Embed Size (px)
Citation preview

Service Learning: A Vehicle for Building Health Equityand Eliminating Health Disparities
Service learning (SL) is a
form of community-centered
experiential education that
placesemerginghealthpro-
fessionals in community-
generated service projects
and provides structured op-
portunities for reflection on
thebroadersocial,economic,
and political contexts of
health.
We describe the elements
and impact of five distinct
week-long intensive SL
courses focused on the con-
text of urban, rural, border,
and indigenous health con-
texts. Students involved in
these SL courses demon-
strated a commitment to
community-engaged schol-
arship and practice in both
their student and profes-
sional lives.
SL is directly in line with
the core public health value
of social justice and serves
as a venue to strengthen
community–campus part-
nerships in addressing
health disparities through
sustained collaboration and
action invulnerablecommu-
nities. (Am J Public Health.
2015;105:S 3 8 – S 4 3 . d o i :
10.2105/AJPH.2014.302364)
Samantha Sabo, DrPH, MPH, Jill de Zapien, BA, Nicolette Teufel-Shone, PhD, Cecilia Rosales, MD, LyndaBergsma, PhD, and Douglas Taren, PhD
THE INSTITUTE OF MEDICINE
has called for integration of eco-logical approaches that considerthe social, economic, and politicalcontext of health into public healtheducation.1 However, there arelimited reports on how to teach andmeasure the outcomes of educa-tion programs that link learningand application of these conceptsin public health.2 Service learning(SL) is one such pedagogy thatcan enhance student awarenessof and commitment to the elimi-nation of health disparities.3---5 SL isa form of community-centeredexperiential education that lo-cates emerging health profes-sionals in community-generated service projects andprovides structured opportunitiesfor reflection on the broader so-cial, economic, and political con-texts of health.4 Through guidedreflection on academic readingsand service, students link theirservice experience to broadersystems-level thinking,5,6 enhancecultural humility,7,8 and increasetheir civic engagement.9 Althoughwidely applied in the clinical healthprofessions of nursing,10 medi-cine,7,11 pharmacy,12 and publichealth,6,13,14 research on the im-pact of SL on students, faculty,and community partners is rela-tively new.4
We present an innovative SLinitiative modeled on the reduc-tion of health disparities throughexploration, reflection, and actionon the social determinants ofhealth. Our program consists offive distinct week-long intensiveSL courses that are focused on
binational, urban, rural, and in-digenous communities in thesouthwestern United States. Spe-cifically, we describe our pro-gram’s contribution to graduatepublic health education and waysin which students, faculty, andcommunity partners discover andact on the social determinants ofhealth.
ORIGINS OF THESERVICE-LEARNINGINSTITUTES
In 2005, the College of PublicHealth started a series of rural andurban field-based courses withfunds from a Health Resourcesand Services Administration Ma-ternal and Child Health Bureau(MCHB) School of Public HealthLeadership training grant thatevolved from a history of havingMCHB certificate students con-ducting service-oriented projects.15
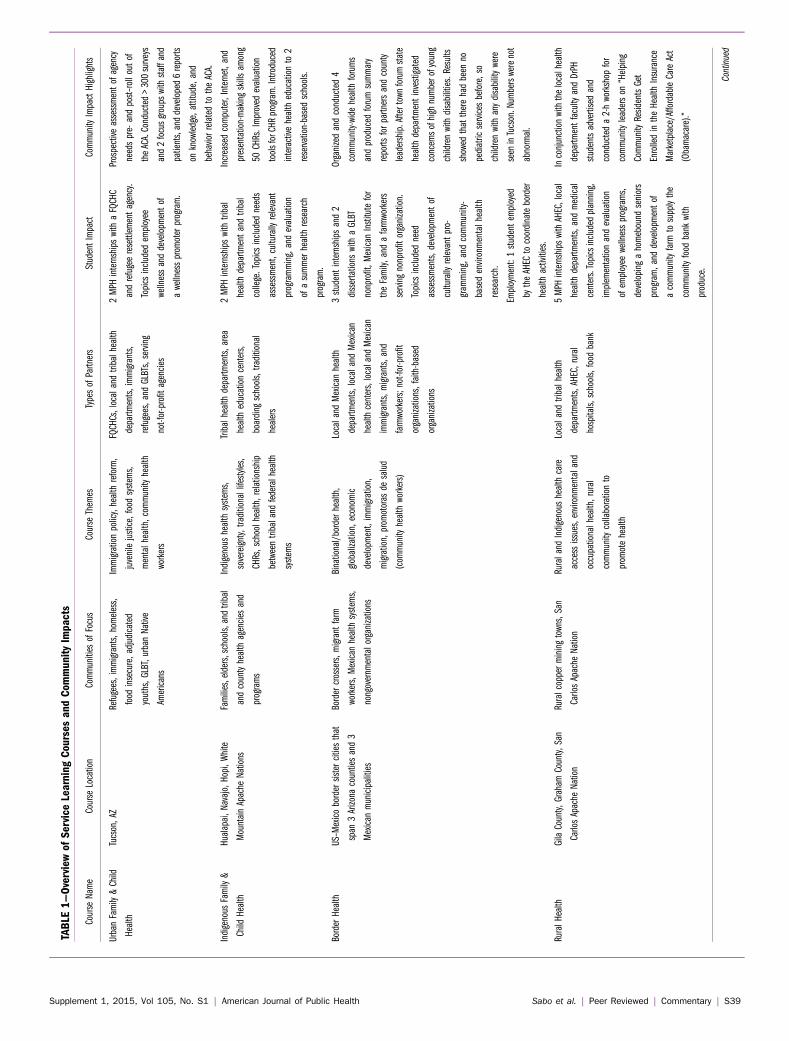
In 2009, the Community---Campus Partnerships for Health,Health Disparities Service-Learning Collaborative providedthe resources and mentorship toexpand and develop an integratedSL program. Since then, five dis-tinct week-long intensive pro-grams have been developed incollaboration with communitypartners and doctoral students(Table 1).
Course development starts byhaving three to five meetings withagencies during the 4 months be-fore the program to identify salientissues, events, needs, and oppor-tunities that exist within theagency and community. Faculty,
the agencies’ program managers,community health workers, andoutreach staff work together todevelop objectives, activities, andreflection questions. In addition,several phone calls and e-mailexchanges are made with regardto materials required for the SLcourse and to co-develop assess-ment tools and promotional ma-terials for community events.
All faculty, and in some cases,partners, develop structured criti-cal reflection opportunities. Indi-vidual journal writing, small andlarge reflections, and summativeoral presentations and papers aretypical reflection strategies. Dailyreflection questions guide the stu-dent’s individual reflections. Smallservice-based group reflectionshelp organize thoughts and feel-ings experienced during uniqueservice activities. During largegroup reflections, faculty andcommunity partners help studentsconnect and contextualize issuesencountered in academic readingsand service activities. Studentsparticipate in a pre-SL orientationregarding ethical conduct; peersand community partners later re-inforce themes.
The Arizona Health EducationCenters Program, the MCBHLeadership Training grant, andinstitutional funds sustain thesecourses. Furthermore, Masters’students are required to take oneSL course in family and childhealth, health behavior and healthpromotion, and policy and man-agement. Doctoral students arerequired to take two courses, butthey can elect to coteach one of
COMMENTARY
S38 | Commentary | Peer Reviewed | Sabo et al. American Journal of Public Health | Supplement 1, 2015, Vol 105, No. S1
TABLE
1—Overviewof
Service
Learning
Courses
andCom
munityImpacts
CourseName
CourseLocation
CommunitiesofFocus
CourseThemes
TypesofPartners
StudentImpact
Community
ImpactHighlights
UrbanFamily&Child
Health
Tucson,AZ
Refugees,immigrants,homeless,
food
insecure,adjudicated
youths,GLBT,urbanNative
Americans
Immigrationpolicy,healthreform,
juvenilejustice,food
systems,
mentalhealth,community
health
workers
FQCHCs,localand
tribalhealth
departm
ents,immigrants,
refugees,andGLBTs,serving
not-for-profitagencies
2MPH
internshipswithaFQCHC
andrefugeeresettlementagency.
Topicsincluded
employee
wellnessanddevelopmentof
awellnesspromoterprogram.
Prospective
assessmentofagency
needspre-andpost–rolloutof
theACA.Conducted>300surveys
and2focusgroupswithstaffand
patients,anddeveloped6reports
onknowledge,attitude,and
behaviorrelatedtotheACA.
Indigenous
Family&
Child
Health
Hualapai,Navajo,Hopi,White
MountainApache
Nations
Families,elders,schools,andtribal
andcountyhealthagenciesand
programs
Indigenous
healthsystems,
sovereignty,traditionallifestyles,
CHRs,schoolhealth,relationship
betweentribaland
federalhealth
systems
Tribalhealthdepartm
ents,area
healtheducationcenters,
boarding
schools,traditional
healers
2MPH
internshipswithtribal
healthdepartm
entandtribal
college.Topicsincluded
needs
assessment,culturallyrelevant
programming,andevaluation
ofasummerhealthresearch
program.
Increasedcomputer,Internet,and
presentation-makingskillsamong
50CHRs.Improved
evaluation
toolsforCHR
program.Introduced
interactive
healtheducationto2
reservation-basedschools.
BorderHealth
US–Mexicobordersistercitiesthat
span
3Arizona
countiesand3
Mexican
municipalities
Bordercrossers,migrantfarm
workers,Mexican
healthsystems,
nongovernmentalorganizations
Binational/borderhealth,
globalization,economic
development,immigration,
migration,promotoras
desalud
(community
healthworkers)
Localand
Mexican
health
departm
ents,localand
Mexican
healthcenters,localand
Mexican
immigrants,migrants,and
farmworkers;not-for-profit
organizations,faith-based
organizations
3studentinternshipsand2
dissertations
withaGLBT
nonprofit,Mexican
Institutefor
theFamily,andafarmworkers
servingnonprofitorganization.
Topicsincluded
need
assessments,developmentof
culturallyrelevantpro-
gram
ming,andcommunity-
basedenvironm
entalhealth
research.
Organizedandconducted4
community-widehealthforums
andproduced
forumsummary
reports
forpartnersandcounty
leadership.Aftertownforumstate
healthdepartm
entinvestigated
concernsofhighnumberofyoung
childrenwithdisabilities.Results
showed
thattherehadbeen
no
pediatric
servicesbefore,so
childrenwithanydisabilitywere
seeninTucson.Numberswerenot
abnormal.
Employment:1studentemployed
bytheAHEC
tocoordinateborder
healthactivities.
RuralHealth
GilaCounty,Graham
County,San
CarlosApache
Nation
Ruralcopperminingtowns,San
CarlosApache
Nation
Ruraland
Indigenous
healthcare
accessissues,environmentaland
occupationalhealth,rural
community
collaborationto
promotehealth
Localand
tribalhealth
departm
ents,AHEC,rural
hospitals,schools,food
bank
5MPH
internshipswithAHEC,local
healthdepartm
ents,andmedical
centers.Topicsincludedplanning,
implementationandevaluation
ofemployee
wellnessprograms,
developing
ahomebound
seniors
program,anddevelopmentof
acommunity
farm
tosupplythe
community
food
bank
with
produce.
Inconjunctionwiththelocalhealth
departm
entfaculty
andDrPH
studentsadvertisedand
conducteda2-hworkshop
for
community
leaderson
“Helping
Community
ResidentsGet
EnrolledintheHealthInsurance
Marketplace/AffordableCareAct
(Obamacare).”
Continued
Supplement 1, 2015, Vol 105, No. S1 | American Journal of Public Health Sabo et al. | Peer Reviewed | Commentary | S39

them. In our most recent stu-dent admissions survey, morethan 58% of the incoming stu-dents said that the SL programwas either very important orimportant in terms of influenc-ing their decision to attend ourcollege. Table 1 provides anoverview and the impact ofeach course.
The urban family and childhealth SL program providesstudents with the opportunity tolearn about current health andsocial policies that affect urbanfamilies and children. Thiscourse responds directly toagencies that serve immigrantand migrating populations, in-cluding undocumented andmixed immigration status fami-lies, resettled refugees, urbanAmerican Indians, and gay, les-bian, bisexual, and transgenderand adjudicated youths. Paneldiscussions and guided obser-vation activities are organizedwith human rights organiza-tions, legal systems, and theMexican Consulate. Students’SL ranges from neighborhoodcleanup and meal preparationto development of culturallyrelevant health education andphysical activity sessions, quan-titative and qualitative forma-tive assessment, analysis, andreport preparation. In 2013, inlight of monumental shifts inhealth reform and the chal-lenges identified by communitypartners, the course focused onthe Affordable Care Act (ACA).Faculty and partners from fed-erally qualified communityhealth centers, tribal clinics, andlocal health department pro-grams prepared opportunitiesfor critical dialogue on the de-velopment of the new healthcare law and implications forhealth care delivery andprevention for immigrant,
indigenous, and refugee families.Faculty and partners codevelopedinstruments to assess ACA knowl-edge and outreach, education, andtraining needs among staff andclients. Student teams conductedassessments and led focus groupswith clients and staff in severalsites, performed all analyses, andprepared policy briefs and pre-sentations on findings and recom-mendations. Faculty and studentsincreased their understanding ofthe ACA and vulnerable popula-tions and provided much neededdata to partners to prepare for therollout of the ACA.
The indigenous family andchild health SL program addressesthe complex interaction of thesocial determinants of family andchild health through working inNative American communities innorthern Arizona. Through col-laborative activities, presentations,and conversations with staffworking for federal, tribal andstate health care agencies, nativehealers, and reservation residents,students learn about the array oflocal health care services and thechallenges and strategies of healthcare systems working to serverural, culturally distinct popula-tions. This course uses exchangeof skills teaching approaches.Students are paired with tribalcommunity health workers orcommunity health representatives(CHRs). CHRs take students ona home visit to observe and assistwith services provided by CHRs.Students provide nutrition andhealth education, reduce the risk ofinjury by rearranging electricalcords and throw rugs, and haulwater. In return, students buildCHR skills in looking for crediblehealth information from the Inter-net, develop simple PowerPoint(Microsoft, Redmond, WA) pre-sentations for community presen-tations and educational handouts,
TABLE
1—Continued
Urban–Metropolitan
Health
GreaterPhoenixmetropolitan
area
Immigrantfamilies,undocumented
immigrantfamilies
andchildren,
urbanNativeAmericans
Healthequity,immigration,stress,
community
art,promotoras
de
salud
Homelessshelter,community
gardens,community
clinic
3MPH
internshipswithstateand
localhealth
departm
entand
nonprofits.Topicsincluded
integrationofbehavioraland
physicalhealth,evaluationof
peer-runorganization,and
developmentofpromotorprogram
foralocalnonprofitand
human
rightsorganization.
Conducted2community
health
assessments;analyzed
and
reporteddata.Bothsurveyresults
wereused
by2differententities:
oneinrebranding
thebehavioral
healthclinicandtheotherin
expandingservicestotargeted
community.Also
increased
numberofstudentvolunteer
servicestononprofit
organizations.
Employment:Studenthiredby
nonprofit.
Note.ACA=AffordableCareAct;AHEC=AreaHealthEducationCenters;CHR=communityhealthrepresentative;DrPH
=DoctorofPublicHealth;FQCHC
=federallyqualified
communityhealthcenters;GLBT=gay,lesbian,bisexual,and
transgender;M
PH=Mastersin
PublicHealth.
S40 | Commentary | Peer Reviewed | Sabo et al. American Journal of Public Health | Supplement 1, 2015, Vol 105, No. S1

and develop simple evaluationforms to gain input from theirclients. Students gain insight intospiritual health and healing by vis-iting traditional and religiousleaders, and experiencing the socialcamaraderie generated by planting,building a ramada (a roofed shel-ter), and breadmaking outside onan open fire.
The border health SL coursefocuses on the complex relation-ship of migration, health, andeconomic development at theUnited States---Mexico border.This course rotates each yearamong United States---Mexico bor-der sister cities, giving students anopportunity to live in an Arizonaborder community; these studentscross the United States---Mexicoborder almost daily. SL opportu-nities include a combination ofapplied traditional public healthopportunities addressed by local,state, and federal health depart-ments of both countries, includingimmunization and vector controlcampaigns, chronic disease pre-vention education, and access tocare. These experiences are cou-pled with service in governmentaland grass roots organizations fo-cused on social determinants ofhealth, including food insecurity,housing, humanitarian aid to bor-der crossers, economic develop-ment, and immigration issues. Thisprogram also incorporates inter-active tours and discussions withagencies and individuals integralto the globalized and militarizedUnited States---Mexico border en-vironment, including the Mexicanconsulate, the US Border Patrol,and associated immigration de-tention centers, humanitarian aidgroups, local policy coalitions, andborder crossers. Students presenttheir final team reflections at theend of the course to communitypartners and faculty, integratingmigration, health, and economic
development within a frameworkof advocacy and elimination ofhealth disparities.
The rural health SL course isdesigned to expose students torural health disparity issues, suchas recruitment and retention ofan adequate health professionalworkforce, and rural health assets,such as the compassionate collab-oration of innovative and dedi-cated rural individuals and groupsto attend to a variety of populationand clinical health needs. Thecourse also focuses on communityeconomic development, the occu-pational and environmental healthissues of copper mining in easternArizona, cattle ranching, and cot-ton production, as well a majoremployers like county, city, andtribal government, tourism, smallbusiness, and a large service sec-tor. Although students learn aboutfactors that influence public healthin a rural and Native Americancommunities, they also performservices such as working with co-operative extension to teach oralhygiene to Head Start childrenwith disabilities; weeding, plant-ing, and digging post holes fora new greenhouse at the commu-nity farm and food bank; organiz-ing sports equipment, cleaning,and painting facilities at a tribalyouth summer campgrounds; andteaching health to Boys and GirlsClub members ages nine to 14years, and encouraging them toconsider a health career.
The Phoenix urban SL courseimmerses students in the day-to-day work of federal, state, tribal,and nonprofit public health pro-grams that serve the ethnic, racial,social, and economic diversitywithin the sixth largest city in thecountry. Students observe, reflect,and discuss how public healthprograms address socioeconomicchallenges, migration issues, cul-tural beliefs, health behaviors, and
access to life-sustaining resourcesin urban settings. This program isdesigned to develop, implement,and evaluate educational activ-ities in collaboration with thecommunity and respond tocommunity-identified concerns.The learning modalities are di-verse, and include communitypanel discussions with residentsand leaders of the area, walkingand talking tours of public art, andhow the integration of art anddesign enhances community well-ness. Students participate withresidents in community gardeningas a form of teaching about fooddeserts and sustainable develop-ment. Students are also exposed toservices designed for the urbanNative American population, andhow these nations address home-lessness among tribal membersand issues related to access to carein nonreservation settings. Stu-dents also witness the criticalneeds of mixed immigrant familiesin a county known for its anti-immigrant attitudes.
EVALUATION ANDDISCUSSION
Process and outcome evalua-tion occurs at student and com-munity levels, whereas facultyassessment remains qualitative.Students conduct a postcourseself-assessment that focuses onhow SL influenced their perspec-tive on learning, view of service,choice of career or specialization,and perspectives on working ina diverse community.16 This eval-uation is coupled with a facultyevaluation of student’s daily jour-nals, final reflection papers, andpresentations.13,17
Table 2 highlights major find-ings from the student results andprovides information on the im-pact of the faculty and communityon these results.
PERSPECTIVES ONSERVICE-LEARNINGCOURSES
Students reported several in-terpersonal changes as a result ofSL, and taken together, demon-strated increased cultural humility,leadership, and commitment tocommunity-engaged scholarshipand practice in student and pro-fessional life. Several studentsdescribed feelings of personaltransformation:
Service as a method fortransformation—that is whatour experience has been here.We were given an opportunity ofa hands-on experience, not just tosay, oh, we did that, that it en-abled us to transform somethinginside of us, and bring it back toother places we work, othercommunities, to create change.
Students also describeda renewed sense for real-worldpublic health:
[T]he classroom became real. Forthe first time as students all of oursenses were engaged. Servicelearning allows us to engage firsthand in communities and seepublic health theories in practicein the real world.
Other students connected theo-ries and policies learned in class tovulnerable populations encoun-tered in service, and as one stu-dent clearly described:
The theories and polices we dis-cuss in class have real worldimplications and we have experi-enced a snapshot of those impli-cations to keep now that we havetaken part in a service-learningproject.
By focusing on health dispar-ities in context and community,students came away with a senseof urgency and action to engageduring their academic program.Since 2009, at least 20% of en-rolled students developed their in-ternships based on the partnershipsmade and the health disparities
COMMENTARY
Supplement 1, 2015, Vol 105, No. S1 | American Journal of Public Health Sabo et al. | Peer Reviewed | Commentary | S41

encountered during these courses.One student described her journeyin the following way:
I was incredibly moved by howdedicated public health workersare to their communities on bothsides of the border, and theamount they are able to accom-plish with many barriers andlimited resources. This coursestrengthened my interest in
working with rural and under-served communities, and this hasled to an internship I’m planningfor this summer.
Some SL students shifted theiracademic and career plans to in-tern and work with communitypartners based on the social justiceissues encountered (Table 1). Twostudent clubs were formed as
a result of SL, including theLearning Understanding Commu-nity Health Advocacy; this clubprovides a venue for students tocontinue to partner and organizesocial justice service events withcommunity partners for the largerstudent body. In 2010, a smallgroup of students taking the borderhealth SL course worked with fac-ulty to develop a course focused onthe Guatemala---Mexico border.This course grew in popularity,and now involves more than 25different students in planning andfinancing.
Although our community part-ners were not directly financiallycompensated for their contribu-tion to the courses, they describeda desire to partner with the uni-versity and a renewed sense ofcommitment to public health andpride in their community; onepartner described how participa-tion in SL, “. . . reconnected mewith my passion to see change.”Others described how workingwith students affected their senseof community, “I felt so proud ofmy community seeing studentsengaged in working in the com-munity.” Faculty members de-scribed transformation and inspi-ration; one faculty memberexplained, “Service-learning trans-forms faculty, students, and com-munity partners in ways thatcontribute to cultural humilityand builds respect for all of ourunique contributions to solvingbig, complex public health problemsof today.” Overall, SL programscontributed to new partnershipsand the development of researchand practice endeavors amongfaculty and community partners.By coming back year after year,faculty, and thus, the university,are seen as long-term partners andas relevant to the technical, re-search, and overall communityneeds.
CHALLENGES
SL courses require an enor-mous amount of time and energyto develop, implement, and sus-tain. To overcome these challenges,our program significantly engageddoctoral students as coinstructors.Once doctoral students completeda SL course, they were invited tocoteach it. Coteaching brings newenergy, directions, and partner-ships to the course and helps toalleviate potential burnout amongfaculty and partners.
Another challenge was measur-ing the nuanced changes in culturalhumility gained by students overtime and how such change affectedacademic and career choices.
CONCLUSIONS
SL was described to be directlyin line with the core public healthvalue of social justice,4,18 andserved as a venue to strengthencommunity---campus partnershipsin addressing health disparitiesthrough sustained connection andaction in effected communities.Academic public health programsengaged in SL strengthened thestudent’s ability to learn and act onsocial and health disparities. Ourexperience with SL was that itcreated the necessary space forstudent, faculty, and communitypartners to coanalyze social de-terminants of health and locatecommunity-centered solutions. j
About the AuthorsAll authors are from the Mel and EnidZuckerman College of Public Health,University of Arizona, Tucson.Correspondence should be sent to Douglas
Taren, PhD, University of Arizona, Mel andEnid Zuckerman College of Public Health,1295N.MartinAve,POBox245163,Tucson,AZ85745 (e-mail: [email protected]).Reprints can be ordered at http://www.ajph.orgby clicking the “Reprints” link.
This article was accepted September 22,2014.
TABLE 2—Selected Demographics and Post–Service-Learning
Assessment Results for Service-Learning Students and
Community Partners
Student Demographics (n = 107) No. (%)
Gender
Women 94 (88)
Men 13 (12)
Ethnicity
White, non-Hispanic 67 (63)
Hispanic 13 (12)
American Indian/Alaska Native 6 (6)
African American 6 (6)
Age, y
20–24 27 (25)
25–29 50 (47)
30–34 11 (10)
‡ 35 19 (18)
Academic program
Maternal and child health 47 (44)
Health behavior health promotion 12 (11)
Doctor of Public Health 11 (10)
Student assessment (n = 107)
Increased a responsibility for own learning 86 (80)
Increased awareness of own bias and prejudices 83 (78)
Increased awareness of many roles of health professions 106 (99)
Service learning helped to define personal strength(s) 93 (97)
Service learning enhanced personal leadership skills 83 (78)
Increased ability to communicate ideas to persons different
than themselves
94 (88)
Service learning helped to defined career path 70 (65)
Plans to continue service with service learning partner 50 (47)
Plan to integrate service learning into career path 97 (91)
Community partner assessment (n = 35)
Felt the benefits outweighed the cost 29 (83)
Felt valued as a teacher by the University faculty 33 (94)
Felt service learning made University aware of community
needs
26 (74)
Felt community served by agency benefited 31 (88)
Anticipate a relationship with the University 97 (91)
COMMENTARY
S42 | Commentary | Peer Reviewed | Sabo et al. American Journal of Public Health | Supplement 1, 2015, Vol 105, No. S1

ContributorsEach author contributed to the de-velopment, writing, and submission ofthe article. Each author has participatedin the service learning courses.
AcknowledgmentsThe service learning program was par-tially supported with funds from theArizona Health Education Centers anda Health Resources and Services Admin-istration Maternal and Child Health Pub-lic Health Training Program (grant#T76MC04925).
We wish to acknowledge SuzanneCashman and Serena Siefer from Com-munity Campus Partnerships for Health---Health Disparities Collaborative for men-toring us through the development of ourcourses and all of the community partnersthat worked with us over the years todevelop these courses.
Note. Information in this article waspreviously presented at Innovations inPublic Health Education conference, Co-lumbia University Mailman School ofPublic Health; June 4, 2013; New York,NY.
Human Participant ProtectionReporting these results are exempt fromthe University of Arizona human subjectprotection program because they areconsidered an evaluation of an educationprogram.
References1. Committee on Educating PublicHealth Professionals for the 21st Century.The future of public health education. In:Who Will Keep the Public Healthy? Edu-cating Public Health Professionals for the21st Century. Washington, DC: The Na-tional Academies Press; 2003.
2. White S. Public health at a cross-roads: assessing teaching on economicglobalization as a social determinant ofhealth. Crit Public Health. 2012;22(3):281---295.
3. Dunlap M, Scoggin J, Green P, DaviA. White students’ experiences of privi-lege and socioeconomic disparities: to-ward a theoretical model. Mich J Commu-nity Serv Learn. 2007;13(2):19---30.
4. Cashman SB, Seifer SD. Service-learning: an integral part of undergradu-ate public health. Am J Prev Med.2008;35(3):273---278.
5. Steinman E. “Making space”: lessonsfrom collaborations with tribal nations.Mich J Community Serv Learn. 2011;18(1):5---18.
6. Camacho MM. Power and privilege:community service learning in Tijuana.Mich J Community Serv Learn. 2004;10(3):31---42.
7. Buckner AV, Ndjakani YD, Banks B,Blumenthal DS. Using service-learning toteach community health: the MorehouseSchool of Medicine community healthcourse. Acad Med. 2010;85(10):1645---1651.
8. Matsunaga DS, Rediger G, MamaclayB, Sato D, Yamada S. Building culturalcompetence in a interdisciplinary com-munity service-learning. Pac HealthDialog. 2003;10(2):34---40.
9. Roschelle AR, Turpin J, Elias R. Wholearns from service learning? Am BehavSci. 2000;43(5):839---847.
10. Lashley M. Nurses on a mission:a professional service learning experiencewith the inner-city homeless. Nurs EducPerspect. 2007;28(1):24---26.
11. Meurer LN, Young SA, Meurer JR,Johnson SL, Gilbert IA, Diehr S. Theurban and community health pathway:preparing socially responsive physicians.Am J Prev Med. 2011;41(4, suppl 3):S228---S236.
12. Brown B, Heaton PC, Wall A. Aservice-learning elective to promote en-hanced understanding of civic, cultural,and social issues and health disparities inpharmacy. Am J Pharm Educ. 2007;71(1):9.
13. Sabo S, Guernsey de Zapien J,Rosales C. Entre fronteras (between bor-ders): the power of service-learning incultural exchange and social action in theUnited States-Mexico borderlands. Int JHeritage Sustainable Dev. In press.
14. Gregorio DI, DeChello LM, Segal J.Service learning within the University ofConnecticut Master of Public Health.Public Health Rep. 2008;123(suppl2):44---52.
15. Taren DL, Varela F, Dotson JA, et al.Developing a university-workforce part-nership to address rural and frontierMCH training needs: the Rocky MountainPublic Health Education Consortium(RMPHEC). Matern Child Health J.2011;15(7):845---850.
16. Shinnamon A, Gelmon S, Holland B.Methods and Strategies for Student As-sessment. San Francisco, CA: Community-Campus Partnership for Health; 1999.
17. Kiely R. A transformative learningmodel for service-learning: a longitudinalcase study. Mich J Community Serv Learn.2005;12(1):5---22.
18. Ottenritter NW. Service learning,social justice, and campus health. J AmColl Health. 2004;52(4):189---191.
COMMENTARY
Supplement 1, 2015, Vol 105, No. S1 | American Journal of Public Health Sabo et al. | Peer Reviewed | Commentary | S43





























