Embed Size (px)
Citation preview
Social and Situational Factors Associated With Contraceptive Switching: Implications for Practitioners1
JAMES JACCARD~ DONALD W. HELBIG University at Albany
State University of New York Health Science Center at Brooklyn
State University of New York
TIMOTHY B. GAGE AND CHOI K. WAN University at Albany
State University of New York
DONNA C. KRITZ-SILVERSTEIN MARJORIE A. GUTMAN University of California, San Diego Robert Wood Johnson Foundation
New York. New York
This study was an investigation of contraceptive switching in the context of a 5-wave panel design of diaphragm and pill users from the New York City metropolitan area. The respondents were 525 women between the ages of 14 and 46, who came to one of 10 family planning clinics to obtain birth control, Results indicated a hazard function for switching in which the hazard rate increased in the initial weeks and then gradually declined over time. Clinic experiences on the part of the women were found to alter survivorship trends. Implications of the data for service providers were developed.
The topic of contraceptive continuity (or its counterpart, switching from one birth control method to another) has received considerable attention in the social science literature. To date, the majority of empirical studies have docu- mented continuity rates for different birth control methods and identified demographic correlates of these rates. In contrast the present study is con- cerned with identifying social psychological factors that influence switching behavior between contraceptive methods. We begin by reviewing general trends in the literature on switching. We then discuss the practical importance of studying switching from a social psychological perspective. We next report data from a large scale longitudinal survey in the New York City metropolitan
'We would like to thank William Grady for his comments on a previous draft of this manuscript. The research was supported by NICHD grant HD031208 from the Demographic and Behavioral Science Branch of the Center for Population.
*Correspondence concerning this article should be addressed to James Jaccard, Department of Psychology, SUNY-Albany, Albany, NY 12222.
1765
Journal of Applied Social Psychology, 1995, 25, 20, pp. 1765-1789. Copyright 0 1995 by V. H. Winston & Son, Inc. All rights reserved.
1766 JACCARD ET AL.
area which provide insights into variables that may mediate switching behavior with respect to use of the diaphragm and use of birth control pills. Finally, we discuss the practical implications of our results.
General Trends in the Literature
Contraceptive continuation has been defined in various ways. Some studies examine continuation of (or switching from) a particular method, while other studies investigate continuation of any or all contraception. We characterize here the literature on contraceptive switching vis-a-vis a particular method and omit studies on general contraceptive continuation. We also exclude research on continuation-discontinuation due to pregnancy occurrence or due to a change in the individual’s desire to become pregnant.
Early studies of method continuation tended to include only married women and most focused on only one or two methods (most prominently the IUD and the pill). For example, early studies in the U.S. and Great Britain found the following approximate continuation rates for oral contraceptives: After 6 months of use, approximately 75% of the women were still using the pill; at 12 months, approximately 69%; and at 18 months, approximately 60% (Studies in Family Planning, 1967). Life table curves suggested that more users discon- tinue in the early months of use, with continuation rates stabilizing after approximately 6 months. More recent studies on married women in the United States have utilized data from Cycles I and I1 of the National Survey of Family Growth from 1973 and 1976 (e.g., Grady, Hirsch, Keen, & Vaughn, 1983; Hammerslough, 1984). Overall, the IUD, the pill, and the rhythm method have the highest continuation rates at 1 year; diaphragm, condom, and “other” being intermediate; and spermicides having the lowest rate (Grady et al., 1983). Grady and his associates (Grady, Hayward, Billy, & Florey, 1989; Grady, Hayward, & Florey, 1988) have examined trends in contraceptive switching in a national sample of married women between the ages of25 and 44 in 1982 and have found similar relative discontinuation rates among methods. Over a 3-year observation period, discontinuation rates were as follows: 16.4% for the rhythm, 21.4% for the IUD, 25.7% for the pill, 28.6% for the condom, 29.5% for the diaphragm, and 45.4% for spermicides.
Another group of studies reports on pill continuation among family plan- ning clinic users. These studies tend to focus on abortion patients, adolescents, and/or clinic discontinuers. Rates for pill continuation have been approximately 80% at 6 months, 65-76% at 1 year, and 52% at 18 months (e.g., Ager, Shea, & Agronow, 1982; Cosgrove, Penn, & Chambers, 1978; Margolis, Rindfuss, Coghlan, & Rochat, 1974; Reichelt, 1978; Siegel, Thomas, Coulter, Tuthill, & Chipman, 1971).
Research on what methods individuals switch to when they change a
CONTRACEPTIVE SWITCHING 1767
method is limited. The few studies that have been conducted tend to be descriptive and/or to utilize qualitative data (e.g., Cosgrove et al., 1978; Gorosh, 1982; Margolis et al., 1974; Miller, 1976). Most of the studies also focus on adolescents (e.g., Foreit & Foreit, 1978; Gorosh, 1982; Hirsch & Zelnik, 1985; Miller, 1976; Reichelt 1978; Zelnik & Kantner, 1981). Some studies focus on the first method switch ever (Gorosh, 1982; Hirsch & Zelnik, 1989, while others examine method switches later in a woman’s contraceptive career (e.g., Cosgrove et al., 1978; Trussell & Westoff, 1980). One commonal- ity is that studies tend to examine method switching either in terms of level of effectiveness (Foreit & Foreit 1978; Gorosh, 1982; Margolis et al., 1974; Trussell & Westoff, 1980) or medical/nonmedical criteria (Hirsch & Zelnick, 1985). Classifying methods by “medical/nonmedical” is similar to classifying them by level of effectiveness because almost all medical methods (with the exception of the diaphragm) are more effective than all nonmedical methods. Overall, the results of the studies are best summarized in three areas: after first method, after adoption at a family planning clinic, and after an abortion.
The first method ever used tends to be the condom or withdrawal and, to a lesser extent, birth-control pills (e.g., Zelnik & Kantner, 1979). The majority of women do not switch methods by the end of the first sexual relationship (Foreit & Foreit, 1978). However, when the first switch does occur, it tends to be from a nonmedical, less effective method to a medical and more effective one (Foreit & Foreit, 1978; Hirsch & Zelnik, 1985). Among family planning clinic users, estimates of clients still using a highly effective method at follow- up vary considerably from study to study, such as 8 1% in one study (Cosgrove et al., 1978) to 50% in another (Ager et al., 1982). For more effective methods, a higher percentage of switches tend to occur in clients who initially used a coital dependent method than among women who obtained noncoital depend- ent methods (Cosgrove et al., 1978). Users of coitally related methods tended to switch to birth control pills, while users of the IUD and the pill tended to switch between these methods. Post-abortion, 25% of the women who accepted contraceptives switched during the first 6 months (Margolis et al., 1974). Twenty-two percent of the pill adopters discontinued use, and 13% of the pill adopters were not using any kind of contraception.
Overall, these findings suggest that a fairly typical sequence among women is that their first contraceptive method is a nonmedical and often less effective one. Then they switch to a medical and more effective method as their sexual careers progress, specifically when they have intercourse more frequently and regularly and have a steadier, more involved relationship.
Early studies that attempted to identify demographic correlates of method continuation tended to find significant education effects for pill continuation rates (Studies in Family Planning, 1967). Some studies also report parity and
1768 JACCARD ET AL.
age effects, whereas other studies find no such effects. A substantial portion of early oral contraceptive dropouts appear to be due to physical side effects.
Studies of American women tend to support the relevance of certain demo- graphic variables for method continuation. Age, race, and socioeconomic status have been major correlates for individual methods considered separately, as well as for all methods combined (Hammerslough, 1984). Parity, religion, and education level also have been included in multivariate models (e.g., Hammerslough, 1984). In recent analyses of a national sample of married women reported by Grady et al. (1988), numerous demographic correlates of method switching were examined. Only race was predictive of switching: Black women had a lower risk of changing methods than did White women. Grady et al. (1989) conducted more extensive analyses of racial differences in switching behavior. They found that Black women, as compared to White women, were more likely to abandon all methods of birth control and were less likely to adopt sterilization after initial use of other contraceptives.
Exploration of social psychological correlates of general method continu- ation has tended to use clinic samples. Situational variables that have been related to continuation in one or more studies include coital frequency, marital status, the number of children living with the woman, the number of women living in the household, having one working parent currently being in school or working, stability of family of origin, partner’s attitude toward contracep- tion, a steady sexual relationship, information from friends, and clinic follow- up calls (e.g., Furstenburg, Shea, Allison, Herceg-Baron, & Webb, 1983; Margolis et al., 1974; Porter, 1984; Siegel et al., 1971). Perception ofthe method, expected parity, and risk-taking orientation are attitudinal variables that have been found to be associated with method continuation (Furstenberg et al., 1983; Porter, 1984). An interaction of menstrual side effects experienced and expec- tations and attitudes concerning those side effects was significantly related to pill and IUD continuation (Zetina-Lozano, 1983). Experience of physical side effects was generally the most frequently noted reason for discontinuing birth control pills, especially in the early months of use (e.g., Ager et al., 1982; Jones, Beniger, & Westoff, 1980; Margolis et al., 1974; Porter, 1984; Siegel et al., 1971; Studies in Family Planning, 1967; Zetina-Lozano, 1983). For example, 42% of adolescents who discontinued birth control pills by 18 months after the first clinic visit cited experience of side effects as the main reason (Ager et al., 1982). Another 17% of these discontinuers reported fear of side effects as their main reason.
Less frequent sexual activity is also a frequently cited reason for pill discontinuation, but only among adolescents. Anywhere from 21% to 37.5% of adolescent clinic attendees reported this as their main reason (Ager et al., 1982; Reichelt, 1978). Other reasons reported for discontinuing pill use were related

CONTRACEPTIVE SWITCHING 1769
to access, cost social influence from mother andor partner, forgetting to take pills, medical treatment requiring discontinuation, and sterilization.
Social-Psychological Analyses of Switching Behavior
Ideally, when a woman chooses a birth-control method as her major method of contraception, she will do so in a fully informed fashion. She will be aware of the various birth-control methods that are available and will chose one that best meets her needs, given her life circumstances. She will be aware of the difficulties and hazards in using the method, and will select a method that is compatible with her current sex life and social and economic constraints. The goal of the family planning professional should be to assist the woman in making a fully informed decision. Once a method has been selected, unforeseen events can occur which render the method unsuitable for the woman. For example, she may experience physical side effects that are intolerable; or aspects of her sex life might change so that the method is no longer appropriate (e.g., the frequency of sexual intercourse may change or her sexual partner may change). To the extent that switching is a function of such unforeseen events, there is little that the family planning professional could have done to “match” the client with a more suitable method (given that the client was well informed about potential side effects). However, switching may also occur for reasons that do not reflect accommodations to a changing environment or to a changing physical condition. Rather, it may be the result of the woman’s failure to adequately appraise and take into account her social context (e.g., partner resistance to the method), her economic status (e.g., the method might be too expensive for the woman), andor her knowledge of what method use entails relative to other methods when the decision about a contraceptive method is made. If such factors underlie switching behavior, then it may be possible to develop counseling and clinic policies that can minimize unnecessary switch- ing between contraceptive methods. The present study was designed to gain perspectives on the prevalence and importance of such factors with respect to the diaphragm and birth control pills.
General Analytic Strategy
Our approach involved first identifying women who attended family planning clinics for purposes of obtaininghsing birth-control pills or the diaphragm. Over the course of the next 16 months, we identified women who switched from the pill (or the diaphragm) and, through open-ended questions, made preliminary determinations of their reasons for switching. All women who identified side effects or medical reasons as the primary reason for a switch were segregated (analytically) from the rest of the sample using stand- ard survival analysis. For women who reported switching for reasons other than
1770 JACCARD ET AL.
side effects, there are at least two possible models that can characterize their hazard function. If these women have not made well-informed decisions in which they have carefully considered partner reactions, the difficulty of method use, and other method and social factors, then there should be a higher probability of switching during the initial stages of use (after a “break-in” period when the method is initially tried by all women). In this scenario, the woman’s expectations do not match with “reality” and when she discovers, for example, that the method is more difficult to use than she thought it would be, she will switch to another method. These mismatches with expectations are likely to occur just after initial use of the method, as compared with later time periods when the woman has become more experienced with the method. Thus, the predicted hazard function is one that initially increases with time and then decreases. In contrast if switching is primarily due to situational and life changes (e.g., partner changes, changes in frequency of sex), then such events should be as likely to occur early in the use cycle as opposed to later in the use cycle (or, if anything, later in the cycle). These “random events” would yield a constant hazard function across time, a distribution that is distinct from that predicted by “mismatched expectations.” The present investigation examined these two different models of contraceptive switching for women whose switching is not side-effect mediated.
We also examined the relationship between switching and several specific social psychological variables to gain additional perspectives on the contracep- tive decision-making process. Although we believe that mismatched expecta- tions are important in switching behavior, it is possible that some women will be more persistent in staying with a method than are others. Stated another way, we believe that there are variables that may make women more tolerant of negative information acquired through use and which will therefore be predic- tive of the tendency to switch methods. We now describe a set of social psychological variables that may be predictive of switching:
1. Initial attitude towards the method. Women have beliefs about the advantages and disadvantages of a given birth control method (pill or diaphragm). The totality of these beliefs is psychologically summarized in the individual’s attitude toward the method. Consistent with Fishbein (1972; Fishbein & Ajzen, 1975), an attitude is defined as the extent to which someone feels favorable or unfavorable toward using the method. In general, a positive attitude usually indicates that the person associates method use with positive consequences and outcomes, whereas a negative attitude indicates that the person associates method use with negative consequences and outcomes (Jaccard, 198 1). Even among women who decide to use a specific method, there will be variability in attitudes (e.g., some women use the pill despite reservations about doing so). It was predicted that women who initially had more positive attitudes about the
CONTRACEPTIVE SWITCHING 1771
pill or diaphragm would be more tolerant of subsequent negative experiences with a method and hence would be less likely to switch from that method at a later time.
2. Partner’s attitude toward the method. We hypothesized that the more negative a woman perceived her main sexual partner to be toward the method, the higher should be the probability that the woman would switch from that method.
3 . General knowledge of contraceptives. Women who know a great deal about birth control in general should be more aware of the advantages and disadvantages of the various methods and, therefore, make a more informed choice. This, in turn, should reduce subsequent switching behavior.
4. Method-specific knowledge. Women who know a great deal about the pill (diaphragm) in particular should also have a greater appreciation for the advantages and disadvantages of the piWdiaphragm before choosing to use it. This, in turn, should lead to a lower incidence of switching.
5 . Clinic experience. Women have different experiences with the clinic staff in terms of how helpful and supportive they perceive the staff as being. It was predicted that the more helphl/supportive the staff was perceived as being, the lower would be the probability of a subsequent method switch.
6. Religious beliefs. It was predicted that women who felt that using the pill is morally questionable should be more likely to switch. Although this variable should be most relevant to pill switching, it also may be indirectly related to diaphragm switching. If a woman believes that the pill is morally unacceptable, then this eliminates this method from the birth-control options that are avail- able to her. With fewer choice alternatives, a diaphragm user may be more likely to remain on the diaphragm rather than switch to another method (such as the pill). Thus, this variable should be negatively associated with switching from the diaphragm.
7. Importance of sexual pleasure. It was hypothesized that for diaphragm users, the more important sexual pleasure is to the woman, the more likely she would be to switch from the diaphragm. This variable also may be predictive of pill switching indirectly, based on the “reduced number of options” logic described above.
8. Reservations about genital contact. It was hypothesized that the more reservations a woman had about touching herself in the genital area, the more likely she would be to switch from the diaphragm. This variable also may be predictive of pill switching indirectly, based on the reduced number of options logic.
There have been numerous analyses of contraceptive switching behavior. Most studies have focused on specifying method discontinuation rates in general and demographic correlates of these rates. There have been relatively
1772 JACCARD ET AL.
few studies that have explored social psychological correlates of switching behavior. None have explicitly considered the problem of switching from the perspective of mismatched expectations and the potential to reduce unneces- sary switching through better family planning counseling. The present study examined switching behavior for a sample of family planning clinic users in a major metropolitan area (New York City) with a primary focus on women who switch from the pill or diaphragm for reasons other than side effects. We first examined hazard functions and self reports of reasons for switching to deter- mine if there is evidence for mismatched expectations. We then explored social psychological correlates of switching behavior for women who switch for nonside-effect based reasons.
Method
Respondents and Design
The women in the study were participants in a larger investigation of contraceptive behavior called the Components of Effective Fertility Regulation (CEFR) study (Helbig, Gutman, & Kritz-Silverstein, 1987). The CEFR study was a five-wave panel design of diaphragm and pill users from the New York City metropolitan area The respondents were women between the ages of 14 and 46, who came to one of 10 family planning clinics to obtain birth control. The sample for the CEFR study consisted of 1,303 women who came to the clinics to obtain either birth control pills or a diaphragm. To be included in the present analysis, women had to be starting for the first time or restarting the use of either oral contraceptives or the diaphragm. Restarters were defined as women who, at enrollment, had used the method (pilVdiaphragm) at some time in their contraceptive history, had stopped using it, and were now starting to use it again. The data for the present analysis were based on interviews conducted at an enrollment period (when respondents agreed to be in the study) and four follow-up periods, each separated by approximately 4 months. There were 201 diaphragm users and 324 pill users in our analysis who met the above criteria and for whom complete data were available. The sample consisted of 36% Catholics, 35% Protestants, 13% other religions, and 16% women who claimed no religious affiliation. Fifty percent of the sample were White, 41 '3'0 were Black, and 9% were Hispanic. Approximately 13% of the sample were currently married. Fifty-six percent were between the ages of 2 1 and 30, 26% were less than 21, and 17% were over 30. Approximately 58% of the sample had less than a 12th-grade education.
Interviews were conducted on a one-to-one basis. Respondents were ap- proached in the clinic by a study staff member and administered a short screening interview. Eligible respondents were then invited to participate in a
CONTRACEPTIVE SWITCHING 1773
more intensive interview. Most of the instruments used in the present research were in the form of questionnaires that were self-administered. In cases where the individual’s reading ability was inadequate, the questionnaire was read to the respondent who completed her answers on a separate questionnaire, hidden from the view of the interviewer. Each interview lasted approximately 2 hr. All measures of social psychological variables described here were ascertained at enrollment.
Measures
Contraceptive use. Contraceptive history over the course of the study was measured using a continuous calendar form, covering each week of study participation. The interviewer began a follow-up interview with a general open-ended question regarding what had happened in the respondent’s life since her last interview. The interviewer then focused on specific questions about changes in such variables as work, school, and relationships, referring to a “personal profile” which highlighted a number of key characteristics re- corded at the previous interview. This was done to orient the respondent to the relevant time period. The interviewer then confirmed the respondents last contraceptive status as recorded at the previous interview. She asked how long that status had continued, as well as other general questions about the birth- control method used. The interviewer then worked forward from the previous interview and identified the week when a method change occurred (including a shift to no method), if it did. The process continued until the current week of the interview was reached. The result was a week-by-week record of method uselswitching, using no more than a 4-month retrospective account that was linked to significant events.
Attitude toward method. Consistent with Fishbein (1972) and other theo- rists (e.g.. Jaccard & Becker, 1985), an attitude is defined as the extent to which the individual feels positive or negative about an attitude object. In the present case, the attitudes are concerned with general objects; namely, using the contraceptive method in question (i.e., the pill or the diaphragm). The attitude toward using the person’s current contraceptive method was measured using a Likert scaling approach with 24 items. Each item represented a belief statement that was rated on a 5-point scale ranging from 1 (strongly disagree) to 5 (strongZy agree; e.g., “Using the diaphragm would be ‘simple”’). Positive items were scored from 1 (strongly disagree) to 5 (strongly agree), while negative items were reverse scored. Thus, scores could range from 24 to 120, with higher scores indicating a more positive attitude.
The belief statements were generated based on categories defined in six studies of contraceptive attitudes (Beckman & Hauser, 1979; Cohen, Severy, & Ahtola, 1978; Davidson & Jaccard, 1975, 1979; Jaccard & Davidson, 1972;
1774 JACCARD ET AL.
Luker, 1975). The content validity of the items was further ensured via consult- ation with experts on sexual and fertility-regulation behavior. Pretests revealed that the scales had excellent test-retest reliabilities (e.g., above .80). Item homogeneity was ensured by means of evaluating item-total correlations. Initially, 32 items for each scale were considered as possible candidates. However, only those with large item-total correlations (greater than .40) were retained.
Partner measures. The perception of the partner’s attitude was measured on a 5-point agree-disagree scale in response to three statements: “Using dia- phragdpill would please my main partner”; “Using diaphragm/pill would bother my main partner”; and “My partner is very much against the contracep- tive method I am using now (or am about to start using).” Before they were summed, these three items were first coded so that higher numbers indicate a more positive attitude. Thus the scores could range from 3 to 15.
Knowledge measures. Two knowledge measures were obtained. The first was a specific measure of knowledge that assessed knowledge about the birth-control method in question. The items used a multiple choice format. An example item for the diaphragm is as follows: “In order for a diaphragm to work best to keep a woman from getting pregnant, it should always be used with . . . .” The response alternatives were (a) a condom, (b) contraceptive cream or jelly, (c) a douche right after having sex, and (d) Vaseline. A “specific knowledge” score was obtained by scoring the response as correct or incorrect and then summing the number of correct responses across the items.
The second knowledge measure assessed contraceptive knowledge in four general domains; knowledge of reproductive anatomy and physiology, general knowledge about contraception, knowledge about the relative effectiveness of methods, and knowledge about how to use specific methods (other than the pill or diaphragm, as appropriate). The items had the same multiple choice format as described above. There was a total of 25 items. Each item was scored as correct or incorrect and then summed across the 25 items.
Clinic experience. The reaction toward the clinic experience was measured on a 5-point agree-disagree scale in response to the following three statements: “The person or persons who talked with you in the clinic today about birth control were polite to you”; “The person or persons who talked with you in the clinic today about birth control were not very helpful”; and “The person or persons who spoke with you in the clinic today about birth control seemed to understand your wishes and fears.” These three items were coded so that lower scores represented a negative clinic experience and higher scores represented a positive experience.
Consistency with moral religious beliefs. The extent to which using the method was perceived as being inconsistent with one’s religion was measured
CONTRACEPTIVE SWITCHING 1775
on a 5-point agree-disagree scale in response to the statement “Using the pill would be against my religious or moral beliefs.” Responses were coded such that higher scores indicated that using contraceptives was more against her moraVreligious beliefs.
Importance of sexual pleasure. Respondents indicated how important sex- ual pleasure was to them using a 5-point rating scale ranging from 1 (relatively less importance) to 5 (relatively more importance).
Self-touching. The attitude toward touching one’s genital areas when using a contraceptive was measured using a single item indicating how negative this would be. The responses could range from 1 to 5, with lower scores indicating a more positive response.
Open-ended questions. If a woman indicated a method switch at any time during her calendar, she was asked an open-ended question: “What were the reasons you stopped using (method)?” All responses were recorded verbatim. Responses were content analyzed by independent coders. If the respondent indicated side effects as a reason, she was also asked to describe the side effects that she experienced.
Results
Bias Analyses
Analyses for three types of bias were performed. The first was selection bias in which demographic characteristics of respondents who were enrolled in the CEFR study as a whole were compared with those of eligible women who were not enrolled in the study. The second type of bias was retention bias, to determine if there were any significant differences between respondents who remained in the study and those who dropped out of the study. Finally, the possibility of testing bias was assessed to determine if there were significant differences between respondents who had been repeatedly exposed to follow- up interviews assessing contraceptive use versus respondents who were only reinterviewed 16 months after they had enrolled in the study.
Selection bias. A total of 1,303 women initially were enrolled in the CEFR study. An additional 2,22 1 women were identified in the participating clinics as eligible for the study, but chose not to participate. All potential respondents, whether they were later enrolled or not enrolled, were asked to complete a form assessing the following demographic characteristics: age, race, educational level, marital status, contraceptive method, contraceptive status (starting/ restarting/continuing), duration of continuous contraceptive use (if the respon- dent was a continuer), number of contraceptive methods used previously, number of previous pregnancies, and number of previous abortions. The
1776 JACCARD ET AL.
enrolled and nonenrolled respondents were compared on the categorical vari- ables with chi-square analyses and on the continuous variables with t tests. Significant differences were only found for 2 of the 10 variables. First there was a significant difference between the enrolled and the nonenrolled respon- dents for ethnic group, x2(df = 3) = 15.01, p < .01, such that more White respondents but fewer Hispanic respondents than expected were enrolled. Although statistically significant the effect size of the comparison (based on Cramer’s V) was trivial (less than 1%). The enrolled respondents were also found to have previously used a greater number of contraceptive methods than were the nonenrolled respondents (Ms = 1.84 and 1.68, respectively), t(3497) =
3 . 7 2 , ~ < .05, q2 = .004. However, the proportion of explained variance for this variable also was less than 1%. Thus, although minor selection biases were operating, the magnitude of the biases was small enough that they should not affect seriously the generalizability of our analyses.
Retention bias. Retention bias was evaluated by comparing respondents who completed each follow-up with those who dropped out at that follow-up or previously. Respondents who dropped out and respondents who were re- tained in the study were compared using chi-square analyses and t tests on the following characteristics: contraceptive method obtained at enrollment, con- traceptive status at enrollment (starting, restarting, or continuing), race, age, marital status, religion, religiosity, involvement in work and school, educa- tional level, percentage poverty level of household, number of pregnancies prior to enrollment, number of abortions prior to enrollment number of contra- ceptive methods used prior to enrollment, proportion of coital acts during the year prior to enrollment at which contraception was used, age at initiation of intercourse, age at initiation of contraception, interval between initiation of intercourse and first use of contraception, first method of contraception used, and last method of contraception used. The comparisons revealed one signifi- cant difference on education level (at Follow-up 2). As before, the effect size was trivial in magnitude (less than 1% explained variance), suggesting that retention biases were minimal.
Retesting bias. In order to evaluate the extent to which repeatedly inter- viewing respondents would affect their later contraceptive use andor unin- tended pregnancies, a subsample of the original respondents were “set aside” after enrollment (N = 122). These women were only reinterviewed once, at the end of 16 months. In contrast the remainder of the original respondents were interviewed every 4 months over the same 16 month period. Our major interest was with whether repeated testing might influence attitudes or use of contra- ceptives. There was no evidence for this, as there were no significant differ- ences between the reinterviewed and the set-aside respondents in mean levels of attitudes or various contraceptive use measures.
CONTRACEPTIVE SWITCHING 1777
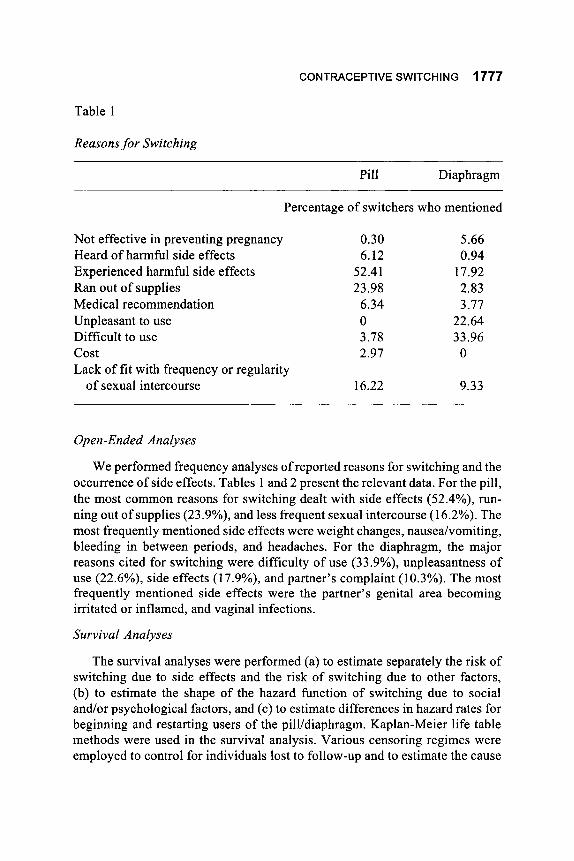
Table 1
Reasons for Switching
Pill Diaphragm
Not effective in preventing pregnancy Heard of harmful side effects Experienced harmful side effects Ran out of supplies Medical recommendation Unpleasant to use Difficult to use cost Lack of fit with frequency or regularity
of sexual intercourse
Percentage of switchers who mentioned
0.30 6.12
52.41 23.98
6.34 0 3.78 2.97
16.22
5.66 0.94
17.92 2.83 3.77
22.64 33.96 0
9.33
Open-Ended Analyses
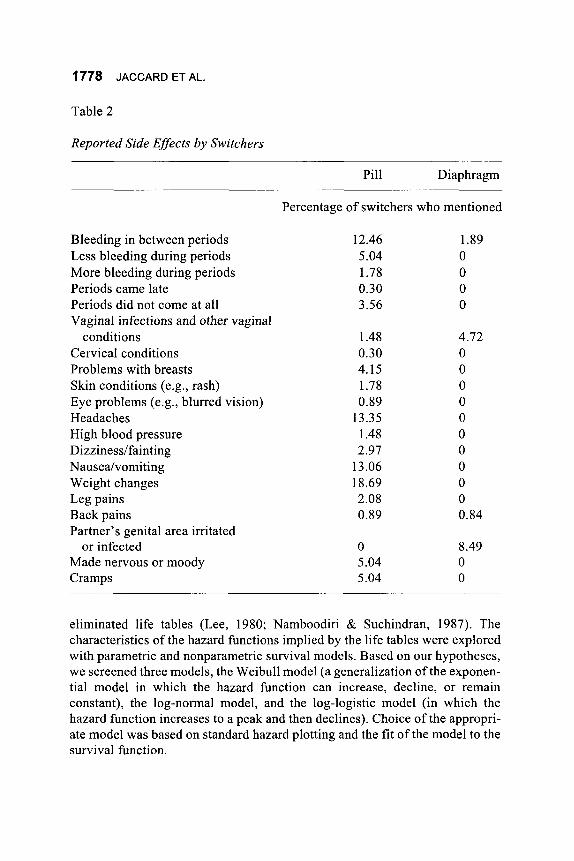
We performed frequency analyses of reported reasons for switching and the occurrence of side effects. Tables 1 and 2 present the relevant data. For the pill, the most common reasons for switching dealt with side effects (52.4%), run- ning out of supplies (23.9%), and less frequent sexual intercourse (16.2%). The most frequently mentioned side effects were weight changes, nausealvomiting, bleeding in between periods, and headaches. For the diaphragm, the major reasons cited for switching were difficulty of use (33.9%), unpleasantness of use (22.6%), side effects (17.9%), and partner’s complaint (10.3%). The most frequently mentioned side effects were the partner’s genital area becoming irritated or inflamed, and vaginal infections.
Survival Analyses
The survival analyses were performed (a) to estimate separately the risk of switching due to side effects and the risk of switching due to other factors, (b) to estimate the shape of the hazard function of switching due to social andlor psychological factors, and (c) to estimate differences in hazard rates for beginning and restarting users of the pill/diaphragm. Kaplan-Meier life table methods were used in the survival analysis. Various censoring regimes were employed to control for individuals lost to follow-up and to estimate the cause
1778 JACCARD ET AL.
Table 2
Reported Side Effects by Switchers
Pill Diaphragm
Percentage of switchers who mentioned
Bleeding in between periods Less bleeding during periods More bleeding during periods Periods came late Periods did not come at all Vaginal infections and other vaginal
Cervical conditions Problems with breasts Skin conditions (e.g., rash) Eye problems (e.g., blurred vision) Headaches High blood pressure Dizzinedfainting Nauseahomiting Weight changes Leg pains Back pains Partner’s genital area irritated
Made nervous or moody Cramps
conditions
or infected
12.46 5.04 1.78 0.30 3.56
1.48 0.30 4.15 1.78 0.89
13.35 1.48 2.97
13.06 18.69 2.08 0.89
0 5.04 5.04
1.89 0 0 0 0
4.72 0 0 0 0 0 0 0 0 0 0 0.84
8.49 0 0
eliminated life tables (Lee, 1980; Namboodiri & Suchindran, 1987). The characteristics of the hazard functions implied by the life tables were explored with parametric and nonparametric survival models. Based on our hypotheses, we screened three models, the Weibull model (a generalization of the exponen- tial model in which the hazard function can increase, decline, or remain constant), the log-normal model, and the log-logistic model (in which the hazard function increases to a peak and then declines). Choice of the appropri- ate model was based on standard hazard plotting and the fit of the model to the survival function.
CONTRACEPTIVE SWITCHING 1779
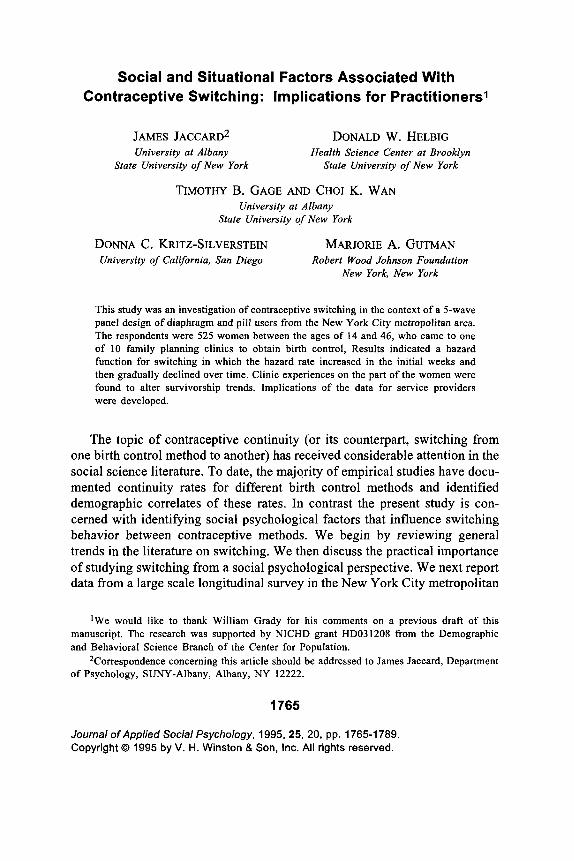
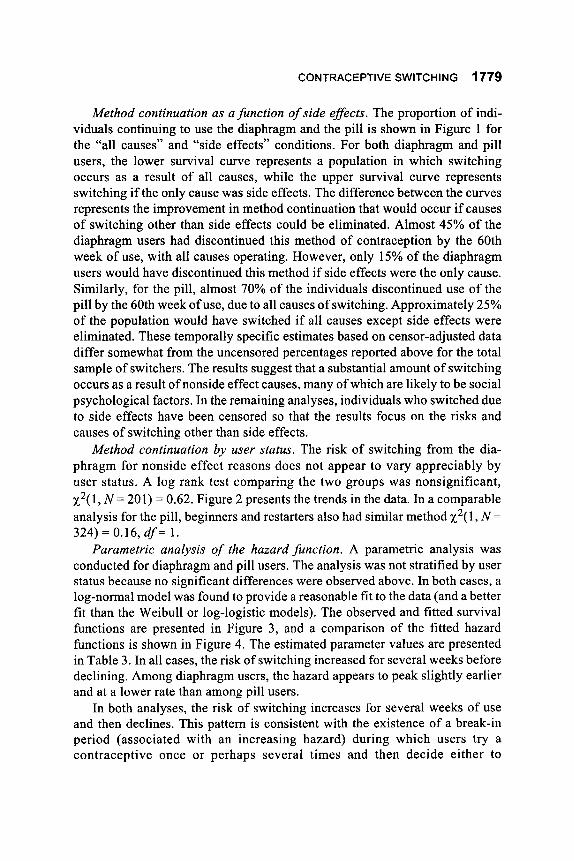
Method continuation as a function of side effects. The proportion of indi- viduals continuing to use the diaphragm and the pill is shown in Figure 1 for the “all causes” and “side effects” conditions. For both diaphragm and pill users, the lower survival curve represents a population in which switching occurs as a result of all causes, while the upper survival curve represents switching if the only cause was side effects. The difference between the curves represents the improvement in method continuation that would occur if causes of switching other than side effects could be eliminated. Almost 45% of the diaphragm users had discontinued this method of contraception by the 60th week of use, with all causes operating. However, only 15% of the diaphragm users would have discontinued this method if side effects were the only cause. Similarly, for the pill, almost 70% of the individuals discontinued use of the pill by the 60th week of use, due to all causes of switching. Approximately 25% of the population would have switched if all causes except side effects were eliminated. These temporally specific estimates based on censor-adjusted data differ somewhat from the uncensored percentages reported above for the total sample of switchers. The results suggest that a substantial amount of switching occurs as a result of nonside effect causes, many of which are likely to be social psychological factors. In the remaining analyses, individuals who switched due to side effects have been censored so that the results focus on the risks and causes of switching other than side effects.
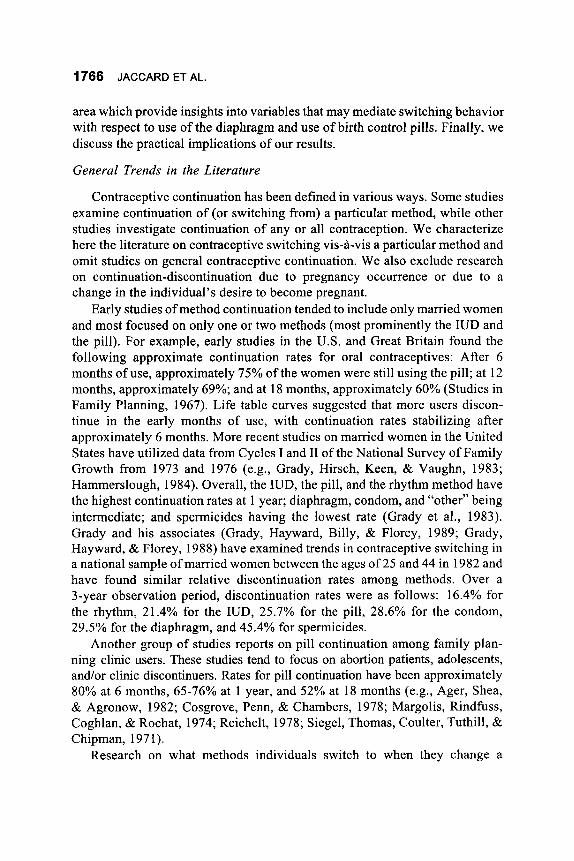
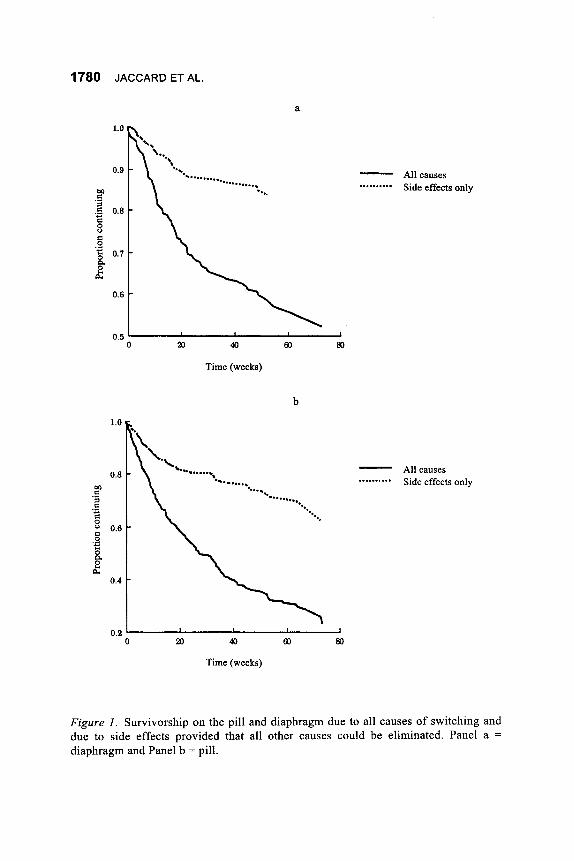
Method continuation by user status. The risk of switching from the dia- phragm for nonside effect reasons does not appear to vary appreciably by user status. A log rank test comparing the two groups was nonsignificant, ~ ~ ( 1 , N = 201) = 0.62. Figure 2 presents the trends in the data. In a comparable analysis for the pill, beginners and restarters also had similar method x2( 1, N =
324) = 0.16, df= 1. Parametric analysis of the hazard function. A parametric analysis was
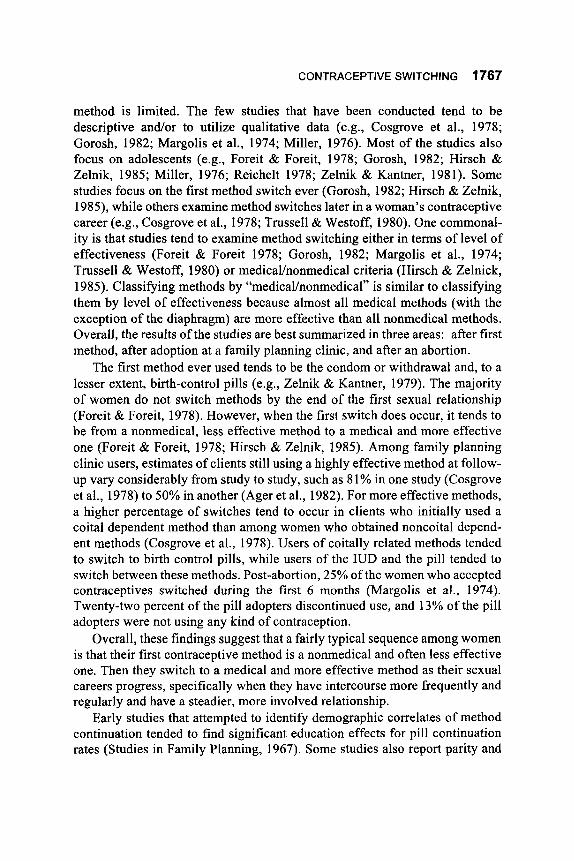
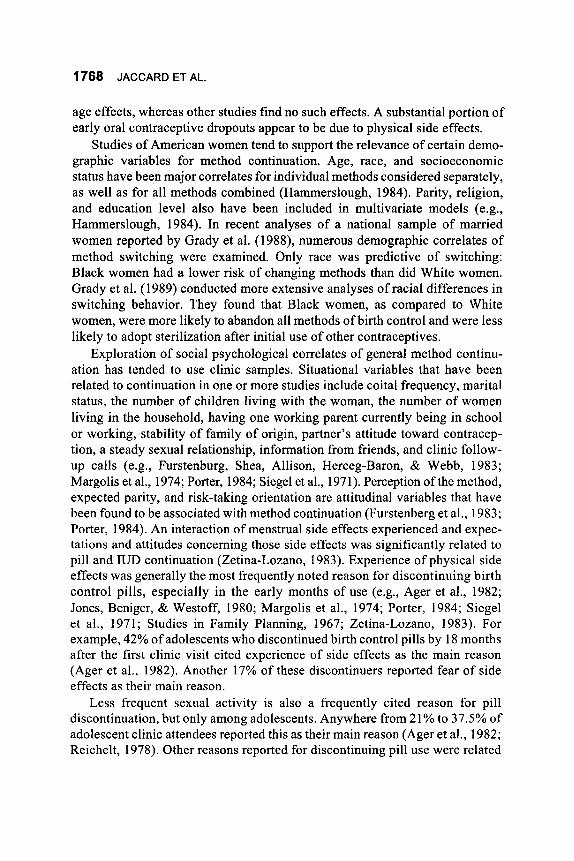
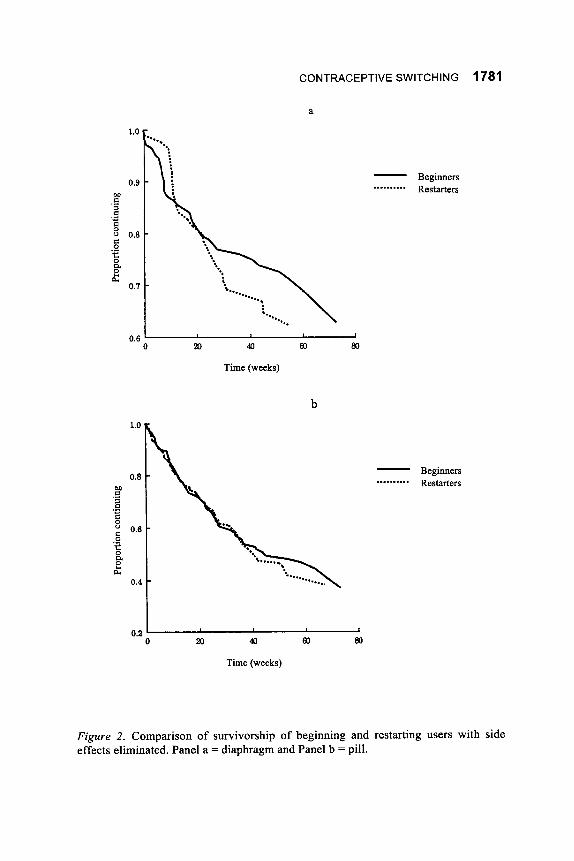
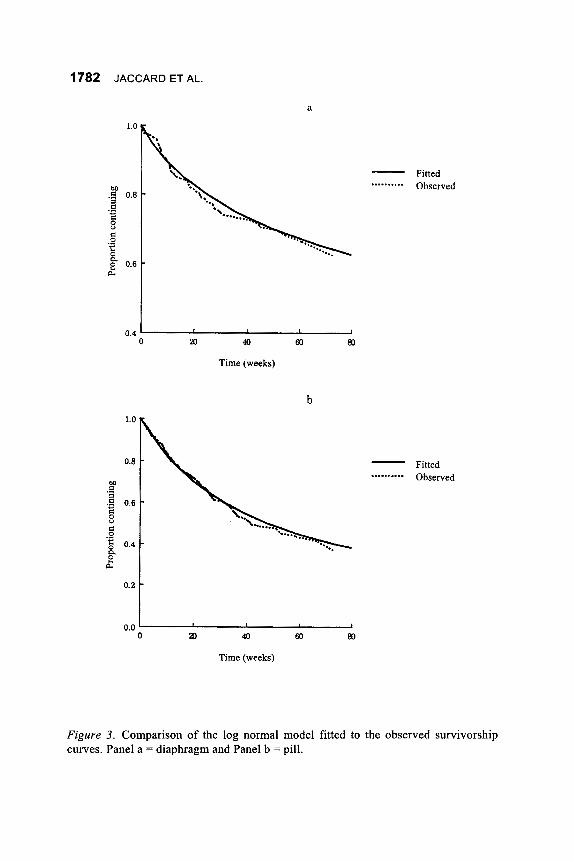
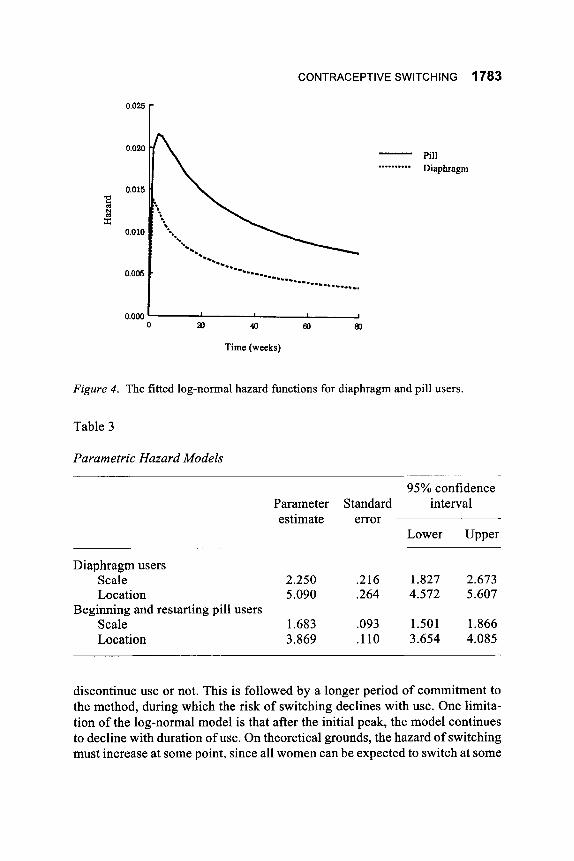
conducted for diaphragm and pill users. The analysis was not stratified by user status because no significant differences were observed above. In both cases, a log-normal model was found to provide a reasonable fit to the data (and a better fit than the Weibull or log-logistic models). The observed and fitted survival functions are presented in Figure 3, and a comparison of the fitted hazard functions is shown in Figure 4. The estimated parameter values are presented in Table 3. In all cases, the risk of switching increased for several weeks before declining. Among diaphragm users, the hazard appears to peak slightly earlier and at a lower rate than among pill users.
In both analyses, the risk of switching increases for several weeks of use and then declines. This pattern is consistent with the existence of a break-in period (associated with an increasing hazard) during which users try a contraceptive once or perhaps several times and then decide either to
1780 JACCARD ET AL.
a
All causes Side effects only
- ..........
0.5 ' 1
0 20 40 60 m
Time (weeks)
1.0
0.8
0.4
b
All causes Side effects only
- ..........
0.2 I I
0 20 40 60 m
Time (weeks)
Figure I. Survivorship on the pill and diaphragm due to all causes of switching and due to side effects provided that all other causes could be eliminated. Panel a =
diaphragm and Panel b = pill.
CONTRACEPTIVE SWITCHING 1781
a
Beginners Restarters
- ..........
0.6 I 0 m 40 60 80
Time (weeks)
b
Beginners Restarters
- ..........
0.2 ' I
0 m 40 60 80
Time (weeks)
Figure 2. Comparison of survivorship of beginning and restarting users with side effects eliminated. Panel a = diaphragm and Panel b = pill.
1782 JACCARD ET AL.
a
Fitted Observed
- ..........
0.4 ' I
0 a0 40 60 m
Time (weeks)
b
Fitted Observed
- ..........
0.0 ' I
0 aD 40 60 m
Time (weeks)
Figure 3. Comparison of the log normal model fitted to the observed survivorship curves. Panel a = diaphragm and Panel b = pill.
CONTRACEPTIVE SWITCHING 1783
Pill Diaphragm
- ..........
0.000 ' I
0 P 40 63 m
Time (weeks)
Figure 4. The fitted log-normal hazard functions for diaphragm and pill users.
Table 3
Parametric Hazard Models
95% confidence Parameter Standard in t e rv a 1 estimate error
Lower Upper
Diaphragm users Scale 2.250 .216 1.827 2.673 Location 5.090 .264 4.572 5.607
Scale 1.683 .093 1.501 1.866 Location 3.869 .110 3.654 4.085
Beginning and restarting pill users
discontinue use or not. This is followed by a longer period of commitment to the method, during which the risk of switching declines with use. One limita- tion of the log-normal model is that after the initial peak, the model continues to decline with duration of use. On theoretical grounds, the hazard of switching must increase at some point, since all women can be expected to switch at some
1784 JACCARD ET AL.
point. This appears to occur well after the follow-up period of the present study. Identijkation of possible prognostic factors. Prognostic factors from the
enrollment assessment that are related to rates of switching were identified using the proportional hazard model (Lee, 1980; Namboodiri & Suchindran, 1987). This model assumes that the influence of a prognostic factor on method continuity is a constant proportion of the baseline hazard. A negative coeffi- cient indicates a longer method continuity for those individuals with large values on the predictor. A total of 17 demographic and psychosocial charac- teristics were considered. Each of the prognostic factors was examined univari- ately and in combination with the other factors.
For the diaphragm, the only significant prognostic factors (over and above the other variables) were clinic experience (coefficient = -0.87, t = 2.43, p < .05) and religious-moral beliefs (coefficient = -0.48, t = 2.03, p < .05), while none of the demographic variables were significant. A positive clinic experi- ence and a belief that other methods (i.e., the pill) are immoral were both associated with increased method continuity. Several factors approach statisti- cal significance. These are method specific knowledge ( t = 1.56) and indicator variables for religion ( t = 1.75, with Catholics being more likely to switch earlier than Protestants). For the pill, the only significant psychosocial prog- nostic factor was clinic experience (coefficient = -0.68, t = 2.86, p < .05). As before, positive clinic experiences were associated with increased method continuity. Religious affiliation was also a significant predictor.
The results with respect to clinic experience are particularly interesting when coupled with the open-ended responses for switching. A significant number of pill switchers reported that they stopped using the pill because they “ran out of supplies.” It may be that these individuals had a bad clinic experi- ence and did not want to return to obtain another prescription because of the “adversity” of dealing with the clinic. Most of our sample consisted of rela- tively poor women who did not have the financial options to attend alternative clinics or a private physician. These women may choose to stop using the pill rather than return to the clinic. Indeed, when we compared the mean scores for the positiveness of the clinic visit for women who reported running out of supplies versus other nonside effect switchers, the means were significantly lower ( t = 2.99, p < .01) in the former as compared to the latter group. For women who identified that they switched from the pill because they ran out of supplies, we identified the method of birth control, if any, to which they switched. Twenty-eight percent of them became nonusers of any form of contraception, even though they remained sexually active and did not desire to become pregnant. Twenty five percent started using relatively unreliable meth- ods (withdrawal, rhythm, suppositories, and foam). These women are at in- creased risk of an unintended pregnancy.
CONTRACEPTIVE SWITCHING 1785
Discussion
The present study observed relatively high levels of contraceptive switch- ing on the part of women. After 5 months, approximately 45% of the diaphragm users had switched from the diaphragm and approximately 70% of the pill users had switched. The extent of switching and their demographic correlates were different in the present study than patterns observed in other research (e.g., Grady et al., 1989). We tended to observe much higher rates of switching than did previous studies, and we failed to observe similar demographic trends (e.g., race differentials). We also found switching to be more prominent in the pill than in the diaphragm, which is at odds with the results of Grady et al.( 1988). One probable reason for the discrepancies is that Grady et al. (1988) focused their analysis on national samples of married women between the ages of 18 and 44. By contrast, our analysis focused on clinic users in a major metropoli- tan area and included primarily younger, single women who were economically disadvantaged. Our data suggest that the degree of switching between methods may be higher for such populations, as compared to the national average of married women. Because such women tend to be at relatively higher risk for unintended pregnancy than the average married female, the analysis of mecha- nisms underlying contraceptive switching is particularly important.
The present data complement existing research on switching behavior by exploring in greater detail the behavior of women who change birth control methods for reasons other than side effects. In addition, the relationship of switching behavior to social psychological variables was explored in greater depth than in previous research. For the diaphragm, the results are consistent with an interpretation that a substantial amount of switching occurs because of mismatched expectations between what a method will be like and what the method is actually like. Responses to the open-ended questions indicated, conservatively, that at least 34% of the switchers changed from the diaphragm because it was more unpleasant or difficult to use than anticipated. The shape of the hazard function in the survival analysis was consistent with a break-in period followed by a declining hazard, as would be predicted by a mismatched- expectations explanation. Unnecessary switching might be minimized by helping women to assess more realistically what is involved in diaphragm use. The data were also consistent with a mismatched-expectations phenomenon for the pill.
Although the shape of the hazard function was consistent with a mis- matched-expectations explanation, other mechanisms may also account for the results. For example, in the introduction it was noted that the occurrence of random events (such as a breakup with a sexual partner) should yield a time invariant hazard of switching. However, it is possible to construct a set of logic
1786 JACCARD ET AL.
where this may not be the case: Everyone has a planning horizon, and the likelihood of certain kinds of events that would lead to a method switch probably can be predicted by many women in the short term. For example, a woman might be able to make an accurate prediction about whether a partner change will occur in the short term but not the long term. It is possible that these short-term predictions enter into a woman’s method-selection process, thereby depressing the early hazard of switching. This would yield the same hazard function as the mismatched-expectations mechanism. Although such logic is plausible, we believe that the results are more consistent with the mismatched- expectations explanation because of the analyses of open-ended questions which showed that over 34% of the switchers changed from the diaphragm because it was more unpleasant or difficult to use than anticipated. Neverthe- less, alternative mechanisms may be operating in conjunction with mismatched expectations, and these need to be explored in future research.
An important finding in the present research was the identification of clinic experiences as an important correlate of switching. Research on switching has tended to emphasize demographic variables and characteristics of the individ- ual as predictors of switching. The present data suggest that clinic variables may be important: Women who had negative experiences during their initial clinic visit were more likely to switch from the pill or the diaphragm than were women who did not. The magnitude of the coefficients for clinic experience in our models was fairly substantial, suggesting a sizable impact of this variable. These results suggest the importance of emphasizing to clinic staff the potential impact that they can have on their clients and the importance of structuring a positive clinic experience.
To the extent that mismatched expectations are operative in switching, clinics may be able to adopt procedures to minimize unnecessary switching. In addition to more in-depth counseling at the initial visit, a follow-up visit or telephone contact might be made within the first 2-3 months. In our experience, many clinics schedule brief visits for diaphragm checks 1 week after dia- phragm adoption. The focus of the visit is on correctness of use; namely, does the woman put the diaphragm inside in an anatomically correct fashion. These visits might also be used for important counseling to discover the woman’s subjective experience of difficulties and unpleasantness of use and to explore ways to cope with these, or as an opportunity to switch methods.
We also found that a significant number of pill switchers reported that they stopped using the pill because they ran out of supplies. We believe that the prognostic ability of negative clinic experiences for the pill may derive from these women. More specifically, if individuals have adverse clinical experi- ences, they may be less likely to return to the clinic for refills. For economi- cally disadvantaged women who have few alternative places to obtain oral

CONTRACEPTIVE SWITCHING 1787
contraceptives, the result may be the eventual nonuse of contraception altogether. Indeed, in our study, over 50% of women who ran out of supplies remained sexually active and did not use any form of birth control or switched to relatively unreliable methods of birth control.
Our data also suggest that self reports of reasons for switching may need further exploration and interpretation. For example, the reason for pill switch- ing “I ran out of supplies” may be partially due to the woman not liking the clinic. However, there may be other reasons why women run out of supplies, such as poor planning skills, lack of goal and task orientation, low commitment to avoiding pregnancy, low acceptance of sexuality, andor the inconvenience of using any contraceptive method. Such mechanisms need to be explored, rather than simply accepting stated reasons at face value.
Most of the social psychological variables that we used to predict switching exhibited statistically nonsignificant explanatory power. Our method of anal- ysis adopted a conservative approach, where the predictive power of a measure was evaluated over and above all other psychological and demographic vari- ables (which were used as covariates). The results for clinic experience were significant when the covariates were included and were replicated with alter- native models (e.g., a log-normal accelerated lifetime model) and within the separate strata of beginners and restarters. In contrast, none of the other social psychological variables achieved satisfactory and reliable predictive power. One reason for this might be our focus only on measures obtained at enroll- ment. Some of the psychological variables may indeed be relevant to switch- ing, but may do so in a dynamic fashion that requires assessment of the measures at each wave of the panel design in order to adequately model their influence. Future research should explore this possibility.
The present analyses are suggestive but, of course, must be interpreted within the constraints of the subject population, the research design, and the measures used. We believe that our study has suggested interesting trends that can serve as a springboard for more intensive study.
References
Ager, J. W., Shea, F. P., & Agronow, S. J. (1982). Method discontinuance in teenage women: Implications for teen contraceptive programs. In 1. R. Stuart & C. F. Wells (Eds.), Pregnancy in adolescence: Needs, problems and management (pp. 236-263). New York, NY: Van Nostrand, Reinhold.
Beckman, L. J., & Hauser, B. B. (1979). Perceived satisfactions and costs of motherhood and employment among married women. Journal of Popula- tion, 2, 306-326.
Cohen, J. B., Severy, L. J., & Ahtola, 0. T. (1978). An extended expectancy-
1788 JACCARD ET AL.
value approach to contraceptive alternatives. Journal of Population, 1,22-24. Cosgrove, P. S., Penn, R., & Chambers, N. (1978). Contraceptive practice after
clinic discontinuation. Family Planning Perspectives, 10, 337-340. Davidson, A. R., & Jaccard, J. J. (1975). Population psychology: A new look
at an old problem. Journal of Personality and Social Psychology, 13,
Davidson, A. R., & Jaccard, J. J. (1979). Variables that moderate the attitude- behavior relation: Results of a longitudinal study. Journal of Personality and Social Psychology, 37, 1364- 1376.
Fishbein, M. (1972). Toward an understanding of family planning behaviors. Journal of Applied Social Psychology, 2 , 214-227.
Fishbein, M., & Ajzen, I. (1 975). Belie$ attitude, intention and behavior: An introduction to theory and research. Reading, MA: Addison-Wesley.
Foreit, J. R., & Foreit, K. G. (1978). Risk-taking and contraceptive behavior among unmarried college students. Population and Environment, 4, 174- 188.
Furstenberg, F., Jr., Shea, J., Allison, P., Herceg-Baron, R., & Webb, D. (1983). Contraceptive continuation among adolescents attending family planning clinics. Family Planning Perspectives, 15,211-217.
Gorosh, M. (1982). Patterns of contraceptive use among female adolescents: Method consistency in a clinic setting. Journal of Adolescent Health, 3 ,
Grady, W. R., Hayward, M., Billy, J., & Florey, F. (1989). Contraceptive switching among currently married women in the United States. Journal ofBiosocia1 Science, 11, 117-132.
Grady, W. R., Hayward, M., & Florey, F. (1988). Contraceptive discontinu- ation among married women in the United States. Studies in Family Planning, 19,227-235.
Grady, W. R., Hirsch, M. B., Keen, N., & Vaughan, B. (1983). Contraceptive failure and continuation among married women in the U.S., 1970-1975. Family Planning Perspectives, 14,9-19.
Hammerslough, C. R. (1984). Characteristics of women who stop using contra- ceptives. Family Planning Perspectives, 16, 14- 18.
Helbig, D., Gutman, M., & Kritz-Silverstein, D. (1987). Components of effec- tive fertility regulation study. Unpublished manuscript, Health Science Center at Brooklyn, State University of New York.
Hirsch, M. B., & Zelnik, M. (1985). Contraceptive method switching among American female adolescents, 1979. Journal of Adolescent Health Care,
Jaccard, J. J. (198 1). Attitudes and behavior: Implications of attitudes toward behavioral alternatives. Journal of Experimental Social Psychology, 17,
1073- 1082.
96- 102.
6,743-757.
286-307.
CONTRACEPTIVE SWITCHING 1789
Jaccard, J. J., & Becker, M. (1985). Attitudes and behavior: An information integration perspective. Journal of Experimental Social Psychology, 32,
Jaccard, J. J., & Davidson, A. R. (1972). Toward an understanding of family planning behavior: An initial investigation. Journal of Applied Social
Jones, E. F., Beniger, J. R., & Westoff, C. F. (1980). Pill and IUD discontinu- ation in the United States, 1970-1975: The influence of the media. Family Planning Perspectives, 12,293-302.
Lee, E. T. (1980). Statistical methods for survival data analysis. Belmont, CA: Lifetime Learning.
Luker, K. (1 975). Taking chances: Abortion and the decision not to contra- cept. Berkeley, CA: University of California Press.
Margolis, A., Rindfuss, R., Coghlan, P., & Rochat, R. (1974). Contraception after abortion. Family Planning Perspectives, 6 , 56-64.
Miller, W. B. (1976). Sexual and contraceptive behavior in young unmarried women. Primary Care, 3,427-453.
Namboodiri, K., & Suchindran, C. (1987). Life table techniques and their applications. Orlando, FL: Academic.
Porter, E. G. (1984). Birth control discontinuance as a diffusion process. Studies in Family Planning, 15, 20-29.
Reichelt, P. A. (1978). Changes in sexual behavior among unmarried teenage women utilizing oral contraceptives. Journal of Population, 1, 57-68.
Siege], E., Thomas, D., Coulter, E., Tuthill, R., & Chipman, S. (1971). Continuation of contraception by low income women: One year follow- up. American Journal ofpublic Health, 61, 1886-1891.
Trussell, J., & Westoff, C. (1980). Contraceptive practice and trends in coital frequency. Family Planning Perspectives, 12,246-263.
Use of oral contraceptives. (1 967). Studies in Family Planning, 24, 1 - 13. Zelnik, M., & Kantner, J. F. (1979). Sexual and contraceptive experience of
young unmarried women in the U.S., 1976 and 1971. Family Planning Perspectives, 9, 55-71.
Zetina-Lozano, G . (1 983). Menstrual bleeding expectations and short-term contraceptive discontinuation in Mexico. Studies in Family Planning, 14,
222-234.
Psychology, 2,228-235.
127- 133.





























