Embed Size (px)
Citation preview
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:31 User ID: muralir 1BlackLining Disabled
C H A P T E R
16
The Child With AlteredRespiratory Status
Do you remember the Diaz fam-ily from Chapter 9, in whichJose has trouble taking his asthma medication,and in Chapter 4, in which Jose’s little sister,Lela, expresses her personality even as a new-born? Jose is 4 years old and was diagnosedwith asthma this past fall, about 6 months ago.Since that time Claudia, his mother, hasnoticed several factors that trigger his asthmaincluding getting sick, pollen, and cold air.
One evening following a warm early-springday, Jose is outside playing as the sun sets andthe air cools. When he comes inside hebegins to cough. Claudia sets up his nebulizerand gives him a treatment of albuterol, whichlessens his coughing. Within an hour, Jose iscoughing constantly again and wheezing. Af-ter one hard coughing fit, Jose has a hard timecatching his breath; he looks pale and ashen,and his wheezing is very pronounced. Clau-dia tells her husband, Ignacio, that she thinksthey should go to the emergency room. They
leave Lela, the baby sister,with Claudia’s mother, Selma,
and head to the hospital.At the hospital the emergency department
nurse observes Jose sitting cross-legged andleaning forward on his hands. His mouth isopen and he is breathing hard with an easilyaudible inspiratory wheeze. He is using hissubclavicular accessory muscles with eachbreath. His respiratory rate is 32 breaths perminute, his pulse is 112 beats per minutes,and he is afebrile. Claudia explains that hewas fine; he was outside running and playing,and then came in and began coughing andwheezing, and she gave him an albuteroltreatment. The nurse places a pulse oximeterprobe on his finger, which takes a few minutesto establish reliability but settles down, vacillat-ing between 89% to 90%. After reporting herassessment and receiving orders, the nurseadjusts the oxygen flow to 30% and places asimple oxygen face mask on Jose.
Case History
651

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:31 User ID: muralir 1BlackLining Disabled
C H A P T E R O B J E C T I V E S
1. Describe the developmental and biologic variances inchildren’s respiratory systems that predispose them torespiratory problems.
2. Describe the common alterations in health patterns withinthe respiratory system in children in terms of etiology,pathophysiology, clinical manifestations, andinterdisciplinary interventions.
3. Describe the nursing assessment of the child withcompromised respiratory function.
4. Discuss the nursing care responsibilities associated withdiagnosis of respiratory difficulties in children.
5. Select the treatments that are most effective for specificrespiratory conditions.
6. Select nursing care interventions to support the child withan acute or chronic respiratory illness.
See for a list of Key Terms.
Respiratory conditions, both acute and chronic, are theleading causes of morbidity in children. Compromises tothe respiratory system are the most common types ofproblem encountered by the nurse caring for infants,children, and youth. Respiratory conditions during child-hood can be acute or chronic, life threatening, and canpresent as either the primary clinical problem or a sec-ondary complication (also called a comorbid condition). Re-spiratory infectious conditions, such as influenza, arewidely recognized as major causes of respiratory mortal-ity and morbidity for young healthy children.
Growth and maturation of the respiratory system dur-ing childhood is characterized by changes in its physio-logic and anatomic features. The physiologic processesof respiratory control and gas exchange in children,although immature, are determined by respiratory mech-anisms similar to those of adults. However, anatomicstructural variations in the respiratory tracts of infantsand young children from those of adults result in substan-tial differences in the manifestations of respiratory distur-bances. A key aspect of providing respiratory care inpediatric patients is recognizing these similarities and dif-ferences. Note these variations when identifying normalversus abnormal symptoms.
Assessment of the respiratory system is critical in pedi-atric care. Key functions of the nurse in the acute or am-bulatory healthcare settings involve identifying changesin respiratory status and quickly instituting correctivemeasures if needed. In respiratory care, developing andrefining assessment skills is essential to providing age-appropriate care for children. Therefore, the skillednurse must have an excellent working knowledge and akeen understanding of the clinical importance of theseunique anatomic and physiologic features of children’srespiratory systems. Because respiratory system infectionsare relatively common in children and are a leading etiol-ogy in respiratory morbidity, understanding how infec-tions can affect the respiratory system is important.
Knowledge of both acute and chronic respiratory condi-tions helps the nurse provide appropriate care through-out the child’s life span.
Developmental and Biologic
Variances
Question: How is it possible the Jose could ‘‘out-grow’’ his asthma as he gets older?
The child’s respiratory system differs in many ways fromthat of the mature adult. The child is physically smallerand functionally immature; thus, the pediatric respiratorysystem has much less reserve capacity. Children are morevulnerable to respiratory illnesses and complications thanadults. Infants and children develop respiratory distress(impaired respiratory function) and respiratory failure(respiratory impairment in which the arterial oxygen ten-sion falls below 60 mm Hg, carbon dioxide tension risesto more than 50 mm Hg, and the arterial pH drops to lessthan 7.35) much more readily. Unique differences in thesize, structure, and function of the respiratory system inchildren are shown in Figure 16–1.
This section summarizes variances in major structuresand provides suggestions regarding ways to modifyassessment skills and intervention techniques to provideoptimal care to the child with altered respiratory status.
Central Nervous System ControlRespiratory rate and depth are controlled by central andperipheral chemoreceptors located in the circulatory sys-tem. Although these receptors are present at birth, fewerexist in the infant and young child than in the matureadult. Term infants and young children respond to hy-poxemia (inadequate oxygen in the blood) and hyper-carbia (excessive carbon dioxide in the blood) as an adultdoes, by increasing the rate and depth of respiration tonormalize blood gas concentrations of oxygen and carbondioxide. The premature infant, however, may respond tolow blood oxygen levels initially with an increased rate ofrespiration, followed by a slowing respiratory rate, apnea,or both. Conditions such as bronchopulmonary dysplasia(BPD), pneumonia, and bronchiolitis put prematureinfants at especially high risk for developing hypoxia andapnea, so nursing care must focus on careful monitoringof blood gases.
AirwaysThe pediatric airway is much smaller in diameter andshorter in length than the adult airway. During child-hood, the airways continue to grow in both diameterand length. For example, in newborns the trachea is4 cm long, and in 18-month-old infants it is 7 cm long.In adults, it is 12 cm long. Airway inflammation or asmall amount of mucus can produce a critical decrease
652 Unit 3 n n Managing Health Challenges
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:31 User ID: muralir 1BlackLining Disabled
in the airway diameter and increases the resistance toairflow dramatically, leading to substantial respiratorydistress or even failure (Fig. 16–2). The pediatric tongueis larger in proportion to other structures than the adulttongue, and therefore causes airway obstruction morereadily.
The pediatric larynx is funnel shaped because of a nar-rowing at the cricoid cartilage, with the narrowest por-tion at the level of the cricoid ring (Fig. 16–3).
caREmindercaREminderThe child younger than age 8 who requires intubationusually does not need a cuffed endotracheal tube. The child’snarrow cricoid provides a ‘‘natural physiologic cuff’’ aroundthe uncuffed or straight tube.
The cartilage surrounding the entire larynx is quite softand can be compressed easily, subsequently causing airwayocclusion when the neck is flexed or hyperextended. Main-taining an optimal neck position (sometimes called thesniffing position) by placing a towel under the occipital areaof the head is an important nursing consideration for thepediatric patient. The right mainstem bronchus, a com-mon location for aspirated foreign bodies, arises from thetrachea at a wide angle in children (versus the muchsharper angle of the left mainstem bronchus).
Chest Wall and Respiratory MusclesThe cartilaginous chest wall is twice as compliant andflexible as the bony chest wall of the adult. Thus, with re-spiratory difficulty, children may display chest retrac-tions, a visible clinical phenomenon in which the bones
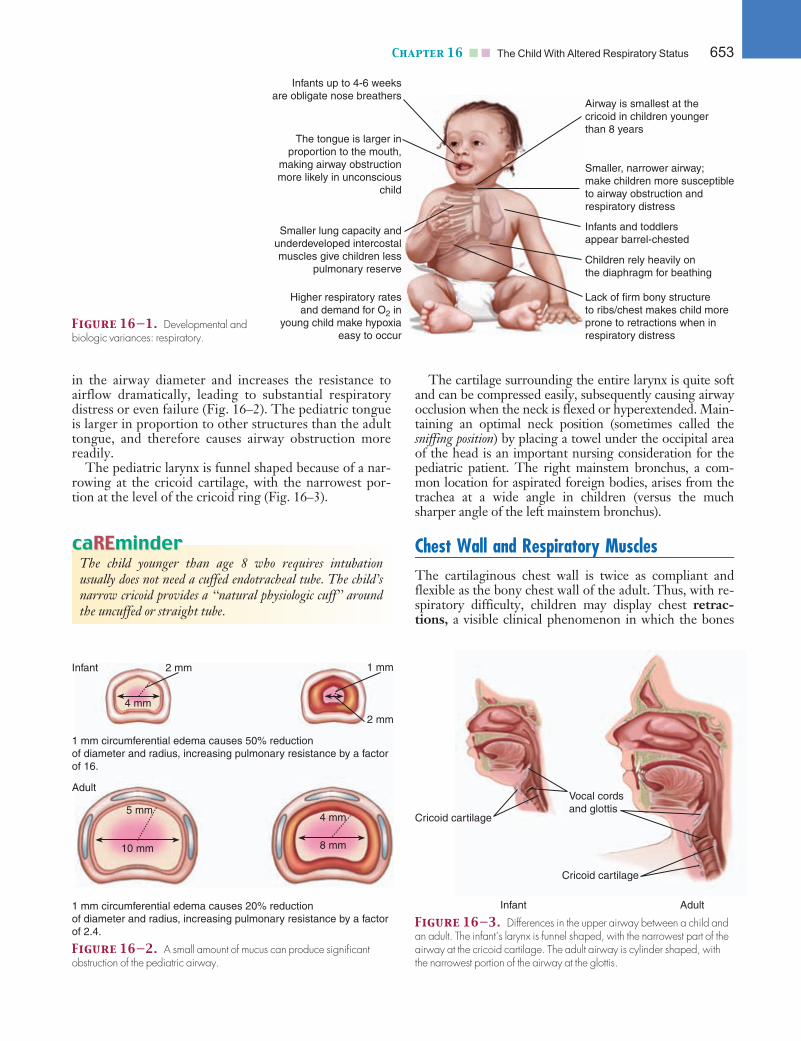
Figure 16—1. Developmental andbiologic variances: respiratory.
Infants up to 4-6 weeksare obligate nose breathers
The tongue is larger inproportion to the mouth,
making airway obstructionmore likely in unconscious
child
Smaller lung capacity andunderdeveloped intercostalmuscles give children less
pulmonary reserve
Higher respiratory ratesand demand for O2 in
young child make hypoxiaeasy to occur
Airway is smallest at thecricoid in children youngerthan 8 years
Smaller, narrower airway;make children more susceptibleto airway obstruction andrespiratory distress
Children rely heavily onthe diaphragm for beathing
Lack of firm bony structureto ribs/chest makes child moreprone to retractions when inrespiratory distress
Infants and toddlersappear barrel-chested
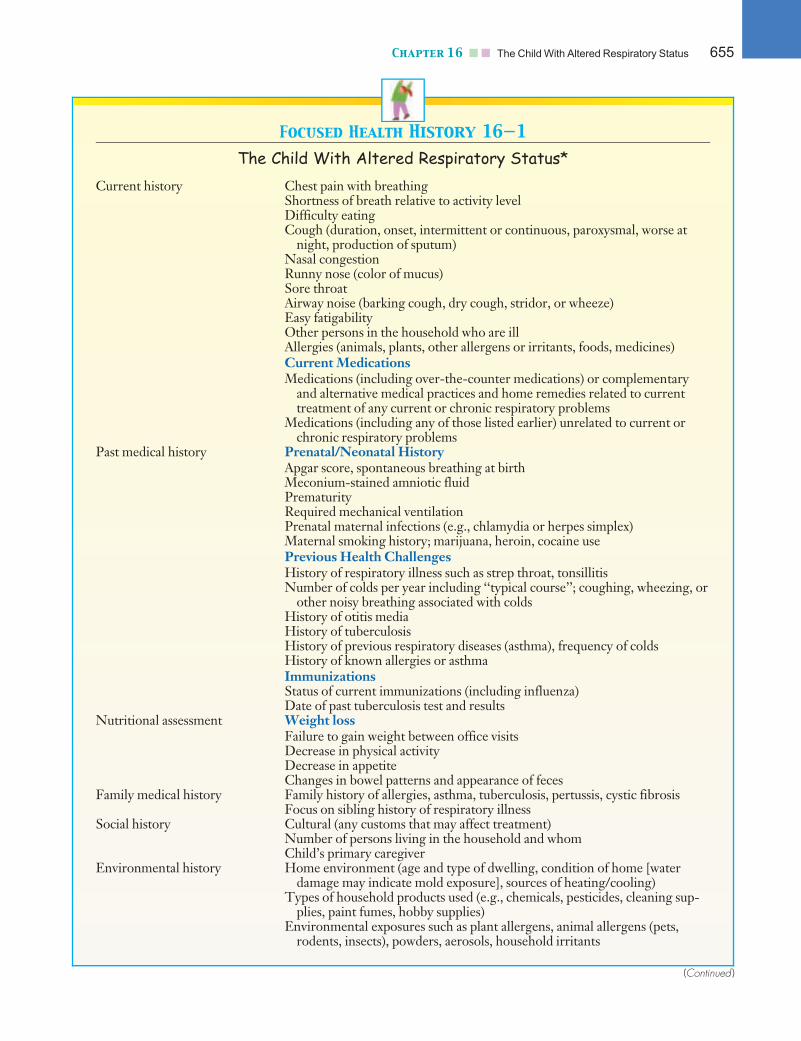
1 mm circumferential edema causes 50% reductionof diameter and radius, increasing pulmonary resistance by a factorof 16.
1 mm circumferential edema causes 20% reductionof diameter and radius, increasing pulmonary resistance by a factorof 2.4.
Adult
Infant
4 mm
2 mm
2 mm
1 mm
5 mm
10 mm
4 mm
8 mm
Figure 16—2. A small amount of mucus can produce significantobstruction of the pediatric airway.
Cricoid cartilage
Cricoid cartilage
Vocal cordsand glottis
AdultInfant
Figure 16—3. Differences in the upper airway between a child andan adult. The infant’s larynx is funnel shaped, with the narrowest part of theairway at the cricoid cartilage. The adult airway is cylinder shaped, withthe narrowest portion of the airway at the glottis.
Chapter 16 n n The Child With Altered Respiratory Status 653

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:31 User ID: muralir 1BlackLining Disabled
and cartilage structures of the chest become more promi-nent with inspirations (see Fig. 8–8). Chest retractionsincrease the work of breathing and reduce the efficiencyof ventilation.
The shape of the chest and the angle of rib articulationrelative to the sternum and vertebrae are other anatomicvariations of the chest wall that adversely affect the me-chanical efficiency of breathing in the infant and youngchild. Until the child reaches 7 or 8 years of age, the ribsare horizontal in orientation, in contrast to the 45-degreeangle present in the older child and adult. This orienta-tion accounts for the barrel-shaped appearance of thechest in the infant and young child. Because of this hori-zontal orientation of the ribs, the intercostal muscles donot have the leverage necessary to lift the ribs and aid inchest expansion during respiration. Young infants andchildren with diagnoses such as pneumonia must beassessed carefully and frequently for the development ofrespiratory fatigue and subsequent respiratory failure asa result of these variations.
The muscles important for efficient and effective respi-rations include the diaphragm, the intercostal muscles,and the muscles supporting the head and the upper andlower airways. These muscles are relatively underdevel-oped in pediatric patients. They lack the tone, strength,and coordination necessary to prevent and effectivelymanage episodes of respiratory distress.
The diaphragm, which is the main muscle of respira-tion in patients of all ages, is located higher in the thoraxin infants and young children and is inserted horizontally,versus obliquely, as in adults. Any condition that impedesdiaphragmatic movement, such as abdominal distentioncaused by accumulation of air or fluid, can substantiallycompromise respiratory status. In addition, the intercos-tal muscles are underdeveloped and function only to sta-bilize, rather than actually lift, the chest wall. Because ofthese important variations in the respiratory muscles,children with neuromuscular weakness or paralysis sec-ondary to disorders such as muscular dystrophy orWerdnig-Hoffmann syndrome may exhibit respiratorycompromise or distress as one of the first presentingsymptoms of their disease.
Lung TissueThe ability of lung tissue to inflate and deflate graduallyincreases throughout childhood, as the tissue grows andmatures. Many factors affect lung tissue in individuals ofall age groups. For example, the presence or absence ofsurfactant (a material secreted by the alveoli), and thenumber and character of elastic fibers in the lung tissuecan affect the ability of the lung tissue to expand anddeflate. Infants born prematurely lack surfactant, whichdevelops relatively late during intrauterine developmentand contributes to the stability of the alveolar surfaces.Without surfactant, the lung tissue’s ability to inflate anddeflate is greatly decreased, and lack of surfactant leads tosevere respiratory distress and even death.
Children also have less elastic tissue in the alveoli thanadults. This variation tends to cause the alveoli to lose
patency, leading to higher incidences of pulmonaryedema, pneumomediastinum, and pneumothorax. Mini-mal elastic recoil properties cause a higher incidence ofatelectasis (partial or complete pulmonary collapse) inpediatric patients than in adults. In addition, poorlydeveloped pathways of collateral ventilation can lead torapid small airway obstruction and significant respiratorydistress. Because of all these variations, neonates areespecially susceptible to the development of pulmonaryedema.
Answer: As Jose gets older, larger, and stronger,his symptoms may decline. He may continue to have
some reactive airway disease, but his larger airways, stron-ger musculature, and more mature lung tissue will result in lessdramatic symptoms.
Assessment of the Child With
Altered Respiratory Status
Collecting the health history and performing the physicalassessment of the child with a respiratory system disturb-ance is the first step in the nursing process. During thehistory, the child and family have an opportunity to telltheir story about the illness and what prompted them toseek care from the healthcare team. Make the assessmenta more positive experience by allaying the child’s fearsand discomfort, and establishing a relationship of trustand communication with the child and parents.
Focused Health History
Question: Review Focused Health History 16–1.Analyze the information in the case study and identify
the information regarding the Diaz family that is missing. Inte-grate the information you have about the Diaz family. Whatare some unique characteristics of the Diaz family that youwill incorporate into your collection of a health history?
When taking a history, begin with the reason for the visitor hospitalization. When possible, use the child’s orparents’ own words to document all descriptions of thechild’s symptoms (Focused Health History 16–1). Whentaking a history of a respiratory system problem, followgeneral history-taking guidelines (see Chapter 8), but alsoinclude questions about the environment—things thatmake the symptoms worse (sometimes called triggers)—and potential comorbid conditions or symptoms. As withgeneral history taking, remember that clear and detailedinformation about the current illness as well as other fac-tors (environment, family, and so forth) helps you to for-mulate an initial plan of care and directs furtherquestioning to confirm or refute any hypothesis regard-ing diagnosis.
654 Unit 3 n n Managing Health Challenges
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:31 User ID: muralir 1BlackLining Disabled
Focused Health History 16—1
The Child With Altered Respiratory Status*
Current history Chest pain with breathingShortness of breath relative to activity levelDifficulty eatingCough (duration, onset, intermittent or continuous, paroxysmal, worse at
night, production of sputum)Nasal congestionRunny nose (color of mucus)Sore throatAirway noise (barking cough, dry cough, stridor, or wheeze)Easy fatigabilityOther persons in the household who are illAllergies (animals, plants, other allergens or irritants, foods, medicines)Current MedicationsMedications (including over-the-counter medications) or complementary
and alternative medical practices and home remedies related to currenttreatment of any current or chronic respiratory problems
Medications (including any of those listed earlier) unrelated to current orchronic respiratory problems
Past medical history Prenatal/Neonatal HistoryApgar score, spontaneous breathing at birthMeconium-stained amniotic fluidPrematurityRequired mechanical ventilationPrenatal maternal infections (e.g., chlamydia or herpes simplex)Maternal smoking history; marijuana, heroin, cocaine usePrevious Health ChallengesHistory of respiratory illness such as strep throat, tonsillitisNumber of colds per year including ‘‘typical course’’; coughing, wheezing, or
other noisy breathing associated with coldsHistory of otitis mediaHistory of tuberculosisHistory of previous respiratory diseases (asthma), frequency of coldsHistory of known allergies or asthmaImmunizationsStatus of current immunizations (including influenza)Date of past tuberculosis test and results
Nutritional assessment Weight lossFailure to gain weight between office visitsDecrease in physical activityDecrease in appetiteChanges in bowel patterns and appearance of feces
Family medical history Family history of allergies, asthma, tuberculosis, pertussis, cystic fibrosisFocus on sibling history of respiratory illness
Social history Cultural (any customs that may affect treatment)Number of persons living in the household and whomChild’s primary caregiver
Environmental history Home environment (age and type of dwelling, condition of home [waterdamage may indicate mold exposure], sources of heating/cooling)
Types of household products used (e.g., chemicals, pesticides, cleaning sup-plies, paint fumes, hobby supplies)
Environmental exposures such as plant allergens, animal allergens (pets,rodents, insects), powders, aerosols, household irritants
(Continued )
Chapter 16 n n The Child With Altered Respiratory Status 655

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:31 User ID: muralir 1BlackLining Disabled
The child’s past medical history, including birth his-tory, previous health problems, childhood illnesses,immunizations (routine and yearly, including yearly fluvaccines), and allergies, helps put the current illness intoperspective. For example, a child presenting with paroxys-mal coughing episodes may cause the nurse to considerforeign body aspiration (FBA), croup, bronchitis, or pneu-monia, depending on the presence of other accompanyingsymptoms. However, if the child was never immunizedagainst pertussis, has not been screened recently for tu-berculosis, or has recently visited or lived in anothercountry, additional possibilities for the symptoms must beconsidered. Focus on birth weight, gestational age, andany complications involved with the child’s birth. Lungsdevelop in utero; therefore, premature infants, whoselungs do not have time to develop fully, may have respira-tory complications throughout the life span.
Ensure that family medical history includes any inher-ited (e.g., genetically linked), chronic, or infectious respi-ratory conditions. Also include a careful environmentalassessment, taking into account where the child usuallyresides (home) and other places in the child’s daily envi-ronment (e.g., school, child care setting, and relatives’home). Using the environmental history, you can examinerelationships between known exposures and symptoms,provide anticipatory guidance to prevent further exposure,empower parents to seek information about environmentalissues, and give parents the knowledge and skills to advo-cate for their children’s health and well-being.
caREmindercaREminderChildren often spend large amounts of time away from theirusual home setting (e.g., school, relative’s home, baby-sitter’s, child care setting). When taking a history aboutenvironmental risks, consider the child’s daily environmentin addition to the regular home setting.
Assess nutrition and general growth and developmentfactors. Growth impairment caused by chronic hypoxiaand poor nutritional intake is sometimes the first sign of
decompensation in the child with chronic respiratoryproblems.
Answer: The case study does not include informa-tion regarding Jose’s birth history, his immunization his-
tory, and nutritional assessment; as well as family, social, andenvironmental history. His medications are covered in moredepth in the Chapter 9 case study. The Diaz family is MexicanAmerican and, although both parents are bilingual, theremay be aspects of the health history that the couple struggle toexplain adequately in English and could relay with more accu-racy and detail in Spanish. Be attuned to the potential needfor a medical translator. It is also appropriate to ask if anycultural remedies have been used with Jose.
Focused Physical Assessment
Question: Which techniques has the nurse usedto assess Jose? What additional information do you
anticipate the nurse will identify as the physical assessment iscompleted?
Use the techniques of observation, inspection, ausculta-tion, palpation, and percussion when performing a physi-cal assessment of the respiratory system in infants,children, and youth. Focused Physical Assessment 16–1summarizes possible physical assessment findings andhighlights abnormalities and their implications.
Note the shape, size, and symmetry of the thoracic cav-ity. Notice the type and quality of breathing, and the depthand regularity of respirations. In the child younger than7 years, respirations are diaphragmatic, and the abdomenrises with inspiration; later, the breathing becomes tho-racic. Note respiratory effort and appearance of retrac-tions, nasal flaring, and use of accessory muscles. Breathingshould be quiet and nonlabored, at a respiratory rate nor-mal for age (see Appendix D), with an inspiratory phase
Outdoor air exposures (e.g., levels of air pollution in local community)Smoking behaviors of other household members or visitors to homeParental occupational exposure (parents’ clothing from work may be a source
of exposure to heavy metals or chemicals)Growth and
developmentPhysical milestonesDevelopmental milestonesHabits: play, sleepSchool attendance and performance
*This history focuses on the respiratory system. See chapter 8 for a comprehensive health history.
Focused Health History 16—1
The Child With Altered Respiratory Status* (Continued)
656 Unit 3 n n Managing Health Challenges
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:32 User ID: muralir 1BlackLining Disabled
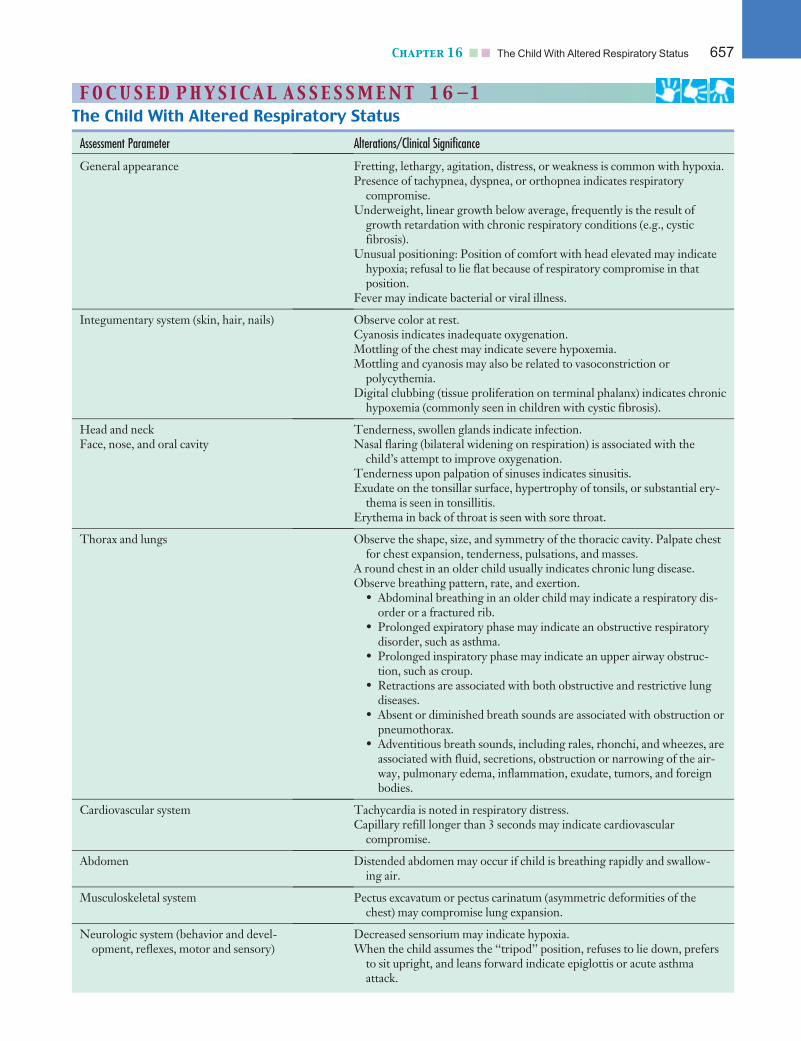
F O CU S E D PHY S I C A L A S S E S SMEN T 1 6—1
The Child With Altered Respiratory Status
Assessment Parameter Alterations/Clinical Significance
General appearance Fretting, lethargy, agitation, distress, or weakness is common with hypoxia.Presence of tachypnea, dyspnea, or orthopnea indicates respiratory
compromise.Underweight, linear growth below average, frequently is the result of
growth retardation with chronic respiratory conditions (e.g., cysticfibrosis).
Unusual positioning: Position of comfort with head elevated may indicatehypoxia; refusal to lie flat because of respiratory compromise in thatposition.
Fever may indicate bacterial or viral illness.
Integumentary system (skin, hair, nails) Observe color at rest.Cyanosis indicates inadequate oxygenation.Mottling of the chest may indicate severe hypoxemia.Mottling and cyanosis may also be related to vasoconstriction or
polycythemia.Digital clubbing (tissue proliferation on terminal phalanx) indicates chronic
hypoxemia (commonly seen in children with cystic fibrosis).
Head and neck Tenderness, swollen glands indicate infection.Face, nose, and oral cavity Nasal flaring (bilateral widening on respiration) is associated with the
child’s attempt to improve oxygenation.Tenderness upon palpation of sinuses indicates sinusitis.Exudate on the tonsillar surface, hypertrophy of tonsils, or substantial ery-
thema is seen in tonsillitis.Erythema in back of throat is seen with sore throat.
Thorax and lungs Observe the shape, size, and symmetry of the thoracic cavity. Palpate chestfor chest expansion, tenderness, pulsations, and masses.
A round chest in an older child usually indicates chronic lung disease.Observe breathing pattern, rate, and exertion.
• Abdominal breathing in an older child may indicate a respiratory dis-order or a fractured rib.
• Prolonged expiratory phase may indicate an obstructive respiratorydisorder, such as asthma.
• Prolonged inspiratory phase may indicate an upper airway obstruc-tion, such as croup.
• Retractions are associated with both obstructive and restrictive lungdiseases.
• Absent or diminished breath sounds are associated with obstruction orpneumothorax.
• Adventitious breath sounds, including rales, rhonchi, and wheezes, areassociated with fluid, secretions, obstruction or narrowing of the air-way, pulmonary edema, inflammation, exudate, tumors, and foreignbodies.
Cardiovascular system Tachycardia is noted in respiratory distress.Capillary refill longer than 3 seconds may indicate cardiovascular
compromise.
Abdomen Distended abdomen may occur if child is breathing rapidly and swallow-ing air.
Musculoskeletal system Pectus excavatum or pectus carinatum (asymmetric deformities of thechest) may compromise lung expansion.
Neurologic system (behavior and devel-opment, reflexes, motor and sensory)
Decreased sensorium may indicate hypoxia.When the child assumes the ‘‘tripod’’ position, refuses to lie down, prefers
to sit upright, and leans forward indicate epiglottis or acute asthmaattack.
Chapter 16 n n The Child With Altered Respiratory Status 657

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:32 User ID: muralir 1BlackLining Disabled
slightly longer than or equal to the expiratory phase.Count the respiratory rate for a full minute, ideally whenthe child is asleep or quiet. Tachypnea (rapid breathing orpanting) may be observed in the presence of fever, anxiety,or stress. Prolonged tachypnea may be an indicator of re-spiratory distress.
The color of the face, trunk, nail beds (and the shapeof the nail beds) also can provide clues to respiratory sta-tus. Skin and mucous membranes should be pink. Nailbeds should be pale or pink, and the nails should be flat,with the angle between the nail and the nail base atapproximately 160 degrees.
While observing respiratory status, assess also forspeech patterns (shortness of breath can be seen in quick,short sentences) and activity level.
During auscultation, assess the quality and intensity ofthe breath sounds as well as noting the area of the chestwhere they are heard (see Table 8–6). Vesicular breathsounds are low-pitched, soft sounds (heard more duringinspiration than during expiration) audible throughoutlung field. Bronchovesicular breath sounds are moderatelypitched, harsh sounds (inspiration ¼ expiration) heardover the manubrium. Bronchotubular breath sounds arehigh-pitched, hollow sounds (inspiratory sounds greaterthan expiratory sounds) heard over the trachea. Adventi-tious (abnormal) breath sounds that can be auscultated
include wheezes, crackles (rales), and rhonchi (FocusedPhysical Assessment 16–2).
Listen for audible abnormalities including stridor andgrunting. Stridor is a harsh, grating, whistling soundheard on inspiration and is produced by turbulent airflowthrough laryngeal or tracheal obstruction. It is usuallymore pronounced when the child is crying or agitated.Grunting is a noise the infant may make as he or sheattempts to provide a self-induced positive end-expiratorypressure. By grunting, the infant closes the glottis andapplies positive pressure to the airway to increase theresting volume of the lung.
Palpate the chest to assess for chest expansion, tender-ness, pulsations, and masses in the thoracic region. Sub-cutaneous emphysema (crepitus) is a manifestation of
Alert! Grunting is usually an ominous sign and may indicate impend-ing respiratory failure in the infant or young child. Other clinical signs of respi-ratory distress and impending respiratory failure that require immediateattention include increased work of breathing (severe retractions and grunting),diminished or absent breath sounds, development of hypoventilation (apnea orgasping respirations), altered level of consciousness (lethargy or inability to beconsoled by parents), poor systemic perfusion (capillary refill of more than 2seconds, mottling, or both), tachycardia, and bradycardia (late sign).
F O CU S E D PHY S I C A L A S S E S SMEN T 1 6—2
Adventitious Breath Sounds
Sound Description Pathology and Examples
Crackles
Fine Intermittent, high-pitched, soft popping sounds.Heard late in inspiration. Sound similar to hairrolling between fingers. Not cleared by coughing.
Fluid in alveoli (pneumonia)
Medium Intermittent and medium-pitched sounds that areloud and coarse sounding. Heard early or duringmid inspiration.
Fluid in bronchioles and bronchi (pulmo-nary edema)
Coarse Loud, bubbling, low-pitched sounds. Heard onexpiration. Cleared by coughing.
Fluid in bronchioles and bronchi that isresolving (bronchitis)
Friction rub Superficial, coarse, low-pitched, grating sound.Sounds similar to two pieces of leather rubbingtogether. Heard on inspiration and expiration.
Pleural inflammation from loss of normallubricating fluid (pleuritis)
Rhonchus
Sonorous Continuous, snoring, low-pitched, moaning,vibrating sound that clears with coughing. Heardthroughout respiratory cycle.
Air flow obstruction (mucus) in largebronchi and trachea (bronchitis, upperrespiratory tract infection)
Wheezes
Sibilant Continuous, high-pitched, musical, hissing sound.Heard predominantly during mid to lateexpiration.
Air flow through narrowed passagewaybecause of inflammation, collapse,secretions, or tumors (asthma)
Audible without stethoscope:inspiratory
Sonorous, musical sounds are heard on inspiration. High obstruction (croup)
Audible without stethoscope:expiratory
Whistling, sighing sounds are heard on expiration. Low obstruction (bronchial foreign body)
658 Unit 3 n n Managing Health Challenges

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:32 User ID: muralir 1BlackLining Disabled
free air that has leaked from the respiratory system intothe subcutaneous tissue, most commonly resulting from apneumomediastinum or pneumothorax. It can usually bepalpated over the neck, shoulders, and upper chest. Assessand palpate for symmetry of chest wall excursions, espe-cially in a child in whom trauma is suspected. Trauma tothe rib cage can result in fractures and a ‘‘flail chest’’(nonsymmetric movement of the chest) with decreasedmovement of the affected side. The position of the tra-chea may deviate from the normal midline in the pres-ence of atelectasis and with pneumothorax, so palpatingthis structure is important.
Use percussion to identify areas of consolidation orother internal changes within the lung. Percuss with a gen-tle motion to achieve sufficient tones, keeping in mind thatthe pediatric patient’s thinner chest wall will produce amore resonant tone. A normal percussion finding includesdullness over the heart and resonance over the lung fields.If a consolidation such as pneumonia is present, the reso-nance over the lungs will change to a dull sound.
Answer: The nurse has used inspection but notauscultation. Did you anticipate that Jose’s breath
sounds may be difficult to assess because of the loud inspira-tory stridor? The nurse does not hear air moving well in thelower lobes, but is not certain if the sound is masked by thestridor or if Jose is truly not moving air well.
Diagnostic Criteria
Question: Of the four groups of diagnostic testsidentified in the following pages, three are typically
used to evaluate a child’s condition with asthma. One is al-ready in use: the pulse oximeter. Which diagnostic test willmost fully reflect the respiratory status of the child?
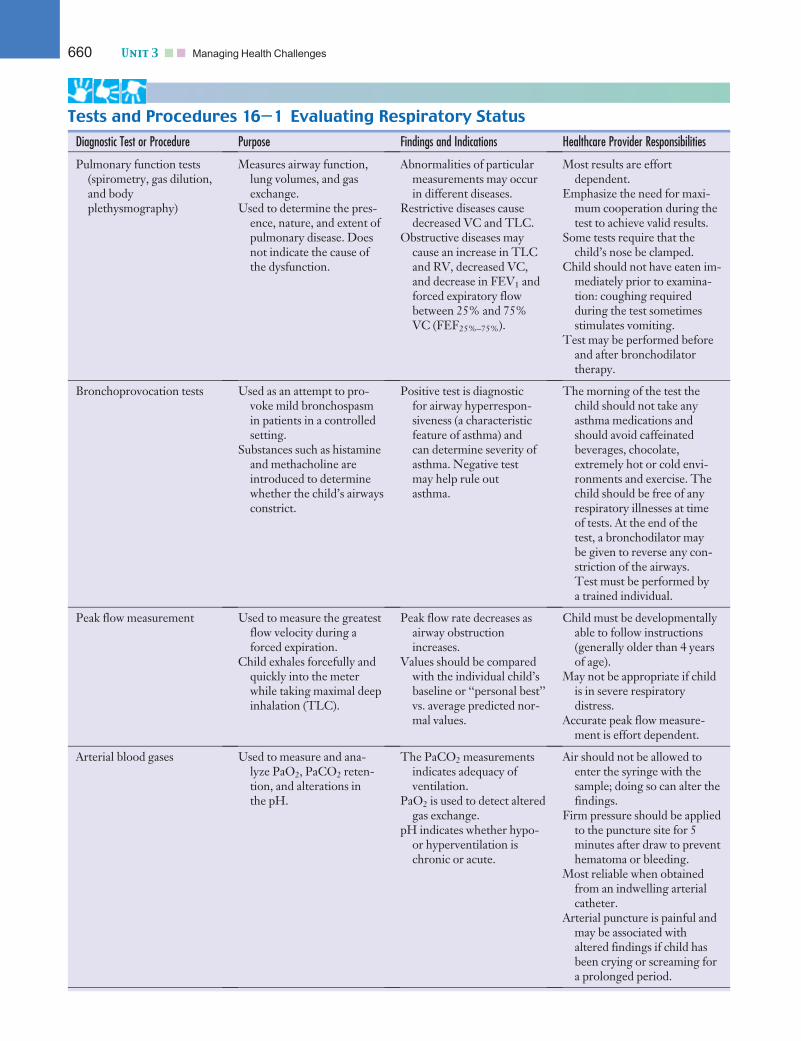
Four major groups of diagnostic tests and proceduresused in the evaluation of the respiratory system and respi-ratory disorders in children include (1) measurement oflung volumes and flow rates (pulmonary function testsand peak flow measurement), (2) direct or indirect bloodand body fluid analysis (arterial blood gases, fluid cul-tures, sweat chloride test), (3) imaging techniques(radiographs, fluoroscopy, bronchography, computed to-mographic scan, scintigraphy, magnetic resonance imag-ing), and (4) direct visualization of the respiratory tree(laryngoscopy, bronchoscopy). These diagnostic tests,used alone or in combination with others, may yield in-formation necessary in the diagnosis and treatment ofacute and chronic lung disease. Tests and Procedures 16–1 describes the purpose, findings, and indications of indi-vidual diagnostic tests, as well as the specific responsibil-ities and considerations for the healthcare provider.
Measurement of arterial blood gases is considered oneof the most useful diagnostic tests when a child presentswith respiratory distress, impending cardiopulmonary
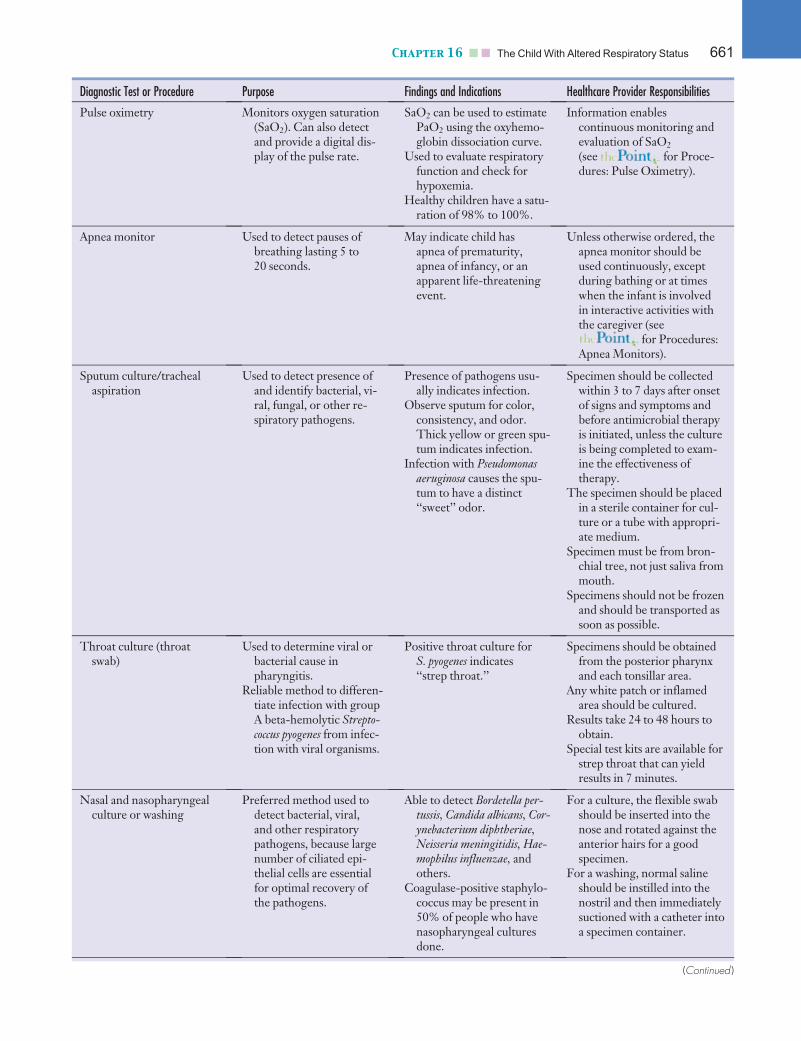
failure, or both. Therefore, knowing normal arterialblood gas values for children is important for the nurseassessing and evaluating the child (Tests and Procedures16–2). Pulse oximetry and apnea monitors are examplesof noninvasive and portable methods to detect respiratorycompromise in the pediatric patient. Pulse oximetry isprimarily used in inpatient and outpatient clinical settingsby healthcare providers (Fig. 16–4). Apnea monitors areused in both clinical and home settings as both a diagnos-tic tool to assess for apnea and a system to alert care pro-viders that a child is experiencing an apneic event andintervention may be warranted (see for Proce-dures: Pulse Oximetry and Apnea Monitoring for supple-mental information).
Answer: Pulse oximetry can read the oxygen satu-ration of Jose’s hemoglobin, but it cannot detect an
increase in carbon dioxide or pH changes. An arterial bloodgas measurement, although invasive, relays information thatcannot be obtained readily through a noninvasive alternative.
Treatment Modalities
Respiratory illnesses in children, both acute and chronicconditions, require aggressive and immediate intervention.Respiratory failure is one of the leading causes of cardio-pulmonary arrest in children (American Heart Association,2005). A thorough assessment of the child’s status, fol-lowed by quick actions that support oxygenation and ven-tilation, can serve to avert an impending arrest situation.In the case of acute respiratory problems, children gener-ally respond well and promptly to the simple adminis-tration of oxygen and medications. For children with achronic respiratory condition, oxygen, medications, airwayclearance techniques (ACTs), and nutritional support canassist them through exacerbations of the illness and pro-vide them with the strength to maintain a high level ofwellness despite their chronic conditions. Some conditionsmay require use of artificial airways, mechanical ventila-tion, or tracheostomy.
Administration of Oxygen
Question: Examine the various modes that oxy-gen can be delivered in Nursing Interventions 16–2.
Why was a simple mask used to deliver oxygen to Joseinstead of nasal cannula?
Oxygen is indicated for the treatment of hypoxemia andcan be the most dramatic, life-saving intervention for thatcondition. Although oxygen is important, assess patencyof the airway first. Oxygen is indicated for the presenceof or risk of low arterial oxygen (PaO2) levels and is alsoindicated to improve oxygenation when cardiac outputis low, to decrease pulmonary vascular resistance, to
Chapter 16 n n The Child With Altered Respiratory Status 659
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:32 User ID: muralir 1BlackLining Disabled
Tests and Procedures 16—1 Evaluating Respiratory Status
Diagnostic Test or Procedure Purpose Findings and Indications Healthcare Provider Responsibilities
Pulmonary function tests(spirometry, gas dilution,and bodyplethysmography)
Measures airway function,lung volumes, and gasexchange.
Used to determine the pres-ence, nature, and extent ofpulmonary disease. Doesnot indicate the cause ofthe dysfunction.
Abnormalities of particularmeasurements may occurin different diseases.
Restrictive diseases causedecreased VC and TLC.
Obstructive diseases maycause an increase in TLCand RV, decreased VC,and decrease in FEV1 andforced expiratory flowbetween 25% and 75%VC (FEF25%–75%).
Most results are effortdependent.
Emphasize the need for maxi-mum cooperation during thetest to achieve valid results.
Some tests require that thechild’s nose be clamped.
Child should not have eaten im-mediately prior to examina-tion: coughing requiredduring the test sometimesstimulates vomiting.
Test may be performed beforeand after bronchodilatortherapy.
Bronchoprovocation tests Used as an attempt to pro-voke mild bronchospasmin patients in a controlledsetting.
Substances such as histamineand methacholine areintroduced to determinewhether the child’s airwaysconstrict.
Positive test is diagnosticfor airway hyperrespon-siveness (a characteristicfeature of asthma) andcan determine severity ofasthma. Negative testmay help rule outasthma.
The morning of the test thechild should not take anyasthma medications andshould avoid caffeinatedbeverages, chocolate,extremely hot or cold envi-ronments and exercise. Thechild should be free of anyrespiratory illnesses at timeof tests. At the end of thetest, a bronchodilator maybe given to reverse any con-striction of the airways.Test must be performed bya trained individual.
Peak flow measurement Used to measure the greatestflow velocity during aforced expiration.
Child exhales forcefully andquickly into the meterwhile taking maximal deepinhalation (TLC).
Peak flow rate decreases asairway obstructionincreases.
Values should be comparedwith the individual child’sbaseline or ‘‘personal best’’vs. average predicted nor-mal values.
Child must be developmentallyable to follow instructions(generally older than 4 yearsof age).
May not be appropriate if childis in severe respiratorydistress.
Accurate peak flow measure-ment is effort dependent.
Arterial blood gases Used to measure and ana-lyze PaO2, PaCO2 reten-tion, and alterations inthe pH.
The PaCO2 measurementsindicates adequacy ofventilation.
PaO2 is used to detect alteredgas exchange.
pH indicates whether hypo-or hyperventilation ischronic or acute.
Air should not be allowed toenter the syringe with thesample; doing so can alter thefindings.
Firm pressure should be appliedto the puncture site for 5minutes after draw to preventhematoma or bleeding.
Most reliable when obtainedfrom an indwelling arterialcatheter.
Arterial puncture is painful andmay be associated withaltered findings if child hasbeen crying or screaming fora prolonged period.
660 Unit 3 n n Managing Health Challenges
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:32 User ID: muralir 1BlackLining Disabled
Diagnostic Test or Procedure Purpose Findings and Indications Healthcare Provider Responsibilities
Pulse oximetry Monitors oxygen saturation(SaO2). Can also detectand provide a digital dis-play of the pulse rate.
SaO2 can be used to estimatePaO2 using the oxyhemo-globin dissociation curve.
Used to evaluate respiratoryfunction and check forhypoxemia.
Healthy children have a satu-ration of 98% to 100%.
Information enablescontinuous monitoring andevaluation of SaO2
(see for Proce-dures: Pulse Oximetry).
Apnea monitor Used to detect pauses ofbreathing lasting 5 to20 seconds.
May indicate child hasapnea of prematurity,apnea of infancy, or anapparent life-threateningevent.
Unless otherwise ordered, theapnea monitor should beused continuously, exceptduring bathing or at timeswhen the infant is involvedin interactive activities withthe caregiver (see
for Procedures:Apnea Monitors).
Sputum culture/trachealaspiration
Used to detect presence ofand identify bacterial, vi-ral, fungal, or other re-spiratory pathogens.
Presence of pathogens usu-ally indicates infection.
Observe sputum for color,consistency, and odor.Thick yellow or green spu-tum indicates infection.
Infection with Pseudomonasaeruginosa causes the spu-tum to have a distinct‘‘sweet’’ odor.
Specimen should be collectedwithin 3 to 7 days after onsetof signs and symptoms andbefore antimicrobial therapyis initiated, unless the cultureis being completed to exam-ine the effectiveness oftherapy.
The specimen should be placedin a sterile container for cul-ture or a tube with appropri-ate medium.
Specimen must be from bron-chial tree, not just saliva frommouth.
Specimens should not be frozenand should be transported assoon as possible.
Throat culture (throatswab)
Used to determine viral orbacterial cause inpharyngitis.
Reliable method to differen-tiate infection with groupA beta-hemolytic Strepto-coccus pyogenes from infec-tion with viral organisms.
Positive throat culture forS. pyogenes indicates‘‘strep throat.’’
Specimens should be obtainedfrom the posterior pharynxand each tonsillar area.
Any white patch or inflamedarea should be cultured.
Results take 24 to 48 hours toobtain.
Special test kits are available forstrep throat that can yieldresults in 7 minutes.
Nasal and nasopharyngealculture or washing
Preferred method used todetect bacterial, viral,and other respiratorypathogens, because largenumber of ciliated epi-thelial cells are essentialfor optimal recovery ofthe pathogens.
Able to detect Bordetella per-tussis, Candida albicans, Cor-ynebacterium diphtheriae,Neisseria meningitidis, Hae-mophilus influenzae, andothers.
Coagulase-positive staphylo-coccus may be present in50% of people who havenasopharyngeal culturesdone.
For a culture, the flexible swabshould be inserted into thenose and rotated against theanterior hairs for a goodspecimen.
For a washing, normal salineshould be instilled into thenostril and then immediatelysuctioned with a catheter intoa specimen container.
(Continued )
Chapter 16 n n The Child With Altered Respiratory Status 661
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:32 User ID: muralir 1BlackLining Disabled
Diagnostic Test or Procedure Purpose Findings and Indications Healthcare Provider Responsibilities
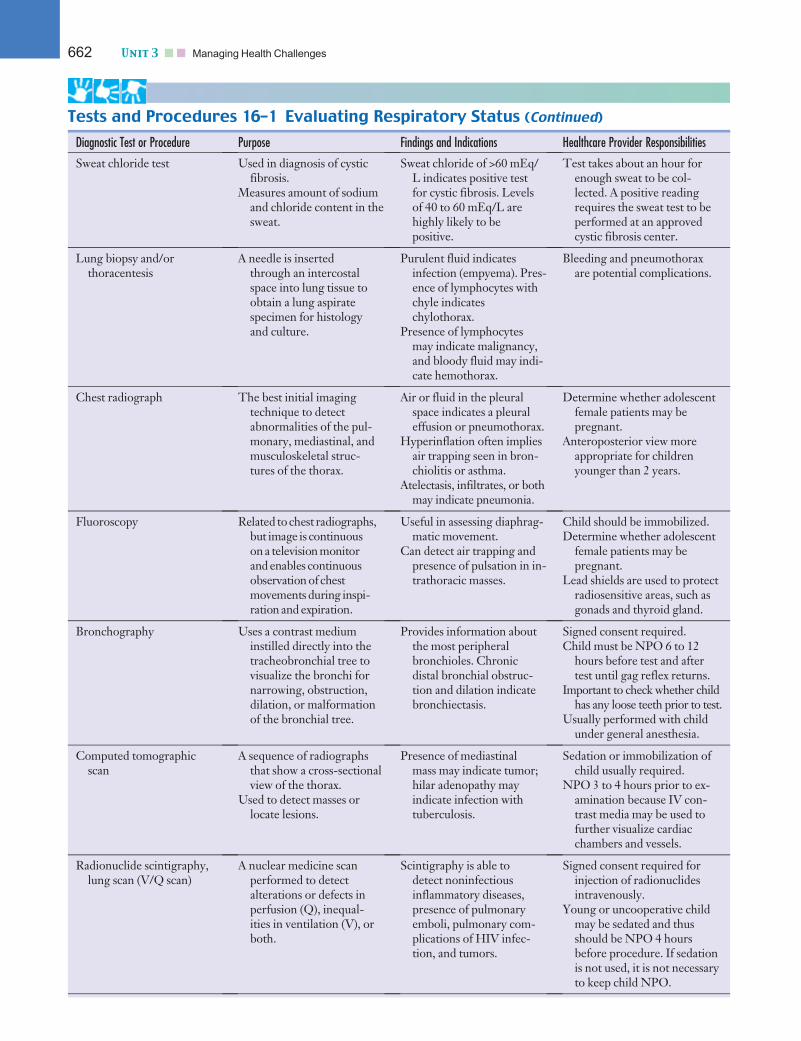
Sweat chloride test Used in diagnosis of cysticfibrosis.
Measures amount of sodiumand chloride content in thesweat.
Sweat chloride of >60 mEq/L indicates positive testfor cystic fibrosis. Levelsof 40 to 60 mEq/L arehighly likely to bepositive.
Test takes about an hour forenough sweat to be col-lected. A positive readingrequires the sweat test to beperformed at an approvedcystic fibrosis center.
Lung biopsy and/orthoracentesis
A needle is insertedthrough an intercostalspace into lung tissue toobtain a lung aspiratespecimen for histologyand culture.
Purulent fluid indicatesinfection (empyema). Pres-ence of lymphocytes withchyle indicateschylothorax.
Presence of lymphocytesmay indicate malignancy,and bloody fluid may indi-cate hemothorax.
Bleeding and pneumothoraxare potential complications.
Chest radiograph The best initial imagingtechnique to detectabnormalities of the pul-monary, mediastinal, andmusculoskeletal struc-tures of the thorax.
Air or fluid in the pleuralspace indicates a pleuraleffusion or pneumothorax.
Hyperinflation often impliesair trapping seen in bron-chiolitis or asthma.
Atelectasis, infiltrates, or bothmay indicate pneumonia.
Determine whether adolescentfemale patients may bepregnant.
Anteroposterior view moreappropriate for childrenyounger than 2 years.
Fluoroscopy Related to chest radiographs,but image is continuouson a television monitorand enables continuousobservation of chestmovements during inspi-ration and expiration.
Useful in assessing diaphrag-matic movement.
Can detect air trapping andpresence of pulsation in in-trathoracic masses.
Child should be immobilized.Determine whether adolescent
female patients may bepregnant.
Lead shields are used to protectradiosensitive areas, such asgonads and thyroid gland.
Bronchography Uses a contrast mediuminstilled directly into thetracheobronchial tree tovisualize the bronchi fornarrowing, obstruction,dilation, or malformationof the bronchial tree.
Provides information aboutthe most peripheralbronchioles. Chronicdistal bronchial obstruc-tion and dilation indicatebronchiectasis.
Signed consent required.Child must be NPO 6 to 12
hours before test and aftertest until gag reflex returns.
Important to check whether childhas any loose teeth prior to test.
Usually performed with childunder general anesthesia.
Computed tomographicscan
A sequence of radiographsthat show a cross-sectionalview of the thorax.
Used to detect masses orlocate lesions.
Presence of mediastinalmass may indicate tumor;hilar adenopathy mayindicate infection withtuberculosis.
Sedation or immobilization ofchild usually required.
NPO 3 to 4 hours prior to ex-amination because IV con-trast media may be used tofurther visualize cardiacchambers and vessels.
Radionuclide scintigraphy,lung scan (V/Q scan)
A nuclear medicine scanperformed to detectalterations or defects inperfusion (Q), inequal-ities in ventilation (V), orboth.
Scintigraphy is able todetect noninfectiousinflammatory diseases,presence of pulmonaryemboli, pulmonary com-plications of HIV infec-tion, and tumors.
Signed consent required forinjection of radionuclidesintravenously.
Young or uncooperative childmay be sedated and thusshould be NPO 4 hoursbefore procedure. If sedationis not used, it is not necessaryto keep child NPO.
Tests and Procedures 16–1 Evaluating Respiratory Status (Continued)
662 Unit 3 n n Managing Health Challenges
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:32 User ID: muralir 1BlackLining Disabled
enhance elimination of carbon dioxide, or to accelerateremoval of nitrogen from air-containing spaces such as apneumothorax.
Oxygen can be delivered by mask (Fig. 16–5), nasalcannula, oxygen hood, oxygen tent, or mechanical venti-lation (see for Procedures: Oxygen Adminis-tration for supplemental information). The mode ofoxygen delivery used is based on the concentration orpercentage of oxygen desired and on the child’s ability tocooperate with therapy. To ensure patient safety, meas-ure and monitor the concentration of inspired oxygencarefully and document response during oxygen therapy.Oxygen therapy in children should use the least amountof oxygen required to normalize PaO2 (more than 60–80mm Hg) and arterial hemoglobin saturation (SaO2)(more than 93%). When oxygen is administered throughan artificial airway such as an endotracheal tube or a tra-cheostomy tube, the gas must be artificially heated andhumidified.
caREmindercaREminderTo decrease the risk of mucociliary dysfunction, injury to therespiratory epithelium, and thickening of secretions, childrenreceiving oxygen therapy through an artificial airway formore than 1 to 2 hours should receive warmed, humidifiedoxygen.
The use of oxygen therapy in the home is becomingmore prevalent. Teaching Intervention Plan (TIP) 16–1
describes care of the child receiving home oxygen ther-apy and the educational needs of the family.
Answer: Jose is breathing primarily through hisopen mouth. For a nasal cannula to be an appropriate
mode of delivery, the child must keep his or her mouth closedand breathe through the nose.
MedicationsMedications are an important component of treating re-spiratory disorders in children. Routes of administrationare oral, inhaled, intravenous, and injectable (subcutane-ous or intramuscular). Inhaled medications are used mostoften to increase respiratory tract absorption and todecrease systemic absorption.
Classes of MedicationsThe main classes of medications used for respiratory dis-orders include bronchodilators, corticosteroids, and leu-kotriene modifiers/mast cell stabilizers. Other groups ofmedications often used in conjunction with these include,but are not limited to, antibiotics, antivirals, mucolyticsand expectorants, decongestants, antihistamines, and diu-retics. The pharmaceutical agents used for particularrespiratory disorders are addressed in the appropriatesections. Principles of inhalation therapy and aerosolizedmedications are addressed here.
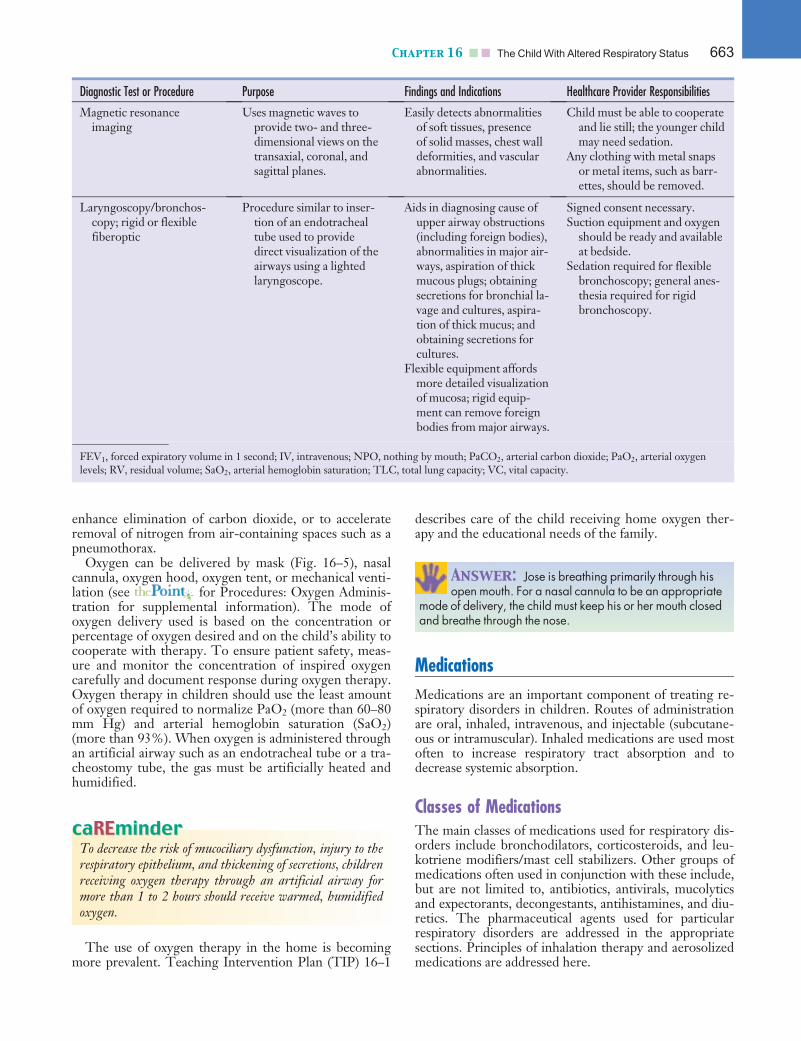
Diagnostic Test or Procedure Purpose Findings and Indications Healthcare Provider Responsibilities
Magnetic resonanceimaging
Uses magnetic waves toprovide two- and three-dimensional views on thetransaxial, coronal, andsagittal planes.
Easily detects abnormalitiesof soft tissues, presenceof solid masses, chest walldeformities, and vascularabnormalities.
Child must be able to cooperateand lie still; the younger childmay need sedation.
Any clothing with metal snapsor metal items, such as barr-ettes, should be removed.
Laryngoscopy/bronchos-copy; rigid or flexiblefiberoptic
Procedure similar to inser-tion of an endotrachealtube used to providedirect visualization of theairways using a lightedlaryngoscope.
Aids in diagnosing cause ofupper airway obstructions(including foreign bodies),abnormalities in major air-ways, aspiration of thickmucous plugs; obtainingsecretions for bronchial la-vage and cultures, aspira-tion of thick mucus; andobtaining secretions forcultures.
Flexible equipment affordsmore detailed visualizationof mucosa; rigid equip-ment can remove foreignbodies from major airways.
Signed consent necessary.Suction equipment and oxygen
should be ready and availableat bedside.
Sedation required for flexiblebronchoscopy; general anes-thesia required for rigidbronchoscopy.
FEV1, forced expiratory volume in 1 second; IV, intravenous; NPO, nothing by mouth; PaCO2, arterial carbon dioxide; PaO2, arterial oxygenlevels; RV, residual volume; SaO2, arterial hemoglobin saturation; TLC, total lung capacity; VC, vital capacity.
Chapter 16 n n The Child With Altered Respiratory Status 663
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:33 User ID: muralir 1BlackLining Disabled
Aerosol Therapy
Question: Jose uses a nebulizer at home. Evalu-ate the other methods of aerosol therapy. What sup-
portive rationale can you offer for why this method ofmedication delivery is an appropriate choice for Jose?
Bronchodilators, corticosteroids, and mast cell stabilizermedications are delivered by inhalers or nebulizers. How-ever, bronchodilators and corticosteroids are also availablein oral and intravenous forms. Administering medicationsby inhalation is effective, because the medication reachesthe small airways and works directly on the lungs. Medica-tions are nebulized or aerosolized by using compressedair or oxygen. A variety of machines (compressors) are
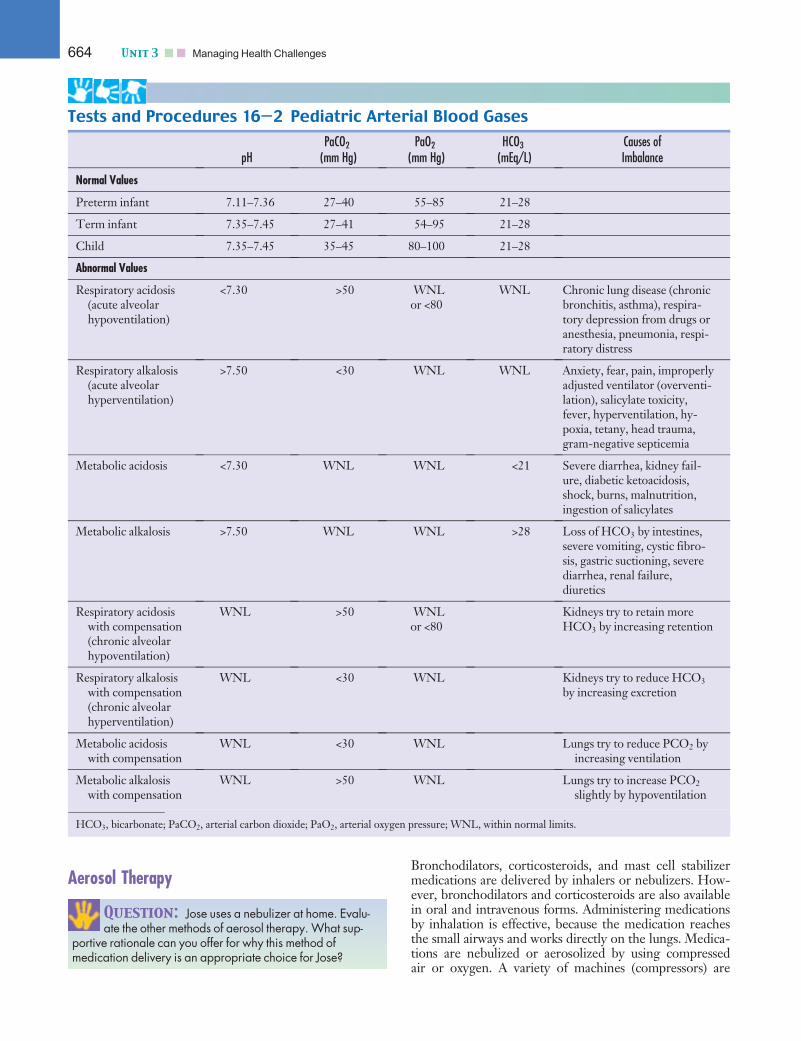
Tests and Procedures 16—2 Pediatric Arterial Blood Gases
pHPaCO2
(mm Hg)PaO2
(mm Hg)HCO3
(mEq/L)Causes ofImbalance
Normal Values
Preterm infant 7.11–7.36 27–40 55–85 21–28
Term infant 7.35–7.45 27–41 54–95 21–28
Child 7.35–7.45 35–45 80–100 21–28
Abnormal Values
Respiratory acidosis(acute alveolarhypoventilation)
<7.30 >50 WNLor <80
WNL Chronic lung disease (chronicbronchitis, asthma), respira-tory depression from drugs oranesthesia, pneumonia, respi-ratory distress
Respiratory alkalosis(acute alveolarhyperventilation)
>7.50 <30 WNL WNL Anxiety, fear, pain, improperlyadjusted ventilator (overventi-lation), salicylate toxicity,fever, hyperventilation, hy-poxia, tetany, head trauma,gram-negative septicemia
Metabolic acidosis <7.30 WNL WNL <21 Severe diarrhea, kidney fail-ure, diabetic ketoacidosis,shock, burns, malnutrition,ingestion of salicylates
Metabolic alkalosis >7.50 WNL WNL >28 Loss of HCO3 by intestines,severe vomiting, cystic fibro-sis, gastric suctioning, severediarrhea, renal failure,diuretics
Respiratory acidosiswith compensation(chronic alveolarhypoventilation)
WNL >50 WNLor <80
Kidneys try to retain moreHCO3 by increasing retention
Respiratory alkalosiswith compensation(chronic alveolarhyperventilation)
WNL <30 WNL Kidneys try to reduce HCO3
by increasing excretion
Metabolic acidosiswith compensation
WNL <30 WNL Lungs try to reduce PCO2 byincreasing ventilation
Metabolic alkalosiswith compensation
WNL >50 WNL Lungs try to increase PCO2
slightly by hypoventilation
HCO3, bicarbonate; PaCO2, arterial carbon dioxide; PaO2, arterial oxygen pressure; WNL, within normal limits.
664 Unit 3 n n Managing Health Challenges
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:33 User ID: muralir 1BlackLining Disabled
available for use with a handheld nebulizer, often for usein the home. The handheld nebulizer has the advantagesof being able to aerosolize almost any drug available in liq-uid form, allowing modification of dose volume and con-centration, and requiring minimal patient coordination.The child or infant usually uses a mask attached to thenebulizer cup, which is held over the nose and mouth.The medication is dispersed as a mist. Older children canuse the mouthpiece and should be instructed to take slow,deep breaths through the mouth during the treatment(Fig. 16–6). Nebulizers are effective for most childrenyounger than 5 years of age and older children who havedifficulty coordinating a metered dose inhaler (MDI).
----------------------------------------------------KidKare Allow the child to hold the mask up to hisor her face instead of using the elastic strap aroundthe head. When the child is getting the treatment, heor she may like to have ‘‘teddy’’ or ‘‘dolly’’ wear amask and ‘‘get a treatment,’’ too.----------------------------------------------------
The MDI is a simple, portable, self-contained handheldcanister that delivers a predetermined amount of the speci-fied medication to the patient. Most bronchodilators, cor-ticosteroids, and mast cell inhibitors are available in anMDI. Although MDIs have the advantage of being veryportable and can provide efficient drug delivery with rapidpreparation and administration time, they do have thedisadvantage of being difficult to coordinate and usecorrectly. A spacer device should be used with MDIsregardless of age (Fig. 16–7). Use of a spacer allows timefor the propellant to remain suspended and achieve smallerparticle size. The spacer device may have a mouthpiece orface mask. Using spacers with mouthpieces requires coor-dination of breathing and drug dispersal, so spacers withmasks may facilitate dosage in younger children.
Another device for inhalation is the drug–powder inhaler.The drug–powder inhaler, which is similar to the MDI,consists of a suspension of microfine, solid particles of drugcontained in a small MDI-sized device with a mouthpiece.
A third type of device for administering inhaled medi-cations is breath-activated inhalers. With these devices,medication is delivered as the patient takes a breath. Thechild must seal their lips around the device before inhal-ing and should hold their breath for 10 seconds. Evaluatethe child’s ability to perform this technique properly be-fore he or she uses the device on a daily basis.
If the infant or child is receiving aerosol or inhalationtherapy, assess response to the treatment. Assess breathsounds and respiratory effort before and after the treat-ment for effectiveness. For the child receiving bronchodi-lators (beta-adrenergic agents), assessing the heart rateis also important, because tachycardia is a common sideeffect of these medications.
caREmindercaREminderBe sure to have the child rinse out the mouth or wash theface after using an inhaled corticosteroid to decrease thechance of systemic absorption and side effects related to themedications.
Answer: Jose is 4 years old. The nebulizer is verysimple to use and requires no special skills. Simply
breathing in and out deeply will allow the medication to workdirectly on the lung tissue.
Airway Clearance Techniques (ACTs)The airway clearance process may be dysfunctional, lead-ing to retained secretions, or there may be hypersecretionof mucus in the airways. Accumulation of secretions inthe airways leads to partial or total obstruction. Ventila-tion and gas exchange are altered, producing a favorableenvironment for infection. For example, children withconditions such as cystic fibrosis (CF), bronchiectasis, ordysfunctional motility of cilia; those receiving mechanicalventilation; and those with acute problems after generalanesthesia can benefit from ACTs.
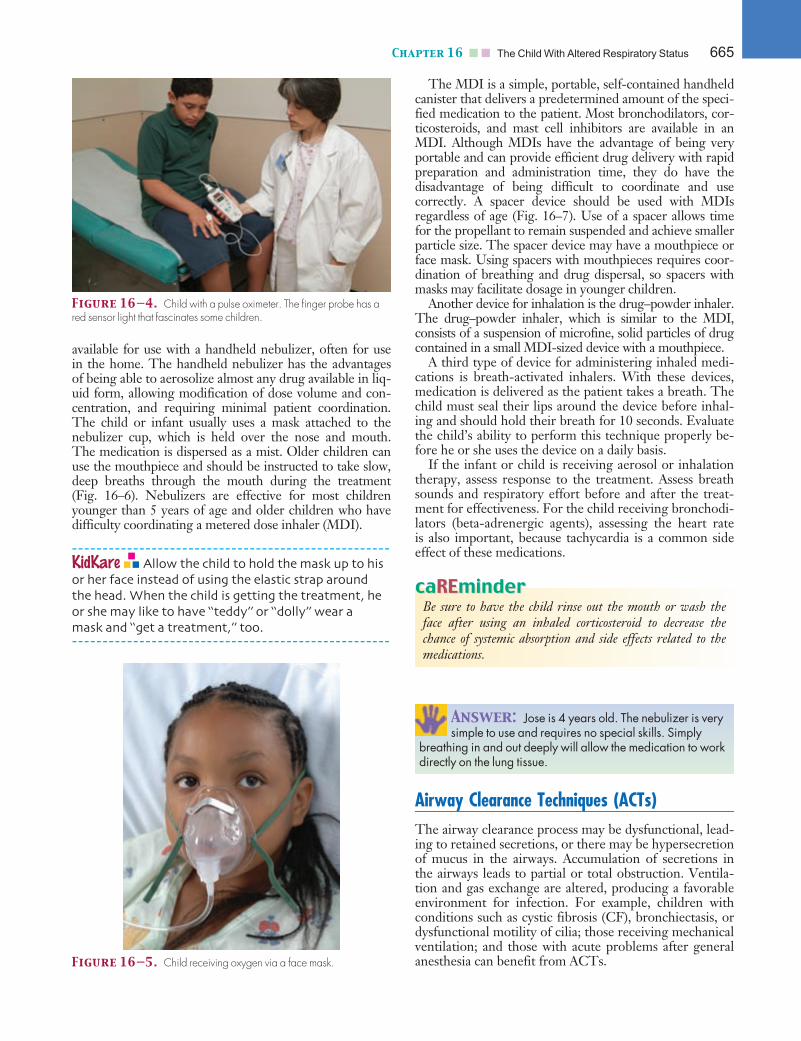
Figure 16—4. Child with a pulse oximeter. The finger probe has ared sensor light that fascinates some children.
Figure 16—5. Child receiving oxygen via a face mask.
Chapter 16 n n The Child With Altered Respiratory Status 665
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:33 User ID: muralir 1BlackLining Disabled
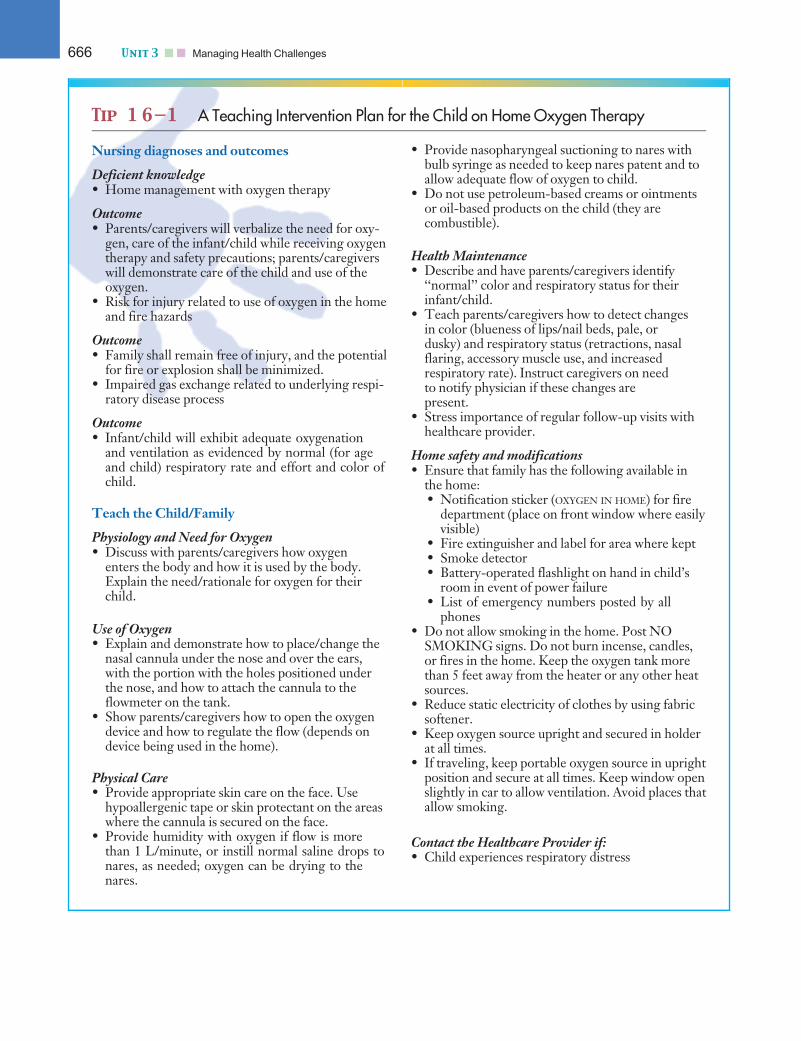
Tip 1 6—1 A Teaching Intervention Plan for the Child on Home Oxygen Therapy
Nursing diagnoses and outcomes
Deficient knowledge• Home management with oxygen therapy
Outcome• Parents/caregivers will verbalize the need for oxy-
gen, care of the infant/child while receiving oxygentherapy and safety precautions; parents/caregiverswill demonstrate care of the child and use of theoxygen.
• Risk for injury related to use of oxygen in the homeand fire hazards
Outcome• Family shall remain free of injury, and the potential
for fire or explosion shall be minimized.• Impaired gas exchange related to underlying respi-
ratory disease process
Outcome• Infant/child will exhibit adequate oxygenation
and ventilation as evidenced by normal (for ageand child) respiratory rate and effort and color ofchild.
Teach the Child/Family
Physiology and Need for Oxygen• Discuss with parents/caregivers how oxygen
enters the body and how it is used by the body.Explain the need/rationale for oxygen for theirchild.
Use of Oxygen• Explain and demonstrate how to place/change the
nasal cannula under the nose and over the ears,with the portion with the holes positioned underthe nose, and how to attach the cannula to theflowmeter on the tank.
• Show parents/caregivers how to open the oxygendevice and how to regulate the flow (depends ondevice being used in the home).
Physical Care• Provide appropriate skin care on the face. Use
hypoallergenic tape or skin protectant on the areaswhere the cannula is secured on the face.
• Provide humidity with oxygen if flow is morethan 1 L/minute, or instill normal saline drops tonares, as needed; oxygen can be drying to thenares.
• Provide nasopharyngeal suctioning to nares withbulb syringe as needed to keep nares patent and toallow adequate flow of oxygen to child.
• Do not use petroleum-based creams or ointmentsor oil-based products on the child (they arecombustible).
Health Maintenance• Describe and have parents/caregivers identify
‘‘normal’’ color and respiratory status for theirinfant/child.
• Teach parents/caregivers how to detect changesin color (blueness of lips/nail beds, pale, ordusky) and respiratory status (retractions, nasalflaring, accessory muscle use, and increasedrespiratory rate). Instruct caregivers on needto notify physician if these changes arepresent.
• Stress importance of regular follow-up visits withhealthcare provider.
Home safety and modifications• Ensure that family has the following available in
the home:• Notification sticker (OXYGEN IN HOME) for fire
department (place on front window where easilyvisible)
• Fire extinguisher and label for area where kept• Smoke detector• Battery-operated flashlight on hand in child’s
room in event of power failure• List of emergency numbers posted by all
phones• Do not allow smoking in the home. Post NO
SMOKING signs. Do not burn incense, candles,or fires in the home. Keep the oxygen tank morethan 5 feet away from the heater or any other heatsources.
• Reduce static electricity of clothes by using fabricsoftener.
• Keep oxygen source upright and secured in holderat all times.
• If traveling, keep portable oxygen source in uprightposition and secure at all times. Keep window openslightly in car to allow ventilation. Avoid places thatallow smoking.
Contact the Healthcare Provider if:• Child experiences respiratory distress
666 Unit 3 n n Managing Health Challenges

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:33 User ID: muralir 1BlackLining Disabled
Suctioning the trachea and nasopharyngeal airway is amethod to enhance airway clearance by removing secre-tions that cannot be removed by the child’s spontaneouscough. Suctioning may also be used to obtain secretionsfor diagnostic purposes (see for Procedures:Nasotracheal Suctioning for supplemental information).
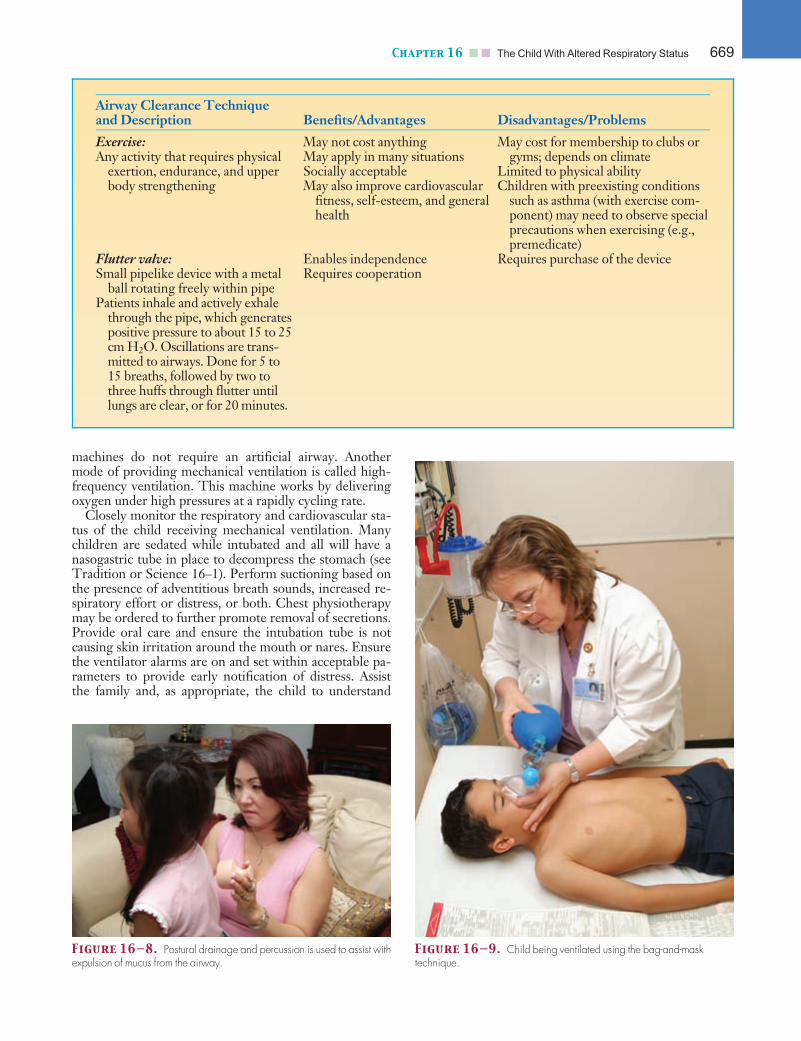
Traditionally, chest physiotherapy (also called posturaldrainage and percussion) has been the primary interventionfor pulmonary conditions with hypersecretion or retainedbronchial secretions. However, more therapy options forairway clearance exist now than were available in therecent past. Ongoing research to match the most effectivetherapy with the individual will improve quality of life inthis rapidly expanding area. Nursing Interventions 16–1summarizes information on these techniques as well as tra-ditional ACTs. Advantages and disadvantages of the newtechniques are also addressed, along with age indicators.
Determining the appropriateness of these newer inter-ventions for a particular patient requires assessing theseverity and type of lung disease, physical ability toperform the technique, effectiveness of the particulartechnique, and age. Other psychosocial factors to be con-sidered are motivation to learn, adherence to treatment,cost, and payer or reimbursement. These techniquesshould be performed 30 minutes before mealtimes, as asafety measure to avoid vomiting and aspiration, and topromote comfort (Fig. 16–8).
caREmindercaREminderSupplemental continuous gastrostomy tube or nasogastrictube feedings must be discontinued for at least 30 minutesbefore postural drainage and percussion.
Artificial Airways and Mechanical VentilationNoninvasive measures such as oxygen therapy and ACTsmay sometimes not meet the needs of all children whorequire oxygenation and ventilation. When respiratoryeffort is increased but inadequate to maintain gas exchangebecause of airway obstruction, intrapulmonary pathophysi-ology, neuromuscular disease, or other factors, artificial ormechanical ventilation may become necessary.
Several methods are available to provide artificial venti-lation. A bag-and-mask unit, or Ambu bag, is used to man-ually ventilate a child who has not been intubated (had anendotracheal tube placed). Effective bag-and-mask ventila-tion is best provided with a self-inflating bag and a maskthat fits properly over the child’s nose and mouth.
To provide an open airway, extend the infant’s orchild’s neck slightly in the sniffing position and lift thejaw (Fig. 16–9). The jaw thrust maneuver is used in thepediatric trauma victim with possible spinal injury or ininfants for whom overextending the neck can occlude theairway. Place the mask, held in your nondominant hand,over the nose and mouth to create a seal. With yourdominant hand, compress the bag rhythmically and insynchrony (or slightly faster) with the child’s spontaneousrespiratory efforts, if present, compressing the bag onlyenough to make the chest rise and fall. Aggressive venti-lating will lead to gastric distention. Ensure that the bagis connected to an oxygen source, with oxygen deliveredat a flow rate of 10 to 15 L/minute.
When prolonged artificial ventilation is neededbecause of respiratory failure or anesthesia, or when theairway is obstructed, intubation—placement of an artifi-cial airway—is necessary, and mechanical ventilation isprovided. Endotracheal intubation is the insertion of anartificial airway (an endotracheal tube) through either thenose (nasotracheal) or the mouth (orotracheal) into thetrachea (Fig. 16–10). Another less invasive device for me-chanical ventilation (used most commonly in the operat-ing room) is the laryngeal mask airway.
Mechanical ventilation replaces the work of breathingand involves inflating the lungs with compressed gas,applied by either positive or negative pressure. Positive-pressure ventilators are more commonly used than nega-tive-pressure machines. They work by creating pressureat the airway opening that is greater than the intra-alveo-lar pressure, thus forcing pressurized gas into the lungs.This flow of compressed gas improves gas exchange andinflation of poorly ventilated portions of the lungs. Nega-tive-pressure machines are more cumbersome and areprimarily used for long-term ventilation in persons withrespiratory failure caused by neuromuscular diseases.The machine works by creating intermittent negativepressure around the thorax, causing the chest to be drawnoutward and inspiration to occur. Negative-pressure
Figure 16—6. Child receiving treatment with a nebulizer.
Figure 16—7. Commercial spacer device.
Chapter 16 n n The Child With Altered Respiratory Status 667
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:33 User ID: muralir 1BlackLining Disabled
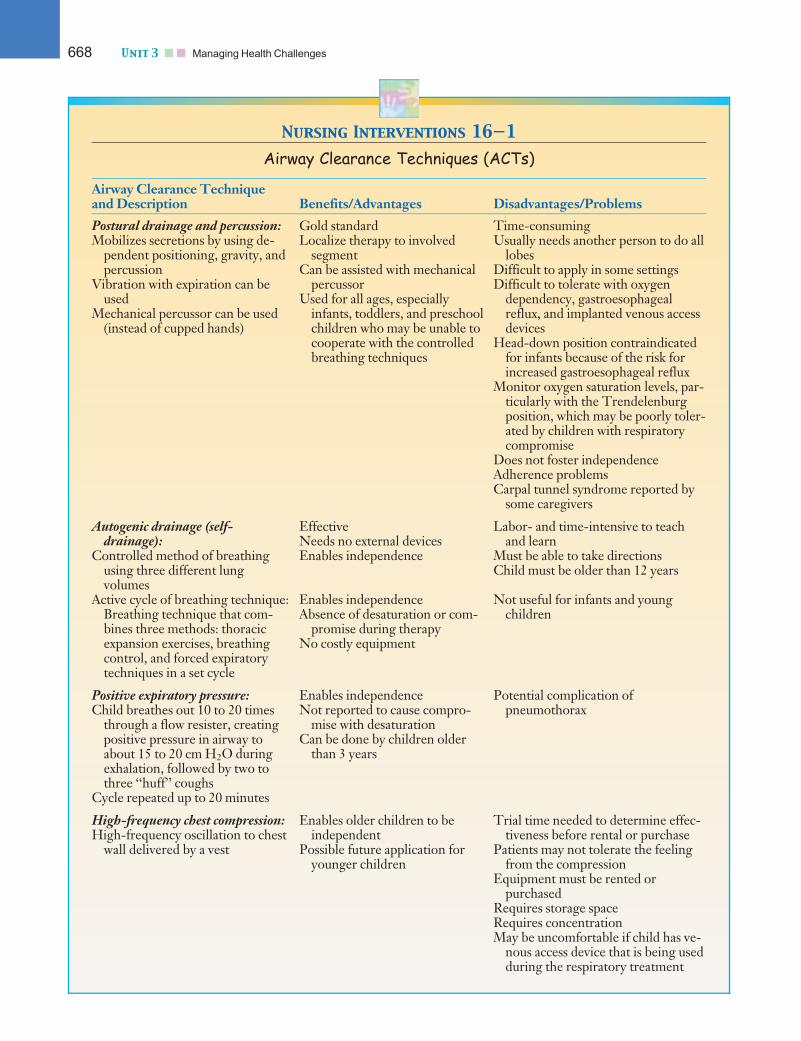
Nursing Interventions 16—1
Airway Clearance Techniques (ACTs)
Airway Clearance Techniqueand Description Benefits/Advantages Disadvantages/Problems
Postural drainage and percussion:Mobilizes secretions by using de-
pendent positioning, gravity, andpercussion
Vibration with expiration can beused
Mechanical percussor can be used(instead of cupped hands)
Gold standardLocalize therapy to involved
segmentCan be assisted with mechanical
percussorUsed for all ages, especially
infants, toddlers, and preschoolchildren who may be unable tocooperate with the controlledbreathing techniques
Time-consumingUsually needs another person to do all
lobesDifficult to apply in some settingsDifficult to tolerate with oxygen
dependency, gastroesophagealreflux, and implanted venous accessdevices
Head-down position contraindicatedfor infants because of the risk forincreased gastroesophageal reflux
Monitor oxygen saturation levels, par-ticularly with the Trendelenburgposition, which may be poorly toler-ated by children with respiratorycompromise
Does not foster independenceAdherence problemsCarpal tunnel syndrome reported by
some caregivers
Autogenic drainage (self-drainage):
Controlled method of breathingusing three different lungvolumes
EffectiveNeeds no external devicesEnables independence
Labor- and time-intensive to teachand learn
Must be able to take directionsChild must be older than 12 years
Active cycle of breathing technique:Breathing technique that com-bines three methods: thoracicexpansion exercises, breathingcontrol, and forced expiratorytechniques in a set cycle
Enables independenceAbsence of desaturation or com-
promise during therapyNo costly equipment
Not useful for infants and youngchildren
Positive expiratory pressure:Child breathes out 10 to 20 times
through a flow resister, creatingpositive pressure in airway toabout 15 to 20 cm H2O duringexhalation, followed by two tothree ‘‘huff’’ coughs
Cycle repeated up to 20 minutes
Enables independenceNot reported to cause compro-
mise with desaturationCan be done by children older
than 3 years
Potential complication ofpneumothorax
High-frequency chest compression:High-frequency oscillation to chest
wall delivered by a vest
Enables older children to beindependent
Possible future application foryounger children
Trial time needed to determine effec-tiveness before rental or purchase
Patients may not tolerate the feelingfrom the compression
Equipment must be rented orpurchased
Requires storage spaceRequires concentrationMay be uncomfortable if child has ve-
nous access device that is being usedduring the respiratory treatment
668 Unit 3 n n Managing Health Challenges
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:33 User ID: muralir 1BlackLining Disabled
machines do not require an artificial airway. Anothermode of providing mechanical ventilation is called high-frequency ventilation. This machine works by deliveringoxygen under high pressures at a rapidly cycling rate.
Closely monitor the respiratory and cardiovascular sta-tus of the child receiving mechanical ventilation. Manychildren are sedated while intubated and all will have anasogastric tube in place to decompress the stomach (seeTradition or Science 16–1). Perform suctioning based onthe presence of adventitious breath sounds, increased re-spiratory effort or distress, or both. Chest physiotherapymay be ordered to further promote removal of secretions.Provide oral care and ensure the intubation tube is notcausing skin irritation around the mouth or nares. Ensurethe ventilator alarms are on and set within acceptable pa-rameters to provide early notification of distress. Assistthe family and, as appropriate, the child to understand
Airway Clearance Techniqueand Description Benefits/Advantages Disadvantages/Problems
Exercise:Any activity that requires physical
exertion, endurance, and upperbody strengthening
May not cost anythingMay apply in many situationsSocially acceptableMay also improve cardiovascular
fitness, self-esteem, and generalhealth
May cost for membership to clubs orgyms; depends on climate
Limited to physical abilityChildren with preexisting conditions
such as asthma (with exercise com-ponent) may need to observe specialprecautions when exercising (e.g.,premedicate)
Flutter valve:Small pipelike device with a metal
ball rotating freely within pipePatients inhale and actively exhale
through the pipe, which generatespositive pressure to about 15 to 25cm H2O. Oscillations are trans-mitted to airways. Done for 5 to15 breaths, followed by two tothree huffs through flutter untillungs are clear, or for 20 minutes.
Enables independenceRequires cooperation
Requires purchase of the device
Figure 16—8. Postural drainage and percussion is used to assist withexpulsion of mucus from the airway.
Figure 16—9. Child being ventilated using the bag-and-masktechnique.
Chapter 16 n n The Child With Altered Respiratory Status 669

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:34 User ID: muralir 1BlackLining Disabled
the rationale for the use of mechanical ventilation. Asappropriate, provide medications to help the child remaincalm and quiet while being ventilated, which will ensureoptimal respiratory outcomes.
TracheostomyA tracheostomy consists of the surgical placement of anartificial airway directly into the trachea below the lar-ynx. Many conditions that can cause upper airwayobstruction, respiratory failure, or prolonged intubationin children may have to be managed by placing a trache-ostomy tube. Emergencies such as epiglottis or foreign
body aspiration (FBA) may require a tracheostomy formore short-term management. In some clinical condi-tions such as laryngotracheomalacia, subglottic stenosis,or vocal cord paralysis, the tracheostomy may be longterm, until the condition is outgrown or corrected. More-over, with some cases, such as in chronic respiratory failurewith long-term mechanical ventilation, the tracheostomymay be permanent.
Tracheostomy tubes are made of Silastic, silicone, ormetal and are available in various sizes and lengths. Theappropriate size is determined by patient age and size.Single-cannula tracheostomy tubes are most commonlyused in pediatric patients, because they have a smallerinner diameter and are usually made of Silastic, whichconforms better than other materials to the shape of thetrachea. For older children, a tracheostomy tube with aninner cannula may be used. The inner cannula is removedfor cleaning, while the outer cannula is left in place.Additionally, some tracheostomy tubes have externalcuffs. Most pediatric tubes do not have an external cuffbecause of the child’s small airway diameter and theincreased risk of trauma to the airway caused by the cuff.Because cuffless single-cannula tracheostomy tubes areused in most children, explanation of the nursing carefocuses on these.
While the child is hospitalized, nursing care involvespreparing child and family preoperatively, providingskilled nursing care and observation postoperatively,and facilitating a successful discharge plan for homemanagement if the tracheostomy will be long term.Preoperatively, explain to the child and parents why thetracheostomy tube is needed, what the basic anatomyand physiology of the airway are, how breathing will bedifferent, what to expect postoperatively, and how thechild will look when he or she returns from surgery. Ifpossible, allow the family to see a tracheostomy tubeand supplies to help decrease anxiety about what toexpect.
Focus postoperative nursing care on close observa-tion to maintain a patent airway and to monitor forpossible complications such as hemorrhage, edema, sub-cutaneous emphysema, pneumothorax, and accidentaldecannulation. Because infants and children are atgreater risk for tracheostomy obstruction related to therelatively smaller airway, they should be initially man-aged in an intensive care or close observation unitpostoperatively.
Respiratory assessments include vital signs and exami-nation of the child’s color, respiratory rate and effort,breath sounds, and type and amount of secretions. Forthe first 5 to 6 days, until the tracheocutaneous tract iswell formed, long sutures (stay sutures) attached to thetrachea are taped to the chest. The sutures can be used to
Figure 16—10. An intubated child. The tube has not yet beensecured in place.
Tradition or Science 16—1
Does infant position affect outcomes of newborninfants receiving mechanical ventilation?
MORE INQUIRY
NEEDEDMORE INQUIRY
NEEDEDIn patients of different ages undergoingmechanical ventilation, research has
indicated that particular positions, such as the prone posi-tion, may improve respiratory parameters. Clinical trialsassessing the position of neonates receiving mechanicalventilation have not substantiated that any particularbody position during mechanical ventilation producessustained and relevant improvements in oxygenation.The prone position has been found to slightly improve ox-ygenation in neonates receiving mechanical ventilation;however, more research is needed to determine the vari-ous risks and benefits associated with different layingpositions for this population of ventilated patients (Bala-guer, Escribano, & Roque, 2003).
Alert! All children with a tracheostomy should have an extra tracheos-tomy tube of the same size available at the bedside in case the tube in place isdislodged or becomes obstructed and cannot be cleared.
670 Unit 3 n n Managing Health Challenges

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:34 User ID: muralir 1BlackLining Disabled
keep the stoma open in the event of an accidental decan-nulation. The surgeon removes the sutures when thetract in the trachea is formed.
The airway must remain patent to prevent obstruc-tion and possible complications. The child may requirefrequent suctioning for several hours immediately afterthe procedure, because excessive and sometimes bloodysecretions are common. Provide suctioning on an as-needed basis thereafter to prevent occlusion of the tra-cheostomy tube by secretions and mucous plugs. Toprevent complications of suctioning, such as hypoxemia,hypotension, bradycardia (vasovagal responses), laryng-ospasm, bronchospasm, atelectasis, and trauma to theairway, gauge the suction pressure (should be 80–100mm Hg), limit the time for suctioning (no longer than4–5 seconds) and the number of suction passes, monitorthe depth of the suction catheter (1=4–1=2 inch [.635 to1.27 cm] beyond the tip of the length of the airway), andprovide manual ventilation with oxygen, rest timebetween suction passes, or both.
caREmindercaREminderDo not instill saline prior to suctioning. Studies do notdemonstrate the efficacy of normal saline in thinning mucussecretions. Studies have shown that instilling saline beforesuctioning has an adverse effect on oxygen saturation, whichmay last up to 5 minutes. Also, instilling saline duringsuctioning dislodges bacteria into the lower airway.
The functions of warming, filtering, and humidifyinginspired air that the upper respiratory tract normally per-forms are bypassed in a child with a tracheostomy. There-fore, the inspired air must be humidified and warmed tomaintain loose secretions, prevent occlusion of the tubeby secretions, and prevent drying of the tracheal mucosa.Nursing care is directed toward maintaining appropriatehumidification via a mist collar. In addition, promotingadequate fluid intake to keep the child well hydrated isimportant. To prevent infection and irritation of the skinaround the tracheostomy tube, provide stoma care tokeep the skin clean and dry. Gently remove the secretionsaround the stoma, using gauze pads soaked with half-strength hydrogen peroxide followed by gauze padssoaked with sterile water. Keep the tracheostomy tiesclean and dry, and change them daily and as needed whensoiled.
The schedule of tracheostomy tube changes variesdepending on the institution or physician preference.The first tube change usually is done by the surgeonabout 5 days after the tracheotomy is performed. Subse-quent tube changes are generally performed once a weekin the child with a well-healed tracheostomy stoma, usu-ally before a feeding or meal to avoid stimulation thatcould cause emesis.
Because many children go home with tracheostomytubes, it has become necessary to teach parents or otherprimary caregivers how to care for the child at home(Fig. 16–11). TIP 16–2 outlines a teaching plan for the
child who has had a tracheostomy tube placed. It is alsohelpful to ensure that visiting nursing is provided afterdischarge to assist the family with routine care.
Nursing Plan of Care for
the Child With Altered
Respiratory Status
Question: One nursing diagnosis for Jose is: Inef-fective breathing pattern related to respiratory disease
process. Based on the information in the case study, what isanother important nursing diagnosis?
Health promotion and disease prevention activities areessential for infants, children, and adolescents with acuteand chronic respiratory conditions. These activitiesshould focus on promoting a child’s growth and develop-ment, and on adequate home management. Preventivecare, monitoring and early detection of symptoms,adequate management (home vs. hospital), and health edu-cation are critical components of respiratory care for chil-dren. For example, sedentary lifestyles and obesity havegrown to epidemic proportions in this country. Healthpromotion and disease prevention activities that focus ondeveloping and encouraging healthy lifestyles can lead toimprovements in overall health, as well as specificallyenhancing respiratory functioning. Therefore, nursingcare in these areas can reduce the risk for complications,exacerbations of respiratory conditions (e.g., asthmaattacks), morbidity (e.g., hospitalizations, emergency roomvisits, school days missed), and development of comorbidconditions related to the child’s preexisting condition. Itcan also reduce or prevent the recurrence of respiratoryillnesses.
Multiple nursing diagnoses may be used to addressaltered respiratory function and status (Nursing Plan ofCare 16–1). For example, ineffective breathing pattern
Figure 16—11. Caregivers should be given ample opportunity totake care of the child’s tracheostomy before the child is discharged.
Chapter 16 n n The Child With Altered Respiratory Status 671
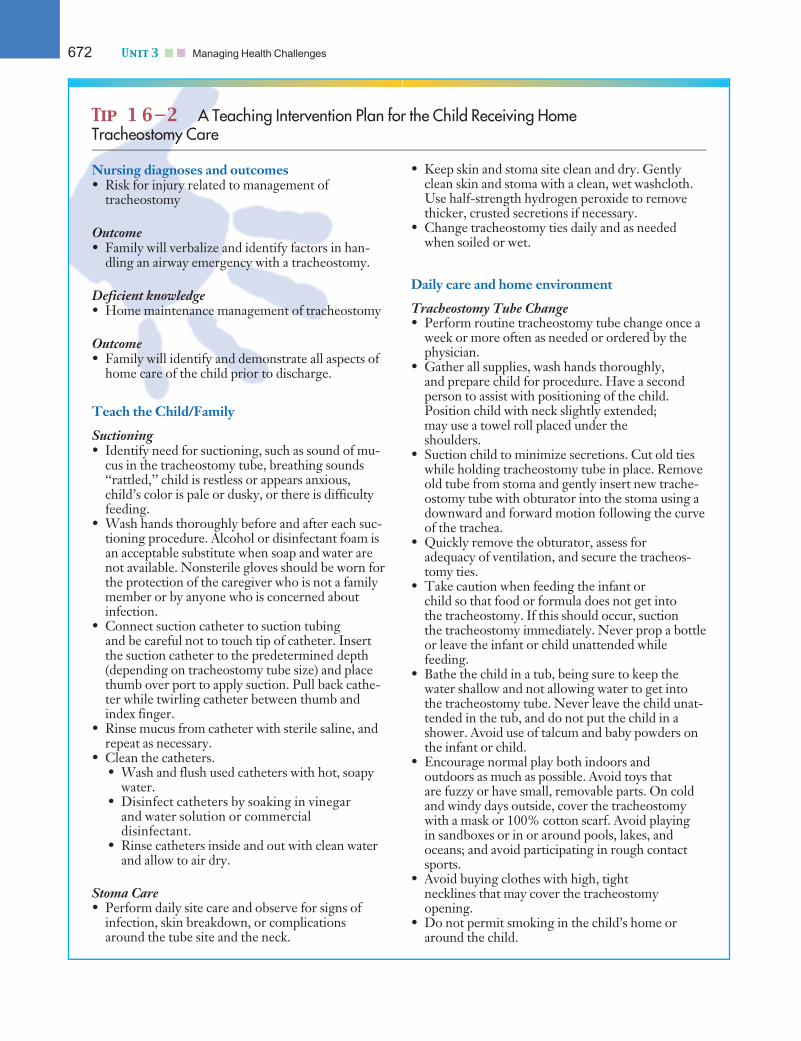
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:35 User ID: muralir 1BlackLining Disabled
Tip 1 6—2 A Teaching Intervention Plan for the Child Receiving HomeTracheostomy Care
Nursing diagnoses and outcomes• Risk for injury related to management of
tracheostomy
Outcome• Family will verbalize and identify factors in han-
dling an airway emergency with a tracheostomy.
Deficient knowledge• Home maintenance management of tracheostomy
Outcome• Family will identify and demonstrate all aspects of
home care of the child prior to discharge.
Teach the Child/Family
Suctioning• Identify need for suctioning, such as sound of mu-
cus in the tracheostomy tube, breathing sounds‘‘rattled,’’ child is restless or appears anxious,child’s color is pale or dusky, or there is difficultyfeeding.
• Wash hands thoroughly before and after each suc-tioning procedure. Alcohol or disinfectant foam isan acceptable substitute when soap and water arenot available. Nonsterile gloves should be worn forthe protection of the caregiver who is not a familymember or by anyone who is concerned aboutinfection.
• Connect suction catheter to suction tubingand be careful not to touch tip of catheter. Insertthe suction catheter to the predetermined depth(depending on tracheostomy tube size) and placethumb over port to apply suction. Pull back cathe-ter while twirling catheter between thumb andindex finger.
• Rinse mucus from catheter with sterile saline, andrepeat as necessary.
• Clean the catheters.• Wash and flush used catheters with hot, soapy
water.• Disinfect catheters by soaking in vinegar
and water solution or commercialdisinfectant.
• Rinse catheters inside and out with clean waterand allow to air dry.
Stoma Care• Perform daily site care and observe for signs of
infection, skin breakdown, or complicationsaround the tube site and the neck.
• Keep skin and stoma site clean and dry. Gentlyclean skin and stoma with a clean, wet washcloth.Use half-strength hydrogen peroxide to removethicker, crusted secretions if necessary.
• Change tracheostomy ties daily and as neededwhen soiled or wet.
Daily care and home environment
Tracheostomy Tube Change• Perform routine tracheostomy tube change once a
week or more often as needed or ordered by thephysician.
• Gather all supplies, wash hands thoroughly,and prepare child for procedure. Have a secondperson to assist with positioning of the child.Position child with neck slightly extended;may use a towel roll placed under theshoulders.
• Suction child to minimize secretions. Cut old tieswhile holding tracheostomy tube in place. Removeold tube from stoma and gently insert new trache-ostomy tube with obturator into the stoma using adownward and forward motion following the curveof the trachea.
• Quickly remove the obturator, assess foradequacy of ventilation, and secure the tracheos-tomy ties.
• Take caution when feeding the infant orchild so that food or formula does not get intothe tracheostomy. If this should occur, suctionthe tracheostomy immediately. Never prop a bottleor leave the infant or child unattended whilefeeding.
• Bathe the child in a tub, being sure to keep thewater shallow and not allowing water to get intothe tracheostomy tube. Never leave the child unat-tended in the tub, and do not put the child in ashower. Avoid use of talcum and baby powders onthe infant or child.
• Encourage normal play both indoors andoutdoors as much as possible. Avoid toys thatare fuzzy or have small, removable parts. On coldand windy days outside, cover the tracheostomywith a mask or 100% cotton scarf. Avoid playingin sandboxes or in or around pools, lakes, andoceans; and avoid participating in rough contactsports.
• Avoid buying clothes with high, tightnecklines that may cover the tracheostomyopening.
• Do not permit smoking in the child’s home oraround the child.
672 Unit 3 n n Managing Health Challenges

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:35 User ID: muralir 1BlackLining Disabled
may be used to describe a child in respiratory distressrelated to an asthma exacerbation (asthma attack). Respi-ratory distress in children also may lead to correlatingproblems in other body systems (e.g., cardiac, immune).In addition, many respiratory conditions are chronic.Refer back to Nursing Plan of Care 12–1 for a summaryof the diagnosis and care interventions for the child witha chronic condition. The nurse’s plan of care shouldencompass all primary and secondary effects of the child’srespiratory illness.
Answer: Based on the information that Jose’soxygen saturation is between 89% to 90%, another
nursing diagnosis is: Impaired gas exchange related tounderlying respiratory disease process.
Alterations in Respiratory
Status
Respiratory conditions are among the most commonmaladies affecting children, ranging from those that de-velop in utero, such as malformations of the palate andtrachea, to chronic conditions such as asthma. Respira-tory health directly affects children’s stamina and theirability to engage in activities in settings that are condu-cive to safe air exchange. The nurse plays a primaryrole in educating children and their families about waysto safeguard their respiratory health. In addition, thenurse plays a critical role in determining if and when achild’s respiratory condition may place other children at
risk for infection. Thus, the role of the nurse is both tocollaborate in improving the health of children with arespiratory condition and to protect the health of chil-dren who may be exposed to contagious respiratoryconditions.
Congenital Abnormalities of the
Respiratory System
Congenital abnormalities or malformations of the respi-ratory systems are fortunately rare. These disordersresult in respiratory dysfunction primarily caused by air-way obstructions or collapse. Congenital conditionsinclude choanal atresia (a unilateral or bilateral bony ormembranous septum between the nose and pharynx),Pierre Robin syndrome (abnormally small jaw withupper airway obstruction [resulting from tongue pro-lapse into the pharyngeal airway] and cleft palate; Fig.16–12), laryngomalacia (weakness and poor tone of thelarynx), and tracheomalacia (weakness and poor tone ofthe trachea).
These abnormalities are generally diagnosed at birthor shortly thereafter, when the child exhibits varyingdegrees of respiratory distress. The presence of cyanosis(bluish skin color caused by inadequate oxygenation ofthe blood) is a key finding. The treatment is largely sup-portive; the primary goal of treatment is to maintaina patent airway. Surgical interventions to relieve theobstruction (such as for choanal atresia) or structurallysupport the airway (such as for severe tracheomalacia)may be necessary. Adequate nutritional support to promote
Safety and emergency care• Change or replace the tracheostomy tube immedi-
ately if accidental dislodgment or occlusion of thetube should occur.
• Keep all emergency telephone numbers bythe telephone and a copy with the family at alltimes.
• Have all necessary equipment (e.g., extra tracheos-tomy tube with ties, suction machine, catheters,Ambu bag) with child when traveling or going on‘‘outings’’ outside the home.
• Keep flashlight handy in case of power failure, andnotify electric and telephone companies that thereis a child with special healthcare life-sustainingneeds in the home.
• Keep all immunizations up to date.• Check tension on tracheostomy ties daily. Trache-
ostomy ties should be tight enough to allow thesmallest finger to be slipped underneath. Twill tapetracheostomy ties can stretch after being initiallysecured, so recheck in 1 to 2 hours for appropriatetightness.
• Place tracheostomy tie knots on the side of theneck to prevent skin breakdown on the back of theneck.
Contact Healthcare Provider if:• Child develops fever more than 101 �F
(38.3 �C)• Child is having difficulty breathing or the breath-
ing pattern changes• Child’s lips or nail beds become bluish or dusky• Child has increase in secretions or change in color,
odor, or consistency of the secretions• Blood (greater than a teaspoon) is leaking from the
tracheostomy• There is difficulty inserting the tube with a routine
tracheostomy tube change• There is a rash, drainage, or unusual odor around
the tracheostomy stoma, or food or formula iscoming through the tracheostomy tube
Chapter 16 n n The Child With Altered Respiratory Status 673
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:35 User ID: muralir 1BlackLining Disabled
Nursing Plan of Care 16—1: Care of the ChildWith Altered
Respiratory Status
Nursing Diagnosis: Ineffective airway clearancerelated to excess thick secretions, obstruction, orinfection
Interventions/Rationale• Conduct a complete respiratory assessment with
each routine vital sign check and as indicated bythe child’s condition.
Enables early detection and correction of abnormal-ities. Thick secretions increase hypoxia and will bereflected by changes in respiratory status. Colored orodorous secretions may indicate bleeding or infections.
• Encourage child to cough, especially after respira-tory treatments. Teach effective cough techniques.
Ineffective cough may be caused by respiratory musclefatigue, severe bronchospasm, and/or thick, tenacioussecretions.
• Provide humidified oxygen as ordered.Decreases viscosity of secretions.
• Encourage increased fluid intake (clear liquids;avoid dairy products) if no contraindications, suchas cardiac or renal disease, are present.
Fluid intake prevents dehydration from insensiblelosses through mouth breathing and increased respira-tory rate. Assists to decrease viscosity of secretions andincrease ciliary action to remove secretions.
• Administer prescribed medications and intrave-nous fluids, monitor for response and side effects.
Intravenous fluids help to maintain adequate hydra-tion. Mucolytic agents, bronchodilators, and antibioticsmay be used to increase effectiveness of cough, enhancework of breathing, and treat infections that may causethick, tenacious secretions.
Expected Outcomes• Child’s airway will be free of secretions, as evi-
denced by normal or improved breathing, normalarterial blood gases, and/or oxygen saturation92% or greater on pulse oximetry.
Nursing Diagnosis: Ineffective breathing patternrelated to effects of respiratory disease process
Interventions/Rationale• Conduct a complete respiratory assessment with
each routine vital sign check and as indicated bythe child’s condition.
Enables early detection and correction of abnormal-ities. Hypoxemia, hypercapnia, and hypocapnia willcause breathing pattern changes as the autonomic nerv-ous system attempts to maintain homeostasis.
• Provide oxygen as needed to the child to maintainoxygen saturation at more than 92% or within pa-rameters defined as child’s personal best.
Oxygen therapy may be required to increase oxygensaturation. A decrease in saturation indicates ineffec-tive oxygenation, which in turn increases the work ofbreathing.
• Place child in an upright position to optimizeventilation.
Partial pressure of arterial oxygen may increase inthe prone position.
• Provide reassurance to the child and allay anxiety.Keep child as calm as possible.
Increased restlessness and anxiety indicate insuffi-cient oxygenation. Increased work of breathing can leadto fatigue. Energy expenditures increase the child’s oxy-gen demands.
• Administer prescribed medications and intrave-nous fluids; monitor for response and side effects.
Steroids may help reduce bronchial inflammation,antibiotics may be used to treat infection or sepsis, andbronchodilators maybe useful to enhance airway clearance.
Expected Outcomes• Child will demonstrate an effective respiratory
rate, rhythm, and effort, and will experienceimproved gas exchange in the lungs, as evi-denced by blood gases within child’s normalparameters.
• Child will verbalize ability to breathe comfortablywithout sensations of dyspnea and related feelingsof fear or anxiety resulting from shortness ofbreath.
Nursing Diagnosis: Impaired gas exchange relatedto consequences of underlying respiratory diseaseprocess
Interventions/Rationale• Conduct a complete respiratory assessment with
each routine vital sign check and as indicated bythe child’s condition.
Signs of hypoxia, such as changes in level of con-sciousness, cyanosis, effortful breathing, ventilation(rate, quality, pattern, and depth), and vital signs indi-cate impaired gas exchange and compensatory efforts tomanage these physiologic changes.
• Closely monitor oxygen saturation levels via pulseoximetry and arterial blood gases, and note changes.
Pulse oximetry provides an estimate of oxygen satu-ration; blood gases (arterial or capillary) are objectiveindications of oxygenation status. Progressive hypoxe-mia is apparent on serial blood gases despite increasedconcentrations of inspired oxygen.
• Provide oxygen as needed to the child to maintainoxygen saturation at more than 92% or in parame-ters defined as child’s personal best.
674 Unit 3 n n Managing Health Challenges
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:35 User ID: muralir 1BlackLining Disabled
Oxygen therapy may be required to increase oxygensaturation. A decrease in saturation indicates ineffec-tive oxygenation, which may indicate that the child’scondition is worsening.
• Anticipate the need for intubation and mechanicalventilation. Assist with these procedures as needed.
Intubation is indicated in the presence of impendingrespiratory failure. Mechanical ventilation providessupportive care to maintain adequate oxygenation andventilation parameters to the child.
Expected Outcomes• Child will demonstrate improved gas exchange in
the lungs, as evidenced by blood gases within child’snormal parameters and an alert, responsive mentalstatus or no further reduction in mental status.
Nursing Diagnosis: Decreased cardiac outputrelated to consequences of respiratory distress andfailure
Interventions/Rationale• Perform a complete assessment of cardiovascular
status including vital signs, hemodynamic pres-sures, urine output, skin temperature, peripheralpulses, and respiratory effort.
Decreasing cardiac output will be reflected bychanges in blood pressure, decreasing strength of pe-ripheral pulses, decreased urine output, cool extremities,and changes in ventilation that may necessitate changesin positive end-expiratory pressure.
• Administer prescribed medications and intrave-nous fluids; monitor for response and side effects.
Inotropic agents may be used to increase cardiac out-put. Sedatives and analgesics are used to relieve painand agitation. Neuromuscular blocking agents may beneeded if the child is ventilated, to promote synchronousbreathing. Intravenous fluids are administered tomaintain fluid balance without causing edema.
Expected Outcomes• Child will demonstrate adequate cardiac output, as
evidenced by strong peripheral pulses; normalvital signs; urine output greater than 2 mL/kg/hour; and warm, pink, dry skin.
Nursing Diagnosis: Risk for infection related topooling of lung secretions, ineffective cough andcontagious nature of condition
Interventions/Rationale• Conduct a complete assessment to monitor for re-
spiratory infection, including auscultating breathsounds; evaluating for changes in sputum; andobserving for fever, chills, increase in cough,shortness of breath, nausea, vomiting, diarrhea,and decreased appetite.
Early assessment of signs of infection will facilitateearly intervention. Bronchial breath sounds and ralesmay indicate pneumonia. Sputum changes such as an
increase in production, changes in consistency, andchanges in color may indicate presence of infection.
• Evaluate child’s and family’s understanding oftechniques to prevent infection, such as carefulhand hygiene, adequate rest and nutrition, avoid-ing contact with sick individuals, and so forth.Provide additional education as needed.
Increased knowledge and subsequent implementationof activities to prevent infection will reduce infection risk.
• Follow standard infection control precautionsduring all contact with the child.
Standard precautions reduces the risk of transmis-sion of microorganisms.
• Encourage child to cough and expectorate secre-tions frequently. Encourage strict handwashingand infection control practices for the child, familymembers, and all care providers.
Retained secretions provide an environment for bac-terial growth.
Expected Outcomes• Child will be free from infection, and the parents
will demonstrate adequate knowledge of risk forinfection, signs/symptoms of infection, and meas-ures to reduce infection risks.
Nursing Diagnosis: Imbalanced nutrition: Less thanbody requirements related to underlying chroniclung disease and increased work of breathing
Interventions/Rationale• Assess child’s nutritional status, including height,
weight, body mass index percentile, diet history,child’s ability to eat, and possible causes for poorappetite.
Assessment provides baseline data to assist in deter-mining interventions. Increased metabolic needs causedby increased work of breathing will require greater ca-loric intake. Work of breathing may leave little energyfor other activities, including eating.
• Assist child/parents to plan well-balanced mealsthat incorporate child’s food preferences and die-tary limitations imposed by disease process (e.g.,low-to-moderate fat, high-protein, high-caloriemeals for the child with cystic fibrosis). Encouragesmall feedings of nutritious soft foods and liquids.Add nutritional supplements as ordered.
These measures minimize metabolic expenditureswhile providing nutritious high-calorie foods that areappealing and easy to digest.
• Ensure frequent oral care is provided.Dry mucous membranes and poor oral hygiene may
contribute to decreased appetite and worsening nutri-tional status.
Expected Outcomes• Child will demonstrate adequate nutritional intake
for age, and parents will identify steps to achieveand maintain ideal body weight.
Chapter 16 n n The Child With Altered Respiratory Status 675

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:35 User ID: muralir 1BlackLining Disabled
optimal weight gain is a key intervention. These condi-tions improve with growth, and in the absence of othercongenital anomalies, the prognosis for normalrespiratory function is good.
Early and ongoing support and education of the parentsis of utmost importance. A diagnosis of a congenital anom-aly creates a crisis for the family. Reinforce the conceptthat in most cases the cause of the defect is unknown andnot the fault of the parents. Also educate the family aboutappropriate positioning and feeding techniques to ensureadequate intake of formula or breast milk (either by actualbreast-feeding or breast milk expressed into a bottle) andsolid foods as the infant reaches the appropriate age forintroducing them. Routine infant healthcare is adminis-tered. Parents need to be informed that the infant’s symp-toms may worsen during respiratory illnesses. If they haveany concern about worsening respiratory distress, instructthem to seek assistance from their healthcare professional.Parents should also be instructed in CPR.
Upper Respiratory Infections
and Obstructions
Upper respiratory tract infections are extremely commonin infants and young children. The upper respiratorytract, or upper airway, consists primarily of the nose,mouth, and oropharynx. For purposes of this book, infec-tions of the epiglottis, larynx, and trachea are consideredin the upper respiratory tract as well. Infections of thisarea of the respiratory system are usually viral and self-limiting. Although the respiratory tract is equipped withseveral natural defense mechanisms, invading organismsfrequently gain access to these structures, resulting in
respiratory conditions that range from mild to life threat-ening. When infection occurs, organisms travel freelyamong the structures of the upper airway, includingthrough the eustachian tubes to the inner and middleears. The severity of resulting illness depends on age, or-ganism, and the integrity of the child’s immune response.Some infections can lead to inflammation or obstructionsof the airway; obstruction can also result from noninfec-tious causes. Most upper respiratory conditions aretreated in the home or in ambulatory care settings.
Allergic Rhinitis
Question: As described in the Chapter 9 casestudy, Jose has seasonal allergies that trigger his
asthma. Summarize the relationship between children withallergic rhinitis and children with asthma.
Allergic rhinitis is a condition characterized by sneezing;nasal itching; thin, watery rhinorrhea; and nasal conges-tion. The conjunctivae and posterior pharynx may also beinvolved. Allergic rhinitis may be seasonal, with symptomsthat correspond to specific pollen peaks in the spring orfall, or may be perennial (year-round symptoms). Somechildren have perennial symptoms with additional flaresduring pollen seasons. Allergic rhinitis is the most com-mon of all allergic disorders, affecting 10% to 20% of thepopulation. Allergic rhinitis accounts for 2 million dayslost from school, 28 million days of restricted activity, anda cost of more than $3.3 billion for physician visits annu-ally (Blaiss, 2004; Gleason et al., 2006, Hayden, 2007, Salibet al., 2008). The prognosis for allergic rhinitis is good ifsymptoms are controlled with treatment.
PathophysiologyAirborne allergens come into contact with mast cells andbasophils at mucosal surfaces. Mast cells have immuno-globulin E (IgE) receptors on their membrane surfacesthat bind to IgE in serum. Exposure to the appropriateairborne allergens cross-links the mast cell IgE receptorsand triggers the release of chemical mediators. This me-diator release causes an immediate reaction, whichincludes sneezing, itching, nasal congestion, and mucussecretion accompanied by nasal mucosa edema. Four to12 hours later, a late-phase reaction occurs, causing a sec-ond, more prolonged period of nasal congestion.
AssessmentDiagnosis of allergic rhinitis is based on clinical history,family history, physical findings, and laboratory (skintest) evaluation. Assess for complaints of nasal conges-tion, pruritus, clear rhinorrhea, and paroxysms of sneez-ing. The nasal congestion may be bilateral, unilateral, orvariable and is often worse at night. Chronic rhinitissymptoms may lead to irritability and fatigue, which cancause inattentiveness and difficulty concentrating inschool. Parents may tell you that their children sniff,
Figure 16—12. In the child with Pierre Robin syndrome, malforma-tion of the mandible makes the chin appear recessed and restricts thetongue to a posterior position, causing easy occlusion of the airway.A tracheostomy is necessary to maintain an open airway.
Alert! The infant with Pierre Robin syndrome must be maintained inthe prone position as much as possible to prevent the tongue from obstructingthe pharynx and causing respiratory distress. Improper positioning can quicklyresult in complete obstruction and death.
676 Unit 3 n n Managing Health Challenges

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:35 User ID: muralir 1BlackLining Disabled
snort, and frequently clear their throats. They may alsotwitch, pick or rub their nose, and have episodes of repet-itive sneezing. In conjunction with nasal symptoms, theeyes may itch and water. Bronchospasm with coughing,shortness of breath, or chest tightness may occur in chil-dren who also have asthma. Other symptoms may includefatigue, irritability, headache, depression, and anorexia.
A predisposition to allergic rhinitis is often familial;therefore, determining whether other family members(parents, siblings, or grandparents) have a history of hayfever or allergies can help make the diagnosis.
On physical examination, look for certain characteristicfeatures that distinguish allergic rhinitis from the com-mon cold (rhinitis) (Table 16–1). The child may havebluish discoloration of the infraorbital area (called allergicshiners), caused by increased venous flow related to thelocal allergic vigor. The child may have a transversecrease across the lower third of the nose caused by rub-bing the nose (called the allergic salute). Examination ofthe nasal cavity using a nasal speculum may reveal edema-tous mucosa, with swollen, boggy, and pale-pink to blue-gray turbinates. Nasal secretions are generally clear,watery, or white.
Microscopic examination of the nasal secretions revealsabundant eosinophils. Skin testing for sensitivity to aller-gens believed to contribute to the nasal symptoms mayhelp establish specific triggers for the allergy symptoms(e.g., dust mite, cat, dog, trees, grass, or ragweed).
Interdisciplinary InterventionsThe mainstay of treatment for allergic rhinitis is avoidingthe offending allergens. Environmental control measuresthat can help relieve symptoms by limiting exposure tocommon indoor allergens are shown in Community Care16–1. Parents of children with seasonal (pollen-induced)allergic rhinitis must be cautioned that pollen counts arehighest in the mornings between 5 and 10 AM. Environ-mental measures to reduce allergen exposure shouldinclude wet-mop dusting, closing household windows atleast during the allergy season, and frequently changingventilation filters. One may be able to further limit expo-sure by limiting household pets and making the homesmoke free.
Medical management involves the use of oral or intra-nasal antihistamines, decongestants, intranasal corticoste-roids, leukotriene modifiers, mast cell stabilizers, andallergen-specific immunotherapy (Blaiss, 2004; Gleasonet al., 2006). Antihistamines are used to block histaminefrom binding at its H1 receptor site, thereby preventingthe vasodilatation, sneezing, and hypersecretion it causes.Decongestants may be helpful in reducing nasal obstruc-tion through vasoconstriction, but the suitability of over-the-counter preparations for the younger child should beverified through the healthcare professional. Nasal corti-costeroids are used to decrease inflammation in the nasalpassages. For moderate to severe cases of allergic rhinitis,leukotriene modifiers and mast cell stabilizers may beused. In children with more severe symptoms, immuno-therapy may be used (Berger, 2004; Blaiss, 2004).
As with any medication, educate parents and childrenregarding the uses and side effects of these medications.Medications for rhinitis include sedating and nonsedatingforms. The availability of over-the-counter cold prepara-tions for children changes; therefore, instruct parents toread the package label carefully.
Answer: Although not all children who have aller-gic rhinitis also have asthma, a significant portion of chil-
dren who do have asthma also have allergies. The allergiescan act as a trigger for their asthma, and therefore controllingtheir allergic response also helps to control their asthma. Whatis difficult for many families is maintaining a preventative medi-cation regime when the child does appear sick.
SinusitisSinusitis in children is usually seen as a viral or bacterialinfection in the paranasal sinus structures. On the aver-age, children have about six to eight colds per year and,of these, 0.5% to 5% will develop into acute sinusitis(Ramaden, 2004). Sinusitis characteristically respondswell to antibiotic therapy, although prolonged coursesmay be required. Complications can occur as a result oflocal extension of the disease, such as orbital cellulitis. In-tracranial infection, with associated neurologic symp-toms, is also a potential sequela of sinusitis. Prompt,appropriate antibiotic therapy usually prevents the onsetof these potentially life-threatening ophthalmologic andneurologic complications.
PathophysiologyThe paranasal sinuses, which encompass the ethmoid,maxillary, sphenoid, and frontal sinuses, are hollowareas in the skull beneath the turbinates in the naso-pharynx. Ethmoid and maxillary sinuses are present atbirth. The sphenoid sinuses are formed by 5 years ofage, and frontal sinuses continue developing until ado-lescence (Figure 16–13). The various functions of thesinuses include warming and humidifying inspired air,trapping inspired particles, secreting mucus, and reduc-ing the weight of the skull.
T A B L E 1 6 —1
Differences Between Allergic Rhinitisand the Common Cold
Symptoms Allergic Rhinitis Common Cold
Family history of atopy Yes No
Conjunctival pruritus Yes No
Fever No Yes
Pharyngitis/laryngitis No Yes
Purulent secretions No Yes
Sinus pain Yes No
Chapter 16 n n The Child With Altered Respiratory Status 677
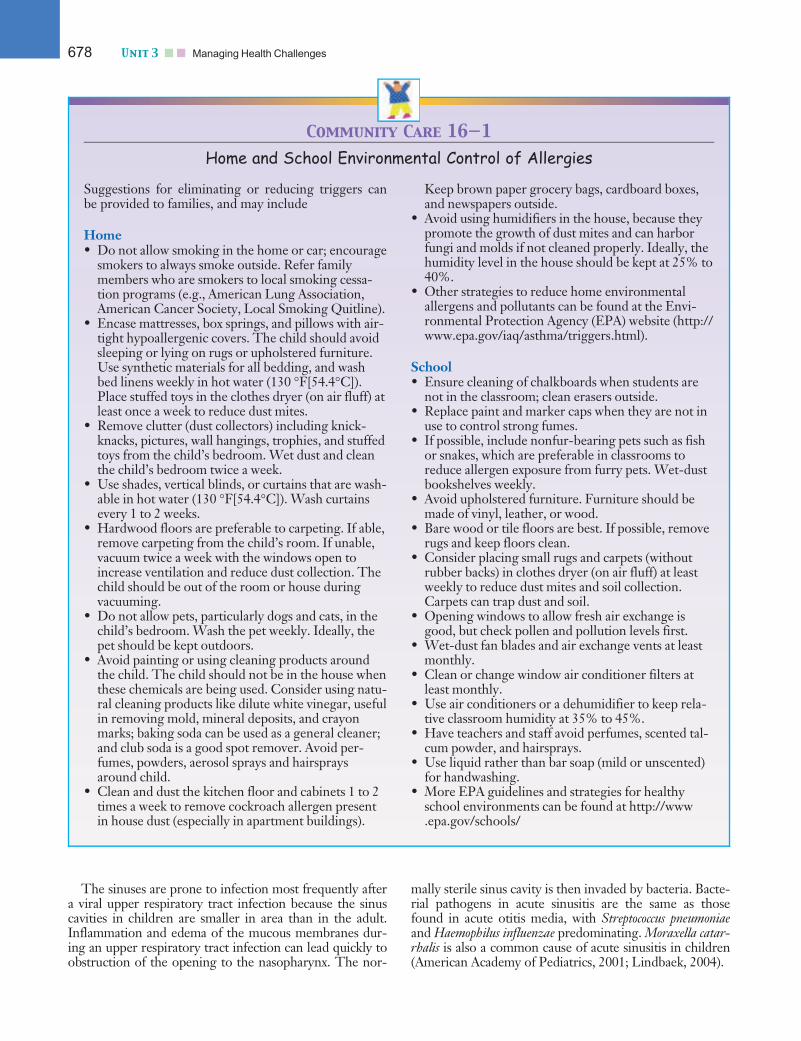
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:35 User ID: muralir 1BlackLining Disabled
The sinuses are prone to infection most frequently aftera viral upper respiratory tract infection because the sinuscavities in children are smaller in area than in the adult.Inflammation and edema of the mucous membranes dur-ing an upper respiratory tract infection can lead quickly toobstruction of the opening to the nasopharynx. The nor-
mally sterile sinus cavity is then invaded by bacteria. Bacte-rial pathogens in acute sinusitis are the same as thosefound in acute otitis media, with Streptococcus pneumoniaeand Haemophilus influenzae predominating. Moraxella catar-rhalis is also a common cause of acute sinusitis in children(American Academy of Pediatrics, 2001; Lindbaek, 2004).
Community Care 16—1
Home and School Environmental Control of Allergies
Suggestions for eliminating or reducing triggers canbe provided to families, and may include
Home• Do not allow smoking in the home or car; encourage
smokers to always smoke outside. Refer familymembers who are smokers to local smoking cessa-tion programs (e.g., American Lung Association,American Cancer Society, Local Smoking Quitline).
• Encase mattresses, box springs, and pillows with air-tight hypoallergenic covers. The child should avoidsleeping or lying on rugs or upholstered furniture.Use synthetic materials for all bedding, and washbed linens weekly in hot water (130 �F[54.4�C]).Place stuffed toys in the clothes dryer (on air fluff) atleast once a week to reduce dust mites.
• Remove clutter (dust collectors) including knick-knacks, pictures, wall hangings, trophies, and stuffedtoys from the child’s bedroom. Wet dust and cleanthe child’s bedroom twice a week.
• Use shades, vertical blinds, or curtains that are wash-able in hot water (130 �F[54.4�C]). Wash curtainsevery 1 to 2 weeks.
• Hardwood floors are preferable to carpeting. If able,remove carpeting from the child’s room. If unable,vacuum twice a week with the windows open toincrease ventilation and reduce dust collection. Thechild should be out of the room or house duringvacuuming.
• Do not allow pets, particularly dogs and cats, in thechild’s bedroom. Wash the pet weekly. Ideally, thepet should be kept outdoors.
• Avoid painting or using cleaning products aroundthe child. The child should not be in the house whenthese chemicals are being used. Consider using natu-ral cleaning products like dilute white vinegar, usefulin removing mold, mineral deposits, and crayonmarks; baking soda can be used as a general cleaner;and club soda is a good spot remover. Avoid per-fumes, powders, aerosol sprays and hairspraysaround child.
• Clean and dust the kitchen floor and cabinets 1 to 2times a week to remove cockroach allergen presentin house dust (especially in apartment buildings).
Keep brown paper grocery bags, cardboard boxes,and newspapers outside.
• Avoid using humidifiers in the house, because theypromote the growth of dust mites and can harborfungi and molds if not cleaned properly. Ideally, thehumidity level in the house should be kept at 25% to40%.
• Other strategies to reduce home environmentalallergens and pollutants can be found at the Envi-ronmental Protection Agency (EPA) website (http://www.epa.gov/iaq/asthma/triggers.html).
School• Ensure cleaning of chalkboards when students are
not in the classroom; clean erasers outside.• Replace paint and marker caps when they are not in
use to control strong fumes.• If possible, include nonfur-bearing pets such as fish
or snakes, which are preferable in classrooms toreduce allergen exposure from furry pets. Wet-dustbookshelves weekly.
• Avoid upholstered furniture. Furniture should bemade of vinyl, leather, or wood.
• Bare wood or tile floors are best. If possible, removerugs and keep floors clean.
• Consider placing small rugs and carpets (withoutrubber backs) in clothes dryer (on air fluff) at leastweekly to reduce dust mites and soil collection.Carpets can trap dust and soil.
• Opening windows to allow fresh air exchange isgood, but check pollen and pollution levels first.
• Wet-dust fan blades and air exchange vents at leastmonthly.
• Clean or change window air conditioner filters atleast monthly.
• Use air conditioners or a dehumidifier to keep rela-tive classroom humidity at 35% to 45%.
• Have teachers and staff avoid perfumes, scented tal-cum powder, and hairsprays.
• Use liquid rather than bar soap (mild or unscented)for handwashing.
• More EPA guidelines and strategies for healthyschool environments can be found at http://www.epa.gov/schools/
678 Unit 3 n n Managing Health Challenges
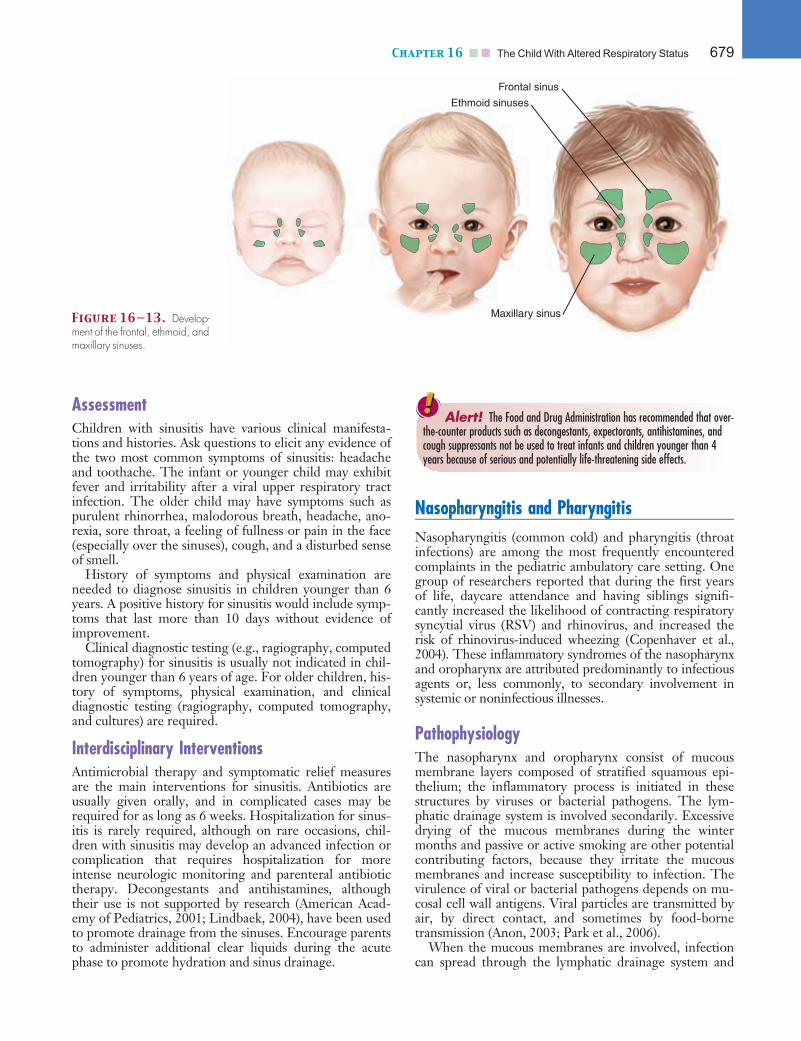
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:35 User ID: muralir 1BlackLining Disabled
AssessmentChildren with sinusitis have various clinical manifesta-tions and histories. Ask questions to elicit any evidence ofthe two most common symptoms of sinusitis: headacheand toothache. The infant or younger child may exhibitfever and irritability after a viral upper respiratory tractinfection. The older child may have symptoms such aspurulent rhinorrhea, malodorous breath, headache, ano-rexia, sore throat, a feeling of fullness or pain in the face(especially over the sinuses), cough, and a disturbed senseof smell.
History of symptoms and physical examination areneeded to diagnose sinusitis in children younger than 6years. A positive history for sinusitis would include symp-toms that last more than 10 days without evidence ofimprovement.
Clinical diagnostic testing (e.g., ragiography, computedtomography) for sinusitis is usually not indicated in chil-dren younger than 6 years of age. For older children, his-tory of symptoms, physical examination, and clinicaldiagnostic testing (ragiography, computed tomography,and cultures) are required.
Interdisciplinary InterventionsAntimicrobial therapy and symptomatic relief measuresare the main interventions for sinusitis. Antibiotics areusually given orally, and in complicated cases may berequired for as long as 6 weeks. Hospitalization for sinus-itis is rarely required, although on rare occasions, chil-dren with sinusitis may develop an advanced infection orcomplication that requires hospitalization for moreintense neurologic monitoring and parenteral antibiotictherapy. Decongestants and antihistamines, althoughtheir use is not supported by research (American Acad-emy of Pediatrics, 2001; Lindbaek, 2004), have been usedto promote drainage from the sinuses. Encourage parentsto administer additional clear liquids during the acutephase to promote hydration and sinus drainage.
Nasopharyngitis and PharyngitisNasopharyngitis (common cold) and pharyngitis (throatinfections) are among the most frequently encounteredcomplaints in the pediatric ambulatory care setting. Onegroup of researchers reported that during the first yearsof life, daycare attendance and having siblings signifi-cantly increased the likelihood of contracting respiratorysyncytial virus (RSV) and rhinovirus, and increased therisk of rhinovirus-induced wheezing (Copenhaver et al.,2004). These inflammatory syndromes of the nasopharynxand oropharynx are attributed predominantly to infectiousagents or, less commonly, to secondary involvement insystemic or noninfectious illnesses.
PathophysiologyThe nasopharynx and oropharynx consist of mucousmembrane layers composed of stratified squamous epi-thelium; the inflammatory process is initiated in thesestructures by viruses or bacterial pathogens. The lym-phatic drainage system is involved secondarily. Excessivedrying of the mucous membranes during the wintermonths and passive or active smoking are other potentialcontributing factors, because they irritate the mucousmembranes and increase susceptibility to infection. Thevirulence of viral or bacterial pathogens depends on mu-cosal cell wall antigens. Viral particles are transmitted byair, by direct contact, and sometimes by food-bornetransmission (Anon, 2003; Park et al., 2006).
When the mucous membranes are involved, infectioncan spread through the lymphatic drainage system and
Alert! The Food and Drug Administration has recommended that over-the-counter products such as decongestants, expectorants, antihistamines, andcough suppressants not be used to treat infants and children younger than 4years because of serious and potentially life-threatening side effects.
Figure 16—13. Develop-ment of the frontal, ethmoid, andmaxillary sinuses.
Frontal sinus
Ethmoid sinuses
Maxillary sinus
Chapter 16 n n The Child With Altered Respiratory Status 679
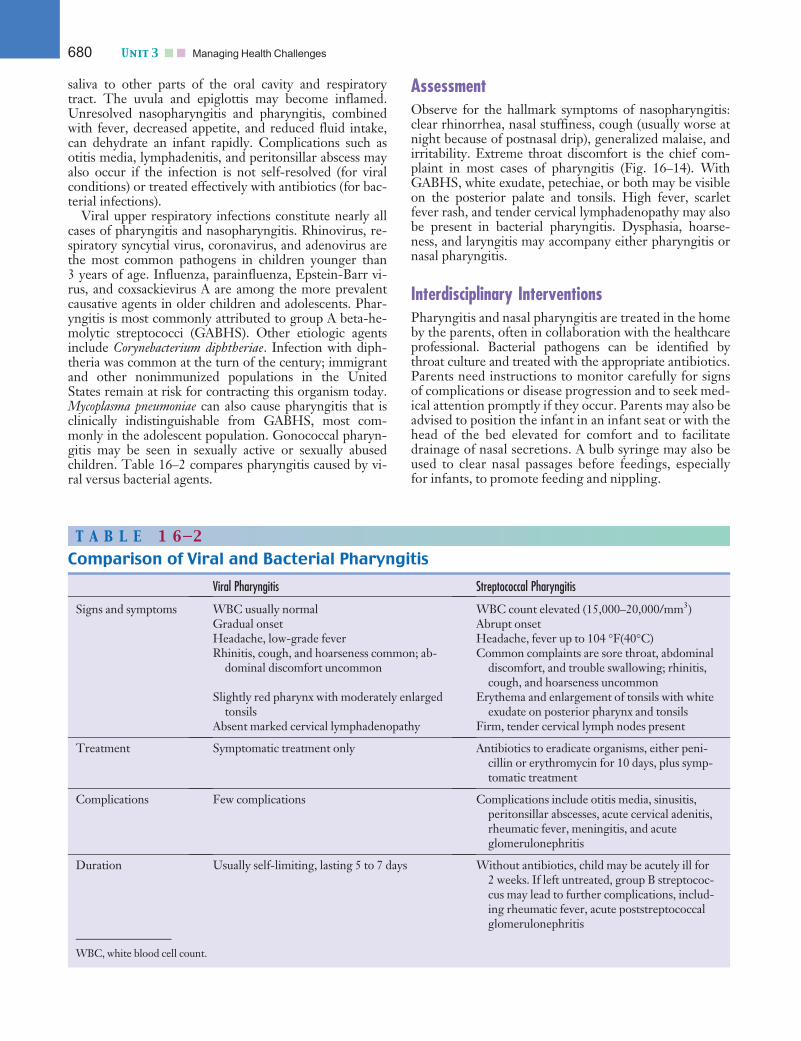
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:35 User ID: muralir 1BlackLining Disabled
saliva to other parts of the oral cavity and respiratorytract. The uvula and epiglottis may become inflamed.Unresolved nasopharyngitis and pharyngitis, combinedwith fever, decreased appetite, and reduced fluid intake,can dehydrate an infant rapidly. Complications such asotitis media, lymphadenitis, and peritonsillar abscess mayalso occur if the infection is not self-resolved (for viralconditions) or treated effectively with antibiotics (for bac-terial infections).
Viral upper respiratory infections constitute nearly allcases of pharyngitis and nasopharyngitis. Rhinovirus, re-spiratory syncytial virus, coronavirus, and adenovirus arethe most common pathogens in children younger than3 years of age. Influenza, parainfluenza, Epstein-Barr vi-rus, and coxsackievirus A are among the more prevalentcausative agents in older children and adolescents. Phar-yngitis is most commonly attributed to group A beta-he-molytic streptococci (GABHS). Other etiologic agentsinclude Corynebacterium diphtheriae. Infection with diph-theria was common at the turn of the century; immigrantand other nonimmunized populations in the UnitedStates remain at risk for contracting this organism today.Mycoplasma pneumoniae can also cause pharyngitis that isclinically indistinguishable from GABHS, most com-monly in the adolescent population. Gonococcal pharyn-gitis may be seen in sexually active or sexually abusedchildren. Table 16–2 compares pharyngitis caused by vi-ral versus bacterial agents.
AssessmentObserve for the hallmark symptoms of nasopharyngitis:clear rhinorrhea, nasal stuffiness, cough (usually worse atnight because of postnasal drip), generalized malaise, andirritability. Extreme throat discomfort is the chief com-plaint in most cases of pharyngitis (Fig. 16–14). WithGABHS, white exudate, petechiae, or both may be visibleon the posterior palate and tonsils. High fever, scarletfever rash, and tender cervical lymphadenopathy may alsobe present in bacterial pharyngitis. Dysphasia, hoarse-ness, and laryngitis may accompany either pharyngitis ornasal pharyngitis.
Interdisciplinary InterventionsPharyngitis and nasal pharyngitis are treated in the homeby the parents, often in collaboration with the healthcareprofessional. Bacterial pathogens can be identified bythroat culture and treated with the appropriate antibiotics.Parents need instructions to monitor carefully for signsof complications or disease progression and to seek med-ical attention promptly if they occur. Parents may also beadvised to position the infant in an infant seat or with thehead of the bed elevated for comfort and to facilitatedrainage of nasal secretions. A bulb syringe may also beused to clear nasal passages before feedings, especiallyfor infants, to promote feeding and nippling.
T A B L E 1 6—2
Comparison of Viral and Bacterial Pharyngitis
Viral Pharyngitis Streptococcal Pharyngitis
Signs and symptoms WBC usually normal WBC count elevated (15,000–20,000/mm3)Gradual onset Abrupt onsetHeadache, low-grade fever Headache, fever up to 104 �F(40�C)Rhinitis, cough, and hoarseness common; ab-
dominal discomfort uncommonCommon complaints are sore throat, abdominal
discomfort, and trouble swallowing; rhinitis,cough, and hoarseness uncommon
Slightly red pharynx with moderately enlargedtonsils
Erythema and enlargement of tonsils with whiteexudate on posterior pharynx and tonsils
Absent marked cervical lymphadenopathy Firm, tender cervical lymph nodes present
Treatment Symptomatic treatment only Antibiotics to eradicate organisms, either peni-cillin or erythromycin for 10 days, plus symp-tomatic treatment
Complications Few complications Complications include otitis media, sinusitis,peritonsillar abscesses, acute cervical adenitis,rheumatic fever, meningitis, and acuteglomerulonephritis
Duration Usually self-limiting, lasting 5 to 7 days Without antibiotics, child may be acutely ill for2 weeks. If left untreated, group B streptococ-cus may lead to further complications, includ-ing rheumatic fever, acute poststreptococcalglomerulonephritis
WBC, white blood cell count.
680 Unit 3 n n Managing Health Challenges
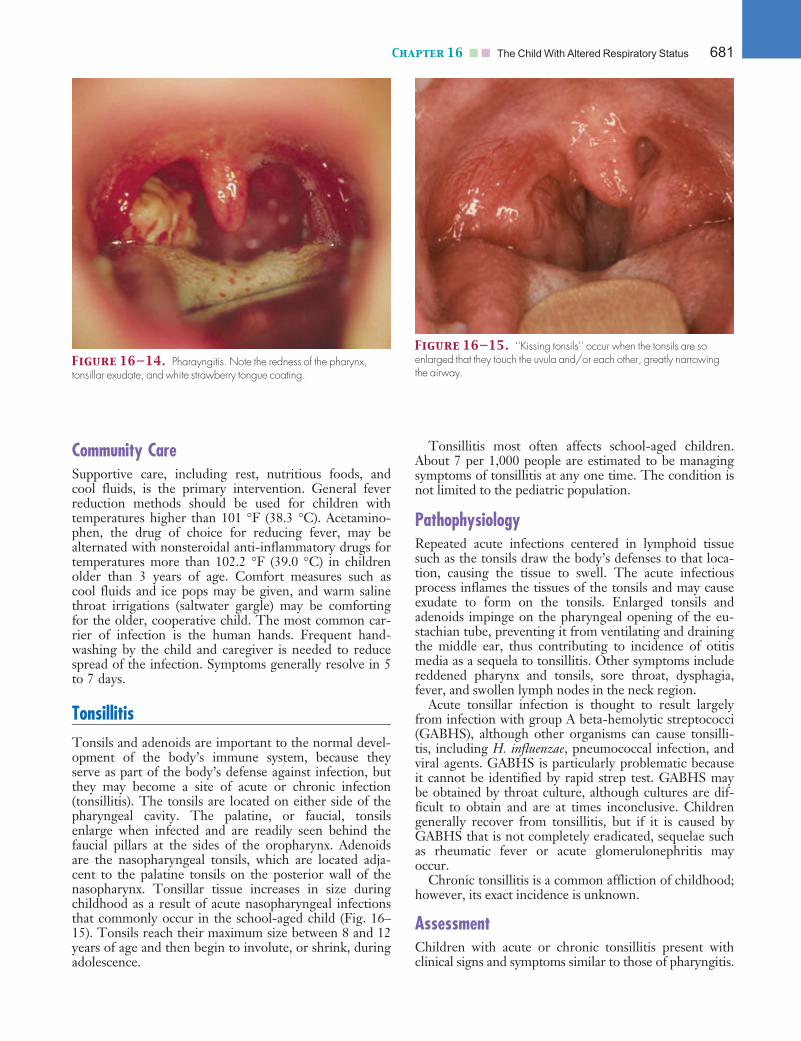
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:35 User ID: muralir 1BlackLining Disabled
Community CareSupportive care, including rest, nutritious foods, andcool fluids, is the primary intervention. General feverreduction methods should be used for children withtemperatures higher than 101 �F (38.3 �C). Acetamino-phen, the drug of choice for reducing fever, may bealternated with nonsteroidal anti-inflammatory drugs fortemperatures more than 102.2 �F (39.0 �C) in childrenolder than 3 years of age. Comfort measures such ascool fluids and ice pops may be given, and warm salinethroat irrigations (saltwater gargle) may be comfortingfor the older, cooperative child. The most common car-rier of infection is the human hands. Frequent hand-washing by the child and caregiver is needed to reducespread of the infection. Symptoms generally resolve in 5to 7 days.
TonsillitisTonsils and adenoids are important to the normal devel-opment of the body’s immune system, because theyserve as part of the body’s defense against infection, butthey may become a site of acute or chronic infection(tonsillitis). The tonsils are located on either side of thepharyngeal cavity. The palatine, or faucial, tonsilsenlarge when infected and are readily seen behind thefaucial pillars at the sides of the oropharynx. Adenoidsare the nasopharyngeal tonsils, which are located adja-cent to the palatine tonsils on the posterior wall of thenasopharynx. Tonsillar tissue increases in size duringchildhood as a result of acute nasopharyngeal infectionsthat commonly occur in the school-aged child (Fig. 16–15). Tonsils reach their maximum size between 8 and 12years of age and then begin to involute, or shrink, duringadolescence.
Tonsillitis most often affects school-aged children.About 7 per 1,000 people are estimated to be managingsymptoms of tonsillitis at any one time. The condition isnot limited to the pediatric population.
PathophysiologyRepeated acute infections centered in lymphoid tissuesuch as the tonsils draw the body’s defenses to that loca-tion, causing the tissue to swell. The acute infectiousprocess inflames the tissues of the tonsils and may causeexudate to form on the tonsils. Enlarged tonsils andadenoids impinge on the pharyngeal opening of the eu-stachian tube, preventing it from ventilating and drainingthe middle ear, thus contributing to incidence of otitismedia as a sequela to tonsillitis. Other symptoms includereddened pharynx and tonsils, sore throat, dysphagia,fever, and swollen lymph nodes in the neck region.
Acute tonsillar infection is thought to result largelyfrom infection with group A beta-hemolytic streptococci(GABHS), although other organisms can cause tonsilli-tis, including H. influenzae, pneumococcal infection, andviral agents. GABHS is particularly problematic becauseit cannot be identified by rapid strep test. GABHS maybe obtained by throat culture, although cultures are dif-ficult to obtain and are at times inconclusive. Childrengenerally recover from tonsillitis, but if it is caused byGABHS that is not completely eradicated, sequelae suchas rheumatic fever or acute glomerulonephritis mayoccur.
Chronic tonsillitis is a common affliction of childhood;however, its exact incidence is unknown.
AssessmentChildren with acute or chronic tonsillitis present withclinical signs and symptoms similar to those of pharyngitis.
Figure 16—14. Pharayngitis. Note the redness of the pharynx,tonsillar exudate, and white strawberry tongue coating.
Figure 16—15. ‘‘Kissing tonsils’’ occur when the tonsils are soenlarged that they touch the uvula and/or each other, greatly narrowingthe airway.
Chapter 16 n n The Child With Altered Respiratory Status 681

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:35 User ID: muralir 1BlackLining Disabled
Inspect for inflammation of the tonsils and surroundingtissues, accompanied by varying degrees of soreness ofthe mucosa. This soreness may cause the child to refuseto eat or drink because of discomfort on swallowing.Additional clinical manifestations include exudate on thetonsillar surface, substantial erythema, recurrent or per-sistent sore throat, and possible obstruction to swallow-ing or breathing caused by hypertrophied tonsils oradenoids. Occasionally, the throat may be dry and irri-tated, and the breath may be offensive. If the tonsils andadenoids are hypertrophied, determine whether they areobstructing the upper airway. This complication,although rare, can cause respiratory distress, withchronic hypoxia and the development of pulmonaryhypertension. Children with tonsils or adenoids that areso enlarged that they partially obstruct the upper airwayoften present as ‘‘mouth breathers’’ and often snore dur-ing sleep. Consider a sleep apnea evaluation for suchchildren.
Hypertrophy or acute infection of the tonsils must becarefully evaluated. Many apparently enlarged tonsilsare, in fact, normal in size. The misinterpretation arisesfrom the fact that, because of frequent nasopharyngealinfections, tonsils are normally larger during early child-hood years than later in life. Tonsils may virtually meetin the midline in some normal, asymptomatic children,especially when the child gags. Ascertain whether hyper-trophy, if present, is chronic or the result of a recentacute infection. Tonsils can increase in size tremen-dously with an acute infection and recede after the infec-tion subsides.
Inspect an older child’s tonsils simply by asking thechild to say ‘‘aaah.’’ If the child is unable to hold thetongue down, use a tongue blade lightly to help. Youngerchildren consider the examination of the mouth andthroat intrusive and may be uncooperative. Infants andyoung children whose cooperation cannot be gained willusually open their mouths during crying to allow a goodview of the oropharynx. If a tongue blade is needed, use itcautiously and quickly.
Interdisciplinary InterventionsWhen tonsillitis is present, it is necessary to screen forGABHS by culturing the tonsillar surface that may con-tain the exudate. A throat culture can be best obtainedusing the same techniques as those for inspecting thethroat. Identifying the causative organism is helpful indetermining the antibiotic course that will be used. Therecommended treatment for acute tonsillitis secondary toGABHS is usually penicillin, unless a contraindication(i.e., penicillin allergy) exists. In cases of penicillin allergy,cephalosporins may be used. Antibiotics are generally ad-ministered orally or intramuscularly; the oral dose shouldbe given for 10 days. Teach the parent that administeringthe complete course of antibiotic is essential because,although symptoms may subside in 24 to 72 hours, thefull course is necessary to prevent complications such asrheumatic fever and glomerulonephritis.
Tonsillectomy and adenoidectomy are controversialsurgical interventions for chronic tonsillitis. Recurrent
throat infections (documented with positive throat cul-tures) remain one of the leading indications for surgery.Tonsillectomy has been documented to decrease thenumber of infections in children with recurrent tonsilli-tis; however, the number of throat infections also declinesin many children who have not had tonsillectomies.Chronic upper airway obstruction is also a major indica-tion for surgery. Symptoms of upper airway obstructionare more prominent during sleep and include mouthbreathing, loud snoring, and, in extreme cases, apnea.The child with upper airway obstruction extensiveenough to warrant tonsillectomy may also exhibit sleepdisturbances and enuresis. Patients with severe obstruc-tion improve after surgery; many patients with mild tomoderate symptoms improve without it. Before consider-ing tonsillectomy, healthcare professionals, in collaborationwith parents, should carefully document that sore throatsare caused by GABHS and are frequent (more than fiveper year), symptomatic (fever, exudate, erythema, adenitis),and costly in terms of missed school and work days andmedical expenses.
Tonsillectomy and adenoidectomy surgeries usuallyare performed on an outpatient basis 2 to 3 weeks afteracute infection. The nurse prepares the child and familyfor the surgery, and teaches both child and family thepostoperative care protocol.
Observe for potential hemorrhage during the postop-erative period. An ice collar is applied externally aroundthe neck. As soon as the child is awake, he or she maysuck on ice chips. The most comfortable and safe posi-tion is prone (on the abdomen) with the head turned tothe side so that mouth drainage can be observed. Smallamounts of bright-red blood may be present soon afterthe surgery. It is normal for the child to have one emesisof old blood after the surgery and small amounts ofblood-streaked mucus within the first few hours afterthe surgery.
caREmindercaREminderPerform any needed suctioning with caution, to avoidtrauma to the oropharynx and surgical site. Instruct thechild to avoid coughing, talking, clearing the throat, orblowing the nose after surgery, to prevent disturbing thesurgical site.
If the child spits up bright-red blood frequently or hasrepeated emesis of old blood from the stomach, or if heor she becomes tachycardic (heart rate >120 beats per mi-nute), pale, and restless, notify the surgeon immediately.Occasionally, it may be necessary for the child to returnto surgery to ligate a bleeding vessel. If no bleedingoccurs, ice chips and water may be given soon after sur-gery, after the child is fully alert. Advance the diet fromclear liquids to full liquids, as tolerated. Give pain medi-cation, in the form of a liquid or syrup if available, withinthe first 2 hours after surgery. The child should receivepain medication every 4 hours during the first 24 to 48hours to control pain and to make swallowing fluids morecomfortable.
682 Unit 3 n n Managing Health Challenges

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:35 User ID: muralir 1BlackLining Disabled
The child may be discharged on the day of surgery orthe following day, but should convalesce at home for sev-eral days. TIP 16–3 highlights key instructions for care ofthe child at home.
Community CareThe child with uncomplicated acute tonsillitis is usuallymanaged on an ambulatory basis. The symptoms of asore throat may be treated in the home with acetamino-phen (nonsteroidal anti-inflammatory drugs for childrenolder than 6 months), throat lozenges or hard candies,cool fluids, ice chips or ice pops, and saltwater gargles tokeep the throat moist. Discourage the use of topical anes-thetics sprays, because their efficacy in young children isunproved and because of the risk of systemic absorptionand allergic sensitization. Stress the importance of clearliquids to encourage hydration (diary products should beavoided, because they promote thickening of mucous).
Occasionally, the throat swelling is severe, symptomsindicate epiglottitis, or the child may become severelydehydrated and therefore require hospitalization fortreatment with intravenous fluids, parenteral antibiotics,and emergency equipment available in case of airwayobstruction.
CroupCroup is one of the most common acute respiratory con-ditions seen during early childhood (6 months–6 years ofage) and the most common cause of upper airwayobstruction (Cherry, 2005; Leung, Keller & Johnson,2004). The term croup represents several distinct dis-orders that cause a characteristic clinical syndromeof hoarseness, inspiratory stridor, a ‘‘croupy’’ or barkingcough, and varying degrees of respiratory distress.
Croup syndromes are generally more common in boysthan in girls and occur more often in the late autumnthrough early winter months. Although croup is gener-ally a benign condition resulting in minimal airwayobstruction, some forms of croup can be life threatening,resulting in respiratory failure. Young children are partic-ularly at risk, because inflammation and narrowing intheir small airways can easily result in obstruction. Croupsyndromes are usually described according to the primaryanatomic area of inflammation: acute epiglottitis (supra-glottitis), laryngotracheobronchitis (LTB; inflammationof one or more of the following structures: vocal cords,larynx, subglottic tissue, trachea, bronchi, bronchioles),spasmodic croup (larynx), and bacterial tracheitis (trachea).
Tip 1 6—3 A Teaching Interventional Plan for the Child After Tonsillectomy orAdenoidectomy
Nursing diagnoses and outcomes• Acute pain related to effects of surgical procedure
Outcome:• Child will demonstrate indicators of comfort and
will receive adequate periods of rest.• Deficient fluid volume related to decreased
intake of fluids and loss of fluids (vomiting,secretions)
Outcome:• Child will have adequate fluid intake with minimal
fluid losses.• Deficient knowledge: signs of postoperative
complications
Outcome:• Family/caregiver verbalizes and describes home
treatment and early signs of postoperativecomplications.
Teach the Child/Family
Home Management of the Child• Allow the child to engage in quiet activity for the
first week after surgery. The child may return toschool in 1 to 2 weeks or after the follow-upappointment.
• Give analgesics for pain every 4 to 6 hours asneeded. Use acetaminophen for pain relief; avoidaspirin and ibuprofen because these may increasebleeding tendencies.
• Apply an ice collar to the child’s neck, which mayhelp with pain management.
• Be aware that halitosis is common for 1 to 2 weeksafter surgery. Provide mouth care by using mouthrinses, instructing the child not to gargle.
• Encourage the child to drink plenty of fluids(1–11=2 quarts) daily.
• Offer tepid fluids or slow-melting fluids such as icepops or Italian ices, and offer a soft diet, avoidingspicy, rough, or coarse foods for the first 7 to 10 days.
• Use caution with straws; utensils; and sharp,pointed toys that may be put in the mouth andinjure the surgical site.
• Avoid crowds and protect the child from contactwith persons who are ill.
• Emphasize the importance of the surgical follow-up appointment, usually 1 to 2 weeks after surgery.
Contact Healthcare Provider if:• Persistent bleeding, frequent swallowing, cough-
ing, or blood in vomitus• Child complains of an earache• Child has a fever more than 101 �F (38.3 �C)
Chapter 16 n n The Child With Altered Respiratory Status 683

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:35 User ID: muralir 1BlackLining Disabled
Croup syndromes may be infectious or noninfectious.Noninfectious croup syndromes, such as spasmodiccroup, may be caused by asthma or allergic reactions, orthey may follow endotracheal extubation or foreign bodyaspiration (FBA). This section focuses on croup syn-dromes with infectious etiologies.
Acute Epiglottitis (Supraglottitis)Epiglottitis is a rare, acute inflammation of the supraglot-tic structures, the epiglottis and aryepiglottic folds. Itcharacteristically does not involve the subglottic and tra-cheal regions. Epiglottitis constitutes one of the truepediatric emergencies. If treatment is delayed, it mayrapidly progress to complete airway obstruction, cardio-pulmonary arrest, and a potentially fatal outcome. Whenprompt diagnosis and coordinated, well-organized man-agement occur, the prognosis for full and uncomplicatedrecovery is excellent.
The incidence of epiglottitis is unknown, Although hasbeen estimated to be fewer than 10 per 10,000 pediatrichospital admissions. Epiglottitis is commonly seen inchildren in all age groups, including infants, but occursmost often in children 2 to 7 years of age, with 80% ofthe cases occurring before 5 years of age (Leung, Kellner,& Johnson, 2004). It occurs year-round, but is morecommon during winter and early spring.
Epiglottitis most commonly results from infection ofthe supraglottic structures by H. influenzae type B (HIB).GABHS, S. pneumoniae, and, rarely, other bacteria andsome viruses have also been reported. The infecting or-ganism can be isolated from the upper airway as well asfrom the blood. Direct invasion by HIB causes inflamma-tion of the supraglottic structures, with subsequent edem-atous swelling of these structures and bacteremia. Since1985, with the licensing of the HIB vaccines, the inci-dence of disease caused by H. influenzae has declined.Still, pediatric health professionals should not dismissthe risks of epiglottitis and its consequences, however,because organisms such as streptococci have risen ascauses of epiglottitis (Faden, 2006). All patients who havethe clinical picture of this disease must be managed withthe same cautious approach.
AssessmentDiagnosis of epiglottitis is made primarily from clinicalsigns. Consider epiglottitis in any child with acute upperairway obstruction and respiratory distress, including stri-dor, of sudden onset (developing over a few hours) accom-panied by high fever (more than 102.2 �F [39 �C]), sorethroat, hoarseness, dysphagia, and drooling. Often thesesymptoms are preceded by symptoms of an upper respira-tory infection. Epiglottitis seldom causes the ‘‘barking’’cough characteristic of other croup syndromes. Agitation,characterized by irritability and restlessness, is almostalways present. Observe whether the child assumes the‘‘tripod’’ position, the hallmark of epiglottitis—the childrefuses to lie down, preferring to sit upright and lean for-ward, mouth open, to attain the best airway possible andto allow secretions to run out of the mouth. As the
obstruction increases, cyanosis may occur and retractionsof the supraclavicular and substernal area may be present.Parents are usually very fearful and anxious as they witnessand describe rapid onset of symptoms.
Never attempt direct visualization of the upper airwayin any child with symptoms of epiglottitis. Direct visual-ization of the upper airway may precipitate complete air-way obstruction and respiratory arrest. It should beattempted only by a person skilled in intubation and withall necessary equipment present at the bedside. Upon vis-ualization, the epiglottis is cherry red, and it and the sur-rounding tissues are extremely swollen. The laryngealorifice may be severely narrowed, and pooling of mucoussecretions often occurs.
A lateral neck radiograph is a useful diagnostic tech-nique. It shows the epiglottis as a large, rounded soft massbelow the base of the tongue.
Interdisciplinary InterventionsSkilled pediatric personnel should carefully monitor chil-dren for whom the diagnosis of epiglottitis is suspected atall times and in a controlled medical environment (e.g.,hospital room or emergency room with airway equip-ment appropriately sized for pediatric use). The child andthe parents are usually extremely anxious, and the mostimportant interdisciplinary intervention is keeping thechild quiet and undisturbed until endotracheal intubationis performed. Minimize episodes of crying by allowingthe child, if possible, to sit upright in the parent’s arms.Never force the child into a supine position, because thisposition may cause the inflamed epiglottis to obstruct theairway, compromise diaphragmatic excursion and airmovement, or enable the child to choke on swallowedsecretions.
Respiratory status, including rate and depth of respira-tions and the presence of retractions, nasal flaring, andstridor, must be carefully monitored. Give humidified ox-ygen by face mask and keep the head of the bed elevatedat all times. Monitor SaO2 levels using pulse oximetry.Intravenous antibiotics (usually ampicillin or cefuroxime)must be given as soon as possible. Upon strong suspicionor confirmation of the diagnosis, intubation should beperformed, ideally in the operating room under generalanesthesia. Intubation sometimes is not possible becauseof laryngospasm or severe swelling, and in these cases,placement of a tracheostomy is required (see TreatmentModalities earlier in the chapter).
Other important interventions include administeringand monitoring sedative medication, because the risk ofaccidental extubation is high. Mild sedation also allowsthe child to breathe spontaneously, making mechanicalventilation unnecessary. Assess for possible respiratorycomplications, monitor body temperature, and provide
Alert! Do not use tongue blades or other instrumentation to visualizethe epiglottis. Such actions can cause the epiglottis to spasm and totally occludethe airway.
684 Unit 3 n n Managing Health Challenges

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:35 User ID: muralir 1BlackLining Disabled
adequate fluid and calorie intake. The child must havenothing by mouth during the acute phase of the illness,and oral fluids and soft foods should not be provided untilthe child has demonstrated ability to tolerate extubation(Clinical Judgment 16–1).
As with any hospitalization, parental anxiety is high,especially if the child is admitted in acute respiratory dis-tress. During this period, provide calm, factual, step-by-step information. Repeat this information as the family’sstress level decreases and they are able to formulate ques-tions. Initial information should include the course ofevents in the immediate future—for example, when andwhere the child will be intubated; where the family maywait; when they may first visit the child after airway man-agement is accomplished; how the child will be givennutrition, hydration, and medication; and how long theyshould expect he or she will need to remain intubatedand sedated.
Recovery from epiglottitis is usually rapid, with endo-tracheal extubation occurring in 2 to 3 days as the feverdissipates, the child can handle secretions, and airwaynarrowing is resolved. Reassuring and supporting theparents is key during this recovery phase, because therapid progression and critical nature of this disorderrender it extremely frightening. Nurses and social work-ers can assist families by providing frequent, accurateeducation and updates on the child’s condition, andallowing parental visitation or ‘‘rooming in’’ as much as
possible. Tell parents when they should expect the childto resume normal dietary habits and when discharge fromthe hospital is expected. Begin teaching about adminis-tration of oral antibiotics at home (to complete a 7-daycourse) when the intravenous line is discontinued.
Community CareUrge immunization with the HIB capsular polysaccha-ride vaccine for the patient and all siblings of appropriateage (see Chapter 8), if they are not already immunized.Prophylaxis with rifampin by mouth is recommended forall household contacts, if at least one contact is youngerthan 4 years, regardless of immunization status. Daycareand nursery school contact groups should be managed onan individual basis. The HIB vaccine and rifampin pro-phylaxis can both be obtained from the county publichealth agency in many states.
Laryngotracheobronchitis (LTB)LTB is the most common type of croup syndrome. Thepeak incidence of this illness is in the 6-month to 3-year-old age group, but LTB can be seen in children as youngas 3 months and as old as 15 years of age (Leung, Keller,& Johnson, 2004). LTB usually occurs during the fall andwinter months.
Clinical Judgment 16—1
The Drooling Child
Jimmy, a 5-year-old child, presents in the emergencyroom with respiratory stridor upon inspiration and atemperature of 102.5 �F (39.2�C). He is drooling andprefers to sit forward with his chin slightly pro-truded. His mother states that he developed the diffi-culty breathing ‘‘so suddenly,’’ and both mother andchild appear anxious.
Questions1. What additional data would you collect during
your initial assessment?2. Is this an upper or lower respiratory problem?3. What actions would your initial interventions
include?4. Is obtaining a throat culture indicated at this time?
Why or why not?5. What interventions should be implemented to
maintain a patent airway in this child?
Answers1. Heart rate, duration of fever, and other signs of re-
spiratory illness. Is the child voiding? When didhe last eat or drink (to assess for dehydration and
shock)? No visual inspection of the oral cavity isever indicated if epiglottis is suspected.
2. An upper respiratory problem, as distinguished byinspiratory stridor resulting from an obstruction.In this case, the obstruction is a swollen cherry-red epiglottis.
3. Interventions include establishing and maintainingan airway. Keep the child with his mother to helpreduce anxiousness and allow him to remain in the‘‘tripod position,’’ because this helps maintain anopen airway. Provide oxygen via mask or blow-byoxygen. If respiratory distress becomes severe,ventilate with a bag–valve mask.
4. A throat culture should not be obtained, becausemanipulation of the oropharynx for visualizationor when obtaining a culture may precipitate airway(trachea) spasm and obstruction from the swollenepiglottis.
5. The primary therapy is to maintain the airway.Therefore, provide oxygen support via face maskor bag–valve mask ventilation as needed until thephysician is ready to intubate the child.
Chapter 16 n n The Child With Altered Respiratory Status 685

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:35 User ID: muralir 1BlackLining Disabled
Infectious agents associated with LTB croup are usu-ally viral and affect the subglottic region. Parainfluenza 1and 2 account for many cases of LTB. Other viral agentsassociated with LTB include influenza, respiratory syncy-tial virus (RSV), adenovirus, rhinovirus, enterovirus, and,more rarely, measles virus and herpes simplex virus (Bra-den, 2006; Leung, Keller, & Johnson, 2004).
PathophysiologyThe underlying pathophysiology of LTB is inflammationand edema of the larynx, trachea, and bronchi; laryngealmuscle spasm; and production of mucus that furtherobstruct the airway. Inflammation in LTB narrows thesubglottic region, the smallest portion of the upper air-way in children, thus producing the classic symptoms ofupper airway obstruction found in children with croup.Hoarseness occurs because the vocal cords swell; thebarking cough is caused by inflammation of the larynxtissues.
AssessmentThe incubation period for LTB is usually 2 to 6 days andis typically preceded by a mild upper respiratory infectionwith symptoms of rhinorrhea, mild cough, and low-gradefever. Children presenting with LTB look ill and appearto be in acute respiratory distress. Listen for hoarseness,inspiratory stridor, and the characteristic ‘‘barking’’ orbrassy cough. The history typically reveals a mild upperrespiratory infection, followed within 2 to 6 days bysymptoms of LTB. Clinical signs, depending on the se-verity of airway obstruction, may include suprasternal,substernal, and intercostal retractions; intermittent cya-nosis during coughing; and altered mental status relatedto hypoxia and carbon dioxide retention. A thorough re-spiratory assessment is important, because the child withupper airway obstruction with mild hypoxia developsmuscle fatigue and hypoventilation that can result insevere hypoxemia and hypercapnia. Rarely, endotrachealintubation is necessary because of complete airwayobstruction or respiratory distress.
A characteristic concern in children with LTB is pa-rental anxiety, which is usually high. However, the degreeof anxiety depends on many factors, including parentalexperience with previous croup episodes, lack of sleepfrom child’s ‘‘barking,’’ and the severity of the child’s re-spiratory distress and degree of anxiety and irritability.
Interdisciplinary InterventionsTreatment of children with LTB depends on its severityand may include general supportive care, corticosteroids,nebulized epinephrine, supplemental oxygen, or somecombination of these therapies. Rarely, emergency meas-ures for ventilation (endotracheal intubation) are required.General supportive measures for the child include hydra-tion, fever reduction measures, and maintaining a calmand reassuring atmosphere for the parents. As with anyrespiratory condition, hydration is an important nursingaction. Encourage clear fluids, particularly fluids the childprefers, unless respiratory distress is severe, in which case
the child should have nothing by mouth and should behydrated intravenously. Give antipyretics if the child isfebrile (fever higher than 101 �F [38.3 �C]). Ensure thatparents understand the distinction between bacterial andviral illnesses, so they are not distressed when antibioticsare not prescribed. LTB is generally a self-limiting illnessin which children’s symptoms subside in 3 to 5 days, andfull recovery without complications is the norm.
Children who present with respiratory distress symp-toms such as cyanosis and who are severely hypoxic,fatigued, in respiratory distress, or unable to drink suffi-cient fluids are hospitalized to receive intravenous fluid,oxygen, and airway support. Observe for any deteriora-tion of respiratory status and monitor vital signs, includ-ing rate, rhythm, and depth of respirations, and cardiacrate and rhythm. Tachycardia, cardiac arrhythmias, orboth may be seen with hypoxia. Ensure that equipmentfor intubation and tracheostomy is readily available.
Mist therapy (croup/mist tents or mist via mask ornasal cannula), widely used in the past, has questionableefficacy for treating LTB (Bradin, 2006). Current therapyrelies on aerosol inhalation therapy with medicationssuch as racemic epinephrine. Racemic epinephrine isbelieved to work via topical alpha-adrenergic stimulation,which causes mucosal vasoconstriction and leads todecreased edema in the subglottic region. Facilitate theadministration of respiratory inhalation treatments at theprescribed frequency, to disrupt regular feeding and sleeppatterns as little as possible.
Community CareTwo of the most important interventions are to minimizeanxiety and maximize opportunities for rest. Providing acomfortable environment free from noxious stimuli less-ens respiratory distress. Encourage children to engage inquiet play that provides diversion and reduces anxiety.Coloring books, watching favorite videos and DVDs, lis-tening to music, reading stories, and doing puzzles aresome examples.
Nutritional supports for children with croup are gen-erally short term. Encourage oral intake of clear fluids,especially fluids the child prefers. Diary products shouldbe avoided until respiratory status is stable. When solidfood is resumed, the child may find frequent, small nutri-tious snacks more appealing than an entire meal.
Teach parents and other caregivers about medications,respiratory inhalation treatments, and ways to assess theirchild’s respiratory status. Although most children recoverwithout complications, caregivers must be able to recog-nize and describe signs of impending respiratory failureand know how to access emergency services. A homehealth referral may be indicated if the parent’s assessmentability is in question and the child’s condition does notwarrant hospitalization. The child should be afebrile andfree from cough before returning to school or daycare.
During the acute phase of the illness, parental anxietymay be very high. Provide information and support,emphasizing the short-lived nature of the illness. For thechild who remains at home, help the parents to mobi-lize their extended family and community resources, to
686 Unit 3 n n Managing Health Challenges

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:35 User ID: muralir 1BlackLining Disabled
relieve them of some care responsibilities and providethem opportunities for adequate rest.
Bacterial TracheitisBacterial tracheitis is an uncommon, but potentially life-threatening, acute bacterial infection of the mucosa ofthe upper trachea. It is also called membranous laryngotra-cheitis or membranous croup. Although it is a very rare dis-ease, it may be seen in children between 1 month and5 years of age; the peak incidence is in the fall and wintermonths (Cha et al., 2006). This condition is unrelated toethnicity, gender, or socioeconomic status. Bacterial tra-cheitis is a serious cause of airway obstruction, severeenough to cause respiratory arrest. The overall mortalityrate is 4%. With early recognition and treatment, out-comes are generally very good. The most common causa-tive organisms are Staphylococcus aureus, H. influenza,Streptococcus pyogenes, and other anaerobic bacteria (Chaet al., 2006).
AssessmentThe child with bacterial tracheitis usually appears quiteill and presents with a history of a prior upper respiratorytract infection, viral croup, or both, followed by a highfever, cough, and increasing inspiratory stridor unaf-fected by position. The trachea is inflamed and appearserythematous and edematous, with thick, tenacious,purulent secretions. Respiratory distress is a key symptomin bacterial tracheitis and requires immediate medicalattention. The physician uses laryngoscopy or bronchos-copy to confirm the diagnosis. Tracheal cultures areobtained during the endoscopic procedure (Cha et al.,2006).
Interdisciplinary InterventionsVigorous management, including early recognition ofbacterial tracheitis and prompt attention to the airway, isnecessary to prevent the airway from being obstructed bythe thick secretions. The child should be hospitalized,and appropriate emergency airway management equip-ment should be available. Frequent tracheal suctioning isnecessary to keep the airway patent, and often the childhas an artificial airway (endotracheal tube) in place. Thismanagement is especially important in the younger child,who is at risk for abrupt airway obstruction. Additionally,the child requires humidified oxygen, parenteral broad-spectrum antibiotics (for 10–14 days), and antipyretics forfever and discomfort.
ApneaApnea is cessation of airflow in to and out of the lungs.Apneic episodes lasting longer than 20 seconds, andshorter respiratory pauses associated with cyanosis, bra-dycardia, pallor (paleness), or limpness, are consideredpathologic apnea. This definition is simply a descriptionof a characteristic clinical syndrome, not a specific diseaseprocess. Three general types of apnea occur:
1. Central apnea is an impairment of the mechanisms thatcontrol breathing, which results in absence of nasal air-flow and ventilatory effort.
2. Obstructive apnea is usually caused by anatomic abnor-malities and occurs when nasal airflow is absent despitenormal or exaggerated respiratory effort. Obstructiveapneas include obstructive sleep apnea (OSA), which isthe most common type of sleep apnea.
3. Mixed apnea includes central and obstructive compo-nents and may require multiple treatment methods.
Although apnea can occur at any age, the prematureinfant is at a greater risk. The incidence of apnea amongchildren younger than 1 year of age has been estimated atbetween 0.5% to 6% (Hall & Zalman, 2005). Normal re-spiratory system development is such that the lungs andrespiratory center of the brain are designed to breatheand control respiration at term, although they are capableof breathing air by 23 weeks’ gestation. Therefore, thelungs and respiratory center of the premature infant havenot fully matured, leading to disruptions in the regularityof respiration.
Apnea of prematurity (AOP) is the occurrence of patho-logic apnea and periodic breathing in an infant of lessthan 37 weeks’ gestation. AOP is a common, natural con-sequence of immaturity and need not be viewed as a dis-ease (Stokowski, 2005).
Apnea of infancy (AOI) describes episodes of breathingcessation or respiratory pauses in a previously healthyinfant of at least 37 weeks’ gestation.
Apparent life-threatening events (ALTEs) is the currentterm for more severe disturbances of a frighteningly seri-ous nature. These episodes have been formerly callednear-miss sudden infant death syndrome (SIDS) episodes;however, the term ALTE is believed to more accuratelydescribe the occurrence. An ALTE is defined as an eventin which an infant has a convincing history of an episodeof apnea that is sudden in onset, considered frighteningto the observer, and is characterized by color change (cy-anosis, pallor, or erythema), marked change in musculartone (limpness, rarely stiffness), and choking, gagging, orboth. It requires substantial intervention (vigorous shak-ing, mouth-to-mouth breathing, or full CPR) to revivethe infant and restore normal breathing (American Acad-emy of Pediatrics, 2003).
Studies of sudden infant death syndrome (SIDS) haveindicated that AOP or AOI is not a precursor or predictorof subsequent SIDS death (American Academy of Pedia-trics, 2003). Healthcare professionals should promote pre-ventive practices to decrease the risk of SIDS. Specificinterventions include supine positioning for sleep, safesleeping environments, and elimination of smoke exposure.
Acute apneic episodes with cyanosis in term infants canhave a variety of treatable causes including seizures;infection; breath-holding spells; congenital heart disease;cardiac dysrhythmia; electrolyte imbalances; congenitalcentral hypoventilation syndrome; brain stem compres-sion; anemia; or exposure to alcohol, sedatives, and nar-cotics. ALTE can also be the result of a profound centralnervous system insult or depression involving structuraldamage to the brain stem (as in trauma, infection, or
Chapter 16 n n The Child With Altered Respiratory Status 687

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:35 User ID: muralir 1BlackLining Disabled
edema) or interference with cerebral metabolic function(e.g., drug overdose, hypotension, severe hypoxia). Theprognosis for these infants depends on the etiology andtreatment of the underlying cause.
AssessmentApnea may present simply as a parental report of pro-longed asymptomatic respiratory pauses during sleepor as dramatically as a witnessed complete cessation ofbreathing and absence of a heart rate. Because apneic epi-sodes, regardless of their severity, typically occur awayfrom the view of the medical team, the significance of theevent is based largely on the caregiver’s recollection ofthe event. A single mild episode that required little or nointervention does not necessitate an extensive diagnosticevaluation or aggressive therapy and has little prognosticimportance. The healthy infant who presents with a his-tory of AOI or an ALTE for whom the obvious treatablecauses have been ruled out presents a greater challenge inevaluation and management.
Infants usually appear entirely normal by the time theyreach medical attention after an ALTE. The most impor-tant element of assessment is, therefore, to obtain a care-ful history from the person who witnessed the event.Interview the witness to determine the color of the childwhen found (pale, or blue/cyanotic), whether the childhad any respirations, and whether the child was limp.Determine whether there was evidence of vomiting. As-certain whether the apneic episode occurred when thechild was asleep or awake. Collaborate with other health-care personnel to gain as much detail as possible aboutthe event itself, the physical condition of the infant beforeand after the event, and circumstances surrounding itsoccurrence. Assess the reliability of the historian and lookfor any signs of child abuse or neglect; also evaluate thepotential for sepsis.
OSA may occur in children of any age. Symptomsinclude snoring, periods of observed apnea, heavy breath-ing, broken or restless sleep, bad dreams, and failure togrow or thrive. Sequelae of OSA may include inattentive-ness, developmental disorders, mood disorders, or exces-sive daytime sleepiness.
One of the primary diagnostic tests in apnea is the pol-ysomnographic study (PSG, or sleep study). Other diag-nostic tests may include but are not limited to arterial orcapillary blood gases (persistent acidosis indicates a severeevent or a chronic metabolic disorder); complete bloodcounts (anemia may precipitate apnea, polycythemiareflects chronic hypoxia, elevated white blood cell countindicates infection); and serum electrolyte, glucose, andblood urea nitrogen levels (numerous abnormalities, suchas hypocalcemia and hypoglycemia, may contribute tothe development of apnea).
The primary diagnostic test for OSA is the nocturnalPSG. Many healthcare professionals diagnose OSA basedon physical examination and nocturnal pulse oximetry.
Interdisciplinary InterventionsOptimal care of infants who have had an episode of apneaaccompanied by color change or who present with a seri-
ous ALTE includes hospitalization for observation, mon-itoring by healthcare personnel, a thorough evaluationfor possible causes, and parent training (seefor Care Paths: An Interdisciplinary Plan of Care for theChild With Apnea). Continuous cardiorespiratory moni-toring and frequent assessment of color, breathing pat-terns and effort, and tone are appropriate healthcareinterventions.
The preterm infant who continues to exhibit sympto-matic apnea during the hospital stay should also be eval-uated carefully for hypoxia or anemia, which can causeapnea in the premature infant. In the absence of hypoxiaor anemia, preterm infants who are still having clinicalepisodes of apnea can be discharged with home apneaand bradycardia monitoring equipment.
Agents such as theophylline, aminophylline, or caffeineare sometimes useful in decreasing the severity and fre-quency of apneic episodes. These medications are centralnervous system stimulants that act on the respiratory cen-ter of the brain and therefore are sometimes effective intreating central apnea only. Besides stimulating the respi-ratory center, these drugs also act on the kidney, heart,and skeletal and smooth muscles. Side effects includetachycardia and increased diuresis. Parents and caregiversmust be taught to draw up and administer the medica-tions and observe for toxic side effects (tachycardia, vom-iting, excessive irritability). Teach them to monitor fortherapeutic drug levels and to report toxic levels.
Treatment of OSA primarily focuses on tonsillectomy,adenoidectomy, or both. Other options include weightreduction, inhaled corticosteroids, or positive-pressureairway breathing (including continuous positive airwaypressure).
Community CareParental anxiety is characteristically the foremost psycho-social issue challenging nurses and other members of thehealthcare team in working with the infant and family af-ter admission to the hospital with an apneic episode or af-ter an ALTE. Much guidance and reassurance is needed,in conjunction with education, to increase parental confi-dence and problem-solving skills.
Because no specific treatment currently exists for infantswith AOI or ALTE of unknown etiology, home apnea andbradycardia monitoring is the primary therapy. Ongoingtherapy can be equally anxiety producing as the initialALTE for parents and families. Home monitors serve onlyto alert the caregiver that an apneic episode is occurring.The parent or caregiver must then respond and act to eval-uate and terminate the apneic episode. Most parents feelthe need to use the monitor at all times when the infant is
Alert! Numerous studies have demonstrated that infants in whom notreatable cause for an ALTE is found have a risk that is 15 times greater thanthat of the general population for subsequent death from SIDS (Edner, Erikson,Milerad, & Katz-Salamon, 2002; Horemuzova, Katz-Salamon, & Milerad, 2002;Mitchell & Thompson, 2001).
688 Unit 3 n n Managing Health Challenges

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:35 User ID: muralir 1BlackLining Disabled
not being directly observed. Home apnea monitoring of-ten adversely affects parents’ ability to work, socialize, nur-ture their other children, and generally maintain theirformer life functions because of their obsessive focus onthe monitor and its every nuance.
Before initiating home apnea monitoring, and whilethe infant is still hospitalized, conduct a thorough reviewof the family’s living arrangements and verify that appro-priate resources are present to successfully support ahome apnea monitoring program. Minimum environ-mental requirements include electricity, a telephonein the home, and availability of caregivers trained torespond to the apnea alarm. This inpatient evaluation ofthe family system is crucial in determining the teachingplan and coordinating follow-up. It may be necessary tocontact community resources when appropriate, accord-ing to the family’s needs.
Parental education for home apnea and bradycardiamonitoring includes information on monitor use, alarms,indications for help, and CPR. Parents and caregivers arealso taught to keep a log or diary of all apnea and brady-cardia alarms, especially those requiring any intervention.If both parents work outside the home, alternative care-givers (extended family members, daycare providers, andso on) must also receive this education (seefor Care Paths: An Interdisciplinary Plan of Care for theChild with Apnea).
Most infants with ALTE require 4 to 6 months ofhome monitoring. The decision to discontinue the apneamonitor should be made jointly between the family andthe healthcare professionals. If the decision is made toend monitoring, give the parents a clear statement of thestatus of the problem and explain that it appears to haveresolved, and that the infant can be expected to grow andprogress normally. Monitoring is discontinued using asimilar protocol as that used in persistent AOP, in thatthe monitor may be safely discontinued after 2 to 3months without apnea or bradycardia spells that requireintervention (American Academy of Pediatrics, 2003).Because of the diligence required for successful homemonitoring, many parents find it difficult to stop homemonitoring when it is no longer required for their infant.The caregiver has learned to rely on the monitor to pro-vide a comforting reassurance that the child is well.
Foreign Body Aspiration (FBA)FBA remains a persistent problem and an important causeof morbidity and mortality in the pediatric age group. For-eign bodies retained in the airway can be potentially lifethreatening and can produce severe lung damage.
Quantifying the overall incidence of FBA is difficult,because nearly all foreign bodies aspirated into the respira-tory tract are probably expelled immediately by spontaneouscoughing and never require medical intervention. However,FBA remains a common cause of mortality and morbidityamong children during the first 3 to 4 years of life.
Most episodes occur during eating or play. Commonlyaspirated objects include foods such as hot dogs, peanuts,other nuts and seeds, grapes, popcorn, and carrots as well
as items such as small plastic toys, marbles, buttons, ear-rings, and latex balloons. Factors related to a youngchild’s physical and developmental status predispose himor her to the risk of FBA (see Chapters 4 and 5). Youngchildren (particularly those 6 months–2 years of age)explore the environment by putting objects in theirmouth and are at highest risk for aspiration. They alsohave insufficient size and number of teeth to thoroughlychew foods. In addition, they may seek relief from theteething process by chewing on hard objects. Exposure tocertain foods thus may be inappropriate for a youngchild’s cognitive and dental stage of development, andmay lead to choking and aspiration.
PathophysiologyThe pathophysiology of FBA varies depending on the sizeof the foreign body, the location of the object in the respi-ratory tract, and the acute or chronic nature of the condi-tion. If an object is too large or of a shape that does notallow it to be expelled by coughing, respiratory symptomsresult. Foreign bodies in the upper airway often cause amechanical or partial obstruction that results in non-specific respiratory signs and symptoms such as cough,wheeze, stridor, dyspnea (labored or difficult breathingresulting from air hunger), voice changes, cyanosis, retrac-tions, and hemoptysis (coughing blood). At times, a care-fully assessed history reveals an episode of coughing,choking, or breathing difficulty that can be traced back toan aspiration event, but on many occasions, the discoveryof an FBA is made without ever obtaining such a history.
AssessmentThe location of the foreign body is a key factor in deter-mining the signs, symptoms, and physical assessmentfindings (Table 16–3). Although nearly all children whohave aspirated a foreign body exhibit a chronic cough, ahistory of an acute coughing episode, or both, othersymptoms vary according to where in the respiratorytract the object is lodged.
Perform a respiratory assessment. The child with a for-eign body that lodges in the upper airway, such as the lar-ynx or trachea, usually presents with an acute and ratherfierce onset of stridor and respiratory distress necessitatingimmediate intervention to dislodge the foreign body. Aforeign body lodged in the bronchus may act as a ball valve,obstructing the airway perhaps partially on inspiration andcompletely on expiration. Wheezing localized to one sideof the chest on inspiration and diminished breath soundson expiration result. In children with an esophageal for-eign body, the distended esophagus compresses the nearbytrachea, thus causing respiratory distress. Physical assess-ment findings may reveal asymmetry of chest wall move-ment, and wheezing or diminished breath sounds in alocalized area of the lungs. If the obstruction is located inthe upper airway, stridor is common.
Radiographs may be normal, may allow clear visualiza-tion of the presence of a foreign body, or may showchanges related to the foreign body directly or caused bysecondary inflammatory changes. Abnormalities are lesslikely to be noted on chest radiograph for foreign bodies
Chapter 16 n n The Child With Altered Respiratory Status 689

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:35 User ID: muralir 1BlackLining Disabled
located above the bifurcation of the mainstem bronchus.Lateral neck films are obtained when this location issuspected.
‘‘Chronically’’ retained foreign bodies can lead to amarked inflammatory response in the respiratory tractand, possibly, death. The right mainstem bronchus is acommon site for foreign body lodgment because of itsangle. Airway inflammation and narrowing secondary toedema often occurs. Materials such as nuts, which containfats, cause an especially intense inflammatory response.Recurrent infections such as lipoid pneumonia or a lungabscess may ensue. Chronic obstruction of air exchangeto the alveoli could mimic obstructive emphysema onchest radiographs. Foreign bodies that have been dis-lodged by coughing can lead to involvement as describedhere in different lung segments.
Interdisciplinary InterventionsEmergency treatment for the choking child includes theuse of abdominal thrusts (the Heimlich maneuver) in thechild older than 1 year of age and use of back blows andchest thrusts in the infant younger than 1 year. Use thesemethods in situations in which the aspiration was wit-nessed or strongly suspected and the child has an ineffec-tive cough with increasing stridor and respiratory distressor has become unconscious and apneic.
In many cases, the object is not coughed up spontane-ously and is lodged farther down in the respiratory tree;therefore, the foreign body has to be removed as soon aspossible to prevent further airway damage. Rigid bron-choscopy to remove the foreign body after aspiration isthe most common medical intervention. This procedure isvery safe and effective when carried out by an experiencedphysician. Rigid bronchoscopy enables removal of theobject and any associated inflammatory material; it alsoprovides a means of assessing the condition of the airway.
Nursing care responsibilities for the infant or childundergoing rigid bronchoscopy focus on preoperativepreparation and postoperative monitoring. Explain thereason for the procedure to the family. Intravenoushydration, emptying of stomach contents, and preopera-tive assessment of respiratory status are fundamentalnursing interventions. Postoperatively, frequently assess
quality and symmetry of breath sounds, vital signs,color, and respiratory effort. Atelectasis, bronchospasm,and pneumothorax all are possible postbronchoscopycomplications.
Community CareThe psychosocial consequences of an FBA incident varyin intensity, depending on the severity of the event. Themost dramatic scenario involves the infant or child with acomplete airway obstruction who is experiencing respira-tory arrest and requires immediate resuscitation. This ex-perience is extremely terrifying for both the child and thecaregivers. Asphyxiation with subsequent brain damageor even death may occur. The grief and guilt that parentsand caregivers experience in this situation are tremen-dous and often incapacitating. Extensive support andcounseling services are crucial for these families. Lesssevere episodes of FBA may also raise feelings of guilt orembarrassment about inadequate supervision or aboutnot recognizing symptoms.
The most effective ‘‘therapy’’ for FBA is prevention.Anyone who works with children should be certified inCPR, including airway obstruction management. Educa-tion for parents and other caregivers of infants and youngchildren regarding aspiration risk factors is an essentialrole for all pediatric healthcare providers. Information oncommon items aspirated, age groups especially at risk,and developmental and environmental considerations canhelp parents be more aware of potential dangers and takeproper precautions.
Environmental factors such as a high degree of distrac-tion during play and mealtimes, and insufficient adultsupervision may also contribute to FBA. Remind parentsthat watching television during meals can be a dangerousdistraction to young children and should be avoided.Caregivers of children at play must be cautioned aboutbeing vigilant with small children, to keep them fromputting objects in their mouths. Visitors to the homeshould place purses and other personal items out of reachof the small child. Last, products containing any small,cylindrical components should bear labels discouraginguse around young children and should detail the agegroups particularly affected.
T A B L E 1 6—3
Locations of Foreign Body Aspirates and Associated Findings
Location of Foreign Body Clinical Findings
Supraglottic Cough, dyspnea, drooling, gagging, changes in phonation
Larynx Cough, stridor, changes in phonation; at times, severe respiratory distress
Trachea, intrathoracic Expiratory wheeze, inspiratory noise
Trachea, extrathoracic Inspiratory stridor, expiratory noise
Bronchi Cough, asymmetric breath sounds or wheeze, hyperresonance
Esophageal Drooling, dysphagia, stridor, respiratory distress
690 Unit 3 n n Managing Health Challenges

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:35 User ID: muralir 1BlackLining Disabled
Lower Respiratory Infections
and Obstructions
Lower respiratory infections and obstructions includeinfluenza, bronchiolitis, bronchitis, and pneumonia.
Question: Because Jose has a preexisting condi-tion (asthma), he is at greater risk from respiratory
infections. Jose will go to kindergarten next year. Whatinformation can the nurse share with Claudia to help her keepJose from catching lower respiratory infections?
InfluenzaInfluenza illnesses have been described and defined epi-demiologically for centuries. Influenza viral agents werethe first proved to be respiratory tract pathogens. Conse-quently, the terms flu and influenza are perhaps the mostoverused diagnostic labels for nondescript infectious con-ditions in both medical and lay circles. This confusion isprobably increased by influenza’s broad range of clinicalmanifestations and its wide prevalence in the community.
Influenza infection often occurs in epidemics that sweepthroughout a community in a matter of 6 to 8 weeks. Thou-sands of individuals die from influenza infections in theUnited States each year. Morbidity is highest in susceptiblepopulations, such as infants and persons older than 65 yearsof age. Children with preexisting conditions such as bron-chopulmonary dysplasia (BPD), cystic fibrosis (CF), asthma,and congenital respiratory conditions (e.g., Pierre Robinsyndrome) are at increased risk for morbidity and mortalityassociated with the flu. It is imperative to recognize the ele-vated vulnerability of this population. The incidence ofinfection is highest, however, in children of school age.
PathophysiologyThe influenza viruses are large, single-stranded RNAviruses. Influenza viruses have a high affinity for epithe-lial cells of the respiratory tract mucosa. The virus causesa lytic infection of the respiratory epithelium with a lossof ciliary function, decreased mucus production, and des-quamation of the epithelial layer. The incubation periodfor influenza virus can be as short as 2 to 3 days, and viralreplication usually continues for 10 to 14 days after pri-mary infection.
There are three influenza virus types, specific in theirprotein and antigen composition: influenza A, B, and C.Influenza A and B cause seasonal outbreaks and epidem-ics. Influenza A causes pandemics (Goldrick & Goetz,2007). Literally hundreds of subtypes of these categories‘‘shift’’ their complement of antigens on a regular basis.These mutations largely account for the ability of influ-enza to produce serious epidemics in populations ofpeople who have been previously immunized or haveexperienced influenza infection. This regular antigenicshift makes the preparation and distribution of influenzavaccines necessary on an annual basis.
AssessmentInfections with influenza viruses may be manifested bymild, moderate, or severe clinical symptoms. Generally,a child with influenza infection has a more sudden onsetof these symptoms than do children with parainfluenza,Respiratory Syncytial Virus or adenovirus infections.Look for fever of sudden onset accompanied by aflushed face, dry throat and nasal mucous membraneswith dry cough, sore throat, muscle pain, headache, andmalaise. During the acute phase of the illness, the childmay be quite ill and require hospitalization if dehy-drated or if a secondary infection develops. Fever, sorethroat, and headache normally subside in 3 to 5 days,whereas other symptoms, such as fatigue and malaise,may persist for several weeks. Provide supportive inter-action to parents to allay anxiety regarding progressionof the illness and complications. Children are often dis-appointed at missing important events and activities, yetthey do not have the strength to participate.
Influenza is difficult to distinguish from other respira-tory illnesses in children. Most recently, commercialrapid diagnostic tests have been developed that can detectinfluenza viruses within 30 minutes (Schrag et al., 2006).Diagnostic tests for influenza also include viral culture,serology, rapid antigen testing, polymerase chain reac-tion, and immunofluorescence assay.
Interdisciplinary InterventionsCommunity Care 16–2 lists the recommendations for useof inactivated influenza vaccine to prevent influenza inchildren. The only specific contraindication for the use
Community Care 16—2
Recommendations for Administeringthe Influenza Vaccine to Children
Who Are at High Risk
All Children Age 6 Months to 23 MonthsChildren with acute or chronic conditions such as
• Chronic pulmonary disease (cystic fibrosis, asthma,bronchopulmonary dysplasia)
• Congenital heart diseases and hemodynamically sig-nificant diseases
• Immunosuppression• Sickle cell disease and other hemoglobinopathies• Diabetes and other chronic metabolic diseases• Chronic renal disease• Symptomatic HIV infection• Children with cognitive impairments, seizure disor-
ders or neuromuscular conditions
Source: Centers for Disease Control, 2005.
Chapter 16 n n The Child With Altered Respiratory Status 691

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:35 User ID: muralir 1BlackLining Disabled
of this inactivated vaccine is anaphylactic hypersensitivityto eggs.
Interventions for children with influenza include sup-portive care to alleviate or minimize symptoms. Antiviralagents such as zanamivir and oseltamivir may also be usedfor influenza A or B within certain populations. Theseagents have shown effectiveness by reducing the influ-enza course by 1 to 3 days when an early diagnosis ismade (Schrag et al., 2006). Administration of acetamino-phen every 4 to 6 hours for fever and muscle aches is alsobeneficial.
Other antipyretic therapies include undressing thechild with a persistent fever to permit radiant heat lossand giving tepid sponge baths.
caREmindercaREminderDo not bathe a shivering child, because the child likely willshiver more and remain febrile.
Teach parents the signs and symptoms of respiratorydeterioration, the signs of dehydration and ways of pre-venting and treating it, and the reason that aspirin admin-istration is contraindicated in children.
Clear liquids for children and oral rehydration formu-las for infants replace losses from fever, tachypnea, andvomiting. Parents should offer oral fluids in smallamounts (30–60 mL) on a frequent basis. If the childbecomes dehydrated and requires hospitalization, he orshe should receive parenteral fluids. Bed rest is importantand should be encouraged for the first 3 to 5 days. If thechild is home, teach the parents or caregiver what towatch for, such as increased lethargy, excessive vomiting,or respiratory distress that may indicate that the childneeds to be seen by a healthcare professional.
Answer: The nurse should share that it is impor-tant that Jose receive the flu vaccine each fall. Addi-
tional teaching may be needed to explain why this vaccine isunlike his other childhood immunizations and a vaccinationis needed each fall. In addition, teaching Jose good handhygiene techniques and emphasizing the importance of handhygiene may well prevent him from catching influenza andother viruses.
Bronchiolitis
Question: How are Jose’s symptoms differentfrom a child with bronchiolitis or bronchitis? Examine
Table 16–4 for more information.
Bronchiolitis is an acute inflammation and obstruction ofthe bronchioles, the smallest, most distal sections of the re-spiratory airway network. It generally occurs during thefirst 2 years of life, with a peak incidence between 2 and 6months of age. Infant susceptibility may be attributable tothe loss of full maternal antibody protection that is univer-sally present at birth and for the first few months of life(Christakis et al., 2005). Premature infants, immunodefi-cient infants, and those with underlying comorbid con-ditions such as BPD, CF, or congenital heart diseaseare extremely vulnerable to respiratory failure and othersevere complications of bronchiolitis. Many infants can bemanaged at home; a few may require hospitalization.
PathophysiologyIn bronchiolitis, the bronchioles become narrowed, andsome even become totally occluded as a result of theinflammatory process, edema of the airway wall, accumu-lation of mucus and cellular debris, and smooth musclespasm. It may also cause thickening of the muscular walland destruction of ciliated cells. This narrowing of theairway lumen can profoundly decrease airflow. Impairedclearance of secretions and decreased airflow lead tobronchiolar obstruction, atelectasis, and hyperinflation,causing impaired gas exchange that results in hypoxemia.Carbon dioxide retention occurs in the severely affectedinfant. The illness is self-limiting and generally resolveswith adequate intervention.
Acute bronchiolitis most often has a viral cause. In someareas of the United States, bronchiolitis is the most commoncause for hospitalization among infants younger than 1 year(Christakis et al., 2005). RSV, which has a high affinity forthe respiratory tract mucosa, is the most common cause ofbronchiolitis (Cooper, Banasiak, & Allen, 2003; Yorita etal., 2007). This virus is highly contagious and extremelyprevalent in communities during the winter and springmonths. Nearly all children have been infected with RSVby the age of 2 (Yorita et al., 2007). Respiratory syncytial vi-rus (RSV) is transmitted by direct contact with infectedsecretions via hands and respiratory droplets. Adults as wellas children are infected with RSV disease; thus, the sourceof viral infection in an infant is usually a family memberwith a mild respiratory illness. Infections with otherviruses, primarily adenovirus, parainfluenza, and influenza,have been associated with bronchiolitis in smaller numbersof cases. In a small percentage of infants with bronchiolitis,suprainfection with a bacterial pathogen can occur.
AssessmentDiagnosis of bronchiolitis is made by history and physicalexamination. Diagnostic criteria include exposure to ill
Alert! Never treat children 18 years of age or younger with aspirin orother salicylate derivatives, because of the relationship among viral syndromes,aspirin, and Reye syndrome.
Alert! Supplemental oxygen may be needed for chronically ill childrenwith an influenza infection because of their poor respiratory reserves andincreased propensity to develop hypoxemia.
692 Unit 3 n n Managing Health Challenges

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:36 User ID: muralir 1BlackLining Disabled
persons, seasonal timing, and upper respiratory symp-toms. The infant with bronchiolitis has typically had anupper respiratory infection for 2 to 3 days. Parents reportsneezing and nasal discharge initially, and then the infantdevelops a harsh, dry cough and low-grade fever. Listenfor wheezing on auscultation. The infant may developincreasingly distressed breathing and tachypnea. Inquireabout feeding difficulties or loss of appetite caused bynasal congestion and the increased work required tobreathe.
Because a major consequence of airway obstructionis impaired gas exchange, the child with bronchiolitishas many of the signs and symptoms of hypoxia and re-spiratory distress. Note the respiratory rate, which iscommonly more than 60 breaths per minute and maybe as high as 100 breaths per minute. Look for chestretractions; rhonchi and wheezes or crackles are gener-ally heard in all lung fields. Check for dehydration,which can be severe because respiratory distress oftenprevents adequate oral fluid intake. In addition, the ele-vated respiratory rate causes insensible fluid loss (seeChapter 17). When the infant becomes ill during win-ter months, dry air may further exacerbate the condi-tion. Hypoxia and hypercarbia result in restlessness andirritability, making the child difficult to console, evenby parents.
A nasal swab may assist in an RSV diagnosis. A chestradiograph may be done if the child is hypoxic.
Interdisciplinary InterventionsThe care of a child with bronchiolitis involves respiratory,pharmacologic, and nutritional support (seefor Care Paths: An Interdisciplinary Plan of Care for theChild With Bronchiolitis). Infants with moderate tosevere respiratory distress caused by bronchiolitis or chil-dren experiencing respiratory distress with feeding diffi-culties are usually hospitalized. Others may require onlysupportive care at home, although oxygen and bronchodi-lators may promote ease of breathing.
Hospitalized infants with RSV bronchiolitis are at highrisk for respiratory failure and may require mechanicalventilation during the acute phase of the illness. Clinicalindications for mechanical ventilation include worseningrespiratory distress with increased work of breathing,increased heart rate, poor peripheral perfusion, apnea,bradycardia, and hypercarbia. Generally, the most criticalphase of the disease is the first 24 to 72 hours.
Because RSV and other causative agents are shed in hightiters for days after the onset of the illness, contact isolationto prevent infecting other patients, staff, and family mem-bers is strongly recommended. RSV is easily transmitted onhands, clothing, equipment, cribs, and so forth. Limitingchild-to-child contact, washing toys between children’s useof them, and careful handwashing are the most effectivemethods of preventing nosocomial infections.
Respiratory SupportOxygen should be administered to infants with all but themildest cases of bronchiolitis. The oxygen is optimally
humidified and of a concentration sufficient to maintainSaO2 at more than or equal to 92%. The child can beweaned from the oxygen when oxygen saturation levelsremain higher than 94% (Cincinnati Children’s HospitalMedical Center, 2006). Continuous pulse oximetry is rec-ommended for infants in acute distress. Take care todocument oxygen saturations when the child is awakeduring quiet time, asleep, and with crying. Desaturationsto less than 90% with crying are likely; therefore, closemonitoring until saturations return to baseline (morethan 92%) is essential. The infant should be suctionedwhen clinically indicated before feedings, prior to inhala-tion therapy, and as needed. The use of chest physiother-apy, cool-mist therapy, and aerosol therapy with salinehave not been found to be helpful (Cincinnati Children’sHospital Medical Center, 2006).
Pharmacologic SupportAlthough treatment of bronchiolitis focuses on support-ive therapy, pharmacologic interventions may proveeffective in certain individuals. These medicationsinclude antiviral agents, bronchodilators, and possiblycorticosteroids.
Ribavirin (Virazole) is an antiviral agent (also used totreat hepatitis C) that has been demonstrated to reducethe severity of bronchiolitis caused by RSV when admin-istered early during the course of the illness. The drugcan be used on the intubated, mechanically ventilatedpatient as well as the nonintubated patient. In mechani-cally ventilated infants, most of whom were previouslyhealthy and had no underlying conditions, ribavirin treat-ment has been demonstrated to be safe and was associ-ated with a reduced need for mechanical ventilation andsupplemental oxygen, shorter duration of hospitalization,and cost-effectiveness (Cooper et al., 2003). Other candi-dates for ribavirin therapy include infants at increasedrisk for respiratory complications and respiratory failurebecause of underlying cardiac, lung, or immunodefi-ciency disease.
caREmindercaREminderNurses and respiratory therapists administering ribavirinshould wear a specially designed mask to prevent exposure toribavirin particles released into the air. Although no studieslink ribavirin use to defects in human embryos, it isrecommended that pregnant personnel wear a mask when inthe room of the child receiving ribavirin.
Bronchodilators and corticosteroids have limitedeffects on a child with bronchiolitis. However, this phar-macologic therapy may assist with respiratory benefits,such as ease of breathing, improved oxygenation, andincreased respiratory drive.
Preventive therapies for bronchiolitis are used in lim-ited populations. Children with bronchopulmonary dys-plasia (BPD) and congenital heart disease should receivemonthly Synagis vaccines during the RSV season.
Chapter 16 n n The Child With Altered Respiratory Status 693

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:36 User ID: muralir 1BlackLining Disabled
Nutrition and RestNutritional care for the infant with bronchiolitis includessupportive fluid and electrolyte replacement. Close mon-itoring of fluid and electrolyte status, including accuratemeasurement of intake and output with urine specificgravities, is essential to assess for dehydration.
caREmindercaREminderIn the case of severe respiratory distress or a respiratory rateof 60 breaths per minute or more, the infant should havenothing by mouth, and fluid should be given intravenously.
Infants hospitalized with acute bronchiolitis are usingall their energy to breathe. These infants are too uncom-fortable to respond to the social stimuli they are accus-tomed to, such as television or interaction with siblings.Minimizing energy expenditure and oxygen consumptionshould remain a primary goal of therapy until oxygen sat-uration levels are continuously within normal limits.Soothing activities, such as play with musical toys andholding and rocking by parents, will help the infant relax.As the child’s condition improves, quiet play activitiesmay be gradually reintroduced.
Respiratory distress or air hunger creates anxiety inboth infant and parents. The irritable, crying, inconsol-able infant is unable to drink fluids and is exhausting tocare for. Parents are often suffering from frustration andworry, as well as being completely exhausted at the timeof admission to the hospital. These parents need the op-portunity to express their feelings and receive support.Nurses or social service personnel are the ideal membersof the healthcare team to provide these interventions tothe family of an ill infant.
Community CareCaregivers play an active role in health management,because most children are not hospitalized and do notrequire 24-hour care by the healthcare team. Parental orcaregiver education is essential, especially if the child isnot hospitalized and is cared for at home. Teach theparents to recognize the signs of increasing respiratorydistress, such as grunting, retractions, pallor, and cyano-sis, and state appropriate actions to take. Also instructhow to count the respiratory rate for a full minute, duringboth sleep and awake times. Encourage parents to pro-mote fluid intake, to measure and record the infant’s oralintake during the illness, and to observe for signs of dehy-dration. Other issues relevant to the care of the infantwith bronchiolitis in the home include positioning withthe head of the bed elevated for comfort and to facilitateremoval of secretions, and quiet play activities as thechild’s energy level permits. Encourage parents to calltheir healthcare provider if they have any doubts abouttheir infant’s respiratory status. Teach families respira-tory infection control measures, such as washing hands,avoiding exposure to illness, and staying current withroutine immunizations. Additional preventive measuresinclude eliminating exposure to cigarette smoke and lim-
iting contact with crowded areas and other children (e.g.,daycare).
BronchitisBronchitis is defined as a transient inflammatory processinvolving the distal trachea and major bronchi. The phar-ynx and nasopharynx may also be involved; the laryngealand subglottic regions are not. Bronchitis can be acute,chronic, or recurrent.
As with most viral respiratory infections, the peak inci-dence is in winter and early spring. The disease appearsto be more common in younger children and in males. Inthe child with a competent immune system, bronchitisusually has a viral cause.
PathophysiologyMost episodes of acute bronchitis caused by bacteriaoccur as secondary infections while airways are vulnera-ble after a prior viral attack or other insult. Although ex-posure to irritants such as gastric acid or passive smokeand environmental pollutants can produce acute symp-toms, these insults contribute more commonly to symp-toms in children with reactive airways (see Asthma).
Chronic and recurrent bronchitis in children are con-ditions that are not clearly understood. Viral or bacterialagents attack the airway mucosa. Pathologic changescommonly seen in chronic bronchitis in childhoodinclude thickened bronchial walls, mucous gland hyper-trophy, and chronic inflammation. The ciliated epithe-lium becomes damaged, mucous gland activity increases,and neutrophils infiltrate the airway wall and lumen. Thisprocess accounts for what sometimes appears to be puru-lent sputum, in the absence of a bacterial infection.Mucociliary transport is disrupted, and this stasis contrib-utes to secondary bacterial infection. Because these char-acteristics are commonly seen in asthmatic patients aswell, a pathologic link between the two conditions is sus-pected (Table 16–4) (Jartti, M€akel€a, Vanto, & Ruuska-nen, 2005).
Chronic bronchitis in children may be a symptom of anunderlying pulmonary disorder and may be an importantfactor in predisposing the child to chronic respiratorysymptoms and lung dysfunction even into the adult years.
AssessmentTake a careful history. The onset of viral bronchitis isgenerally gradual, beginning with upper respiratorysymptoms such as rhinitis and a minimal cough. Three to4 days later, the cough becomes more pronounced. Notethe quality of the cough; a bronchial cough begins as dryand nonproductive, and progresses to become looser andmore productive. Auscultation of the chest may be unre-markable during the early stages; rhonchi and wheezingmay be heard as the cough progresses. Low-grade fever(<101 �F [38.3 �C]) is common. Young children generallyswallow the mucus, often resulting in vomiting and par-oxysmal coughing. During the recovery phase of the last7 to 10 days, the cough subsides, and the fever resolves. If
694 Unit 3 n n Managing Health Challenges
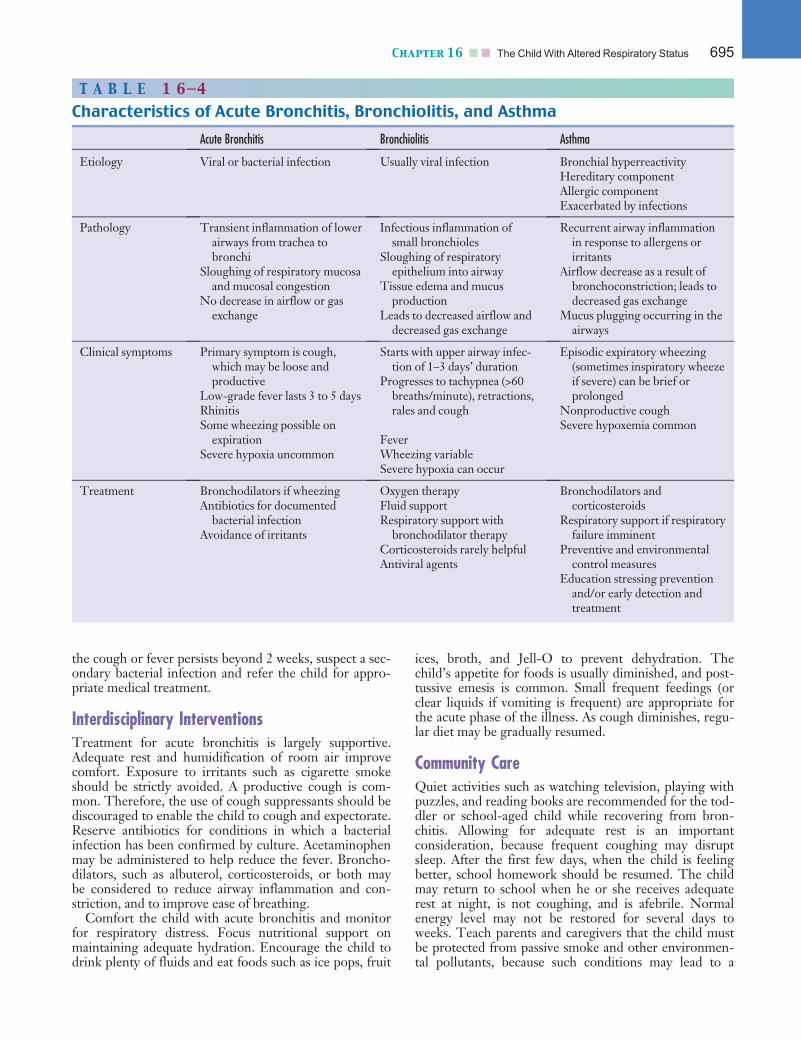
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:36 User ID: muralir 1BlackLining Disabled
the cough or fever persists beyond 2 weeks, suspect a sec-ondary bacterial infection and refer the child for appro-priate medical treatment.
Interdisciplinary InterventionsTreatment for acute bronchitis is largely supportive.Adequate rest and humidification of room air improvecomfort. Exposure to irritants such as cigarette smokeshould be strictly avoided. A productive cough is com-mon. Therefore, the use of cough suppressants should bediscouraged to enable the child to cough and expectorate.Reserve antibiotics for conditions in which a bacterialinfection has been confirmed by culture. Acetaminophenmay be administered to help reduce the fever. Broncho-dilators, such as albuterol, corticosteroids, or both maybe considered to reduce airway inflammation and con-striction, and to improve ease of breathing.
Comfort the child with acute bronchitis and monitorfor respiratory distress. Focus nutritional support onmaintaining adequate hydration. Encourage the child todrink plenty of fluids and eat foods such as ice pops, fruit
ices, broth, and Jell-O to prevent dehydration. Thechild’s appetite for foods is usually diminished, and post-tussive emesis is common. Small frequent feedings (orclear liquids if vomiting is frequent) are appropriate forthe acute phase of the illness. As cough diminishes, regu-lar diet may be gradually resumed.
Community CareQuiet activities such as watching television, playing withpuzzles, and reading books are recommended for the tod-dler or school-aged child while recovering from bron-chitis. Allowing for adequate rest is an importantconsideration, because frequent coughing may disruptsleep. After the first few days, when the child is feelingbetter, school homework should be resumed. The childmay return to school when he or she receives adequaterest at night, is not coughing, and is afebrile. Normalenergy level may not be restored for several days toweeks. Teach parents and caregivers that the child mustbe protected from passive smoke and other environmen-tal pollutants, because such conditions may lead to a
T A B L E 1 6—4
Characteristics of Acute Bronchitis, Bronchiolitis, and Asthma
Acute Bronchitis Bronchiolitis Asthma
Etiology Viral or bacterial infection Usually viral infection Bronchial hyperreactivityHereditary componentAllergic componentExacerbated by infections
Pathology Transient inflammation of lowerairways from trachea tobronchi
Sloughing of respiratory mucosaand mucosal congestion
No decrease in airflow or gasexchange
Infectious inflammation ofsmall bronchioles
Sloughing of respiratoryepithelium into airway
Tissue edema and mucusproduction
Leads to decreased airflow anddecreased gas exchange
Recurrent airway inflammationin response to allergens orirritants
Airflow decrease as a result ofbronchoconstriction; leads todecreased gas exchange
Mucus plugging occurring in theairways
Clinical symptoms Primary symptom is cough,which may be loose andproductive
Low-grade fever lasts 3 to 5 daysRhinitisSome wheezing possible on
expirationSevere hypoxia uncommon
Starts with upper airway infec-tion of 1–3 days’ duration
Progresses to tachypnea (>60breaths/minute), retractions,rales and cough
FeverWheezing variableSevere hypoxia can occur
Episodic expiratory wheezing(sometimes inspiratory wheezeif severe) can be brief orprolonged
Nonproductive coughSevere hypoxemia common
Treatment Bronchodilators if wheezingAntibiotics for documented
bacterial infectionAvoidance of irritants
Oxygen therapyFluid supportRespiratory support with
bronchodilator therapyCorticosteroids rarely helpfulAntiviral agents
Bronchodilators andcorticosteroids
Respiratory support if respiratoryfailure imminent
Preventive and environmentalcontrol measures
Education stressing preventionand/or early detection andtreatment
Chapter 16 n n The Child With Altered Respiratory Status 695

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:36 User ID: muralir 1BlackLining Disabled
repeated bronchitis episode. Dust and allergy proofingthe home environment, especially sleeping quarters,helps prevent subsequent recurrences (see CommunityCare 16–2).
Answer: Cough is one of the presenting symptomswith bronchiolitis, bronchitis, and asthma. However,
Jose is afebrile and wheezing, which are solely symptoms ofasthma.
PneumoniaThe term pneumonia describes any inflammatory condi-tion of the lung parenchyma, resulting most frequentlyfrom infection, in which the alveoli are filled with fluid,blood cells, or both, and oxygen exchange is impaired.Pneumonia can be a primary illness (often called community-acquired pneumonia or CAP) or can develop as a complica-tion of another respiratory infection or underlying illness.It is distinguished from the more common upper respira-tory tract infections by the presence of lower respiratorytract signs and symptoms such as tachypnea, rales, and asso-ciated areas of infiltration on chest radiographs.
The annual incidence of pneumonia is 34 to 40 casesper 1,000 in children younger than 5 years of age (Tay-lor, 2003). Although this incidence is not high, pneu-monia is a major cause of morbidity and mortality inchildren worldwide. Most deaths from pneumonia occurin third world countries, yet pneumonia also remains animportant factor in morbidity in developed countries,especially among the chronically ill pediatric population.
The causes of pneumonia in children vary dependingon the season and the child’s age and health status. Pneu-monia most likely develops when the body is unable todefend against infectious agents. Infectious agents may be
viruses, bacteria (Chart 16–1), mycoplasma, fungi, chemi-cals, foreign substances, or various other organisms ormaterials. Newborn infants acquire pneumonia patho-gens by several means. Transplacental infection, aspira-tion of organisms during passage through the birth canal,and contact with humans or contaminated equipment im-mediately after birth are the most common mechanisms.After 1 month of age, viruses become the most commoncause of pneumonia. Bacterial pneumonias occur year-round but are most common during the winter months(Cooper, Banasiak, & Allen, 2003).
Children with chronic illnesses, such as asthma, BPD,or CF, often develop recurrent or persistent pneumoniasbecause of respiratory compromise. Immunodeficiencies,congenital heart disease, neuromuscular diseases, andvarious hematologic and oncologic diseases all are condi-tions that can render the child compromised in the abilityto fight pneumonias and other infections.
Not all inflammation of the lung is infectious in origin.Pneumonia can be caused by aspiration of foreign sub-stances. Gastroesophageal reflux with aspiration, smokeinhalation, hydrocarbon ingestion, aspiration of baby tal-cum powder, near-drowning, and some autoimmuneprocesses (such as pulmonary hemosiderosis) all canresult in a pneumonialike syndrome.
PathophysiologyAlthough the term pneumonia refers to a multitude of dis-orders that differ widely depending on causative agent,each involves an inflammatory response. The respiratorytract is normally equipped with a variety of natural mech-anisms to guard the lungs against infection. The nose fil-ters air, the cough reflex expels objects or organisms inthe laryngeal airway, and cilia in the walls of the tracheaand bronchi trap small particles and remove them in mu-cus. When any of these defenses is impaired, pathogensinvade and initiate the inflammatory response.
CHART 16–1 Common Viral and Bacterial Causes of Pneumonia
Causative Agent Age Season
Viral
Respiratory syncytial virus Infants, young preschool Winter
Parainfluenza viruses 1 and 2 Preschool Fall
Parainfluenza virus 3 Infants and preschool Spring
Influenza viruses A and B Preschool, school age Winter
Adenoviruses All ages Year-round
Bacterial
Chlamydia pneumoniae Acquired during birthing processAll ages
Year-round
Mycoplasma pneumoniae School age Year-round with peaks in fall and early winter
Streptococcus pneumoniae Acquired during birthing processAll ages
Year-round
696 Unit 3 n n Managing Health Challenges

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:37 User ID: muralir 1BlackLining Disabled
Viral pathogens enter the upper respiratory tract andspread through the airways. The severity of the inflamma-tory response and the associated pathophysiology vary.Characteristic features include loss of alveolar cell wall in-tegrity, resulting in accumulation and stasis of fluid andmucus, and smooth muscle contraction. These changesobstruct airflow and cause ventilation–perfusion mis-match, a condition in which the diminished alveolar–capillary gas exchange is no longer adequate for theblood supply, thus resulting in hypoxia and hypercapnia.
Bacteria are introduced into the lungs through the in-halation of infectious droplets or through the blood-stream. Alveolar involvement in bacterial pneumonia ischaracteristically more intense than that seen in viralinfections. The alveoli can fill rapidly with proteinaceousfluid, causing ventilation–perfusion mismatch, or bacte-rial agents can cause necrosis of intra-alveolar septa, caus-ing abscesses and destruction of lung architecture.
Similar processes occur in aspiration pneumonia. Whengastric contents, secretions, blood, or volatile chemicalcompounds enter the lung, the presence of one or more ofthese irritants initiates the characteristic inflammatoryresponse. Gastroesophageal reflux is associated with pneu-monia when the acidic contents enter the pharynx, where,if protective mechanisms fail, it is aspirated. Baby talcumpowder and other fine-particle materials inhaled into thepharynx and lower airways precipitate tissue inflammation.Hydrocarbons (organic solvents found in gasoline, furniturepolish, cleaning compounds, lighter fluid, paint thinner,kerosene, and other substances) aspirated into the alveolarspace dissolve surfactant lipids and impair surface tension,thereby reducing activity of surfactant. Atelectasis, alveolarcell damage, edema, granulocyte infiltration, hemorrhage,and necrosis can result. Smoke inhalation also can causechemical irritation, depending on the source of the smoke.
AssessmentPneumonia, regardless of etiology, is generally distin-guished from less severe respiratory tract infections by thetype of cough (sputum producing, rather than dry and hack-ing) and by tachypnea, crackles, and cyanosis. Althoughdistinguishing viral from bacterial pneumonia by clinicalmanifestations alone usually is not possible, understandingthe characteristic presentation of each is important.
Viral pneumonia typically has a gradual onset, begin-ning with an upper respiratory tract infection of 3 to 4days’ duration. This initial illness may include low-gradefever and rhinorrhea, with a gradual development ofcough and increasing respiratory distress. The child inrespiratory distress may manifest cyanosis, grunting res-pirations, retractions, coarse crackles, or wheezing.
Bacterial pneumonia has a more acute pattern of onset.Suspect bacterial pneumonia in a child with the symp-toms already listed, plus a cough that produces thickgreen, yellow, or blood-tinged sputum, and an overallappearance of lethargy and malaise. Chest pain may alsobe present. Fever and increased respiratory rate arehallmark manifestations of bacterial pneumonia. Checkfor dehydration stemming from poor oral intake andincreased insensible fluid losses from fever and tachypnea.
Tachycardia, hypotension, and poor perfusion may indi-cate sepsis and early shock.
The young child with fever, retractions, tachypnea, orgrunting will be irritable and difficult to console. Hypoxiaand hypercarbia result in decreased level of consciousnessin a child of any age. Be ready to help parents cope withanxiety related to the often severe acute onset of respira-tory symptoms.
Families of children with chronic conditions live withconstant concerns regarding exposure to a potentiallyfatal infection and may exhibit and act on feelings of guiltand anger upon diagnosis of pneumonia. Counseling andsupport for these families during acute illness episodes isimperative.
Culture confirms the diagnosis of bacterial pneumonia.Common bacterial pathogens include S. pneumoniae, H.influenzae, S. aureus, group B streptococci, Chlamydia pneu-moniae, and M. pneumoniae. Chest radiographs may be usedto determine the lung fields affected by the pneumonia or ifadditional problems exist (e.g., atelectasis, pleural effusions).
Interdisciplinary InterventionsInterventions for pneumonia involve careful assessmentof respiratory status and general supportive care (see
for Care Paths: An Interdisciplinary Plan ofCare for the Child With Pneumonia). Whether a childwith pneumonia requires hospitalization depends onage, general health status, and the suspected organism.Because infants readily develop respiratory distress withaccompanying hypoxia, apnea, poor feeding, and dehy-dration, hospitalization is common.
For the hospitalized child, careful and frequent respira-tory assessment, including evaluation of respiratory rateand effort, color, presence and location of retractions,breath sounds, and oxygen saturation levels, is requiredfor the infant or child with pneumonia. Report changesin respiratory status immediately for further medical eval-uation. Supplemental oxygen may be needed to keep sat-uration levels more than or equal to 92%. For somechildren, continuous pulse oximetry is indicated. Imple-ment chest physiotherapy (percussion, vibration, and pos-tural drainage) to facilitate clearing of secretions, withspecial attention paid to any identified areas of involve-ment or infiltration on the chest radiograph (see Treat-ment Modalities earlier in this chapter).
In most viral pneumonia cases, especially in infants,antibiotics are given because secondary bacterial involve-ment cannot be ruled out. Many experts consider thisapproach the safest and most practical, although it maynot alter the course of the illness. Infants are generallytreated with broad-spectrum antibiotics such as ampicil-lin and an aminoglycoside. Specific antiviral therapy forRSV (ribavirin) is considered for infants and childrenwith chronic illnesses (see Bronchiolitis).
caREmindercaREminderChildren in severe respiratory distress should receive nothingby mouth because of the increased work of breathing and therisk of aspiration.
Chapter 16 n n The Child With Altered Respiratory Status 697

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:37 User ID: muralir 1BlackLining Disabled
Fluids and medications are administered by the intrave-nous route. Fever and tachypnea result in insensible fluidloss; thus, the child with pneumonia is at risk for dehydra-tion. Intake and urine output, and urine specific gravity aremeasured frequently, and skin turgor is assessed to monitorhydration status. Body temperature is monitored, andfevers are treated with acetaminophen, because a high bodytemperature can increase oxygen requirements and exacer-bate insensible fluid loss. As respiratory status improves,the diet can be advanced from clear liquids to regular dietas tolerated. For recurrent aspiration pneumonia, suck andswallow coordination and gastroesophageal reflux may beevaluated to identify risk for aspiration before full oralfeedings are resumed. If oral intake is allowed, feedingsshould be given with caution, to avoid aspiration.
The child and family require constant information andsupport from all health professionals during an acute pneu-monia episode. Social services may provide counseling serv-ices or referrals in the event of life-threatening or chronicillness. After the child’s condition becomes more stable,parents, nurses, and child life specialists should collaboratein planning quiet diversionary activities appropriate for age.
Community CareHome health support for parents who must learn to per-form respiratory assessment and administer medication isan option for the older child being treated at home. Chil-dren with pneumonia are usually evaluated in an ambu-latory care setting 2 to 3 weeks after treatment iscompleted, to ensure that their respiratory symptoms arefully resolved or, if a chronic condition exists, to ensurethat they are being managed effectively at home. Repeatchest radiographs may be completed to evaluate persis-tent symptoms or confirm complete recovery.
Chronic Conditions of the
Respiratory System
Chronic conditions of the respiratory system can have aserious affect on children and adolescents, and may sub-stantially alter their quality of life and physical and socialdevelopment (see Chapter 12 for a more extensive discus-sion of the affect of chronic conditions on the child andthe family). Such conditions can affect all other aspects ofthe child’s and family’s physical and emotional health,and can lead to development of comorbid conditions,increased risks for morbidity, and, at times, early death.The most common chronic conditions seen in childhoodand adolescence are asthma, BPD, and CF. Chronic pul-monary conditions during childhood and adolescence arecharacterized by periods of relative wellness interspersedwith periods of acute exacerbation, often necessitat-ing healthcare interventions (e.g., ambulatory care visits,emergency room visits, or hospitalization). Although no‘‘cures’’ exist for these chronic conditions, self-care man-agement is essential. Extensive child and family educationis required, related to prevention, recognition of symp-toms, early and ongoing medical treatments, and optimi-zation of self-care and home care strategies.
AsthmaAsthma is defined by the National Heart, Lung andBlood Institute (2007) as the following:
A chronic inflammatory disorder of the airways in whichmany cells and cellular elements play a role; in particular,mast cells, eosinophils, neutrophils (especially in suddenonset, fatal exacerbations, occupational asthma, and patientswho smoke), T lymphocytes, macrophages, and epithelialcells. In susceptible individuals, this inflammatory processcauses recurrent episodes of coughing (particularly at nightor early in the morning), wheezing, breathlessness, and chesttightness. These episodes are usually associated with wide-spread but variable airflow obstruction that is often reversibleeither spontaneously or with treatment. (p. 9)
During childhood and adolescence, pediatric asthmacan have a profound effect on growth and development,and on the daily lives of families. During the past fewdecades, assessment, management, and self-care strat-egies for children and adolescents with asthma haveresulted in increased longevity, along with an increasedshift from hospital to home care. Significant advances inevidenced-based management guidelines, pharmacologicproducts, and durable medical equipment have resultedin improved disease outcomes and quality of life for thesechildren and their families. Comprehensive asthma man-agement programs that address important issues such asaccurate diagnosis, patient and family education, environ-mental control, and early treatment of asthma exacer-bations have been shown to significantly improve theoverall health of children with asthma (Liu and NationalInstitutes of Health, 2004; National Heart, Lung andBlood Institute, 2007). The following discussion ofasthma incorporates the most recent management guide-lines provided by the National Heart, Lung and BloodInstitute. A complete version of the guidelines is availableat http://www.nhlbi.nih.gov/guidelines/asthma. The fourcomponents of care presented in the guidelines and dis-cussed in this section include
1. Assessment and monitoring2. Education3. Control of environmental factors and comorbid
conditions4. Medications
Question: In following discussion, does Jose rep-resent the typical incidence and prevalence of asthma
in children?
Pediatric asthma is the single largest public health bur-den, with more than 6.5 million children and adolescentswith asthma in the United States (National Heart, Lungand Blood Institute, 2007). Asthma is the third leadingcause of hospitalization among children younger than15 years of age. It is the leading cause of school absentee-ism caused by a chronic condition (Asthma and AllergyFoundation of America, 2008).
698 Unit 3 n n Managing Health Challenges

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:37 User ID: muralir 1BlackLining Disabled
WORLDVIEW: Social disparities play a large role in pediatricasthma prevalence, morbidity, and mortality. Populations from lowsocioeconomic and urban, inner city areas have high rates of asthmaand asthma-related morbidity and mortality. Prevalence of asthmaamong African American children is high (38% higher than amongwhites and 95% higher than among Hispanics). Compared with nonmi-nority peers, African American adolescents are more likely to havepoorly controlled asthma, to experience restrictions in activity, to behospitalized, and to report severe functional disability because of theirasthma. In addition, African American children covered by Medicaidhave worse asthma and use less preventive asthma medications thanother children in the same managed Medicaid population (AmericanLung Association, 2005).
Answer: Jose is Mexican American, lives in a sub-urban environment, and thus does not represent the
prevalence of asthma among inner city African American chil-dren. However, Jose is typical in that he does have seasonalallergies and his allergies are a trigger for his asthma.
PathophysiologyThe pathology of asthma is best described as a conditioncharacterized by reversible (in most cases) changes in theairway that lead to bronchoconstriction, airway hyperres-ponsiveness, and airway edema. At a cellular level, mastcells in the airways release inflammatory and chemotacticmediators, such as histamine, causing smooth musclecontraction and bronchoconstriction. Increased mucussecretion by goblet cells causes epithelial damage. Theincrease in mucus secretion then leads to increased per-meability and sensitivity to inhaled allergens, irritants,and inflammatory mediators. The result is airway edema,mucus hypersecretion and plugging, and substantial air-way narrowing, leading to rapid airway obstruction (Fig.16–16). This acute reaction, called the early asthmatic
response, generally resolves with bronchodilator treatmentwithin 1 to 3 hours.
‘‘Remodeling’’ or permanent changes in the airwaymay occur. Persistent changes in the airway structure,such as subbasement fibrosis, mucous hypersecretion,injury to epithelial cells, smooth muscle hypertrophy, andangiogenesis, may occur (National Heart, Lung andBlood Institute, 2007, p. 9).
The physiologic changes that occur during an acuteepisode contribute to the clinical findings characteristicof asthma exacerbation. Air becomes trapped behind thenarrowed airways and the functional residual capacityincreases, causing hyperinflation of the lungs, which canbe seen on a chest radiograph. This hyperinflation helpskeep the airways open that are already narrowed frombronchoconstriction, mucosal edema, and mucus. Theaccessory muscles of respiration help to maintain thelungs in a hyperinflated state; therefore, the child haschest retractions. Hypoxemia results from ventilation–perfusion mismatch, because areas of the lung are notbeing well ventilated.
A key development in the study of asthma has beenthe recognition that a late asthmatic response alsooccurs. Mediator release from the mast cells causesdirect migration and activation of inflammatory infil-trates, predominantly eosinophils and neutrophils, andmast cell degranulation causes the release of leuko-trienes and prostaglandins, which leads to furtherinflammation. Airway response in the form of obstruc-tion can occur 4 to 6 hours later and can last 24 hours ormore. The late asthmatic response has a number of fea-tures characteristic of chronic asthma: reduced respon-siveness to bronchodilators, increased mucus secretion,heightened airway responsiveness, and the developmentof airway inflammation. With the onset of the lateasthmatic response, a vicious self-perpetuating cycleof asthma symptoms ensues.
The precise cause of the inflammatory response seenin asthma is yet to be discovered. Three potential causesinclude innate immunity, genetics, and environmentalfactors. Innate immunity refers to the balance betweenTh1-type and Th2-type cytokine responses in early life.Numerous factors are believed to affect this balance andpotentially lead to immune changes in which the Th1immune response that fights infection is dominated byTh2 cells, leading to the expression of allergic diseasesand asthma. It is hypothesized that exposure to otherchildren, less frequent use of antibiotics, and ‘‘countryliving’’ are factors that enhance the Th1 response andlower the incidence of asthma (National Heart, Lung andBlood Institute, 2007, p. 10).
Scientific evidence exists that asthma is partly hereditary.Studies have shown that the risk of having an asthmaticchild is significantly greater when one or both parents haveasthma than if neither parent is affected (Ober, 2005). At-opy (an increased predisposition to form antibodies on ex-posure to common environmental antigens) is present inmost patients with asthma. Atopy is at least partially heredi-tary, although exposure to certain allergens early in life(e.g., pollens, animal dander) may influence the develop-ment of asthma in a child who is genetically predisposed.
Muscle
Muscletightening
Lining
Normal airway Asthmatic airway
Inflammationand swelling
Excessivemucus
Figure 16—16. Asthmatic airway compared with a normal airway.
Chapter 16 n n The Child With Altered Respiratory Status 699

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:37 User ID: muralir 1BlackLining Disabled
Food allergens, however, are rarely responsible for airwayreactions in children. Although the link between asthmaand atopy is not completely clear, exposure to allergensmay cause airway inflammation and may lead to increasedairway responsiveness.
Other factors felt to be involved in the development ofairway reactivity and asthma include respiratory infec-tions and environmental pollutants (many which may beseasonal in nature; see Tradition or Science 16–2). RSVbronchiolitis, for example, has been causally linked toenhanced airway reactivity, especially in children with afamily history of atopy. Indoor air pollutants play a majorrole in asthma exacerbations, and outdoor air pollutantshave been found to reduce lung function in children incities with high levels of outdoor air pollution (Gauder-man et al., 2004).
Assessment
Question: The peak expiratory flow rate (PEFR) isan important assessment tool. Why would the nurse
assessing Jose in the emergency department not obtain aPEFR?
According to National Heart, Lung and Blood Institute(2007) guidelines, a careful history is one of most impor-tant elements in evaluating the child. Historical data canidentify possible high-risk patients and assist in planning
for appropriate interventions. The key information tocompile is listed in Focused Health History 16–2. Thehistory can help to rule out other conditions that maypresent with cough, wheezing, and shortness of breath.Additionally, if the child presents with recurring epi-sodes, the history can identify possible precipitating fac-tors and treatments that have been effective in the past.
Suspect asthma in a child with wheezing and varyingdegrees of respiratory distress. And, for many childrena history of chronic cough (worse at night) is a classicsymptom. The hallmark manifestation of asthma is theresult of airway obstruction. The child may present witha worsening cough and wheezing, and may complainof chest tightness (Clinical Judgment 16–2). Because ofbronchospasm, airway inflammation, and mucous plug-ging, expiration becomes increasingly difficult, and thereis air trapping. The child with a persistent asthma exacer-bation may be unable or unwilling to lie flat becausebreathing is more difficult in this position.
The National Heart, Lung and Blood Institute (2007)guidelines suggest using multiple measures of the child’slevel of current impairment (frequency and intensity ofsymptoms, low lung function, and limitations of dailyactivities) and future risk (risk of exacerbations, progres-sive loss of lung function, or adverse side effects frommedications) to assess the child’s status. Some childrencan be at high risk for frequent exacerbations even if theyhave few day-to-day effects of asthma. Some childrenmay have early or prodromal signs and symptoms hoursto days before an asthma exacerbation.
Focus the physical examination on general health,including growth and development, hydration status, andany signs of drug-related side effects.
Hypoxemia is universal in the child with moderate tosevere symptoms. Monitor blood gases. Carbon dioxideretention is also a common finding. Hypoxemia andhypercarbia result from air trapping in the alveoli andventilation–perfusion mismatch. A PaCO2 level morethan 50 mm Hg indicates ventilatory failure unless thechild has a preexisting chronic lung disease. Review radi-ograph reports. Typical radiograph findings in the childwith extensive asthma symptoms are hyperexpansion, ate-lectasis, and a flattened diaphragm. Younger children areparticularly prone to develop atelectasis because of theirsmall airways and underdeveloped collateral ventilation.Infiltrates and pneumothoraces are uncommon findings.
Tradition or Science 16—2
Does secondhand smoke exacerbate asthmasymptoms?
EVIDENCE-BASED
PRACTICEEVIDENCE-BASED
PRACTICEEnvironmental pollutants such as tobaccosmoke have been clearly linked to
asthma exacerbations in children (Centers for DiseaseControl, 2006; Institute of Medicine Committee on theAssessment of Asthma and Indoor Air, Division of HealthPromotion and Disease Prevention, 2000). In childrenwith asthma, parental (particularly maternal) smoking hasbeen associated with increases in symptom severity andhospitalizations. Exposure rates among children arehigh, with approximately 60% of children age 3 to 11years in the United States exposed to secondhand smoke(Centers for Disease Control, 2006). In 2002, the Cen-ters for Disease Control estimated that more than $157billion in annual economic costs and more than440,000 premature deaths were attributable to second-hand smoke. The relationship of secondhand smoke ex-posure to the development of asthma is less well defined;however, some research has suggested that maternalsmoking may cause alteration in the developing lungbefore birth (Institute of Medicine Committee on theAssessment of Asthma and Indoor Air, Division of HealthPromotion and Disease Prevention, 2000).
Alert! Pay special attention to children at high risk of asthma-relateddeath. Children with a history of the following events are at increased risk:
� Prior admission to an intensive care unit for asthma (with or withoutintubation)
� Two or more hospitalizations for asthma, three or more emergency roomvisits for asthma, or both, during the past year
� Hospitalization or emergency room visit for asthma during the past month� Current use of or recent withdrawal from systemic corticosteroids� History of psychiatric disease or psychosocial issues� History of nonadherence to asthma treatment plan (National Heart, Lung
and Blood Institute, 2007)
700 Unit 3 n n Managing Health Challenges

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:37 User ID: muralir 1BlackLining Disabled
Monitor blood pressure. Pulsus paradoxus (a decreasein systemic blood pressure with inspiration) occursbecause the negative pleural pressures become more neg-ative as a result of lung hyperinflation. A decrease of12 mm Hg or more in systolic blood pressure with inspi-ration rather than with expiration indicates moderate dis-tress. A decrease of 20 mm Hg or more occurs in severeasthma exacerbations. Pulsus paradoxus may be difficultto assess in the young child because of rapid heart and re-spiratory rates. In the preverbal child, also evaluate thequality of the cry (weak vs. lusty).
Diagnostic studies helpful in evaluating the child withasthma symptoms include spirometry, PEFR, pulmonaryfunction tests, bronchoprovocation (with methacholine,histamine, cold air, or exercise), arterial blood gases,pulse oximetry, and chest radiographs (see Tests and Pro-cedures 16–1 earlier in this chapter). In addition, exami-nation of biomarkers of inflammation are demonstrating
promise as useful tools for diagnosis and assessment ofasthma. Biomarker assessment includes total and differ-ential cell count; and mediator assays of sputum, blood,urine, and exhaled air (National Heart, Lung and BloodInstitute, 2007, p. 12).
Spirometry is used to obtain objective measures of lungfunction. During the initial assessment, spirometry helpsto establish a diagnosis of asthma. Spirometry is also rec-ommended after treatment is initiated and peak inspira-tory function is stabilized, during periods of progressiveor prolonged loss of asthma control, and finally, as anassessment tool every 1 to 2 years to evaluate response totherapy.
In contrast, peak flow meters are used to measurePEFR and are designed for monitoring purposes ratherthan diagnostic purposes. PEFR is considered a valuablemeasurement in assessing asthma severity and in evaluat-ing response to therapy. PEFR is the greatest velocity of
Focused Health History 16—2
The Child With Asthma
Nature of symptoms Shortness of breath, wheeze, cough, chest tightness, rhinorrhea, con-ditions such as sinusitis, eczema
Pattern of symptoms Frequency (daily, weekly, monthly), timing (morning vs. nighttime),onset and duration, severity, seasonal, perennial, diurnal variation,associated with physical activity
Aggravating factors or triggers Upper respiratory infections, environmental allergens and irritants(dust mites, mold, inhalants, chemicals, pollens), secondhand smokeexposure or smoke, strong emotional expressions (crying, laughinghard), exercise, weather changes, pets, air pollution, foods or medi-cations, menstruation cycle, stress
Typical exacerbation Prodromal signs and symptoms, temporal progress, and usual man-agement and response to treatment
Previous and current drug therapy Dosage, mode of delivery, response, side effectsDevelopment of disease Age at onset, age at diagnosis, progress of disease, previous evalua-
tions, treatments, and response to current managementEffect of disease Number of emergency room visits, hospitalizations and intensive care
unit admissions in past year, school attendance and performance,activity limitations and exercise tolerance, sleep disturbances, child’sgrowth and development, child’s behavior, effect on siblings, eco-nomic impact
Living situation/environment Presence of smokers in home, pets, housing conditions, home age,heating/air conditioning, carpeting, humidifier, cockroaches
Family and patient perception ofasthma
Knowledge of and belief in chronic nature of asthma, coping styles,family support systems, capacity to recognize exacerbation, eco-nomic resources
General medical history Presence of or history of allergic disorders (allergic rhinitis, atopicdermatitis), recurrent respiratory tract infections, birth history(early injury to lung tissue), symptoms of gastroesophageal reflux,detailed review of systems
History of allergies History of adverse reactions to medications, food, or allergens (pollen,mold, pets)
Family medical history History of IgE-mediated allergy in close relatives, asthma in closerelatives
Chapter 16 n n The Child With Altered Respiratory Status 701
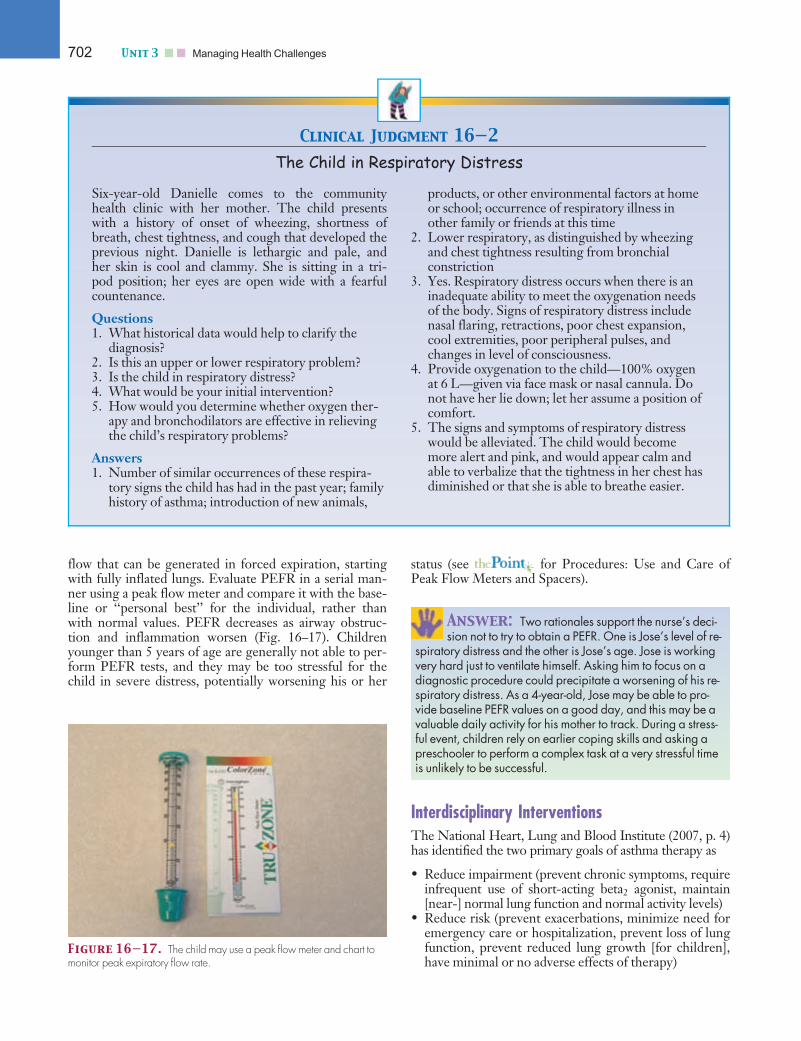
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:37 User ID: muralir 1BlackLining Disabled
flow that can be generated in forced expiration, startingwith fully inflated lungs. Evaluate PEFR in a serial man-ner using a peak flow meter and compare it with the base-line or ‘‘personal best’’ for the individual, rather thanwith normal values. PEFR decreases as airway obstruc-tion and inflammation worsen (Fig. 16–17). Childrenyounger than 5 years of age are generally not able to per-form PEFR tests, and they may be too stressful for thechild in severe distress, potentially worsening his or her
status (see for Procedures: Use and Care ofPeak Flow Meters and Spacers).
Answer: Two rationales support the nurse’s deci-sion not to try to obtain a PEFR. One is Jose’s level of re-
spiratory distress and the other is Jose’s age. Jose is workingvery hard just to ventilate himself. Asking him to focus on adiagnostic procedure could precipitate a worsening of his re-spiratory distress. As a 4-year-old, Jose may be able to pro-vide baseline PEFR values on a good day, and this may be avaluable daily activity for his mother to track. During a stress-ful event, children rely on earlier coping skills and asking apreschooler to perform a complex task at a very stressful timeis unlikely to be successful.
Interdisciplinary InterventionsThe National Heart, Lung and Blood Institute (2007, p. 4)has identified the two primary goals of asthma therapy as
• Reduce impairment (prevent chronic symptoms, requireinfrequent use of short-acting beta2 agonist, maintain[near-] normal lung function and normal activity levels)
• Reduce risk (prevent exacerbations, minimize need foremergency care or hospitalization, prevent loss of lungfunction, prevent reduced lung growth [for children],have minimal or no adverse effects of therapy)
Clinical Judgment 16—2
The Child in Respiratory Distress
Six-year-old Danielle comes to the communityhealth clinic with her mother. The child presentswith a history of onset of wheezing, shortness ofbreath, chest tightness, and cough that developed theprevious night. Danielle is lethargic and pale, andher skin is cool and clammy. She is sitting in a tri-pod position; her eyes are open wide with a fearfulcountenance.
Questions1. What historical data would help to clarify the
diagnosis?2. Is this an upper or lower respiratory problem?3. Is the child in respiratory distress?4. What would be your initial intervention?5. How would you determine whether oxygen ther-
apy and bronchodilators are effective in relievingthe child’s respiratory problems?
Answers1. Number of similar occurrences of these respira-
tory signs the child has had in the past year; familyhistory of asthma; introduction of new animals,
products, or other environmental factors at homeor school; occurrence of respiratory illness inother family or friends at this time
2. Lower respiratory, as distinguished by wheezingand chest tightness resulting from bronchialconstriction
3. Yes. Respiratory distress occurs when there is aninadequate ability to meet the oxygenation needsof the body. Signs of respiratory distress includenasal flaring, retractions, poor chest expansion,cool extremities, poor peripheral pulses, andchanges in level of consciousness.
4. Provide oxygenation to the child—100% oxygenat 6 L—given via face mask or nasal cannula. Donot have her lie down; let her assume a position ofcomfort.
5. The signs and symptoms of respiratory distresswould be alleviated. The child would becomemore alert and pink, and would appear calm andable to verbalize that the tightness in her chest hasdiminished or that she is able to breathe easier.
Figure 16—17. The child may use a peak flow meter and chart tomonitor peak expiratory flow rate.
702 Unit 3 n n Managing Health Challenges

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:38 User ID: muralir 1BlackLining Disabled
As previously mentioned, these goals are accomplishedthrough an interdisciplinary plan that includes assessmentand monitoring, education, control of environmental fac-tors, and careful selection of medication and deliverydevices to meet the child’s needs and individual circum-stances. The following section discusses these care com-ponents as well as the management and treatment ofexacerbations.
Effective asthma management enables children to pur-sue active lifestyles both at home and at school, and toenjoy sleep uninterrupted by asthma symptoms. How-ever, attaining this goal requires special attention tochildren’s unique physiologic states (different from theadult), growth and development, and maturing self-careabilities in light of the tasks of effective asthma manage-ment. These tasks must also be continued while in otherenvironments, such as the school or recreational activitysettings.
Assessment and Monitoring
Question: Does the case study regarding Jose inChapter 10 provide enough information to classify the
severity of his asthma?
Assessment for purposes of diagnosis are discussed in thepreceding section. This section discusses the ongoingassessment and monitoring of the child with asthma.Activities associated with assessment and monitoringinclude assessing the asthma severity to initiate treat-ment, assessing asthma control and adjusting therapy asneeded, and ensuring the child is periodically monitoredby the healthcare provider.
Severity classification of asthma is based on symptomfrequency, nighttime symptoms, character and frequencyof exacerbations, and lung function variability beforetreatment. When asthma is well controlled, the child’soverall asthma severity is classified as intermittent or per-sistent (mild, moderate, or severe) and a ‘‘stepwise’’approach to managing asthma is used to adjust therapy.Therapy is initiated depending on the child’s age groupand the assessed degree of impairment and risk. Impair-ment refers to the frequency and intensity of symptomsand functional limitations being experienced by the child.Risk refers to the likelihood of asthma exacerbations,progressive decline in lung function, or risk of adverseeffects of medication (National Heart, Lung and BloodInstitute, 2007). Tables 16–5 to 16–10 provide an over-view, by age (0–4 years, 5–11 years, and youths �12years) of the National Heart, Lung and Blood Instituteguidelines for initiating therapy and adjusting therapy.In addition, the tables provide the stepwise approachto increase therapy (stepped up) or decrease therapy(stepped down) as indicated by the child’s condition.
Assessment of the child with asthma begins by classify-ing asthma severity. If the child is presenting with symp-toms, identify the precipitating factors for the currentepisodic symptoms (e.g., child was exercising at school,child spent night at friend’s house where cats are
present). Determine whether comorbid conditions existthat may affect asthma management, such as sinusitis,obesity, or stress. Last, assess the child’s knowledge andskills for self-management (National Heart, Lung andBlood Institute, 2007).
Monitoring of the child includes an evaluation of thechild’s daily peak flow monitoring records and using spi-rometry to assess current status. Samples of peak flowmonitoring charts are provided by National Heart, Lungand Blood Institute or makers of peak flow meters, andcan be downloaded from the Internet.
Schedule follow-up visits for the child. The child isseen at 2- to 6-week intervals while gaining control ofasthma symptoms, at 1 to 6 months after asthma controlis achieved and to ensure control is maintained, and at3-month intervals if a step-down therapy is anticipated(National Heart, Lung and Blood Institute, 2007).
Answer: Jose is on albuterol and cromolyn sodiummorning and evening. In addition, he has another
recent episode of an exacerbation of his asthma. However,we still do not have a clear picture of his incidence of daytimeand nighttime symptoms.
Education
Question: What is the role of the nurse regardingthe education about Jose’s asthma?
A primary goal of asthma management is to ensure thechild and the family have the tools and knowledge to self-monitor and manage the child’s condition. Educationfocuses on promoting optimal physical growth and func-tion by minimizing airway obstruction, maximizing phys-ical function despite airway obstruction, and preventingand treating exacerbations and complications of asthmaand its therapy. The child should also achieve and main-tain normal psychosocial growth and function by main-taining optimal psychosocial development and maximalparticipation in his or her own healthcare. To promoteoptimal family functioning, these interventions are inte-grated into the normal daily lifestyle of the family.
Child and family education must be an integral part ofasthma care. Parents and children with asthma often havea poor or incomplete understanding of the disease and itsmanagement, and this lack of knowledge may lead toincreased need for hospitalization and increased health-care costs. Self-care management in children and adoles-cents depends on the individual’s cognitive abilities,maturity, and fine and gross motor skills to manage thedaily responsibilities of asthma care. Cognitive and lan-guage abilities will affect how well the child is able to per-ceive and communicate changes in breathing patterns.Both the parents and the child should assess daily forasthma symptoms, such as increased cough, wheezing,shortness of breath, or irritability, then initiate additionaltherapy as instructed. Beginning in the preschool years,
Chapter 16 n n The Child With Altered Respiratory Status 703
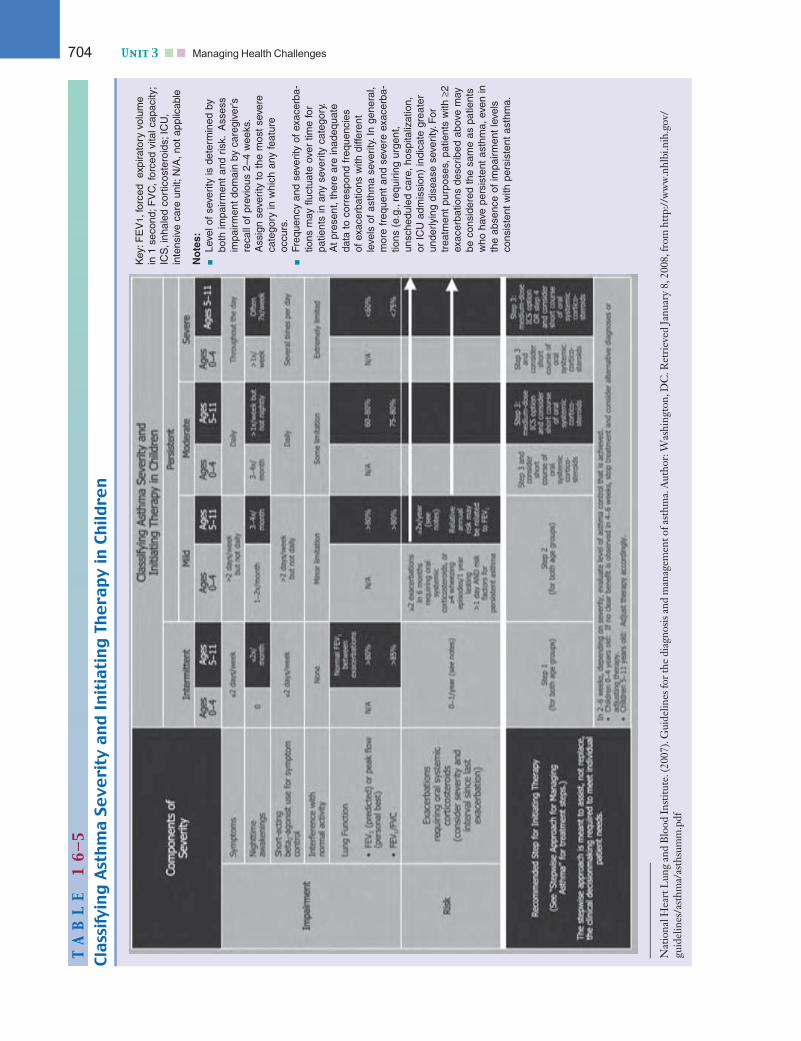
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:38 User ID: muralir 1BlackLining Disabled
TA
BL
E1
6—5
ClassifyingAsthmaSe
verity
andInitiatingTh
era
pyin
Childre
n
Key
: FE
V1,
forc
ed
expi
rato
ry v
olum
e in
1 s
econ
d; F
VC
, for
ced
vita
l cap
acity
;IC
S,i
nhal
ed c
ortic
oste
roid
s; I
CU
,in
tens
ive
care
uni
t; N
/A, n
ot a
pplic
able
No
tes:
Leve
l of
seve
rity
is d
eter
min
ed b
ybo
th im
pair
men
t an
d ris
k.A
sses
sim
pair
men
t do
mai
n by
car
egiv
er’s
reca
ll of
pre
viou
s 2–
4 w
eeks
.A
ssig
n se
verit
y to
the
mos
t se
vere
cate
gory
in w
hich
any
feat
ure
occu
rs.
Freq
uenc
y an
d se
verit
y of
exa
cerb
a-tio
ns m
ay f
luct
uate
ove
r tim
e fo
rpa
tient
s in
any
sev
erity
cat
egor
y.A
t pr
esen
t, th
ere
are
inad
equa
teda
ta t
o co
rres
pond
fre
quen
cies
of
exa
cerb
atio
ns w
ith d
iffer
ent
leve
ls o
f as
thm
a se
verit
y. In
gen
eral
,m
ore
freq
uent
and
sev
ere
exac
erba
-tio
ns (
e.g.
,req
uirin
g ur
gent
,un
sche
dule
d ca
re, h
ospi
taliz
atio
n,or
IC
U a
dmis
sion
) in
dica
te g
reat
erun
derly
ing
dise
ase
seve
rity.
For
trea
tmen
t pu
rpos
es, p
atie
nts
with
≥2
exac
erba
tions
des
crib
ed a
bove
may
be c
onsi
dere
d th
e sa
me
as p
atie
nts
who
hav
e pe
rsis
tent
ast
hma,
eve
n in
the
abse
nce
of im
pair
men
t le
vels
co
nsis
tent
with
per
sist
ent
asth
ma.
Nat
iona
lHea
rtL
ung
and
Blo
odIn
stitu
te.(
2007
).G
uide
lines
fort
hedi
agno
sisa
ndm
anag
emen
tofa
sthm
a.A
utho
r:W
ashi
ngto
n,D
C.R
etri
eved
Janu
ary
8,20
08,f
rom
http
://w
ww
.nhl
bi.n
ih.g
ov/
guid
elin
es/a
sthm
a/as
thsu
mm
704 Unit 3 n n Managing Health Challenges
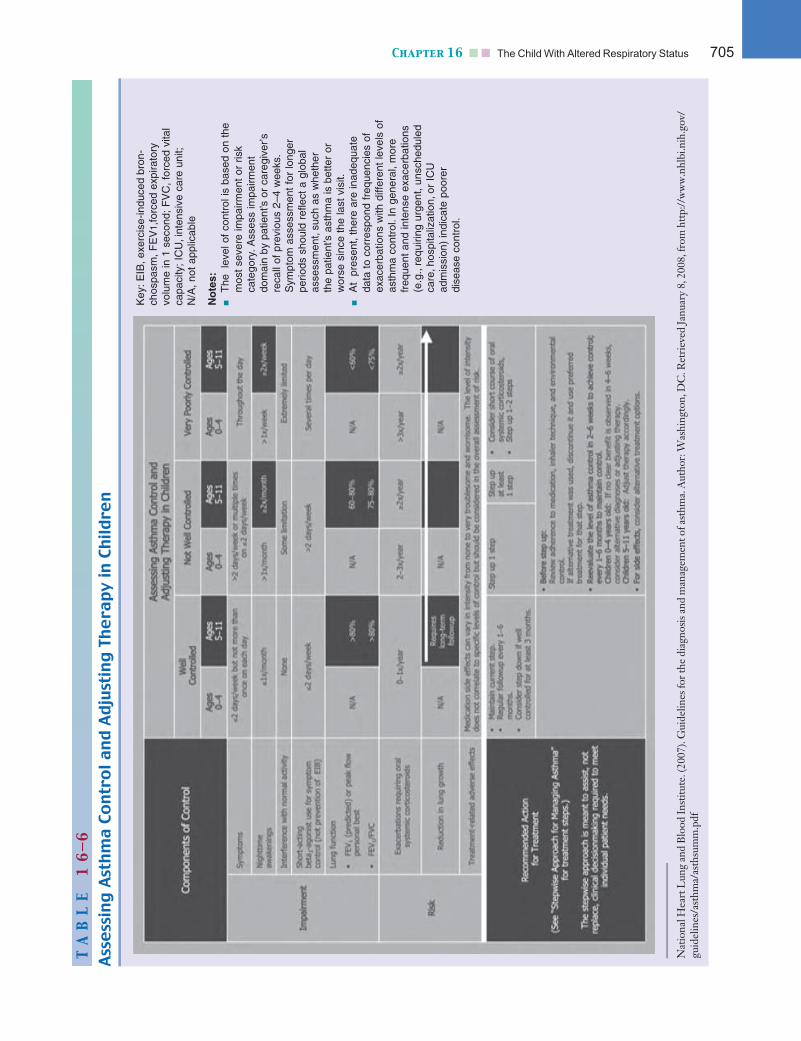
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:38 User ID: muralir 1BlackLining Disabled
TA
BL
E1
6—6
AssessingAsthmaControlandAdjustingTh
era
pyin
Childre
n
Key
: EIB
, exe
rcis
e-in
duce
d br
on-
chos
pasm
, FE
V1,
forc
ed e
xpira
tory
vo
lum
e in
1 s
econ
d; F
VC
, for
ced
vita
lca
paci
ty;
ICU
,int
ensi
ve c
are
unit;
N
/A, n
ot a
pplic
able
No
tes:
The
le
vel o
f co
ntro
l is
base
d on
the
mos
t se
vere
impa
irmen
t or
ris
k ca
tego
ry. A
sses
s im
pairm
ent
dom
ain
by p
atie
nt’s
or
care
give
r’s
reca
ll of
pre
viou
s 2–
4 w
eeks
.S
ympt
om a
sses
smen
t fo
r lo
nger
perio
ds s
houl
d re
flect
a g
loba
las
sess
men
t,su
ch a
s w
heth
er
the
patie
nt’s
ast
hma
is b
ette
r or
wor
se s
ince
the
last
vis
it.A
t pr
esen
t, th
ere
are
inad
equa
teda
ta t
o co
rres
pond
fre
quen
cies
of
exac
erba
tions
with
diff
eren
t le
vels
of
asth
ma
cont
rol.
In g
ener
al, m
ore
freq
uent
and
inte
nse
exac
erba
tions
(e.g
.,re
quiri
ng u
rgen
t, un
sche
dule
dca
re,h
ospi
taliz
atio
n,or
IC
U
adm
issi
on)
indi
cate
poo
rer
dise
ase
cont
rol.
Nat
iona
lHea
rtL
ung
and
Blo
odIn
stitu
te.(
2007
).G
uide
lines
fort
hedi
agno
sisa
ndm
anag
emen
tofa
sthm
a.A
utho
r:W
ashi
ngto
n,D
C.R
etri
eved
Janu
ary
8,20
08,f
rom
http
://w
ww
.nhl
bi.n
ih.g
ov/
guid
elin
es/a
sthm
a/as
thsu
mm
Chapter 16 n n The Child With Altered Respiratory Status 705
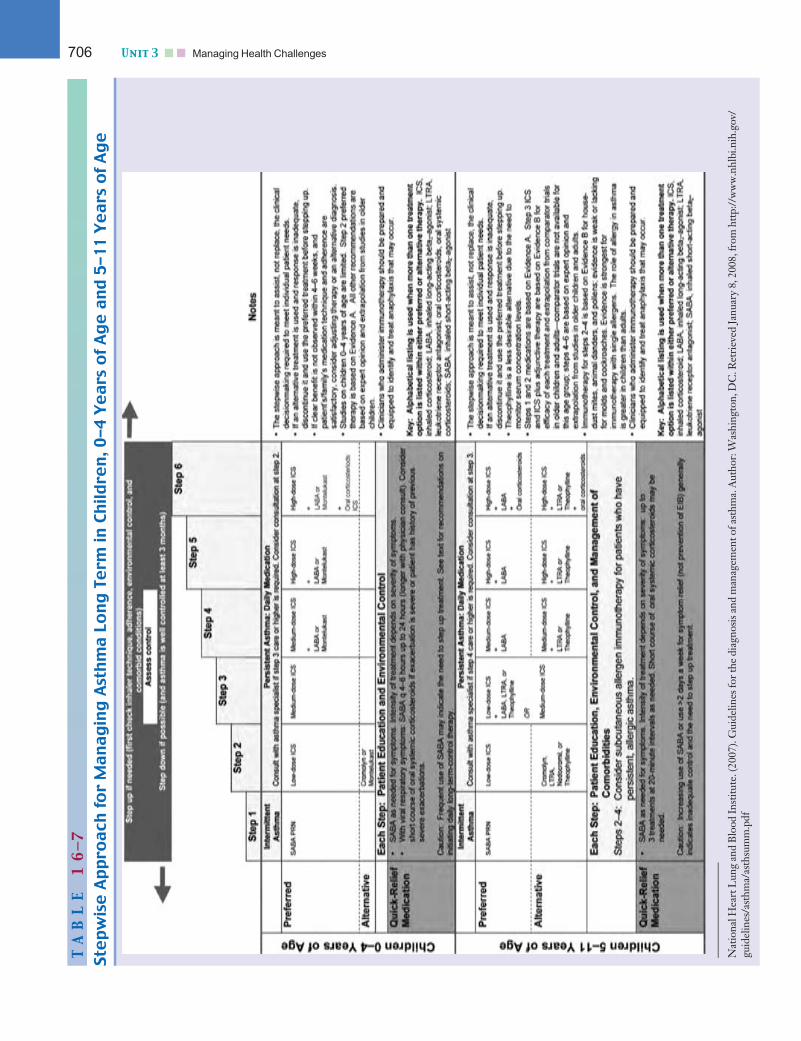
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:38 User ID: muralir 1BlackLining Disabled
TA
BL
E1
6—7
StepwiseAppro
ach
forManagingAsthmaLo
ngTe
rmin
Childre
n,0-4Years
ofAgeand5-11Years
ofAge
Nat
iona
lHea
rtL
ung
and
Blo
odIn
stitu
te.(
2007
).G
uide
lines
fort
hedi
agno
sisa
ndm
anag
emen
tofa
sthm
a.A
utho
r:W
ashi
ngto
n,D
C.R
etri
eved
Janu
ary
8,20
08,f
rom
http
://w
ww
.nhl
bi.n
ih.g
ov/
guid
elin
es/a
sthm
a/as
thsu
mm
706 Unit 3 n n Managing Health Challenges
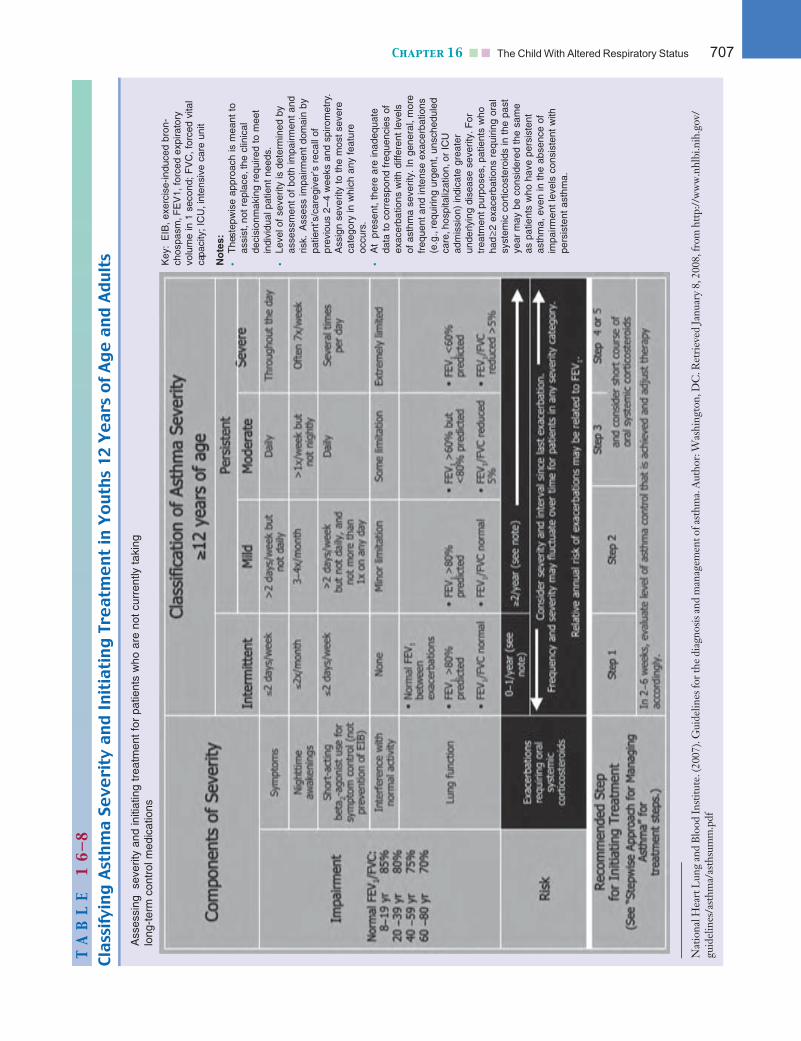
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:38 User ID: muralir 1BlackLining Disabled
TA
BL
E1
6—8
ClassifyingAsthmaSe
verity
andInitiatingTreatm
entin
Youth
s12Years
ofAgeandAdults
Ass
essi
ng
seve
rity
and
initi
atin
g tr
eatm
ent
for
patie
nts
who
are
not
cur
rent
ly t
akin
glo
ng-t
erm
con
trol
med
icat
ions
Key
:E
IB, e
xerc
ise-
indu
ced
bron
-ch
ospa
sm,F
EV
1, fo
rced
exp
irato
ry
volu
me
in 1
sec
ond;
FV
C, f
orce
d vi
tal
capa
city
; IC
U,i
nten
sive
car
e un
it
No
tes:
•T
he s
tepw
ise
appr
oach
is m
eant
to
assi
st,n
ot r
epla
ce,t
he c
linic
al
deci
sion
mak
ing
requ
ired
to m
eet
indi
vidu
al p
atie
nt n
eeds
.•
Leve
l of
seve
rity
is d
eter
min
ed b
yas
sess
men
t of
bot
h im
pairm
ent
and
risk.
Ass
ess
impa
irmen
t do
mai
n by
patie
nt’s
/car
egiv
er’s
rec
all o
f pr
evio
us 2
–4
wee
ks a
nd s
piro
met
ry.
Ass
ign
seve
rity
to t
he m
ost
seve
reca
tego
ry in
whi
ch a
ny f
eatu
reoc
curs
.•
At
pres
ent,
ther
e ar
e in
adeq
uate
data
to
corr
espo
nd f
requ
enci
es o
fex
acer
batio
ns w
ith d
iffer
ent
leve
ls
of a
sthm
a se
verit
y. In
gen
eral
, mor
efr
eque
nt a
nd in
tens
e ex
acer
batio
ns(e
.g.,
requ
iring
urg
ent,
unsc
hedu
led
care
,hos
pita
lizat
ion,
or I
CU
ad
mis
sion
) in
dica
te g
reat
er
unde
rlyin
g di
seas
e se
verit
y. F
ortr
eatm
ent
purp
oses
, pat
ient
s w
hoha
d≥2
exa
cerb
atio
ns r
equi
ring
oral
sy
stem
ic c
ortic
oste
roid
s in
the
pas
tye
ar m
ay b
e co
nsid
ered
the
sam
e as
pat
ient
s w
ho h
ave
pers
iste
ntas
thm
a, e
ven
in t
he a
bsen
ce o
fim
pairm
ent
leve
ls c
onsi
sten
t w
ithpe
rsis
tent
ast
hma.
Nat
iona
lHea
rtL
ung
and
Blo
odIn
stitu
te.(
2007
).G
uide
lines
fort
hedi
agno
sisa
ndm
anag
emen
tofa
sthm
a.A
utho
r:W
ashi
ngto
n,D
C.R
etri
eved
Janu
ary
8,20
08,f
rom
http
://w
ww
.nhl
bi.n
ih.g
ov/
guid
elin
es/a
sthm
a/as
thsu
mm
Chapter 16 n n The Child With Altered Respiratory Status 707
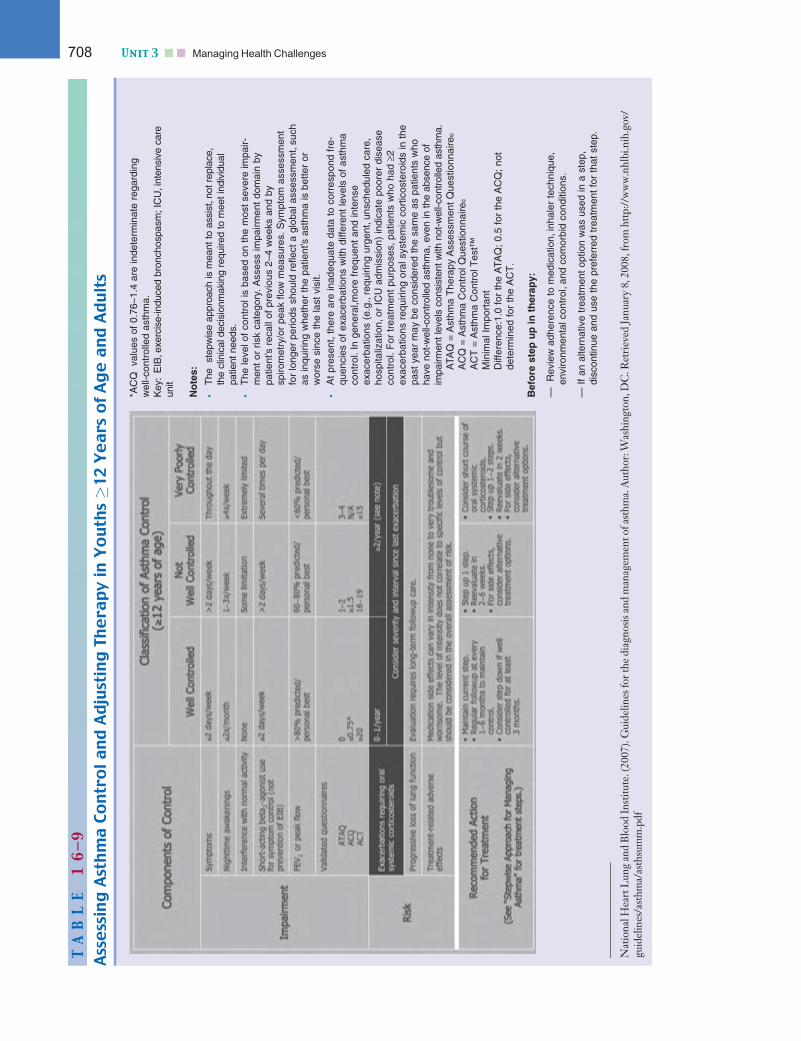
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:38 User ID: muralir 1BlackLining Disabled
TA
BL
E1
6—9
AssessingAsthmaControlandAdjustingTh
era
pyin
Youth
s�12Years
ofAgeandAdults
*AC
Q
valu
es o
f 0.
76–1
.4 a
re in
dete
rmin
ate
rega
rdin
g w
ell-c
ontr
olle
d as
thm
a.K
ey:
EIB
,exe
rcis
e-in
duce
d br
onch
ospa
sm; I
CU
,int
ensi
ve c
are
unit
No
tes:
•T
he s
tepw
ise
appr
oach
is m
eant
to a
ssis
t,no
t rep
lace
,th
e cl
inic
al d
ecis
ionm
akin
g re
quire
d to
mee
t ind
ivid
ual
patie
nt n
eeds
.•
The
leve
l of
cont
rol i
s ba
sed
on t
he m
ost s
ever
e im
pair-
men
t or
ris
k ca
tego
ry. A
sses
s im
pairm
ent
dom
ain
bypa
tient
’s r
ecal
l of
prev
ious
2–4
wee
ks a
nd b
y sp
irom
etry
/or
peak
flo
w m
easu
res.
Sym
ptom
ass
essm
ent
for
long
er p
erio
ds s
houl
d re
flect
a g
loba
l ass
essm
ent,
such
as in
quiri
ng w
heth
er t
he p
atie
nt’s
ast
hma
is b
ette
r or
wor
se s
ince
the
last
vis
it.•
At
pres
ent,
ther
e ar
e in
adeq
uate
dat
a to
cor
resp
ond
fre-
quen
cies
of
exac
erba
tions
with
diff
eren
t le
vels
of
asth
ma
cont
rol.
In g
ener
al,m
ore
freq
uent
and
inte
nse
exac
erba
tions
(e.
g.,r
equi
ring
urge
nt,u
nsch
edul
ed c
are,
hosp
italiz
atio
n,or
IC
U a
dmis
sion
) in
dica
te p
oore
r di
seas
eco
ntro
l. F
or t
reat
men
t pu
rpos
es, p
atie
nts
who
had
≥2
exac
erba
tions
req
uirin
g or
al s
yste
mic
cor
ticos
tero
ids
in t
hepa
st y
ear
may
be
cons
ider
ed t
he s
ame
as p
atie
nts
who
have
not
-wel
l-con
trol
led
asth
ma,
eve
n in
the
abse
nce
ofim
pairm
ent l
evel
s co
nsis
tent
with
not
-wel
l-con
trol
led
asth
ma.
ATA
Q =
Ast
hma
The
rapy
Ass
essm
ent
Que
stio
nnai
re©
AC
Q =
Ast
hma
Con
trol
Que
stio
nnai
re©
AC
T =
Ast
hma
Con
trol
Tes
t™
M
inim
al I
mpo
rtan
t D
iffer
ence
:1.0
for
the
ATA
Q;
0.5
for
the
AC
Q;
not
dete
rmin
ed f
or t
he A
CT
.
Bef
ore
ste
p u
p in
th
erap
y:
—
Rev
iew
adh
eren
ce t
o m
edic
atio
n,in
hale
r te
chni
que,
envi
ronm
enta
l con
trol
,and
com
orbi
d co
nditi
ons.
— I
f an
alte
rnat
ive
trea
tmen
t op
tion
was
use
d in
a s
tep,
disc
ontin
ue a
nd u
se t
he p
refe
rred
tre
atm
ent
for
that
ste
p.
Nat
iona
lHea
rtL
ung
and
Blo
odIn
stitu
te.(
2007
).G
uide
lines
fort
hedi
agno
sisa
ndm
anag
emen
tofa
sthm
a.A
utho
r:W
ashi
ngto
n,D
C.R
etri
eved
Janu
ary
8,20
08,f
rom
http
://w
ww
.nhl
bi.n
ih.g
ov/
guid
elin
es/a
sthm
a/as
thsu
mm
708 Unit 3 n n Managing Health Challenges
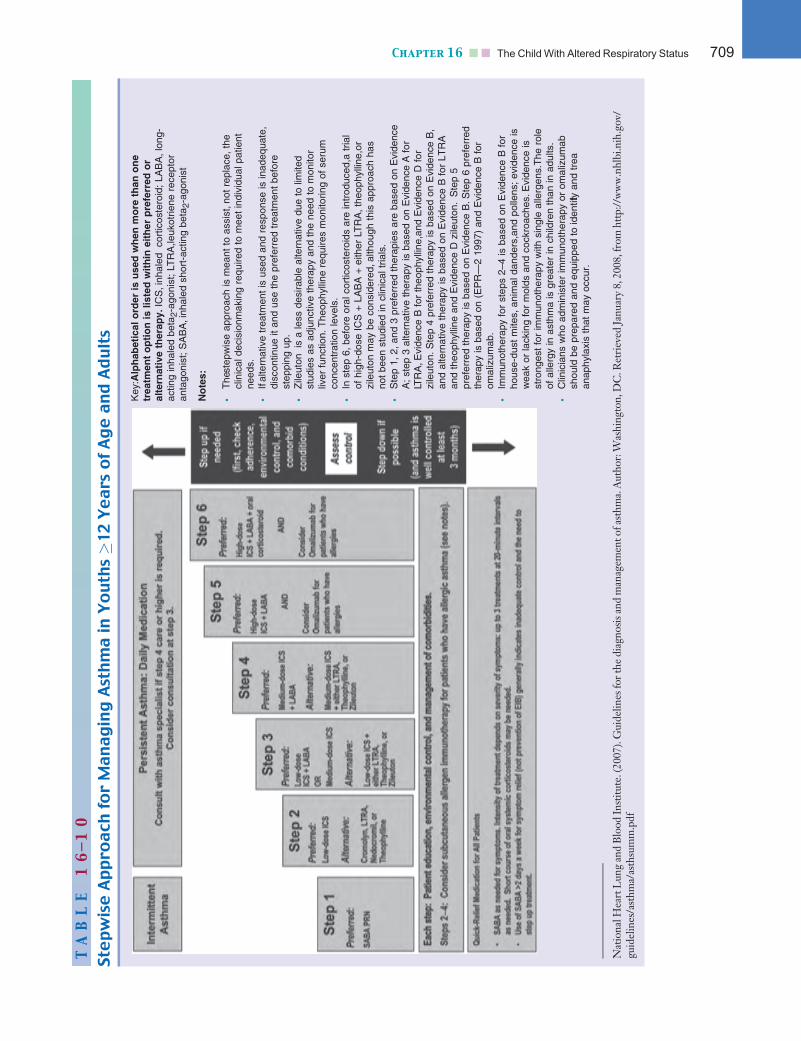
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:38 User ID: muralir 1BlackLining Disabled
TA
BL
E1
6—1
0
StepwiseAppro
ach
forManagingAsthmain
Youth
s�12Years
ofAgeandAdults
Key
:Alp
hab
etic
al o
rder
is u
sed
wh
en m
ore
th
an o
ne
trea
tmen
t o
pti
on
is li
sted
wit
hin
eit
her
pre
ferr
ed o
ral
tern
ativ
e th
erap
y. IC
S,i
nhal
ed
cort
icos
tero
id;
LAB
A, l
ong-
actin
g in
hale
d be
ta2-
agon
ist;
LTR
A,le
ukot
riene
rec
epto
ran
tago
nist
; S
AB
A,i
nhal
ed s
hort
-act
ing
beta
2-ag
onis
t
No
tes:
•T
he s
tepw
ise
appr
oach
is m
eant
to
assi
st,n
ot r
epla
ce, t
hecl
inic
al d
ecis
ionm
akin
g re
quire
d to
mee
t in
divi
dual
pat
ient
need
s.•
If al
tern
ativ
e tr
eatm
ent
is u
sed
and
resp
onse
is in
adeq
uate
,di
scon
tinue
it a
nd u
se t
he p
refe
rred
tre
atm
ent
befo
re
step
ping
up.
•Z
ileut
on
is a
less
des
irabl
e al
tern
ativ
e du
e to
lim
ited
stud
ies
as a
djun
ctiv
e th
erap
y an
d th
e ne
ed t
o m
onito
r liv
er f
unct
ion.
The
ophy
lline
req
uire
s m
onito
ring
of s
erum
conc
entr
atio
n le
vels
.•
In s
tep
6, b
efor
e or
al c
ortic
oste
roid
s ar
e in
trod
uced
,a t
rial
of h
igh-
dose
IC
S +
LA
BA
+ e
ither
LT
RA
, the
ophy
lline
,or
zile
uton
may
be
cons
ider
ed,a
lthou
gh t
his
appr
oach
has
not
been
stu
died
in c
linic
al t
rials
.•
Ste
p 1,
2, a
nd 3
pre
ferr
ed t
hera
pies
are
bas
ed o
n E
vide
nce
A;
step
3 a
ltern
ativ
e th
erap
y is
bas
ed o
n E
vide
nce
A f
orLT
RA
,Evi
denc
e B
for
the
ophy
lline
,and
Evi
denc
e D
for
zile
uton
. Ste
p 4
pref
erre
d th
erap
y is
bas
ed o
n E
vide
nce
B,
and
alte
rnat
ive
ther
apy
is b
ased
on
Evi
denc
e B
for
LT
RA
and
theo
phyl
line
and
Evi
denc
e D
zile
uton
.S
tep
5 pr
efer
red
ther
apy
is b
ased
on
Evi
denc
e B
.Ste
p 6
pref
erre
dth
erap
y is
bas
ed o
n (E
PR
—2
1997
) an
d E
vide
nce
B f
or
omal
izum
ab.
•Im
mun
othe
rapy
for
ste
ps 2
–4 is
bas
ed o
n E
vide
nce
B f
orho
use-
dust
mite
s, a
nim
al d
ande
rs,a
nd p
olle
ns;
evid
ence
isw
eak
or la
ckin
g fo
r m
olds
and
coc
kroa
ches
.Evi
denc
e is
stro
nges
t fo
r im
mun
othe
rapy
with
sin
gle
alle
rgen
s.T
he r
ole
of a
llerg
y in
ast
hma
is g
reat
er in
chi
ldre
n th
an in
adu
lts.
•C
linic
ians
who
adm
inis
ter
imm
unot
hera
py o
r om
aliz
umab
shou
ld b
e pr
epar
ed a
nd e
quip
ped
to id
entif
y an
d tr
eat
anap
hyla
xis
that
may
occ
ur.
Nat
iona
lHea
rtL
ung
and
Blo
odIn
stitu
te.(
2007
).G
uide
lines
fort
hedi
agno
sisa
ndm
anag
emen
tofa
sthm
a.A
utho
r:W
ashi
ngto
n,D
C.R
etri
eved
Janu
ary
8,20
08,f
rom
http
://w
ww
.nhl
bi.n
ih.g
ov/
guid
elin
es/a
sthm
a/as
thsu
mm
Chapter 16 n n The Child With Altered Respiratory Status 709
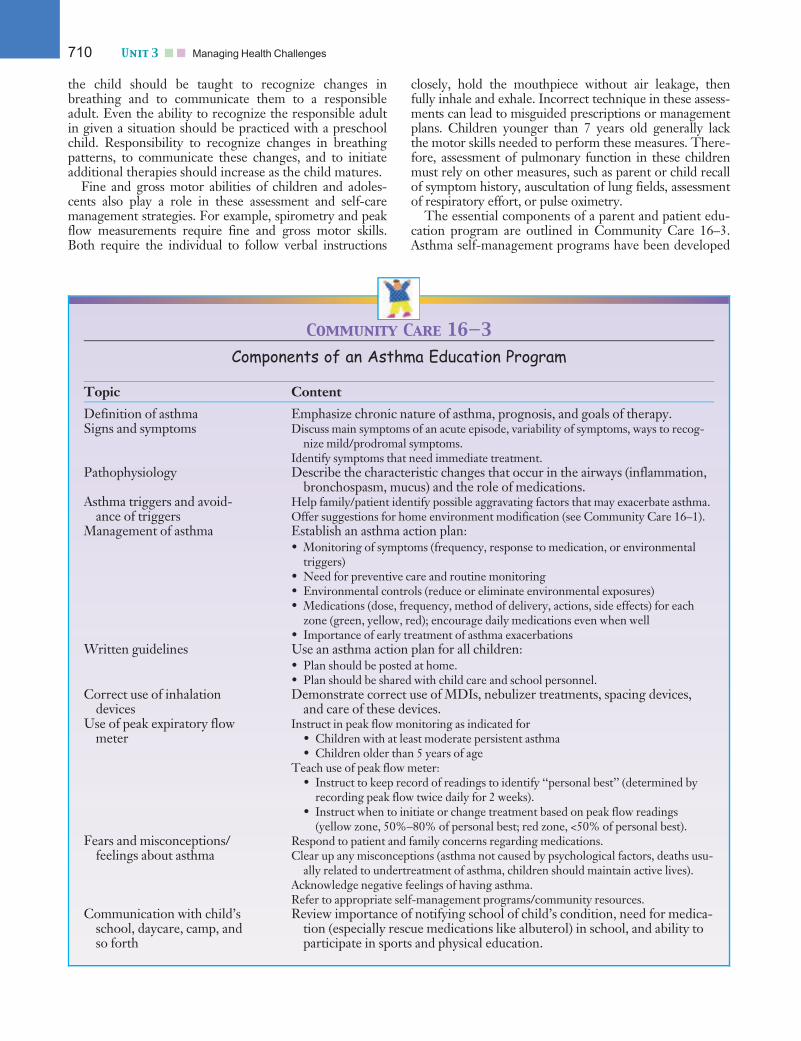
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:38 User ID: muralir 1BlackLining Disabled
the child should be taught to recognize changes inbreathing and to communicate them to a responsibleadult. Even the ability to recognize the responsible adultin given a situation should be practiced with a preschoolchild. Responsibility to recognize changes in breathingpatterns, to communicate these changes, and to initiateadditional therapies should increase as the child matures.
Fine and gross motor abilities of children and adoles-cents also play a role in these assessment and self-caremanagement strategies. For example, spirometry and peakflow measurements require fine and gross motor skills.Both require the individual to follow verbal instructions
closely, hold the mouthpiece without air leakage, thenfully inhale and exhale. Incorrect technique in these assess-ments can lead to misguided prescriptions or managementplans. Children younger than 7 years old generally lackthe motor skills needed to perform these measures. There-fore, assessment of pulmonary function in these childrenmust rely on other measures, such as parent or child recallof symptom history, auscultation of lung fields, assessmentof respiratory effort, or pulse oximetry.
The essential components of a parent and patient edu-cation program are outlined in Community Care 16–3.Asthma self-management programs have been developed
Community Care 16—3
Components of an Asthma Education Program
Topic Content
Definition of asthma Emphasize chronic nature of asthma, prognosis, and goals of therapy.Signs and symptoms Discuss main symptoms of an acute episode, variability of symptoms, ways to recog-
nize mild/prodromal symptoms.Identify symptoms that need immediate treatment.
Pathophysiology Describe the characteristic changes that occur in the airways (inflammation,bronchospasm, mucus) and the role of medications.
Asthma triggers and avoid-ance of triggers
Help family/patient identify possible aggravating factors that may exacerbate asthma.Offer suggestions for home environment modification (see Community Care 16–1).
Management of asthma Establish an asthma action plan:• Monitoring of symptoms (frequency, response to medication, or environmental
triggers)• Need for preventive care and routine monitoring• Environmental controls (reduce or eliminate environmental exposures)• Medications (dose, frequency, method of delivery, actions, side effects) for each
zone (green, yellow, red); encourage daily medications even when well• Importance of early treatment of asthma exacerbations
Written guidelines Use an asthma action plan for all children:• Plan should be posted at home.• Plan should be shared with child care and school personnel.
Correct use of inhalationdevices
Demonstrate correct use of MDIs, nebulizer treatments, spacing devices,and care of these devices.
Use of peak expiratory flowmeter
Instruct in peak flow monitoring as indicated for• Children with at least moderate persistent asthma• Children older than 5 years of age
Teach use of peak flow meter:• Instruct to keep record of readings to identify ‘‘personal best’’ (determined by
recording peak flow twice daily for 2 weeks).• Instruct when to initiate or change treatment based on peak flow readings
(yellow zone, 50%–80% of personal best; red zone, <50% of personal best).Fears and misconceptions/
feelings about asthmaRespond to patient and family concerns regarding medications.Clear up any misconceptions (asthma not caused by psychological factors, deaths usu-
ally related to undertreatment of asthma, children should maintain active lives).Acknowledge negative feelings of having asthma.Refer to appropriate self-management programs/community resources.
Communication with child’sschool, daycare, camp, andso forth
Review importance of notifying school of child’s condition, need for medica-tion (especially rescue medications like albuterol) in school, and ability toparticipate in sports and physical education.
710 Unit 3 n n Managing Health Challenges

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:38 User ID: muralir 1BlackLining Disabled
for various settings to promote awareness, knowledge,and treatment adherence. Several of these programs andeducational brochures are available through the Ameri-can Lung Association (Open Airways) or the Asthma andAllergy Foundation of America (Wee Wheezers, PowerBreathing) (see for organizations) and are pre-sented in the National Heart, Lung and Blood Institute(2007) document. Educational programs that focus onself-management skills help shift the often crisis-orientednature of asthma care to one of proactive interventionand prevention.
Gear any education and materials to the child’s cogni-tive, affective, and developmental levels. Ensure that the in-formation given to parents and families is also provided toschool teachers, the school nurse, coaches, camp counse-lors, and other community personnel to ensure awarenessof asthma, ensure continuity of treatment, and facilitateproblem solving if the child has an acute episode. The im-portance of regular follow-up with a consistent healthcareprovider cannot be overemphasized. Progress must beclosely monitored in relation to history of acute exacerba-tions, responses to therapy, and adherence to treatment.
Answer: The nurse has an obligation to provideongoing education to the family about the disease and
about the medical system. If Claudia made a good decisionabout when to access care in a hospital, then that should bemade clear to Claudia. One of the greatest problems in themanagement of childhood chronic disease is the lack of conti-nuity of care. Claudia takes her children to the health depart-ment for immunizations, to the pediatrician for problems, andnow she and Jose have had their first visit to the hospital emer-gency department. The nurse can ensure the family leaveswith a record of the visit so that the pediatrician can fullyunderstand this exacerbation.
Control of Environmental Factors andComorbid ConditionsAssessment of the environmental factors and comorbidconditions that affect asthma severity can be completedin several ways. A verbal history provided by the childand parent can determine recent exposures, and a historyof the symptoms associated with increasing asthma sever-ity. An assessment of the home may reveal the presenceof previously unknown or unsuspected allergens (seeTradition or Science 16–3). Advise the family on ways toreduce exposure to environmental allergens within thehome and community that may exacerbate asthma (seeCommunity Care 16–1 earlier in this chapter).
Skin or in vitro testing may also be used to assess sensi-tivity to allergens. Allergen immunotherapy may be con-sidered for children with persistent asthma when there isclear evidence that the asthma symptoms are related to ex-posure to specific allergens to which the child is sensitive.
A history and treatment of comorbid symptoms mayimprove overall asthma control. Conditions that mayadversely affect asthma control include allergic broncho-pulmonary aspergillosis, gastroesophageal reflux, obesity,
obstructive sleep apnea, rhinitis, sinusitis, stress, anddepression. Advise children with these conditions to seekor maintain care provided by a medical specialist toensure that recognition and treatment of these conditionsis maintained.
MedicationsA stepwise approach is used to select the medication anddelivery devices to meet the child’s needs and presentingsymptoms (see Tables 16–7 to 16–10). After a diagnosishas been made and therapy has been initiated, the child’slevel of asthma control is monitored daily, and therapy isadjusted accordingly. The goal of therapy is to identifythe minimum amount of medication required to help thechild maintain asthma control.
Medications have two primary roles in the treatmentof asthma. The first role of medication use is to providelong-term control by preventing symptoms. The secondrole of medications is to treat acute symptoms andexacerbations.
Corticosteroids are considered to be the most effectivemethod to achieve long-term control of asthma. Theseanti-inflammatory agents reduce airway hyperresponsive-ness, inhibit inflammatory cell migration and activation,and block late-phase reaction to allergens (NationalHeart, Lung and Blood Institute, 2007). Inhaled cortico-steroids are the most consistently effective at all steps ofcare for persistent asthma. Oral corticosteroids may beused to gain prompt control of asthma and are requiredfor severe persistent asthma (see Tables 16–7 and 16-10).
Tradition or Science 16—3
Should pets be removed from the home to preventallergic sensitization in children?
MORE INQUIRY
NEEDEDMORE INQUIRY
NEEDEDNumerous studies have demonstratedthat pet allergies are clearly associated
with wheezing and bronchial hyperresponsiveness inadults. Thus, asthma has been thought to be worsenedby exposure to pets. However, recent studies indicatethat living with a pet early in life reduces the incidence ofasthma and may have a possible protective effect. Theselongitudinal studies demonstrated that children exposedto pets in the home as newborns and during the first yearof life had a lower incidence of asthma at ages 12 to 13than children not exposed to pets. Pet allergen exposureitself does not appear to be the protective factor; rather,endotoxin exposure from presence of the pet in the homeis hypothesized to provide the protective influence. Endo-toxin, a component of gram-negative bacterial cell walls,is found throughout nature. High levels of allergen expo-sure are also thought to induce immunologic tolerance.Clearly, more research is needed to better understandthe relationship between pet exposure and asthma sensi-tivity. In the meantime, prospective parents need notremove pets from the home before a child’s arrival(Bacharier & Strunk, 2003).
Chapter 16 n n The Child With Altered Respiratory Status 711

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:39 User ID: muralir 1BlackLining Disabled
Other medications used to gain long-term controlinclude cromolyn sodium and nedocromil. These anti-inflammatory agents inhibit activation and release ofmediators from mast cells, thus maintaining airway stabil-ity. Immunomodulators (omalizumab) is a monoclonalantibody given intramuscularly to prevent binding of IgEto the high-affinity receptors on basophils and mast cells(National Heart, Lung and Blood Institute, 2007). This isused an adjunctive therapy for children 12 years andolder who have demonstrated sensitivity to specific aller-gens and who require a step up in care to manage theirpersistent asthma. Leukotriene modifiers are used forchildren requiring step 2 care for mild persistent asthma.These products interfere with the pathway of leukotrienemediators that are released from mast cells, eosinophils,and basophils (National Heart, Lung and Blood Institute,2007). Long-acting beta2 agonists such as salmeterol andformoterol are bronchodilators that open the airways byrelaxing smooth muscle contraction and reducing bron-chospasm, which thereby enhances mucociliary clearanceand decreases vascular permeability. Methylxanthine is asustained-release theophylline that has some mild anti-inflammatory effects and can be used as adjunctive ther-apy with inhaled corticosteroids for children older than5 years. For a more detailed description of these medica-tions and their recommended use, dose, adverse effects,and care concerns, please refer to the National Heart,Lung and Blood Institute (2007) asthma guidelines.
Medications are also used to provide quick relief foracute symptoms and exacerbations. These acute symp-toms may be brought on by environmental exposures (asdescribed earlier) or perhaps by exercise-induced bron-chospasm that was not effectively managed by the me-dications previously described to step up or down carefor long-term asthma control. Quick-relief medicationsinclude anticholinergics given via an MDI or nebulizersolution. These agents inhibit muscarinic cholinergicreceptors and reduce the intrinsic vagal tone of the air-ways (National Heart, Lung and Blood Institute, 2007).Short-acting beta2 agonists (SABAs) such as albuterol,levalbuterol, and pirbuterol are rapid-acting bronchodila-tors that open the airways by relaxing smooth musclecontraction, enhancing mucociliary clearance, and reduc-ing bronchospasm. Systemic corticosteroids may be usedin addition to SABAs for moderate and severe exacerba-tions to speed recovery and to prevent recurrence of theexacerbation (National Heart, Lung and Blood Institute,2007) (see the National Heart, Lung and Blood Institute[2007] asthma guidelines for further information on med-ications to treat acute symptoms of asthma).
Determine the medications the child is using and whetherany complimentary and alternative medications or treat-ments (chiropractic medicine, acupuncture) are be used.
Ask to view any records the child has been keeping of hisor her symptoms and/or peak flow monitoring. Advise chil-dren with moderate or severe persistent asthma to keepdaily peak flow monitoring records. These tools will aidthe child and family to recognize adequate and inadequateasthma control. Watch the child using their peak flow me-ter and inhaler. Although the steps in this process seemeasy, incorrect use of the inhaler means less medication isgetting to the airways. Provide instruction materials andsample peak flow charts to the family (see forProcedures: Use and Care of Peak Flow Meters andSpacers). Each healthcare encounter should include anassessment of asthma severity, measures to maintain controland the child’s responsiveness to the therapies initiated.
Management and Treatment of Exacerbations
Question: Based on the following informationand Jose’s condition, what do you anticipate the nurse
in the emergency department will do next?
An acute or subacute episode of asthma is identified asprogressive and worsening shortness of breath, cough,wheezing, and/or chest tightness. These symptoms indi-cate decreases in expiratory airflow and require immedi-ate intervention. Children whose asthma has been wellcontrolled using inhaled corticosteroids are less likely tohave an exacerbation; however, all children are at risk forexacerbations. Respiratory infections, exercise-inducedbronchospasm, extreme changes in weather, exposure toa known (or unknown) allergen, and stress can precipitatea worsening of asthma symptoms. Severe exacerbationscan be life threatening. Act quickly to assess the degreeof severity and to determine the measures already takento relieve the child’s symptoms. Use the child’s writtenasthma plan to help the family determine how to adjustthe medications. School nurses should have copies of thiswritten plan at the child’s school site. Remove or with-draw the child from allergens in the environment thatmay be contributing to the exacerbation. If the child doesnot have a written asthma plan, or if the child continuesto deteriorate despite the increased use of inhaled corti-costeroids and SABAs, then management in an urgent oremergency care or hospital setting is warranted.
When the child presents in the healthcare setting withan acute exacerbation, assess and carefully monitor alert-ness, heart rate, respiratory rate, breath sounds, pulse oxi-metry, and PEFR (if the child is able); and perform a fullpulmonary assessment, including visual inspection ofchest (accessory muscles), auscultation of breath sounds,and other respiratory assessments. Typically, supplemen-tal oxygen is ordered to correct hypoxemia. Administerrepetitive or continuous SABA treatments to reverse air-flow obstruction rapidly. Oral systemic corticosteroidsany be ordered to decrease airway inflammation if thechild does not respond promptly to the SABA treat-ments. Usually, the child will prefer a high Fowler’position or sitting up and leaning slightly forward. Con-tinuously monitor the child in acute distress, including
Alert! There is insufficient evidence to support recommending the useof complimentary and alternative medications for treatment of allergy. Familieswho use herbal treatments for asthma should be cautioned about the interac-tions that some of the ingredients may have with their prescribed asthmamedications.
712 Unit 3 n n Managing Health Challenges

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:39 User ID: muralir 1BlackLining Disabled
comprehensive reassessments of the child’s response totherapy after the first hour. For acute exacerbation thatresponds poorly to initial interventions, or when ongoingobservation and stabilization of the child is needed, hos-pitalization may be indicated. If the child is becoming lessalert or drowsy, this may indicate impending respiratoryfailure. Endotracheal intubation and assisted ventilationmust be considered if steady clinical deterioration occursdespite continued intensive therapy.
Answer: Jose’s history, presentation of physicalsymptoms, and oxygen saturation will affect the deci-
sion regarding whether Jose will receive inhaled SABA bynebulizer or MDI, up to three doses during the first hour, andoral corticosteroids if needed. If Jose is responding to thenebulized medication and his respiratory distress is resolving,inhaled SABA will be continued every 60 minutes. This treat-ment will continue for 1 to 3 hours. If he continues in respira-tory distress, despite his initial treatments, oxygen will beadministered. Hospitalization may be warranted for ongoingadministration of oxygen, nebulized SABAs, oral or intrave-nous corticosteroids and intravenous therapy.
Community CareThe National Heart, Lung and Blood Institute (2007)asthma guidelines represent the best evidence to dateregarding the assessment, monitoring, and management ofasthma. The primary emphasis of these standards of careis to encourage early diagnosis and ongoing assessment bythe child’s medical home providers, and to provide teach-ing and preventive measures that will ensure the child’soverall health and well-being. Patient education shouldoccur at all points of care with the child and family. Sur-veillance of environmental triggers must also occur in allsettings (home, school, daycare, and so forth) in which thechild is likely to spend time. Review the National Heart,Lung and Blood Institute (2007) standards thoroughly andutilize the information and products provided by thisagency and others to help children and their families effec-tively manage the child’s chronic condition.
Bronchopulmonary Dysplasia (BPD)BPD is a chronic lung disease of children that begins ininfancy. BPD was first described as the radiographic andclinical syndrome seen in infants who had been treatedwith mechanical ventilation and high levels of inspired ox-ygen, and who survived respiratory distress syndrome.Although timing of diagnosis varies, the clinical diagnosisis generally made at approximately 1 month of age ininfants who required mechanical ventilation for at least 1week; have symptoms of persistent respiratory distress; aredependent on supplemental oxygen; and have chest radio-graphs that show hyperinflation, atelectasis, increased den-sity, and fibrotic areas (American Thoracic Society, 2003).
Because the diagnostic criteria for BPD are not preciseand universally distinct, the incidence of this disease isdifficult to ascertain. Some retrospective studies of neo-
nates suggest that BPD occurs in 35% of prematurebirths, with the incidence being inversely related to birthweight (Smith et al., 2005). This condition is seen pre-dominantly in infants born prematurely (more than 10weeks before their due date), infants less than 1,000 g atbirth, and in infants with multiple pulmonary disorderswho require ventilator support with high positive airwaypressures and oxygen during the first 2 weeks of life.
Early deaths from BPD are generally attributed tountreatable respiratory failure, with later deaths beingassociated with infection, pulmonary hypertension, andcor pulmonale, or an acute severe cyanotic episode thatdoes not respond to rapid institution of CPR. The effectsof BPD may last several months to years. Althoughinfants with BPD have a prolonged and complicated neo-natal course, the long-term pulmonary prognosis for sur-vivors of BPD is relatively good.
PathophysiologyThe pathophysiology of BPD is complex and of multie-tiologic and multisystem origins. It starts with an acuteinsult to the neonate’s lungs, such as respiratory distresssyndrome, pneumonia, or meconium aspiration, thatrequires positive pressure ventilation and high concentra-tions of oxygen over an extended time. These therapiesresult in tissue and cellular injury to the immature lung.The epithelium of the conducting airways developslesions from injury thought to be related to hyperoxia andpositive pressure. Excessive pulmonary fluid, collection ofcellular debris in the alveoli, and recurrent bacterial andviral infections are additional factors contributing to thealveolar tissue damage. Infants with BPD often exhibit a‘‘state of chronic undernutrition’’ that affects the lung’sability to resist injury and repair damaged tissue (Ameri-can Thoracic Society, 2003; Huysman et al., 2003).
The most important underlying pathologic process inBPD is the profound alteration of lung compliance,which is reduced as a result of a combination of factors.These factors include fibrosis of the airways and markedhyperplasia of the bronchial epithelium, which occur sec-ondary to alveolar damage; and increased fluid in thelung, as a result of disruption of the alveolar–capillarymembrane. Damage to the alveolar supporting structuresresults in overdistension and leads to air trapping, fibro-sis, airway edema, and bronchoconstriction, increasingairway resistance and decreasing compliance. Increasedairway resistance increases the work of breathing, result-ing in tachypnea and wheezing.
Pulmonary gas exchange is impaired by several factors.Hypoxia occurs secondary to ventilation–perfusion mis-match in the areas of alveolar collapse. Increased pulmo-nary vascular resistance causes intrapulmonic shunting,thus also contributing to hypoxia. Hypercarbia is com-mon and is also caused by ventilation–perfusion mis-match, as well as by hypoventilation.
Large airway pathology (i.e., in the trachea and bron-chi) was not originally described as a component of BPDbut has since been recognized to be a frequent finding asthe disease progresses. Both tracheomalacia and bron-chomalacia are commonly found in this population and
Chapter 16 n n The Child With Altered Respiratory Status 713

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:39 User ID: muralir 1BlackLining Disabled
are postulated to be the cause of acute, severe cyanoticepisodes in the older infant with BPD.
Growth failure in infants with BPD is almost universaland results from increased caloric needs, caused by theincreased work of breathing, and high resting oxygenconsumption. Growth failure and lung disease may alsobe complicated by gastroesophageal reflux with frequentemesis, poor oral feeding skills, and recurrent respiratoryinfections (Huysman et al., 2003).
Cor pulmonale (hypertrophy or failure of the right ven-tricle caused by disorders of the lungs, pulmonary vessels, orchest wall), pulmonary hypertension, systemic hypertension,and left ventricular hypertrophy are complications of BPDthat result from the fibrosis and chronic hypoxia. The pul-monary vasculature of these infants develops increased reac-tivity to hypoxia, resulting in pulmonary hypertension andleft ventricular hypertrophy with congestive heart failure.
The effect of therapies such as high-frequency oscilla-tory ventilation and surfactant replacement on the overallincidence of BPD remains to be fully demonstrated.High-frequency oscillatory ventilation delivers gas atextremely high frequencies (>200 ‘‘breaths’’/minute) andconsiderably lower pressures than those used for standardmechanical ventilation, thus reducing barotrauma to thealveoli. Studies have shown that surfactant therapyreduces the severity of respiratory distress syndrome anddecreases the amount of time on mechanical ventilation.
AssessmentThe clinical manifestations of BPD are a direct reflectionof the pathophysiology of this disorder. Tachypnea, dysp-nea, and wheezing are intermittently or chronically presentsecondary to airway obstruction and increased airway re-sistance. Increased work of breathing, as evidenced by in-tercostal or substernal retractions and use of accessorymuscles, is common in the infant with BPD. Infants whohave been intubated for long periods may develop subglot-tic stenosis, which results in inspiratory stridor. Further-more, hypoxemia and hypercapnia are chronic states thatcontribute to the problem. The child might turn cyanoticwhen crying or after a few moments without supplementaloxygen. Infants with moderate to severe BPD are fre-quently described as irritable and difficult to comfort. Thisbehavior may result from hypoxia or underlying neurologicdysfunction. They may develop irregular sleep patterns asa result of frequent medical treatments, medications, andtherapies. Inguinal hernias are often present, which may bea result of the continuous increase in abdominal pressurecaused by high airway resistance and use of accessory respi-ratory muscles. These infants also have extraordinarilylarge insensible fluid losses because of tachypnea and ex-cessive perspiration related to hypercarbia.
The incidence of neurologic abnormalities and develop-mental delay in infants with bronchopulmonary dysplasiavaries, but these problems are known to occur in childrenwith BPD. Infants who are born prematurely likely experi-ence some degree of developmental delay with or withoutneurologic insult. Even if there is no evident damage to theneurologic system during hospitalization in the neonatal in-tensive care unit, children with BPD may show signs of
problems when they are school age. These problems canrange from vision and hearing loss to speech delays, learningdisabilities, and poor attention span. Developmental delaysresult from long-term ventilatory support, poor nutritionalstatus, inadequate sensory stimulation, neurologic sequelae,and decreased energy and respiratory reserves.
Nursing assessment requires close observation andawareness of BPD signs and symptoms. Take a thoroughhistory, including the child’s baseline symptoms (retractions,respiratory effort), requirements (oxygen needs), and nutri-tional intake. Next, complete a physical examination focus-ing on respiratory, cardiac, nutritional, and developmentalstatus. An interdisciplinary team may assist in a comprehen-sive evaluation. Report any abnormal findings to the teamand implement appropriate interventions and referrals.
Interdisciplinary InterventionsJust as the pathophysiology of BPD is multifactorial, itstreatment is multifaceted. Medical management of BPDcenters on preventing and minimizing hypoxia andhypercarbia, treating bronchoconstriction and airwayhyperreactivity and inflammation, treating pulmonaryedema, and promoting repair of chronic lung injury.
These desired ends are achieved in varying degrees bymedical therapies such as supplemental oxygen, diuretics,bronchodilators, anti-inflammatory agents, and variousmodes of assisted mechanical ventilation. Pulmonaryhypertension responds at least in part to oxygen, a potentpulmonary vasodilator. Low-flow supplemental oxygen isadministered, at times on a long-term basis, in an attemptto prevent chronic hypoxia and subsequent complications.Tracheostomy is considered for those who require assistedventilation for more than 3 months as a neonate or whohave chronic hypercarbia and increased work of breathing.
Management of HypoxiaThe primary and most important aspect of therapy ininfants with BPD is managing hypoxia. Maintainingadequate tissue oxygenation is imperative to prevent severemorbidity and potential death. Supplemental oxygen ther-apy is prescribed to promote growth and neurodevelop-ment, and to prevent or control pulmonary hypertension.Administering and monitoring oxygen therapy is a majornursing responsibility in the care of an infant with BPD.Pulse oximetry or transcutaneous oxygen monitors areused to continuously or intermittently display oxygen satu-ration. Oxygen saturation levels (SaO2) of 92% to 95%,depending on severity of illness, are necessary to facilitatean improved rate of weight gain and to control pulmonaryhypertension. The nurse must respond to the infant’schanging oxygen needs, titrating oxygen flow to keep satu-rations within the prescribed parameters. Feedings, peri-ods of increased activity, and periods of sleep are occasionswhen desaturations are most likely.
Tailor the mode of oxygen delivery to the specificneeds of the infant. Most infants with mild to moderateBPD can tolerate a nasal oxygen cannula. Children withtracheostomies may use a tracheostomy mist collar (Fig.16–18). Humidification is necessary for liter flow equal toor greater than 1 L/minute to prevent airway irritation
714 Unit 3 n n Managing Health Challenges
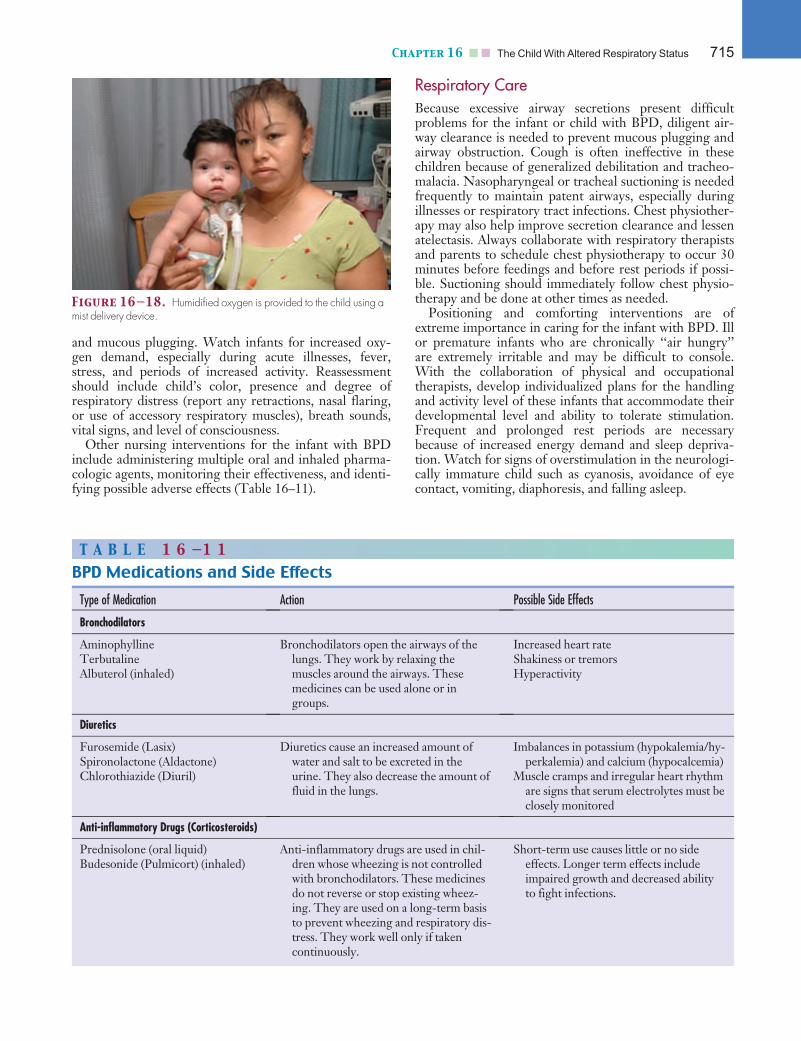
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:39 User ID: muralir 1BlackLining Disabled
and mucous plugging. Watch infants for increased oxy-gen demand, especially during acute illnesses, fever,stress, and periods of increased activity. Reassessmentshould include child’s color, presence and degree ofrespiratory distress (report any retractions, nasal flaring,or use of accessory respiratory muscles), breath sounds,vital signs, and level of consciousness.
Other nursing interventions for the infant with BPDinclude administering multiple oral and inhaled pharma-cologic agents, monitoring their effectiveness, and identi-fying possible adverse effects (Table 16–11).
Respiratory CareBecause excessive airway secretions present difficultproblems for the infant or child with BPD, diligent air-way clearance is needed to prevent mucous plugging andairway obstruction. Cough is often ineffective in thesechildren because of generalized debilitation and tracheo-malacia. Nasopharyngeal or tracheal suctioning is neededfrequently to maintain patent airways, especially duringillnesses or respiratory tract infections. Chest physiother-apy may also help improve secretion clearance and lessenatelectasis. Always collaborate with respiratory therapistsand parents to schedule chest physiotherapy to occur 30minutes before feedings and before rest periods if possi-ble. Suctioning should immediately follow chest physio-therapy and be done at other times as needed.
Positioning and comforting interventions are ofextreme importance in caring for the infant with BPD. Illor premature infants who are chronically ‘‘air hungry’’are extremely irritable and may be difficult to console.With the collaboration of physical and occupationaltherapists, develop individualized plans for the handlingand activity level of these infants that accommodate theirdevelopmental level and ability to tolerate stimulation.Frequent and prolonged rest periods are necessarybecause of increased energy demand and sleep depriva-tion. Watch for signs of overstimulation in the neurologi-cally immature child such as cyanosis, avoidance of eyecontact, vomiting, diaphoresis, and falling asleep.
Figure 16—18. Humidified oxygen is provided to the child using amist delivery device.
T A B L E 1 6 —1 1
BPD Medications and Side Effects
Type of Medication Action Possible Side Effects
Bronchodilators
AminophyllineTerbutalineAlbuterol (inhaled)
Bronchodilators open the airways of thelungs. They work by relaxing themuscles around the airways. Thesemedicines can be used alone or ingroups.
Increased heart rateShakiness or tremorsHyperactivity
Diuretics
Furosemide (Lasix)Spironolactone (Aldactone)Chlorothiazide (Diuril)
Diuretics cause an increased amount ofwater and salt to be excreted in theurine. They also decrease the amount offluid in the lungs.
Imbalances in potassium (hypokalemia/hy-perkalemia) and calcium (hypocalcemia)
Muscle cramps and irregular heart rhythmare signs that serum electrolytes must beclosely monitored
Anti-inflammatory Drugs (Corticosteroids)
Prednisolone (oral liquid)Budesonide (Pulmicort) (inhaled)
Anti-inflammatory drugs are used in chil-dren whose wheezing is not controlledwith bronchodilators. These medicinesdo not reverse or stop existing wheez-ing. They are used on a long-term basisto prevent wheezing and respiratory dis-tress. They work well only if takencontinuously.
Short-term use causes little or no sideeffects. Longer term effects includeimpaired growth and decreased abilityto fight infections.
Chapter 16 n n The Child With Altered Respiratory Status 715

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:39 User ID: muralir 1BlackLining Disabled
Nutritional SupportBecause growth failure is common in the infant with BPD,providing nutritional support is a crucial, although diffi-cult, aspect of caring for these children. Management offeedings in infants and young children with BPD hasdirect implications for long-term outcome, because anadequate caloric intake is necessary for growth of healthylung tissue and resolution of the disease. Yet, these infantssuffer from a myriad of conditions that impair their abilityto feed: gastroesophageal reflux, often with aspiration;emesis; chronic fatigue; behavioral oral aversion; and swal-lowing dysfunction caused by poor oral–motor develop-ment. For the healthy infant, feeding is generally viewed asa pleasant and positive experience; however, for the childwith BPD, it is often perceived as a battle. It can seem thatthe more that nurses and parents are concerned and anx-ious about nutrition and place pressure on the infant orchild to eat, the less the child eats. Feeding with the infantor child with BPD can be a frustrating and challenging ex-perience, and coordinated interdisciplinary effort is thekey to successfully approaching these problems.
Begin with an nutritional assessment that includes docu-mentation of anthropometric (precise measurement of thebody includes weight, height, and head circumference) andbiochemical data, dietary intake, and clinical status. Strat-egies in nutritional support then focus on optimizing thecaloric intake to meet individual needs. Concentrating for-mula to provide more calories per ounce; medication tocontrol gastroesophageal reflux; and small, frequent feed-ings all are appropriate for mild to moderate growth failure.
Infants with severe growth failure, or for whom the pre-viously listed strategies are unsuccessful, should be consid-
ered for surgical placement of a gastrostomy tube orpercutaneous endoscopic gastrostomy tube. This proce-dure may or may not be performed in conjunction with aNissen fundoplication, depending on the severity of gas-troesophageal reflux. Because parents sometimes view theneed for a gastrostomy tube as a sign of their failure to feedtheir infant orally, the entire healthcare team must providesupport and stress the benefits of this mode of therapy.Calorie-dense formulas can be administered with minimalrisk of aspiration, in a continuous infusion if necessary, topromote optimal growth. Feeding specialists and caregiverscan provide therapy to develop and refine suck and swal-low coordination skills concurrently, so that as the infant’sgrowth, strength, and ability to orally feed improve; tubefeedings can be slowly weaned and the frequency andamount of oral feedings can be increased (Nursing Inter-ventions 16–2). This strategy temporarily relaxes theintense focus on eating and can transform parental anxietyinto energy devoted to interventions such as positive oralstimulation and nonnutritive sucking during tube feedings.
Family Education and SupportOther nursing and social service interventions shouldfocus on providing education and support. Teach parentsabout all aspects of BPD, especially topics related tohome care. If the child is to receive oxygen, arrangementsmust be made for administering the oxygen (CommunityCare 16–4). Medication administration, feeding andnutrition, developmental interventions, chest physiother-apy, and suctioning are among the most important topicsof education for the parents and family of a child withBPD. Family members are taught CPR. Teach them the
Nursing Interventions 16—2
How to Improve Feeding Capabilities in an Infant With BPD
• Have baby in a calm, alert state before beginningto feed.
• Position the baby in the caregiver’s lap with thebaby’s neck in a neutral position, hips and knees at90 degrees of flexion, both upper extremities withelbows flexed at 90 degrees, and swaddled acrossthe chest. Note: If the baby becomes excessively hotor sweaty with swaddling of the entire body, thenfold a thin pillowcase or light towel in a long rec-tangle and swaddle only around the arms and par-tial trunk to prevent excessive scapular retraction,arching, and flailing of the upper extremities.
• Carefully monitor physiologic parameters, espe-cially respiratory rate. Feedings may need to belimited or postponed if the infant remainstachypneic.
• Choose a nipple that allows moderate resistanceto flow without excessive energy expenditure.Standard-shaped nipples are preferred.
• Present the nipple slowly and calmly, with minimalintraoral stimulation.
• Emphasize normal total body posture during feed-ing. Head and neck posture can alter oral–motorpatterns during sucking. Ideally, marked neckextension should be reduced to aid oral–motorcontrol. The goal of improving head and neckpositioning may need to be approached slowly,to minimize stress to the infant.
• Allow baby to set the nippling pace, with rests asneeded.
• Stop nippling if baby begins to sweat or criesinconsolably for 1 minute or longer; if respiratoryrate or heart rate increases excessively, as deter-mined by the physician; or if feeding takes longerthan 20 minutes.
716 Unit 3 n n Managing Health Challenges
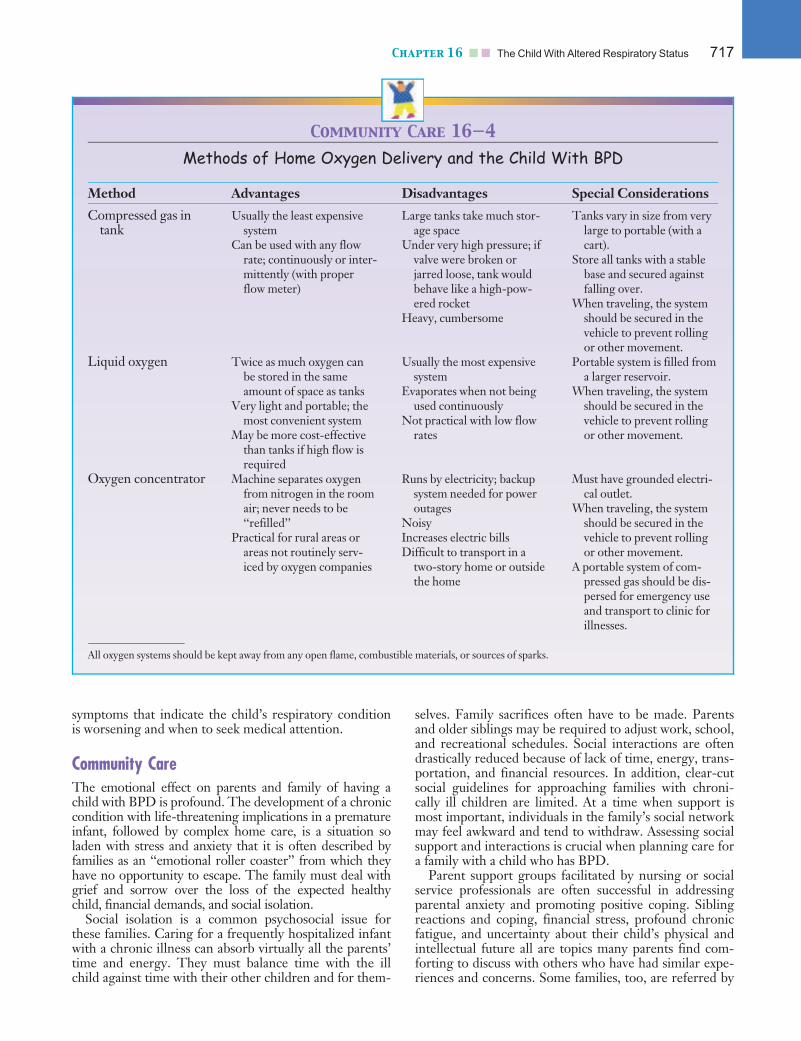
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:39 User ID: muralir 1BlackLining Disabled
symptoms that indicate the child’s respiratory conditionis worsening and when to seek medical attention.
Community CareThe emotional effect on parents and family of having achild with BPD is profound. The development of a chroniccondition with life-threatening implications in a prematureinfant, followed by complex home care, is a situation soladen with stress and anxiety that it is often described byfamilies as an ‘‘emotional roller coaster’’ from which theyhave no opportunity to escape. The family must deal withgrief and sorrow over the loss of the expected healthychild, financial demands, and social isolation.
Social isolation is a common psychosocial issue forthese families. Caring for a frequently hospitalized infantwith a chronic illness can absorb virtually all the parents’time and energy. They must balance time with the illchild against time with their other children and for them-
selves. Family sacrifices often have to be made. Parentsand older siblings may be required to adjust work, school,and recreational schedules. Social interactions are oftendrastically reduced because of lack of time, energy, trans-portation, and financial resources. In addition, clear-cutsocial guidelines for approaching families with chroni-cally ill children are limited. At a time when support ismost important, individuals in the family’s social networkmay feel awkward and tend to withdraw. Assessing socialsupport and interactions is crucial when planning care fora family with a child who has BPD.
Parent support groups facilitated by nursing or socialservice professionals are often successful in addressingparental anxiety and promoting positive coping. Siblingreactions and coping, financial stress, profound chronicfatigue, and uncertainty about their child’s physical andintellectual future all are topics many parents find com-forting to discuss with others who have had similar expe-riences and concerns. Some families, too, are referred by
Community Care 16—4
Methods of Home Oxygen Delivery and the Child With BPD
Method Advantages Disadvantages Special Considerations
Compressed gas intank
Usually the least expensivesystem
Can be used with any flowrate; continuously or inter-mittently (with properflow meter)
Large tanks take much stor-age space
Under very high pressure; ifvalve were broken orjarred loose, tank wouldbehave like a high-pow-ered rocket
Heavy, cumbersome
Tanks vary in size from verylarge to portable (with acart).
Store all tanks with a stablebase and secured againstfalling over.
When traveling, the systemshould be secured in thevehicle to prevent rollingor other movement.
Liquid oxygen Twice as much oxygen canbe stored in the sameamount of space as tanks
Very light and portable; themost convenient system
May be more cost-effectivethan tanks if high flow isrequired
Usually the most expensivesystem
Evaporates when not beingused continuously
Not practical with low flowrates
Portable system is filled froma larger reservoir.
When traveling, the systemshould be secured in thevehicle to prevent rollingor other movement.
Oxygen concentrator Machine separates oxygenfrom nitrogen in the roomair; never needs to be‘‘refilled’’
Practical for rural areas orareas not routinely serv-iced by oxygen companies
Runs by electricity; backupsystem needed for poweroutages
NoisyIncreases electric billsDifficult to transport in a
two-story home or outsidethe home
Must have grounded electri-cal outlet.
When traveling, the systemshould be secured in thevehicle to prevent rollingor other movement.
A portable system of com-pressed gas should be dis-persed for emergency useand transport to clinic forillnesses.
All oxygen systems should be kept away from any open flame, combustible materials, or sources of sparks.
Chapter 16 n n The Child With Altered Respiratory Status 717

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:39 User ID: muralir 1BlackLining Disabled
social services for private counseling to address and facili-tate stress management.
Cystic Fibrosis (CF)Once considered a fatal childhood disease, CF is achronic, multisystem condition. Ongoing advances inunderstanding the pathophysiology of CF, particularly itsgenetic and molecular mechanisms, has greatly improveddiagnosis and treatment, and thus improved survivalrates, life expectancy, and quality of life for children andadolescents with CF. The median age of survival for indi-viduals with CF has increased to 37 years in 2004, upfrom 32 years in 2003 (Cystic Fibrosis Foundation,2007). Intensive research has also resulted in betterscreening tests to detect carriers through genetic testing.
CF is a highly complex disease and requires a holisticapproach to care by a trained, interdisciplinary team,including physicians, advance practice nurses, nurses, die-titians, social workers, psychologists, and respiratory caretherapists. Coordination and communication with thechild, family, and other healthcare providers are essential.Specialist care in a dedicated CF center has been associ-ated with improved survival and quality of life in children.As with any chronic condition, the primary objectives ofCF care for children should focus on (1) ensuring optimalcare, including treatments, routine monitoring, and gen-eral pediatric preventive care; (2) facilitating access topertinent healthcare resources and support; (3) assistingthe family in coordinating care among specialists and pri-mary care providers, and in accessing medications, die-tary supplements, and durable medical equipment; and(4) supporting quality of life and independence.
Although CF is rare overall, it is more common amongwhite northern Europeans. The overall prevalence of CFin the U.S. population is estimated to be 1 in 3,700 livebirths (Green et al., 2005). Based on reports from theCenters for Disease Control (2004), the prevalence is 1 in2,500 to 3,500 births among non-Hispanic whites, 1 in4,000 to 10,000 births among Hispanics, and 1 in 15,000to 20,000 births among non-Hispanic blacks.
PathophysiologyCF is an autosomal recessive genetic condition. In suchconditions, the risk of disease transmission is 25% if bothparents carry the gene, and the chance that the child willbe a carrier of the disease is 50% (see Fig. 3–3). Prenatalscreening is common in women from populations thathave an elevated prevalence of CF, or in women withknown or suspected family histories. Prenatal testing isalso done when obstructed fetal bowel is detected by ultra-sound, because CF is associated with meconium ileus.
The gene responsible for CF is located on chromo-some 7. CF results from mutations in the cystic fibrosistransmembrane regulator (CFTR), a protein that regu-lates chloride and sodium transport in secretory epithelialcells of the body’s exocrine glands. The alteration in theCFTR protein results in abnormal ion concentrationacross the apical membranes of these cells: They do notrelease chloride, resulting in an improper salt balance.This imbalance causes the mucus secretions of the
pulmonary, gastrointestinal, and reproductive systems tobecome thick and sticky, and to block ducts in thoseorgans. The sweat glands are also affected by blocked orabnormal transport and produce sweat with elevated so-dium and chloride concentrations (Fig. 16–19).
The most CF common mutation, DF508, occurs inmore than 90% of individuals with CF in the UnitedStates (Rowe, Miller, & Sorscher, 2005). More than 1,000other gene mutations of CFTR genes have been described.A small number of these mutations occur with reasonablefrequency, but most are rare. Thus, the clinical manifesta-tions (the phenotypic expressions) of CF vary widely. Forexample, 99% of those who are homozygous for theDF508 allele have pancreatic insufficiency, whereas only36% of people with CF with other mutations are pancre-atic insufficient (Rowe, Miller, & Sorscher, 2005).
Clinical consequences of CF are progressive pulmonarydamage (e.g., airway obstruction, inflammation, infection,scarring), pancreatic dysfunction, liver disease that maylead to cirrhosis, gut motility problems, and elevated sweatelectrolyte levels. Approximately 80% to 85% of childrenwith CF are pancreatic insufficient, resulting in mal-absorption of important nutrients, fats, and proteins.Approximately 98% of males are sterile, because of block-age of the vas deferens by thick secretions, or from abnor-mal development (atresia of the vas deferens) that preventspassage of sperm. Females can become pregnant, but thethick cervical mucus acts as a natural barrier to sperm.Although the true biologic fertility in CF remains un-known, females with normal lung function appear to expe-rience relatively few problems with pregnancy; those withdecreased lung function and chronic infection tend to havepoorer pregnancy outcomes (Edenborough, 2001).
The thickened, sticky mucus of a child with CF is inef-fective in removing bacteria from the body, and in fact con-stitutes an ideal medium for bacterial growth. Thus, thechild with CF is especially prone to pulmonary infection.Bacterial lung infections are responsible for most morbidityand mortality among children with CF, and these infec-tions are often caused by multiple pathogens. The mostcommon cultured bacteria are Pseudomonas aeruginosa,S. aureus, Burkholderia cepacia, and H. influenzae. Childrenwith CF often remain colonized with organisms such asP. aeruginosa, which is never eradicated from the lungs.
Children with CF often experience acute pulmonaryexacerbations, many of which are caused by respiratoryviruses. Infections such as RSV may result in severe pul-monary complications, particularly in infants. Exacer-bations cause fatigue, decreased appetite, weight loss,increased sputum production, increased cough, hemopty-sis, decreased spirometry values, and poor response tooutpatient therapeutic measures such as oral antibioticsand increased pulmonary treatments at home. Treating
Alert! Pseudomonas (Burkholderia) cepacia cause extremelyvirulent infections and have been associated with rapid deterioration ofpulmonary function. B. cepacia has been associated with death in approxi-mately 2% of children with mild or moderate forms of CF. To prevent spreading,children with B. cepacia should not have contact with CF patients.
718 Unit 3 n n Managing Health Challenges
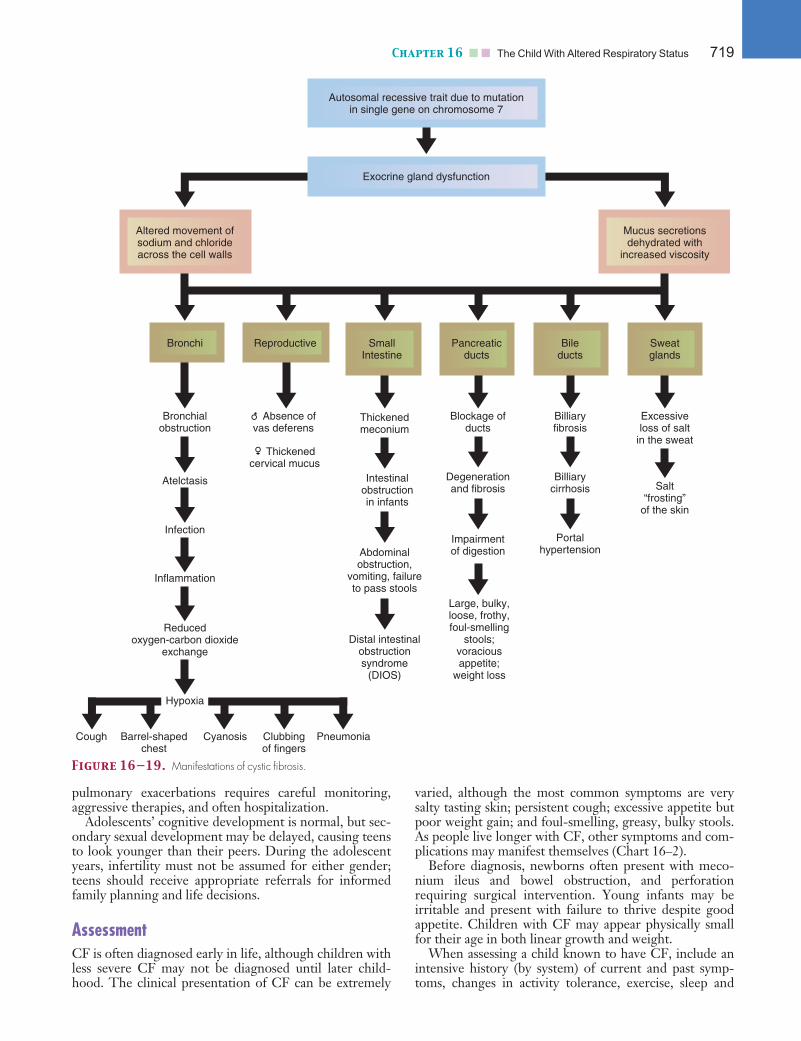
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:39 User ID: muralir 1BlackLining Disabled
pulmonary exacerbations requires careful monitoring,aggressive therapies, and often hospitalization.
Adolescents’ cognitive development is normal, but sec-ondary sexual development may be delayed, causing teensto look younger than their peers. During the adolescentyears, infertility must not be assumed for either gender;teens should receive appropriate referrals for informedfamily planning and life decisions.
AssessmentCF is often diagnosed early in life, although children withless severe CF may not be diagnosed until later child-hood. The clinical presentation of CF can be extremely
varied, although the most common symptoms are verysalty tasting skin; persistent cough; excessive appetite butpoor weight gain; and foul-smelling, greasy, bulky stools.As people live longer with CF, other symptoms and com-plications may manifest themselves (Chart 16–2).
Before diagnosis, newborns often present with meco-nium ileus and bowel obstruction, and perforationrequiring surgical intervention. Young infants may beirritable and present with failure to thrive despite goodappetite. Children with CF may appear physically smallfor their age in both linear growth and weight.
When assessing a child known to have CF, include anintensive history (by system) of current and past symp-toms, changes in activity tolerance, exercise, sleep and
Autosomal recessive trait due to mutationin single gene on chromosome 7
Exocrine gland dysfunction
Altered movement ofsodium and chlorideacross the cell walls
Bronchi Reproductive
Mucus secretionsdehydrated with
increased viscosity
SmallIntestine
Pancreaticducts
Bileducts
Sweatglands
Bronchialobstruction
Thickenedmeconium
Blockage ofducts
Billiaryfibrosis
Excessiveloss of salt
in the sweat
Atelctasis Intestinalobstructionin infants
Degenerationand fibrosis
Billiarycirrhosis
Infection
Abdominalobstruction,
vomiting, failureto pass stools
Impairmentof digestion
Portalhypertension
Inflammation
Reducedoxygen-carbon dioxide
exchange
Hypoxia
Cough Barrel-shapedchest
Cyanosis Clubbingof fingers
Pneumonia
Distal intestinalobstructionsyndrome
(DIOS)
Large, bulky,loose, frothy,foul-smelling
stools;voraciousappetite;
weight loss
Salt“frosting”
of the skin
Thickenedcervical mucus
Absence ofvas deferens
Figure 16—19. Manifestations of cystic fibrosis.
Chapter 16 n n The Child With Altered Respiratory Status 719
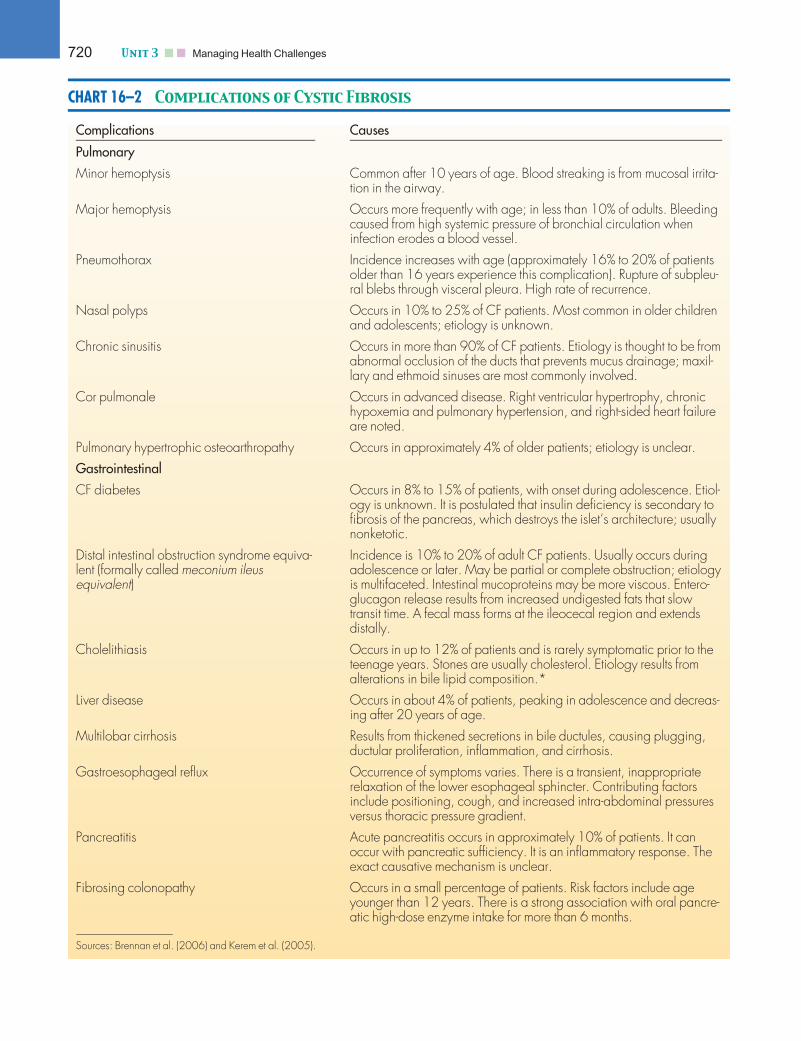
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:39 User ID: muralir 1BlackLining Disabled
CHART 16–2 Complications of Cystic Fibrosis
Complications Causes
Pulmonary
Minor hemoptysis Common after 10 years of age. Blood streaking is from mucosal irrita-tion in the airway.
Major hemoptysis Occurs more frequently with age; in less than 10% of adults. Bleedingcaused from high systemic pressure of bronchial circulation wheninfection erodes a blood vessel.
Pneumothorax Incidence increases with age (approximately 16% to 20% of patientsolder than 16 years experience this complication). Rupture of subpleu-ral blebs through visceral pleura. High rate of recurrence.
Nasal polyps Occurs in 10% to 25% of CF patients. Most common in older childrenand adolescents; etiology is unknown.
Chronic sinusitis Occurs in more than 90% of CF patients. Etiology is thought to be fromabnormal occlusion of the ducts that prevents mucus drainage; maxil-lary and ethmoid sinuses are most commonly involved.
Cor pulmonale Occurs in advanced disease. Right ventricular hypertrophy, chronichypoxemia and pulmonary hypertension, and right-sided heart failureare noted.
Pulmonary hypertrophic osteoarthropathy Occurs in approximately 4% of older patients; etiology is unclear.
Gastrointestinal
CF diabetes Occurs in 8% to 15% of patients, with onset during adolescence. Etiol-ogy is unknown. It is postulated that insulin deficiency is secondary tofibrosis of the pancreas, which destroys the islet’s architecture; usuallynonketotic.
Distal intestinal obstruction syndrome equiva-lent (formally called meconium ileusequivalent)
Incidence is 10% to 20% of adult CF patients. Usually occurs duringadolescence or later. May be partial or complete obstruction; etiologyis multifaceted. Intestinal mucoproteins may be more viscous. Entero-glucagon release results from increased undigested fats that slowtransit time. A fecal mass forms at the ileocecal region and extendsdistally.
Cholelithiasis Occurs in up to 12% of patients and is rarely symptomatic prior to theteenage years. Stones are usually cholesterol. Etiology results fromalterations in bile lipid composition.*
Liver disease Occurs in about 4% of patients, peaking in adolescence and decreas-ing after 20 years of age.
Multilobar cirrhosis Results from thickened secretions in bile ductules, causing plugging,ductular proliferation, inflammation, and cirrhosis.
Gastroesophageal reflux Occurrence of symptoms varies. There is a transient, inappropriaterelaxation of the lower esophageal sphincter. Contributing factorsinclude positioning, cough, and increased intra-abdominal pressuresversus thoracic pressure gradient.
Pancreatitis Acute pancreatitis occurs in approximately 10% of patients. It canoccur with pancreatic sufficiency. It is an inflammatory response. Theexact causative mechanism is unclear.
Fibrosing colonopathy Occurs in a small percentage of patients. Risk factors include ageyounger than 12 years. There is a strong association with oral pancre-atic high-dose enzyme intake for more than 6 months.
Sources: Brennan et al. (2006) and Kerem et al. (2005).
720 Unit 3 n n Managing Health Challenges

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:40 User ID: muralir 1BlackLining Disabled
rest disturbances, and sleep position. Although youshould carefully assess all systems, the primary focusshould be on the respiratory system.
The respiratory assessment may reveal a ‘‘barrel-shaped’’ chest with increased anteroposterior diameter,caused by hyperaeration and increased work of breathing.Another physical finding characteristic of hypoxia andcommon in young children with severe CF is mild tosevere clubbing of the nail beds, caused by chronic hy-poxia. Assess oxygenation by inspecting the color of themucous membranes, nail beds, and skin. Use pulse oxi-metry to monitor oxygen saturation. Assess breath soundsfor equal aeration of all lung fields and for presence orabsence of rales, crackles, and wheezing, particularly inthe upper lobes and the right middle lobe. Assess breath-ing for rate, depth, effort, and use of accessory muscles.Obtain a history on sputum characteristics, includingcolor changes, volume, viscosity, and presence or absenceof blood. Also elicit history of headaches and pain,changes in breathing during activities of a typical day,and cough pattern. The characteristic cough of CF mayincrease during pulmonary exacerbations, can be paroxys-mal, and frequently ends with posttussive emesis. Thecomprehensive pulmonary assessment in CF includes acomparison of the current chest radiograph with baselinefilms and spirometry values with prior results.
On physical examination, note the child’s overall size,general condition, muscle tone, and muscle mass. Somechildren with CF may have a protuberant abdomen. Assessthe skin for bruising; old surgical scars; and indicators ofadequate, excessive, or inadequate fluid balance. Assess theoral mucous membranes, especially of infants, for orallesions, which may result from CF medications (pancreaticoral enzymes) or from thrush, a fungal superinfection thatmay be caused by long-term use of oral antibiotics. Thrushmay also manifest as candidal vaginitis in the female ado-lescent or monilial diaper rash in the infant. Examine therectal area of infants for perirectal irritation from unab-sorbed supplemental pancreatic enzymes. Ask questions toelicit a history of a prolapsed rectum. Other history andsymptoms that require assessment are irritability and anyassociated behaviors; emesis; stool pattern (frequency andcharacteristics); and reports of abdominal pain, discomfort,‘‘heartburn,’’ or any combination of symptoms that mayindicate gastroesophageal reflux.
The sweat test is the definitive test for CF. An elevatedsweat sodium chloride level greater than 60 mEq/L is apositive diagnostic result that should be confirmed by asecond test at a CF center (Cystic Fibrosis Foundation,2007). The sweat sample is usually obtained by stimulatinga small patch of sweat glands on the inner aspect of theforearm. An adequate quantity of sweat, at least 50 mg andpreferably 100 mg, must be collected to ensure reliableresults. Two positive sweat test results and the presence ofclinical symptoms or a family history confirm the diagno-sis. False-negative skin tests are associated with technicalproblems (failure to dry skin before collecting sweat;errors in weighing, dilution, elution, or computation) orphysiologic factors (inadequate volume secondary to lowsweat rate, edema) (Beauchamp & 2005). Siblings are usu-ally tested when a diagnosis is confirmed.
Interdisciplinary InterventionsThe care and treatment of CF is often complex and thusrequires a multidisciplinary approach. Specialized CFcenters that meet specific criteria and are accredited bythe Cystic Fibrosis Foundation deliver quality care andmaintain strict standards of practice. Although most CFcenters are directed by pediatric pulmonologists, otherpediatric specialists such as gastroenterologists, infectiousdiseases specialists, geneticists, and endocrinologists alsoare involved. Additional team members include nurses,advance practice nurses (pediatric nurse practitioner orclinical nurse specialist), registered dietitian, respiratorycare practitioner, medical social worker, physical thera-pist, child life specialist, and genetic counselor. As the lifeexpectancy for CF increases, and more patients surviveinto adulthood, pediatric healthcare teams must foster a‘‘wellness’’ focus and incorporate planning for adult CFcare. Planning for a productive life is the norm.
The family is central to chronic disease managementteams. The child should be an active member in the CFcare team. Working together, the child, parents, family,and the interdisciplinary team develop individualized man-agement plans to treat the complex needs of the childand family (see for Care Paths: An Interdisci-plinary Plan of Care for the Child With Cystic Fibrosis).Although each member of the CF care team has special-ized knowledge and a clearly defined role, overlap in rolefunctions may occur, depending on the needs of the indi-vidual family. The goal of the team is to ‘‘normalize’’ thelives of the family, maintain existing pulmonary function,and prevent further pulmonary damage so the child canbenefit as new treatment options become available.
WORLDVIEW: CF is a condition that primarily affects people ofwhite European genetic background. The CF care team must be sensitiveto cultural issues for individuals and families from varying back-grounds. Families may experience a sense of isolation within their cul-tural environment. Lifestyle practices within certain cultures may affectthe care of an infant or child. The CF team members must work tounderstand these cultural differences and support choices that will sup-port the child’s healthcare maintenance needs. Further research isneeded to examine the effects of cultural differences and practicesamong families on chronic disease management.
Because of the chronic pulmonary infections, activitiesand lifestyles for children with CF may be altered. Forexample, B. cepacia is extremely communicable among theCF population, so room isolation, limited social interac-tions with others with CF, and infection control measuresare required during hospitalization and communityevents for children colonized or infected with this orga-nism. For example the Cystic Fibrosis Foundation hasa policy that prohibits the participation of anyone withCF and B. cepacia from participating at CF Foundation-sponsored events. Because of the highly communicablenature of B. cepacia, the CF Foundation believes this pol-icy enables people with CF who are not infected withB. cepacia to more safely participate in its events (CysticFibrosis Foundation, 2008).
Chapter 16 n n The Child With Altered Respiratory Status 721

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:40 User ID: muralir 1BlackLining Disabled
Medical ManagementMedical management of CF is multifaceted. Successfulchronic disease management requires complete assess-ments and routine monitoring of treatments. A compre-hensive annual review, generally conducted at CF centersby the multidisciplinary team, should include assessmentssuch as a full clinical examination and respiratory, nutri-tional, and psychosocial assessments, as well as a criti-cal review of current therapies and treatments. Clinicaldiagnostic tests during the annual review may include com-plete blood count including iron status, blood chemistries,microbial cultures, bone density examinations (to evaluatefor osteoporosis secondary to poor nutritional intake), andauditory assessments. In addition to the annual reviews,documenting overall health maintenance (immunizations,annual flu vaccine, and adherence history) is important.
For some children with early symptoms of pulmonaryexacerbations, treatment may be managed in the home set-ting with oral antibiotics, aggressive pulmonary therapy,and close follow-up. Hospitalization is required for chil-dren who have declining pulmonary status, infection, orboth. Such stays are often called ‘‘tune-ups.’’ During the‘‘tune-up’’ period, aggressive pulmonary and nutritionaltherapies are instituted, along with intravenous antibioticsand an exercise program, and response to these therapiesis evaluated. Frequency of aerosol treatments and airwayclearance therapies is increased. A daily program toincrease or prevent loss of endurance during hospitaliza-tion is part of the plan of care. The gastrointestinal thera-pies include nutritional assessment and evaluation of bloodchemistries for nutritional deficits, including measurementof hematocrit, hemoglobin, albumin, prealbumin, andvitamins A and E levels (see Nutritional Support).
Today, with a shift toward ambulatory services, manyindividuals with CF initiate their ‘‘tune-ups’’ in the hospitaland complete them at home. During the hospital phase,antibiotics are administered as appropriate, based on find-ings from sputum cultures. The shift to home care depends
on factors such as severity of illness, venous access, abilityand resources of the family, and payer source.
The daily medications required to maintain the base-line health include a long list of pharmaceutical agents(Table 16–12). Long-term use of oral antibiotics forchronic bacterial suppression has raised concern thatantimicrobial-resistant infections will develop amongchildren and youth with CF (Kerem et al., 2005). Suscep-tibility testing may be required for some pathogens todetermine the effectiveness of unusual antibiotics.
Monitoring all therapies (with laboratory tests, pulmo-nary function tests, bone density studies, and radiographicstudies) and coordinating the team consults are both partof the medical management of CF. Identifying new symp-toms that may indicate complications is an ongoing proc-ess. Managing CF by intervening promptly when newsymptoms occur contributes to improved outcomes.
Nutritional SupportKey components of the nutritional assessment in CF careare to determine baseline nutritional requirements andneed for pancreatic enzyme replacement or vitamin ther-apy and to monitor for changing nutritional needs ifcomorbidities (e.g., diabetes) develop. Nutritional assess-ments are conducted at each encounter and hospitalization.Plot physical growth (e.g., height, body mass index) on thegrowth chart to monitor progress and response to thera-peutic interventions. The dietitian assesses physical growth,conducts a nutritional assessment at each admission, identi-fies dietary requirements and goals, and initiates an overallplan to meet the child’s high-caloric nutritional needs. Se-rum laboratory results such as albumin, prealbumin, glu-cose, electrolytes, and complete blood count are assessed.Levels of vitamins A and E are assessed annually, and skin-fold measurements are obtained as indicated. Guidelinesfor administering pancreatic enzymes are provided inNursing Interventions 16–3. Effectiveness of replacementenzymes is monitored through fecal fat studies.
T A B L E 1 6—1 2
Pharmaceutical Agents Used in the Care of the Child With Cystic Fibrosis
Category Purpose
AerosolsBronchodilators
Open up airways
Inhaled antibiotics Antimicrobial, for lung treatment
Mucolytic enzyme Thins mucus
Pancreatic enzymes Increase food/nutrient absorption
Vitamins/minerals (A, D, E, K) Fat-soluble vitamin supplement in water-miscible form; supplement overall diet
H2 blocker Alters gastrointestinal acidic environment; gastroesophageal reflux therapy
Prokinetic agents Enhances gastrointestinal motility; gastroesophageal reflux therapy
Oral and intravenous antibiotics Antimicrobial for S. aureusAntimicrobial for H. influenzaeAntimicrobial for P. aeruginosa
722 Unit 3 n n Managing Health Challenges

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:40 User ID: muralir 1BlackLining Disabled
Infants are usually given an elemental formula tooptimize absorption. Elemental formulas are composedof simple and easily absorbed forms of carbohydrates(glucose polymers or monosaccharides), proteins (aminoacids or casein hydrolysates), and fat as medium-chain tri-glycerides. Elemental formulas are relatively expensive,and costs may vary across individual pharmacies. Specialstate-funded programs may provide assistance. Infantsmay thrive adequately on breast milk or standard infantformula without gastrointestinal complications, as long asenzymes are adjusted appropriately. The older child ismanaged with a high-calorie, high-protein diet, includingsnacks and nutritional oral supplements to boost caloriesand nutrition. Pancreatic enzymes are administered at eachfeeding, meal, and snack to optimize nutrient absorption.
If weight gain and progress toward nutritional goals arenot demonstrated, alternate feeding routes are considered.Gastrostomy tubes, (such as percutaneous endoscopicgastrostomy tubes), low-profile (‘‘button’’) gastrostomies,or jejunostomy tubes (J-tubes) are possible options (seeChapter 18). Nocturnal drip feedings through the gas-trostomy tube are recommended to supplement oralintake.
Respiratory SupportA respiratory care practitioner works under the supervisionof the physician, as do all team members. The respiratorycare practitioner instructs the families on the most effectiveairway clearance technique (ACT), which is individualizedto the patient. The gold standard for airway clearance con-sists of postural drainage and percussion done after aero-solized treatments, depending on respiratory and generalstatus (e.g., during pulmonary exacerbations, treatmentsmay need to be increased to four times per day).
Nursing SupportThe nurse’s primary role is provide direct care. In thehospital setting, this role is central, because the nurse isthe person most consistently at the bedside. Coordinatingcare and monitoring the overall response to therapies(e.g., breathing treatments, self-care participation, activ-ity level, elimination pattern, and appetite) provide essen-tial information to determine progression toward clinicaloutcomes. The nurse also initiates and maintains intrave-nous lines for antibiotic therapy and other intravenousmedications as needed. Measuring accurate height andweight on admission is essential, along with daily weightmeasurement to monitor nutritional progress. Addition-ally, the nurse provides emotional support for the childand parent during frequent and long hospitalizations.
The CF team nurse, usually an advanced practice nurse,assists in coordinating overall care, ensuring that the teamfunctions smoothly, that roles within the team are under-stood, and that clinical care is properly coordinated. Im-portant functions include assessing for the need for teamand family conferences and education regarding treat-ment, medicines, options for venous access, and alternateroutes for nutritional supplementation; assessing for homeintravenous antibiotic therapy and discharge readiness;providing follow-up telephone calls to the caregivers andto the schools, when indicated; and ensuring continuity ofcare by providing care at office or clinic visits. Thisarrangement puts the nurse in a unique position to followup and provide interventions from an ambulatory and aninpatient perspective. The nurse, in some centers, may beable to perform school visits and assist with school reinte-gration, if indicated. Early identification and preparationfor procedures, including preparation for changes in levelof care, are also central to the CF team nurse’s role. Addi-tionally, the CF team nurse educates the team and coordi-nates their involvement when a new diagnosis is made.
Social ServicesThe medical social worker helps caregivers and childrento cope with and integrate CF into their lives. The fami-lies are helped to obtain linkage with the appropriate stateand federal programs for medical care, such as Children’sMedical Services (Title V), state Medicaid, Aid to Fami-lies with Dependent Children, and Supplemental SecurityIncome for the Aged, Blind and Disabled. The socialworker also is a source of emotional support and providesappropriate referrals as needed. The social workeracknowledges that each family is unique, with individual
Nursing Interventions 16—3
Administering Pancreatic Enzymes
Recommended dose of lipase: 1,000 to 3,000 lipaseunits/kg/meal.
• Encourage three meals and two to three snacks perday.
• Discourage eating throughout the entire day.• Administer enzymes before or with meals (and with
vitamins), with snacks, with milk and oral or bolusednutritional supplements, and before nocturnal feedsbegin (and occasionally after completion, as pre-scribed). Usually, half the standard pancreatic lipasedose is given with snacks.
• Open capsules and mix contents with a small amountof applesauce, rice, carrots, or ice cream, or othernonalkaline food. Do not crush microcapsules.
• Avoid allowing microcapsules to sit in alkaline food,which disrupts the enteric coating.
• Assess the oral mucosa and perirectal area for irrita-tion from contact with unswallowed or unabsorbedenzymes.
• Monitor stool pattern and characteristics.• Be alert to complaints such as bloating, flatus, ab-
dominal pain, loose and frequent stools with steator-rhea, poor growth, or some combination of thesesymptoms.
• Instruct parent and patient not to adjust the dose.• Instruct parent and child to check the expiration
dates and store enzymes in a cool place.
Chapter 16 n n The Child With Altered Respiratory Status 723

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:40 User ID: muralir 1BlackLining Disabled
needs and stresses. Many social workers facilitate supportgroups and provide parent-to-parent networking.
Physical TherapyThe physical therapist evaluates the muscles used forbreathing and posture and assesses the child’s ability tocarry out daily activities. The physical therapist also pre-scribes individualized exercise programs and monitorsendurance. The roles of the physical therapist and respi-ratory care practitioner may overlap in certain regions ofthe country. The child with CF is assessed on a regularbasis and is provided a home exercise program.
Child Life ServicesThe child life specialist’s focus of practice is on therapeuticplay along with recreational and diversional activities. Thisprofessional helps the child cope with hospitalization,medical visits, and procedures through play, and can con-tribute to motivational and behavioral programs to encour-age children to do their treatments, drink their nutritionalsupplements, cooperate with therapy, and take medicines.Some child life departments may offer school programs orassist with arrangements for home-bound teachers.
Education regarding self-care and ways to integrate CFcare into daily schedules is necessary to help the familyfoster independence and age-appropriate skills of dailyliving. All too often, the healthcare team may be sofocused on the disease process that lags occur in educat-ing families to integrate developmentally appropriatestrategies as a part of the child’s care. Each developmentalstage merits review with the family and the patient, whenage appropriate, to facilitate strategies that will allow thisspecialized care to be provided daily (DevelopmentalConsiderations 16–1). Parents must understand conceptssuch as offering the toddler a choice of juice to take withmedicines; thus, there is no unacceptable choice and thetoddler maintains the ‘‘control’’ for mastery of that stage.
Parents, caregivers, and patients must also be keptinformed regarding changes in condition and updateson expanding and newer therapies. They must be edu-cated when new therapies are introduced for mainte-nance care, such as oxygen, enteral home nutritionprograms, home intravenous antibiotic administration,home maintenance of venous access devices, administra-tion of aerosolized antibiotics, or the use of newly pre-scribed medications.
Community CareCF presents challenges, obstacles, and opportunities thatcan shape the child’s future. For parents, childrearing rolesand responsibilities can be complicated by the increaseddemands and restrictions imposed by CF (e.g., constantneed for daily treatments), numerous contacts with health-care services, altered plans for family outings and vacations,fatigue, depression, and, possibly, financial constraints.
Children living with CF must incorporate a variety oftreatments into their daily life, and these treatmentdemands and restrictions can often result in psychologicalstress and burdens for children and their families. Psycho-
logical functioning of the child and family depends onmultiple factors, such as family income, family structure,parental education levels, social support, and coping styles.Thus, nurses caring for these children and families mustcarefully assess for developmental and psychosocial risks.
The general approach for children with CF is to ‘‘nor-malize’’ their daily living activities (e.g., home, school,recreational) within the child’s specific limitations. Typi-cal childhood events such as a common cold can createsubstantial problems for the child with CF. Thus, parentsneed to use strict respiratory infection prevention strat-egies such as handwashing, isolating the child from peo-ple with respiratory or other infections, and isolating thechild from others with CF. Provide anticipatory guidancefor parents and children as they seek to maintain nor-malcy in their daily home lives.
For the parents of an infant or child newly diagnosedwith CF, the process of adjustment may be compared withthe grief process. Parents often have difficulty regainingstability for 6 months to 1 year after diagnosis. Patientsand their families may generally function adequately, butneed additional support during times of crisis. Some exam-ples are the first hospitalization after diagnosis, the deathof another child at the CF center, the transition to adultcare, addition of new home therapies such as oxygen or in-travenous antibiotics, or the first day of school.
Work closely with school personnel to develop an edu-cational plan that will promote learning and to reduceCF-associated risks. Encourage parents to provide schoolpersonnel with information (available through local CFcenters) about CF and about their child’s specific needs.Parent–teacher conferences at the beginning of eachschool year are an effective way to provide informationand establish communication to reduce the sense of dif-ference the child may feel at school. Encourage schoolattendance, so that the child can socialize and diversifyhis or her strengths to prepare for future goals. Social iso-lation because of sporadic school attendance can lead toother psychosocial issues, such as depression.
During adolescence, planning for the future and choosinga career are central tasks. Children must choose careers thatwill fulfill their ability to work despite changing conditions.Career and vocational counselors can assist in this planningprocess. Transitional care during the adolescent years, nec-essary to guarantee lifetime continuity of care, requires closecooperation between the patient’s pediatric and adult CFcenters. Transition to adult care usually occurs around age16 to 18 years, but the timing should be determined by theadolescent’s social maturity and health status.
The CF team members work in concert with each other,the families, and the children to support a common goal.Because of the complexities and variations of CF, many ofthe team’s functions overlap or may be carried out differ-ently across different centers. Supporting a family throughthe decision-making process of the end-of-life stage is gen-erally a process shared by all team members, but may bethe primary responsibility of the clinical social worker. It isalso critical for the CF team members to acknowledge thesupport systems of the family and to consult other profes-sionals, such as pastoral care services or psychologists.
See for a summary of Key Concepts.
724 Unit 3 n n Managing Health Challenges
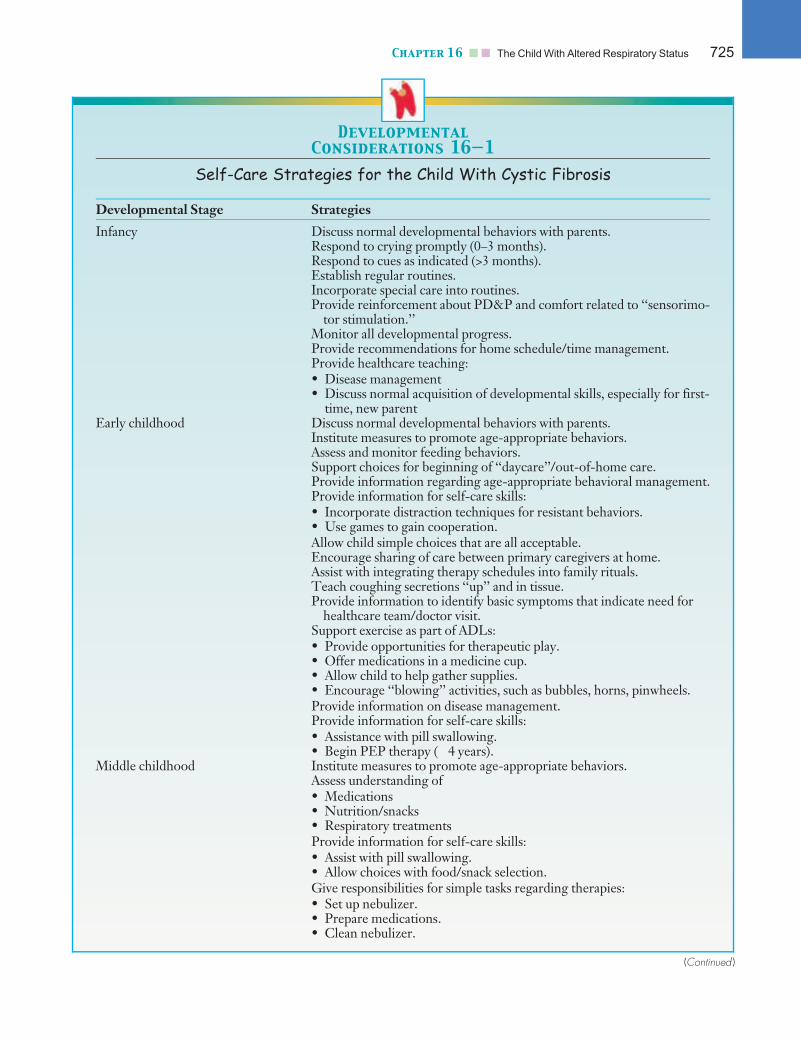
Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:40 User ID: muralir 1BlackLining Disabled
Developmental
Considerations 16—1
Self-Care Strategies for the Child With Cystic Fibrosis
Developmental Stage Strategies
Infancy Discuss normal developmental behaviors with parents.Respond to crying promptly (0–3 months).Respond to cues as indicated (>3 months).Establish regular routines.Incorporate special care into routines.Provide reinforcement about PD&P and comfort related to ‘‘sensorimo-
tor stimulation.’’Monitor all developmental progress.Provide recommendations for home schedule/time management.Provide healthcare teaching:• Disease management• Discuss normal acquisition of developmental skills, especially for first-
time, new parentEarly childhood Discuss normal developmental behaviors with parents.
Institute measures to promote age-appropriate behaviors.Assess and monitor feeding behaviors.Support choices for beginning of ‘‘daycare’’/out-of-home care.Provide information regarding age-appropriate behavioral management.Provide information for self-care skills:• Incorporate distraction techniques for resistant behaviors.• Use games to gain cooperation.Allow child simple choices that are all acceptable.Encourage sharing of care between primary caregivers at home.Assist with integrating therapy schedules into family rituals.Teach coughing secretions ‘‘up’’ and in tissue.Provide information to identify basic symptoms that indicate need for
healthcare team/doctor visit.Support exercise as part of ADLs:• Provide opportunities for therapeutic play.• Offer medications in a medicine cup.• Allow child to help gather supplies.• Encourage ‘‘blowing’’ activities, such as bubbles, horns, pinwheels.Provide information on disease management.Provide information for self-care skills:• Assistance with pill swallowing.• Begin PEP therapy (�4 years).
Middle childhood Institute measures to promote age-appropriate behaviors.Assess understanding of• Medications• Nutrition/snacks• Respiratory treatmentsProvide information for self-care skills:• Assist with pill swallowing.• Allow choices with food/snack selection.Give responsibilities for simple tasks regarding therapies:• Set up nebulizer.• Prepare medications.• Clean nebulizer.
(Continued )
Chapter 16 n n The Child With Altered Respiratory Status 725

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:40 User ID: muralir 1BlackLining Disabled
ReferencesAmerican Academy of Pediatrics. (2001). Clinical practice guideline:
Management of sinusitis. Pediatrics, 108(3), 798–808.American Academy of Pediatrics. (2003). Apnea, sudden infant death
syndrome, and home monitoring. Pediatrics, 111, 914–917.American Heart Association. (2005). Pediatric advanced life support.
Circulation, 112, IV-67 – IV-87.merican Lung Association. (2005). Lung disease data in culturally diverse
communities. Retrieved June 22, 2006, from www.lungusa.orgAmerican Thoracic Society. (2003). Statement on the care of the child
with chronic lung disease of infancy and childhood. American Journalof Respiratory and Critical Care Medicine, 168, 356–396.
Anon, J. B. (2003). Acute bacterial rhinosinusitis in pediatric medicine:Current issues in diagnosis and management. Pediatric Drugs,5(Suppl.), 25–33.
Asthma and Allergy Foundation of America. (2008). Asthma facts and fig-ures. Retrieved March 24, 2008, from http://www.aafa.org/display.cfm?id¼8&sub¼42
Bacharier, L., & Strunk, R. (2003). Pets and childhood asthma: Howshould the pediatrician respond to new information that pets may pre-vent asthma? Pediatrics, 111, 974–975.
Balaguer, A., Escribano, J., & Roque, M. (2003). Infant position in neo-nates receiving mechanical ventilation. The Cochrane Database of Sys-tematic Reviews, 2, CD003668.
Developmental Stage Strategies
Remind child to initiate ACT time.Have child answer health team’s questions.Include child in decision making.Incorporate exercise as part of ADLs: group or solo sports.Encourage use of wind instruments (horns).Coach during PEP/ACT therapy by caregiver.Discuss school performance/attendance and ways to ensure self-care at
school.Provide information on disease management.
Adolescence Institute measures to promote age-appropriate behaviors.Discuss/assess/monitor normal developmental concerns/issues.Provide information to facilitate increased self-care skills:• Self-administer medications, aerosol treatments, snack/meals, ACT.• Take inventory of medications.• Arrange for refills for medications.• Schedule clinic appointments.• Set up nocturnal/daily oxygen and check flow rate.Assess and monitor:• Understanding of disease process• Medication• Problem-solving skills• Current self-care behaviorsProvide information on disease management.Encourage and facilitate with individual and caregiver:• Monitoring of self-care by caregiver from afar• Decision for when parental presence is desired at clinic• Involvement in decision making• Negotiation of schedule with special eventsSupport exercise as part of ADLs:• Aerobic and anaerobic• Upper body strengthening• Stretching• Energy conservation techniquesProvide information on education and career planning.Facilitate discussion of peer relationships/dating.Discuss transitioning plans and process.Initiate referrals to support choices:• Genetic counseling• Sexuality issuesProvide information on insurance and healthcare systems.
ACT, airway clearance techniques; ADLs, activities of daily living; PD&P, postural drainage and percussion; PEP, positive expiratorypressure.Developed by Linda Tirabassi Davidson. Reprinted with permission of Long Beach Memorial Medical Center, Long Beach, CA.
726 Unit 3 n n Managing Health Challenges

Path: K:/LWW-BOWDEN-09-0101/Application/LWW-BOWDEN-09-0101-016.3dDate: 3rd July 2009 Time: 16:40 User ID: muralir 1BlackLining Disabled
Beauchamp, M., & Lands, L. C. (2005). Sweat-testing: A review of cur-rent technical requirements. Pediatric Pulmonology, 39, 507–511.
Berger, W. (2004). Allergic rhinitis in children: Diagnosis and manage-ment strategies. Pediatric Drugs, 6(4), 233–240.
Blaiss, M. S., on behalf of The Allergic Rhinitis in Schoolchildren Con-sensus Group. (2004). Allergic rhinitis and impairment issues inschoolchildren: A consensus report. Current Medical Research and Opin-ions, 20, 1937–1952.
Bradin, S. (2006). Croup and bronchiolitis: Classic childhood maladiesstill pack a punch. Consultant for Pediatricians, 5(1), 23–30.
Brennan, A. L., Gyi, K. M., Wood, D. M., Hodson, M. E., Geddes,D. M., & Baker, E. H. (2006). Relationship between glycosylatedhaemoglobin and mean plasma glucose concentration in cystic fibrosis.Journal of Cystic Fibrosis, 5, 27–31.
Centers for Disease Control. (2002). Annual smoking-attributable mor-tality, years potential life lost, and economic costs—United States,1995–1999. Morbidity and Mortality Weekly Reports, 51, 300–303.
Centers for Disease Control. (2004). Newborn screening for cystic fibrosis:Evaluation of benefits and risks and recommendations for state newbornscreening programs. Morbidity and Mortality Weekly Reports 53, 1–36.
Centers for Disease Control. (2005). Prevention and control of influ-enza. Morbidity and Mortality Weekly Reports, 54, 1–40.
Centers for Disease Control. (2006). The health consequences of invol-untary exposure to tobacco smoke: A report of the surgeon general.Retrieved July 12, 2006, from http://www.cdc.gov/tobacco/sgr/sgr_2006/index.htm
Cha, S., Kim, C., Park, J., & Jung, T. (2006). Bacterial tracheitis. Journalof Bronchology, 13(1), 35–36.
Cherry, J. (2005). State of the evidence for standard-of-care treatmentsfor croup: Are we where we need to be? Pediatric Infectious Disease Jour-nal, 24(Suppl.), S198–S202.
Christakis, D. A., Cowan, C. A., Garrison, M. M., Molteni, R., Marcuse,E., & Zerr, D. M. (2005). Variation in inpatient diagnostic testing andmanagement of bronchiolitis. Pediatrics, 115, 878–884.
Cincinnati Children’s Hospital Medical Center. (2006). Evidence-basedclinical practice guideline for medical management of bronchiolitis in infantsless than 1 year of age presenting with a first time episode. Cincinnati, OH:Author. Also available at www.guideline.gov
Copenhaver, C. C., Gern, J. E., Li, Z., et al. (2004). Cytokine response pat-terns, exposure to viruses, and respiratory infections in the first year of life.American Journal of Respiratory and Critical Care Medicine, 170, 175–180.
Cooper, A. C., Banasiak, N. C., & Allen, P. J. (2003). Management andprevention strategies for respiratory syncytial virus (RSV) bronchioli-tis in infants and young children: A review of evidence-based practiceinterventions. Pediatric Nursing, 29, 452–456.
Cystic Fibrosis Foundation. (2007). Cystic fibrosis: What you need to know.Retrieved April 15, 2008, from http://www.cff.org/AboutCF/
Cystic Fibrosis Foundation. (2008). Burkholderia cepacia and the CFfoundation’s participation policy. Retrieved April 15, 2008, from http://www.cff.org/LivingWithCF/StayingHealthy/Germs/Bcepacia/
Edenborough, F. (2001). Women with cystic fibrosis and their potentialfor reproduction. Thorax, 56, 649–655.
Edner, A., Ericson, M., & Katz-Salamon, M. (2002). Abnormal heartrate response to hypercapnia in boys with an apparent life-threateningevent. Acta Paediatrics, 91, 1318–1323.
Faden, H. (2006). The dramatic change in the epidemiology of pediatricepiglottitis. Pediatric Emergency Care, 22(6), 443–444.
Gauderman, W. J., Avol, E., Gilliland, F., et al. (2004). The effect of airpollution on lung development from 10 to 18 years of age. The NewEngland Journal of Medicine, 351, 1057–1067.
Gleason, M., Meltzer, E., Mullen, A., & Nicol, N. (2006). Childhood al-lergic rhinitis: Using clinical cues and optimizing management. TheAmerican Journal for Nurse Practitioners, 10(4), 45–52.
Goldrick, B., & Goetz, A. (2007). Pandemic influenza: What infection controlprofessionals should know. American Journal of Infection Control, 35, 7–13.
Green, D., Grosse, S., Earley, M., & Mei, J. (2005). Newborn screeningfor cystic fibrosis: A public health response. In M. Gwinn, S. Bedro-
sian, D. Ottmann, & M. Khoury (Eds.), Genomics and population health2005 (pp. 41–47). Atlanta, GA: Centers for Disease Control.
Hall, K. L., & Zalman, B. (2005). Evaluation and management of appa-rent life-threatening events in children. American Family Physician, 71,2301–2308.
Hayden, M. (2007). Caring for patients with allergic rhinitis. Journal ofthe American Academy of Nurse Practitioners, 19, 290–298.
Horemuzova, E., Katz-Salamon, M., & Milerad, J. (2002). Increasedinspiratory effort in infants with a history of apparent life-threateningevent. Acta Paediatrics, 91, 280–286.
Huysman, W. A., deRidder, M., deBruin, N. C., et al. (2003). Growthand body composition in preterm infants with bronchopulmonarydysplasia. Archives of Diseases in Children, Fetal, Neonatal Education, 88,F46–F51.
Institute of Medicine Committee on the Assessment of Asthma andIndoor Air, Division of Health Promotion and Disease Prevention.(2000). Clearing the air: Asthma and indoor air exposures. Washington,DC: National Academy Press.
Jartti, T., M€akel€a, M. J., Vanto, T., Ruuskanen, O. (2005). The linkbetween bronchiolitis and asthma. Infectious Disease Clinics of NorthAmerica, 19, 667–689.
Kerem, E., Conway, S., Elborn, S., & Hijerman, H. (2005). Standards ofcare for patients with cystic fibrosis: A European consensus. Journal ofCystic Fibrosis, 4, 7–26.
Leung, A. K. C., Keller, J. D., & Johnson, D. W. (2004). Viral croup: Acurrent perspective. Journal of Pediatric Healthcare, 18, 297–301.
Lindbaek, M. (2004). Acute sinusitis: Guide to selection of antibacterialtherapy. Drugs, 64(8), 805–819.
Liu, A. H., & National Institutes of Health. (2004). Optimizing child-hood asthma management: The role of National Institutes of Healthsponsored study groups. Proceedings of the American Academy of Allergyand Asthma, 25, 365–369.
Mitchell, E. A., & Thompson, J. (2001). Parental reported apnea, admis-sions to hospital and sudden infant death syndrome. Acta Paediatrics,90, 417–422.
National Heart, Blood and Lung Institute. (2007). National Asthma Educa-tion and Prevention Program expert panel report 3: Guidelines for the diagno-sis and management of asthma. NIH publication no. 08-5846. RetrievedMarch 24, 2008, from http://www.nhlbi.nih.gov/guidelines/asthma
Ober, C. (2005). Perspectives on the past decade of asthma genetics.Journal of Allergy and Clinical Immunology, 116, 274–278.
Park, S., Gerber, R., Tanz, R., Hickner, J., Galliher, J., Chuang, I., &Besser, R. (2006). Clinicians’ management of children and adolescentswith acute pharyngitis. Pediatrics, 117(6), 1871–1878.
Ramaden, H. (2004). Surgical management of chronic sinusitis in chil-dren. Laryngoscope, 114, 2103–2109.
Rowe, S. M., Miller, S., & Sorscher, E. J. (2005). Mechanisms of disease:Cystic fibrosis. New England Journal of Medicine, 352, 1992–2001.
Salib, R., Harries, P., Nair, S., & Howarth, P. (2008). Mechanisms andmediators of nasal symptoms in non-allergic rhinitis. Clinical & Envi-ronmental Allergy, 38, 393–404.
Schrag, S., Shay, D., Gershman, K., et al. (2006). Multistate surveillancefor laboratory-confirmed, influenza-associated hospitalizations in chil-dren: 2003–2004. Pediatric Infectious Disease Journal, 25(5), 395–400.
Smith, V. C., Zupanoc, J. A. F., McCormick, M. C., et al. (2005). Trendsin severe bronchopulmonary dysplasia rates between 1994 and 2002.Journal of Pediatrics, 146, 469–473.
Stokowski, L. (2005). A primer on apnea of prematurity. Advances in Neo-natal Care, 5(3), 155–170.
Taylor, S. (2003). Infections in children. Topics in Emergency Medicine,25(2), 166–173.
Yorita, K., Holman, R., Steiner, C., Effler, P., Miyamura, J., Forbes, S.,Anderson, L., & Balaramen, V. (2007). Severe bronchiolitis and respi-ratory syncytial virus among young children in Hawaii. Pediatric Infec-tious Disease Journal, 26, 1081–1088.
See for additional organizations.
Chapter 16 n n The Child With Altered Respiratory Status 727





























