Embed Size (px)
Citation preview

RESEARCH PAPER
Dantrolene for cerebral vasospasm aftersubarachnoid haemorrhage: a randomised doubleblind placebo-controlled safety trialSusanne Muehlschlegel,1,2,3 Raphael Carandang,1,3 Wiley Hall,1,3 Nisha Kini,4
Saef Izzy,1 Bridget Garland,1 Cynthia Ouillette,1 Imramsjah M J van der Bom,5
Thomas F Flood,5 Matthew J Gounis,5 John P Weaver,6 Bruce Barton,4
Ajay K Wakhloo1,5,6
▸ Additional material ispublished online only. To viewplease visit the journal online(http://dx.doi.org/10.1136/jnnp-2014-308778).
For numbered affiliations seeend of article.
Correspondence toDr Susanne Muehlschlegel,Departments of Neurology(Neurocritical Care),Anesthesia/Critical Care andSurgery, University ofMassachusetts Medical School,55 Lake Ave. North, S5,Worcester, MA 01655, USA;[email protected]
Received 12 June 2014Revised 29 September 2014Accepted 30 September 2014
To cite: Muehlschlegel S,Carandang R, Hall W, et al.J Neurol NeurosurgPsychiatry Published OnlineFirst: [please include DayMonth Year] doi:10.1136/jnnp-2014-308778
ABSTRACTBackground Dantrolene is neuroprotective in animalmodels and may attenuate cerebral vasospasm (cVSP) inhuman aneurysmal subarachnoid haemorrhage (aSAH).We evaluated safety, feasibility and tolerability ofintravenous dantrolene (IV-D) in patients with aSAH.Methods In this single-centre, randomised, doubleblind, placebo-controlled trial, 31 patients with aSAHwere randomised to IV-D 1.25 mg every 6 h for 7 days(n=16) or equiosmolar free water/5% mannitol (placebo;n=15). Primary safety end points were incidence ofhyponatraemia (sNa≤132 mmol/L) and liver toxicity(proportion of patients alanine transaminase, aspartateaminotransferase and AlkPhos >5× upper-limit-of-normal). Secondary end points included tolerability,systemic hypotension and intracranial hypertension.Efficacy was explored for clinical/radiological cVSP,delayed cerebral ischaemia (DCI), and 3-month functionaloutcomes. Quantitative analyses of angiograms and dailytranscranial Doppler (TCD) were performed.Results Between IV-D versus placebo, no differenceswere observed in the primary outcomes (hyponatremia44% vs 67% (p=0.29); liver toxicity 6% vs 0% (p=1.0)).Three patients in the IV-D versus two in the placebogroup had severe adverse events possibly attributable toinfusion and reached stop criteria: one IV-D patientdeveloped liver toxicity; two patients in each groupdeveloped brain oedema requiring osmotherapy. Themajority of adverse events were not related to infusion(17 vs 5 (RR 2.2; 95% CI 0.7 to 6.7; p=0.16) in IV-D vsplacebo). No differences in any categorical cVSPoutcomes, DCI, 3-month outcomes or quantitativeangiogram and TCD analyses were seen in this smallsafety trial not powered to detect efficacy.Conclusions In this small trial, IV-D after aSAH wasfeasible, tolerable and safe.Trial registration number http://clinicaltrials.govNCT01024972.
INTRODUCTIONCerebral vasospasm (cVSP) after aneurysmal sub-arachnoid haemorrhage (aSAH) has been associatedwith delayed cerebral ischaemia (DCI) and to dateis thought to be largest contributor of morbidityand mortality after aSAH.1 Treatments amelioratingnot only cVSP but also improving neurological out-comes after aSAH are lacking.1
Dantrolene, an already US Food and DrugAdministration (FDA) approved ryanodine-receptor(RyR) blocker, is a promising pharmacological agentfor improving outcomes after aSAH given its dualmechanism; it is neuroprotective,2 3 and in animalmodels inhibits cerebral vasoconstriction alone andexponentially more in combination with nimodi-pine.4 In fact, the common pathway for cVSP andneurotoxicity is the continuous elevation of intracel-lular Ca2+, resulting from the influx of extracellularCa2+ and, to a much higher degree, release from thelargest intracellular Ca2+-store, the endo/sarcoplas-matic reticulum, mediated by the RyR.5 6 Thus, thecombined blockage of L-type specific Ca2+-channels(by nimodipine) and RyRs (by dantrolene) may be akey downstream mechanism in ameliorating cVSPand neurotoxicity. Two small human studies have sug-gested that a single dose of intravenous dantrolene(IV-D) may attenuate cVSP after aSAH,7 8 but thefeasibility and safety profile of IV-D in critically-illpatients with aSAH over several days is unknown,and effects on outcome have never been explored.The temporal pattern of cVSP and IV-D’s
pharmacology calls for repeated IV-D infusionsduring the cVSP period. IV-D’s chemical structurerequires reconstitution in free water with 5% man-nitol.9 Hence, safety concerns of IV-D in criticallyill aSAH include exacerbation of hyponatraemiaand brain oedema. Other potential concernsinclude systemic hypotension (combined withnimodipine), and liver toxicity, as enteric dantro-lene (but not IV-D) carries a ‘black-box warning’for liver toxicity9 and patients with aSAH com-monly receive other liver-metabolised medicationsconcurrently (paracetamol, phenytoin/fospheny-toin, statin).We conducted a single-centre, randomised,
double blind, placebo-controlled phase-II trial toevaluate the feasibility, safety and tolerability ofrepeated IV-D doses in critically ill patients withaSAH. We tested the null-hypothesis that IV-D,compared to placebo, increases the incidence anddegree of hyponatraemia, liver toxicity, brainoedema and systemic hypotension.
MATERIALS AND METHODSThe University of Massachusetts Medical School(UMMS) institutional review board (IRB) approved
Muehlschlegel S, et al. J Neurol Neurosurg Psychiatry 2014;0:1–7. doi:10.1136/jnnp-2014-308778 1
Cerebrovascular disease JNNP Online First, published on October 24, 2014 as 10.1136/jnnp-2014-308778
Copyright Article author (or their employer) 2014. Produced by BMJ Publishing Group Ltd under licence.
group.bmj.com on October 27, 2014 - Published by http://jnnp.bmj.com/Downloaded from

this investigator-initiated trial (http://clinicaltrials.govNCT01024972). Written, informed consent was obtained fromall patients or the healthcare proxies prior to the occurrence ofcVSP in order to increase the likelihood of patients self-consenting to the study, as required by our IRB. We followed the2010 CONSORT guidelines for reporting parallel group trials.10
All patients presenting with aSAH to our institution werescreened for study eligibility between October 2009 and October2012. The main inclusion criteria were aSAH ≥18 years, aneur-ysm fully secured by coiling or clipping, Hunt & Hess grade <5,modified Fisher Scale >1, alanine transaminase (ALT), aspartateaminotransferase (AST) and AlkPhos <3× upper limit ofnormal, serum sodium (sNa) ≥135 mmol/L and no mannitol orhypertonic saline administered prior to study drug infusion(details in online supplement).
During the infusion period we measured sNa, ALT, AST,AlkPhos and osmolarity daily, and the research study nursevisited participants daily, reviewing flow sheets and speaking tothe clinical team to assess for primary and secondary outcomes.
To standardise hyponatremia treatment, we instituted a step-wise protocol (online supplement), based on pretrial consensusby our neurointensivists and vascular neurosurgeon. To studythe possible effects of IV-D on cVSP, but without increasingrisks for patients, all study patients received baseline (beforestudy drug) and daily transcranial Doppler (TCD) for 7 daysduring the study drug infusion period. One of three trainedstudy TCD examiners performed these TCD, with the sameexaminer performing all TCD in a participant, when possible(details in online supplement and supplementary figure SI).Owing to safety concerns regarding radiation and contrast-dyeexposure, repeat angiography was performed only when indi-cated clinically for suspicion of clinical cVSP (onlinesupplement).
Routine patient managementAll patients with aSAH were treated according to our institu-tional protocol following published aSAH critical care guide-lines,11 12 including admission to our closed neuroscienceintensive care unit with board-certified neurointensivsts as theprimary attending. Details are listed in the online supplement.
Randomisation and interventionEligible patients were randomised 1:1 to IV-D 1.25 mg/kg every6 h for 7 days or equi-osmolar placebo, consisting of the samesolution (free water with 5% mannitol) as IV-D, without activedrug, using block randomisation in blocks of four (kept insealed envelopes in the research pharmacy until patient consent;generated by SAS V.9.2 (PROC PLAN), SAS Institute Inc, Cary,North Carolina, USA; figure 1). We chose this placebo overnormal saline as we wanted to specifically explore the safety ofdantrolene, and differentiate the effects of dantrolene fromthose of its solution. The dose was determined by our previoussingle-dose study in which we explored two doses (1.25 mg/kgand 2.5 mg/kg, both within the maximum FDA approved dose)and found that there was no further vasodilatatory effect withthe higher dose.8 To maintain rigorous double blinding, theresearch pharmacy covered the entire length of the tubing andinfusion bag with a brown plastic bag because of IV-D’s brightyellow colour. We administered study drug over a 7-day period,initiated within the first week after the sentinel headache indi-cating aSAH onset. While funding did not permit a longeradministration period, we were confident that IV-D would beadministered during the most critical time period for cVSPdevelopment.
Outcome measuresThe primary safety outcomes were hyponatremia, liver toxicity,and number of severe adverse events (SAEs) and adverse events(AE); secondary safety outcomes were systemic hypotension,intracranial hypertension, brain oedema and overall tolerability.Detailed outcome definitions and stop rules are listed in onlinesupplementary table SI and the online supplement. Efficacy out-comes explored were TCD, angiographic and clinical cVSP, mor-tality and delayed ischaemic deficits, assessed at discharge.Modified Rankin Scale (mRS), Glasgow Outcome Scale (GOS)and Barthel Index (BI) were assessed at 3 months post-aSAH.Additionally, changes in daily TCD peak systolic (PSV) andmean flow velocities (MVF) for each vessel at prespecifieddepths, as well as angiographic vessel diameters were quantita-tively analysed to explore the effect of IV-D on vessel diameters(online supplement).
Safety monitoringThe FDA granted an IND exemption (IND 106340). All SAEswere reported to our IRB within 24 h. Additionally, a datasafety monitoring board (DSMB) reviewed the results of aplanned interim analysis after 50% of patients were enrolled,and ruled that the study be continued without need for studyprotocol modifications. The DSMB additionally asked toanalyse daily white cell count, haematocrit and platelets, whichwere part of clinical routine laboratory measurements, as aplas-tic anaemia and leukopoenia are rare IV-D side effects.9
Sample size calculationBased on detecting a clinically important difference in thechange in mean sNa from baseline (≥5 mmol/L; details in theonline supplement), one planned interim analysis, assuming atwo-sided α=0.05, and allowing for attrition, we planned toenrol a total n=30 (n=15 per arm) over a 3-year period, pro-viding a power of 93%. After the interim analysis, we increasedthe sample size to n=32 because two patients withdrew consentfrom the study for subjective reasons (‘nervous about research’).Sample size calculation was performed using EAST (V.5, CytelInc, Cambridge, Massachusetts, USA).
Statistical analysisWe applied intention-to-treat analysis throughout. Categoricaldata were analysed using Fisher Exact test, while continuousand ordinal data were analysed with Student’s t test orWilcoxon signed-rank test, as appropriate. The odds of AE/SAEwere calculated with Generalised Estimation Equation with thepatient as the clustering unit. Quantitative TCD and angiogrammeasurements were analysed using hierarchical linear models,allowing nesting of multiple observations per patient. We calcu-lated the difference between each specific vessel at prespecifiedlocations and each patient’s baseline, per previously publishedmethods13 (details in online supplement), and adjusted this dif-ference to each patient’s baseline value. Unlike the daily per-protocol TCD assessments, angiograms were only performedwhen clinically indicated for suspected cVSP, with a small pro-portion undergoing follow-up angiogram during the infusionperiod. Therefore, we differentiated angiogram assessments as‘during’ the infusion period, from ‘after’. Some patients receivedadditional TCD examinations per clinical routine after the 7-dayinfusion period for suspicion of cVSP. Post hoc we assessedthese TCD for ‘delayed TCD cVSP’, without quantitative ana-lysis, as different examiners, but not our trained study TCDexaminers, performed these studies. p Values <0.05 were
2 Muehlschlegel S, et al. J Neurol Neurosurg Psychiatry 2014;0:1–7. doi:10.1136/jnnp-2014-308778
Cerebrovascular disease
group.bmj.com on October 27, 2014 - Published by http://jnnp.bmj.com/Downloaded from

considered significant. Analyses were performed using SAS V.9.3(SAS Institute Inc, Cary, North Carolina, USA). Graphs werecreated using Prism 6.0 (GraphPad Software Inc, La Jolla,California, USA).
RESULTSOf 134 patients screened, 32 patients were consented (24%), and31 (23%) randomised (IV-D: n=16, placebo: n=15; figure 2).One patient withdrew consent prior to randomisation, as wewere unable to comply with the request to receive active studydrug only. Two patients in the placebo group withdrew consent
during the infusion period for any subsequent blood draws orfollow-up (‘nervous about research’), resulting in 13 patients ana-lysed in the placebo group. Baseline characteristics all enrolledparticipants are presented in table 1 and see online supplemen-tary table II, and revealed grossly balanced groups.
Laboratory and physiological dataThe proportion of participants who developed hyponatraemia(sNa ≤132 mmol/L) was similar between groups: seven (43.8%)in the IV-D, and 10 (66.7%) in the placebo group (p=0.29). Atthe same time, there was no difference in the number of
Figure 1 Study design. The baseline TCD and screening labs were performed prior to randomisation to ensure that eligibility criteria were still met.ALT, alanine transaminase; AST, aspartate aminotransferase; AlkPhos, alkaline phosphatase; BP, blood pressure; DCI, delayed cerebral ischaemia;GOS, Glasgow Outcome Scale; ICP, intracranial pressure; IV, intravenous; mRS, modified Rankin Scale; Na, sodium; aSAH, (aneurysmal) subarachnoidhemorrhaege; TCD, transcranial Doppler.
Figure 2 CONSORT diagram. The number of participants screened, enrolled, completed infusions and analysed is shown. Patients were notenrolled for various reasons listed.
Muehlschlegel S, et al. J Neurol Neurosurg Psychiatry 2014;0:1–7. doi:10.1136/jnnp-2014-308778 3
Cerebrovascular disease
group.bmj.com on October 27, 2014 - Published by http://jnnp.bmj.com/Downloaded from
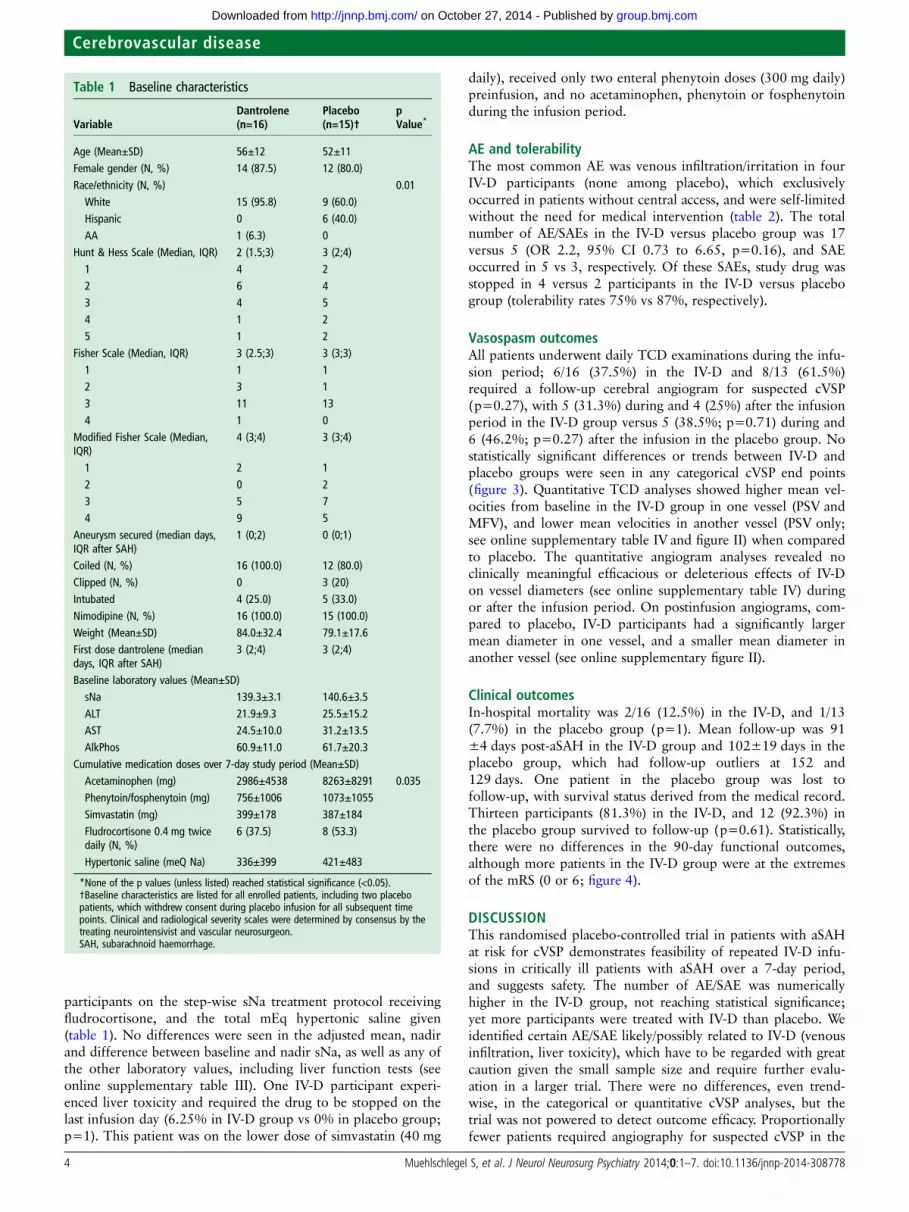
participants on the step-wise sNa treatment protocol receivingfludrocortisone, and the total mEq hypertonic saline given(table 1). No differences were seen in the adjusted mean, nadirand difference between baseline and nadir sNa, as well as any ofthe other laboratory values, including liver function tests (seeonline supplementary table III). One IV-D participant experi-enced liver toxicity and required the drug to be stopped on thelast infusion day (6.25% in IV-D group vs 0% in placebo group;p=1). This patient was on the lower dose of simvastatin (40 mg
daily), received only two enteral phenytoin doses (300 mg daily)preinfusion, and no acetaminophen, phenytoin or fosphenytoinduring the infusion period.
AE and tolerabilityThe most common AE was venous infiltration/irritation in fourIV-D participants (none among placebo), which exclusivelyoccurred in patients without central access, and were self-limitedwithout the need for medical intervention (table 2). The totalnumber of AE/SAEs in the IV-D versus placebo group was 17versus 5 (OR 2.2, 95% CI 0.73 to 6.65, p=0.16), and SAEoccurred in 5 vs 3, respectively. Of these SAEs, study drug wasstopped in 4 versus 2 participants in the IV-D versus placebogroup (tolerability rates 75% vs 87%, respectively).
Vasospasm outcomesAll patients underwent daily TCD examinations during the infu-sion period; 6/16 (37.5%) in the IV-D and 8/13 (61.5%)required a follow-up cerebral angiogram for suspected cVSP(p=0.27), with 5 (31.3%) during and 4 (25%) after the infusionperiod in the IV-D group versus 5 (38.5%; p=0.71) during and6 (46.2%; p=0.27) after the infusion in the placebo group. Nostatistically significant differences or trends between IV-D andplacebo groups were seen in any categorical cVSP end points(figure 3). Quantitative TCD analyses showed higher mean vel-ocities from baseline in the IV-D group in one vessel (PSV andMFV), and lower mean velocities in another vessel (PSV only;see online supplementary table IV and figure II) when comparedto placebo. The quantitative angiogram analyses revealed noclinically meaningful efficacious or deleterious effects of IV-Don vessel diameters (see online supplementary table IV) duringor after the infusion period. On postinfusion angiograms, com-pared to placebo, IV-D participants had a significantly largermean diameter in one vessel, and a smaller mean diameter inanother vessel (see online supplementary figure II).
Clinical outcomesIn-hospital mortality was 2/16 (12.5%) in the IV-D, and 1/13(7.7%) in the placebo group (p=1). Mean follow-up was 91±4 days post-aSAH in the IV-D group and 102±19 days in theplacebo group, which had follow-up outliers at 152 and129 days. One patient in the placebo group was lost tofollow-up, with survival status derived from the medical record.Thirteen participants (81.3%) in the IV-D, and 12 (92.3%) inthe placebo group survived to follow-up (p=0.61). Statistically,there were no differences in the 90-day functional outcomes,although more patients in the IV-D group were at the extremesof the mRS (0 or 6; figure 4).
DISCUSSIONThis randomised placebo-controlled trial in patients with aSAHat risk for cVSP demonstrates feasibility of repeated IV-D infu-sions in critically ill patients with aSAH over a 7-day period,and suggests safety. The number of AE/SAE was numericallyhigher in the IV-D group, not reaching statistical significance;yet more participants were treated with IV-D than placebo. Weidentified certain AE/SAE likely/possibly related to IV-D (venousinfiltration, liver toxicity), which have to be regarded with greatcaution given the small sample size and require further evalu-ation in a larger trial. There were no differences, even trend-wise, in the categorical or quantitative cVSP analyses, but thetrial was not powered to detect outcome efficacy. Proportionallyfewer patients required angiography for suspected cVSP in the
Table 1 Baseline characteristics
VariableDantrolene(n=16)
Placebo(n=15)†
pValue*
Age (Mean±SD) 56±12 52±11Female gender (N, %) 14 (87.5) 12 (80.0)Race/ethnicity (N, %) 0.01White 15 (95.8) 9 (60.0)Hispanic 0 6 (40.0)AA 1 (6.3) 0
Hunt & Hess Scale (Median, IQR) 2 (1.5;3) 3 (2;4)1 4 22 6 43 4 54 1 25 1 2
Fisher Scale (Median, IQR) 3 (2.5;3) 3 (3;3)1 1 12 3 13 11 134 1 0
Modified Fisher Scale (Median,IQR)
4 (3;4) 3 (3;4)
1 2 12 0 23 5 74 9 5
Aneurysm secured (median days,IQR after SAH)
1 (0;2) 0 (0;1)
Coiled (N, %) 16 (100.0) 12 (80.0)Clipped (N, %) 0 3 (20)Intubated 4 (25.0) 5 (33.0)Nimodipine (N, %) 16 (100.0) 15 (100.0)Weight (Mean±SD) 84.0±32.4 79.1±17.6First dose dantrolene (mediandays, IQR after SAH)
3 (2;4) 3 (2;4)
Baseline laboratory values (Mean±SD)sNa 139.3±3.1 140.6±3.5ALT 21.9±9.3 25.5±15.2AST 24.5±10.0 31.2±13.5AlkPhos 60.9±11.0 61.7±20.3
Cumulative medication doses over 7-day study period (Mean±SD)Acetaminophen (mg) 2986±4538 8263±8291 0.035Phenytoin/fosphenytoin (mg) 756±1006 1073±1055Simvastatin (mg) 399±178 387±184Fludrocortisone 0.4 mg twicedaily (N, %)
6 (37.5) 8 (53.3)
Hypertonic saline (meQ Na) 336±399 421±483
*None of the p values (unless listed) reached statistical significance (<0.05).†Baseline characteristics are listed for all enrolled patients, including two placebopatients, which withdrew consent during placebo infusion for all subsequent timepoints. Clinical and radiological severity scales were determined by consensus by thetreating neurointensivist and vascular neurosurgeon.SAH, subarachnoid haemorrhage.
4 Muehlschlegel S, et al. J Neurol Neurosurg Psychiatry 2014;0:1–7. doi:10.1136/jnnp-2014-308778
Cerebrovascular disease
group.bmj.com on October 27, 2014 - Published by http://jnnp.bmj.com/Downloaded from

IV-D compared to placebo group, but this was not statisticallysignificant.
Important clinical observations, confirmed by preclinicalstudies, and a plausible biological mechanism mediated byblockade of intracellular calcium release led to this trial. Our
first observations on TCD were made during the administrationof IV-D for shiver control associated with induced normother-mia in patients with aSAH with cVSP. We incidentally observedimprovement in TCD velocities in one patient shortly after adose, and systematically studied this phenomenon in two
Table 2 Adverse events
Type of AE/SAE n Per cent Severity Reported as SAE? SAE/AE related to study drug Stopped study drug?
DantroleneVein irritation/infiltration 4 23.5 Mild/Moderate LikelyNeurological deterioration requiring osmotherapy 2 11.8 Severe ✓ Possibly ✓(both)LFT elevation >5× upper limit of normal 1 5.9 Severe ✓ Possibly ✓
Acute respiratory failure 2 11.8 Severe ✓ Doubtful ✓(one)Nausea/vomiting 3 17.7 Mild DoubtfulHeadache 2 11.8 Mild PossiblyUTI 1 5.9 Moderate Not relatedNon-ST-elevation myocardial infarction 1 5.9 Moderate Not relatedConstipation leading to nausea/vomiting 1 5.9 Moderate Possibly
PlaceboRash 1 20 Moderate DoubtfulNeurological deterioration requiring osmotherapy 1 20 Severe ✓ Possibly ✓
Nausea/vomiting 1 20 Mild DoubtfulHeadache treated with mannitol 1 20 Severe ✓ Possibly ✓
Administration error 1 20 Severe ✓ Not related
Adverse events (AE) and severe adverse events (SAEs) are listed by study group. Those AE/SAE which were likely or possibly related to study drug infusion are highlighted in grey. SAEswere reported to our local IRB, as well as to the pharmaceutical company per request.IRB, institutional review board; LFT, liver function test; UTI, urinary tract infection.
Figure 3 Categorical vasospasm outcomes. Different predefined categories of vasospasm were analysed and shown. ‘Delayed’ transcranial Doppler(TCD) and angiogram vasospasm represents occurrence after the 7-day infusion period. This was analysed to determine presence of reboundvasospasm after the completion of study drug infusion. ‘TCD vasospasm’ refers to only the 7-day infusion period. Clinical vasospasm and delayedcerebral ischaemia (DCI) refer to the entire hospital course. p Values <0.05 were considered significant.
Muehlschlegel S, et al. J Neurol Neurosurg Psychiatry 2014;0:1–7. doi:10.1136/jnnp-2014-308778 5
Cerebrovascular disease
group.bmj.com on October 27, 2014 - Published by http://jnnp.bmj.com/Downloaded from

additional patients before and after a dose of IV-D.7
Subsequently, in an ex vivo rat vasoconstriction model,4 andthen in patients with aSAH receiving a single dose of IV-D,vasorelaxation was noted.8 Most recently, intra-arterially
administered dantrolene induced a sustained improvement ofsevere, refractory cVSP in a single patient with aSAH.14
Dantrolene’s additional advantageous effect, neuroprotection,should be specifically highlighted.2 3 15 16 Two recent largetrials testing the endothelin-1 antagonist clazosentan for cVSPafter aSAH17 18 dampened the enthusiasm for drugs only target-ing vasoconstriction after aSAH. Both studies showed improve-ments in cVSP without gains in functional neurologicaloutcome. Therefore, pharmacological interventions providingadditional neuroprotective effects and not merely treating cVSPmay offer more hope of improving outcome.
Our trial has several limitations. First, its single-centre designrestricts generalisability. Next, instead of normal saline theplacebo group consisted of free water with 5% mannitol toachieve the same equiosmolar solution as IV-D, which requiresreconstitution in free water. Therefore, we could not differentiatewhether the effects on hyponatraemia or brain oedema may havebeen due to IV-D or its solution. We chose this placebo overnormal saline in this initial safety study to evaluate whether dan-trolene itself, and not its solution, may have detrimental effectson patients with aSAH. Mannitol may have contributed to hypo-natraemia; however, both groups received the same concentra-tion of mannitol, and therefore a differential effect of mannitolon hyponatraemia on one of the treatment groups is unlikely.The small sample size warrants great caution when interpretingour outcomes, even when statistical significance lacked.Furthermore, 76% of patients screened were excluded. Lookingclosely at the screen failures, many patients were excludedbecause they were too sick and at extremely high risk for death,or were angio negative. The 7-day infusion time-period may nothave covered the entire cVSP risk period, limiting full explorationof potential efficacy on cVSP and functional outcomes. We didobserve, however, but did not systematically analyse, hesitancy ofpatients and surrogates to consent to the trial due to thenever-previously-studied length of IV-D infusion. A 14-day infu-sion may have resulted in much lower consent rates, renderingthe study protocol unfeasible. The method of block randomisa-tion did not fully prevent group imbalances regarding baselinecharacteristics. However, we feel that the racial and minor imbal-ances in aneurysm location did not contribute to the primaryoutcome, and unlikely contributed to the secondary outcomes.19
Finally, difficulties with technique resulted in a very low numberof TCD Lindegaard ratios. Therefore, we cannot confidentlyclaim that elevated TCD velocities were due to cVSP.
To our knowledge, this is the first randomised trial ofrepeated IV-D infusions conducted in critically ill patients withaSAH. Its strengths include bias avoidance by randomisation,double blind design and treatment standardisation by protocols.
CONCLUSIONWe have demonstrated that repeated IV-D infusions over 7 daysare feasible, and likely safe and well tolerated in critically illpatients with aSAH. A larger multicentre study using normalsaline as placebo is required to confirm safety and explore effi-cacy trends prior to moving to a phase-III trial.
Author affiliations1Departments of Neurology (Neurocritical Care), University of Massachusetts MedicalSchool, Worcester, Massachusetts, USA2Department of Anesthesia/Critical Care, University of Massachusetts MedicalSchool, Worcester, Massachusetts, USA3Department of Surgery, University of Massachusetts Medical School, Worcester,Massachusetts, USA4Department of Quantitative Health Sciences, University of Massachusetts MedicalSchool, Worcester, Massachusetts, USA
Figure 4 Functional outcomes. Depicted are functional neurologicaloutcomes at 3 months postaneurysmal subarachnoid haemorrhage. Inthe placebo group, two patients withdrew consent during the infusionperiod, and one patient was lost to follow-up. Figure legends indicatethe number of participants for each scale category. Barthel Index isshown as median with IQR, and individual data points. p Values <0.05were considered significant.
6 Muehlschlegel S, et al. J Neurol Neurosurg Psychiatry 2014;0:1–7. doi:10.1136/jnnp-2014-308778
Cerebrovascular disease
group.bmj.com on October 27, 2014 - Published by http://jnnp.bmj.com/Downloaded from

5Department of Radiology, University of Massachusetts Medical School, Worcester,Massachusetts, USA6Department of Neurosurgery, University of Massachusetts Medical School,Worcester, Massachusetts, USA
Acknowledgements The authors appreciate the tremendous support of theLakeside2-ICU clinical staff for their support and adherence to study protocols. Theauthors thank the DSMB: Raul Nogueira, MD and Stephen Baker, MScPH, PhD(ABD).
Contributors SM designed the trial, obtained funding, implemented the trial,designed data collection tools, recruited patients, performed transcranial Dopplerstudies, monitored data collection for the whole trial, wrote the statistical analysisplan, cleaned and analysed the data, drafted and revised the paper. She isguarantor. RC recruited patients, performed transcranial Doppler studies and revisedthe paper. WH recruited patients and revised the paper. NK cleaned and analysedthe data, drafted and revised parts of the paper. SI cleaned part of the data,performed quantitative angiogram measurements and monitored data collection forpart of the trial. BG designed data collection tools, recruited patients, cleaned partof the data, performed quantitative angiogram measurements, performedtranscranial Doppler studies, monitored data collection for part of the trial andrevised the paper. CO recruited patients, cleaned part of the data, performedtranscranial Doppler studies, monitored data collection for part of the trial andrevised the paper. IMJV performed quantitative angiogram measurements andrevised the paper. TFF performed quantitative angiogram measurements and revisedthe paper. MJG designed data collection tools, performed quantitative angiogrammeasurements, cleaned and analysed part of the data. JPW implemented the trialand revised the paper. BB wrote the statistical analysis plan, and analysed the data.He is guarantor. AKW implemented the trial and revised the paper.
Funding American Heart Association (09SDG2030022), Worcester Foundation forBiomedical Research, UMASS Medical School Faculty Scholar Award, UMASS Centerfor Clinical & Translational Science, funded by the National Center for AdvancingTranslational Sciences at the National Institutes of Health (NIH Grant#UL1TR000161). The study drug dantrolene (Dantrium IV) was donated by JHPPharmaceuticals (Parsippany, New Jersey, USA).
Competing interests The study was entirely investigator-initiated.
Ethics approval UMASS Medical School Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.
REFERENCES1 Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke statistics—2014
update: a report from the American Heart Association. Circulation 2014;129:e28–292.2 Frandsen A, Schousboe A. Dantrolene prevents glutamate cytotoxicity and Ca2+
release from intracellular stores in cultured cerebral cortical neurons. J Neurochem1991;56:1075–8.
3 Muehlschlegel S, Sims JR. Dantrolene: mechanisms of neuroprotection and possibleclinical applications in the neurointensive care unit. Neurocrit Care 2009;10:103–15.
4 Salomone S, Soydan G, Moskowitz MA, et al. Inhibition of cerebral vasoconstrictionby dantrolene and nimodipine. Neurocrit Care 2009;10:93–102.
5 Tani E, Matsumoto T. Continuous elevation of intracellular Ca2+ is essentialfor the development of cerebral vasospasm. Curr Vasc Pharmacol 2004;2:13–21.
6 Williams DA, Becker PL, Fay FS. Regional changes in calcium underlying contractionof single smooth muscle cells. Science 1987;235:1644–8.
7 Muehlschlegel S, Rordorf G, Bodock M, et al. Dantrolene mediatesvasorelaxation in cerebral vasoconstriction: a case series. Neurocrit Care2009;10:116–21.
8 Muehlschlegel S, Rordorf G, Sims J. Effects of a single dose of dantrolene inpatients with cerebral vasospasm after subarachnoid hemorrhage: a prospectivepilot study. Stroke 2011;42:1301–6.
9 Dantrolene. Secondary Dantrolene. Last Update 10/2009. http://dailymed.nlm.nih.gov/dailymed/lookup.cfm?setid=4df35098–8702-46be-ac67-30cfdf1aa570(accessed 4 Aug 2014).
10 Schulz KF, Altman DG, Moher D, et al. CONSORT 2010 statement:updated guidelines for reporting parallel group randomised trials. BMJ 2010;340:c332.
11 Bederson JB, Connolly ES Jr, Batjer HH, et al. Guidelines for the management ofaneurysmal subarachnoid hemorrhage: a statement for healthcare professionals froma special writing group of the Stroke Council, American Heart Association. Stroke2009;40:994–1025.
12 Diringer MN, Bleck TP, Claude Hemphill J III, et al. Critical care management ofpatients following aneurysmal subarachnoid hemorrhage: recommendations fromthe Neurocritical Care Society’s Multidisciplinary Consensus Conference. NeurocritCare 2011;15:211–40.
13 Linfante I, Delgado-Mederos R, Andreone V, et al. Angiographic and hemodynamiceffect of high concentration of intra-arterial nicardipine in cerebral vasospasm.Neurosurgery 2008;63:1080–6; discussion 86–7.
14 Majidi S, Grigoryan M, Tekle WG, et al. Intra-arterial dantrolene for refractorycerebral vasospasm after aneurysmal subarachnoid hemorrhage. Neurocrit Care2012;17:245–9.
15 Frandsen A, Schousboe A. Mobilization of dantrolene-sensitive intracellular calciumpools is involved in the cytotoxicity induced by quisqualate andN-methyl-D-aspartate but not by 2-amino-3-(3-hydroxy-5-methylisoxazol-4-yl)propionate and kainate in cultured cerebral cortical neurons. Proc Natl Acad SciUSA 1992;89:2590–4.
16 Zhang L, Andou Y, Masuda S, et al. Dantrolene protects against ischemic, delayedneuronal death in gerbil brain. Neurosci Lett 1993;158:105–8.
17 Macdonald RL, Higashida RT, Keller E, et al. Clazosentan, an endothelin receptorantagonist, in patients with aneurysmal subarachnoid haemorrhage undergoingsurgical clipping: a randomised, double-blind, placebo-controlled phase 3 trial(CONSCIOUS-2). Lancet Neurol 2011;10:618–25.
18 Macdonald RL, Higashida RT, Keller E, et al. Randomised trial of clazosentan, anendothelin receptor antagonist, in patients with aneurysmal subarachnoidhemorrhage undergoing surgical clipping (CONSCIOUS-2). Acta Neurochir Suppl2013;115:27–31.
19 Rosen D, Novakovic R, Goldenberg FD, et al. Racial differences in demographics,acute complications, and outcomes in patients with subarachnoid hemorrhage: alarge patient series. J Neurosurg 2005;103:18–24.
Muehlschlegel S, et al. J Neurol Neurosurg Psychiatry 2014;0:1–7. doi:10.1136/jnnp-2014-308778 7
Cerebrovascular disease
group.bmj.com on October 27, 2014 - Published by http://jnnp.bmj.com/Downloaded from

double blind placebo-controlled safety trialsubarachnoid haemorrhage: a randomised Dantrolene for cerebral vasospasm after
and Ajay K WakhlooBom, Thomas F Flood, Matthew J Gounis, John P Weaver, Bruce BartonSaef Izzy, Bridget Garland, Cynthia Ouillette, Imramsjah M J van der Susanne Muehlschlegel, Raphael Carandang, Wiley Hall, Nisha Kini,
published online October 24, 2014J Neurol Neurosurg Psychiatry
http://jnnp.bmj.com/content/early/2014/10/24/jnnp-2014-308778Updated information and services can be found at:
MaterialSupplementary
htmlhttp://jnnp.bmj.com/content/suppl/2014/10/24/jnnp-2014-308778.DC1.Supplementary material can be found at:
These include:
References #BIBLhttp://jnnp.bmj.com/content/early/2014/10/24/jnnp-2014-308778
This article cites 18 articles, 6 of which you can access for free at:
serviceEmail alerting
box at the top right corner of the online article. Receive free email alerts when new articles cite this article. Sign up in the
CollectionsTopic Articles on similar topics can be found in the following collections
(1329)Stroke (344)Hypertension
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on October 27, 2014 - Published by http://jnnp.bmj.com/Downloaded from





























