Embed Size (px)
Citation preview

Surveillance of bacterial pathogens of diarrhea disease in Indonesia
Buhari A. Oyofoa,*, Murad Lesmanaa,b, Decy Subektia, Periska Tjaniadia, Wita Larasatia,Maidy Putria, Cyrus H. Simanjuntakc, Narain H. Punjabia, Wasis Santosob, Muzahare,
Sukarmaf, Sriwatig, Soritua Sarumpaeth, Mursad Abdii, Ramadhan Tjindij, Hanifah Ma’anik,Atiek Sumardiatil, Hilda Handayanim, James R. Campbella, William K. Alexandera,
H. James Beecham IIIa, Andrew L. Corwina
aU.S. Naval Medical Research Unit No.2, Jakarta, IndonesiabMedical Faculty Trisakti University, Jakarta, Indonesia
cNational Institute of Health Research and Development, Jakarta, IndonesiadPersahabatan Hospital, Jakarta, Indonesia
ePirngadi Hospital, Medan, IndonesiafSanglah Hospital, Denpasar, Bali, Indonesia
gWangaya Hospital, Denpasar, Bali, IndonesiahOtorita Hospital, Batam, Indonesia
iProvincial Health Laboratory, Makassar, IndonesiajLabuan Baji Hospital, Makassar, Indonesia
kM. Jamil Hospital, Padang, IndonesialRegional office of Health Ministry, Pontianak, Indonesia
mProvincial Health Laboratory, Pontianak, Indonesia
Received 10 May 2002; accepted 15 July 2002
Abstract
Emerging or reemerging infections due to bacterial disease may be a local, regional or global problem. Bacterial acute gastroenteritisis a potential cause of substantial morbidity in travelers and deployed U.S. military personnel. A surveillance study was conducted over atwo-year period in Indonesia among 6760 patients with debilitating diarrheal diseases. Of the 6,760 patients, 587 (9%) of the patient stoolswere positive for bacteria. The proportions of bacteria isolated from the 587 patients were:Shigella flexneri (39%),Salmonella spp. (26%),Vibrio spp. (17%),S. sonnei (7%), Campylobacter jejuni (4.4%),Salmonella typhi (3%) andS. dysenteriae (2.3%).Shigella flexneri wasthe most prevalent pathogen isolated, overVibrio spp. No V. cholerae was isolated in the cities of Pontianak, Padang or Batam in Indonesia.Shigella dysenteriae reemergence was noted in Bali, Kalimantan, Batam and Jakarta after an absence of 15 years. Isolation of a highproportion ofS. flexneri, andVibrio spp. occurred during the rainy months. All bacterial isolates were susceptible to quinolones, with theexception ofC. jejuni andSalmonella spp., which were resistant to ciprofloxacin, norfloxacin and nalidixic acid. Our findings highlight thedecline ofV. cholerae, the rise ofS. flexneri and the reemergence ofS. dysenteriae in Indonesia. The study also documents the emergenceof quinolone-resistantCampylobacter spp. in the Indonesia archipelago. © 2002 Elsevier Science Inc. All rights reserved.
1. Introduction
Diarrheal disease has long been a leading cause of mor-bidity and mortality in the developing world. This threatcontinues to pose a major health problem in these areas forresident immunologicly naive children and visitors fromindustrialized nations (Walsh et al., 1979; Synder et al.,
1980; Budiarso et al., 1985). Studies have reported thatbetween 30 and 50% of such visitors to developing regionsdevelop diarrhea (Simanjuntak et al., 1988; Obi et al.,1997). In Indonesia, household surveys reveal that diarrhealdisease is the third leading cause of morbidity, with amorbidity rate of 7.8 per 1,000 populations per year(121,266 people surveyed) (Budiarso et al., 1985). In addi-tion, diarrheal disease in Indonesia is the leading cause ofdeath in infants, causing 24.1% of all infant deaths and 40%of all deaths in the first 2 years of life (Simanjuntak et al.,1998). These figures are likely to be low, as many patients
* Corresponding author. Tel.:�11-6221-421-4457/58; fax:�11-6221-424-4457.
E-mail address: [email protected] (B. A. Oyofo).
www.elsevier.com/locate/diagmicrobioDiagnostic Microbiology and Infectious Disease
44 (2002) 227–234
0732-8893/02/$ – see front matter © 2002 Elsevier Science Inc. All rights reserved.PII: S0732-8893(02)00454-6

do not have access to the limited number of treatmentfacilities that are available, leading to under reporting.
Notable changes in the epidemiology of enteric patho-gens have been documented during the last decades of the20th century, relative to worldwide occurrence. For exam-ple, in more developed (industrialized) regions, S. dysente-riae was first replaced by S. flexneri and then S. sonnei forpredominance among the sub-species (Asheknazi et al.,1993; Lee et al., 1991). In contrast, S. flexneri remains theleading cause of shigellosis in most of the developing world(Keusch et al., 1989; Navia et al., 1999; Simanjuntak et al.,1983).
A prerequisite to the development of an enteric vaccinefor use in Indonesia, is the need to continue to expandepidemiologic and etiologic surveillance of diarrheal dis-ease among residents and travelers in Indonesia. Surveil-lance of enteric pathogens circulating in Indonesia, alongwith prevalence data, will form the basis for a rational,evidence-based approach to effective vaccine developmentfor the region.
Little information exists from Indonesia outside of thecapital city of Jakarta, regarding the emergence or reemer-gence of bacterial pathogens across an expansive archipel-ago consisting of 17,000 islands, and extending over 3,000miles from east to west. Globally, infectious diseases re-main the leading cause of death. In the early 1990s publichealth experts at the U.S. National Academy of Science,Centers for Disease Control (CDC), National Institute ofHealth (NIH) and the World Health Organization (WHO)developed plans for addressing and mitigating the threat ofemerging infections. The U.S. Department of Defense(DoD), owing to its wide-ranging assets for disease control,was prominent in their recommendation to conduct surveil-lance to detect and monitor emerging pathogens, the dis-eases they cause, and the factors influencing their emer-gence. Their recommendations culminated in PresidentialDecision Directives NSTC-7 in June 1996, which formallyexpanded the mission of DoD to support global emerginginfections surveillance (GEIS).
As a result, only bacterial causes of diarrhea were soughtand reported because of the GEIS initiative goals. Thisreport provides a complete, Indonesia-wide geographicalprofile of emerging or reemerging bacterial pathogens as-sociated with diarrheal disease that may have impact uponthe population. The study uses a systematic surveillanceapproach that provides for standardized detailed bacterio-logic examinations to identify the relative importance ofbacterial pathogens in acute diarrheal disease occurrence.
2. Materials and methods
2.1. Subjects and specimen collection
A diarrhea disease surveillance associated with bacterialpathogens only was conducted during the period of January
1999 through December 2000 among 6,760 children andadults seeking treatment for debilitating diarrheal diseases.The study sites included eight hospitals in Medan, NorthSumatra; Padang, West Sumatra; Batam, Riau Islands;Jakarta, Java Island; Denpasar, Bali (two hospitals); Ponti-anak, West Kalimantan and Makassar, South Sulawesi.These hospitals have between 200–300 beds and includeMinistry of Health laboratories where samples were pro-cessed. These communities are densely populated with pop-ulations of 900,000 to 1.5 million. Some of these commu-nities are served by one or two hospitals with at least onehealth center. The participating children and adults live inthe surrounding catchment area. Sanitation is very poor andsewage drains into open gutters next to homes. Regardlessof the age of the patients and the severity of illness (mild,moderate or severe), the participating hospital staff wasinstructed to obtain stool or rectal swab samples from eachdiarrhea patient on the day of admission or presentation,before antibiotic was given.
Diarrhea was defined as three or more loose stools in theprevious 24 to 72 h. Personal data and symptoms of theillness including the type of diarrhea were obtained. Fol-lowing parental informed consent for children and informedconsent for adults, the diarrheic patients were enrolled in thestudy. Specimens were transported to the U.S. Naval Med-ical Research Unit No. 2 (NAMRU-2) laboratory in Cary-Blair (BBL) within 4 h after collection and processed im-mediately. Specimens obtained in the evening or at nightwere kept in the refrigerator at 2–8°C and transported in acool box the following day.
This study was reviewed and approved by theNAMRU-2 Committee for the Protection of Human Sub-jects and by the Indonesian Ministry of Health Research andDevelopment Ethics Committee. Voluntary, written, in-formed consent was obtained from the participants, a parentor guardian (in pediatric cases) of every child, prior toenrollment in this study.
2.2. Laboratory processing
Stools or fecal swabs collected were stored at 2–8°C inCary-Blair media and processed within 4 h of collection.Initial plating for bacterial enteropathogens was performedat each site. Stools were inoculated onto Cary-Blair trans-port media for later transportation by air to NAMRU-2.Fever was defined as body temperature �38°C. Waterystool was defined as stool that takes the form of the con-tainer. Bloody stool was stool containing visible blood. Thetype of stool was observed, and not measured. Fever wasmeasured using a thermometer. Upon arrival at the labora-tory, rectal swabs with samples were inoculated directlyonto MacConkey (MAC) agar, Salmonella-Shigella (SS)agar, Campylobacter blood agar (CAB) and thiosulfate-citrate-bile-sucrose (TCBS) agar. One of the two swabs wasplaced into mannitol selenite enrichment broth (MSB) forSalmonella enrichment and the other one into alkaline pep-
228 B. Oyofo et al. / Diagnostic Microbiology and Infectious Disease 44 (2002) 227–234
tone water (APW) for Vibrio enrichment. Agar plates exceptCAB plates and broth tubes were incubated under aerobicconditions at 37°C for 18–20 h. Campy blood agar plateswere incubated under microaerophilic conditions with oxy-gen concentration reduced to 3–5% using gas pak jar andcampy pak plus at 42°C for 48–72 h. Cultures in MSB wereinoculated onto SS agar and those in APW onto TCBSplates. Plates were incubated at 37°C aerobically for 18–20h. Non-lactose fermenting colonies of Salmonella and Shi-gella grown on MAC and SS agar plates and colonies onTCBS resembling those of Vibrio spp. were selected andtested for their biochemical reactions on Kligler’s iron agar,sucrose semisolid agar and motility-indole-ornithine (Pen-ner et al., 1991; Farmer et al., 1991; Kelly et al., 1991). Noattempt was made to detect E. coli 0157. In a previous studyconducted in our laboratory in Indonesia, which involvedover 4000 stool samples from patients with diarrhea, no E.coli 0157 was detected (unpublished data). We therefore,did not feel there was any benefit in attempting to detect itin the current study. Antimicrobial susceptibility of theisolates was performed by the disk diffusion test of Kirby-Bauer (Bauer et al., 1966) employing ampicillin, tri-
methoprim/sulfamethoxazole, chloramphenicol, tetracy-cline, cephalothin, ceftriaxone, azithromycin, nalidixic acid,norfloxacin and ciprofloxacin.
2.3. Statistics
�2 and Fisher’s exact tests were used to compare differ-ences between the groups. A p-value of �0.005 was con-sidered to be significant.
3. Results
As shown, the proportion of bacterial pathogens isolatedfrom 587 persons were Shigella flexneri (39%), Salmonellaspp. (26%), Vibrio spp. (17%), Shigella sonnei (7%),Campylobacter jejuni (4.4%), S. typhi (3%) and S. dysen-teriae (2.3%) (Table 1). Overall, bacterial isolates identifiedfrom the eight hospital study sites are presented in Table 2.Bacterial pathogens were detected in 587 of 6760 (9%)reported cases of diarrhea. Of the 587 identifiable cases, 222(38%) were from two hospitals located in the tourist area ofBali and 159 (27%) were from Jakarta. There was a signif-icant difference (p � 0.005) between the rate of isolation ofpathogens from the two hospital sites in Jakarta and Bali.The two sites are popular with tourists visiting Indonesia.No V. cholerae was isolated in the cities of Pontianak,Padang and Batam. There was also no V. parahaemolyticusisolated in Padang and Medan. Salmonella typhi was notedto be predominant in Pontianak. Fewer mixed pathogenswere isolated from cases as shown in Table 2.
The age and sex distribution of study subjects with di-arrhea, for all enteric bacterial pathogens, is shown on Table3. More pathogens were isolated from patients �14 yrs of
Table 1Proportional distribution of bacterial pathogens from patients withdiarrhea in Indonesia
Isolate Proportion (%)
Shigella flexneri 39.3%Salmonella spp. 26.0%Vibrio spp. 17.0%Shigella sonnei 7.0%Campylobacter jejuni 4.4%Salmonella typhi 3.0%Shigella dysenteriae 2.3%
Table 2Distribution of bacterial pathogens from patients with diarrhea in Indonesia
No. of positive isolates Sites/no. of specimens tested (%) Total6760
Jakarta794
Bali2713
Makassar984
Pontianak1089
Medan761
Padang162
Batam257
V. cholerae O1 15 (1.9) 8 (0.3) 18 (1.8) 0 3 (0.4) 0 0 44 (0.7)V. cholerae non O1 4 (0.5) 6 (0.2) 2 (0.2) 0 0 0 0 12 (0.2)V. parahaemolyticus 2 (0.3) 30 (1.1) 10 (1.0) 1 (0.1) 0 0 1 (0.4) 44 (0.7)C. jejuni 3 (0.4) 16 (0.6) 3 (0.3) 2 (0.2) 1 (0.1) 0 1 (0.4) 26 (0.4)S. typhi 2 (0.3) 0 3 (0.3) 12 (1.1) 0 0 1 (0.4) 18 (0.3)Salmonella spp. 47 (5.9) 49 (1.8) 13 (1.3) 19 (1.7) 6 (0.8) 2 (1.2) 14 (5.4) 150 (2.2)S. dysenteriae 8 (1.0) 4 (0.2) 0 1 (0.1) 0 0 1 (0.4) 14 (0.2)S. flexneri 67 (8.4) 89 (3.3) 31 (3.2) 29 (2.7) 8 (1.1) 5 (3.1) 2 (0.8) 231 (3.4)S. sonnei 9 (1.1) 18 (0.7) 9 (0.9) 3 (0.3) 0 0 2 (0.8) 41 (0.6)C. jejuni � S. flexneri 0 0 1 (0.1) 0 0 0 0 1 (0.01)C. jejuni � V. cholerae O1 0 1 (0.1) 1 (0.1) 0 0 0 0 2 (0.03)S. dysenteriae � Salmonella sp. 0 1 (0.1) 0 0 0 0 0 1 (0.01)S. sonnei � Salmonella sp. 1 (0.1) 0 0 0 0 0 0 1 (0.01)S. typhi � V. parahaemolyticus 1 (0.1) 0 0 0 0 0 0 1 (0.01)Salmonella sp. � V. cholerae O1 0 0 1 (0.1) 0 0 0 0 1 (0.01)Total 159 (20.0) 222 (8.2) 92 (9.4) 67 (6.2) 18 (2.4) 7 (4.3) 22 (8.6) 587 (8.7)
229B. Oyofo et al. / Diagnostic Microbiology and Infectious Disease 44 (2002) 227–234
age. The numbers of pathogens isolated from the female andmale sexes were almost similar, with values of 302 formales and 284 for females.
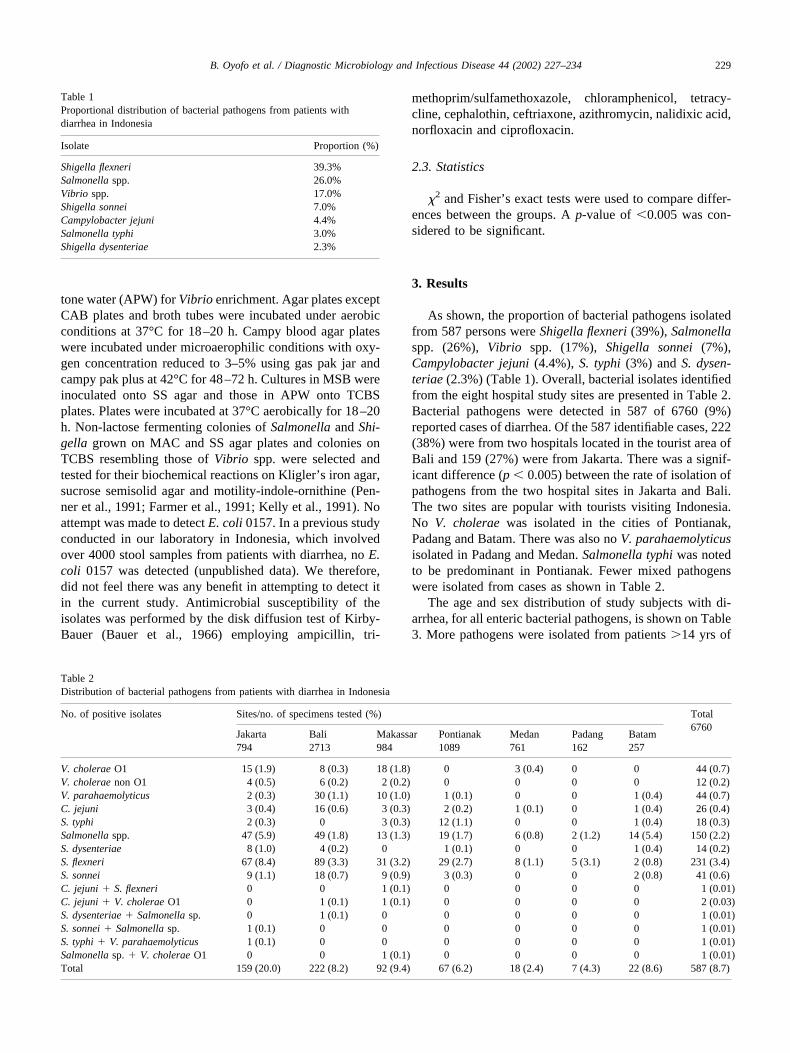
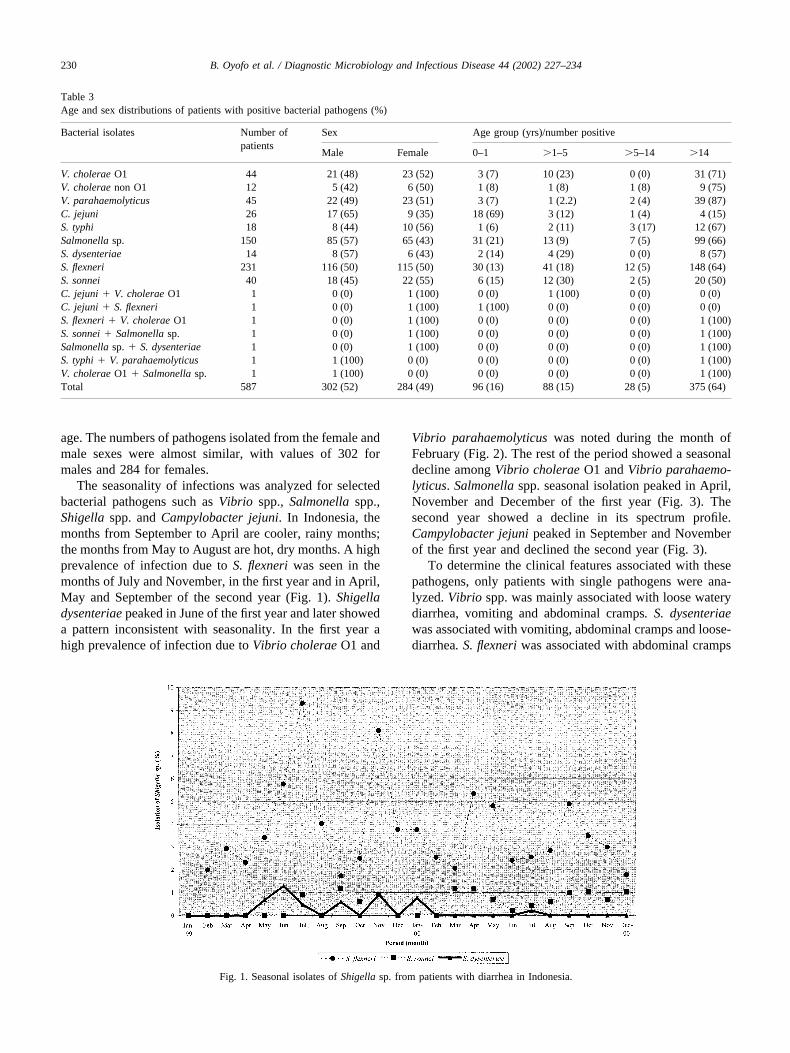
The seasonality of infections was analyzed for selectedbacterial pathogens such as Vibrio spp., Salmonella spp.,Shigella spp. and Campylobacter jejuni. In Indonesia, themonths from September to April are cooler, rainy months;the months from May to August are hot, dry months. A highprevalence of infection due to S. flexneri was seen in themonths of July and November, in the first year and in April,May and September of the second year (Fig. 1). Shigelladysenteriae peaked in June of the first year and later showeda pattern inconsistent with seasonality. In the first year ahigh prevalence of infection due to Vibrio cholerae O1 and
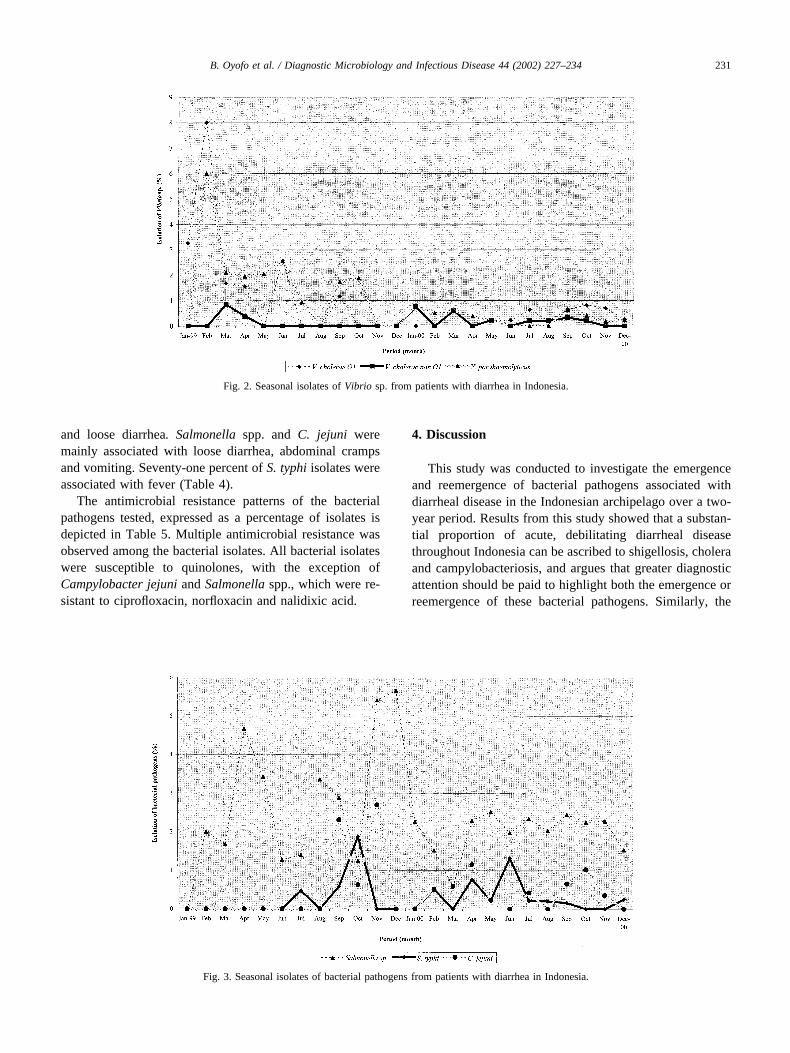
Vibrio parahaemolyticus was noted during the month ofFebruary (Fig. 2). The rest of the period showed a seasonaldecline among Vibrio cholerae O1 and Vibrio parahaemo-lyticus. Salmonella spp. seasonal isolation peaked in April,November and December of the first year (Fig. 3). Thesecond year showed a decline in its spectrum profile.Campylobacter jejuni peaked in September and Novemberof the first year and declined the second year (Fig. 3).
To determine the clinical features associated with thesepathogens, only patients with single pathogens were ana-lyzed. Vibrio spp. was mainly associated with loose waterydiarrhea, vomiting and abdominal cramps. S. dysenteriaewas associated with vomiting, abdominal cramps and loose-diarrhea. S. flexneri was associated with abdominal cramps
Fig. 1. Seasonal isolates of Shigella sp. from patients with diarrhea in Indonesia.
Table 3Age and sex distributions of patients with positive bacterial pathogens (%)
Bacterial isolates Number ofpatients
Sex Age group (yrs)/number positive
Male Female 0–1 �1–5 �5–14 �14
V. cholerae O1 44 21 (48) 23 (52) 3 (7) 10 (23) 0 (0) 31 (71)V. cholerae non O1 12 5 (42) 6 (50) 1 (8) 1 (8) 1 (8) 9 (75)V. parahaemolyticus 45 22 (49) 23 (51) 3 (7) 1 (2.2) 2 (4) 39 (87)C. jejuni 26 17 (65) 9 (35) 18 (69) 3 (12) 1 (4) 4 (15)S. typhi 18 8 (44) 10 (56) 1 (6) 2 (11) 3 (17) 12 (67)Salmonella sp. 150 85 (57) 65 (43) 31 (21) 13 (9) 7 (5) 99 (66)S. dysenteriae 14 8 (57) 6 (43) 2 (14) 4 (29) 0 (0) 8 (57)S. flexneri 231 116 (50) 115 (50) 30 (13) 41 (18) 12 (5) 148 (64)S. sonnei 40 18 (45) 22 (55) 6 (15) 12 (30) 2 (5) 20 (50)C. jejuni � V. cholerae O1 1 0 (0) 1 (100) 0 (0) 1 (100) 0 (0) 0 (0)C. jejuni � S. flexneri 1 0 (0) 1 (100) 1 (100) 0 (0) 0 (0) 0 (0)S. flexneri � V. cholerae O1 1 0 (0) 1 (100) 0 (0) 0 (0) 0 (0) 1 (100)S. sonnei � Salmonella sp. 1 0 (0) 1 (100) 0 (0) 0 (0) 0 (0) 1 (100)Salmonella sp. � S. dysenteriae 1 0 (0) 1 (100) 0 (0) 0 (0) 0 (0) 1 (100)S. typhi � V. parahaemolyticus 1 1 (100) 0 (0) 0 (0) 0 (0) 0 (0) 1 (100)V. cholerae O1 � Salmonella sp. 1 1 (100) 0 (0) 0 (0) 0 (0) 0 (0) 1 (100)Total 587 302 (52) 284 (49) 96 (16) 88 (15) 28 (5) 375 (64)
230 B. Oyofo et al. / Diagnostic Microbiology and Infectious Disease 44 (2002) 227–234
and loose diarrhea. Salmonella spp. and C. jejuni weremainly associated with loose diarrhea, abdominal crampsand vomiting. Seventy-one percent of S. typhi isolates wereassociated with fever (Table 4).
The antimicrobial resistance patterns of the bacterialpathogens tested, expressed as a percentage of isolates isdepicted in Table 5. Multiple antimicrobial resistance wasobserved among the bacterial isolates. All bacterial isolateswere susceptible to quinolones, with the exception ofCampylobacter jejuni and Salmonella spp., which were re-sistant to ciprofloxacin, norfloxacin and nalidixic acid.
4. Discussion
This study was conducted to investigate the emergenceand reemergence of bacterial pathogens associated withdiarrheal disease in the Indonesian archipelago over a two-year period. Results from this study showed that a substan-tial proportion of acute, debilitating diarrheal diseasethroughout Indonesia can be ascribed to shigellosis, choleraand campylobacteriosis, and argues that greater diagnosticattention should be paid to highlight both the emergence orreemergence of these bacterial pathogens. Similarly, the
Fig. 2. Seasonal isolates of Vibrio sp. from patients with diarrhea in Indonesia.
Fig. 3. Seasonal isolates of bacterial pathogens from patients with diarrhea in Indonesia.
231B. Oyofo et al. / Diagnostic Microbiology and Infectious Disease 44 (2002) 227–234
reemergence of S. dysenteriae from various geographicallocations throughout the archipelago confirms the value ofenhancing laboratory detection capabilities, to ensure amore complete and accurate profile of new or previouslyundetected causes of enteric diseases (Subekti et al., 2001).Recognition of emerging and or re-emerging disease patho-gens requires reliable baseline and ongoing surveillancedata. Diarrhea was most often caused by Shigella spp.,followed by Salmonella spp. in this surveillance study. Thefact that S. flexneri was the most predominant pathogenisolated may have been due to the tendency of this organismto cause severe diarrhea, thus making infected individualsmore likely to seek medical attention at a hospital. Otherisolated pathogens of importance were Vibrio spp., C. jejuniand S. typhi. Of noted importance was the prevalence of S.flexneri over V. cholerae in Indonesia. In the past two yearswe have seen a decline in cholera associated diseases, fol-lowed by the emergence or prevalence of S. flexneri over V.cholerae. This sudden change in the prevalence of these twopathogens may be due to the economic or climatic condi-tions in Indonesia that have occurred since the start of thepolitical problems in 1997. The exact reasons for this sud-den shift in the bacterial spectrum profile between Shigellaand Vibrio cholerae is not clear. Vibrio parahaemolyticus,rarely isolated from children under 5 years old (Adkins et
al., 1987), was isolated from four children in the currentstudy. In a previous report, children under 5 years of agewere most often infected with Shigella spp., Campylobacterspp. and Salmonella spp. (Georges et al., 1984). Results ofthis study implicate Shigella spp. as the most frequentlyisolated pathogen associated with diarrhea in Indonesia.Fourteen Shigella dysenteriae isolates were found in thisstudy. The fourteen isolated cases represent the reemer-gence of S. dysenteriae in Indonesia after a hiatus of 15years (Subekti et al., 2001). The reemergence of S. dysen-teriae from several locations in Indonesia is cause for con-cern to public health officials in Indonesia, particularlyconsidering the need to monitor acute, debilitating diarrhealoutbreak disease occurrence. The epidemic potential attrib-uted to S. dysenteriae, as documented in Central America,Asia and Africa, in conjunction with notably high case-fatalities rates, warrants close attention to the re-emergenceof this pathogen in Indonesia (Sack et al., 1997; Malakootiet al., 1997; Mendizabal-Morris et al., 1971). However, in aprevious study conducted in hospitalized patients with di-arrhea in Jakarta, Indonesia, Salmonella spp was found to bethe predominant etiologic agent of diarrhea followed byCampylobacter spp. and Vibrio spp. (Subekti et al., 1993).In another study conducted in North Jakarta-an urban area,Salmonella spp were detected in 3.3% of patients with
Table 4Clinical symptoms associated with patients with diarrhea diseases (%)
Enteropathogens(number of incidences)
% diarrheic patients with following symptoms
Vomit Abdominal cramp Fever Watery Bloody Malaise
Salmonella sp. (149) 74 84 62 94 27 61S. typhi (18) 78 66 71 76 17 50S. flexneri (230) 62 88 67 85 32 62S. sonnei (42) 73 84 71 91 44 58S. dysenteriae (7) 100 100 50 100 0 62Vibrio cholerae O1 (44) 97 82 15 85 0 18Vibrio cholerae non O1 (13) 80 70 11 100 0 33V. parahaemolyticus (45) 92 97 18 98 0 59C. jejuni (25) 76 78 87 100 25 53
Table 5Antimicrobial resistance patterns of bacterial pathogens isolated from patients with diarrhea
Organism/No. of isolates % of isolates resistant toa
Am C Te Sxt Cf Cro Cip Nor Na
S. flexneri (222) 90 78 73 75 0 0 0 0 0V. cholerae O1 (48) 2 2 2 2 0 0 0 0 0V. parahaemolyticus (44) 93 2 0 0 82 0 0 0 0S. sonnei (41) 39 34 80 63 5 0 0 0 0V. cholerae non O1 (10) 30 0 0 10 0 0 0 0 0C. jejuni (24) 55 0 32 77 96 14 32 41 37S. dysenteriae (14) 63 13 52 75 38 0 0 0 0S. typhi (18) 0 0 0 0 0 0 0 0 0Salmonella sp. (140) 20 15 22 9 8 0 2 1 5
a Abbreviations: Am: ampicillin; C: chloramphenicol; Te: tetracycline; Sxt: sulfamethoxazole-trimethoprim; Cf: cephalothin; Cro: ceftriaxone; Cip:ciprofloxacin; Nor: norfloxacin; Na: nalidixic acid.
232 B. Oyofo et al. / Diagnostic Microbiology and Infectious Disease 44 (2002) 227–234

diarrhea followed by V. parahaemolyticus (1.2%), Shigellaspp (0.8%) and V. cholerae (0.4%) (Sutoto et al., 1982).
The prevalence peak for V. cholerae O1 correlated tem-porally with high seasonal rainfall during the month ofMarch. However, isolation rates of Salmonella spp. andShigella spp. correlated with periods of low rainfall.
In the current study, multiple infections were detected invery few patients, although infection with multiple patho-gens has previously been reported (Farugue et al., 1994;Stoll et al., 1982). Infection with multiple pathogens mayreflect spurious environmental contamination, making it dif-ficult to identify the causative agent of diarrhea (Albert etal., 1999). It may also be that multiple pathogens act syn-ergistically to produce diarrhea infections, causing moresuch patients to seek medical treatment.
The role of parasites, enteric viruses, and other unrelateddiarrheal disease pathogens were not explored. This is be-cause the DoD does not consider these pathogens amongthose pathogens most problematic to deployed troops andtravelers. However, the role of nonbacterial pathogens pre-viously has been elucidated in a study conducted in Yogy-akarta, Indonesia (Soenarto et al., 1983). The isolation ratefor bacterial pathogens from the laboratory in Jakarta was20.0%, compared to other isolation rates from samples ob-tained from other cities (range 2.4–9.4). This discrepancymay be due to the problem associated with the transporta-tion of specimens from these remote sites to the laboratoryat NAMRU-2. The minimum flight time between Jakartaand the remote laboratories is about 2–3 h by air. In mostcases, specimens being transported are left unattended bythe courier service company during transport through theairports. As a result, some of the bacteria may no longer beviable when cultured on plates after arrival in the laboratoryat NAMRU-2. The other explanation may be due to the factthat other pathogens such as enteric viruses, parasites werenot sought. These reasons may explain the low rate (9%) ofisolation in this study. But the proportionality of the bacteriaisolated from patients with diarrhea depicts the trend of themost common bacterial isolate associated with diarrhea pa-tients in Indonesia. In a study that was conducted amongpatients with diarrhea in neighboring Singapore reporting tothe National University Hospital for hospitalization, it wasfound that E. coli (ETEC) was the most common pathogenisolated, followed by Salmonella spp. and other bacteria. B.hominis was detected in 4.3% of diarrheal stools and noCryptosporidium was detected (Mendis et al., 1995).
Shifting patterns of antimicrobial drug resistance, partic-ularly in developing countries, are generally a function ofthe overuse and misuse of antibiotic drug therapies. Thespread of drug resistance is the result of poorly regulatedand enforced policies. In Indonesia, the use of fluoroquino-lones such as ciprofloxacin for treatment of patients withdiarrhea is very expensive. Less expensive drugs are thefirst-line drugs of choice for the treatment of diarrhea. Dueto the cost factor, fluoroquinolones are not used for agricul-tural purposes in Indonesia. We strongly believe that resis-
tance due to fluoroquinolones is due to drug misuse fromimportation from neighboring Southeast Asian countries.Multiple antimicrobial resistance was common for mostbacterial pathogens tested, however isolates of S. typhi weresusceptible to all drugs tested. The fact that C. jejuni wasresistant to ciprofloxacin and norfloxacin suggests the emer-gence of quinolone resistant C. jejuni in Indonesia. Shigellaflexneri was resistant to ampicillin, chloramphenicol andtetracycline, while S. sonnei was resistant to sulfamethoza-xole-trimethroprim and tetracycline. This finding may re-flect the possible importation of new drug resistant strains ofthese pathogens from neighboring Southeast Asian coun-tries, although the over-prescribing and inappropriate use ofthese antibiotics is a more likely explanation. Resistance tonalidixic acid (100%) among isolates of S. dysenteriae wasreported in Bangladesh (Albert et al., 1999), however thiswas not evident from the current findings. In a previousreport from Indonesia (Subekti et al., 2001), Shigella flex-neri was found to be resistant to tetracycline (98%), but lessthan 90% resistant to chloramphenicol, trimethroprim-sul-famethoxazole and ampicillin. Previous studies from Ban-gladesh and Tanzania (Sack et al., 1997; Navia et al., 1999)on Shigella spp. showed that almost all of the tested isolateswere resistant to the antibiotics used for diarrhea treatment.Similar antimicrobial resistance profiles for Shigella spp.were reported from Thailand (Moolasart et al., 1994), wherehigh resistance to ampicillin, trimethoprim-sulfamethox-azole, chloramphenicol and tetracycline was documented.
In this surveillance study, bacterial agents were detectedmore frequently among patients older than 14 years thanamong younger patients. However a previous study showedthat in developing countries, the first attack of acute diarrheaoccurred among children ages 0–6 months (Soenarto et al.,1983), initiating a recurring cycle of malnutrition and in-creased susceptibility to enteric infection, which could ul-timately lead to death.
This study was based on the use of a systematic surveil-lance approach that included a standardized detailed bacte-riologic examination, providing an Indonesia-wide geo-graphic profile of emerging or reemerging bacterialpathogens associated with diarrheal disease.
Acknowledgments
We are grateful to Sanhawi Sadeli, Nunung Safari andTaufik Hidayat for laboratory support. We thank the staffmembers of the affiliated Ministry of Health for their indi-vidual role in this study.
Financial support: This work was supported by the NavalMedical Research Command, Silver Spring, MD 20889work unit number: D0016.
The opinions or assertions expressed herein are the pri-vate views of the authors and are not to be construed asrepresenting those of the U.S. Navy, the Department ofDefense or the Indonesian Ministry of Health.
233B. Oyofo et al. / Diagnostic Microbiology and Infectious Disease 44 (2002) 227–234
References
Albert, M. J., Faruque, A. S. G., Sack, R. B., & Mahalanabis, D. (1999).Case-control study of enteropathogens associated with childhood diar-rhea in Dhaka, Bangladesh. Journal of Clinical Microbiology, 37,3458–3464.
Adkins, H. J., Escamilla, J., Santiago, L. T., Ranoa, C., Escheverria, P., &Cross, J. H. (1987). Two-year survey of etiologic agents of diarrhealdisease at San Lazaro hospital, Manila, Republic of the Philippines.Journal of Clinical Microbiology, 25, 1143–1147.
Ashkenazi, S., May-Zahav, M., Dinari, G., Gabbay, U., Zilberberg, R., &Samra, Z. (1993). Recent trends in the epidemiology of Shigella speciesin Israel. Clinical Infectious Diseases, 17, 897–899.
Bauer, A. W., Kirby, W. M., Sherris, J. C., & Hurck, M. (1966). Antibioticsusceptibility testing by a standardized single disk method. AmericanJournal of Clinical Pathology, 45, 493–496.
Budiarso, L. R., Putrali I dan Muchtarudin. (1985). Monograf laporanpenelitan: Survai Kesehatan Rumah Tangga 1980. Badan Penelitiandan Pengembangan Kesehatan Departemen Kesehatan R. I. Jakarta.
Farmer, J. J., III, & Kelly, M. T. (1991). Enterobacteriaceae. In A. Balows,W. J. Hausler Jr., K. L. Herrmann, H. D. Isenberg, & H. J. Shadomy(Eds.), Manual of Clinical Microbiology (5th ed.) (pp. 360–383).Washington, DC: American Society of Microbiology.
Farugue, A. S.G., Mahalanabis, D., Islam, A., & Hoque, S. S. (1994).Severity of cholera due to Vibrio cholerae during concurrent infectionswith other enteric pathogens. Journal of Diarrhoeal Disease Research,12, 214–218.
Georges, Mc, Wachmuth, I. K., Meunier, M. V., Nebout, N., Didier, F.,Siopathis, M. R., & Georges, A. J. (1984). Parasitic, bacterial and viralenteric pathogens associated with diarrhea in Central African Republic.Journal of Clinical Microbiology, 19, 571–575.
Kelly, M. T., Hicman-Brenner, F. W., & Farmer III, J. J. (1991). Vibrio. InA. Balows, W. J. Hausler Jr., K. L. Herrmann, H. D. Isenberg, & H. J.Shadomy (Eds.), Manual of Clinical Microbiology (5th ed.) (pp. 384–395). Washington, DC: American Society for Microbiology.
Keusch, G. T., & Bennish, M. L. (1989). Shigellosis: recent progress,persisting problems and research issues. Pediatric Infectious DiseaseJournal, 8, 713–719.
Lee, L. A., Shapiro, C. N., Hargrett-Bean, N., & Tauxe, R. V. (1991).Hyperendemic shigellosis in the United States: a review of surveillancedata for 1967–1988. Journal of Infectious Diseases, 64, 894–900.
Malakooti, M. A., Alaii, J., Shanks, G. D., & Phillips-Howard, P. A.(1997). Epidemic dysentery in western Kenya. Transactions of RoyalSociety of Tropical Medicine and Hygiene, 91, 541–543.
Mendis, L., Kumarasinghe, G., Chow, C., Liew, H. Y., Ramachandran,N. P., Yayawardane, K., Thong, K. T., Howe, J. L. C., Lim, E. W., &Zaman, V. (1995). Bacteria, Viruses, Yeasts and Protozoans associatedwith diarrheal disease in Singapore. Pathology, 27, 48–52.
Mendizabal-Morris, C. A., Malta, L., Gangarosa, E. J., & Guzman, G.(1971). Epidemic. Shiga-bacillus dysentery in Central America. Deri-vation of the epidemic and its progression in Guatemala, 1968–69.American Journal of Tropical Medicine and Hygiene, 20, 927–933.
Moolasart, P. (1994). Shigellosis in Thai people, Journal of AmericanMedical Association (Southeast Asian) May, 9–10.
Navia, M. M., Capitano, L., Ruiz, J., Vargas, M., Urassa, H., Schellemberg,D., Gascon, J., & Vila, J. (1999). Typing and characterization ofmechanisms of resistance of Shigella spp. isolated from feces of chil-dren under 5 years of age from Ifakara, Tanzania. Journal of ClinicalMicrobiology, 37, 3113–3117.
Obi, C., Coker. A., Epoke, J., & Ndip, R. N. (1997). Enteric bacterialpathogens in stools of residents of urban and rural regions in Nigeria:a comparison of patients with and without diarrhea and controls with-out diarrhea. Journal of Diarrhoeal Disease Research, 15 (4), 241–247.
Penner, J. L. (1991). Campylobacter, Helicobacter and related spiral bac-teria. In A. Balows, W. J. Hausler Jr., K. L. Herrmann, H. D. Isenberg,& H. J. Shadomy (Eds.). Manual of Clinical Microbiology (5th ed.)(pp. 402–409). Washington, DC: American Society for Microbiology.
Sack, R. B., Rahman, M., Yunus, M., & E. H. Khan. (1997). Antimicrobialresistance in organisms causing diarrheal disease. Clinical InfectiousDiseases, 24 (suppl 1), S102–S105.
Simanjuntak, C. H., Hardjining, S., Hasibuan, M. A., Pujarwoto, & Ko-iman, I. (1988). Gastrointestinal Infections in Southeast Asia (V).Technical Meeting of Counterparts on Seamic Data Exchange Programon Infectious Diseases. SEAMIC, Japan.
Simanjuntak, C. H., Hasibuan, M. A., Siregar, L. O., & Koiman, I. (1983).Microbial etiology of acute diarrhea (Indonesian). Health Studies In-donesia, 11 (2), 1–9.
Soenarto, Y., Seobodo, T., Suryantoro, P., Krisnomurti, Haksohusodo, S.,Ilyas, Kusniyo, Ristanto, Romas, M. A., Noerhajati, Siti, M., Rohde,J. E., Ryan, N. J., Luke, R. K. J., Barnes, G. L., & Bishop, R. F. (1983).Bacteria, parasitic agents and rotaviruses associated with acute diarrheain hospital patient Indonesia children. Transactions of Royal Society ofTropical Medicine and Hygiene, 77, 724–730.
Stoll, B. J., Glass, R. I., Huq, M. I., Khan, M. U., Holt, J. E., & Banu, H.(1982). Surveillance of patients attending diarrheal disease hospital inBangladesh. British Medical Journal, 285, 1185–1188.
Subekti, D., Lesmana, M., Komalarini, S., Tjaniadi, P., Burr, D., & Paz-zaglia, G. (1993). Enterotoxigenic Escherichia coli and other causes ofinfectious pediatric diarrheas in Jakarta, Indonesia. Southeast AsianJournal Tropical Medicine Public Health, 24, 420–424.
Subekti, D., Oyofo, B. A., Tjaniadi, P., Corwin, A. L., Larasati, W., Putri,M., Simanjuntak, C. H., Punjabi, N. H., Taslim, J., Setiawan, B.,Djelantik, A. A. G. S., Sriwati, L., Sumardiati, A., Putra, E., Campbell,J. R., & Lesmana, M. (2001). Shigella spp. surveillance in Indonesia:the emergence or reemergence of S. dysenteriae. Emerging InfectiousDisease, 1, 137–140.
Sutoto, Mochtar, M. A., Karyadi, & Wasisto, B. (1982). Morbidity andmortality study on diarrhoeal diseases in North Jakarta—an urban area.Southeast Asian Journal Tropical Medicine Public Health, 13, 405–411.
Synder, J. D., & Merson, M. H. (1980). The magnitude of the problem ofacute diarrheal disease: a review on active surveillance data. BulletinWorld Health Organization, 60, 605–613.
Walsh, J. A., & Warren, K. S. (1979). Selective primary health care. Aninterim strategy for disease control in developing countries. New En-gland Journal of Medicine, 301, 967–974.
234 B. Oyofo et al. / Diagnostic Microbiology and Infectious Disease 44 (2002) 227–234





























