Embed Size (px)
Citation preview

Synovial Fluid Lipid Abnormalities in Various Disease States: Review and Classification
By Christopher M. Wise, Randal E. White,* and Carlos A. Agudelo
IPIDS L CONSTITUTE a significant part of the soft tissues of the body, including areas
in and around the joints. Among the articular structures, the synovium, intraarticular fat pad, and bone marrow are the richest in lipid compo- nents, being composed of 70% to 90% lipids by
dry weight. Neutral lipids, particularly triglycer- ides, constitute most of the lipid content of these tissues. Articular cartilage, ligaments, and
menisci, on the other hand, contain only 58% to 68% lipids.’
Synovial fluid is considered to be a filtrate of
plasma combined with locally synthesized hyal- uranic acid, and most biochemical investigations of synovial fluid have focused on protein and polysaccharide constituents. Because of the rela- tive paucity of lipid components in most synovial fluids and the lack of generally recognized clini- cal correlates to abnormalities when they do
occur, little attention has been devoted to the discussion of synovial fluid lipid components,
even in recent reviews of synovial fluid analy- sis.2-4 This report reviews what is known about
the lipid content of normal synovial fluid and that found in common joint diseases. Previously reported abnormalities of synovial fluid lipids are also reviewed and classified.
LIPIDS IN “TYPICAL” SYNOVIAL FLUIDS
Although lipids are present in synovial fluid,
their levels are much less than those usually
Christopher M. Wise, MD: Assistant Professor of Medi-
cine (Rheumatology). Randal E. White, MD: Fellow in
Rheumatology, and Carlos A. Agudelo, MD: Associate Professor of Medicine (Rheumatology), Bowman Gray
School of Medicine, Wake Forest University, Winston- Salem, NC.
From the Section on Rheumatology, Bowman Gray
School of Medicine of Wake Forest University, Winston-
Salem, NC. *Dr White is currently Assistant Clinical Professor of
Medicine, East Carolina University School of Medicine,
Greenville, NC. Address reprint requests to Christopher M. Wise, MD,
Assistant Professor of Medicine (Rheumatology), Bowman Gray School of Medicine, 300 S Hawthorne Rd. Winston- Salem, NC 27103.
0 I987 by Grune & Stratton, Inc.
0049~172/87/1603-0007%5.00/0
found in plasma. In 1962, Bole5 first reported that normal synovial fluid contained only trace amounts of cholesterol and phospholipids (~10 to 1.5 mg/dL each), and almost no triglycerides or other neutral lipids.5 In subsequent studies of synovial fluid from patients with rheumatoid
arthritis (RA) and osteoarthritis (OA), concen- trations of these components and fatty acids have been found to be in the range of 20% to 60% of
that found in plasma.5-8 Generally, very little difference in synovial fluid lipid levels has been noted between these two conditions, and there has been no correlation between lipid levels, synovial fluid leukocyte (WBC) count, or sev- erity or duration of disease in RA.
Differences have also been noted between the lipoproteins found in synovial fluid and those found in plasma. Chung et al” first noted that the ratio of cholesterol to phospholipid in synovial fluid was comparable with that found in lower-
density (< 1.063) lipoproteins in serum. Small et al9 found that total lipoprotein levels in synovial
fluid average 40% of those found in serum, and that levels were higher in inflammatory (RA and gout) than in noninflammatory (OA) effusions. Differences in distribution of lipoproteins were also noted. Certain classes (classes I and II) of low-density lipoproteins were reduced, compared with serum levels, while others (classes III and IV) were similar. In addition, all synovial fluids contained increased amounts of a particular frac- tion of high-density lipoprotein (class Va). More recently, Altman et al’ have shown that the
distribution of apoproteins AI and AI1 was shifted toward lower densities in synovial fluid from patients with RA and OA. In addition, a preponderance of large, high-density lipoproteins rich in cholesterol, apoprotein AI, and apopro- tein E was also noted.
Thus, most systematic studies of synovial fluids have shown quantitative and qualitative differences from plasma in lipid and lipoprotein components. Although the relative permeability of the synovium to these components may par- tially explain these findings, many other factors apparently play a role. Viscosity changes due to hyaluronate degradation, altered synovial mem-
222 Seminars in Arthritis and Rheumatism, Vol 16, No 3 (February), 1987: pp 222-230

SYNOVIAL FLUID LIPID ABNORMALITIES 223
brane metabolism, differences in the absorption rate of different lipoprotein classes, and local biosynthesis have all been considered possible mechanisms. Most data suggest that alteration of filtered plasma lipoproteins, particularly high- density lipoproteins, by synovial tissue accounts for most of the findings of lipids and lipoproteins in “typical” synovial fluids.’
To our knowledge, there have been no system- atic studies of synovial fluid lipid components in disease states other than RA or OA. Even in the various syndromes of hyperlipoproteinemia, in which articular symptoms and even synovitis are well described, synovial fluid lipids approximate 40% to 60% of plasma values, as in RA and OA, and striking abnormalities have not been noted.” Nevertheless, abnormal accumulations of lipids within synovial fluid have been the subject of numerous reports over the years, and recognition of synovial fluid lipid abnormalities and their clinical significance may be important in certain circumstances. Although there is considerable overlap, previous descriptions fall loosely into three categories, as summarized in Table 1: (1) cholesterol-rich effusions, (2) lipid droplets within synovial fluid, and (3) chylous synovial effusions.
Cholesterol-Rich Eflusions
Synovial fluids containing abnormally high levels of cholesterol with microscopically identi- fiable cholesterol crystals (flat, plate-like struc- tures with variable birefringence; Fig I) are rare, constituting only approximately 0.1% to 0.3% of all synovial fluids examined.1’*‘2 The appearance of cholesterol-rich fluid may vary from straw colored to thick, yellow, milky (chylous), and semisolid.“-‘9 Synovial fluid cholesterol levels in these effusions may range from that of serum to as high as 2,600 mg/dL (10 to 15 times that of serum), while triglyceride levels in these effu- sions range from “normal” to two to three times that of serum levels.
Previous descriptions of synovial fluid contain- ing cholesterol crystals are limited almost exclu- sively to fluid from patients with chronic RA,“-18 although there have been occasional reports in patients with ankylosing spondylitis, idiopathic bursitis,” and 0A.19 In the largest published series of these fluids, cholesterol crystals were described in 16 fluids from 12 patients, ten of
whom had RA.” All RA patients had chronic seropositive disease, and most were anatomic stage III or IV with extraarticular manifesta- tions. The knee and olecranon bursa were the most common sources of fluid with cholesterol crystals. Interestingly, three of 14 fluids obtained from patients with RA were associated with a superimposed infectious arthritis. The investiga- tors did not feel that synovial fluid cholesterol played a role in predisposing to these infections, but speculated that infection might have played a role in the development of cholesterol crystals. To our knowledge, however, such crystals have never been described in other cases of infectious arthritis.
Synovial fluid WBC counts in cholesterol- containing effusions are highly variable, proba- bly reflecting the activity of the underlying dis- ease. Because of this, most investigators believe that cholesterol crystals themselves have rela- tively weak phlogistic properties. Pritzker et al confirmed this in an animal model, evoking only a mild acute inflammatory response in rabbit knees injected with cholesterol crystals.20
As outlined in Table 1, several mechanisms have been proposed to account for the abnormal accumulations of cholesterol in these patients. Excessive local tissue destruction,” intraarticu- lar hemorrhage with defective clearance of RBC products,‘3 and defective synovial sterol metabo- lism16 were suggested on the basis of clinical observations in some early patients. Newcombe and CohenI demonstrated a marked increase in radiolabeled sterol after injection of 14C into the joint space of such a patient, suggesting that local synovial biosynthesis was responsible for cholesterol accumulation, On the basis of com- parative crystal analysis, Nye et alI5 suggested that lipids were liberated after partial degrada- tion of plasma lipoproteins and trapped within the synovial space by recombination with pro- teins and crystallization. Ettlinger and Hunder” theorized that recently described anti-lipoprotein antibodies2’ might be responsible for such a phenomenon.
Cholesterol crystals have also been described in pleural and pericardial fluids from occasional RA, and similar mechanisms for these accumu- lations have been proposed.22-24 However, the association of pleural and pericardial cholesterol crystals with several other conditions (tuberculo-
224 WISE, WHITE, AND AGUDELO
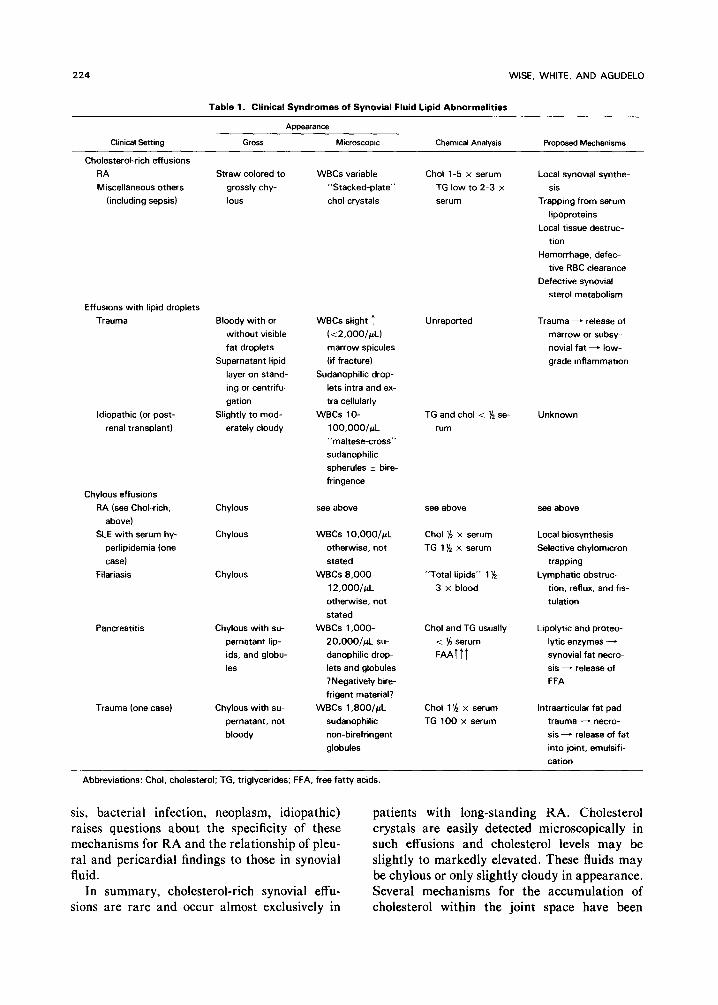
Table 1. Clinical Syndromes of Synovial Fluid Lipid Abnormalities
Clinical Settrng Gross Microscopic Chemical Analysis Proposed Mechanisms
Cholesterol-rich effusions
RA
Miscellaneous others
(including sepsis)
Straw colored to
grossly chy-
lous
WBCs variable
“Stacked-plate”
chol crystals
Chol l-5 x serum
TG low to 2-3 x
serum
Local synovial synthe-
sis
Trappmg from serum
lipoproteins
Local tissue destruc-
tion
Hemorrhage, defec-
tive RBC clearance
Defective synovial
sterol metabolism
Effusions with lipid droplets
Trauma Bloody with or
without visible
fat droplets
Supernatant lipid
layer on stand-
ing or centrifu-
gation
Idiopathic (or post- Slightly to mod-
renal transplant) erately cloudy
Chylous effusions
RA (see Chol-rich,
above)
SLE with serum hy-
perlipidemia (one
case)
Filariasis
Pancreatitis
Trauma (one case)
Chylous see above
Chvlous WBCs lO,OOO/~L
otherwise, not
stated
WBCs B.OOO-
12,OOO/~L
otherwise, not
stated
WBCs 1 ,OOO-
20,000/~L su-
danophilic drop-
lets end globules
lNegatively bire-
frigent material?
WBCs 1 ,BOO/jrL
sudanophilic
non-birefringent
globules
Chylous with su-
pernatant lip-
ids, and globu-
les
Chylous with su-
pernatant, not
bloody
WBCs slight 1
f<2.000/~L)
marrow spicules
(if fracture)
Sudanophilic drop-
lets intra and ex-
tra cellularly
WBCs lo-
100.000l~L
“maltese-cross”
sudanophilic
spherules 2 bire-
fringence
Unreported
TG and chol < ‘x se-
rum
see above
Chol ‘h x serum
TG 1% x serum
“Total lipids” 1 $-
3 x blood
Chol and TG usually
i ‘h serum
FAAttT
Chol 1% x serum
TG 100 x serum
Trauma - release of
marrow or subsy-
novial fat - low-
grade inflammation
Unknown
see above
Local biosynthesis
Selective chylomicron
trapping
Lymphatic obstruc-
tion, reflux, and fis-
tulation
Lipolytic and proteo-
lytic enzymes -
synovial fat necro-
sis - release of
FFA
lntraarticular fat pad
trauma - necro-
sis - release of fat
into joint. emulsifi-
cation
Abbreviations: Chol, cholesterol: TG, triglycerides; FFA, free fatty acids.
sis, bacterial infection, neoplasm, idiopathic) raises questions about the specificity of these mechanisms for RA and the relationship of pleu- ral and pericardial findings to those in synovial fluid.
In summary, cholesterol-rich synovial effu- sions are rare and occur almost exclusively in
patients with long-standing RA. Cholesterol crystals are easily detected microscopically in such effusions and cholesterol levels may be slightly to markedly elevated. These fluids may be chylous or only slightly cloudy in appearance. Several mechanisms for the accumulation of cholesterol within the joint space have been
SYNOVIAL FLUID LIPID ABNORMALITIES 225
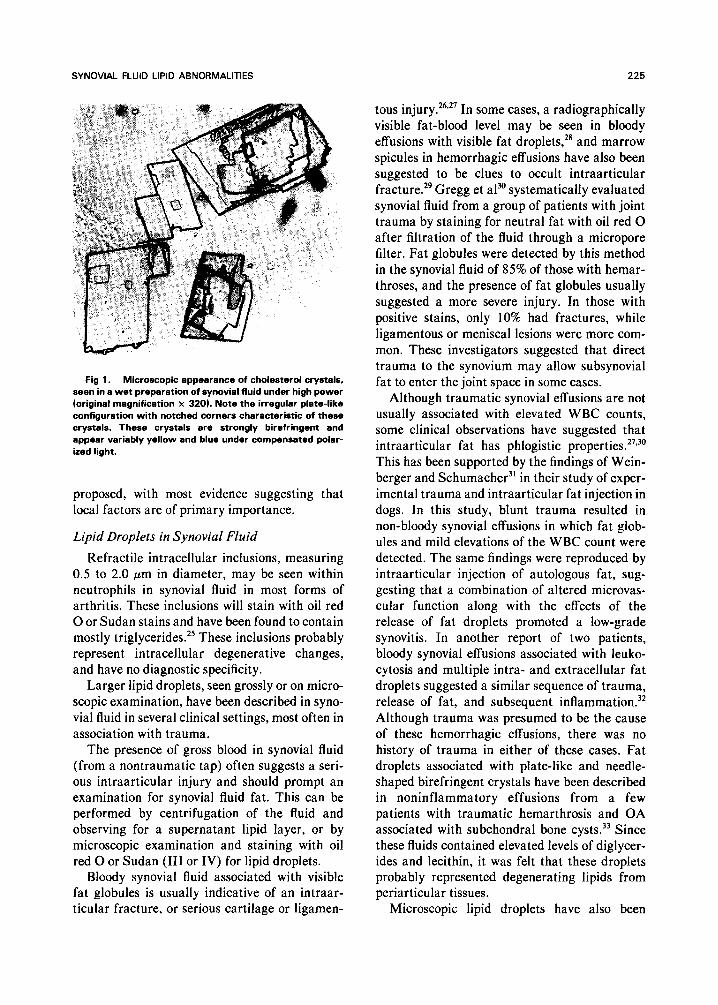
Fig 1. Microscopic appearance of cholesterol crystals, seen in a wet preparation of synovial fluid under high power (original magnification x 3201. Note the irregular plate-like configuration with notched corners characteristic of these crystals. These crystals are strongly birefringent and appear variably yellow and blue under compensated polar- ized light.
proposed, with most evidence suggesting that local factors are of primary importance.
Lipid Droplets in Synovial Fluid
Refractile intracellular inclusions, measuring 0.5 to 2.0 pm in diameter, may be seen within neutrophils in synovial fluid in most forms of arthritis. These inclusions will stain with oil red 0 or Sudan stains and have been found to contain mostly triglycerides.” These inclusions probably represent intracellular degenerative changes, and have no diagnostic specificity.
Larger lipid droplets, seen grossly or on micro- scopic examination, have been described in syno- vial fluid in several clinical settings, most often in association with trauma.
The presence of gross blood in synovial fluid (from a nontraumatic tap) often suggests a seri- ous intraarticular injury and should prompt an examination for synovial fluid fat. This can be performed by centrifugation of the fluid and observing for a supernatant lipid layer, or by microscopic examination and staining with oil red 0 or Sudan (III or IV) for lipid droplets.
Bloody synovial fluid associated with visible fat globules is usually indicative of an intraar- titular fracture, or serious cartilage or ligamen-
tous injury. 26P27 In some cases, a radiographically visible fat-blood level may be seen in bloody effusions with visible fat droplets,28 and marrow spicules in hemorrhagic effusions have also been suggested to be clues to occult intraarticular fracture.29 Gregg et a?’ systematically evaluated synovial fluid from a group of patients with joint trauma by staining for neutral fat with oil red 0 after filtration of the fluid through a micropore filter. Fat globules were detected by this method in the synovial fluid of 85% of those with hemar- throses, and the presence of fat globules usually suggested a more severe injury. In those with positive stains, only 10% had fractures, while ligamentous or meniscal lesions were more com- mon. These investigators suggested that direct trauma to the synovium may allow subsynovial fat to enter the joint space in some cases.
Although traumatic synovial effusions are not usually associated with elevated WBC counts, some clinical observations have suggested that intraarticular fat has phlogistic properties.27’0 This has been supported by the findings of Wein- berger and Schumacher3’ in their study of exper- imental trauma and intraarticular fat injection in dogs. In this study, blunt trauma resulted in non-bloody synovial effusions in which fat glob- ules and mild elevations of the WBC count were detected. The same findings were reproduced by intraarticular injection of autologous fat, sug- gesting that a combination of altered microvas- cular function along with the effects of the release of fat droplets promoted a low-grade synovitis. In another report of two patients, bloody synovial effusions associated with leuko- cytosis and multiple intra- and extracellular fat droplets suggested a similar sequence of trauma, release of fat, and subsequent inflammation.32 Although trauma was presumed to be the cause of these hemorrhagic effusions, there was no history of trauma in either of these cases. Fat droplets associated with plate-like and needle- shaped birefringent crystals have been described in noninflammatory effusions from a few patients with traumatic hemarthrosis and OA associated with subchondral bone cysts.33 Since these fluids contained elevated levels of diglycer- ides and lecithin, it was felt that these droplets probably represented degenerating lipids from periarticular tissues.
Microscopic lipid droplets have also been

226 WISE, WHITE, AND AGUDELO
described in patients without a history of trauma
or gross hemarthrosis. Weinstein described a patient with an acute monoarthritis associated with synovial fluid leukocytosis and intracellular “Maltese cross” lipid inclusions, and only mild elevations of synovial fluid cholesterol and trigly- ceride.34 The presence of birefringent intra-and extracellular lipid microspherules has also been associated with acute inflammatory arthritis in
three other patients.35 Although all three of these patients had some possibly associated condition
(sarcoidosis, minor trauma, cirrhosis), serum and synovial fluid lipid levels were normal and no obvious mechanism for entry of these crystals into the joint space was apparent. In further reports from the same institution, Maltese cross inclusions were reproduced by intraarticular
injection of blood,36 and transient synovitis was
induced in rabbits by intraarticular injection of these liposomes3’ These findings suggest that such “lipid liquid crystals” may be derived from
the breakdown of RBCs and have phlogistic
properties. Schlesinger et a13’ described a chronic unex-
plained polyarthritis in a 14-year-old boy whose
synovial fluid contained from 5,000 to 100,000 macrophages/pL filled with Maltese cross lipid inclusions and low (< 40% serum) levels of cho- lesterol and triglycerides. Finally, small numbers of lipid droplets have been described in synovial fluid from patients with aseptic necrosis or syno- vitis after renal transplantation.39
Chylous Synovial Effusions
The occurrence of massive amounts of emul-
sified lipid in synovial fluid resulting in a chylous, or milky-appearing, effusion is extremely rare. Although initially appearing to be purulentchy- lous synovial effusions usually contain only mildly elevated WBC counts, and the appear- ance can be attributed to lipid components within the fluid, which can be measured by chemical
methods or seen microscopically. Chylous syno- vial effusions have been reported in association with RA, systemic lupus erythematosus (SLE; with hyperlipidemia), filariasis, pancreatitis, and
trauma. Chylous synovial effusions in RA are very
uncommon, having been reported in only a few instances, as discussed previously.‘2V’4.‘8 When
associated with RA, these effusions usually con- tain markedly increased levels of cholesterol and
are associated with the presence of easily identi- fiable cholesterol crystals. As noted, several mechanisms for this phenomenon have been pro- posed, with most suggesting that local factors are responsible for the accumulation of cholesterol in these amounts within the joint space.
A single case of chylous synovial effusion has been reported in a patient with SLE.40 In this
patient, there was a subacute monoarticular arthritis in which a thick synovial fluid contain-
ing 10,000 WBCs/pL was removed. This patient was found to have elevated serum cholesterol and
triglycerides, with a pattern suggestive of what would now be considered a type 11-b hyperlipo- proteinemia. The synovial fluid contained a cho- lesterol level of approximately one half that of serum (3 14 mg/dL v 566 mg/dL), while trigly-
cerides were 1,500 mg/dL, compared with a serum level of 930 mg/dL. The investigators suggested that local biosynthesis was the most likely cause of excess lipids, since no serum
lipoproteins could be detected in the synovial fluid. Selective trapping of chylomicrons was also considered a possible pathogenetic mecha- nism.
Several cases of chylous synovial effusions simulating septic arthritis have been reported in association with filariasis4’ In most of these patients, an acute arthritis presented with marked swelling and fever, and symptoms sub- sided with bedrest in seven to ten days. Estima-
tions of total synovial fluid lipids showed levels from 1’/2 to three times that of normal blood.
Since most of these patients had clinical or radiographic evidence of lymphatic obstruction, a phenomenon of “chylous reflux” and lymphatic fistulation with extravasation of chyle into the joint space was suggested as the mechanism for the development of these effusions. Synovial his- topathology in these patients demonstrated a suppurative synovitis acutely followed by chronic granulation tissue, lymphocytic infiltration, and synovial hyperplasia.
The syndrome of pancreatitis associated with fat necrosis and arthritis (the pancreatitic arthri- tis syndrome) may also be associated with chy- lous synovial effusions42-45 or bursal effusions.46 Although most early reports of this syndrome
SYNOVIAL FLUID LIPID ABNORMALITIES
Table 2. Synovial Fluid Findings Suggesting
Lipid Abnormalities
Gross analysis
“Purulent” appearance with few WBCs (Chylous)
Visible lipid droplets
Supematant lipid layer after standing or centrifugation
Microscopic analysis
Cholesterol crystals (stacked rectangular plates with
notched corners, variable birefringence)
Globules or spherules
Intra- or extracellular (small 0.5-2.0 jrm refractile inclu-
sions in neutrophils are nonspecific)
May be birefringent, with a “maltese cross” appear-
ance
Stain with oil red 0, or Sudan Ill or IV
Chemical analysis
Cholesterol or triglycerides in most fluids are 40% to 60%
serum levels
7 Cholesterol may suggest RA, other miscellaneous condi-
tions
7 Triglycerides may suggest RA (occasionally), SLE (rare-
ly), trauma
1 Free fatty acids suggest pancreatitis
Amylase or lipase may be elevated in pancreatitis
described non-inflammatory “sympathetic” ef- fusions, Smuckler et a142 described an opaque fluid with a WBC count of only 4,OOO/pL and multiple fat droplets and birefringent crystalline material on microscopic examination. Synovial histopathology showed evidence of fat necrosis within the synovium itself, suggesting that the direct release of fat into the synovial space resulted in an inflammatory reaction. Similar
227
findings were noted in the single case of chylous bursal effusion described.46 Further observations in these patients demonstrated marked elevation of serum levels of lipolytic and proteolytic enzymes (lipase, phospholipase A, trypsin), and marked increases in synovial fluid free non- esterified fatty acids ( FFA).44,45 Synovial fluid amylase44 and lipase4’ have been elevated in some cases, but normal in others. Although none of the above cases have been associated with serum lipid abnormalities, some fluids have shown mod- est elevations of triglyceride and cholesterol lev- els over those of plasma. In addition, pathologic fractures and osteonecrosis in adjacent bones were noted in at least two of these patients.42346
Synovial fluid WBC counts in this syndrome generally reflect mild to moderate inflammation (1,000 to 20,000 WBCs/pL), suggesting that FFAs have phlogistic properties. Simkin et a145 confirmed this experimentally by injecting an FFA-albumin complex into rabbit knees and demonstrating increased synovial fluid WBCs compared with opposite knees injected with con- trol substances. Stainable fat globules were dem- onstrated within polymorphonuclear leukocytes in these fluids. Since injected FFAs were not stainable, these findings suggested that FFAs were cleared from the synovial fluid by WBCs and re-esterified into triglycerides, resulting in sudanophilic globules.
Although synovial fluid after trauma may be
228
bloody with fat droplets present (see previous discussion), we recently described a patient with a chylous nonhemorrhagic knee effusion follow- ing direct trauma.47 In this case, extensive radio-
logic evaluation revealed no evidence of fracture, synovial fluid triglycerides were markedly ele-
vated (11,300 mg/dL v serum 142 mg/dL), and
cholesterol was moderately elevated (370 mg/dL v serum 218 mg/dL). Microscopically, numerous extracellular non-birefringent lipid globules were seen, and the synovial fluid WBC count was only 1,800 cells/pL. This effusion resolved sponta- neously within 8 weeks. This case suggests that a chylous effusion may result from intraarticular
fat pad necrosis, disruption of the synovium, and subsynovial fat release.
SUMMARY
Although lipids are not usually present in large quantities in normal synovial fluids or in the usual synovial fluid seen in most rheumato- logic conditions, their presence in synovial fluid may have diagnostic importance.
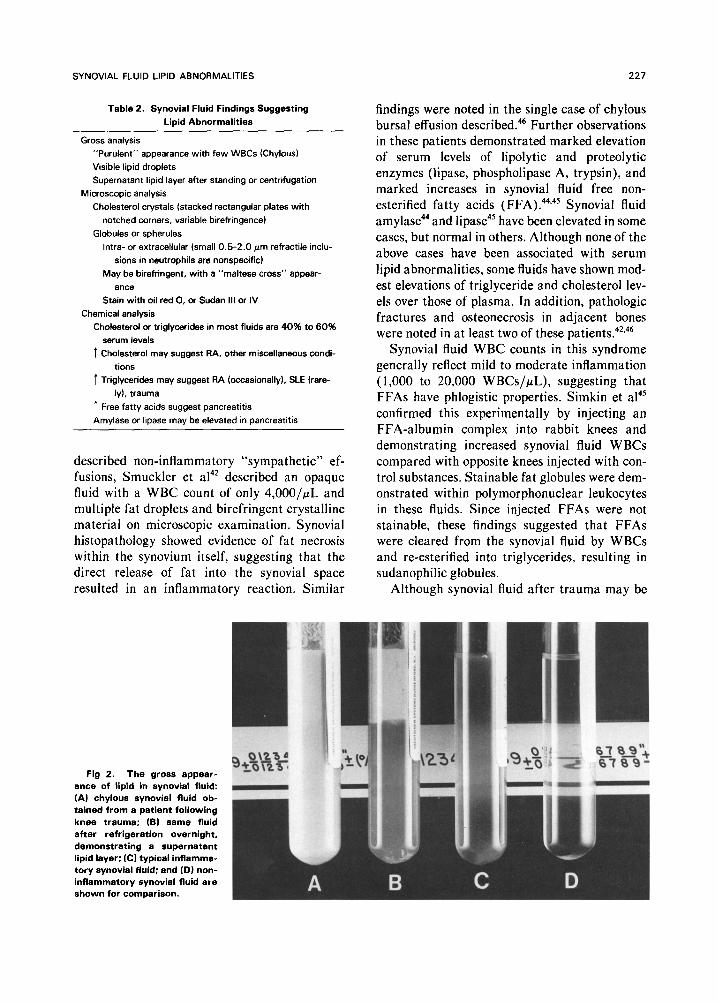
As summarized in Table 2, analysis of synovial fluids for lipid constituents is relatively simple. On standing or after centrifugation, significant amounts of lipids may layer out and be visible as a supernatant (Fig 2). On microscopic examina- tion, lipid droplets are usually easily seen and
should be stainable with appropriate dyes (oil red 0 or Sudan III or IV) (Fig 3), or may occasion-
WISE, WHITE, AND AGUDELO
ally be visualized as intracellular or extracellular inclusions by polarized microscopy. Small (0.5 to
2.0 pm) intracellular inclusions containing tri- glycerides may be seen in neutrophils from most synovial fluids, and are of no diagnostic impor-
tance. Cholesterol crystals may be readily recog- nized microscopically by their characteristic flat, plate-like appearance and notched corners (Fig
1). Synovial fluid may also be analyzed for cholesterol and triglycerides in routine clinical laboratories, and free fatty acids and lipolytic enzymes in special lipid laboratories.
The presence of massive increases in choles- terol associated with microscopically visible cho-
lesterol crystals is usually associated with chronic RA, occasionally in the setting of super- imposed bacterial infection. The presence of gross or microscopic lipid droplets is usually
associated with trauma and hemorrhagic effu- sions. When present in this setting, the clinican should entertain a high suspicion for a significant intraarticular injury, such as fracture, meniscal tear, or severe ligamentous injury. In addition, however, several instances of non-traumatic inflammatory effusions associated with intracel- lular and extracellular lipid droplets have been
reported. The clinical significance of these cases has not been clarified. Finally, chylous effusions
are extremely rare and associated with only a limited number of conditions. RA, SLE with
hyperlipidemia, filariasis with associated lym-
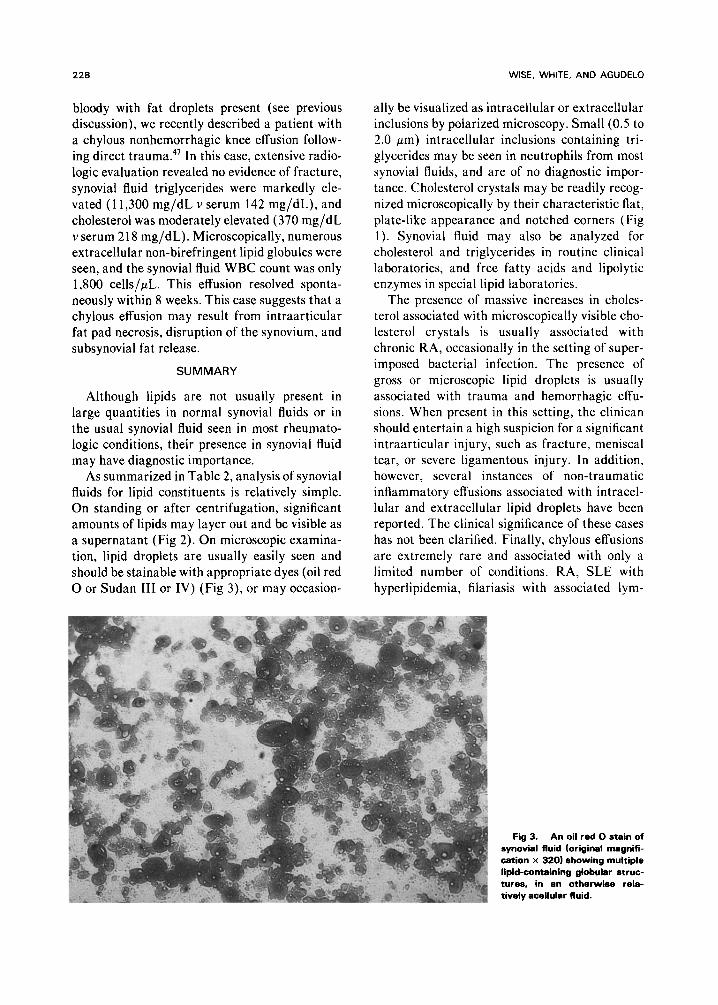
Fig 3. An oil red 0 stain of I i synovial fluid (original magnifi-
cation x 320) showing multiple lipid-containing globular struc- tures, in an otherwise rela- tively acellular fluid.
SYNOVIAL FLUID LIPID ABNORMALITIES 229
phatic obstruction, pancreatitis with fat necrosis, vated in those patients with rheumatoid-asso- and trauma have all been described in associa- ciated effusions, free fatty acids in those with the tion with chylous effusions. Determination of syndrome associated with pancreatitis, and tri- synovial fluid lipids may be of value in differen- glycerides in the case associated with direct tiating these, since cholesterol tends to be ele- trauma.
REFERENCES
1. Rabinowitz JL, Gregg JR, Nixon JE, et al: Lipid
composition of the tissues of human knee joints. Clin Orthop
143:260-265, 1979
2. Platt PN: Examination of synovial fluid. Clin Rheum
Dis 9:51-67, 1983
3. Gatter RA: A Practical Handbook of Joint Fluid Anal-
ysis. Philadelphia, Lea & Febiger, 1984
4. Schumacher HR: Synovial fluid analysis, in Kelley
WN, Harris ED, Ruddy S, et al (eds): Textbook of Rheuma-
tology (ed 2). Philadelphia, Saunders, 1985, pp 561-568
5. Bole GG: Synovial fluid lipid in normal individuals and
patients with rheumatoid arthritis. Arthritis Rheum 5:589-
601, 1962
6. Chung AC, Shanahan JR, Brown EM: Synovial fluid in
rheumatoid and osteoarthritis. Arthritis Rheum 5:176-182,
1962
7. Altman RD, Goldberg RB, Gibson JC, et al: Synovial
fluid contains large cholesterol-rich high density lipoproteins.
Arthritis Rheum 29:S39, 1986 (abstr)
8. Kim C, Cohen AS: Synovial fluid fatty acid composi-
tion in patients with rheumatoid arthritis, gout, and degener-
ative joint disease. Proc Sot Exp Biol Med 123:77-80, 1966
9. Small DM, Cohen AS, Schmid K: Lipoproteins of
synovial fluid as studied by analytical ultracentrifugation. J
Clin Invest 43:207&2079, 1964
10. Bole GG: Arthritis associated with hyperlipidemia
and hypercholesterolemia, in Kelly WN, Harris ED, Ruddy
S, et al (eds): Textbook of Rheumatology (ed 1). Philadel-
phia, Saunders, 1981, pp 1638-1646
11. Ropes MW, Bauer W: Synovial Fluid Changes in
Joint Disease. Cambridge, MA, Harvard University Press,
1953
12. Ettlinger RE, Hunder GG: Synovial effusions contain-
ing cholesterol crystals. Report of 12 patients and review.
Mayo Clin Proc 54:366-374, 1979
13. Zuckner J, Uddin J, Gantner GE, et al: Cholesterol
crystals in synovial fluid. Ann Intern Med 60:436-446, 1964
14. Newcombe DS, Cohen AS: Chylous synovial effusion
in rheumatoid arthritis. Am J Med 38:156-164, 1965
15. Nye WHR, Terry R, Rosenbaum DL: Two forms of
crystalline lipid in “cholesterol” effusions. Am J Clin Pathol
49:718-728,1968
16. Griffen PE, Bole GG: Cholesterol-containing synovial
effusions and cholesterosis of the synovial membrane. Univ
Mich Med Cent J 35: 170-l 76, 1969
17. Bland JH, Gierthy JF, Suhre ED: Cholesterol in
connective tissue of joints. Stand J Rheumatol 3:199-203, 1974
18. Meyers OL, Watermeyer GS: Cholesterol rich syno-
vial effusions. Afr Med J 50:973-975, 1976
19. Fam AC, Pritzker KPH, Cheng PT, et al: Cholesterol
crystals in osteoarthritic joint effusions. J Rheumatol 8:273-
280, 1981
20. Pritzker KPH, Fam AC, Omar SA, et al: Experimen-
tal cholesterol crystal arthropathy. J Rheumatol 8:281-290,
1981
21. Noseda G: Anti-Lipoprotein-Autoantikorper mit Hy-
polipidamie bei entzundlichem Rheumatismus. Schweiz Med
Wochenschr 105:1-58, 1975 (suppl)
22. Shiel WC, Prete PE: Pleuropulmonary manifestations
of rheumatoid arthritis. Semin Arthritis Rheum 13:235-243,
1984
23. Ferguson CC: Cholesterol pleural effusion in rheuma-
toid lung disease. Thorax 21:577-582, 1966
24. Kindred LH, Heilbrunn A, Dunn M: Cholesterol
pericarditis associated with rheumatoid arthritis, Treatment
by pericardiectomy. Am J Cardiol 23:464-468, 1969
25. Hersko C, Michaeli D, Schibolet S, et al: The nature
of refractile inclusions in leukocytes of synovial effusions. Isr
J Med Sci 3:838-846, 1967
26. Kling DH: Fat in traumatic effusions of knee joints.
Am J Surg 6171-74, 1929
27. Schumacher HR: Traumatic joint effusion and the
synovium. J Sports Med 3:108-l 14, 1975
28. Berk RN: Liquid fat in the knee joint after trauma. N
Engl J Med 277:1411-1412, 1967
29. Lawrence C, Seife B: Bone marrow in joint fluid. A
clue to fracture. Ann Intern Med 74:740-742, 1971
30. Gregg JR, Nixon JE, DiStefano V: Neutral fat globu-
les in traumatized knees. Clin Orthop 132:219-224, 1978
31. Weinberger A, Schumacher HR: Experimental joint
trauma: Synovial response to blunt trauma and inflammatory
reaction to intraarticular injection of fat. J Rheumatol
8:38&389, 198 1
32. Graham J, Goldman JA: Fat droplets and synovial
fluid leukocytosis in traumatic arthritis. Arthritis Rheum
21:76-80, 1978
33. Reginato AJ, Choi SJ, Schumacher HR, et al: Unu-
sual birefringent crystals in synovial fluid of patients with
osteoarthritis and subchondral bone cysts and in hemarthro-
sis. Athritis Rheum 29:SlS, 1986 (abstr)
34. Weinstein J: Synovial fluid leukocytosis associated
with intracellular lipid inclusions. Arch Intern Med 140:560-
561,198O
35. Reginato AJ, Schumacher HR, Allan DA, et al: Acute
monoarthritis associated with lipid liquid crystals, Ann
Rheum Dis 44:537-543, 1985
36. Choi SJ, Clayburne G, Schumacher HR: Experimen-
tal hemarthrosis produces mild inflammation associated with
intracellular Maltese crosses. Arthritis Rheum 29:S90, 1986
(abstr)
37. Choi SJ, Schumacher HR, Clayburne G, et al: Lipo-

230 WISE, WHITE, AND AGUDELO
some-induced synovitis in rabbits. Arthritis Rheum 28S79,
1985 (abstr)
38. Schlesinger PA, Stillman MT, Peterson L: Polyarthri-
tis with birefringent lipid within synovial fluid macrophages:
Case report and ultrastructural study. Arthritis Rheum
25:1365-1367,1982
39. Bravo JF, Herman JD, Smyth CJ: Musculoskeletal
disorders after renal homotransplantation-A clinical and
laboratory analysis of 60 cases. Ann Intern Med 66:87-104,
1967
40. Ryan WE, Ellefson RD, Ward LE: Lipid synovial
effusion-unique occurrence in systemic lupus erythematosus.
Arthritis Rheum 16:759-764, 1973
41. Das GC, Sen SB: Chylous arthritis. Br Med J 2:27-29,
I968
42. Smukler NM, Schumacher HR, Pascual E, et al:
Synovial fat necrosis associated with ischemic pancreatic
diseases. Arthritis Rheum 22:547-553, 1979
43. Phillips RM, Sulser RE, Songharoen S: Inflammatory
arthritis and subcutaneous fat necrosis associated with acute
and chronic pancreatitis. Arthritis Rheum 23:355-360, 1980
44. Wilson HA, Askari AD, Neiderhiser DH, et al: Pan-
creatitis with arthropathy and subcutaneous fat necrosis.
Evidence for pathogenicity of lipolytic enzymes. Arthritis
Rheum 23:121-126,1983
45. Simkin PA, Brunzell JD, Wisner D, et al: Free fatty
acids in the pancreatitic arthritis syndrome. Arthritis Rheum
26:127-132, 1983
46. Halla JT, Schumacher HR, Trotter ME: Bursal fat
necrosis as the presenting manifestation of pancreatic dis-
ease: Light and electron microscopic studies. J Rheumatol
12:359-364, 1985
47. White RE, Wise CM, Agudelo CA: Posttraumatic
chylous joint effusion. Arthritis Rheum 28:1303-l 306, 1985





























