Embed Size (px)
Citation preview

TATA INSTITUTE OF SOCIAL SCIENCE (Deemed University)
Post Graduate Diploma in WATER, SANITATION & HYGIENE
(WASH)
Biswajit Maity
ROLE OF RURAL SANITARY MART (RSM) IN PROVIDING
SANITATION
A Study of Ramakrishna Mission Lokasiksha Parishad’s
Experience
MENTOR:- PROF. RAMESH SAKTHIVEL, PhD
DECLARATION OF AUTHORSHIP
i
CERTIFICATE
ii
ACKNOWLEDGEMENT
At the outset I would like to express my gratitude to Ramakrishna Mission Lokasiksha
Parishad for entrusting me to conduct this study.
I would like to place on record my heartfelt thanks to Swami Pranananda – Joint
Director, RKMLP, and Mr. Chandi Charan Dey for their extensive support which
advanced me with basic understanding of the “Supply Chain Management” of RKMLP in
Sanitation sector. The study would not be possible without Mr. Dey’s guidance, planning
and subsequent field arrangement in four districts, viz. East Midnapore, West
Midnapore, Howrah and South 24 PGS.
I am also thankful to the Mr. Ajay Pal A.D.M (Development) and Swastha Karmadhakya
of East Midnapore district for fruitful discussion regarding present status of Sanitation
Movement (Specially NBA)
The District Officer, Mr. Swarup Ranjan Bera-Sanitation Cell, Purba Midnapore Zilla
Parishadhas shared valuable inputs on various aspects related to the study. I would like
to note my thanks to him also.
During field visit, respective RSM’s managers, District Coordinators of concerned district
& Divisional Co-ordinators have accompanied me and helped me to understand the
prevailing supply chain mechanism in the State at ground level. I have visited eight
villages with them covering 160 households. More than that, I also interacted with few
“Village Youth Clubs” and satellite RSMs,discussed with the manager-RSM and other
workers associated with the programme, met Gram Pradhans, Household members,
Teachers & Students in different villages. They have gladly replied all the queries made
in connection with the study and spared their time spontaneously for participating in
the interaction.
I appreciate their co-operative attitude and take the opportunity to thank them.
I would like to thank Dr. S. Peppin (Ex-Dean, TISS), Dr. Reshmi Peppin (Ex-Coordinator,
WASH) and Prof. Bipin Das for their overwhelming support from the beginning of the
work.
Lastly, I would like to thank Dr. Ramesh Sakthivel –(Professor, TISS) for his continuous
support and direction as a mentor to complete the study within stipulated time period.
iii
ACRONYMS
ADO (P) Additional Development Officer (Planning)
BCC Behavioural Change Communication
CBO Community Based Organisation
CRSP Central Rural Sanitation Programme
DRDA District Rural Development Authority
FGD Focused Group Discussion
GP Gram Panchayat
IAY Indira Awas Yojna
ICDP Integrated Child Development Programme
IEC Information, Education and Communication
IPC Inter-personal Communication
HH Household
HHL Household level/latrine
HP Himachal Pradesh
M&E Monitoring & Evalution
MDG Millennium Development Goal
MGNREGA Mahatma Gandhi National Rural Employment GuranteeAct
NBA Nirmal Bharat Abhiyan
NGO Non Government Organisation
NGP Nirmal Gram Puraskar
OD Open Defecation
PC Production Centre
PPP Purchase Power Parity
PRI Panchayati Raj Institute
R & D Research and Development
RKMLP Ramakrishna Mission Lokasiksha Parishad
RSM Rural Sanitary Mart
SCM Supply Chain Management
SDC Swiss Agency for Development and Cooperation
SHG Self Help Group
SIPRD State Institute of Panchayats and Rural Development
SLWM Solid Liquid Waste Management
SME Small and Medium Enterprises
TSC Total Sanitation Campaign
UN United Nation
UNDP United Nations Development Programme
WQMS Water Quality Monitoring System
CKNOWLEDGEMENT
iv
CONTENTS
1. INTRODUCTION 2
2. METHODOLOGY
2.1 Desk Research 4
2.2 Preparatory Study and Discussion 4
2.3 Visits to District’s RSMs and Respective Villages 5
2.4 Tools used for collection of data/information 5
2.5 Household Questionnaire: Latrine Knowledge,
Attitudes and Practices 9
3. OBJECTIVE 11
4. LITERATURE REVIEW
4.1 Study Supply-Chain (RSM/PC) 12
4.2 Global scenario of Supply-Chain mechanism in Sanitation 12
4.3 Demand Driven Approach for Sustainability 13
4.4 Sanitation as Business 14
4.5 Supply Chain Concept and Its Relevance to TSC/NBA 14
4.6 TSC/NBA Guidelines in Supply Chain 16
4.7 Sustainability of RSMs/PCs 17
4.8. Reluctance among Government functionaries/ Stake holders 19
4.9 Success story of RSM lead by RKMLP, West Bengal 21
4.10 Need of the study 22
5. RESULT & ANALYSIS
5.1 Activity Analysis 23
5.2 Factors for Sustainability 25
5.3 Operational & Financial viability of RSM/PC 30
5.4 Factors affecting Demand for Toilets: RSMs perspective 31
5.5 Seasonal Demand Forecasting 33
5.6 Analysis on Village level Latrine coverage 34
5.7 Perception about RSM: From villager’s point of view 36
5.8 Incidence of Diarrhoea 37
5.9 Latrine Coverage 37
5.10 Motivational Instrument 38
5.11 Description of Existing Latrine 39
5.12 Categorisation: APL & BPL 41
5.13 Institutional Credibility 42
5.14 Market Analysis 42
5.15 Source of Information 45
5.16 Other Reasons for Success 46
5.17 Scope for Improvement: Analytical view 46
v
6. RECOMMENDATION & CONCLUSION 48
7. REFERENCES 50
8. ANNEXURE I 52
9. ANNEXURE II 56
10. ANNEXURE III 57
11. ANNEXURE IV 61
12. ANNEXURE V 63
List of Figures
1. GP members: Lakshya village, Haldia Block, P. Midnapure 5
2. Marked surveyed Districts 6
3. Action area of RSMs in P. Midnapure 6
4. Action area of RSMs in Pa. Midnapure 6
5. Action area of RSMs in Howrah 7
6. Action area of RSMs in S-24 PGS 7
7. Data collection at household level 7
8. RKMLP accredited Tamralipta Guchha Samity 8
9. FGD in Amreswar village, S-24 PGS 8
10. Integrated Technical Component Sanitation 13
11. Ideal RSM, UP, India 14
12. Faulty construction- Vent pipe on Leach pit, Howrah, W.B 18
13. Latrine using SSP Model in P. Midnapure 21
14. PC in Vivekananda Yuba Parishad (Cluster/RSM), W.B 21
15. SSP Model 25
16. SSP model in BPL family, Pa. Midnapure 26
17. Factors for better performance (RSM) 26
18. Soil & Water Testing Labs in RSM 27
19. Responses from RSM managers regarding Sustainability of RSM 27
20. Retail outlet of SHG made Food products in A.N.P.S 28
21. Toilet up-gradation under NBA & MGNREGA 29
22. Number of Latrine constructed by the RSMs (April – Oct, 2013) 30
23. Annual Turnover (2012-’13) 31
24. Responses from RSM Managers on factor affecting
such of RSM’s demand for toilets 32
25. Trend of Demand for Latrine 33
26. Comparison of W.B performance in view of National overall progress 35
vi
27. Cases of Diarrhoea from respondent HH 37
28. Latrine Coverage 37
29. Type of Latrine built in the study area (I) 39
30. Meeting of Village Youth Club with Mother Committee,
Lokojagaran RSM 40
31. Type of Latrine built in the study area (II) 40
32. Type of Latrine built in the study area (III) 40
33. Latrine constructed APL & BPL families 41
34. Reason for choosing local RSM 42
35. Priority given to various benefits of Latrine by Latrine-owners 44
36. Priority given to various benefits of Latrine by non Latrine-owners 45
37. Source of Sanitation advice 45
38. Knowledge about “Water Table Rising” 46
List of Diagrams
1. Basic Supply System 15
2. Action Plan for a RSM 15
3. Operational Structure of RKMLP 24
List of Tables
1. Demographics of surveyed village 9
2. Comparative List of TSC/NBA Guidelines 17
3. Snapshot of RSM Level questionnaire 23
4. Comparative study about the hardware components used in latrine 29
5. Snapshot of Village survey details 34
6. Snapshot of FGD results with villagers 36
7. List of motivational factors 38
8. Snapshot of Assessment for Toilet affordability 43
9. Household constructed under IAY 47
vii

EXECUTIVE SUMMERY
Lack of access to drinking water and
sanitation is perhaps the most passive
and pervasive human rights violation in
the country. Imagine about the day to
day life of approx. 19.5 million rural
people who don’t have access to safe
drinking water. And even we consider,
those (in rural areas) not having access
to water, having partial access to water
and people whose water sources are
contaminated, 77 million Indians come
on the platform, who are facing problem
with his/her water both in quantity or
quality. On sanitation, the situation is
more or less same with same story. Two
out of every three Indians defecates in
the open, more due to constraints than
behaviour. The health burden of
inadequate sanitation is so high that the
country spends more on health than on
direct sanitation provision. And 1.5
million children die of diarrhoea every
year.
This report presents an assessment of
structural and operational functionality
of five; Ramakrishna Mission
Lokasikasha Parishad (RKMLP)
accredited RSMs in two districts of West
Bengal, viz. Purba Midnapure and
Paschim Midnapure and three other
NGO/CBO run RSMs in other two
districts, viz. Howrah and South 24 PGS.
The objective of the study was to
understand perceptions, desires, and
practices regarding latrine use as a basis
for designing interventions to stimulate
demand. Village and household level
interviews and focus group discussions
were conducted in four districts. In total
eight villages and 160 households were
surveyed, including both latrine owners
and non-owners. In addition, eight focus
group discussions were conducted with
eight RSMs including their managing
committee members.
The results of the survey and focus
group discussions provide information
and insights relating to sequential
strategic intervention of RKMLP in
Water Quality Management and overall
sanitation (HHL, Community Level,
School & Anganwadi toilets) in a unique
way unlike other NGOs, which run
“Movement of Toilet Construction”
rather than focusing on Information
Education &Communication activities.
Among the survey population, 96% of
RKMLP led area and 80% of others led
area households own a latrine. The
techniques of interventions are equally
adopted by the other NGOs, with a
difference in objectives.
Latrine ownership was quite common in
RKMLP led areas (Two Midnapures) as
it became their basic need through
extensive and in depth behavioural
change programme, unlike other areas
where it is still based on subsidy
oriented motivational factors.
1

INTRODUCTION
1980-’90 is considered as
“International Water Supply and
Sanitation decade”, designated by
United Nation, which witnessed
enhanced attention towards both the
sectors, viz. Water supply and
Sanitation. An ambitious target of 100
per cent coverage for water, 80 per
cent for urban sanitation and 25
percent of rural sanitation was
decided by the Govt. of India1. But, on
ground, the country was able to
achieve only 9% in rural areas2.
In, 1986, Ministry of Rural
Development launched, first centrally
sponsored sanitation programme
titled Central Rural Sanitation
Programme (CRSP).The programme
was highly subsidized and supply
driven. That’s why it (CRSP – Central
Rural Sanitation Programme 1986-
99) failed to achieve the desired
objective of sustainability. The CRSP,
which was restructured in1999 under
the banner of the TSC strongly
advocated for a demand driven,
gender-sensitive community-led,
participatory approach which provide
scope for the private organisation,
other than govt. agencies. Synergized
action among government, people
and active NGOs was considered as
the key driver for success of this
campaign.
Total Sanitation Campaign (TSC) that
started in 1999, as a part of the sector
reform, mainly focus on demand
driven approach with increased
emphasis on awareness creation and
demand generation for sanitary
facilities unlike CRSP. In order to
meet the generated demand the
program also envisaged appropriate
delivery along with various technical
options and price range in the form of
Rural Sanitary Marts and Production
centres.
Apart from creating demand for
sanitation through Information,
Education, and Communication (IEC),
establishing an effective supply chain
to respond to the demand generated
at the community level is considered
as critical component of the
programme. Evidently, the “Demand
Responsive Approach” (DRA) will yield
results only when effective “Supply
Chains” (the totality of processes
spanning from supplier to end
customer, focused on material work
and information flow) are in place.
The clarity in terms of effective and
sustained supply chain system was
evolved gradually from TSC to NBA.
The major difference lies among the
guidelines issued from Government of
India time to time is ambiguity in
terms of functionality of RSMs in long
term.
Target was
fixed up
without detail
consideration
about the
infrastructural
set up to
facilitate Supply
Chain system of
sanitary
products and
facilities.
2
1 Park, 2000 2 Alok, 2010

It is deemed necessary to design
situation specific supply chain to cope
with emerging demand for sanitation at
the grassroots. The Supply Chain
Mechanism, thus established is
expected to ensure that the right
products, information and services
reach the target groups. The services
are expected to be in accordance with
the choices and affordability of the
target groups and delivered in the most
resource-effective manner without
sacrificing quality, services as well as
sustainability.
Therefore, a comparative study was
necessary to find out the controlling
factors, which determine the fate of the
Rural Sanitary Mart. Due to certain
constraints (time, mobility, cost etc),
the sampling size was not too big, which
helps to minimize sampling error. For
comparative study purpose, a
successful RSM operation was selected
and that was none other than
Ramakrishna Mission Lokasiksha
Parishad lead RSMs scattered mainly in
Purba Midnapure and Pachim
Midnapure. Individual NGO lead two
RSMs from Howrah and one RSM from
South 24 PGS, were also selected to
compare with RKMLP lead RSMs. Apart
from that, the study was also conducted
to figure out the driving forces for the
sustainability of RSMs along with
proposed recommendation to achieve
it, in absence.
3
METHODOLOGY
2.1 Desk Research Prior to visit to the state, the necessary
available documents (National and
International perspective) on Supply
Chain Management of Sanitation were
studied. Physical and Financial progress
reports of TSC programme, available in
the DDWS (Department of Drinking
Water Supply) web site, was also
considered. The Review Reports of TSC
programme for various districts of West
Bengal vs. other states were also
consulted to ascertain different critical
issues including supply chain
management related with
implementation of TSC programme in
the state. The TSC Review Report of
Purba Midnapure, Paschim Midnapure,
Howrah and South 24 PGS districts of
West Bengal helped in developing the
understanding of critical programme
issues.
To get an insight of the Rural Sanitary
Mart and Production Centre, I went
through important articles, research
papers or Govt. documents, which are
listed under Reference list. There are
few international papers on SCM
(Supply Chain Management), mostly
written by WSP and UNICEF. Except
that, forums of Solution Exchange and
India Sanitation Portals have provided
lots of information regarding various
aspects of RSM/PC, and the reason
behind its failure (or limited success) on
a sustainable basis.
2.2Preparatory Study and Discussion The Objective and Scope of the study was discussed with senior professors of TISS, viz. Prof. R. Sakthivel, Prof. S. Peepin, Prof. B. Das, Prof. Kunhaman and Prof. N. Dhar including the domain experts from various national and international bodies like, Mr. A. Ghodke-
WATSAN Consultant, Asia Development Bank, Mr. Y. Kabir-WASH Officer, UNICEF Mumbai, Mr. H. Raj-Consultant, World Bank and the broad purpose of the study was clarified before going to West Bengal. Except that, the other steps were,
At the office of the RKMLP the documents available in the form of policy guidelines/Government Orders etc on supply chain system of the state collected, studied and discussed with Mr. Chandi Charan Dey- WASH Coordinator.
Status of Supply Chain System in the state was reviewed with Swami Pranananda – Joint Director, RKMLP and state level officials, Mr. A. Pal (A.D.M). Tentative plan of visit to various district’s RSM was worked out with the help of Mr. Dey.
Focused discussions was also held in visited RSMs with grassroots level workers of Project Mangers, Block supervisors, Motivators, Representative of Cluster, PRI members, ASHA workers etc.
A briefing meeting was organised at the end of the field work in RKMLP’s office. The major findings of the study were discussed with the state level functionaries of RKMLP.
4
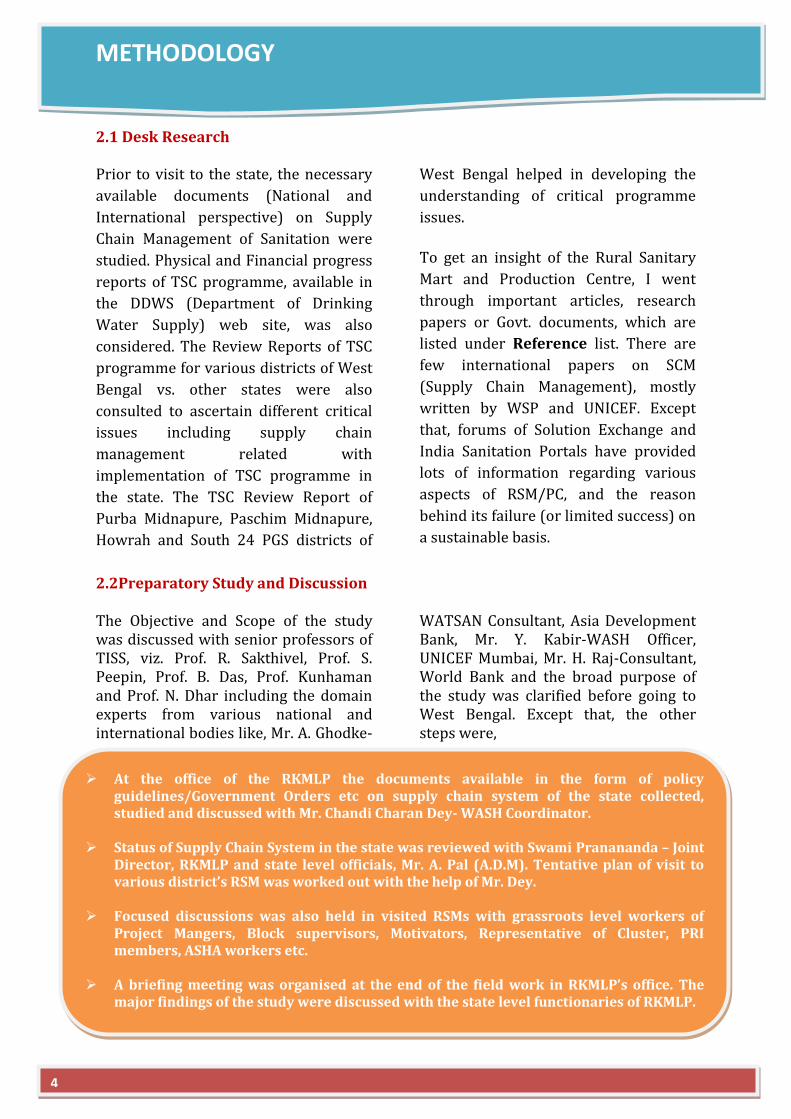
2.3 Visits to District’s RSMs and Respective Villages As part of field work, Purba Midnapore, Pachim Midnapore, Howrah and South 24-PGS districts were visited. Visited supply-chain units including RSMs which are accredited by RKMLP and those run independently. I also enquired about the received revolving fund from TSC programme to ascertain ground realities of present supply chain system. Visit was also arranged to observe sanitation arrangements in schools, Anganwadis, and specially household level, implemented through TSC and as well as other programmes. Fig 1:-GP members: Lakshya village, Haldia
Block, P. Midnapure
2.4 Tools used for collection of data/information
2.4.1 Survey Tools Questionnaires
Two questionnaires were developed for
the study: one to collect household-level
data and another to collect village-level
data along with concerned RSM/PC
details. Both the questionnaires were
circulated among concerned professors
and domain experts and several
comments and suggestions were
received and incorporated. Copies of the
questionnaires in English are included
in Annex I, II and III.
Field work for the survey occurred over
a fortnight period from 10th November
to 25th November, 2013. Questionnaire
interviews were conducted by me along
with Project Coordinators from RKMLP
or RSM manager.
Data from the completed questionnaire
forms was entered into a Microsoft
Access database by me after the
completion of the field work.
Focus Group Discussion
Focus group discussions were used to counter check, a number of topics touched on by the questionnaire. All the discussions were based on same guidelines for greater consistency. During each discussion, project coordinator was acted as facilitator and assisted me while taking note of the discussion. Discussions were also tape recorded and important points transcribed in English (Annex IV).
5
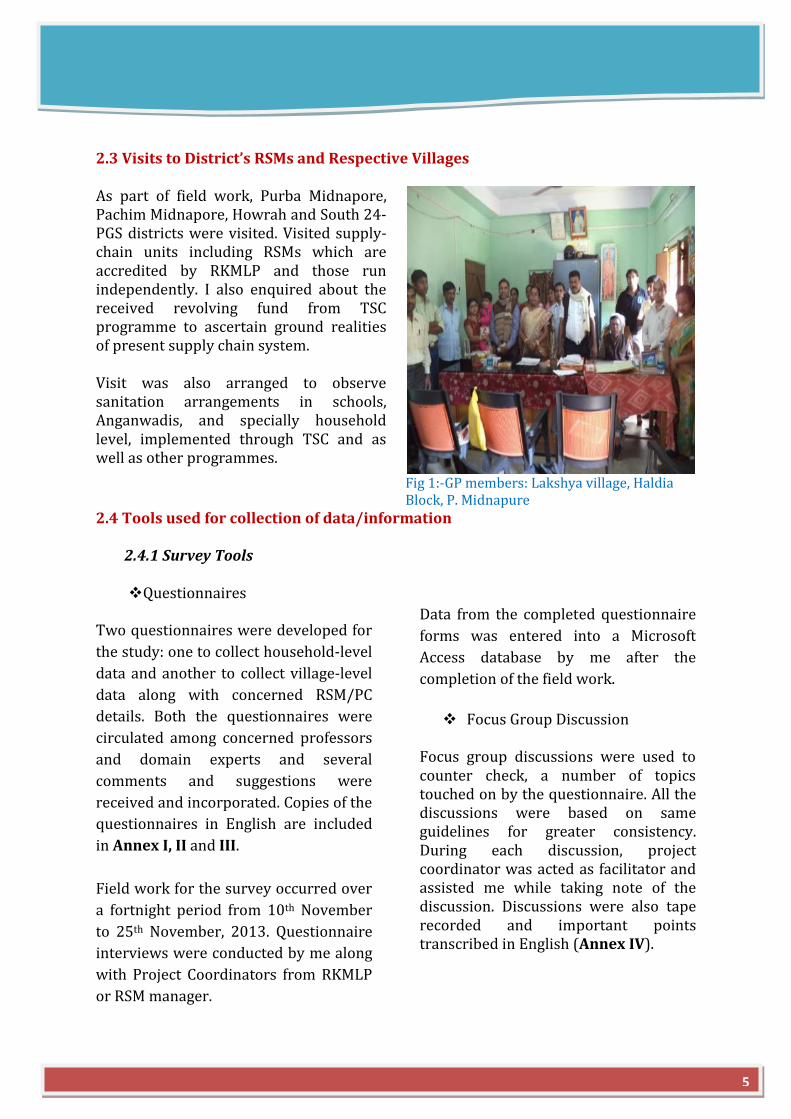
2.4.2 Sample Selection Selection of Study Area
Practical considerations of time and
budget, limited the survey to eight RSMs
and adjacent eight villages. Two districts
were selected in consultation with
RKMLP, where they already mobilized
the people through five cluster
organisations (Mother RSMs/PCs) and
achieved almost 100% HHL sanitation
coverage, except few schools and
anganwadis. More on that, on the basis
of advice and subsequent planning by
Mr. C. C. Dey, two more districts and
three more RSMs/PCs were included in
survey plan, which might be indirectly
influenced by RKMLP work process, but
don’t have any direct control under
RKMLP. The selected study locations are
indicated in Fig (2-6).
Fig. 2:- Marked surveyed Districts
Fig. 3:- Action area of RSMs in P. Midnapure Fig. 4:- Action area of RSMs in Pa. Midnapure
6
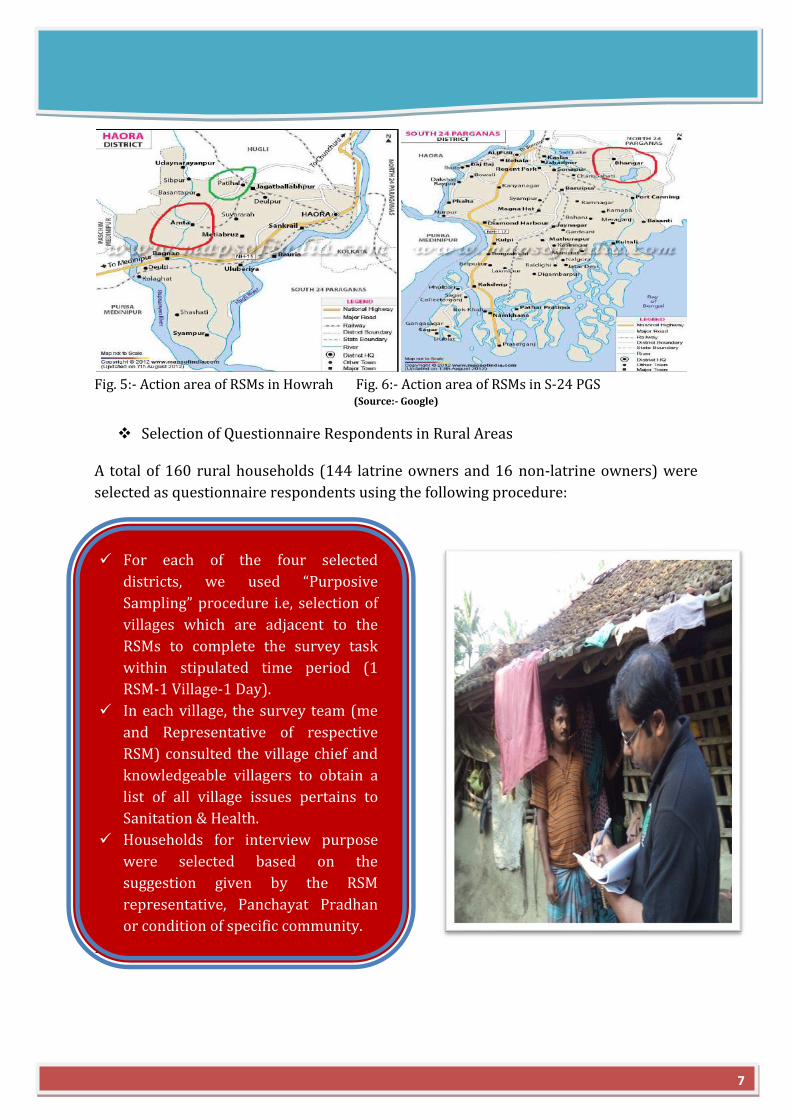
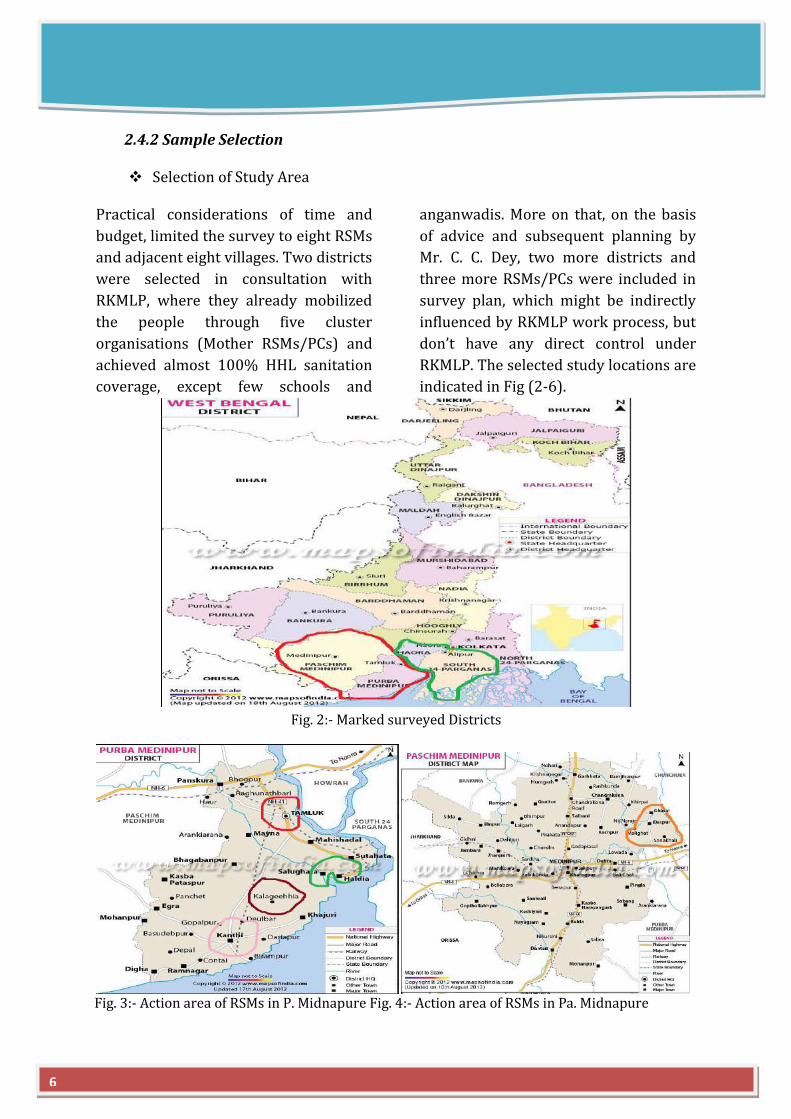
Fig. 5:- Action area of RSMs in Howrah Fig. 6:- Action area of RSMs in S-24 PGS
(Source:- Google)
Selection of Questionnaire Respondents in Rural Areas
A total of 160 rural households (144 latrine owners and 16 non-latrine owners) were
selected as questionnaire respondents using the following procedure:
Fig. 7:- Data collection on household level
For each of the four selected
districts, we used “Purposive
Sampling” procedure i.e, selection of
villages which are adjacent to the
RSMs to complete the survey task
within stipulated time period (1
RSM-1 Village-1 Day).
In each village, the survey team (me
and Representative of respective
RSM) consulted the village chief and
knowledgeable villagers to obtain a
list of all village issues pertains to
Sanitation & Health.
Households for interview purpose
were selected based on the
suggestion given by the RSM
representative, Panchayat Pradhan
or condition of specific community.
7
Selection of RSMs
Selection of Focus Group Participants
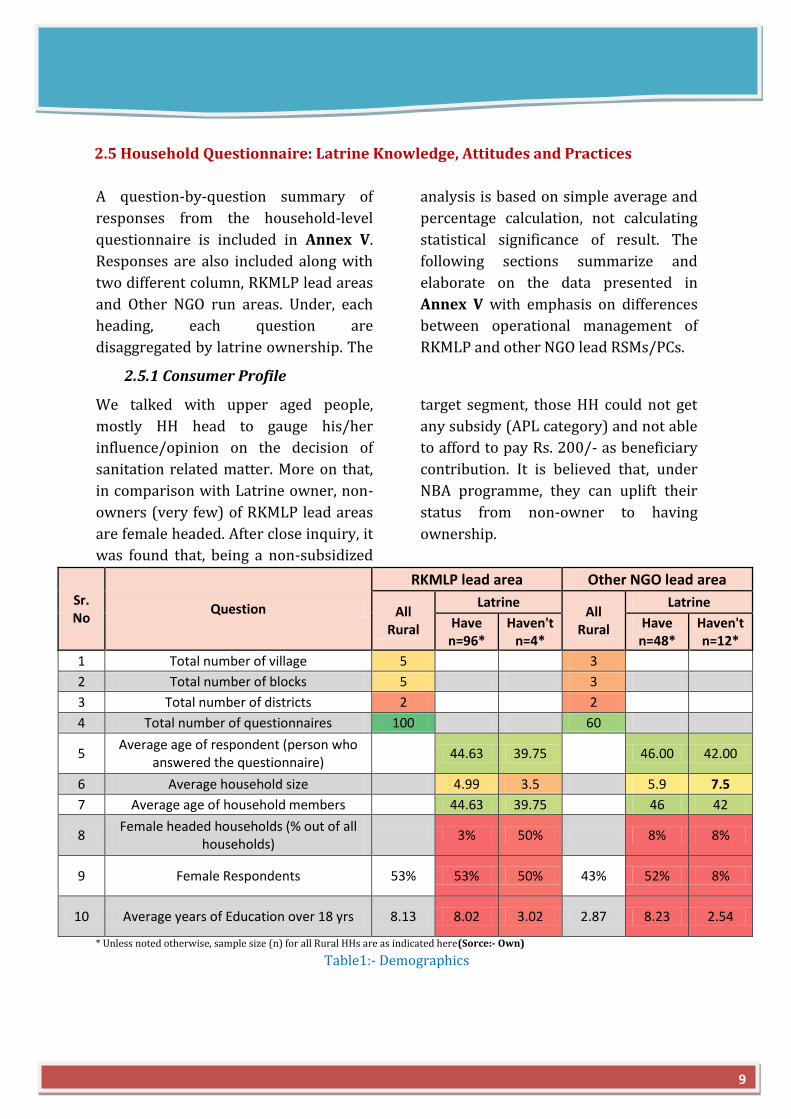
A total of 53 people participated in eight focus group discussions—one group in each
village area. Participants were selected according to the following procedure:
Fig. 9:- FGD in Amreswar village, S-24 PGS
As the objective of the study, was to
find out the reasons behind the
success of RKMLP accredited RSMs
and other RSMs, run by other
NGO/CBO or Zila Panchayat Udyog
(Chattopadhya, 2008), 5 RSMs were
selected from RKMLP accredited list
and 3 from others for a comparative
study.
The selection was once again based
on “Purposive Sampling” as per the
easiness of the work.
After questionnaires were completed in
each survey area, the Survey Team invited
six-seven of the questionnaire respondents
to participate in a focus group discussion
on the following day.
The invitees were selected based on the
Survey Team’s assessment of their specific
interest or knowledge and ability to
contribute to a group discussion.
The Survey Team sought a balance of
women and men, and latrine owners and
non-owners.
All invited participants took part in the
focus group discussions except for one
case where only four of the invitees
showed up due to a miscommunication
about the meeting place. A summary list of
the focus group participants is included in
Annex IV.
8
Fig. 8:-RKMLP accredited Tamralipta Guchha Samity (RSM)
2.5 Household Questionnaire: Latrine Knowledge, Attitudes and Practices
A question-by-question summary of
responses from the household-level
questionnaire is included in Annex V.
Responses are also included along with
two different column, RKMLP lead areas
and Other NGO run areas. Under, each
heading, each question are
disaggregated by latrine ownership. The
analysis is based on simple average and
percentage calculation, not calculating
statistical significance of result. The
following sections summarize and
elaborate on the data presented in
Annex V with emphasis on differences
between operational management of
RKMLP and other NGO lead RSMs/PCs.
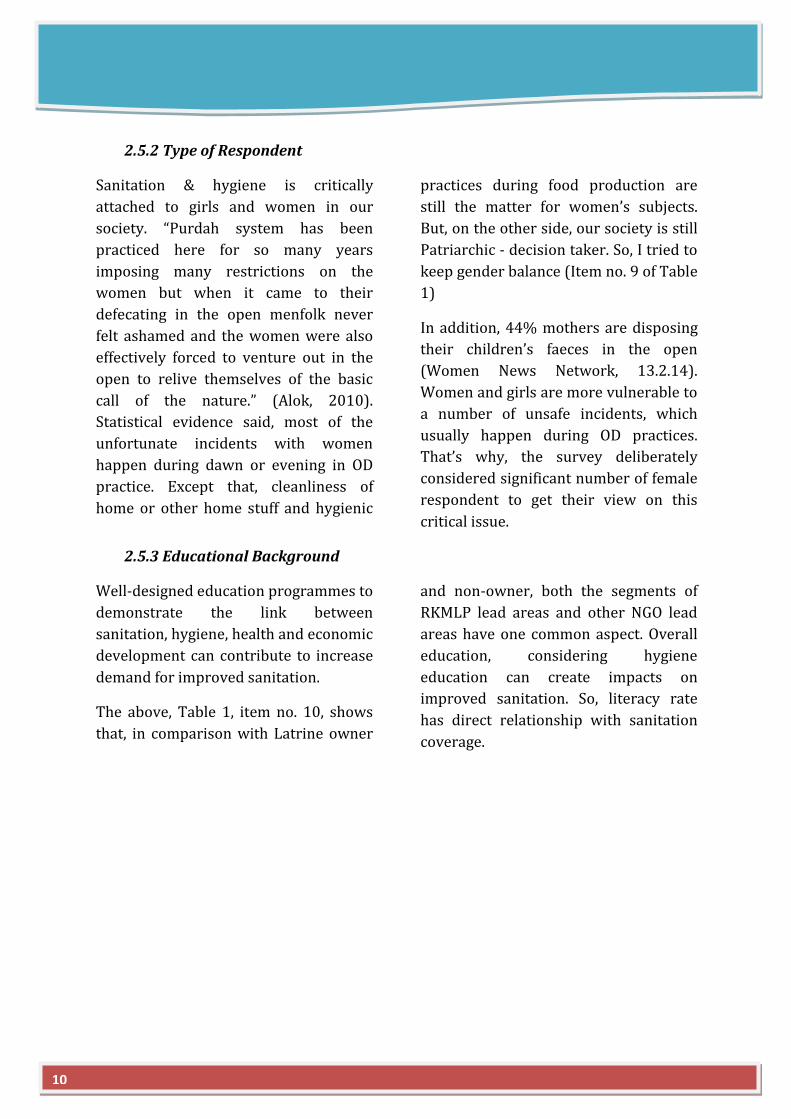
2.5.1 Consumer Profile
We talked with upper aged people,
mostly HH head to gauge his/her
influence/opinion on the decision of
sanitation related matter. More on that,
in comparison with Latrine owner, non-
owners (very few) of RKMLP lead areas
are female headed. After close inquiry, it
was found that, being a non-subsidized
target segment, those HH could not get
any subsidy (APL category) and not able
to afford to pay Rs. 200/- as beneficiary
contribution. It is believed that, under
NBA programme, they can uplift their
status from non-owner to having
ownership.
Sr. No
Question
RKMLP lead area Other NGO lead area
All Rural
Latrine All
Rural
Latrine
Have n=96*
Haven't n=4*
Have n=48*
Haven't n=12*
1 Total number of village 5 3
2 Total number of blocks 5 3
3 Total number of districts 2 2
4 Total number of questionnaires 100 60
5 Average age of respondent (person who
answered the questionnaire) 44.63 39.75 46.00 42.00
6 Average household size 4.99 3.5 5.9 7.5
7 Average age of household members 44.63 39.75 46 42
8 Female headed households (% out of all
households) 3% 50% 8% 8%
9 Female Respondents 53% 53% 50% 43% 52% 8%
10 Average years of Education over 18 yrs 8.13 8.02 3.02 2.87 8.23 2.54
* Unless noted otherwise, sample size (n) for all Rural HHs are as indicated here(Sorce:- Own)
Table1:- Demographics
9
2.5.2 Type of Respondent
Sanitation & hygiene is critically
attached to girls and women in our
society. “Purdah system has been
practiced here for so many years
imposing many restrictions on the
women but when it came to their
defecating in the open menfolk never
felt ashamed and the women were also
effectively forced to venture out in the
open to relive themselves of the basic
call of the nature.” (Alok, 2010).
Statistical evidence said, most of the
unfortunate incidents with women
happen during dawn or evening in OD
practice. Except that, cleanliness of
home or other home stuff and hygienic
practices during food production are
still the matter for women’s subjects.
But, on the other side, our society is still
Patriarchic - decision taker. So, I tried to
keep gender balance (Item no. 9 of Table
1)
In addition, 44% mothers are disposing
their children’s faeces in the open
(Women News Network, 13.2.14).
Women and girls are more vulnerable to
a number of unsafe incidents, which
usually happen during OD practices.
That’s why, the survey deliberately
considered significant number of female
respondent to get their view on this
critical issue.
2.5.3 Educational Background
Well-designed education programmes to
demonstrate the link between
sanitation, hygiene, health and economic
development can contribute to increase
demand for improved sanitation.
The above, Table 1, item no. 10, shows
that, in comparison with Latrine owner
and non-owner, both the segments of
RKMLP lead areas and other NGO lead
areas have one common aspect. Overall
education, considering hygiene
education can create impacts on
improved sanitation. So, literacy rate
has direct relationship with sanitation
coverage.
10
OBJECTIVES
The major objective of the study was to
assess the adequacy and effectiveness of
the RSM as a key propelling component
of the Total Sanitation Program (TSC)
and ongoing NBA programme with a
view to compare it’s structural and
functional differences in-between
RKMLP accredited RSM and others.
Keeping this major objective in mind the
specific objectives of the study were:
1) To study the RKMLP accredited RSM’s
structure through Mednipure Model
2) To find out the link in between
promotional campaign and community
achievement in terms of Sanitation
coverage
3) To study the strategies adopted by
the RKMLP to diversify the activities of
RSMs for sustainability
4) To figure out the relativity of “Zero
Subsidy1” concept with higher subsidy
demand in accordance with the intrinsic
and extrinsic motivation
1Zero Subsidy:- It is contextual to the Sanitation Movement lead by RKMLP in Midnapur district in West Bengal at early twenty. As
per RKMLP, INSTALLATION OF Sanitation facilities can be promoted without giving any kind of subsidy to people, if there are proper
Sanitation Education activities involving village level CBOs. Subsidy will come into discussion, whenever there will be a
differentiation between the financial need of two or more societal segments. As RKMLP believes that, there should be proper
planning for an integrated area with the objective of saturating all the families with household toilets.
11

LITERATURE REVIEW
“Water and Sanitation is one of the primary
drivers of Public health. I often refer to it as ‘Health 101’,
which means that once we can secure access to clean water and to adequate sanitation facilities for
all people, irrespective of the difference
in their living conditions, a huge battle against all kinds of
diseases will be won.”
-Dr. Lee Jong-wook, Director-General World Health Organisation (WHO, 2004b)
4.1 Study Supply-Chain (RSM/PC) Access to sanitation is essential for
human well-being, dignity and economic
development. Changing hygienic
behaviour of rural people, through
demand creation innovations such as
Community Led Total Sanitation will not
be sustained unless a number of key
supporting conditions are met. One of
these conditions is access to affordable
and appropriate sanitation hardware
and services.
Empirical study shows that, Market-based
sanitation solutions have the most
potential for economic of scale and
sustainability. But, due to non-
prioritization for a long time, poorly
developed rural sanitation market still
remains unorganised and outreach is
limited. Sanitary shops selling hardware
and masons building toilets exist in any
country, but the challenge is to reach to
the marginalised section mainly across
the socio-economic spectrum. Affluent
section, due to sensitivity or status
identification can walk to the shops. But,
actual problems lies with those,
demotivated, illiterate, poor people, for
which shops (RSM) need to walk upto
them. Special attention is very much
required to cater the different consumer
segments, most notably marginalised
section, households living in poverty,
ethnic minorities and low caste groups.
Because rural sanitation supply chains
and finance often need to be
strengthened, work should start in this
area before and then be conducted in
parallel to demand creation activities.
4.2 Global scenario of Supply-Chain mechanism in Sanitation Rural Sanitation Supply Chains and
Finance is also a part of the global
SNV/IRC Sustainable Sanitation and
Hygiene programme, which mainly focus
on improving the quality of life of rural
people in five Asian countries (Bhutan,
Cambodia, Laos, Nepal and Vietnam).The
programme consists of four integrated
technical components (see diagram in
next page)
12

These four strategies will work hand to
hand, empowering local capacities for a
rural sanitation service delivery with a
district-wide approach. Along with that,
integrated management system based on
departmental convergence is ultimate
demand on the grassroots level as well as
policy designing part.
Fig. 10:- Integrated Technical Component Sanitation
Source: SNV and IRC, March, 2012 (Source:- SNV-IRC Report, 2012)
4.3 Demand Driven Approach for Sustainability
As per SDC report, in 2000, around 1 billion
urban dwellers still lacked adequate
quantity and quality drinking and
improved sanitation. The figure is even
worst in rural areas. Yet practical examples
from all over the world increasingly
demonstrate that this gap can be mitigated
through demand creation by mass
mobilization. Thriving for the inclusive
sanitation converges without any cast,
creed, economic or regional discrimination
may lead to achieve Millennium
Development Goals (MDG). (SDC, 2004)
The report also talked about, cultural
taboos, which most of the time overshadow
sanitation demand, making it too complex
to deal. People are used to talking about
food, but not about excreta. And although
everybody likes to stay in a green clean
environment to a dirty one, no one is ready
to take initiative to keep it clean.
Sometimes, demand may also depend on
behavioural characteristics. For instance, in
our country, people prefer open defecation
because they do not want to pollute the
vicinity of the house; as they perceive a
latrine as a source of pollution, especially, if
it is close to the kitchen. But such attitudes
and perception may change, mostly due to
presence of active mobilizers and right
kind of offering in right place at right time.
Adopters of latrines in India – have their
own perception about what is “pure” and
what is “polluted” – which is strongly
influence by their neighbours. Similarly,
one reason why we wash ourselves every
morning is the pleasure we derive from
feeling “clean”, but to a great extent we are
also influenced by social factors. Nobody
wants to smell of sweat or dirt and give a
bad impression. Prestige and social
pressure are absolutely crucial motives for
sanitation and hygiene campaigns.
13

Once demand for latrines is generated, an
opportunity has arisen for the private
sector as well as for social entrepreneur
to design, make and deliver a solution
that fully satisfies this demand. If the
customer is poor, then the product must –
above all – be modestly priced. If the
customer is wealthier, then the product
may be of a higher quality and a better
design. There is never only one solution:
it is not true that “one size fits all”(SDC,
2004).
4.4 Sanitation as Business
According to Dyalchand, profitable supply
chains guarantee continuous supply. In
developed countries, the markets for
sanitation and hygiene are reaching
saturation, fulfilling their basic need.
Nevertheless, the sanitation and hygiene
sector sustains itself through constant
innovation and aggressive marketing.
Looking from marketing point of view,
sanitation business has emerged and
diversified luxury and more comfortness
like “jacuzzis” or “whirlpools” into the still
growing “wellness” markets. The soap
and cosmetics industry is also constantly
positioning new products into markets
that are already very competitive.
Fig. 11- Ideal RSM, UP, India
In comparison to that, the sanitation
coverage rate with minimum acceptable
degree is far-far away from saturation, so
the markets for sanitation and hygiene in
developing countries appear to be almost
endless. Once the “affordability” barriers
crossed, demand can grow more or less
continuously. However, empirical
evidences showed that, the real challenge
lies in maintenance of profitable and
performing supply chains. For example, in
south-east countries construction labours
(Usually, plumbers and masons) are
available in a good number. They are
mostly semi-skilled, having low status
and work mostly in the informal sector.
This means that they cannot create
markets on their own, but if there is a
demand, they can deliver goods and
services at very low costs. (Dyalchand,
2001)
4.5 Supply Chain Concept and Its Relevance to TSC/NBA
In order to understand how the supply
chain system pertaining to rural
sanitation functions it is necessary to
know what a supply chain is. In simple
terms a supply chain is a network of
facilities that procure raw materials,
14
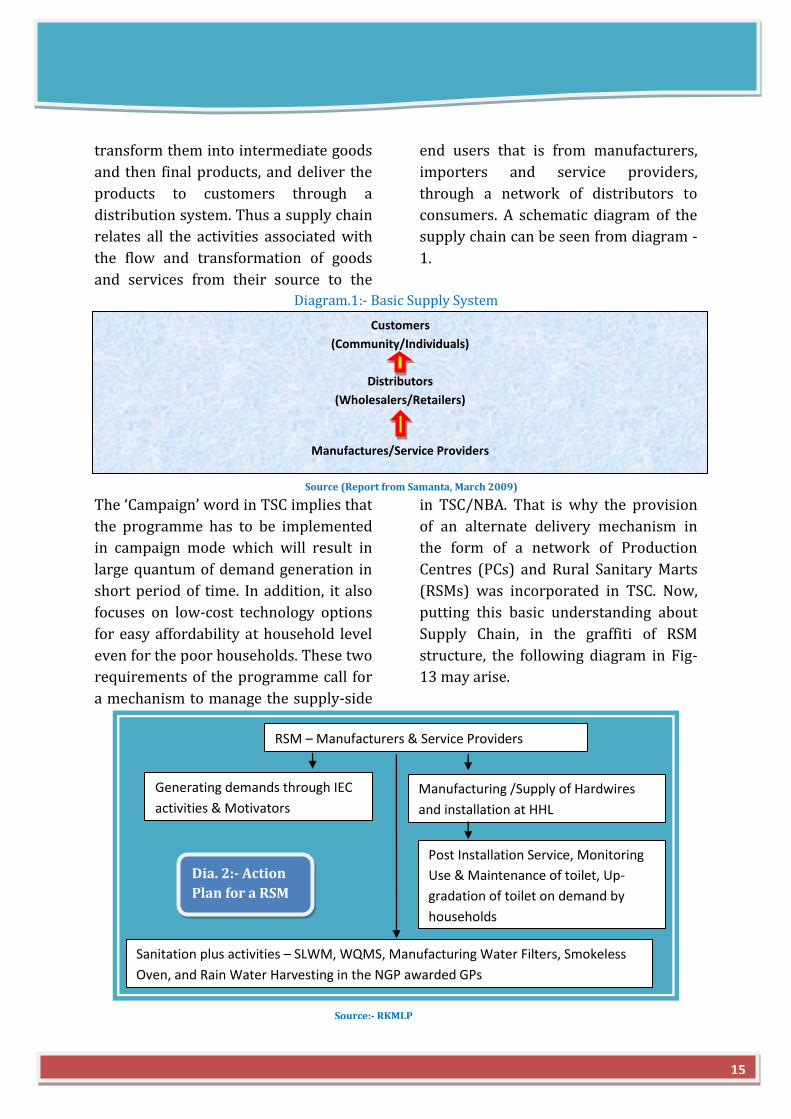
transform them into intermediate goods
and then final products, and deliver the
products to customers through a
distribution system. Thus a supply chain
relates all the activities associated with
the flow and transformation of goods
and services from their source to the
end users that is from manufacturers,
importers and service providers,
through a network of distributors to
consumers. A schematic diagram of the
supply chain can be seen from diagram -
1.
Diagram.1:- Basic Supply System
Source (Report from Samanta, March 2009)
The ‘Campaign’ word in TSC implies that
the programme has to be implemented
in campaign mode which will result in
large quantum of demand generation in
short period of time. In addition, it also
focuses on low-cost technology options
for easy affordability at household level
even for the poor households. These two
requirements of the programme call for
a mechanism to manage the supply-side
in TSC/NBA. That is why the provision
of an alternate delivery mechanism in
the form of a network of Production
Centres (PCs) and Rural Sanitary Marts
(RSMs) was incorporated in TSC. Now,
putting this basic understanding about
Supply Chain, in the graffiti of RSM
structure, the following diagram in Fig-
13 may arise.
RSM – Manufacturers & Service Providers
Generating demands through IEC
activities & Motivators
Manufacturing /Supply of Hardwires
and installation at HHL
Sanitation plus activities – SLWM, WQMS, Manufacturing Water Filters, Smokeless
Oven, and Rain Water Harvesting in the NGP awarded GPs
Post Installation Service, Monitoring
Use & Maintenance of toilet, Up-
gradation of toilet on demand by
households
Dia. 2:- Action
Plan for a RSM
Customers
(Community/Individuals)
Distributors
(Wholesalers/Retailers)
Manufactures/Service Providers
15
Source:- RKMLP

4.6 TSC/NBA Guidelines in Supply Chain The Central Rural Sanitation Program
(CRSP), in its 1993 Revised Guidelines,
had, for the first time, brought out the
concept of Rural Sanitary Mart (RSM) to
address the problem of supply chain in
rural sanitation. This was based on the
successful initiation of the concept by
UNICEF in some States. Since then the
concept has been carried through
various revisions of the CRSP including
the TSC (1999) and subsequently NBA
(2012). As per the TSC/NBA Guidelines,
the Rural Sanitary Mart (RSM), as a
stand alone or combined with the
Production Center (PC), is an effective
strategy of TSC/NBA to meet sanitary
ware and services demand. It is to
function as a hub for providing
Alternative Delivery Mechanism in
terms of low cost sanitary items and
services.
RSMs are supposed to have those items
that are required as a part of the
sanitation package that goes beyond
toilet construction. Production centres
are the means to improve production of
cost effective affordable sanitary
materials that are marketed through
RSMs generally managed by
NGOs/SHGs/Panchayats. The objective
of establishing RSM is not limited to its
functioning to accelerate the pace of the
sanitation program but also to provide
need based, locale specific people
centred system of outreach services of
trained masons, economically viable low
cost sanitation options including the
various low cost designs of the super
structure and catalyze the change in
behaviour and adoption of hygiene
facilities through IEC materials such as
pamphlets, posters, brochures, stickers,
etc.
As per the 2004 guideline, the TSC has
envisaged an investment, which can be
more than 5% of the total project outlay
(subject to a maximum of Rs 35.00 lakhs
per districts) of the total Government
outlay for the establishment of RSM and
production Centre. In 2007 guidelines, it
remained same, where as in 2012
(NBA), it is fixed upto 5% of the project
outlay (subject to a maximum of Rs
35.00 lakhs per districts). Funding for
this component is in the ratio of 80:20
between GOI and the State Government.
The upper financial limit for the
establishment of an RSM/PC has been
kept at Rs 3.5 lakhs. The amount is to be
utilized for construction of a shed
(including curing tank), training of
masons and also as a revolving fund.
Source:- google
16
After an RSM/PC attains a certain level
of sustainability, the revolving fund was
to be refunded to the District
Implementing Agency.
The District Implementing Agency is
required to identify key training
institutions/resource persons to train
the RSM/PC Mangers. An MOU is to be
signed with the agency establishing
RSM/PC and a system of joint
monitoring evolved to ensure that the
RSMs/PCs are successful as an
enterprise and function in accordance
with the objectives of the TSC/NBA.
Other than that, chronologically the
guidelines reflect clarity regarding the
policy along with specifying the
attributes towards RSM/PC’s operation.
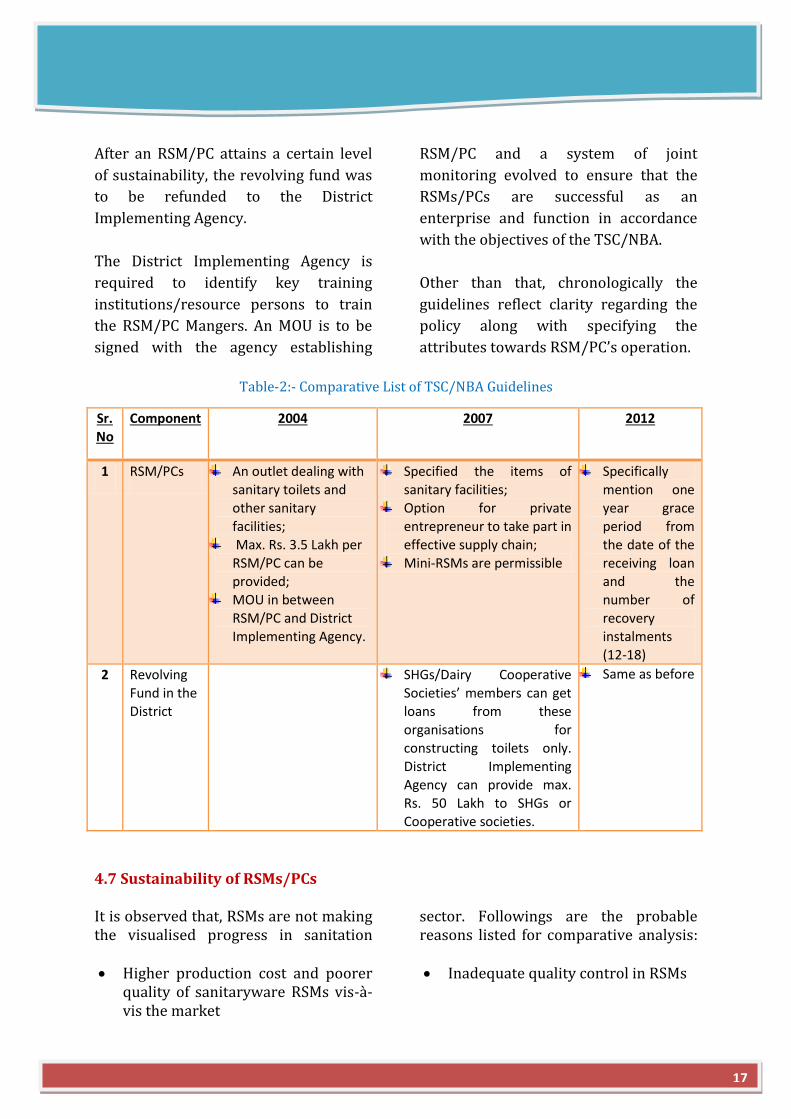
Table-2:- Comparative List of TSC/NBA Guidelines
Sr. No
Component 2004 2007 2012
1 RSM/PCs An outlet dealing with sanitary toilets and other sanitary
facilities;
Max. Rs. 3.5 Lakh per RSM/PC can be provided;
MOU in between RSM/PC and District
Implementing Agency.
Specified the items of sanitary facilities;
Option for private
entrepreneur to take part in
effective supply chain; Mini-RSMs are permissible
Specifically mention one year grace
period from
the date of the receiving loan and the
number of recovery
instalments (12-18)
2 Revolving Fund in the District
SHGs/Dairy Cooperative Societies’ members can get loans from these
organisations for constructing toilets only.
District Implementing Agency can provide max.
Rs. 50 Lakh to SHGs or Cooperative societies.
Same as before
4.7 Sustainability of RSMs/PCs It is observed that, RSMs are not making the visualised progress in sanitation
sector. Followings are the probable reasons listed for comparative analysis:
Higher production cost and poorer
quality of sanitaryware RSMs vis-à-vis the market
Inadequate quality control in RSMs
17
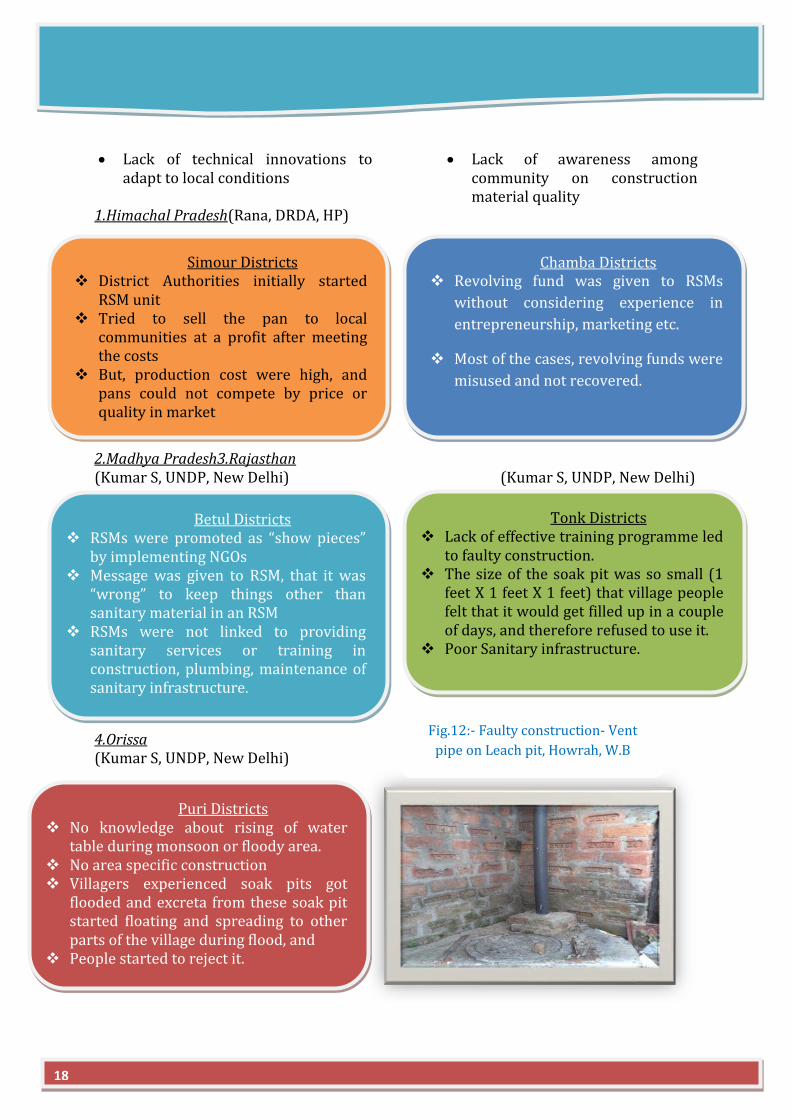
Lack of technical innovations to adapt to local conditions
Lack of awareness among community on construction material quality
1.Himachal Pradesh(Rana, DRDA, HP) 2.Madhya Pradesh3.Rajasthan (Kumar S, UNDP, New Delhi) (Kumar S, UNDP, New Delhi) 4.Orissa (Kumar S, UNDP, New Delhi)
Simour Districts District Authorities initially started
RSM unit Tried to sell the pan to local
communities at a profit after meeting the costs
But, production cost were high, and pans could not compete by price or quality in market
Chamba Districts Revolving fund was given to RSMs
without considering experience in
entrepreneurship, marketing etc.
Most of the cases, revolving funds were
misused and not recovered.
Betul Districts RSMs were promoted as “show pieces”
by implementing NGOs Message was given to RSM, that it was
“wrong” to keep things other than sanitary material in an RSM
RSMs were not linked to providing sanitary services or training in construction, plumbing, maintenance of sanitary infrastructure.
Tonk Districts Lack of effective training programme led
to faulty construction. The size of the soak pit was so small (1
feet X 1 feet X 1 feet) that village people felt that it would get filled up in a couple of days, and therefore refused to use it.
Poor Sanitary infrastructure.
Puri Districts No knowledge about rising of water
table during monsoon or floody area. No area specific construction Villagers experienced soak pits got
flooded and excreta from these soak pit started floating and spreading to other parts of the village during flood, and
People started to reject it.
Fig.12:- Faulty construction- Vent
pipe on Leach pit, Howrah, W.B
18
4.8. Reluctance among Government functionaries/ Stake holders The government system is so
used to well-defined guidelines
and instructions on every minor
detail that the flexibility given to
the districts in operationalizing
the supply chain mechanism was
not very much appreciated by
many states and during
interaction with them they used
to ask for further details
guidelines. For example, the
money available for setting up
RSM or PC could be used partly
for creating infrastructure and
partly as revolving fund or the
entire amount could also be used
as revolving fund but no such
percentage was decided in the
TSC guidelines. It was done
deliberately to give flexibility to
the TSC implementing agencies to
decide the best possible option as
per the ground reality. Afraid of
taking financial decision, informal
requests used to be made to the
ministry to issue further detailed
guidelines, which was fortunately
not agreed to and the basic
character of a flexible TSC
framework was retained. (Kumar
Alok, 2010)
According to Mr. Chattopadhyay
(WBCS), due to systematic failure
to disseminate “right information,
at right time” about the change in
choice (Mosaic pan to Ceramic
pan) for RSMs or PCs, leads to
unbalanced competition with
private entrepreneur. In Uttar
Pradesh, Private Entrepreneurs
reached to remote villages for
construction of toilets with
ceramic pan and readymade fiber
doors which attracted
households and they became
disinterested to use mosaic pans
manufactured by RSMs. The
RSMs have failed to compete with
them due to financial reason and
stopped functioning. As there is
no production unit of ceramic
pan in Uttar Pradesh, RSMs used
to procure the same directly from
Gujarat resulting in closure of
production centres of RSMs. Lack
of capacity of NGOs running RSM
to compete with the Private
entrepreneurs and the minimum
profit RSMs were getting on ‘No
Profit, No Loss’ has created
discouragement among the NGO
run RSMs. Now there is no NGO
managed RSM is functional in U.P.
Lack of convergence among
various associated departments
is one of the key reason of the
non sustainability of RSMs in case
of project or paper approval,
inspection, payment release etc.
During his field study in U.P, Mr.
Chattopadhyay found that, Block
Development Officer is not an
active partner of the Programme.
ADO (P) posted in the Block, on
behalf of the Panchayati Raj
Department looks after TSC. In
Even in Bengal
also, payment to
RSM at regular
interval is a
problem. People
used to say, “
Upare
Bhagaban, Niche
Pradhan”. Like
god, GP Pradhan
is the decider of
due payment
19

the Block level meeting, ADO(P)
normally does not get the opportunity to
mention progress & problems of TSC
implementation. DPROs opined that the
main problem of TSC implementation is
the non-cooperation / non-involvement
of the Block Development Officers. The
problem is that BDO is an officer of the
Rural Development Department and the
Nodal Department for TSC happens to
be Panchayati Raj Department. So fund
is directly placed with the Gram
Panchayats not through Block
Development Officer. This is a serious
problem of Convergence of important
stakeholders.
Even in Orissa, there are also
multifarious agencies with in a district
that are involved in the supply-chain
management. There is hardly any
coordination among them. The focus
being more on achieving the targets set,
the capability of the implementing
agencies is given a go-by. Barring
ceramic pan/trap/footrest and PVC
pipes, for most other components there
are no standards and hence quality
poses a big problem. Ensuring quality of
materials and services is the greatest
weakness in the present supply chain
system in Orissa. As a result the quality
of items available from the production
centres and the quality of toilets
constructed is much below the desired
level. For example, the reinforcement
given for cement rings is very weak
leading their breakage during
transportation (Samanta, March, 2009).
Adding to that, according to Mr.
Chattopadhyay, in U.P, there is no
Technical Officer in all District & Blocks
to give training of Masons. Masons’
training is held normally for 4/5 days
which is not residential. Training period
should be residential and at least for 8
days for acquiring proper skill. In
absence of Technical Officer, Quality
Control of the construction and
materials are not possible. Regular
monitoring meeting are not held at GP
level. / Block level. Many of the toilets
are not being used for the purpose it
was built. [Chattopadhyay, (WBCS),
W.B]
It was found through the study
conducted by Mr. Chakraborty that, in
Maharashtra, Social marketing
strategies focusing on demand creation
persuading consumer to consider
alternate and more affordable options
found to be absent to a great extent in
the present system. Various feasible
technological options for constructions
are not packaged in a way easily
accessible to consumer with clear
pricing information mapping out a step
by step upgrade path for lower cost
initial investment model. In absence of
proper knowledge and suitable supply
chain, end users constructing latrines of
expensive designs consisting of an offset
pit, a pour flush pan (many times
without adequate slope) , and brick
walls and C.G.I roof – as an entirely one-
time investment. This is done without
exploring the options of upgrading
latrines over a period of time. The
20

beneficiary community do not generally
have proper information and correct
understanding of technology. Neither
are they advised to invest on the asset in
a judicious manner. Though while
submitting the proposal for TSC
programme to GOI, DWSC committed
them for developing effective supply
chain setting up RSM/PC, but during the
implementation no due attention was
given in this regard. In spite of
substantial investment for setting up
RSM in Maharashtra, the supply chain
system is dominated primarily by
private sector with commercial motive
with very little attention towards
attaining social objective. Furthermore,
as those private-sector actors do not
have adequate technical understanding
on various aspects of sanitation, various
non-negotiable aspects have been
getting seriously compromised
(Chakraborty,2009).
4.9 Success story of RSM lead by RKMLP, West Bengal The programme for promotion of
sanitation was dependent not on the
needs of the country but on availability
of funds for subsidy from the
Government exchequer for construction
of toilets in rural households under
Central Rural Sanitation Programme
(CRSP).It was assumed by the planners
and policy makers that high rate of
subsidy will act as a means for creating
demand for household toilets but it was
observed later that strategically the
concept was weak. The yearly rate of
household toilet coverage in the country
was very insignificant against the total
number of non-toilet households. As a
result household toilet coverage in rural
areas was very marginal.
Realising the weaknesses in Government
operated sanitation programmes,
various experiments were carried out in
the country during end 80’s.
Ramakrishna Mission Lokasiksha
Parishad, Narendrapur conceived one
Demand Driven and People Centred
Sanitation programme in Medinipur
district of West Bengal in collaboration
with UNICEF. Medinipur is the most
populous district of the country.
Population was 8.3 million in 1991.
Fig. 13:- Latrine using SSP
Model in P. Midnapure
Fig. 14:- PC in Vivekananda Yuba Parishad (Cluster/RSM), W.B
21
Followings are the Salient Physical Achievements in Medinipur Sanitation Programme.
(Swami Asaktananda& Dey, 2005)
As a result of this intensive
endeavor, household toilet coverage
increased to 100% in Purba
Medinipur (total household
7,83,623) and 91% in Paschim
Medinipur (total household
9,14,042) district in December 2006,
against 4.74% in 1991.
Itwas noticed that Incidence of
diarrhoeal diseases has
tremendously reduced in the 100%
toilet access blocks and Gram
Panchayats.
Out of a total 7376 nos. of Rural
Primary Schools of Purba and
Paschim Medinipur districts, School
Toilet Blocks installed in 7376
Primary Schools till December 2006
Nandigram-II Block of Purba
Medinipur district is the First block
in the Country which has Achieved
100% Household Toilet Coverage in
December 2001.
Presently all 25 blocks of Purba
Medinipur district have achieved
100% household Toilet coverage and
the district has applied for “Nirmal
Zilla Puraskar” this year.
More than 30 International
delegations from China, Vietnam,
Bangladesh, Pakistan, Sri Lanka,
Indonesia, Burma, Nepal, Nigeria,
Tanzania, South Africa, Zimbabwe
and International Aid Agencies
(UNICEF, WHO, DFID, SIDA, AUS-Aid,
Water Aid, World Bank-WSP etc.)
paid study visits to understand the
innovative approach and strategies
developed and practised in
Medinipur Demand Driven
Sanitation Programme.
Government of West Bengal is
regularly using the expertise and
infrastructure of RKMLP for
imparting various training and
orientation programme for the TSC
functionaries of this state.
4.10 Need of the study From the discussion till now, it is cleared
that, the success of effective supply
chain system (RSM/PC) in Sanitation is
restricted in few pockets of the country
(like RKMLP’s Mednipure model) in
spite of equivalent guideline. As the
operational factors for the sustainability
of the RSM/PC varied from state to state,
having almost same universal Business
Model, it exhibits worst performance to
more than desired output depending
upon management, organizational
structure, role of motivator, back to back
supply following demand creation. The
study is to figure out all those positive
structural attributes which are the
reason for success of RSMs in some
region along with comparative study of
the impacts of the RSM on Sanitation
coverage, Behavioural change, based on
region specific socio-economic
condition.
22
RESULT AND ANALYSIS
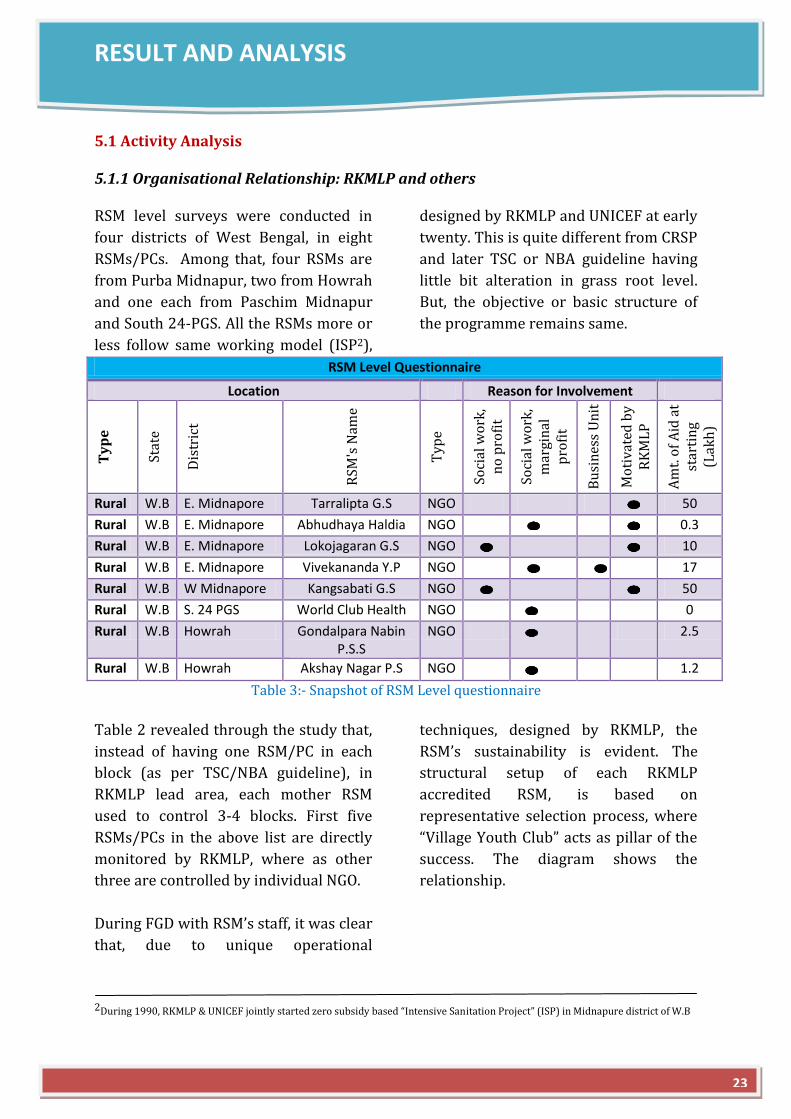
5.1 Activity Analysis 5.1.1 Organisational Relationship: RKMLP and others RSM level surveys were conducted in
four districts of West Bengal, in eight
RSMs/PCs. Among that, four RSMs are
from Purba Midnapur, two from Howrah
and one each from Paschim Midnapur
and South 24-PGS. All the RSMs more or
less follow same working model (ISP2),
designed by RKMLP and UNICEF at early
twenty. This is quite different from CRSP
and later TSC or NBA guideline having
little bit alteration in grass root level.
But, the objective or basic structure of
the programme remains same.
RSM Level Questionnaire
Location Reason for Involvement
Ty
pe
Stat
e
Dis
tric
t
RSM
's N
ame
Typ
e
Soci
al w
ork
, n
o p
rofi
t
Soci
al w
ork
, m
argi
nal
p
rofi
t
Bu
sin
ess
Un
it
Mo
tiva
ted
by
RK
ML
P
Am
t. o
f A
id a
t st
arti
ng
(Lak
h)
Rural W.B E. Midnapore Tarralipta G.S NGO
50
Rural W.B E. Midnapore Abhudhaya Haldia NGO
0.3
Rural W.B E. Midnapore Lokojagaran G.S NGO
10
Rural W.B E. Midnapore Vivekananda Y.P NGO
17
Rural W.B W Midnapore Kangsabati G.S NGO
50
Rural W.B S. 24 PGS World Club Health NGO
0
Rural W.B Howrah Gondalpara Nabin P.S.S
NGO
2.5
Rural W.B Howrah Akshay Nagar P.S NGO
1.2
Table 3:- Snapshot of RSM Level questionnaire
Table 2 revealed through the study that,
instead of having one RSM/PC in each
block (as per TSC/NBA guideline), in
RKMLP lead area, each mother RSM
used to control 3-4 blocks. First five
RSMs/PCs in the above list are directly
monitored by RKMLP, where as other
three are controlled by individual NGO.
During FGD with RSM’s staff, it was clear
that, due to unique operational
techniques, designed by RKMLP, the
RSM’s sustainability is evident. The
structural setup of each RKMLP
accredited RSM, is based on
representative selection process, where
“Village Youth Club” acts as pillar of the
success. The diagram shows the
relationship.
2During 1990, RKMLP & UNICEF jointly started zero subsidy based “Intensive Sanitation Project” (ISP) in Midnapure district of W.B
23
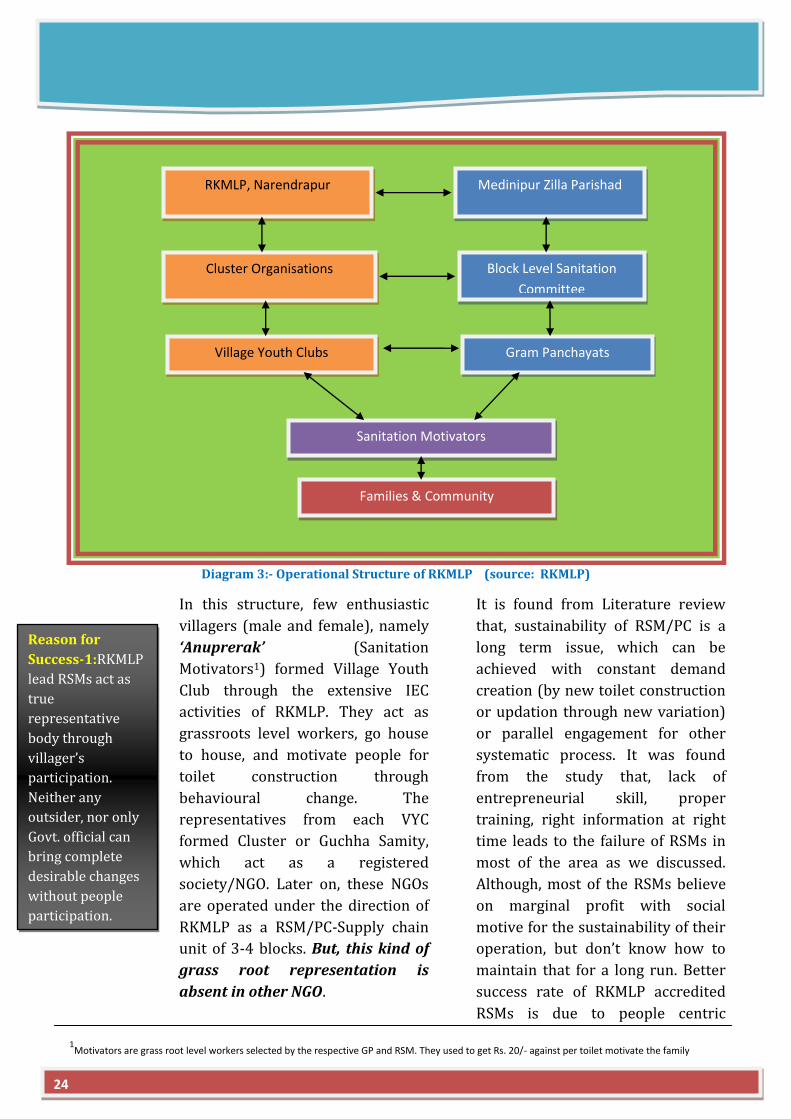
Diagram 3:- Operational Structure of RKMLP (source: RKMLP)
In this structure, few enthusiastic
villagers (male and female), namely
‘Anuprerak’ (Sanitation
Motivators1) formed Village Youth
Club through the extensive IEC
activities of RKMLP. They act as
grassroots level workers, go house
to house, and motivate people for
toilet construction through
behavioural change. The
representatives from each VYC
formed Cluster or Guchha Samity,
which act as a registered
society/NGO. Later on, these NGOs
are operated under the direction of
RKMLP as a RSM/PC-Supply chain
unit of 3-4 blocks. But, this kind of
grass root representation is
absent in other NGO.
It is found from Literature review
that, sustainability of RSM/PC is a
long term issue, which can be
achieved with constant demand
creation (by new toilet construction
or updation through new variation)
or parallel engagement for other
systematic process. It was found
from the study that, lack of
entrepreneurial skill, proper
training, right information at right
time leads to the failure of RSMs in
most of the area as we discussed.
Although, most of the RSMs believe
on marginal profit with social
motive for the sustainability of their
operation, but don’t know how to
maintain that for a long run. Better
success rate of RKMLP accredited
RSMs is due to people centric
Medinipur Zilla Parishad
Sanitation Committee
Cluster Organisations
(PC and SM operators)
RKMLP, Narendrapur
Block Level Sanitation
Committee
Village Youth Clubs Gram Panchayats
Sanitation Motivators
Families & Community
Reason for
Success-1:RKMLP
lead RSMs act as
true
representative
body through
villager’s
participation.
Neither any
outsider, nor only
Govt. official can
bring complete
desirable changes
without people
participation.
24
1Motivators are grass root level workers selected by the respective GP and RSM. They used to get Rs. 20/- against per toilet motivate the family

innovation, better management along
with regular M & E provide them
unprecedented millage.
During my study, I found other three
RSMs are also doing well internalising
the operational concepts of RKMLP, but
their motive is too much business
centric, deviating from social objectives.
Their main focus is “number of toilet
construction” to fulfil the target set by
Zilla Parisad rather than bringing any
permanent behavioural change through
intrinsic motivation. This part is well
observed in other areas of the country
which is one of the key reason for short
term achievement (NGP status), but fail
to maintain “Open Defecation Free
Village” for long term.
The operation process of RKMLP is quite
similar to “The Micro franchising
model” (Progress Brief; SNV, IRC 2012)
where one larger enterprise engages a
number of other people or small units to
implement the idea at scale.
5.1.2 Inequity in Financial help
Looking at the funding pattern from
Table 2, it gives clear indication, that all
the five RKMLP lead RSMs got sufficient
amount of fund (from UNICEF) at the
staring of their operation unlike rest of
three. So, in that case, the proportional
expenditures on Hardware and Software
are quite logical and effective for the
Clusters to bring the societal changes
upto a greater extent, unlike others (Non
RKMLP lead RSMs), who mainly
invested all the money on Hardware and
waited for the demand call from GP or
individual villagers.
5.2 Factors for Sustainability
If we consider the reply given by Mart
Managers, the success of Medinapur
model lies strongly on mainly five
attributes,
5.2.1 Less Operational Cost
Most of the RSM managers require
additional financial support to meet the
operational cost. It closely related to
production and transportation through
“economy of scale”.
Reason for Success-2:The concept RKMLP’s
“MOTHER RSM/PC (Cluster)” centre, taking
care of 3-4 blocks through “Satellite RSM” is a
well established formulae for long term
sustainability.
Reason for Success-3:Government Institutions (Water or Sanitation cell or Financing
Institution) or other donor agency (UNICEF) provided fund strengthened the base of the RSMs
to create more demand creation as well as infrastructure build up in Mednipur Model.
Reason for Success:One RSM/PC for 3-4 block leads
to larger action area More demand Less
production cost
Full load transport
Less Operational Cost Less unit transport cost
Fig
15:
SSP
Model
25
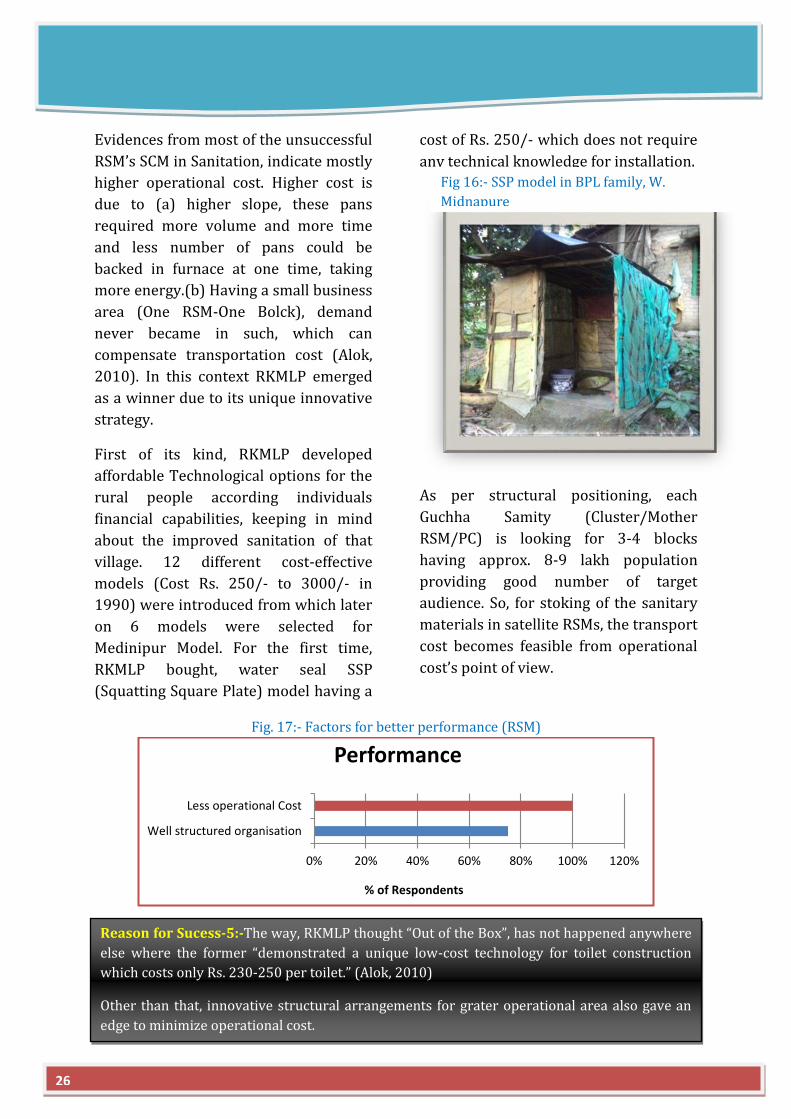
Evidences from most of the unsuccessful
RSM’s SCM in Sanitation, indicate mostly
higher operational cost. Higher cost is
due to (a) higher slope, these pans
required more volume and more time
and less number of pans could be
backed in furnace at one time, taking
more energy.(b) Having a small business
area (One RSM-One Bolck), demand
never became in such, which can
compensate transportation cost (Alok,
2010). In this context RKMLP emerged
as a winner due to its unique innovative
strategy.
First of its kind, RKMLP developed
affordable Technological options for the
rural people according individuals
financial capabilities, keeping in mind
about the improved sanitation of that
village. 12 different cost-effective
models (Cost Rs. 250/- to 3000/- in
1990) were introduced from which later
on 6 models were selected for
Medinipur Model. For the first time,
RKMLP bought, water seal SSP
(Squatting Square Plate) model having a
cost of Rs. 250/- which does not require
any technical knowledge for installation.
As per structural positioning, each
Guchha Samity (Cluster/Mother
RSM/PC) is looking for 3-4 blocks
having approx. 8-9 lakh population
providing good number of target
audience. So, for stoking of the sanitary
materials in satellite RSMs, the transport
cost becomes feasible from operational
cost’s point of view.
Fig. 17:- Factors for better performance (RSM)
0% 20% 40% 60% 80% 100% 120%
Well structured organisation
Less operational Cost
% of Respondents
Performance
Reason for Sucess-5:-The way, RKMLP thought “Out of the Box”, has not happened anywhere
else where the former “demonstrated a unique low-cost technology for toilet construction
which costs only Rs. 230-250 per toilet.” (Alok, 2010)
Other than that, innovative structural arrangements for grater operational area also gave an
edge to minimize operational cost.
Fig 16:- SSP model in BPL family, W.
Midnapure
26
5.2.2 Well Structured Organisation
Diagram 3, reveals organisational
structure of the Cluster/RSM’s
operation, involving people
participation in a unique way under the
guidance of RKMLP. Subsequently, Fig.
17, also indicate the importance given
by the mart managers or other staffs, to
structural superiority for better
performance. Although, few other NGO
driven RSMs/PCs are trying to follow
the model, but due to lack of proper
ideology, social motive and professional
approach, the success of the later still
remains rudiment.
At the beginning of the programme
(1990), Zilla administration of Midnapur
district also played pivotal role along
with RKMLP for regular monitoring and
inter-departmental coordination in a
unique way. It was fixed up that, every
Monday, there will be GP meeting along
with all the functionaries of sanitation,
Tuesday block level meeting,
Wednesday Sub-division meeting,
Friday district review meeting along
with all BDO, GP pradhan, Zilla
Sabhadhipati and RSM representatives.
End of every month, there is Review
meeting in RKMLP Head office with all
cluster representatives to check the
progress about the ongoing projects.
5.2.3 Water and Soil Testing Lab
Attachment of Water and Soil Testing
Lab with each Guchha Samity by RKMLP
and PRI pushed Cluster/RSMs one step
ahead for Sustainability. As per the
NRDWP guidelines, the water quality of
the village water source or resource
need to checked in 3 months interval.
Except that, it also facilitated farmers
with soil testing facility to know the
fertility of their sowing fields.
0% 20% 40% 60% 80% 100% 120%
Demand for New toilets/upgradation
Involved in other social activities
Full fledged Sanitary Retail outlet
Water/ Soil testing Lab
% of Respondents
Reason for Sucess-7:-Diversification of Water & Soil Testing Laboratory. 90% of the Mart
Manager tagged it as one of the priority zone for Sustainability
Reason for Sucess-6:-Unique
Organisational structure for better
intervention.
Fig 18:- Soil & Water Testing Labs in RSM
Fig. 19:- Responses from RSM managers regarding Sustainability of RSM
27

5.2.4Involvement in other Social Activities
All these Cluster organisation of
RKMLP are not only associated with
Sanitation Movement through toilet
construction, but they are closely
associated with other activities (Dey,
2005) lead by RKMLP (Fig.22).
Adult and Non Formal Education
Integrated Women and Child
Development
Preventive Health Care and
general Health services
Agriculture and Animal resource
Development
Forest Management and Social
Forestry
Promotion of Self-Help group
activities
Promotion of Solar energy, Water
purifier
Training on vocational skills,
Entrepreneurship and
organizational management
Promotion of Youth groups/
organisations for social
development
Following the same principle, Akshay
Nagar Pallisri Sangha (Studied RSM,
outside RKMLP authorisation) also
provides marketing tools& access to
local SHG for their processed food
products.
5.2.5 Demand for New Toilet/Up gradation
After the launching of NBA programme
(2012) along with convergence with
MGNREGA for giving Rs. 10,000/- as
subsidy for toilet construction, all the
villagers from the studied area (Latrine
or Non Latrine holders) are very much
interested for new latrine construction
or up-gradation. In, South 24PGS and
Howrah, already toilet construction has
took place under NBA model, where as
in both the Midnapur(s), it is still under
process due to some administrative
hindrance (till September, 2013). People
are also contributing on their own to
make the toilet more attractive or build
toilet cum bathroom. This also adds
value asserting long term demand at this
moment, which is reflected on the graph
(Fig. 19).
Reason for
Sucess-8:-
Involvement
of other
social
mobilization
programmes
among the
same target
segment
provides
increased
contacts for
the
maximum
coverage.
28
Fig 20:- Retail outlet of SHG made Food products in A.N.P.S
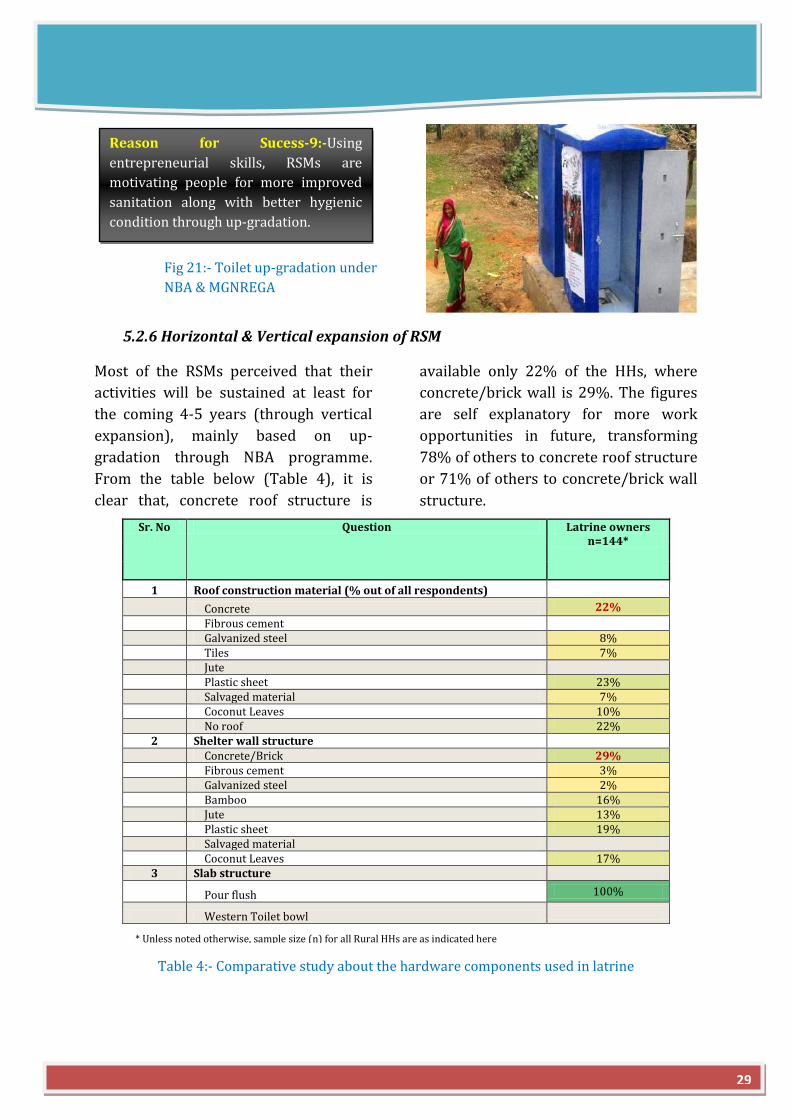
5.2.6 Horizontal & Vertical expansion of RSM
Most of the RSMs perceived that their
activities will be sustained at least for
the coming 4-5 years (through vertical
expansion), mainly based on up-
gradation through NBA programme.
From the table below (Table 4), it is
clear that, concrete roof structure is
available only 22% of the HHs, where
concrete/brick wall is 29%. The figures
are self explanatory for more work
opportunities in future, transforming
78% of others to concrete roof structure
or 71% of others to concrete/brick wall
structure.
Sr. No Question Latrine owners n=144*
1 Roof construction material (% out of all respondents)
Concrete 22%
Fibrous cement
Galvanized steel 8%
Tiles 7%
Jute
Plastic sheet 23%
Salvaged material 7%
Coconut Leaves 10%
No roof 22%
2 Shelter wall structure
Concrete/Brick 29%
Fibrous cement 3%
Galvanized steel 2%
Bamboo 16%
Jute 13%
Plastic sheet 19%
Salvaged material
Coconut Leaves 17%
3 Slab structure
Pour flush 100%
Western Toilet bowl
Table 4:- Comparative study about the hardware components used in latrine
Fig 21:- Toilet up-gradation under
NBA & MGNREGA
* Unless noted otherwise, sample size (n) for all Rural HHs are as indicated here
29
Reason for Sucess-9:-Using
entrepreneurial skills, RSMs are
motivating people for more improved
sanitation along with better hygienic
condition through up-gradation.
To achieve sustainability for the longer
period, horizontal expansion plan need
to be adopted, which is discussed in
detailed in “Recommendation &
Conclusion” section.
In addition, the report titled “Rural
Sanitation Supply Chains and Finance”
(2012), published by SNV & IRC
revealed that the success of sanitation
coverage depends on “demand
aggregation and better linkages between
SME and consumers”. For example, in
Cambodia, ‘village sales agent’ plays
same role as ‘sanitation motivator’
appointed by RKMLP. Even, in Nepal, the
experiment was done to establish
relationship in between shops at district
headquarters and village level ‘outlet’
through existing village shops. More on
that, micro-finance plays an important
role. In south India (Trichy), the
subsidiary unit of Gramalaya, viz,
Gramalaya Microfin Foundation
provides micro-finance for toilet
construction.
5.3 Operational & Financial viability of RSM/PC
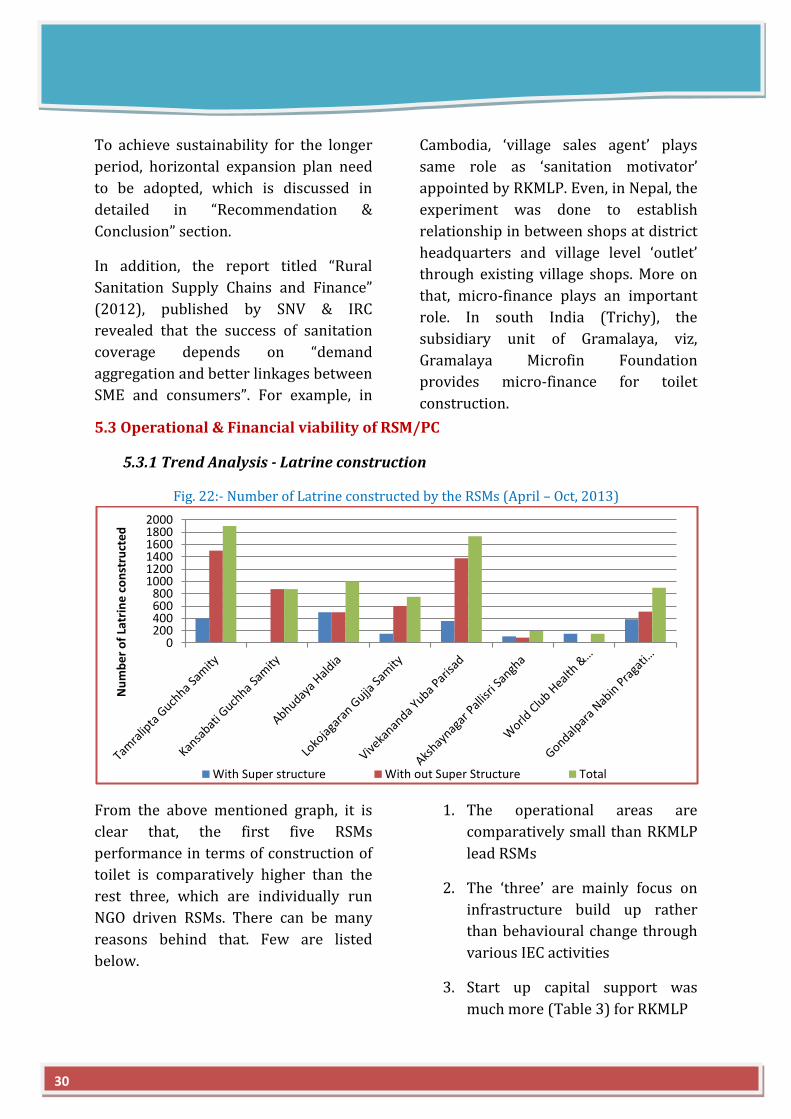
5.3.1 Trend Analysis - Latrine construction
Fig. 22:- Number of Latrine constructed by the RSMs (April – Oct, 2013)
From the above mentioned graph, it is
clear that, the first five RSMs
performance in terms of construction of
toilet is comparatively higher than the
rest three, which are individually run
NGO driven RSMs. There can be many
reasons behind that. Few are listed
below.
1. The operational areas are
comparatively small than RKMLP
lead RSMs
2. The ‘three’ are mainly focus on
infrastructure build up rather
than behavioural change through
various IEC activities
3. Start up capital support was
much more (Table 3) for RKMLP
0200400600800
100012001400160018002000
Nu
mb
er
of
Latr
ine
co
nst
ruct
ed
With Super structure With out Super Structure Total
30
lead RSMs compared to others,
which led to infrastructural
disparity
4. Five said RSMs usually get each
other support in case of
production, supply and shifting of
ideal manpower under single
umbrella (RKMLP), which is not
available for others.
5. Abundance of other activities by
RKMLP facilitates RSMs to gain
more trust and respect from the
people, where others remain as a
“Toilet Constructing Unit”
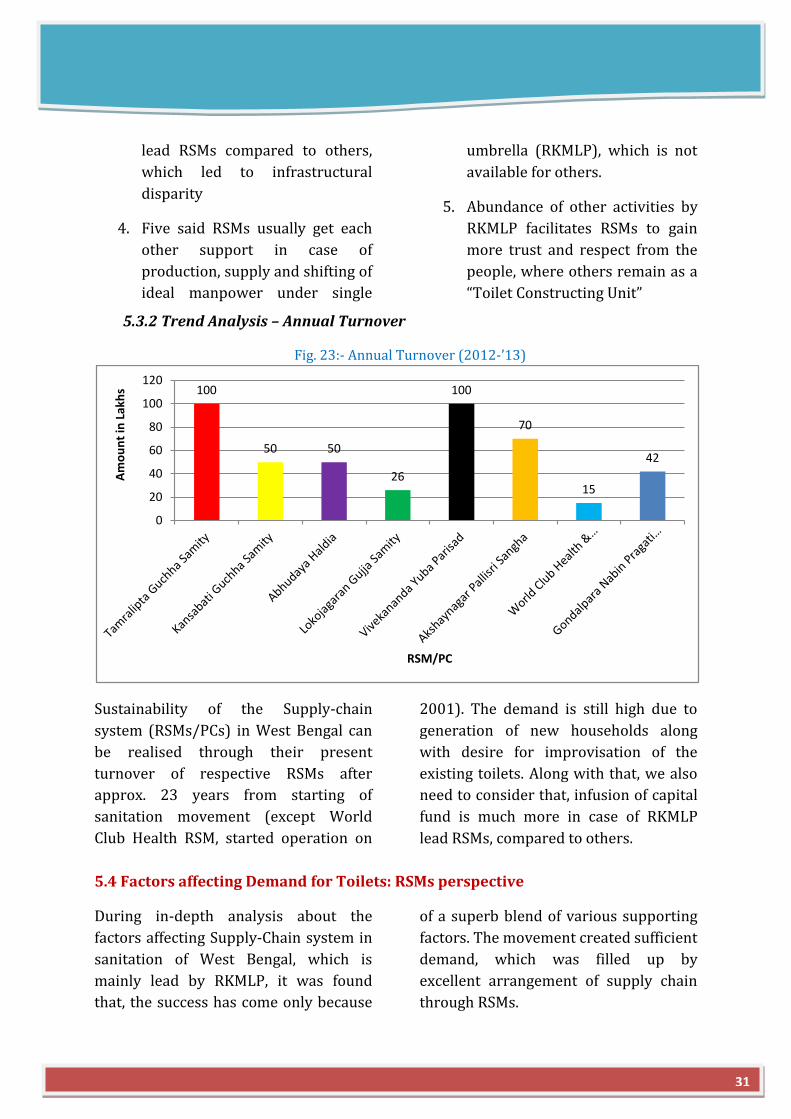
5.3.2 Trend Analysis – Annual Turnover
Fig. 23:- Annual Turnover (2012-’13)
Sustainability of the Supply-chain
system (RSMs/PCs) in West Bengal can
be realised through their present
turnover of respective RSMs after
approx. 23 years from starting of
sanitation movement (except World
Club Health RSM, started operation on
2001). The demand is still high due to
generation of new households along
with desire for improvisation of the
existing toilets. Along with that, we also
need to consider that, infusion of capital
fund is much more in case of RKMLP
lead RSMs, compared to others.
5.4 Factors affecting Demand for Toilets: RSMs perspective
During in-depth analysis about the
factors affecting Supply-Chain system in
sanitation of West Bengal, which is
mainly lead by RKMLP, it was found
that, the success has come only because
of a superb blend of various supporting
factors. The movement created sufficient
demand, which was filled up by
excellent arrangement of supply chain
through RSMs.
100
50 50
26
100
70
15
42
0
20
40
60
80
100
120
Am
ou
nt
in L
akh
s
RSM/PC
31
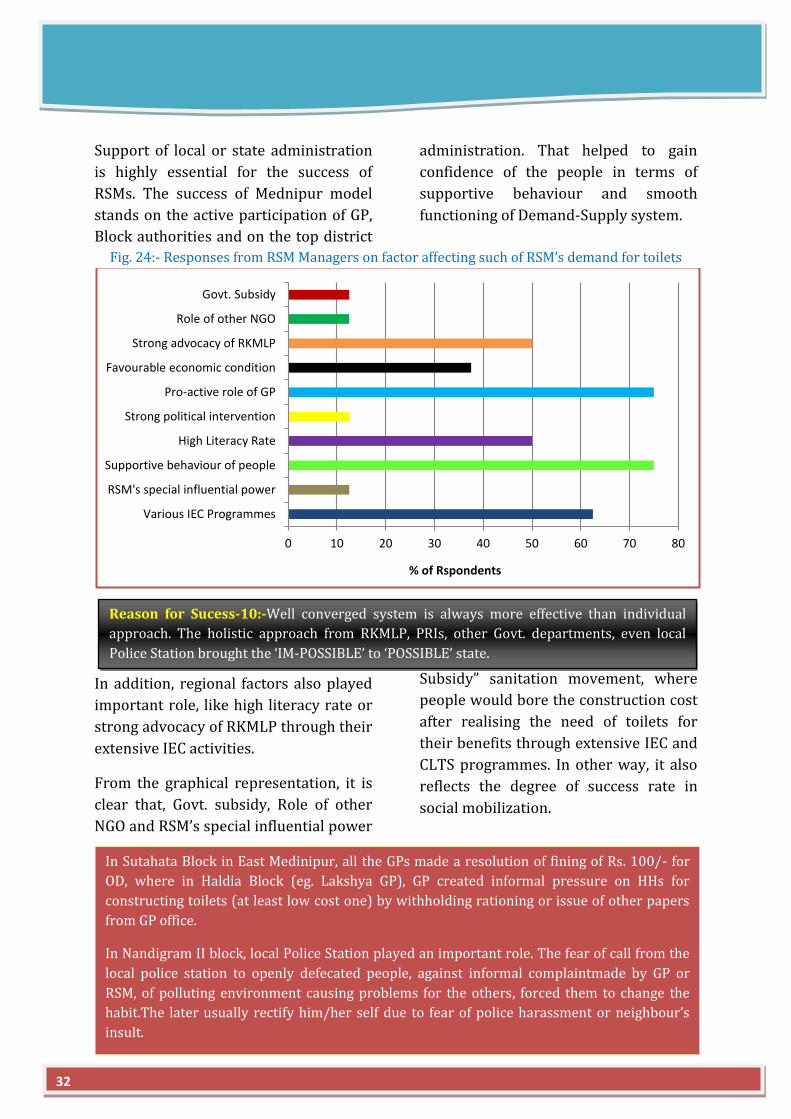
Support of local or state administration
is highly essential for the success of
RSMs. The success of Mednipur model
stands on the active participation of GP,
Block authorities and on the top district
administration. That helped to gain
confidence of the people in terms of
supportive behaviour and smooth
functioning of Demand-Supply system.
Fig. 24:- Responses from RSM Managers on factor affecting such of RSM’s demand for toilets
In addition, regional factors also played
important role, like high literacy rate or
strong advocacy of RKMLP through their
extensive IEC activities.
From the graphical representation, it is
clear that, Govt. subsidy, Role of other
NGO and RSM’s special influential power
played less important role in Sanitation
movement. From the beginning, unlike
others, RKMLP’s focus was “Zero
Subsidy” sanitation movement, where
people would bore the construction cost
after realising the need of toilets for
their benefits through extensive IEC and
CLTS programmes. In other way, it also
reflects the degree of success rate in
social mobilization.
0 10 20 30 40 50 60 70 80
Various IEC Programmes
RSM's special influential power
Supportive behaviour of people
High Literacy Rate
Strong political intervention
Pro-active role of GP
Favourable economic condition
Strong advocacy of RKMLP
Role of other NGO
Govt. Subsidy
% of Rspondents
Reason for Sucess-10:-Well converged system is always more effective than individual
approach. The holistic approach from RKMLP, PRIs, other Govt. departments, even local
Police Station brought the ‘IM-POSSIBLE’ to ‘POSSIBLE’ state.
In Sutahata Block in East Medinipur, all the GPs made a resolution of fining of Rs. 100/- for
OD, where in Haldia Block (eg. Lakshya GP), GP created informal pressure on HHs for
constructing toilets (at least low cost one) by withholding rationing or issue of other papers
from GP office.
In Nandigram II block, local Police Station played an important role. The fear of call from the
local police station to openly defecated people, against informal complaintmade by GP or
RSM, of polluting environment causing problems for the others, forced them to change the
habit.The later usually rectify him/her self due to fear of police harassment or neighbour’s
insult.
32
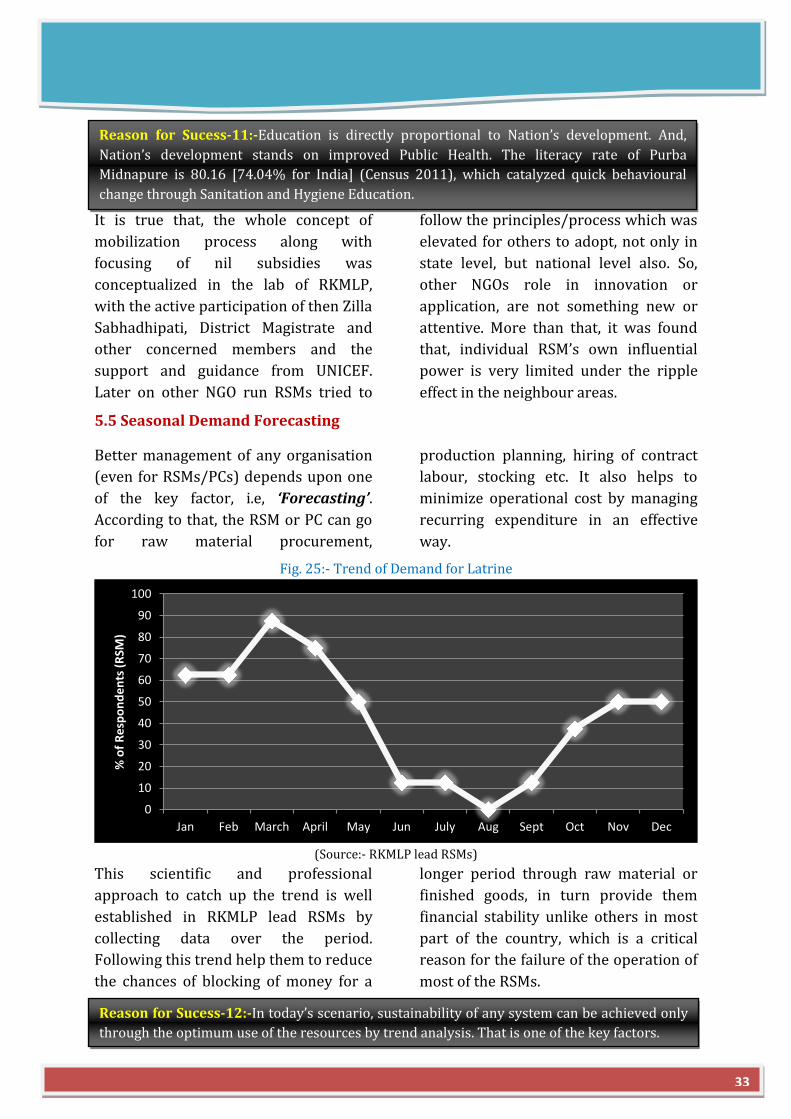
It is true that, the whole concept of
mobilization process along with
focusing of nil subsidies was
conceptualized in the lab of RKMLP,
with the active participation of then Zilla
Sabhadhipati, District Magistrate and
other concerned members and the
support and guidance from UNICEF.
Later on other NGO run RSMs tried to
follow the principles/process which was
elevated for others to adopt, not only in
state level, but national level also. So,
other NGOs role in innovation or
application, are not something new or
attentive. More than that, it was found
that, individual RSM’s own influential
power is very limited under the ripple
effect in the neighbour areas.
5.5 Seasonal Demand Forecasting
Better management of any organisation
(even for RSMs/PCs) depends upon one
of the key factor, i.e, ‘Forecasting’.
According to that, the RSM or PC can go
for raw material procurement,
production planning, hiring of contract
labour, stocking etc. It also helps to
minimize operational cost by managing
recurring expenditure in an effective
way.
Fig. 25:- Trend of Demand for Latrine
(Source:- RKMLP lead RSMs)
This scientific and professional
approach to catch up the trend is well
established in RKMLP lead RSMs by
collecting data over the period.
Following this trend help them to reduce
the chances of blocking of money for a
longer period through raw material or
finished goods, in turn provide them
financial stability unlike others in most
part of the country, which is a critical
reason for the failure of the operation of
most of the RSMs.
0
10
20
30
40
50
60
70
80
90
100
Jan Feb March April May Jun July Aug Sept Oct Nov Dec
% o
f R
esp
on
de
nts
(R
SM)
Reason for Sucess-12:-In today’s scenario, sustainability of any system can be achieved only
through the optimum use of the resources by trend analysis. That is one of the key factors.
33
Reason for Sucess-11:-Education is directly proportional to Nation’s development. And,
Nation’s development stands on improved Public Health. The literacy rate of Purba
Midnapure is 80.16 [74.04% for India] (Census 2011), which catalyzed quick behavioural
change through Sanitation and Hygiene Education.
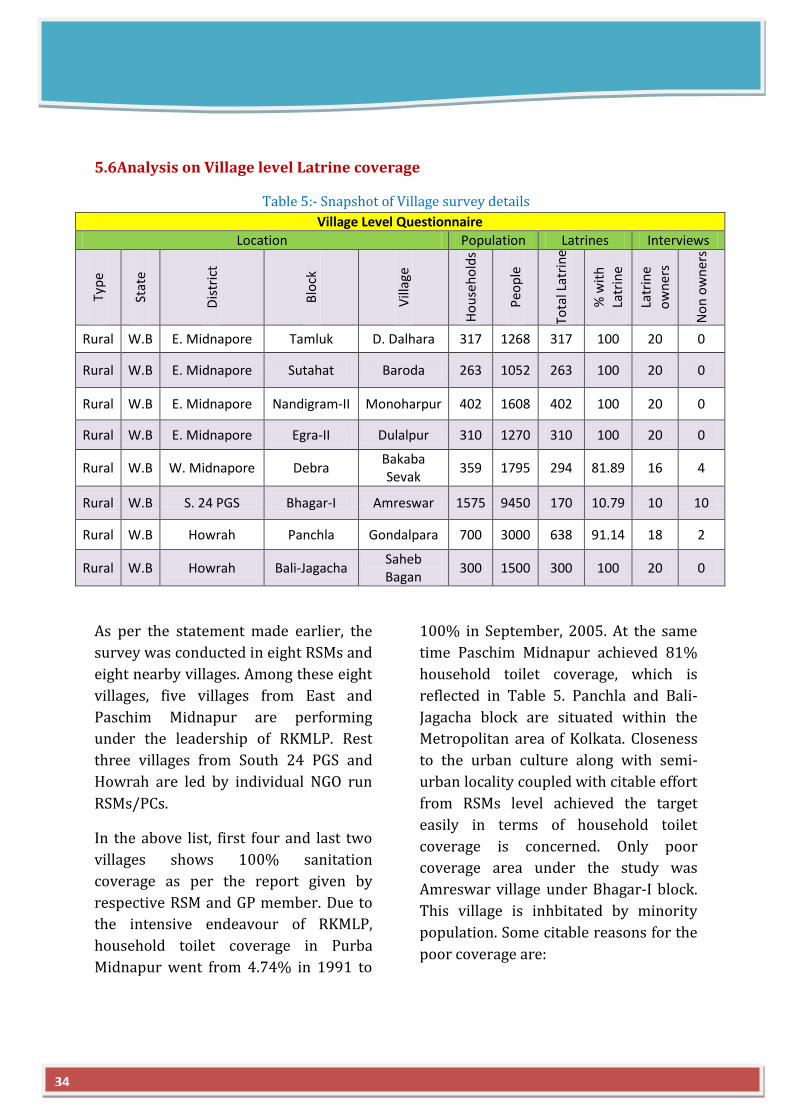
5.6Analysis on Village level Latrine coverage
Table 5:- Snapshot of Village survey details
Village Level Questionnaire
Location Population Latrines Interviews
Typ
e
Stat
e
Dis
tric
t
Blo
ck
Vill
age
Ho
use
ho
lds
Peo
ple
Tota
l Lat
rin
e
% w
ith
La
trin
e
Latr
ine
ow
ner
s
No
n o
wn
ers
Rural W.B E. Midnapore Tamluk D. Dalhara 317 1268 317 100 20 0
Rural W.B E. Midnapore Sutahat Baroda 263 1052 263 100 20 0
Rural W.B E. Midnapore Nandigram-II Monoharpur 402 1608 402 100 20 0
Rural W.B E. Midnapore Egra-II Dulalpur 310 1270 310 100 20 0
Rural W.B W. Midnapore Debra Bakaba Sevak
359 1795 294 81.89 16 4
Rural W.B S. 24 PGS Bhagar-I Amreswar 1575 9450 170 10.79 10 10
Rural W.B Howrah Panchla Gondalpara 700 3000 638 91.14 18 2
Rural W.B Howrah Bali-Jagacha Saheb Bagan
300 1500 300 100 20 0
As per the statement made earlier, the
survey was conducted in eight RSMs and
eight nearby villages. Among these eight
villages, five villages from East and
Paschim Midnapur are performing
under the leadership of RKMLP. Rest
three villages from South 24 PGS and
Howrah are led by individual NGO run
RSMs/PCs.
In the above list, first four and last two
villages shows 100% sanitation
coverage as per the report given by
respective RSM and GP member. Due to
the intensive endeavour of RKMLP,
household toilet coverage in Purba
Midnapur went from 4.74% in 1991 to
100% in September, 2005. At the same
time Paschim Midnapur achieved 81%
household toilet coverage, which is
reflected in Table 5. Panchla and Bali-
Jagacha block are situated within the
Metropolitan area of Kolkata. Closeness
to the urban culture along with semi-
urban locality coupled with citable effort
from RSMs level achieved the target
easily in terms of household toilet
coverage is concerned. Only poor
coverage area under the study was
Amreswar village under Bhagar-I block.
This village is inhbitated by minority
population. Some citable reasons for the
poor coverage are:
34
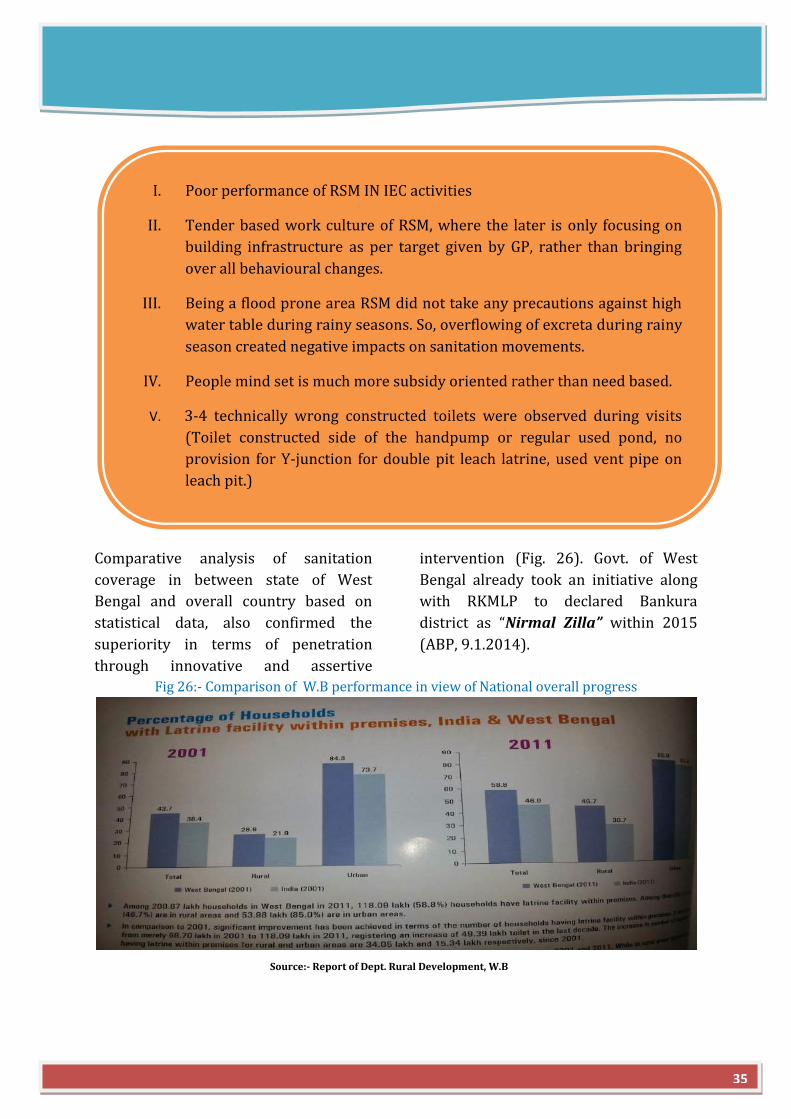
Comparative analysis of sanitation
coverage in between state of West
Bengal and overall country based on
statistical data, also confirmed the
superiority in terms of penetration
through innovative and assertive
intervention (Fig. 26). Govt. of West
Bengal already took an initiative along
with RKMLP to declared Bankura
district as “Nirmal Zilla” within 2015
(ABP, 9.1.2014).
Fig 26:- Comparison of W.B performance in view of National overall progress
I. Poor performance of RSM IN IEC activities
II. Tender based work culture of RSM, where the later is only focusing on
building infrastructure as per target given by GP, rather than bringing
over all behavioural changes.
III. Being a flood prone area RSM did not take any precautions against high
water table during rainy seasons. So, overflowing of excreta during rainy
season created negative impacts on sanitation movements.
IV. People mind set is much more subsidy oriented rather than need based.
V. 3-4 technically wrong constructed toilets were observed during visits
(Toilet constructed side of the handpump or regular used pond, no
provision for Y-junction for double pit leach latrine, used vent pipe on
leach pit.)
Source:- Report of Dept. Rural Development, W.B
35
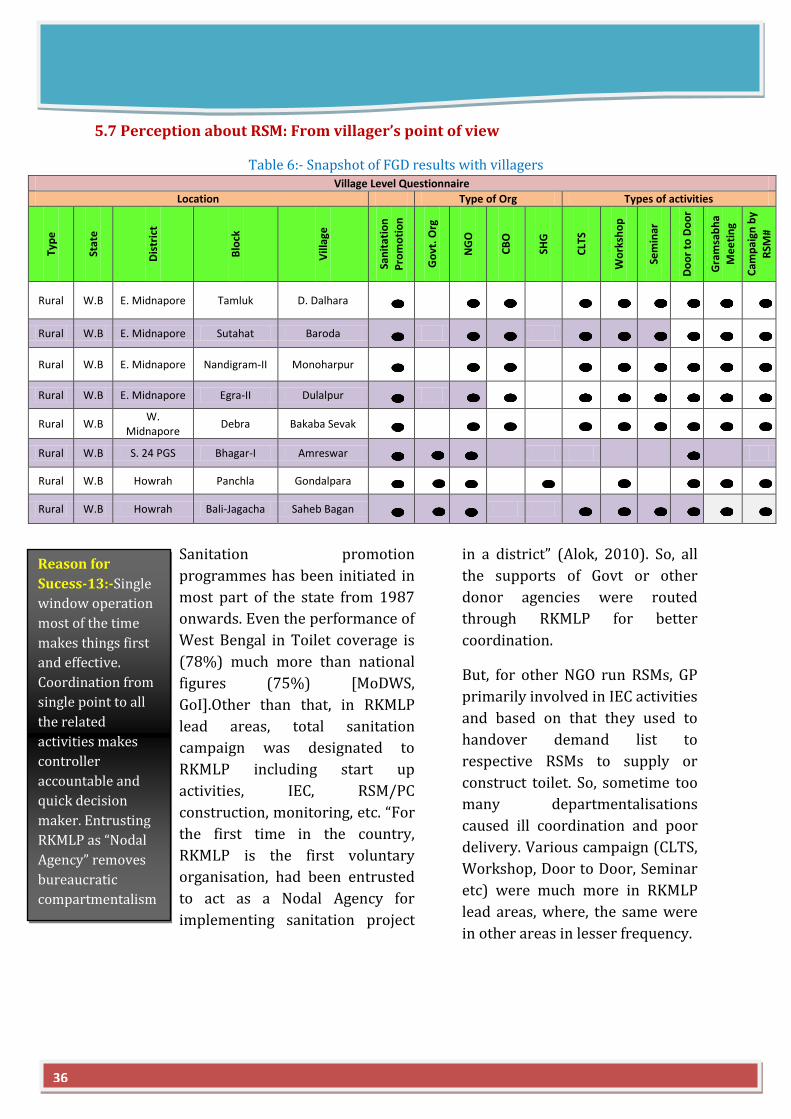
5.7 Perception about RSM: From villager’s point of view
Table 6:- Snapshot of FGD results with villagers Village Level Questionnaire
Location Type of Org Types of activities
Typ
e
Stat
e
Dis
tric
t
Blo
ck
Vill
age
San
itat
ion
P
rom
oti
on
Go
vt. O
rg
NG
O
CB
O
SHG
CLT
S
Wo
rksh
op
Sem
inar
Do
or
to D
oo
r
Gra
msa
bh
a
Me
eti
ng
Cam
pai
gn b
y
RSM
#
Rural W.B E. Midnapore Tamluk D. Dalhara
Rural W.B E. Midnapore Sutahat Baroda
Rural W.B E. Midnapore Nandigram-II Monoharpur
Rural W.B E. Midnapore Egra-II Dulalpur
Rural W.B W.
Midnapore Debra Bakaba Sevak
Rural W.B S. 24 PGS Bhagar-I Amreswar
Rural W.B Howrah Panchla Gondalpara
Rural W.B Howrah Bali-Jagacha Saheb Bagan
Sanitation promotion
programmes has been initiated in
most part of the state from 1987
onwards. Even the performance of
West Bengal in Toilet coverage is
(78%) much more than national
figures (75%) [MoDWS,
GoI].Other than that, in RKMLP
lead areas, total sanitation
campaign was designated to
RKMLP including start up
activities, IEC, RSM/PC
construction, monitoring, etc. “For
the first time in the country,
RKMLP is the first voluntary
organisation, had been entrusted
to act as a Nodal Agency for
implementing sanitation project
in a district” (Alok, 2010). So, all
the supports of Govt or other
donor agencies were routed
through RKMLP for better
coordination.
But, for other NGO run RSMs, GP
primarily involved in IEC activities
and based on that they used to
handover demand list to
respective RSMs to supply or
construct toilet. So, sometime too
many departmentalisations
caused ill coordination and poor
delivery. Various campaign (CLTS,
Workshop, Door to Door, Seminar
etc) were much more in RKMLP
lead areas, where, the same were
in other areas in lesser frequency.
36
Reason for
Sucess-13:-Single
window operation
most of the time
makes things first
and effective.
Coordination from
single point to all
the related
activities makes
controller
accountable and
quick decision
maker. Entrusting
RKMLP as “Nodal
Agency” removes
bureaucratic
compartmentalism
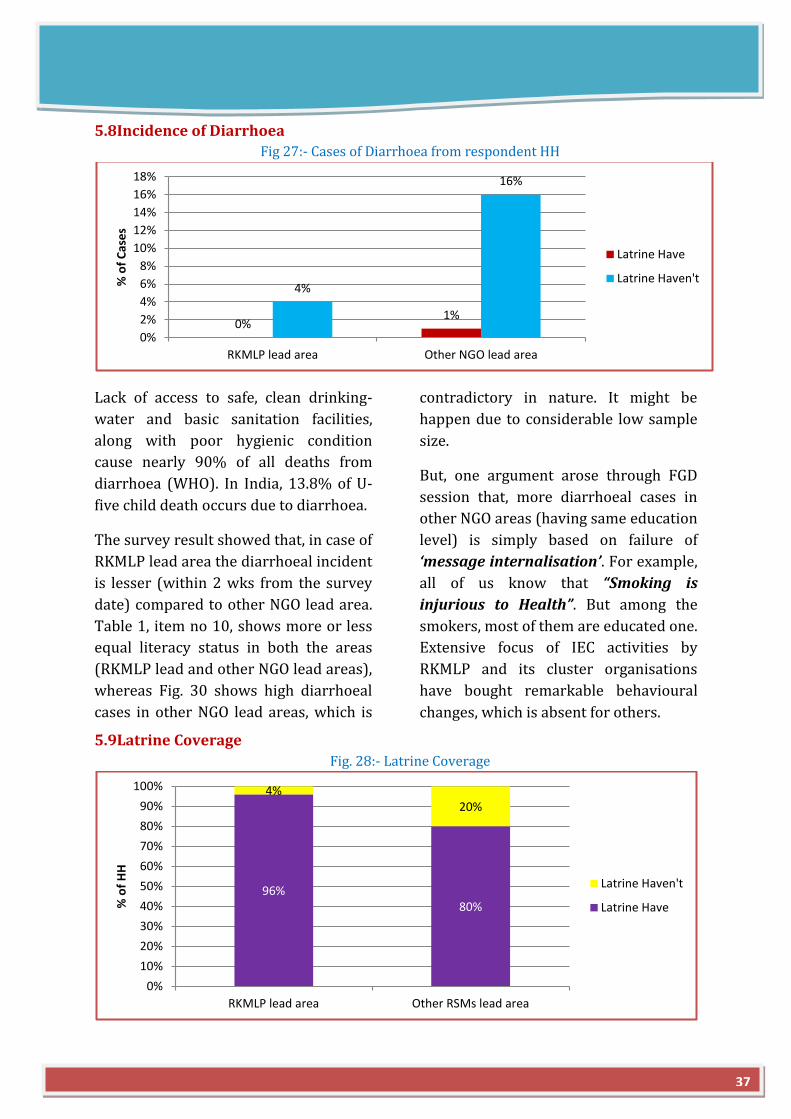
5.8Incidence of Diarrhoea
Fig 27:- Cases of Diarrhoea from respondent HH
Lack of access to safe, clean drinking-
water and basic sanitation facilities,
along with poor hygienic condition
cause nearly 90% of all deaths from
diarrhoea (WHO). In India, 13.8% of U-
five child death occurs due to diarrhoea.
The survey result showed that, in case of
RKMLP lead area the diarrhoeal incident
is lesser (within 2 wks from the survey
date) compared to other NGO lead area.
Table 1, item no 10, shows more or less
equal literacy status in both the areas
(RKMLP lead and other NGO lead areas),
whereas Fig. 30 shows high diarrhoeal
cases in other NGO lead areas, which is
contradictory in nature. It might be
happen due to considerable low sample
size.
But, one argument arose through FGD
session that, more diarrhoeal cases in
other NGO areas (having same education
level) is simply based on failure of
‘message internalisation’. For example,
all of us know that “Smoking is
injurious to Health”. But among the
smokers, most of them are educated one.
Extensive focus of IEC activities by
RKMLP and its cluster organisations
have bought remarkable behavioural
changes, which is absent for others.
5.9Latrine Coverage
Fig. 28:- Latrine Coverage
0% 1%
4%
16%
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
RKMLP lead area Other NGO lead area
% o
f C
ase
s
Latrine Have
Latrine Haven't
96% 80%
4% 20%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
RKMLP lead area Other RSMs lead area
% o
f H
H
Latrine Haven't
Latrine Have
37
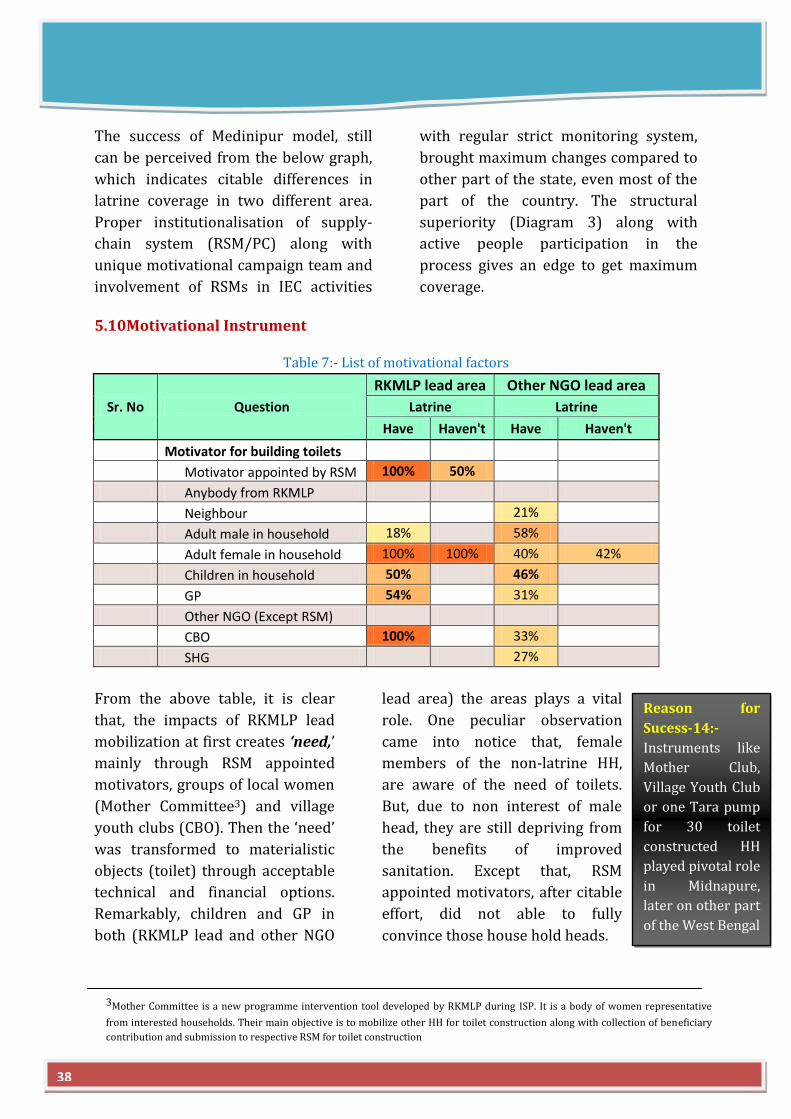
The success of Medinipur model, still
can be perceived from the below graph,
which indicates citable differences in
latrine coverage in two different area.
Proper institutionalisation of supply-
chain system (RSM/PC) along with
unique motivational campaign team and
involvement of RSMs in IEC activities
with regular strict monitoring system,
brought maximum changes compared to
other part of the state, even most of the
part of the country. The structural
superiority (Diagram 3) along with
active people participation in the
process gives an edge to get maximum
coverage.
5.10Motivational Instrument
Table 7:- List of motivational factors
Sr. No Question
RKMLP lead area Other NGO lead area
Latrine Latrine
Have Haven't Have Haven't
Motivator for building toilets
Motivator appointed by RSM 100% 50%
Anybody from RKMLP
Neighbour 21%
Adult male in household 18% 58%
Adult female in household 100% 100% 40% 42%
Children in household 50% 46%
GP 54% 31%
Other NGO (Except RSM)
CBO 100% 33%
SHG 27%
From the above table, it is clear
that, the impacts of RKMLP lead
mobilization at first creates ‘need,’
mainly through RSM appointed
motivators, groups of local women
(Mother Committee3) and village
youth clubs (CBO). Then the ‘need’
was transformed to materialistic
objects (toilet) through acceptable
technical and financial options.
Remarkably, children and GP in
both (RKMLP lead and other NGO
lead area) the areas plays a vital
role. One peculiar observation
came into notice that, female
members of the non-latrine HH,
are aware of the need of toilets.
But, due to non interest of male
head, they are still depriving from
the benefits of improved
sanitation. Except that, RSM
appointed motivators, after citable
effort, did not able to fully
convince those house hold heads.
Reason for
Sucess-14:-
Instruments like
Mother Club,
Village Youth Club
or one Tara pump
for 30 toilet
constructed HH
played pivotal role
in Midnapure,
later on other part
of the West Bengal
38
3Mother Committee is a new programme intervention tool developed by RKMLP during ISP. It is a body of women representative
from interested households. Their main objective is to mobilize other HH for toilet construction along with collection of beneficiary
contribution and submission to respective RSM for toilet construction
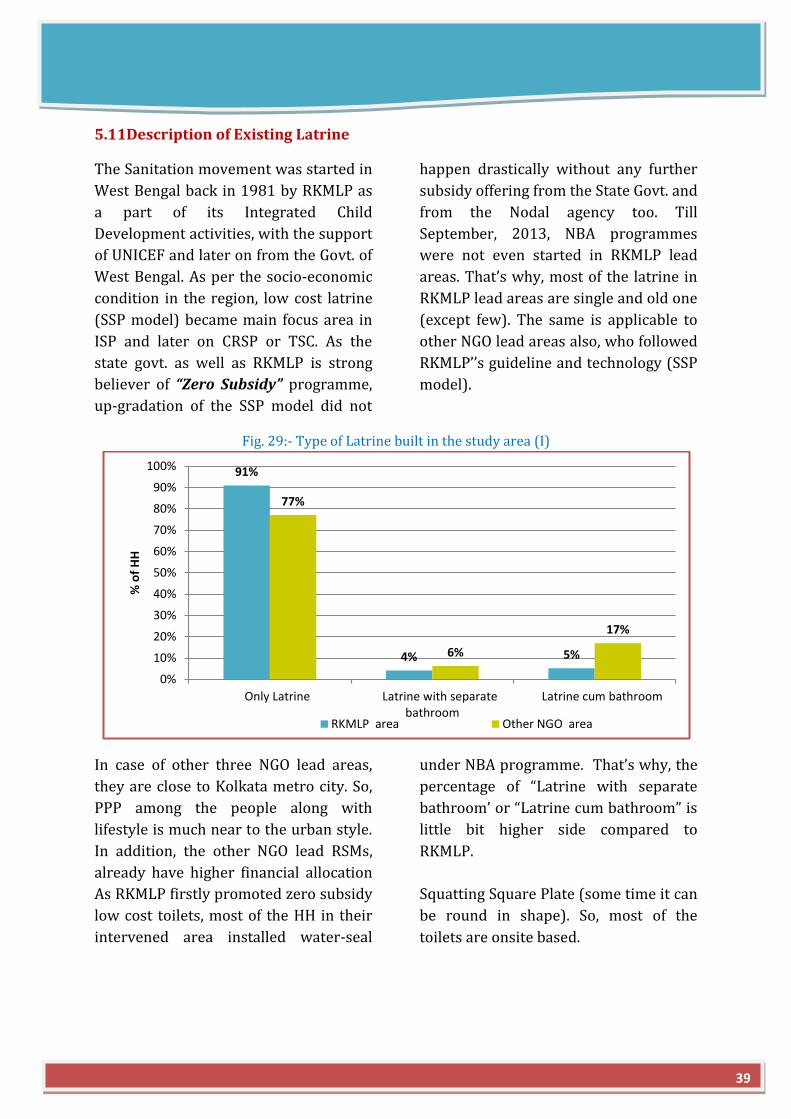
5.11Description of Existing Latrine
The Sanitation movement was started in
West Bengal back in 1981 by RKMLP as
a part of its Integrated Child
Development activities, with the support
of UNICEF and later on from the Govt. of
West Bengal. As per the socio-economic
condition in the region, low cost latrine
(SSP model) became main focus area in
ISP and later on CRSP or TSC. As the
state govt. as well as RKMLP is strong
believer of “Zero Subsidy” programme,
up-gradation of the SSP model did not
happen drastically without any further
subsidy offering from the State Govt. and
from the Nodal agency too. Till
September, 2013, NBA programmes
were not even started in RKMLP lead
areas. That’s why, most of the latrine in
RKMLP lead areas are single and old one
(except few). The same is applicable to
other NGO lead areas also, who followed
RKMLP’’s guideline and technology (SSP
model).
Fig. 29:- Type of Latrine built in the study area (I)
In case of other three NGO lead areas,
they are close to Kolkata metro city. So,
PPP among the people along with
lifestyle is much near to the urban style.
In addition, the other NGO lead RSMs,
already have higher financial allocation
under NBA programme. That’s why, the
percentage of “Latrine with separate
bathroom’ or “Latrine cum bathroom” is
little bit higher side compared to
RKMLP.
As RKMLP firstly promoted zero subsidy
low cost toilets, most of the HH in their
intervened area installed water-seal
Squatting Square Plate (some time it can
be round in shape). So, most of the
toilets are onsite based.
91%
4% 5%
77%
6%
17%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Only Latrine Latrine with separatebathroom
Latrine cum bathroom
% o
f H
H
RKMLP area Other NGO area
39
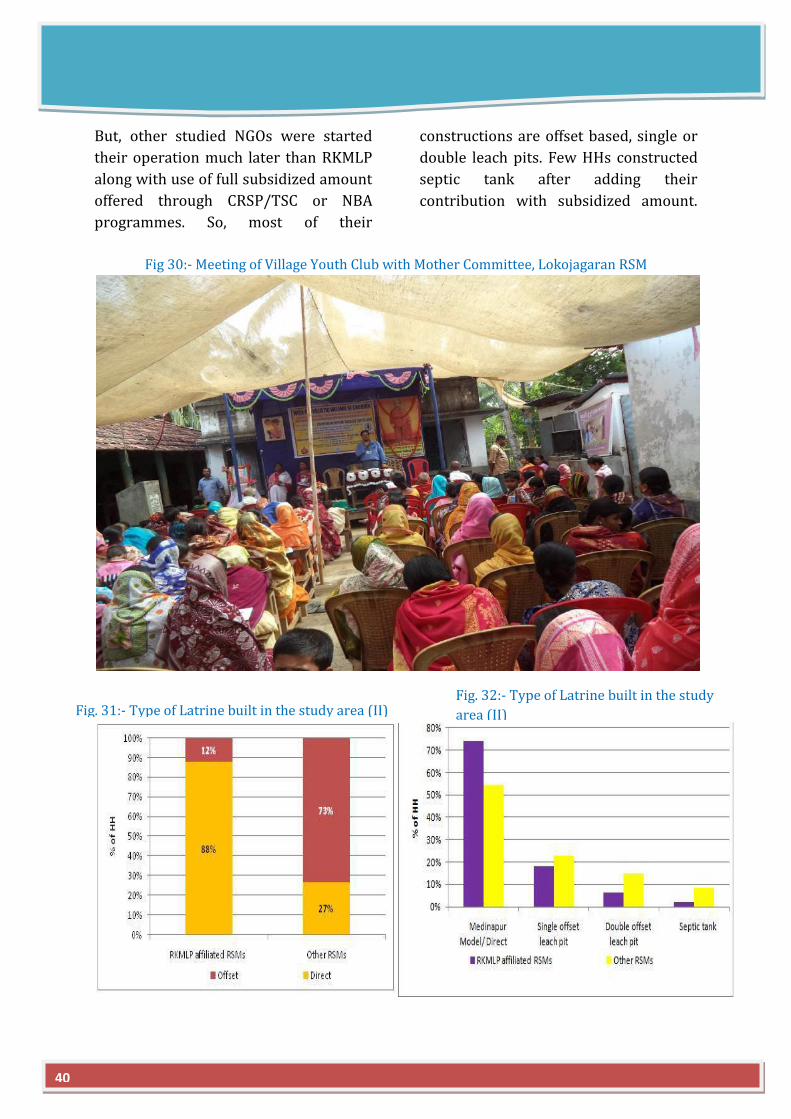
But, other studied NGOs were started
their operation much later than RKMLP
along with use of full subsidized amount
offered through CRSP/TSC or NBA
programmes. So, most of their
constructions are offset based, single or
double leach pits. Few HHs constructed
septic tank after adding their
contribution with subsidized amount.
Fig 30:- Meeting of Village Youth Club with Mother Committee, Lokojagaran RSM
40
Fig. 32:- Type of Latrine built in the study
area (II)
Fig. 31:- Type of Latrine built in the study area (II)
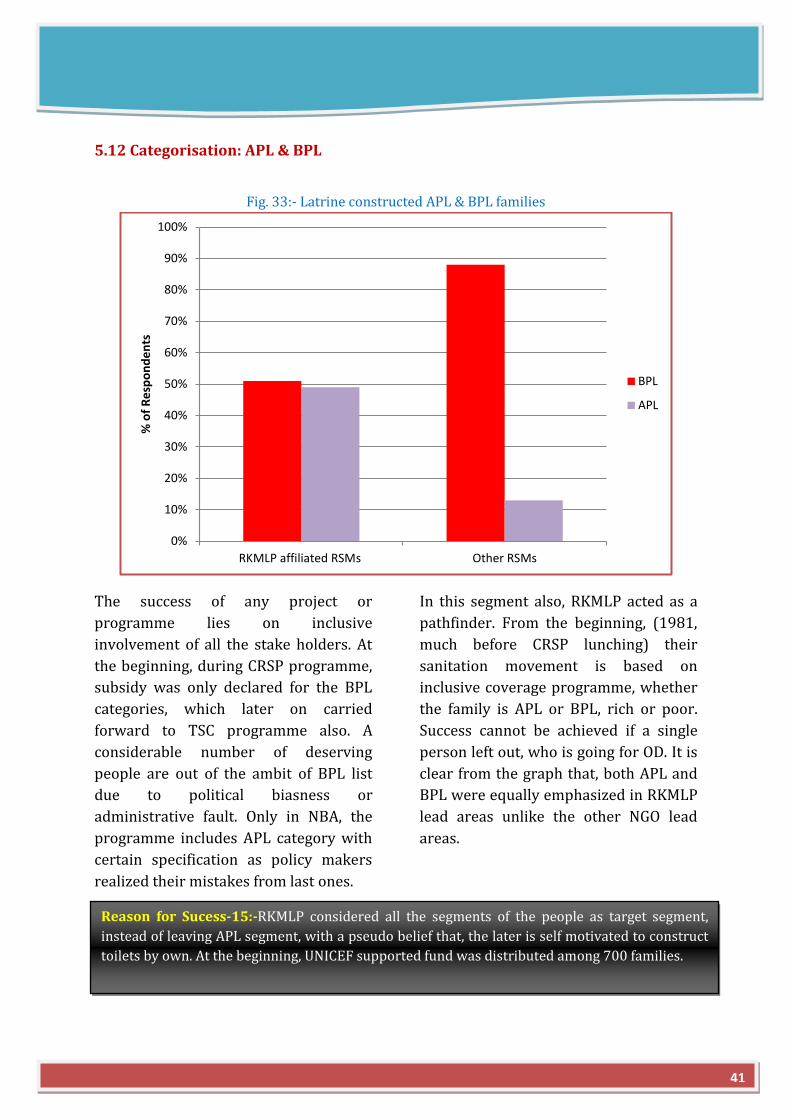
5.12 Categorisation: APL & BPL
Fig. 33:- Latrine constructed APL & BPL families
The success of any project or
programme lies on inclusive
involvement of all the stake holders. At
the beginning, during CRSP programme,
subsidy was only declared for the BPL
categories, which later on carried
forward to TSC programme also. A
considerable number of deserving
people are out of the ambit of BPL list
due to political biasness or
administrative fault. Only in NBA, the
programme includes APL category with
certain specification as policy makers
realized their mistakes from last ones.
In this segment also, RKMLP acted as a
pathfinder. From the beginning, (1981,
much before CRSP lunching) their
sanitation movement is based on
inclusive coverage programme, whether
the family is APL or BPL, rich or poor.
Success cannot be achieved if a single
person left out, who is going for OD. It is
clear from the graph that, both APL and
BPL were equally emphasized in RKMLP
lead areas unlike the other NGO lead
areas.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
RKMLP affiliated RSMs Other RSMs
% o
f R
esp
on
de
nts
BPL
APL
Reason for Sucess-15:-RKMLP considered all the segments of the people as target segment,
instead of leaving APL segment, with a pseudo belief that, the later is self motivated to construct
toilets by own. At the beginning, UNICEF supported fund was distributed among 700 families.
41
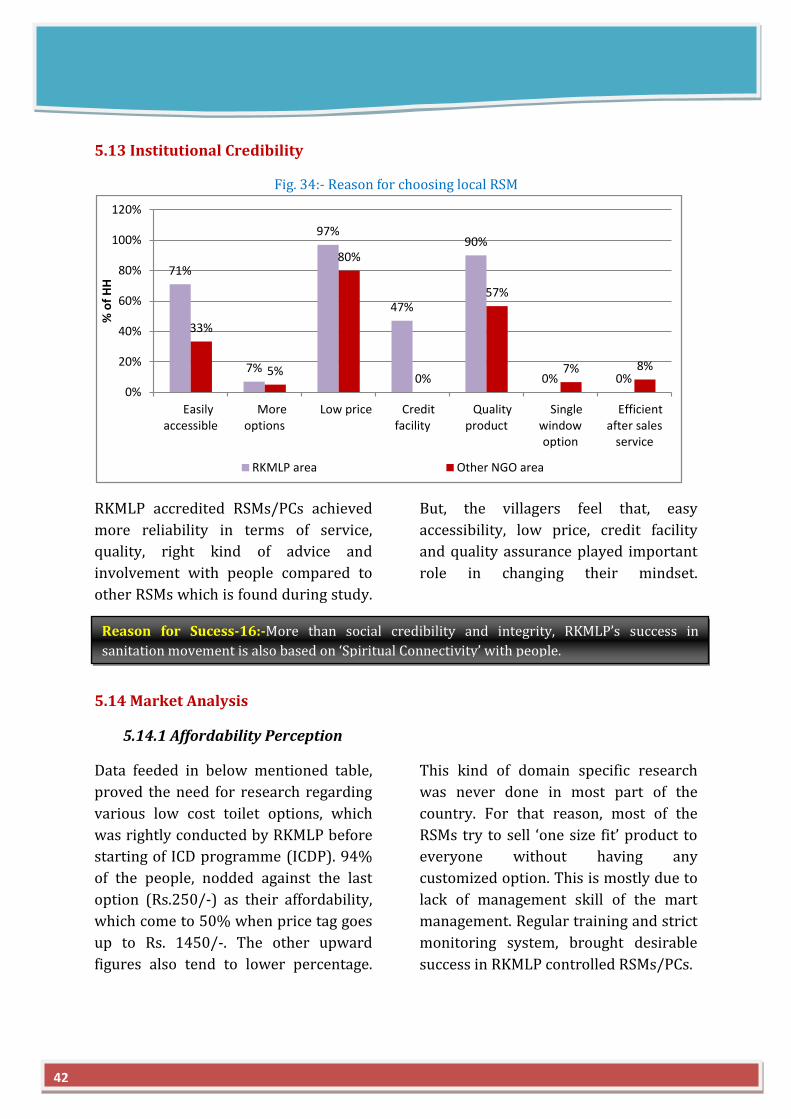
5.13 Institutional Credibility
Fig. 34:- Reason for choosing local RSM
RKMLP accredited RSMs/PCs achieved
more reliability in terms of service,
quality, right kind of advice and
involvement with people compared to
other RSMs which is found during study.
But, the villagers feel that, easy
accessibility, low price, credit facility
and quality assurance played important
role in changing their mindset.
5.14 Market Analysis
5.14.1 Affordability Perception
Data feeded in below mentioned table,
proved the need for research regarding
various low cost toilet options, which
was rightly conducted by RKMLP before
starting of ICD programme (ICDP). 94%
of the people, nodded against the last
option (Rs.250/-) as their affordability,
which come to 50% when price tag goes
up to Rs. 1450/-. The other upward
figures also tend to lower percentage.
This kind of domain specific research
was never done in most part of the
country. For that reason, most of the
RSMs try to sell ‘one size fit’ product to
everyone without having any
customized option. This is mostly due to
lack of management skill of the mart
management. Regular training and strict
monitoring system, brought desirable
success in RKMLP controlled RSMs/PCs.
71%
7%
97%
47%
90%
0% 0%
33%
5%
80%
0%
57%
7% 8%
0%
20%
40%
60%
80%
100%
120%
Easilyaccessible
Moreoptions
Low price Creditfacility
Qualityproduct
Singlewindowoption
Efficientafter sales
service
% o
f H
H
RKMLP area Other NGO area
Reason for Sucess-16:-More than social credibility and integrity, RKMLP’s success in
sanitation movement is also based on ‘Spiritual Connectivity’ with people.
42
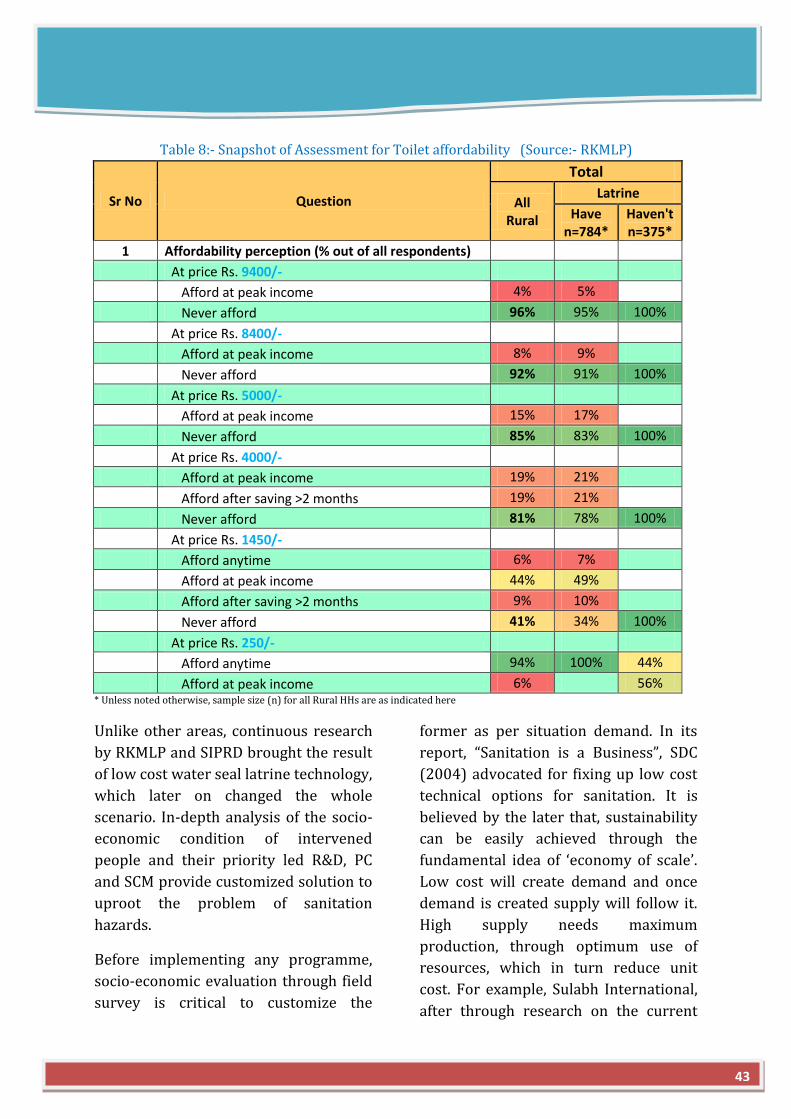
Table 8:- Snapshot of Assessment for Toilet affordability (Source:- RKMLP)
Sr No Question
Total
All Rural
Latrine
Have n=784*
Haven't n=375*
1 Affordability perception (% out of all respondents)
At price Rs. 9400/-
Afford at peak income 4% 5%
Never afford 96% 95% 100%
At price Rs. 8400/-
Afford at peak income 8% 9%
Never afford 92% 91% 100%
At price Rs. 5000/-
Afford at peak income 15% 17%
Never afford 85% 83% 100%
At price Rs. 4000/-
Afford at peak income 19% 21%
Afford after saving >2 months 19% 21%
Never afford 81% 78% 100%
At price Rs. 1450/-
Afford anytime 6% 7%
Afford at peak income 44% 49%
Afford after saving >2 months 9% 10%
Never afford 41% 34% 100%
At price Rs. 250/-
Afford anytime 94% 100% 44%
Afford at peak income 6% 56% * Unless noted otherwise, sample size (n) for all Rural HHs are as indicated here
Unlike other areas, continuous research
by RKMLP and SIPRD brought the result
of low cost water seal latrine technology,
which later on changed the whole
scenario. In-depth analysis of the socio-
economic condition of intervened
people and their priority led R&D, PC
and SCM provide customized solution to
uproot the problem of sanitation
hazards.
Before implementing any programme,
socio-economic evaluation through field
survey is critical to customize the
former as per situation demand. In its
report, “Sanitation is a Business”, SDC
(2004) advocated for fixing up low cost
technical options for sanitation. It is
believed by the later that, sustainability
can be easily achieved through the
fundamental idea of ‘economy of scale’.
Low cost will create demand and once
demand is created supply will follow it.
High supply needs maximum
production, through optimum use of
resources, which in turn reduce unit
cost. For example, Sulabh International,
after through research on the current
43
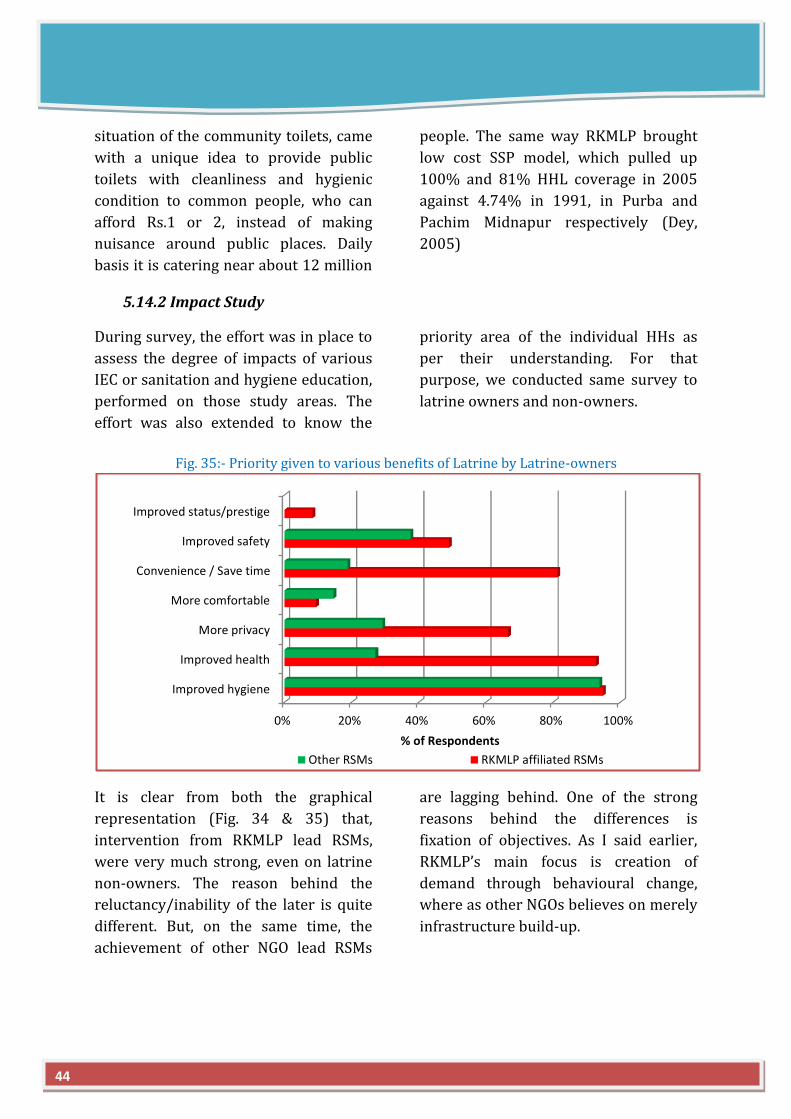
situation of the community toilets, came
with a unique idea to provide public
toilets with cleanliness and hygienic
condition to common people, who can
afford Rs.1 or 2, instead of making
nuisance around public places. Daily
basis it is catering near about 12 million
people. The same way RKMLP brought
low cost SSP model, which pulled up
100% and 81% HHL coverage in 2005
against 4.74% in 1991, in Purba and
Pachim Midnapur respectively (Dey,
2005)
5.14.2 Impact Study
During survey, the effort was in place to
assess the degree of impacts of various
IEC or sanitation and hygiene education,
performed on those study areas. The
effort was also extended to know the
priority area of the individual HHs as
per their understanding. For that
purpose, we conducted same survey to
latrine owners and non-owners.
Fig. 35:- Priority given to various benefits of Latrine by Latrine-owners
It is clear from both the graphical
representation (Fig. 34 & 35) that,
intervention from RKMLP lead RSMs,
were very much strong, even on latrine
non-owners. The reason behind the
reluctancy/inability of the later is quite
different. But, on the same time, the
achievement of other NGO lead RSMs
are lagging behind. One of the strong
reasons behind the differences is
fixation of objectives. As I said earlier,
RKMLP’s main focus is creation of
demand through behavioural change,
where as other NGOs believes on merely
infrastructure build-up.
0% 20% 40% 60% 80% 100%
Improved hygiene
Improved health
More privacy
More comfortable
Convenience / Save time
Improved safety
Improved status/prestige
% of Respondents
Other RSMs RKMLP affiliated RSMs
44
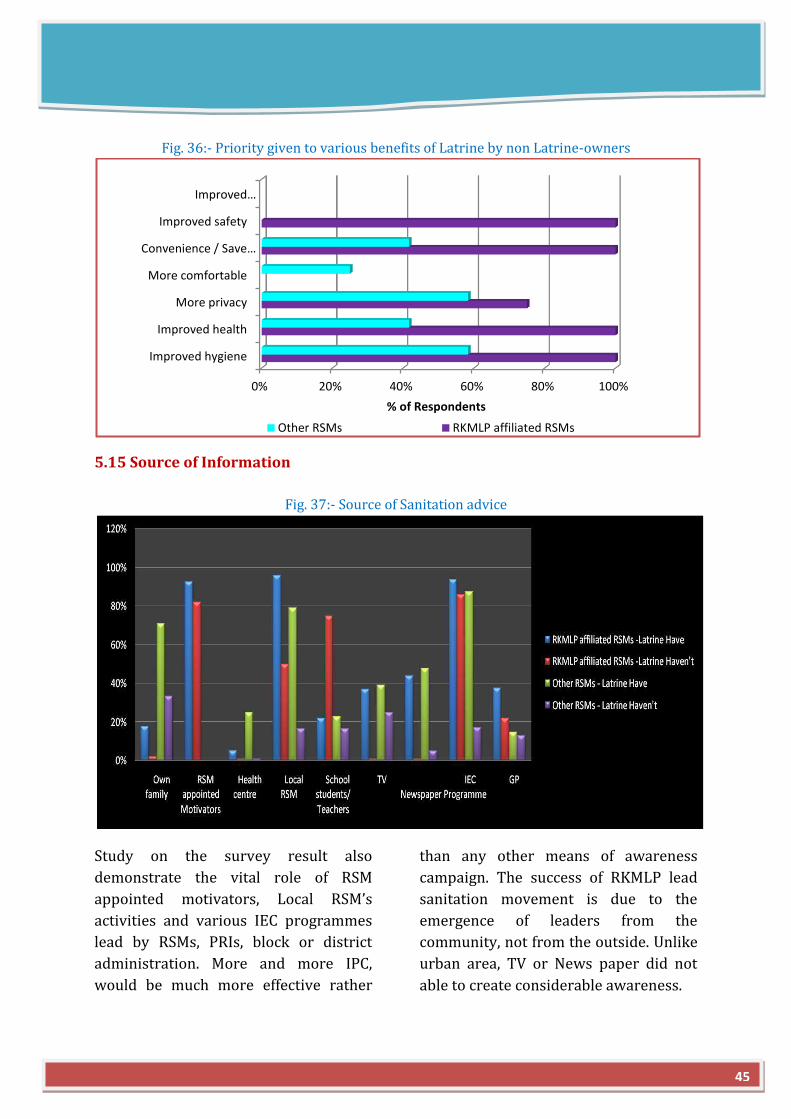
Fig. 36:- Priority given to various benefits of Latrine by non Latrine-owners
5.15 Source of Information
Fig. 37:- Source of Sanitation advice
Study on the survey result also
demonstrate the vital role of RSM
appointed motivators, Local RSM’s
activities and various IEC programmes
lead by RSMs, PRIs, block or district
administration. More and more IPC,
would be much more effective rather
than any other means of awareness
campaign. The success of RKMLP lead
sanitation movement is due to the
emergence of leaders from the
community, not from the outside. Unlike
urban area, TV or News paper did not
able to create considerable awareness.
0% 20% 40% 60% 80% 100%
Improved hygiene
Improved health
More privacy
More comfortable
Convenience / Save…
Improved safety
Improved…
% of Respondents
Other RSMs RKMLP affiliated RSMs
45
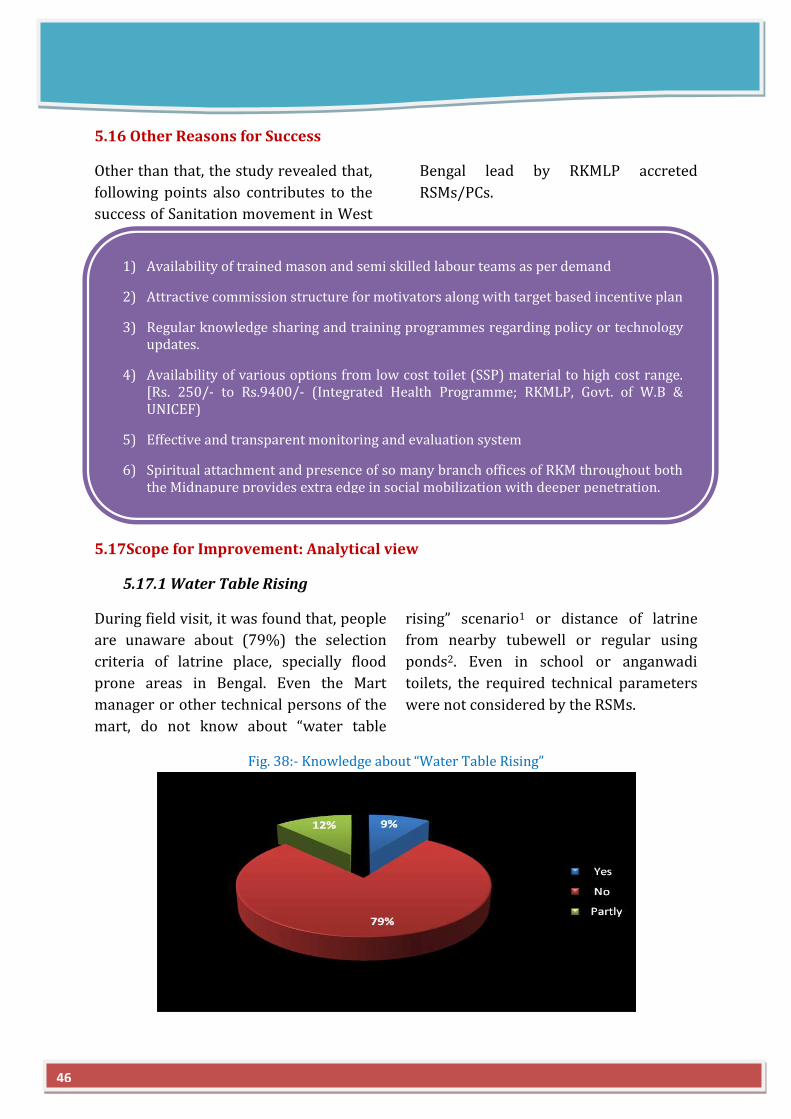
5.16 Other Reasons for Success
Other than that, the study revealed that,
following points also contributes to the
success of Sanitation movement in West
Bengal lead by RKMLP accreted
RSMs/PCs.
5.17Scope for Improvement: Analytical view
5.17.1 Water Table Rising
During field visit, it was found that, people
are unaware about (79%) the selection
criteria of latrine place, specially flood
prone areas in Bengal. Even the Mart
manager or other technical persons of the
mart, do not know about “water table
rising” scenario1 or distance of latrine
from nearby tubewell or regular using
ponds2. Even in school or anganwadi
toilets, the required technical parameters
were not considered by the RSMs.
Fig. 38:- Knowledge about “Water Table Rising”
1) Availability of trained mason and semi skilled labour teams as per demand
2) Attractive commission structure for motivators along with target based incentive plan
3) Regular knowledge sharing and training programmes regarding policy or technology updates.
4) Availability of various options from low cost toilet (SSP) material to high cost range. [Rs. 250/- to Rs.9400/- (Integrated Health Programme; RKMLP, Govt. of W.B & UNICEF)
5) Effective and transparent monitoring and evaluation system
6) Spiritual attachment and presence of so many branch offices of RKM throughout both the Midnapure provides extra edge in social mobilization with deeper penetration.
46
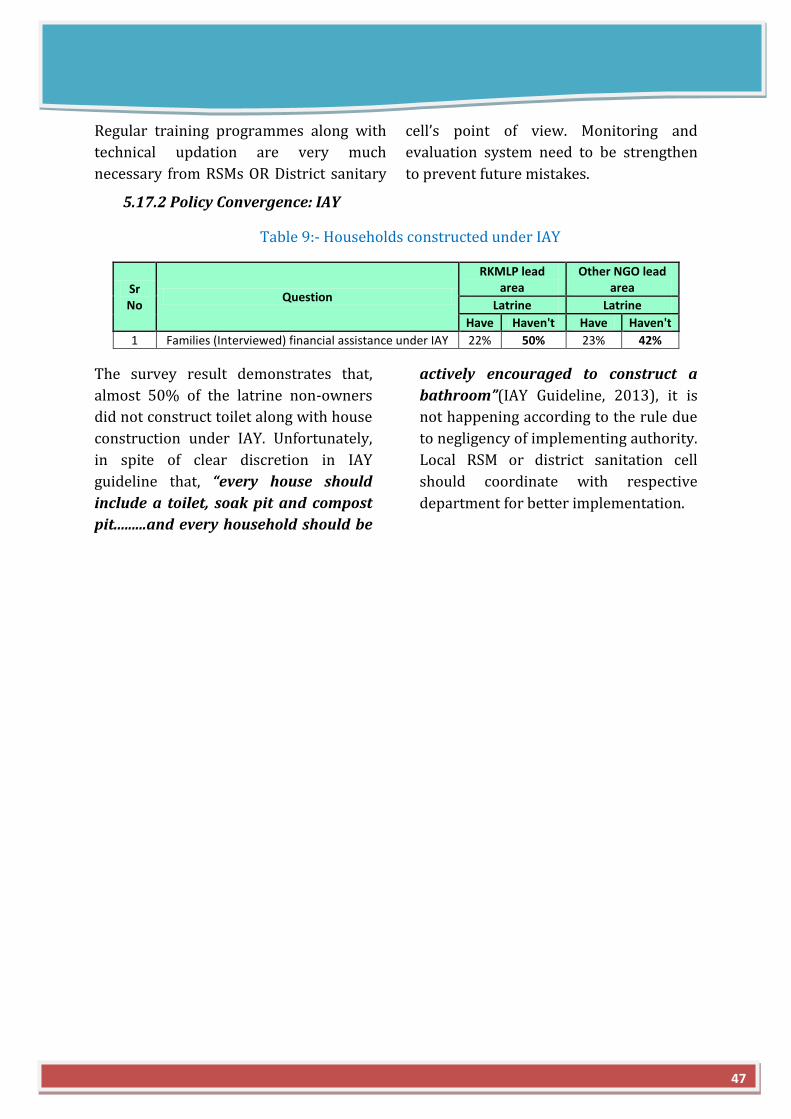
Regular training programmes along with
technical updation are very much
necessary from RSMs OR District sanitary
cell’s point of view. Monitoring and
evaluation system need to be strengthen
to prevent future mistakes.
5.17.2 Policy Convergence: IAY
Table 9:- Households constructed under IAY
Sr No
Question
RKMLP lead area
Other NGO lead area
Latrine Latrine
Have Haven't Have Haven't
1 Families (Interviewed) financial assistance under IAY 22% 50% 23% 42%
The survey result demonstrates that,
almost 50% of the latrine non-owners
did not construct toilet along with house
construction under IAY. Unfortunately,
in spite of clear discretion in IAY
guideline that, “every house should
include a toilet, soak pit and compost
pit.........and every household should be
actively encouraged to construct a
bathroom”(IAY Guideline, 2013), it is
not happening according to the rule due
to negligency of implementing authority.
Local RSM or district sanitation cell
should coordinate with respective
department for better implementation.
47
RECOMMENDATION AND CONCLUSION
The study was conducted mainly for two reasons,
Merely constructing infrastructure will
not serve the purpose. Without proper
motivational technique, persistency of
behavioural change is questionable.
Flexibility in terms of organisational
structure and management system, need
to be allowed as per the region specific
socio-economic condition of target
groups, instead of sticking to the line by
line policy guidelines. The spirit of the
law or policy needs to be maintained for
a uniform, transparent execution and
monitoring & evaluation system. It is
good to see the changes are taking place
gradually through the good practices of
successful RSMs through various
private-public partnership. Now, it is not
only just a issue but a burning issue even
in socio-political arena, where it is also
put in the same line with Roti(food),
Kapradh(apparel) and Makan(house).
The situation has aroused to say that,
“Pahale Souchalaya, Fir Devalaya
(Presence of Toilet even come first then
Worship place)
To bring the sustainability in RSMs
operation is a vital and inevitable need
to meet the MDG, set up by UN body. For
this purpose, following
recommendations are made.
1)
48
I. To do comparative study between operational procedure of RKMLP and other failed RSMs/PCs in most of the part of our country and
II. To find out the contributing factors for achieving sustainability of RSM
1) Highlight or award all those successful RSM or PC centres which consistently performing well, adding value into the system (like NGP)
2) Ensure active participation of RSMs in design or suggesting IEC activities along with allocation of funds for said purpose to RSMs. The controlling power should not be in one hand (decentralisation), otherwise the fund will be misused (observed few instances during Purba Midnapur vist)
3) It is good to involve local people in mobilization processes, rather than efforts from outsider. (Hardly people knew, that Vidya Bhalan is promoting NBA programme!)
4) All the RSMs should build professional attitude and work culture to deal with such kind of critical issues. Regular intensive training programme needs to be arranged (may be by the help of renowned institute having expertise in Rural development and Rural marketing) to upgrade skills of functionaries.
5) Research on customized solutions need to be encouraged to explore new technical options which are affordable by the common people.

After conducting the study and pen
down the work on paper for analytical
purpose, it is evident that Rural Sanitary
Mart is a critical junction point in supply
chain system of sanitation. The success
of any programme (ISP, CRSP, TSC or
NBA) is directly proportional to the
organisational set up of the RSM along
with its involvement in grass root level.
The inferences came through the
comparative study among the RSMs,
managed by different stakeholders. It is
just a chain reaction. Effective
mobilization process creates demand
vacuum, which need to be filled up by
efficient supply chain (RSM/PC) on
immediate manner. This will provide
RSMs to build up rapport with target
consumers for future up-gradation or
selling of other products (low cost water
purifier, smokeless chulla, solar lantern),
which in turn ensure sustainability of
the enterprise. The study tried to
diagnose the problem associated with
the non-functionality of RSM and
recommended possible remedies.
“A sense of national or social sanitation is not a virtue among us. We may take kind of bath,
but we don’t mind dirtying the well or the tank or the river by whose side or in which we
perform ablutions. I regard this defect as a great vice which is responsible for the
disgraceful state of our villages and the sacred banks of the sacred rivers and for the
disease that spring from insanitation”
-Gandhi (1947)
6) More focus on effective Sanitation & Hygiene education rather than infrastructure.
7) The focus has to shift from ‘Subsidy driven’ to ‘Demand driven’ mode
8) RSM should be located at a central point of the block (or cluster of blocks), which can ensure accessibility to all the targeted communities.
9) RSMs should be supported by sufficient financial allocation right at beginning and even during the course of its existence. Banks can provide loans to RSMs under SME unit.
10) State and Central Govt. should offer sales tax exemption along with provision like free electricity for certain period, leasing of waste land to RSMs for Production centre.
49
REFERENCES
B. B. Samanta, 2009. STUDY OF SUPPLY CHAIN SYSTEM IN TSC ORISSA CASE STUDY
REPORT
Chandi Charan Dey, 2010.Production Centers cum Rural Sanitary Marts: An alternate
delivery mechanism for sanitation promotion in West Bengal
CMS, 2011. Assessment Study of Impact and Sustainability of Nirmal Gram Puraskar
Jacqueline Devine and Craig Kullmann, 2011. Introductory Guide to Sanitation
Marketing. pp. 6-10
IDE, 2011.Easy Shower Latrine, Technical Handbook
India Together, [viewed on 24.10.2013].
file:///D:/Sanitation%20Marketing/Success%20in%20rural%20sanitation%20-
%20July%202003%20-%20India%20Together.htm
Indira Khurana and Richard Mahapatra, 2009.Right to Water and Sanitation
Kamal Kar & Robert Chember, 2008. Handbook on Community-Led Total Sanitation
K. K. Jadeja, 2009.Study of supply chain management under Total Sanitation Project in
Gujarat
Kumar Alok, 2010. Squatting with Dignity: Lessons from India
Kumar Alok & Sumita Ganguly, 2007. Rural Sanitary Marts: Developing a sustainable
alternate delivery mechanism for sanitation in West Bengal
Leonie Kappauf, 2011. Opportunities and Constraints for more Sustainable Sanitation
through Sanitation Marketing in Malawi, 2011. pp. 21-27
Michael Roberts, M.S. and Anthea Long, 2007. Demand Assessment for Sanitary
Latrines in Rural and Urban Areas of Cambodia
Michael Roberts, Aaron Tanner, and Andrew McNaughton, 2007.Supply Chain
Assessment for Sanitary Latrines in Rural and Peri-Urban Areas of Cambodia
Ministry of Rural Development, GoI, 2013. INDIRA AWAAS YOJANA. pp. 5-7
Nilaya Deep, 2007. Total Sanitation Campaign in West Bengal A Study of the Supply
Chain Mechanism
Shri P K Chakraborty, 2009. STUDY OF SUPPLY CHAIN IN TSC MAHARASHTRA CASE
STUDY
50

S. K. Chattopadhyay, 2008. STUDY OF SUPPLY CHAIN SYSTEM IN TSCUTTAR PRADESH
CASE STUDY REPORT
Solution Exchange-Water Community, 2007. Making Rural Sanitary Marts viable and
more effective – Experiences, Examples.
Solution Exchange-Water Community, 2008. Strategy for Scaling Up Rural Sanitation
Coverage
SNV & IRC Report, 2012.Rural Sanitation Supply Chains and Finance
S. R. Mendiratta, 2000. Sanitation Promotion through Rural Sanitary Mart. pp. 156-157
Swami Asaktananda and Chandi Charan Dey, 2005. Sanitation is a Movement :
Ramakrishna Mission Lokasiksha Parishad’s Experiences
UNICEF, 2004. Rural Sanitary Marts and Production Centres – An Evaluation
UNICEF, 2007. Technology options for HOUSEHOLD SANITATION. pp. 6-23
UNICEF, 2011. Water, Sanitation and Hygiene Annual Report 2011.pp. 43-46
WaterAid, 2000. Marketing Sanitation in Rural India
Water SHED,2010.WASH Marketing ProjectKampong Speu Baseline Survey
WSP, 2004.Sanitation is a business: Approaches for demand-oriented policies
WSP, 2009. Learning at Scale: Total Sanitation and Sanitation Marketing Project. pp. 5-8,
10
WSP, 2010. From Dreams to Reality: Compendium of Best Practices in Rural Sanitation in
India. pp. 19-25
WSP, 2010. THE ECONOMIC IMPACTS OF INADEQUATE SANITATION IN INDIA
WSP, 2012. Sanitation Marketing Lessons from Cambodia: A Market-Based Approachto
Delivering Sanitation
51
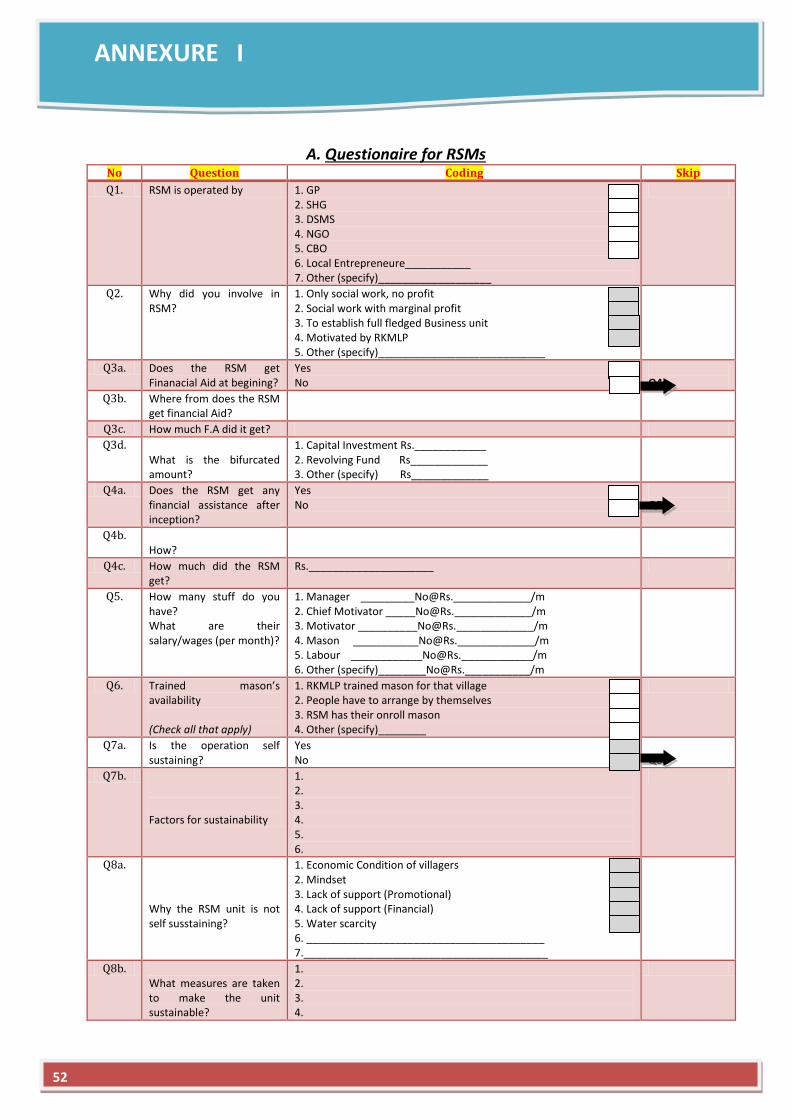
ANNEXURE I
A. Questionaire for RSMs No Question Coding Skip
Q1. RSM is operated by 1. GP 2. SHG 3. DSMS 4. NGO 5. CBO 6. Local Entrepreneure___________ 7. Other (specify)___________________
Q2. Why did you involve in RSM?
1. Only social work, no profit 2. Social work with marginal profit 3. To establish full fledged Business unit 4. Motivated by RKMLP 5. Other (specify)____________________________
Q3a. Does the RSM get Finanacial Aid at begining?
Yes No
Q4a.
Q3b. Where from does the RSM get financial Aid?
Q3c. How much F.A did it get?
Q3d. What is the bifurcated amount?
1. Capital Investment Rs.____________ 2. Revolving Fund Rs_____________ 3. Other (specify) Rs_____________
Q4a. Does the RSM get any financial assistance after inception?
Yes No
Q5.
Q4b. How?
Q4c. How much did the RSM get?
Rs._____________________
Q5. How many stuff do you have? What are their salary/wages (per month)?
1. Manager _________No@Rs._____________/m 2. Chief Motivator _____No@Rs._____________/m 3. Motivator __________No@Rs._____________/m 4. Mason ___________No@Rs._____________/m 5. Labour ____________No@Rs.____________/m 6. Other (specify)________No@Rs.___________/m
Q6. Trained mason’s availability (Check all that apply)
1. RKMLP trained mason for that village 2. People have to arrange by themselves 3. RSM has their onroll mason 4. Other (specify)________
Q7a. Is the operation self sustaining?
Yes No
Q8a
Q7b. Factors for sustainability
1. 2. 3. 4. 5. 6.
Q8a. Why the RSM unit is not self susstaining?
1. Economic Condition of villagers 2. Mindset 3. Lack of support (Promotional) 4. Lack of support (Financial) 5. Water scarcity 6. ________________________________________ 7._________________________________________
Q8b. What measures are taken to make the unit sustainable?
1. 2. 3. 4.
52
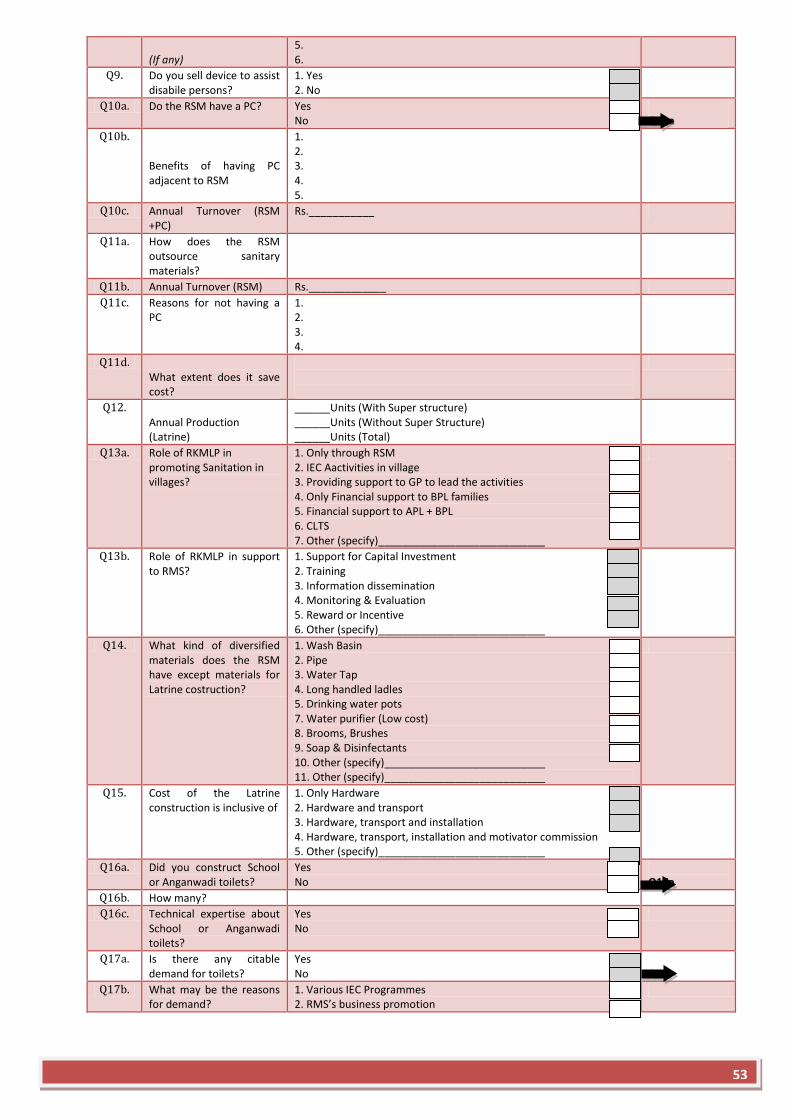
(If any)
5. 6.
Q9. Do you sell device to assist disabile persons?
1. Yes 2. No
Q10a. Do the RSM have a PC? Yes No
Q11a
Q10b. Benefits of having PC adjacent to RSM
1. 2. 3. 4. 5.
Q10c. Annual Turnover (RSM +PC)
Rs.___________
Q11a. How does the RSM outsource sanitary materials?
Q11b. Annual Turnover (RSM) Rs._____________
Q11c. Reasons for not having a PC
1. 2. 3. 4.
Q11d. What extent does it save cost?
Q12. Annual Production (Latrine)
______Units (With Super structure) ______Units (Without Super Structure) ______Units (Total)
Q13a. Role of RKMLP in promoting Sanitation in villages?
1. Only through RSM 2. IEC Aactivities in village 3. Providing support to GP to lead the activities 4. Only Financial support to BPL families 5. Financial support to APL + BPL 6. CLTS 7. Other (specify)____________________________
Q13b. Role of RKMLP in support to RMS?
1. Support for Capital Investment 2. Training 3. Information dissemination 4. Monitoring & Evaluation 5. Reward or Incentive 6. Other (specify)____________________________
Q14. What kind of diversified materials does the RSM have except materials for Latrine costruction?
1. Wash Basin 2. Pipe 3. Water Tap 4. Long handled ladles 5. Drinking water pots 7. Water purifier (Low cost) 8. Brooms, Brushes 9. Soap & Disinfectants 10. Other (specify)___________________________ 11. Other (specify)___________________________
Q15. Cost of the Latrine construction is inclusive of
1. Only Hardware 2. Hardware and transport 3. Hardware, transport and installation 4. Hardware, transport, installation and motivator commission 5. Other (specify)____________________________
Q16a. Did you construct School or Anganwadi toilets?
Yes No
Q17a
Q16b. How many?
Q16c. Technical expertise about School or Anganwadi toilets?
Yes No
Q17a. Is there any citable demand for toilets?
Yes No
Q18
Q17b. What may be the reasons for demand?
1. Various IEC Programmes 2. RMS’s business promotion
53
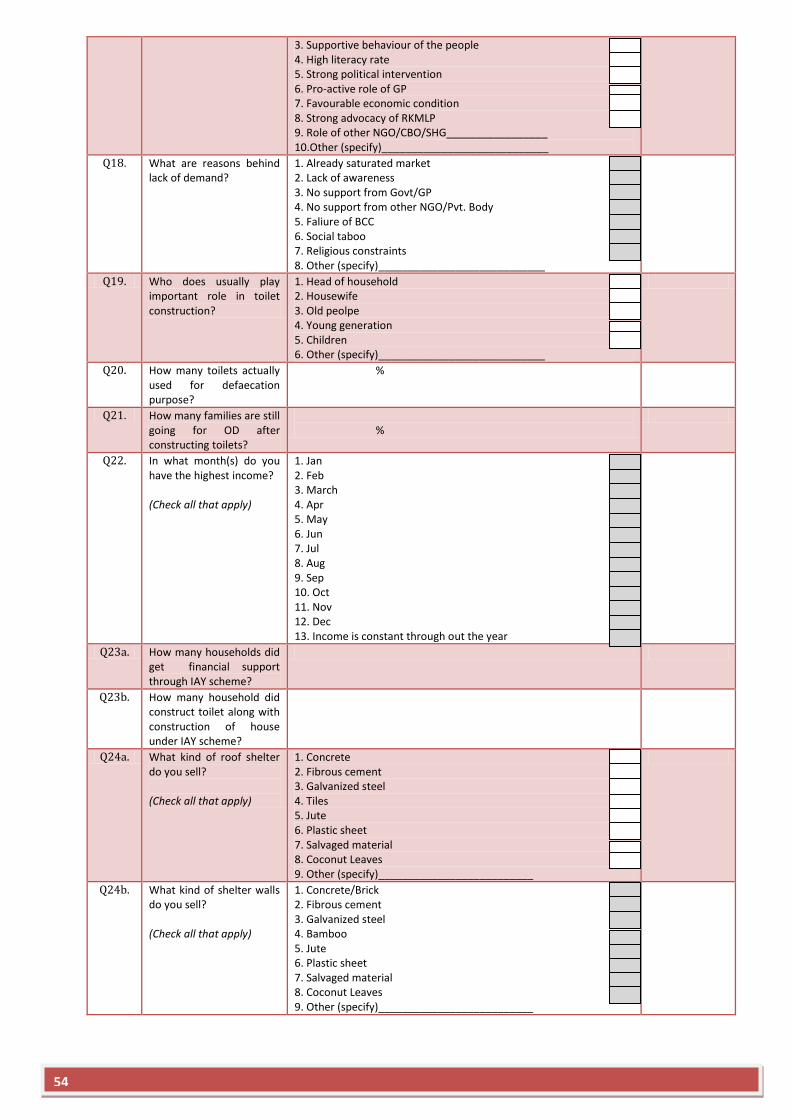
3. Supportive behaviour of the people 4. High literacy rate 5. Strong political intervention 6. Pro-active role of GP 7. Favourable economic condition 8. Strong advocacy of RKMLP 9. Role of other NGO/CBO/SHG_________________ 10.Other (specify)____________________________
Q18. What are reasons behind lack of demand?
1. Already saturated market 2. Lack of awareness 3. No support from Govt/GP 4. No support from other NGO/Pvt. Body 5. Faliure of BCC 6. Social taboo 7. Religious constraints 8. Other (specify)____________________________
Q19. Who does usually play important role in toilet construction?
1. Head of household 2. Housewife 3. Old peolpe 4. Young generation 5. Children 6. Other (specify)____________________________
Q20. How many toilets actually used for defaecation purpose?
%
Q21. How many families are still going for OD after constructing toilets?
%
Q22. In what month(s) do you have the highest income? (Check all that apply)
1. Jan 2. Feb 3. March 4. Apr 5. May 6. Jun 7. Jul 8. Aug 9. Sep 10. Oct 11. Nov 12. Dec 13. Income is constant through out the year
Q23a. How many households did get financial support through IAY scheme?
Q23b. How many household did construct toilet along with construction of house under IAY scheme?
Q24a. What kind of roof shelter do you sell? (Check all that apply)
1. Concrete 2. Fibrous cement 3. Galvanized steel 4. Tiles 5. Jute 6. Plastic sheet 7. Salvaged material 8. Coconut Leaves 9. Other (specify)__________________________
Q24b. What kind of shelter walls do you sell? (Check all that apply)
1. Concrete/Brick 2. Fibrous cement 3. Galvanized steel 4. Bamboo 5. Jute 6. Plastic sheet 7. Salvaged material 8. Coconut Leaves 9. Other (specify)__________________________
54

Q24c. What kind of slab do you sell? (Check all that apply)
1. Open hole-woden slab 2. Open hole –concrete slab 3. Pour flush 4. Western Toilet bowl 5. Other___________________________________
Other Comments:-
55
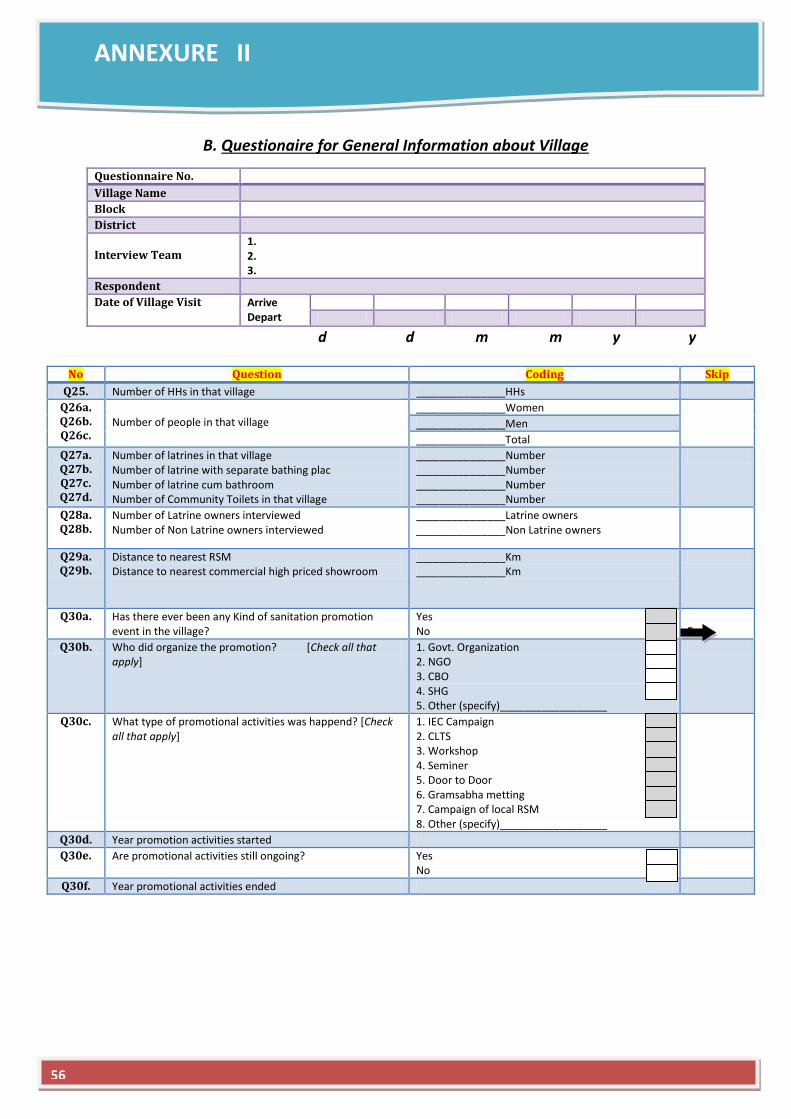
ANNEXURE II
B. Questionaire for General Information about Village
d d m m y y
No Question Coding Skip
Q25. Number of HHs in that village _______________HHs
Q26a. Q26b. Q26c.
Number of people in that village
_______________Women
_______________Men
_______________Total
Q27a. Q27b. Q27c. Q27d.
Number of latrines in that village Number of latrine with separate bathing plac Number of latrine cum bathroom Number of Community Toilets in that village
_______________Number _______________Number _______________Number _______________Number
Q28a. Q28b.
Number of Latrine owners interviewed Number of Non Latrine owners interviewed
_______________Latrine owners _______________Non Latrine owners
Q29a. Q29b.
Distance to nearest RSM Distance to nearest commercial high priced showroom
_______________Km _______________Km
Q30a. Has there ever been any Kind of sanitation promotion event in the village?
Yes No
End
Q30b. Who did organize the promotion? [Check all that apply]
1. Govt. Organization 2. NGO 3. CBO 4. SHG 5. Other (specify)__________________
Q30c. What type of promotional activities was happend? [Check all that apply]
1. IEC Campaign 2. CLTS 3. Workshop 4. Seminer 5. Door to Door 6. Gramsabha metting 7. Campaign of local RSM 8. Other (specify)__________________
Q30d. Year promotion activities started
Q30e. Are promotional activities still ongoing? Yes No
Q30f. Year promotional activities ended
Questionnaire No.
Village Name
Block
District
Interview Team
1. 2. 3.
Respondent
Date of Village Visit Arrive Depart
56
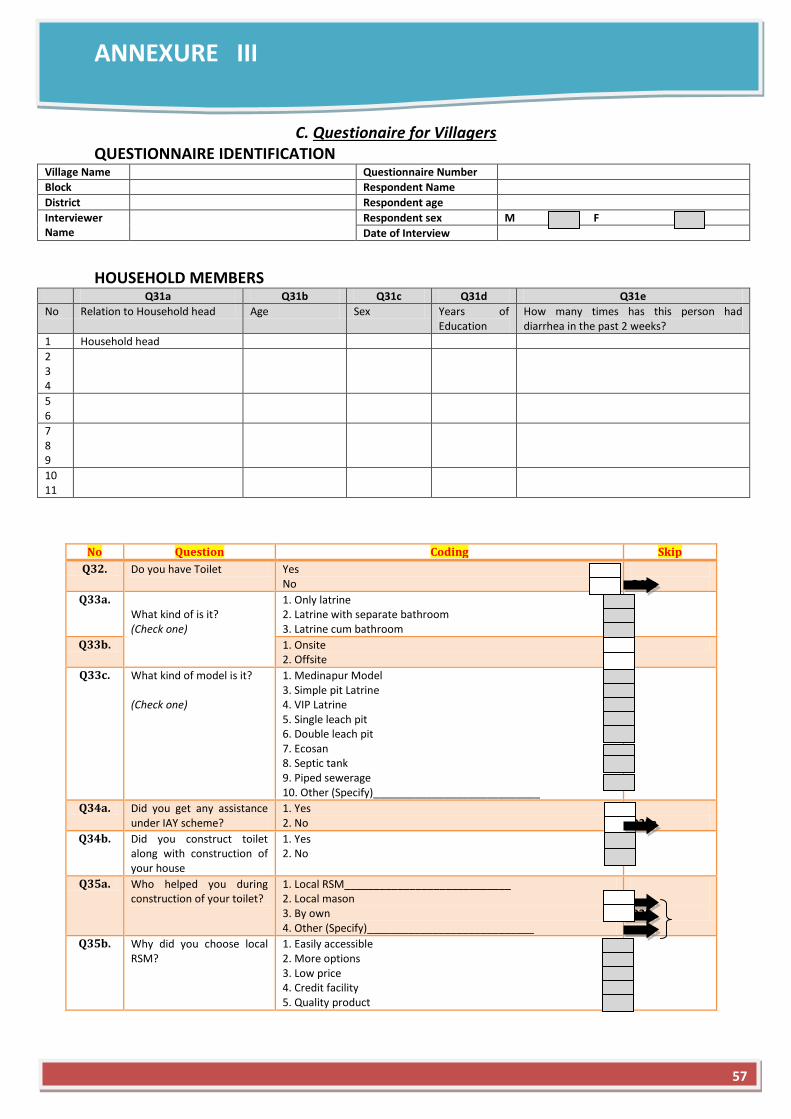
ANNEXURE III
C. Questionaire for Villagers QUESTIONNAIRE IDENTIFICATION
Village Name Questionnaire Number
Block Respondent Name
District Respondent age
Interviewer Name
Respondent sex M F
Date of Interview
HOUSEHOLD MEMBERS
Q31a Q31b Q31c Q31d Q31e
No Relation to Household head Age Sex Years of Education
How many times has this person had diarrhea in the past 2 weeks?
1 Household head
2 3 4
5 6
7 8 9
10 11
No Question Coding Skip
Q32. Do you have Toilet Yes No
Q43a
Q33a. What kind of is it? (Check one)
1. Only latrine 2. Latrine with separate bathroom 3. Latrine cum bathroom
Q33b. 1. Onsite 2. Offsite
Q33c. What kind of model is it? (Check one)
1. Medinapur Model 3. Simple pit Latrine 4. VIP Latrine 5. Single leach pit 6. Double leach pit 7. Ecosan 8. Septic tank 9. Piped sewerage 10. Other (Specify)____________________________
Q34a. Did you get any assistance under IAY scheme?
1. Yes 2. No
Q35a
Q34b. Did you construct toilet along with construction of your house
1. Yes 2. No
Q35a. Who helped you during construction of your toilet?
1. Local RSM____________________________ 2. Local mason 3. By own 4. Other (Specify)____________________________
Q36
Q35b. Why did you choose local RSM?
1. Easily accessible 2. More options 3. Low price 4. Credit facility 5. Quality product
57
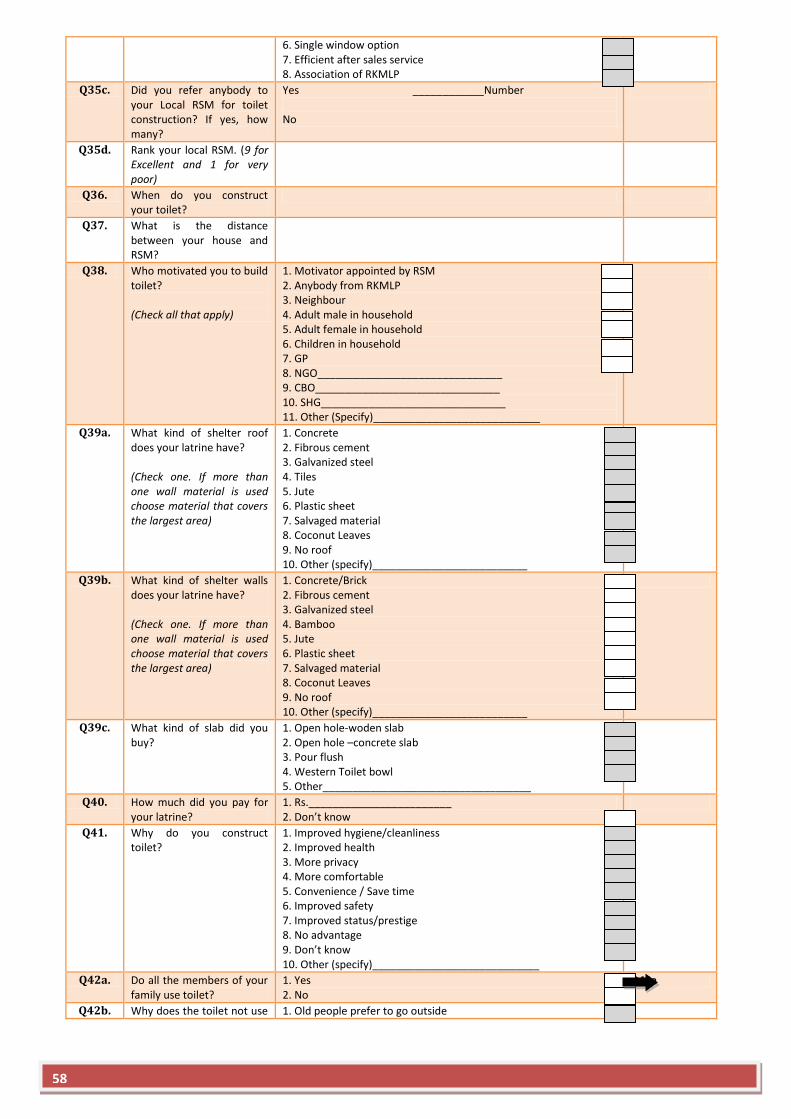
6. Single window option 7. Efficient after sales service 8. Association of RKMLP
Q35c. Did you refer anybody to your Local RSM for toilet construction? If yes, how many?
Yes ____________Number No
Q35d. Rank your local RSM. (9 for Excellent and 1 for very poor)
Q36. When do you construct your toilet?
Q37. What is the distance between your house and RSM?
Q38. Who motivated you to build toilet? (Check all that apply)
1. Motivator appointed by RSM 2. Anybody from RKMLP 3. Neighbour 4. Adult male in household 5. Adult female in household 6. Children in household 7. GP 8. NGO_______________________________ 9. CBO_______________________________ 10. SHG_______________________________ 11. Other (Specify)____________________________
Q39a. What kind of shelter roof does your latrine have? (Check one. If more than one wall material is used choose material that covers the largest area)
1. Concrete 2. Fibrous cement 3. Galvanized steel 4. Tiles 5. Jute 6. Plastic sheet 7. Salvaged material 8. Coconut Leaves 9. No roof 10. Other (specify)__________________________
Q39b. What kind of shelter walls does your latrine have? (Check one. If more than one wall material is used choose material that covers the largest area)
1. Concrete/Brick 2. Fibrous cement 3. Galvanized steel 4. Bamboo 5. Jute 6. Plastic sheet 7. Salvaged material 8. Coconut Leaves 9. No roof 10. Other (specify)__________________________
Q39c. What kind of slab did you buy?
1. Open hole-woden slab 2. Open hole –concrete slab 3. Pour flush 4. Western Toilet bowl 5. Other___________________________________
Q40. How much did you pay for your latrine?
1. Rs.________________________ 2. Don’t know
Q41. Why do you construct toilet?
1. Improved hygiene/cleanliness 2. Improved health 3. More privacy 4. More comfortable 5. Convenience / Save time 6. Improved safety 7. Improved status/prestige 8. No advantage 9. Don’t know 10. Other (specify)____________________________
Q42a. Do all the members of your family use toilet?
1. Yes 2. No
Q44a
Q42b. Why does the toilet not use 1. Old people prefer to go outside
58
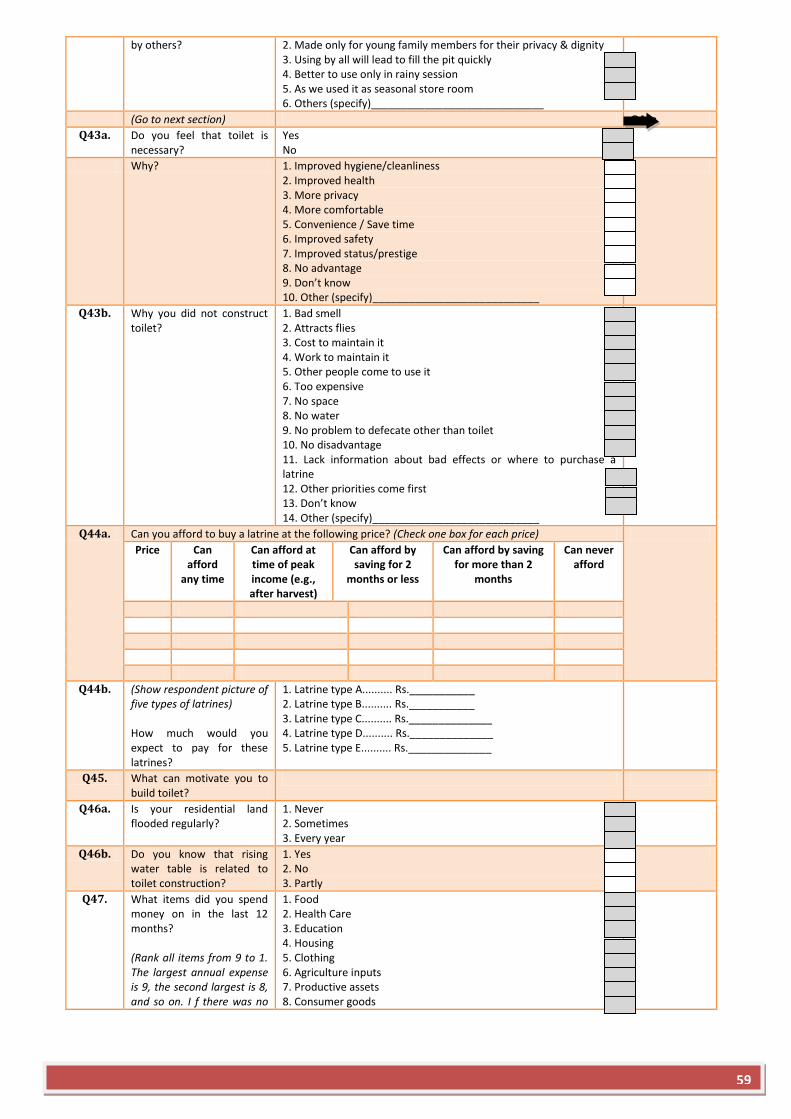
by others? 2. Made only for young family members for their privacy & dignity 3. Using by all will lead to fill the pit quickly 4. Better to use only in rainy session 5. As we used it as seasonal store room 6. Others (specify)_____________________________
(Go to next section) Q44a
Q43a. Do you feel that toilet is necessary?
Yes No
Why? 1. Improved hygiene/cleanliness 2. Improved health 3. More privacy 4. More comfortable 5. Convenience / Save time 6. Improved safety 7. Improved status/prestige 8. No advantage 9. Don’t know 10. Other (specify)____________________________
Q43b. Why you did not construct toilet?
1. Bad smell 2. Attracts flies 3. Cost to maintain it 4. Work to maintain it 5. Other people come to use it 6. Too expensive 7. No space 8. No water 9. No problem to defecate other than toilet 10. No disadvantage 11. Lack information about bad effects or where to purchase a latrine 12. Other priorities come first 13. Don’t know 14. Other (specify)____________________________
Q44a. Can you afford to buy a latrine at the following price? (Check one box for each price)
Price Can afford
any time
Can afford at time of peak income (e.g., after harvest)
Can afford by saving for 2
months or less
Can afford by saving for more than 2
months
Can never afford
Q44b. (Show respondent picture of five types of latrines) How much would you expect to pay for these latrines?
1. Latrine type A.......... Rs.___________ 2. Latrine type B.......... Rs.___________ 3. Latrine type C.......... Rs.______________ 4. Latrine type D.......... Rs.______________ 5. Latrine type E.......... Rs.______________
Q45. What can motivate you to build toilet?
Q46a. Is your residential land flooded regularly?
1. Never 2. Sometimes 3. Every year
Q46b. Do you know that rising water table is related to toilet construction?
1. Yes 2. No 3. Partly
Q47. What items did you spend money on in the last 12 months? (Rank all items from 9 to 1. The largest annual expense is 9, the second largest is 8, and so on. I f there was no
1. Food 2. Health Care 3. Education 4. Housing 5. Clothing 6. Agriculture inputs 7. Productive assets 8. Consumer goods
59
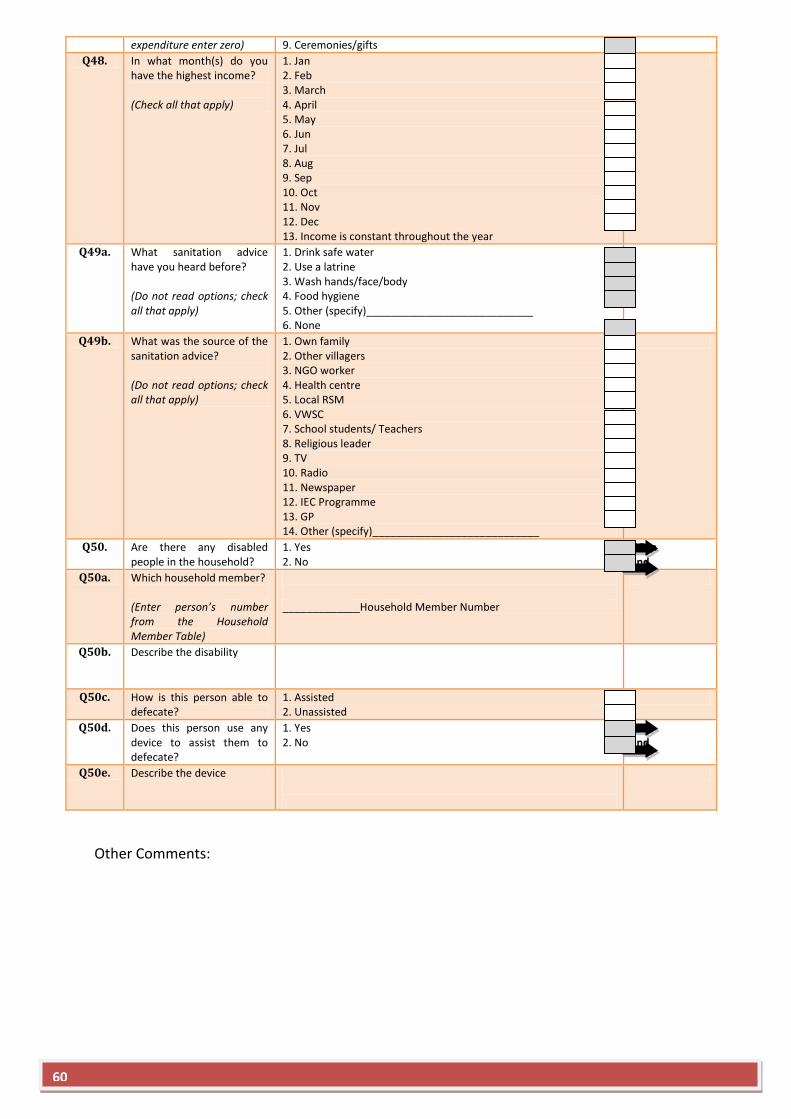
expenditure enter zero) 9. Ceremonies/gifts
Q48. In what month(s) do you have the highest income? (Check all that apply)
1. Jan 2. Feb 3. March 4. April 5. May 6. Jun 7. Jul 8. Aug 9. Sep 10. Oct 11. Nov 12. Dec 13. Income is constant throughout the year
Q49a. What sanitation advice have you heard before? (Do not read options; check all that apply)
1. Drink safe water 2. Use a latrine 3. Wash hands/face/body 4. Food hygiene 5. Other (specify)____________________________ 6. None
Q49b. What was the source of the sanitation advice? (Do not read options; check all that apply)
1. Own family 2. Other villagers 3. NGO worker 4. Health centre 5. Local RSM 6. VWSC 7. School students/ Teachers 8. Religious leader 9. TV 10. Radio 11. Newspaper 12. IEC Programme 13. GP 14. Other (specify)____________________________
Q50. Are there any disabled people in the household?
1. Yes 2. No
Q50a End
Q50a. Which household member? (Enter person’s number from the Household Member Table)
_____________Household Member Number
Q50b. Describe the disability
Q50c. How is this person able to defecate?
1. Assisted 2. Unassisted
Q50d. Does this person use any device to assist them to defecate?
1. Yes 2. No
Q50 End
Q50e. Describe the device
Other Comments:
60
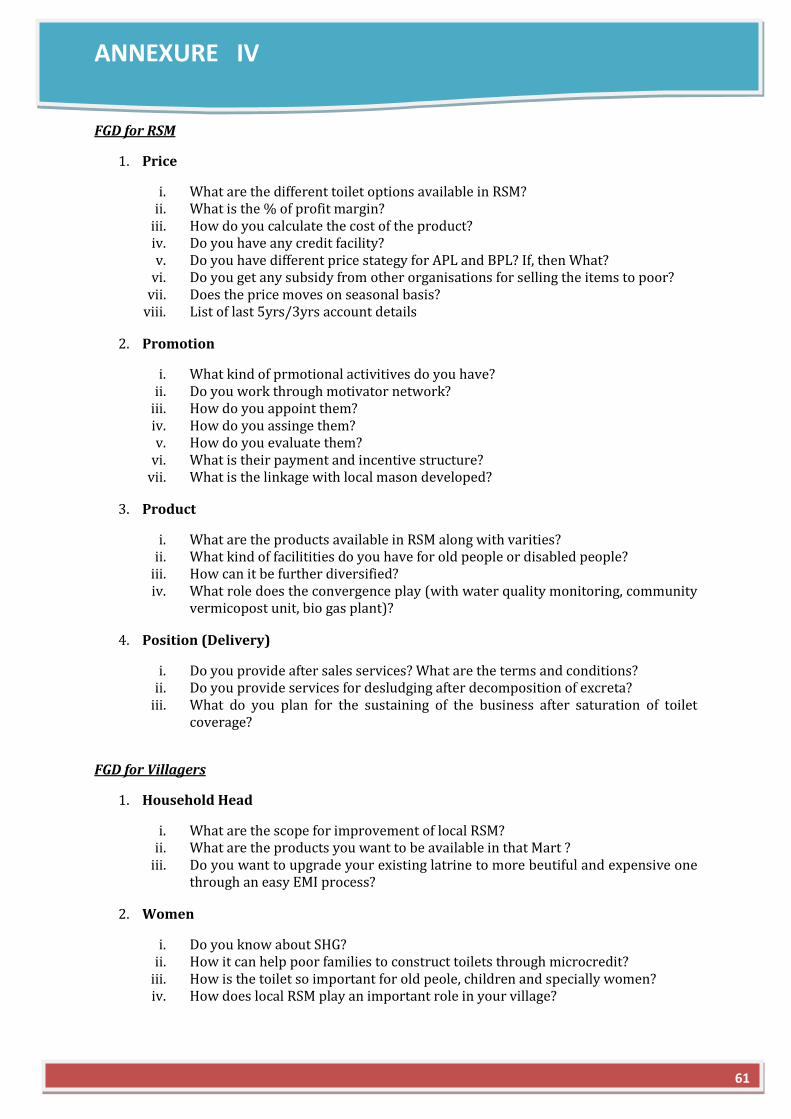
ANNEXURE IV
FGD for RSM
1. Price
i. What are the different toilet options available in RSM? ii. What is the % of profit margin?
iii. How do you calculate the cost of the product? iv. Do you have any credit facility? v. Do you have different price stategy for APL and BPL? If, then What?
vi. Do you get any subsidy from other organisations for selling the items to poor? vii. Does the price moves on seasonal basis?
viii. List of last 5yrs/3yrs account details
2. Promotion
i. What kind of prmotional activitives do you have? ii. Do you work through motivator network?
iii. How do you appoint them? iv. How do you assinge them? v. How do you evaluate them?
vi. What is their payment and incentive structure? vii. What is the linkage with local mason developed?
3. Product
i. What are the products available in RSM along with varities? ii. What kind of facilitities do you have for old people or disabled people?
iii. How can it be further diversified? iv. What role does the convergence play (with water quality monitoring, community
vermicopost unit, bio gas plant)?
4. Position (Delivery)
i. Do you provide after sales services? What are the terms and conditions? ii. Do you provide services for desludging after decomposition of excreta?
iii. What do you plan for the sustaining of the business after saturation of toilet coverage?
FGD for Villagers
1. Household Head
i. What are the scope for improvement of local RSM? ii. What are the products you want to be available in that Mart ?
iii. Do you want to upgrade your existing latrine to more beutiful and expensive one through an easy EMI process?
2. Women
i. Do you know about SHG? ii. How it can help poor families to construct toilets through microcredit?
iii. How is the toilet so important for old peole, children and specially women? iv. How does local RSM play an important role in your village?
61
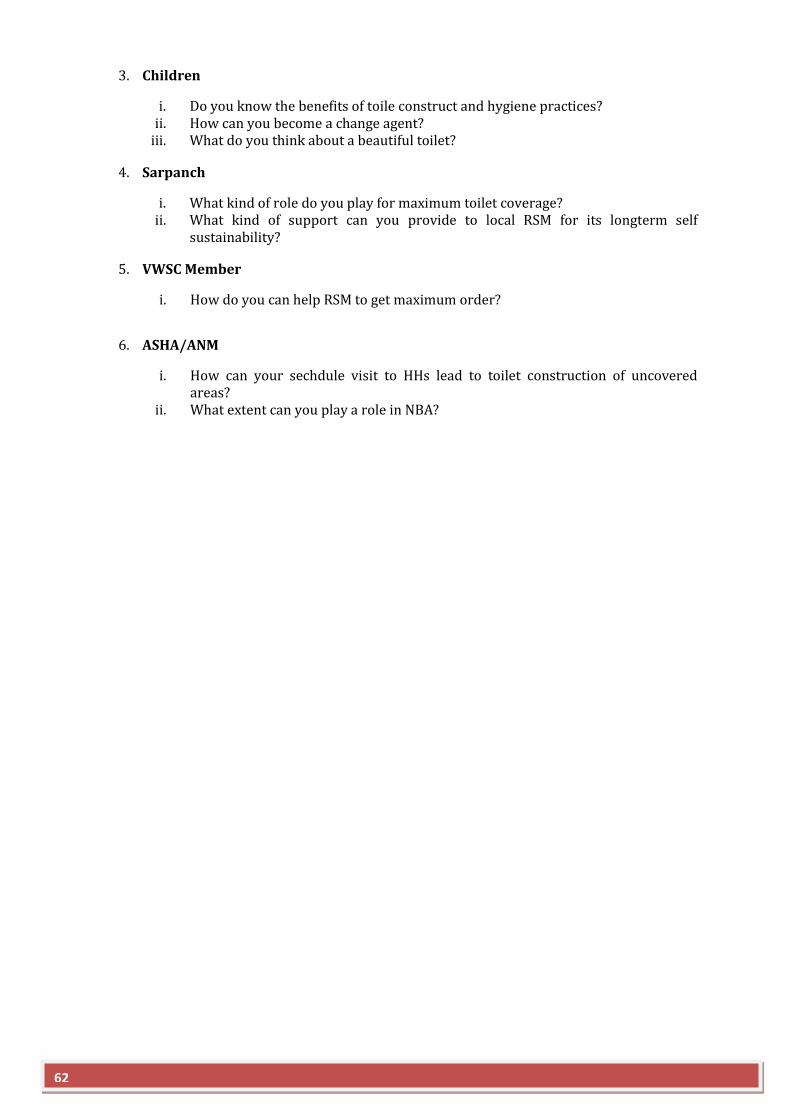
3. Children
i. Do you know the benefits of toile construct and hygiene practices? ii. How can you become a change agent?
iii. What do you think about a beautiful toilet?
4. Sarpanch
i. What kind of role do you play for maximum toilet coverage? ii. What kind of support can you provide to local RSM for its longterm self
sustainability?
5. VWSC Member
i. How do you can help RSM to get maximum order?
6. ASHA/ANM
i. How can your sechdule visit to HHs lead to toilet construction of uncovered areas?
ii. What extent can you play a role in NBA?
62
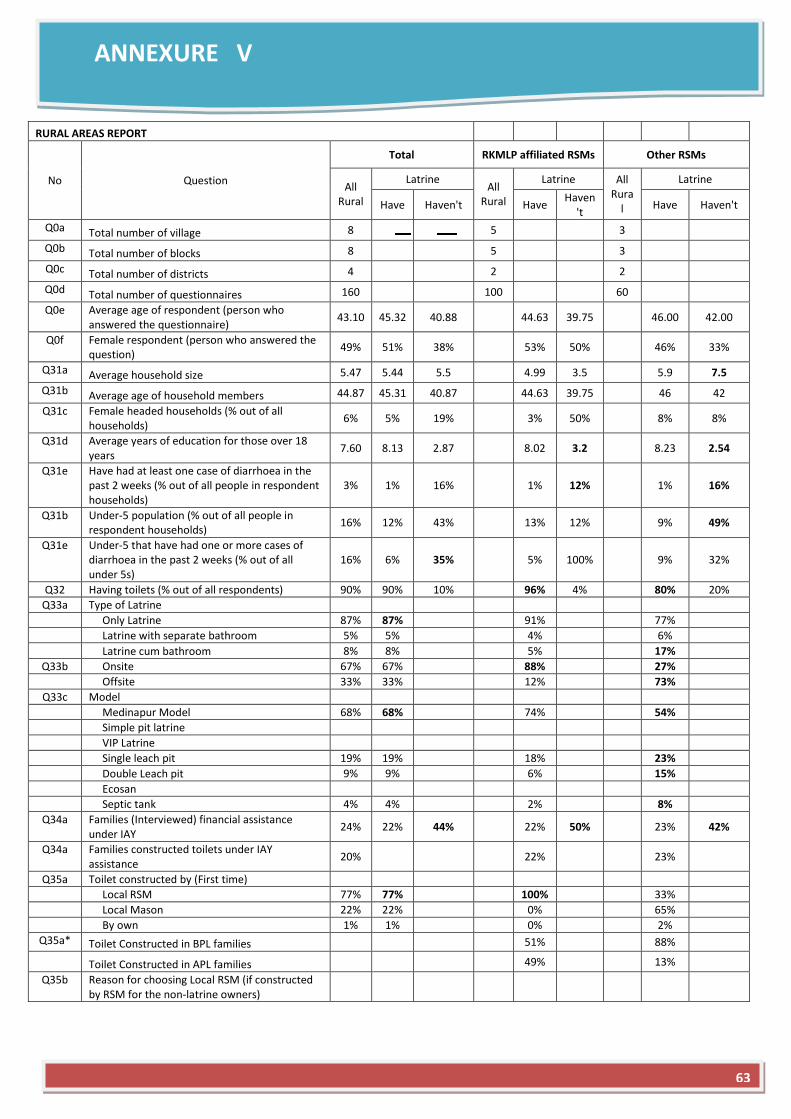
ANNEXURE V
RURAL AREAS REPORT
No Question
Total RKMLP affiliated RSMs Other RSMs
All Rural
Latrine All
Rural
Latrine All Rura
l
Latrine
Have Haven't Have Haven
't Have Haven't
Q0a Total number of village 8
5
3
Q0b Total number of blocks 8
5
3
Q0c Total number of districts 4
2
2
Q0d Total number of questionnaires 160
100
60
Q0e Average age of respondent (person who answered the questionnaire)
43.10 45.32 40.88
44.63 39.75
46.00 42.00
Q0f Female respondent (person who answered the question)
49% 51% 38%
53% 50%
46% 33%
Q31a Average household size 5.47 5.44 5.5
4.99 3.5
5.9 7.5
Q31b Average age of household members 44.87 45.31 40.87
44.63 39.75
46 42
Q31c Female headed households (% out of all households)
6% 5% 19%
3% 50%
8% 8%
Q31d Average years of education for those over 18 years
7.60 8.13 2.87
8.02 3.2
8.23 2.54
Q31e Have had at least one case of diarrhoea in the past 2 weeks (% out of all people in respondent households)
3% 1% 16%
1% 12%
1% 16%
Q31b Under-5 population (% out of all people in respondent households)
16% 12% 43%
13% 12%
9% 49%
Q31e Under-5 that have had one or more cases of diarrhoea in the past 2 weeks (% out of all under 5s)
16% 6% 35%
5% 100%
9% 32%
Q32 Having toilets (% out of all respondents) 90% 90% 10%
96% 4%
80% 20%
Q33a Type of Latrine
Only Latrine 87% 87%
91%
77%
Latrine with separate bathroom 5% 5%
4%
6%
Latrine cum bathroom 8% 8%
5%
17%
Q33b Onsite 67% 67%
88%
27%
Offsite 33% 33%
12%
73%
Q33c Model
Medinapur Model 68% 68%
74%
54%
Simple pit latrine
VIP Latrine
Single leach pit 19% 19%
18%
23%
Double Leach pit 9% 9%
6%
15%
Ecosan
Septic tank 4% 4%
2%
8%
Q34a Families (Interviewed) financial assistance under IAY
24% 22% 44%
22% 50%
23% 42%
Q34a Families constructed toilets under IAY assistance
20%
22%
23%
Q35a Toilet constructed by (First time)
Local RSM 77% 77%
100%
33%
Local Mason 22% 22%
0%
65%
By own 1% 1%
0%
2%
Q35a* Toilet Constructed in BPL families
51%
88%
Toilet Constructed in APL families 49%
13%
Q35b Reason for choosing Local RSM (if constructed
by RSM for the non-latrine owners)
63
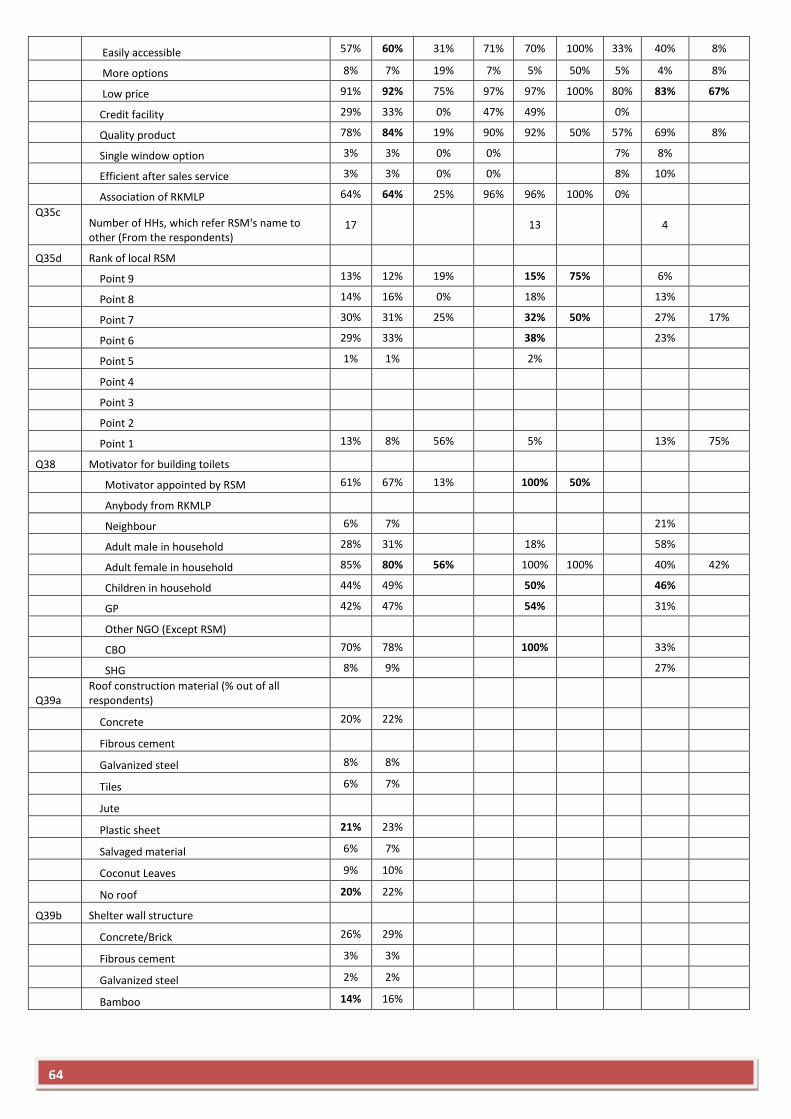
Easily accessible 57% 60% 31% 71% 70% 100% 33% 40% 8%
More options 8% 7% 19% 7% 5% 50% 5% 4% 8%
Low price 91% 92% 75% 97% 97% 100% 80% 83% 67%
Credit facility 29% 33% 0% 47% 49%
0%
Quality product 78% 84% 19% 90% 92% 50% 57% 69% 8%
Single window option 3% 3% 0% 0%
7% 8%
Efficient after sales service 3% 3% 0% 0%
8% 10%
Association of RKMLP 64% 64% 25% 96% 96% 100% 0%
Q35c
Number of HHs, which refer RSM's name to other (From the respondents)
17
13
4
Q35d Rank of local RSM
Point 9 13% 12% 19%
15% 75%
6%
Point 8 14% 16% 0%
18%
13%
Point 7 30% 31% 25%
32% 50%
27% 17%
Point 6 29% 33%
38%
23%
Point 5 1% 1%
2%
Point 4
Point 3
Point 2
Point 1 13% 8% 56%
5%
13% 75%
Q38 Motivator for building toilets
Motivator appointed by RSM 61% 67% 13%
100% 50%
Anybody from RKMLP
Neighbour 6% 7%
21%
Adult male in household 28% 31%
18%
58%
Adult female in household 85% 80% 56%
100% 100%
40% 42%
Children in household 44% 49%
50%
46%
GP 42% 47%
54%
31%
Other NGO (Except RSM)
CBO 70% 78%
100%
33%
SHG 8% 9%
27%
Q39a Roof construction material (% out of all respondents)
Concrete 20% 22%
Fibrous cement
Galvanized steel 8% 8%
Tiles 6% 7%
Jute
Plastic sheet 21% 23%
Salvaged material 6% 7%
Coconut Leaves 9% 10%
No roof 20% 22%
Q39b Shelter wall structure
Concrete/Brick 26% 29%
Fibrous cement 3% 3%
Galvanized steel 2% 2%
Bamboo 14% 16%
64
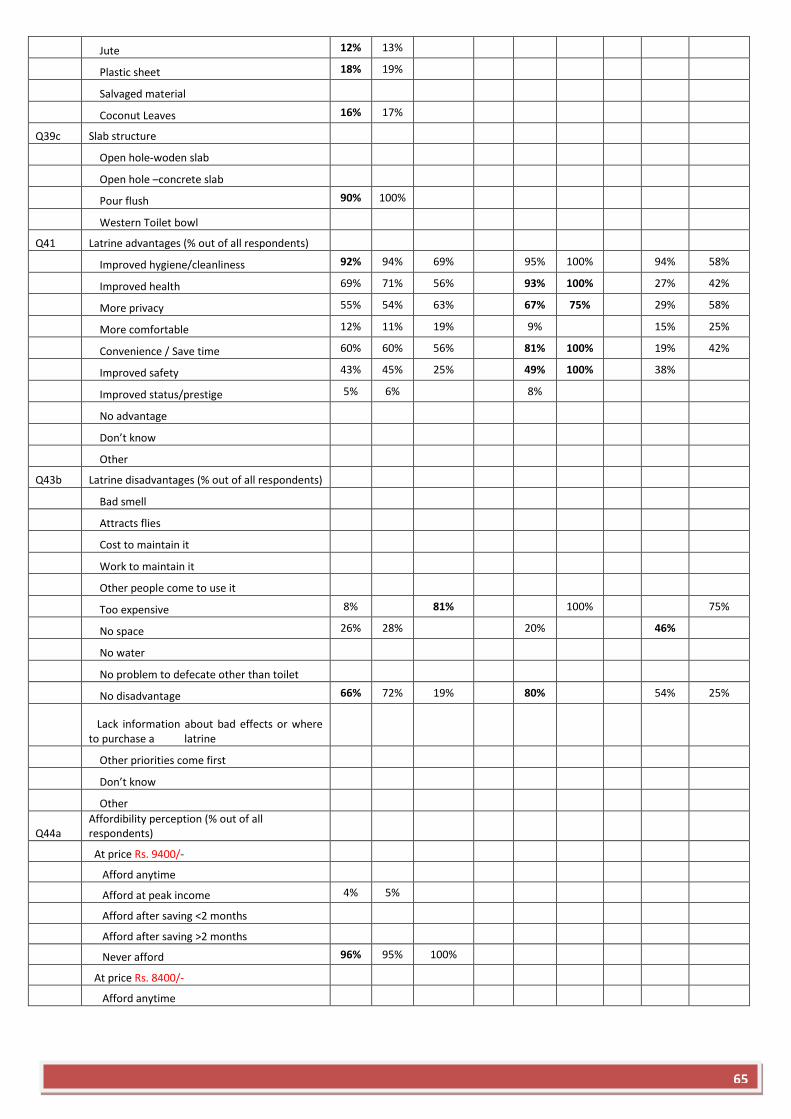
Jute 12% 13%
Plastic sheet 18% 19%
Salvaged material
Coconut Leaves 16% 17%
Q39c Slab structure
Open hole-woden slab
Open hole –concrete slab
Pour flush 90% 100%
Western Toilet bowl
Q41 Latrine advantages (% out of all respondents)
Improved hygiene/cleanliness 92% 94% 69%
95% 100%
94% 58%
Improved health 69% 71% 56%
93% 100%
27% 42%
More privacy 55% 54% 63%
67% 75%
29% 58%
More comfortable 12% 11% 19%
9%
15% 25%
Convenience / Save time 60% 60% 56%
81% 100%
19% 42%
Improved safety 43% 45% 25%
49% 100%
38%
Improved status/prestige 5% 6%
8%
No advantage
Don’t know
Other
Q43b Latrine disadvantages (% out of all respondents)
Bad smell
Attracts flies
Cost to maintain it
Work to maintain it
Other people come to use it
Too expensive 8%
81%
100%
75%
No space 26% 28%
20%
46%
No water
No problem to defecate other than toilet
No disadvantage 66% 72% 19%
80%
54% 25%
Lack information about bad effects or where to purchase a latrine
Other priorities come first
Don’t know
Other
Q44a Affordibility perception (% out of all respondents)
At price Rs. 9400/-
Afford anytime
Afford at peak income 4% 5%
Afford after saving <2 months
Afford after saving >2 months
Never afford 96% 95% 100%
At price Rs. 8400/-
Afford anytime
65
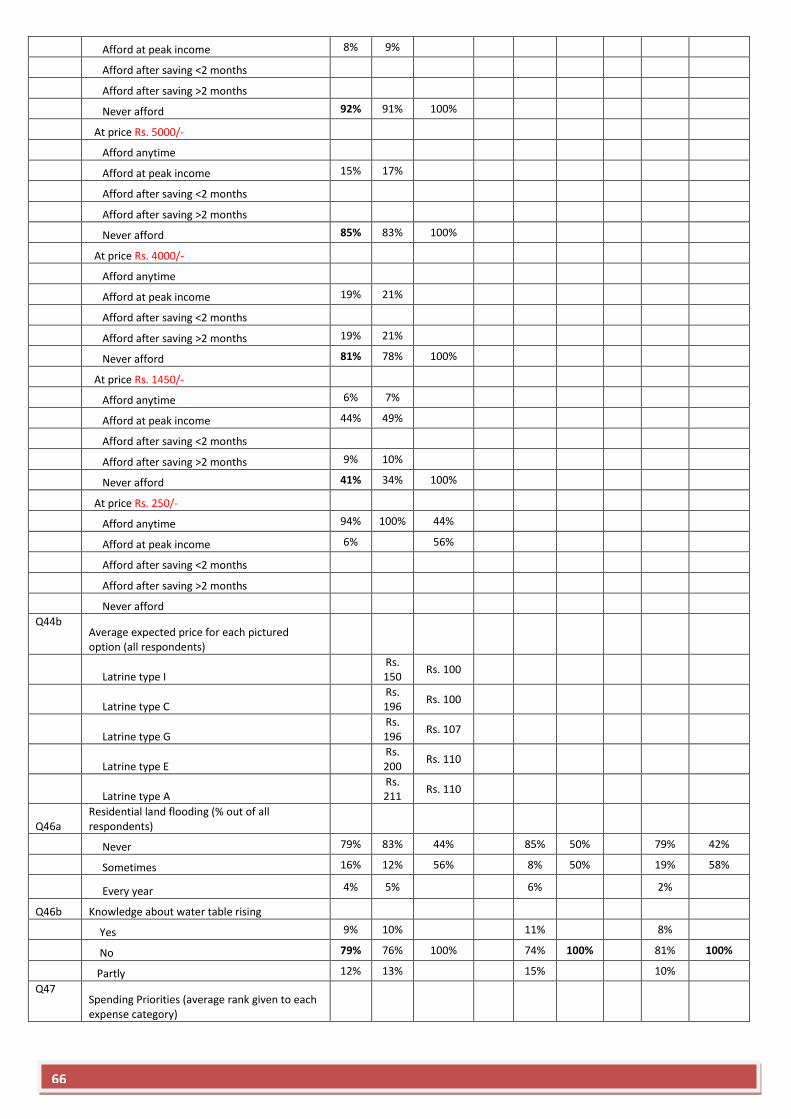
Afford at peak income 8% 9%
Afford after saving <2 months
Afford after saving >2 months
Never afford 92% 91% 100%
At price Rs. 5000/-
Afford anytime
Afford at peak income 15% 17%
Afford after saving <2 months
Afford after saving >2 months
Never afford 85% 83% 100%
At price Rs. 4000/-
Afford anytime
Afford at peak income 19% 21%
Afford after saving <2 months
Afford after saving >2 months 19% 21%
Never afford 81% 78% 100%
At price Rs. 1450/-
Afford anytime 6% 7%
Afford at peak income 44% 49%
Afford after saving <2 months
Afford after saving >2 months 9% 10%
Never afford 41% 34% 100%
At price Rs. 250/-
Afford anytime 94% 100% 44%
Afford at peak income 6%
56%
Afford after saving <2 months
Afford after saving >2 months
Never afford
Q44b Average expected price for each pictured option (all respondents)
Latrine type I
Rs. 150
Rs. 100
Latrine type C
Rs. 196
Rs. 100
Latrine type G
Rs. 196
Rs. 107
Latrine type E
Rs. 200
Rs. 110
Latrine type A
Rs. 211
Rs. 110
Q46a Residential land flooding (% out of all respondents)
Never 79% 83% 44%
85% 50%
79% 42%
Sometimes 16% 12% 56%
8% 50%
19% 58%
Every year 4% 5%
6%
2%
Q46b Knowledge about water table rising
Yes 9% 10%
11%
8%
No 79% 76% 100%
74% 100%
81% 100%
Partly 12% 13%
15%
10%
Q47
Spending Priorities (average rank given to each expense category)
66
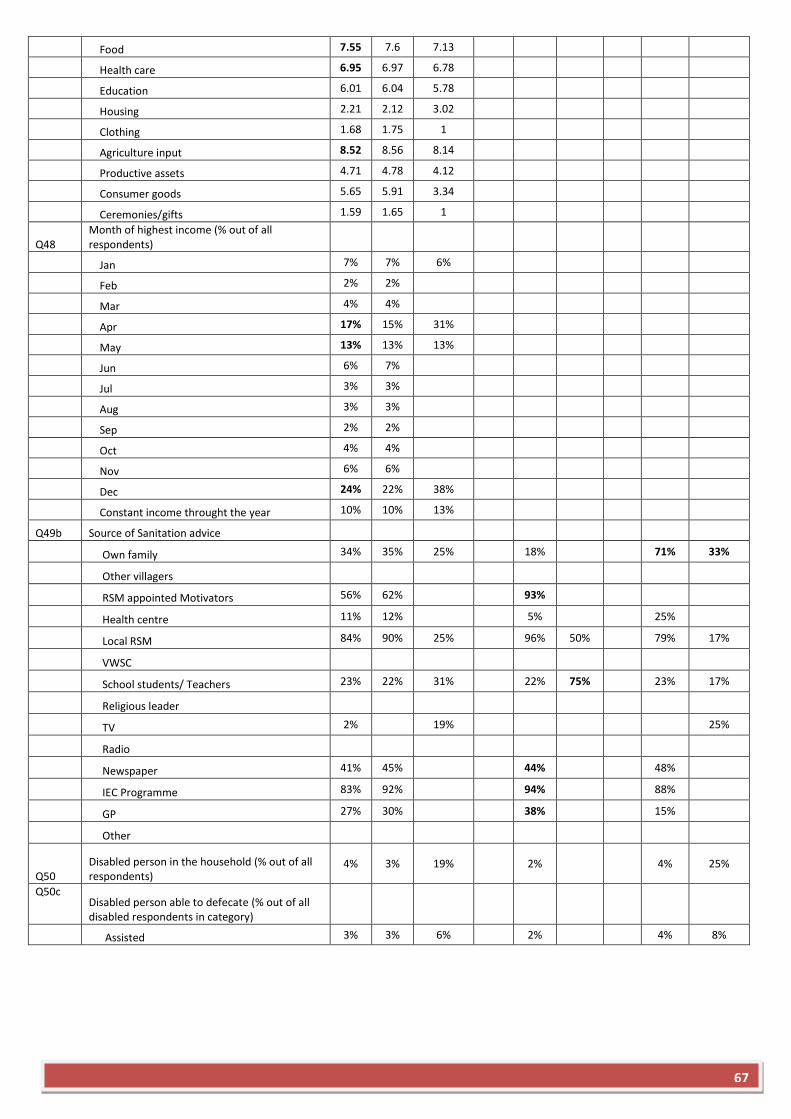
Food 7.55 7.6 7.13
Health care 6.95 6.97 6.78
Education 6.01 6.04 5.78
Housing 2.21 2.12 3.02
Clothing 1.68 1.75 1
Agriculture input 8.52 8.56 8.14
Productive assets 4.71 4.78 4.12
Consumer goods 5.65 5.91 3.34
Ceremonies/gifts 1.59 1.65 1
Q48 Month of highest income (% out of all respondents)
Jan 7% 7% 6%
Feb 2% 2%
Mar 4% 4%
Apr 17% 15% 31%
May 13% 13% 13%
Jun 6% 7%
Jul 3% 3%
Aug 3% 3%
Sep 2% 2%
Oct 4% 4%
Nov 6% 6%
Dec 24% 22% 38%
Constant income throught the year 10% 10% 13%
Q49b Source of Sanitation advice
Own family 34% 35% 25%
18%
71% 33%
Other villagers
RSM appointed Motivators 56% 62%
93%
Health centre 11% 12%
5%
25%
Local RSM 84% 90% 25%
96% 50%
79% 17%
VWSC
School students/ Teachers 23% 22% 31%
22% 75%
23% 17%
Religious leader
TV 2%
19%
25%
Radio
Newspaper 41% 45%
44%
48%
IEC Programme 83% 92%
94%
88%
GP 27% 30%
38%
15%
Other
Q50 Disabled person in the household (% out of all respondents)
4% 3% 19%
2%
4% 25%
Q50c Disabled person able to defecate (% out of all disabled respondents in category)
Assisted 3% 3% 6%
2%
4% 8%
67





























