Embed Size (px)
Citation preview
128 Journal of Pain and Symptom Management Vol. 13 No. 3 March 1997
Original Article
The Memorial Delirium Assessment Scale Wil l iam Breitbart , MD, Barry Rosenfeld, PhD, Andrew Roth, MD, Mark J. Smith, MD, Ken Cohen , MD, and Steven Passik, PhD Department of Psychiatry (W.B., B.t~, A.t~, K.C., S.P.), Memorial Sloan-Kettering Cancer Center, and Department of Psychiatry (M.J.S.), Mount Sinai Medical Center, New Yo~k, New Yo~k
Abstract We conducted two studies with medically hospitalized cancer and acquired immunodeficiency syndrome (AB)S) patients to assess the reliability and validity of a new measure of delirium severity, the Memorial Delirium Assessment Scale (MDAS). The first study used multiple raters who jointly administered the MDAS to 33 patients, 17 of whom met DSM III-R/DSM IV criteria for delirium, 8 met diagnostic criteria for another cognitive impairment disorder (for example, dementia), and 8 had non-cognitive psychiatric disorders (for example, adjustment disorder). Results indicate high levels of inter-rater reliability for the MDAS (0.92) and the individual MDAS items (ranging from O. 64 to O. 99), as well as high levels of internal consistency (coefficient alpha = O. 91). Mean MDAS ratings differed significantly between delirious patients and the comparison sample of patients with other cognitive impairment disorders or no cognitive impairment (P < 0.0002). The second study compared MDAS ratings of 51 medically hospitalized delirious patients with cancer and AIDS made by one clinician to ratings on several other measures of delirium (Delirium Rating Scale, clinician's ratings of delirium severity) and cognitive functioning (Mini-Mental State Examination) made by a second clinician. Results demonstrated a high correlation between MDAS scores and ratings on the Delirium Rating Scale (r = 0.88, p < 0.0001), the Mini-Mental State Examination (r= - 0.91, P < 0.0001), and clinician's global ratings of delirium severity (r = 0.89, P < 0.0001). Thus, ourfindings indicate that theMDAS is a brief, reliable tool for assessing delirium severity among medically ill populations that can be reliably scored by multiple raters. The MDAS is highly correlated with existing measures of delirium and cognitive impairment, yet offers several advantages over these instruments for repeated assessments which are often necessary in clinical research. J Pain Symptom Manage 1997;13:128-137. © U.S. Cancer Pain Relief Committee, 1997.
Key Words Delirium, rating scales, cance~; AIDS
Introduction Delirium is a common disorder among the
medically ill, and has significant implications for the management of patients with medical
Address reprint requests to: William Breitbart, MD, Depar tment of Psychiatry, Memorial Sloan- Kettering Cancer Center, 1275 York Avenue, New York, NY 10021, USA. Accepted for publication: November 18, 1996.
disorders . Est imates of the p reva lence of d e l i r i u m a m o n g m e d i c a l l y h o s p i t a l i z e d patients generally range f rom 10% to 50%, and vary with the popu la t ion studied (for e x a m p l e , p o s t o p e r a t i v e pa t i en t s , c a n c e r patients, or patients with chronic diseases).1-5 Up to 80% of patients with terminal illness develop delirium near death. 6 A number of ins t ruments have been deve loped to accu- r a t e ly d i a g n o s e d e l i r i u m , i n c l u d i n g the
© U.S. Cancer Pain Relief Committee, 1997 0885-3924/97/$17.00 Published by Elsevier, New York, New York PII S0885-3924(96)00316-8

Vol. 13 No. 3 March 1997 Memorial Delirium Assessment Scale 129
Delirium Rating Scale (DRS), 7 the Confusion Assessment M e t h o d (CAM), s the Del i r ium Symptom Interview (DSI),9 and the Saskatoon Delir ium Checklist (SDC).1° These diagnostic tools have b e e n used fo r ep idemio log i ca l research regarding the prevalence of delir ium or for assisting in the clinical diagnosis of delir ium (for example, as screening tools).
The application of existing delirium diagnos- tic tools to quantify delirium severity or measure treatment response in clinical intervention trials has revealed significant shor tcomings . ~A°-13 Delirium diagnostic tools often elicit symptom information regarding an entire 24-hr period, and are therefore not designed tor repeated assessments within the same day or to moni tor short-term changes in delirium severity that may result f rom clinical interventions (for example, the DRS or the CAM). Several instruments also include items that do not vary f rom day to day, such as the speed of onset of confusional symp- toms (for example, the DRS). Many diagnostic scales also contain items that are useful for the diagnosis of delirium, but are not related to the severity of the disorder. For example, higher scores are assigned for symptoms that have greater relevance to the diagnosis of delirium or d i f fe ren t i a te de l i r ium f r o m d e m e n t i a and schizophrenia (for example, abrupt onset versus gradual onset of symptoms, tactile versus audi- tory hallucinations, or disorganized versus orga- nized delusions ) , but may not be related to the severity of the disorder. 3'9 Other instruments include items regarding the presence of an iden- tifiable organic etiology, which is relevant to diagnosis but not to severity of delirium. 3 Thus, scores elicited by these diagnostic instruments reflect the likelihood of a patient meeting diag- nostic criteria for delirium, not necessarily the severity of that delirium.
Because of the above-noted shor tcomings with existing delirium assessment instruments, we developed a measure specifically designed to quantify the severity of delir ium symptoms for use in clinical i n t e rven t ion trials. The Memorial Delirium Assessment Scale (MDAS) was designed with the intent that the instru- men t could be adminis tered repeatedly within the same day, to allow for objective measure- m e n t of c h a n g e s in d e l i r i u m sever i ty in response to medical changes or clinical inter- ventions. Potential items were developed by the principal investigators (W.B., M.S.) and
were reviewed with regard to content validity by a group of exper ienced consultation-liaison psychiatrists. The resul t ing ins t rument , the MDAS is described below.
Memorial Delirium Assessment Scale T h e MDAS is a t e n - i t e m , f o u r - p o i n t
c l inician-rated scale (possible range, 0-30) designed to quantify the severity of delir ium in medically ill patients (see Appendix 1). I tems included in the MDAS reflect the diagnostic criteria for delir ium in the DSM IV, 14 as well as symptoms of delir ium t~om earlier or alterna- tive classification systems (for example, DSM III, DSM III-R, ICD-9).a
Scale i tems assess disturbances in arousal and level o f consciousness, as well as several areas of cognitive funct ioning (memory, atten- tion, or ienta t ion, dis turbances in thinking) a n d p s y c h o m o t o r ac t iv i ty . I t e m s w e r e anchored with statements reflecting the sever- ity or intensi ty of the symptom, and were reviewed by exper ienced clinicians to ensure ease of administrat ion and ability to generate accurate (reliable) ratings. The resulting scale, which r equ i r e s a p p r o x i m a t e l y 10 m i n to administer (not including additional t ime nec- essa ry to es tab l i sh r a p p o r t , review c h a r t records, and speak to staff/family members ) , integrates behavioral observations and objec- tive cognitive testing. When items cannot be administered, scores can be prora ted f rom the r e m a i n i n g i tems to an equivalent ten- i tem score, however this process was never neces- sary in the studies repor ted below, b
Validation of the MDAS was accomplished th rough two separate studies, both conducted at the Memoria l Sloan-Kettering Cancer Cen- ter between 1992 and 1995. The first study evaluated the reliability and discriminant valid- ity of the MDAS and the second study assessed the concur ren t validity of the instrument.
a Although the MDAS was developed prior to the publication of DSM IV, the MDAS items were devel- oped to be consistent with the proposed DSM IV diagnostic criteria for delirium. 1~ b Prorated scores are calculated by averaging the items completed and multiplying by 10. No data exist at present regarding the reliability or validity of prorated scores or the minimum number of items needed for accurate prorating. Whenever possible, the entire scale should be administered.

130 Breitbart et al. Vol. 13 No. 3 March 1997
Study 1
M e t h o d s
Subjects. Thirty-three patients hospitalized at Memorial Sloan-Kettering Cancer Center took par t in the initial MDAS validation study. The sample comprised 15 men and 18 women with an average age of 56.14 years. The majority of these patients (N = 30) were diagnosed with cancer ; two pa t ien t s were d i a g n o s e d with a c q u i r e d i m m u n o d e f i c i e n c y s y n d r o m e (AIDS), and one was d iagnosed with non- cancerous pancreatitis. All patients had been refer red to the Psychiatry Service for consulta- tion and t reatment , and provided verbal con- sent to be evaluated for the purposes of this study after discussion of the risks and benefits o f p a r t i c i p a t i o n w i t h an e x p e r i e n c e d c o n s u l t a t i o n - l i a i s o n p s y c h i a t r i s t (W.B.) . Because the study procedures required very little deviation f rom standard clinical practice (the presence of two additional psychiatrists inquiring abou t symptoms of delir ium during clinical rounds ) and p re sen t ed no risk of ha rm to patients, written in fo rmed consent was not obtained.
Procedures. All patients were evaluated simul- taneously by two psychiatrists (W.B. and M.S.) using the MDAS during the course of their hospi ta l izat ion. All pat ients had previously b e e n e v a l u a t e d a n d / o r t r e a t e d by a consultation-liaison psychiatrist i n d e p e n d e n t of this study within the 24 hr preceding data collection, and were assessed for study pur- poses dur ing weekly clinical rounds. The diag- noses genera ted by these independen t evalua- tions were not made available to research staff until after comple t ion of the MDAS. These i n d e p e n d e n t e v a l u a t i o n s r e s u l t e d in 17 p a t i e n t s d i a g n o s e d as hav ing a d e l i r i u m according to DSM III-R and proposed DSM IV criteria, 8 m e t DSM III-R and proposed DSM 1V criteria for dement ia or o ther non-delirious cognitive disorders, and 8 were diagnosed with o t h e r psychia t r ic d i so rders ( for e x a m p l e , ad jus tmen t d i sorder or schizophrenia) but had no cognitive disorder. Because this study primarily focused on establishing the reliabil- ity of MDAS ratings, additional informat ion regarding pat ient demographic characteristics, course of illness, or o ther measures of psycho- logical funct ioning were not collected.
Statistical analyses. In te r - i t em reliabil i ty of MDAS was established by calculat ing Cron- bach 's coefficient a lpha for the ten-item scale. I tems were considered for el imination if they were not sufficiently corre la ted with the over- all scale, or resulted in a substantial dec remen t in the scale a lpha coefficient. Inter-rater reli- ability was established by calculating an intrac- lass correlation coefficient 16 for both the total scale, as well as the individual items. Finally, analysis of var iance (ANOVA) was used to assess whether the MDAS significantly differ- en t i a t ed pa t ien ts d i agnosed with de l i r ium f rom patients with o ther cognitive impa i rmen t disorders and patients without any cognitive impa i rmen t disorder. In addition, because our p l a n n e d analyses d e m o n s t r a t e d t ha t the MDAS significantly d i f f e r en t i a t ed be tween delirious and non-delirious patients, we calcu- lated sensitivity and specificity coefficients for var ious cu t -of f scores for c lassif icat ion of patients as having delirium.
R e su l t s
Correlat ional analyses revealed an overall Cronbach ' s a lpha coefficient of 0.91 based on the MDAS ratings of the principal investigator (WB). Only two of the ten i tems analyzed resulted in a reduced overall a lpha coefficient (items 7 and 8, see Append ix 1), and the increment in overall a lpha f rom removal of these two items was minimal (less than 0.01). The item-total correlations for the ten items ranged f rom 0.31 to 0.91, with only items 7 and 8 having i tem total corre la t ions below 0.60. The individual i tem-total corre la t ions and intraclass c o r r e l a t i o n coeff ic ients are detailed in Table 1.
An intra-class correlat ion coefficient for the two psychiatrists' ratings (W.B., M.S.), calcu-
Table 1 Memorial Delirium Assessment Scale
(MDAS) Reliability Data
MDAS Alpha if Item- Intra- item Mean SD removed total r class r
1 1.18 1.10 0.89 0.79 0.86 2 1.03 1.07 0.90 0.68 0.89 3 1.70 1.12 0.90 0.67 0.99 4 1.33 1.14 0.91 0.60 0.94 5 1.52 1.06 0.89 0.86 0.80 6 1.33 1.08 0.89 0.91 0.70 7 0.56 0.98 0.91 0.44 0.74 8 0.44 0.84 0.92 0.31 0.68 9 1.48 0.87 0.90 0.72 0.64 10 1.36 0.96 0.90 0.75 0.72

Vol. 13 No. 3 March 1997 Memorial Delirium Assessment Scale 131
Table 2 Sensitivity, Specificity, and Predictive Accuracy (PA) Using Alternative
Memorial Delirium Assessment Scale (MDAS) Cut-Offs Cut-off score ~ Sensitivity Specificity +PA -PA
10 82.35 75.00 77.78 80.00 11 76.47 81.25 81.25 76.47 12 76.47 87.50 86.67 77.78 13 70.59 93.75 92.31 75.00 14 64.71 93.75 91.67 71.43 15 64.71 100 100 72.73 16 64.71 100 100 72.73
Scores below tile cut-off score were classified as non-delirious.
lated for the entire scale, genera ted an overall c o r r e l a t i o n coef f ic ien t o f 0.92. Ind iv idua l items varied in terms of inter-rater reliability, with intra-class correlat ion coefficients ranging f rom 0.64 to 0.99 (Table 1). Five of the ten i tems yielded inter-rater cor re la t ion coeffi- cients above 0.80 and eight were above 0.70.
Total MDAS scores also differed significantly between the three groups of patients studied [F(2,30) = 11.69, P < 0.0002]. Average MDAS scores for the delirious group were 16.94 (SD = 7.64) versus 8.50 (SD = 2.78) for the sample of eight patients with other (non-delirium) cogni- tive disorders and 5.38 (SD = 4.17) for the eight patients with other (non-cognitive) psychiatric disorders. Post-hoc contrast analyses demon- strated that patients with delirium had signifi- cantly h igher MDAS scores than did the 8 patients with other (non-delirium) cognitive dis- orders (F = 10.49, P<0.003) and the eight patients with non-cognitive psychiatric disorders (F = 19.69, P < 0.0001). There was no significant difference in MDAS scores between patients with other (non-delirium) cognitive disorders and those patients with non-cognitive psychiatric dis- orders (F= 1.06, P = NS).
Because our initial analyses of the MDAS demons t ra ted that the measure significantly discriminated delirious and non-delirious sub- jects, we calculated sensitivity, specificity, posi- tive predictive accuracy and negative predic- tive accuracy rat ios us ing several poss ible MDAS cut-off scores (Table 2). These analyses revealed high levels of specificity and positive predictive accuracy, but modes t levels of sensi- tivity. The cut-off score that opt imized the vari- ous measures of predictive power in our data was 13 (with scores of 13 or above likely reflect ing the presence of del i r ium). Using this cut-off score, 13 patients were identified as likely having delirium, and 12 of these patients were so diagnosed (92.3% positive predictive
accuracy). However, only 12 of 17 delirious pa t i en t s were co r r ec t l y iden t i f i ed by this MDAS cut-off score (70.6% sensitivity). Con- versely, 15 of the 16 patients without delir ium were correctly classified using this MDAS cut- o f f score (93.8% specif ic i ty) , a l t h o u g h 5 patients were falsely classified as not having a delir ium (75.0% negative predictive power).
Study 2
M e t h o d
Subjects. This study included 51 patients (29 male, 22 female) hospi ta l ized at Memor ia l Sloan-Kettering Cancer Center for t rea tment of cancer (N = 48) or AIDS (N= 3). The aver- age age was 57.8 years old, with a range f rom 27 to 88 years. All patients met DSM IV crite- ria for delirium after a diagnostic evaluation by a consultation-liaison psychiatrist or clinical psychologist (within 24 hr prior to data collec- tion), and were ei ther receiving, or were about to begin receiving t rea tment for this disorder at the t ime of the study. All patients provided oral consent after discussion of the study with an exper i enced consultation-liaison psychia- trist (WB). A por t ion of the sample also pro- vided written in fo rmed consent pr ior to devel- oping delir ium as par t of a larger prospective study, a p p r o v e d by the Memor ia l Hospi ta l Institutional Review Board, on the incidence of delir ium a m o n g patients receiving opioid infusion for pain.
Procedures. All patients were evaluated simul- taneously by two expe r i enced consultat ion- liaison psychiatrists within 24 hr after a diag- nosis of delir ium was established by a treating consultat ion-l iaison psychiatr is t /psychologis t in the Psychiatry Service. One clinician (W.B.) rated patients using the Memorial Delir ium

132 Breitbart et al. Vol. 13 No. 3 March 1997
Assessment Scale (MDAS), while a second cli- nician (K.C. or A.R.) rated patients with the following instruments: (a) the Delirium Rating Scale (DRS),7 (b) the Mini-Mental State Exam (MMSE), 17 and (c) Clinician's Global Rating of d e l i r i u m sever i ty (mild, m o d e r a t e , or severe) and delirium type (hypoactive, hyper- active, or mixed) . Demographic and medical informat ion was obtained f rom patients ' hos- pital record.
Delirium Rating Scale (DRS). The DRS is a ten-item diagnostic tool designed to generate valid, reliable diagnoses of del i r ium a m o n g medically ill patients. This inst rument , which is among the most widely used delir ium assess- m e n t instruments, has demonst ra ted reliability and validity in discriminating between deliri- ous and non-delirious patients, and has been used as a measure of delirium severity despite limitations described above.
Mini -Men ta l State Exam (MMSE). T h e MMSE is one of the most frequently utilized cognitive screening tools. The MMSE assesses or ienta t ion , shor t - te rm memory , a t t e n t i o n / concent ra t ion , language, reading, ability to follow instructions, and wri t ing/copying abil- ity. Scores on the MMSE range f rom 30 (no impai rment ) to 0, and several cut-off scores have been r e c o m m e n d e d as indication of sig- nificant cognitive impairment . Although the MMSE has demonst ra ted internal consistency and test-retest reliability, it is not in tended as a diagnostic ins t rument per se. Scores sugges- tive of impa i rmen t cor respond to some form of cognitive disorder, but because of the wide array of abilities tapped, the de te rmina t ion of impa i rmen t is not specific to delirium.
Clinician's Global Rating of delirium severity and delirium type. An ordinal classification sys- tem in which a clinician rates the severity of delir ium along a 0-3 scale cor responding to none, mild, modera te , and severe. In addition, patients were classified as to the sub-type of t h e i r d e l i r i u m ( h y p e r a c t i v e , h y p o a c t i v e , mixed) based on the classification system developed by Liptzin and Levkoff 18
Statistical analyses. Concur ren t validity of the MDAS was established by calculating Pearson p r o d u c t - m o m e n t correlat ion coefficients for the MDAS total score and the ind iv idua l MDAS i tem ratings with the DRS and MMSE. Spearman correlat ion coefficients were used
to assess the relationship between MDAS total score and the individual MDAS items with cli- n ic ian ' s gobal ra t ings of de l i r ium severity because of the ordinal nature of these global ratings. Separate analyses were conducted for the total sample, as well as after stratification by type of delir ium (hypoactive, hyperactive, and mixed). Analysis of covariance was used to ascertain whether or not the MDAS provided any additional predictive utility after statisti- cally controlling for DRS and MMSE scores.
Results
The majority of patients inc luded in this study were classified as having a hypoactive delir ium (N = 30, 59%), while 5 (9%) had hyperact ive del i r ium, and 17 (33%) had a mixed del i r ium with bo th hyperact ive and hypoac t ive fea tures . Twenty- th ree pa t ien ts (45%) were rated (using clinician's global rat- ings) as having a mild del ir ium, 16 (31%) were rated as having a modera te delirium, and 12 (24%) were r a t e d as hav ing a severe delirium. Median Karnofsky Per fo rmance Sta- tus score was 30, i nd ica t ing a s ignif icant d e g r e e of physical disability. Total MDAS scores averaged 15.1 across the sample, with a range f rom 2 to 27. For the subset of patients (N = 23) rated by clinicians as having "mi ld" delirium, average MDAS scores were 8.43 (SD = 3.22; range, 3-16). Patients rated as having " m o d e r a t e " delir ium ( N = 16) obta ined aver- age MDAS scores of 19.67 (SD = 2.38; range, 15-25) and patients rated as having "severe" del i r ium (N = 12) ob ta ined average MDAS scores of 23.70 (SD = 3.13; range, 18-27).
Scores on the MDAS were significantly cor- related with all three alternative measures of delir ium (DRS r = 0.88, P < 0.0001; MMSE r = -0 .91 , P < 0.0001; clinician's global rating of delir ium severity r = 0.89, P < 0.0001). With the exception of items rating perceptual dis- tu rbance (i tem 7) and delusions ( i tem 8), individual MDAS items were highly correlated with total scores on these three alternative measures of delir ium (DRS r range f rom 0.60 to 0.78; MMSE r r ange f rom - 0 . 6 0 to -0 .86, clinician ratings r f rom 0.64 to 0.84). The cor- relations between individual MDAS items and the three alternative measures Of delir ium are repor ted in Table 3.
Similar results were found when patients were s t rat i f ied by type o f de l i r ium. Total

Vol. 13 No. 3 March 1997 Memorial Delirium Assessment Scale 133
Table 3 Correlations with Alternative Measures o f Delirium
Global MDAS item DRS MMSE rating a
Total score 0.88 -0 .91 0.89 1 0.72 -0 .83 0.82 2 0.68 -0.81 0.84 3 0.71 -0 .82 0.76 4 0.60 -0 .86 0.74 5 0.72 -0 .82 0.82 6 0.78 -0 .74 0.74 7 0.54 -0 .20 0.23 8 0.50 -0 .22 0.27 9 0.61 -0.61 0.64 10 0.71 -0.71 0.74
MDAS, Memorial Delirium Assessment Scale; DRS, Delirium Rating Scale; MMSE, Mini-Mental State Exam.
Based on Spearman correlation coefficients for ordinal data.
MDAS score was highly corre la ted with scores on the three alternative measures of delir ium (DRS, MMSE, and clinician's global ratings) tor patients with a hyperactive delir ium (r = 0.91, -0 .99 , and 0.97, respectively), a hypoac- tive de l i r ium (r = 0.82, - 0 . 9 0 , and 0.87, respectively), and mixed delir ium (r = 0.89, -0 .83 , and 0.91, respectively). The pa t te rn of correlations between individual MDAS items was also similar for patients with hyperactive, hypoactive, and mixed delirium.
An analysis of covariance predict ing clini- d a n ' s global ratings of delir ium severity dem- onstrated that MDAS scores significantly pre- dicted clinician's global ratings of del i r ium severity [F(1,44) = 163.48, P < 0.0001, R e = 0.79], however, there was no incrementa l ben- efit f rom adding DRS a n d / o r MMSE scores to this predict ion model . MDAS scores, on the o ther hand, remained statistically significant in the predict ion of clinicians' global ratings even after control l ing for DRS and MMSE scores.
Using a classification cut-off score of 13 based on the results of study 1, the MDAS cor- rectly classified all of the patients with "mod- era te" and "severe" delir ium according to cli- nician's global ratings of delir ium severity (N= 16 and N= 12, respectively). All bu t one of the 23 patients with "m i l d" del ir ium, however, were incorrect ly classified using this cut-off score. Nevertheless, n ine of the 23 patients with a "mi ld" delir ium (39%) obta ined MSAS scores of 10 or more, and 13 obta ined scores of 8 or more (56%).
Discussion
These studies suppor t the use of the MDAS as a measure of delir ium severity among medi- cally ill patients. Prel iminary analyses demon- strate high reliability, and validity as a measure of delir ium severity. The ten-item MDAS has a high degree of internal consistency, and was rated with high levels of inter-rater reliability between two independen t psychiatrist raters. In addition, the MDAS demonst ra ted a high degree of concur ren t validity with o ther mea- sures of delir ium and delir ium severity.
T h e des ign of the MDAS offers several advantages over existing measures of delir ium for clinical research purposes. Unlike existing measu re s o f de l i r ium, the MDAS pe rmi t s repeated administrat ion within a 24-hr per iod and does no t require the incorpora t ion of o the r clinical measu re s (for example , the MMSE) to rate cognitive functioning (as rec- o m m e n d e d in the DRS). We did not, however, specifically validate this measure for repeated use and fur ther research is necessary to sup- por t this use of the MDAS. Our analyses sug- gest, however, that the MDAS is a bet ter mea- sure of delir ium severity than either the DRS or the MMSE. In a multiple regression model predict ing clinician's global ratings of severity, the MDAS proved to be the strongest predic- tor of clinician's ratings, with no addit ional benefi t gained f rom the addition of ei ther the DRS or the MMSE. Conversely, the MDAS sig- nificantly improved the predict ion of clini- cian's ratings of delir ium severity beyond that achieved with the DRS and MMSE. Thus, the MDAS is particularly well suited tbr use in de l i r ium t r e a t m e n t research , where rapid , repea ted assessments of delir ium severity may be desirable in order to assess the efficacy of a clinical in te rven t ion or study the p h e n o m - enology of delir ium in a particular setting.
Although the scale was developed as a mea- sure for assessing severity of delirium symp- toms, ra ther than as a diagnostic tool, these data suggest that the MDAS may also be a use- ful tool for establishing a diagnosis of delir ium in medically ill patients. The MDAS signifi- cantly d i f fe ren t ia ted be tween pat ients with delir ium and patients with other cognitive dis- orders or non-cognitive psychiatric disorders. The MDAS also accurately classified patients with " m o d e r a t e " and "severe" delirium, how-

134 Breitbart et al. Vol. 13 No. 3 March 1997
ever patients with "mi ld" delir ium were not accurately classified using the cut-off score of 13 developed in study 1. This finding may be partly due to our reliance on a small sample of patients in de te rmin ing the opt imal cut-off score for a diagnosis of delirium. It is also pos- sible that, because t rea tment for delirium was often initiated before MDAS ratings, MDAS rat ings o b t a i n e d unde res t ima te the cut-off score tha t would be most a p p r o p r i a t e for screening purposes in untreated patients. Fur- ther research with larger, more diverse non- delirious pa t ien t popula t ions (for example , patients diagnosed with psychotic disorders) may be h e l p fu l in d e t e r m i n i n g the m o s t appropr ia te cut-off score for making determi- nations of whether or not an individual meets diagnostic criteria for delirium. Similarly, the above-noted clinical in tervent ions that pre- c e d e d MDAS d a t a c o l l e c t i o n m a y have resulted in the classification of some patients as having a "mi ld" delirium, who in fact had only minimal residual symptoms of delir ium at the t ime of assessment and may have no longer m e t diagnostic criteria for delirium. Hence , addi t ional research is necessary to clarify whether or not the MDAS is valid as a diagnostic tool, and, if so, to de te rmine the most appropr ia te cut-off score for diagnostic purposes. Until such fur ther validation occurs, however, the MDAS should be utilized in con- junct ion with an established m e t hod for diag- nosing the presence of delirium (for example, DSM IV, CAM).
These validation studies have several limita- tions that must be noted. Foremost a m o n g these is the relatively modest sample size used in these analyses. Because of our setting in a cancer hospital, we had difficulty obtaining large samples of patients with non-delirious cognitive disorders (for example, dement ia) or severe non-cognitive psychiatric disorders (for example , schizophrenia) . Similarly, our analysis of differences within type of delir ium (hypoactive, hyperactive, or mixed) were lim- ited by the small samples available within each g roup (only five patients were classified as hyperactive). Thus, al though the MDAS elicits informat ion regarding the type of delirium, and fur ther research with larger sample sizes and m o r e sophis t ica ted statistical m e t h o d s (that is, factor analysis) may help clarify differ- ences across d i f ferent subtypes of delirious
patients, we were unable to do such analyses with our sample. Fur ther research may also help to develop a more formal classification system for categorizing patients into delirium subtypes based on MDAS item profiles.
We also conducted this research in a clinical context, and therefore the clinical management of patients with delirium took precedence over our research agenda. As a result, many patients had received some degree of t r ea tmen t for delirium prior to our assessments (although a substantial n u m b e r of patients had "severe" delirium nonetheless). It is therefore conceiv- able that treatment may have influenced the pat- tern of MDAS ratings we obtained. For example, if clinical interventions are particularly effective in resolving hallucinations a n d / o r delusions, these symptoms might be observed less fre- quently and appear to be less valid as predictors of delirium severity. In fact, our data indicated that two of the ten MDAS items (items 7 and 8, measuring hallucinations and delusions, respec- tively) were less highly correlated with both over- all MDAS scores and scores on alternative mea- sures of delirium. While this may be the result of treatment (as noted above), it may also reflect the multifactorial phenomenology of delirium, where hallucinations and delusions are more fre- quent in hyperactive delirium, 17 a group that was under- represented in:-.our sample. Thus, i tems 7 and 8 had t imi[ed variance in our sample, and therefore genera ted lower item- total correlations, lower inter-rater reliability coefficients, and lower correlations with other measures of cognitive impairment. Nevertheless, because these items measure important aspects of delirium (hallucinations and delusions), and the obtained correlations and reliability coeffi- cients were still satisfactory (item-total correla- tions were above 0.3 and reliability coefficients above 0.6), we chose to retain the items because of the clinical and diagnostic importance of such symptoms when they do occur. In addition, the item measuring psychomotor activity (item 9) also generated a somewhat lower, but still saris- factory, inter-rater reliability coefficient than the other items. Despite this modest level of inter- rater agreement in ratings, this i tem did not appear to have an adverse impact on the overall scale reliability, and was significantly correlated with other measures of delirium in the validation study.

Vol. 13 No. 3 March 1997 Memorial Delirium Assessment Scale 135
Despite the above limitations, these results suppor t the use of the MDAS as a clinical research tool that alleviates many problems associated with existing measures of delirium severity. This measure can be reliably scored and generates a useful index of symptom severity for assessing the efficacy of treatments for delirium, the severity of cognitive side effects from other interventions, or for study- ing tile phenomenology of delirium in various populations. Because of our limited support to t the use of the MDAS as a delirium diagnos- tic tool, it should be used along with other methods to establish a diagnosis of delirium. Further research with this instrument is neces- sary to clarify the strengths and weaknesses of the MDAS in different clinical and research settings (for example, palliative care facilities, nursing homes, and postoperative settings).
Acknowledgment Dr. William Breitbart's work on this project
was supported by the Faculty Scholars Pro- gram, O p e n Society Inst i tute , Pro jec t on Death in America, and hy the Emily Davie and Joseph S. Kornfeld Foundation. We are grate- ful to the many patients and their families who participated in this research and to the clinical staff of the Memorial Sloan-Kettering Cancer C e n t e r D e p a r t m e n t o f P s y c h i a t r y , a n d Monique Kaim, PhD, in particular, for assist- ing in the completion of this project.
References 1. Breitbart W, Steifel F, Kornblith AB, Pannullo S.
Nenropsychiatric disturbance in cancer patients with epidural spinal cord compression receiving high dose corticosteroids: a prospective comparison study. Psycho-oncology 1993;2:233-245
2. Lipowski zJ. Delirium (acute confusional states). JAMA 1987;258:1789-1792.
3. Smith MJ, Breitbart WM, Platt MM. A critique of instruments and methods to detect, diagnose, and rate delirium.J Pain Symptom Manage 1994;10:35-77.
4. Trzepacz PT, Maue FR, Coffman G, van Thiel DH. Neuropsychiatric assessment of liver transplanta- tion candidates: delirium and other psychiatric disor- ders. IntJ Psychiatry Med 1986-1987;16:101-111.
5. Tune LE. Post-operative delirium. Int Psychoge- riatr 1991;3:325-332.
6. Massie MJ, Holland J, Glass E. Delirium in ter- minally ill cancer patients. Am J Psychiatry 1983; 140:1048-1050.
7. Trzepacz PT, Baker RW, Greenhouse J. A symp- tom rating scale for delirium. Psychiatry Res 1988; 23:89-97.
8. Inouye SK, van Dyck CH, Alessi CA, Balkin S, Siegal AP, Horwitz RI. Clarifying confusion: the confusion assessment method. Ann Intern Med 1990; 113:941-948.
9. Albert MS, Levkoff S, Reilly C, et al. The delirium symptom interview: an interview for the detection of delirium symptoms in hospitalized patients. J Geriatr Psychiatry Neurol 1992;5:14-21.
10. Miller PS, Richardson JS, Jyu CA. Association of low serum anticholinergic levels and cognitive impairment in elderly presurgical patients. Am J Psychiatry 1988;145:342-345.
11. Breitbart W, Marotta R, Platt MM, et al. A double-blind trial of haloperidol, chlorpromazine, and lorazapam in the treatment of delirium in hos- pitalized AIDS patients. Am J Psychiatry 1996;153: 231-237.
12. Meagher DJ, O'Hanlon D, O'Mahoney E, Casey PR. The use of environmental strategies and psy- chotropic medications in the management of delirium. BrJ Psychiatry 1996;168:512-515.
13. van der Mast RC, van der Broek WW, Roest FHJ. Clinical course and outcome of delirium after cardiac surgery. Unpublished doctoral dis- sertation. Rotterdam, Netherlands: Erasmus Uni- versity, 1994.
14. Diagnostic and statistical manual of mental dis- orders, 3rd ed, revised. Washington, DC: American Psychiatric Association Press, 1987.
15. Tucker GJ and the DSM-IV Organic Disorders Work Group DSM-1V. Proposals for revision of diag- nostic criteria for delirium. Int Geriatr 1991;3:197- 208.
16. Shrout PE, Fleiss JL. Interclass correlations: uses in assessing rater reliability. Psychol Bull 1979; 86:420-428.
17. Folstein MF, Folstein SE, McHugh PR. "Mini Mental State:" a practical method of grading tile cognitive state of patients for the clinician. J Psychi- atr Res 1975;12:189-198.
18. Liptzin B, Levkoff SE. An empirical study of delirium subtypes. BrJ Psychiatry 1992;161:843-84.

136 Breitbart et al. Vol. 13 No. 3 March 1997
Appendix 1 Memoria l Del ir ium A s s e s s m e n t Scale (MDAS) ©1996
INSTRUCTIONS: Rate the severity of the following symptoms of delirium based on current interaction with subject or assessment of h i s /her behavior or experience over past several hours (as indicated in each time.)
ITEM I-REDUCED LEVEL OF CONSCIOUSNESS (AWARENESS): Rate the patient's current awareness of and interaction with the environment (interviewer, other people/objects in tile room; for example, ask patients to describe their surroundings).
[ ] 0: none (patient spontaneously fully aware of environment and interacts appropriately) [ ] 1: mild (patient is unaware of some elements in the environment, or not spontaneously interacting
appropriately with the interviewer; becomes fully aware and appropriately interactive when prodded strongly; inteiMew is prolonged but not seriously disrupted)
[ ] 2: moderate (patient is unaware of some or all elements in the environment, or not spontaneously interacting with the interviewer; becomes incompletely aware and inappropriately interactive when prodded strongly; interview is prolonged but not seriously disrupted)
[ ] 3: severe (patient is unaware of all elements in the environment with no spontaneous interaction or awareness of the interviewer, so that the interview is difficult-to-impossible, even with maximal prodding
ITEM 2-DISORIENTATION: Rate current state by asking the following 10 orientation items: date, month, day, year, season, floor, name of hospital, city state, and country.
[ ] 0: none (patient knows 9-10 items) [ ] 1: mild (patient knows 7-8 items) [ ] 2: moderate (patient knows 5-6 items) [ ] 3: severe (patient knows no more than 4 items)
ITEM 3-SHORT-TERM MEMORY IMPAIRMENT: Rate current state by using repetition and delayed recall of 3 words [patient must immediately repeat and recall words 5 min later after an intervening task. Use alternate sets of 3 words for successive evaluations (for example, apple, table, tomorrow; sky, cigar, justice)].
[ ] 0: none (all 3 words repeated and recalled) [ ] 1: mild (all 3 repeated, patient fails to recall 1) [ ] 2: moderate (all 3 repeated, patient fails to recall 23) [ ] 3: severe (patient fails to repeat 1 or more words)
ITEM 4--IMPAIRED DIGIT SPAN: Rate current performance by asking subjects to repeat first 3, 4, then 5 digits forward and then 3, then 4 backwards; continue to the next step only if patient succeeds at the previous one.
[ ] 0: none (patient can do at least 5 numbers forward and 4 backward) [ ] 1: mild (patient can do at least 5 numbers forward, 3 backward) [ ] 2: moderate (patient can do 4-5 numbers forward, cannot do 3 backward) [ ] 3: severe (patient can do no more than 3 numbers forward)
ITEM 5-REDUCED ABILITY TO MAINTAIN AND SHIFT ATTENTION: As indicated during the interview by questions needing to be rephrased a n d / o r repeated because patient's attention wanders, patient loses track, patient is distracted by outside stimuli or over-absorbed in a task.
[ ] 0: none (none of the above; patient maintains and shifts attention normally) [ ] 1: mild (above attentional problems occur once or twice without prolonging the interview) [ ] 2: moderate (above attentional problems occur often, prolonging the interview without seriously disrupting it) [ ] 3: severe (above attentional problems occur constantly, disrupting and making the interview
difficult-to-impossible)
ITEM 6-DISORGANIZED THINKING: As indicated during the interview by rambling, irrelevant, or incoherent speech, or by tangential, circumstantial, or faulty reasoning. Ask patient a somewhat complex question (for example, "Describe your current medical condition.").
[ ] 0: none (patient's speech is coherent and goal-directed) [ ] 1: mild (patient's speech is slightly difficult to follow; responses to questions are slightly off target but not
so much as to prolong the interview) [ ] 2: moderate (disorganized thoughts or speech are clearly present, such that interview is prolonged but not
disrupted) [ ] 3: severe (examination is very difficult or impossible due to disorganized thinking or speech)
Vol. 13 No. 3 March 1997 Memorial Delirium Assessment Scale 137
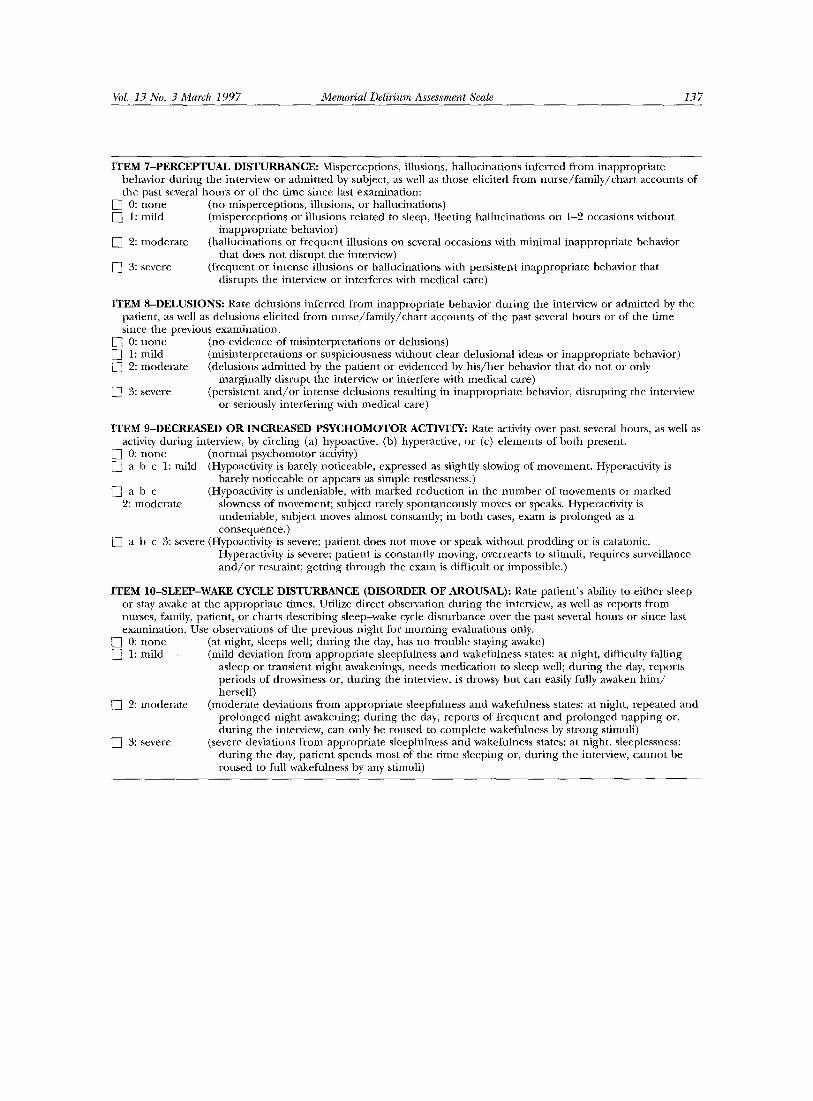
ITEM 7-PERCEPTUAL DISTURBANCE: Misperceptions, illusions, hallucinations inferred from inappropriate behavior during the interview or admitted by subject, as well as those elicited from nurse/family/chart accounts of the past several hours or of the time since last examination:
[ ] 0: none (no misperceptions, illusions, or hallucinations) [ ] 1: mild (misperceptions or illusions related to sleep, fleeting hallucinations on 1-2 occasions without
inappropriate behavior) [ ] 9: moderate (hallucinations or frequent illusions on several occasions with minimal inappropriate behavior
that does not disrupt the interview) [ ] 3: severe (frequent or intense illusions or hallucinations with persistent inappropriate behavior that
disrupts the interview or interferes with medical care)
ITEM 8-DELUSIONS: Rate delusions inferred from inappropriate behavior during the interview or admitted by the patient, as well as delusions elicited from nurse/family/chart accounts of the past several hours or of the time since the previous examination.
[ ] 0: none (no evidence of misinterpretations or delusions) [ ] 1: mild (misinterpretations or suspiciousness without clear delusional ideas or inappropriate behavior [ ] 2: moderate (delusions admitted by the patient or evidenced by h is /her behavior that do not or only
marginally disrupt the interview or interfere with medical care) [ ] 3: severe (persistent a n d / o r intense delusions resulting in inappropriate behavior, disrupting the interview
or seriously interfering with medical care)
ITEM 9-DECREASED OR INCREASED PSYCHOMOTOR ACTIVITY: Rate activity over past several hours, as well as activity during interview, by circling (a) hypoactive, (b) hyperactive, or (c) elements of both present.
[ ] 0: none (normal psychomotor activity) [ ] a b c 1: mild (Hypoactivity is barely noticeable, expressed as slightiy slowing of movement. Hyperactivity is
barely noticeable or appears as simple restlessness.) [ ] a b c (Hypoactivity is undeniable, with marked reduction in the number of movements or marked
2: moderate slowness of movement; subject rarely spontaneously moves or speaks. Hyperactivity is undeniable, subject moves almost constantly; in both cases, exam is prolonged as a consequence.)
[ ] a b c 3: severe (Hypoactivity is severe; patient does not move or speak without prodding or is catatonic. Hyperactivity is severe; patient is constantly moving, overreacts to stimuli, requires surveillance a n d / o r restraint; getting through the exam is difficult or impossible.)
ITEM 10-SLEEP-WAKE CYCLE DISTURBANCE (DISORDER OF AROUSAL): Rate patient's ability to either sleep or stay awake at the appropriate times. Utilize direct observation during the interview, as well as reports from nurses, family, patient, or charts describing sleep-wake cycle disturbance over the past several hours or since last examination. Use observations of the previous night for morning evaluations only.
[ ] 0: none (at night, sleeps well; during the day, has no trouble staying awake) [ ] 1: mild (mild deviation from appropriate sleepfulness and wakefulness states: at night, difficulty falling
asleep or transient night awakenings, needs medication to sleep well; during the day, reports periods of drowsiness or, during the interview, is drowsy but can easily fully awaken h i m / herself)
[ ] 2: moderate (moderate deviations from appropriate sleepfulness and wakefulness states: at night, repeated and prolonged night awakening; during the day, reports of frequent and prolonged napping or, during the interview, can only be roused to complete wakefulness by strong stimuli)
[ ] 3: severe (severe deviations from appropriate sleepfulness and wakefulness states: at night, sleeplessness; during the day, patient spends most of the time sleeping or, during the interview, cannot be roused to full wakefulness by any stimuli)





























