Embed Size (px)
Citation preview
Sertraline Safety and Efficacy in Major Depression: A Double-Blind Fixed-Dose Comparison with Placebo
Louis F. Fabre, F.S. Abuzzahab, M. Amin, J.L. Claghorn, J. Mendels,
William M. Petrie, S. Dub6, and Joyce G. Small
In a 6-week, randomized, double-blind, multicenter trial, sertraline 50 mg, IO0 mg, or 200 mg, or placebo, wa~ administered once daily to 369 patients with DSM-lll-defined major depression. Efficacy variables included changes from baseline scores for total Hamilton Rating Scale for Depression (HAMD). HAMD Bech Depression Cluster, Clinical Global Impressions (CGI) Severity, CGI Improvement, and Profile of Mood States Depression/ Dejection Factor. For the evaluable-patients analysis, all sertraline groups showed signifi- cantly (p < 0.05 or better) greater improvements in all efficacy variables except one when compared with the placebo group. For the all-patients analysis, all efficacy variables in the 50 mg group were statistically signi[icantly (p < 0.05) better than placebo. Side effects increased with increasing dosage but were usually mild and well tolerated. The results of this study show that sertraline 50 mg once daily is as effective as higher dosages Cbr the treatment of major depression with )ewer side effects and therapy discontinuations.
Key Words: Major depression, selective serotonin reuptake inhibitor, sertraline
BIOL PsvcrnArr'~ 1995:38:592-602
Introduction Neurotransmission is influenced by the rate of neurotrans- mitter synthesis, neurotransmitter concentration in the synapse, rates of neurotransmitter reuptake and break- down, and number and affinity of target postsynaptic receptors to which a particular neurotransmitter can bind (Richelson 1988). Research findings suggest depression may be associated with decreased functional neurotrans- mission that results from depletion of the availability ofaminergic neurotransmitters--dopamine, norepineph-
From the Fabre Research Clinics Inc.. Hl~ush,n, Texas, Address reprint requests to Louis F Fabre. MD. Phi), Fabrc Research Clinics Inc.
5503 Crawford, Houston, TX 77111)4. Received May 23, 1994; revised October 21, 19¢14
rine, serotonin--in the vesicles at the presynaptic nerve endings (Garver and Davis 1979).
The new antidepressant drugs known as selective sero- tonin reuptake inhibitors (SSRIs) have molecular struc- tures distinctly different from those of the standard tricy- clics or monoamine oxidase inhibitors and biochemical effects that are different from those customarily observed with the older classes of antidepressant agents. These new compounds make more serotonin functionally available [or receptor stimulation (Shopsin et al 19811, and their efficacy is equivalent to that of other drugs used to treat depressive disorders (Mendels 1987). The SSRIs, which include sertraline, fluoxetine, fluvoxamine, citalopram, and paroxetine (Lemberger et al 1985; Tulloch and John- son 1992), also exhibit fewer anticholinergic and cardio-
© 1995 Society of Biological Psvchiatr~ 0006-3223/95/$09.50 SSDI 0006-3223(95)00178-J

Sertraline for Major Depression BIOL PSYCHIATRY 593 1995;38:592-602
toxic side effects and, therefore, may be the preferred treatment in a variety of patients (Mendels 1987).
Sertraline hydrochloride (C 17 H ~ 7 N CI 2HC1) is a structur- ally unique and highly selective serotonin reuptake inhib- itor. Of the SSRIs approved for use in the United States, sertraline is the most selective agent with respect to blocking reuptake of serotonin over norepinephrine (Bolden-Watson and Richelson 1993). It is also one of the most potent inhibitors of serotonin reuptake, being 20 times more potent than amitriptyline, 10 times more potent than fluvoxamine, and 5 times more potent than fluoxetine (Koe et al 1983). Sertraline is 200 times less active than desipramine against norepinephrine reuptake, is weakly active against dopamine reuptake, and has no inhibitory effect on monoamine oxidase (Koe et al 1983). Sertraline has a low affinity for muscarinic receptors--60 times less than amitriptyline--and, therefore, has markedly lower anticholinergic activity. The major metabolite, desmethyl- sertraline, is over 20 times less potent than the parent compound in blocking serotonin reuptake and is consid- ered inactive as an antidepressant (Bolden-Watson and Richelson 1993).
In the open field test, an animal model of depression considered predictive of efficacy for antidepressant drugs, administration of sertraline attenuated the behavioral ef- fects of stress in rats (Kennett et al 1987). Sertraline exerts its antidepressant effects through a variety of mechanisms, including facilitation of serotonergic activity and induc- tion of downregulation of beta-adrenoreceptor systems (Koe et al 1987).
The average half-life of sertraline in healthy volunteers is 26 hours, with peak plasma concentrations occurring 5-8 hours after an oral dose. Single- and multiple-dose studies have shown linear pharmacokinetics, indicating consistent bioavailability over the recommended dose range (50-200 mg daily) (Fouda et al 1987).
The purpose of this study was to identify the dosage of sertraline that is most useful in clinical practice. The effectiveness, tolerability, and safety of three fixed dosage levels of sertraline (50, 100, 200 mg) given once a day for 6 weeks were compared to placebo. A portion of the data contained herein has been presented in poster format (Fabre 1991a) and as an abstract (Fabre 1991b); in addition, data from one of the eight centers have been published previously (Amin et al 1989).
Subjects and Methods
Subject Description A total of 369 patients (both symptomatic volunteers and patients already undergoing treatment) with major depres- sive disorder were entered into this 6-week, eight-center
study. The patient population consisted of 172 men and 197 women between the ages of 18 and 65 years. The women were postmenopausal, surgically sterile, or prac- ticing an adequate method of contraception. All subjects were required to meet the DSM-III (American Psychiatric Association 1980) criteria for major depressive disorder and to have a minimum score of 22 on the 17-item Hamilton Rating Scale for Depression (HAMD; Hamilton 1960) following an antidepressant drug washout period of 4-14 days; however, 11 patients entered double-blind treatment with HAMD scores less than 22, primarily because their symptoms improved between screening and baseline.
Excluded from the study were (1) pregnant or lactating women; (2) anyone taking concomitant psychotherapeutic medications or certain other concomitant medications; (3) those with a history of serious intolerance or resistance to any antidepressant drug or use of any other investigational drug in the 4 weeks preceding this study; (4) persons with a history of schizophrenia, schizoaffective disorders, or significant medical disease, including convulsive disor- ders; and (5) persons with continuous alcohol and/or drug abuse, including those experiencing recent symptoms of withdrawal.
Study Design This study was conducted in compliance with institutional review board and informed consent regulations, and all centers followed an identical protocol. Participants who had been previously receiving monoamine oxidase inhib- itors were required to undergo a single-blind placebo washout period of 2 weeks. Those previously receiving other psychoactive drugs or who had been receiving a monoamine oxidase inhibitor and had deteriorated clini- cally underwent a washout period of 1 week. All others went through a washout period of 4-14 days. The length of the washout period was determined based on the investigator's judgment.
Patients were randomly assigned to one of four groups of equal size and were placed on a regimen of placebo or sertraline, the latter in a fixed dosage of 50 mg, 100 rag, or 200 m g a day, without any period of upward titration. In the event of the occurrence of a clinically unacceptable reaction in which the patient's intolerance to study medi- cation was more than transient, study drug was discontin- ued. Those patients who discontinued before 2 weeks of active drug therapy because of inadequate response, inter- current medical problems, or unacceptable concomitant medications were replaced. All drug and placebo doses were prepared in identical capsules and administered once daily. If sleep-inducing medication was needed, patients were permitted only intermittent chloral hydrate, with the
594 BIOL PSYCHIATRY L.F. Fabre et al 1905"38:592-602
exception of the nights before psychiatric scale testing, when chloral hydrate was not allowed.
Data Collection
In order to assess efficacy, the HAMD scale, Clinical Global Impressions (CGI; Guy 1976) scale, and Profile of Mood States (POMS; McNair et al 1980) were adminis- tered at screening, baseline, and each week thereafter during the 6-week trial. Safety evaluations included inves- tigator observations and laboratory parameters. Electrocar- diography was performed, and temperature, supine and standing blood pressures, pulse rate, and weight were recorded at each visit. Laboratory tests, conducted at screening, baseline, and every 2 weeks during the study, included a complete blood count with differential, platelet count, serum chemistry (lactate dehydrogenase, serum glutamic oxaloacetic transaminase (SGOT), serum glu- tamic pyruvic transaminase (SGPT), alkaline phosphatase, total bilirubin, creatinine, blood urea nitrogen (BUN), glucose, and electrolytes), and a routine urinalysis. A physical examination was performed at baseline and at termination of the study.
Statistical Analysis
Efficacy variables included the change in total 17-item HAMD score from baseline to the last visit, the percentage change in total 17-item HAMD score from baseline to the last visit, the change in CGI Severity score from baseline to the last visit, the CGI Improvement score at the last visit, and the change in the POMS Depression/Dejection Factor score from baseline to the last visit. Scores were also calculated for the Bech Depression Cluster (Bech et al 1975), a 6-item subscale of the HAMD (items 1-depressed mood; 2-guilt; 7-work and interests; 8-retardation; 10- anxiety, psychic; and 13-somatic symptoms, general).
For safety data, formal statistical analyses were per- formed on vital signs data, body weights, and the compar- ative incidence of side effects for all side effects that occurred with an incidence of at least 3% in any of the sertraline dosing groups.
Two descriptive analyses of laboratory test results were also performed for each dosing group: the incidence of patients with clinically significant laboratory abnormali- ties and the mean change from baseline (pre-double- blind) to the final visit for each laboratory parameter.
Statistical analyses on efficacy variables were per- formed for both an evaluable-patients group and an all- patients group. Evaluable patients were classified as those who took study medication on or after the 1 lth day of the double-blind phase, who had efficacy assessments on or after study day 11, and who were not major protocol
violators. The all-patients group included those who took at least one dose of double-blind medication and had at least one double-blind efficacy assessment.
All safety evaluations, including descriptive statistics of laboratory test results and formal analyses of vital signs, body weights, and side effects incidence, were performed for an all-patients group that included all patients who took at least one dose of double-blind medication and had at least one relevant double-blind safety-related observa- tion.
HAMD and POMS variables were tested in a two-way analysis-of-variance (ANOVA) framework with PROC GLM of SAS followed by t tests on the least squares means via the ESTIMATE option (SAS Institute 1985). The CGI variables were analyzed nonparametrically with a Wilcoxon Rank Sum test blocked on center (Hollander and Wolfe 1973). The contrasts of interest were sertraline (both individual dosing level groups and all doses com- bined) versus placebo, and were assessed with two-sided significance. No adjustment of p values was made for multiple comparisons. The HAMD total scores at last visit were also analyzed in an analysis of covariance (AN- COVA) framework using the baseline HAMD total scores as covariates.
For the safety analyses, vital signs and body weight analyses were performed with a one-way ANOVA, while comparisons of side-effects incidence were performed with Fisher's Exact Test. For safety analyses, the quoted p values are two-sided.
Results
Patients
The demographic characteristics of the patients randomly assigned to a treatment group are shown in Table 1. Although depressive illness is diagnosed in twice as many women as men (American Psychiatric Association 1980), women made up only 53% of the study population. (Women of childbearing potential became eligible for entry about midway through the study.) Most patients were relatively young, with a mean age of 37.6 years. The mean weight for men was 80.2 kg; for women, 64.3. The racial composition of the trial population was 91% white, 7% black, and 2% other.
The largest segment (38%) of the patient population had a depressive illness for more than 10 years (Table 1), followed in order of incidence by 31% with 1-5 years' duration, 15% with 5-10 years' duration, and 14% with less than 1 year's duration. The average duration of depressive illness was 9.5 years.
The majority (64%) of patients (Table 1) were diag- nosed as having major depression, recurrent, with or
Sertraline for Major Depression BIOL PSYCHIATRY 595 1995;38:592-602
Table 1. D e m o g r a p h i c Character is t ics , Depress ive History, and Pr imary Psychia t r ic D iagnos i s for All Patients Enter ing Doub le -Bl ind The rapy
Sertraline
50 mg 100 mg 200 mg Placebo Parameter (n = 95) (n ~: 92) (n = 91) (n = t~l)
Sex Male 47 411 34 51 Female 48 52 5 7 4( I
Age (yr) 18-44 74 72 68 ~7 45- 64 2(I 20 23 24 >65 1 0 0 i) Mean age (yr) 37.3 37.1 38.6 37.3
Mean weight (kg) Male 77.t~ 82.4 77.3 83. I Female 63.t~ 64.4 64.7 64.2
Race White 91 85 81 7~ Black 2 6 7 11 Other 2 1 3 2
Duration of depressive history (yr)
< 1 21) N 8 15 1 5 22 31 3O 31 5-10 15 14 14 14 >10 34 38 38 3(I Not specified 4 I 1 1 Mean duration (yr) S.6 10.6 1(I.3 8.¢~
DSM-II1 classification Bipolar disorder, 1 _~, _ ~ .a
depressed Major depression. 36 2~ 27 33
single episode: With melancholia 7 7 5 8 Without melancholia 16 13 13 15 Unspecified as to 13 6 9 1 I)
melancholia Major depression, 58 f~3 62 55
recurrent: With psychotic II II [) 1
features With melancholia 21 I f~ 16 15 Without melancholia 26 3(I 28 21 Unspecified as to I 1 17 18 18
melancholia
without melancholic features. Fewer (33%) were diag- nosed as having major depression, single episode, and only 2% were diagnosed as having bipolar disorder, depressed. The distribution of those diagnoses did not vary appreciably among the four treatment groups.
The number of patients that entered double-blind treat- ment was 95 in the sertraline 50 rag/day group, 92 in the 100 rag/day group, 91 in the 200 rag/day group, and 91 in the placebo group. A total of 191 patients (52%) com- pleted the study (Table 2). Of the 369 patients randomly assigned to double-blind treatment, a total of 289 (78%)
Table 2. Completion and Discontinuation Rates for Patients Entering Double-Blind Therapy
No. of Patients (%)
Sertraline
50 mg 100 mg 200 mg Placebo (n = 95) (n = 92) (n = 91) (n = 9U
Cornpleters 59 (62) 47 (51) 39 (43) 46 (51) Evaluable patients" 82 (86) 75 (82) 56 (62) 76 (84) Discontinued 36 (38) 45 (49) 52 (57) 45 (49)
Lack of efficacy 14 (15) 18 (20) 9 (10) 25 (27) Side effects 10 (11) 15 (16) 33 (36) 4 (4) Laboratory - - - - - - 1 abnormalities Non-study- 12 (13) 10 (11) 10 (11) 15 (16)
medication-related t'
" Defined as patients who took study medication on or after the llth day of the double*blind phase, who had efficacy assessments on or after study day 11, and who were not major protocol violators.
J' Primarily patient default.
remained to be included in the evaluable-patients efficacy analysis.
Twenty-two patients had at least one dose of double- blind medication, but no double-blind efficacy assess- ments: 5 in the sertraline 50 mg/day group, 3 in 100 rag/day group, 9 in the 200 mg/day group, and 5 in the placebo group. These patients were excluded from the all-patients (intention-to-treat) efficacy analyses.
A total of 178 patients (48%) discontinued prematurely from this study (Table 2). Side effects and lack of efficacy were the most frequently cited reasons for discontinuation. The number of patients in each group who discontinued because of side effects prior to study day 11 and who were thus excluded from the evaluable-patients efficacy analy- sis was 4 (4%) in the sertraline 50 rag/day group, 10 (11%) in the 100 rag/day group, 23 (25%) in the 200 mg/day group, and 2 (2%) in the placebo group.
The mean duration of double-blind therapy was 33, 30, and 24 days in the sertraline 50 mg/day, 100 mg/day, and 200 rag/day groups, respectively, and 31 days in the placebo group. Thus, the shortest mean duration of therapy was in the 200 rag/day group, with 33 patients (36%) discontinuing within the first 10 days, indicating that in the absence of dose titration, the drug was better tolerated at the 50 mg/day and 100 rag/day doses.
The final dosages of double-blind sertraline did not differ substantially from the treatment dosages originally assigned. The mean final daily dose was 50 mg for the 50 rag/day group, 98 mg for the 100 mg/day group, and 190 nag for the 200 mg/day group.
Efficacy In the evaluable-patients analysis, there was significantly (p <- 0.05) greater improvement from baseline in the
596 BIOL PSYCHIATRY L.F. Fabre et al 1995;38:592-602
26
2 4 -
2 2 -
20- 2 8 o~ 18-
o 16-
-1- 14-
12-
10- " " " ' " l
Baseline 1 2 3 4 5 6
Week
Sertraline 50 mg/day - I ! - (N=82)*
Sertraline 100 mg/ --O-- day (N-74)*
Sertraline 200 mg/ '"'&'"' day (N=56)'1"
Sertraline Combined - • - (N=212)t
-C3,- Placebo (N=76)
*p < 0.05 compared with placebo at last visit
l"p< 0.01 compared with placebo at last visit
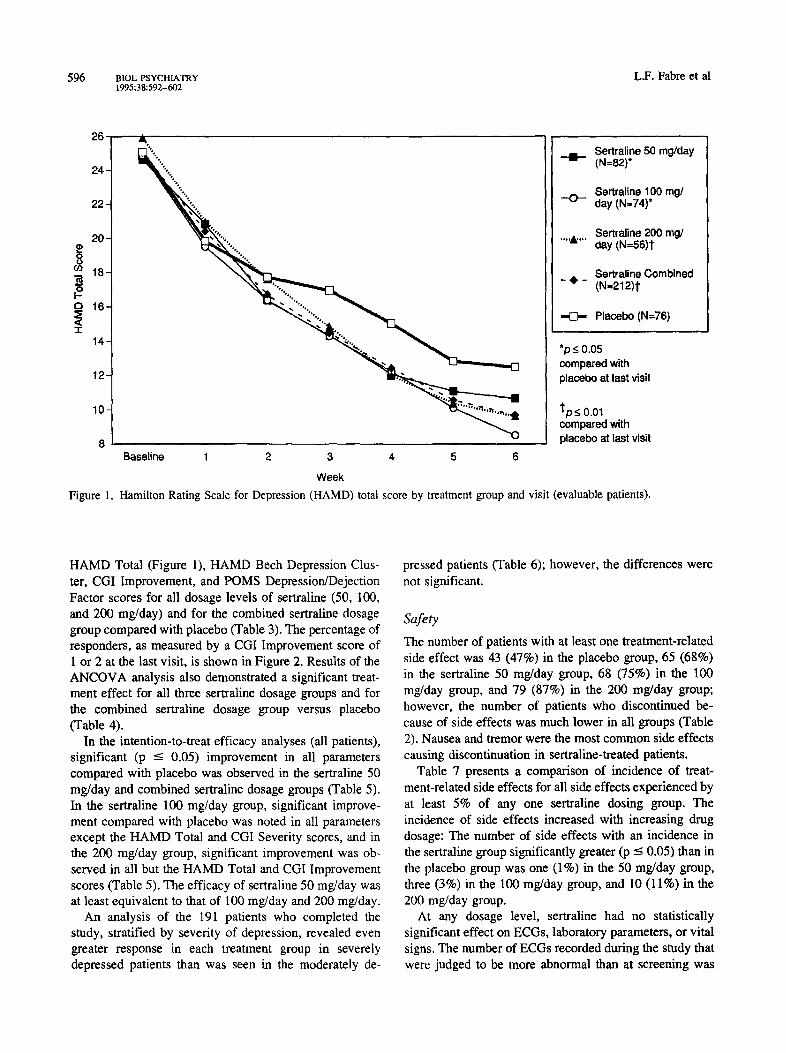
Figure 1. Hamilton Rating Scale for Depression (HAMD) total score by treatment group and visit (evaluable patients).
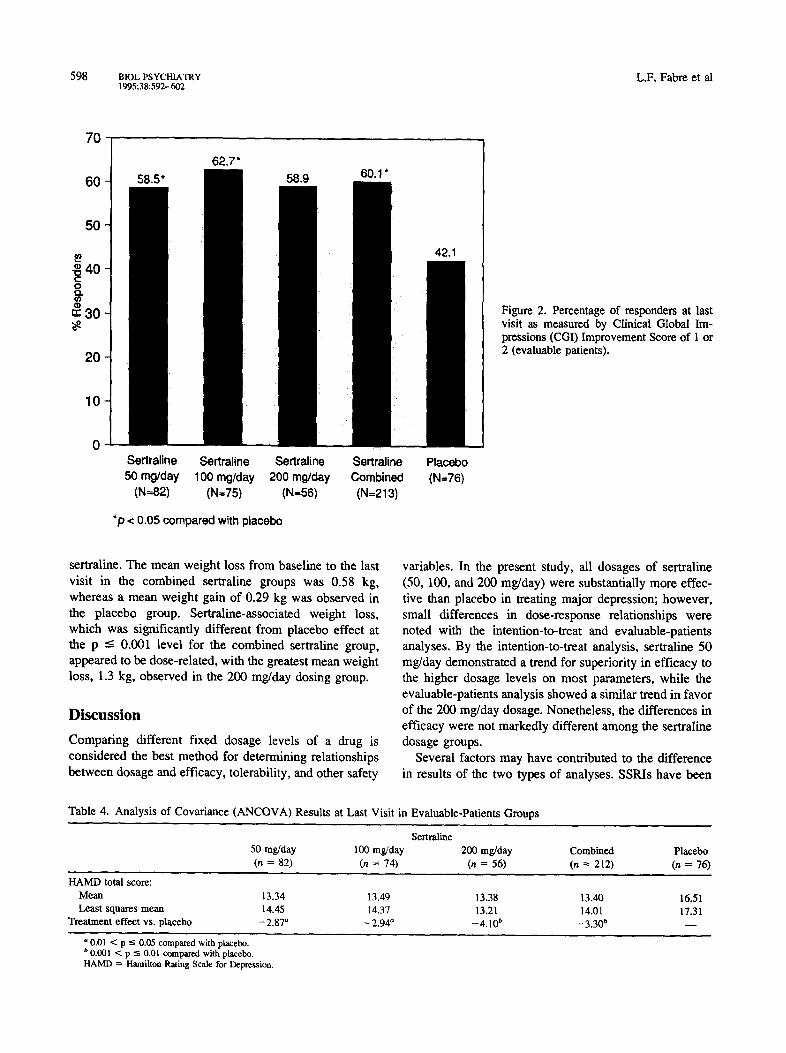
HAMD Total (Figure 1), HAMD Bech Depression Clus- ter, CGI Improvement, and POMS Depression/Dejection Factor scores for all dosage levels of sertraline (50, 100, and 200 mg/day) and for the combined sertraline dosage group compared with placebo (Table 3). The percentage of responders, as measured by a CGI Improvement score of 1 or 2 at the last visit, is shown in Figure 2. Results of the ANCOVA analysis also demonstrated a significant treat- ment effect for all three sertraline dosage groups and for the combined sertraline dosage group versus placebo (Table 4).
In the intention-to-treat efficacy analyses (all patients), significant (p <- 0.05) improvement in all parameters compared with placebo was observed in the sertraline 50 mg/day and combined sertraline dosage groups (Table 5). In the sertraline 100 mg/day group, significant improve- ment compared with placebo was noted in all parameters except the HAMD Total and CGI Severity scores, and in the 200 mg/day group, significant improvement was ob- served in all but the HAMD Total and CGI Improvement scores (Table 5). The efficacy of sertraline 50 rag/day was at least equivalent to that of 100 mg/day and 200 mg/day.
An analysis of the 191 patients who completed the study, stratified by severity of depression, revealed even greater response in each treatment group in severely depressed patients than was seen in the moderately de-
pressed patients (Table 6); however, the differences were not significant.
Safety The number of patients with at least one treatment-related side effect was 43 (47%) in the placebo group, 65 (68%) in the sertraline 50 mg/day group, 68 (75%) in the 100 mg/day group, and 79 (87%) in the 200 rag/day group; however, the number of patients who discontinued be- cause of side effects was much lower in all groups (Table 2). Nausea and tremor were the most common side effects causing discontinuation in sertraline-treated patients.
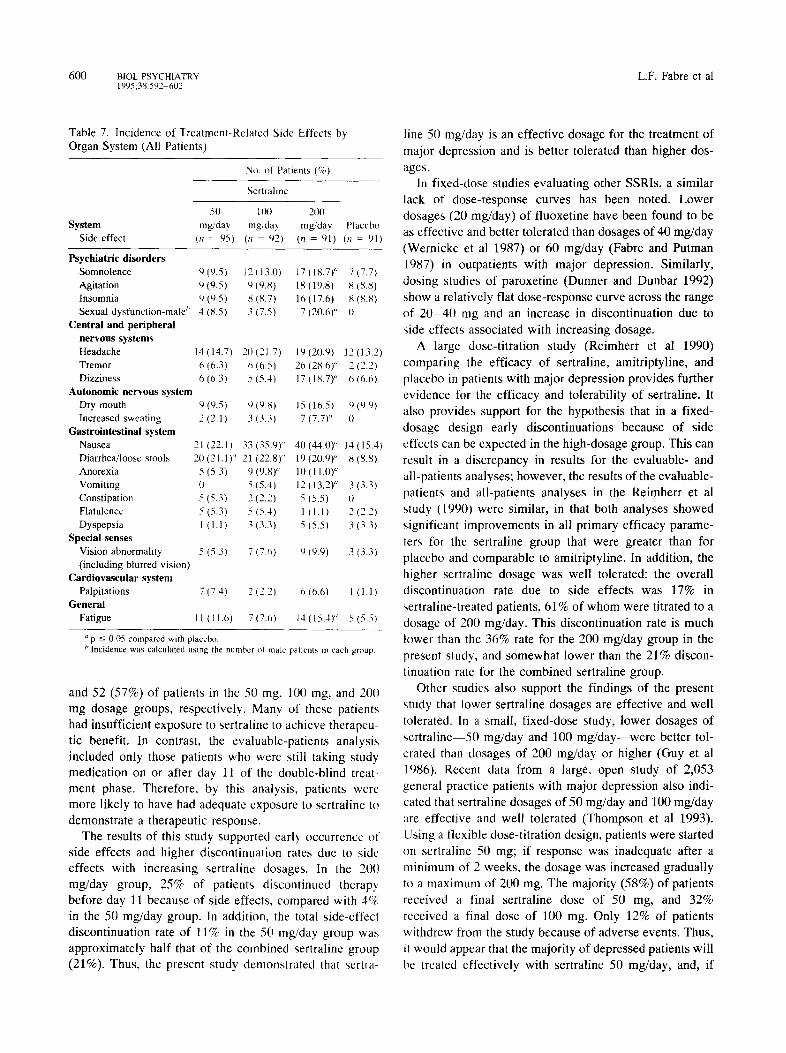
Table 7 presents a comparison of incidence of treat- ment-related side effects for all side effects experienced by at least 5% of any one sertraline dosing group. The incidence of side effects increased with increasing drug dosage: The number of side effects with an incidence in the sertraline group significantly greater (p ----- 0.05) than in the placebo group was one (1%) in the 50 mg/day group, three (3%) in the 100 mg/day group, and 10 (11%) in the 200 rag/day group.
At any dosage level, sertraline had no statistically significant effect on ECGs, laboratory parameters, or vital signs. The number of ECGs recorded during the study that were judged to be more abnormal than at screening was
Sertraline for Major Depression BIOL PSYCHIATRY 597 1995;38:592-602
T a b l e 3. M e a n E f f i c a c y P a r a m e t e r s ( _ + S D ) at L a s t V i s i t in E v a l u a b l e - P a t i e n t s G r o u p s "
Sertral ine
50 m g l d a y 100 rag/day 200 m g / d a y C o m b i n e d P lacebo
Pa ram e te r (n = 7 9 - 8 2 ) (n = 7 1 - 7 5 ) (n = 5 4 - 5 6 ) (n = 2 0 4 - 2 1 2 ) (n = 7 3 - 7 6 )
H A M D total
Basel ine score 24.~ + 3.0 24.9 ~: 3.1 25.9 ± 3.5 25.1 -+ 3.2 25.1 ± 2.6
Change f rom basel ine I 1.3 _+ 8 .7 ' I 1.4 ~ 8.7 ~ 12.5 + 7 .0 t - 1 1 . 7 --_ 8.2 f - 8 . 6 -+ 7.8
% change f rom base l ine ~' - 4 5 . 5 + 34.7 - 4 5 . 9 + 35.1 50.1 -+ 28.9 - 4 6 . 8 -+ 33.3 - 3 4 . 6 _+ 30.9
H A M D Bech Depress ion
C lus t e r '
Basel ine score 12.3 ~ 1.9 12.4 - _. ~ I 12.9 _+ 1.6 12.5 _ + 1.9 12.7 _ + 1.5
Change f rom base l ine - 5 . 5 -+ 4.Y" - 5 . 7 ~ 4.9" - 6 . 7 ± 3.8 ~ - 5 . 9 ± 4.4 g - 3 . 9 + 4.2
C G I Sever i ty
Basel ine score 4.,. ~ I).6 4.3 ~ 0.5 4.4 ± 0 .6 4.3 ± 0.6 4.2 ± 0.5
Change f rom base l ine 1.2 -~ 1.3 .... 1.3 + 1.3 '~ - 1 . 6 ± 1.0 g 1.3 ± 1.2 r - 0 . 8 ± 1.1
C G I I m p r o v e m e n t Score" 2.4 ~ 14 ' 2.4 + 1.5 ̀~ 2.2 ± 1.2 f 2 .4 _+ 1.4 r 2.9 ± 1.4
P O M S Depress ion /De jec t ion
Factor
Basel ine score 2.7 ± 1.1 2.6 : 1.0 2.5 + 1.0 2.6 _+ 1.0 2.6 ___ 1.1
C h a n g e f rom basel ine - 1).5 _+ 1.1 i - -0 .5 ~ 1.0" - 0 . 5 + 0.7 e - 0 : 5 -+ 1.0 t - 0 . 1 ± 0.7
The significance levels given for individual items are for comparison of that sertraline group (individual sertraline dosing groups or the combined sertraline group) vs. placebo for the parameter in question.
" Ranges are given for n values because data tot all parameters were not a'~ailable for all patients. ~' Statistical comparisons by individual sertralinc dosing groups (50, 100. 2()1] rag/day) vs. the placebo dosing group were not done for % change from baseline. ' Items I (depressed mood), 2 (guilt), 7 (work and interest), 8 (retardation/, 10 (anxiety, psychic), and 13 (somatic symptoms, general) of the HAMD. a Smaller positive values for this variable indicate greater improvement; scores are given only at assessments after the start of double-blind therapy, and only positive
values are given. For all other variables in the lablc, larger negative scnres indicate greater improvement. p -< 0.05 compared with placebo.
S p < 0.01 compared with placebo ,e p < 0.001 compared with placebo. HAMD - Hamilton Rating Scale h~r Depression: C(il Clinical Global hrTprcssions; POMS ;: Profile of Mood States.
not greater for any sertraline group than for the placebo group.
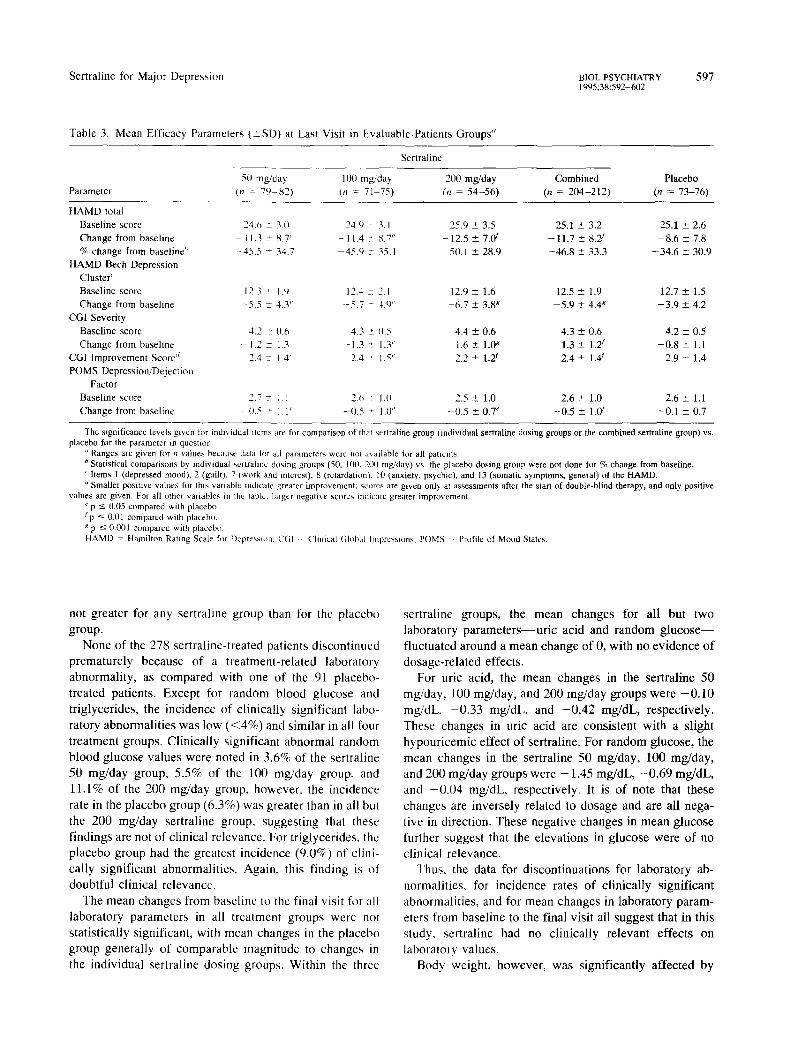
None of the 278 sertraline-treated patients discontinued prematurely because of a treatment-related laboratory abnormality, as compared with one of the 91 placebo- treated patients. Except for random blood glucose and triglycerides, the incidence of clinically significant labo- ratory abnormalities was low (<4%) and similar in all four treatment groups. Clinically significant abnormal random blood glucose values were noted in 3.6% of the sertraline 50 mg/day group, 5.5% of the 100 rag/day group, and 11.1% of the 200 mg/day group, however, the incidence rate in the placebo group (6.3%) was greater than in all but the 200 rag/day sertraline group, suggesting that these findings are not of clinical relevance. For triglycerides, the placebo group had the greatest incidence (9.0%) of clini- cally significant abnormalities. Again, this finding is of doubtful clinical relevance.
The mean changes from baseline to the final visit for all laboratory parameters in all treatment groups were not statistically significant, with mean changes in the placebo group generally of comparable magnitude to changes in the individual sertraline dosing groups. Within the three
sertraline groups, the mean changes for all but two laboratory parameters--uric acid and random glucose-- fluctuated around a mean change of 0, with no evidence of dosage-related effects.
For uric acid, the mean changes in the sertraline 50 rag/day, 100 mg/day, and 200 mg/day groups were -0 .10 mg/dL, -0 .33 mg/dL, and -0 .42 mg/dL, respectively. These changes in uric acid are consistent with a slight hypouricemic effect of sertraline. For random glucose, the mean changes in the sertraline 50 mg/day, 100 mg/day, and 200 rag/day groups were - 1.45 mg/dL, -0 .69 mg/dL, and -0 .04 mg/dL, respectively. It is of note that these changes are inversely related to dosage and are all nega- tive in direction. These negative changes in mean glucose further suggest that the elevations in glucose were of no clinical relevance.
Thus, the data for discontinuations for laboratory ab- normalities, for incidence rates of clinically significant abnormalities, and for mean changes in laboratory param- eters from baseline to the final visit all suggest that in this study, sertraline had no clinically relevant effects on laboratory values.
Body weight, however, was significantly affected by
598 BIOL PSYCHIATRY L.F, Fabre et al 1995;38:592-602
70
60
50
-~ 40
~: 30
20
10
Sertraline Sertraline Sertraline Sertraline 50 rng/day 100 mg/day 200 mg/day Combined
(N=82) (N=75) (N=56) (N=213)
*p < 0.05 compared with placebo
Placebo (N=76)
Figure 2. Percentage of responders at last visit as measured by Clinical Global Im- pressions (CGI) Improvement Score of 1 or 2 (evaluable patients).
sertraline. The mean weight loss from baseline to the last visit in the combined sertraline groups was 0.58 kg, whereas a mean weight gain of 0.29 kg was observed in the placebo group. Sertraline-associated weight loss, which was significantly different from placebo effect at the p <-- 0.001 level for the combined sertraline group, appeared to be dose-related, with the greatest mean weight loss, 1.3 kg, observed in the 200 mg/day dosing group.
Discussion
Comparing different fixed dosage levels of a drug is considered the best method for determining relationships between dosage and efficacy, tolerability, and other safety
Table 4. Analysis of Covariance (ANCOVA) Results at Last Visit
variables. In the present study, all dosages of sertraline (50, 100, and 200 mg/day) were substantially more effec- tive than placebo in treating major depression; however, small differences in dose-response relationships were noted with the intention-to-treat and evaluable-patients analyses. By the intention-to-treat analysis, sertraline 50 mg/day demonstrated a trend for superiority in efficacy to the higher dosage levels on most parameters, while the evaluable-patients analysis showed a similar trend in favor of the 200 rag/day dosage. Nonetheless, the differences in efficacy were not markedly different among the sertraline dosage groups.
Several factors may have contributed to the difference in results of the two types of analyses. SSRIs have been
in Evaluable-Patients Groups
Sertraline
50 nag/day 100 nag/day 200 mg/day Combined Placebo
(n = 82) (n = 74) (n = 56) (n = 212) (n = 76)
H A M D total score:
Mean 13.34 13.49 13.38 13.40 16.51
Least squares mean 14.45 14.37 13.21 14.01 17.31 Treatment effect vs. placebo - 2.87 ~ - 2.94 a - 4. l0 b - 3.30 t' - -
° 0.01 < p -< 0.05 compared with placebo. b 0 .001 < p "~ 0.01 compared with placebo. HAMD ~ Hamilton Rating Scale for Depression.
Sertraline for Major Depression BIOL PSYCHIATRY 599 1995;38:592-602
Table 5. Mean Efficacy, Parameters (_+SD) at Last Visit in All-Patients Groups
Parameter
Sertraline
5(1 mg/day l(t0 mg/da 5, 200 mg/day Combined Placebo (n = 9(1) (,7 = 89) (n = 82) (n = 261) (n = 86)
HAMD total Baseline score 24.8 +_: 3.0 24. t) : 3.0 25.7 ± 3.2 25.1 ± 3.1 25.3 + 2.9 Change from baseline 10.6 + 8.6 J - 9.8 ~ 8.9 -9.2 -+ 8.2 9.9 ± 8.6 a -7 .6 ± 7.5 % change from baseline" 42.6 2 34.4 39.3 ~ 30.1 --36.9 +- 33.4 --39.7 ± 34.6 -30.7 + 30.2
HAMD Bech Depression Cluster b
Baseline score 12.4 ~ 1.8 12.4 ~ 2.0 12.9 ± 1.5 12.5 _+ 1.8 12.8 + 1.5 Change from baseline - 5 2 + 4.3 '~ - 5.0 ~. 4.8 '~ -5.:l + 4.3 J 5.1 + 4.5 ~ -3.5 ± 4.0
CGI Severity Baseline score 4.3 :: 0.6 4.3 ~ 0.5 4.3 ± 0.6 4.3 -+ 0.5 4.2 ± 0.5 Change from baseline I.l ~ 1.3 J 1.1 ~: 1.3 l.l ± 1.2 '~ -1.1 + 1.2 a -0 .7 + 1.1
CGI Improvement Score' 2.5 + 1.4 J 2.(~ ~: 1.5 a 2.8 ± 1.6 2.7 ± 1.5 a 3.1 ± 1.4 POMS Depression/Dejection
Factor Baseline score 2.8 + 1.1 2.7 '~ 1.0 2.5 +- 1.0 2.7 ± 1.1 2.6 + 1.1 Change from baseline 0.5 ~ 1.1' (I.5 :. 1.1" 0.4 +- 0.7 J (1.5 ± 1.~ -0.1 + 0.7
The significance levels given for individual items are tk~r comparison ot lhal sertraline group (individual senraline dosing groups or the combined sertraline group) vs. placebo for the parameter in question.
Statistical comparisons by individual sertraline dosing groups (511. 1110, and 2(10 mg/day/vs, the placebo group were not done for % change from baseline. ~' Items 1 (depressed mood), 2 (guilt), 7 (work and interest), g (retardation). 1(1 (anxiety, psychic), and 13 (somatic symptoms, general) of the HAMD. ' Smaller positive values for this variable indicate greater improvement: scores are given only at assessments after the start of double-blind therapy, and only positive
values are given. For all other variables in the table, larger negative scores indicate greater improvement. ,l p ~ 0.05 compared with placebo.
p < 0.01 compared with placebo. fp --< 0.00l compared with placebo. HAMD = Hamilton Rating Score tot Depression: CGI - Clinical (;lgbai Impressions: PCMS " Profile of Mood States.
r epo r t ed to s h o w fiat d o s e - r e s p o n s e curves : I n c r e a s i n g
d o s a g e d o e s not m a r k e d l y inc rease t h e r a p e u t i c r e s p o n s e
bu t does i nc rease the inc idence o f s ide e f fec t s (R icke l s and
S c h w e i z e r 1990). A c o m m o n f ind ing w i t h m a n y ant ide-
p r e s s a n t d r u g s is that s ide e f fec t s o c c u r m o r e f r equen t ly
w h e n t he r apy is ini t ia ted w i th d o s e s at the h igh end o f the
t h e r a p e u t i c r a n g e ra the r than t i t ra t ing f r o m a l o w to a h igh
dose . In addi t ion , the r e s p o n s e to a n t i d e p r e s s a n t d r u g
the rapy , i n c l u d i n g t he r apy wi th S S R I s , o c c u r s in two
phase s . T h e benef ic i a l e f fec t s are not o b s e r v e d imrned i -
a t e l y - - 2 - 3 w e e k s m a y be r e qu i r e d be f o r e an i m p r o v e m e n t
in s y m p t o m s is o b s e r v e d - - w h i l e s ide e f fec t s re la ted to
a n t i d e p r e s s a n t d r u g t he r apy are e x p e r i e n c e d w i t h i n seve ra l
d a y s o f s t a r t ing t r e a t m e n t ( K a r a s u 1989).
In this s tudy , the in t en t ion - to - t r ea t a na ly s i s i nc lud ed all
pa t i en t s en t e red in the s tudy w h o had at leas t o n e e f f i cacy
a s s e s s m e n t d u r i n g the d o u b l e - b l i n d t r e a t m e n t pha s e . O f
note, h o w e v e r , is that the n u m b e r o f p r e m a t u r e d i s c o n t i n u -
a t ions i nc reased wi th i n c r e a s i n g dosa ge ; the 6 - w e e k treat-
m e n t p h a s e w a s no t c o m p l e t e d by 36 ( 38% ) , 45 (4 9 %) ,
Table 6. Mean HAMD Scores ( ± S D ) at Last Visit by Severity, of Depression in Patients Who Completed the Study
Nertraline
50 mg, da~, 100 rag/day 200 rag/day Combined Placebo Parameter (~ = 59) (it .... 46l (n = 38) (n = 143) (n = 48)
Moderately depressed" HAMD Total:
Baseline score 22.6 + 0.3 22.7 + 0.2 22.9 ± 0.2 22.7 ± 0.1 23.0 + 0.2 Change from baseline 12.9 ± 1.3 15.4 +_ l.(I -15.0 ± 1.1 -14.3 ± 0.7 -11.9 +- 1.0 % change from baseline -56.6 _+ 6.0 ~8.3 + 4.6 --65.6 ± 4.8 62.8 ± 3.1 -52.0 ± 4.4
Severely depressed" HAMD Total:
Baseline score 26.7 ~ 0.4 20.8 + (I.4 27.2 _+ 0.5 26.9 ± 0.3 27.0 ± 0.5 Change from baseline 14.3 + 1.4 16.8 ± 1.3 16.1 -+ 1.5 15.6 ± 0.8 -12.8 ± 1.4 % change from baseline 53.8 -+ 4.8 62.7 ± 4.5 -59.7 ± 5.8 -58.2 ± 2.9 -42.0 ± 5.2
Moderately depressed indicates a HAMD score at baseline of 17-24: severely depressed indicates a HAMD score at baseline ->25. HAMD = Hamilton Rating Scale for Depression.
600 BIOL PSYCHIATRY L.F. Fabre et al 1995;38:592 602
Table 7. Incidence of Treatment-Related Side Effects by Organ System (All Patients)
System Side effect
No. of Patients (%)
Sertraline
50 100 mg/day mg/day
(n 95) (n = 92)
200 mg/day Placebo
(n = 91) (n : 911
Psychiatric disorders Somnolence '4 (9.5) Agitation 9 (9.51 Insomnia 9 (9.5) Sexual dysfunction-male ~' 4 (8.5)
Central and peripheral nervous systems Headache 14 (14.7) Tremor 6 (6.3) Dizziness 6 (6.3)
Autonomic nervous system Dry mouth 9 Increased sweating 2
Gastrointestinal system Nausea 21 Diarrhea/loose stools 2(1 Anorexia 5 Vomiting (l Constipation 5 Flatulence 5 Dyspepsia I
Special senses Vision abnormality 5 (including blurred vision)
Cardiovascular system Palpitations 7 ( 7.4 )
General Fatigue 11 ( 11.6)
12{13.01 17 (18.7)" 7(7.7) 9 (9.8) 18 (19.81 8 (8,8) 8{8.7) 16(17.6) 8(8.8) 3 (7.5) 7 (20.6)" (}
20(21.7) 19(20.91 12 (13.21 6 (6.5) 26 (28.6)" 2 (2.2) 5(5.4) 17(18.7)" 6(6.6)
(9.5) (~ (9.81 15 (1~,51 ~ (9.9) (2.1) 3(3.3) 7(7.7)" (t
(22.11 33 (21.1)" 21 (5.3) 9
5 (5.3) 2 (5.3) 5 ( I .1) 3
(35.9)" 40(44,01" t4(15.41 (22.8)" 19 (20,9)" 8 (8.8) (9.8)" 10 (11.0) ~ (5.4) 12 (13.2)" 3(3.3) (2.2) 5 (5.5) It (5.4) 1 I 1.1 ) 2 (2.2) (3.3) 5 (5.5) 3 (3.3)
(5.3) 7 (7,6) t) (9.9) 3 (3.3)
2(2.2) 6(6.6) 1 (1.1)
7 (7.t~) 14 (15.4)" 5 (5.5)
"p -< 0.05 compared with placebo. b Incidence was calculated using the number of male patients in each group
and 52 (57%) of patients in the 50 mg, 100 mg, and 20(1 mg dosage groups, respectively. Many of these patients had insufficient exposure to sertraline to achieve therapeu- tic benefit. In contrast, the evaluable-patients analysis included only those patients who were still taking study medication on or after day 11 of the double-blind treat- ment phase. Therefore, by this analysis, patients were more likely to have had adequate exposure to sertraline to demonstrate a therapeutic response.
The results of this study supported early occurrence of side effects and higher discontinuation rates due to side effects with increasing sertraline dosages. In the 200 mg/day group, 25% of patients discontinued therapy before day 11 because of side effects, compared with 4q,~ in the 50 rag/day group. In addition, the total side-effect discontinuation rate of 11% in the 50 mg/day group was approximately half that of the combined sertraline group (21%). Thus, the present study demonstrated that sertra-
line 50 mg/day is an effective dosage for the treatment of major depression and is better tolerated than higher dos- ages.
In fixed-dose studies evaluating other SSRls, a similar lack of dose-response curves has been noted. Lower dosages (20 rag/day) of fluoxetine have been found to be as effective and better tolerated than dosages of 40 mg/day (Wemicke et al 1987) or 60 mg/day (Fabre and Putman 1987) in outpatients with major depression. Similarly, dosing studies of paroxetine (Dunner and Dunbar 1992) show a relatively flat dose-response curve across the range of 20-40 nag and an increase in discontinuation due to side effects associated with increasing dosage,
A large dose-titration study (Reimherr et al 1990) comparing the efficacy of sertraline, amitriptyline, and placebo in patients with major depression provides further evidence for the efficacy and tolerability of sertraline. It also provides support for the hypothesis that in a fixed- dosage design early discontinuations because of side effects can be expected in the high-dosage group. This can result in a discrepancy in results for the evaluable- and all-patients analyses; however, the results of the evaluable- patients and all-patients analyses in the Reimherr et al study (1990) were similar, in that both analyses showed significant improvements in all primary efficacy parame- ters for the sertraline group that were greater than for placebo and comparable to amitriptyline. In addition, the higher sertraline dosage was well tolerated: the overall discontinuation rate due to side effects was 17% in sertraline-treated patients, 61% of whom were titrated to a dosage of 200 mg/day. This discontinuation rate is much lower than the 36% rate for the 200 mg/day group in the present study, and somewhat lower than the 21% discon- tinuation rate for the combined sertraline group.
Other studies also support the findings of the present study that lower sertraline dosages are effective and well tolerated. In a small, fixed-dose study, lower dosages of sertraline--50 mg/day and 100 mg/day--were better tol- erated than dosages of 200 rag/day or higher (Guy et al 1986). Recent data from a large, open study of 2,053 general practice patients with major depression also indi- cated that sertraline dosages of 50 mg/day and 100 rag/day are effective and well tolerated (Thompson et al 1993). Using a flexible dose-titration design, patients were started on sertraline 50 rag; if response was inadequate after a minimum of 2 weeks, the dosage was increased gradually to a maximum of 200 mg. The majority (58%) of patients received a final sertraline dose of 50 mg, and 32% received a final dose of 100 mg. Only 12% of patients withdrew from the study because of adverse events. Thus, it would appear that the majority of depressed patients will be treated effectively with sertraline 50 mg/day, and, if

Sertraline for Major Depression BIOL PSYCHIATRY 601 1995;38:592-602
higher dosages are required, they will be better tolerated if achieved through dose titration.
In the present study, most of the commonly reported side effects were dose related. The principal side effects of sertraline were related to the gastrointestinal tract--nau- sea, vomiting, and diarrhea~and are commonly reported with other SSRIs. The 21% incidence of male sexual dysfunction, mainly transient or intermittent ejaculation disturbance, in the sertraline 200-mg/day group in this study is similar to that reported with imipramine treatment (Harrison et al 1986) and other SSRIs (Herman et al 1990; Mendels 1987; Musher 1990; Zajecka et al 1991; Preskorn 1994).
Unlike tricyclic antidepressants, which promote an in- crease in appetite, carbohydrate craving, and weight gain, sertraline caused a small but significant weight loss in this study. Drugs with a serotonergic effect, such as the SSRIs that selectively inhibit serotonin reuptake, are more likely to promote weight loss, whereas serotonin antagonists are more likely to stimulate weight gain (Bernstein 1988). The literature suggests that weight gain is a major reason for premature discontinuation of tricyclic antidepressant ther- apy; therefore, patient compliance may be improved with sertraline treatment.
Summary The results of this study show that sertraline 50 ms/day is as effective as dosages of 100 ms/day and 200 ms/day for the treatment of major depression. The 50 ms/day dosage was associated with fewer side effects and premature discontinuations of thcrapy. This study confirmed the flat dose-response curve previously reported with other SSRIs: Increasing doses of scrtraline were not associated with marked increases in therapeutic benefit but were associ- ated with an increased occurrence of side effects. These data corroborate previous findings that the 50 mg dose of sertraline, the lowest recommended dose, appears to be cffectivc for the majority of depressed patients.
Supported by a grant from Pfizer Inc. From Fabre Research Clinics, Inc., Houston, TX (LFF); Clinical Psychopharmacology Consultants, P.A., Minneapolis, MN (FSA); Lakeshore General Hospital, Pointe Claire, Quebec, Canada (MA); Clinical Research Associates, Inc., Houston, TX (JLC); Therapeutics, Inc., Philadelphia, PA (JM); Psychiatric Consult- ants, P.C., Nashville, TN (WMP); Wayne State University (Lafayette Clinic), Detroit, MI (SD); and Larue D. Carter Memorial Hospital, Indianapolis, IN (JGS).
References American Psychiatric Association (1980): Diagnostic and Sta
tistical Manual of Mental Disorders, 3rd ed rev. Washington DC: American Psychiatric Association.
Amin M, Lehmann H, Mirmiran J (t989): A double-blind, placebo-controlled dose-finding study with sertraline. Psv- chopharmacol Bull 25:164-167.
Bech P, Gram LF, Dein E, et al (1975): Quantitative rating of depressive states. Acta Psvchiatr Scand 51 : 161-170.
Bernstein JG (1988): Psychotropic drug induced weight gain: Mechanisms and management. Clin Neuropharmacol 11: 194-206.
Bolden-Watson C, Richelson E (1993): Blockade by newly- developed antidepressants of biogenic amine uptake into rat brain synaptosomes. Life Sci 52:1023-1029.
Dunner DL, Dunbar GC (1992): Optimal dose regimen for paroxetine. J Clin Ps'ychiatry 53 (suppl 2):21-26.
Fabre LF (1991a): A double-blind multicenter study comparing the safety and efficacy of sertralinc with placebo in major depression. Presented at the 5th World Congress of Biological Psychiatry, Florence, Italy, June 9-14
Fabre LF (1991b): A double-blind, multicenter study comparing the safety and efficacy of sertraline with placebo in major depression. Biol Psvchiatr~ 21:353S.
Fabre LF, Putman HP (1987): A fixed-dose clinical trial of fluoxetine in outpatients with major depression. J Clm P~v- chiatr 3, 48:406-408.
Fouda HG, Ronfeld RA. Weidler DJ (1987): Gas chromato- graphic-mass spectrometric analysis and preliminary human
pharmacokinetics of sertraline, a new antidepressant drug. J Chromatogr 417:197-202.
Garret DL, Davis JM (1979): Biogenic amine hypothesis of affective disorders. Life Sci 24:383-394.
Guy W (1976): ECDEU Assessment Manual for Psychopharma- cology, US Department of Health, Education, and Welfare publication No. (ADM) 76-338. Rockville, MD: National Institute of Mental Health.
Guy W. Manov G, Wilson WH (1986): A double-blind dose determination study of a new antidepressant-sertraline. Drug Dev Res 9:267-272.
Hamilton M (1960): A rating scale for depression. J Neurol Neurosurg Psychiat~' 23:56-62.
Harrison WM, Rabkin JG, Ehrhardt AA, et al (1986): Effects of antidepressant medication of sexual function: A controlled study. J Clin Psychopharmacol 6:144-149.
Herman JB, Brotman AW, Pollack MH, et al (1990): Fluoxetine- induced sexual dysfunction. J Clin Psychiatry 51:25-27.
Hollander M, Wolfe DA (1973): Nonparametric Statistical Methods. New York: Wiley.
Karasu TB (ed) (1989): Antidepressants: Pharmacology and clinical use. In Treatment of Psychiatric Disorders. Washing- Ion DC: American Psychiatric Association, pp 1773-1787.
Kennett GA, Dourish CT, Curzon G (1987): Antidepressant-like action of 5HT~A agonists and conventional antidepressants in an animal model of depression. Eur J Pharmacol 134:265- 274.
Koe BK, Koch SW, Lebel LA, et al (1987): Sertraline, a selective
602 BIOL PSYCHIATRY L.F. Fabre et al 1995;38:592-602
inhibitor of serotonin uptake, induces subsensitivity of beta- adrenoceptor system of rat brain. Eur J Pharmacol 141:187- 194.
Koe BK, Weissman A, Welch WM, et al (1983): Sertraline, 1S, 4S-N-methyl-4- (3,4-dichlorophenyl) -1,2,3,4-tetrahydro- 1-naphthylamine, a new uptake inhibitor with selectivity for serotonin. J Pharmacol Exp Ther 226:686-700.
Lemberger L, Fuller RW, Zerbe RE (1985): Use of specific serotonin uptake inhibitors as antidepressants. Clin Neuro- pharmacol 8:299-317.
McNair DM, Lorr M, Droppleman LF (1980): Profile of Mood States. San Diego, CA: Education and Industrial Testing Service.
Mendels J (1987): Clinical experience with serotonin reuptake inhibiting antidepressants. J Clin Psychiatry 48(3):26-30.
Musher JS (1990): Anorgasmia with the use of fluoxetine [letter]. Am J Psychiatry 147:948.
Preskorn SH (1994): Outpatient Management of Depression. New York, NY: Professional Communications Inc.
Reimherr RW, Chouinard G, Cohn CK, et al (1990): Antidepres- sant efficacy of sertraline: a double-blind, placebo- and amitriptyline-controlled, multicenter comparison study in outpatients with major depression. J Clin Psychiatry 51(B): 18-27.
Richelson E (1988): Synaptic pharmacology of antidepressants: an update. McLean Hosp J 13:67-88.
Rickels K, Schweizer E (1990): Clinical overview of serotonin reuptake inhibitors. J Clin Psychiatry 51(suppl B):9-12.
SAS Institute, Inc (1985): SAS ® User's Guide: Statistics Version. 5th ed. Cary, NC: SAS Institute.
Shopsin B, Cassano GB, Conti L (1981): An overview of new "second generation" antidepressant compounds: research and treatment implications. In Enna S J, Malick JB, Richelson E (eds), Antidepressants: Neurochemical, Behavioral, and Clinical Perspectives. New York, NY: Raven Press.
Thompson C, Martindale JJ, Doogan D (1993): Sertraline in the Treatment of Depression in Primary Care. Presented at the 9th World Congress of Psychiatry. Rio de Janeiro, Brazil: June 6-12.
Tulloch IF, Johnson AM (1992): The pharmacologic profile of paroxetine, a new selective serotonin reuptake inhibitor. J Clin Psychiatry 53(2, suppl):7-12.
Wernicke JF, Dunlop SR, Dornseif BE, Zerbe RL (1987): Fixed-dose fluoxetine therapy for depression. Psychopharma- col Bull 23:164-168.
Zajecka J, Fawcett J, Schaff M, et al (1991): The role of serotonin in sexual dysfunction: fluoxetine-associated orgasm dysfunction. J Clin Psychiatry 52:66-68.





























