Embed Size (px)
Citation preview

753
ReseaRch aRticle
ISSN 1750-743XImmunotherapy (2009) 1(5), 753–76410.2217/IMT.09.47 © 2009 Future Medicine Ltd Immunotherapy (2009) 1(5), 753–764
Safety ana lysis of ex vivo-expanded NK and NK-like T cells administered to cancer patients: a Phase I clinical study
Adoptive transfer of cytotoxic effector cells with tumor cell-killing potential in order to induce a graft-versus-tumor (GvT) effect has been one of the most attractive approaches against cancer. Natural killer (NK) and NK-like T cells consti-tute a relatively high cytotoxic capacity among other effector-cell populations having a potential antitumor effect [1–3]. However, the low numbers of these cells in peripheral blood mononuclear cells (PBMCs) and effector-cell preparations, such as lymphokine-activated killer (LAK) cells, represents one main barrier for their use in clini-cal trials and future use as a cancer therapy [4,5]. We have previously reported a novel method that embraces components compliant with current good manufacturing practice (cGMP) condi-tions that enables the expansion of polyclonal NK and NK-like T cells using PBMCs acquired from healthy donors [6] and patients with B-cell chronic lymphocytic leukemia (B-CLL) [7] and multiple myeloma [8]. These cells showed cyto-toxic activity against fresh human tumor cells in vitro [8] and in experimental models of human tumors [9], a response that stimulated evaluation in clinical settings. This cell preparation strongly differs from LAK and cytokine-induced killer (CIK) cells both in terms of NK cell content and antitumor activity [10–13]. Our previous [6–8] and present data show that during the 20-day ex vivo expansion period, the main increase in both NK
cell number and antitumor activity starts after 5 days of culture, which is the upper time limit for LAK cell cultures [14]. In addition, our final product is rich in CD3- CD56+ NK cells unlike CIK cells [6–8].
In the present study, we evaluated the safety of such effector cell populations as donor lym-phocyte infusions (DLIs) following allogeneic hematopoietic stem cell transplantation (SCT) to patients with progressive malignant disease. The PBMCs were obtained from individuals who had earlier donated allogeneic stem cells grafted to the patients. This study is the first to report the safety of ex vivo-expanded NK and NK-like T cells with a feeder-free cGMP compatible expansion strategy administered to humans as a potential immunotherapy for cancer.
Patients, donors & methods � Clinical protocol
The local research ethics committee of Karolinska University Hospital Huddinge, Stockholm, Sweden, approved the proto-col. Informed consent was obtained from all patients and donors of PBMCs for cell expan-sion. Donors of PBMCs were the HLA-A, -B, -DRb1, -DQa1 and -DQb1 identical siblings who had previously donated hematopoietic stem cells for transplantation in all patients. Apheresis was performed without preceding granulocyte
The chimeric state after allogeneic hematopoietic stem cell transplantation provides a platform for adoptive immunotherapy using donor-derived immune cells. The major risk with donor lymphocyte infusions (DLIs) is the development of graft-versus-host disease (GvHD). Development of new DLI products with antitumor reactivity and reduced GvHD risk represents a challenging task in cancer immunotherapy. Although natural killer (NK) and NK-like T cells are promising owing to their antitumor activity, their low concentrations in peripheral blood mononuclear cells reduces their utility in DLIs. We have recently developed a system that allows expansion of clinical-grade NK and NK-like T cells in large numbers. In this study, the safety of donor-derived long-term ex vivo-expanded human NK and NK-like T cells given as DLIs was investigated as immunotherapy for cancer in five patients following allogeneic stem cell infusion. Infusion of the cells was safe whether administered alone or with IL-2 subcutaneously. No signs of acute GvHD were observed. One patient with hepatocellular carcinoma showed markedly decreased serum a-fetoprotein levels following cell infusions. These findings suggest that the use of ex vivo-expanded NK and NK-like T cells is safe and appears an attractive approach for further clinical evaluation in cancer patients.
KEYWORDS: cellular immunotherapy � donor lymphocyte infusion � ex vivo expansion � hematopoietic stem cell transplantation � NK cell � NK-like T cell
Lisbeth Barkholt1†, Evren Alici1, Reka Conrad1, Tolga Sutlu1, Mari Gilljam1, Birgitta Stellan1, Birger Christensson1,
Hayrettin Guven1, Niklas K Björkström1, Gunnar Söderdahl1, Kerstin Cederlund1,Eva Kimby1, Johan Aschan1, Olle Ringdén1, Hans-Gustaf Ljunggren1,
& M Sirac Dilber1
†Author for correspondence:1Karolinska University Hospital Huddinge F79, SE-14186, Stockholm, SwedenTel.: +46 858 580 000 ext. 81388 Fax: +46 87 46 [email protected]
For reprint orders, please contact: [email protected]

Immunotherapy (2009) 1(5)754 future science group
ReseaRch aRticle Barkholt, Alici, Conrad et al.
colony-stimulating factor stimulation. The patients included in this study protocol had undergone allogeneic SCT for colorectal car-cinoma (CRC; P1), hepatocellular carcinoma (HCC; P2), renal cell carcinoma (RCC; P3 and P5) and B-CLL (P4). The patient characteristics are presented in Table 1. Donors and patients were tested for active virus infections (HIV, hepatitis B virus, hepatitis C virus [HCV], cytomegalo-virus and Epstein–Barr virus) using PCR before PBMC donation as well as after infusion of the ex vivo-expanded cells.
� Ex vivo cell expansionPeripheral blood mononuclear cells were harvested by apheresis using a Baxter CS 3000 unit (Baxter AB, Sweden). Expansion of apheresis products ex vivo was performed under conditions that were compliant with GMP conditions. Briefly, after assessing viability by Trypan blue dye exclu-sion, PBMCs were cultured at 0.5 × 106 cells/ml in serum-free medium, Cellgro (CellGenix, Freiburg, Germany) containing 5% heat-inacti-vated human AB serum (Biowhittaker, MD, USA) and 500 U/ml recombinant IL-2 (Proleukin, Chiron, Amsterdam, The Netherlands) for 20 days. Cells in the culture were stimulated with anti-CD3 antibody (OKT3, Orthoclone, Ortho Biotech Inc., NJ, USA) at a final concentration of 10 ng/ml for the first 5 days. After day 5, IL-2 sup-plementation together with fresh medium without OKT3 continued throughout the remaining cul-ture period on a regular basis. Absolute nucleated cell numbers and viability were analyzed on days 0, 9, 14, and 19 of culture. The first infusion was
given to patients from the cultured cells freshly, and the remaining expanded cells were cryopre-served at -170°C for subsequent infusions unless o therwise noted.
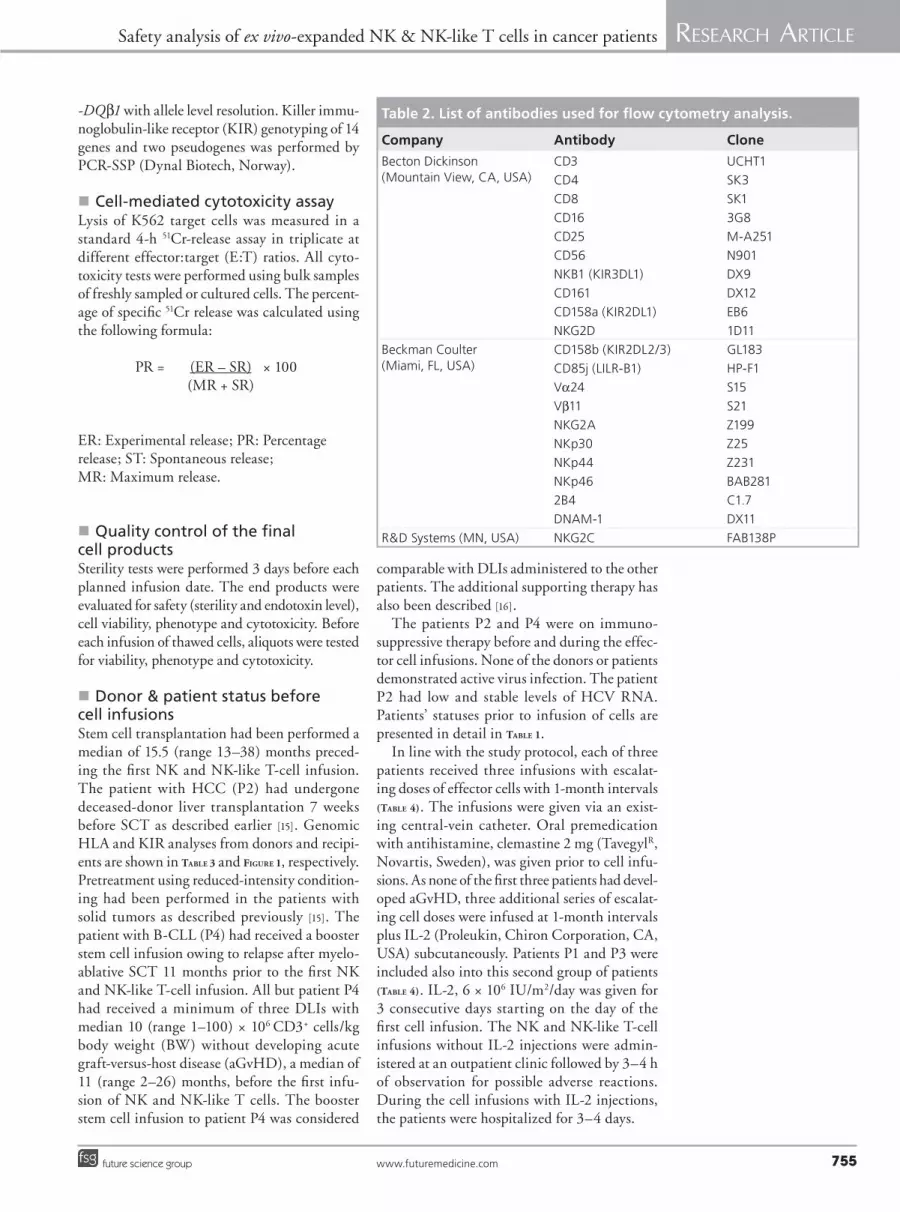
� Phenotypic ana lysisThe phenotype of expanded cells was analyzed by flow cytometry on days 0, 9, 14 and 19 of culture. Briefly, cells were mixed with appropriate concen-trations of fluorochrome-conjugated monoclonal antibodies (mAbs) to cell surface markers accord-ing to Table 2. After the addition of mAbs and incubation for 30 min at +4ºC, cells were washed with phosphate-buffered saline (PBS) before ana-lysis. Propidium iodide (PI) staining was used for exclusion of dead cells. For data acquisition and ana lysis either four-color or nine-parameter flow cytometry was used. Four-color flow cytom-etry was performed with a FACSCalibur (BD, Becton Dickinson, CA, USA) and Cell Quest software (BD). Nine-parameter f low cytom-etry was done with a Cyan ADP flow cytometer (DAKO Cytomation Norden AB, Sweden) and Summit software (DAKO Cytomation Norden AB, Sweden). Each sample contained a mini-mum of 10,000 (FACSCalibur) or 100,000 gated lymphocytes (Cyan ADP).
� HLA & killer immunoglobulin-like receptor typingGenomic HLA typing was performed using PCR amplification with sequence-specific prim-ers (PCR-SSP) (Olerup SSPTM, Sweden). Donors and patients were typed for HLA-A and -B at low resolution and for HLA-C, -DRb1, -DQa1 and
Table 1. Patient characteristics and status before the first NK/NK-like T-cell (CD56+) infusion.
Patient Diagnosis Sex Age (years)
PBLchimerism
Immuno-suppression
Location of metastases§
Time since last DLI (months)
GvHD Additional tumor debulking (months)
KIR allo-reactivity
P1 CRC M 67 DC No 1, 2, 3, 4 7 No RFA liver met/(3.5)
No
P2 HCC M 48 DC Yes* 3, 4 2 No 0 No
P3 RCC M 50 DC No 1, 2, 3, 4 13 Limited cGvHD#
RFA liver met/(16)IRD lung met/(16)
No
P4 CLL F 59 100% recipient CD19+ cells
Yes‡ 5 11¶ No 0 No
P5 RCC M 54 DC No 1,3 26 Limited cGvHD#
surgery of lung met/(2)
Yes
*Tacrolimus 0.006–0.1 mg/kg BW; ‡Prednisolon 0.8 mg/kg BW; §1 = lymph node (LN) mediastinum; 2 = liver; 3 = lung; 4 = pleura; 5 = LN abdomen; ¶After booster stem cell infusion; #No active chronic GvHD 11 months prior to the first NK/NK-like T-cell infusion.All donors were siblings. KIR alloreactivity was determined by donor KIR ligand missing in the recipient.BW: Body weight; CLL: Chronic lymphocytic leukemia; CRC: Colorectal carcinoma; DC: Total donor chimera of CD3+, CD19+, CD33+ cells; DLI: Donor lymphocyte infusion; F: Female; GvHD: Graft-versus-host disease; HCC: Hepatocellular carcinoma; IRD: Stereotactic irradiation; KIR: Killer immunoglobulin-like receptor; M: Male; met: Metastases; PBL: Peripheral blood lymphocytes; RCC: Renal cell carcinoma; RFA: Radiofrequency ablation.
www.futuremedicine.com 755future science group
Safety ana lysis of ex vivo-expanded NK & NK-like T cells in cancer patients ReseaRch aRticle
-DQb1 with allele level resolution. Killer immu-noglobulin-like receptor (KIR) genotyping of 14 genes and two pseudogenes was p erformed by PCR-SSP (Dynal Biotech, Norway).
� Cell-mediated cytotoxicity assayLysis of K562 target cells was measured in a standard 4-h 51Cr-release assay in triplicate at different effector:target (E:T) ratios. All cyto-toxicity tests were performed using bulk samples of freshly sampled or cultured cells. The percent-age of specific 51Cr release was calculated using the following formula:
PR = (ER – SR) (MR + SR)
ER: Experimental release; PR: Percentage release; ST: Spontaneous release; MR: Maximum release.
� Quality control of the final cell productsSterility tests were performed 3 days before each planned infusion date. The end products were evaluated for safety (sterility and endotoxin level), cell viability, phenotype and cytotoxicity. Before each infusion of thawed cells, aliquots were tested for viability, phenotype and cytotoxicity.
� Donor & patient status before cell infusionsStem cell transplantation had been performed a median of 15.5 (range 13–38) months preced-ing the first NK and NK-like T-cell infusion. The patient with HCC (P2) had undergone deceased-donor liver transplantation 7 weeks before SCT as described earlier [15]. Genomic HLA and KIR analyses from donors and recipi-ents are shown in Table 3 and Figure 1, respectively. Pretreatment using reduced-intensity condition-ing had been performed in the patients with solid tumors as described previously [15]. The patient with B-CLL (P4) had received a booster stem cell infusion owing to relapse after myelo-ablative SCT 11 months prior to the first NK and NK-like T-cell infusion. All but patient P4 had received a minimum of three DLIs with median 10 (range 1–100) × 106 CD3+ cells/kg body weight (BW) without developing acute graft-versus-host disease (aGvHD), a median of 11 (range 2–26) months, before the first infu-sion of NK and NK-like T cells. The booster stem cell infusion to patient P4 was considered
comparable with DLIs administered to the other patients. The additional supporting therapy has also been described [16].
The patients P2 and P4 were on immuno-suppressive therapy before and during the effec-tor cell infusions. None of the donors or patients demonstrated active virus infection. The patient P2 had low and stable levels of HCV RNA. Patients’ statuses prior to infusion of cells are presented in detail in Table 1.
In line with the study protocol, each of three patients received three infusions with escalat-ing doses of effector cells with 1-month intervals (Table 4). The infusions were given via an exist-ing central-vein catheter. Oral premedication with antihistamine, clemastine 2 mg (TavegylR, Novartis, Sweden), was given prior to cell infu-sions. As none of the first three patients had devel-oped aGvHD, three additional series of escalat-ing cell doses were infused at 1-month intervals plus IL-2 (Proleukin, Chiron Corporation, CA, USA) subcutaneously. Patients P1 and P3 were included also into this second group of patients (Table 4). IL-2, 6 × 106 IU/m2/day was given for 3 consecutive days starting on the day of the first cell infusion. The NK and NK-like T-cell infusions without IL-2 injections were admin-istered at an outpatient clinic followed by 3–4 h of observation for possible adverse reactions. During the cell infusions with IL-2 injections, the patients were hospitalized for 3–4 days.
Table 2. List of antibodies used for flow cytometry ana lysis.
Company Antibody Clone
Becton Dickinson(Mountain View, CA, USA)
CD3 UCHT1
CD4 SK3
CD8 SK1
CD16 3G8
CD25 M-A251
CD56 N901
NKB1 (KIR3DL1) DX9
CD161 DX12
CD158a (KIR2DL1) EB6
NKG2D 1D11
Beckman Coulter(Miami, FL, USA)
CD158b (KIR2DL2/3) GL183
CD85j (LILR-B1) HP-F1
Va24 S15
Vb11 S21
NKG2A Z199
NKp30 Z25
NKp44 Z231
NKp46 BAB281
2B4 C1.7
DNAM-1 DX11
R&D Systems (MN, USA) NKG2C FAB138P
× 100

Immunotherapy (2009) 1(5)756 future science group
ReseaRch aRticle Barkholt, Alici, Conrad et al.
� Follow-up of patientsVital signs and symptoms of patients were moni-tored on the days they received cell infusions and the days they provided blood samples. Peripheral blood samples were obtained 1 h before, 1 h after, 1 week after, and monthly for 3 months following each cell infusion. Blood chemistry analyses for safety included hemoglobin (Hb), total white blood cell, neutrophil and platelet counts, C-reactive protein (CRP), liver, kidney and pancreas function tests. a-fetoprotein (AFP) and HCV load were assessed for the patient P2
with HCC using quantitative PCR. The patients’ peripheral blood samples were analyzed for sol-uble serum cytokines (sIL-2R, IL-6, TNF-a, IL-8 and IL-10) using ELISA (Immulite, DPC, CA, USA or Quantikine ELISA kits, R&D Systems, MN, USA) and for lymphocyte sur-face molecules (CD3, CD4, CD5, CD8, CD16, CD19, CD25, CD52, CD56, CD69; BD) using flow cytometry.
Tumor load was evaluated using computed tomography (CT) performed within 1 month before and at 3 as well as 6 (if possible) months
Table 3. Genotyping of HLA in infused patients and their respective donors.
Patient/ donor
HLA-A HLA-B HLA-C HLA-DRb1 HLA-DQa1 HLA-DQb1
P1D1
A*02, A*03A*02, A*03
B*44, B*62B*44, B*62
C*0304, C*0501C*0304, C*0501
DRb1*0401DRb1*0401
DQa1*0301, DQa1*0303DQa1*0301, DQa1*0303
DQb1*0301, DQb1*0302DQb1*0301, DQb1*0302
P2D2
A*02A*02
B*08, B*44B*08, B*44
C*0501, C*0701C*0501, C*0701
DRb1*0101, DRb1*0301DRb1*0101, DRb1* 0301
DQa1*0101, DQa1*0501DQa1*0101, DQa1*0501
DQb1*0201, DQb1*0501DQb1*0201, DQb1*0501
P3D3
A*02, A*11A*02, A*11
B*56, B*57B*56, B*57
C*0102, C*0602C*0102, C*0602
DRb1*0101, DRb1*0701DRb1*0101, DRb1*0701
DQa1*0101, DQa1*0201DQa1*0101, DQa1*0201
DQb1*0301, DQb1*0501DQb1*0301, DQb1*0501
P4D4
A*01, A*19A*01, A*19
B*05, B*08B*05, B*08
C*0102, C*0704C*0102, C*0704
DRb1*1301, DRb1*1302DRb1*1301, DRb1*1302
DQa1*0102, DQa1*0302DQa1*0102, DQa1*0302
DQb1*0303, DQb1*0609DQb1*0303, DQb1*0609
P5D5
A*02, A*03A*02, A*03
B*14, B*15B*14, B*15
C*0303, C*0802C*0303, C*0802
DRb1*0103, DRb1*1301DRb1*0103, DRb1*1301
DQa1*0103, DQa1*0505DQa1*0103, DQa1*0505
DQb1*0301, DQb1*0601DQb1*0301, DQb1*0601
3DL3
2DL3
2DL3
2DL2
2DL2
2DL33DL3
3DL3
3DL3
3DL3
3DL3
3DL3
3DL3
3DL3
3DL3
3DL3
2DL22DL3
2DL22DL3
2DL22DL3
2DL22DL3
2DL22DL3
3DS13DL1
3DS13DL1
2DS32DS5 2DL1
2DL1 2DL4
2DL4
2DL4
2DL4
2DL4
2DL4
2DL4
2DL4
2DL4
2DL4
2DL1
2DL1
2DL1
2DL1
2DL1
2DL1
2DL1
2DL1
2DL1
2DL42DP1
2DP1
2DP1
2DP1
2DP1
2DP1
2DP1
2DP1
2DP1
2DP1
2DP1
3DP1
3DP1
3DP1
3DP1
3DP1
3DP1
3DP1
3DP1
3DP1
3DP1
3DP1
2DL5B
2DL5B
2DL5B
2DL5B
2DL5 3DL2
3DL23DL1
3DL1
3DL1
3DL1
3DL1
3DL1
3DL1
3DL1
3DL1
3DL2
3DL2
3DL2
3DL2
3DL2
3DL2
3DL2
3DL2
3DL2
2DS2
2DS3
2DS3
2DS3
2DS3
2DS2
2DS2
2DS2
2DS2
2DS2
2DS2
2DS3 2DS5 2DS1
2DS1
2DS4
2DS4
2DS4
2DS4
2DS4
2DS4
2DS4
2DS4
2DS4
2DS4
2DS4
Human KIR locus
Ligands ? ? ? ? ? ?- -Asn80 Asn80 Lys80 Lys80 Lys80HLA-G HLA-ABw4
P1
D1
P2
D2
P3
D3
P4
D4
P5
D6
Figure 1. Genotyping of killer immunoglobulin-like receptor in infused patients and their representative donors. Asn80, HLA-C type 1; Lys80, HLA-C type 2.

www.futuremedicine.com 757future science group
Safety ana lysis of ex vivo-expanded NK & NK-like T cells in cancer patients ReseaRch aRticle
after the last cell infusion. The follow-up of patients for this study was 6 months after the last NK and NK-like T-cell infusions.
� DefinitionsAcute GvHD was graded from 0 to IV as previ-ously reported [17]. Chronic GvHD was evaluated in patients surviving more than 90 days after SCT and classified as limited or extensive [18]. Tumor response was scored according to the international Response Evaluation Criteria in Solid Tumors (RECIST) using CT scanning of thorax and abdomen. Partial regression of solid malignancy was defined as greater than 30% decrease in the sum of the largest diameters of metastases com-pared with measurements before SCT. Progressive disease was defined as greater than 20% increase of measurable sites of the disease at time of SCT. Total donor chimerism was defined as greater than 95% of each cell population being of donor type (CD3+, CD19+ and CD33+). Adverse events were coded using the bleeding score taken into account the highest value per item giving a maximum score of 64 [19] and the Common Terminology Criteria for Adverse Events (CTCAE) version 3.0.
Results � Expansion & characterization of
cells ex vivo For ex vivo expansion of NK and NK-like T-effector cell populations, apheresis products from peripheral blood of donors were either cul-tured immediately or frozen for future expan-sion. The expansion rates were similar whether cells were cultured freshly or cultured after being frozen and thawed (data not shown). The end product was harvested at day 19 after initiation
of cell culture. By the end of the expansion, the total cell population had expanded on average 1036-fold (Figure 2A).
Preceding infusions, the end product of ex vivo-expanded cells passed the quality con-trols. The median viability of thawed cells before each infusion was 88% (range from 82 to 95%). The effector cell population was analyzed for a detailed phenotypic characterization. The ex vivo expansion protocol promoted growth of CD56+ cells as previously observed (Figures 2b, 2C,
3 & 4) [6]. In line with previous observations [6], the expanded cells showed a marked increase in cytotoxicity against K562 cells compared with freshly isolated (day 0) effector cells (Figure 5).
� Cell infusionsEach of the first three patients (P1, P2 and P3) received three escalating doses of expanded NK and NK-like T cells at 1-month intervals: 1 × 106, 10 × 106 and a median of 13.2 (range from 8.1 to 40.3) × 106 NK and NK-like T cells/kg BW in the first, second, and the third infusion, respectively. These patients were not given IL-2 subcutaneous. Since none of these patients presented aGvHD, the next group of patients (P1A2, P3A2, P4 and P5) was given similar escalating doses of effector cells at one-month intervals together with sub-cutaneous IL-2 injections. Infused doses of total effectors as well as NK and NK-like T-cell num-bers are presented in Table 4. The third infusion was less than the aimed 108 CD56+ cells/kg BW due to the per protocol-defined expansion time.
� Signs & side effectsInfusion of the ex vivo-expanded effector cells was performed in the first three patients at an
Table 4. NK/NK-like T (CD56+) cell infusions.
Patient 1st infusion 2nd infusion 3rd infusion* sc. IL-2 injec-tions
Time after SCT (months)
Totalcell dose(×106/kg)
CD56+ cell dose(×106/kg)
Time after SCT (months)
Totalcell dose(×106/kg)
CD56+ cell dose(×106/kg)
Time after SCT (months)
Total cell dose(×106/kg)
CD56+ cell dose(×106/kg)
P1 13 2.9 1.0 14 26.3# 8.2# 15 26.3# 8.1# No
P2 15 2.4 1.0 16 29.0 # 9.6 # 17 48.2# 13.2# No
P3 28 1.4 # 1.0 # 29 13.3# 9.9# 30 49.8 # 40.3# No
P1A2§ 20 10 5 NG NG Yes
P3A2¶ 36 1.8 # 1.0 # 37 19.1# 10.1# 40 48.2 28.8 Yes
P4 15.5‡ 4.6 1.0 16.5 44.5 # 9.6 # 26.5 42.3# 17.3# Yes
P5 38 2.0 1.1 39 23.8 7.0 41 21.3# 7.4 # Yes
*Less than per protocol dose of 100 × 106 CD56+ cells/kg infused owing to limited cell expansion time to 19 days.‡After booster stem cell infusion.§Patient P1A2 received only one cell dose owing to Staphylococcus epidermidis-contaminated cells and was treated with systemic antibiotics giving a subsequent recover after 1 week. ¶Cells infused from second apheresis.#Infusion of frozen and thawed product.NG: Not given; sc.: Subcutaneous; SCT: Stem cell transplantation.

Immunotherapy (2009) 1(5)758 future science group
ReseaRch aRticle Barkholt, Alici, Conrad et al.
outpatient clinic and was well tolerated. No aGvHD was observed. P2 presented melena (bleeding score 15/64) 4 days after the second and 37 days after the third effector-cell infu-sion (Table 5). The patient had an extensive por-tal thrombosis at the time of liver transplanta-tion and the portal vein of the graft had to be connected end-to-end to the patient’s inferior caval vein (portocaval transposition). Thus, the patient still presented portal hypertension
and recurrent hemorrhagic episodes due to esophageal and rectal varices 1 year following liver transplantation (5 months prior to the NK and NK-like T-cell infusions). The same varices were demonstrated by repeated gastroscopy and colonoscopy examinations performed between the first and second, as well as 7 weeks after the third effector cell infusion, respectively. Patient P3 presented a sicca syndrome 1 week after the third cell infusion (Table 5). This patient had a history of aGvHD grade II 6 months after the SCT followed by a limited chronic GvHD of the skin. However, the patient had no clinical GvHD activity since 11 months before the first NK and NK-like T cell infusions (P3; Table 1).
Patients in the second group received NK and NK-like T-cell infusions and subcutaneous IL-2 injections at the hospital ward. All of them developed low-grade fever up to 1 week after the infusions (Table 5). Patient P1A2 developed septicemia of Staphylococcus epidermidis with high fever and chills (grade 4; CTCAE) due to infusion of contaminated NK and NKT cell patch. The patient was treated with intra venous antibiotics and recovered within 1 week with-out sequel. Two other patients (P4 and P5) suffered from reversible dermatological side effects (Table 5). Two patients (P3A2 and P5) with previous progression of lung metastases had hemoptysis with spontaneous regression within 24 h (bleeding score 4/64). Eventually, one developed pneumonia and the other an upper respiratory tract infection (grades 3 and 2, respectively; CTCAE). Overall, no signs attributable to aGvHD were observed.
� Laboratory parameters in patients following cell infusionsPatients’ PBMCs were analyzed before and routinely after the cell infusions for up to 3 months. Interestingly, as indicated in Figure 6, numbers of NK, NK-like T, aswell as T cells in the patients’ peripheral blood were elevated approximately 1 week following each effector cell infusion. Preceding these elevations, lym-phocyte numbers had decreased immediately after each infusion (Figure 6). The effector-cell infusions were generally associated with ele-vated CRP levels (Table 5). The highest CRP value, 345 µM (normal level <10 µM), was observed in patient P3A2 during the course of pneumonia. Patient 4 showed lymphocytosis and thrombocytopenia in line with B-CLL activity (Table 5). Liver, pancreas and kidney function tests did not highlight any effects in any patient.
1500
1000
500
00 5 10 15 20
Days
Fo
ld e
xpan
sio
nF
old
exp
ansi
on
Per
cen
t ce
lls
80
20
40
60
00 5 10 15 20
Days
00 5 10 15 20
Days
CD56+
CD56+CD3-
CD56+CD3+
CD56-CD3+
CD56+
CD56+CD3-
CD56+CD3+
CD56-CD3+
10,000
8000
6000
4000
2000
Figure 2. Ex vivo expansion of NK and NK-like T cells. (A) Fold expansion of total PBMCs during the culture period. (B) Dynamics of lymphocyte subpopulations during expansion. (C) Fold expansion of lymphocyte subpopulations during expansion.PBMC: Peripheral blood mononuclear cell.

www.futuremedicine.com 759future science group
Safety ana lysis of ex vivo-expanded NK & NK-like T cells in cancer patients ReseaRch aRticle
� Tumor load & patient outcome following cell infusionsAfter 2 months following classical DLI treat-ment, patient P2 presented a 2-week history of fatigue, coughing and dyspnea without fever. Physical examination, including tachypnea and pulmonary auscultation, revealed patho-logical breath sounds laterally on the right side. The AFP levels increased from less than 15 to 117 ng/ml (Figure 7). Other laboratory param-eters were within normal values apart from slight anemia (Hb: 103 g/l) and slightly ele-vated alanine aminotransferase/aspartate ami-notransferase (ALT/AST). The patient’s CT images showed a progression of two right-sided and two new left-sided subpleural nodular lung parenchyma changes. Although cytological
analyses of bronchoalveolar lavage were not conclusive indicators of malignancy, the clini-cal, laboratory and CT findings indicated metastases of HCC. The patient then received the first dose of the NK and NK-like T-cell infusion followed by two more infusions at 1-month intervals (Table 4). The cell therapy was monitored regularly and tolerated well. This patient’s performance status and respiratory function improved. Interestingly, AFP level gradually decreased after the first (89 ng/ml) and the second (42 ng/ml) cell infusions, and became normal (13 ng/ml) 11 weeks after the third cell infusion (Figure 7). After 6 weeks fol-lowing the third NK and NK-like T-cell infu-sion, the patient’s CT scan showed no further changes in the lung parenchyma, a finding that
Day 0
Day 19
Day 0
Day 19
Day 0
Day 19
SS
CS
SC
CD
56
CD
56C
D56
CD
56C
D56
CD
56
FS
FSC CD3
CD3 CD16
CD16
KIR2DL1
NKp30 NKp44 NKp46
KIR2DL2/3 KIR3DL1 NKG2A
NKG2D NKG2C
LILR-B1
DNAM-1
Figure 3. Phenotypic characterization of NK (CD3-CD56+) cells from one representative haplotype A donor (D5). (A) Phenotype of NK (CD3-CD56+) cells before (day 0) and after (day 19) ex vivo expansion. Expression of different (B) inhibitory and (C) activation receptors on NK cells are shown. Although most CD3-CD56+ NK cells had a CD56bright phenotype, they differed from resting CD56bright cells in that they expressed CD16 and killer-cell immunoglobulin-like receptors (KIRs). KIR expression remained rather stable throughout the expansion period. The expression levels of the inhibitory NK cell receptors CD94/NKG2A and LILR-B1 was higher on expanded NK cells. The expansion protocol also lead to a final product with increased expression levels of several activating receptors on the NK cells, including NKp30, NKp44, NKp46 and NKG2D.

Immunotherapy (2009) 1(5)760 future science group
ReseaRch aRticle Barkholt, Alici, Conrad et al.
suggested no tumor growth progression. The level of HCV RNA in his serum was stable during and after the cell infusions. However, the episodes of gastrointestinal hemorrhage due to remaining portal hypertension re-occurred 3.5 months after the last cell infusion. In spite of further investigations to pinpoint the source of bleeding (Meckel’s scintigraphy, push enter-oscopy, CT and MR), the patient died. Autopsy
showed no macroscopic or microscopic bleed-ing source, but there was blood in the jejunum and in a distal direction. His death was attrib-uted to varices resulting from portal hyperten-sion, yet no metastases of HCC were found. In all remaining patients, the malignancy pro-gressed (Table 6). Two patients (P3, P5) had fatal outcome from progressive disease within the 6-month follow-up time.
Day 0
Day 19
SS
SS
CD
56
FS
FS
CD
56
CD
56C
D56
CD
4C
D4
CD3
CD3 CD8
CD8 CD25
CD25Valpha24
Vβ1
1Vβ1
1
Valpha24
Figure 4. Phenotypic characterization of NK-like T (CD3+CD56+) and T (CD3+CD56-) cells from one representative haplotype A donor (D5) before (day 0) and after (day 19) ex vivo expansion. Although CD56+ cells showed the best expansion kinetics, there was no marked expansion of classical CD1-restricted NKT cells expressing the Va24, Vb11 T-cell receptor among the expanded CD3+CD56+ cell population.
Table 5. Blood chemistry and side effects after the NK/NK-like T (CD56+) cell infusions.
Infusion Patient Blood chemistry Symptoms and signs
CRP**
(max)WBC**
(×109/l)Fever(max,°C)
Allergy Infectious Other
First P1 Normal Normal No No No No
P2 12 Normal No No No No
P3 33 Normal No No No No
P1A2 240 16 39.8 NoStaphylococcus epidermis septicemia
No
P3A2* 88 Normal 38.6 No No Hemoptysis# day +10
P4* 45 77‡ 38.6 Papulae at injection site No No
P5* 20 Normal 38.6 Urticaria day +7 No No
Second P1 Normal Normal No No No No
P2 28 Normal No No No Melena¶ day +4, Hb 72
P3 28 Normal No No No No
P3A2* 345 18 38.8 No Pneumonia day +11§ Coughing#
P4* 105 155‡ No Papulae at injection site No No
P5* 25 Normal No No No Hemoptysis# day +36
Third P1 Normal Normal No No No No
P2 19 Normal No No No Melena¶ day +37, Hb 88
P3 58 Normal No Sicca eyes, mouth No No
P3A2* 125 18 No No No Hemoptysis# day +10
P4* 73 155‡ 38.8 Papulae at injection site No Nausea
P5* 213 Normal No NoUpper respiratory tract infection§
Coughing#, negative cultures
*Patient received subcutaneous IL-2 injections; ‡Lymphocytosis of CLL; §Negative blood and nasopharynx cultures; ¶Esophageal varices observed by gastroscopy; #Known lung metastases; **Normal values <10 µM (CRP) and 9–12 × 109/l (WBC).CRP: C-reactive protein; CLL: Chronic lymphoid leukemia; Hb: Hemoglobin; WBC: White blood cell count.

www.futuremedicine.com 761future science group
Safety ana lysis of ex vivo-expanded NK & NK-like T cells in cancer patients ReseaRch aRticle
DiscussionIn this Phase I clinical trial, we explored the safety and feasibility of administering ex vivo expanded NK and NK-like T-effector cells as DLI to five cancer patients after SCT. Cell infusions, with or without s.c. IL-2 injections, seemed to be safe as no aGvHD was observed. One patient suffered from to the procedure associated septicemia. At present, our labora-tory facilities allow the NK and NK-like T cell expansion using an automated and closed system to avoid any contaminations.
Currently, treatment options using pure NK cells or NK-enriched effector cell preparations are being investigated in Phase I/II clinical trials using purified/resting [20,21], short-term [22–24] or long-term [25] activated NK cells. Most of these studies report NK cell infusions to be well tol-erated and partially effective; especially, in the haploidentical setting [26] and as DLI following SCT against various human cancers. One obsta-cle in clinical studies with these cells originates from their low number in PBMCs and in various ex vivo-expanded effector cell preparations such
as cytotoxic T lymphocytes, LAK and CIK cells. Obtaining a large number of NK and NK-like T cells may be instrumental in controlling cer-tain tumors and GvHD. This would add to suc-cess gained in tailoring DLI regimens using a stepwise escalating-dose regimens demanding increasing cell numbers [27,28].
Standard protocols for the enrichment of NK cells from leukapheresis products under GMP conditions exist [13]. Enriched cells can then be infused directly without IL-2 activation [21] or after overnight culture with IL-2 [24]. In addi-tion to this, some of the protocols developed for ex vivo expansion of NK cells yield NK cell-enriched cellular populations under GMP conditions [6,29]. We have previously shown that OKT3 stimulation during the first 5 days is cru-cial for our culture system. Along with IL-2 sup-plementation, OKT3 stimulation is indispensa-ble for the expansion of NK cells under these culture conditions, yet the exact role of it is not investigated in detail. It is evident that OKT3 stimulates CD3+ cells in the culture, thereby helping them to expand and support CD56+ cell growth by either contact or secretion of soluble factors. We have observed that upon withdrawal of OKT3 from the culture at day 5, the prolifera-tion of CD3+CD56- T cells declines and CD56+ cells take over the culture. Yet, the stimulation of T cells at the beginning of the culture seems to be crucial for the later sustained growth of NK and NK-like T cells. It is also possible that OKT3 bound to the surface of CD3+cells is rec-ognized by the Fc receptor CD16 on NK cells, thereby helping both the elimination of T cells from the culture as well as stimulation of CD16+ NK cells. In the present study, no purification step preceded the expansion process, and the expanded effector cell population was admin-istered to cancer patients without depletion of T cells. Since clinical experience gained in recent years by adoptive T-cell therapy suggests that a maximum tolerated cell dose is one critical
Table 6. Tumor and patient status 3 and 6 months after the last NK/NK-like T (CD56+) cell Infusion.
Patient Tumor status* Patient outcome 6 months after the last infusion3 months after the last infusion 6 months after the last infusion
P1 P (lung, liver met) P (lung met), SD (liver met) Alive
P2 SD (lung met) SD (lung met) Dead‡
P3 P (pleura, LN, lung, bone met), SD (liver met) NA Dead
P4 P (LN met), lymphocytosis P (LN met), lymphocytosis Alive
P5 P (pleura, LN, lung met) NA Dead*RECIST: Response Evaluation Criteria in Solid Tumor. ‡Fatal outcome as a result of intestinal bleeding.LN: Lymph node; met: Metastases; NA: Not applicable; P: Progression; SD: Stable disease.
80
60
40
20
010:1 3:1 1:1 1:3
Effector:target
Day 0Day 10Day 15Day 19
K-5
62 ly
sis
(%)
Figure 5. Percent specific lysis of K562 cell line by ex vivo-expanded cells at different time points of culture compared with day-0 cells. A total of five independent samples from donors were analyzed. K562 cells were used as targets. Shown is a median specific lysis with interquartile range (0.25).

Immunotherapy (2009) 1(5)762 future science group
ReseaRch aRticle Barkholt, Alici, Conrad et al.
issue of GvT effect [30], optimizing protocols for ex vivo NK and NK-like T-cell expansion such as the protocol used in this study may be c linically important.
Interestingly, although a high number of T cells were infused to patients, no severe or immediate side effects were observed. Sicca syndrome (P3) was temporary and not consid-ered to be in line with chronic GvHD since it was not reported in connection with the later
effector-cell infusions using in vivo stimulating IL-2 injections. Gastrointestinal bleeding (P2) was considered not to be associated with the effector-cell infusions but already existing por-tal hypertension. The HLA-matched setting in the present protocol is to avoid the T-cell-caused GvHD. No clinically diagnosed GvHD could also partly be attributed to the impairment of T-cell alloreactivity following cell culture. In line with other researchers [31–35], we have previously shown that T cells cultured more than 7 days under the present conditions lose their alloreac-tive potentials [36]. The mechanisms underlying this impairment are unknown. Deletion of allo-reactive cells by activation-induced cell death, involvement of split anergy, loss of alloreactive precursors during expansion, and loss of naive cells or induction of suppressive cells may have influenced the results observed [34,37,38]. Owing to their reduced alloreactivity, T cells remaining in the mixed culture might have functioned as accessory cells rather than effector cells possibly providing cytokines and/or growth factors to other expanding cells.
The genotyping of KIRs in infused patients and their representative donors did not show any mismatch in KIR locus/ligand pairs to sup-port allogeneic antitumor activity based on the ‘missing-self ’ theory. An alternative explanation might be based on the elevated expression level
Su
bse
ts in
per
iph
eral
blo
od
(%
)
40
30
20
10
0
Infusion 1 Infusion 2 Infusion 3CD3+CD56+
CD3+CD56-
CD3-CD56+
1 h
befo
re in
f 1
1 h
befo
re in
f 3
1 h
afte
r in
f 3
1 w
eek
afte
r in
f 3
1mon
th a
fter
inf 3
2 m
onth
s af
ter
inf 3
3 m
onth
s af
ter
inf 3
1 h
befo
re in
f 2
1 h
afte
r in
f 2
1 h
afte
r in
f 1
1 w
eek
afte
r in
f 1
1 w
eek
afte
r in
f 2
Figure 6. Lymphocyte subset ana lysis of total peripheral blood leukocytes from five patients infused with NK and NK-like T cells (CD56+). Results are presented as median with interquartile range (0.25). Inf: Infusion.
α-F
P le
vels
(n
g/m
l)
Time (months after SCT)0
0
20
40
60
80
100
120
12 18 20
DLI1 DLI2
lnf3
lnf2
lnf1
Figure 7. a-FP levels in patient with hepatocellular cancer (P2) at different time points after infusion of expanded NK and NK-like T cell. a-FP: a-fetoprotein; DLI: Classical donor lymphocyte infusion; Inf: Expanded NK and NK-like T-cell infusion; SCT: Stem cell transplantation.

www.futuremedicine.com 763future science group
Safety ana lysis of ex vivo-expanded NK & NK-like T cells in cancer patients ReseaRch aRticle
Executive summary
� Expansion of donor-derived NK and NK-like T cells using a feeder-free GMP-compatible expansion strategy is feasible and provides high number of cells for immunotherapy approaches.
� Infusion of such ex vivo-expanded NK and NK-like T cells to cancer patients with or without IL-2 is safe with a possible antitumor activity. � Further clinical studies to investigate the efficiency of this approach of cancer immunotherapy are warranted.
of activating NK cell receptors. Phenotyping of the final product before infusion demonstrated increased expression levels of several activat-ing receptors (Figures 3 and 4), which may take part in shifting the signalling balance towards activation and target cell cytolysis.
After concluding that the expanded NK enriched cells did not cause significant side effects, we infused them to the remaining patients with subcutaneous IL-2 injection for 3 days. The aim was to determine the necessity of administering external IL-2 to patients together with expanded cells, having in mind future trials to further scru-tinize the efficacy of this cell preparation. Mild, reversible symptoms attributed to IL-2 admin-istration were observed. Even with the escalat-ing doses up to 3 × 107 CD56+ cells/kg and IL-2 administration, no signs of classical acute GvHD were observed. Hemoptysis is a common sign of vascularized lung metastases in RCC and thus, locus minoris for associated infections. In periph-eral blood, there was no significant difference in NK, NK-like T, and T cell counts between the two groups.
With the present insights into clinical effects of NK and NK-like T cells and the development of ex vivo expansion protocols under GMP-conditions for immunotherapy, possibilities emerge for the design of new cell-based immu-notherapy products against human cancer [39]. We have shown that infusions of ex vivo expanded donor-derived NK and NK-like T cells are safe and do not cause aGvHD or other severe side effects either with or without subcutaneous IL-2
injections. Although tumor response was not a primary goal of this study, the decrease of AFP and autopsy results in the patient P2 with HCC indicated a possible antitumor effect. Thus, use of NK and NK-like T cells for induction of GvT effects while avoiding GvHD appears to be an attractive approach for further development of cancer immunotherapy.
AcknowledgementsWe thank staff at the Center for Allogeneic Stem Cell Transplantation (CAST) for conscientious blood sample col-lection and excellent patient care. Also, Karl-Johan Malmberg for his assistance during the design of the multicolor flow cytometry panel, Marie Schaffer for KIR typing.
Ethical conduct of research The authors state that they have obtained appropriate insti-tutional review board approval or have followed the princi-ples outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investi gations involving human subjects, informed consent has been obtained from the participants involved.
Financial & competing interests disclosureThis work was supported by grants from the Swedish Cancer Society, the Swedish Research Council, the Swedish Children’s Cancer Foundation, and the EU grant Clinigene LSHB-CT-2006–018933.s. The authors have no other rel-evant affiliations or financial involvement with any organi-zation or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed. No writing assistance was utilized in the production of this manuscript.
Bibliography1 Schmidt-Wolf IG, Lefterova P, Mehta BA
et al.: Phenotypic characterization and identification of effector cells involved in tumor cell recognition of cytokine-induced killer cells. Exp. Hematol. 21, 1673–1679 (1993).
2 Lu PH, Negrin RS: A novel population of expanded human CD3+CD56+ cells derived from T cells with potent in vivo antitumor activity in mice with severe combined immunodeficiency. J. Immunol. 153, 1687–1696 (1994).
3 Scheffold C, Brandt K, Johnston V et al.: Potential of autologous immunologic effector
cells for bone marrow purging in patients with chronic myeloid leukemia. Bone Marrow Transplant 15, 33–39 (1995).
4 Grimm EA, Mazumder A, Zhang HZ, Rosenberg SA: Lymphokine-activated killer cell phenomenon. Lysis of natural killer-resistant fresh solid tumor cells by interleukin 2-activated autologous human peripheral blood lymphocytes. J. Exp. Med. 155, 1823–1841 (1982).
5 Rosenberg S: Lymphokine-activated killer cells: a new approach to immunotherapy of cancer. J. Natl Cancer Inst. 75, 595–603 (1985).
6 Carlens S, Gilljam M, Chambers BJ et al.: A new method for in vitro expansion of cytotoxic human CD3-CD56+ natural killer cells. Hum. Immunol. 62, 1092–1098 (2001).
7 Guven H, Gilljam M, Chambers BJ et al.: Expansion of natural killer (NK) and natural killer-like T (NKT)-cell populations derived from patients with B-chronic lymphocytic leukemia (B-CLL): a potential source for cellular immunotherapy. Leukemia 17, 1973–1980 (2003).
8 Alici E, Sutlu T, Bjorkstrand B et al.: Autologous antitumor activity by NK cells expanded from myeloma patients using GMP-compliant components. Blood 111, 3155–3162 (2008).

Immunotherapy (2009) 1(5)764 future science group
ReseaRch aRticle Barkholt, Alici, Conrad et al.
9 Guimaraes F, Guven H, Donati D et al.: Evaluation of ex vivo expanded human NK cells on antileukemia activity in SCID-beige mice. Leukemia 20, 833–839 (2006).
10 Bordignon C, Carlo-Stella C, Colombo MP et al.: Cell therapy: achievements and perspectives. Haematologica 84, 1110–1149 (1999).
11 Kammula US,Marincola FM: Cancer immunotherapy: is there real progress at last? BioDrugs 11, 249–260 (1999).
12 Ramsdell FJ, Golub SH: Generation of lymphokine-activated killer cell activity from human thymocytes. J. Immunol. 139, 1446–1453 (1987).
13 Klingemann HG: Natural killer cell-based immunotherapeutic strategies. Cytotherapy 7, 16–22 (2005).
14 Chan JK, Hamilton CA, Cheung MK et al.: Enhanced killing of primary ovarian cancer by retargeting autologous cytokine-induced killer cells with bispecific antibodies: a preclinical study. Clin. Cancer Res. 12, 1859–1867 (2006).
15 Soderdahl G, Barkholt L, Hentschke P et al.: Liver transplantation followed by adjuvant nonmyeloablative hemopoietic stem cell transplantation for advanced primary liver cancer in humans. Transplantation 75, 1061–1066 (2003).
16 Ringden O, Lonnqvist B, Hagglund H et al.: Transplantation with peripheral blood stem cells from unrelated donors without serious graft-versus-host disease. Bone Marrow Transplant 16, 856–857 (1995).
17 Mattsson J, Uzunel M, Remberger M et al.: Minimal residual disease is common after allogeneic stem cell transplantation in patients with B cell chronic lymphocytic leukemia and may be controlled by graft-versus-host disease. Leukemia 14, 247–254 (2000).
18 Glucksberg H, Storb R, Fefer A et al.: Clinical manifestations of graft-versus-host disease in human recipients of marrow from HL-A-matched sibling donors. Transplantation 18, 295–304 (1974).
19 Godeau B, Chevret S, Varet B et al.: Intravenous immunoglobulin or high-dose methylprednisolone, with or without oral prednisone, for adults with untreated severe autoimmune thrombocytopenic purpura: a randomised, multicentre trial. Lancet 359, 23–29 (2002).
20 Frohn C, Doehn C, Durek C et al.: Feasibility of the adoptive transfusion of allogenic human leukocyte antigen-matched natural killer cells in patients with renal cell carcinoma. J. Immunother. (1997) 23, 499–504 (2000).
21 Passweg JR, Tichelli A, Meyer-Monard S et al.: Purified donor NK-lymphocyte infusion to consolidate engraftment after haploidentical stem cell transplantation. Leukemia 18, 1835–1838 (2004).
22 Ishikawa E, Tsuboi K, Saijo K et al.: Autologous natural killer cell therapy for human recurrent malignant glioma. Anticancer Res. 24, 1861–1871 (2004).
23 Krause SW, Gastpar R, Andreesen R et al.: Treatment of colon and lung cancer patients with ex vivo heat shock protein 70-peptide-activated, autologous natural killer cells: a clinical Phase I trial. Clin. Cancer Res. 10, 3699–3707 (2004).
24 Miller JS, Soignier Y, Panoskaltsis-Mortari A et al.: Successful adoptive transfer and in vivo expansion of human haploidentical NK cells in patients with cancer. Blood 105, 3051–3057 (2005).
25 Koehl U, Esser R, Zimmermann S et al.: Ex vivo expansion of highly purified NK cells for immunotherapy after haploidentical stem cell transplantation in children. Klin. Padiatr. 217, 345–350 (2005).
26 Ruggeri L, Mancusi A, Capanni M, Martelli MF,Velardi A: Exploitation of alloreactive NK cells in adoptive immunotherapy of cancer. Curr. Opin. Immunol. 17, 211–217 (2005).
27 Guglielmi C, Arcese W, Dazzi F et al.: Donor lymphocyte infusion for relapsed chronic myelogenous leukemia: prognostic relevance of the initial cell dose. Blood 100, 397–405 (2002).
28 Mackinnon S, Papadopoulos EB, Carabasi MH et al.: Adoptive immunotherapy evaluating escalating doses of donor leukocytes for relapse of chronic myeloid leukemia after bone marrow transplantation: separation of graft-versus-leukemia responses from graft-versus-host disease. Blood 86, 1261–1268 (1995).
29 Klingemann HG,Martinson J: Ex vivo expansion of natural killer cells for clinical applications. Cytotherapy 6, 15–22 (2004).
30 Sprangers B, Van Wijmeersch B, Fevery S, Waer M,Billiau AD: Experimental and clinical approaches for optimization of the graft-versus-leukemia effect. Nat. Clin. Pract. Oncol. 4, 404–414 (2007).
31 Prevost-Blondel A, Zimmermann C, Stemmer C et al.: Tumor-infiltrating lymphocytes exhibiting high ex vivo cytolytic activity fail to prevent murine melanoma tumor growth in vivo. J. Immunol. 161, 2187–2194 (1998).
32 Wrzesinski C,Restifo NP: Less is more: lymphodepletion followed by hematopoietic stem cell transplant augments adoptive T-cell-based anti-tumor immunotherapy. Curr. Opin. Immunol. 17, 195–201 (2005).
33 Speiser DE,Romero P: Toward improved immunocompetence of adoptively transferred CD8+ T cells. J. Clin. Invest. 115, 1467–1469 (2005).
34 Gattinoni L, Klebanoff CA, Palmer DC et al.: Acquisition of full effector function in vitro paradoxically impairs the in vivo antitumor efficacy of adoptively transferred CD8+ T cells. J. Clin. Invest. 115, 1616–1626 (2005).
35 Matter M, Pavelic V, Pinschewer DD et al.: Decreased tumor surveillance after adoptive T-cell therapy. Cancer Res. 67, 7467–7476 (2007).
36 Carlens S, Liu D, Ringden O et al.: Cytolytic T cell reactivity to Epstein-Barr virus is lost during in vitro T cell expansion. J. Hematother. Stem Cell Res. 11, 669–674 (2002).
37 Wolf H, Muller Y, Salmen S, Wilmanns W, Jung G: Induction of anergy in resting human T lymphocytes by immobilized anti-CD3 antibodies. Eur. J. Immunol. 24, 1410–1417 (1994).
38 Mesel-Lemoine M, Cherai M, Le Gouvello S et al.: Initial depletion of regulatory T cells: the missing solution to preserve the immune functions of T lymphocytes designed for cell therapy. Blood 107, 381–388 (2006).
39 Ljunggren HG, Malmberg KJ: Prospects for the use of NK cells in immunotherapy of human cancer. Nat. Rev. Immunol. 7, 329–339 (2007).





























