Embed Size (px)
Citation preview

Robotic surgeryHWR Schreuder, RHM Verheijen
Department of Women and Baby, University Medical Centre Utrecht, Utrecht, the Netherlands
Correspondence: Prof RHM Verheijen, Department of Woman and Baby, University Medical Centre Utrecht, PO Box 85500, Room F05-126, 3508
GA, Utrecht, the Netherlands. Email [email protected]
Accepted 12 October 2008.
Over the past decade, there has been an exponential growth of
robot-assisted procedures and of publications concerning robotic-
assisted laparoscopic surgery. From a review of the available
literature, it becomes apparent that this technology is safe and
allows more complex procedures in many fields of surgery, be it at
relatively high costs. Although randomised controlled trials in
gynaecology are lacking, available evidence suggests that
particularly in gynaecology robotic surgery might not only reduce
morbidity but also be cost effective if performed in high-volume
centres. Training in robotic surgery and programs for safe and
effective implementation are necessary.
Keywords Gynaecology, laparoscopy, robotics, robotic surgery,
training.
Please cite this paper as: Schreuder H, Verheijen R. Robotic surgery. BJOG 2009;116:198–213.
Introduction
The use of robots is rapidly increasing with a market growth
worldwide from less than 5 billion in 2000 to an expected 25
billion in 2010.1 Robotic technology offers the unique oppor-
tunity to control the operational process outside the actual
location, with the skilled and often expert operators not nec-
essarily being physically present. Probably, more important
than the teleoperating features are opportunities for ext-
remely precise, controlled and fatigueless acts of the robot.
This will make it possible to replace human movements that
are limited both in time and in space to make complicated
processes more secure and safe. Interestingly, until recently
robotic technology was mainly applied in manufacturing pro-
cesses but is now becoming increasingly important in
machines for personal use. It is expected that after the current
surge in the public domain, the medical field will also start to
make increasing use of robotics.
In this paper, we review the use of surgical robots in lap-
aroscopy applied in different subspecialties and in gynaecol-
ogy in particular. An inventory of the current applications is
made on the basis of published series. The efficacy, costs,
training and future developments are discussed.
Search strategy
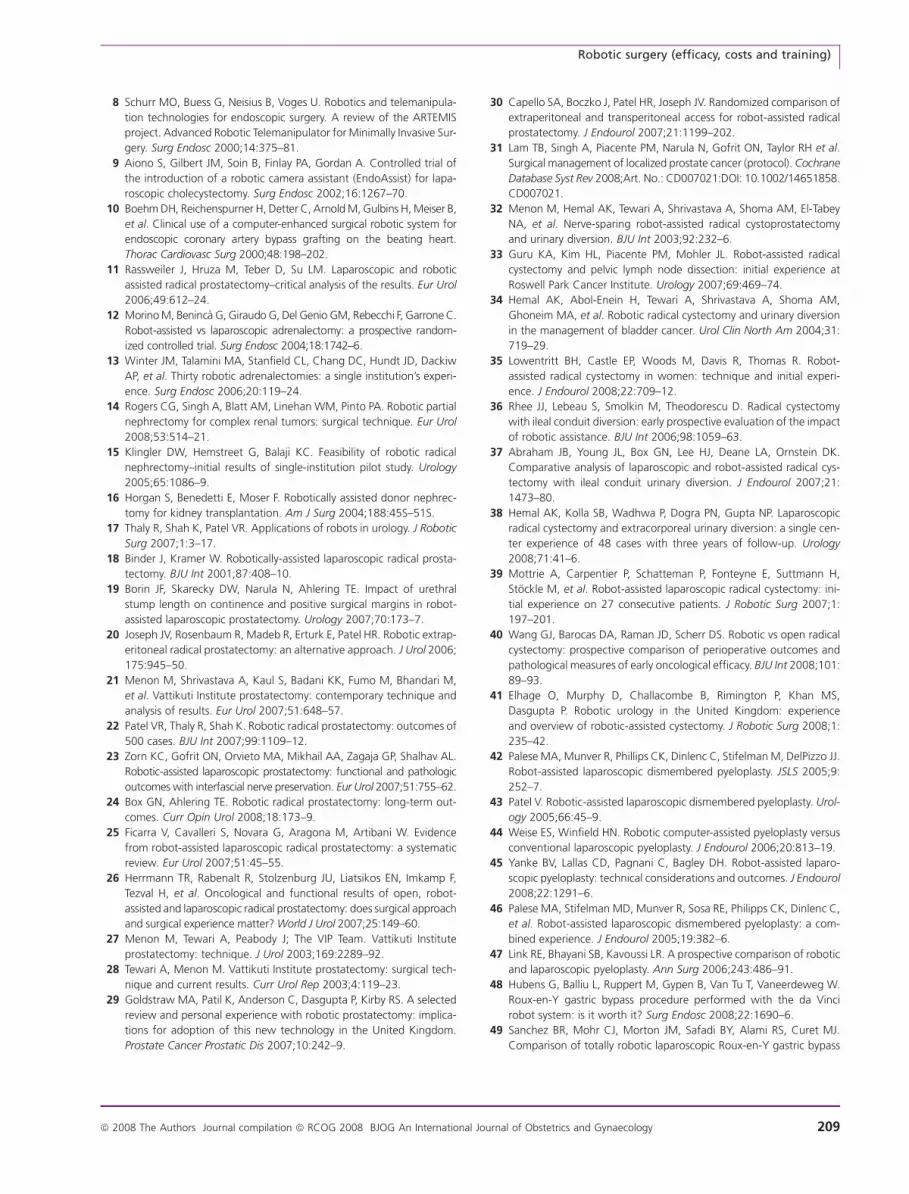
Over the past two decades, the number of publications on
robotic surgery has risen exponentially (Figure 1). A com-
puter aided and manual search for systematic reviews of rand-
omised controlled trials, prospective observational studies,
retrospective studies and case reports published between
1970 and 2008, assessing robotic surgery was carried out
defined by search strings including ‘robotics’ or ‘robot’ or
‘robot-assisted’ or ‘da Vinci’. Different searches were per-
formed for each of the specific subspecialties.
Data sourcesWe searched the following computerised bibliographic data-
bases from 1970 to 2008: MEDLINE, Embase, the Cochrane
Database of systematic reviews, the Cochrane controlled trials
register, the specialist register of trials maintained by Cochrane
Effective Practice and Organisation of Care Group, NHS
Economic Evaluation Database, Database of Abstracts on
Reviews and Effectiveness.
MethodsThe search was performed with the limits English and reports
published between 1 January 1970 and July 2008. Full reports of
each study likely to be relevant were then assessed including the
reference lists. First randomised controlled trials were searched
and subsequently prospective case–control studies, prospective
cohort studies, retrospective studies and case reports were
assessed. Finally, we included all different types of relevant
clinical research because little (randomised) data were available.
History
The first concept of surgical robotics was developed in the late
1980s at the National Aeronautics and Space Centre (NASA).2
Together with the Stanford Research Institute, virtual reality
198 ª 2008 The Authors Journal compilation ª RCOG 2008 BJOG An International Journal of Obstetrics and Gynaecology
DOI: 10.1111/j.1471-0528.2008.02038.x
www.blackwellpublishing.com/bjogReview article

and surgical robotics were integrated and the first steps
towards telepresence surgery were made. The commercialisa-
tion of robotic surgery started in the early 1990s. The next
step was the development of complete robotic systems. The
Zeus robotic system (Computer Motion, Goleta, CA, USA)
and the da Vinci robotic system (Intuitive Surgery, Mountain
View, CA, USA) were introduced in the late 1990s. Both
systems have remote manipulators that are controlled from
a surgical workstation; in less than 20 years’ time, there had
been a major development in robotic surgery (Table 1). In
2003, Computer Motion was taken over by Intuitive Surgery
and today the Zeus system is no longer commercially avail-
able. The da Vinci platform is the only telerobotic system
currently commercially available. The da Vinci system was
approved for general surgery by the US Food and Drug
Administration (FDA) in 2000, for the use in urology in
2001 and for gynaecology in 2005.
Description of technique
The da Vinci robotic system (Intuitive Surgery) has three
major components (Figure 2). The first component is the
surgeon console. The surgeon sits ergonomically behind the
console and controls the robotic system remotely. The con-
sole can be placed anywhere in or even outside the operating
room. While operating, the surgeon is viewing a stereoscopic
image projected in the console and controls the robotic arms
with hand manipulators and food pedals. The position pro-
vides an optimal hand–eye alignment. The surgeon has lim-
ited haptic feedback, so one should rely on visual feedback.
The second component is the Insite Vision System�
(Figure 3). A three-dimensional (3D) view is created with
the use of two camera control units and two light sources,
built in the unit. A 12-mm endoscope (0� or 30�) is used. Theviewer gives a six to ten times magnification of the operating
field. Because of the 3D view, the visual feedback is excellent
and allows the surgeon to work very precisely, even without
haptic feedback. High-definition vision is available in the
robotic visualisation system, providing higher resolution
and improved clarity and detail. Finally, the digital zoom
reduces the interference between endoscope and instruments.
The third component is the patient side cart with the
robotic arms. The first series of da Vinci systems had three
robotic arms, and the new series all have four robotic arms.
Attached to the robotic arms are the EndoWrist� instru-
ments. These instruments are one of the key components of
the system. The wrist has a total of 7 df similar to the human
hand (Figure 4). The surgeon’s hand (fingertip) movements
are translated by the computer to the same movements of the
instruments. Motion scaling (up to 1:10) is making it possible
to perform very precise tasks. The computer also filters out
normal physiological hand tremor and avoids the reverse-
fulcrum effect that occurs in traditional laparoscopy. Depend-
ing on the type of surgery to be performed, there are various
instruments available (Figure 5). The software is important
not only for the functioning of the robot but also to provide
safety features, such as a multi-input display allowing an inte-
grated view of patient critical information and the built-in
telestration for proctoring and team communication.
Robotics in nongynaecological surgery
UrologyRadical prostatectomy has been the fastest growing applica-
tion of robotic surgery in urology and becoming standard
procedure in many centres in the United States.11 Robot assis-
tance is also applied for cystectomy, pyeloplasty, adrenalec-
tomy,12,13 renal surgery,14 radical nephrectomy,15 donor
nephrectomy,16 urogynaecology and paediatric urology.17
Since the first da Vinci robot-assisted radical prostatectomy
was published in 2000,18 multiple large prospective trials
(300–2652 cases) have been published.19–23 Reviewing these
data, Box and Ahlering concluded that the robot-assisted rad-
ical prostatectomy is superior in preventing excessive blood
loss, major surgical complications and the development of
venous thromboembolic events. Oncologic outcomes suggest
Table 1. Robotic surgery in time
1985 First robot used for stereotactic brain surgery3
1989 PROBOT, first robot used for prostatectomies4
1992 ROBODOC use for hip replacement5
1993 AESOP, first commercially available robot
approved by the FDA6,7
1996 ARTREMIS, master slave manipulator system8
1996 EndoAssist, robot camera holder9
1998 Zeus robotic system commercially available10
2000 da Vinci robotic system FDA approved
0
200
400
600
800
1000
1200
1400
Nu
mb
er
of
art
icle
s
1980 1990 1995 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
Year
Articles published
Figure 1. Publications about robotics in www.embase.com (search terms
robot or robotics).
Robotic surgery (efficacy, costs and training)
ª 2008 The Authors Journal compilation ª RCOG 2008 BJOG An International Journal of Obstetrics and Gynaecology 199

that in experienced hands, the percentage of positive surgical
margins in the robot-assisted procedure is equivalent or bet-
ter compared with the open radical prostatectomy. Conti-
nence rates achieved with the robot-assisted procedure are
excellent and the return of sexual function is very good.24
Other reviews draw almost the same conclusions.11,25,26 The
technique of the robot-assisted radical prostatectomy is
described in detail by Tewari and Menon.27,28 The adoption
of the robotic-assisted radical prostatectomy on a large scale
in Europe is slower than in the USA. This could be a related to
Figure 2. da Vinci S HD robotic system (surgeons console, patient side card with robot arms, InSite� vision system) (ª[2008] Intuitive Surgical, Inc.).
Figure 3. InSite� Vision, three dimensional view, with console master
(ª [2008] Intuitive Surgical, Inc.).
Figure 4. EndoWrist� instrument, 7 df, just like the human wrist (ª[2008]
Intuitive Surgical, Inc.).
Schreuder, Verheijen
200 ª 2008 The Authors Journal compilation ª RCOG 2008 BJOG An International Journal of Obstetrics and Gynaecology

the high level of experience in conventional laparoscopy
already available in Europe. Also, Europeans are more expec-
tant for more evidence to show the advantage above conven-
tional laparoscopy. The high costs of setting up a robotic
program could also be a burden for centres. Randomised
clinical trials comparing the open with the robot technique
are unlikely to take place and other tools of assessment are
needed.29 Randomised clinical trials between different robot-
assisted procedures are more likely to take place.30 In 2008,
Lam et al. started to write a Cochrane review about the sur-
gical management of prostate cancer. This review will also
address the issues concerning robot surgery.31 Cystectomy is
mainly used for the treatment of bladder cancer. The first
robot-assisted laparoscopic radical cystectomy was described
in 2003.32 Since then several other authors have published
their initial experiences with this procedure.33–36 The proce-
dure is safe with acceptable operating times and good short-
term functional and oncological results.37–40 In 2008 Elhage
et al. described their surgical technique and looked at the
financial aspect from a British perspective.41 Another difficult
laparoscopic procedure in urology is the ureteropelvic junc-
tion reconstruction (pyeloplasty). Although short-term
results seem to be similar to those of the conventional lapa-
roscopic pyeloplasty42–45 and open repair,46 for experienced
laparoscopists, there was no significant clinical advantage
using robot assistance.47
General surgeryRobotic-assisted laparoscopy is used forNissen fundoplications,
cholecystectomies, gastric bypass surgery,48,49 colectomies,50
mediastinal lymphadenectomy and esophagectomy,51,52
mediastinal parathyroidectomy and thymectomy.53 In 1997,
the first robot-assisted Nissen fundoplications for gastro-
esophageal reflux were performed.54 Notably, this is the only
robotic procedure in which proper randomised trials are
published. Four, relatively small, randomised trials found
no differences in terms of feasibility and outcome, but the
costs of the robot-assisted procedure were higher.55–58 How-
ever, in contrast to primary procedures, repeat fundoplica-
tions are often more demanding and could benefit by robot
assistance.59 The first studies addressing the robot-assisted
cholecystectomy were performed using the Zeus robotic sys-
tem60–62 and later studies with the da Vinci robotic system.63–66
Based on these studies, there is not enough evidence for
routine use of the robot for this procedure.64 A Cochrane
review concerning robotic surgery for the cholecystectomy is
under way.67
Other subspecialtiesRobot assistance is used in cardiovascular surgery for mitral
valve repair, atrial fibrillation surgery, coronary revascularisa-
tion, left ventricular lead placement and congenital heart dis-
ease surgery.68–70 In 2005, the FDA approved the da Vinci
robot for mitral valve surgery and it has become an accepted
procedure.71 The da Vinci robot is also used for aortobife-
moral bypasses72 and aortoileac reconstruction.73 The use of
robotics in paediatric surgery is rapidly growing and it is now
used in the field of general surgery, urology and cardiotho-
racic surgery.74–76 A pilot randomised controlled trial between
robot and conventional laparoscopic fundoplication in chil-
dren was performed.57 A recent overview of the current status
of robot-assisted surgery in children is given by Sinha and
Haddad.77 Other areas where the da Vinci system has been
used include otolaryngeal surgery (FDA approval is expected
this year); endocrine surgery, where the first cases have been
described78,79 and neurosurgery, where results are not yet
published.80 One of the major problems for these robots is
the different types of tissue, bone and soft tissue to be hand-
led. Different robots are used in neurosurgery for microscopy,
navigation, instrumentation, optics and imaging.81–83 The da
Vinci system is not used in orthopaedics, but different robots
are used.84
Robotics in gynaecology
Reproductive surgeryTubal reanastomosisAlthough this microsurgical operation seems to suit the fea-
tures of robotic surgery, there is not much literature available.
The first complete robotic-assisted tubal anastomosis in
humans was performed in 1997 with the Zeus robotic sys-
tem in Cleveland, USA.85 In 2003, Goldberg and Falcone
compared the robotic-assisted procedure with conventional
laparoscopic procedure. The operation time was 2 hours
longer with the robot, and there were no significant differ-
ences in tubal patency and clinical pregnancy rates.86 The
tubal anastomosis by robotic assistance was compared with
Figure 5. EndoWrist� instruments belonging to the da Vinci Robotic
system (ª[2008] Intuitive Surgical, Inc.).
Robotic surgery (efficacy, costs and training)
ª 2008 The Authors Journal compilation ª RCOG 2008 BJOG An International Journal of Obstetrics and Gynaecology 201

minilaparotomy by Rodgers et al. They performed 26 robot-
assisted cases and 41 minilaparotomy cases. Mean anaesthesia
time and surgical time were 283 and 229 minutes, respectively,
for the robot group compared with 205 and 181 minutes for
the minilaparotomy group. There were no differences in hos-
pital stay, pregnancy rates and ectopic pregnancy rates. Costs
were significantly higher in the robot group and return to
normal activity was significantly shorter in the robot group.87
The first reanastomosis with the da Vinci robotic system were
published by Degueldre et al. After a feasibility series of eight
women,88 they evaluated 28 women in 2001. The mean oper-
ating time for bilateral anastomosis was 122minutes, and there
were no complications.Median hospital stay was 1 day (1–2).89
MyomectomyA laparoscopic approach to myomectomy results in less
postoperative pain and faster recovery compared with
laparotomy.90 There is no significant difference between
laparotomy and laparoscopy concerning pregnancy rates,
miscarriage rates, preterm delivery or caesarean section.91
Laparoscopic myomectomy is an advanced procedure that
needs multilayer laparoscopic suturing, resulting in a long
learning curve. This could be the main reason laparotomy
still remains the primary access route to surgical treatment
of intramural and subserosal fibroids. Nevertheless, the robot
could be very helpful with enucleation and suturing. The first
experience with robot-assisted laparoscopic myomectomy
was published in 2004.92 In a case series of 35 women, this
was presented as a promising new technique that may over-
come the surgical limitations of conventional laparoscopy.
A second series by the same author was a retrospective case
matched (age, body mass and myoma weight) analysis of 58
women treated with robot-assisted laparoscopy and laparo-
tomy.93 The robotic approach had less blood loss, shorter
hospital stay and lower complication rates but was more
expensive. The technique of the robotic-assisted laparoscopic
myomectomy used in these two studies is explained in detail.94
A case of a robot-assisted enucleation of a large myoma is
described by Mao et al.95 Sroga et al. described 15 women in
whom they performed a robot-assisted myomectomies and
found operative time to range from 159 to 389 minutes, with
an average blood loss of 160 mL.96 In a retrospective matched
control study of 15 cases comparing robot-assisted laparo-
scopic myomectomy and laparoscopic myomectomy, no dif-
ference in blood loss, hospital stay and postoperative
complications was found. The robot procedure took little,
but significantly, longer (234 versus 203 minutes).97
General gynaecologyAlthough robot assistance in general gynaecology is most
widely used for hysterectomy, no randomised trials have been
reported. The first robot-assisted hysterectomy was published
in 2001.89 The first series of the robot-assisted hysterectomy
for various indications was described in 2002 by Diaz-Arrastia
et al., who performed the procedure in 11 women including
a 10-hour case of full staging for ovarian cancer where repo-
sitioning of the robot was needed twice.98 Three years later,
Beste et al. published their first ten cases, with an operative
time similar to the standard laparoscopic hysterectomy; they
reported that the robot has unique advantages for knot tying,
suturing and adhesiolysis.99 In the same year, Marchal et al.
published 30 cases (18 benign and 12 endometrial cancer
stage I). The mean set-up time for the robot was 30 minutes,
the mean operative time was 185 minutes and the mean robot
use time was 120 minutes. There was no morbidity related to
the robotic system.100 Twenty cases were described in 2006 by
Fiorentino et al.Mean operative time was 200 minutes, mean
blood loss was 81 ml and hospital stay was 2 days. There were
two conversions due to poor visualisation.101 Sixteen cases of
a robot-assisted laparoscopic hysterectomy were published by
Reynolds et al. Their mean operative time was 242 minutes
(170–432) and mean hospital stay was 1.5 days.102 The details
of their technique have been described separately.103 Robot
assistance can be particular of help in difficult cases to over-
come the surgical limitations of conventional laparoscopy. Six
cases with scarred or obliterated anterior cul-de-sac under-
went a robot-assisted hysterectomy without conversion with
satisfactory outcome.104 Nezhat et al. described his first expe-
rience in robot-assisted surgery in a diverse case series of 15
women (hysterectomy, endometriosis, lysis of adhesions and
cystectomy). The visualisation, great surgical precision,
decreasing fatigue and tension tremor of the surgeon and
added wrist motion appeared an advantage. The costs added
operating time and the bulkiness of the equipment were con-
sidered a disadvantage.105 A large prospective study of 91
women was published by Kho et al. Robot-assisted laparo-
scopic hysterectomy took a mean operating time of 128
minutes, with a mean console time of 73 minutes. As
expected, console time decreased with experience and was
significantly associated with uterine weight and adhesiolysis.
Mean blood loss was 79 ml and the mean hospital stay was 1.3
days. There were no conversions, no bladder or urethral inju-
ries occurred, but one enterotomy was repaired robotically.
Six women were readmitted postsurgically because of ileus,
pneumonia, vaginal cuff abscess, colitis and two for pain con-
trol. From this large series, it can be concluded that robot-
assisted laparoscopic hysterectomy can be performed safely
and effectively with acceptable operating times. The robot
overcomes many limitations of the conventional laparos-
copy.106 In 2008 an equally large retrospective comparison
between 100 women who underwent a total laparoscopic hys-
terectomy and 100 women who underwent a robot-assisted
laparoscopic hysterectomy was published. Overall, the oper-
ating time was 27 minutes longer in the robot group. But the
last 25 robotic cases compared with the conventional
Schreuder, Verheijen
202 ª 2008 The Authors Journal compilation ª RCOG 2008 BJOG An International Journal of Obstetrics and Gynaecology

laparoscopy cohort had a significant shorter operating time of
79 versus 92 minutes. The mean blood loss was significantly
less in the robot group (61 versus 113 ml), the mean length of
hospital stay significantly shorter (1.1 versus 1.6 days), while
the incidence of adverse events was the same. The conversion
rate in the robot group was lower (4 versus 9%). Others have
also found that once the learning curve is completed, there is
a reduced operative time, reduced blood loss and a reduced
hospital stay in patients treated robotically.107
Other procedures performed successful with robot assis-
tance are ovarian transposition.108 A recent innovative and
promising application is abdominal cerclage for cervical
insufficiency.109
Pelvic surgery (urogynaecology)Robot-assisted surgery with the da Vinci robot is used in
vesicovaginal fistula repair, sacrocolpopexy and rectovagino-
pexy. Laparoscopic repair of vesicovaginal fistulas is rarely
performed because of its technical difficulty, and there are
few case reports reporting robot-assisted repair.110,111 A case
series of five was performed with a mean operative time of 233
minutes and a blood loss of less than 70 ml, with a 100%
closure rate.112 Robot-assisted laparoscopic sacrocolpopexy
was first described in 2004.113 In 20 women, the mean oper-
ative time was 212 minutes.114 In a subsequent series of 31
women, the same author reported exactly the same mean
operative time of 212 minutes.115 At 1-year follow up, 4 of
30 of these cases had recurrence of prolapse or extrusion of
mesh.116 Ayav et al. described 18 consecutive cases of pelvic
organ prolapse successfully operated with the da Vinci robotic
system. They concluded that using the da Vinci robotic sys-
tem is feasible, safe and effective for the treatment of pelvic
organ prolapse.117 Robot-assisted rectovaginopexy was
described in 15 women by Draaisma et al.118 Median set-up
robot time was 10 minutes, and median skin-to-skin operat-
ing time was 160 minutes, median blood loss less than 50 ml
and median hospital stay was 4 days. Two other small series of
six and ten women also showed the feasibility of this
procedure.119,120
Gynaecological oncologyLaparoscopy can be safely and adequately used in the treat-
ment of endometrial, ovarian and cervical cancer.121 The ini-
tial experience and the first publications of robot assistance in
gynaecological oncology date from recent years. Reynolds
et al. performed seven staging procedures in ovarian and
endometrial cancer patients, with a mean operating time of
257 minutes.122 Twelve hysterectomies for endometrial cancer
(stage I) were performed by the group of Marchal et al.;
robotic surgery was safely performed and had a major advan-
tage for the surgeon’s ergonomics.100 A series of 20 diverse
procedures in gynaecological oncology has been described by
Field et al.123 Boggess presented 43 robotic versus 101 laparo-
scopic staging procedures for endometrial cancer at the
American College of Surgeons. There were no conversions
in the robotic group versus 3% in the laparoscopic group.
In the robot group, the operative time was significantly
shorter (163 versus 213 minutes), significantly more nodes
were received (30 versus 23), there was significantly less blood
loss (63 versus 142 ml) and shorter hospital stay (1 versus 1.2
days). Notably, surgeons were better able to perform compre-
hensive staging on obese women with the robot.124 A large
series was published by Seamon et al.125 Seventy women with
endometrial cancer underwent a robot-assisted hysterectomy
with pelvic and para-aortic lymphadenectomy. Next to a very
detailed overview of their set-up protocol including patient
positioning, trocar placement and instruments used, they also
included video material in the online publication. Such visual
presentations can certainly help others to shorten their learn-
ing curve. For all women in whom the robotic procedure
could be completed, the median total time skin-to-skin time
was 257 minutes (159–380). The average time from entering
the theatre to incision was 45 minutes, the average time from
incision to docking robot was 25 minutes, the time for the
hysterectomy with bilateral salpingectomy was 86 minutes
and the time for the pelvic and aortic lymphadenectomy
was 45 minutes each. When comparing the first ten cases with
the last ten, there was a significant improvement, with short-
ening in time at all different stages of the procedure. The
conversion rate was rather high (9.86%), mean blood loss
was 75 ml and mean hospital stay was 1 day. Veljovich et al.
published their first year experience, performing 118 robot-
assisted oncology procedures for different gynaecologic onco-
logic conditions. They compared their robot procedures with
open and conventional laparoscopic procedures. They found
less blood loss, shorter hospital stay and longer operating time
in the robot procedures (but operating time significantly
decreasing with experience).126 The technique of the robotic
retroperitoneal para-aortic lymphadenectomy has been
described by Vergrote et al.127
The first radical hysterectomy in cervical cancer with robot
assistance was described by Sert and Abeler.128 They con-
cluded that radical dissection could be performed much more
precise than with conventional laparoscopy. In 2007, they
described 15 women with early-stage cervical cancer as a pilot
case–control study and compared robotic-assisted laparo-
scopic radical hysterectomy with conventional total laparo-
scopic radical hysterectomy. There was a significant difference
in mean operating time (241 minutes in the robot group and
300 minutes in the conventional group). No difference in the
number of lymph nodes and size of parametrial tissue was
found. In the robot group, there was significant less bleeding
and shorter hospital stay.129 A prospective analysis of 27
women with early-stage cervical cancer undergoing a robotic
radical hysterectomy was performed by Margina et al., and
a comparison was made with matched patients operated by
Robotic surgery (efficacy, costs and training)
ª 2008 The Authors Journal compilation ª RCOG 2008 BJOG An International Journal of Obstetrics and Gynaecology 203

conventional laparoscopy and laparotomy. They concluded
that operating times for robot surgery and laparotomy were
similar (189 and 166 minutes) and significantly shorter com-
pared with laparoscopy (220 minutes). Blood loss and length
of hospital stay were similar in robotics and laparoscopy and
significantly longer in laparotomy. At a mean follow up of 31
months, there were no recurrences at all.130 Kim et al. per-
formed robotic radical hysterectomy and pelvic lymphade-
nectomy in ten cases and found a mean operating time of
207 minutes. The mean docking time was 26 minutes, but
this was reduced significantly with experience (from 35 to 10
minutes).131 Kowalski et al. compared 14 robotic versus 17
open radical hysterectomies. Their mean operating time was
significantly longer in the robot group (204 versus 121
minutes).132 These small series, however, do not report the
outcome of surgery in terms of lymph node yield and radical-
ity and also lack sufficient oncological follow up. Boggess
found no difference in the operating time (242 versus 240
minutes).124 He performed 13 robot-assisted radical hysterec-
tomies and compared them with 48 open radical hysterecto-
mies. Significantly more lymph nodes were collected in the
robot group (33 versus 22). All the robotic patients were dis-
charged within 24 hours. He also describes how to set up
a robotic programme in gynaecological oncology. A robotic
radical hysterectomy in 20 women was described by Fanning
et al.Operating console time reduced from 8.5 to 3.5 hours in
20 cases. Less blood loss and shorter hospital stay was found.
There were no recurrences at a median follow up of 2 years.133
There are currently no randomised trials concerning robotic
surgery in gynaecological oncology, and none of the pub-
lished studies provides information on long-term effects, such
as survival, lymph oedema, continence and sexual function.
Robotics and anaesthesia
Danic et al. describe anaesthetic considerations in 1500 rad-
ical prostatectomies.134 Some special arrangements have to be
made when performing robot-assisted surgery in the pelvis.
Preoperatively, there is no need for a full bowel preparation,
but it is advisable to use a laxative on the day before surgery.
During the operation, special attention must be given to the
positioning of the patient. Cushioned stirrups should be used
to place the patient in lithotomy position. During the oper-
ation, 45� steep Trendelenburg position is used and the
patient is prone to slip of the table. One can use a chest
binding in an ‘x’-like pattern over the acromia to prevent this,
paying attention to pressure areas. The most common anaes-
thesia-related complication (3% of the cases) was corneal
abrasion, despite the use of eye tape. This could be signifi-
cantly reduced with the use of eye patches. Constant positive
airway pressure of 5 cmH2O preserves arterial oxygenation
during prolonged pneumoperitoneum.135 Baltayian pub-
lished a comprehensive overview of anaesthetic considera-
tions and detailed anaesthetic management for robot-assisted
radical prostatectomy. This could be of help for centres
starting a robotic program and where the anaesthetists are
not familiar with the specific measures for these type of
procedures.136
Cost-effectiveness
An important issue in robotic surgery are the higher costs
compared with regular surgery. Several costs comparisons
have been made in the past few years. We will only discuss
the costs for the use of the da Vinci robotic system since this is
the only robotic platform available at this moment. The latest
robotic da Vinci S system will cost approximately e1.5 million
in Europe plus e150.000 yearly for maintenance. Instruments
are available at approximately e250 per instrument used,
however, price changes are expected with current currency
fluctuations. Finally, extra costs for training, delay in set-up
and extraoperative time during the learning curve should be
anticipated. A recent description of the cost patterns using
a robotic system is given by Prewitt et al. They analysed 224
procedures in different subspecialties in a single institution
and found $1470 greater direct costs for the use of the robotic
system.137 Analyses of costs for different procedures are made:
for robot-assisted laparoscopic rectopexy, there was an
increase in operative costs of e557 or $745 (including material
and time).138 For tubal anastomosis, the increase was $1,446.87
For myomectomy,93 pyeloplasty,47 cholecystectomy64,139 and
Nissen fundiplication,58,140 higher costs were also found for
robot-assisted procedure. Most, if not all, cost-effectiveness
analyses do not or only partly take into account indirect costs.
Morgan et al. compared all ‘in hospital’ costs for the use in
cardiac surgery. When leaving out the initial capital invest-
ment for the robotic system, there was no significant differ-
ence in costs between the robot procedure and the sternotomy
procedure.141 Most cost analyses have been performed for
radical prostatectomy. The cost of the open conventional lap-
aroscopic and robot-assisted radical prostatectomy has been
compared by different groups. Burgess et al. found signifi-
cantly higher operative costs for the robot-assisted procedure,
although these costs decreased after the learning curve was
completed.142 The intraoperative costs were higher in the
robot-assisted procedure but the shorter hospital stay in the
laparoscopic/robot procedure should be taken into
account.143 In relation to this, it is important to realise that
the costs of hospital beds vary between hospitals, especially
between community hospitals and academic medical centres.
So, a robotic program will be most competitive in a high-cost
hospital combined with a high volume of cases.144 An exten-
sive cost analysis for pyeloplasty by experienced surgeons
excluding the learning curve showed cost-effectiveness if
operating time is less then 130 minutes and the yearly cases
are above 500.145 Steinberg also concluded that after the initial
Schreuder, Verheijen
204 ª 2008 The Authors Journal compilation ª RCOG 2008 BJOG An International Journal of Obstetrics and Gynaecology

learning curve, a program of robot-assisted radical prostatec-
tomy, the procedure can be profitable, but that one should
maintain a high volume to pay for the robot and its service.146
The costs of the initial learning curve are high and can vary
widely. A theoretical model of the expenses of the learning
curve was made by including eight series. The costs of the
initial learning curve varied from $49,613 to $554,694 with an
average of $217,034. To overcome these high costs, the con-
cept of high-volume centres is of great importance. In such
centres, the learning curve can be rapidly traversed and costs
minimised.147
Training and education in robotics
With the implementation of robot-assisted laparoscopic sur-
gery, there is also an increasing need for training. Conven-
tional laparoscopic surgery requires different skills and
training compared with open surgery. Basic laparoscopic
skills can be obtained in a box trainer, in a cadaver or with
virtual reality.148 Training for specific procedures is possible
in a cadaver or in a virtual reality environment. In conven-
tional laparoscopy, the surgeon has a two-dimensional (2D)
view, while in robotic surgery, the view is 3D, allowing tasks
to be performed quicker and more efficiently.149–151 In con-
trast to open surgery, the basic laparoscopic and robotic skills
can improve significantly in a relatively short-intensive
course.152 Question is how to maintain this improvement
after a course and whether this improvement translates to
better surgery?
Robot-assisted surgery can be learned in different ways
than conventional laparoscopy. Training on human cadavers
still gives the best anatomic training, but fresh human cadav-
ers are not always available. Coordination for multiple
cadaver use increases the availability of human material and
is advisable.153 The advantage of using fresh tissue models
(like porcine intestine) is obvious in developing delicate tissue
handling. A complex sewing task, like a robotic-sutured in-
testinal anastomosis, can be reproduced successfully by
residents.154 For vascular surgery, a standardized and repro-
ducible training module, using pigs and rats, was devel-
oped.155 Robotic surgery is specifically suitable for virtual
reality training, as the operation itself is computer guided.
Different companies are developing virtual reality simulators
for robotic surgery and this is likely to be the training of
choice for the surgeons of tomorrow.156 The dV-trainer
robotic simulator (Mimic Technologies, Inc., Seattle, WA,
USA) has modules for system training and for skills train-
ing.157 Face, content and construct validity for the virtual
reality dV-Trainer were established.158,159 Another virtual
reality trainer is the SEP� robotic surgery simulator
(SimSurgery, Oslo, Norway, USA)160 (Figure 6). Training
on basic robot-assisted suturing skills using this simulator
equalled training using a mechanical simulator.161 At the Uni-
versity of Nebraska, a virtual reality trainer using da Vinci
instruments and training task platform (dry lab) has been
developed. This 3D virtual reality program can be projected
inside the actual console of the da Vinci robot. Some tasks
were adequately simulated but others need improvement in
the complexity of the virtual reality simulation.162 The same
group developed a more complex robotic surgical task, mesh
alignment, in virtual reality. There were no great differences
between the actual and the virtual environment, and a virtual
reality environment projected inside the console was found to
mimic more than any other surgical training system the actual
environment.163 At the University of Hong Kong, a compre-
hensive computer-based simulator for the da Vinci robotic
system is being developed. The simulator reproduces the
behaviour of the da Vinci system by implementing its kine-
matics and thus providing a promising tool for training and
a way to plan operations.164 Students of today easily and
readily adopt virtual reality as part of their regular training
program.165 The new generation of medical students has
grown up in the age of computer technology and it has been
shown that prior videogame experience can shorten the time
to learn basic skills in virtual reality simulation for minimal
invasive surgery,166 except for robotic suturing, where prior
videogame experience had a negative impact on robotic per-
formance.167 New developments are the use of a mentoring
console. The prototype of the da Vinci mentoring system was
tested by Hanly et al. It facilitates collaboration between the
mentor and the resident during robotic surgery. It improves
performance of complex three-handed tasks. This feature can
also contribute to the patient’s safety in hospitals with robotic
surgical training programs. On the other hand, it improves
resident participation and resident education.168 Other new
developments in training robotics are the use of augmented
visual feedback to enhance robotic surgical training.169 The
Figure 6. SEP da Vinci robotic simulator (ª[2008] SimSurgery).
Robotic surgery (efficacy, costs and training)
ª 2008 The Authors Journal compilation ª RCOG 2008 BJOG An International Journal of Obstetrics and Gynaecology 205

use of 3D telestration technology during an actual operation
not only provides immediate feedback but it is also safer for
the patient through immediate guidance of the surgeon by
a more experienced mentor.170 Together with the approval of
the FDA, the manufacturer of the da Vinci robotic system
(Intuitive Surgery) was demanded to provide comprehensive
training for all teams and surgeons planning to use the robot
clinically. The registered training centres, located all over the
world, can be found on their website. Today 23 official train-
ing centres are noted.171 The first training curriculum for
robotic surgery was developed at the East California Univer-
sity, California.172
Special attention should be given to the training of resi-
dents and fellows. In the early days, the exposure of residents
to robotic training was low.173 In 2003, the interest of general
surgery residents in robotic training was 57%.174 In 2006,
already 75% of the residents surveyed would pursue a fellow-
ship robotic surgery.175 A growing interest is noticeable and
more attention is given to robotic training of residents and
fellows. A systematic approach should be used, starting as
table site assistant and followed by a stepwise approach of
the actual surgery as a console surgeon.176 Unlike open sur-
gery, robotic surgery provides safe and easy opportunity to
divide the operation into smaller segments, enabling partici-
pation as a console surgeon depending on the experience of
the resident or fellow. It is advisable to develop a structured
training program in advance. In this way, a complex opera-
tion can be incorporated in a residency or fellow training
program and has less influence on the total operating time
and patient safety.177 The surgical margins and blood loss are
not negatively affected when using a systematically stepwise
training approach.178
Another aspect of training is the learning curve. The term
‘learning curve’ is used to describe the process of gaining
knowledge and skills in the field of surgical technology. As
a minimum, reporting of learning should include the number
and experience of the operators and a detailed description of
data collection.179 There is a difference between the learning
curve of conventional laparoscopy and robot surgery. Sutur-
ing and dexterity skills can be performed quicker in robot-
assisted laparoscopy than in conventional laparoscopy.180 The
3D view in robotic surgery improves surgical performance
and learning compared with the traditional 2D view laparos-
copy.181 The learning curve for robotic surgical techniques is
therefore relatively short and may be even shorter for a new
generation as residents have a greater ability to interact with
the new robotic instruments.182 Several studies addressed the
issue of how learning of robotic skills best can be assessed. It is
important to identify objective variables for quantifying the
extent of proficiency. Hernandez et al. demonstrate a rapid
learning curve for suturing with the da Vinci robotic system.
Besides time and open structured assessment of technical
skills,183 they used motion analysis and found this a useful
tool.184 Other variables used to show the rapid learning curve
in robotic tasks are bimanual coordination and muscular
activation.185 A computerised assessment system (ProMIS�)
was used to demonstrate the faster and more precise perfor-
mance of the robotic system compared with conventional
laparoscopy.186 An overview of assessment of simulation-
based surgical skills training was published in the Journal of
Surgical Education.187 The learning curve for robot surgical
procedures varies widely. Factors of influence are experience
and expertise of the surgeon, type of surgery and volume of
the surgery. There are various variables that can be used to
define the end-point of the learning curve.188 Most data con-
cerning the learning curve in robotic surgery come from the
radical prostatectomy. They show a relatively short learning
curve if volume is high enough.189 The learning curve for
robot-assisted radical prostatectomy seems to be similar for
a fellowship-trained surgeon and a laparoscopically naıve
experienced surgeon of open radical prostatectomies.190 In
gynaecology, the issue of the learning curve has not yet been
properly described. However, from the small series that
describe reduced docking times and console time with
increased experience, it can be concluded that learning curves
are as steep as in other types of surgery.106 Finally, the rela-
tively large series from Seamon et al. clearly show a significant
effect of experience with gynaecological operations.125
Setting up a robotic program
With the growing interest in robotic surgery and the prom-
ising results, there is an increasing need for information how
to set up a robotic program. Palmer et al. describe five essen-
tial phases to set up a successful robotic program. The first
step is the development of a business plan, defining the initial
robotic program and arrange proper administrative support.
The second phase is the implementation in which one must
think of the theatre design, the theatre team, the purchase of
a robotic system, sterilisation facilities, marketing and an
expert lead surgeon.191 The third phase is the execution of
the program. Followed by a phase of maintenance. In this
fourth phase, one should have a proper data system for qual-
ity control and efficiency and outcomes as well as patient
satisfaction should be registered. A structured program for
training and education of fellow’s/residents should be avail-
able. The last phase is growth to make the program profitable,
where one could think of recruitment or training of new
surgeons working together with other subspecialties.192 Very
importantly, there is a need for a dedicated theatre team.193
Transforming an existing high-volume conventional laparo-
scopic program to a robot-assisted program for radical pros-
tatectomy can be achieved while maintaining reasonable
profits. However, equal profit is not possible without a sub-
stantial increase of caseload.146 All the above programs were
launched in the USA. The situation in Europe is different
Schreuder, Verheijen
206 ª 2008 The Authors Journal compilation ª RCOG 2008 BJOG An International Journal of Obstetrics and Gynaecology

from country to country because of different healthcare sys-
tems and insurance systems. For the UK, some general impli-
cations, similar to those for the USA, for adoption of a robotic
surgery program are described by Goldstraw et al.29
Litigation and ethical issues
The increasing complexity of modern surgical technology will
require more stringent guidelines for operation and practice
similar to the discipline exercised in aviation. Using a surgical
robot implies that the surgeon is no longer in direct physical
of visual contact with the patient. The surgeon not only oper-
ates through computer commands but there is also a physical
distance to the assistants attending the operation table.
Unfortunately, the current systems lack a satisfactory way to
communicate between the operator and the assistants. As
with many new technological advances, communication
might appear the Achilles’ heel of robotic surgery. More
appropriate equipment of communication and more strict
discipline in follow up of the commands from the primary
responsible person, the surgeon, will be essential for a safe and
successful procedure.
With the possibility of telemedicine and robotics new legal
and ethical issues arise. Telemedicine makes cross-border
treatment possible. How to deal with liability and licensure
across borders? Cross-border care should not change usual
medical ethics but makes treatment possible of patients in
areas the specialist cannot reach in person. In this way, under-
served regions and countries could be helped. But the tech-
nology could also aggravate migration of specialists from
poor to rich areas/countries.194 Also, the security of the trans-
mitted data between the surgeon and the (distant) robot is at
stake. Should data be treated the same way as written medical
records? Who is responsible if complications arise due to
transmission cuts, a breakdown of the system or instability
of the software? Malfunction of the robotic system will occur
more frequently with its increasing use; fortunately, it
appeared that less than 5% of device failures resulted in
patient complications. In addition, the rate of open conver-
sions due to device malfunction decreased from 94% in 2003
to 16% in 2007.195 Although robots seem to act autono-
mously, all their movements and actions are operated by
the surgeon and as such do not differ from any other surgical
equipment. Nevertheless, as with any complex system, safety
precautions will be more essential than with the use of simple
instruments. Local as well as national and international guide-
lines will need to be developed to address specific issues. In
2007, the first policy guidelines for the robot-assisted prosta-
tectomy were suggested in an editorial by Valvo et al.196 The
Society of American Gastrointestinal and Endoscopic Sur-
geons and the Minimally Invasive Robotic Association
believed that guidelines for the use of robotics were lacking.
To overcome this gap, they published a consensus statement
on robotic surgery including guidelines for training and cre-
dentialing.197 The World Medical Association (WMA) made
a statement on the ethics of telemedicine on their last meeting
in Copenhagen (October 2007). Included are principles for
the patient–physician relationship and confidentiality, the
responsibilities of the physician and the quality of care. The
WMA is encouraging the development of national legislation
and international agreements on telemedicine.198
Pros and cons
The robotic surgical system has some clear advantages com-
pared with conventional laparoscopy. A summary of the
advantages and disadvantages of robot-assisted laparoscopic
surgery is given in Table 2.
Future of robotics in gynaecology
Considering the development of robotics in general and assis-
ted surgery in particular, it is to be expected that the appli-
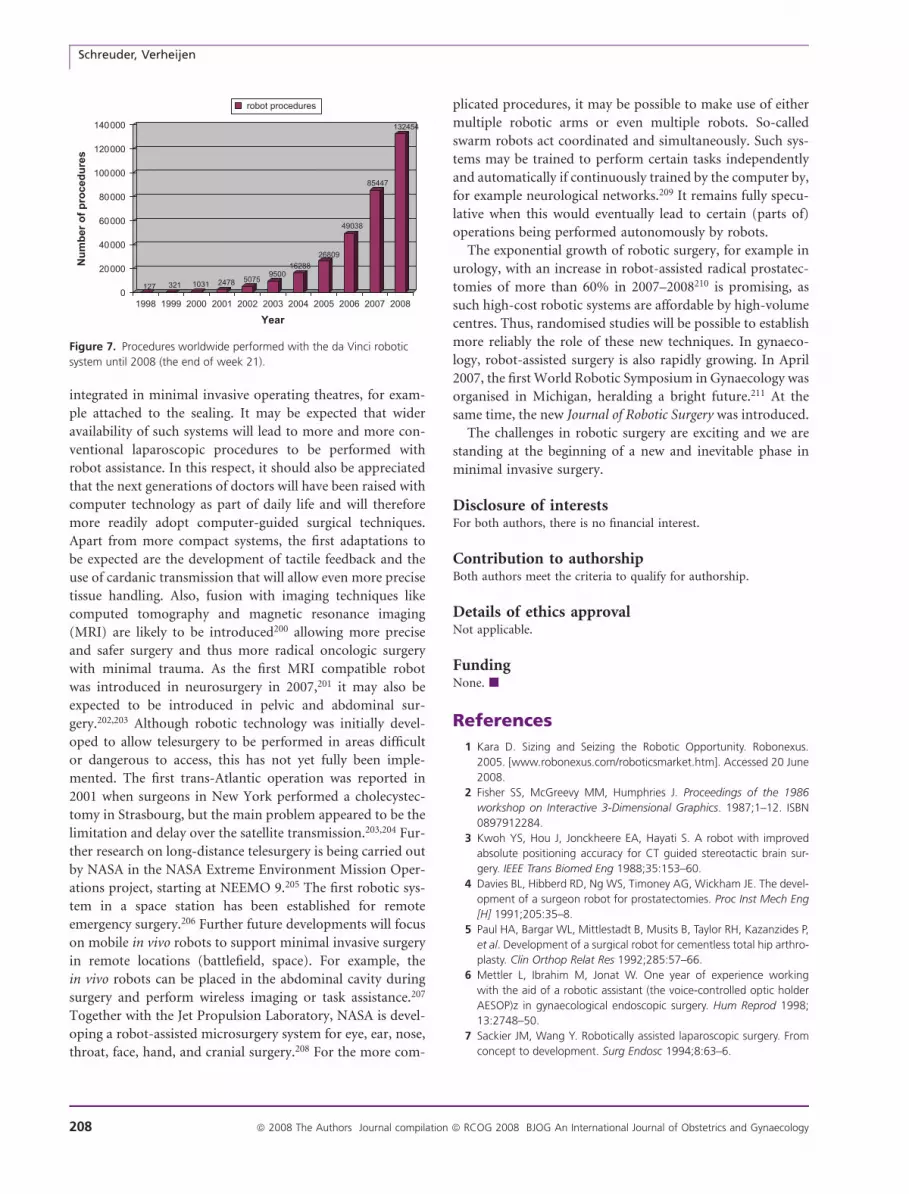
cation of this technology will only increase.199 The
exponential growth of the da Vinci robotic surgical system
worldwide, with more than 867 systems sold up to march
2008,171 will lead to an exponential growth of procedures
performed (Figure 7). As with every innovation that introdu-
ces new technology, initial scepticism with respect to neces-
sity, applicability and affordability will mean a delay in wider
introduction.
In the near future, the robotic systems will become
smaller and easier to handle. Whereas they now constitute
stand-alone systems, it is expected that they will become
Table 2. Advantages and disadvantages of robotic surgery
Advantage Disadvantage
Surgical system advantages High costs
Better InSIte� vision (3D) Robotic system
Digital camera zoom Maintenance system
Camera stability Start up
Greater df (Endowrist�) Bulky size of the robotic system
Improved dexterity Sometimes difficult access
to patient
Elimination of fulcrum effect Separation surgeon from the
operating field
Better ergonomics
for surgeon
No tactile feedback
Motion scaling Chance of breakdown
Elimination of physiological
hand tremor
Use of 8 mm ports
Telesurgery possible Monopoly of single market
leader
Telementoring possible
Robotic surgery (efficacy, costs and training)
ª 2008 The Authors Journal compilation ª RCOG 2008 BJOG An International Journal of Obstetrics and Gynaecology 207
integrated in minimal invasive operating theatres, for exam-
ple attached to the sealing. It may be expected that wider
availability of such systems will lead to more and more con-
ventional laparoscopic procedures to be performed with
robot assistance. In this respect, it should also be appreciated
that the next generations of doctors will have been raised with
computer technology as part of daily life and will therefore
more readily adopt computer-guided surgical techniques.
Apart from more compact systems, the first adaptations to
be expected are the development of tactile feedback and the
use of cardanic transmission that will allow even more precise
tissue handling. Also, fusion with imaging techniques like
computed tomography and magnetic resonance imaging
(MRI) are likely to be introduced200 allowing more precise
and safer surgery and thus more radical oncologic surgery
with minimal trauma. As the first MRI compatible robot
was introduced in neurosurgery in 2007,201 it may also be
expected to be introduced in pelvic and abdominal sur-
gery.202,203 Although robotic technology was initially devel-
oped to allow telesurgery to be performed in areas difficult
or dangerous to access, this has not yet fully been imple-
mented. The first trans-Atlantic operation was reported in
2001 when surgeons in New York performed a cholecystec-
tomy in Strasbourg, but the main problem appeared to be the
limitation and delay over the satellite transmission.203,204 Fur-
ther research on long-distance telesurgery is being carried out
by NASA in the NASA Extreme Environment Mission Oper-
ations project, starting at NEEMO 9.205 The first robotic sys-
tem in a space station has been established for remote
emergency surgery.206 Further future developments will focus
on mobile in vivo robots to support minimal invasive surgery
in remote locations (battlefield, space). For example, the
in vivo robots can be placed in the abdominal cavity during
surgery and perform wireless imaging or task assistance.207
Together with the Jet Propulsion Laboratory, NASA is devel-
oping a robot-assisted microsurgery system for eye, ear, nose,
throat, face, hand, and cranial surgery.208 For the more com-
plicated procedures, it may be possible to make use of either
multiple robotic arms or even multiple robots. So-called
swarm robots act coordinated and simultaneously. Such sys-
tems may be trained to perform certain tasks independently
and automatically if continuously trained by the computer by,
for example neurological networks.209 It remains fully specu-
lative when this would eventually lead to certain (parts of)
operations being performed autonomously by robots.
The exponential growth of robotic surgery, for example in
urology, with an increase in robot-assisted radical prostatec-
tomies of more than 60% in 2007–2008210 is promising, as
such high-cost robotic systems are affordable by high-volume
centres. Thus, randomised studies will be possible to establish
more reliably the role of these new techniques. In gynaeco-
logy, robot-assisted surgery is also rapidly growing. In April
2007, the first World Robotic Symposium in Gynaecology was
organised in Michigan, heralding a bright future.211 At the
same time, the new Journal of Robotic Surgery was introduced.
The challenges in robotic surgery are exciting and we are
standing at the beginning of a new and inevitable phase in
minimal invasive surgery.
Disclosure of interestsFor both authors, there is no financial interest.
Contribution to authorshipBoth authors meet the criteria to qualify for authorship.
Details of ethics approvalNot applicable.
FundingNone. j
References
1 Kara D. Sizing and Seizing the Robotic Opportunity. Robonexus.
2005. [www.robonexus.com/roboticsmarket.htm]. Accessed 20 June
2008.
2 Fisher SS, McGreevy MM, Humphries J. Proceedings of the 1986
workshop on Interactive 3-Dimensional Graphics. 1987;1–12. ISBN
0897912284.
3 Kwoh YS, Hou J, Jonckheere EA, Hayati S. A robot with improved
absolute positioning accuracy for CT guided stereotactic brain sur-
gery. IEEE Trans Biomed Eng 1988;35:153–60.
4 Davies BL, Hibberd RD, Ng WS, Timoney AG, Wickham JE. The devel-
opment of a surgeon robot for prostatectomies. Proc Inst Mech Eng
[H] 1991;205:35–8.
5 Paul HA, Bargar WL, Mittlestadt B, Musits B, Taylor RH, Kazanzides P,
et al. Development of a surgical robot for cementless total hip arthro-
plasty. Clin Orthop Relat Res 1992;285:57–66.
6 Mettler L, Ibrahim M, Jonat W. One year of experience working
with the aid of a robotic assistant (the voice-controlled optic holder
AESOP)z in gynaecological endoscopic surgery. Hum Reprod 1998;
13:2748–50.
7 Sackier JM, Wang Y. Robotically assisted laparoscopic surgery. From
concept to development. Surg Endosc 1994;8:63–6.
127 321 1031 2478 50759500
16288
26809
49038
85447
132454
0
20000
40000
60000
80000
100000
120000
140000
Nu
mb
er
of
pro
ce
du
res
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008
Year
robot procedures
Figure 7. Procedures worldwide performed with the da Vinci robotic
system until 2008 (the end of week 21).
Schreuder, Verheijen
208 ª 2008 The Authors Journal compilation ª RCOG 2008 BJOG An International Journal of Obstetrics and Gynaecology
8 Schurr MO, Buess G, Neisius B, Voges U. Robotics and telemanipula-
tion technologies for endoscopic surgery. A review of the ARTEMIS
project. Advanced Robotic Telemanipulator for Minimally Invasive Sur-
gery. Surg Endosc 2000;14:375–81.
9 Aiono S, Gilbert JM, Soin B, Finlay PA, Gordan A. Controlled trial of
the introduction of a robotic camera assistant (EndoAssist) for lapa-
roscopic cholecystectomy. Surg Endosc 2002;16:1267–70.
10 BoehmDH, Reichenspurner H, Detter C, ArnoldM,Gulbins H,Meiser B,
et al. Clinical use of a computer-enhanced surgical robotic system for
endoscopic coronary artery bypass grafting on the beating heart.
Thorac Cardiovasc Surg 2000;48:198–202.
11 Rassweiler J, Hruza M, Teber D, Su LM. Laparoscopic and robotic
assisted radical prostatectomy–critical analysis of the results. Eur Urol
2006;49:612–24.
12 MorinoM, Beninca G, Giraudo G, Del Genio GM, Rebecchi F, GarroneC.
Robot-assisted vs laparoscopic adrenalectomy: a prospective random-
ized controlled trial. Surg Endosc 2004;18:1742–6.
13 Winter JM, Talamini MA, Stanfield CL, Chang DC, Hundt JD, Dackiw
AP, et al. Thirty robotic adrenalectomies: a single institution’s experi-
ence. Surg Endosc 2006;20:119–24.
14 Rogers CG, Singh A, Blatt AM, Linehan WM, Pinto PA. Robotic partial
nephrectomy for complex renal tumors: surgical technique. Eur Urol
2008;53:514–21.
15 Klingler DW, Hemstreet G, Balaji KC. Feasibility of robotic radical
nephrectomy–initial results of single-institution pilot study. Urology
2005;65:1086–9.
16 Horgan S, Benedetti E, Moser F. Robotically assisted donor nephrec-
tomy for kidney transplantation. Am J Surg 2004;188:45S–51S.
17 Thaly R, Shah K, Patel VR. Applications of robots in urology. J Robotic
Surg 2007;1:3–17.
18 Binder J, Kramer W. Robotically-assisted laparoscopic radical prosta-
tectomy. BJU Int 2001;87:408–10.
19 Borin JF, Skarecky DW, Narula N, Ahlering TE. Impact of urethral
stump length on continence and positive surgical margins in robot-
assisted laparoscopic prostatectomy. Urology 2007;70:173–7.
20 Joseph JV, Rosenbaum R, Madeb R, Erturk E, Patel HR. Robotic extrap-
eritoneal radical prostatectomy: an alternative approach. J Urol 2006;
175:945–50.
21 Menon M, Shrivastava A, Kaul S, Badani KK, Fumo M, Bhandari M,
et al. Vattikuti Institute prostatectomy: contemporary technique and
analysis of results. Eur Urol 2007;51:648–57.
22 Patel VR, Thaly R, Shah K. Robotic radical prostatectomy: outcomes of
500 cases. BJU Int 2007;99:1109–12.
23 Zorn KC, Gofrit ON, Orvieto MA, Mikhail AA, Zagaja GP, Shalhav AL.
Robotic-assisted laparoscopic prostatectomy: functional and pathologic
outcomes with interfascial nerve preservation. Eur Urol 2007;51:755–62.
24 Box GN, Ahlering TE. Robotic radical prostatectomy: long-term out-
comes. Curr Opin Urol 2008;18:173–9.
25 Ficarra V, Cavalleri S, Novara G, Aragona M, Artibani W. Evidence
from robot-assisted laparoscopic radical prostatectomy: a systematic
review. Eur Urol 2007;51:45–55.
26 Herrmann TR, Rabenalt R, Stolzenburg JU, Liatsikos EN, Imkamp F,
Tezval H, et al. Oncological and functional results of open, robot-
assisted and laparoscopic radical prostatectomy: does surgical approach
and surgical experience matter?World J Urol 2007;25:149–60.
27 Menon M, Tewari A, Peabody J; The VIP Team. Vattikuti Institute
prostatectomy: technique. J Urol 2003;169:2289–92.
28 Tewari A, Menon M. Vattikuti Institute prostatectomy: surgical tech-
nique and current results. Curr Urol Rep 2003;4:119–23.
29 Goldstraw MA, Patil K, Anderson C, Dasgupta P, Kirby RS. A selected
review and personal experience with robotic prostatectomy: implica-
tions for adoption of this new technology in the United Kingdom.
Prostate Cancer Prostatic Dis 2007;10:242–9.
30 Capello SA, Boczko J, Patel HR, Joseph JV. Randomized comparison of
extraperitoneal and transperitoneal access for robot-assisted radical
prostatectomy. J Endourol 2007;21:1199–202.
31 Lam TB, Singh A, Piacente PM, Narula N, Gofrit ON, Taylor RH et al.
Surgical management of localized prostate cancer (protocol). Cochrane
Database Syst Rev 2008;Art. No.: CD007021:DOI: 10.1002/14651858.
CD007021.
32 Menon M, Hemal AK, Tewari A, Shrivastava A, Shoma AM, El-Tabey
NA, et al. Nerve-sparing robot-assisted radical cystoprostatectomy
and urinary diversion. BJU Int 2003;92:232–6.
33 Guru KA, Kim HL, Piacente PM, Mohler JL. Robot-assisted radical
cystectomy and pelvic lymph node dissection: initial experience at
Roswell Park Cancer Institute. Urology 2007;69:469–74.
34 Hemal AK, Abol-Enein H, Tewari A, Shrivastava A, Shoma AM,
Ghoneim MA, et al. Robotic radical cystectomy and urinary diversion
in the management of bladder cancer. Urol Clin North Am 2004;31:
719–29.
35 Lowentritt BH, Castle EP, Woods M, Davis R, Thomas R. Robot-
assisted radical cystectomy in women: technique and initial experi-
ence. J Endourol 2008;22:709–12.
36 Rhee JJ, Lebeau S, Smolkin M, Theodorescu D. Radical cystectomy
with ileal conduit diversion: early prospective evaluation of the impact
of robotic assistance. BJU Int 2006;98:1059–63.
37 Abraham JB, Young JL, Box GN, Lee HJ, Deane LA, Ornstein DK.
Comparative analysis of laparoscopic and robot-assisted radical cys-
tectomy with ileal conduit urinary diversion. J Endourol 2007;21:
1473–80.
38 Hemal AK, Kolla SB, Wadhwa P, Dogra PN, Gupta NP. Laparoscopic
radical cystectomy and extracorporeal urinary diversion: a single cen-
ter experience of 48 cases with three years of follow-up. Urology
2008;71:41–6.
39 Mottrie A, Carpentier P, Schatteman P, Fonteyne E, Suttmann H,
Stockle M, et al. Robot-assisted laparoscopic radical cystectomy: ini-
tial experience on 27 consecutive patients. J Robotic Surg 2007;1:
197–201.
40 Wang GJ, Barocas DA, Raman JD, Scherr DS. Robotic vs open radical
cystectomy: prospective comparison of perioperative outcomes and
pathological measures of early oncological efficacy. BJU Int 2008;101:
89–93.
41 Elhage O, Murphy D, Challacombe B, Rimington P, Khan MS,
Dasgupta P. Robotic urology in the United Kingdom: experience
and overview of robotic-assisted cystectomy. J Robotic Surg 2008;1:
235–42.
42 Palese MA, Munver R, Phillips CK, Dinlenc C, Stifelman M, DelPizzo JJ.
Robot-assisted laparoscopic dismembered pyeloplasty. JSLS 2005;9:
252–7.
43 Patel V. Robotic-assisted laparoscopic dismembered pyeloplasty. Urol-
ogy 2005;66:45–9.
44 Weise ES, Winfield HN. Robotic computer-assisted pyeloplasty versus
conventional laparoscopic pyeloplasty. J Endourol 2006;20:813–19.
45 Yanke BV, Lallas CD, Pagnani C, Bagley DH. Robot-assisted laparo-
scopic pyeloplasty: technical considerations and outcomes. J Endourol
2008;22:1291–6.
46 Palese MA, Stifelman MD, Munver R, Sosa RE, Philipps CK, Dinlenc C,
et al. Robot-assisted laparoscopic dismembered pyeloplasty: a com-
bined experience. J Endourol 2005;19:382–6.
47 Link RE, Bhayani SB, Kavoussi LR. A prospective comparison of robotic
and laparoscopic pyeloplasty. Ann Surg 2006;243:486–91.
48 Hubens G, Balliu L, Ruppert M, Gypen B, Van Tu T, Vaneerdeweg W.
Roux-en-Y gastric bypass procedure performed with the da Vinci
robot system: is it worth it? Surg Endosc 2008;22:1690–6.
49 Sanchez BR, Mohr CJ, Morton JM, Safadi BY, Alami RS, Curet MJ.
Comparison of totally robotic laparoscopic Roux-en-Y gastric bypass
Robotic surgery (efficacy, costs and training)
ª 2008 The Authors Journal compilation ª RCOG 2008 BJOG An International Journal of Obstetrics and Gynaecology 209

and traditional laparoscopic Roux-en-Y gastric bypass. Surg Obes
Relat Dis 2005;1:549–54.
50 Rawlings AL, Woodland JH, Vegunta RK, Crawford DL. Robotic versus
laparoscopic colectomy. Surg Endosc 2007;21:1701–8.
51 van Hillegersberg R, Boone J, Draaisma WA, Broeders IA, Giezeman
MJ, Borel Rinkes IH. First experience with robot-assisted thoraco-
scopic esophagolymphadenectomy for esophageal cancer. Surg
Endosc 2006;20:1435–9.
52 Kernstine KH, DeArmond DT, Shamoun DM, Campos JH. The first
series of completely robotic esophagectomies with three-field lym-
phadenectomy: initial experience. Surg Endosc 2007;21:2285–92.
53 Augustin F, Schmid T, Bodner J. The robotic approach for mediastinal
lesions. Int J Med Robot 2006;2:262–70.
54 Cadiere GB, Himpens J, Vertruyen M, Bruyns J, Germay O, Leman G,
et al. Evaluation of telesurgical (robotic) NISSEN fundoplication. Surg
Endosc 2001;15:918–23.
55 Draaisma WA, Ruurda JP, Scheffer RC, Simmermacher RK, Gooszen
HG, Rijnhart-de Jong HG, et al. Randomized clinical trial of stan-
dard laparoscopic versus robot-assisted laparoscopic Nissen fundoplica-
tion for gastro-oesophageal reflux disease. Br J Surg 2006;93:1351–9.
56 Morino M, Pellegrino L, Giaccone C, Garrone C, Rebecchi F. Random-
ized clinical trial of robot-assisted versus laparoscopic Nissen fundo-
plication. Br J Surg 2006;93:553–8.
57 Muller-Stich BP, Reiter MA, Wente MN, Bintintan VV, Koninger J,
Buchler MW, et al. Robot-assisted versus conventional laparoscopic
fundoplication: short-term outcome of a pilot randomized controlled
trial. Surg Endosc 2007;21:1800–5.
58 Nakadi IE, Melot C, Closset J, DeMoor V, Betroune K, Feron P, et al.
Evaluation of da Vinci Nissen fundoplication clinical results and cost
minimization. World J Surg 2006;30:1050–4.
59 Wykypiel H, Bodner J, Wetscher G, Schmid T. Robot-assisted versus
conventional laparoscopic fundoplication: short-term outcome of
a pilot randomized controlled study. Surg Endosc 2008;22:1407.
60 Marescaux J, Smith MK, Folscher D, Jamali F, Malassagne B, Leroy J.
Telerobotic laparoscopic cholecystectomy: initial clinical experience
with 25 patients. Ann Surg 2001;234:1–7.
61 Nio D, Bemelman WA, Busch OR, Vrouenraets BC, Gouma DJ. Robot-
assisted laparoscopic cholecystectomy versus conventional laparo-
scopic cholecystectomy: a comparative study. Surg Endosc 2004;18:
379–82.
62 Zhou HX, Guo YH, Yu XF, Bao SY, Liu JL, Zhang Y, et al. Zeus robot-
assisted laparoscopic cholecystectomy in comparison with conven-
tional laparoscopic cholecystectomy. Hepatobiliary Pancreat Dis Int
2006;5:115–18.
63 Bodner J, Hoeller E, Wykypiel H, Klingler P, Schmid T. Long-term
follow-up after robotic cholecystectomy. Am Surg 2005;71:281–5.
64 Breitenstein S, Nocito A, Puhan M, Held U, Weber M, Clavien PA.
Robotic-assisted versus laparoscopic cholecystectomy: outcome and cost
analyses of a case-matched control study. Ann Surg 2008;247:987–93.
65 Langer D, Pudil J, Ryska M. [Robotic laparoscopic cholecystectomy].
Rozhl Chir 2006;85:450–4.
66 Vidovszky TJ, Smith W, Ghosh J, Ali MR. Robotic cholecystectomy:
learning curve, advantages, and limitations. J Surg Res 2006;136:
172–8.
67 Gurusamy KS, Samraj K, Davidsaon BR. Robot assistant for laparo-
scopic cholecystectomy (protocol). Cochrane Database Syst Rev 2008;
Art. No.: CD006578:DOI: 10.1002/14651858.CD006578.
68 Folliguet T, Vanhuyse F, Constantino X, Realli M, Laborde F. Mitral
valve repair robotic versus sternotomy. Eur J Cardiothorac Surg
2006;29:362–6.
69 Nifong LW, Chitwood WR, Pappas PS, Smith CR, Argenziano M,
Starnes VA, et al. Robotic mitral valve surgery: a United States mul-
ticenter trial. J Thorac Cardiovasc Surg 2005;129:1395–404.
70 Rodriguez E, Chitwood WR. Outcomes in robotic cardiac surgery.
J Robotic Surg 2008;1:19–23.
71 Anderson CA, Kypson AP, Chitwood WR Jr. Robotic mitral surgery:
current and future roles. Curr Opin Cardiol 2008;23:117–20.
72 Diks J, Nio D, Jongkind V, Cuesta MA, Rauwerda JA, Wisselink W.
Robot-assisted laparoscopic surgery of the infrarenal aorta: the early
learning curve. Surg Endosc 2007;21:1760–3.
73 Stadler P, Matous P, Vitasek P, Spacek M. Robot-assisted aortoiliac
reconstruction: a review of 30 cases. J Vasc Surg 2006;44:915–19.
74 Anderberg M, Kockum CC, Arnbjornsson E. Robotic fundoplication in
children. Pediatr Surg Int 2007;23:123–7.
75 Meehan JJ, Sandler A. Pediatric robotic surgery: a single-institutional
review of the first 100 consecutive cases. Surg Endosc 2008;22:177–82.
76 Woo R, Le D, Krummel TM, Albanese C. Robot-assisted pediatric
surgery. Am J Surg 2004;188:27S–37S.
77 Sinha CK, Haddad M. Robot-assisted surgery in children: current sta-
tus. J Robotic Surg 2008;1:233–6.
78 McLeod IK, Melder PC. Da Vinci robot-assisted excision of a vallecular
cyst: a case report. Ear Nose Throat J 2005;84:170–2.
79 Tanna N, Joshi AS, Glade RS, Zalkind D, Sadeghi N. Da Vinci robot-
assisted endocrine surgery: novel applications in otolaryngology. Oto-
laryngol Head Neck Surg 2006;135:633–5.
80 Karas CS, Chiocca EA. Neurosurgical robotics: a review of brain and
spine applications. J Robotic Surg 2008;1:39–43.
81 Goto T, Hongo K, Kakizawa Y, Muraoka H, Miyairi Y, Tanaka Y, et al.
Clinical application of robotic telemanipulation system in neurosur-
gery. Case report. J Neurosurg 2003;99:1082–4.
82 Nathoo N, Cavusxoglu MC, VogelbaumMA, Barnett GH. In touch with
robotics: neurosurgery for the future. Neurosurgery 2005;56:421–33.
83 Zimmermann M, Krishnan R, Raabe A, Seifert V. Robot-assisted navi-
gated endoscopic ventriculostomy: implementation of a new technol-
ogy and first clinical results. Acta Neurochir (Wien) 2004;146:697–704.
84 Bargar WL. Robots in orthopaedic surgery: past, present, and future.
Clin Orthop Relat Res 2007;463:31–6.
85 Falcone T, Goldberg JM, Margossian H, Stevens L. Robotic-assisted
laparoscopic microsurgical tubal anastomosis: a human pilot study.
Fertil Steril 2000;73:1040–2.
86 Goldberg JM, Falcone T. Laparoscopic microsurgical tubal anastomo-
sis with and without robotic assistance. Hum Reprod 2003;18:145–7.
87 Rodgers AK, Goldberg JM, Hammel JP, Falcone T. Tubal anastomosis
by robotic compared with outpatient minilaparotomy. Obstet Gyne-
col 2007;109:1375–80.
88 Degueldre M, Vandromme J, Huong PT, Cadiere GB. Robotically assis-
ted laparoscopic microsurgical tubal reanastomosis: a feasibility study.
Fertil Steril 2000;74:1020–3.
89 Cadiere GB, Himpens J, Germay O, Izizaw R, Degueldre M,
Vandromme J, et al. Feasibility of robotic laparoscopic surgery: 146
cases. World J Surg 2001;25:1467–77.
90 Mais V, Ajossa S, Guerriero S, Mascia M, Solla E, Melis GB. Laparo-
scopic versus abdominal myomectomy: a prospective, randomized
trial to evaluate benefits in early outcome. Am J Obstet Gynecol
1996;174:654–8.
91 Seracchioli R, Rossi S, Govoni F, Rossi E, Venturoli S, Bulletti C, et al.
Fertility and obstetric outcome after laparoscopic myomectomy of
large myomata: a randomized comparison with abdominal myomec-
tomy. Hum Reprod 2000;15:2663–8.
92 Advincula AP, Song A, Burke W, Reynolds RK. Preliminary experience
with robot-assisted laparoscopic myomectomy. J Am Assoc Gynecol
Laparosc 2004;11:511–18.
93 Advincula AP, Xu X, Goudeau S IV, Ransom SB. Robot-assisted lapa-
roscopic myomectomy versus abdominal myomectomy: a comparison
of short-term surgical outcomes and immediate costs. J Minim Inva-
sive Gynecol 2007;14:698–705.
Schreuder, Verheijen
210 ª 2008 The Authors Journal compilation ª RCOG 2008 BJOG An International Journal of Obstetrics and Gynaecology

94 Senapati S, Advincula AP. Surgical techniques: robot-assisted laparo-
scopic myomectomy with the da Vinci� surgical system. J Robotic
Surg 2007;1:69–74.
95 Mao SP, Lai HC, Chang FW, Yu MH, Chang CC. Laparoscopy-assisted
robotic myomectomy using the da Vinci system. Taiwan J Obstet
Gynecol 2007;46:174–6.
96 Sroga J, Patel SD. Robotic applications in reproductive endocrinology
and infertility. J Robotic Surg 2008;2:3–10.
97 Nezhat C, Lavie O, Hsu S, Watson J, Barnett O, Lemyre M. Robotic-
assisted laparoscopic myomectomy compared with standard laparo-
scopic myomectomy-a retrospective matched control study. Fertil
Steril;18:2008.
98 Diaz-Arrastia C, Jurnalov C, Gomez G, Townsend C Jr. Laparoscopic
hysterectomy using a computer-enhanced surgical robot. Surg Endosc
2002;16:1271–3.
99 Beste TM, Nelson KH, Daucher JA. Total laparoscopic hysterectomy
utilizing a robotic surgical system. JSLS 2005;9:13–15.
100 Marchal F, Rauch P, Vandromme J, Laurent I, Lobontiu A, Ahcel B,
et al. Telerobotic-assisted laparoscopic hysterectomy for benign and
oncologic pathologies: initial clinical experience with 30 patients.
Surg Endosc 2005;19:826–31.
101 Fiorentino RP, Zepeda MA, Goldstein BH, John CR, Rettenmaier MA.
Pilot study assessing robotic laparoscopic hysterectomy and patient
outcomes. J Minim Invasive Gynecol 2006;13:60–3.
102 Reynolds RK, Advincula AP. Robot-assisted laparoscopic hyster-
ectomy: technique and initial experience. Am J Surg 2006;191:
555–60.
103 Advincula AP. Surgical techniques: robot-assisted laparoscopic hyster-
ectomy with the da Vinci surgical system. Int J Med Robot 2006;2:
305–11.
104 Advincula AP, Reynolds RK. The use of robot-assisted laparoscopic
hysterectomy in the patient with a scarred or obliterated anterior
cul-de-sac. JSLS 2005;9:287–91.
105 Nezhat C, Saberi NS, Shahmohamady B, Nezhat F. Robotic-assisted
laparoscopy in gynecological surgery. JSLS 2006;10:317–20.
106 Kho RM, Hilger WS, Hentz JG, Magtibay PM, Magrina JF. Robotic
hysterectomy: technique and initial outcomes. Am J Obstet Gynecol
2007;197:113–14.
107 Payne TN, Dauterive FR. A comparison of total laparoscopic hyster-
ectomy to robotically assisted hysterectomy: surgical outcomes in
a community practice. J Minim Invasive Gynecol 2008;15:286–91.
108 Molpus KL, Wedergren JS, Carlson MA. Robotically assisted endo-
scopic ovarian transposition. JSLS 2003;7:59–62.
109 Barmat L, Glaser G, Davis G, Craparo F. Da Vinci-assisted abdominal
cerclage. Fertil Steril 2007;88:1437–3.
110 Melamud O, Eichel L, Turbow B, Shanberg A. Laparoscopic vesicovagi-
nal fistula repair with robotic reconstruction. Urology 2005;65:163–6.
111 Schimpf MO, Morgenstern JH, Tulikangas PK, Wagner JR. Vesicova-
ginal fistula repair without intentional cystotomy using the laparo-
scopic robotic approach: a case report. JSLS 2007;11:378–80.
112 Sundaram BM, Kalidasan G, Hemal AK. Robotic repair of vesicovagi-
nal fistula: case series of five patients. Urology 2006;67:970–3.
113 Di Marco DS, Chow GK, Gettman MT, Elliott DS. Robotic-assisted
laparoscopic sacrocolpopexy for treatment of vaginal vault prolapse.
Urology 2004;63:373–6.
114 Elliott DS, Frank I, Dimarco DS, Chow GK. Gynecologic use of roboti-
cally assisted laparoscopy: Sacrocolpopexy for the treatment of high-
grade vaginal vault prolapse. Am J Surg 2004;188 (4A Suppl):52S–6S.
115 Elliott DS, Chow GK, Gettman M. Current status of robotics in female
urology and gynecology. World J Urol 2006;24:188–92.
116 Elliott DS, Krambeck AE, Chow GK. Long-term results of robotic
assisted laparoscopic sacrocolpopexy for the treatment of high grade
vaginal vault prolapse. J Urol 2006;176:655–9.
117 Ayav A, Bresler L, Hubert J, Brunaud L, Boissel P. Robotic-assisted
pelvic organ prolapse surgery. Surg Endosc 2005;19:1200–3.
118 Draaisma WA, Nieuwenhuis DH, Janssen LWM, Broeders IAMJ.
Robot-assisted laparoscopic rectovaginopexy for rectal prolapse:
a prospective cohort study on feasibility and safety. J Robotic Surg
2008;1:273–7.
119 Moreno Sierra J, Galante Romo I, Ortiz Oshiro E, Nunez Mora C,
Silmi Moyano A. [Robotic assisted laparoscopic colposacropexy in
the treatment of pelvic organ prolapse]. Arch Esp Urol 2007;60:481–8.
120 Munz Y, Moorthy K, Kudchadkar R, Hernandez JD, Martin S, Darzi A,
et al. Robotic assisted rectopexy. Am J Surg 2004;187:88–92.
121 Decloedt J, Vergote I. Laparoscopy in gynaecologic oncology:
a review. Crit Rev Oncol Hematol 1999;31:15–26.
122 Reynolds RK, Burke WM, Advincula AP. Preliminary experience with
robot-assisted laparoscopic staging of gynecologic malignancies. JSLS
2005;9:149–58.
123 Field JB, Benoit MF, Dinh TA, Diaz-Arrastia C. Computer-enhanced
robotic surgery in gynecologic oncology. Surg Endosc 2007;21:244–6.
124 Boggess JF. Robotic surgery in gynecologic oncology: evolution of
a new surgical paradigm. J Robotic Surg 2007;1:31–7.
125 Seamon LG, Cohn DE, Valmadre S, Richardson DL, Jayjohn LA, Jenson C,
et al. Robotic hysterectomy and lymphadenectomy for endometrial can-
cer: technical aspects and details of success – the Ohio State University
method. J Robotic Surg 2008;2:71–6.
126 Veljovich DS, Paley PJ, Dreschner CW, Everett EN, Shah C, Peters WA.
Robotic surgery in gynecologic oncology: program initiation and
outcomes after the first year with comparison with laparotomy for
endometrial cancer staging. Am J Obstet Gynecol 2008;198:
679.e1–679.e10.
127 Vergote I, Pouseele B, Van Gorp T, Vanacker B, Leunen K, Cadron I,
et al. Robotic retroperitoneal lower para-aortic lymphadenectomy in
cervical carcinoma: first report on the technique used in 5 patients.
Acta Obstet Gynecol Scand 2008;87:783–7.
128 Sert BM, Abeler VM. Robotic-assisted laparoscopic radical hysterec-
tomy (Piver type III) with pelvic node dissection–case report. Eur J
Gynaecol Oncol 2006;27:531–3.
129 Sert B, Abeler V. Robotic radical hysterectomy in early-stage cervical
carcinoma patients, comparing results with total laparoscopic radical
hysterectomy cases. The future is now? Int J Med Robot 2007;3:
224–8.
130 Magrina JF, Kho RM, Weaver AL, Montero RP, Magtibay PM. Robotic
radical hysterectomy: comparison with laparoscopy and laparotomy.
Gynecol Oncol 2008;109:86–91.
131 Kim YT, Kim SW, Hyung WJ, Lee SJ, Nam EJ, Lee WJ. Robotic radical
hysterectomy with pelvic lymphadenectomy for cervical carcinoma:
a pilot study. Gynecol Oncol 2008;108:312–16.
132 Kowalski L, Falkner CA, Wishnev SA. Robotic versus abdominal rad-
ical hysterectomy for gynaecological cancer.Gynecol Oncol 2008;108
(Suppl Abstract 141):S32–S155.
133 Fanning J, Fenton B, Purohit M. Robot radical hysterectomy. Am J
Obstet Gynecol 2008;198:649.e1–649.e4.
134 Danic MJ, Chow M, Alexander G, Bhandari A, Menon M, Brown M.
Anesthesia considerations for robotic-assisted laparoscopic prostatec-
tomy: a review of 1,500 cases. J Robotic Surg 2008;1:119–23.
135 Meininger D, Byhahn C, Mierdl S, Westphal K, Zwissler B. Positive
end-expiratory pressure improves arterial oxygenation during pro-
longed pneumoperitoneum. Acta Anaesthesiol Scand 2005;49:
778–83.
136 Baltayian S. A brief review: anesthesia for robotic prostatectomy.
J Robotic Surg 2008;2:59–61.
137 Prewitt R, Bochkarev V, McBride CL, Kinny S, Oleynikov D. The pat-
terns and costs of the Da Vinci robotic surgery system in a large
academic institution. J Robotic Surg 2008;2:17–20.
Robotic surgery (efficacy, costs and training)
ª 2008 The Authors Journal compilation ª RCOG 2008 BJOG An International Journal of Obstetrics and Gynaecology 211

138 Heemskerk J, de Hoog DE, van Gemert WG, Baeten CG, Greve JW,
Bouvy ND. Robot-assisted vs. conventional laparoscopic rectopexy for
rectal prolapse: a comparative study on costs and time. Dis Colon
Rectum 2007;50:1825–30.
139 Heemskerk J, van Dam R, van Gemert WG, Beets GL, Greve JW,
Jacobs MJ, et al. First results after introduction of the four-armed
da Vinci Surgical System in fully robotic laparoscopic cholecystectomy.
Dig Surg 2005;22:426–31.
140 Heemskerk J, van Gemert WG, de Vries J, Greve J, Bouvy ND. Learn-
ing curves of robot-assisted laparoscopic surgery compared with con-
ventional laparoscopic surgery: an experimental study evaluating skill
acquisition of robot-assisted laparoscopic tasks compared with con-
ventional laparoscopic tasks in inexperienced users. Surg Laparosc
Endosc Percutan Tech 2007;17:171–4.
141 Morgan JA, Thornton BA, Peacock JC, Hollingsworth KW, Smith CR,
Oz MC, et al. Does robotic technology make minimally invasive car-
diac surgery too expensive? A hospital cost analysis of robotic and
conventional techniques. J Card Surg 2005;20:246–51.
142 Burgess SV, Atug F, Castle EP, Davis R, Thomas R. Cost analysis of
radical retropubic, perineal, and robotic prostatectomy. J Endourol
2006;20:827–30.
143 Joseph JV, Leonhart A, Patel HRH. The cost of radical prostatectomy:
retrospective comparison of open, laparoscopic, and robot-assisted
approaches. J Robotic Surg 2008;2:21–4.
144 Scales CD Jr, Jones PJ, Eisenstein EL, Preminger GM, Albala DM. Local
cost structures and the economics of robot assisted radical prostatec-
tomy. J Urol 2005;174:2323–9.
145 Bhayani SB, Link RE, Varkarakis JM, Kavoussi LR. Complete daVinci
versus laparoscopic pyeloplasty: cost analysis. J Endourol 2005;19:
327–32.
146 Steinberg PL, Merguerian PA, Bihrle W III, Heaney JA, Seigne JD. A da
Vinci robot system can make sense for a mature laparoscopic prosta-
tectomy program. JSLS 2008;12:9–12.
147 Steinberg PL, Merguerian PA, Bihrle IW, Seigne JD. The cost of learn-
ing robotic-assisted prostatectomy. Urology 2008;72:1068–72.
148 Munz Y, Kumar BD, Moorthy K, Bann S, Darzi A. Laparoscopic virtual
reality and box trainers: is one superior to the other? Surg Endosc
2004;18:485–94.
149 Blavier A, Gaudissart Q, Cadiere GB, Nyssen AS. Impact of 2D and 3D
vision on performance of novice subjects using da Vinci robotic sys-
tem. Acta Chir Belg 2006;106:662–4.
150 Blavier A, Gaudissart Q, Cadiere GB, Nyssen AS. Perceptual and
instrumental impacts of robotic laparoscopy on surgical performance.
Surg Endosc 2007;21:1875–82.
151 Hubens G, Coveliers H, Balliu L, Ruppert M, Vaneerdeweg W. A per-
formance study comparing manual and robotically assisted laparo-
scopic surgery using the da Vinci system. Surg Endosc 2003;17:
1595–9.
152 Vlaovic PD, Sargent ER, Boker JR, Corica FA, Chou DS, Abdelshehid
CS, et al. Immediate impact of an intensive one-week laparoscopy
training program on laparoscopic skills among postgraduate urolo-
gists. JSLS 2008;12:1–8.
153 Blaschko SD, Brooks HM, Dhuy SM, Charest-Shell C, Clayman RV,
McDougall EM. Coordinated multiple cadaver use for minimally inva-
sive surgical training. JSLS 2007;11:403–7.
154 Marecik SJ, Chaudhry V, Jan A, Pearl RK, Park JJ, Prasad LM.
A comparison of robotic, laparoscopic, and hand-sewn intestinal
sutured anastomoses performed by residents. Am J Surg 2007;193:
349–55.
155 Mehrabi A, Yetimoglu CL, Nickkholgh A, Kashfi A, Kienle P,
Konstantinides L, et al. Development and evaluation of a training
module for the clinical introduction of the da Vinci robotic system
in visceral and vascular surgery. Surg Endosc 2006;20:1376–82.
156 Albani JM, Lee DI. Virtual reality-assisted robotic surgery simulation.
J Endourol 2007;21:285–7.
157 Mimic Technologies, Inc. [www.mimic.ws]. Accessed 16 June 2008.
158 Lendvay TS, Casale P, Sweet R, Peters C. VR robotic surgery: random-
ized blinded study of the dV-Trainer robotic simulator. Stud Health
Technol Inform 2008;132:242–4.
159 Lendvay TS, Casale P, Sweet R, Peters C. Initial validation of a virtual-
reality robotic simulator. J Robotic Surg 2008;2:145–9.
160 SimSurgery AG. [www.simsurgery.com]. Accessed 16 June 2008.
161 HalvorsenFH,ElleOJ,DalininVV,MørkBE,SørhusV,Røtnes JS,etal. Virtual
reality simulator training equals mechanical robotic training in improving
robot-assisted basic suturing skills. Surg Endosc 2006;20:1565–9.
162 Katsavelis D, Siu KC, Brown-Clerk B, Lee IH, Lee YK, Oleynikov D,
et al. Validated robotic laparoscopic surgical training in a virtual-reality
environment. Surg Endosc 2008.
163 Brown-Clerk B, Siu KC, Katsavelis D, Lee I, Oleynikov D, Stergiou N.
Validating advanced robot-assisted laparoscopic training task in vir-
tual reality. Stud Health Technol Inform 2008;132:45–9.
164 Sun LW, Van Meer F, Schmid J, Bailly Y, Thakre AA, Yeung CK.
Advanced da Vinci Surgical System simulator for surgeon training
and operation planning. Int J Med Robot 2007;3:245–51.
165 Fiedler MJ, Chen SJ, Judkins TN, Oleynikov D, Stergiou N. Virtual
reality for robotic laparoscopic surgical training. Stud Health Technol
Inform 2007;125:127–9.
166 Shane MD, Pettitt BJ, Morgenthal CB, Smith CD. Should surgical
novices trade their retractors for joysticks? Videogame experience
decreases the time needed to acquire surgical skills. Surg Endosc
2007;22:1294–7.
167 Harper JD, Kaiser S, Ebrahimi K, Lamberton GR, Hadley HR, Ruckle
HC, et al. Prior video game exposure does not enhance robotic sur-
gical performance. J Endourol 2007;21:1207–10.
168 Hanly EJ, Miller BE, Kumar R, Hasser CJ, Coste-Maniere E, Talamini MA,
et al. Mentoring console improves collaboration and teaching
in surgical robotics. J Laparoendosc Adv Surg Tech A 2006;16:445–51.
169 Judkins TN, Oleynikov D, Stergiou N. Enhanced robotic surgical train-
ing using augmented visual feedback. Surg Innov 2008;15:59–68.
170 Ali MR, Loggins JP, Fuller WD, Miller BE, Hasser CJ, Yellowlees P, et al.
3-D telestration: a teaching tool for robotic surgery. J Laparoendosc
Adv Surg Tech A 2008;18:107–12.
171 Training Centres, Intuitive Surgical. [www.intuitivesurgical.com].
Accessed 16 June 2008.
172 Chitwood WR Jr, Nifong LW, Chapman WH, Felger JE, Bailey BM,
Ballint T, et al. Robotic surgical training in an academic institution.
Ann Surg 2001;234:475–84.
173 Donias HW, Karamanoukian RL, Glick PL, Bergsland J, Karamanoukian
HL. Survey of resident training in robotic surgery. Am Surg 2002;68:
177–81.
174 Patel YR, Donias HW, Boyd DW, Pande RU, Amodeo JL, Karamanoukian
RL, et al. Are you ready to become a robo-surgeon? Am Surg 2003;69:
599–603.
175 Guru KA, Kuvshinoff BW, Pavlov-Shapiro S, Bienko MB, Aftab MN,
Brady WE, et al. Impact of robotics and laparoscopy on surgical skills:
a comparative study. J Am Coll Surg 2007;204:96–101.
176 Rashid HH, Leung YY, Rashid MJ, Oleyourryk G, Valvo JR, Eichel L.
Robotic surgical education: a systematic approach to training urology
residents to perform robotic-assisted laparoscopic radical prostatec-
tomy. Urology 2006;68:75–9.
177 Thiel DD, Francis P, Heckman MG, Winfield HN. Prospective evalua-
tion of factors affecting operating time in a residency/fellowship
training program incorporating robot-assisted laparoscopic prosta-
tectomy. J Endourol 2008;22:1331–8.
178 Schroeck FR, de Sousa CA, Kalman RA, Kalia MS, Pierre SA, Haleblian
GE, et al. Trainees do not negatively impact the institutional learning
Schreuder, Verheijen
212 ª 2008 The Authors Journal compilation ª RCOG 2008 BJOG An International Journal of Obstetrics and Gynaecology

curve for robotic prostatectomy as characterized by operative time,
estimated blood loss, and positive surgical margin rate. Urology 2008;
71:597–601.
179 Ramsay CR, Grant AM, Wallace SA, Garthwaite PH, Monk AF,
Russell IT. Assessment of the learning curve in health technologies. A
systematic review. Int J Technol Assess Health Care 2000;16:1095–108.
180 Yohannes P, Rotariu P, Pinto P, Smith AD, Lee BR. Comparison of
robotic versus laparoscopic skills: is there a difference in the learning
curve? Urology 2002;60:39–45.
181 Blavier A, Gaudissart Q, Cadiere GB, Nyssen AS. Comparison of learn-
ing curves and skill transfer between classical and robotic laparoscopy
according to the viewing conditions: implications for training. Am J
Surg 2007;194:115–21.
182 DiLorenzo N, Coscarella G, Faraci L, Konopacki D, Pietrantuono M,
Gaspari AL. Robotic systems and surgical education. JSLS 2005;9:3–12.
183 Martin JA, Regehr G, Reznick R, MacRae H, Murnaghan J, Hutchison C,
et al. Objective structured assessment of technical skill (OSATS) for
surgical residents. Br J Surg 1997;84:273–8.
184 Hernandez JD, Bann SD, Munz Y, Moorthy K, Datta V, Martin S, et al.
Qualitative and quantitative analysis of the learning curve of a simulated
surgical task on the da Vinci system. Surg Endosc 2004;18:372–8.
185 Narazaki K, Oleynikov D, Stergiou N. Robotic surgery training and
performance: identifying objective variables for quantifying the
extent of proficiency. Surg Endosc 2006;20:96–103.
186 Narula VK, Watson WC, Davis SS, Hinshaw K, Needleman BJ, Mikami
DJ, et al. A computerized analysis of robotic versus laparoscopic task
performance. Surg Endosc 2007;21:2258–61.
187 Tavakol M, Mohagheghi MA, Dennick R. Assessing the skills of surgi-
cal residents using simulation. J Surg Educ 2008;65:77–83.
188 Herrell SD, Smith JA Jr. Robotic-assisted laparoscopic prostatectomy:
what is the learning curve? Urology 2005;66:105–7.
189 Artibani W, Fracalanza S, Cavalleri S, Iafrate M, Aragona M, Novara
G, et al. Learning curve and preliminary experience with da Vinci-
assisted laparoscopic radical prostatectomy. Urol Int 2008;80:
237–44.
190 Zorn KC, Orvieto MA, Gong EM, Mikhail AA, Gofrit ON, Zagaja GP,
et al. Robotic radical prostatectomy learning curve of a fellowship-
trained laparoscopic surgeon. J Endourol 2007;21:441–7.
191 Steers WD. Tips on establishing a robotics program in an academic
setting. ScientificWorldJournal 2006;6:2531–41.
192 Palmer KJ, Lowe GJ, Coughlin GD, Patil N, Patel VR. Launching a suc-
cessful robotic surgery program. J Endourol 2008;22:819–824.
193 Patel VR. Essential elements to the establishment and design of a
successful robotic surgery programme. Int J Med Robot 2006;2:
28–35.
194 Dickens BM, Cook RJ. Legal and ethical issues in telemedicine and
robotics. Int J Gynaecol Obstet 2006;94:73–8.
195 Andonian S, Okeke Z, Okeke DA, Rastinehad A, Vanderbrink BA,
Richstone L, et al. Device failures associated with patient injuries
during robot-assisted laparoscopic surgeries: a comprehensive review
of FDA MAUDE database. Can J Urol 2008;15:3912–16.
196 Valvo JR, Madeb R, Gilbert R, Nicholson C, Oleyoeryk G, Perrapato S,
et al. Policy guidelines suggested for robot-assisted prostatectomy.
J Robotic Surg 2007;1:173–6.
197 Herron DM, Marohn M. A consensus document on robotic surgery.
Surg Endosc 2008;22:313–25.
198 World Medical Assocation Statement On The Ethics Of Telemedicine.
October 2007 [www.wma.net/e/policy/t3.htm]. Accessed 20 June
2008.
199 Berlinger NT. Robotic surgery–squeezing into tight places. N Engl J
Med 2006;354:2099–101.
200 Gassert R, Burdet E, Chinzei K. MRI-compatible robotics. IEEE Eng
Med Biol Mag 2008;27:12–14.
201 Sutherland GR, Latour I, Greer AD, Fielding T, Feil G, Newhook P. An
image-guided magnetic resonance-compatible surgical robot. Neuro-
surgery 2008;62:286–92.
202 Hashizume M. MRI-guided laparoscopic and robotic surgery for
malignancies. Int J Clin Oncol 2007;12:94–8.
203 Melzer A, Gutmann B, Remmele T, Wolf R, Lukoscheck A, Bock M,
et al. INNOMOTION for percutaneous image-guided interventions:
principles and evaluation of this MR- and CT-compatible robotic sys-
tem. IEEE Eng Med Biol Mag 2008;27:66–73.
204 Marescaux J, Leroy J, Gagner M, Rubino F, Mutter D, Vix M, et al.
Transatlantic robot-assisted telesurgery. Nature 2001;413:379–80.
205 NASA Prepares for Space Exploration in Undersea Lab. [www.nasa.
gov/home/hqnews/2006/mar/HQ_06109_NEEMO_9.html]. Accessed
20 June 2008.
206 Anvari M. Telesurgery: remote knowledge translation in clinical sur-
gery. World J Surg 2007;31:1545–50.
207 Rentschler ME, Platt SR, Berg K, Dumpert J, Oleynikov D, Farritor SM.
Miniature in vivo robots for remote and harsh environments. IEEE
Trans Inf Technol Biomed 2008;12:66–75.
208 NASA project: The RAMS Arms. [www-robotics.jpl.nasa.gov/systems/
system]. Accessed 20 June 2008.
209 Sahin E, Winfield A. Special Issue: Swarm Robotics. Swarm Intelli-
gence 2008;2:69–72.
210 Dasgupta P. Robotics in urology. Int J Med Robot 2008;4:1–2.
211 Advincula AP. 2007 World Robotic Gyn Symposium: the dawn of
a new age in minimally invasive gynecologic surgery. J Robotic Surg
2008;1:177–8.
Robotic surgery (efficacy, costs and training)
ª 2008 The Authors Journal compilation ª RCOG 2008 BJOG An International Journal of Obstetrics and Gynaecology 213



























