Embed Size (px)
Citation preview

The Journal of Arthroplasty Vol. 14 No. 4 1999
Eliminating Patellofemoral Complications in Total Knee Arthroplasty
Clinical and Radiographic Results of 121 Consecutive Cases Using the Duracon System
M i c h a e l A. M o n t , M D , T a e k - R i m Y o o n , M D , K e n n e t h A. K r a c k o w , M D ,
a n d D a v i d S. H u n g e r f o r d , M D
Abstract: This study reports the minimum 5-year follow-up of our experience with the Duracon Total Knee Arthroplasty System. A total of 121 consecutive total knee replacements using the Duracon system (Howmedica, Rutherford, N J) were per- formed in 104 patients. Three patients died before the 5-year follow-up and were excluded from the final evaluation. The remaining 118 knees (10i patients) were assessed at a mean follow-up of 65 months (range, 60-80 months). The knee diagnoses were osteoarthritis in 97 patients, rheumatoid arthritis in 2 patients, osteonecrosis in 1 patient, and pigmented villonodular synovitis in 1 patient. The mean age was 70 years (range, 28-85 years). There were no reoperations for aseptic loosening, and there have been no reoperations for patellofemoral problems. At final follow-up evaluation, 112 knees (96%) had good or excellent results, and 6 knees (4%) had poor clinical results or went on to revision. For the surviving knees, the preoperative Knee Society objective score improved from a mean of 52 points (range, 20-72 points) to a final follow-up mean of 94 points (range, 66-100 points). Five knees needed reoperations: 2 knees in I patient because of acute hematogenous infection at 12 months, 1 knee because of a supracondylar femur fracture, 1 because of a patellar tendon rupture, and 1 to increase polyethylene thickness because of instability. The lack of aseptic loosening at the minimum 5-year follow-up compares favorably with any cemented or cementless series of knee replacement. The almost complete absence of patellofemoral complications in this series also indicates that the design changes, with particular attention to the trochlea design and patellofemoral contact throughout full flexion, have achieved their intended purpose. The results are encouraging at midterm, awaiting true long-term (15-20 years) follow-up. Key words: total knee arthroplasty, trochlear groove, patellofemoral joint.
The m o d e m era of total knee arthroplasty (TKA) began in the late 1960s and early 1970s with the introduction of the ICLH (Howmedica, Rutherford,
From the Department of Orthopaedic Surgery, Division of Arthritis Surgery, The Johns Hopkins University School of Medicine, The Good Samaritan Hospital, Baltimore, Maryland.
Submitted March 9, 1998; accepted October 6, 1998. Reprint requests: David S. Hungerford, MD, Department of
Orthopaedic Surgery, The Good Samaritan Hospital, 5601 Loch Raven Boulevard, Baltimore, MD 21239. E-mail: DHunger@ JHMI.edu
Copyright © I999 by Churchill Livingstone ® 0883-5403•99• 1404-0007510.00/0
N J), Townley Anatomic (Depuy, Warsaw, IN), and Total Condylar prostheses (Howmedica, Rutherford, N J) [1-6]. These prostheses had in c o m m o n uncon- strained resurfacing of all 3 compartments of the knee. Prior arthroplasties included hinged prosthe- ses with high infection [7] and aseptic loosening rates [8] and unicompartmental and bicompartmen- tal prostheses, which did not address the patello- femoral articulation [9,I0]. Although long-term (15-20 years) follow-up studies of some of these early prosthetic iterations from highly specialized centers have codified the validity of the concepts, other reports from that time showed significant
446

Eliminating Patellofemoral Problems inTKA • Mont et al. 447
short-term and long-term complications [lI-19]. Moreover, none of these early prostheses continue in clinical use.
Evolution of designs, and particularly instrumen- tation, for the accurate triaxial placement of the components has led to the current state of high achievement for TKA [ 13,17,18,20]. The problems with the metal-backed patellar components from the I980s, producing excessive wear, patellar plastic wear-through, component fracture, and metallosis, are well documented [21-30]. The problems with the extensor mechanism were only heightened by the inherent weakness of metal backing. The early tricompartmental prostheses were intended only to obtain and usually achieved 90 ° flexion [31]. Pa- tients and surgeons wanted more flexion. Conse- quently, in full flexion (> 110°), the patella is drawn into contact with the margins of the intercondylar notch, a position for which these early components were not originally designed. In 1988, Brick and Scott [22] reported that patellofemoral complica- tions constituted up to 50% of all TKA complica- tions. Mokris et al. [32] reported a 3% patellar reoperation rate for a modern total knee replace- ment followed 3 to 6 years. We report the minimum 5-year follow-up results of the Duracon Total Knee Prosthesis, which has design characteristics that specifically address normal kinematics of the patello- femoral joint throughout a full range of knee flex- ion.
Materials and Methods
Prosthesis
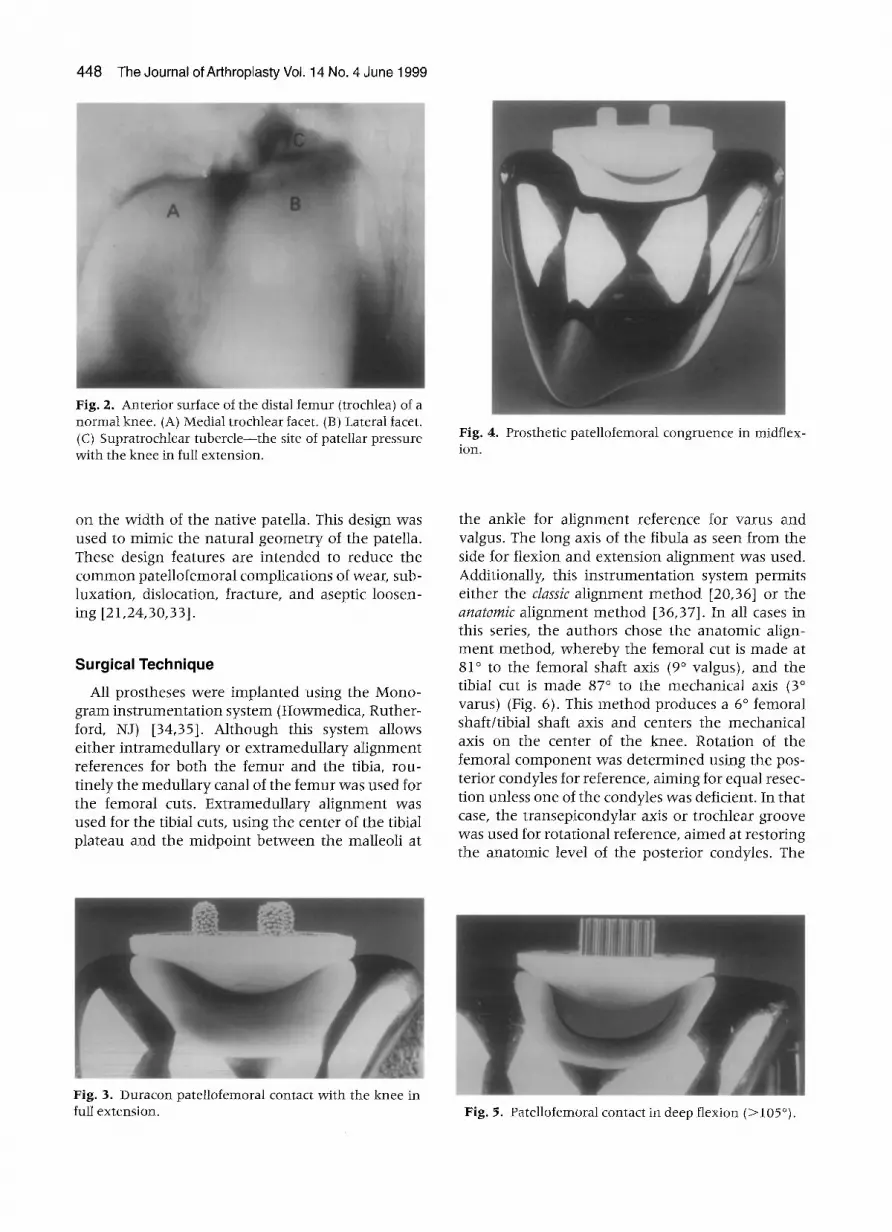
The Duracon Total Knee System is a modular tricompartmental design with both porous-coated and non-porous-coated components for use with or without cement according to the surgeon's choice. The tibial component design was available with cruciform stem design or a universal compo- nent with available modular stems. The femoral component was available with or without a cruciate- substituting box. In this series, only a cruciate- sparing design was used. The femoral component has a unique anterior flange, which is designed to accommodate the normal tracking of the patella, which begins lateral to the patellofemoral groove (Fig. 1). The lateral-proximal trochlea accommo- dates the lateral position of the patella with the knee in full extension and the quadriceps tightened (Fig. 2). The lateral flange then guides the patella into the trochlear groove as knee flexion draws the patella distally (Fig. 3). The contour of the trochlear groove is designed to make congruent contact with the polyethylene of the patelIar component or with the articular cartilage of the unresurfaced patella (Fig. 4). The concave shape of the medial and lateral margins of the trochlea are blended onto the lateral margin of the medial condyle and the medial mar- gin of the lateral condyle to provide congruent contact between the patellar surface (replaced or unreplaced) in deep flexion ( > l l 0 °) (Fig. 5). The patellar component was an all-polyethylene, oblong- shaped prosthesis that came in 3 sizes, dependent
Demographics
Between July 1, I991, and April 30, 1992, 121 Duracon Total Knee Prostheses (Howmedica, Ruth- erford, N J) were consecutively implanted by the authors in 104 patients. Three patients died before 5-year follow-up and were excluded from the final evaluation. All 3 patients had knees that were functioning well (Knee Society Scores >85 points) at the time of death. The remaining 118 knees (101 patients) were assessed at a minimum 5-year fol- low-up (mean, 65 months; range, 60-80 months). All patients were interviewed; were examined; had x-rays taken; and filled out a standardized question- naire that allowed evaluation of activity levels, degree of satisfaction, and total function scores. The diagnosis was osteoarthritis in 97 patients (113 knees), rheumatoid arthritis in 2 patients (3 knees), osteonecrosis in 1 patient (1 knee), and pigmented villonodular synovitis in 1 patient (1 knee). The mean age was 70 years (range, 28-85 years), and there were 38 men and 63 women.
Fig. 1. View of the trochlear flange of the femoral component. Note the unique proximal-lateral pad, which corresponds to the supratrochlear tubercle in Fig. 2.
448 The Journal ofArthroplasty Vol. 14 No. 4 June 1999
Fig. 2. Anterior surface of the distal femur (trochlea) of a normal knee. (A) Medial trochlear facet. (B) Lateral facet. (C) Supratrochlear tubercle--the site of pateltar pressure with the knee in full extension.
Fig. 4. Prosthetic patellofemoral congruence in midflex- ion.
on the width of the nat ive patella. This design was used to mimic the natural geomet ry of the patella. These design features are in tended to reduce the c o m m o n patel lofemoral complications of wear, sub- luxation, dislocation, fracture, and aseptic loosen- ing [21,24,30,33].
Surgical Technique All prostheses were implanted using the Mono-
gram ins t rumenta t ion system (Howmedica, Ruther- ford, NJ) [34,351. Al though this system allows ei ther in t ramedul lary or ex t ramedul lary a l ignment references for both the f emur and the tibia, rou- t inely the medul la ry canal of the femur was used for the femoral cuts. Extramedul lary a l ignment was used for the tibial cuts, using the center of the tibial plateau and the midpoint be tween the malleoli at
the ankle for a l ignment reference for varus and valgus. The long axis of the fibula as seen f rom the side for flexion and extension a l ignment was used. Additionally, this ins t rumenta t ion system permits ei ther the classic al ignment m e t h o d [20,36] or the anatomic al ignment m e t h o d [36,37]. In all cases in this series, the authors chose the ana tomic align- m e n t method , whe reby the femoral cut is made at 81 ° to the femoral shaft axis (9 ° valgus), and the tibial cut is made 87 ° to the mechanica l axis (3 ° varus) (Fig. 6). This m e t h o d produces a 6 ° femoral shaft/tibial shaft axis and centers the mechanical axis on the center of the knee. Rotat ion of the femoral c o m p o n e n t was de te rmined using the pos- terior condyles for reference, a iming for equal resec- tion unless one of the condyles was deficient. In that case, the t ransepicondylar axis or t rochlear groove was used for rotat ional reference, a imed at restoring the ana tomic level of the posterior condyles. The
Fig. 3. Duracon patellofemoral contact with the knee in full extension. Fig. 5. Patellofemoral contact in deep flexion (>105°).

Eliminating Patellofemoral Problems in TKA • Mont et al. 449
posterior condyles were also used as a reference for antero-poster ior posit ioning of the femoral compo- nents. Ligament balance was achieved by measured resection, that is, mainta in ing the level of the distal and femoral joint lines by resecting a quant i ty of bone to equal the thickness of the distal and poste- rior femoral c o m p o n e n t (Fig. 7). Any residual liga- m e n t instability encounte red at trial reduct ion was resolved by loosening the tight l igament and im- plant ing a thicker modu la r tibial insert.
Patellar Preparation
No specific ins t rumenta t ion was used for the patellar resurfacing. Because the patellar compo- nen t comes in 3 sizes, 3 templates were used to drill peg holes for the 3 pegs. One was found medial and 2 lateral for each of these different-sized patellar components . Resection of the patella was per- formed in all cases wi th the knee flexed and the patella everted, a posit ion that facilitates stabiliza- t ion of the patella for cutting. An assistant used 2 towel clips placed in the extensor m e c h a n i s m proxi- mal and distal to the patella for fur ther stabilization of the bone for the oscillating saw-cuts. The goal was to resect the min imal a m o u n t of bone to excise the facets and create a flat surface for the seating of the component . The patellar c o m p o n e n t was posi- t ioned wi thout mediolateral tilt and in the center of the nat ive bone proximal ly and distally. Positioning was slightly medial in some cases because the
Fig. 7. With the measz~red resection method of ligament balance, the distal and posterior joint levels are restored by resection of bone, equal to the thickness of the prosthesis.
medial border of the c o m p o n e n t was always co- apted with the medial border of the remain ing bone. Adequate rotat ion was ascertained with the patella posit ioned over tlhe femoral component . Tracking was ascertained with all trial componen t s in place, checking for stability of the patellar c o m p o n e n t to lateral migrat ion th roughou t the entire range of mot ion. If necessary, 2 t empora ry sutures were used to oppose the extensor m e c h a n i s m to check for this tracking th roughou t the range of mot ion. The goal was for the patellar c o m p o n e n t to stay located within the troch][ear groove wi thout any lateral finger pressure (no thumbs technique). If there was still a t endency for lateral subluxat ion or dislocation of the patella, a lateral ret inacular release was used (18 cases, 15%).
Fig. 6. Schematic diagram of normal limb alignment. The typical resection orientation for the anatomic alignment method parallels the joint line (T).
Fixation
The various combinat ions of cemented or cement- less fixation for all patients are outl ined in Table 1. The decision to use cemented or cementless fixation was based on an evaluat ion of the parameters of age, bone quality, and c o m p o n e n t stability. If the femoral bone was of poor quality or the stability of the trial c o m p o n e n t was suboptimal, the femoral c o m p o n e n t was cemented. For patients younger than age 50 years, a cementless tibial c o m p o n e n t was considered. In 18 cases, a decision was made not to resurface the patella based on preservat ion of patellar articular cartilage. The patellar c o m p o n e n t

450 The Journal of Arthroplasty Vol. 14 No. 4 June 1999
Table l. Method of Fixation
C o m p o n e n t No. Age (y)
Femur (n = 118) Cemen ted 70 70 (31-85) Cement less 48 68 (28-84)
Tibia (n = 118) Cemen ted 91 69 (28-85) Cement less 27 68 (48-82)
Both cemen ted 70 Both u n c e m e n t e d 27 Hybrid ( f e m u r - - n o t cemented; 21
t ib ia - -cemented) Patella (n = 118)
Cemen ted 96 Metal back 3 No rep lacement 18 Prior patel lectomy 1
was cemented in all but 4 of the remaining knees (3 meta l -backed cementless, 1 prior patel lectomy).
Rehabilitation
Patients were al lowed 50% weight bearing in the first 6 weeks wi th the aid of a cane, crutches, or a walker. Patients were then advanced to full weight bearing wi thout ambula tory aids as tolerated. Range- of -mot ion exercises were begun on the second postoperat ive day. A cont inuous passive mot ion machine was not used.
Clinical Evaluation
Final fol low-up was either by clinic a t tendance ( 100 patients) or by te lephone contact wi th both the pat ient and his present or thopedic surgeon (1 pa- t ient) . All pa t ien ts we re eva lua ted using the Knee Society objective and functional rating scales {38]. A score of 90 points or more was considered an excel lent outcome; a score be tween 80 and 89 points was considered a good outcome; a score of 70 to 79 points was considered a fair outcome; and a score fewer than 70 points was considered a poor outcome. All patients wi th scores of fewer than 80 points were considered unsuccess- ful clinical outcomes as were any knees requiring a revision procedure. Scores of 80 points or more were considered successful clinical outcomes.
Funct ional evaluat ion used a modificat ion of the Charnley classification as applied to the knee [39]. Class A denoted unilateral disease of the knee, class B denoted bilateral knee involvement , and class C denoted mult iple system or joint invo lvement that compromised the patient 's ability to ambulate .
Radiographic Analysis
Each postoperat ive and final fol low-up TKA was analyzed radiographically on long-standing antero- posterior, s tandard lateral, and axial patellar views. Fluoroscopically posit ioned anteroposter ior and lat- eral views were used as necessary to v iew the b o n e - c e m e n t - p r o s t h e s i s interface. More specifi- cally, the following radiographic parameters (which are described in detail in the appendix) were exam- ined [36]: mechanical axis, femoral anteroposter ior al ignment, and lateral femoral and tibial angles. Zonal analysis of all componen t s was used to evalu- ate progressive radiolucencies {36,40].
Results
Clinical Results
Overall, 5 knees needed reoperations; 2 knees in I pat ient were revised because of late hematog- enous infection at 12 months , 1 knee because of a supracondylar f emur fracture 2 years after surgery, 1 because of a patellar t endon rupture, and 1 because a polyethylene insert change was needed. At final fol low-up evaluation, 112 knees (96%) had good or excellent clinical results, and 6 knees (4%) had poor clinical results or wen t on to revision. For the surviving knees, the preoperat ive Knee Society objective score improved f rom a m e a n of 52 points (range, 20-72 points) to a final fol low-up m e a n of 94 points (range, 6 6 - I 0 0 points). The Knee Society total funct ion score improved f rom a m e a n of 42 points (range, 0-80 points) preoperat ively to a m e a n of 70 points (range, 0-100 points) at final follow-up. Range of mot ion improved f rom a m e a n of 92 ° flexion Preoperat ively (range, 30°-125 °) to a m e a n of 110 ° flexion postoperat ively (range, 60 °- 130°).
Charnley class C patients showed a statistically significant lower functional score than patients in Charnley classes A or B (P < .001). There were no differences no ted w h e n various other clinical or demographic factors were correlated wi th clinical success or failure. These factors included me thod of fixation, pat ient weight, and activity indices (dis- tance and impact) (Table 2).
Reoperations
There were no reoperat ions for aseptic loosening, and there have been no reoperat ions for patello- femoral problems. One 52-year-old pat ient wi th rheuma to id arthritis had a po lye thy lene insert change w h e n 2 years after operat ion he was no ted

Eliminating Patellofemoral Problems in TKA • Mont et al. 451
Table 2. Results by Various Functional Parameters
Final Functional Parameter Preoperative Fol low-up
Pain None 0 80 Mild-occasional 0 38 Moderate-tolerable 65 0 Marked-serious limitations 53 0 Totally disabling pain 0 0
Limp None 6 92 SIight 26 19 Moderate 61 6 Severe 23 I Unable to walk 2 0
Support None 43 95 Cane for long walks 16 15 Cane most of time 40 4 1 Crutch 7 1 2 Canes 4 1 2 Crutches or walker 6 2 Unable to walk 2 0
Stair climbing Unsupported 18 65 Unilateral support 81 48 In any manne r 16 5 Unable to climb stairs 3 0
Distance walked Unlimited 14 74 6-20 Blocks 41 20 2-5 Blocks 1 i 14 1 Block 33 10 Indoors only 17 0 Unable to walk 2 0
Activity level Requires assistance for all 0 0
activities Self-care independent 1 2 Indoor activities of daily 15 5
living Outdoor activities of daily 73 69
living Low hip stress sports 28 40 High hip stress sports 1 2
to have medial / la teral instability in flexion and extension. A 9 - m m spacer was upgraded to an l l - m m spacer wi thou t complications. At 3 years after spacer change, he has a Knee Society objective score of 97 points. A 49-year-old w o m a n with insul in-dependent diabetes had a p resumably hema- togenous infection of both prostheses requiring bilateral 2-stage exchange ar throplas ty 3 years after her p r imary knee arthroplasties. Presently, she is free of infection at 2 years pos texchange wi th Knee Society objective scores of 84 and 86 points. One pat ient wi th severe systemic osteoporosis and a history of mult iple lumbar compress ion fractures suffered a supracondylar f emur fracture requiring conversion to a l ong - s t emmed modu la r c o m p o n e n t
2 years after surgery. The fracture is healed, but knee funct ion is poor at 2 years ' fol low-up (Knee Society objective score of 62 points). Another pa- t ient wi th rheumato id arthritis u n d e r w e n t bilateral knee replacements and re rup tured her left patellar t endon following a fall 2 weeks after surgery. Pri- m a r y repair was unsuccessful, but a second surgery in which the semitendinosus and gracilis tendons were used to supp lement the repair was successful. At 5 years after this repair, the pat ient has a Knee Society objective score of 82 points.
Radiographic Results
A minimal ly displaced fracture of the patella was no ted in 1 pat ient on x- ray at 11 mon ths postsur- gery, but no fur ther t r ea tmen t was needed. The pat ient present ly has a Knee Society objective score of 92 points at final fol low-up of 66 months . Apparently, this fracture was secondary to overresec- t ion of the patella at the p r imary surgery (Fig. 8). On radiographic evaluation, heterotopic ossification was noted in 2 knees, one of the patellar t endon and the other of the quadriceps mechanism. The 2 patients have slightly lower mot ion than the group (96 ° and 94 ° arc of mot ion) but are otherwise doing well wi th Knee Society objective scores of 92 and 94 points.
Alignment
There were 60 knees wi th min imal deformity (range, 30-9 ° of neut ra l b iomechanical axis). There were 36 varus knees (>3 ° varus deformity) wi th a m e a n a l ignment of 11.1 ° (range, 0-26 °) and 22 valgus knees wi th a m e a n a l ignment of 12.4 ° (range, 0-37°). Postoperatively, femoral antero-poster ior a l ignment averaged 98.8 ° (goal, 99°; range, 95 ° to 102 °) wi th only 1 pat ient outside the range of _+3 °. Lateral femoral angles average 0.54 ° . No pat ient was outside the range of +_3 °. Antero-poster ior tibia angle averaged 87 ° (goal, 87 °) wi th only 1 pat ient outside the goal of _+3 ° . Lateral tibia angle was 86 ° (goal, 87 ° ) wi th all patients wi thin _+3 ° . The me- chanical axis (center of hip to center of ankle) was wi thin +_1 cm of the center of the knee in all patients.
Radiolucencies
Radiolucencies were found a round 35% of the cemented femurs and 40% of the cementless fe- murs (Table 3). Tihese were small (<2 m m ) and nonprogress ive and found most ly in zones 1 and 4 (Fig. 9). Radiolucencies were found a round 24% of the cemented tibial componen t s and 16% of the

452 The Journal of Arthroplasty Vol. 14 No. 4 June 1999
Fig. 8. (A) Lateral radiograph of the patella in the immediate postoperative period. (B) Minimally dis- placed distal pole stress fracture found incidentally on the 6-month follow-up film.
cementless tibial components . These were also small and nonprogress ive and typically found in zone 1. No componen t s had complete or progressive radio- lucencies. Covering the patellar components , for the 103 that were resurfaced, 1 unde rwen t a fracture as previously described. Radiolucencies a round the patellar c o m p o n e n t were found a round 12% of the 96 cemented cases. These were all small (<2 ram) and nonprogressive, and there were no radiolucen- cies visualized in the knee cementless meta l -backed patella cases.
Discussion
Throughout the history of m o d e r n total knee replacement , the most f requent ly repor ted compli- cations involve the patel lofemoral joint [16,21- 24,26-30,33,41-43] . The earliest designs of TKA ignored the extensor articulation completely. The
Table 3. Radiolucencies Around Components
Femoral Radiolucent Zone No.
zone 1 25 zone 2 2 zone 3 1 zone 4 22
Tibial Radiolucent Zone
(Anteroposterior) zone 1 22 zone 2 8 zone 3 5 zone 4 6
Geomedic (Howmedica, Rutherford, N J), M a r m o r Modular (Smith & Nephew (Richards) Memphis , TN), and Polycentric prostheses (Howmedica, Ruth- erford, NJ) all had in c o m m o n no provision for rep lacement of the patel lofemoral joint. The early t r icompar tmenta l prostheses, such as the Total Con- dylar (Howmedica, Rutherford, N J), Townley Ana- tomic (Howmedica, Rutherford, NJ), and Kinemat ic prostheses (Howmedica, Rutherford, N J), provided a t rochlear flange for the femoral c o m p o n e n t and a
Fig. 9. Lateral radiograph of a femoral component show- ing minimal (nonprogressive) radiolucencies opposite the trochlea and posterior condyle.

Eliminating Patellofemoral Problems inTKA • Mont et al. 453
polyethylene component to resurface the patella. Attention, however, had not been directed toward the patellofemoral articulation with the knee either in full extension with the quadriceps muscle con- tracted or in full flexion with the patella contacting the margins of the intercondylar notch (Fig. 10) or throughout the full course of motion of the knee.
The design of the Duracon prosthesis has focused on the patellofemoral articulation throughout the full range of motion. In the normal knee, with the leg in full extension and the quadriceps muscle contracted, the patella articulates with the lateral distal femoral metaphysis proximal and lateral to the trochlea (Fig. 2). There is characteristically an impression in the prefemoral fat pad that marks this point of contact. As the knee is flexed, the patella is drawn medially and distally to engage the trochlea with a concentric contact pattern over the width of the patellar articular cartilage. After 90 ° flexion, the patella comes out of contact with the distal end of the trochlea and engages the lateral margin of the medial condyle and the medial margin of the lateral condyle. In this way, the patella enjoys a broad, stable contact with the femur throughout its exten- sive course of motion. TKA design has only lately recognized the necessity to respect the details of these naturally occurring phenomena to minimize the complications involving the extensor mecha- nism.
The almost complete absence of patellofemoral complications in this series at the minimum 5-year
follow-up indicates that the design goals, with particular attention, to the trochlea and the patello- femoral contact areas, have achieved their intended purpose. The only minor complication involving this articulation consisted of a patellar stress fracture that required no alteration in treatment in a well- functioning knee. We believe that some of the design changes described (deepening of the troch- lear groove, conforming patella) may account for the excellent results found in this report. The senior authors had both performed more than 1,000 knee replacements before the use of this prosthesis with similar instrumentation. Therefore, we do not believe that the excellent results are necessarily due to any changes in the instrumentation or surgical technique.
In the present study, all patellae were medialized by lining up the medial edge of the component with the medial edge at the patella. The incidence of lateral release was low in the present series (15%), which is in agreement with a study by Hofmann et al. {44], who found that medialization lowered the incidence of ]atera
454 The Journal of Arthroplasty Vol. 14 No. 4 June 1999
A l i g n m e n t of t he k n e e is desc r ibed in t e rms of the t i b i o f e m o r a l angle . The f e m o r a l shaft axis was de- f ined as a l ine d r a w n b e t w e e n a p o i n t in t he c e n t e r of t he p r o x i m a l f e m o r a l shaf t a n d the c e n t e r of t h e knee . The m e c h a n i c a l axis a t t he l o w e r leg was de f i ned as the l ine b e t w e e n the c e n t e r of t he k n e e a n d the c e n t e r of t he ank le . The t i b i o f e m o r a l ang le was m e a s u r e d as t he ang le f o r m e d at t he k n e e b y the i n t e r s e c t i o n of t he f e m o r a l shaft a n a t o m i c axis a n d the m e c h a n i c a l axis of t he l o w e r leg. A n y d e v i a t i o n of t he l ine f rom the c e n t e r of t he f e m o r a l h e a d to t he cen t e r of t he k n e e a n d the l ine f rom the cen t e r of t he k n e e to t he c e n t e r of t he a n k l e was
c o n s i d e r e d a va rus or va lgus de formi ty . The a m o u n t of t ibial a n d f e m o r a l c o m p o n e n t
d e f o r m i t y in t he co rona l p l a n e was ca l cu l a t ed b y m e a s u r e m e n t s of j o i n t - l i n e angles . F e m o r a l (a lpha) a n d t ibial (beta) j o i n t - l i n e angles w e r e also m e a - sured . Beta angles of 84 ° to 90 ° w e r e c o n s i d e r e d to be in t he normal range . Ou t s ide t h e s e va lue s w e r e va rus or va lgus a b n o r m a l i t i e s of t ibia l c o m p o n e n t p l a c e m e n t . A l p h a angles of 91 ° to 100 ° w e r e cons id- e r ed n o r m a l . Outs ide t hese va lues w e r e va lgus or va rus a b n o r m a l i t i e s of f e m o r a l c o m p o n e n t p l ace -
m e n t .
References
1. Freeman MAR, McLeon HC, Levari JB: Cementless fixation of ICLH tibial component. Orthop Clin North Am 13:141, 1982
2. Gibbs AN, Green GA, Taylor JG: A comparison of the Freeman/Swanson (ICLEI) and Waldius prosthesis in total knee replacement. J Bone Joint Surg Br 61:358, 1979
3. Goldberg VM, Henderson BT: The Freeman-Swanson ICLH total knee arthroplasty. J Bone Joint Surg Am 62:1338, I990
4. Levai JP, Freeman MA: Patellar complications of ICLH knee prosthesis. Rev Chir Orthop Reparatrice Appar Mot 70:41, I984
5. Ranawat CS, Shine J: Duo-condylar total knee arthro- plasty. Clin Orthop 94:185, i973
6. Townley C: Total knee arthroplasty. Clin Orthop 236:8, i988
7. Deburge A: GUEPAR hinge prosthesis: complications and results with two year follow-up. Clin Orthop 120:47, 1976
8. Ducheyne P, Kagan A, Lacey JA: Failure of total knee arthroplasty due to loosening and deformation of tibial component. J Bone Joint Surg Am 60:384, 1978
9. Callahan CM, Drake BG, Heck DA, et al: Patient outcomes following unicompartmental or bicompart- mental knee arthroplasty: a meta analysis. J Arthro- plasty I0:141, 1995
I 0. Heck DA, Marmor L, Gibson A, et al: Unicompartmen- tal knee arthroplasty: a multicenter investigation
with long term follow-up evaluation. C/in Orthop 286:154, 1993
11. Blunn GW, Joshi AB, Minns RJ, et al: Wear in retrieved condylar knee arthroplasties: a comparison of wear in different designs of 280 retrieved condylar knee prostheses. J Arthroplasty 12:281, 1997
12. Ewald FC, Jacobs MA, Miegel RE, et al: Kinematic total knee replacement. J Bone Joint Surg Am 66:1032, 1984
13. Insall JN, Kelly M: The total condylar prosthesis. Clin Orthop 205:43, 1986
14. Insall JN, Lachiewcz PE Burstein AH: The posterior stabilized condylar prostheses: a modification of the total condylar design: two to four year clinical experi- ence. J Bone Joint Surg Am 64:1317, 1982
15. Malkani AL, Rand JA, Bryan RS, Wallrichs SL: Total knee arthroplasty with the kinematic condylar pros- thesis: a ten-year follow-up study. J Bone Joint Surg Am 77:423, 1995
16. Moreland JR: Mechanisms of failure in total knee arthroplasty. Clin Orthop 226:49, 1988
17. Ranawat CS, Boachie-Adjei O: Survivorship analysis and results of total condylar knee arthroplasty: eight- to 11-year follow-up period. Clin Orthop 226:6, 1988
18. Ranawat CS, Flynn WE Saddler S, et al: Long-term result of the total condylar knee arthroplasty: a 15-year survivorship study. Clin Orthop 286:94, 1993
19. Rand JA, Ilstrup DM: Survivorship analysis of total knee arthroplasty: cumulative rates of survival of 9200 total knee arthroplasties. J Bone Joint Surg Am 73:397, 1991
20. Krackow KA: The technique of total knee arthro- plasty. CV Mosby, St. Louis, I990
21. Bayley JC, Scott RD, Ewald FC, Homes GB: Failure of metal-backed patellar component after total knee replacement. J Bone Joint Surg Am 70:668, 1988
22. Brick GW, Scott RD: The patellofemoral component of total knee arthroplasty. Clin Orthop 231:163, 1988
23. Clayton ME, Thimpathi R: Patellar complications after total condylar arthroplasty. Clin Orthop 170:152, 1982
24. Healy WL, Wasilewski SA, Takei R, Oberlander M: Patellofemoral complications following total knee arthroplasty: correlation with implant design and patient risk factors. J Arthroplasty 10:197, 1995
25. Krackow KA, Hungerford DS: Uncemented total knee arthroplasty: a two to eight year survey and analysis of multi-center, multi-system result. Am J Knee Surg 1:42, 1988
26. Lee TQ, Gerken AP, Glaser FE, et al: Patellofemoral joint kinematics and contact pressures in total knee arthroplasty. Clin Orthop 340:257, 1997
27. Lombardi AV Jr, Engh GA, Volz RG, et al: Fracture/ dissociation of the polyethylene in metal-backed patellar components in total knee arthroplasty. J Bone Joint Surg Am 70:675, 1988
28. Rader CP, Lohr J, Wittman R, Eulert J: Results of total knee arthroplasty with a metal-backed patellar com- ponent: a 6-year follow-up study. J Arthroplasty 11:923, 1996

Eliminating Patellofemoral Problems in TKA • Mont et al. 455
29. Ranawat CS: The patellofemoral joint in total condylar knee arthroplasty: pros and cons based on five- to ten- year follow-up observations. Clin Orthop 205:93, 1986
30. Stulberg SD, Stulberg BN, Hamati Y, Tsao A: Failure mechanisms of metal-backed patellar components. Clin Orthop 236:88, 1988
31. Insall JN, Ranawat CS, Aglietti P, et al: A comparison of four models of total knee-replacement prostheses. J Bone Joint Surg Am 58:754, 1976
32. Mokris JG, Smith SW, Anderson SE: Primary total knee arthroplasty using the Genesis Total Knee Ar- throplasty System: 3 to 6 year follow-up study of 105 knees. J Arthroplasty 12:9 I, 1997
33. Rosenberg AG, Andriacchi TP, Barden R, Galante JO: Patellar component failure in cementless total knee arthroplasty. Clin Orthop 236:106, 1988
34. Hungerford DS, Kenna RV: Preliminary experience with a total knee prosthesis with porous coating used without cement. Clin Orthop 176:95, 1983
35. Hungerford DS, Krackow KA, Kenna RV (eds): Total knee arthroplasty: a comprehensive approach. Wil- liams & Wilkins, Baltimore, 1984
36. Mont MA, Fairbank AC, Yammamoto V, et al: Radio- graphic characterization of aseptically loosened cement- less total knee replacement: a comparison to a directly matched control group. Clin Orthop 321:73, 1995
37. Bargren JH, Blaha JD, Freeman MAR: Alignment in total knee arthroplasty: correlated biomechanical and clinical observations. Clin Orthop 173:178, 1983
38. Insall JN, Dorr LD, Scott RS, Scott WN: Rationale of the Knee Society clinical rating system. Clin Orthop 248:13, 1989
39. Dorr LD, Takei GK, Conaty JP: Total hip arthroplasties in patients less than forty-five years old. J Bone Joint Surg Am 65:474, I983
40. Ewald FC: The Knee Society total knee arthroplasty roentgenographic evaluations scoring system. Clin Orthop 248:9, 1989
41. Hsu RW-W, Fan G-E Ho W-P: A follow-up study of porous-coated anatomic knee arthroplasty. J Arthro- plasty 10:29, 1995
42. Karachalios T, Sarngi PP, Newman JH: Severe varus and valgus deformities treated by total knee arthro- plasty. J Bone Joint Surg Br 76:938, 1994
43. Kjaersgaard-Andersen P, Hvid I, Wethelund J-O, Snep- pen O: Total condylar knee arthroplasty in osteoarthri- tis: a four-to-six year follow-up evaluation of 103 cases. Clin Orthop 238:167, I989
44. Hofmann AA, Tkach TK, Evanich C J, et al: Patellar component medialization in total knee arthroplasty. J Arthroplasty 12:155, 1997





























