. Hahn, “Two-dimensional/three dimensional hybrid interstitial diffuse optical tomogra-phy of human prostate during photodynamic therapy: Phantom and clini-cal results,” Proc. SPIE 6434, 64341Y–64352Y �2007�.
48C. Li, R. Liengsawangwong, H. Choi, and R. Cheung, “Using a prioristructural information from magnetic resonance imaging to investigate thefeasibility of prostate diffuse optical tomography and spectroscopy: Asimulation study,” Med. Phys. 34, 266–274 �2007�.
49X. Zhou and T. C. Zhu, “Interstitial diffuse optical tomography using anadjoint model with linear sources,” Proc. SPIE 6845, 68450C–68459C�2008�.
50A. F. Low, G. J. Tearney, B. E. Bouma, and I. K. Jang, “TechnologyInsight: optical coherence tomography–Current status and future develop-ment,” Nat. Clin. Pract. Cardiovasc. Med. 3, 154–162 �2006�.
51B. W. Pogue, S. C. Davis, X. Song, B. A. Brooksby, H. Dehghani, and K.D. Paulsen, “Image analysis methods for diffuse optical tomography,” J.Biomed. Opt. 11, 033001–033017 �2006�.
52A. P. Gibson, J. C. Hebden, and S. R. Arridge, “Recent advances indiffuse optical imaging,” Phys. Med. Biol. 50, R1–R43 �2005�.
53R. Richards-Kortum and E. Sevick-Muraca, “Quantitative optical spec-troscopy for tissue diagnosis,” Annu. Rev. Phys. Chem. 47, 555–606�1996�.
54B. Swinson, W. Jerjes, M. El-Maaytah, P. Norris, and C. Hopper, “Opticaltechniques in diagnosis of head and neck malignancy,” Oral Oncol. 42,221–228 �2006�.
55I. J. Bigio and S. G. Bown, “Spectroscopic sensing of cancer and cancertherapy: current status of translational research,” Cancer Biol. Ther. 3,259–267 �2004�.
56J. C. Finlay, T. C. Zhu, A. Dimofte, D. Stripp, S. B. Malkowicz, T. M.Busch, and S. M. Hahn, “Interstitial fluorescence spectroscopy in thehuman prostate during motexafin lutetium-mediated photodynamictherapy,” Photochem. Photobiol. 82, 1270–1278 �2006�.
57A. V. Hill, “The possible effects of the aggregation of the molecules ofhemoglobin on its dissociation curves,” J. Physiol. �Proc.� 40, iv–vii�1910�.
58G. Yu, T. Durduran, C. Zhou, H. W. Wang, M. E. Putt, H. M. Saunders, C.M. Sehgal, E. Glatstein, A. G. Yodh, and T. M. Busch, “Noninvasivemonitoring of murine tumor blood flow during and after photodynamictherapy provides early assessment of therapeutic efficacy,” Clin. Cancer
Res. 11, 3543–3552 �2005�.Medical Physics, Vol. 35, No. 7, July 2008
59H. W. Wang, M. E. Putt, M. J. Emanuele, D. B. Shin, E. Glatstein, A. G.Yodh, and T. M. Busch, “Treatment-induced changes in tumor oxygen-ation predict photodynamic therapy outcome,” Cancer Res. 64, 7553–7561 �2004�.
60M. C. Berenbaum, S. L. Akande, R. Bonnett, H. Kaur, S. Ioannou, R. D.White, and U. J. Winfield, “Meso-tetra�hydroxyphenyl�porphyrins, a newclass of potent tumour photosensitisers with favourable selectivity,” Br. J.Cancer 54, 717–725 �1986�.
61I. P. van Geel, H. Oppelaar, Y. G. Oussoren, M. A. van der Valk, and F. A.Stewart, “Photosensitizing efficacy of mTHPC-PDT compared tophotofrin-PDT in the RIF1 mouse tumour and normal skin,” Int. J. Cancer60, 388–394 �1995�.
62W. Rauschning, I. B. Tan, and G. Dolivet, “Photodynamic therapy �PDT�with mTHPC in the palliation of advanced head and neck cancer in pa-tients who have failed prior therapies and are unsuitable for radiatio-therapy, surgery or systemic chemotherapy,” J. Clin. Oncol. 22�14�, 5596�2004�.
63M. Biel, “Advances in photodynamic therapy for the treatment of headand neck cancers,” Lasers Surg. Med. 38, 349–355 �2006�.
64L. B. Lovat, N. F. Jamieson, M. R. Novelli, C. A. Mosse, C. Selvasekar,G. D. Mackenzie, S. M. Thorpe, and S. G. Bown, “Photodynamic therapywith m-tetrahydroxyphenyl chlorin for high-grade dysplasia and earlycancer in Barrett’s columnar lined esophagus,” Gastrointest. Endosc. 62,617–623 �2005�.
65J. Etienne, N. Dorme, G. Bourg-Heckly, P. Raimbert, and J. F. Flejou,“Photodynamic therapy with green light and m-tetrahydroxyphenyl chlo-rin for intramucosal adenocarcinoma and high-grade dysplasia in Barrett’sesophagus,” Gastrointest. Endosc. 59, 880–889 �2004�.
66C. M. Moore, T. R. Nathan, W. R. Lees, C. A. Mosse, A. Freeman, M.Emberton, and S. G. Bown, “Photodynamic therapy using meso tetrahydroxy phenyl chlorin �mTHPC� in early prostate cancer,” Lasers Surg.Med. 38, 356–363 �2006�.
67S. P. Pereira, L. Ayaru, A. Rogowska, A. Moose, A. R. Hatfield, and S. G.Bown, “Photodynamic therapy of malignant biliary strictures using meso-tetrahydroxyphenylchlorin,” Eur. J. Gastroenterol. Hepatol. 19, 479–485�2007�.
68A. Hansch, O. Frey, M. Gajda, G. Susanna, J. Boettcher, R. Brauer, andW. A. Kaiser, “Photodynamic treatment as a novel approach in thetherapy of arthritic joints,” Lasers Surg. Med. 40, 265–272 �2008�.
69M. Triesscheijn, M. Ruevekamp, N. Antonini, H. Neering, F. A. Stewart,and P. Baas, “Optimizing meso-tetra-hydroxyphenyl-chlorin-mediatedphotodynamic therapy for basal cell carcinoma,” Photochem. Photobiol.82, 1686–1690 �2006�.
70N. L. Oleinick, R. L. Morris, and I. Belichenko, “The role of apoptosis inresponse to photodynamic therapy: What, where, why, and how,” Photo-chem. Photobiol. Sci. 1, 1–21 �2002�.
71E. Buytaert, M. Dewaele, and P. Agostinis, “Molecular effectors of mul-tiple cell death pathways initiated by photodynamic therapy,” Biochim.Biophys. Acta 1776, 86–107 �2007�.
72B. Chen, B. W. Pogue, P. J. Hoopes, and T. Hasan, “Vascular and cellulartargeting for photodynamic therapy,” Crit. Rev. Eukaryot. Gene Expr. 16,279–305 �2006�.
73T. M. Busch, “Local physiological changes during photodynamictherapy,” Lasers Surg. Med. 38, 494–499 �2006�.
74M. Korbelik, “PDT-associated host response and its role in the therapyoutcome,” Lasers Surg. Med. 38, 500–508 �2006�.
75M. Korbelik, “Induction of tumor immunity by photodynamic therapy,” J.Clin. Laser Med. Surg. 14, 329–334 �1996�.
76P. Baas, L. Murrer, F. A. Zoetmulder, F. A. Stewart, H. B. Ris, N. vanZandwijk, J. L. Peterse, and E. J. Rutgers, “Photodynamic therapy asadjuvant therapy in surgically treated pleural malignancies,” Br. J. Cancer76, 819–826 �1997�.
77L. K. Lee, C. Whiteburst, M. L. Pantelides, and J. V. Moore, “In situcomparison of 665 nm light and 633 nm wavelength light penetration inthe human prostate gland,” Photochem. Photobiol. 62, 882–886 �1995�.
78M. L. Pantelides, C. Whitehurst, J. V. Moore, T. A. King, and N. J.Blacklock, “Photodynamic therapy for localised prostatic cancer: lightpenetration in the human prostate gland,” J. Urol. 143, 398–401 �1990�.
79T. C. Zhu, A. Dimofte, J. C. Finlay, D. Stripp, T. Busch, J. Miles, R.Whittington, S. B. Malkowicz, Z. Tochner, E. Glatstein, and S. M. Hahn,“Optical properties of human prostate at 732 nm measured in vivo duringmotexafin lutetium-mediated photodyanmic therapy,” Photochem. Photo-
biol. 81, 96–105 �2005�.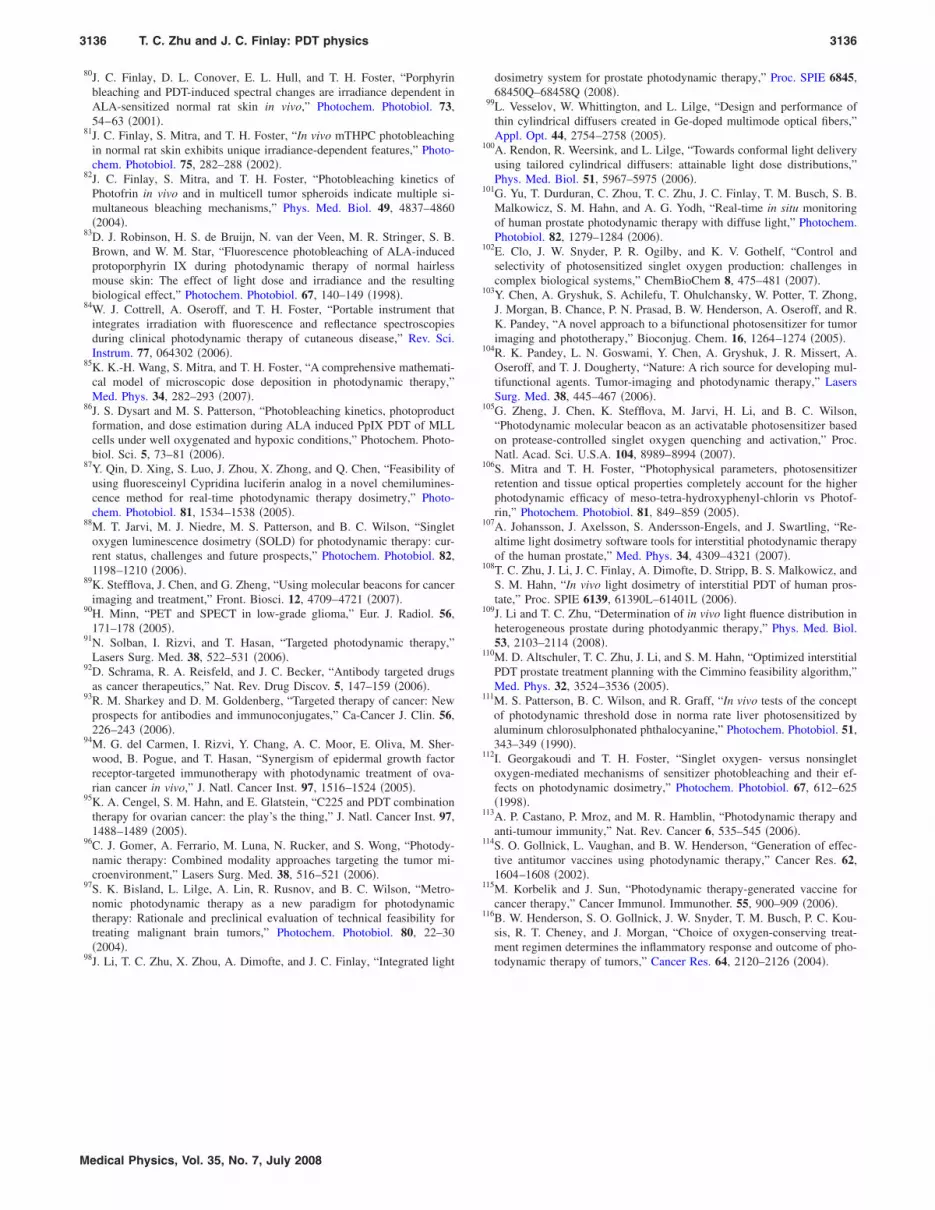
3136 T. C. Zhu and J. C. Finlay: PDT physics 3136
80J. C. Finlay, D. L. Conover, E. L. Hull, and T. H. Foster, “Porphyrinbleaching and PDT-induced spectral changes are irradiance dependent inALA-sensitized normal rat skin in vivo,” Photochem. Photobiol. 73,54–63 �2001�.
81J. C. Finlay, S. Mitra, and T. H. Foster, “In vivo mTHPC photobleachingin normal rat skin exhibits unique irradiance-dependent features,” Photo-chem. Photobiol. 75, 282–288 �2002�.
82J. C. Finlay, S. Mitra, and T. H. Foster, “Photobleaching kinetics ofPhotofrin in vivo and in multicell tumor spheroids indicate multiple si-multaneous bleaching mechanisms,” Phys. Med. Biol. 49, 4837–4860�2004�.
83D. J. Robinson, H. S. de Bruijn, N. van der Veen, M. R. Stringer, S. B.Brown, and W. M. Star, “Fluorescence photobleaching of ALA-inducedprotoporphyrin IX during photodynamic therapy of normal hairlessmouse skin: The effect of light dose and irradiance and the resultingbiological effect,” Photochem. Photobiol. 67, 140–149 �1998�.
84W. J. Cottrell, A. Oseroff, and T. H. Foster, “Portable instrument thatintegrates irradiation with fluorescence and reflectance spectroscopiesduring clinical photodynamic therapy of cutaneous disease,” Rev. Sci.Instrum. 77, 064302 �2006�.
85K. K.-H. Wang, S. Mitra, and T. H. Foster, “A comprehensive mathemati-cal model of microscopic dose deposition in photodynamic therapy,”Med. Phys. 34, 282–293 �2007�.
86J. S. Dysart and M. S. Patterson, “Photobleaching kinetics, photoproductformation, and dose estimation during ALA induced PpIX PDT of MLLcells under well oxygenated and hypoxic conditions,” Photochem. Photo-biol. Sci. 5, 73–81 �2006�.
87Y. Qin, D. Xing, S. Luo, J. Zhou, X. Zhong, and Q. Chen, “Feasibility ofusing fluoresceinyl Cypridina luciferin analog in a novel chemilumines-cence method for real-time photodynamic therapy dosimetry,” Photo-chem. Photobiol. 81, 1534–1538 �2005�.
88M. T. Jarvi, M. J. Niedre, M. S. Patterson, and B. C. Wilson, “Singletoxygen luminescence dosimetry �SOLD� for photodynamic therapy: cur-rent status, challenges and future prospects,” Photochem. Photobiol. 82,1198–1210 �2006�.
89K. Stefflova, J. Chen, and G. Zheng, “Using molecular beacons for cancerimaging and treatment,” Front. Biosci. 12, 4709–4721 �2007�.
90H. Minn, “PET and SPECT in low-grade glioma,” Eur. J. Radiol. 56,171–178 �2005�.
91N. Solban, I. Rizvi, and T. Hasan, “Targeted photodynamic therapy,”Lasers Surg. Med. 38, 522–531 �2006�.
92D. Schrama, R. A. Reisfeld, and J. C. Becker, “Antibody targeted drugsas cancer therapeutics,” Nat. Rev. Drug Discov. 5, 147–159 �2006�.
93R. M. Sharkey and D. M. Goldenberg, “Targeted therapy of cancer: Newprospects for antibodies and immunoconjugates,” Ca-Cancer J. Clin. 56,226–243 �2006�.
94M. G. del Carmen, I. Rizvi, Y. Chang, A. C. Moor, E. Oliva, M. Sher-wood, B. Pogue, and T. Hasan, “Synergism of epidermal growth factorreceptor-targeted immunotherapy with photodynamic treatment of ova-rian cancer in vivo,” J. Natl. Cancer Inst. 97, 1516–1524 �2005�.
95K. A. Cengel, S. M. Hahn, and E. Glatstein, “C225 and PDT combinationtherapy for ovarian cancer: the play’s the thing,” J. Natl. Cancer Inst. 97,1488–1489 �2005�.
96C. J. Gomer, A. Ferrario, M. Luna, N. Rucker, and S. Wong, “Photody-namic therapy: Combined modality approaches targeting the tumor mi-croenvironment,” Lasers Surg. Med. 38, 516–521 �2006�.
97S. K. Bisland, L. Lilge, A. Lin, R. Rusnov, and B. C. Wilson, “Metro-nomic photodynamic therapy as a new paradigm for photodynamictherapy: Rationale and preclinical evaluation of technical feasibility fortreating malignant brain tumors,” Photochem. Photobiol. 80, 22–30�2004�.
98J. Li, T. C. Zhu, X. Zhou, A. Dimofte, and J. C. Finlay, “Integrated light
Medical Physics, Vol. 35, No. 7, July 2008
dosimetry system for prostate photodynamic therapy,” Proc. SPIE 6845,68450Q–68458Q �2008�.
99L. Vesselov, W. Whittington, and L. Lilge, “Design and performance ofthin cylindrical diffusers created in Ge-doped multimode optical fibers,”Appl. Opt. 44, 2754–2758 �2005�.
100A. Rendon, R. Weersink, and L. Lilge, “Towards conformal light deliveryusing tailored cylindrical diffusers: attainable light dose distributions,”Phys. Med. Biol. 51, 5967–5975 �2006�.
101G. Yu, T. Durduran, C. Zhou, T. C. Zhu, J. C. Finlay, T. M. Busch, S. B.Malkowicz, S. M. Hahn, and A. G. Yodh, “Real-time in situ monitoringof human prostate photodynamic therapy with diffuse light,” Photochem.Photobiol. 82, 1279–1284 �2006�.
102E. Clo, J. W. Snyder, P. R. Ogilby, and K. V. Gothelf, “Control andselectivity of photosensitized singlet oxygen production: challenges incomplex biological systems,” ChemBioChem 8, 475–481 �2007�.
103Y. Chen, A. Gryshuk, S. Achilefu, T. Ohulchansky, W. Potter, T. Zhong,J. Morgan, B. Chance, P. N. Prasad, B. W. Henderson, A. Oseroff, and R.K. Pandey, “A novel approach to a bifunctional photosensitizer for tumorimaging and phototherapy,” Bioconjug. Chem. 16, 1264–1274 �2005�.
104R. K. Pandey, L. N. Goswami, Y. Chen, A. Gryshuk, J. R. Missert, A.Oseroff, and T. J. Dougherty, “Nature: A rich source for developing mul-tifunctional agents. Tumor-imaging and photodynamic therapy,” LasersSurg. Med. 38, 445–467 �2006�.
105G. Zheng, J. Chen, K. Stefflova, M. Jarvi, H. Li, and B. C. Wilson,“Photodynamic molecular beacon as an activatable photosensitizer basedon protease-controlled singlet oxygen quenching and activation,” Proc.Natl. Acad. Sci. U.S.A. 104, 8989–8994 �2007�.
106S. Mitra and T. H. Foster, “Photophysical parameters, photosensitizerretention and tissue optical properties completely account for the higherphotodynamic efficacy of meso-tetra-hydroxyphenyl-chlorin vs Photof-rin,” Photochem. Photobiol. 81, 849–859 �2005�.
107A. Johansson, J. Axelsson, S. Andersson-Engels, and J. Swartling, “Re-altime light dosimetry software tools for interstitial photodynamic therapyof the human prostate,” Med. Phys. 34, 4309–4321 �2007�.
108T. C. Zhu, J. Li, J. C. Finlay, A. Dimofte, D. Stripp, B. S. Malkowicz, andS. M. Hahn, “In vivo light dosimetry of interstitial PDT of human pros-tate,” Proc. SPIE 6139, 61390L–61401L �2006�.
109J. Li and T. C. Zhu, “Determination of in vivo light fluence distribution inheterogeneous prostate during photodyanmic therapy,” Phys. Med. Biol.53, 2103–2114 �2008�.
110M. D. Altschuler, T. C. Zhu, J. Li, and S. M. Hahn, “Optimized interstitialPDT prostate treatment planning with the Cimmino feasibility algorithm,”Med. Phys. 32, 3524–3536 �2005�.
111M. S. Patterson, B. C. Wilson, and R. Graff, “In vivo tests of the conceptof photodynamic threshold dose in norma rate liver photosensitized byaluminum chlorosulphonated phthalocyanine,” Photochem. Photobiol. 51,343–349 �1990�.
112I. Georgakoudi and T. H. Foster, “Singlet oxygen- versus nonsingletoxygen-mediated mechanisms of sensitizer photobleaching and their ef-fects on photodynamic dosimetry,” Photochem. Photobiol. 67, 612–625�1998�.
113A. P. Castano, P. Mroz, and M. R. Hamblin, “Photodynamic therapy andanti-tumour immunity,” Nat. Rev. Cancer 6, 535–545 �2006�.
114S. O. Gollnick, L. Vaughan, and B. W. Henderson, “Generation of effec-tive antitumor vaccines using photodynamic therapy,” Cancer Res. 62,1604–1608 �2002�.
115M. Korbelik and J. Sun, “Photodynamic therapy-generated vaccine forcancer therapy,” Cancer Immunol. Immunother. 55, 900–909 �2006�.
116B. W. Henderson, S. O. Gollnick, J. W. Snyder, T. M. Busch, P. C. Kou-sis, R. T. Cheney, and J. Morgan, “Choice of oxygen-conserving treat-ment regimen determines the inflammatory response and outcome of pho-todynamic therapy of tumors,” Cancer Res. 64, 2120–2126 �2004�.





























