Embed Size (px)
Citation preview

Classification of small bowel Crohn’s subtypes based on
multimodality imaging
Dean D.T. Maglinte, MDa,*, Nicholas Gourtsoyiannis, MDb,Douglas Rex, MD, FACGc, Thomas J. Howard, MD, FACSd,
Frederick M. Kelvin, MDe
aDepartment of Radiology, Indiana University School of Medicine, University Hospital and Outpatient Center,
550 North University Boulevard, Room 0279, Indianapolis, IN 46202-5253, USAbDepartment of Radiology, University Hospital of Heraklion, Faculty of Medicine, University of Crete, Crete, Greece
cDivision of Gastroenterology and Hepatology, Indiana University School of Medicine,
University Hospital and Outpatient Center, 550 North University Boulevard, Room 0279, Indianapolis, IN 46202-5253, USAdDivision of Surgery, Indiana University School of Medicine, University Hospital and Outpatient Center,
550 North University Boulevard, Room 0279, Indianapolis, IN 46202-5253, USAeDepartment of Radiology, Methodist Hospital of Indiana, 1701 North Senate Boulevard, Indianapolis, IN 46202, USA
Crohn’s disease is a chronic, segmental, trans-
mural inflammatory disorder that frequently involves
the small bowel. The disease has a distinct tendency
to recur and result in complications such as
abscesses and fistulae. Its etiology is unknown,
although there is mounting evidence that the con-
dition represents an abnormal mucosal response to
unknown luminal antigens [1]. Crohn’s disease most
commonly affects the terminal ileum and proximal
colon, although it can occur anywhere in the gastro-
intestinal tract from the mouth to the anus. Radio-
logic evaluation remains of particular importance
when involvement is confined to or involves the
mesenteric small intestine between the ligament of
Trietz and the ileocecal valve, because this part of
the gastrointestinal tract is not generally evaluable
endoscopically [2,3]. Barium examinations, includ-
ing small bowel follow-through, enteroclysis, and
CT are the main radiologic techniques used to
show the various manifestations of Crohn’s disease
[3–20]. More recently, CT enteroclysis has been
developed and employed in patients with Crohn’s
disease [21,25]. MR imaging currently is being
studied in the small bowel and holds great promise
for the evaluation of this disease [26,30].
Crohn’s disease is unpredictable in both its clin-
ical presentation and evolution. Its variable behavior
has led investigators to classify the disease into
subtypes that include active inflammatory, fibroste-
nosing, and fistulizing/perforating categories. Clas-
sification of patients by subtype has clinical utility
because accurate classification can help to guide
decisions regarding medical and surgical therapy.
Classification of subtypes requires accurate informa-
tion concerning the presence of ulceration, edema,
spasm, stricture, fistula formation, and associated
inflammatory mass. For the small bowel, this
information is traditionally provided by barium
examination and CT. Newer techniques such as enter-
oclysis, multislice CT, MR imaging, CT enteroclysis,
and MR enteroclysis are now increasingly used in
clinical practice and provide additional detail that is
useful for the accurate classification of subtypes. This
article provides a pictorial atlas of the imaging find-
ings that distinguish the subtypes of Crohn’s disease
as they are seen in the small bowel utilizing conven-
tional and newer imaging technologies. The rel-
0033-8389/03/$ – see front matter D 2003, Elsevier Science (USA). All rights reserved.
doi:10.1016/S0033-8389(02)00117-3
* Corresponding author.
E-mail address: [email protected] (D.D.T. Maglinte).
Radiol Clin N Am 41 (2003) 285–303

evance to clinical management of this morphologic
imaging-based classification scheme is discussed.
Imaging classification of small bowel
Crohn’s disease
The management of Crohn’s disease continues to
evolve both medically and surgically [1]. Classifica-
tion of disease activity in Crohn’s disease based
solely on clinical and laboratory parameters has not
been clinically reproducible [31,32]. The use of
imaging findings as part of the information that
supports the classification of a given disease sub-
type has the potential to make the classification
system more objective and reproducible. An
imaging-based classification system of Crohn’s dis-
ease subtypes can help clinicians to plan appropriate
therapy. For example, obstruction caused by active
inflammation may respond to intensive medical ther-
apy, whereas obstruction due to a fibrotic stricture is
generally unresponsive and frequently requires sur-
gical intervention (resection, stricturoplasty), pro-
vided there is no acute inflammation or phlegmon
at the strictured site.
The imaging classification presented in this
pictorial review (Table 1) represents a combination
of a clinical classification scheme based on disease
behavior [31,32] and a radiographic classification
scheme based on both degree of involvement and
anatomic extent of disease as seen on barium
examination supplemented by newer imaging tech-
nologies [33]. A characteristic feature of Crohn’s
disease of the small bowel is the wide variety of
radiologic features and multiplicity of abnormalities
that can be present in any individual patient. Fig. 1
is a diagram depicting the evolution and complex-
ity of the course of Crohn’s disease. Disease
progression is often influenced by disease severity
and by clinical intervention [31,32]. More than one
subtype of the disease process may be noted in a
segment or in multiple adjacent segments in the
same patient.
Active inflammatory disease subtype
The active inflammatory subtype of Crohn’s dis-
ease is characterized by focal inflammation, super-
ficial (aphthoid) and deep ulcers, an often transmural
inflammatory reaction with lymphoid aggregates and
granuloma formation. Minimal inflammatory activity
is characterized on barium examinations as blunting,
thickening, straightening, or distortion of the small
bowel folds secondary to edema [34,35]. Subtle
minimal bowel wall thickening may be seen. Small
ulcers can be shown by carefully performed radio-
logic examinations. Barium examination, particularly
air enteroclysis, is superior to other imaging studies
with regard to diagnosis in this subtype [9], although
early experience shows that MR enteroclysis may
also be more effective in the demonstration of
minimal disease [30]. The typical findings on barium
examination of minimal active inflammatory subtype
are shown in Fig. 2. The air double-contrast entero-
clysis method shows subtle surface changes—such as
mucosal granularity and aphthae—better than do
other radiologic methods, but consistently reliable
images may be more difficult to obtain [36] (Fig. 3;
see also Fig. 4D in the article by Maglinte et al
entitled ‘‘Technical Refinements in Enteroclysis,’’
this issue).
The subtle findings at CT in this subtype are
minimal and nonspecific (Fig. 4). Small ulcers or
aphthae are not shown by CT. Mucosal hyperemia
and mild submucosal edema are better evaluated by
multidetector intravenous (IV) contrast-enhanced CT
Table 1
Radiologic classification of small bowel Crohn’s disease
Active inflammatory subtype
Minimal changes
Superficial ulcerations (aphthae)
Minimal fold thickening or distortion (edema)
Severe changes
Deep ulcers, cobblestone mucosa (longitudinal and
transverse ulcers)
Marked wall thickening due to transmural
inflammation (mural stratification and target sign)
Obstruction secondary to spasm
‘‘Comb sign’’
Fibrostenotic subtype
Minimal stenosis
Minimal decrease in luminal diameter, mild
prestenotic dilatation
Minimal wall thickening, no bowel wall edema
Severe stenosis
Marked decrease in luminal diameter, with obvious
prestenotic dilatation
Marked wall thickening of soft tissue density, no
mural edema
Fistulizing/perforating subtype
Deep fissuring ulcers, sinus tracts
Fistulae to adjacent organs, bowel, skin
Associated inflammatory mass
Reparative or regenerative subtype
Mucosal atrophy
Regenerative polyps
Minimal decrease in luminal diameter—no mural edema
D.D.T. Maglinte et al / Radiol Clin N Am 41 (2003) 285–303286

Fig. 1. Complexity of course of Crohn’s disease of the small bowel.
Fig. 2. Active inflammatory subtype, minimal changes. Findings on barium examination. (A) Enteroclysis of an 18-year-old
female with recurrent lower abdominal pain and diarrhea shows minimal diffuse fold abnormality (thickening and prominent
lymphoid follicles) in the terminal ileum with the scattered small ulcers (arrow in one). Colonoscopy to the terminal ileum
showed multiple aphthae. C, cecum. (B) Enteroclysis of a 28-year-old male with acute abdominal pain and diarrhea shows
thickened slightly irregular folds consistent with submucosal edema (arrow). No ulcers are demonstrated, but endoscopy
showed ulcerations. (From Maglinte DDT, Chernish SM, Kelvin FM, et al. Crohn disease of the small intestine: accuracy and
relevance of enteroclysis. Radiology 1992;184:541–5; with permission.)
D.D.T. Maglinte et al / Radiol Clin N Am 41 (2003) 285–303 287

anteroclysis with methylcellulose as intraluminal con-
trast agent [25]. Because conventional CTexamination
commonly is performed first in the evaluation of a
patient with known or suspected Crohn’s disease,
radiologists should recognize the mild subtle thick-
ening that should lead to a confirmatory examination.
Severe inflammatory activity is characterized
on barium examinations by deep ulcers seen as
contrast collections or marginal addition defects
(protrusion) in a thickened bowel wall or as a
‘‘cobblestone mucosa’’ (Fig. 5). The cobblestone
mucosa reflects severe edema between longitudinal
and transverse ulcerations that result in a cobblestone
street-like appearance of the mucosa. This cobble-
stone mucosa appears similar on both barium exam-
ination and CT enteroclysis with positive enteral
contrast (Fig. 6).
Unlike mild inflammatory disease activity, the
changes of severe inflammatory disease activity on
CT are easily appreciated. Contrast-enhanced CT
with positive intraluminal and IV contrast enhance-
ment will show moderate to marked bowel wall
thickening. The deep ulcers are manifested by
enteral contrast protrusions into the edematous wall
(Fig. 7). The demonstration on IV contrast-enhanced
CT of ‘‘mural stratification’’ indicates edema from
active inflammation [11]. This mural stratification is
composed of an inner ring of mucosal enhancement
surrounded by an outer ring of muscular and serosal
enhancement, with an intermediate low-density ring
due to submucosal edema [11,19,20]. The enhancing
layers reflect underlying active inflammatory dis-
ease. With effective treatment, the stratification
diminishes or resolves. When positive oral contrast
is used in CT with IV contrast, the inner ring of
mucosal enhancement is isoattenuated by the density
of the luminal contrast, but still can be faintly
discerned (Fig. 8). The ‘‘target’’ or ‘‘halo’’ sign
from active inflammatory disease subtype should
be differentiated from the ‘‘halo’’ produced by
submucosal fat deposition seen in chronic disease
(Fig. 9). Although mucosal hyperemia may not be
appreciated readily when positive intraluminal con-
trast is used, presence of the ‘‘comb sign’’ suggests
perienteric hyperemia and bowel wall inflammation
(Fig. 10) [37]. The comb sign should be differentiated
from mesenteric stranding that does not necessarily
indicate inflammation.
MR enteroclysis may disclose similar appearances
of the inflamed, thickened bowel wall after gadolin-
ium IVadministration (Fig. 11). A hyperemic mucosal
layer is identified by its high signal intensity due to
increased gadolinium uptake, whereas submucosal
edema has a low signal intensity, surrounded by a
seromuscular layer with moderate signal intensity that
results in a ‘‘target-type’’ configuration. The signal
intensity on postgadolinium T1-weighted images of
the thickened bowel wall is considered to be an
indicator of disease activity [38,39]. In addition, MR
enteroclysis demonstrates mesenteric inflammatory
changes in the form of vascular engorgement, the
comb sign, and lymphadenopathy in patients with
active Crohn’s disease (Fig. 12). The comb sign,
which corresponds to increased mesenteric vascular-
ity, can be seen ideally on true fast imaging with
steady-state free precession (FISP) images close to the
mesenteric border of a small bowel segment in the
form of short, parallel, low signal intensity, linear
structures perpendicular to the intestinal long axis of
the bowel [30]. Small mesenteric lymph nodes are
easily detected by their low signal intensity scattered
within the bright mesenteric fat on true FISP images.
The presence of lymph nodes is not as obvious with
the use of other MR enteroclysis sequences because of
short T2 filtering effects on half-Fourier acquisition
single-shot turbo spin echo (HASTE) images and to
saturation effects of mesenteric fat signal on three-
Fig. 3. Double-contrast enteroclysis with air showing subtle
mucosal granularity in a segment of small bowel (open arrow)
indicating mucosal atrophy. In addition, an ulcer (curved
arrow) is noted, andmultiple aphthae (small arrow in one) are
present, suggesting early recurrance. Chronic disease is seen
in a more distal segment. (Courtesy of M. Maruyama, MD,
Tokyo, Japan).
D.D.T. Maglinte et al / Radiol Clin N Am 41 (2003) 285–303288
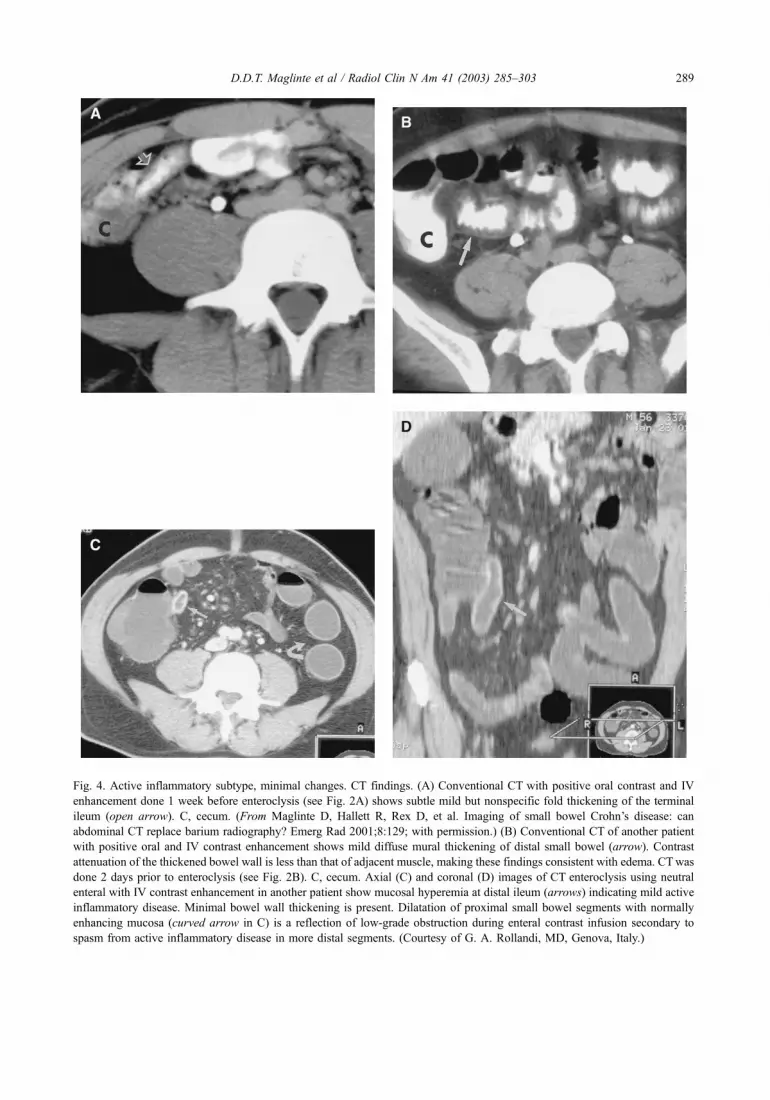
Fig. 4. Active inflammatory subtype, minimal changes. CT findings. (A) Conventional CT with positive oral contrast and IV
enhancement done 1 week before enteroclysis (see Fig. 2A) shows subtle mild but nonspecific fold thickening of the terminal
ileum (open arrow). C, cecum. (From Maglinte D, Hallett R, Rex D, et al. Imaging of small bowel Crohn’s disease: can
abdominal CT replace barium radiography? Emerg Rad 2001;8:129; with permission.) (B) Conventional CT of another patient
with positive oral and IV contrast enhancement shows mild diffuse mural thickening of distal small bowel (arrow). Contrast
attenuation of the thickened bowel wall is less than that of adjacent muscle, making these findings consistent with edema. CTwas
done 2 days prior to enteroclysis (see Fig. 2B). C, cecum. Axial (C) and coronal (D) images of CT enteroclysis using neutral
enteral with IV contrast enhancement in another patient show mucosal hyperemia at distal ileum (arrows) indicating mild active
inflammatory disease. Minimal bowel wall thickening is present. Dilatation of proximal small bowel segments with normally
enhancing mucosa (curved arrow in C) is a reflection of low-grade obstruction during enteral contrast infusion secondary to
spasm from active inflammatory disease in more distal segments. (Courtesy of G. A. Rollandi, MD, Genova, Italy.)
D.D.T. Maglinte et al / Radiol Clin N Am 41 (2003) 285–303 289

dimensional (3D) fast long angle shot (FLASH)
images [30].
Fistulizing/perforating disease subtype
This Crohn’s subtype is characterized by active
inflammation with a tendency toward or eventual
progression to transmural extension of the inflamma-
tory process with resultant fistula formation or
perforation. Deep ulcers precede sinus and fistulae
formation to adjacent organs. The features of this
subtype of Crohn’s disease include demonstration of
deep fissuring ulcers and sinus tracts, fistulae to
adjacent bowel loops or other organs, the demon-
stration of an associated abscess, and extraintesti-
nal involvement on barium examination and CT
(Fig. 13).
MR enteroclysis also may be used to depict and
define extraintestinal complications of Crohn’s dis-
ease; deep ulcers, sinus tracts, and fistulas can be
accurately disclosed on true FISP MR enteroclysis
images (Figs. 14, 15). The characteristic deep linear
ulcers typically seen in Crohn’s disease can be
identified on MR enteroclysis as transversely or
longitudinally oriented thin, high-intensity lines
within the bowel wall on true FISP images. True
FISP sequence is superior to HASTE in demonstrat-
ing discrete ulcers and intramural tracts, whereas 3D
FLASH sequence has lower performance in this
regard [30].
Fibrostenotic disease subtype
Small bowel obstruction is the predominant
clinical manifestation of this disease subtype. When
severe, this subtype can be seen on abdominal plain
radiographs. Barium examination shows fixed seg-
ments of stenosis without thickening of the folds.
There is marked prestenotic dilatation (Fig. 16). CT
imaging demonstrates a fixed narrowing of the
involved bowel with associated wall thickening.
This is seen during IV contrast-enhanced examina-
tions as a homogeneous soft tissue attenuation of
the thickened wall with no evidence of edema
(Fig. 17). The degree of stenosis is variable, ranging
from mild to severe. This subtype should be differ-
entiated from small bowel obstruction secondary to
spasm associated with active inflammatory disease
(see Fig. 8A).
Fig. 5. Active inflammatory subtype, severe changes. Findings on barium examination. (A) Enteroclysis of 30-year-old patient
with worsening diarrhea and abdominal pain shows deep marginal protrusions (arrows) along mesenteric margin of distal ileum
consistent with deep ulcers. A cobblestone mucosa also is seen. Separation between bowel loops suggests wall thickening
exaggerated by the compression paddle. C, cecum. (B) Cobblestone mucosa manifested by crisscrossing linear ulcers separated
by mounds of edema suggestive of severe inflammation of a long segment of distal ileum (arrow) in another patient.
D.D.T. Maglinte et al / Radiol Clin N Am 41 (2003) 285–303290

On MR enteroclysis, the rich tissue contrast
intrinsic to the nuclear MR phenomenon helps
to facilitate the differentiation between fibrotic
(Fig. 18) and edematous bowel wall thickening.
Collagen, the main component of the fibrotic wall
thickening, has long T1 and short T2 relaxation
times, thus exhibiting low signal intensity on both
T1 and T2 relaxation times while rendering high
signal intensity on T2-weighted images and low
signal intensity on T1-weighted images. Differenti-
ation between fibrotic and edematous stenosis
based on MR imaging properties is useful for
selecting patients for medical (edematous) versus
surgical (fibrotic) treatment.
Reparative or regenerative disease subtype
This subtype reflects inactive Crohn’s disease and
may be associated with other phases of Crohn’s
disease located in different locations in the same
small bowel. Mucosal atrophy and regenerative
polyps characterize this phase (Fig. 19). There may
be a decrease in lumen diameter, but there is no
evidence of active inflammation.
Selection of imaging modality and clinical
relevance of radiologic findings in small bowel
Crohn’s disease
Barium examination and CT are currently the
most commonly used radiologic methods of exam-
ination in the assessment of small bowel Crohn’s
disease. In many patients, both procedures are used
to determine the severity of disease activity and the
extent of the disease process [40]. The choice of
initial examination depends on the clinical issue in
question. The differences between conventional CT
and barium enteroclysis in demonstrating diagnostic
features and complications of small bowel Crohn’s
disease in 33 patients who had both procedures done
for the same indications recently were reported
(Table 2) [40]. Statistically significant differences
favoring enteroclysis were shown in the ability to
diagnose ulceration, obstruction, and strictures in the
small bowel. Unique and complementary diagnostic
information was provided by both methods of
examination. MR enteroclysis is an emerging tech-
nique for small bowel imaging that combines the
advantages of barium enteroclysis with those of
cross-sectional imaging [41,42]. MR imaging is
the emerging modality of choice for imaging of
small bowel Crohn’s disease, because of its superb
soft tissue contrast, the static and dynamic three-
dimensional imaging capabilities, and the absence
of ionizing radiation exposure. The availability of
ultrafast sequences is a new added advantage.
Realistically, however, cost and availability of this
technology may be significant limitations to its
widespread use.
Historically, barium studies have correlated
poorly with the clinical stage of the disease and
with the response of patients to treatment [43]. This
discrepancy is due, in part, to suboptimal barium
examination methods being employed. Significant
advances in the radiologic investigation of small
bowel Crohn’s disease have been made since these
original comparisons, primarily due to refinements
in enteroclysis, multidetector helical CT, and MR
imaging. In the National Cooperative Crohn’s Dis-
ease Study [43], the radiographic demonstration of a
stricture that caused obstruction or of a fistula was
associated with poor clinical response to medical
treatment. In a comparative study of small bowel
Fig. 6. CT enteroclysis with positive enteral contrast of a
17-year-old male with worsening diarrhea and weight loss
shows cobblestone mucosa of a long segment of distal small
bowel. Mounds of edema are manifest by ovoid or nodular
defects and ulcerations manifest as irregular marginal
protrusions (arrow in one) in the bowel wall. The involved
segment also shows a thickened wall.
D.D.T. Maglinte et al / Radiol Clin N Am 41 (2003) 285–303 291
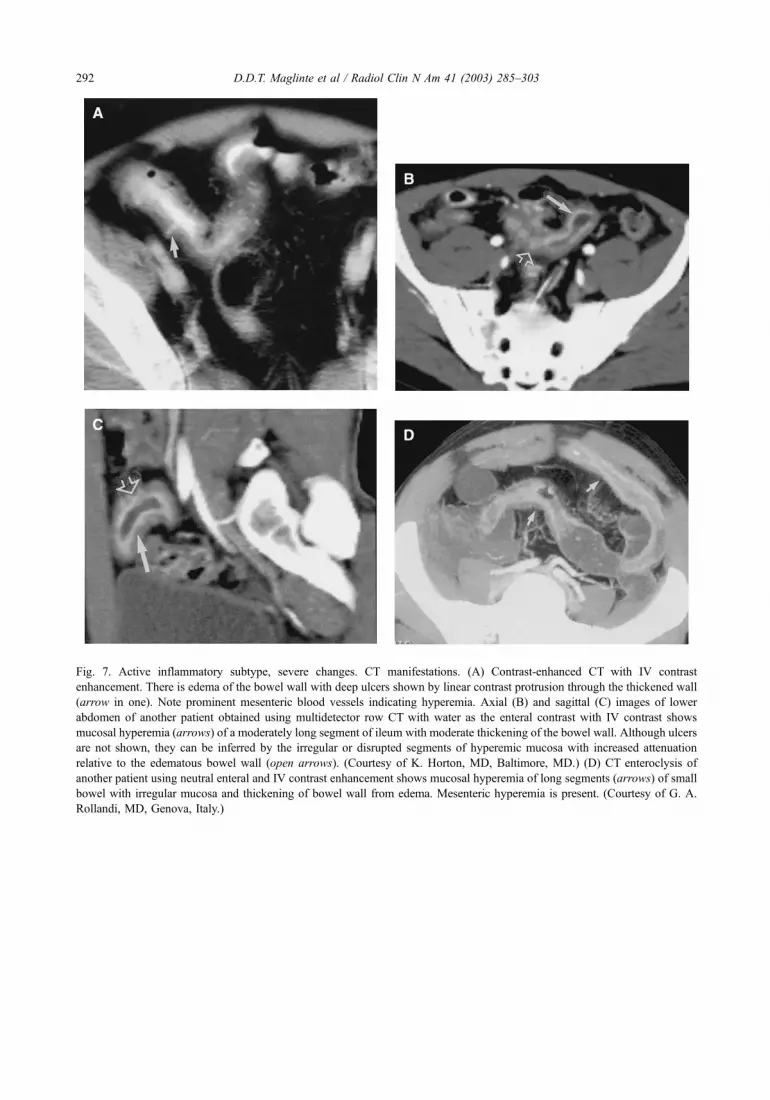
Fig. 7. Active inflammatory subtype, severe changes. CT manifestations. (A) Contrast-enhanced CT with IV contrast
enhancement. There is edema of the bowel wall with deep ulcers shown by linear contrast protrusion through the thickened wall
(arrow in one). Note prominent mesenteric blood vessels indicating hyperemia. Axial (B) and sagittal (C) images of lower
abdomen of another patient obtained using multidetector row CT with water as the enteral contrast with IV contrast shows
mucosal hyperemia (arrows) of a moderately long segment of ileum with moderate thickening of the bowel wall. Although ulcers
are not shown, they can be inferred by the irregular or disrupted segments of hyperemic mucosa with increased attenuation
relative to the edematous bowel wall (open arrows). (Courtesy of K. Horton, MD, Baltimore, MD.) (D) CT enteroclysis of
another patient using neutral enteral and IV contrast enhancement shows mucosal hyperemia of long segments (arrows) of small
bowel with irregular mucosa and thickening of bowel wall from edema. Mesenteric hyperemia is present. (Courtesy of G. A.
Rollandi, MD, Genova, Italy.)
D.D.T. Maglinte et al / Radiol Clin N Am 41 (2003) 285–303292

Fig. 8. Active inflammatory disease subtype manifested by the ‘‘target sign’’ and ‘‘mural stratification’’ on IV contrast-enhanced
CT with water as the enteral contrast agent. (A) Seen on end, the target sign is indicated by the small inner ring of mucosal
enhancement surrounding the fluid in the lumen (small arrow), separated by an intermediate low-density ring from the outer ring
of muscular and serosal enhancement (curved arrow). Note distention of more proximal small bowel loops, which is a reflection
of spasm from active disease. (B) When seen tangentially, active inflammatory disease is manifested by mural stratification. The
inner line of mucosal enhancement (small arrow) is separated by the intermediate low-density (edema) thickening from the
enhancement (curved arrow), indicating muscular and serosal hyperemia. Note accompanying ascites. U, uterus. (From
Maglinte D, Hallett R, Rex D, et al. Imaging of small bowel Crohn’s disease: can abdominal CT replace barium radiography?
Emerg Rad 2001;8:129; with permission.) (C) Mucosal hyperemia (arrow) can be discerned from the positive intraluminal
contrast as a faint thin density and the outer layer of bowel wall edema of another patient. Note enlarged mesenteric nodes.
D.D.T. Maglinte et al / Radiol Clin N Am 41 (2003) 285–303 293

follow-through versus enteroclysis [44], obstruction,
fistula, and other diagnostic aspects of Crohn’s
disease were better shown by enteroclysis. A more
detailed demonstration of the fold abnormalities seen
in inflammatory bowel disease is shown with the
infusion method [4,9,44,45]. Nevertheless, oral
methods of examination that visualize the entire
small bowel, when combined with intermittent fluo-
roscopy and adequate compression, may approach
the accuracy of enteroclysis [3,7]. The gas-enhanced
follow-through examination [46] and the peroral
pneumocolon method [47] have been recommended
for use with peroral methods to improve evaluation
of the distal small bowel in the region of the
ileocecal valve or ileocolic anastomosis.
Although CT is unable to identify early mucosal
changes of the disease, it is far superior for showing
mural abnormalities and extraintestinal manifesta-
tions including bowel wall thickening, and mes-
enteric inflammatory changes including adenopathy.
CT can determine whether a mesenteric mass repre-
sents phlegmon, abscess, or adenopathy [10,16,18],
which influences management decisions consid-
erably. Once identified, CT-guided catheter drainage
of an intra-abdominal abscess can be instituted. CT
also has been useful for the diagnosis of entero-
vesical fistula [48]. The widespread availability of
CT makes it an ideal initial method of examination.
The use of IV contrast-enhanced multidetector row
CT with water or methylcellulose as enteral contrast
agent, using reformatting in different planes or
volume rendering might be able to answer most
clinical queries relevant to patients management.
Barium enteroclysis, CT enteroclysis, or MR entero-
clysis could then be used if further assessment
is needed.
It remains to be seen whether CT enteroclysis, a
method that combines the advantages of the cross-
sectional display of CT and the volume challenge of
the small bowel induced by enteroclysis infusion, is
an ideal method of examination for showing the
complications of Crohn’s disease [21–25]. The
advantages of helical CT in demonstrating a greater
degree of mural enhancement following IV contrast
administration when compared with conventional CT
and the use of multiplanar reformatting may improve
its ability to delineate the extent of small bowel
disease [20]. The advantages of CT enteroclysis also
apply to MR enteroclysis; the latter technique has
the added advantages of increased soft tissue con-
trast and direct multiplanar capabilities [26–30,
Fig. 9. Submucosal fat deposition in chronic Crohn’s
disease. Arrow points to deposit of fat in submucosa
surrounding positive intraluminal contrast. Other manifes-
tations of Crohn’s disease are also present. Note mesenteric
stranding (open arrow).
Fig 10. ‘‘Comb sign’’ on IV contrast-enhanced CT. Prom-
inent vasa recta (arrow) are seen, indicating perienteric hy-
peremia. Edema of the bowel wall is also present. The ‘‘comb
sign’’ indicates severe active inflammatory disease subtype.
D.D.T. Maglinte et al / Radiol Clin N Am 41 (2003) 285–303294

Fig. 11. MR imaging of active inflammatory disease subtype. (A) 29-year-old male with abdominal pain and diarrhea. MR
enteroclysis postgadolinium 3D FLASH image (TR/TE/a = 4.8 ms/1.6 ms/45, 40 partitions, 2.5-mm thickness, 256 � 512 image
matrix, 22-second breath-hold duration). Stratified pattern of enhancement in active Crohn’s disease generates the target sign
(arrow) by the moderate signal intensity of the serosa, low signal intensity of the edematous submucosa, and high signal intensity
of the hyperemic mucosa. (B) True FISP (TR/TE/a = 6.5 ms/3 ms/70, 4-mm section thickness, 256 � 256 image matrix,
19-second breath-hold duration) coronal image demonstrates with high signal intensity (arrow) edematous wall thickening in
another patient with Crohn’s disease. (C) 3D FLASH with fat saturation (TR/TE/a= 4.8 ms/1.6 ms/45, 40 partitions, 2.5-mm
thickness, 256 � 512 image matrix, 22-second breath-hold duration) coronal image acquired after glucagon and IV gadolinium
administration of same patient (in B). Submucosal edema presents with low signal intensity against the high signal intensity
serosa and mucosal layers, generating an MR ‘‘mural stratification’’ (arrow).
D.D.T. Maglinte et al / Radiol Clin N Am 41 (2003) 285–303 295

38,39,41,42]. High contrast resolution ultrafast
sequences such as single-shot turbo spin echo, true
FISP, HASTE, and contrast-enhanced 3D FLASH
applied to a well-distended small bowel make MR
enteroclysis a powerful tool in demonstrating the
wide spectrum of disease abnormalities and compli-
cations of small bowel Crohn’s disease, while simul-
taneously providing information regarding disease
activity [30]. MR enteroclysis correlates with barium
enteroclysis in disclosing superficial and transmural
abnormalities of the disease, and musters all the
advantages of cross-sectional imaging in disclosing
extraintestinal manifestations and complications of
the disease. Changes in small bowel kinetics may
also be evaluated on MR fluoroscopy. In addition,
initial experience shows that MR imaging can pro-
vide an adequate pictorial assessment of local
inflammatory disease activity, thus directly influ-
encing patient management. It has been suggested
that MR imaging could be the evolving ‘‘all-in-one’’
examination technique that can answer all major
clinical questions that arise in the course of Crohn’s
disease [49]. The precise role of this technique
awaits further experience and research.
As noted above, imaging features, considered in
the context of clinical and endoscopic information,
helps to establish the subtype of Crohn’s affecting
individual patients. Patients with active inflamma-
tory disease respond best to medical therapy, and
may respond to a range of medical therapies.
Patients with fistulizing/perforating disease tend to
be most responsive to infliximab (Centocor, Inc.,
Malvern, PA) or azathioprine (Faro Pharmaceuticals,
Inc., Bedminster, NJ). Cyclosporine (Novartis
Pharm-Corp, East Hanover, NJ) may be effective
in fistulizing disease subtypes refractory to other
agents. Surgery is indicated in fistulizing disease
that is not responsive to medical treatment. Symp-
tomatic fibrostenosing disease may require manage-
ment by surgical resection, stricturoplasty, or
endoscopic balloon dilation in cases in which stric-
tures are short and endoscopically accessible.
Clearly there is overlap between different subtypes,
and individual patients may manifest features of
multiple subtypes at the same or different points
in time.
Summary
This article has reviewed the imaging features
that correspond to and support the classification of
patients into clinical subtypes of Crohn’s disease.
One study [50] showed that radiologic features on
barium studies closely correlated with the Crohn’s
Disease Activity Index, and another study [10]
indicated that CT findings changed patient manage-
ment in up to 29% of cases. Knowledge of the
location, severity, and presence of complications
assist in providing patients with appropriate treat-
ment options.
Reports of radiologic studies in Crohn’s disease
should include the presence or absence of imaging
features that support these different subtypes. An
additional advantage of the use of a reproducible
imaging classification that emphasizes morphologic
features would be improved comparison of the
results of different investigators and treatment pro-
tocols. Whatever method of radiologic investigation
is employed, it should be targeted to answer ques-
tions relevant to patient management. The imaging
modalities used should be able to classify the small
bowel Crohn’s subtypes and should be reflected in
the radiologists’ reports.
Fig 12. Increased mesenteric vascularity (comb sign) and
lymphadenopathy in a 26-year-old male patient with active
Crohn’s disease (Crohn’s disease activity index = 233).
Luminal narrowing and thickening of the bowel wall of
distal ileal loops. Dilated vasa recta at the mesenteric border
of the affected segment are clearly shown on true FISP
images (TR/TE/a = 6.5 ms/3 ms/70, 4-mm section thickness,
256 � 256 image matrix, 19-second breath-hold duration).
Multiple mesenteric lymph nodes measuring less than 1 cm
in diameter (arrows).
D.D.T. Maglinte et al / Radiol Clin N Am 41 (2003) 285–303296

Fig. 13. Imaging findings of fistulizing/perforating subtype Crohn’s disease. (A) Barium enteroclysis of a 40-year-old patient
with known Crohn’s disease showing multiple ileoilial and ileosigmoid fistulae. The distal ileum forms the central pocket
(curved arrow) where the cecum and adjacent small bowel loops are ‘‘sucked’’ in and from which multiple fistulae originate.
R, rectum. (B) Enteroclysis examination of another patient shows multiple deep ulcers (small arrow in one) in long edematous
neodistal ileum with a long sinus tract communicating with a large cavity (arrow). (From Kelvin F, Herlinger H. Crohn’s
disease. In: Herlinger H, Maglinte D, Birnbaum B, editors. Clinical imaging of the small intestine. 2nd edition. New York:
Springer; 1999. p. 281; with permission.) (C) CT of same patient (in B) shows a large gas-containing abscess adjacent to the
diseased ileum. Deep ulcer (arrow) is seen in diseased neodistal ileum. (From Kelvin F, Herlinger H. Crohn’s disease. In:
Herlinger H, Maglinte D, Birnbaum B, editors. Clinical imaging of the small intestine. 2nd edition. New York: Springer; 1999.
p. 281; with permission.) (D) Anterior abdominal wall abscess (arrow) in another patient with adjacent anterior intraperitoneal
(curved arrow) abscess infiltrating the parietal peritoneum. Narrowed markedly edematous ileum (open arrow) is seen in right
lower abdomen.
D.D.T. Maglinte et al / Radiol Clin N Am 41 (2003) 285–303 297

Fig. 14. 46-year-old male with Crohn’s disease diagnosed
10 years ago. Wall thickening associated with discrete
ulcers (arrows) is shown on a coronal spot view with a
true FISP sequence (TR/TE/a = 6.5 ms/3 ms/70, 4-mm
section thickness, 256 � 256 image matrix, 19-second
breath-hold duration). (From Gourtsoyiannis N, Papaniko-
laou N, Grammatikakis J, Maris T, Prassopoulos P. MR
enteroclysis protocol optimization: comparison between 3D
FLASH with fat saturation after intravenous gadolinium
injection and true FISP sequences. Eur Radiol 2001;11(6):
911; with permission.)
Fig 15. Fistulizing Crohn’s disease. Multiple enteroenteric
fistulas are seen on axial true FISP (TR/TE/a = 6.5 ms/3 ms/
70, 4-mm section thickness, 256 � 256 image matrix,
19-second breath-hold duration) image (arrows). (From
Gourtsoyiannis N, Papanikolaou N, Grammatikakis J, Maris
T, Prassopoulos P. MR enteroclysis protocol optimization:
comparison between 3D FLASH with fat saturation after
intravenous gadolinium injection and true FISP sequences.
Eur Radiol 2001;11(6):911; with permission.)
D.D.T. Maglinte et al / Radiol Clin N Am 41 (2003) 285–303298

Fig. 16. Fibrostenosing Crohn’s disease subtype. (A) Enteroclysis of a patient with known Crohn’s disease who presented
with worsening abdominal pain. These are fixed segments of narrowing (curved arrows) with marked prestenotic dilatation.
The narrowed segments are not edematous. Filiform polyps are identified (small arrow in one). Note ileosigmoid fistula
(open arrow). (From Maglinte DDT, Chernish SM, Kelvin FM, et al. Crohn disease of the small intestine: accuracy and
relevance of enteroclysis. Radiology 1992;184:541–5; with permission.) (B) CT shows a segment of small bowel narrowing
with soft tissue attenuation (fibrosis) of thickened bowel wall (arrow). There is marked prestenotic dilatation.
Fig. 17. Multidetector row helical CT with water as enteral contrast with IV contrast enhancement in stenosing disease subtype.
(A) Axial image at level of midabdomen shows markedly dilated loops of small bowel with fluid and gas. Note normal mucosal
enhancement and thickness of uninvolved dilated loops (arrow). (B) Axial image at level of upper pelvis shows point of
obstruction (arrow). The attenuation of the stenosed segment is similar to that of soft tissue, consistent with fibrosis. There is no
evidence of mucosal hyperemia or mural stratification. (Courtesy of K. Horton, MD, Baltimore, MD.)
D.D.T. Maglinte et al / Radiol Clin N Am 41 (2003) 285–303 299

Fig. 18. 28-year-old female with longstanding Crohn’s disease presented with ileus. (A) True FISP (TR/TE/a = 6.5 ms/3 ms/70,
4-mm section thickness, 256 � 256 image matrix, 19-second breath-hold duration) coronal section. A short fibrostenotic ideal
segment with significant prestenotic dilation (B) 3D FLASH with fat saturation (TR/TE/a = 4.8 ms/1.6 ms/45, 40 partitions,
2.5-mm thickness, 256 � 512 image matrix, 22-second breath-hold duration). Coronal image shows homogeneous contrast
enhancement in the region of the fibrotic stricture (open arrow).
Fig. 19. CT enteroclysis showing filiform polyps (arrows) in a long segment of small bowel indicating reparative subtype of
Crohn’s disease. There is no evidence of fold thickening or ulcers (see also Fig. 16A).
D.D.T. Maglinte et al / Radiol Clin N Am 41 (2003) 285–303300

Table 2
Diagnostic differences between CT and enteroclysis in demonstrating features of small bowel Crohn’s disease
CT Enteroclysis
No. patients % No. patients %
Ulcerations 7 19 29 78
Mural edema 15 41 17 46
Obstruction 6 16 17 46
Stricture 4 11 14 38
Sinus tract 2 5 10 27
Fistula 3 8 9 24
Abscess 10 27 7 19
Extraintestinal disease 3 0 0 0
Total sites 47 54
Data from Maglinte D, Hallett R, Rex D, et al. Imaging of small bowel Crohn’s disease: can abdominal CT replace
barium radiography? Emerg Rad 2001;8:127–33.
D.D.T. Maglinte et al / Radiol Clin N Am 41 (2003) 285–303 301

References
[1] Przemioslo RT, Ciclitira PJ. Pathogenesis of Crohn’s
disease. Q J Med 1995;88:525–7.
[2] Chernish SM, Maglinte DDT, O’Connor K. Evaluation
of the small intestine by enteroclysis for Crohn’s dis-
ease. Am J Gastroenterol 1992;87:696–701.
[3] Bartram CI. Radiology in inflammatory bowel disease.
New York: Marcel Dekker; 1983. p. 121–5.
[4] Nolan DJ, Gourtsoyiannis NC. Crohn’s disease of
the small intestine: a review of the radiological ap-
pearances in 100 consecutive patients examined by a
barium infusion technique. Clin Radiol 1980;31(5):
597–603.
[5] Kelvin FM, Maglinte DDT. The small bowl: Crohn’s
disease. In: Taveras JM, Ferrucci JT, editors. Radiolo-
gy diagnosis—imaging—intervention. Philadelphia:
Lippincott-Raven; 1998. p. 1–11.
[6] Ott DJ, Chen YM, Gelfand DW, et al. Detailed per oral
small bowel examination versus enteroclysis. Radiol-
ogy 1985;155:29–34.
[7] Carlson JHC. Perspective: the small bowel examina-
tion in the diagnosis of Crohn’s disease. AJR Am J
Roentgenol 1986;147:63–5.
[8] Herlinger H. The small bowel enema and the diagnosis
of Crohn’s disease. Radiol Clin North Am 1982;20:
721–42.
[9] Maglinte DDT, Chernish SM, Kelvin FM, et al. Crohn
disease of the small intestine: accuracy and relevance
of enteroclysis. Radiology 1992;184:541–5.
[10] Fishman EK, Wolf EJ, Jones B, Bayless TM, Siegle-
man SS. CT evaluation of Crohn’s disease: effect on
patient management. AJR Am J Roentgenol 1987;148:
537–40.
[11] Gore RM. CT of inflammatory bowel disease. Radiol
Clin North Am 1989;27:717–23.
[12] Goldberg HI, Gore RM, Margulis AR, Moss AA,
Baker EL. Computed tomography in the evaluation
of Crohn’s disease. AJR Am J Roentgenol 1983;140:
277–82.
[13] Berliner L, Redmond P, Purow E, Megna D, Sottile V.
Computed tomography in Crohn’s disease. Am J Gas-
troenterol 1982;77:548–53.
[14] Wills JS, Lobis IF, Denstman FJ. Crohn disease: state
of the art. Radiology 1997;202:597–610.
[15] Kerber GW, Greenberg M, Rubin J. Computed tomog-
raphy evaluation of local and extraintestinal complica-
tions of Crohn’s disease. Gastrointest Radiol 1984;9:
143–8.
[16] Lubat E, Balthazar EJ. The current role of computed
tomography in inflammatory disease of bowel. Am J
Gastroenterol 1988;83:107–13.
[17] Frager DH, Goldman M, Beneventano TC. Computed
tomography in Crohn disease. J Comput Assist To-
mogr 1983;7:819–24.
[18] Orel SG, Rebesin SE, Jones B, Fishman EK, Bayless
TM, Siegelman SS. Computed tomography vs barium
studies in the acutely symptomatic patient with Crohn
disease. J Comput Assist Tomogr 1987;11:1009–16.
[19] Gore RM, Balthazar EJ, Ghahremani GG, Miller FH.
CT features of ulcerative colitis and Crohn’s disease.
AJR Am J Roentgenol 1996;167:3–15.
[20] Raptopoulos V, Schwartz RK, McNicholas MMJ,
Mouson J, Pearlman J, Joffe N. Multiplanar helical
CT enterography in patients with Crohn’s disease.
AJR Am J Roentgenol 1997;169:1545–50.
[21] Kloppel R, Thiele J, Bosse J. The Sellink CT method
[in German]. Roto Fortschr Geb Roentgenstr Neven
Bildgeb Vertahr 1992;156:291–2.
[22] Bender GN, Maglinte DDT, Kloppel VR, Timmons
JH. CT enteroclysis: a superfluous diagnostic proce-
dure or valuable when investigating small-bowel dis-
ease? AJR Am J Roentgenol 1999;172:373–8.
[23] Schober E, Turetschek K, Sschima W, et al. Methyl-
cellulose enteroclysis spiral CT in the preoperative as-
sessment of Crohn’s disease: radiologic pathologic
correlation [abstract]. Radiology 1997;717:205.
[24] Mako EK, Mester AR, Tarzan Z, et al. Enteroclysis and
spiral CT examination in diagnosis and evaluation of
small bowel Crohn’s disease. Eur J Radiol 2000;35:
168–75.
[25] DiMizio R, Cerro P, Hassan C, Semeiotica TC. Del
morbo di Crohn del tenue. In: DiMizio R, editor.
Morbo di Crohn del tenue. Atlante di radiologia.
Rome: Verducci Editore; 2002. p. 189–93.
[26] Shoenut JP, Semelka RC, Magro CM, et al. Compar-
ison of magnetic resonance imaging and endoscopy in
distinguishing the type and severity of inflammatory
bowel disease. J Clin Gastroenterol 1994;19:31–5.
[27] Low RN, Francis IR, Politoske D, Bennett M. Crohn’s
disease evaluation: comparison of contrast-enhanced
MR imaging and single phase helical CT scanning.
J Magn Reson Imaging 2000;11:127–35.
[28] Maglinte DDT, Siegelman ES, Kelvin FM. MR enter-
oclysis: the future of small-bowel imaging? Radiology
2000;215:639–41.
[29] Umschaden HW, Szolar D, Gasser J, et al. Small bowel
disease: comparison of MR enteroclysis images with
conventional enteroclysis and surgical findings. Radi-
ology 2000;215:717–25.
[30] Prassopoulos P, Papanikolaou N, Grammatikakis J,
Rousomoustakaki M, Maris T, Gourtsoyiannis N.
MR enteroclysis imaging of Crohns disease. Radio-
graphics 2001;21(Spec No):S161–72.
[31] Camillieri M, Proano M. Advances in the assessment
of disease activity in inflammatory bowel disease.
Mayo Clin Proc 1989;64:800–7.
[32] Sachar DB, Andrews HA, Farmer RG, et al. Proposed
classification of patients’ subgroups in Crohn’s disease.
Gastroenterol Int 1992;5:141–54.
[33] Engleholm L, de Toeuff C, Herlinger H, Maglinte
DDT. Crohn’s disease of the small bowel. In: Herlin-
ger H, Maglinte D, editors. Clinical radiology of
the small intestine. Philadelphia: Saunders; 1989.
p. 295–334.
[34] Glick SN, Teplick SK. Crohn’s disease of the small
intestine: diffuse mucosal granularity. Radiology
1985;154:313–7.
D.D.T. Maglinte et al / Radiol Clin N Am 41 (2003) 285–303302

[35] Jones B, Hamilton SR, et al. Granular small bowel
mucosa: a reflection of villous abnormality. Gastroint-
est Radiol 1987;12:219–25.
[36] Ekberg O. Barium/air double contrast examination of
the small bowel in Crohn’s disease. Fortschr Ront-
genstr 1984;140:379–86.
[37] Meyers MA, MacGuire PV. Spiral CT demonstration
of hypervascularity in Crohn’s disease: ‘‘vascular jeju-
nization’’ of the ileum or the ‘‘comb sign’’. Abdom
Imaging 1995;20:327–32.
[38] Gourtsoyiannis N, Papanikolaou N, Grammatikakis J,
Prassopoulos P. MR enteroclysis: technical considera-
tions and clinical applications. Eur Radiol 2002,
in press.
[39] Marcos HB, Semelka RC. Evaluation of Crohn’s dis-
ease using half-Fourier RARE and gadolinium-en-
hanced SGE sequences: initial results. Magn Reson
Imaging 2002;18(3):263–8.
[40] Maglinte D, Hallett R, Rex D, et al. Imaging of small
bowel Crohn’s disease: can abdominal CT replace bar-
ium radiography? Emerg Rad 2001;8:127–33.
[41] Gourtsoyiannis N, Papanikolaou N, Grammatikakis J,
Maris T, Prassopoulos P. Magnetic resonance imaging
of the small bowel using a true-FISP sequence after
enteroclysis with water solution. Invest Radiol 2000;
35(12):707–11.
[42] Gourtsoyiannis N, Papanikolaou N, Grammatikakis J,
Maris T, Prassopoulos P. MR enteroclysis protocol
optimization: comparison between 3D FLASH with
fat saturation after intravenous gadolinium injection
and true FISP sequences. Eur Radiol 2001;11(6):
908–13.
[43] Goldberg HI, Caruthers SB, Nelson JA, Singleton JW.
Radiographic findings of the National Cooperative
Crohn’s Disease Study. Gastroenterology 1979;77:
925–37.
[44] Ekberg O. Crohn’s disease of the small intestine ex-
amined by double contrast technique. A comparison
with the oral technique. Gastrointest Radiol 1977;1:
355–9.
[45] Nolan DJ, Piris J. Crohn’s disease of the small intes-
tine: a comparative study of the radiological and patho-
logical appearances. Clin Radiol 1980;31:591–6.
[46] Fraser GM, Preston PG. The small bowel follow-
through enhanced with an oral effervescent agent. Clin
Radiol 1983;34:673–9.
[47] Glick SN. Crohn’s disease of the small intestine. Ra-
diol Clin North Am 1987;25:25–45.
[48] Goldman SM, Fishman ED, Gatewood OMB, et al. CT
in the diagnosis of enterovesical fistula. AJR Am J
Roentgenol 1985;144:1229–33.
[49] Gourtsoyiannis N, Papanikolaou N, Rieber A, Brambs
P, Prassopoulos P. Evaluation of the small intestine by
MR imaging. In: Gourtsoyiannis N, editor. Radiolog-
ical imaging of the small intestine. Berlin: Springer;
2002. p. 157–70.
[50] Tao T, Okada M, Fuchigami T, et al. The relationship
between the radiological and clinical features in pa-
tients with Crohn’s disease. Clin Radiol 1989;40:
389–92.
D.D.T. Maglinte et al / Radiol Clin N Am 41 (2003) 285–303 303





























