Embed Size (px)
Citation preview
doi:10.1016/j.jcmg.2009.06.006 2009;2;1126-1140 J. Am. Coll. Cardiol. Img.
Torre-Amione, and William A. Zoghbi Jerry D. Estep, Dipan J. Shah, Sherif F. Nagueh, John J. Mahmarian, Guillermo
The Role of Multimodality Cardiac Imaging in the Transplanted Heart
This information is current as of May 10, 2011
http://imaging.onlinejacc.org/cgi/content/full/2/9/1126located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by on May 10, 2011 imaging.onlinejacc.orgDownloaded from
S
Ti
JG
H
H
f
a
T
r
s
i
c
C
Hleirlmviatdpsio(t(n
FI
M
J A C C : C A R D I O V A S C U L A R I M A G I N G V O L . 2 , N O . 9 , 2 0 0 9
© 2 0 0 9 B Y T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N I S S N 1 9 3 6 - 8 7 8 X / 0 9 / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R I N C . D O I : 1 0 . 1 0 1 6 / j . j c m g . 2 0 0 9 . 0 6 . 0 0 6
T A T E - O F - T H E - A R T P A P E R
he Role of Multimodality Cardiac Imagingn the Transplanted Heart
erry D. Estep, MD, Dipan J. Shah, MD, Sherif F. Nagueh, MD, John J. Mahmarian, MD,uillermo Torre-Amione, MD, PHD, William A. Zoghbi, MD
ouston, Texas
eart transplantation (HT) is an established life-saving treatment option for patients with end-stage heart
ailure. Despite many advances in the field, the development of acute cellular rejection (ACR) and cardiac
llograft vasculopathy (CAV) represent significant causes of 1- and 5-year morbidity and mortality, respectively.
he search for noninvasive techniques to assess cardiac allograft function and detect treatable ACR and CAV
emains a priority objective for heart transplant professionals. In this review we will: 1) highlight the clinical
ignificance of ACR and CAV in adult cardiac transplant recipients and 2) discuss how different noninvasive
maging modalities (echocardiography, cardiac computed tomography, myocardial perfusion imaging, and
ardiac magnetic resonance) have been used in the evaluation of these clinical challenges after HT. (J Am Coll
ardiol Img 2009;2:1126–40) © 2009 by the American College of Cardiology Foundation
oaara1aaio
A
Cmmtwar
Hen, T
eart transplantation (HT) is an establishedife-saving treatment option for patients withnd-stage heart failure. Despite many advancesn the field, the development of acute cellularejection (ACR) and cardiac allograft vascu-opathy (CAV) represent significant causes of
orbidity and mortality (1). Historically, sur-eillance for ACR and CAV has been based onnvasive procedures, which carry inherent risksnd high costs. The search for noninvasiveechniques to assess allograft function andetect treatable ACR and CAV remains ariority objective for heart transplant profes-ionals. Noninvasive imaging techniques usedn this regard include transthoracic echocardi-graphy, multidetector computed tomographyMDCT), single-photon emission computedomography-myocardial perfusion imagingSPECT-MPI), and cardiac magnetic reso-ance (CMR). The ideal test for the detection
rom the Department of Cardiology, Section of Heart Failure andnstitute, Methodist DeBakey Heart and Vascular Center, Housto
anuscript received April 9, 2009; revised manuscript received June 1
imaging.onlinejacc.Downloaded from
f ACR and CAV should be highly sensitivend specific, able to evaluate changes beforend after treatment, noninvasive with higheproducibility, and associated with low costnd favorable outcome. In this review, we will:) highlight the clinical significance of ACRnd CAV in adult cardiac transplant recipients;nd 2) discuss how different noninvasive imag-ng modalities have been used in the evaluationf these clinical challenges after HT.
CR
linical significance. In ACR, effector T cellsediate an inflammatory response that leads toyocardial edema and myocyte damage. Rou-
ine surveillance of ACR is currently performedith endomyocardial biopsy (EMB) and is
ssociated with good clinical results. The cur-ent management strategy depends on the his-
art Transplantation, and Cardiovascular Imagingexas.
9, 2009, accepted June 24, 2009.
by on May 10, 2011 org

toasaEiuuh
fbwunaAWmsf(tAcwEC
meiewrpheweoa
S
didiaAlpaD
ctphcd(talptobs2t(btdftepLtt
T
rbIppr([cfa9abvEEus(Dlw
tissue Doppler imaging
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 2 , N O . 9 , 2 0 0 9
S E P T E M B E R 2 0 0 9 : 1 1 2 6 – 4 0
Estep et al.
Multimodality Cardiac Imaging in the Transplanted Heart
1127
ologic type and grade of rejection and the presencer absence of hemodynamic compromise (decreasedllograft systolic function and/or hemodynamic in-tability). Using the International Society of Heartnd Lung Transplantation revised grading system,MB grade 2R (previously 3A) or higher rejection
s considered clinically significant and prompts these of high-dose corticosteroids and possibly these of lymphocyte-depleting agents in patients withemodynamic compromise.Although EMB is considered the gold standard
or the diagnosis of ACR, its value may be limitedy sampling error, interobserver variability, andide variability in the frequency and duration of itsse as surveillance among transplant centers. Severaloninvasive imaging techniques (clinically acceptednd investigational) have been performed to detectCR at different stages in the disease process (Fig. 1).ith current advances in immunosuppression, theajority of patients who develop ACR have no
ignificant changes in left ventricular (LV) ejectionraction regardless of the imaging modality used2–4). However, monitoring cardiac allograft sys-olic function is important in suspected or provenCR because more aggressive immunosuppression
an lead to improvement in LV function in patientsith depressed function.chocardiography and ACR. CONVENTIONAL ECHO-
ARDIOGRAPHY. Although wall thickness and LVass measured by M-mode and 2-dimensional
chocardiography have been shown to increase dur-ng ACR episodes (5), ACR-induced myocardialdema may manifest by subtle changes in relativeall thickness, accounting in part for the conflicting
esults on the usefulness of these echocardiographyarameters to detect ACR (6–8). Investigatorsave also noted that the presence of a pericardialffusion in cardiac transplant recipients is associatedith a higher incidence of ACR (9). Pericardial
ffusion, however, occurs frequently in the post-perative period, hence its low sensitivity (�49%)nd specificity (�74%) to detect ACR (10).
PECTRAL DOPPLER IMAGING. Early investigationsemonstrated altered LV diastolic twist mechanics
n the absence of systolic dysfunction to suggest thatiastolic dysfunction precedes systolic abnormalities
n patients with ACR (11). Multiple studies havelso evaluated LV Doppler inflow indexes to detectCR, including early diastolic (E) peak velocity,
ate diastolic (A) peak velocity, E/A ratio, E-waveressure half time (PHT), and isovolumic relax-tion time (IVRT) (12,13). Standard transmitral
oppler-derived indexes in cardiac transplant re- eimagDownloaded from
ipients have had limitations in predicting ACR;hese limitations relate to the influence of severalarameters on these indexes including donor age,eart rate (which may be variable in the setting ofardiac denervation), loading conditions, and theissociation between the electrical activity of 2 atriaespecially important with the biatrial anastomosisechnique when evaluating older studies). Mena etl. (12) performed a systematic review of the pub-ished literature between 1967 and 2005 and re-orted that the majority of studies that examinedhe change in the mitral E and A peak velocitiesver time did not predict ACR and the correlationetween ACR and PHT and IVRT was not con-istent (sensitivity and specificity range for PHT3% to 87% and 76% to 98%; IVRT 28%o 85% and 80% to 98%, respectively)12). The discordance in the literature maye in part related to significant interpa-ient and intrapatient variability and theependence of these indexes on multipleactors in addition to ACR (8). In addi-ion to transmitral Doppler indexes, sev-ral studies have examined changes inulmonary vein flow indexes (8,10,14),V diastolic flow propagation (8,15), and
he myocardial performance index (16,17)o detect ACR—with conflicting results.
ISSUE DOPPLER IMAGING (TDI). Moreecently, the use of TDI to detect ACR haseen investigated, with improved results.nvestigators from Berlin, Germany, usingulsed wave–TDI obtained from the basalosterior wall, have demonstrated that aeduction in peak systolic radial velocitySm) and peak early diastolic velocity (Emalso known as Ea]) is helpful in detectingardiac rejection (sensitivity and specificityor Sm reduction �10%, �87% and �94%; sensitivitynd specificity for Em reduction �10%, 90% and6%, respectively) (3,18). These investigators havelso reported on the value of serial TDI screeningased on the high negative and positive predictivealues of changes in diastolic parameters (i.e., �10%m reduction) for ACR to guide the effective use ofMBs (19). In contrast, with the mitral valve annulussed as the site for analysis, some studies have foundignificant decreases in systolic velocities with ACR8,20), whereas other investigators have not (15).iscordant results have also been seen by color Dopp-
er or conventional TDI (12,20). These discrepanciesith regard to the clinical usefulness of these param-
A B B
A N D
ACR �
CAV �
vascu
CMR �
reson
DSE �
echoc
EMB �
HT �
IVUS
LV �
MACE
event
MDCT
comp
SPECT
emiss
tomog
perfus
TDI �
ters may be secondary to differences in method
by on May 10, 2011 ing.onlinejacc.org
R E V I A T I O N S
A C R O N YM S
acute cellular rejection
cardiac allograft
lopathy
cardiac magnetic
ance
dobutamine stress
ardiography
endomyocardial biopsy
heart transplantation
� intravascular ultrasound
left ventricular
� major adverse cardiac
s
� multidetector
uted tomography
-MPI � single-photon
ion computed
raphy-myocardial
ion imaging
ology,

suwFehg(iptnt
P
NceritpmldcmctlCus
tcaatdccavmshcdasdtscauf
tbmdCi
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 2 , N O . 9 , 2 0 0 9
S E P T E M B E R 2 0 0 9 : 1 1 2 6 – 4 0
Estep et al.
Multimodality Cardiac Imaging in the Transplanted Heart
1128
ome studies using pulsed wave versus color TDI andsing tissue Doppler Ea from different myocardialalls or mitral valve annulus locations (3,14,15,20).inally, the E/Ea ratio—a validated parameter forstimation of LV filling pressure in the transplantedeart (21) (Fig. 2)—has been evaluated by 2 differentroups to detect ACR, with conflicting results10,14). The clinical usefulness of this TDI-derivedndex to detect ACR remains unclear given thataradoxical septal motion is noted often in cardiacransplant recipients and in the current era of immu-osuppression, patients with ACR are often asymp-omatic with normal ventricular filling pressure.
ROMISING ECHOCARDIOGRAPHIC TECHNIQUES.
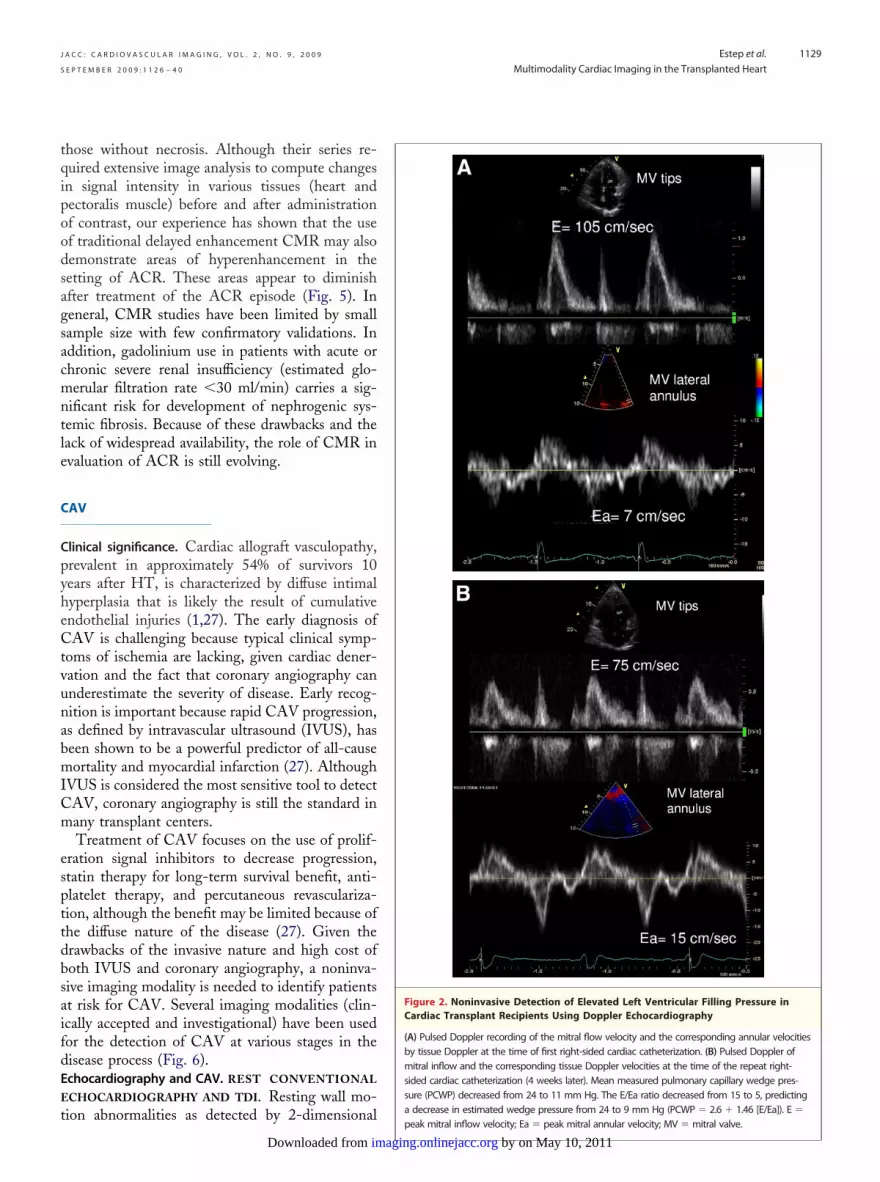
ovel echocardiographic techniques have been re-ently developed and have been applied to thevaluation of ACR. These include strain and strainate imaging (22) (Fig. 3), 2-dimensional derivedntegrated backscatter (6), automated border detec-ion with acoustic quantification to measure LVeak filling rate (23), and color Doppler imaging toeasure late isovolumic relaxation myocardial ve-
ocity gradients and early diastolic timing intervalifferences (14) (Table 1). These quantitative echo-ardiographic techniques of regional and globalyocardial function show promise to identify sub-
linical LV dysfunction in a small number of cardiacransplant recipients and need further validation inarger studies.MR and ACR. Although many transplant centersse echocardiography to detect cardiac allograft
CMR*
*
*Echocardiography
Immune-Mediated Cardiac Allograft Injury
Myocardial Mononuclear Cell Infiltration
Myocardial Necrosisand Edema
Cardiac Allograft Diastolic Dysfunction
Figure 1. Different Noninvasive Imaging Techniques PerformedCellular Rejection
ACR � acute cellular rejection; CMR � cardiac magnetic resonanceand Lung Transplantation.
ystolic dysfunction in the setting of cardiac rejec- p
bimaging.onlinejacc.orgDownloaded from
ion, CMR enables imaging throughout the cardiacycle and provides excellent spatial resolution toccurately measure diastolic and systolic volumesnd hence left and right ventricular ejection frac-ions (24) (Fig. 4). CMR may also be useful in theetection of ACR by its ability to quantitatehanges in myocardial mass (25) or more specifi-ally to detect myocardial edema. The latter isccomplished by measurement of myocardial T2alues, which are elevated in the setting of increasedyocardial water content. Marie et al. (26) demon-
trated in 68 cardiac transplant recipients that aigher than normal T2 value (�56 ms) was suffi-iently accurate (sensitivity 89%; specificity 70%) toetect ACR defined by EMB (grade �2R). Anbnormal T2 value was also a strong predictor ofubsequent biopsy-defined ACR, suggesting earlyetection of ACR. Although promising, this inves-igation involved a select cohort of patients withuspected rejection on the basis of clinical or echo-ardiographic data; therefore, the true sensitivitynd specificity of this method to detect ACR innselected cohorts is currently unknown and needsurther evaluation.
With the administration of a paramagnetic con-rast medium, gadolinium, CMR studies have alsoeen used to detect inflammatory changes in theyocardium. Almenar et al. (2), using gadolinium-
iethylene triamine pentaacetic acid-enhancedMR in 40 cardiac transplant recipients, showed an
ncrease in relative myocardial contrast uptake in
Clinically Accepted
Investigational**
Cardiac AllograftSystolic Dysfunction
ISHLT Biopsy Grading (2004)Grade 0R No ACRGrade 1R Mild, Low-gradeGrade 2R Moderate, IntermediateGrade 3R Severe, High-grade
*
**
*
EchocardiographyScintigraphy CMR and Cardiac CT
arious Stages of Cardiac Involvement to Detect Acute
� computed tomography; ISHLT � International Society of Heart
at V
; CT
atients with necrosis on EMB compared with
y on May 10, 2011
tqipoodsagsacmntle
C
CpyheCtvunabmICm
espttdbsaifdEE
t
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 2 , N O . 9 , 2 0 0 9
S E P T E M B E R 2 0 0 9 : 1 1 2 6 – 4 0
Estep et al.
Multimodality Cardiac Imaging in the Transplanted Heart
1129
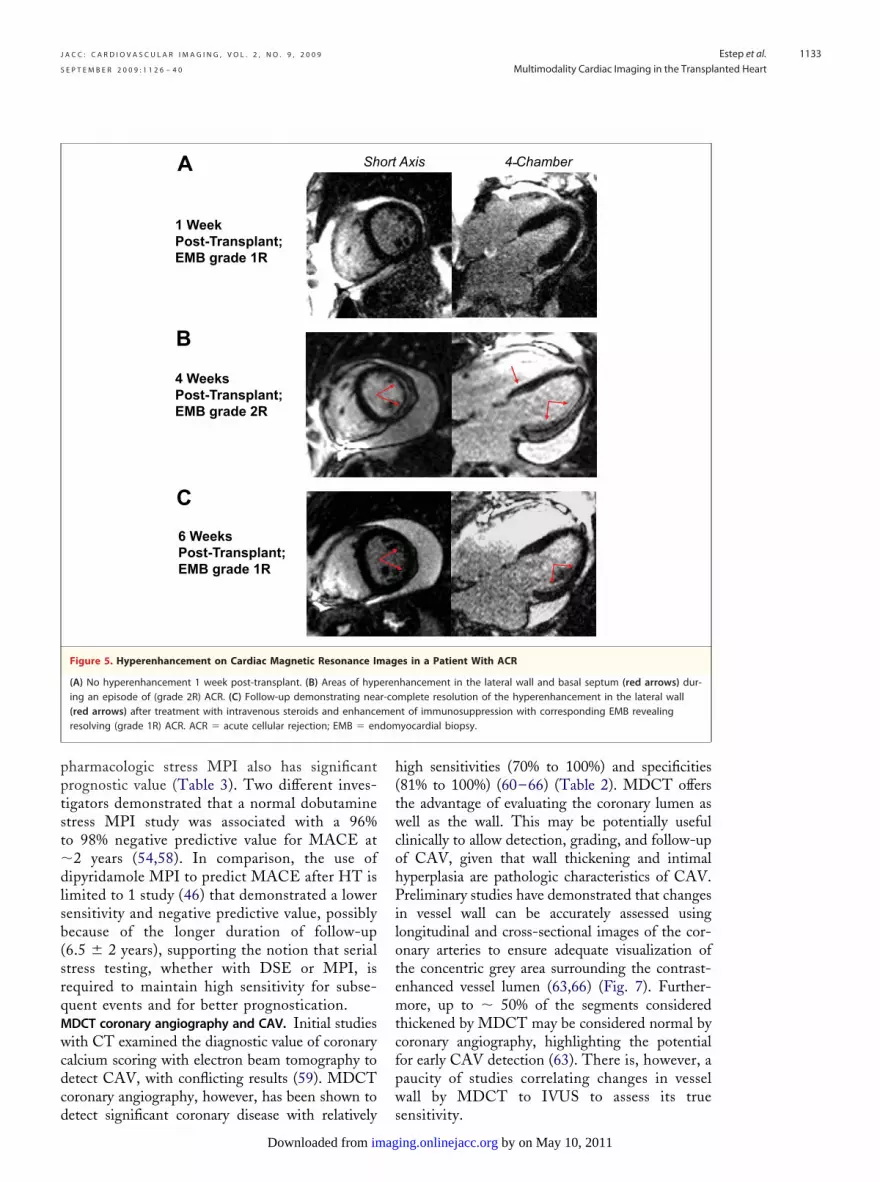
hose without necrosis. Although their series re-uired extensive image analysis to compute changesn signal intensity in various tissues (heart andectoralis muscle) before and after administrationf contrast, our experience has shown that the usef traditional delayed enhancement CMR may alsoemonstrate areas of hyperenhancement in theetting of ACR. These areas appear to diminishfter treatment of the ACR episode (Fig. 5). Ineneral, CMR studies have been limited by smallample size with few confirmatory validations. Inddition, gadolinium use in patients with acute orhronic severe renal insufficiency (estimated glo-erular filtration rate �30 ml/min) carries a sig-
ificant risk for development of nephrogenic sys-emic fibrosis. Because of these drawbacks and theack of widespread availability, the role of CMR invaluation of ACR is still evolving.
AV
linical significance. Cardiac allograft vasculopathy,revalent in approximately 54% of survivors 10ears after HT, is characterized by diffuse intimalyperplasia that is likely the result of cumulativendothelial injuries (1,27). The early diagnosis ofAV is challenging because typical clinical symp-
oms of ischemia are lacking, given cardiac dener-ation and the fact that coronary angiography cannderestimate the severity of disease. Early recog-ition is important because rapid CAV progression,s defined by intravascular ultrasound (IVUS), haseen shown to be a powerful predictor of all-causeortality and myocardial infarction (27). Although
VUS is considered the most sensitive tool to detectAV, coronary angiography is still the standard inany transplant centers.Treatment of CAV focuses on the use of prolif-
ration signal inhibitors to decrease progression,tatin therapy for long-term survival benefit, anti-latelet therapy, and percutaneous revasculariza-ion, although the benefit may be limited because ofhe diffuse nature of the disease (27). Given therawbacks of the invasive nature and high cost ofoth IVUS and coronary angiography, a noninva-ive imaging modality is needed to identify patientst risk for CAV. Several imaging modalities (clin-cally accepted and investigational) have been usedor the detection of CAV at various stages in theisease process (Fig. 6).chocardiography and CAV. REST CONVENTIONAL
CHOCARDIOGRAPHY AND TDI. Resting wall mo-
ion abnormalities as detected by 2-dimensionalimagDownloaded from
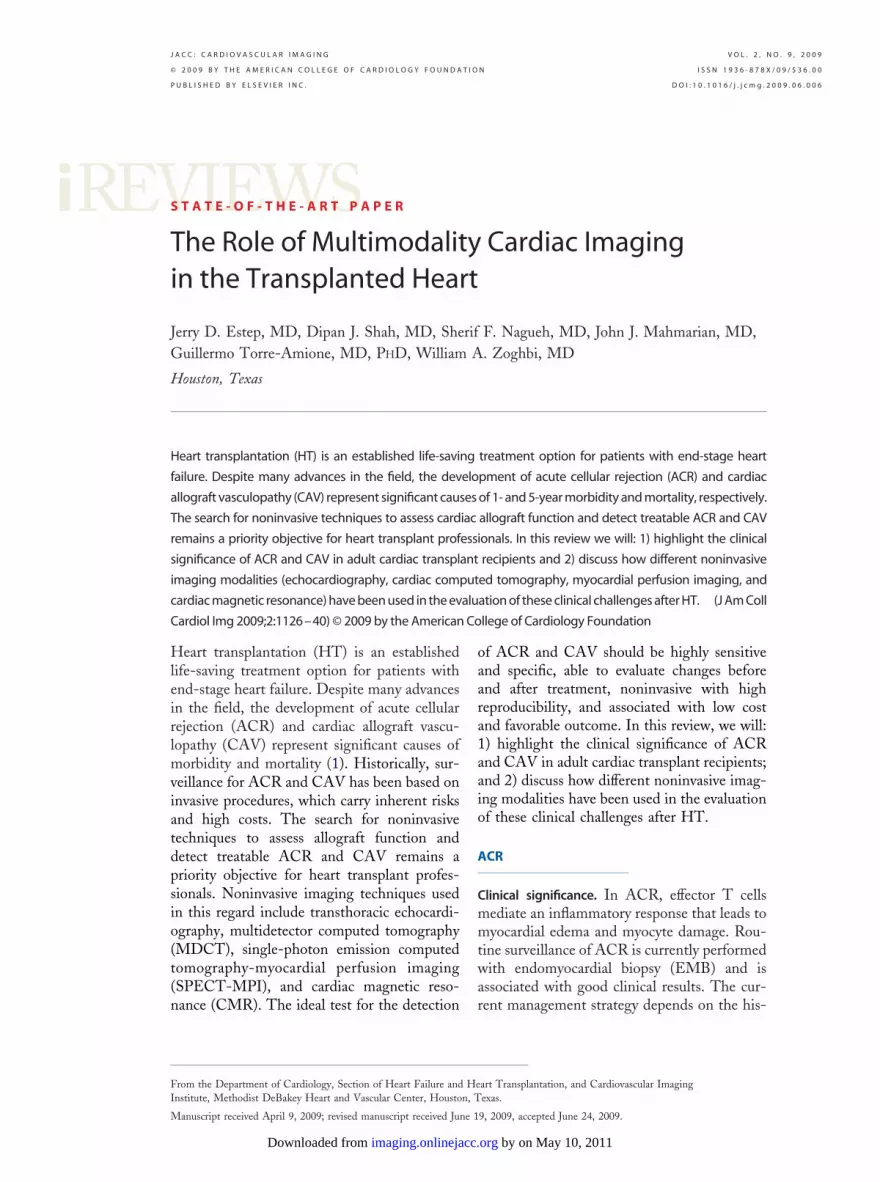
Figure 2. Noninvasive Detection of Elevated Left Ventricular Filling Pressure inCardiac Transplant Recipients Using Doppler Echocardiography
(A) Pulsed Doppler recording of the mitral flow velocity and the corresponding annular velocitiesby tissue Doppler at the time of first right-sided cardiac catheterization. (B) Pulsed Doppler ofmitral inflow and the corresponding tissue Doppler velocities at the time of the repeat right-sided cardiac catheterization (4 weeks later). Mean measured pulmonary capillary wedge pres-sure (PCWP) decreased from 24 to 11 mm Hg. The E/Ea ratio decreased from 15 to 5, predictinga decrease in estimated wedge pressure from 24 to 9 mm Hg (PCWP � 2.6 � 1.46 [E/Ea]). E �
peak mitral inflow velocity; Ea � peak mitral annular velocity; MV � mitral valve.
by on May 10, 2011 ing.onlinejacc.org
ea(tsps(rsav9d
p(vi
S
rhbctI(bt4pdcIfi(siasp
P
cC(smchtcsHTwoebwcoati
P
C
AVC � aortic valve clo
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 2 , N O . 9 , 2 0 0 9
S E P T E M B E R 2 0 0 9 : 1 1 2 6 – 4 0
Estep et al.
Multimodality Cardiac Imaging in the Transplanted Heart
1130
chocardiography derived from 12 different studiesre in general associated with low sensitivities�47%; range 12% to 80%) but high specificity forhe presence of CAV (�84%; range 69% to 100%),upporting the notion that this finding shouldrompt further testing to exclude CAV (13). A fewtudies have examined resting TDI to detect CAV18,28). After excluding ACR, Hummel et al. (18)eported that pulse wave TDI-derived radial peakystolic velocity (Sm value �10 cm/s) was associ-ted with a 97% likelihood for CAV, whereas Smalues �11 cm/s excluded accelerated CAV with0% probability. This group of investigators also
al Strain Derived From the Speckle-Tracking Technique
(38%), peak 47%, obtained from the parasternal short axis viewst-heart transplantation (biopsy grade 2R performed on the samein the global radial strain (58%), peak 68%, 2 weeks later afternosuppression (biopsy grade 1R). ACR � acute cellular rejection;sure.
emonstrated that serial TDI can potentially spare t
bimaging.onlinejacc.orgDownloaded from
atients unnecessary routine invasive examinations28). These are promising results that need furtheralidation but may point to advanced CAV, affect-ng myocardial properties at rest.
TRESS ECHOCARDIOGRAPHY. Stress echocardiog-aphy using exercise, dipyridamole, and dobutamineas been evaluated to detect CAV (Table 2). Thelunted heart rate response to exercise because ofardiac denervation limits the sensitivity (range 15%o 33%) of exercise testing to detect CAV (29–31).n contrast, the use of pharmacologic stress testingdipyridamole and dobutamine) to detect CAV haseen shown to be more sensitive (�85%; range 50%o 100%) (32–43). The variable specificity (range1% to 95%) of dobutamine stress echocardiogra-hy (DSE) is likely a reflection of the differences inefining the presence and severity of CAV byoronary angiography. When compared withVUS—a more sensitive gold standard—the speci-city of DSE for CAV is higher (83% to 88%)42,43). In comparison, Eroglu et al. (40) demon-trated that quantitative DSE using strain ratemaging detects CAV accurately regardless of thengiographic significance and that a post-systolictrain index �34% at peak stress was the bestarameter.
ROGNOSTIC VALUE OF ECHOCARDIOGRAPHY. Thelinical usefulness of noninvasive imaging inAV relates also to the test’s prognostic value
Table 3). Several investigators have demon-trated the impact of resting wall motion abnor-alities and DSE findings on major adverse
ardiac events (MACE) after HT, includingeart failure, unstable angina, myocardial infarc-ion, revascularization, retransplantation, andardiac death (32–37,42,44 – 48). The majority oftudies were performed more than 3 years afterT, with a follow-up on average of �3 years.he negative predictive value of a normal DSEas very high (�3% risk of experiencing MACEver the ensuing year). As demonstrated by Spest al. (42), serial DSE may best prognosticateased on the finding that worsening DSE resultsere as predictive of subsequent events as serial
oronary angiography or IVUS. Based on theseverall results, annual evaluation with DSE is ancceptable alternative to invasive means for de-ection of CAV in transplant centers experiencedn stress echocardiography.
ROMISING ECHOCARDIOGRAPHIC TECHNIQUES.
ontrast-enhanced echocardiography is a recent
Figure 3. Global Radi
(A) Global radial strainin a patient 1 week poday). (B) Improvementenhancement in immu
echnique that allows quantification of coronary
y on May 10, 2011

fltisrCdvero
ttMDc(otme
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 2 , N O . 9 , 2 0 0 9
S E P T E M B E R 2 0 0 9 : 1 1 2 6 – 4 0
Estep et al.
Multimodality Cardiac Imaging in the Transplanted Heart
1131
ow reserve and/or myocardial perfusion mismatcho detect significant coronary artery disease. Prelim-nary studies in cardiac transplant recipients usingtress echocardiography with contrast (49,50) showelatively high accuracy (85% to 89%) to detectAV (Table 2). Moreover, Tona et al. (51) haveemonstrated the validity of a lower coronary flowelocity pattern and flow reserve with contrastchocardiography as noninvasive markers of CAV-elated MACE. These results, however, are based
Table 1. Studies Evaluating the Accuracy of Different Echocardi
Author, Year (Ref. #)Total Patients
(Prevalence of ACR)
Angermann et al., 1997 (6) 52 (18%*) Integrate
(PW 2D-
(Septal 2
Puleo et al., 1998 (15) 121 (13%) PW-TDI
(Ea of in
Mankad et al., 1999 (20) 78 (18%) Color-co
(combindiasto
(posteriotime-g
Moidl et al., 1999 (23) 94 (20%) Automat
(peak fill
(peak fill�18%
Stengel et al., 2001 (8) 41 (39%) PW-TDI
(Aa of la
Dandel et al., 2002 (3) 190 (17%*) PW-TDI
(Sm of b
(Ea of ba
Palka et al., 2005 (14) 44 (27%) PW and
(Ea of se
(peak lat
(onset E
(onset ET
Sun et al., 2005 (10) 2-D and standard Doppler Grade �
(�2 amo
223 (37%*) Post-HT
183 (27%*) Post-HT
264 (29%*) PW-TDI
(Aa of se
Marciniak et al., 2007 (22) 31 (32%) Color TD
(mid-LVP
(mid-LVP
*Prevalence of ACR based on the percentage of biopsies with ACR defined by tclinical symptoms. ‡Peak late isovolumic relaxation myocardial velocity gradientand early diastolic septal MV annulus velocity (EMed). �Timing difference betwvelocity (EMitr).Aa � peak late diastolic velocity; ACR � acute cellular rejection; dB � decibe
transplantation; IVRT � isovolumic relaxation time; LVPW � left ventricular poswave 2-dimensional-integrated backscatter; Sm � peak radial systolic velocity;
n a small number of patients, and further valida- a
imagDownloaded from
ion studies are warranted before widespread adop-ion can be advocated.PI and CAV. MPI DIAGNOSTIC VALUE. Similar toSE, several studies have examined MPI using exer-
ise, dipyridamole, and dobutamine to detect CAVTable 2). The overall sensitivity and specificity rangef MPI to detect CAV is broad (21% to 92% and 55%o 100%, respectively) (45,46,52–56). This variabilityay be explained by differences in the timing of the
xaminations, the stressors and/or MPI agents used,
phy Techniques to Detect Acute Cellular Rejection
Methodrameter Cutoff Value)
Gold Standard(EMB Score) Sensitivity
ackscatter Grade �1B
crease �1.5 dB) 88%
increase �1.5 dB) 83%
Grade �3A
r wall �16 cm/s) 76%
TDI Grade �1B
eak MV systolic and peakelocity �135 mm/s)
93%
ll tissue Doppler diastolicient integral �0.26)
91%
order detection Grade �2
rate �4.0 EDV/s) 100%
rate �4.0 EDV/s anduction)
100%
Grade �3A
l MV annulus �8.7 cm/s) 82%
Clinically relevant†
posterior wall reduction �10%) 88%
posterior wall reduction �10%) 89%
r M-mode TDI Grade �3A
MV annulus �12 cm/s) 69%
R MVG‡ �0.1/s) 88%
e –onset Emed§ ��35 ms) 81%
–onset EMitr� �15 ms) 81%
PE, IVRT �90 ms E/A �1.7)
months 57%
months 60%
/lateral MV annulus �9.0 cm/s) 67%
Grade �1B
adial peak systolic strain �30%) 85%
adial peak systolic SR �3.0 s-1) 80%
MB score. †Clinically relevant ACR defined as EMB grade �2 plus grades 1A and 1e left ventricular posterior wall. §Timing difference between onset of mitral earlynset of early diastolic velocity at lateral tricuspid (ETric) annulus and LV early di
� peak early diastolic velocity; EDV � end diastolic volume; EMB � endomyocr wall; MV � mitral valve; NPV � negative predictive value; PE � pericardial effustrain rate; TDI � tissue Doppler imaging.
ogra
(Pa Specificity NPV
d b
IB in 89% 97%
D-IB 85% 96%
ferio 88% 96%
ded
ed plic v
71% 98%
r warad
61% 97%
ed b
ing 70% 100%
ingred
95% 100%
tera 53% 82%
asal 95% 97%
sal 97% 98%
colo
ptal 46% 80%
e IV 58% 93%
wav 84% 92%
ric 84% 92%
1B
ng
�6 54% 68%
�6 93% 86%
ptal 49% 78%
I
W r 90% 93%
W r 86% 90%
he E B when accompanied byof th diastolic velocity (E wave)een o astolic lateral MV annulus
ls; Ea ardial biopsy; HT � heartterio sion; PW 2D-IB � pulsedSR �
nd the variable criteria used to diagnosis CAV.
by on May 10, 2011 ing.onlinejacc.org

SCdawtcm�
asieutCflsr
ssMM
tilataspeadttsp
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 2 , N O . 9 , 2 0 0 9
S E P T E M B E R 2 0 0 9 : 1 1 2 6 – 4 0
Estep et al.
Multimodality Cardiac Imaging in the Transplanted Heart
1132
imilar to the DSE literature, the sensitivity to detectAV overall increases with the inclusion of studies thatefine CAV as coronary stenosis �50% (45,54,57). Inddition, early studies were performed using thallium,hich may encounter more attenuation artifacts than
echnetium-labeled radiopharmaceuticals and may ac-ount for the reported reduced accuracy compared withore recent studies (sensitivity �86% and specificity80%) using technetium-labeled agents (46,52–54).Compared with exercise and dipyridamole, dobut-
mine has been reported to be advantageous as atressor because of its more reliable induction ofschemia in cardiac transplant recipients (inotropicffect, less blunted heart rate response). Moreover, these of vasodilators with MPI may be limited in cardiacransplant recipients because the diffuse, microvascularAV may impair the necessary increase in coronaryow reserve to trigger the flow heterogeneity to detectignificant stenosis. Despite these observations, more
A
B
Figure 4. CMR Assessment of Left and Right Ventricular Systolic FCardiac Rejection
(A) Pre-treatment biventricular dysfunction with a large thrombus inthere was substantial improvement in biventricular function, and ththerapy. Full-motion cine images can be viewed online. LVEF � leftfraction.
ecent studies using dipyridamole MPI have demon-
bimaging.onlinejacc.orgDownloaded from
trated comparable sensitivity (range 80% to 92%) andpecificity (range 86% to 92%) to dobutamine stress
PI to detect CAV (46,52–54).PI PROGNOSTIC VALUE. Similar to DSE, the po-
ential clinical usefulness of SPECT-MPI relates tots prognostic value. Although exercise testinginked with echocardiography and MPI is associ-ted with low sensitivity to detect CAV, investiga-ors have demonstrated that a normal exercise MPIt 1 year is a significant predictor of 1- and 5-yearurvival (45,48). Elhendy et al. (58) reported on 65atients who underwent symptom-limited bicyclexercise with technetium-99m tetrofosmin MPInd demonstrated a similar ability to predict cardiaceath in comparison with dobutamine. In contrasto these studies, Bacal et al. (34) reported thathallium scintigraphy with treadmill testing in amaller number of patients was not an independentredictor of long-term 4-year survival.
tion Pre- and Post-Treatment of an Episode of
e right ventricular apex (arrow). (B) Two weeks post-treatmentrombus appears to have decreased in size with anticoagulationtricular ejection fraction; RVEF � right ventricular ejection
unc
the thven
Similar to the overall results of exercise MPI,
y on May 10, 2011
pptst�dlsb(srqMwcdcd
h(twcohPilotemtcfpw
dom
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 2 , N O . 9 , 2 0 0 9
S E P T E M B E R 2 0 0 9 : 1 1 2 6 – 4 0
Estep et al.
Multimodality Cardiac Imaging in the Transplanted Heart
1133
harmacologic stress MPI also has significantrognostic value (Table 3). Two different inves-igators demonstrated that a normal dobutaminetress MPI study was associated with a 96%o 98% negative predictive value for MACE at
2 years (54,58). In comparison, the use ofipyridamole MPI to predict MACE after HT is
imited to 1 study (46) that demonstrated a lowerensitivity and negative predictive value, possiblyecause of the longer duration of follow-up6.5 � 2 years), supporting the notion that serialtress testing, whether with DSE or MPI, isequired to maintain high sensitivity for subse-uent events and for better prognostication.DCT coronary angiography and CAV. Initial studiesith CT examined the diagnostic value of coronary
alcium scoring with electron beam tomography toetect CAV, with conflicting results (59). MDCToronary angiography, however, has been shown to
ShA
1 Week Post-Transplant; EMB grade 1R
B
4 WeeksPost-Transplant;EMB grade 2R
C
6 Weeks Post-Transplant;EMB grade 1R
Figure 5. Hyperenhancement on Cardiac Magnetic Resonance Im
(A) No hyperenhancement 1 week post-transplant. (B) Areas of hyping an episode of (grade 2R) ACR. (C) Follow-up demonstrating nea(red arrows) after treatment with intravenous steroids and enhanceresolving (grade 1R) ACR. ACR � acute cellular rejection; EMB � en
etect significant coronary disease with relatively s
imagDownloaded from
igh sensitivities (70% to 100%) and specificities81% to 100%) (60–66) (Table 2). MDCT offershe advantage of evaluating the coronary lumen asell as the wall. This may be potentially useful
linically to allow detection, grading, and follow-upf CAV, given that wall thickening and intimalyperplasia are pathologic characteristics of CAV.reliminary studies have demonstrated that changes
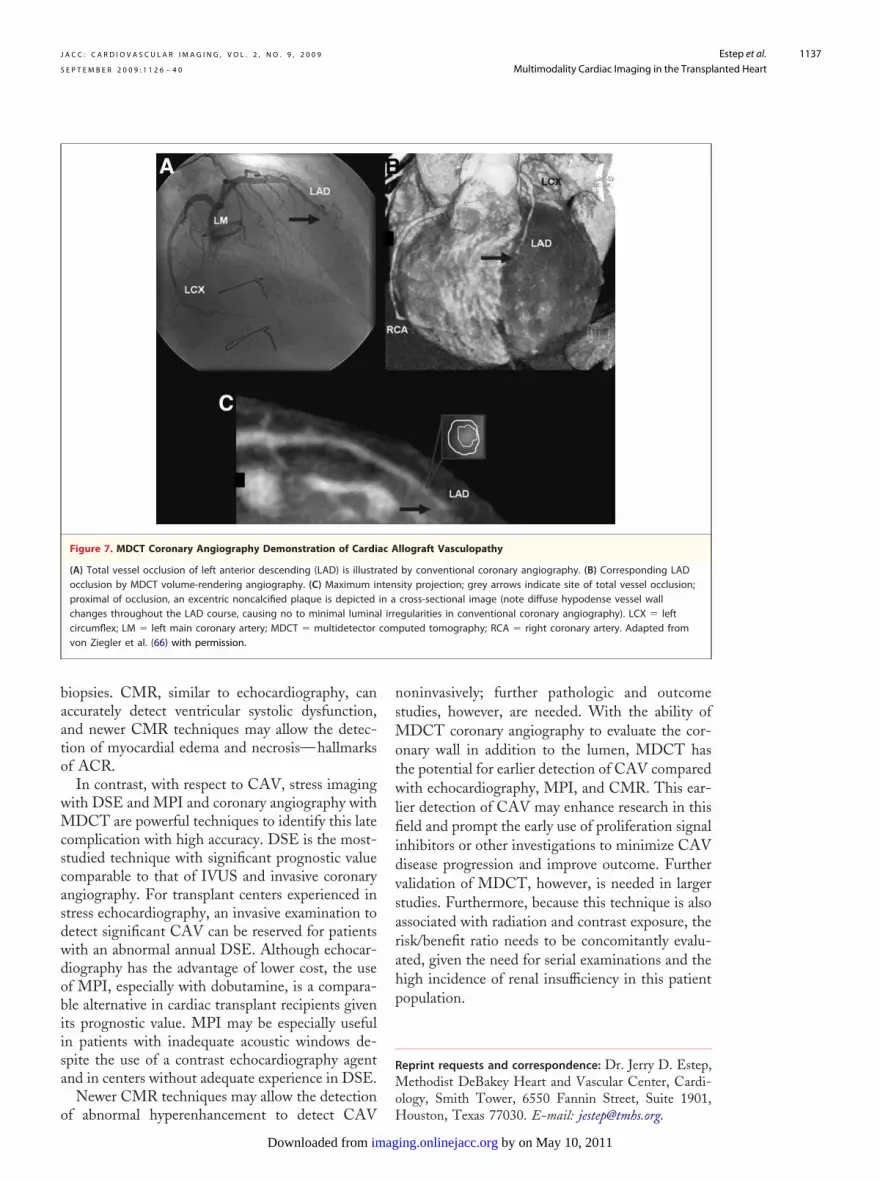
n vessel wall can be accurately assessed usingongitudinal and cross-sectional images of the cor-nary arteries to ensure adequate visualization ofhe concentric grey area surrounding the contrast-nhanced vessel lumen (63,66) (Fig. 7). Further-ore, up to � 50% of the segments considered
hickened by MDCT may be considered normal byoronary angiography, highlighting the potentialor early CAV detection (63). There is, however, aaucity of studies correlating changes in vesselall by MDCT to IVUS to assess its true
Axis 4 Chamber -
es in a Patient With ACR
hancement in the lateral wall and basal septum (red arrows) dur-mplete resolution of the hyperenhancement in the lateral wallt of immunosuppression with corresponding EMB revealingyocardial biopsy.
ort
ag
erenr-comen
ensitivity.
by on May 10, 2011 ing.onlinejacc.org
c�ribwcmfrlrssP2m6sb
r9dc
oCoCoiMlaiirihdwr(Cuthdcm
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 2 , N O . 9 , 2 0 0 9
S E P T E M B E R 2 0 0 9 : 1 1 2 6 – 4 0
Estep et al.
Multimodality Cardiac Imaging in the Transplanted Heart
1134
The use of MDCT does pose the technicalhallenge of reducing the heart rate enough (ideally65 beats/min) to minimize motion artifact. As a
esult of cardiac denervation, the resting heart raten cardiac transplant recipients is typically elevated,etween 80 and 110 beats/min. Pre-medicationith beta-blockers has been associated with a de-
rease and delay in heart rate reduction. Pre-edication with relatively high doses and increased
requency of beta-blockers have reduced the heartate in cardiac transplant recipients to an acceptableevel in some studies (63,67), whereas heart ratesemained high, despite similar efforts, in anothertudy (66). A high mean heart rate during MDCTcanning can impair image quality, as reported byichler et al. (62) with incomplete visualization in7% of patients (mean heart rate 87 � 9.7 beats/in) mainly owing to cardiac motion. With newer
4-slice scanner technology and multisector recon-truction algorithms, however, a heart rate of �80eats/min may permit adequate visualization.Despite this limitation, several studies report a
elatively high diagnostic image quality with 81% to6% of the coronary segments defined as either ofiagnostic or satisfactory quality (60,62,63,66). A
DE-CMR*
IVUS*
Echocardiography*(Doppler, TDI, SRI)
IVUS*Coronary
Angiography*MDCT*
ED
CoroH
CardInduc
M
Cardiac Allograft Diastolic Dysfunction
Epicardial Coronary Stenosis
FactorsReperfusion Injury, Cardiac Rejection, CMV,HTN, Dyslipidemia, Insulin Resistance, Immunosuppression Medication
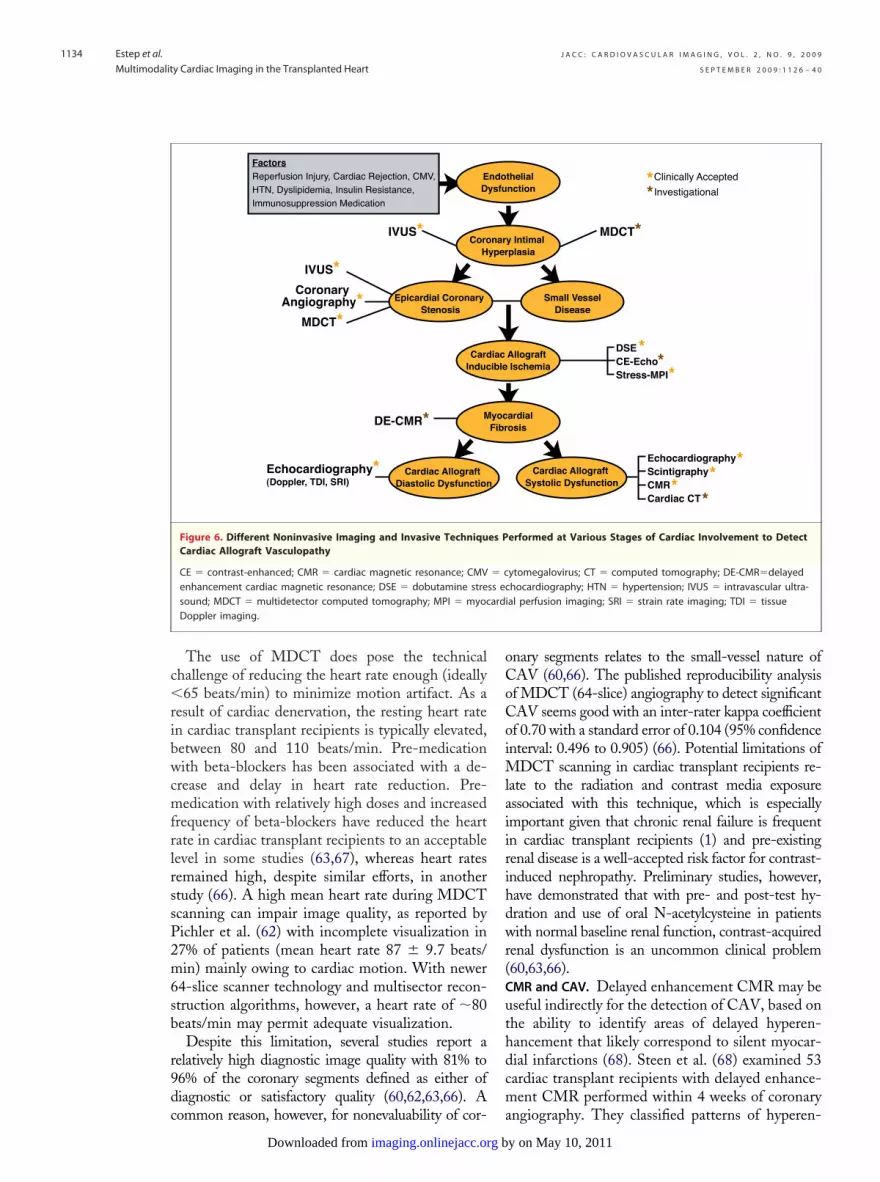
Figure 6. Different Noninvasive Imaging and Invasive TechniquCardiac Allograft Vasculopathy
CE � contrast-enhanced; CMR � cardiac magnetic resonance; CMVenhancement cardiac magnetic resonance; DSE � dobutamine stresound; MDCT � multidetector computed tomography; MPI � myocDoppler imaging.
ommon reason, however, for nonevaluability of cor- a
bimaging.onlinejacc.orgDownloaded from
nary segments relates to the small-vessel nature ofAV (60,66). The published reproducibility analysisf MDCT (64-slice) angiography to detect significantAV seems good with an inter-rater kappa coefficientf 0.70 with a standard error of 0.104 (95% confidencenterval: 0.496 to 0.905) (66). Potential limitations of
DCT scanning in cardiac transplant recipients re-ate to the radiation and contrast media exposuressociated with this technique, which is especiallymportant given that chronic renal failure is frequentn cardiac transplant recipients (1) and pre-existingenal disease is a well-accepted risk factor for contrast-nduced nephropathy. Preliminary studies, however,ave demonstrated that with pre- and post-test hy-ration and use of oral N-acetylcysteine in patientsith normal baseline renal function, contrast-acquired
enal dysfunction is an uncommon clinical problem60,63,66).MR and CAV. Delayed enhancement CMR may beseful indirectly for the detection of CAV, based onhe ability to identify areas of delayed hyperen-ancement that likely correspond to silent myocar-ial infarctions (68). Steen et al. (68) examined 53ardiac transplant recipients with delayed enhance-ent CMR performed within 4 weeks of coronary
MDCT*
Clinically Accepted
Investigational**thelial
nction
y Intimal plasia
Allograft Ischemia
ardialosis
Cardiac Allograft Systolic Dysfunction
Small VesselDisease
*
**
*
EchocardiographyScintigraphy CMR Cardiac CT
**
*
DSECE-Echo Stress-MPI
erformed at Various Stages of Cardiac Involvement to Detect
ytomegalovirus; CT � computed tomography; DE-CMR�delayedhocardiography; HTN � hypertension; IVUS � intravascular ultra-al perfusion imaging; SRI � strain rate imaging; TDI � tissue
ndoysfu
naryper
iac ible
yocFibr
es P
� css ecardi
ngiography. They classified patterns of hyperen-
y on May 10, 2011
hmmto
wpae
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 2 , N O . 9 , 2 0 0 9
S E P T E M B E R 2 0 0 9 : 1 1 2 6 – 4 0
Estep et al.
Multimodality Cardiac Imaging in the Transplanted Heart
1135
ancement with distinct subendocardial involve-ent as “infarct typical” and likely indicative ofyocardial infarction. The prevalence of this pat-
ern increased with worsening of CAV (present in
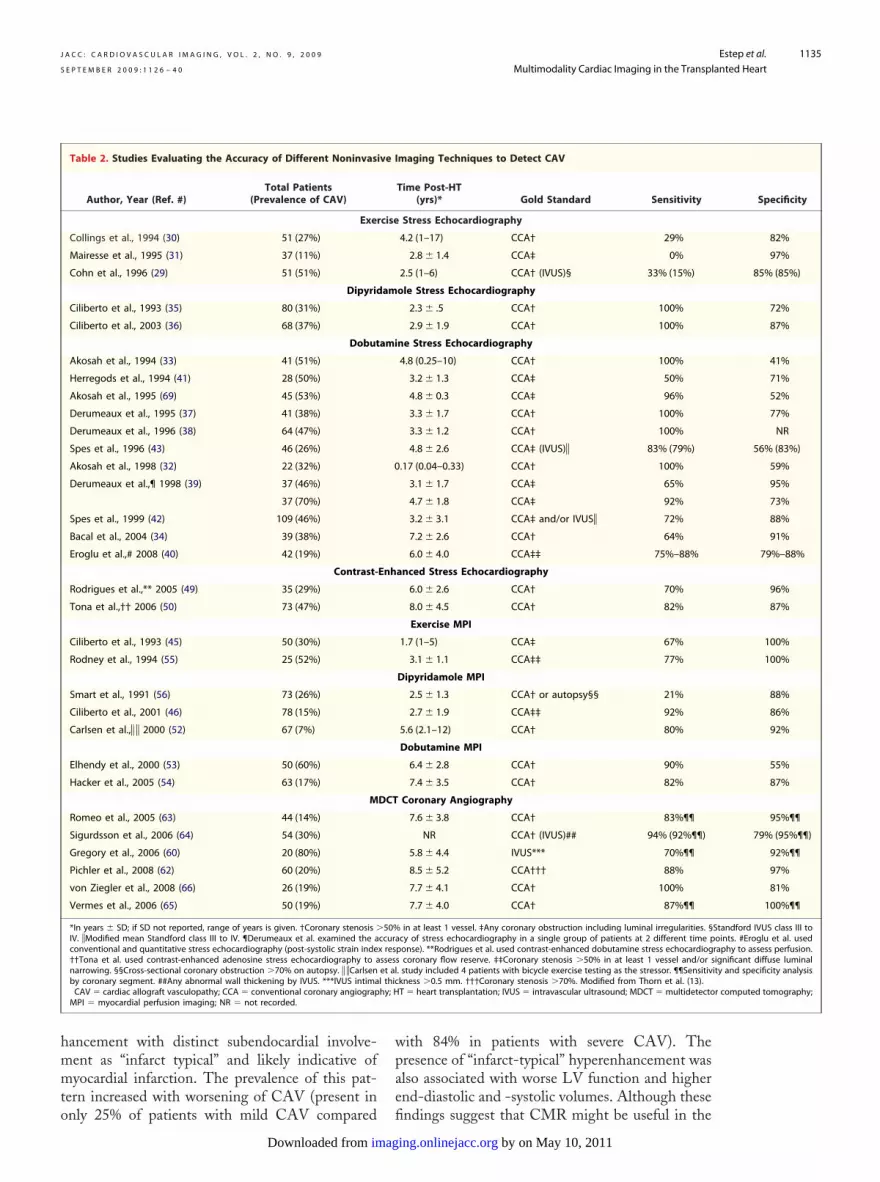
Table 2. Studies Evaluating the Accuracy of Different Noninvasi
Author, Year (Ref. #)Total Patients
(Prevalence of CAV)
Exer
Collings et al., 1994 (30) 51 (27%)
Mairesse et al., 1995 (31) 37 (11%)
Cohn et al., 1996 (29) 51 (51%)
Dipyrid
Ciliberto et al., 1993 (35) 80 (31%)
Ciliberto et al., 2003 (36) 68 (37%)
Dobut
Akosah et al., 1994 (33) 41 (51%)
Herregods et al., 1994 (41) 28 (50%)
Akosah et al., 1995 (69) 45 (53%)
Derumeaux et al., 1995 (37) 41 (38%)
Derumeaux et al., 1996 (38) 64 (47%)
Spes et al., 1996 (43) 46 (26%)
Akosah et al., 1998 (32) 22 (32%)
Derumeaux et al.,¶ 1998 (39) 37 (46%)
37 (70%)
Spes et al., 1999 (42) 109 (46%)
Bacal et al., 2004 (34) 39 (38%)
Eroglu et al.,# 2008 (40) 42 (19%)
Contrast-
Rodrigues et al.,** 2005 (49) 35 (29%)
Tona et al.,†† 2006 (50) 73 (47%)
Ciliberto et al., 1993 (45) 50 (30%)
Rodney et al., 1994 (55) 25 (52%)
Smart et al., 1991 (56) 73 (26%)
Ciliberto et al., 2001 (46) 78 (15%)
Carlsen et al.,� � 2000 (52) 67 (7%)
Elhendy et al., 2000 (53) 50 (60%)
Hacker et al., 2005 (54) 63 (17%)
M
Romeo et al., 2005 (63) 44 (14%)
Sigurdsson et al., 2006 (64) 54 (30%)
Gregory et al., 2006 (60) 20 (80%)
Pichler et al., 2008 (62) 60 (20%)
von Ziegler et al., 2008 (66) 26 (19%)
Vermes et al., 2006 (65) 50 (19%)
*In years � SD; if SD not reported, range of years is given. †Coronary stenosis �IV. �Modified mean Standford class III to IV. ¶Derumeaux et al. examined the aconventional and quantitative stress echocardiography (post-systolic strain inde††Tona et al. used contrast-enhanced adenosine stress echocardiography to anarrowing. §§Cross-sectional coronary obstruction �70% on autopsy. � �Carlsenby coronary segment. ##Any abnormal wall thickening by IVUS. ***IVUS intimaCAV � cardiac allograft vasculopathy; CCA � conventional coronary angiograpMPI � myocardial perfusion imaging; NR � not recorded.
nly 25% of patients with mild CAV compared fi
imagDownloaded from
ith 84% in patients with severe CAV). Theresence of “infarct-typical” hyperenhancement waslso associated with worse LV function and highernd-diastolic and -systolic volumes. Although these
maging Techniques to Detect CAV
Time Post-HT(yrs)* Gold Standard Sensitivity
Stress Echocardiography
4.2 (1–17) CCA† 29%
2.8 � 1.4 CCA‡ 0%
2.5 (1–6) CCA† (IVUS)§ 33% (15%)
ole Stress Echocardiography
2.3 � .5 CCA† 100%
2.9 � 1.9 CCA† 100%
ne Stress Echocardiography
4.8 (0.25–10) CCA† 100%
3.2 � 1.3 CCA‡ 50%
4.8 � 0.3 CCA‡ 96%
3.3 � 1.7 CCA† 100%
3.3 � 1.2 CCA† 100%
4.8 � 2.6 CCA‡ (IVUS)� 83% (79%)
.17 (0.04–0.33) CCA† 100%
3.1 � 1.7 CCA‡ 65%
4.7 � 1.8 CCA‡ 92%
3.2 � 3.1 CCA‡ and/or IVUS� 72%
7.2 � 2.6 CCA† 64%
6.0 � 4.0 CCA‡‡ 75%–88%
anced Stress Echocardiography
6.0 � 2.6 CCA† 70%
8.0 � 4.5 CCA† 82%
Exercise MPI
1.7 (1–5) CCA‡ 67%
3.1 � 1.1 CCA‡‡ 77%
Dipyridamole MPI
2.5 � 1.3 CCA† or autopsy§§ 21%
2.7 � 1.9 CCA‡‡ 92%
5.6 (2.1–12) CCA† 80%
Dobutamine MPI
6.4 � 2.8 CCA† 90%
7.4 � 3.5 CCA† 82%
Coronary Angiography
7.6 � 3.8 CCA† 83%¶¶
NR CCA† (IVUS)## 94% (92%¶¶)
5.8 � 4.4 IVUS*** 70%¶¶
8.5 � 5.2 CCA††† 88%
7.7 � 4.1 CCA† 100%
7.7 � 4.0 CCA† 87%¶¶
in at least 1 vessel. ‡Any coronary obstruction including luminal irregularities. §cy of stress echocardiography in a single group of patients at 2 different time pponse). **Rodrigues et al. used contrast-enhanced dobutamine stress echocardiogs coronary flow reserve. ‡‡Coronary stenosis �50% in at least 1 vessel and/or s. study included 4 patients with bicycle exercise testing as the stressor. ¶¶Sensitivkness �0.5 mm. †††Coronary stenosis �70%. Modified from Thorn et al. (13).T � heart transplantation; IVUS � intravascular ultrasound; MDCT � multidetecto
ve I
Specificity
cise
82%
97%
85% (85%)
am
72%
87%
ami
41%
71%
52%
77%
NR
56% (83%)
0 59%
95%
73%
88%
91%
79%–88%
Enh
96%
87%
100%
100%
88%
86%
92%
55%
87%
DCT
95%¶¶
79% (95%¶¶)
92%¶¶
97%
81%
100%¶¶
50% Standford IVUS class III toccura oints. #Eroglu et al. usedx res raphy to assess perfusion.sses ignificant diffuse luminalet al ity and specificity analysisl thichy; H r computed tomography;
ndings suggest that CMR might be useful in the
by on May 10, 2011 ing.onlinejacc.org

dpVa
C
DaliSapIntdp
ppr
etbtcptrPTttoe
WMA � wall motion abno
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 2 , N O . 9 , 2 0 0 9
S E P T E M B E R 2 0 0 9 : 1 1 2 6 – 4 0
Estep et al.
Multimodality Cardiac Imaging in the Transplanted Heart
1136
etection of CAV, the clinical significance andathologic basis of these findings are unknown.alidation and prospective outcome-based studies
re currently underway.
onclusions
espite many advances in the field of HT, ACR,nd CAV represent significant causes of early andate morbidity and mortality, respectively. Differentmaging modalities, including echocardiography,PECT-MPI, MDCT, and CMR have been usedfter HT to monitor multiple clinically importantarameters of cardiac graft structure and function.n general, echocardiography represents the primaryoninvasive modality for monitoring cardiac func-ion in transplant recipients based on its ability toetect abnormalities of ventricular systolic function,
uating the Accuracy of Different Noninvasive Imaging Technique
#)Total Patients
(Prevalence of MACE)Time Post-HT
(yrs)*Le
2-Dimensional Echocardiogra
5) 80 (9%) 2.3 � 1.5
(48) 46 (11%) NR
109 (15%) 3.2 � 3.1 �
6) 78 (22%) 2.7 � 1.9
6) 68 (28%) 2.9 � 1.9
Dipyridamole Stress Echocard
5) 80 (9%) 2.3 � 0.5
6) 68 (28%) 2.9 � 1.9
Dobutamine Stress Echocard
) 76 (16%) 4.8 (0.25–10)
(37) 41 (5%) 3.3 � 1.7
) 64 (25%) 4.8 � 2.4
63 (56%) 4.8 � 2.6
) 22 (10%) 0.17 (0.04–0.33)
109 (15%) 3.2 � 3.1 �
39 (25%) �4.0
CE-Stress Echocardiogra
66 (17%) 9.0 � 4.0
Dipyridamole MPI
6) 78 (22%) 2.7 � 1.9
Dobutamine MPI
) 77 (13%) 7.4 � 3.5
(58) 166 (10%) 7.4 � 2.5
le, range is provided. †Tona et al. used CE echocardiography to assess accuracy o�2.6). �Hacker et al. compared visual¶ and semiquantitative# (summed stress scoesting; however, both stress modalities shared similar ability to predict cardiac d; HT � heart transplantation; MACE � major adverse cardiac event; MPI � myormality.
rovide estimation of right- and left-sided filling a
bimaging.onlinejacc.orgDownloaded from
ressures with reasonable accuracy, and evaluateericardial effusions or other complications fromepeated biopsies.
With regard to the detection of ACR, when thechocardiography literature is taken as a whole,here are inconsistencies among various reportsrought about by small sample size, variability inhe reference gold standard used, and differentutoff points for the different echocardiographyarameters evaluated. Today, echocardiographicechniques lack the sensitivity and specificity toeplace EMBs to detect clinically significant ACR.romising echocardiography techniques involvingDI and strain imaging are associated with rela-
ively high negative predictive values in the detec-ion of ACR. However, further validation andutcome-based studies are required before a specificchocardiography parameter can be recommended
Detect MACE
h of Follow-Up(Months)
Detection of MACE
NPVSensitivity Specificity
WMA
9.8 � 4.5 100% 73% 100%
45 � 20 40% 98% 93%
in some cases 75% 65% 94%
78 � 24 41% 97% 85%
72 � 36 80% 68% 90%
raphy
9.8 � 4.5 100% 71% 100%
72 � 36 80% 68% 90%
aphy
10 � 2 100% 41% 100%
6.0 100% 66% 100%
24 (18–28) 100% 69% 100%
.0 (4–14) 83% NR NR
32 � 11 100% 61% 100%
in some cases 94% 57% 98%
48 60% 86% 87%
19 � 5 86%‡ 75%‡ 97%
91%§ 62%§ 97%
78 � 24 53% 82% 86%
22 (12–48) 90%¶ 72%¶ 98%
90%# 88%# 98%
30 69% 71% 95%
celeration time of diastolic flow velocity ‡(cutoff value �840 ms) and coronary3) analysis. **Elhendy et al. study (65 of the 166 patients reportedly underwent). Modified from Thorn et al. (13).ial perfusion imaging; NPV � negative predictive value; NR � not recorded;
Table 3. Studies Eval s to
Author, Year (Ref.ngt
phy
Ciliberto et al., 1993 (3
Verhoeven et al., 1996
Spes et al., 1999 (42) 60
Ciliberto et al., 2001 (4
Ciliberto et al., 2003 (3
iog
Ciliberto et al., 1993 (3
Ciliberto et al., 2003 (3
iogr
Akosah et al., 1994 (33
Derumeaux et al., 1995
Akosah et al., 1996 (44
Lewis et al., 1997 (47) 8
Akosah et al., 1998 (32
Spes et al., 1999 (42) 60
Bacal et al., 2004 (34)
phy
Tona et al.,† 2006 (51)
Ciliberto et al., 2001 (4
Hacker et al.,� 2005 (54
Elhendy et al.,** 2002
*Mean � SD; if not availab f deflow reserve §(cutoff value re �exercise not dobutamine t eathCE � contrast enhanced card
s a screening index to minimize the use of serial
y on May 10, 2011
baato
wMcscasdwdobiisa
o
nsMotwlfiidvsarahp
R
Mo
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 2 , N O . 9 , 2 0 0 9
S E P T E M B E R 2 0 0 9 : 1 1 2 6 – 4 0
Estep et al.
Multimodality Cardiac Imaging in the Transplanted Heart
1137
iopsies. CMR, similar to echocardiography, canccurately detect ventricular systolic dysfunction,nd newer CMR techniques may allow the detec-ion of myocardial edema and necrosis—hallmarksf ACR.In contrast, with respect to CAV, stress imaging
ith DSE and MPI and coronary angiography withDCT are powerful techniques to identify this late
omplication with high accuracy. DSE is the most-tudied technique with significant prognostic valueomparable to that of IVUS and invasive coronaryngiography. For transplant centers experienced intress echocardiography, an invasive examination toetect significant CAV can be reserved for patientsith an abnormal annual DSE. Although echocar-iography has the advantage of lower cost, the usef MPI, especially with dobutamine, is a compara-le alternative in cardiac transplant recipients givents prognostic value. MPI may be especially usefuln patients with inadequate acoustic windows de-pite the use of a contrast echocardiography agentnd in centers without adequate experience in DSE.
Newer CMR techniques may allow the detection
Figure 7. MDCT Coronary Angiography Demonstration of Cardi
(A) Total vessel occlusion of left anterior descending (LAD) is illustrocclusion by MDCT volume-rendering angiography. (C) Maximum inproximal of occlusion, an excentric noncalcified plaque is depictedchanges throughout the LAD course, causing no to minimal luminacircumflex; LM � left main coronary artery; MDCT � multidetectorvon Ziegler et al. (66) with permission.
f abnormal hyperenhancement to detect CAV H
imagDownloaded from
oninvasively; further pathologic and outcometudies, however, are needed. With the ability of
DCT coronary angiography to evaluate the cor-nary wall in addition to the lumen, MDCT hashe potential for earlier detection of CAV comparedith echocardiography, MPI, and CMR. This ear-
ier detection of CAV may enhance research in thiseld and prompt the early use of proliferation signal
nhibitors or other investigations to minimize CAVisease progression and improve outcome. Furtheralidation of MDCT, however, is needed in largertudies. Furthermore, because this technique is alsossociated with radiation and contrast exposure, theisk/benefit ratio needs to be concomitantly evalu-ted, given the need for serial examinations and theigh incidence of renal insufficiency in this patientopulation.
eprint requests and correspondence: Dr. Jerry D. Estep,ethodist DeBakey Heart and Vascular Center, Cardi-
logy, Smith Tower, 6550 Fannin Street, Suite 1901,
llograft Vasculopathy
by conventional coronary angiography. (B) Corresponding LADsity projection; grey arrows indicate site of total vessel occlusion;cross-sectional image (note diffuse hypodense vessel wallgularities in conventional coronary angiography). LCX � leftputed tomography; RCA � right coronary artery. Adapted from
ac A
atedtenin al irrecom
ouston, Texas 77030. E-mail: [email protected].
by on May 10, 2011 ing.onlinejacc.org

J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 2 , N O . 9 , 2 0 0 9
S E P T E M B E R 2 0 0 9 : 1 1 2 6 – 4 0
Estep et al.
Multimodality Cardiac Imaging in the Transplanted Heart
1138
R
1
1
1
2
2
2
2
2
2
3
3
3
3
E F E R E N C E S
1. Taylor DO, Edwards LB, Aurora P,et al. Registry of the InternationalSociety for Heart and Lung Trans-plantation: twenty-fifth official adultheart transplant report—2008. J HeartLung Transplant 2008;27:943–56.
2. Almenar L, Igual B, Martinez-DolzL, et al. Utility of cardiac magneticresonance imaging for the diagnosisof heart transplant rejection. Trans-plant Proc 2003;35:1962– 4.
3. Dandel M, Hummel M, Meyer R, etal. Left ventricular dysfunction dur-ing cardiac allograft rejection: earlydiagnosis, relationship to the histo-logical severity grade, and therapeuticimplications. Transplant Proc 2002;34:2169 –73.
4. Follansbee WP, Kiernan JM, Curtiss EI,Zerbe TR, Mock C, Kormos RL.Changes in left ventricular systolic func-tion that accompany rejection of the trans-planted heart: a serial radionuclide assess-ment of fifty-three consecutive cases. AmHeart J 1991;121:548–56.
5. Sagar KB, Hastillo A, Wolfgang TC,Lower RR, Hess ML. Left ventricularmass by M-mode echocardiography incardiac transplant patients with acute re-jection. Circulation 1981;64:II217–20.
6. Angermann CE, Nassau K, StempfleHU, et al. Recognition of acute car-diac allograft rejection from serial in-tegrated backscatter analyses in hu-man orthotopic heart transplantrecipients. Comparison with conven-tional echocardiography. Circulation1997;95:140–50.
7. Ciliberto GR, Mascarello M, GrondaE, et al. Acute rejection after hearttransplantation: noninvasive echocar-diographic evaluation. J Am Coll Car-diol 1994;23:1156–61.
8. Stengel SM, Allemann Y, ZimmerliM, et al. Doppler tissue imaging forassessing left ventricular diastolic dys-function in heart transplant rejection.Heart 2001;86:432–7.
9. Ciliberto GR, Anjos MC, Gronda E,et al. Significance of pericardial effu-sion after heart transplantation. Am JCardiol 1995;76:297–300.
0. Sun JP, Abdalla IA, Asher CR, et al.Non-invasive evaluation of orthotopicheart transplant rejection by echocar-diography. J Heart Lung Transplant2005;24:160–5.
1. Yun KL, Niczyporuk MA, DaughtersGT II, et al. Alterations in left ventriculardiastolic twist mechanics during acute hu-man cardiac allograft rejection. Circula-tion 1991;83:962–73.
2. Mena C, Wencker D, Krumholz
HM, McNamara RL. Detection ofheart transplant rejection in adults byimagDownloaded from
echocardiographic diastolic indices: asystematic review of the literature.J Am Soc Echocardiogr 2006;19:1295–300.
13. Thorn EM, de Filippi CR. Echocardi-ography in the cardiac transplant recipient.Heart Fail Clin 2007;3:51–67.
14. Palka P, Lange A, Galbraith A, et al.The role of left and right ventricularearly diastolic Doppler tissue echocar-diographic indices in the evaluation ofacute rejection in orthotopic hearttransplant. J Am Soc Echocardiogr2005;18:107–15.
15. Puleo JA, Aranda JM, Weston MW,et al. Noninvasive detection of allo-graft rejection in heart transplant re-cipients by use of Doppler tissue im-aging. J Heart Lung Transplant 1998;17:176–84.
16. Burgess MI, Bright-Thomas RJ, Yo-nan N, Ray SG. Can the index ofmyocardial performance be used todetect acute cellular rejection afterheart transplantation? Am J Cardiol2003;92:308–11.
17. Vivekananthan K, Kalapura T, MehraM, et al. Usefulness of the combinedindex of systolic and diastolic myocar-dial performance to identify cardiacallograft rejection. Am J Cardiol 2002;90:517–20.
18. Hummel M, Dandel M, KnollmannF, et al. Long-term surveillance ofheart-transplanted patients: noninva-sive monitoring of acute rejection ep-isodes and transplant vasculopathy.Transplant Proc 2001;33:3539–42.
19. Dandel M, Hummel M, Muller J, etal. Reliability of tissue Doppler wallmotion monitoring after heart trans-plantation for replacement of invasiveroutine screenings by optimally timedcardiac biopsies and catheterizations.Circulation 2001;104:I184–91.
20. Mankad S, Murali S, Kormos RL,Mandarino WA, Gorcsan J 3rd. Eval-uation of the potential role of color-coded tissue Doppler echocardiogra-phy in the detection of allograftrejection in heart transplant recipients.Am Heart J 1999;138:721–30.
21. Sundereswaran L, Nagueh SF, VardanS, et al. Estimation of left and rightventricular filling pressures after hearttransplantation by tissue Doppler imag-ing. Am J Cardiol 1998;82:352–7.
22. Marciniak A, Eroglu E, Marciniak M,et al. The potential clinical role ofultrasonic strain and strain rate imag-ing in diagnosing acute rejection afterheart transplantation. Eur J Echocar-diogr 2007;8:213–21.
23. Moidl R, Chevtchik O, Simon P, et al.
Noninvasive monitoring of peak fillingrate with acoustic quantification echo-by on May 10, 2011 ing.onlinejacc.org
cardiography accurately detects acutecardiac allograft rejection. J Heart LungTransplant 1999;18:194–201.
4. Bellenger NG, Marcus NJ, Davies C,Yacoub M, Banner NR, Pennell DJ.Left ventricular function and massafter orthotopic heart transplantation:a comparison of cardiovascular mag-netic resonance with echocardiogra-phy. J Heart Lung Transplant 2000;19:444–52.
5. Revel D, Chapelon C, Mathieu D, et al.Magnetic resonance imaging of humanorthotopic heart transplantation: corre-lation with endomyocardial biopsy.J Heart Transplant 1989;8:139–46.
6. Marie PY, Angioi M, Carteaux JP, etal. Detection and prediction of acuteheart transplant rejection with themyocardial T2 determination pro-vided by a black-blood magnetic res-onance imaging sequence. J Am CollCardiol 2001;37:825–31.
7. Schmauss D, Weis M. Cardiac allograftvasculopathy: recent developments. Cir-culation 2008;117:2131–41.
8. Dandel M, Knollmann FD, Welln-hofer E, Hummel M, Kapell S,Hetzer R. Noninvasive surveillancestrategy for early identification ofheart transplant recipients with possi-ble coronary stenoses. Transplant Proc2003;35:2113–6.
9. Cohn JM, Wilensky RL, O’DonnellJA, Bourdillon PD, Dillon JC,Feigenbaum H. Exercise echocardiog-raphy, angiography, and intracoronaryultrasound after cardiac transplanta-tion. Am J Cardiol 1996;77:1216–9.
0. Collings CA, Pinto FJ, ValantineHA, Popylisen S, Puryear JV, Schnit-tger I. Exercise echocardiography inheart transplant recipients: a compar-ison with angiography and intracoro-nary ultrasonography. J Heart LungTransplant 1994;13:604–13.
1. Mairesse GH, Marwick TH, Melin JA,et al. Use of exercise electrocardiogra-phy, technetium-99m-MIBI perfusiontomography, and two-dimensionalechocardiography for coronary diseasesurveillance in a low-prevalence pop-ulation of heart transplant recipients.J Heart Lung Transplant 1995;14:222–9.
2. Akosah KO, McDaniel S, Hanrahan JS,Mohanty PK. Dobutamine stress echo-cardiography early after heart transplanta-tion predicts development of allograft cor-onary artery disease and outcome. J AmColl Cardiol 1998;31:1607–14.
3. Akosah KO, Mohanty PK, Funai JT, etal. Noninvasive detection of transplantcoronary artery disease by dobutamine
stress echocardiography. J Heart LungTransplant 1994;13:1024–38.
3
3
3
3
3
3
4
4
4
4
4
5
5
5
5
6
6
6
6
6
6
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 2 , N O . 9 , 2 0 0 9
S E P T E M B E R 2 0 0 9 : 1 1 2 6 – 4 0
Estep et al.
Multimodality Cardiac Imaging in the Transplanted Heart
1139
4. Bacal F, Moreira L, Souza G, et al.Dobutamine stress echocardiographypredicts cardiac events or death inasymptomatic patients long-term afterheart transplantation: 4-year prospec-tive evaluation. J Heart Lung Trans-plant 2004;23:1238–44.
5. Ciliberto GR, Massa D, Mangiavac-chi M, et al. High-dose dipyridamoleechocardiography test in coronary ar-tery disease after heart transplanta-tion. Eur Heart J 1993;14:48–52.
6. Ciliberto GR, Parodi O, Cataldo G,et al. Prognostic value of contractileresponse during high-dose dipyridam-ole echocardiography test in hearttransplant recipients. J Heart LungTransplant 2003;22:526–32.
7. Derumeaux G, Redonnet M, Mouton-Schleifer D, et al. Dobutamine stressechocardiography in orthotopic hearttransplant recipients. VACOMED Re-search Group. J Am Coll Cardiol 1995;25:1665–72.
8. Derumeaux G, Redonnet M, Mouton-Schleifer D, Cribier A, Soyer R, LetacB. [Value of dobutamine echocardiog-raphy in the detection of coronarydisease in heart transplant patient.Groupe de Recherche VACOMED].Arch Mal Coeur Vaiss 1996;89:687–94.
9. Derumeaux G, Redonnet M, Soyer R,Cribier A, Letac B. Assessment of theprogression of cardiac allograft vascu-lopathy by dobutamine stress echocar-diography. J Heart Lung Transplant1998;17:259–67.
0. Eroglu E, D’Hooge J, Sutherland GR,et al. Quantitative dobutamine stressechocardiography for the early detec-tion of cardiac allograft vasculopathyin heart transplant recipients. Heart2008;94:e3.
1. Herregods MC, Anastassiou I, VanCleemput J, et al. Dobutamine stressechocardiography after heart trans-plantation. J Heart Lung Transplant1994;13:1039–44.
2. Spes CH, Klauss V, Mudra H, et al.Diagnostic and prognostic value ofserial dobutamine stress echocardiog-raphy for noninvasive assessment ofcardiac allograft vasculopathy: a com-parison with coronary angiographyand intravascular ultrasound. Circula-tion 1999;100:509–15.
3. Spes CH, Mudra H, Schnaack SD,et al. Dobutamine stress echocardi-ography for noninvasive diagnosis ofcardiac allograft vasculopathy: acomparison with angiography andintravascular ultrasound. Am J Car-diol 1996;78:168 –74.
4. Akosah KO, Olsovsky M, KirchbergD, Salter D, Mohanty PK. Dobut-amine stress echocardiography pre-
dicts cardiac events in heart trans-Do
plant patients. Circulation 1996;94:II283– 8.
45. Ciliberto GR, Mangiavacchi M, BanfiF, et al. Coronary artery disease afterheart transplantation: non-invasiveevaluation with exercise thallium scin-tigraphy. Eur Heart J 1993;14:226–9.
46. Ciliberto GR, Ruffini L, Mangiavac-chi M, et al. Resting echocardiogra-phy and quantitative dipyridamoletechnetium-99m sestamibi tomogra-phy in the identification of cardiacallograft vasculopathy and the predic-tion of long-term prognosis after hearttransplantation. Eur Heart J 2001;22:964–71.
47. Lewis JF, Selman SB, Murphy JD,Mills RM Jr, Geiser EA, Conti CR.Dobutamine echocardiography forprediction of ischemic events in hearttransplant recipients. J Heart LungTransplant 1997;16:390–3.
48. Verhoeven PP, Lee FA, Ramahi TM,et al. Prognostic value of noninvasivetesting one year after orthotopic car-diac transplantation. J Am Coll Car-diol 1996;28:183–9.
49. Rodrigues AC, Bacal F, MedeirosCC, et al. Noninvasive detection ofcoronary allograft vasculopathy bymyocardial contrast echocardiogra-phy. J Am Soc Echocardiogr 2005;18:116 –21.
50. Tona F, Caforio AL, Montisci R, etal. Coronary flow reserve by contrast-enhanced echocardiography: a newnoninvasive diagnostic tool for cardiacallograft vasculopathy. Am J Trans-plant 2006;6:998–1003.
51. Tona F, Caforio AL, Montisci R, etal. Coronary flow velocity pattern andcoronary flow reserve by contrast-enhanced transthoracic echocardiog-raphy predict long-term outcome inheart transplantation. Circulation2006;114:I49–55.
52. Carlsen J, Toft JC, Mortensen SA,Arendrup H, Aldershvile J, Hesse B.Myocardial perfusion scintigraphy as ascreening method for significant cor-onary artery stenosis in cardiac trans-plant recipients. J Heart Lung Trans-plant 2000;19:873–8.
53. Elhendy A, Sozzi FB, van DomburgRT, et al. Accuracy of dobutaminetetrofosmin myocardial perfusion im-aging for the noninvasive diagnosis oftransplant coronary artery stenosis.J Heart Lung Transplant 2000;19:360–6.
54. Hacker M, Tausig A, Romuller B, etal. Dobutamine myocardial scintigra-phy for the prediction of cardiacevents after heart transplantation.Nucl Med Commun 2005;26:607–12.
55. Rodney RA, Johnson LL, Blood DK,
Barr ML. Myocardial perfusion scintig-raphy in heart transplant recipients withbimaging.onlinejacc.orgwnloaded from
and without allograft atherosclerosis: acomparison of thallium-201 and tech-netium 99m sestamibi. J Heart LungTransplant 1994;13:173–80.
6. Smart FW, Ballantyne CM, Coca-nougher B, et al. Insensitivity of non-invasive tests to detect coronary arteryvasculopathy after heart transplant.Am J Cardiol 1991;67:243–7.
7. Howarth DM, Forstrom LA, Sam-udrala V, Sinak LJ, McGregor CG,Rodeheffer RJ. Evaluation of 201TlSPET myocardial perfusion imaging inthe detection of coronary artery diseaseafter orthotopic heart transplantation.Nucl Med Commun 1996;17:105–13.
8. Elhendy A, van Domburg RT, Vant-rimpont P, et al. Prediction of mortal-ity in heart transplant recipients bystress technetium-99m tetrofosminmyocardial perfusion imaging. Am JCardiol 2002;89:964–8.
9. Ratliff NB III, Jorgensen CR, GobelFL, Hodges M, Knickelbine T, Pritz-ker MR. Lack of usefulness of electronbeam computed tomography for de-tecting coronary allograft vasculopa-thy. Am J Cardiol 2004;94:202–6.
0. Gregory SA, Ferencik M, AchenbachS, et al. Comparison of sixty-four-slicemultidetector computed tomographiccoronary angiography to coronary an-giography with intravascular ultra-sound for the detection of transplantvasculopathy. Am J Cardiol 2006;98:877–84.
1. Iyengar S, Feldman DS, Cooke GE,Leier CV, Raman SV. Detection ofcoronary artery disease in orthotopicheart transplant recipients with 64-detector row computed tomographyangiography. J Heart Lung Trans-plant 2006;25:1363–6.
2. Pichler P, Loewe C, Roedler S, et al.Detection of high-grade stenoses withmultislice computed tomography inheart transplant patients. J HeartLung Transplant 2008;27:310–6.
3. Romeo G, Houyel L, Angel CY, Bre-not P, Riou JY, Paul JF. Coronarystenosis detection by 16-slice com-puted tomography in heart transplantpatients: comparison with conven-tional angiography and impact onclinical management. J Am Coll Car-diol 2005;45:1826–31.
4. Sigurdsson G, Carrascosa P, YamaniMH, et al. Detection of transplantcoronary artery disease using multide-tector computed tomography with ad-aptative multisegment reconstruction.J Am Coll Cardiol 2006;48:772–8.
5. Vermes E, Dupouy P, Kirsch M, Per-nes J, Loisance D. Can multislice CTscan replace systematic coronarogra-phy in heart transplant recipients?
J Heart Lung Tranplant 2006;25Suppl:S99.y on May 10, 2011

6
6
Ka
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 2 , N O . 9 , 2 0 0 9
S E P T E M B E R 2 0 0 9 : 1 1 2 6 – 4 0
Estep et al.
Multimodality Cardiac Imaging in the Transplanted Heart
1140
6. von Ziegler F, Leber AW, Becker A,et al. Detection of significant coronaryartery stenosis with 64-slice computedtomography in heart transplant re-cipients: a comparative study withconventional coronary angiography.Int J Cardiovasc Imaging 2009;25:91–100.
7. Bogot NR, Durst R, Shaham D, Ad-
mon D. Cardiac CT of the trans-imagDownloaded from
planted heart: indications, technique,appearance, and complications. Ra-diographics 2007;27:1297–309.
68. Steen H, Merten C, Refle S, et al.Prevalence of different gadolinium en-hancement patterns in patients afterheart transplantation. J Am Coll Car-diol 2008;52:1160–7.
69. Akosah K, Olsovsky M, Mohanty
PK. Dobutamine stress-induced an- vby on May 10, 2011 ing.onlinejacc.org
gina in patients with denervated car-diac transplants. Clinical and angio-graphic correlates. Chest 1995;108:695–700.
ey Words: heart transplant ycute cellular rejection y
asculopathy y cardiac imaging.
doi:10.1016/j.jcmg.2009.06.006 2009;2;1126-1140 J. Am. Coll. Cardiol. Img.
Torre-Amione, and William A. Zoghbi Jerry D. Estep, Dipan J. Shah, Sherif F. Nagueh, John J. Mahmarian, Guillermo
The Role of Multimodality Cardiac Imaging in the Transplanted Heart
This information is current as of May 10, 2011
& ServicesUpdated Information
http://imaging.onlinejacc.org/cgi/content/full/2/9/1126including high-resolution figures, can be found at:
References
http://imaging.onlinejacc.org/cgi/content/full/2/9/1126#BIBLfree at: This article cites 69 articles, 20 of which you can access for
Citations
ticleshttp://imaging.onlinejacc.org/cgi/content/full/2/9/1126#otherarThis article has been cited by 1 HighWire-hosted articles:
Rights & Permissions
http://imaging.onlinejacc.org/misc/permissions.dtltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://imaging.onlinejacc.org/misc/reprints.dtl
Information about ordering reprints can be found online:
by on May 10, 2011 imaging.onlinejacc.orgDownloaded from





























