Embed Size (px)
Citation preview

CLIN.CHEM.34/11, 2196-2201 (1988)
2196 CLINICAL CHEMISTRY, Vol. 34, No.11, 1988
Strategyto Diagnose MonoclonalGammopathies in Serum: High-ResolutionElectrophoresis,Immunofixation,and ,cIX QuantificationDavid F. Karen,1 Jeffrey S. Warren,1 and John B. Lowe2
Identificationof monoclonal gammopathies in serum hasinvolvedelectrophoresisof serum proteins, immunoelectro-phoresis (IEP), and quantificationof IgG, lgA, and 1gM.Recent innovationsin technology-including high-resolutionelectrophoresis(HRE), immunofixation(IFX), and quantifica-tion of kappa- and lambda-containingimmunoglobulins-allow for more rapid and precise assessmentof serum formonoclonalproteins.We present a series of guidelinestodeterminewhen high-resolutionelectrophoresisand quantifi-cationof immunoglobulins(includingkappaand lambda) aresufficientand when additionalIFX is requiredto characterizethe monoclonalgammopathy.Of the samples studied,88%were correctly diagnosed by HRE with quantificationofimmunoglobulinsand c/X; only 12% required that IFX beperformed. The guidelines allow us to detect monoclonalgammopathiesquicker and more efficientlyby avoiding re-dundant IEP or IFX testing. For the vast majority of cases,these guidelinesallowfor a correct diagnosiswithinone day.Afterone year of follow-upsincecompletionof the study,noundetectedcases of monoclonalgammopathyhave eventu-ated.
AddItIonalKeyphreses:immunofixation immunoelectrophore-laboratory efficiency . immunoglobulin quantification
index of monoclonality .
Traditional methods to detect serum monoclonal gammo-pathies included electrophoresis of serum proteins on cellu-lose acetate; quantification of IgG, IgA, and 1gM; andimmunoelectrophoresis (IEP).3 Unfortunately, because cel-lulose acetate electrophoresis fails to detect small monoclo-nal proteins and some proteins that migrate in the betaregion (1, 2), IEP and quantification of IgG, IgA, and 1gMwere necessary to screen serum from patients for whom amonoclonal gammopathy was part of their differential diag-nosis. Although this did detect the vast majority of monoclo-nal proteins, the use of IEP in this process was inefficient.Further, it was often difficult to detect monoclonal gainmo-pathies by IEP when only small quantities of the monoclo-nal proteins were present or when 1gM or IgA polymericmonoclonal proteins of larger molecular mass were present(3-5). These larger or self-aggregating proteins often re-quired reduction and repeated examination or chromatogra-
‘Biochemistry Section, Department of Pathology, and 2TheHoward Hughes Medical Institute, The University of Michigan,Ann Arbor, MI 48109.
3Nonstandard abbreviations: IEP, immunoelectrophoresis; HEE,high-resolution electrophoresis; and IFX, immunofixation.
Received May 23, 1988; accepted July 14, 1988.
phy with repeated electrophoresis to detect the monoclonalprotein.
The advent of high-resolution electrophoresis (liRE), im-munofixation (IFX), and quantification of kappa-(K) andlambda-(X)contaunung immunoglobulins facilitated the de-tection of monoclonal proteins. LIRE allows small monocle-nal proteins to be distinguished more readily than is possi-ble with the cellulose acetate method (1, 6). IFX is per-formed more quickly than IEP (in less than one day for somemethods), and detects both small monoclonal proteins andlarge, polymerized monoclonal proteins more readily thanIEP (3, 7-11). Quantification of i- and X-containing immu-noglobuluns provides objective information that can be usedin conjunction with electrophoresis to screen for monoclonalproteins (12-16).
There is considerable controversy as to which combina-tion of these available procedures will provide sensitive andspecific diagnosis of monoclonal gainmopathies and efficien-cies for laboratory utilization. Here, we evaluate a series ofguidelines for combined use of these newer techniques tostreamline and improve the detection and characterizationof monoclonal gammopathies in serum. With this strategy,we detected most monoclonal gammopathies in one day,missed no monoclonal gammopathies, and cut needless IFXor IEP procedures by almost 90%.
Materials and Methods
Specimens
From July 1, 1986, to June 30, 1987, we received 336 seraat the Clinical Immunopathology Laboratory at The Uni-versity of Michigan Hospital to determine whether a mono-clonal gammopathy was present. Control samples consistedof 94 sera obtained from healthy hospital workers, ages 19-58 y.
Strategyfor DetectingMonoclonalGammopathy in Serum
We analyzed each serum by a HIRE in agarose, andquantified the IgO, IgA, 1gM, K, and X by nephelometry. Weused the following criteria to determine whether furtherstudies were needed:
1. If the HRE result was normal, or showed an obviouspattern such as acute phase reaction, nephrotic pattern, etc.(7), and the quantities of immunoglobulins and the ,clX ratiowere normal, we concluded that further studies on theserum for monoclonal protein were not indicated.
2. If the HIRE showed a polyclonal increase in the gamma(y) or beta () and y region with an accompanying increasein one or more of the heavy chain isotypes and a normal c/Xratio, the sample was interpreted as having a polyclonalincrease in the appropriate immunoglobulin type.
1804948
18295 (88%)
3232
4
41(12%)
CLINICAL CHEMISTRY, Vol. 34, No. 11, 1988 2197
3. If the I-IRE revealed an immune complex pattern(“tented restriction in the y region”) with a normal c/X and apolyclonal increase in y globulins, the sample was interpret-ed as showing a tented restriction in y region of the typethat often occurs in patients with circulating immunecomplexes (17, 18).
4. If the HIRE result was normal or showed a polyclonalincrease in y globulins, but the ,c/Xratio was abnormal, weperformed IFX.
5. II the LIRE demonstrated an obvious monoclonal re-striction and one heavy-chain isotype was increased, and the,c/X ratio was abnormal, we concluded that a monoclonalgammopathy was present (type specified) and we recom-mended urine studies to rule out a Bence Jones protein.
6. lithe LIRE demonstrated a monoclonal restriction, butthe K/A ratio was normal, we performed IFX.
7. If our ifies indicated that the patient had a previouslydocumented serum monoclonal protein, we performed LIREwith quantification of the migrating restriction (19). lItherestriction was in the beta region, we quantified the specificisotype of the monoclonal protein by nephelometry to followthe patient’s course. ic/A determinations and IFX were notperformed on these patients unless there was a change inthe migration pattern on HRE.
8. if the patient had hypogammaglobulinemia on LIRE,or on quantification of IgG, we recommended a urine studyto rule out Bence Jones protein.
High-resolidion electrophoresis. For HIRE we used thePanagel (Worthington Diagnostics, Freehold, NJ) agarosesystem, applying 5-uL samples of a fourfold-diluted serumto the application mask. After allowing this to absorb intothe gel for 7 mm, we placed the cooling block on the gel andapplied current (200 V, 90-240 mA) across the gel for 40mm. Barbital-sodium barbital buffer, pH 8.6, was used. Wefixed the gels with picric acid (1.5 g in 120 mL of diluteacetic acid, 170 mLIL) for 10 mm, followed by two 3-mmwashes in dilute (50 mJJL) acetic acid solution. Afterpressing and drying the gels, we stained them for 10 mmwith Amido Black, 1 g/L in dilute acetic acid. Gels weredestained in three successive rinses (1 mm, 10 mm, and 10mm) with a mixture of glacial acetic acid, methanol, anddistilled water, 1/3/7 by vol. The gels were dried and scannedwith a densitometer (“Appraise”; Beckman Instruments,Brea, CA) (19).
Immunofixation. This was done as described in detailpreviously (7). Briefly, we adjusted the concentration of theserum samples so the concentration of the protein of interestwas -1 g/L (based on the nephelometric results), andsubmitted samples to agarose electrophoresis as above. Foreach immunoglobulin to be assayed-typically, IgG, IgA,1gM, K, and A-we applied a separate sample of appropriate-ly diluted patient’s serum to the gel. IgD or IgE was alsooccasionally quantified. After electrophoresis, we overlaidthe samples with a strip of cellulose acetate containing 50L of specific antiserum (Kallestad Labs., Austin, TX).After 60 mm, we washed the gels with buffer and stainedthem with Coomassie Blue, 50 g/L, in ethanol/glacial aceticacid/water (4.1/1/4.5 by vol). After destaining as describedabove, we dried the gels and examined them for specificrestriction as described previously (7).
Nephelometry. IgG, IgA, 1gM, K, and A were quantifiedwith the Auto ICS (Beckman) system as described previous-ly (19). Antisera specific for IgG, IgA, and 1gM (Beckman)and for K- and A-containing immunoglobulins (Kallestad)were reacted with appropriate dilution of the patients’ sera.
This nephelometer is programmed to make specific dilutions
of the serum sample.
Results
Concentrations of serum immunoglobulins in the controlpopulation. The normal ranges for IgG, IgA, 1gM, K, and Aconcentrations in our control population were similar tothose described by others (12,20,21). The single most usefulvariable for determining monoclonality was the average idAratio, 1.91 (SD 0.36). The ratios we measured ranged from1.15 to 3.43. Results for six of the 94 samples fell outside ofmean ± 2 SD range, as would be expected statistically.
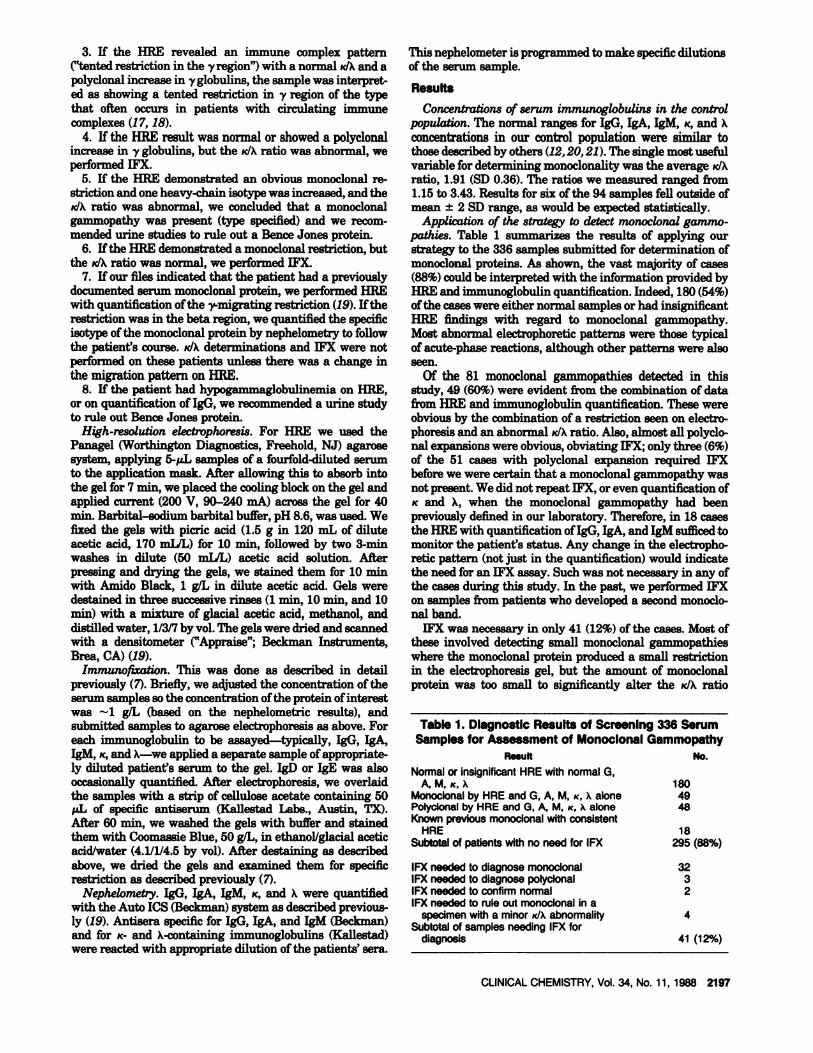
Application of the strategy to detect monoclonal gammo-pathies. Table 1 summarizes the results of applying ourstrategy to the 336 samples submitted for determination ofmonoclonal proteins. As shown, the vast majority of cases(88%) could be interpreted with the information provided byHIRE and immunoglobulin quantification. Indeed, 180(54%)of the cases were either normal samples or had insignificantLIRE findings with regard to monoclonal gammopathy.Most abnormal electrophoretic patterns were those typicalof acute-phase reactions, although other patterns were alsoseen.
Of the 81 monoclonal ganunopathies detected in thisstudy, 49(60%) were evident from the combination of datafrom LIRE and immunoglobulin quantification. These wereobvious by the combination of a restriction seen on electro-phoresis and an abnormal idA ratio. Also, almost all polyclo-nal expansions were obvious, obviating IFX; only three (6%)of the 51 cases with polyclonal expansion required IFXbefore we were certain that a monoclonal gammopathy wasnot present. We did not repeat IFX, or even quantification ofK and A, when the monoclonal gammopathy had beenpreviously defined in our laboratory. Therefore, in 18 casesthe HIRE with quantification of IgG, IgA, and 1gM sufficed tomonitor the patient’s status. Any change in the electropho-retic pattern (not just in the quantification) would indicatethe need for an IFX assay. Such was not necessary in any ofthe cases during this study. In the past, we performed IFXon samples from patients who developed a second monocle-nal band.
IFX was necessary in only 41 (12%) of the cases. Most ofthese involved detecting small monoclonal gainmopathieswhere the monoclonal protein produced a small restrictionin the electrophoresis gel, but the amount of monoclonalprotein was too small to significantly alter the K/A ratio
Table 1. DiagnostIc Results of ScreenIng 336 SerumSamples for Assessment of Monoclonal Gammopathy
Result No.
Normalor insignificantHRE withnormalG,A, M, K, K
Monoclonalby HRE and G, A, M, ic, K alonePolyclonal by HRE and G, A, M, .c, K aloneKnownpreviousmonoclonalwithconsistent
HRESubtotalof patientswithno need for IFX
IFX needed to diagnosemonoclonalIFX needed to diagnosepolyclonalIFX needed to confirmnormalIFX needed to ruleout monoclonalin a
specimenwitha minor idA abnormalitySubtotalof samplesneedingIFX for
diagnosis

Table 2. Monoclonal Gammopathles Detected by Abnormal ic/A wIth Obscure or No Monoclonai BandsSeen by HRE
Concentratlon,g/L
Diagnosis Appearance In electrophoresis IFXb ic/A lgG gA gM
CLL Faint mid-y band K 0.25 2.74 .50 .59MGUSC Weak band at origin IgGK 1.10 8.30 .94 1.74CLLSNeuropathyMGUSC
Small fast y bandNone. HypogammaglobulinemiaNone. Hidden behind transferrin
lgMKigMKIgAX
0.800.401.18
6.421.115.16
1.480.292.16
5.021.711.81
MGUSC None. Hidden behind C3 IgAX 0.60 8.77 8.76 0.65Neuropathy Faint slow y band IgGK 1.00 4.88 0.19 0.72Myoloma Faint, broad slow p band igGic 3.30 4.61 1.56 0.26MGUSC Weak broad p band IgAic 2.74 10.01 6.78 1.27Myeloma Broad mid-y band IgDic 2.70 11.88 1.49 0.89
CU_ chronic lymphocytic leukemia.bMj gammopathydetected by IFX.CMGUS,monoclonalgammopathyof undeterminedsignificance.
2198 CLINICALCHEMISTRY, Vol. 34, No. 11, 1988
(Figure 1). A few cases involved ruling out monoclonalitywhen there were small K/A alterations but no restrictionswere seen by electrophoresis. There were also two normaland three polyclonal samples.
Whereas the utility of K/A to facilitate the diagnosis incases with large monoclonal gammopathies is obvious, theliterature is less clear as to whether determining K/Aoffersuseful information in samples when only minor or noalterations are seen on electrophoresis of serum proteins. Inthe present series, we identified 10 patients with monocle-nal gammopathies who had either no or minor alterationsby serum protein electrophoresis but who had an abnormalK/A ratio (Table 2). In these cases, the abnormal idA ratiowas a major factor in deciding to perform the IFX, whichconfirmed the presence of a monoclonal gammopathy. Onlythree of these samples had monoclonal proteins that werenot seen on initial examination of the gel. One, from apatient with neuropathy associated from an 1gM monoclonalprotein, showed only hypogammaglobulin and an abnormalic/A on our screening. Both of the others were from patientswith p-migrating IgA monoclonal gammopathies, whichwere obscured by transferrin and C3 (Figure 2). Two of the10 samples were from patients with multiple myeloma: anewly diagnosed patient with rare IgDic gammopathy,whose serum displayed a broad y band on electrophoresis,
N
UM 20BEA
aF
M
o toN0CL0NAL
<.25O.0.5O.72 t 1.2S t.51.Th 2 2.2.52.72 a a.asa.ea.ie
WXBYNEPEHLOMETRY
FIg. 1. Histogram for kappallarnbda ratiosThe ic/K ratio of the monoclonalgammcpathiesthat requiredIFX for diagnosiswere inor near the normal range
and a patient with treated IgGK myeloma, in whose serumhypogammaglobulinemia was evident, but with a veryfaint, broad, slow (3band that could be mistaken for residualfibrinogen (Figure 3). The remaining five samples also hadweak bands, which, by our strategy, would require IFX evenif the K/Aratio had been normal. However, the K/Aresultswere useful because some of these bands might have beenmissed by less-experienced observors.
Monoclonal gammopathies detected. There was little dif-ference in the ability to detect a monoclonal protein of anyparticular isotype by these methods. Of considerable inter-est was the ability of the methods to detect monoclonalgammopathies in specific clinical situations. In Table 3, wereview the clinical diagnoses of the patients with monocle-nal gammopathies newly detected by our laboratory duringthis study (some were known monoclonal gammopathiesdetected in outside laboratories, but were not on ifie in ourlaboratory). All four cases of WaldenstrOm’s macroglobulin-emma and 14 (87.5%) cases of myeloma were correctlyidentified by electrophoresis with quantification of iinmuno-globulins and ic/A. Only two cases of myeloma required IFX.One of these was previously detected at another institution.As expected, most cases (58%) were monoclonal gammo-pathies of undetermined significance. Several cases withsmall monoclonal proteins were associated with neuropathy.Other cases included chronic lymphocytic leukemia andlymphoma, detection of which usually required IFX. Casesof plasmacytoma and amyloidosis were detected by LIREand idA ratio alone.
With 12 months of follow-up since completion of the studygroup, no then-undetected monoclonal gammopathies havebeen found. We recognize that it may take several years forsmall monoclonal proteins to evolve into full-blown clinicaldisease, but patients who had sufficient symptoms to initiatea request for monoclonal gammopathy evaluation shouldhave shown evidence of progression in this time if themonoclonal process was responsible for their symptoms.
DiscussIon
In the present study we applied a strategy to screen forand characterize monoclonal gammopathies in all serumsamples that were sent to the laboratory for evaluation of apossible monoclonal gammopathy. Previously, each samplewould have been analyzed by electrophoresis on celluloseacetate; quantification of IgG, IgA, and 1gM; and IEP. Thelatter evaluation took a minimum of three days and occa-sionally as long as a week when reduction by 2-mercapto-

Fig. 2. Monoclonal proteinsobscured by transfernn and C3Left:The p fracirshowsa large y restriction,whichwas readilydiagnosedas an tgGicgammopathybyHREandquantificationof 19G.lgA, 1gM.sc and K. The secondbadcshowsa slightlymoredensetransfernnbandwith a faintcathodaltail(arrow).An IgAXmonoclorialgammopathywas detectedat thetransform position.The thirdand fourth backsarefrom a normalserum and our freeze-dried control(C3 hasdeterioratedto C3c). respectively.Right: The top track showsa polyclonalincreasein yglobulin. The second track has increaseda-i. a-2, andC3 bands.As,IFX was performed because of anabnormalpc/Kand an elevatedlgk This revealedthe I9AKmonoclonalgammopathyat theC3 position.Thesamplesin tracks 3 and4 werea normalserumand our freeze-driedcontrol,respectively
i_i..Ti ‘!‘
rFIg. 3. Samplewithmonocionalprotein not seen on initial examinationThe kp Mu ttadcs containour freeze-riled controlsample.The U*d track has aprofounddecreasein -,globulinand a veryfaint,broadband(anuv. just cathodelto C3. Becauseof the abnormalsc/Aan IFX was performed,which revealedtheIgGicmonoclonalproteinat this site
CLINICALCHEMISTRY,Vol. 34, No. 11, 1988 2199
ethanol or column-chromatographic purification was re-quired for us to characterize the monoclonal proteins. Whenusing this older strategy, we observed that most of thesamples turned out to be normal, or that many weremonoclonal proteins that we had already characterized (22).Furthermore, most of the clinically significant monoclonalgainmopathies (those that were useful in defining lympho-reticular proliferations or amyloid) were obvious on cellu-lose acetate electrophoresis. However, the combination ofcellulose acetate electrophoresis and quantification of IgG,IgA, and 1gM was ineffective for screening samples, becausethese procedures were not sufficiently sensitive to detectsmall monoclonal gammopathies.
By combining LIRE with quantification of ic and A, wewere able to effectively screen serum samples for the pres-ence of monoclonal gammopathies. The essence of thisstrategy is to perform IFX on any sample that has abnor-malities suggesting a monoclonal process, as detailed in theMethods section. Further, we stress to new users of this
strategy that they should perform IFX whenever they areuncertain about a diagnosis. We found that, with increasedexperience, the number of redundant IFX declined consider-ably. With this strategy, we eliminated 88% of unnecessaryIFX, and our reports on most patients who have monoclonalgammopathies are available the same day that the sampleis drawn. This hastens the diagnostic process and alsoresults in a net saving of the time for the skilled medicaltechnologists.
The few samples that did require IFX were typicallysmall monoclonal gainmopathies, most of which fell into thecategory of monoclonal gammopathy of undetermined sig-nificance. Samples from two patients with multiple myelo-ma required IFX for diagnosis. One had been receivingtreatment at another institution, the other had an IgDicmonoclonal protein. Neither had been evaluated previouslyin our laboratory. A few of the samples requiring IFX werefrom patients with chronic lymphocytic leukemia or lym-phoma. Earlier studies indicated that the incidence ofmonoclonal proteins in patients with these conditions wassmall (23), but more recent work indicates that the vast
Table 3. ClInical DIagnoses of MonoclonalGammopathies
MG(.JSMyelomaWaldenstrOm’sNeuropathy associated
with monoclonal proteinChronic lymphocytic
leukemiaLymphomaPlasmacytomaAmloldosisTotal
Total idA ,b
47 26(55%) 21 (45%)16 14(87.5%) 2(12.5%)4 4(100%) 08 3(37.5%) 5(62.5%)
3 1(33%) 2(66%)
1 0 11 1 01 1 0
81 50(62%) 31 (38%)
Cases detected bythe high resolutionscreen with quantificationof serumimmunoglobulins.
b8 requiringIFX todetect the monoclonalprotein.All were detectedbythe screen, but requIredIFX forcharacterization.

2200 CLINICALCHEMISTRY, Vol.34, No. 11, 1988
majority of these patients will have such proteins in theirserum or urine (11, 24). Optimal detection requires IFX,isoelectric focusing, or affinity chromatography (11,24-26).The most common histopathological pattern is a diffuselymphoma of small lymphocytes, with or without plasmacy-toid differentiation (27). Interestingly, while one might haveassumed that these patients would have 1gM as the predom-inant immunoglobulin type, a recent study by Noel andKyle (24) indicates that IgG was present in 51% while 1gMwas found in only 38% of the patients. Some monoclonalsdetected from about 2% of patients with lymphoma wereshown to possess cold agglutinin activity (28). Monoclonalgammopathies were also reported in patients with smallnoncleaved follicular center cell lymphomas (8,29). The onecase of biclonal gainmopathy in the present series alsorequired IFX for characterization. The need for IFX in suchcases was noted previously (16,30). Biclonal gammopathieswere reported recently in several cases of non-Hodgkin’slymphoma and leukemia (30-33). It is likely that theincreased numbers of these cases reported recently reflectsthe greater sensitivity of lIRE and IFX.
A few recent studies explored the possibility of using icand K quantification to replace the standard methods ofserum protein electrophoresis and JEP. Predictably, largemonoclonal proteins were virtually always detected andsmaller monoclonals were often missed (21). This strategyalso yields significant numbers of false positives for mono-clonal gammopathies (21). Clearly, icand A without electro-phoresis and IFX or LEP as backups are inadequate as ascreen. In the present study, cases with polyclonal increasesas well as cases with hypogammaglobulinemia had occa-sional ic/A outside of the normal range. With IFX, it wasobvious that these cases did not represent monoclonalgammopathies. However, when used with LIRE, and whenviewed in the context of the strategy described in this paper,scand Aquantification provides the information one needs toanalyze correctly the vast majority of the serum samplessubmitted.
Normal values for K and A in some laboratories will differfrom manufacturer’s recommendations. Normansell (12)found the mean ic/A ratio to be 1.77, with a standarddeviation of 0.337. This is similar to our ic/A of 1.91 andstandard deviation of 0.360. Theoretically, the total of K + Ashould equal IgG + IgA + 1gM. In fact, these do not add upperfectly, because of the heterogeneity of both reagentantisera and of the antigens in this system (12, 13, 34).Another interesting feature reported by Normansell wasthat for 47% of pediatric sera the heavy/light chain ratio wasoutside of the normal range. Other workers (20), however,have found the mean ic/Aratio for children to be the same asthat for adults (1.81, SD 0.4). Our laboratory does notroutinely quantifr ic/Aor do IFX on pediatric sera. We foundthat most clinicians order IEP on children as part of anevaluation for immunodeficiency. While one can find tinymonoclonal proteins in the serum of children with Burkitt’slymphoma, this is clearly not the way to screen for thatdiagnosis (8).
In the present study, the key to being able to screen formonoclonal proteins is the combination of the sensitivity ofLIRE with ic/A and judicious use of IFX to answer specificquestions. The method for HRE used in this study allows fordensitometric scanning, which can be useful as an adjunctin interpretation (2, 7, 19). IFX is an especially goodtechnique to detect the small monoclonal proteins thatcannot be readily distinguished with HRE and ic/A alone.
However, it is important to dilute each sample according tothe amount of serum immunoglobulin present individually.When standard dilutions are used, antigen-excess effectscan result in a false-negative result (7, 35, 36).
Methods for detecting monoclonal gammopathies willcontinue to improve. Several methods to improve sensitivityinclude isoelectric focusing, Western blotting, and two-dimensional electrophoresis. Whether such methods will beclinically useful and practical for diagnostic laboratoriesremains to be determined. The present study presents astrategy that allows for the rapid, accurate diagnosis ofmonoclonal gammopathies by screening the serum withHRE and quantification of IgG, IgA, and 1gM, and ic and A.When necessary (see Methods), IFX is performed to be surethat small monoclonal proteins are not missed. With thestrategy outlined in this study, JFX was necessary only 12%of the time. Considering that we are a large referralhospital, we anticipate that the percentage of samplesrequiring IFX would be smaller in the average communityhospital or in a large commercial laboratory.
References1. Howerton DA, Check U, Hunter RL. Densitometric quantitationof high resolution agarose gel protein electrophoresis. Am J ClinPathol 1986;85:213-8.2. Dennis PM, Biegler B, Papas R. Improved measurement ofmonoclonal paraproteins in serum using agaroae gel electrophore-sis. Ann Chem Biochem 1987;24:73-6.3. Chu SY, MacLeod JE, Bocci L, Monteith M. Characterization ofsmall monoclonal protein bands with Beckman’s “Paragon”iinmunoflxation system [Tech Brief]. Clin Chem 1987;33:617.4. Normansell DE. Comparison of five methods for the analysis ofthe light chain type of monoclonal serum 1gM proteins. Am J ClinPathol 1985;84:469-75.5. Lane JR. Bowlea KJ, Normansell DE. Detection of 1gM monoclo-nal proteins in serum enhanced by removal of IgG. Lab Med1985;16:676-8.6. Crawford J, Eye MK, Cohen HJ. Evaluation of monoclonalgammopathies in the “well” elderly. Am J Med 1987;82:39-45.7. Keren DF. High-resolution electrophoresis and immunofixation:techniques and interpretation. Boston and London: Butterworths,1987.
8. Braunstein All, Keren DF. Monoclonal gaminopathy (IgMic) in apatient with Burkitt’s lyniphoma. Arch Pathol Lab Med1983;107:235-8.9. Sun T, Lien YY, Degnan T. Study of gammopathies withinununofixation electrophoresis. Am J Clin Pathol 1979;72:5-ll.10. Gerard SK, Chen KH, Khayain-Bashi H. linmunofixationcompared with immunoelectrophoresis for the routine characteriza-tion of paraprotein disorders. Am J Clin Pathol 1987;88:198-203.11. Deegan MJ, Abraham JP, Sawdyk M, Van Slyck EJ. Highincidence of monoclonal proteins in the serum and urine of chroniclymphocytic leukemia patients. Blood1984;64:1207-11.12. Normansell DE. Use of kappa and lambda chain quantitationfor the detection of isnmunoglobulin abnormalities in serum. DiagnClin Immunol 1987;5:100-3.13. Rees J, Ohrmundt J. The usefulness of quantiiring kappa andlambda light chains [Tech Brief]. Clin Chem 1986;32:899.
14. Wallage MJ, Whicher JT. “Quantimetric” kappa:lanibda ratiotest [Letter]. Clin Chem 1987;33:448.
15. Whicher JT, Wallage M, Fifield R. Use of irnrnunoglobulinheavy- and light-chain measurements compared with existingtechniques as a means of typing monoclonal immunoglobulins. ClinChem 1987;33:1771-3.16. Schultz AL, Fink LM. What is the most efficient way toevaluate iznmunoglobulins? Clin Chem 1986;32:391-2.17. Kelly RH, Scholl MA, Harvey S, Devenyi AG. Qualitativetesting for circulating immune complexes by use of zone electropho-

CLINICALCHEMISTRY, Vol.34, No. 11, 1988 2201
resis on agarose. Chin Chem 1980;26:396-402.18. Levinson SS, Keren DF, Carey JC, Goldman JO. Identificationof circulating immune complexes (CIC) by high resolution electro-phoresis [Abstract]. Clin Chem 1987;33:904.19. Keren DF, DiSante AC, Bordine SL Densitometric scanning ofhigh resolution electrophoresis of serum: methodology and clinicalapplication. Am J Chin Pathol 1986;85:348-52.
20. Renckens ALJM, Jansen MJH, van Munster PJJ, WeemaesCMR, Bakkeren JAJM. Nephelometry of the kappa/lambda lightchain ratio in serum of normal and diseased children. Clin Chem1986;32:2147-9.21. Guinan JEC, Kenny DF, Gatenby PA. Detection and typing ofserum paraproteins with the quantimetric kappa:lambda ratio test[Tech Brief]. Clin Chem 1986;32:1981-2.22. Rao KMK, Bordine SL, Keren DF. Decision making by patholo-gists. A strategy for curtailing the number of inappropriate tests.Arch Pathol Lab Med 1982;106:55-6.23. Reed M, McKenna RW, Bridges R, Parkin J, Frizzera G,Brunning RD. Morphologic manifestations of monoclonal gammo-pathies. Am J Chin Pathol 1981;76:8-23.24. Noel P, Kyle BA. Monoclonal proteins in chronic lympocyticleukemia. Am J Clin Pathol 1987;87:385-8.25. Sinclair D, Dagg JH, Mowatt AMcI, Parrott DMV, Stott DI.Serum paraproteins in chronic lyznphocytic leukaemia. J ClinPathol 1984;37:463-6.26. Qian GX, Fu SM, Solanki DL, Rai KR. Circulating monoclonal1gMproteins in B cell chronic lymphocytic leukemia: their identifi-cation, characterization and relationship to membrane IgM. J
Immunol 1984;133:3396-400.27. Alexanian R. Monoclonal gammopathy in lymphoma. ArchIntern Med 1975;135:62-6.28. Sandhaus LM, Raska K, Vai Wu H. Diffuse large cell lympho-ma with monoclonal IgMic and cold agglutinin. Am J Clin Pathol1986;86:120-3.29. Magrath I, Benjamin D, Papadopoulous N. Serum monoclonal#{252}nmunoglobulinbands in undifferentiated lymphomas of Burkittand non-Burkitt types. Blood 1983;61:726-31.30. Guarner J, Austin GE, Nassar VII, Sarma RP, Boedecker E.Biclonal gammopathy (IgGic and IgGA) in a patient with non-Hodgkin’s lymphoma. Arch Pathol Lab Med 1986;1lO:445-8.3L Graziani MS, Lippi U. Multiple myeloma with serum 1gMkappa and Bence Jones lambda biclonal gammopathy. Clin Chem1986;32:2220-1.32. Finco B, Schiavon R. Multiple myeloma with serum IgO kappaand Bence Jones lambda biclonal gammopathy [Letter]. Clin Chem1987;33:1305-6.33 Grau E, SolerJ, PuigJ, et al. Coincident multiple myeloma andnon-Hodgkin’s lymphoma with 2 serum monoclonal immunoglob-ulins. Acta Haematol 1986;75:183-5.34. Silverman GJ, Carson DA, Solomon A, Fong S. Human kappalight chain subgroup analysis with synthetic peptide-induced anti-sera. J Immunol Methods 1986;95:249-57.35. BaarsJD, Lombarts AJPF. Imprecision of protein electrophore-sis [Letter]. Clin Chem 1986;32:1425-6.36. Ooi DS, Perkins SL. Immunofixation electrophoresis with useof Beckman Paragon SPE gels [Letter]. Clin Chem 1986;32:1979.





























